Embed Size (px)
Citation preview
P R A C T I C E I N S I G H T S
National Survey of Pharmacist Certified DiabetesEducators
Laura Shane-McWhorter, Pharm.D., FASCP, Joli D. Fermo, Pharm.D., Nanette C. Bultemeier, Pharm.D., and Gary M. Oderda, Pharm.D., M.P.H.
We sought to determine the demographics of pharmacists who were certifieddiabetes educators (CDEs) and information about their training, professionalaffiliations, and types of diabetes education services that they provide. Wealso queried these pharmacists about clinical activities, reimbursement,impact of certification, and intent to pursue CDE recertification. A list ofpharmacists who were CDEs as of August 31, 2000, was obtained from theNational Certification Board for Diabetes Educators. We then sent a six-pageanonymous survey to 415 pharmacist CDEs; 233 surveys (56.1%) werereturned. Of these respondents, 140 are women and 93 are men, with a meanage of 41.5 years. Most reside in Southern or Western states. Average timesince pharmacist licensure was 17 years, and average time as a CDE was 5years. Most had completed postgraduate training, including residenciesand/or fellowships; 52.8% had faculty appointments; 46.7% stated they werebilling for their services; and 45.9% were obtaining reimbursement. Mostpharmacists (84.4%) stated that they intended to pursue CDE recertification.Providing details about pharmacist CDEs and their clinical activities maymotivate other pharmacists to pursue this credential. Pharmacists are oftenthe most accessible of all health care providers, and earning the CDEcredential may be an important contribution to diabetes care and education.(Pharmacotherapy 2002:22(12):1579–1593)
Patients with diabetes mellitus present anenormous challenge to the health care system.Diabetes is a costly disease in which manycomplications may occur, and yet maintainingappropriate blood glucose control prevents
occurrence and progression of many of thesecomplications.1–6 New statistics indicate that 17million people in the United States (or 6.2% ofthe population) have diabetes. It has beendiagnosed in 11.1 million Americans. Another5.9 million are estimated to have diabetes, but asyet the disease is undiagnosed.7 There are800,000 new cases of diabetes diagnosed everyyear or 2200/day.8, 9 Diabetes treatment costsapproximately $98 billion/year.10, 11 Statisticscompiled by the Centers for Disease Control andPrevention indicate the prevalence of preventivecare practices is suboptimal, and compliancewith national health recommendations is poor.12
This 1997 survey of people with diabetes in 41states demonstrated that only 61.6% of theseindividuals reported receiving a dilated-eyeexamination within the previous year, 54.6%reported receiving a foot examination within the
From the Department of Pharmacy Practice, College ofPharmacy (Drs. Shane-McWhorter and Oderda) and theDepartment of Family and Preventive Medicine, School ofMedicine (Dr. Shane-McWhorter), University of Utah, SaltLake City, Utah; the Department of Pharmacy Practice,Medical University of South Carolina, Charleston, SouthCarolina (Dr. Fermo); and the Oregon Health and ScienceUniversity, Portland, Oregon (Dr. Bultemeier).
Supported in part by Parke-Davis, Somerville, New Jersey.Presented as a poster at the American College of Clinical
Pharmacy 2001 Spring Practice and Research Forum, April22–25, 2001, Salt Lake City, Utah.
Address reprint requests to Laura Shane-McWhorter,Pharm.D., University of Utah College of Pharmacy,Department of Pharmacy Practice, 30 South 2000 E #260,Salt Lake City, UT 84112.

PHARMACOTHERAPY Volume 22, Number 12, 2002
previous year, 39.6% reported self-monitoring ofblood glucose at least once/day, and 18.4%reported having their hemoglobin A1c (A1C)levels checked in the previous year.12
One of the most important aspects of diabetesmanagement is patient education so thatindividuals with diabetes have the necessaryinformation to optimize diabetes control; thismay help maintain wellness and preventdiabetes-related complications. Certified diabeteseducators (CDEs) provide self-managementeducation with the target goal of maintainingappropriate blood glucose control and therebypreventing diabetes-related complications. Whendiabetes initially is diagnosed, however, theprovider (often a primary care provider) does nothave the time necessary to provide the patientwith self-management education. Ancillaryhealth care professionals are key in the continuedsupport and education of these patients.However, an adequate number of professionalswith advanced training to whom patients may bereferred is lacking. Pharmacists lack providerstatus under Medicare and consequently are oftennot recognized by other health care professionalsor by billing services as medical providers. Thus,patients might not be referred to them fordiabetes education.
To provide quality diabetes care and education,health care professionals must receive basicpreparation and continuing education in specificeducational strategies and behavioral interven-tions.13–19 Behavioral and lifestyle modificationsare the keys to successful self-management ofdiabetes.20, 21 In one study, four different educationprograms produced lowering of A1C and bodymass index, but behavioral programs producedgreater patient satisfaction and greater likelihoodto seek the services of ancillary health careproviders, such as podiatrists.20 In an assessmentof attitudes of dietitians, nurses, and physicianstoward diabetes, diabetes specialists had morepositive attitudes than did nonspecialists and yetall were in favor of a team approach to care.21
Instructors without specialized training indiabetes,15, 16, 22–27 behavioral interventions,20, 21,
28–31 teaching and learning skills,17, 32–36 as well ascounseling skills,14, 18 may not focus on patientbehavioral changes and, therefore, may notimprove clinical outcomes. Several reports haveaddressed the issue of specialized training indiabetes to improve clinical outcomes. Forinstance, some reports have shown a mismatch inperceived versus actual diabetes knowledgeamong staff nurses15, 24, 26; those who actually
spend more time in diabetes practice and diabetescontinuing education have higher knowledgescores and provide more comprehensive exerciseteaching than those who have less training.16
Those with specialized training in screening andpatient education for diabetic foot ulcers havehelped prevent lower extremity amputations,23, 25
yet because of a lack of provider education inpreventive diabetes foot care, a Medicare benefitfor therapeutic shoes was extremely underused.27
Also, training in behavioral interventions isimportant. Besides increased patient satisfaction20
or a more positive attitude,21 educators who hadformal training had a positive association withgreater use of behavioral techniques.28 In onereport, subjects had improved metabolic controlwhen they were taught coping skills, a type ofbehavioral intervention, from an educator.29
Another report stated that over half the educatorshad received behavioral training to help withlifestyle modifications.30 Some behavioraltechniques they cited included goal setting,behavioral modification, positive reinforcement,making contracts with patients, and stressreduction.30 In another setting, practitionersstated they found benefit from training theyreceived in behavioral techniques that includedagenda-setting techniques, motivational inter-viewing, and assessing readiness for change.31
Instruction in teaching and learning skills alsomay have an effect on outcomes. In one study,nurses questioned the adequacy of theirknowledge of diabetes and how competent theyfelt in caring for patients with diabetes.17
Another report eloquently discussed the scarcityof techniques to train health care professionals toprovide education so that patients may betterself-manage their diabetes.32 The authors statedthat education must be aligned with patients’sociocultural characteristics, personal beliefsregarding diabetes, and ability to cope with thedisease and with the realization that the patient isthe locus of control.32 Other investigatorsmentioned using techniques of adult educationto address a psychosocial variable, such asattitude, as an important contributor to positivediabetes management.33 Training of health careprofessionals improves patient teaching skills.34
Patient education that produces behavioralchanges requires that health care professionalshave specific training, good communication andteaching skills, a supportive attitude, a readinessto listen and negotiate,35 as well as time andadequate teaching skills.36
Without training in counseling skills, providers
1580
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
may not be able to positively affect patientbehavior. In one study, physicians were providedspecialized training and were taught to conductdietary risk assessments and provide patient-centered counseling to change dietary patterns.14
Other types of counseling, including patienteducation and adherence promotion skills, arenot always part of dietitians’ training, butsupplemental training may improve theseteaching skills.15 In summary, health careprofessionals require greater knowledge andutilization of behavioral interventions in patientswith any chronic disease.18, 19, 28, 37, 38
One option for pharmacists to obtain diabetes-focused postgraduate education is preparation forthe CDE examination. This certification by theNational Certification Board for DiabetesEducators (NCBDE) is one way that health careprofessionals may demonstrate mastery of aspecific body of knowledge. The CDE hasbecome the accepted credential for diabetes self-management education,39 which is an interactive,collaborative, ongoing process involving theperson with diabetes and the educator(s).40 Thisprocess involves assessment of the individual’sspecific education needs, identification of theindividual’s specific diabetes self-managementgoals, education and behavioral interventionsdirected toward helping the individual achieveidentified self-management goals, and evaluationof the individual’s attainment of identified self-management goals.40
Passing an examination administered throughthe NCBDE is a requirement to becoming a CDE.Also, those qualifying for certification must meetcertain professional and/or educational criteriaand demonstrate that they have provided acertain amount of direct diabetes self-manage-ment education in the 2–5 years before taking theexamination.41 The many health care profes-sionals who are CDEs include nurses, dietitians,social workers, physicians, physical therapists,
and pharmacists. According to the NCBDE, therewere 415 pharmacists as of August 31, 2000.The current total number of CDEs is over12,000.42
We sought to determine several characteristicsof pharmacist CDEs regarding their training,professional organization memberships, workactivities, work sites, motives for certification, andimpact of certification. We also hoped to elucidateinformation about clinical activities, reimburse-ment, and intent to obtain recertification.
Methods
After obtaining investigational review boardapproval, a list of pharmacists who were CDEs asof August 31, 2000, was obtained from theNCBDE. A six-page anonymous survey was sentto all 415 pharmacist CDEs. After 1 month, asecond mailing was sent to nonrespondents.
The survey asked questions about academicdegrees and postgraduate training, professionaland academic affiliations, practice sites, and workactivities. Other questions examined motives forcertification and impact of certification. Thesurvey also asked questions about pharmaceuticalcare services, patient education, physicalassessment provided, billing and reimbursementfor diabetes services, and outcome measures.The survey queried individuals about intent torecertify as a CDE and to obtain the newadvanced practice multidisciplinary credential,the board certified-advanced diabetes management(BC-ADM) certification. The BC-ADM is the firstadvanced practice certification examination indiabetes care available to a variety of professionaldisciplines with advanced degrees; it emphasizesclinical assessment and disease-state management,in addition to patient education and counseling.More information regarding the advanced practicecredential is available from www.aadenet.org orwww.nursingworld.org/ancc.
1581
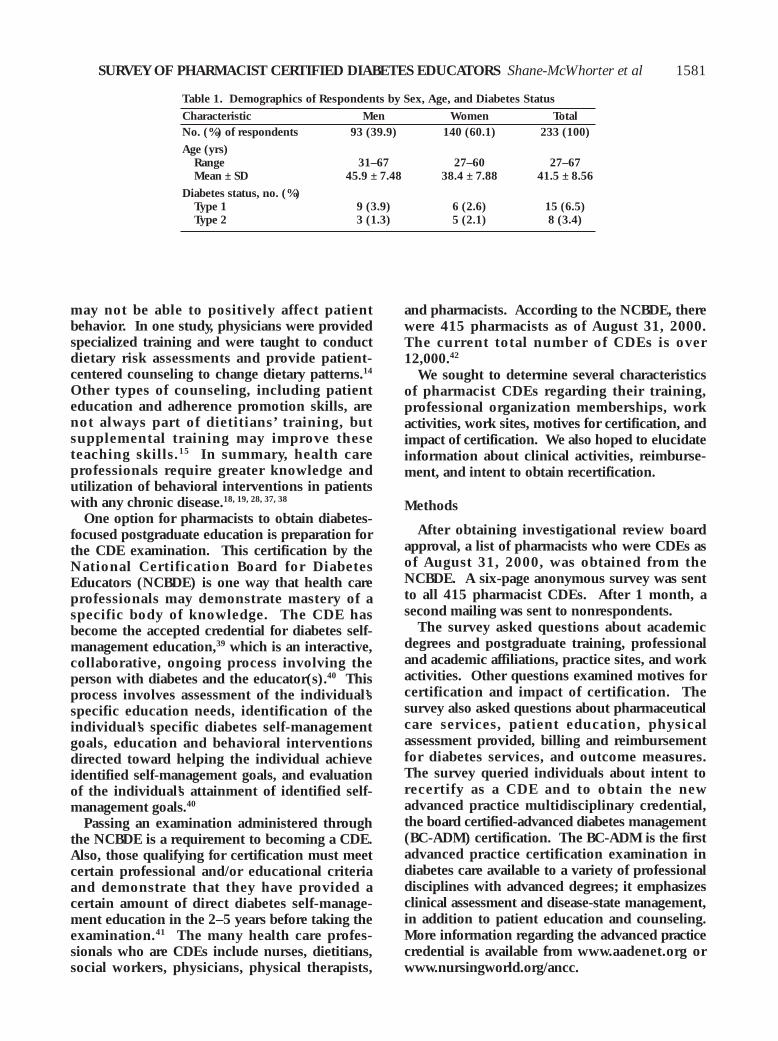
Table 1. Demographics of Respondents by Sex, Age, and Diabetes Status
Characteristic Men Women TotalNo. (%) of respondents 93 (39.9) 140 (60.1) 233 (100)
Age (yrs)Range 31–67 27–60 27–67Mean ± SD 45.9 ± 7.48 38.4 ± 7.88 41.5 ± 8.56
Diabetes status, no. (%)Type 1 9 (3.9) 6 (2.6) 15 (6.5)Type 2 3 (1.3) 5 (2.1) 8 (3.4)
PHARMACOTHERAPY Volume 22, Number 12, 2002
Results
Demographics, Education, Training, and WorkExperience
Of 415 questionnaires, 233 (56.1%) werereturned. Responses were received from 93 men(39.9%) and 140 women (60.1%). Mean age ofmale pharmacists was 45.9 ± 7.48 years, and thatof female pharmacists was 38.4 ± 7.88 years.Mean age of all respondents was 41.5 ± 8.56years. Twenty-three (9.9%) of 232 respondentswho answered the question about diabetes statusstated they had diabetes. Table 1 summarizes thedemographics of respondents by sex, age, anddiabetes status.
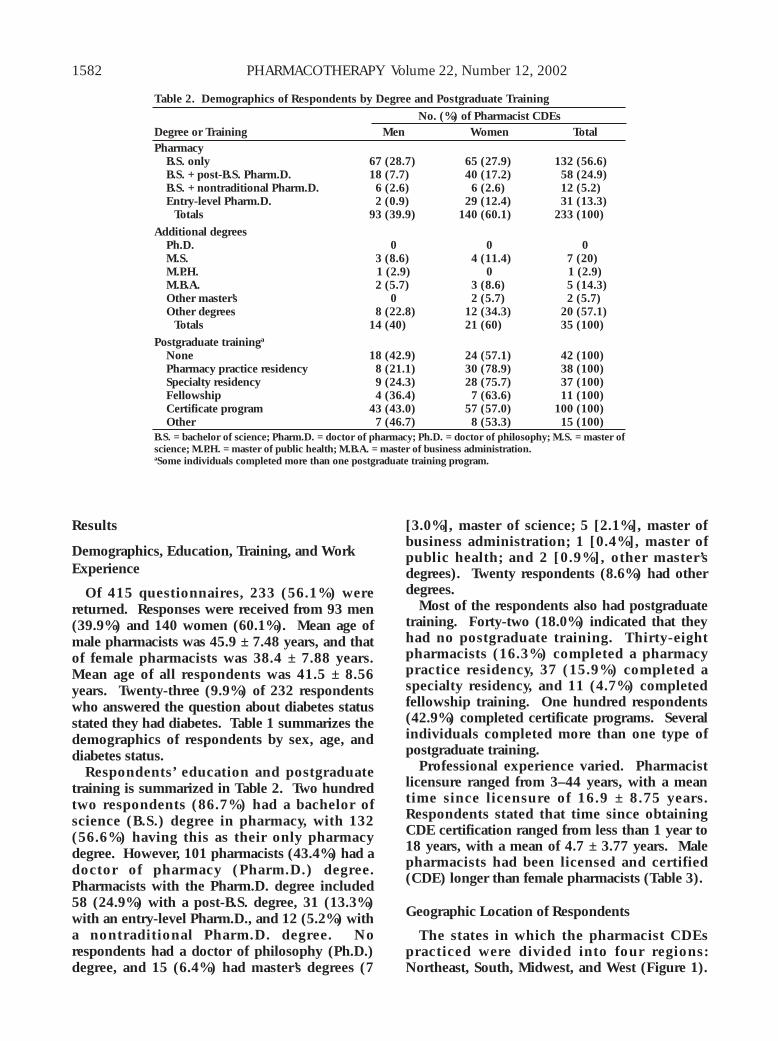
Respondents’ education and postgraduatetraining is summarized in Table 2. Two hundredtwo respondents (86.7%) had a bachelor ofscience (B.S.) degree in pharmacy, with 132(56.6%) having this as their only pharmacydegree. However, 101 pharmacists (43.4%) had adoctor of pharmacy (Pharm.D.) degree.Pharmacists with the Pharm.D. degree included58 (24.9%) with a post-B.S. degree, 31 (13.3%)with an entry-level Pharm.D., and 12 (5.2%) witha nontraditional Pharm.D. degree. Norespondents had a doctor of philosophy (Ph.D.)degree, and 15 (6.4%) had master’s degrees (7
[3.0%], master of science; 5 [2.1%], master ofbusiness administration; 1 [0.4%], master ofpublic health; and 2 [0.9%], other master’sdegrees). Twenty respondents (8.6%) had otherdegrees.
Most of the respondents also had postgraduatetraining. Forty-two (18.0%) indicated that theyhad no postgraduate training. Thirty-eightpharmacists (16.3%) completed a pharmacypractice residency, 37 (15.9%) completed aspecialty residency, and 11 (4.7%) completedfellowship training. One hundred respondents(42.9%) completed certificate programs. Severalindividuals completed more than one type ofpostgraduate training.
Professional experience varied. Pharmacistlicensure ranged from 3–44 years, with a meantime since licensure of 16.9 ± 8.75 years.Respondents stated that time since obtainingCDE certification ranged from less than 1 year to18 years, with a mean of 4.7 ± 3.77 years. Malepharmacists had been licensed and certified(CDE) longer than female pharmacists (Table 3).
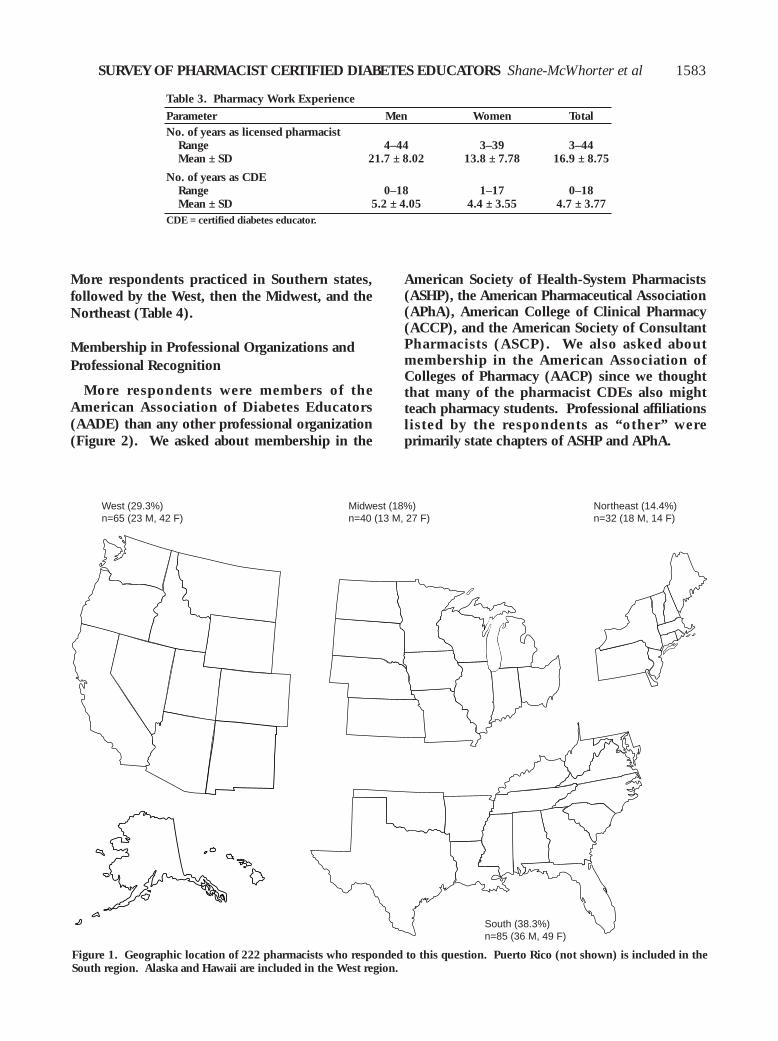
Geographic Location of Respondents
The states in which the pharmacist CDEspracticed were divided into four regions:Northeast, South, Midwest, and West (Figure 1).
1582
Table 2. Demographics of Respondents by Degree and Postgraduate Training
No. (%) of Pharmacist CDEsDegree or Training Men Women TotalPharmacy
B.S. only 67 (28.7) 65 (27.9) 132 (56.6)B.S. + post-B.S. Pharm.D. 18 (7.7) 40 (17.2) 58 (24.9)B.S. + nontraditional Pharm.D. 6 (2.6) 6 (2.6) 12 (5.2)Entry-level Pharm.D. 2 (0.9) 29 (12.4) 31 (13.3)
Totals 93 (39.9) 140 (60.1) 233 (100)
Additional degreesPh.D. 0 0 0M.S. 3 (8.6) 4 (11.4) 7 (20)M.P.H. 1 (2.9) 0 1 (2.9)M.B.A. 2 (5.7) 3 (8.6) 5 (14.3)Other master’s 0 2 (5.7) 2 (5.7)Other degrees 8 (22.8) 12 (34.3) 20 (57.1)
Totals 14 (40) 21 (60) 35 (100)
Postgraduate traininga
None 18 (42.9) 24 (57.1) 42 (100)Pharmacy practice residency 8 (21.1) 30 (78.9) 38 (100)Specialty residency 9 (24.3) 28 (75.7) 37 (100)Fellowship 4 (36.4) 7 (63.6) 11 (100)Certificate program 43 (43.0) 57 (57.0) 100 (100)Other 7 (46.7) 8 (53.3) 15 (100)
B.S. = bachelor of science; Pharm.D. = doctor of pharmacy; Ph.D. = doctor of philosophy; M.S. = master ofscience; M.P.H. = master of public health; M.B.A. = master of business administration.aSome individuals completed more than one postgraduate training program.
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
More respondents practiced in Southern states,followed by the West, then the Midwest, and theNortheast (Table 4).
Membership in Professional Organizations andProfessional Recognition
More respondents were members of theAmerican Association of Diabetes Educators(AADE) than any other professional organization(Figure 2). We asked about membership in the
American Society of Health-System Pharmacists(ASHP), the American Pharmaceutical Association(APhA), American College of Clinical Pharmacy(ACCP), and the American Society of ConsultantPharmacists (ASCP). We also asked aboutmembership in the American Association ofColleges of Pharmacy (AACP) since we thoughtthat many of the pharmacist CDEs also mightteach pharmacy students. Professional affiliationslisted by the respondents as “other” wereprimarily state chapters of ASHP and APhA.
1583
Table 3. Pharmacy Work Experience
Parameter Men Women TotalNo. of years as licensed pharmacist
Range 4–44 3–39 3–44Mean ± SD 21.7 ± 8.02 13.8 ± 7.78 16.9 ± 8.75
No. of years as CDERange 0–18 1–17 0–18Mean ± SD 5.2 ± 4.05 4.4 ± 3.55 4.7 ± 3.77
CDE = certified diabetes educator.
Figure 1. Geographic location of 222 pharmacists who responded to this question. Puerto Rico (not shown) is included in theSouth region. Alaska and Hawaii are included in the West region.
ME
West (29.3%)n=65 (23 M, 42 F)
Midwest (18%)n=40 (13 M, 27 F)
Northeast (14.4%)n=32 (18 M, 14 F)
South (38.3%)n=85 (36 M, 49 F)
PHARMACOTHERAPY Volume 22, Number 12, 2002
Many pharmacists had proven expertise inother areas as well as diabetes. Thirtypharmacists (12.9%) obtained board certificationin pharmacotherapy, one in psychiatry, and one
1584
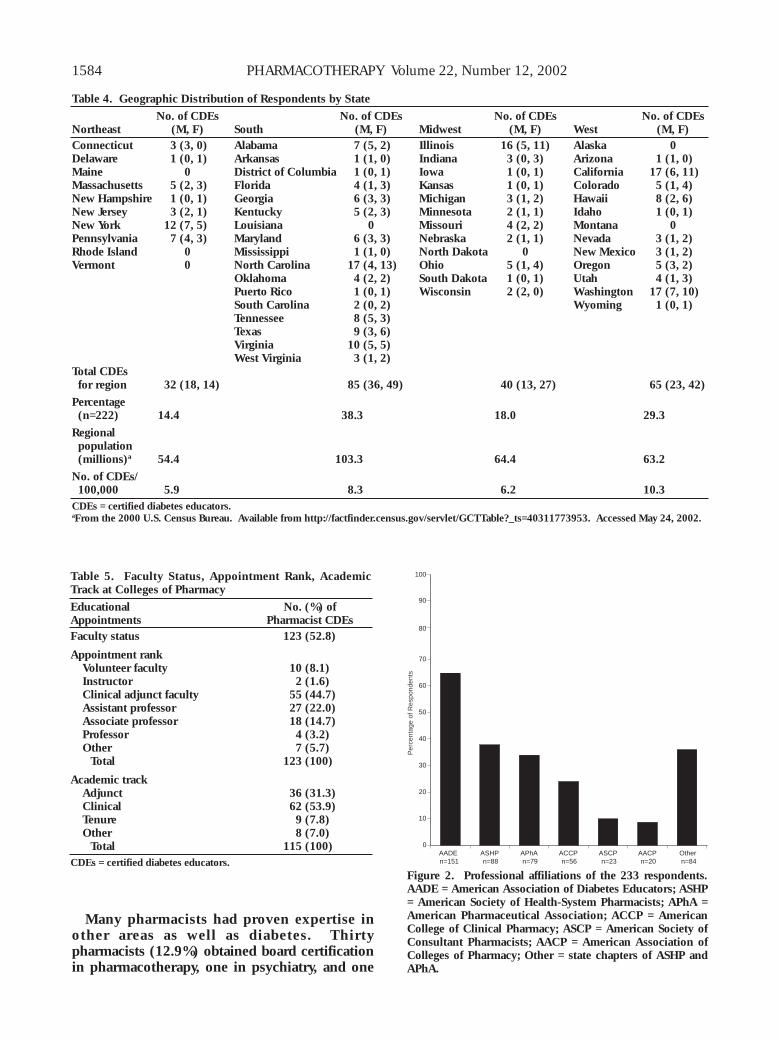
Table 4. Geographic Distribution of Respondents by State
No. of CDEs No. of CDEs No. of CDEs No. of CDEsNortheast (M, F) South (M, F) Midwest (M, F) West (M, F)Connecticut 3 (3, 0) Alabama 7 (5, 2) Illinois 16 (5, 11) Alaska 0Delaware 1 (0, 1) Arkansas 1 (1, 0) Indiana 3 (0, 3) Arizona 1 (1, 0)Maine 0 District of Columbia 1 (0, 1) Iowa 1 (0, 1) California 17 (6, 11)Massachusetts 5 (2, 3) Florida 4 (1, 3) Kansas 1 (0, 1) Colorado 5 (1, 4)New Hampshire 1 (0, 1) Georgia 6 (3, 3) Michigan 3 (1, 2) Hawaii 8 (2, 6)New Jersey 3 (2, 1) Kentucky 5 (2, 3) Minnesota 2 (1, 1) Idaho 1 (0, 1)New York 12 (7, 5) Louisiana 0 Missouri 4 (2, 2) Montana 0Pennsylvania 7 (4, 3) Maryland 6 (3, 3) Nebraska 2 (1, 1) Nevada 3 (1, 2)Rhode Island 0 Mississippi 1 (1, 0) North Dakota 0 New Mexico 3 (1, 2)Vermont 0 North Carolina 17 (4, 13) Ohio 5 (1, 4) Oregon 5 (3, 2)
Oklahoma 4 (2, 2) South Dakota 1 (0, 1) Utah 4 (1, 3)Puerto Rico 1 (0, 1) Wisconsin 2 (2, 0) Washington 17 (7, 10)South Carolina 2 (0, 2) Wyoming 1 (0, 1)Tennessee 8 (5, 3)Texas 9 (3, 6)Virginia 10 (5, 5)West Virginia 3 (1, 2)
Total CDEsfor region 32 (18, 14) 85 (36, 49) 40 (13, 27) 65 (23, 42)
Percentage(n=222) 14.4 38.3 18.0 29.3
Regionalpopulation(millions)a 54.4 103.3 64.4 63.2
No. of CDEs/100,000 5.9 8.3 6.2 10.3
CDEs = certified diabetes educators.aFrom the 2000 U.S. Census Bureau. Available from http://factfinder.census.gov/servlet/GCTTable?_ts=40311773953. Accessed May 24, 2002.
Figure 2. Professional affiliations of the 233 respondents.AADE = American Association of Diabetes Educators; ASHP= American Society of Health-System Pharmacists; APhA =American Pharmaceutical Association; ACCP = AmericanCollege of Clinical Pharmacy; ASCP = American Society ofConsultant Pharmacists; AACP = American Association ofColleges of Pharmacy; Other = state chapters of ASHP andAPhA.
AADE n=151
ASHP n=88
APhA n=79
ACCP n=56
ASCP n=23
AACP n=20
Other n=84
0
10
20
30
40
50
60
70
Per
cent
age
of R
espo
nden
ts
80
90
100Table 5. Faculty Status, Appointment Rank, AcademicTrack at Colleges of Pharmacy
Educational No. (%) ofAppointments Pharmacist CDEsFaculty status 123 (52.8)
Appointment rankVolunteer faculty 10 (8.1)Instructor 2 (1.6)Clinical adjunct faculty 55 (44.7)Assistant professor 27 (22.0)Associate professor 18 (14.7)Professor 4 (3.2)Other 7 (5.7)
Total 123 (100)
Academic trackAdjunct 36 (31.3)Clinical 62 (53.9)Tenure 9 (7.8)Other 8 (7.0)
Total 115 (100)CDEs = certified diabetes educators.
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
in nutrition support. Furthermore, several alsohad obtained recognition from differentprofessional organizations. Six pharmacists hadachieved fellowship status in ACCP, five in ASHP,four in ASCP, and three in APhA.
Educational Appointments at Colleges ofPharmacy
A total of 123 (52.8%) respondents had collegeof pharmacy faculty appointments. Mostrespondents were clinical adjunct faculty,whereas others had various faculty appointments.Faculty status, rank, and academic track arelisted in Table 5 for respondents who answeredthese questions.
Position Description
Of 216 responses, 167 pharmacists (77.3%)indicated their position as full time, and 49(22.7%) stated their position as part time.Responses varied for the percentage of timedevoted to diabetes care: 127 (61.1%) of 208respondents indicated 1–25% of their time wasdevoted to diabetes care activities; 46 (22.1%),26–50% of their time; 15 (7.2%), 51–75% of theirtime; and 20 (9.6%), 76–100% of their time.
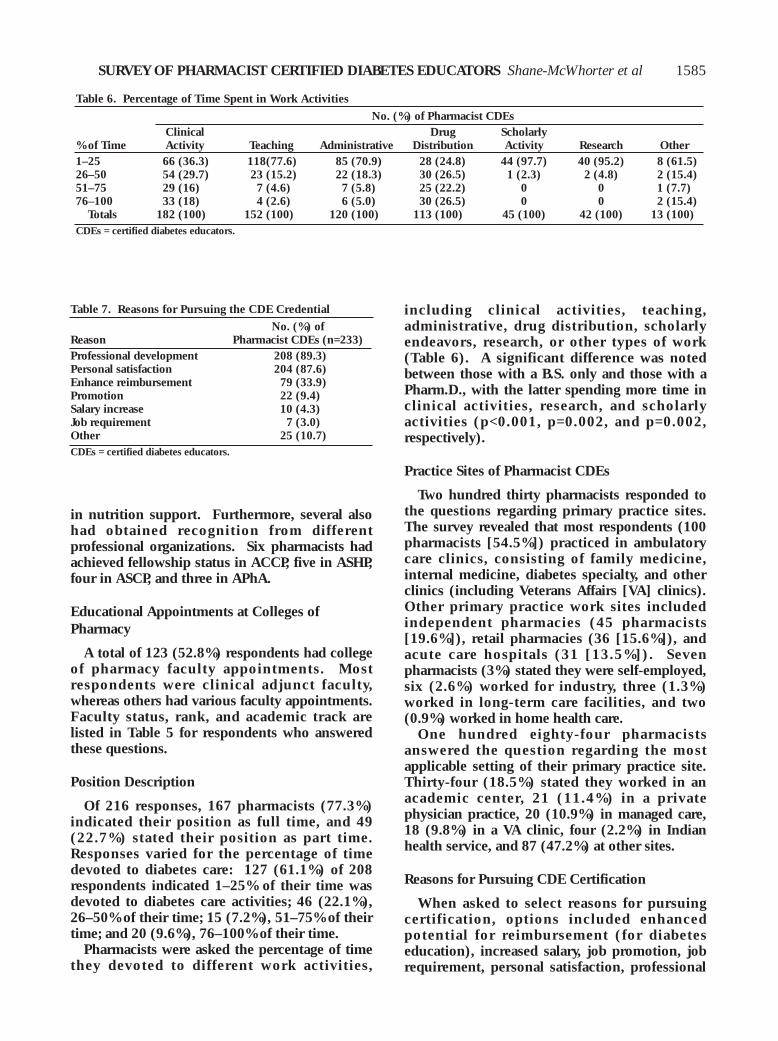
Pharmacists were asked the percentage of timethey devoted to different work activities,
including clinical activities, teaching,administrative, drug distribution, scholarlyendeavors, research, or other types of work(Table 6). A significant difference was notedbetween those with a B.S. only and those with aPharm.D., with the latter spending more time inclinical activities, research, and scholarlyactivities (p<0.001, p=0.002, and p=0.002,respectively).
Practice Sites of Pharmacist CDEs
Two hundred thirty pharmacists responded tothe questions regarding primary practice sites.The survey revealed that most respondents (100pharmacists [54.5%]) practiced in ambulatorycare clinics, consisting of family medicine,internal medicine, diabetes specialty, and otherclinics (including Veterans Affairs [VA] clinics).Other primary practice work sites includedindependent pharmacies (45 pharmacists[19.6%]), retail pharmacies (36 [15.6%]), andacute care hospitals (31 [13.5%]). Sevenpharmacists (3%) stated they were self-employed,six (2.6%) worked for industry, three (1.3%)worked in long-term care facilities, and two(0.9%) worked in home health care.
One hundred eighty-four pharmacistsanswered the question regarding the mostapplicable setting of their primary practice site.Thirty-four (18.5%) stated they worked in anacademic center, 21 (11.4%) in a privatephysician practice, 20 (10.9%) in managed care,18 (9.8%) in a VA clinic, four (2.2%) in Indianhealth service, and 87 (47.2%) at other sites.
Reasons for Pursuing CDE Certification
When asked to select reasons for pursuingcertification, options included enhancedpotential for reimbursement (for diabeteseducation), increased salary, job promotion, jobrequirement, personal satisfaction, professional
1585
Table 6. Percentage of Time Spent in Work Activities
No. (%) of Pharmacist CDEsClinical Drug Scholarly
% of Time Activity Teaching Administrative Distribution Activity Research Other1–25 66 (36.3) 118(77.6) 85 (70.9) 28 (24.8) 44 (97.7) 40 (95.2) 8 (61.5)26–50 54 (29.7) 23 (15.2) 22 (18.3) 30 (26.5) 1 (2.3) 2 (4.8) 2 (15.4)51–75 29 (16) 7 (4.6) 7 (5.8) 25 (22.2) 0 0 1 (7.7)76–100 33 (18) 4 (2.6) 6 (5.0) 30 (26.5) 0 0 2 (15.4)
Totals 182 (100) 152 (100) 120 (100) 113 (100) 45 (100) 42 (100) 13 (100)CDEs = certified diabetes educators.
Table 7. Reasons for Pursuing the CDE Credential
No. (%) ofReason Pharmacist CDEs (n=233)Professional development 208 (89.3)Personal satisfaction 204 (87.6)Enhance reimbursement 79 (33.9)Promotion 22 (9.4)Salary increase 10 (4.3)Job requirement 7 (3.0)Other 25 (10.7)CDEs = certified diabetes educators.
PHARMACOTHERAPY Volume 22, Number 12, 2002
development, or other reasons. The two mostcommonly cited reasons were professionaldevelopment and personal satisfaction (Table 7).
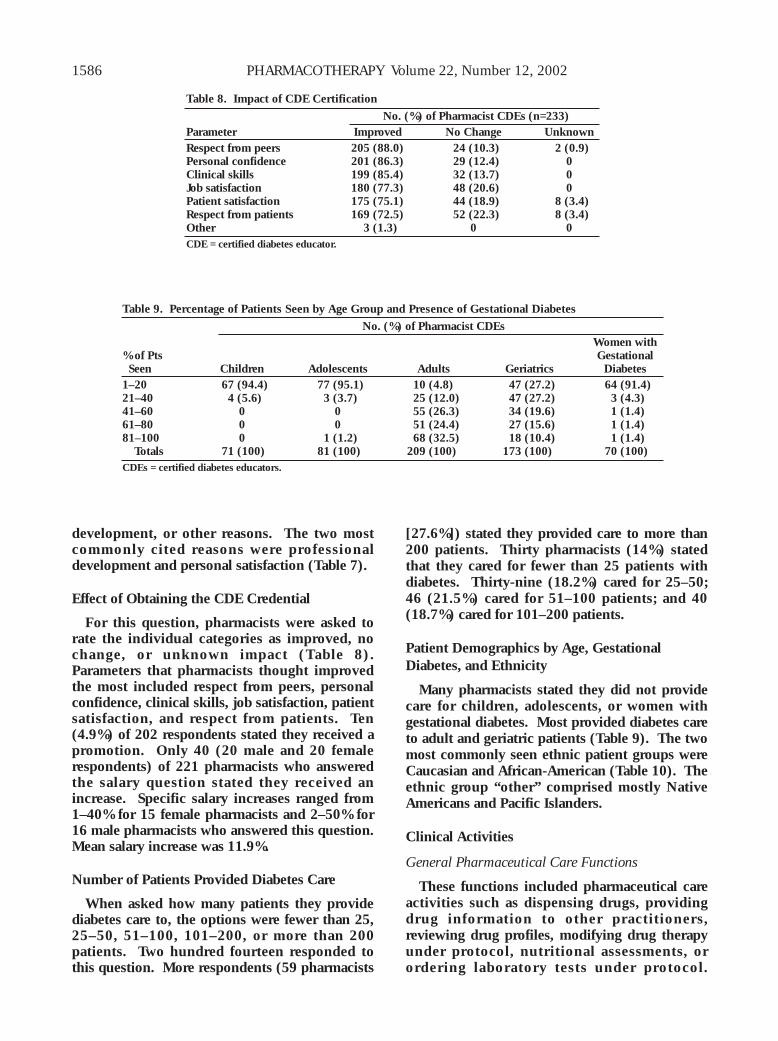
Effect of Obtaining the CDE Credential
For this question, pharmacists were asked torate the individual categories as improved, nochange, or unknown impact (Table 8).Parameters that pharmacists thought improvedthe most included respect from peers, personalconfidence, clinical skills, job satisfaction, patientsatisfaction, and respect from patients. Ten(4.9%) of 202 respondents stated they received apromotion. Only 40 (20 male and 20 femalerespondents) of 221 pharmacists who answeredthe salary question stated they received anincrease. Specific salary increases ranged from1–40% for 15 female pharmacists and 2–50% for16 male pharmacists who answered this question.Mean salary increase was 11.9%.
Number of Patients Provided Diabetes Care
When asked how many patients they providediabetes care to, the options were fewer than 25,25–50, 51–100, 101–200, or more than 200patients. Two hundred fourteen responded tothis question. More respondents (59 pharmacists
[27.6%]) stated they provided care to more than200 patients. Thirty pharmacists (14%) statedthat they cared for fewer than 25 patients withdiabetes. Thirty-nine (18.2%) cared for 25–50;46 (21.5%) cared for 51–100 patients; and 40(18.7%) cared for 101–200 patients.
Patient Demographics by Age, GestationalDiabetes, and Ethnicity
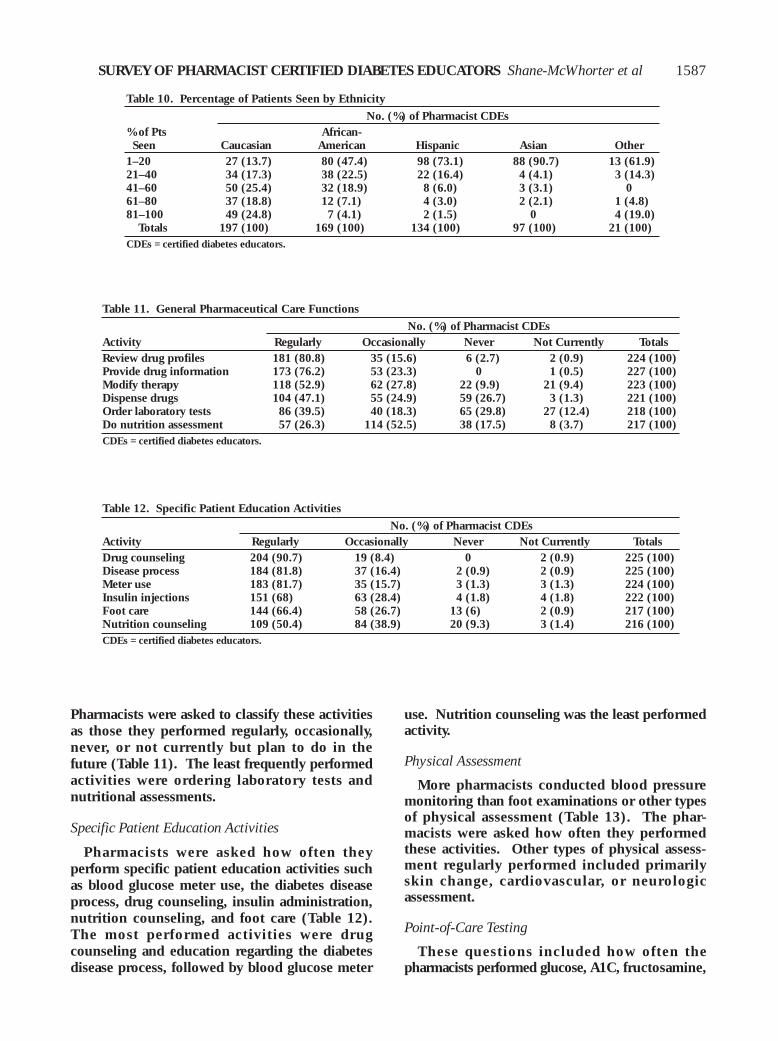
Many pharmacists stated they did not providecare for children, adolescents, or women withgestational diabetes. Most provided diabetes careto adult and geriatric patients (Table 9). The twomost commonly seen ethnic patient groups wereCaucasian and African-American (Table 10). Theethnic group “other” comprised mostly NativeAmericans and Pacific Islanders.
Clinical Activities
General Pharmaceutical Care Functions
These functions included pharmaceutical careactivities such as dispensing drugs, providingdrug information to other practitioners,reviewing drug profiles, modifying drug therapyunder protocol, nutritional assessments, orordering laboratory tests under protocol.
1586
Table 8. Impact of CDE Certification
No. (%) of Pharmacist CDEs (n=233)Parameter Improved No Change UnknownRespect from peers 205 (88.0) 24 (10.3) 2 (0.9)Personal confidence 201 (86.3) 29 (12.4) 0Clinical skills 199 (85.4) 32 (13.7) 0Job satisfaction 180 (77.3) 48 (20.6) 0Patient satisfaction 175 (75.1) 44 (18.9) 8 (3.4)Respect from patients 169 (72.5) 52 (22.3) 8 (3.4)Other 3 (1.3) 0 0CDE = certified diabetes educator.
Table 9. Percentage of Patients Seen by Age Group and Presence of Gestational Diabetes
No. (%) of Pharmacist CDEsWomen with
% of Pts GestationalSeen Children Adolescents Adults Geriatrics Diabetes
1–20 67 (94.4) 77 (95.1) 10 (4.8) 47 (27.2) 64 (91.4)21–40 4 (5.6) 3 (3.7) 25 (12.0) 47 (27.2) 3 (4.3)41–60 0 0 55 (26.3) 34 (19.6) 1 (1.4)61–80 0 0 51 (24.4) 27 (15.6) 1 (1.4)81–100 0 1 (1.2) 68 (32.5) 18 (10.4) 1 (1.4)
Totals 71 (100) 81 (100) 209 (100) 173 (100) 70 (100)CDEs = certified diabetes educators.
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
Pharmacists were asked to classify these activitiesas those they performed regularly, occasionally,never, or not currently but plan to do in thefuture (Table 11). The least frequently performedactivities were ordering laboratory tests andnutritional assessments.
Specific Patient Education Activities
Pharmacists were asked how often theyperform specific patient education activities suchas blood glucose meter use, the diabetes diseaseprocess, drug counseling, insulin administration,nutrition counseling, and foot care (Table 12).The most performed activities were drugcounseling and education regarding the diabetesdisease process, followed by blood glucose meter
use. Nutrition counseling was the least performedactivity.
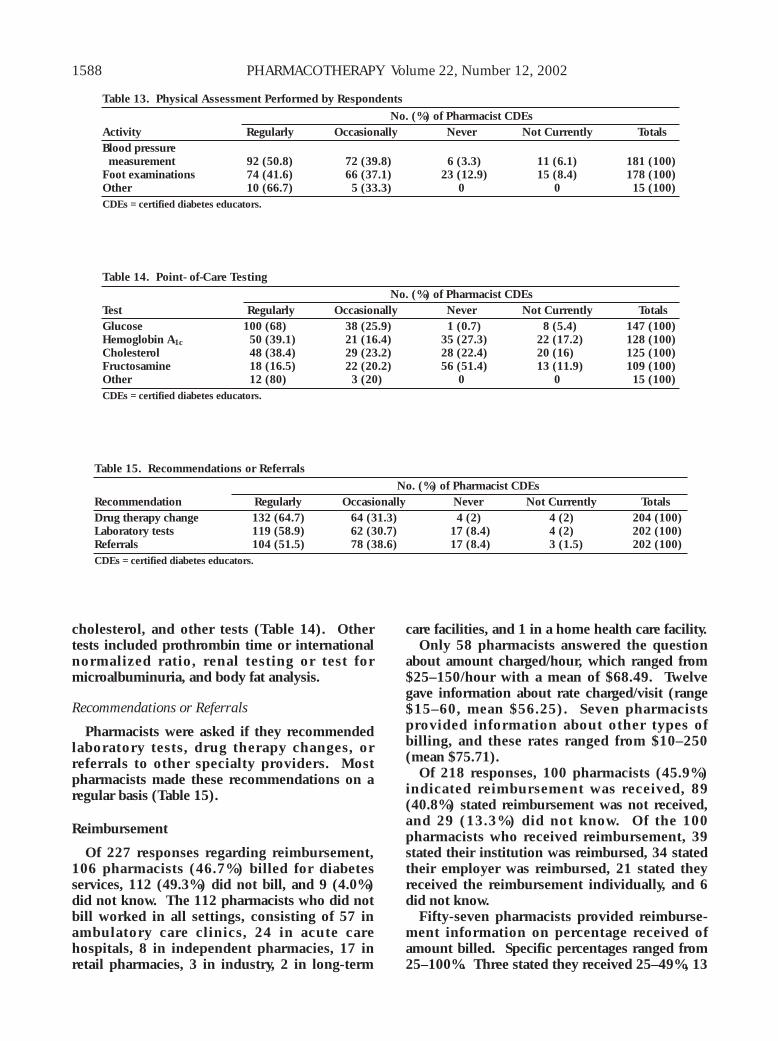
Physical Assessment
More pharmacists conducted blood pressuremonitoring than foot examinations or other typesof physical assessment (Table 13). The phar-macists were asked how often they performedthese activities. Other types of physical assess-ment regularly performed included primarilyskin change, cardiovascular, or neurologicassessment.
Point-of-Care Testing
These questions included how often thepharmacists performed glucose, A1C, fructosamine,
1587
Table 10. Percentage of Patients Seen by Ethnicity
No. (%) of Pharmacist CDEs% of Pts African-Seen Caucasian American Hispanic Asian Other
1–20 27 (13.7) 80 (47.4) 98 (73.1) 88 (90.7) 13 (61.9)21–40 34 (17.3) 38 (22.5) 22 (16.4) 4 (4.1) 3 (14.3)41–60 50 (25.4) 32 (18.9) 8 (6.0) 3 (3.1) 061–80 37 (18.8) 12 (7.1) 4 (3.0) 2 (2.1) 1 (4.8)81–100 49 (24.8) 7 (4.1) 2 (1.5) 0 4 (19.0)
Totals 197 (100) 169 (100) 134 (100) 97 (100) 21 (100)CDEs = certified diabetes educators.
Table 11. General Pharmaceutical Care Functions
No. (%) of Pharmacist CDEsActivity Regularly Occasionally Never Not Currently TotalsReview drug profiles 181 (80.8) 35 (15.6) 6 (2.7) 2 (0.9) 224 (100)Provide drug information 173 (76.2) 53 (23.3) 0 1 (0.5) 227 (100)Modify therapy 118 (52.9) 62 (27.8) 22 (9.9) 21 (9.4) 223 (100)Dispense drugs 104 (47.1) 55 (24.9) 59 (26.7) 3 (1.3) 221 (100)Order laboratory tests 86 (39.5) 40 (18.3) 65 (29.8) 27 (12.4) 218 (100)Do nutrition assessment 57 (26.3) 114 (52.5) 38 (17.5) 8 (3.7) 217 (100)CDEs = certified diabetes educators.
Table 12. Specific Patient Education Activities
No. (%) of Pharmacist CDEsActivity Regularly Occasionally Never Not Currently TotalsDrug counseling 204 (90.7) 19 (8.4) 0 2 (0.9) 225 (100)Disease process 184 (81.8) 37 (16.4) 2 (0.9) 2 (0.9) 225 (100)Meter use 183 (81.7) 35 (15.7) 3 (1.3) 3 (1.3) 224 (100)Insulin injections 151 (68) 63 (28.4) 4 (1.8) 4 (1.8) 222 (100)Foot care 144 (66.4) 58 (26.7) 13 (6) 2 (0.9) 217 (100)Nutrition counseling 109 (50.4) 84 (38.9) 20 (9.3) 3 (1.4) 216 (100)CDEs = certified diabetes educators.
PHARMACOTHERAPY Volume 22, Number 12, 2002
cholesterol, and other tests (Table 14). Othertests included prothrombin time or internationalnormalized ratio, renal testing or test formicroalbuminuria, and body fat analysis.
Recommendations or Referrals
Pharmacists were asked if they recommendedlaboratory tests, drug therapy changes, orreferrals to other specialty providers. Mostpharmacists made these recommendations on aregular basis (Table 15).
Reimbursement
Of 227 responses regarding reimbursement,106 pharmacists (46.7%) billed for diabetesservices, 112 (49.3%) did not bill, and 9 (4.0%)did not know. The 112 pharmacists who did notbill worked in all settings, consisting of 57 inambulatory care clinics, 24 in acute carehospitals, 8 in independent pharmacies, 17 inretail pharmacies, 3 in industry, 2 in long-term
care facilities, and 1 in a home health care facility. Only 58 pharmacists answered the question
about amount charged/hour, which ranged from$25–150/hour with a mean of $68.49. Twelvegave information about rate charged/visit (range$15–60, mean $56.25). Seven pharmacistsprovided information about other types ofbilling, and these rates ranged from $10–250(mean $75.71).
Of 218 responses, 100 pharmacists (45.9%)indicated reimbursement was received, 89(40.8%) stated reimbursement was not received,and 29 (13.3%) did not know. Of the 100pharmacists who received reimbursement, 39stated their institution was reimbursed, 34 statedtheir employer was reimbursed, 21 stated theyreceived the reimbursement individually, and 6did not know.
Fifty-seven pharmacists provided reimburse-ment information on percentage received ofamount billed. Specific percentages ranged from25–100%. Three stated they received 25–49%, 13
1588
Table 13. Physical Assessment Performed by Respondents
No. (%) of Pharmacist CDEsActivity Regularly Occasionally Never Not Currently TotalsBlood pressuremeasurement 92 (50.8) 72 (39.8) 6 (3.3) 11 (6.1) 181 (100)
Foot examinations 74 (41.6) 66 (37.1) 23 (12.9) 15 (8.4) 178 (100)Other 10 (66.7) 5 (33.3) 0 0 15 (100)CDEs = certified diabetes educators.
Table 14. Point- of-Care Testing
No. (%) of Pharmacist CDEsTest Regularly Occasionally Never Not Currently TotalsGlucose 100 (68) 38 (25.9) 1 (0.7) 8 (5.4) 147 (100)Hemoglobin A1c 50 (39.1) 21 (16.4) 35 (27.3) 22 (17.2) 128 (100)Cholesterol 48 (38.4) 29 (23.2) 28 (22.4) 20 (16) 125 (100)Fructosamine 18 (16.5) 22 (20.2) 56 (51.4) 13 (11.9) 109 (100)Other 12 (80) 3 (20) 0 0 15 (100)CDEs = certified diabetes educators.
Table 15. Recommendations or Referrals
No. (%) of Pharmacist CDEsRecommendation Regularly Occasionally Never Not Currently TotalsDrug therapy change 132 (64.7) 64 (31.3) 4 (2) 4 (2) 204 (100)Laboratory tests 119 (58.9) 62 (30.7) 17 (8.4) 4 (2) 202 (100)Referrals 104 (51.5) 78 (38.6) 17 (8.4) 3 (1.5) 202 (100)CDEs = certified diabetes educators.

SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
received 50–79%, and 41 received 80–100% ofamount billed.
System for Measuring Outcomes
Of 226 responses to this question, 129pharmacists (57.1%) stated they had a system inplace for measuring outcomes, 84 (37.1%) hadno system, and 13 (5.8%) did not know.Outcomes measurements included trackingspecific clinical parameters such as A1C, lipids,and blood pressure; frequency of self-monitoringof blood glucose levels; testing before and afterdiabetes education; behavioral outcomes; patientsatisfaction surveys; chart reviews and drugadministration evaluations; hospitalizations oremergency department visits; and missedworkdays. Several respondents indicated theyused spreadsheets or computer databases fortracking outcomes.
Future Credentialing and Recommendation toOther Pharmacists
Of 231 responses, 195 pharmacists (84.4%)stated they planned to pursue recertification as aCDE. However, 30 (13%) were unsure, and 6(2.6%) stated they were not planning to pursueCDE recertification. When asked if theyrecommended CDE credentialing to otherpharmacists interested in providing diabetes care,209 (90.5%) of 231 stated yes, 16 (6.9%) wereunsure, and 6 (2.6%) stated no.
When queried about BC-ADM credentialing,47 (20.5%) of 230 respondents stated they wouldapply to obtain this credential, 70 (30.4%) statedthey would not, and 113 (49.1%) stated theywere unsure.
Discussion
Pharmacists have been involved in diabetescare and education for many years. Severalreports of pharmacists providing diabetes patientcare and monitoring have been published, withsome reports including community pharmaciesas the site of diabetes education.43–46 In thesestudies, pharmacists have looked at baseline andfollow-up blood glucose values, as well asadherence to diabetes drugs,43 monitoring ofadverse drug-related events, evaluation of patientunderstanding of diabetes, and quality-of-lifeevaluations.44 Clinical parameters such as A1C,blood pressure, and lipids also have beentracked.45 Monetary savings were reported in theAsheville, North Carolina, project in which
community pharmacists saved the city more than$900/patient/year on diabetes care.46 In VAclinics, pharmacist-based diabetes programs inwhich insulin was started and adjusted alsoreported cost savings, as well as improvedglycemic parameters.47 Other studies conductedin pharmacist-based programs in a university-based outpatient clinic48 and a primary careclinic49 showed improved clinical parameters inboth studies and 99% adherence to AmericanDiabetes Association standards as well as lowerA1C versus regular physician care in the latterstudy. Even in an indigent care clinic,pharmacist-managed patients with diabetes had asignificantly greater decline in A1C from baselinethan that of patients in a general clinic.50 Manyof these published reports involved pharmacistswho are CDEs.
The results of a recent study in Canadaindicate that pharmacists agree they should bepart of the diabetes management team andshould be required to have specialized training toprovide diabetes care.51 In a recent survey inArizona, however, pharmacists’ attitudes towarddiabetes indicated that they believe diabetes is atreatable disease, but they do not frequentlyprovide diabetes education.52 The authorsspeculated a reason for not providing educationis that pharmacists may believe they haveinsufficient training to educate patients. Theauthors also acknowledged that more diabeteseducation through community pharmacists isneeded.
Extensive information about pharmacist CDEsis not readily available. Providing details aboutthese individuals and their clinical activities maymotivate other pharmacists to pursue the CDEcredential. Because pharmacists are often themost accessible of all health care providers,obtaining the credential may be an importantcontribution to diabetes care and education.People with diabetes see their pharmacists 7times more often than they see their primary carephysician.53 An encouraging factor is that thereare over 400 pharmacists with this training.These individuals are uniquely positioned tomentor other pharmacists to become CDEs andincrease the number of readily accessiblepharmacist educators to patients with diabetes.
Our survey indicated that the mean age of thepharmacists was 41.5 years and 56.6% have a B.S.degree only, whereas 43.4% have a Pharm.D.Overall, pharmacists had been licensed for anaverage of 17 years and had been a CDE for anaverage of 5 years, although there were some
1589
PHARMACOTHERAPY Volume 22, Number 12, 2002
differences between the sexes. For instance,more than half the CDE pharmacists are women(60.1%) who are a few years younger than themale pharmacists (38 vs 46 yrs) and had beenlicensed pharmacists for a shorter time (14 vs 22yrs). However, they had been CDEs for only aslightly shorter time (4.4 vs 5.2 yrs).
Respondents practice mostly in Southern andWestern states. The states with the largestnumber of CDE respondents were Washington,California, North Carolina, New York, andVirginia. However, many states had no CDEs,including Alaska, Rhode Island, Maine, Vermont,Montana, North Dakota, and Louisiana, a statewith a large number of individuals with diabetes.Also, many states had only one CDE, includingArkansas, Arizona, Delaware, Iowa, Idaho,Kansas, Mississippi, New Hampshire, SouthDakota, Wyoming, Puerto Rico, and District ofColumbia. This should be a call to action forpharmacists to increase the number of CDEs inthese states. The ratio of pharmacist CDEs topatient population is only 0.6–1 pharmacistCDEs:million people.
Respondents reported membership in severalprofessional organizations. A large percentage(65%) were members of AADE, which is animportant organization for CDEs. Pharmacistsshould maintain an active presence in thisorganization, so they can network with otherCDEs from different disciplines and seekcontinuing education opportunities. The threeother major organizations to which respondentshad memberships were ASHP, APhA, and ACCP,although a few also belong to ASCP and AACP.
Respondents included several individuals whohave pursued many opportunities to increasetheir learning and training. Most had completedpostgraduate training, including residency orfellowship training, and several had completedmore than one type of postgraduate training.Specifically, of the 38 individuals who hadcompleted a pharmacy practice residency, 12 alsocompleted a specialty residency, 7 also completeda certificate program, one also did a fellowship,and another person also completed another typeof postgraduate program.
Over half the respondents had facultyappointments at colleges of pharmacy. Thisgroup may help to inculcate an interest inpharmacists in training to also become CDEs. Asshown by the geographic distribution ofrespondents, many areas do not have pharmacistCDEs, and these may be particularly importantareas to target.
Most respondents practiced in ambulatory careclinics and independent or retail pharmacies.This is also an important finding because thesepharmacists are highly visible and readilyavailable to promote patient education. However,for the number of pharmacists in inpatientsettings, this may provide an opportunity to referpatients for follow-up with pharmacists inoutpatient settings.
Major reasons for credentialing were personalsatisfaction or professional development,although enhanced reimbursement also wascited. Impact of certification included improvedclinical skills, job satisfaction, patient satisfactionand respect, as well as improved personalconfidence and respect from peers.
More pharmacists stated they provideddiabetes care to more than 200 patients who wereprimarily adult or geriatric patients and wereCaucasian or African-American. Few pharmacistswere involved with children, adolescents, andwomen with gestational diabetes. The mostfrequently provided pharmaceutical carefunctions included reviewing drug profiles,providing drug information to other practi-tioners, and modifying drug therapy. Educationactivities most commonly provided includeddrug counseling, blood glucose meter education,and information about the diabetes diseaseprocess, insulin administration, and foot care.Physical assessments most frequently performedincluded blood pressure monitoring and footexaminations. Most commonly provided point-of-care tests were for glucose, cholesterol, andA1C. Common recommendations were made fordrug therapy changes and obtaining laboratorytests. A total of 47% of the pharmacists statedthey billed for diabetes services, and 46% statedthat reimbursement was received. Over half ofthe pharmacists stated they had a system in placefor measuring outcomes.
Many pharmacists were not doing assessmentsor providing information in areas that are crucialto effective behavioral change in diabeteseducation. Specifically, 17.5% stated they did notperform nutritional assessments and 38.9% onlyoccasionally provided nutrition counseling.However, respondents were not afforded anopportunity to state the reason. The reason forthe large number not providing this type ofeducation may be that they may work as part of amultidisciplinary team in which nutritionistsprovide this information. Furthermore, surveyresponses were not received from manyindividuals, and these persons may be providing
1590
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
this education. Thus, it is difficult to state thatthese activities are typical of all pharmacistCDEs. Nevertheless, a CDE should be able toassess a patient’s nutritional status. An importantmessage is that if these pharmacists were notproviding nutrition education because they lackappropriate training, these skills may beenhanced.14 Furthermore, 16.4% stated they onlyoccasionally and 0.9% never discussed thedisease process of diabetes. Only 26.7%occasionally and 6% never discussed foot care.Again, these issues are important, particularlyfoot care since studies have shown thataddressing this as an education point mayprevent lower extremity amputation.23, 25, 27 Onepossible explanation for not adequatelyaddressing this issue was if podiatrists were partof the multidisciplinary team.
There are many challenges for pharmacists inthe management of patients with diabetes,including obtaining appropriate training,gathering data that support improved clinicaloutcomes, and securing provider recognition byMedicare, which would allow reimbursement.Options for pharmacists to provide diabeteseducation include preparation for the CDEexamination, the BC-ADM examination, andcertificate training programs. Most pharmacistssurveyed stated that they planned to pursue CDErecertification. Approximately 20% of thepharmacists stated they intended to apply for thenew advanced credential, BC-ADM.
The BC-ADM is a multidisciplinary credential,developed by the AADE and the AmericanNurses Credentialing Center, in collaborationwith the American Diabetes Association, theAmerican Dietetic Association, and the APhA.54
This is the first advanced practice certification indiabetes care emphasizing clinical assessmentand disease-state management. A separatecertification examination is offered for registerednurses, registered dietitians, and pharmacists.The new certification differs from the CDE inthat it focuses on advanced management issuesand an advanced degree is required before onemay sit for the examination. The BC-ADMexamination was offered for the first time in2001. Of the 164 health professionals who wereawarded this credential, 126 were registerednurses and nurse practitioners, 32 wereregistered dietitians, and 6 were pharmacists.
Certificate programs are an additional optionfor pharmacists to obtain diabetes training.These are programs offered by colleges ofpharmacy, state and national pharmacy
organizations, and the pharmaceutical industry.The programs are intended to upgrade clinicalskills and knowledge of practicing pharmacistswho are interested in expanding their practice toinclude patients with diabetes.
There are several limitations of this survey.Choices provided in the survey for clinicalactivities may not reflect all activities performedby pharmacist CDEs. Recall bias may haveoccurred on certain questions, such as the ageand ethnicity of patients or the types of activitiesperformed. Another example of recall bias mayhave occurred when respondents were asked howlong they had been a CDE. One individualanswered 18 years and another 17 years, yet thefirst CDE examination was given in 1986.42
Respondents who did not bill for their serviceswere not given an opportunity to explain whythey did not seek reimbursement. The surveydid not query whether anyone worked inindigent or free clinics. In the questions onpoint-of-care testing, the survey did notdistinguish whether the pharmacists themselveswere doing the testing, reviewing the data, orboth. The survey did not provide sufficientdiscrete choices for measuring outcomes.Respondents were not provided an opportunityto state why they would or would not pursueCDE recertification and why they would orwould not recommend CDE credentialing toother pharmacists.
Strengths of the survey include the number ofrespondents and the variety of questions therespondents answered. Another strength iscalling attention to the large number ofpharmacists who are CDEs, as well as to theirprofessional affiliations. This may establishmentoring opportunities for other pharmaciststhrough membership in different professionalorganizations. Describing the education andpostgraduate training also emphasizes thecharacteristics of individuals who are highlymotivated, and perhaps this is what is required toovercome the many difficult obstacles inbecoming a CDE. Nevertheless, these individualshave shown it is possible to overcome theobstacles. Delineating where these pharmacistsare located is another strength, since this mayhelp increase their referral base and promotepatients’ access to diabetes care. Callingattention to the variety of clinical activities mayhelp enhance awareness of the pharmacist as aprovider of diabetes education. Another strengthwas calling attention to the large number that arebilling and obtaining reimbursement for diabetes
1591

PHARMACOTHERAPY Volume 22, Number 12, 2002
services and emphasizing that almost half havesystems in place for measuring outcomes.
Although recent articles have provided someinformation on economic evaluation ofpharmacist involvement in diabetes care,46, 47, 55–57
more studies are needed that assess the long-termeconomic impact of pharmacist-provideddiabetes care. More studies than those availableon patients’ knowledge of self-care58 or those thatassess patients’ knowledge about their drugs59 orimpact of pharmacists on patients’ knowledgeand compliance with drugs60 are needed.Another necessary study is one comparingpatient outcomes when care is provided bypharmacist CDEs versus non-CDE pharmacisteducators. Our survey indicated that pharmacistsare providing little or no care to Hispanics, AsianAmericans, children, adolescents, and womenwith gestational diabetes. Further study isneeded to assess pharmacist care in these targetpopulations. Other potential studies are thosethat address the impact of patients’ satisfactionwith pharmacist care or pharmacist impact onpatients’ quality of life.
Conclusions
Many pharmacists CDEs in the United Statesprovide care to patients with diabetes. Most haveextensive postgraduate training and belong to avariety of professional organizations, and overhalf have faculty appointments at colleges ofpharmacy. Most of these pharmacists arepracticing in outpatient settings and are not onlyproviding numerous clinical services, but alsohave systems in place for tracking outcomes, andare billing and obtaining reimbursement for theseactivities. It is hoped that by providing detailsabout these pharmacist CDEs, other pharmacistswill be motivated to pursue this credential.
Acknowledgment
The authors thank Mr. Richard H. Shane for hisvaluable advice and technical assistance in thepreparation of this manuscript.
References1. The Diabetes Control and Complications Trial Research
Group. The effects of intensive treatment of diabetes on thedevelopment and progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl J Med1993;329:977–86.
2. UK Prospective Diabetes Study (UKPDS) Group. Intensiveblood-glucose control with sulphonylureas or insulin comparedwith conventional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lancet1998;352:837–53.
3. UK Prospective Diabetes Study (UKPDS) Group. Effect ofintensive blood-glucose control with metformin oncomplications in overweight patients with type 2 diabetes(UKPDS 34). Lancet 1998;352:854–65.
4. Stratton IM, Adler AI, Neil Ha, et al. Association of glycaemiawith macrovascular and microvascular complications of type 2diabetes (UKPDS 35): prospective observational study. BMJ2000;321:405–12.
5. The Diabetes Control and Complications Trial/Epidemiologyof Diabetes Interventions and Complications ResearchGroup. Retinopathy and nephropathy in patients with type 1diabetes four years after a trial of intensive therapy. N Engl JMed 2000;342:381–9.
6. Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulintherapy prevents the progression of diabetic microvascularcomplications in Japanese patients with non-insulin-dependentdiabetes mellitus: a randomized prospective 6-year study.Diabetes Res Clin Pract 1995;28:103–17.
7. Centers for Disease Control and Prevention. Public healthresource. National estimates on diabetes. Available fromhttp://www.cdc.gov/diabetes/pubs/factsheet.htm. Accessed June21, 2002.
8. Clark CM Jr. How should we respond to the worldwidediabetes epidemic? Diabetes Care 1998;21:475–6.
9. Burke JP, Williams K, Gaskill SP, Hazuda HP, Haffner SM,Stern MP. Rapid rise in the incidence of type 2 diabetes from1987 to 1996: results from the San Antonio heart study. ArchIntern Med 1999;159:1450–6.
10. American Diabetes Association. Economic consequences ofdiabetes mellitus in the U.S. in 1997. Diabetes Care1998;21:296–309.
11. Hodgson T, Cohen AJ. Medical care expenditures for diabetes,its chronic complications and its comorbidities. Prev Med1999;29:173–86.
12. Centers for Disease Control and Prevention . Diabetessurveillance, 1999. Chapter 1: the public health burden ofdiabetes mellitus in the United States. Available fromhttp://www.cdc.gov/diabetes/statistics/survl99/chap1/preventive.htm. Accessed June 21, 2002.
13. Lorenz RA, Bubb J, Davis D, et al. Changing behavior:practical lessons from the diabetes control and complicationstrial. Diabetes Care 1996;19:648–52.
14. Ockene JK, Ockene IS, Quirk ME, et al. Physician training forpatient-centered nutrition counseling in a lipid interventiontrial. Prev Med 1995;24:563–70.
15. Baxley SG, Brown ST, Pokorny ME, Swanson MS. Perceivedcompetence and actual level of knowledge of diabetes mellitusamong nurses. J Nurs Staff Dev 1997;13:93–8.
16. Ruby KL, Blainey CA, Haas LB, Patrick M. The knowledge andpractices of registered nurse, certified diabetes educators:teaching elderly clients about exercise. Diabetes Educ1993;19:299–306.
17. Jayne RL, Rankin SH. Revisiting nurse knowledge aboutdiabetes: an update and implications for practice. DiabetesEduc 1993;19:497–502.
18. Stetson BA, Pichert JW, Roach RR, Lorenz RA, Boswell EJ,Schlundt DG. Registered dietitians’ teaching and adherencepromotion skills during routine patient education. Patient EducCouns 1992;19:273–80.
19. Anderson RM, Donnelly MB, Funnell MM, Johnson PD. Thecontinuing education needs of diabetes nurse educators. JContin Educ Nurs 1991;22:163–6.
20. Campbell EM, Redman S, Moffitt PS, Sanson-Fisher RW. Therelative effectiveness of educational and behavioral instructionprograms for patients with NIDDM: a randomized trial.Diabetes Educ 1996;22:379–86.
21. Anderson RM, Donnelly MB, Gressard CP. The attitudes ofnurses, dietitians, and physicians toward diabetes. DiabetesEduc 1991;17:261–8.
22. Young-Hyman D. Provider impact in diabetes education: whatwe know, what we would like to know, paradigms for asking.Diabetes Educ 1999;25(suppl 6):34–42.
23. Boulton AJ. Why bother educating the multi-disciplinary team
1592
SURVEY OF PHARMACIST CERTIFIED DIABETES EDUCATORS Shane-McWhorter et al
and the patient? The example of prevention of lower extremityamputation in diabetes. Patient Educ Couns 1995;26:183–8.
24. Drass JA, Muir-Nash J, Boykin P, Turek J, Baker K. Perceivedand actual level of knowledge of diabetes mellitus amongnurses. Diabetes Care 1989;12:351–6.
25. Litzelman DK, Slemenda CW, Langefeld CD, et al. Reductionof lower extremity clinical abnormalities in patients with non-insulin-dependent diabetes mellitus: a randomized, controlledtrial. Ann Intern Med 1993;119:36–41.
26. Scheiderich SD, Freibaum CN, Peterson LM. Registerednurses’ knowledge about diabetes mellitus. Diabetes Care1983;6:57–61.
27. Wooldridge J, Bergeron J, Thornton C. Preventing diabeticfoot disease: lessons from the Medicare shoe demonstration.Am J Public Health 1996;86:935–8.
28. Cypress M, Wylie-Rosett J, Engel SS, Stager TB. The scope ofpractice of diabetes educators in a metropolitan area. DiabetesEduc 1992;18:111–14.
29. Grey M, Boland EA, Davidson M, Yu C, Tamborlane WV.Coping skills training for youths with diabetes on intensivetherapy. Appl Nurs Res 1999;12:3–12.
30. Kaufman MW, All AC, Davis H. The scope and practice ofdiabetes educators in the state of Georgia. Diabetes Educ1999;25:56–63.
31. Stott NCH, Rees M, Rollnick S, Pill RM, Hackett P .Professional responses to innovation in clinical method:diabetes care and negotiating skills. Patient Educ Couns1996;29:67–73.
32. Assal JP, Jacquemet S, Morel Y. The added value of therapy indiabetes: the education of patients for self-management of theirdisease. Metabolism 1997;46:61–4.
33. Greene DS, Beaudin BP, Bryan JM. Addressing attitudes duringdiabetes education: suggestions from adult education. DiabetesEduc 1991;17:470–3.
34. Lorenz RA. Teaching skills of health professionals. DiabetesEduc 1989;15:149–52.
35. Maldonato A, Bloise D, Ceci M, Fraticelli E, Fallucca F.Diabetes mellitus: lessons from patient education. Patient EducCouns 1995;26:57–66.
36. Moriarty D, Stephens L. Factors that influence diabetes patientteaching performed by hospital staff nurses. Diabetes Educ1990;16:31–5.
37. Brown SL, Pope JF, Hunt AE, Tolman NM. Motivationalstrategies used by dietitians to counsel individuals withdiabetes. Diabetes Educ 1998;24:313–18.
38. Pill R, Stot NC, Rollnick SR, Rees M. A randomized controlledtrial of an intervention designed to improve the care given ingeneral practice to type II diabetic patients: patient outcomesand professional ability to change behavior. Fam Pract1998;15:229–35.
39. American Association of Diabetes Educators. The 1999 scopeof practice for diabetes educators and the standards of practicefor diabetes educators. Diabetes Educ 2000;26:519–25.
40. American Diabetes Association . Clinical practicerecommendations 2002: national standards for diabetes self-management education. Diabetes Care 2002;25(suppl1):S140–7.
41. National Certification Board for Diabetes Educators.
Eligibility requirements for CDE. Available fromhttp://www.ncbde.org/eligibilityreq.html. Accessed May 13,2002.
42. National Certification Board for Diabetes Educators. NCBDEnews: a publication of the National Certification Board forDiabetes Educators. Winter/Spring 2002;12:7.
43. Berringer R, Shibley MCH, Cary C, Pugh CB, Powers PAG,Rafi JA. Outcomes of a community pharmacy-based diabetesmonitoring program. J Am Pharm Assoc 1999;39:791–7.
44. Baran RW, Crumlish K, Patterson H, et al. Improvingoutcomes of community-dwelling older patients with diabetesthrough pharmacist counseling. Am J Health-Syst Pharm1999;56:1535–9.
45. Nau DP, Ponte CD. Effects of a community pharmacist–baseddiabetes patient–management program on intermediate clinicaloutcome measures. J Managed Care Pharm 2001;8:48–53.
46. Cranor C. Ouctomes of the Asheville diabetes project. PharmTimes October 1998;(suppl):19–25.
47. Coast–Senior EA, Kroner BA, Kelley CI, Trilli LE .Management of patients with type 2 diabetes by pharmacists inprimary care clinics. Ann Pharmacother 1998;32:636–41.
48. Jaber LA, Halapy H, Fernet M, Tummalapalli S, Diwakaran H.Evaluation of a pharmaceutical care model on diabetesmanagement. Ann Pharmacother 1996;30:238–43.
49. Yanchick JK. Implementation of a drug therapy monitoringclinic in a primary-care setting. Am J Health-Syst Pharm2000;57(suppl 4):S30–4.
50. Davidson MB, Karlan VJ, Hair TL. Effect of a pharmacist-managed diabetes care program in a free medical clinic. Am JMed Qual 2000;15:137–42.
51. Schapansky LM, Johnson JA. Pharmacists’ attitudes towarddiabetes. J Am Pharm Assoc 2000;40:371–7.
52. Younis WS, Campbell S, Slack MK. Pharmacists’ attitudestoward diabetes and their involvement in diabetes education.Ann Pharmacother 2001;35:841–5.
53. Kroon LA, Coleman LT, Koda-Kimble MA. The management oftype 2 diabetes mellitus: a call to action for pharmacists. USPharmacist 1997;May(suppl 1):1–18.
54. Daly A, Kulkarni K, Boucher J. The new credential: advanceddiabetes management. J Am Diet Assoc 2001;101:940–3.
55. Fincham JE, Lofholm PW. Saving money and lives: pharmacistcare for diabetes patients. America’s Pharm 1998;120:49–52.
56. Munroe WP, Kunz K, Dalmady-Israel C, Potter L, SchonfeldWH. Economic evaluation of pharmacist involvement indisease management in a community pharmacy setting. ClinTher 1997;19:113–23.
57 . Lobas NH, Lepinski PW, Abramowitz PW. Effects of pharma-ceutical care on medication cost and quality of patient care inan ambulatory-care clinic. Am J Hosp Pharm 1992;49:1681–8.
58. West JD, Goldberg KL. Diabetes self-care knowledge amongoutpatients at a veterans affairs medical center. Am J Health-Syst Pharm 2002;59:849–52.
59. Browne DL, Avery L, Turner BC, Kerr D, Cavan DA. What dopatients with diabetes know about their tablets? Diabet Med2000;17:528–31.
60. De Young M. Research on the effects of pharmacist-patientcommunication in institutions and ambulatory care sites,1969–1994. Am J Health-Syst Pharm 1996;53:1277–91.
1593





























