Embed Size (px)
Citation preview

Nasopharyngeal Intracavitary BrachytherapyThe Controversy of T2b Disease
To-Wai LeungStewart Y. TungVicty Y. W. Wong, M.Sc.
Wing-Kin SzeCollin M. M. Lui, B.Sc.
Frank C. S. WongAnn-Shing LeeSai-Ki O
Department of Clinical Oncology, Tuen Mun Hos-pital, Hong Kong SAR, People’s Republic of China.
Presented in part at the Fourth International UnionAgainst Cancer Symposium on NasopharyngealCarcinoma, Hong Kong, People’s Republic ofChina, February 2003.
The authors thank the staff of the Department ofClinical Oncology (Tuen Mun Hospital) for theircontribution to this study.
Address for reprints: To-Wai Leung, Department ofClinical Oncology, Tuen Mun Hospital, Tsing ChungKoon Road, Hong Kong SAR, People’s Republic ofChina; Fax: (011) 852 2468 5097; E-mail:[email protected]
Received February 1, 2005; revision received April25, 2005; accepted May 16, 2005.
BACKGROUND. Locally persistent nasopharyngeal carcinoma (NPC) carries an in-
creased risk of local failure if additional treatment is not given. It has been shown
that intracavitary brachytherapy is effective in the treatment of patients with T1
and T2a NPC, although its role in the treatment of T2b disease had remained
uncertain. The objectives of the current study were to evaluate the outcomes of
patients with T2b, locally persistent NPC who were treated with high-dose-rate
(HDR) intracavitary brachytherapy and to explore whether routine brachytherapy
boost could improve the local control of patients who had T2b NPC at initial
diagnosis.
METHODS. Thirty-four patients with locally persistent NPC who were treated during
1992–2000 with HDR intracavitary brachytherapy were analyzed retrospectively. All
patients had T2b disease at initial diagnosis. They were treated with HDR intra-
cavitary brachytherapy at doses of 22.5–24.0 grays (Gy) in 3 weekly sessions. To
compare the efficacy of brachytherapy, another 403 consecutive patients with
nonmetastatic T2b NPC who were treated with curative intent by external radio-
therapy (ERT) during the same period were evaluated.
RESULTS. An improvement in the 5-year actuarial local failure-free survival rate
(brachytherapy group vs. ERT group: 96.9% vs. 81.5%; P � 0.024), the disease-
specific survival rate (84.5% vs. 68.1%; P � 0.021), and the overall survival rate
(78.3% vs. 63.1%; P � 0.034) was demonstrated in the group that had locally
persistent NPC who were salvaged with brachytherapy. In assessing local control,
the addition of brachytherapy was just short of statistical significance on multi-
variate analysis (P � 0.054). The complication rates were comparable between the
brachytherapy group and the ERT group.
CONCLUSIONS. The results suggested that patients with T2b NPC who have locally
persistent disease can be salvaged effectively with brachytherapy. Their local
control was even better than that achieved by patients who had clinical remission
of local disease at the completion of ERT. Furthermore, it is possible that routine
brachytherapy boost, after the completion of ERT, may improve local control in
patients who have T2b disease at initial diagnosis. However, its exact benefit can be
elucidated only by prospective, randomized studies. Cancer 2005;104:1648 –55.
© 2005 American Cancer Society.
KEYWORDS: nasopharyngeal carcinoma, parapharyngeal disease, intracavitarybrachytherapy, persistent disease, routine boost.
Persistent nasopharyngeal carcinoma (NPC) carries an increasedrisk of local recurrence. The local control rate among patients with
persistent local disease reportedly was approximately 40% and wasmuch worse than the local control rate among patients who achievedclinical or histologic remission.1,2 To date, the effectiveness of naso-pharyngeal intracavitary brachytherapy in salvaging patients who
1648
© 2005 American Cancer SocietyDOI 10.1002/cncr.21371Published online 23 August 2005 in Wiley InterScience (www.interscience.wiley.com).

have locally persistent T2b NPC at initial diagnosis hasnot been addressed in the literature.
Despite advances in imaging technology andtreatment techniques, local failure still occurred in20 –37% of patients who received adequate treatmentto the nasopharynx in several contemporary seriesusing 2-dimensional (2D) treatment techniques.3– 6
Maximizing local control is important for the follow-ing reasons: 1) Treatment results of locally recurrentNPC are unsatisfactory, with a 5-year actuarial localcontrol rate in the range of 15–37.8%.6 –9 2) Retreat-ment of locally recurrent NPC is associated with a highrisk of complications. We previously reported a 5-yearmajor complication-free rate (MCFR) of 26.7% afterreirradiation.7 3) Patients with locoregional failurehave an increased risk of distant metastasis.10 Giventhe poor outcome and associated complications withretreatment, more aggressive primary treatment is re-quired to secure a higher level of local control with theleast toxicity.
Whether aggressive local treatment with brachy-therapy boost improves the outcomes of patients withT2b disease is a question that remains unan-swered.11–13 To address this question, we reviewed thetreatment results of a series of patients who had lo-cally persistent, T2b NPC at their initial diagnosis. Inthis study, we evaluated the effectiveness of salvagebrachytherapy for this group of patients and providesome grounds for exploration of any possible thera-peutic gain from dose escalation with brachytherapy.
MATERIALS AND METHODSPatientsIn the Department of Clinical Oncology at the TuenMun Hospital, 34 patients with locally persistent NPC,after a radical course of external radiotherapy (ERT),were treated with high-dose-rate (HDR), intracavitarybrachytherapy during the period from 1992 to 2000.All patients had T2b disease at initial diagnosis. Toevaluate the efficacy of brachytherapy, another 403patients with nonmetastatic T2b disease who weretreated with radical ERT during the same period wereincluded in the analysis. All patients underwent awork-up that included fiber optic nasopharyngoscopyand a computed tomography (CT) scan of the naso-pharynx during initial diagnosis. They were restagedaccording to the 1997 International Union AgainstCancer (UICC) staging system.14 All patients were ob-served until death or for a minimum of 18 months.The demographic details are shown in Table 1.
The radiotherapy (RT) techniques used for thecurrent study were reported initially by Ho.15 Briefly,most patients received equivalent doses of 63– 66grays (Gy) to the nasopharynx with fraction sizes of
2.0 –2.5 Gy per day (Table 2). Most patients with para-pharyngeal space involvement were boosted by a pos-terior oblique field with 10 –24 MV photons, for a totalof 10 Gy in 4 –5 daily fractions. The neck was treatedwith an anterior cervical field, delivering an equivalentdose of 60 – 66 Gy with a fraction size of 2.0 –5.6 Gy.Various schedules were used to treat the neck duringthe study period, ranging from daily to weekly treat-ments. Brachytherapy was reserved as salvage for pa-tients who had persistent disease.
Fiber optic nasopharyngoscopy was performed3– 6 weeks after the completion of the primary RT forthe assessment of tumor response. Biopsies weretaken from suspicious areas. Tumor mapping was notperformed. Thirty-four patients had biopsy-proven,persistent disease at a median of 6 weeks after RT. CTscans for restaging were not obtained after the docu-mentation of persistent disease. Patients were treatedwith HDR intracavitary brachytherapy using an Irid-ium 192 source (microSelectron; Nucletron). The me-
TABLE 1Characteristics of 437 Patients at Presentation
Characteristic
No. of patients (%)
Brachytherapygroup(n � 34)
ERT group(n � 403)
P value(chi-square test)
GenderMale 29 (85) 287 (71) 0.078Female 5 (15) 116 (29)
Age� 45 yrs 18 (53) 191 (47) 0.53� 45 yrs 16 (47) 212 (53)
HistologyUndifferentiated CA 32 (94) 372 (92) 0.7Nonkeratinizing SCC 2 (6) 31 (8)
UICC stagingIIB 22 (65) 236 (59) 0.69III 9 (26) 113 (28)IV 3 (9) 54 (13)
N stagingN0 12 (35) 79 (20) 0.18N1 10 (29) 157 (39)N2 9 (27) 113 (28)N3 3 (9) 54 (13)
Top up PPSGiven 26 (76) 334 (83) 0.35Not given 8 (24) 69 (17)
Neoadjuvant chemotherapyGiven 10 (29) 100 (25) 0.55Not given 24 (71) 303 (75)
Median FU for survivingpatients 86 mos 80 mos
ERT: external radiotherapy; CA: carcinoma; SC: squamous cell carcinoma; UICC: International Union
Against Cancer; PPS: parapharyngeal space; FU: follow-up.
Brachytherapy for Persistent T2b NPC/Leung et al. 1649

dian time between the completion of ERT and the firstbrachytherapy procedure was 8 weeks (range, 5–12weeks). A 6-French gauge bronchial applicator wasplaced inside a 3.2-mm diameter nylon tube and wasused as a nasopharyngeal applicator (Fig. 1). The ap-plicators were positioned under topical anesthesiawith fiber optic endoscopic guidance. The mediantreatment length for the nasal applicators was 3 cm.Patients who were treated prior to 1995 were given24.0 Gy in 3 weekly fractions. This dose was reduced to22.5 Gy in 3 weekly fractions after mid-1995. The ra-tionale for this dose reduction has been reported else-where.16 This dose was prescribed at a distance of 1cm from the center of the surface defined by thesources. Computerized dosimetry based on geometricoptimization was performed using the configurationof the catheters as generated by the 3D, semiorthogo-nal image reconstruction method provided by the mi-croSelectron planning system. Any displacement ofthe catheters was verified by 3D reconstruction beforeand after the treatment. For most patients, the dis-placement was within 1 mm.16
Statistical AnalysisSurvival rates were calculated based on the date ofhistologic diagnosis. Both persistent tumors and re-current local tumors, after brachytherapy, were in-cluded as endpoints for local failure-free survival(LFFS). Disease-specific death and death related tocomplications were used as endpoints for calculatingactuarial disease-specific survival. Actuarial survivalwas calculated according to the method of Kaplan andMeier.17 For comparison of survival curves, the log-rank test was used.18 Multivariate analyses were per-formed using the Cox proportional hazards model.19
RESULTSOne patient in the persistent group and 67 patients inthe ERT group developed a local recurrence. In theERT group, the distribution of patients with local re-currence according to their T stage at recurrence (rT)was as follow: rT1, 17 patients (25.4%); rT2a, 3 patients(4.4%); rT2b, 24 patients (35.8%); rT3, 8 patients (12%);and rT4, 15 patients (22.4%). Forty-four of 67 patients(66%) had early T stage (rT1–rT2) at recurrence. Inassessing local control, only the addition of brachy-therapy (local persistence) was significant in the log-rank test. The 5-year actuarial LFFS rate for thebrachytherapy group and the ERT alone group, re-spectively, was 96.9% and 81.5% (P � 0.024) (Fig. 2).Other parameters, such as patient age, tumor histol-ogy, gender, lymph node status, and carotid spaceinvasion, were nonsignificant. The addition of brachy-therapy was just short of statistical significance onmultivariate analysis for LFFS (P � 0.054). Patientswho had local recurrences that were amenable to rad-ical treatment were offered salvage RT/nasopharyn-gectomy with or without chemotherapy, as indicated.The ultimate local control rate at 5 years for thebrachytherapy group and the ERT group, respectively,was 96.7% and 89.9% (P � 0.13).
Improvements in the 5-year disease-specific sur-vival rate (84.5% vs. 68.1%; P � 0.021) and the overallsurvival rate (78.3% vs. 63.1%; P � 0.034) were dem-onstrated in the group with locally persistent NPC whowere salvaged with brachytherapy. The 5-year actuar-ial progression-free survival rate (71.6% vs. 59.2%; P� 0.058), the actuarial regional failure-free survivalrate (86.5% vs. 92.6%; P � 0.42), and the distant me-tastasis-free survival rate (81.0% vs. 72.6%; P � 0.17)were comparable between the brachytherapy groupand the ERT group.
TABLE 2Various Fractionation Schedules Used to the Nasopharynx
No. of patients (%)
Fractionation scheduleTotal dose(Gy)
Equivalentdose (Gy)a
BED3(Gy3)b
ERTgroup
Brachytherapygroup
216 (54.0) 17 (50.0) 2.0 Gy (5 fr/wk) � 20 fr � 2.5 Gy (5 fr/wk) � 9 fr 62.5 63.4 108.0150 (37.0) 11 (32.0) 2.0 Gy (5 fr/wk) � 33 fr 66.0 66.0 110.0
13 (3.0) 4 (12.0) 2.5 Gy (4–5 fr/wk) � 24 fr 60.0 62.5 110.010 (2.5) 0 (0.0) 2.0 Gy (5 fr/wk) � 18 fr � 2.5 Gy (5 fr/wk) � 11 fr 63.5 64.6 110.412 (3.0) 1 (3.0) 2.3 Gy (5 fr/wk) � 17 fr � 2.5 Gy (5 fr/wk) � 9 fr 61.6 63.5 110.4
2 (0.5) 1 (3.0) 2.0 Gy (5 fr/wk) � 36 fr 72.0 72.0 120.0
ERT: external radiotherapy; fr: fractions; Gy: grays; BED: biologic effective dose.a The equivalent dose according to linear-quadratic formula assuming an �/� of 10 Gy with no correction of time factor.b The BED assuming an �/� of 3.0 Gy.
1650 CANCER October 15, 2005 / Volume 104 / Number 8

With regard to treatment complications, variousdegrees of xerostomia, neck fibrosis, and hearing im-pairment were seen commonly. The complicationrates were comparable when all patients in thebrachytherapy and ERT groups were compared. The5-year MCFR for all patients in the brachytherapygroup and the ERT group was 76.7% and 80.1%, re-spectively (P � 0.47). Damage to the central nervoussystem (CNS) was the most devastating late complica-tion (cranial nerve palsy and temporal lobe necrosis).The corresponding 5-year CNS complication-freerates (CFR) were 89.6% and 87.4%, respectively (P� 0.7).
To evaluate whether there were increased compli-cations with the addition of brachytherapy, 369 pa-tients who achieved local control with 1 course of RTwere included for further analysis. Table 3 depicts thevarious late complications encountered. Ten patientsin the brachytherapy group and 54 patients in the ERTgroup experienced � 1 major complication. This cor-responded to a 5-year MCFR of 76.3% and 85.3% for
FIGURE 1. The nylon tube nasal technique is illustrated with radioopaque dummies in situ. The isodose distribution is superimposed on this lateral skull
radiograph. The dose was prescribed at 1 cm from the center of the surface, as defined by the sources.
FIGURE 2. Actuarial local failure-free survival is illustrated for the brachy-
therapy group and the external radiotherapy (RT) groups. In the brachytherapy
group, the numbers of patients at risk were 34 patients at 0 years, 33 patients
at 2 years, 27 patients at 4 years, 18 patients at 6 years, 11 patients at 8 years,
and 6 patients at 10 years. In the external RT group, the numbers of patients
at risk were 403 patients at 0 years, 303 patients at 2 years, 231 patients at
4 years, 136 patients at 6 years, 80 patients at 8 years, and 36 patients at 10
years.
Brachytherapy for Persistent T2b NPC/Leung et al. 1651
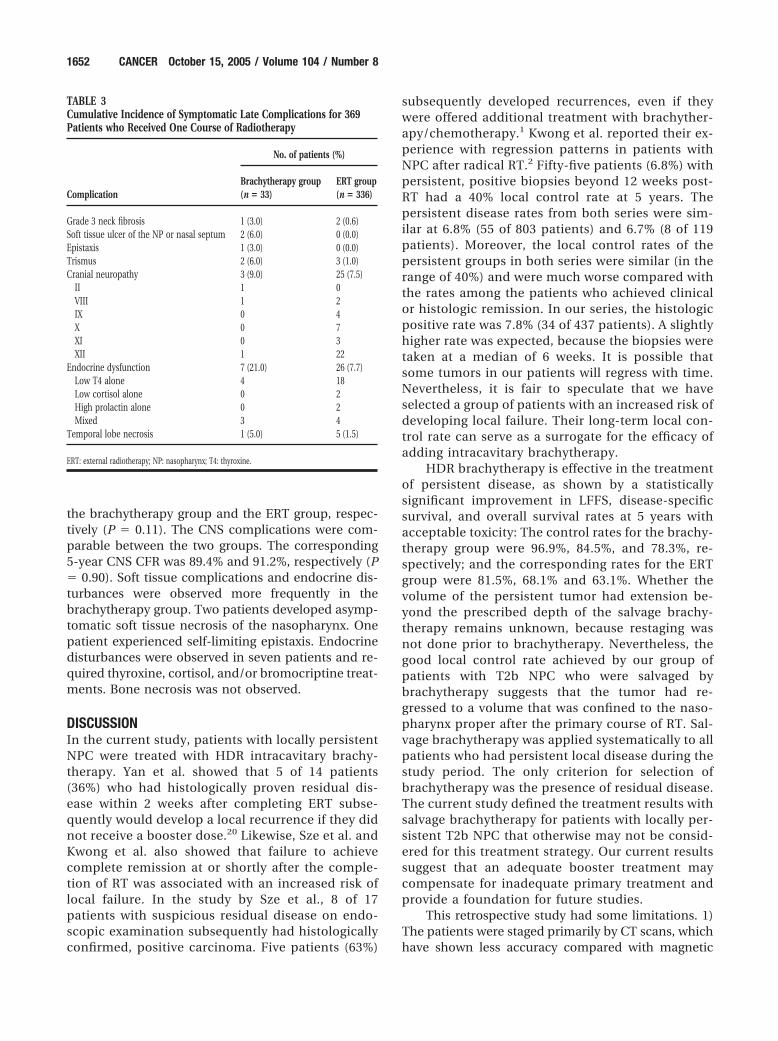
the brachytherapy group and the ERT group, respec-tively (P � 0.11). The CNS complications were com-parable between the two groups. The corresponding5-year CNS CFR was 89.4% and 91.2%, respectively (P� 0.90). Soft tissue complications and endocrine dis-turbances were observed more frequently in thebrachytherapy group. Two patients developed asymp-tomatic soft tissue necrosis of the nasopharynx. Onepatient experienced self-limiting epistaxis. Endocrinedisturbances were observed in seven patients and re-quired thyroxine, cortisol, and/or bromocriptine treat-ments. Bone necrosis was not observed.
DISCUSSIONIn the current study, patients with locally persistentNPC were treated with HDR intracavitary brachy-therapy. Yan et al. showed that 5 of 14 patients(36%) who had histologically proven residual dis-ease within 2 weeks after completing ERT subse-quently would develop a local recurrence if they didnot receive a booster dose.20 Likewise, Sze et al. andKwong et al. also showed that failure to achievecomplete remission at or shortly after the comple-tion of RT was associated with an increased risk oflocal failure. In the study by Sze et al., 8 of 17patients with suspicious residual disease on endo-scopic examination subsequently had histologicallyconfirmed, positive carcinoma. Five patients (63%)
subsequently developed recurrences, even if theywere offered additional treatment with brachyther-apy/chemotherapy.1 Kwong et al. reported their ex-perience with regression patterns in patients withNPC after radical RT.2 Fifty-five patients (6.8%) withpersistent, positive biopsies beyond 12 weeks post-RT had a 40% local control rate at 5 years. Thepersistent disease rates from both series were sim-ilar at 6.8% (55 of 803 patients) and 6.7% (8 of 119patients). Moreover, the local control rates of thepersistent groups in both series were similar (in therange of 40%) and were much worse compared withthe rates among the patients who achieved clinicalor histologic remission. In our series, the histologicpositive rate was 7.8% (34 of 437 patients). A slightlyhigher rate was expected, because the biopsies weretaken at a median of 6 weeks. It is possible thatsome tumors in our patients will regress with time.Nevertheless, it is fair to speculate that we haveselected a group of patients with an increased risk ofdeveloping local failure. Their long-term local con-trol rate can serve as a surrogate for the efficacy ofadding intracavitary brachytherapy.
HDR brachytherapy is effective in the treatmentof persistent disease, as shown by a statisticallysignificant improvement in LFFS, disease-specificsurvival, and overall survival rates at 5 years withacceptable toxicity: The control rates for the brachy-therapy group were 96.9%, 84.5%, and 78.3%, re-spectively; and the corresponding rates for the ERTgroup were 81.5%, 68.1% and 63.1%. Whether thevolume of the persistent tumor had extension be-yond the prescribed depth of the salvage brachy-therapy remains unknown, because restaging wasnot done prior to brachytherapy. Nevertheless, thegood local control rate achieved by our group ofpatients with T2b NPC who were salvaged bybrachytherapy suggests that the tumor had re-gressed to a volume that was confined to the naso-pharynx proper after the primary course of RT. Sal-vage brachytherapy was applied systematically to allpatients who had persistent local disease during thestudy period. The only criterion for selection ofbrachytherapy was the presence of residual disease.The current study defined the treatment results withsalvage brachytherapy for patients with locally per-sistent T2b NPC that otherwise may not be consid-ered for this treatment strategy. Our current resultssuggest that an adequate booster treatment maycompensate for inadequate primary treatment andprovide a foundation for future studies.
This retrospective study had some limitations. 1)The patients were staged primarily by CT scans, whichhave shown less accuracy compared with magnetic
TABLE 3Cumulative Incidence of Symptomatic Late Complications for 369Patients who Received One Course of Radiotherapy
Complication
No. of patients (%)
Brachytherapy group(n � 33)
ERT group(n � 336)
Grade 3 neck fibrosis 1 (3.0) 2 (0.6)Soft tissue ulcer of the NP or nasal septum 2 (6.0) 0 (0.0)Epistaxis 1 (3.0) 0 (0.0)Trismus 2 (6.0) 3 (1.0)Cranial neuropathy 3 (9.0) 25 (7.5)
II 1 0VIII 1 2IX 0 4X 0 7XI 0 3XII 1 22
Endocrine dysfunction 7 (21.0) 26 (7.7)Low T4 alone 4 18Low cortisol alone 0 2High prolactin alone 0 2Mixed 3 4
Temporal lobe necrosis 1 (5.0) 5 (1.5)
ERT: external radiotherapy; NP: nasopharynx; T4: thyroxine.
1652 CANCER October 15, 2005 / Volume 104 / Number 8

resonance imaging (MRI) in evaluating parapharyn-geal invasion. This may pose some uncertainties in thestaging of our patients and, thus, may have an impacton the results. MRI of the nasopharynx has been usedfor staging in our department since 2002. 2) There wasan imbalance in the lymph node status (N stage) be-tween the two groups, although the difference (Pvalue) was deemed not statistically significant. Agreater proportion of patients with more favorable N0disease (35% vs. 20%) and lower proportion of patientswith unfavorable N3 disease (9% vs. 13%) in thebrachytherapy group may have led to expectationsthat they would contribute to the favorable and sig-nificant survival rates observed. We previously re-ported results from 1070 patients with NPC who weretreated between the years 1990 and 1998; however, inthat study, UICC N stage was not a significant prog-nosticator for local control on multivariate analysis.21
3) Chemo-RT and 3D conformal RT/intensity-modu-lated RT, which have resulted in improved outcomesin patients with NPC, were not offered routinely to ourpatients due to resources constraints.22–24 It is likelythat local control may be improved with the use ofthese sophisticated techniques and that the chance oflocal persistence may be reduced. However, the desir-able 3D techniques may not be available freely inevery country. Despite these limitations, we are con-fident that the benefit in improving the local control isreal, as demonstrated by the fact that we have com-pared a poor-risk group with a normal-risk controlgroup.
Other sophisticated approaches in treating pa-tients with locally persistent NPC using conformal/stereotactic techniques have been reported.25–27 Yauet al. reported the use of fractionated stereotactic RTfor 21 patients who had locally persistent NPC. The3-year LFFS rate in their study was comparable tothe rate achieved by a control group of patients whohad achieved complete remission after their pri-mary course of RT (82% vs. 86%; P �.71).25 Chua etal. employed linear accelerator-based stereotacticradiosurgery as salvage treatment for seven patientswith early-stage, locally persistent NPC. The mediandose in that study was 12.5 Gy delivered to the 80%isodose line. All seven patients had maintained localcontrol at the time of analysis.26 The choice of var-ious boost techniques depends on the availability oftechnology and expertise. Brachytherapy boostshould be considered an effective treatment modal-ity, especially in regions where conformal/stereo-tactic facilities are not readily available. The easyaccessibility of afterloading machines, coupled witha relatively simple procedure, makes this technique
attractive to centers with no 3D facilities or withtight machine times.
The benefit of dose escalation with brachytherapyfor patients with T2b disease has not been addressedin prospective randomized studies. There is conflict-ing information in the literature regarding the efficacyof brachytherapy boost for patients with T2b disease.Teo et al. showed that the benefit in local control withbrachytherapy boost was confined to patients withT1–T2a disease.28 Levendag et al. suggested thatbrachytherapy boost would benefit not only patientswith T1 and T2a tumors but also those T2b tumorsthat had regressed to a clinical target volume confinedto the nasopharynx proper after pretreatment withERT and/or chemotherapy.12 Wang included brachy-therapy as a boost in the primary treatment of patientswith T1–T2 disease (according to 1997 UICC criteria)and showed a statistically significant improvement inlocal control.11
To address whether brachytherapy boost is ben-eficial for patients with T2b disease, we attemptedto approach the problem by examining the failurepatterns of T2b disease and the efficacy of salvagebrachytherapy for patients with locally persistentNPC who had T2b disease at initial diagnosis. In theERT group, 20 of 67 patients (30%) who had localrecurrences had their recurrences classified as rT1–T2a disease. The local failure likely is attributed tosuboptimal dose or intrinsic radioresistance of thetumors. The possibility of geographic misses is lesslikely, because the tumors recur within the targetvolume. T1–T2a disease should be covered ade-quately by intracavitary brachytherapy. This was ev-ident by the findings of Levendag et al.12 and Law etal.29 Law et al. reported the results of 118 consecu-tive patients with T1–T2a, recurrent NPC who weretreated with intracavitary mold treatment. Thoseauthors reported a 5-year local control rate of 85%.From the dosimetric viewpoint, T1–T2a NPC shouldbe covered adequately with intracavitary brachy-therapy irrespective of whether the tumor beingtreated is a primary or recurrent NPC. Levendag etal.12 and Wang11 showed improvements in localcontrol with primary treatment by incorporatingbrachytherapy boost for T1–T2 disease, as discussedabove. Therefore, it is likely that the T1–T2a recur-rences, which account for approximately 30% of thelocal recurrences in the ERT group, may be prevent-able if a brachytherapy boost is incorporated intothe primary treatment program. Thirty-six percent(24 of 67) of local recurrences recurred as rT2bdisease. Whether up-front brachytherapy boost mayprevent rT2b recurrence is a question that remainsunanswered. We are optimistic that up-front
Brachytherapy for Persistent T2b NPC/Leung et al. 1653

brachytherapy boost may be beneficial to patientswith T2b NPC, as demonstrated by the fact that eventhe poor-risk patients with locally persistent NPCcould be salvaged successfully by brachytherapy.The 96.9% LFFS rate at 5 years is very encouraging.
To the best of our knowledge, the current series isthe largest of its kind that has been reported in theliterature. Furthermore, the median follow-up for oursurviving patients was approximately 80 months. It islikely that most of the local recurrences would haveoccurred. However, it is difficult to draw any conclu-sion based on this retrospective series with such smallpatient numbers. Nevertheless, this information willadd to our understanding with regard to the possiblebenefit of brachytherapy for patients with T2b NPC.
In summary, we have shown that locally persis-tent NPC carries an increased risk of local recurrenceif adequate additional treatment is not given. Ourexperience suggests that patients with T2b NPC whohave local persistence can be salvaged effectively withbrachytherapy. Their local control is even better thanthat achieved among patients who have a clinical re-mission of local disease at the completion of ERT.Furthermore, it is possible that routine brachytherapyboost, after the completion of ERT, may improve thelocal control of patients who have T2b disease at ini-tial diagnosis. The exact benefit, however, can be elu-cidated only by prospective, randomized studies.
REFERENCES1. Sze WM, Lee AW, Yau TK, et al. The prognostic value of
endoscopic findings after radical radiotherapy for nasopha-ryngeal carcinoma. Proceedings of the UICC Workshop onNasopharyngeal Cancer. Singapore: Armour PublishingPTE, Ltd., 1998:239.
2. Kwong DL, Nicholls J, Wei WI, et al. The time course ofhistologic remission after treatment of patients with naso-pharyngeal carcinoma. Cancer. 1999;85:1446 –1453.
3. Lee AW, Law SC, Foo W, et al. Retrospective analysis ofpatients with nasopharyngeal carcinoma treated during1976 –1985: survival after local recurrence. Int J Radiat OncolBiol Phys. 1993;26:773–782.
4. Johansen LV, Mestre M, Overgaard J. Carcinoma of thenasopharynx: analysis of treatment results in 167 consecu-tively admitted patients. Head Neck Surg. 1992;14:200 –207.
5. Choy D, Sham JS, Wei WI, Ho CM, Wu PM. Transpalatalinsertion of radioactive gold grain for the treatment of per-sistent and recurrent nasopharyngeal carcinoma. Int J Ra-diat Oncol Biol Phys. 1993;25:505–512.
6. Teo PM, Kwan WH, Chan AT, Lee WY, King WW, Mok CO.How successful is high-dose (� 60 Gy) reirradiation usingmainly external beams in salvaging local failures of naso-pharyngeal carcinoma? Int J Radiat Oncol Biol Phys. 1998;40:897–913.
7. Leung TW, Tung SY, Sze WK, et al. Salvage radiation therapyfor locally recurrent nasopharyngeal carcinoma. Int J RadiatOncol Biol Phys. 2000;48:1331–1338.
8. Lee AW, Foo W, Law SC, et al. Reirradiation for recurrent
nasopharyngeal carcinoma: factors affecting the therapeuticratio and ways for improvement. Int J Radiat Oncol BiolPhys. 1997;38:43–52.
9. Chua DT, Sham JS, Kwong DL, Wei WI, Au GK, Choy D.Locally recurrent nasopharyngeal carcinoma: treatment re-sults for patients with computed tomography assessment.Int J Radiat Oncol Biol Phys. 1998;41:379 –386.
10. Kwong DL, Sham JS, Choy D. The effect of loco-regionalcontrol on distant metastatic dissemination in carcinoma ofthe nasopharynx: an analysis of 1301 patients. Int J RadiatOncol Biol Phys. 1994;30:1029 –1036.
11. Wang CC. Improved local control of nasopharyngeal carci-noma after intracavitary brachytherapy boost. Am J ClinOncol. 1991;14:5– 8.
12. Levendag PC, Lagerwaard FJ, Noever I, et al. Role of endo-cavitary brachytherapy with or without chemotherapy incancer of the nasopharynx. Int J Radiat Oncol Biol Phys.2002;52:755–768.
13. Teo PM, Leung SF, Lee WY, Zee B. Intracavitary brachyther-apy significantly enhances local control of early T-stagenasopharyngeal carcinoma—the existence of a dose-tu-mour-control relationship above conventional tumoricidaldose. Int J Radiat Oncol Biol Phys. 2000;46:445– 458.
14. Sobin LH, Wittekind C, editors. International Union AgainstCancer (UICC): TNM classification of malignant tumors, 5thed. New York: John Wiley & Sons, Inc., 1997.
15. Ho JHC. An epidemiologic and clinical study of nasopha-ryngeal carcinoma. Int J Radiat Oncol Biol Phys. 1978;4:183–198.
16. Leung TW, Wong VY, Tung SY, et al. The importance ofthree-dimensional brachytherapy treatment planning fornasopharyngeal carcinoma. Clin Oncol. 1997;9:35– 40.
17. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc. 1958;53:457– 481.
18. Peto R, Pike MC, Armitage P, et al. Design and analysis ofrandomized clinical trials requiring prolonged observationof each patient. Br J Cancer. 1958;35:1–39.
19. Cox DR, Oakes D. Analysis of survival data. London: Chap-man and Hall, 1974.
20. Yan JH, Xu GZ, Hu YH, et al. Management of local residualprimary lesion of nasopharyngeal carcinoma: II. Results ofprospective randomised trial on booster dose. Int J RadiatOncol Biol Phys. 1990;18:295–298.
21. Leung TW, Tung SY, Sze WK, et al. Treatment results of 1070patients with nasopharyngeal carcinoma: an analysis of sur-vival and failure patterns. Head Neck. 2005;27:555–565.
22. Langendijk JA, Leemans CR, Buter J, Berkhof J, Slotman BJ.The additional value of chemotherapy to radiotherapy inlocally advanced nasopharyngeal carcinoma: a meta-analy-sis of the published literature. J Clin Oncol. 2004;22:4604 –4612.
23. Le QT, Tate D, Koong A, et al. Improved local control withstereotactic radiosurgical boost in patients with nasopha-ryngeal carcinoma. Int J Radiat Oncol Biol Phys. 2003;56:1046 –1054.
24. Lee N, Xia P, Quivey JM, et al. Intensity-modulated radio-therapy in the treatment of nasopharyngeal carcinoma: anupdate of the UCSF experience. Int J Radiat Oncol Biol Phys.2002;53:12–22.
25. Yau TK, Sze WM, Lee WM, et al. Effectiveness of brachyther-apy and fractionated stereotactic radiotherapy boost forpersistent nasopharyngeal carcinoma. Head Neck. 2004;26:1024 –1030.
1654 CANCER October 15, 2005 / Volume 104 / Number 8

26. Chua DT, Sham JS, Kwong PW, Hung KN, Leung LH. Linearaccelerator-based stereotactic radiosurgery for limited lo-cally persistent, and recurrent nasopharyngeal carcinoma:efficacy and complications. Int J Radiat Oncol Biol Phys.2003;56:177–183.
27. Zheng XK, Chen LH, Chen YQ, Deng XG. Three-dimen-sional conformal radiotherapy versus intracavitarybrachytherapy for salvage treatment of locally persistentnasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys.2004;60:165–170.
28. Teo PM, Kwan WH, Yu P, Lee WY, Leung SF, Choi P. Aretrospective study of the role of intracavitary brachyther-apy and prognostic factors determining local tumour con-trol after primary radical radiotherapy in 903 non-dissemi-nated nasopharyngeal carcinoma patients. Clin Oncol. 1996;8:160 –166.
29. Law SC, Lam WK, Ng MF, Au SK, Mak WT, Lau WH. Reirra-diation of nasopharyngeal carcinoma with intracavitarymold brachytherapy: an effective means of local salvage. IntJ Radiat Oncol Biol Phys. 2002;54:1095–1113.
Brachytherapy for Persistent T2b NPC/Leung et al. 1655





























