Embed Size (px)
Citation preview

ALBANY MEDICAL COLLEGE
ALBANY MEDICAL CENTER
OBJECTIVE
BACKGROUND
METHODS
RECONSTRUCTION HARVESTING TECHNIQUE
The nasal cavity floor free mucosal graft showed no increased nasal morbidity. There were no postoperative CSF leaks in our series, despite aggressive tumor resection and manipulation of the diaphragm as demonstrated with 38.6% of intraoperative CSF leak. No lumbar drains or fat graft were used. One month postoperative follow up shows near total or complete mucosalization of the donor site. The free mucosal graft can be easily taken down from the sella and reused in case of revision surgery.
To present an easy and safe technique for sellar region reconstruction with free mucosal graft from the nasal cavity floor including mucosa from the inferior meatus and septum 1. This technique aims to decrease nasal morbidity avoiding the nasoseptal flap for pituitary surgery and keeping the advantage of excellent mucosal coverage of the sellar defect.
CONCLUSIONS
• Prospective study. • 44 consecutive patients with pituitary tumors (41
macroadenomas and 3 microadenomas). • 18 males / 27 females • Average age: 56.9 (16 – 87) / Median: 59 • Postoperative follow-up from 1 to 15 months. • Reconstruction:
Reconstruction after endoscopic endonasal approaches to the skull base, including the pituitary region is of paramount importance to avoid postoperative cerebrospinal fluid (CSF) leak. The postoperative leak rate after endoscopic pituitary surgery ranges from 1.9-9% in different series 2-5. The introduction of the vascularized flaps has reduced the incidence of postoperative CSF leak, however it carries important nasal morbidity. Mucosalization of the septum requires 12 weeks, multiple debridements in the office, and frequent saline rinses 6.
Figure 2. Donor site. Picture obtained with a 0 degree endoscope from the right nasal cavity. (A) Inferior meatus. Observe the relation of the lateral incision (dashed line) and the opening of the nasolacrimal duct. The incison should be performed inferior to that opening leaving the mucosa around the duct opening. (B) Nasal cavity view after positioning back the inferior turbinate. Oulined the septal incision. A plastic splint is placed between the turbinate and the septum. The splint is removed 1 week after surgery.
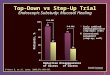
Figure 1. Pictures obtained with a 0 degree endoscope from the right nasal cavity. (A) Preoperative view. (B) Sharp and vertical incision at the head of the inferior turbinate. This allows mobilization of the inferior turbinate superiorly and great exposure of the inferior meatus. (C) After elevation of the inferior turbinate. Observe the dashed lines. Yellow – posterior cut close to the transition between hard and soft palate. Green – Lateral incision close to the attachment of the inferior turbinate. Blue – Anterior incision is performed from the head of the turbinate to the septum. It can also be carried anteriorly to the nostril if a larger flap is warranted. Red – Medial cut is performed to include a strip of mucosa from the septum. This can be tailored depending on the size of the defect. Usually including 2-3mm of the septum mucosa offers a excellent coverage for the majority of the defects. (D) Inferior meatus view of the incisions performed with a needle tip bovie. (E) View of anterior and medial cuts after placing the turbinate in its natural position. (F) Elevation of the graft from the septum. (G) Final elevation of the graft. (H) The mucosal surface of the graft is marked with a marking pen.
CORRESPONDING AUTHOR
Surgical VIDEO
Nasal cavity floor free mucosal graft for endoscopic reconstruction of the sellar region: technical note and results in consecutive 44 cases
Maria Peris-Celda MD PhD1, Mark Chaskes2, Robert Engle MD3, Tyler Kenning MD1, Carlos D. Pinheiro-Neto MD PhD3 1 Department of Neurosurgery, Albany Medical College, Albany, New York.
2 Medical Student, Albany Medical College, Albany, New York 3 Division of Otolaryngology and Head-Neck Surgery, Department of Surgery, Albany Medical College, Albany, New York.
References 1. Peris-Celda M, Pinheiro-Neto CD, Funaki T, Fernandez-Miranda JC, Gardner P, Snyderman C, Rhoton AL. The extended nasoseptal flap for skull base
reconstruction of the clival region: an anatomical and radiological study. J Neurol Surg B Skull Base. 2013 Dec;74(6):369-85. 2. Dehdashti AR, Ganna A, Karabatsou K, Gentili F. Pure endoscopic endonasal approach for pituitary adenomas: early surgical results in 200 patients and
comparison with previous microsurgical series. Neurosurgery. May 2008;62(5):1006-1015; discussion 1015-1007. 3. Paluzzi A, Fernandez-Miranda JC, Tonya Stefko S, Challinor S, Snyderman CH, Gardner PA. Endoscopic endonasal approach for pituitary adenomas: a
series of 555 patients. Pituitary. Aug 2014;17(4):307-319. 4. Torales J, Halperin I, Hanzu F, et al. Endoscopic endonasal surgery for pituitary tumors. Results in a series of 121 patients operated at the same center and
by the same neurosurgeon. Endocrinologia y nutricion : organo de la Sociedad Espanola de Endocrinologia y Nutricion. Oct 2014;61(8):410-416. 5. Sanders-Taylor C, Anaizi A, Kosty J, Zimmer LA, Theodosopoulos PV. Sellar Reconstruction and Rates of Delayed Cerebrospinal Fluid Leak after
Endoscopic Pituitary Surgery. J Neurol Surg B Skull Base. 2015 Aug;76(4):281-5 6. Kimple AJ, Leight WD, Wheless SA, Zanation AM. Reducing nasal morbidity after skull base reconstruction with the nasoseptal flap: free middle turbinate
mucosal grafts. Laryngoscope. 2012 Sep;122(9):1920-4.
Carlos D. Pinheiro-Neto, MD PhD
Division of Otolaryngology – Head & Neck Surgery Albany Medical Center 47 New Scotland Avenue MC-41 Albany, NY 12208 Phone: (518) 262-5575 Fax: (518) 262-5184 Email: [email protected]
Inlay collagen dural graft
Free mucosal graft
Oxidized cellulose at the borders of the graft
Dural sealant
Bioresorbable sphenoid packing
• The harvested graft was approximately 3 x 2,5 cm. • Sinonasal outcome test (SNOT-22) was obtained
before surgery, one month, and three months after surgery.
Figure 3. Pictures obtained with a 0 degree endoscope. (A) Inlay collagen dural graft. (B) Overlay free mucosal graft covering the entire defect. All borders of the flap should be in contact with bone. This is why the extra-mucosa harvested from the septum is important to guarantee good contact and healing of the graft to the bone. (C) Oxidized cellulose at the borders of the graft. (D) Dural sealant. After that a bioresorbable packing is used to fill the sphenoid and support the reconstruction.
Figure 4. Postoperative pictures taken in the office 4 weeks after surgery. (A) Right nasal cavity. Observe the donor site is completely mucosalized and the turbinate incision healed as well. (B) Sphenoid. Note the graft well healed to the skull base.
Figure 5. Postoperative pictures taken in the office 3 months after surgery. (A) Right nasal cavity. The donor site is completely healed. (B) Sphenoid. Excellent integration of the graft to the skull base.
• 38.6% of intraoperative leaks. • NO postoperative leaks. • 1 month after surgery - near total or complete
mucosalization of the donor site with minimal or no crusting in the nasal cavity floor.
• In one case of reoperation due to tumor recurrence, the healed graft was taken down and reused for reconstruction.
• No fat grafts or lumbar drains were used. • No significant difference was found in the
SNOT-22 comparing the preoperative scores, 1-month and 3-month follow-up.
• No epiphora or intranasal synechiae.
RESULTS