Embed Size (px)
Citation preview

Naguib Hilmy GPSI Milton Keynes
John Parnell Manager Health:MK

ONS (2001); Cowie MR et al (2000) Heart 83: 505-510
www.heartstats.org
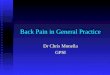
One-year survival rates, heart failure and major cancers compared,
mid-1990's, England and Wales
0 10 20 30 40 50 60 70 80 90 100
Cancer of the pancreas
Lung cancer
Cancer of the oesophagus
Stomach cancer
Leukaemia
Cancer of the kidney
Ovarian cancer
Heart failure
Colon cancer
Non-Hodgkins lymphoma
Cancer of the lip, mouth and pharynx
Prostate cancer
Bladder cancer
Cancer of the uterus
Breast cancer
Melanoma of skin
One year survival rate (%)




Ellis C et al (2001) Health Statistics Quarterly 11: 17-24
www.heartstats.org
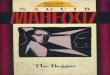
Prevalence of heart failure by age and sex, most deprived and least deprived areas compared, 1998, England and Wales
0
50
100
150
200
250
45-54 55-64 65-74 75-84 85 and over Total
Age group
Pre
vale
nce
per 1
,000
pop
ulat
ion
Most deprived (Q5)
Least deprived (Q1)

“Health: MK” is a practice based commissioning collaborative with 26 member practices and serving a population of >245,000 (total MK population >250,000).

MK Community cardiac service2 GPSIs, Admin, HCAs & Practice nurses
GPSI in North MK Dr Mahendran MKPCT CHD Lead
Support from MK NHS trust Cardiology Dr David Gwilt . Dr Attila Kardos

GP Referral Form MK Community Cardiac service
Signed by GP Print Name………………………………………………. Date ……………………………………
Please complete and return to: Dr Naguib Hilmy Whaddon House Surgery, 221 Whaddon Way, Bletchley, MK3 7EA 01908 272700 Fax01908 630076
Patient Details Patient Name ………………………………..Miss/Mrs/Ms/Mr NHS Number …………………………………. Address ……………………………………………………. Special Needs……………………………....... ………………………………………………………………. Date of Birth …………………………………… Post Code …………………………………… Tel no. …………………………………………. Mobile……………………………………………
GP Details [Stamp] GP Name …………………………………….. Tel no. ……………………….. Address ………………………………………. Fax no. ……………………….
Reasons for referral (Please be specific) Test&report only/ Test & advice Past Cardiac History: Hypertension MI Angioplasty/CABG AF Past Medical History: Diabetes Asthma Allergies COPD Medication:
Investigations Date Result Not Available
ECG
Hb
Sugar
Lipids TFTs

CCS workflow 2008
Paper, Fax , C&B
Cardiology OP Community Cardiac
Rehabilitation G.Ps
Triage by Admin & GPSI PCT
Database Red Book
Referral data entered on vision
Patient booked into clinic by telephone
Batch of letters passed to Admin for record keeping
Confirmation of appointment letter to patient + Information leaflets
HCA : ECG +Monitor / BNP Patient attends clinic, Clinical
assessment, ECG +/ Echocardiogram
Patient phoned to confirm attendance
Monitor /Echo reported & Summary letter to GP & Patient
Follow-up appointment
required
Patient discharged to care of GP and/or rehab
Referral to secondary care
Letters & Monitors attached to vision, Notes Filed
Clinic schedule produced for GPSI with referral letters/patient info
Reject referrals Phoned back/ Fax
to G.P

Patients on database 2558
Sept 08

24 Hour ECGs- Event recorders2008 4002007 3562006 2522005 1362004 49

RegistersHeart Failure Prevalence on 31/3/08
Practice Prevalence vs MKPCT and National Average
0.0%
0.1%
0.2%
0.3%
0.4%
0.5%
0.6%
0.7%
0.8%
0.9%
1.0%
Wal
nut T
ree
Wes
tcro
ft
MK
Vill
age
Wat
ling
Val
e
Fish
erm
ead
CM
K
Dra
yton
Roa
d
Pur
beck
MC
Wes
tfiel
d R
oad
Ash
field
Kin
gfis
her
Sov
erei
gn M
C
Nea
th H
ill
Sto
nede
an
Sta
nton
bury
HC
Wol
verto
n
Hill
tops
Sto
ny S
tratfo
rd
Will
en V
illag
e
Wat
er E
aton
The
Gro
ve
NP
MC
Cob
bs G
arde
n
Bed
ford
Stre
et
Wha
ddon
Hou
se
Par
ksid
e
Red
Hou
se
Practice Prevalence
National Prevalence
MKPCT Prevalence

North Central London sector-wide Heart failure QOF data National estimated prevalence: 2.3%National recorded prevalence: 1.8%

Heart Failure 2 (Echo)

Heart Failure 3 -ACEI


AuditPCT is providing help to practices to look at
their registers.
We have trialled a series of data audits and actions to pick-up missing and lost patients from the Heart Failure Registers. In both trial practices patients have been added to the registers.
The audits are being rolled out, either to be done by the practice or by PCT Heart Failure Nurse facilitator

RegistersChange in 2007 from implicit coding to
explicit, GPs or CHD nurse involvement now needed.
OPD letters rarely stated Heart Failure as a diagnosis.
Registration is geared to providing therapeutic management.

SupportThe process involves checking and advising
summarisers of the read code issues, and identify any learning issues for incorporation into training.
Heart Failure discussed with practice’s CHD nurse to ensure HF patients are seen. In this process we will also identify any training needs.
Updated Heart Failure Manual is being produced.

Heart Failure Rehabilitation ServiceA new service will start in May 2009 (probably)
which will provide exercise and psychological support for patients with a new diagnosis of Heart Failure.
Direct referral from GPs, Practice Nurses and MKFT.
Direct referral from HF Rehab to Community Cardiology Services.
With a pathway to provide long term self-care support.

Experience from initial searches at pilot practices
Until recently there was no universal definition for Heart Failure and a complicated system of read coding has evolved for QOF.
GMS QOF HF indicators include patients with - LVSD-LVDD
About half of the patients with measurable left ventricular dysfunction in the MONICA and ECHOES studies - had no symptoms.

Echocardiogram Data missing – ejection fractions and
ventricular function status.
For QOF purposes echo code needs to be linked to G58 codes.

Method of Case ReviewLoop Diuretics search (exclusions), problem
lists, medical history, current therapy, echocardiogram results if available.
Some empirical management of patients with symptoms, especially elderly patients.
Healthcare Commission found that nationally, only 33.4% of patients discharged with heart failure were prescribed beta-blockers and issues remain over follow up and titration of medication.

LVD/ Heart Registers Access To diagnostics
Coding
Co-morbidities
Has the patient been given the diagnosis? “Weak Heart “ 'fluid on your lungs - your heart is
not pumping hard enough‘ “a diagnosis of 'heart failure' was rarely
communicated to patients to avoid causing anxiety”

Heart failure services in the UK – in figuresHeart failure services in the UK – in figures
16%16%proportion of GPs who have direct proportion of GPs who have direct access to echocardiography within access to echocardiography within
one monthone month
8%8%proportion of GPs who have access proportion of GPs who have access
through a specialist to through a specialist to echocardiography within one monthechocardiography within one month
22%22% GPs who never prescribe beta-GPs who never prescribe beta-blockersblockers
36% 36% GPs who always prescribe ACE GPs who always prescribe ACE inhibitorsinhibitors
Source: European Heart Journal, early online, 27 May 2008Source: European Heart Journal, early online, 27 May 2008



Heart Failure 1 (READ2)Heart Failure (G58%)Rheumatic Left ventricular failure (G1yz1)NYHA classification –class I (662f)NYHA classification- class II (662g)NYHA classification –class III (662h)NYHA classification- class IV (662i)

Codes not included as heart failureDilated cardiomyopathyIschaemic cadiomyopathyLeft ventricular systolic dysfunctionLeft ventricular diastolic dysfunction

Heart Failure 2 EchocardiographyEcho shows LVSD 585fEcho shows LVDDF
585gU-S heart scan 5853Echo abnormal 58531Echo equivocal 5C20Echo requested 33BDReferral for echo 8HQ7Echo abnormal R1320Ultrasound cardiog
abn R1322
Ref to cardio sp int gp 8H4R
Priv ref to cardiologist 8HVJCardiological referral 8H44Angiocardiography 5531, 5532, 5533,5538 79380, 79382

Should every body with suspected heart failure have an Echocardiogram?
How many?How often?

If investigation is limited to patients with more definite symptoms and signs of heart failure, fewer than 50% of cases will be identified and a large number of patients with mild symptoms will be missed EPICA

EPICAAbnormal ECG 81% sensitivity
Abnormal CXR 57% sensitivty
25% of CHF patients had normal ECG or CXR




Heart failure is most unlikely in a patient with a normal ECG or normal plasma concentration of BNP or NT-proBNP given the high sensitivity of these tests
The sensitivity of BNP may be as high as 90-97% in patients presenting with new symptoms , depending on assay used & cut off point
The sensitivity of ECG is as high as 94%

Tests used to diagnose significant CHD:
Treadmill test: sensitivity of 68%, specificity of 77%
Nuclear test: sensitivity of 81%, specificity of 85-95%
Portable Echo ( LVSD) : sensitivity 96%, specificity 98% NPV 99.6%
PSA for Prostate Cancer >4 sensitivity 70—79 %
specificity 59—90%
one in 8 men with PSA < 4 will have prostate cancer

Predictive ValueBNP (Biosite)
NPV 88.2% at 40pg/ml
Avoid 51 referrals – but miss 6 with LVSD
PPV 55% at 40pg/ml
NT pro-BNP (Roche)
NPV 97.3% at 150pg/ml
Avoid 37 referrals – miss 1 with mild LVSD
PPV 52% at 150pg/ml


What proportion of patients referred for suspected HF have heart failure ?
29 % Cowie 19995-8% in asymptomatic patients ?

Suspected Heart failureSOB , Fatigue, Oedema
Clinical assessment
NT-ProBNP ECG
NormalHeart failure
unlikely
AbnormalEchocardiogram
Murmurs Blackouts: Echo &
monitors

MK Community Cardiac Service Protocol for Heart Failure Diagnosis Patient name: Date: NHS number DOB Symptoms: SOB None(NYHA I) moderate exertion( II) mild exertion( III) At rest (IV) Orthopnea PND Fatigue Leg swelling Syncope Chest pain PMH : Hypertension Diabetes IHD Angina MI CABG Stent AF FH Examination: Pulse : Regular Irregular BP: Murmur: Oedema: Investigations: ECG: Normal Abnormal: old MI LVH LAD LBBB AF NT-Pro BNP: pg/ml Date:
Pasted from <http://www.diavant.com/diavant/CMSFront.html?pgid=1,10006,10006,1> Acute heart failure cut off point > 450 for patients < 50 years old > 900 for patients > 50 years old < 300 excludes acute destabilized heart failure IHD -adverse prognosis if persistent > 250 Cardioembolic stroke > 286 Diabetics -Higher risk > 160 Diastolic Dysfunction > 110 NYHA class I [97.5 pg/mL (77.2–120.6) vs. controls 55.7 pg/mL (32.7–86.3), NYHA class II [177.3 pg/mL (74.1–293.3) vs. 97.5 pg/mL (77.2–120.6), NYHA class III [334.7 pg/mL (180.2–976.8) vs. 177.3 pg/mL (74.1–293.3) In heart failure patients, each 100 pg/ml increase was associated with a 35% increase in the relative risk of death Pasted from <http://www.bmj.com/cgi/content/abstract/330/7492/625?maxtoshow=&HITS=10&hits=10&RESULTFORMAT=&fulltext=diabetes+BNP&searchid=1&FIRSTINDEX=0&resourcetype=HWCIT> Interpretation & Recommendations:
NT-proBNP levels in patients with reduced left ventricular function Median
Normal (n = 1,291)
56 pg/ml
NYHA I (n = 182)
342 pg/ml
NYHA II (n = 250)
951 pg/ml
NYHA III (n = 234)
1,571 pg/ml
NYHA IV (n = 35)
1,707 pg/ml

59 Males 59 Males Average Age 72 yearsAverage Age 72 years 44-97 , 8>85 Years44-97 , 8>85 Years41 Females 41 Females Average age 71 yearsAverage age 71 years 45-92 , 4>85 Years45-92 , 4>85 Years
<60 pg/ml<60 pg/ml Female Female 77<60 pg/ml<60 pg/ml Male Male 141460-300 pg/ml60-300 pg/ml Female Female 191960-300 pg/ml60-300 pg/ml Male Male 2626300-500 pg/ml300-500 pg/ml Female Female 44
300-500 pg/ml 300-500 pg/ml Male Male 22500-1000 pg/ml500-1000 pg/ml Female Female 66500-1000 pg/ml500-1000 pg/ml Male Male 661000-3000 pg/ml1000-3000 pg/ml Female Female 441000-3000 pg/ml1000-3000 pg/ml Male Male 77>3000 pg/ml>3000 pg/ml Female Female 11>3000 pg/ml>3000 pg/ml Male Male 44
First 100 NT-ProBNP( Jan to June 08)

Results of less than 60 pg/ ml 21 patients
Results of less than 100pg/ml 37 patients
Results of less than 150pg/ml 39 patients
Results of less than 200 pg/ ml 54 patients
Results of less than 300 pg/ml 66 patients
Results of 300 to 500 pg/ ml 6 patients Results of 500 to 1000 pg/ ml 12 patients Results over 1000 pg/ml 16 patientsResults over 3000 pg/ml 5 patients

RESULTS
45/100 did not require a new or repeat Echocardiogram.
Heart failure with evidence of LVSD: eight patients.Heart failure due to diastolic dysfunction:
twelve patients.

16 patients with readings >1000 pg/ ml:
8 had LVSD, 3 LVDD, 3 Aortic stenosis, one had urgent AVR1 Significant MR

12 patients with readings between 500 & 1000 pg/ml
4 had diastolic dysfunction1 known heart failure with normal EF,
MV repair & AF

LVSD
EF 50% 388 & 2025 pg/mlEF 40% 1929 & 1468 pg/mlEF 30% 2435 , 2526 & > 3000
pg/mlEF 26% >3000 pg/ml

ECGs:
Normal: 51
Abnormal: 46
Not available: 3

Echos done 54
Normal ( 11 patients) levels (pg/ml): <60 x5, 60, 81, 165, 187, 278, 336
LVSD ( 8 patients ) levels (pg/ml): 388 (AF, EF 50%), 1468, 1929, 2025. 2435,
2526, > 3000 x2

LVDD with or without heart failure (12 patients) levels (pg/ml):
74, 92, 273, 293, 332, 513, 613, 680, 772, 1057, 1239, > 3000

20 patients Other abnormalities
including mitral regurgitation, aortic valve disease, small pericardial effusion, left ventricular hypertrophy etc:

Hospital referrals2 patients were admitted to hospital: one on
diagnosis & one with increasing symptoms
6 patients already attending cardiology
11 patients referred to cardiology: 3 AS, 1 MR, 1 PAF, 1 for pacing

45 Echos were not done or repeated6 were not repeated, One had been undertaken by hospital15 patients : COPD, asthma, chest infection 4 patients : advanced cancer Massive Ascites due to cirrhosis, panic
attacks, dementia , glitazone oedema

LimitationsThis is not an academic study: no blindingSome of these patients may not have been
referred to cardiology Some patients had previous echosPatients who had Echocardiogram followed
by NT-proBNP were included

Conclusions
NT-pro-BNP near patient testing combined with clinical assessment and ECG by PSI in the community appear to offer a method for prompt risk assessment for patients presenting with suspected heart failure

It helps to triage and prioritise patients that need immediate echocardiography and reassure those who do not require an echocardiogram and differentiate the ones that can have routine echocardiogram
We should continue to listen to our patients and not dismiss the value of careful clinical evaluation

Stage AStage A
At high risk, no At high risk, no structural structural
diseasedisease
Stage BStage B
Structural Structural heart disease, heart disease, asymptomaticasymptomatic
Stage DStage D
Refractory HF Refractory HF requiring requiring
specialized specialized interventionsinterventions
TherapyTherapy•Treat Treat
HypertensionHypertension•Treat lipid Treat lipid
disordersdisorders•Encourage Encourage
regular exerciseregular exercise•Discourage Discourage
alcohol intakealcohol intake•ACE inhibitionACE inhibition
TherapyTherapy•All measures All measures
under stage Aunder stage A•ACE inhibitors ACE inhibitors
in appropriate in appropriate patientspatients
•Beta-blockers in Beta-blockers in appropriate appropriate patientspatients
TherapyTherapy•All measures All measures
under stage Aunder stage A
Drugs:Drugs:•DiureticsDiuretics•ACE inhibitorsACE inhibitors•Beta-blockersBeta-blockers•DigitalisDigitalis•Dietary salt Dietary salt
restrictionrestriction
TherapyTherapy•All measures All measures
under stages under stages A,B, and CA,B, and C
•Mechanical Mechanical assist devicesassist devices
•Heart Heart transplantationtransplantation
•Continuous (not Continuous (not intermittent) IV intermittent) IV inotropic inotropic infusions for infusions for palliationpalliation
•Hospice careHospice care
Stage CStage C
Structural Structural heart disease heart disease
with with prior/current prior/current symptoms of symptoms of
HFHF
Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult, 2001Management of Chronic Heart Failure in the Adult, 2001


Problem solvingHarmful substances: -Smoking, Excess alcohol - Inappropriate type or dosing of B blocker - NSAIDS, Coxibs, Glitazones
Community Matrons, Heart Failure Nurses

http://depts.washington.edu/shfm/app.php?accept
=1&enter=Enter














![[MS-GPSI]: Group Policy: Software Installation Protocol](https://img.pdfslide.net/doc/110x75/617e636eaba150394e69a819/ms-gpsi-group-policy-software-installation-protocol-.jpg)