Embed Size (px)
Citation preview
Systematic Review
Natural Orifice Translumenal Endoscopic Surgery (NOTES)TM for Intra-abdominal Surgery
ASERNIP-S REPORT NO. 62
Australian Safety & Efficacy Register of New Interventional Procedures – Surgical
The Royal Australasian College of Surgeons
ASERNIP S Australian Safety
and Efficacy
Register of New
Interventional
Procedures - Surgical


- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
A Systematic Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES)TM for Intra-Abdominal Surgery
ISBN 0909844 84 4
Published July 2007
This report should be cited in the following manner:
Della Flora E, et al. A Systematic Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES)TM for Intra-abdominal Surgery. ASERNIP-S Report No. 62. Adelaide, South Australia: ASERNIP-S, July 2007.
Copies of these reports can be obtained from:
ASERNIP-S PO Box 553, Stepney, SA 5069 AUSTRALIA Ph: 61-8-8363 7513 Fax: 61-8-8362 2077 E-Mail: [email protected] http://www.surgeons.org/asernip-s
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
The Safety and Efficacy Classification for the
Systematic Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES)TM for Intra-Abdominal Surgery
was ratified by:
The ASERNIP-S Management Committee on
June 2007
and
The Council of the Royal Australasian College of Surgeons on
July 2007

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
i
Table of Contents
Executive Summary ........................................................................ iv
The ASERNIP-S Classification System ........................................vii
The ASERNIP-S Review Group..................................................... ix
Introduction ..................................................................................... 1
Objective .......................................................................................................... 1
Intra-abdominal Surgery ................................................................................ 1
Conditions treatable by intra-abdominal surgery.................................. 1
Burden of disease in Australia ................................................................. 2
Comparative treatments ........................................................................... 3
Open abdominal surgery/laparotomy.................................................... 3
Minimally invasive surgery ....................................................................... 4
New interventional Procedure...................................................................... 6
Natural Orifice Transluminal Endoscopic Surgery.............................. 6
Summary .......................................................................................................... 7
Research questions ......................................................................................... 8
Methods ........................................................................................... 9
Literature search protocol ............................................................................. 9
Inclusion criteria ........................................................................................ 9
Literature search strategies ..........................................................................10
Search terms .............................................................................................11
Literature database & exclusions...........................................................12
Data extraction and assessment of study quality .....................................12
Data analysis ..................................................................................................12
Studies Included in the Review ......................................................13
Literature Search Results .............................................................................13
Ongoing and unpublished trials .................................................................13
SAGES 2006 and 2007 Meeting Abstracts...............................................13
Description of studies ..................................................................................15
Results............................................................................................ 20
Efficacy...........................................................................................................20
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
ii
Success of surgical techniques ...............................................................20
Success of NOTES intervention and techniques ...............................31
Duration of surgery .................................................................................37
Safety...............................................................................................................39
Post-operative mortality..........................................................................39
Post-operative recovery ..........................................................................40
Infection-related complications .............................................................40
Procedure-Related Complications.........................................................42
Discussion ......................................................................................44
Conclusions ....................................................................................53
Classification and Recommendations ........................................................53
Classifications ...........................................................................................53
Clinical and Research Recommendations ............................................53
Acknowledgments.........................................................................................54
References ......................................................................................55
Appendix A – Hierarchy Of Evidence......................................................66
Appendix B – Conference proceedings ....................................................69
SAGES 2006 Presentations....................................................................69
SAGES 2007 presentations....................................................................70
Appendix C – Excluded Studies.................................................................75
Appendix D – Glossary ...............................................................................77
Appendix E – Equipment descriptions.....................................................79
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
iii
List of Tables
Table 1. Summary of included studies .............................................................................. 16
Table 2: Summary of subjects............................................................................................. 19
Table 3: Sites chosen for NOTES viscerotomy .............................................................. 21
Table 4: NOTES gastrotomy closure................................................................................ 24
Table 5: Success of visualisation using NOTES.............................................................. 27
Table 6: Success of NOTES anastomosis creation......................................................... 32
Table 7: Success of NOTES cholecystectomy................................................................. 33
Table 8: Success of NOTES biopsy .................................................................................. 34
Table 9: Duration of Surgery.............................................................................................. 38
Table 10: Post-operative mortality..................................................................................... 39
Table 11: Post-operative feeding and weight gain........................................................... 40
Table 12: Infection-related complications ........................................................................ 41
SAGES 2006 Abstracts ....................................................................................................... 69
Excluded Studies .................................................................................................................. 75
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
iv
Executive Summary
Objective To assess the safety and efficacy of various intra-abdominal Natural Orifice Translumenal* Endoscopic SurgeryTM (NOTESTM) procedures which do not cut the dermis, in comparison with traditional intra-abdominal surgery which cuts the dermis, through a systematic review of the literature.
Methods Search strategy – Studies were identified by performing electronic searches of MEDLINE, EMBASE, CINAHL, Current Contents, the Cochrane Library and Entrez-PubMed from 2000 to March 2007. The clinical trials database (US), NHS CRD databases and National Research Register (UK) were also searched in March 2007 and the SAGES 2006 and 2007 annual meeting abstracts for were sourced for information.
Study selection – Studies conducted in live humans or animals involving surgical procedures in the intra-abdominal region using natural orifice access were included for review; however studies in cadavers were excluded. Studies where the new intervention involved an incision to the dermis were excluded and studies reporting established endoscopic procedures that are not transluminal such as abscess or cyst drainage or debridement were not included as they are standard practice. Efficacy outcomes included procedure success-rate, viscerotomy creation and closure and operation time. Safety outcomes included mortality, infection, toxic or adverse effects, pain, intraoperative/procedural complications and recovery times.
Data collection and analysis – Data from the included studies were extracted by the ASERNIP-S researcher using standard data extraction tables developed a priori and checked by a second researcher.
Results The evidence base for this review was very limited, as there were no comparative studies and all the 22 included studies were conducted in animals, their purpose being to test the feasibility of NOTES. There were no comparative studies, study numbers were low, and safety and efficacy outcomes were limited, thus it was difficult to compare the safety and efficacy of using NOTES to perform intra-abdominal surgery with existing techniques. However, it can be determined that at the present stage of development, NOTES does not appear to be as safe or effective as current surgical techniques. This indicates that the use of NOTES for intra-
* Trans lumenal i s used in the t rademarked name ‘Natura l Or i f i ce Trans lumenal Endoscop ic Surgery ’ , however t rans luminal i s accepted Aust ra l ian ver s ion o f the word.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
v
abdominal surgery requires further development before it can be considered in a clinical setting. Although intra-abdominal access via oral, anal or urethral orifices could be achieved reliably in all cases, the evidence does not indicate the optimal access route and method. Viscerotomy closure could not be achieved reliably in all cases and risk of peritoneal infection has not been adequately minimised.
Although the majority of interventions were able to be performed in animals using NOTES, a number of technical problems were encountered that will need to be resolved. The large number of abstracts relating to NOTES at the recent SAGES 2007 meeting suggests that this area of surgery is developing rapidly and accordingly, the evidence base will increase substantially. The review does indicate that it is feasible to use NOTES for some intra-abdominal surgical procedures, however it is too early to determine if these will be comparable to current procedures and if the advantages of using NOTES outweigh the disadvantages.
Classification and Recommendations
Classifications Evidence rating The available evidence was assessed as being poor.
Safety At this point in time, NOTES for intra-abdominal surgery is less safe than laparoscopic and laparotomic alternatives.
Efficacy Presently, NOTES for intra-abdominal surgery is currently less efficacious than laparoscopic and laparotomic alternatives.
Clinical and Research Recommendations NOTES is still in early stages of development and more robust technologies will be needed to achieve reliable closure and overcome technical challenges. Well-managed human studies need to be conducted to determine the safety and efficacy of NOTES in a clinical setting. This may be approached by performing hybrid NOTES/laparoscopic procedures, which may help to evaluate the safety of NOTES in a human model, before moving into larger trials. NOTES procedures and studies should be performed under strict guidelines, such as the membership criteria developed by NOSCAR.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
vi
Important note The information contained in this report is a distillation of the best available evidence located at the time the searches were completed as stated in the protocol. Please consult with your medical practitioner if you have further questions relating to the information provided, as the clinical context may vary from patient to patient.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
vii
The ASERNIP-S Classification System
Evidence Rating The evidence for ASERNIP-S systematic reviews is classified as Good, Average or Poor, based on the quality and availability of this evidence. High quality evidence is defined here as having a low risk of bias and no other significant flaws. While high quality randomised controlled trials are regarded as the best kind of evidence for comparing interventions, it may not be practical or ethical to undertake them for some surgical procedures, or the relevant randomised controlled trials may not yet have been carried out. This means that it may not be possible for the evidence on some procedures to be classified as good.
Good Most of the evidence is from a high quality systematic review of all relevant randomised trials or from at least one high quality randomised controlled trial of sufficient power. The component studies should show consistent results, the differences between the interventions being compared should be large enough to be important, and the results should be precise with minimal uncertainty.
Average Most of the evidence is from high quality quasi-randomised controlled trials, or from non-randomised comparative studies without significant flaws, such as large losses to follow-up and obvious baseline differences between the comparison groups. There is a greater risk of bias, confounding and chance relationships compared to high-quality randomised controlled trials, but there is still a moderate probability that the relationships are causal.
An inconclusive systematic review based on small randomised controlled trials that lack the power to detect a difference between interventions and randomized controlled trials of moderate or uncertain quality may attract a rating of average.
Poor Most of the evidence is from case series, or studies of the above designs with significant flaws or a high risk of bias. A poor rating may also be given if there is insufficient evidence.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
viii
Safety and Efficacy Classification Safety At least as safe compared to comparator* procedure(s)
This grading is based on the systematic review showing that the new intervention is at least as safe as the comparator.
Safety cannot be determined This grading is given if the evidence is insufficient to determine the safety of the new intervention.
Less safe compared to comparator* procedure(s) This grading is based on the systematic review showing that the new intervention is not as safe as the comparator.
Efficacy At least as efficacious compared to comparator* procedure(s)
This grading is based on the systematic review showing that the new intervention is at least as efficacious as the comparator.
Efficacy cannot be determined This grading is given if the evidence is insufficient to determine the efficacy of the new intervention.
Less efficacious compared to comparator* procedure(s) This grading is based on the systematic review showing that the new intervention is not as efficacious as the comparator.
Research Recommendations It may be recommended that an audit or a controlled (ideally randomised) clinical trial be undertaken in order to strengthen the evidence base.
Clinical Recommendations Additional recommendations for use of the new intervention in clinical practice may be provided to ensure appropriate use of the procedure by sufficiently qualified/ experienced centres and on specific patient types (where appropriate).
* A comparator may be the current ‘gold standard’ procedure, and alternative procedure, a non-surgical procedure or no treatment (natural history)
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
ix
The ASERNIP-S Review Group ASERNIP-S Director
Professor Guy Maddern, FRACS ASERNIP-S Royal Australasian College of Surgeons Stepney SA 5069
Protocol Surgeon
Dr Ian J Martin, FRACS Wesley Medical Centre Auchenflower Brisbane 4066
Advisory Surgeons
Mr Thomas Graham Wilson, FRACS Consultant Surgeon Flinders Medical Centre Bedford Park SA 5041 Mr Nicholas O’Rourke, FRACS Royal Brisbane Hospital Brisbane QLD 4001
ASERNIP-S Researcher
Ms Eliana Della Flora ASERNIP-S Royal Australasian College of Surgeons Stepney SA 5069
Conflict of Interest
None of the authors declared a conflict of interest.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 1 INTRODUCTION 1
Introduction
Objective To assess the safety and efficacy of intra-abdominal Natural Orifice Translumenal* Endoscopic SurgeryTM (NOTESTM) procedures, in comparison with traditional intra-abdominal surgery which cuts the dermis, through a systematic review of the literature.
Intra-abdominal Surgery For many years surgical procedures involving tissue resection and repair have been performed for the diagnosis and/or treatment of numerous diseases affecting organs located in the abdominal cavity, including:
the digestive tract (stomach, duodenum, jejunum, ileum and colon)
the liver, gallbladder, pancreas, spleen and appendix
the female reproductive organs (uterus, ovaries and fallopian tubes)
the retroperitoneum (kidneys, aorta and abdominal lymph nodes)
Intra-abdominal surgical procedures may be performed for the removal/resection of diseased tissue/whole organs, such as cancerous, infected or necrotic tissue, tissue repair such as hernia repair, gastric bypass surgery or fallopian tube ligation or for diagnostic purposes in exploratory surgery. As intra-abdominal surgery may be implemented to treat a large number of conditions, only the more common conditions will be described below.
Conditions treatable by intra-abdominal surgery Digestive tract
Morbid obesity and neoplastic disease of the digestive tract are treatable by gastrojejunostomy (gastric bypass surgery) (Martin 2004).
Liver, gallbladder, pancreas, spleen and appendix Neoplastic liver disease (including hepatocellular carcinoma and hepatic
haemangioma) and cirrhosis caused by diabetes (Moscatiello et al. 2007), drug or alcohol abuse or viral hepatitis (Cameron and Busuttil 2006; O'Grady and Williams 1990; Rongey and Kaplowitz 2006) may be treated by hepatectomy (liver resection) or transplantation (Barbare et al. 2006; Mehrabi et al. 2006; Volk et al. 2006).
Gallbladder disease, including cholecystitis, may be treated by cholecystectomy, which is usually performed laparoscopically due to a
* Trans lumenal i s used in the t rademarked name ‘Natura l Or i f i ce Trans lumenal Endoscop ic Surgery ’ , however t rans luminal i s the cor rect spe l l ing in Aus tra l ia .
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
2 SECT ION 1 INTRODUCTION
much faster recovery time compared to laparotomy (Calland et al. 2001; Keus et al. 2006; O'Rourke NA and Fielding; Zehetner et al. 2007).
Pancreatic cancer, a leading cause of death from cancer in the developed world, may be treated by pancreatoduodenectomy (Whipple procedure), although only 20% of pancreatic tumours are removable by surgery (Eckel et al. 2006; Greenhalf 2006; Wakeman et al. 2004). Pancreatoduodenectomy may also be performed for severe cases of chronic pancreatitis (Bengmark 2006; Kaido 2006; Larson et al. 2006).
Splenectomy is commonly performed to treat many haematologic conditions including splenic trauma or spontaneous rupture, idiopathic thrombocytopenia purpura(Koene 2006), haemolytic anaemia, portal hypertension and hypersplenism, lymphoma and leukaemia (Forsythe et al. 2006; Katz and Pachter 2006; Koene 2006; Rhodes et al.).
Appendicectomy is one of the most common emergency abdominal surgical procedures (Humes and Simpson 2006; Sauerland et al. 2004; Tchana-Sato et al. 2006).
Female reproductive organs Ovarian cancer, problematic ovarian cysts and polycystic ovary disease are
usually diagnosed and treated surgically. Treatment usually involves surgical resection or oophorectomy (Bunyavejchevin and Phupong 2006; Hilger et al. 2006; King 2006; Mastorakos et al. 2006).
A hysterectomy may be performed to treat conditions such as endometriosis, adenomyosis, uterine fibroids, prolapse, heavy or abnormal menstrual bleeding and malignant disease (Nezhat et al. 2006).
Women desiring permanent contraception may undergo surgery such as fallopian tube ligation (Kulier et al. 2004).
The retroperitoneum Kidney disease as a result of congenital abnormalities, trauma, infection,
hypertension, tumours or chronic bleeding may be treated by nephrectomy (Kemmer et al. 2007; Liao et al. 2007; Power et al. 2006; Romero et al. 2006), and sometimes subsequent transplantation.
Lymphadenectomy may be performed laproscopically on severely inflamed or cancerous abdominal lymph nodes to prevent further spread of disease (Aletti et al. 2006).
Burden of disease in Australia It is difficult to accurately define the burden of disease of disorders which may be treated using intra-abdominal surgery, as these procedures are used to treat and diagnose a wide variety of illnesses. In Australia during 2004-2005, 43,144 cholecystectomies were performed, with 39,800 of these performed laparoscopically. In the same year, 23,601 appendicectomies and 64,628 hernia procedures were also performed. During this time, a large number of surgical procedures were performed on the female reproductive system, many of these to treat malignant disease. In addition, there were 27,890 hysterectomies for non-malignancy and 17,468 female reproductive system reconstructive procedures. In the same period, 436
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 1 INTRODUCTION 3
splenectomies and 3,532 other haematological-related operating room procedures were carried out, in addition to 165 liver transplants and other surgical procedures involving the liver (Australian Institute of Health and Welfare - National Hospital Morbidity Database 2006).
Comparative treatments In order to perform surgery on the intra-abdominal organs, access must first be gained to the abdominal cavity (peritoneal cavity). Surgical section of the abdominal wall has traditionally been used to access the abdominal cavity and is commonly referred to as open abdominal surgery or laparotomy, a technique that is still widely used today to perform a host of surgical procedures (Fu Louis Kuo Tai 1999). More recently, less invasive methods of accessing the abdominal cavity have been developed, including laparoscopic procedures in which only a small incision is made in the abdominal wall, or endoscopy, where access is gained through a natural orifice such as the mouth, anus or vagina.
Open abdominal surgery/laparotomy Laparotomy allows the abdominal cavity to be well visualised and easily accessed. Methods for performing these procedures have been optimised and well researched and their long term consequences are known (Fu Louis Kuo Tai 1999). As open surgical procedures have evolved over a long period of time, the learning curve for implementing new laparotomic procedures is not great and surgeons may readily adapt to the gradual advances in the area. Like any medical procedure however, there are complications associated with open abdominal surgery, many of which are related to the incision of the abdominal wall:
Wound infections can be problematic, with surgical site infections (SSIs) occurring in 2-25% of patients undergoing laparotomy in the US (Boni et al. 2006; McGee et al. 2006b).
Incisional hernias are another common complication, experienced by 4-18% of US patients (McGee et al. 2006b).
Post-operative pain can be quite severe for some patients at the incision site.
Scarring at the incision site is a cosmetic concern for many patients.
Slow wound healing and convalescence.
Intra-abdominal adhesions
Other complications related to the procedure include laceration of organs, intra-abdominal abscesses and complications related to general anaesthesia (Boni et al. 2006).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
4 SECT ION 1 INTRODUCTION
Minimally invasive surgery Minimally invasive surgery (MIS), also referred to as minimal access surgery (MAS), has become very popular in recent years. MIS is usually performed by endoscopy, where luminal areas are accessed through a natural orifice, or by laparoscopy, where access to internal organs is achieved via a small incision made on the body’s surface. MIS has been associated with a significant decrease in morbidity associated with access-related incisions, as well as better patient outcomes including reduced scarring and length of hospital stay (Boni et al. 2006; McGee et al. 2006b).
Endoscopic surgery Initial applications of endoscopy were purely diagnostic, however it is now one of the fastest growing fields of therapeutic surgery and flexible endoscopy is one of the most frequently reported procedures of surgeons applying for recertification from the American Board of Surgery (Richards and Rattner 2005).
The endoscope is a long, rigid or flexible tube containing a light delivery system that is usually delivered via fibre optics from outside of the body and which may also have a channel for mechanical devices to enable functions such as taking biopsies and retrieval of foreign objects (Ellsmere et al. 2006; Malik et al. 2006; Vitale et al. 2005). The endoscope may be inserted through a natural orifice to reach many areas of the body including the gastrointestinal tract, respiratory tract, urinary tract or reproductive system, to visualize and collect specimens or perform simple procedures. Currently, endoscopy is used to treat and diagnose a number of conditions of the gastrointestinal system such as gastric reflux disease, pancreatic pseudocysts, gastrointestinal bleeding and gall stones and strictures (Vitale et al. 2005), alteration of bowel habit, lower gastrointestinal bleeding, colonic neoplasia and inflammatory bowel disease. As most of these procedures are relatively painless, general anaesthesia is usually not required. In addition, complications are rare, with the most serious complication being perforation of the organ under inspection with the endoscope or biopsy instrument.
Laparoscopic surgery Laparoscopy, which has been performed since the late 1980s, is the visual examination and/or operation inside the abdominal cavity via one or more small incisions in the abdominal wall using a laparoscope (Hochberger and Lamade 2005; Vitale et al. 2005). Following an incision of the abdominal wall, the area is filled with gas (usually CO2) to create a pneumoperitoneum to lift the abdominal wall away from the internal organs. The laparoscope is inserted into this space via the incision in order to visualise the area, and surgery may be performed via multiple small incisions to create multiple working ports.
Advantages of laparoscopy over laparotomy As laparoscopic incisions are much smaller than those created during laparotomy, incision-related complications are greatly reduced, although not entirely eliminated.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 1 INTRODUCTION 5
This gives laparoscopic surgery the advantage of reduced post-operative pain, scarring and recovery time. A trend towards a faster recovery, decrease in wound-related infections and reduction in postoperative pain after laparoscopic surgery has been noted in clinical trials comparing laparoscopic with open appendicectomy (Humes and Simpson 2006; Kapischke et al. 2006; Sauerland et al. 2004). In a systematic review comparing laparoscopic vs open appendicectomy it was found that wound infections were less likely, hospital stays and return to work times were shortened following laparoscopic appendicectomy (Sauerland et al. 2004). Gynaecological laparoscopy has been associated with less post-surgical ICU admissions than laparotomy (Hayes et al. 1996).
Laparoscopy has proven to be favourable for a variety of procedures (Johnson 1996; Osborne et al. 2006), such as laparoscopic cholecystectomy, which can now be performed as an outpatient procedure, resulting in faster recovery times and decreased hospital stays and decreased use of medical resources (Calland et al. 2001). The advantages of endoscopy and laparoscopy are especially clear for diagnostic purposes.
Disadvantages of laparoscopy over laparotomy In addition to some of the risks associated with open surgery, laparoscopic surgery carries further, technique-specific risks. Procedural complications can occur as a result of a combination of difficulties with visibility and manoeuvrability, as well as the learning and optimisation of this relatively complicated procedure. Laparoscopic procedures that require very precise hand-eye coordination are performed with awkwardly long instruments lacking in tactile feedback and limited, 2-dimensional vision is used to visualise a complex 3-dimensional situation (Osborne et al. 2006; Wolf, Jr. 2005). In addition, the trials that have been conducted predominately involved surgeons who were experts in laparoscopy, thus reducing complications from procedural errors (Sauerland et al. 2004).
Complications include intra-abdominal abscesses and adhesions, the development of CO2 gas emboli due to the creation of the pneumoperitoneum and injuries to vascular structures from needles, trochars and electrical arching of instruments, with injury rates up to three times those of laparotomy (Boni et al. 2006; Humes and Simpson 2006; Johnson 1996; Kapischke et al. 2006; Saltzman 2004; Sauerland et al. 2004). While the rates of these complications have been reduced in recent years, the high incidence of injury following the hasty introduction of laparoscopic surgery should be remembered when developing and introducing other new surgical procedures. As laparoscopy was the result of a technological leap, there was a much greater learning curve for this technique compared to open procedures, where there have been gradual advancements, and this may explain the high rate of procedural errors whilst learning laparoscopic surgical procedures (Johnson 1996; Sauerland et al. 2004).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
6 SECT ION 1 INTRODUCTION
Additionally, the present costs of the highly advanced instrumentation required, makes laparoscopic surgery a more expensive alternative to open abdominal surgery (Sauerland et al. 2004), but with further technological advances and the widespread adoption of laparoscopy, costs will continue to decrease. Further to this, societal costs are reduced when compared to open surgery, due to reduced length of hospital stay and return to work time (Sauerland et al. 2004).
New interventional Procedure
Natural Orifice Transluminal Endoscopic Surgery Historically, limitations of endoscopic technology have been the barrier of the lumenal wall (gastrointestinal or vaginal). The idea of using endoscopic procedures to perform intra-abdominal surgery via a natural orifice started to become a reality when endoscopy researchers in Japan noted no apparent ill effects following an accidental puncture of the stomach wall during removal of large stomach tumours. This led to the exciting new concept of puncturing the gastric wall to access intraperitoneal organs such as the liver, appendix, gallbladder, spleen or fallopian tubes, without making incisions on the surface of the body. Thus, access to the abdominal cavity could potentially be gained via natural orifices such as the mouth, vagina, anus or possibly, the urethra. In recent years transgastric peritoneal access, gained by perforation of the stomach wall with a needle-knife, has been used for some simple endoscopic procedures including drainage of pancreatic pseudocysts and abscesses. Today, endoscopic ultrasound guided pancreatic pseudocyst or abscess drainage is a standard procedure and complete removal of a necrotic spleen by transgastric debridement has also been reported by Siffert in 2000. Kantsevoy et al. (2006) reported that the first description of surgery via a natural orifice was in 2000 at Digestive Diseases Week, by the Apollo group (Kantsevoy et al. 2006a)
The use of flexible endoscopy to perform transluminal surgery via a natural orifice has been referred to by a number of names, such as ‘incisionless surgery’, but the official term agreed upon to describe these procedures is ‘Natural Orifice Translumenal Endoscopic Surgery’ (NOTES) (Rattner and Kalloo 2006). Essentially, NOTES involves the insertion of a flexible endoscopic device through a natural orifice (mouth, anus, vagina, urethra), followed by transvisceral incision to gain access to abdominal organs, i.e. those in the peritoneal cavity, where surgery is performed. While this concept is not complex, the reality of performing these procedures is fraught with many challenges (Saltzman 2004).
Potential advantages and disadvantages over traditional techniques There are a number of potential benefits to using NOTES over traditional surgical techniques such as laparotomy or laparoscopy. The most substantial potential advantages are associated with the lack of any surface incision, including the elimination of SSIs and any visible scarring, as well as a reduced need for anaesthesia. NOTES procedures also have the potential to be used for the treatment of morbidly
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 1 INTRODUCTION 7
obese patients or those with obstructive carcinomas, in whom access to the intra-abdominal organs via the abdominal wall is very difficult and the risk of wound related complications are increased (Hawn et al. 2005). The potential application of NOTES in children is another possibility, as incision-related complications can lead to adverse effects in the longer term (McGee et al. 2006b).
On the other hand, NOTES shares the potential for many of the complications associated with laparoscopic surgery and difficulties with poor visibility, manoeuvrability and grasping are likely to be increased as distances are further and the equipment required is more specialised. However, it is expected that technological advances in laparoscopic and endoscopic devices will lead to the advancement of NOTES, reducing the aforementioned expected difficulties with visualisation and manoeuvrability.
Development and implementation Amidst the enthusiasm for the use of NOTES there is also trepidation, particularly considering the problems that occurred following the rapid adoption of laparoscopic operations by surgeons, many of whom had little experience or training in the area. While NOTES procedures may be technically feasible and challenges may be theoretically addressed, the reality is more complex, with initial studies in animals revealing a series of complications that need to be addressed in order for these procedures to become viable (Lamade et al. 2006; Saltzman 2004).
Summary Access to the abdominal cavity is required for the surgical treatment and diagnosis of diseases affecting the abdominal organs. Traditional methods of accessing the abdominal cavity have involved incision of the abdominal wall, which has been the source of complications such as infection, scarring and post-operative pain. The smaller incisions required for performing laparoscopic surgery have reduced these incision-related complications, but have not entirely eliminated them.
More recently, technological advances have allowed the extension of endoscopy into the peritoneal cavity via a transvisceral incision, created with endoscopic equipment inserted through a natural orifice. These developments have led to the investigation of NOTES, which has the potential to revolutionise abdominal surgery through the elimination of all abdominal wall incision-related complications. However, a number of challenges to the safe and efficacious performance of NOTES have been identified and must be addressed prior to the implementation of these procedures.
Thus the aim of this review is to systematically assess the safety and efficacy of NOTES to perform various abdominal procedures which do not cut the skin, compared with traditional abdominal surgical procedures which cut the skin.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
8 SECT ION 1 INTRODUCTION
Research questions The specific research questions that will be addressed in this review are as follows
For clinical studies in patients to assess if there is a true clinical advantage to avoiding incisions of the abdominal wall?
Is there a clinically significant reduction in healing time following surgery?
Are infection rates lower when abdominal incisions are avoided?
Is patient survival following procedures avoiding abdominal wall incisions comparable to survival rates following laparotomy or laparoscopy?
Do the cosmetic benefits of NOTES, such as the lack of any visible scarring, outweigh the disadvantages?
For studies in animals
Can traditional surgical procedures be performed successfully using NOTES?
Can infection of the abdominal cavity be suitably avoided or minimised?
Can a reliable means of viscerotomy closure be achieved?
Can adverse effects such as organ laceration and haemorrhage be minimised to an acceptable level?
Are survival rates and recovery times following NOTES procedures comparable to those following similar procedures performed using traditional access methods (i.e. laparoscopy or laparotomy)?
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 2 METHODS 9
Methods
Literature search protocol
Inclusion criteria Articles were selected for inclusion in this systematic review on the basis of the following criteria.
Participants Studies in live humans were included; however studies in human cadavers were excluded because they do not provide any indication of safety or efficacy in a clinical setting. As NOTES procedures are still in the early stages of development, studies in live animals were also included. Studies involving transluminal surgical procedures in the abdominal region where access was gained via a natural orifice were included. Studies where the new intervention involved an incision to the dermis were excluded and studies reporting established endoscopic procedures that do not traverse the luminal wall such as abscess or cyst drainage or debridement were not included.
New intervention Natural orifice translumenal endoscopic surgery for intra-abdominal interventions
Comparative intervention Surgical procedures in the abdominal cavity that cut the dermis, including laparotomy and laparoscopic surgery
Outcomes for studies in humans Studies that report at least one of the following outcomes were included:
Safety which could include, but not be limited to:
morbidity and mortality of patients
infection
adverse effects
pain
intraoperative/procedural complications
Efficacy which could include, but not be limited to:
operation time
early re-intervention
procedure success-rate
cosmesis (lack of scarring)
patient satisfaction, quality of life
healing time
Cost/resource use
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
10 SECT ION 2 METHODS
Outcomes for studies in animals Studies that report at least one of the following outcomes were included:
survival
recovery times
infection
procedure success-rate
viscerotomy closure
other intraoperative/procedural complications
Types of studies Systematic reviews, randomised controlled trials (RCTs), non-randomised comparative studies, case series and case reports were included for review. Where appropriate, additional relevant published material in the form of letters, conference material, commentary, editorials and abstracts was included as background information.
Language restriction Searches were conducted without language restriction. Foreign language articles were subsequently excluded unless the findings provide additional information over that reported in well designed studies published in the English language.
Date restriction Searches were conducted in March 2007 and were limited to articles published since 2000 as NOTES technology has only been developed in recent years and was first described in 2000. SAGES 2007 abstracts were searched in April 2007.
Literature search strategies Databases searched
Ovid MEDLINE
Ovid EMBASE
Webspurs CINAHL
ISI Current Contents Connect
The Cochrane Library
Entrez-PubMed
NHS CRD databases
SAGES annual meeting abstracts for 2006 and 2007*
* Note: As NOTES is a very new procedure the availability of peer-reviewed publications was limited, so abstracts from SAGES Annual Meetings were also searched to provide information about recent NOTES developments.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 2 METHODS 11
Search terms In the Cochrane Library, CINAHL and NHS CRD the following search terms were used
transgastric
transluminal (Cochrane Library only)
natural orifice
flexible endoscopy (not NRR)
The National Research Register, Clinicaltrials.gov, Meta-Register and the Australian Clinical Trials Registry were also searched using the above search terms for trials in progress.
For MEDLINE, EMBASE and Current Contents the following search terms were used*:
1. ‘natural orifice’ 2. peritoneal cavity/su [Surgery][MeSH] 3. abdominal cavity/[MeSH] OR abdominal cavity 4. transgastric OR trans gastric 5. transluminal OR translumenal 6. 2 OR 3 OR 4 OR 5 7. orifice 8. peroral 9. per-oral 10. transoral 11. endoscopy[MeSH] or endoscop$ 12. transvaginal OR trans vaginal 13. transurethral OR trans urethral 14. transanal OR trans anal 15. transrectal OR trans rectal 16. transcolonic OR trans colonic 17. transvesical OR trans vesical 18. 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 19. 1 OR 6 AND 18
* Note: * is a truncation character that retrieves all possible suffix variations of the root word e.g. surg* retrieves surgery, surgical, surgeon, etc. In Cochrane the truncation character is *; in Current Contents, EMBASE, CINAHL and MEDLINE (Ovid) it is $. # is a wildcard symbol that substitutes for one required character in Current Contents, EMBASE, CINAHL and MEDLINE (Ovid).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
12 SECT ION 2 METHODS
For PubMed the following search terms were used
(“abdominal cavity” [MeSH] OR "Peritoneal Cavity"[MeSH] OR transgastric) AND (peroral OR transoral OR trans oral OR endoscopic surgery OR transvaginal OR “trans vaginal” OR transanal OR “trans anal” OR transrectal OR “trans rectal” OR transcolonic OR “trans colonic” transurethral OR “trans urethral” OR transvesical OR “trans vesical” OR transluminal OR transvisceral)
Literature database & exclusions Articles were retrieved if they are judged to possibly meet the inclusion criteria based on their abstracts. Two ASERNIP-S Researchers independently applied the selection criteria and any differences resolved through discussion. Full publications subsequently found to not meet the inclusion criteria were excluded and reasons were documented when this occurred. The bibliographies of all publications retrieved were manually searched for relevant references that may have been missed in the database search (pearling).
Data extraction and assessment of study quality Data from all included studies were extracted by one researcher and checked by a second using standardised data extraction tables that have been developed a priori. Appendix 1 contains the guidelines that were used to assess the level of evidence of the studies to enable the filtering and inclusion of studies. As these were animal studies, their quality could not be critically appraised.
Data analysis If the data was suitable for statistical pooling, meta-analyses of the main outcomes was performed. Where possible, the data was stratified into clinically relevant groups. Otherwise, data for the main outcomes was reported narratively.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 13
Studies Included in the Review
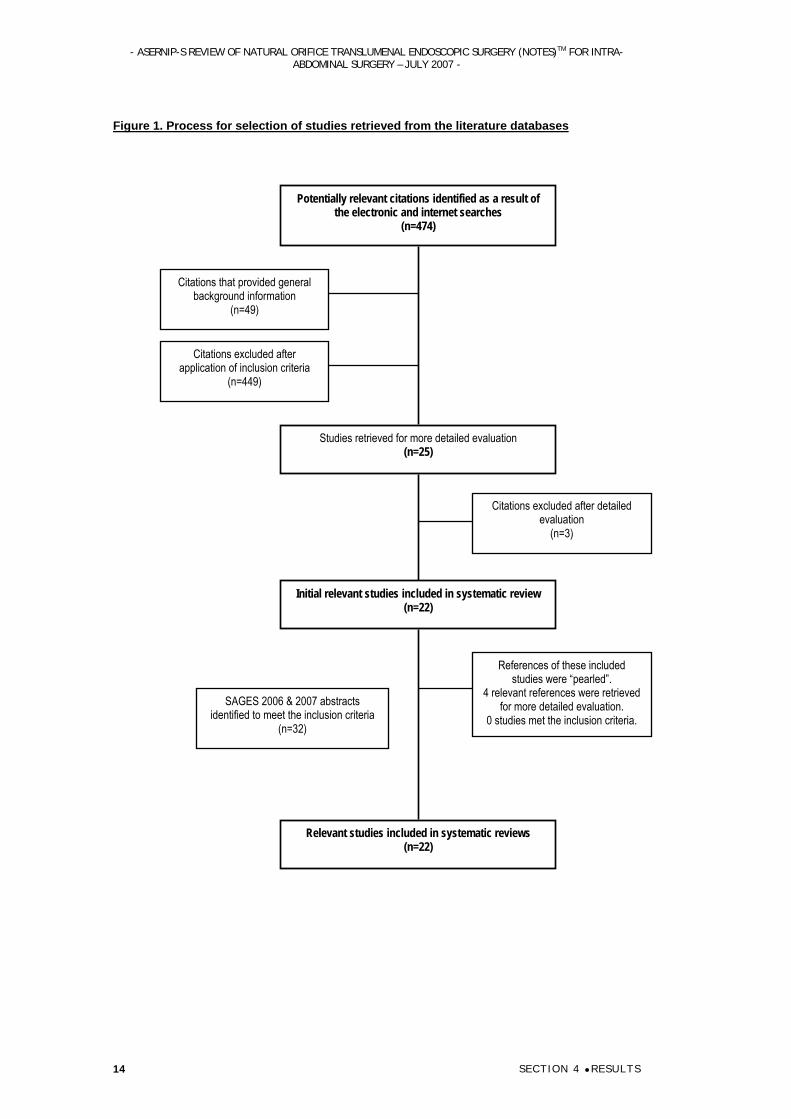
Literature Search Results Details of the number of articles retrieved from the literature search are shown in Figure 1.
Ongoing and unpublished trials Searches of the Clinical Trials Database, NHS CRD, NHS HTA, Current Controlled Trials and the National Research Register failed to identify any ongoing or unpublished trials.
SAGES 2006 and 2007 Meeting Abstracts Searches of the SAGES 2006 conference proceedings identified four Scientific Session (presentation) abstracts, two of which have been published as peer-reviewed articles, which were retrieved thorough the above literature search. One video abstract was identified, which appears to contain footage of procedures published in other abstracts or retrieved articles. Three poster abstracts were also identified. Thus five SAGES 2006 abstracts were sourced for information (Appendix B).
Searches of the SAGES 2007 ten Scientific Session (presentation) abstracts, nine video abstracts and ten poster abstracts that were relevant to NOTES development, none of which have been subsequently published in peer-reviewed literature, although some groups presented both a video and a poster or scientific session on the same topic. Thus 27 SAGES 2007 abstracts were sourced for information (Appendix B).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 14
Figure 1. Process for selection of studies retrieved from the literature databases
Potentially relevant citations identified as a result of the electronic and internet searches
(n=474)
Citations that provided general background information
(n=49)
Citations excluded after application of inclusion criteria
(n=449)
Studies retrieved for more detailed evaluation (n=25)
Initial relevant studies included in systematic review (n=22)
Relevant studies included in systematic reviews (n=22)
References of these included studies were “pearled”.
4 relevant references were retrieved for more detailed evaluation.
0 studies met the inclusion criteria.
Citations excluded after detailed evaluation
(n=3)
SAGES 2006 & 2007 abstracts identified to meet the inclusion criteria
(n=32)

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 15
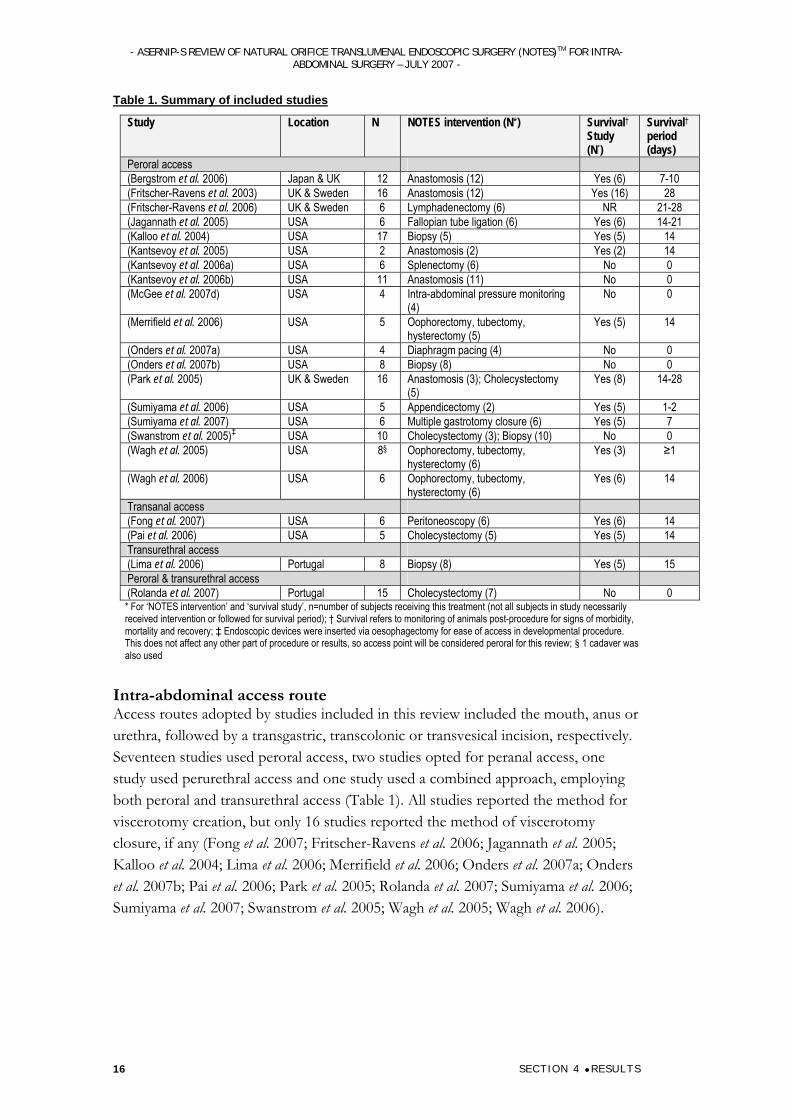
Description of studies A total of 22 studies that reported NOTES procedures (intra-abdominal) were included in this review, while five SAGES 2006 and 27 SAGES 2007 abstracts were also sourced for information that was used for background information and future directions (Appendix B). The included studies are shown in Table 1, and the methodological assessment and study design details are given in Appendix C. Various aspects of NOTES procedures have been reported by a select number of groups worldwide. As a result, there are some studies published by the same group that are likely to include some of the same animals and such studies have been identified as such in this report.
All included studies were non-comparative animal studies, which were designated level IV evidence. Although a few of the studies included in this review followed animals for a short survival period after NOTES procedures were performed, all of the included studies were essentially pilot/feasibility studies. As no comparative studies were included in this review, it is not possible to compare NOTES procedures with current intra-abdominal surgery alternatives. Additionally, as the included studies are feasibility studies in animals, outcomes are not necessarily comparable with those in a clinical setting treating human patients.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 16
Table 1. Summary of included studies
Study Location N NOTES intervention (N*) Survival† Study (N*)
Survival† period (days)
Peroral access (Bergstrom et al. 2006) Japan & UK 12 Anastomosis (12) Yes (6) 7-10 (Fritscher-Ravens et al. 2003) UK & Sweden 16 Anastomosis (12) Yes (16) 28 (Fritscher-Ravens et al. 2006) UK & Sweden 6 Lymphadenectomy (6) NR 21-28 (Jagannath et al. 2005) USA 6 Fallopian tube ligation (6) Yes (6) 14-21 (Kalloo et al. 2004) USA 17 Biopsy (5) Yes (5) 14 (Kantsevoy et al. 2005) USA 2 Anastomosis (2) Yes (2) 14 (Kantsevoy et al. 2006a) USA 6 Splenectomy (6) No 0 (Kantsevoy et al. 2006b) USA 11 Anastomosis (11) No 0 (McGee et al. 2007d) USA 4 Intra-abdominal pressure monitoring
(4) No 0
(Merrifield et al. 2006) USA 5 Oophorectomy, tubectomy, hysterectomy (5)
Yes (5) 14
(Onders et al. 2007a) USA 4 Diaphragm pacing (4) No 0 (Onders et al. 2007b) USA 8 Biopsy (8) No 0 (Park et al. 2005) UK & Sweden 16 Anastomosis (3); Cholecystectomy
(5) Yes (8) 14-28
(Sumiyama et al. 2006) USA 5 Appendicectomy (2) Yes (5) 1-2 (Sumiyama et al. 2007) USA 6 Multiple gastrotomy closure (6) Yes (5) 7 (Swanstrom et al. 2005)‡ USA 10 Cholecystectomy (3); Biopsy (10) No 0 (Wagh et al. 2005) USA 8§ Oophorectomy, tubectomy,
hysterectomy (6) Yes (3) ≥1
(Wagh et al. 2006) USA 6 Oophorectomy, tubectomy, hysterectomy (6)
Yes (6) 14
Transanal access (Fong et al. 2007) USA 6 Peritoneoscopy (6) Yes (6) 14 (Pai et al. 2006) USA 5 Cholecystectomy (5) Yes (5) 14 Transurethral access (Lima et al. 2006) Portugal 8 Biopsy (8) Yes (5) 15 Peroral & transurethral access (Rolanda et al. 2007) Portugal 15 Cholecystectomy (7) No 0 * For ‘NOTES intervention’ and ‘survival study’, n=number of subjects receiving this treatment (not all subjects in study necessarily received intervention or followed for survival period); † Survival refers to monitoring of animals post-procedure for signs of morbidity, mortality and recovery; ‡ Endoscopic devices were inserted via oesophagectomy for ease of access in developmental procedure. This does not affect any other part of procedure or results, so access point will be considered peroral for this review; § 1 cadaver was also used
Intra-abdominal access route Access routes adopted by studies included in this review included the mouth, anus or urethra, followed by a transgastric, transcolonic or transvesical incision, respectively. Seventeen studies used peroral access, two studies opted for peranal access, one study used perurethral access and one study used a combined approach, employing both peroral and transurethral access (Table 1). All studies reported the method for viscerotomy creation, but only 16 studies reported the method of viscerotomy closure, if any (Fong et al. 2007; Fritscher-Ravens et al. 2006; Jagannath et al. 2005; Kalloo et al. 2004; Lima et al. 2006; Merrifield et al. 2006; Onders et al. 2007a; Onders et al. 2007b; Pai et al. 2006; Park et al. 2005; Rolanda et al. 2007; Sumiyama et al. 2006; Sumiyama et al. 2007; Swanstrom et al. 2005; Wagh et al. 2005; Wagh et al. 2006).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 17
NOTES interventions Anastomosis
Five studies reported anastomosis creation using NOTES, all of which were performed per-orally. Various novel devices to aid anastomosis creation were tested in these studies and specific aspects such as thread firing, were also reported. One study trialled a novel anastomosis method which only required access to a single lumen, the stomach (Fritscher-Ravens et al. 2003), while another study investigated the use of an Endoscopic Transilluminator (ET) in assisting NOTES anastomosis creation (Kantsevoy et al. 2006b). Four of these studies followed the animals for a period of 1-4 weeks following surgery to assess recovery and survival (Bergstrom et al. 2006; Fritscher-Ravens et al. 2003; Kantsevoy et al. 2005; Park et al. 2005), however one study euthanized the animals immediately following surgery (Kantsevoy et al. 2006b). Four of the five studies investigating NOTES anastomosis creation performed gastrojejunal anastomosis (Bergstrom et al. 2006; Fritscher-Ravens et al. 2003; Kantsevoy et al. 2005; Kantsevoy et al. 2006b) and two of the studies performed cholecystogastric anastomosis (Fritscher-Ravens et al. 2003; Park et al. 2005).
Cholecystectomy Four articles reported cholecystectomy performed using NOTES. Two of these studies used transgastric access (Park et al. 2005; Swanstrom et al. 2005), one used transcolonic access (Pai et al. 2006) and one used transgastric access combined with transurethral access (Rolanda et al. 2007). Two studies followed the animals for a survival period of 2-4 weeks following surgery (Pai et al. 2006; Park et al. 2005), but animals were euthanized immediately following surgery in the other two studies.
Appendicectomy One study investigated the use of NOTES to perform appendicectomies (Sumiyama et al. 2006). The procedure, performed transgastricly, was not strictly an appendicectomy, but a model of appendicectomy using injected porcine uterine horns to imitate acute appendicitis. The procedure involved two NOTES procedures: the first procedure used transgastric access to locate and inject uterine horns to create a model of appendicitis, followed by gastrotomy closure; the second procedure involved creation of a new gastrotomy at the previous site to assess the appendicitis model and to perform the ‘appendicectomy’. The study was not strictly a survival study, but animals were followed for a period of 1-2 days in between procedures and euthanized after the model appendicectomy.
Splenectomy One study reported transgastric splenectomies using NOTES (Kantsevoy et al. 2006a). Animals in this study were euthanized following surgery.
Oophorectomy, tubectomy and hysterectomy Four studies reported NOTES oophorectomy, tubectomy and/or partial hysterectomy. All procedures were transgastric (Merrifield et al. 2006; Sumiyama et al. 2006; Wagh et al. 2005; Wagh et al. 2006). Two studies reported transgastric
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 18
oophorectomy and tubectomy (Wagh et al. 2005; Wagh et al. 2006) and three studies reported partial hysterectomy (Merrifield et al. 2006; Sumiyama et al. 2006; Wagh et al. 2005). The study by Sumiyama et al. (2006) investigating model appendicectomy used partial hysterectomy as the model for appendicitis, but will be discussed under appendicectomy in this review.
Fallopian tube ligation One of the studies included in this review reported transgastric fallopian tube ligation using NOTES (Jagannath et al. 2005).
Lymphadenectomy One study reported a novel method of transgastric lymphadenectomy using NOTES (Fritscher-Ravens et al. 2006).
Diaphragm pacing One of the included studies investigated the use of NOTES for temporary diaphragm pacing (Onders et al. 2007a). This study reported a transgastric approach to inserting a diaphragm mapping device and diaphragm pacing system (DPS) to electrically stimulate diaphragm contractions in difficult to wean (from mechanical ventilation) ICU patients.
Intra-abdominal pressure monitoring One study included in this review investigated the reliability of monitoring intra-abdominal pressure during NOTES procedures using several different methods in order to determine a suitable pressure-monitoring method for future NOTES procedures (McGee et al. 2007d). In this study, intra-abdominal pressure was recorded using various methods while NOTES was used to perform transgastric peritoneoscopy.
Peritoneoscopy and biopsy Most of the included studies used NOTES to perform peritoneoscopy, often in addition to other procedures, however in some cases, peritoneoscopy was the main intervention following viscerotomy creation. In four of these studies, a biopsy was also performed (Kalloo et al. 2004; Lima et al. 2006; Onders et al. 2007b; Swanstrom et al. 2005).
Subject characteristics All of the included studies used pigs, with the exception of one study, which used four mongrel dogs in addition to six pigs (Swanstrom et al. 2005). Many studies reported outcomes for a group of animals, where the first few animals were used to trial and optimise the novel procedure and learn new surgical techniques. One study used a cadaver for the development and learning of NOTES techniques that were used in eight subsequent live animals (Wagh et al. 2005). In this study, outcomes using the cadaver were often pooled with the live animals and were not distinguished from the live animals. It is noted where this was the case.
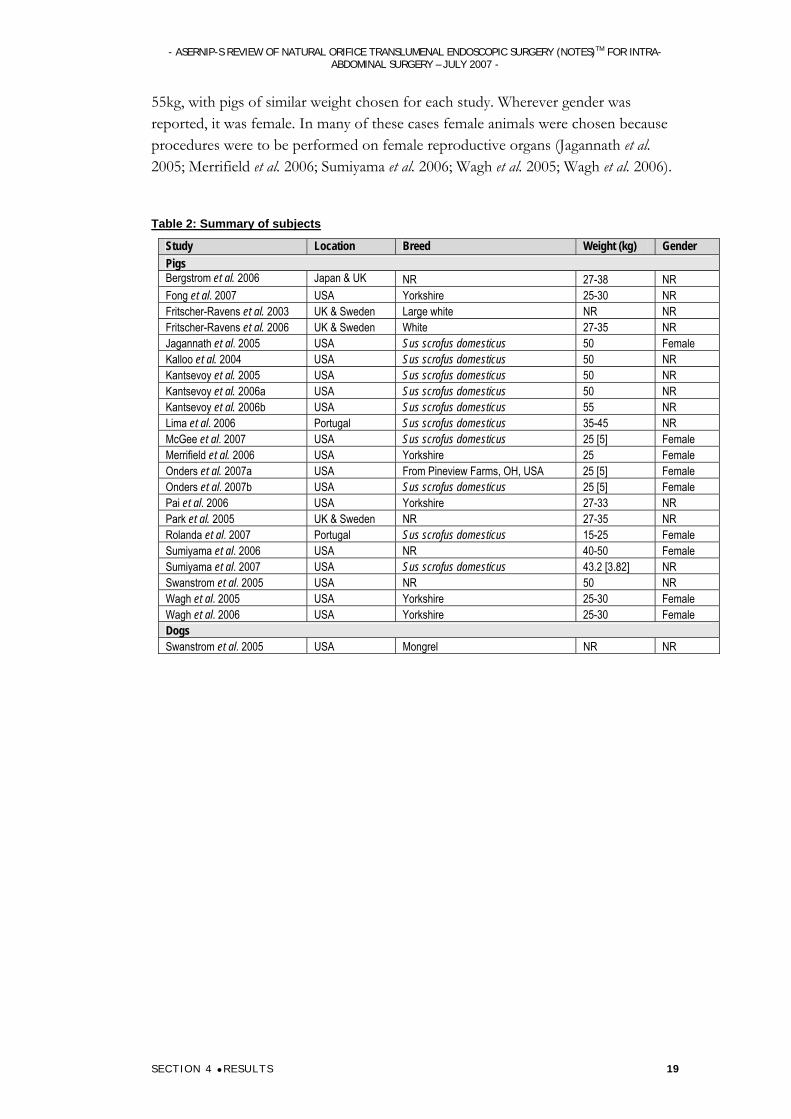
The pigs used in these studies were predominately Sus scrofus domesticus, however some Yorkshire and White pigs were also used (Table 2). Animal weight ranged from 15-
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 19
55kg, with pigs of similar weight chosen for each study. Wherever gender was reported, it was female. In many of these cases female animals were chosen because procedures were to be performed on female reproductive organs (Jagannath et al. 2005; Merrifield et al. 2006; Sumiyama et al. 2006; Wagh et al. 2005; Wagh et al. 2006).
Table 2: Summary of subjects
Study Location Breed Weight (kg) Gender Pigs Bergstrom et al. 2006 Japan & UK NR 27-38 NR Fong et al. 2007 USA Yorkshire 25-30 NR Fritscher-Ravens et al. 2003 UK & Sweden Large white NR NR Fritscher-Ravens et al. 2006 UK & Sweden White 27-35 NR Jagannath et al. 2005 USA Sus scrofus domesticus 50 Female Kalloo et al. 2004 USA Sus scrofus domesticus 50 NR Kantsevoy et al. 2005 USA Sus scrofus domesticus 50 NR Kantsevoy et al. 2006a USA Sus scrofus domesticus 50 NR Kantsevoy et al. 2006b USA Sus scrofus domesticus 55 NR Lima et al. 2006 Portugal Sus scrofus domesticus 35-45 NR McGee et al. 2007 USA Sus scrofus domesticus 25 [5] Female Merrifield et al. 2006 USA Yorkshire 25 Female Onders et al. 2007a USA From Pineview Farms, OH, USA 25 [5] Female Onders et al. 2007b USA Sus scrofus domesticus 25 [5] Female Pai et al. 2006 USA Yorkshire 27-33 NR Park et al. 2005 UK & Sweden NR 27-35 NR Rolanda et al. 2007 Portugal Sus scrofus domesticus 15-25 Female Sumiyama et al. 2006 USA NR 40-50 Female Sumiyama et al. 2007 USA Sus scrofus domesticus 43.2 [3.82] NR Swanstrom et al. 2005 USA NR 50 NR Wagh et al. 2005 USA Yorkshire 25-30 Female Wagh et al. 2006 USA Yorkshire 25-30 Female Dogs Swanstrom et al. 2005 USA Mongrel NR NR
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 20
Results
Efficacy
Success of surgical techniques The following outcomes are related to the efficacy of individual components of NOTES rather than the efficacy of the NOTES intervention as a whole. Efficacy of viscerotomy creation and closure will be reported in this section, followed by pneumoperitoneum-related issues and then efficacy and challenges of visualisation, manoeuvrability and grasping during NOTES. Efficacy of whole NOTES procedures will be discussed later, under ‘Success of NOTES intervention and techniques’. As these studies are all performed in animals they can only give an indication of the feasibility of NOTES in future human patient studies.
NOTES viscerotomy creation All studies reported viscerotomy creation method, however only some of these studies made any mention of success or complications encountered. In most cases, the visceral incision site was carefully chosen to minimise complications and optimise peritoneal access for the chosen procedure.
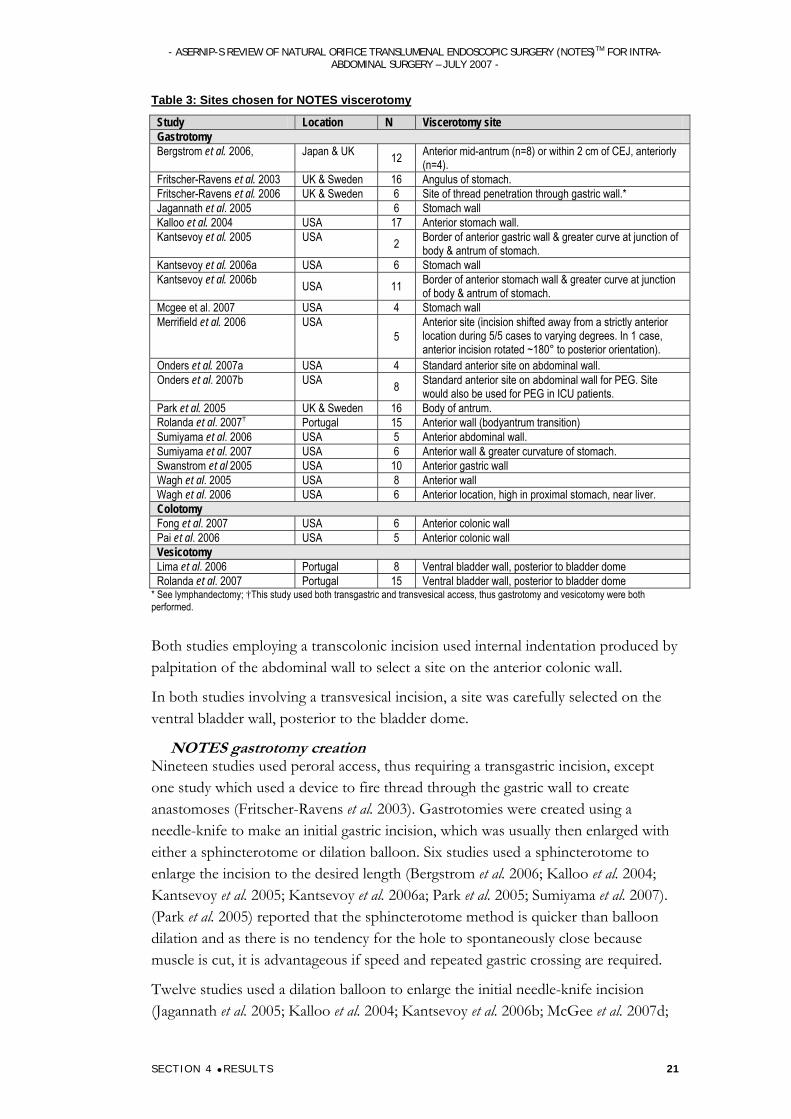
NOTES viscerotomy site Gastrotomy sites were generally chosen in an anterior location to avoid cutting into blood vessels and to minimise complications such as bleeding and spillage of gastric contents (Table 3). Park et al. (2005) chose a site a few centimetres away from the gallbladder instead of immediately adjacent to allow better access to the gallbladder in a recurved position and ease of pulling it through gastric incision to make the anastomosis. Great care was taken using transillumination and abdominal compression to penetrate the stomach anteriorly, as the lesser sac was entered on two occasions in early experience.
Rolanda et al. (2007) used a gastroscope observing internal stomach indentation produced by external abdominal palpation as well as external gastric-wall images obtained with a transvesically inserted EndoEye or ureteroscope, to select an optimal incision site and to avoid damage to gastric vessels and surrounding organs. Other studies also reported using external finger palpitation of anterior abdominal wall to locate the site for incision on the gastric wall (Bergstrom et al. 2006; Merrifield et al. 2006; Sumiyama et al. 2006; Wagh et al. 2006), sometimes aided by transillumination (Bergstrom et al. 2006; Rolanda et al. 2007; Sumiyama et al. 2006) or endoscopic ultrasound(EUS) (Wagh et al. 2006), to help to avoid adjacent organs and major vessels.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 21
Table 3: Sites chosen for NOTES viscerotomy
Study Location N Viscerotomy site Gastrotomy Bergstrom et al. 2006, Japan & UK 12 Anterior mid-antrum (n=8) or within 2 cm of CEJ, anteriorly
(n=4). Fritscher-Ravens et al. 2003 UK & Sweden 16 Angulus of stomach. Fritscher-Ravens et al. 2006 UK & Sweden 6 Site of thread penetration through gastric wall.* Jagannath et al. 2005 6 Stomach wall Kalloo et al. 2004 USA 17 Anterior stomach wall. Kantsevoy et al. 2005 USA 2 Border of anterior gastric wall & greater curve at junction of
body & antrum of stomach. Kantsevoy et al. 2006a USA 6 Stomach wall Kantsevoy et al. 2006b USA 11 Border of anterior stomach wall & greater curve at junction
of body & antrum of stomach. Mcgee et al. 2007 USA 4 Stomach wall Merrifield et al. 2006 USA
5 Anterior site (incision shifted away from a strictly anterior location during 5/5 cases to varying degrees. In 1 case, anterior incision rotated ~180° to posterior orientation).
Onders et al. 2007a USA 4 Standard anterior site on abdominal wall. Onders et al. 2007b USA 8 Standard anterior site on abdominal wall for PEG. Site
would also be used for PEG in ICU patients. Park et al. 2005 UK & Sweden 16 Body of antrum. Rolanda et al. 2007† Portugal 15 Anterior wall (bodyantrum transition) Sumiyama et al. 2006 USA 5 Anterior abdominal wall. Sumiyama et al. 2007 USA 6 Anterior wall & greater curvature of stomach. Swanstrom et al 2005 USA 10 Anterior gastric wall Wagh et al. 2005 USA 8 Anterior wall Wagh et al. 2006 USA 6 Anterior location, high in proximal stomach, near liver. Colotomy Fong et al. 2007 USA 6 Anterior colonic wall Pai et al. 2006 USA 5 Anterior colonic wall Vesicotomy Lima et al. 2006 Portugal 8 Ventral bladder wall, posterior to bladder dome Rolanda et al. 2007 Portugal 15 Ventral bladder wall, posterior to bladder dome
* See lymphandectomy; †This study used both transgastric and transvesical access, thus gastrotomy and vesicotomy were both performed.
Both studies employing a transcolonic incision used internal indentation produced by palpitation of the abdominal wall to select a site on the anterior colonic wall.
In both studies involving a transvesical incision, a site was carefully selected on the ventral bladder wall, posterior to the bladder dome.
NOTES gastrotomy creation Nineteen studies used peroral access, thus requiring a transgastric incision, except one study which used a device to fire thread through the gastric wall to create anastomoses (Fritscher-Ravens et al. 2003). Gastrotomies were created using a needle-knife to make an initial gastric incision, which was usually then enlarged with either a sphincterotome or dilation balloon. Six studies used a sphincterotome to enlarge the incision to the desired length (Bergstrom et al. 2006; Kalloo et al. 2004; Kantsevoy et al. 2005; Kantsevoy et al. 2006a; Park et al. 2005; Sumiyama et al. 2007). (Park et al. 2005) reported that the sphincterotome method is quicker than balloon dilation and as there is no tendency for the hole to spontaneously close because muscle is cut, it is advantageous if speed and repeated gastric crossing are required.
Twelve studies used a dilation balloon to enlarge the initial needle-knife incision (Jagannath et al. 2005; Kalloo et al. 2004; Kantsevoy et al. 2006b; McGee et al. 2007d;
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 22
Merrifield et al. 2006; Onders et al. 2007a; Onders et al. 2007b; Park et al. 2005; Rolanda et al. 2007; Sumiyama et al. 2006; Wagh et al. 2005; Wagh et al. 2006). Park et al. (2005) noted that the balloon dilation method has the advantage that following endoscope withdrawal, the muscle layers tend to spring back together, partially closing the defect. This can also be a disadvantage, as it can be difficult to get back through the defect with the endoscope.
Many articles reported that using a guidewire aided gastrotomy creation (Bergstrom et al. 2006; Kalloo et al. 2004; McGee et al. 2007d; Onders et al. 2007a; Park et al. 2005; Rolanda et al. 2007). One study did not report details of gastrotomy creation, only stating that the gastrotomy was created using standard energy sources (Swanstrom et al. 2005). In a study employing a combination of transgastric and transvesical access, Rolanda et al (2007) found that the uteroscope inserted through the vesicotomy was very useful in assisting the passage of the gastroscope through the transgastric incision.
One study used a slightly different technique for gastrotomy creation, as the incision was made after device firing through the gastric wall to capture and pull a lymph node back to the exterior stomach wall (Fritscher-Ravens et al. 2006). In this case, the incision was made with a needle-knife by repetitively cutting at the site of the thread that was fired through the gastric wall, to create an incision large enough to pull the captured lymph node through and was aided by pulling on the thread.
Gastrotomies were successfully created in all cases and where reported, were performed easily and without complications such as bleeding, regardless of incision method (Bergstrom et al. 2006; Kalloo et al. 2004; Kantsevoy et al. 2005; Onders et al. 2007b; Park et al. 2005; Rolanda et al. 2007; Swanstrom et al. 2005; Wagh et al. 2005). Where nothing was reported in relation to success or complications relating to gastrotomy creation, it is probable that the gastrotomy was created without major complication.
NOTES colotomy creation Two studies used a transcolonic route to access the peritoneal cavity, necessitating a transcolonic incision. Colonotomies required a different method of incision to gastrotomy creation and also necessitated extensive site preparation to remove and disinfect faecal matter that could obstruct equipment and pose a great risk of infection (Fong et al. 2007; Pai et al. 2006) (see infection related complications).
Fong et al. (2007) used a standard needle-knife in two of their six pigs and a prototype incision and closure device in the other four. A purse-string suture was deployed around the planned incision site using a dual ferrule mechanism and the incision was created using a blade mechanism at the tip of the device. Transcolonic incisions were successfully performed in all six pigs (100%) without complication and balloon (or sphincterotome) dilation was not required because colonotomies were easily dilated.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 23
Pai et al. (2006) also used a needle knife to create colonic incisions, which did not require dilation. In this study a catheter was advanced through the incision before endoscope insertion. This method was successful in 5/5 cases (100%).
NOTES vesicotomy creation Two studies used a transurethral route to access the peritoneal cavity, which required a transvesical incision (Lima et al. 2006; Rolanda et al. 2007). Incisions were created with scissors introduced through the uteroscope working channel and an opened uretal catheter was pushed through this incision into the peritoneal cavity. The vesical hole was enlarged with the dilator of the ureterorenoscope sheath, which was enveloped by a flexible over tube. The dilator was guided through the bladder wall by passage over a flexible tip guidewire, which spared muscle cutting. Lima et al. (2006) used three non-survival pigs to acquire the skills necessary to perform transvesical peritoneoscopy and performed the vesicotomy without complication in the remaining five pigs. Rolanda et al (2007) performed the vesicotomy without complication in all pigs, but as they are the same investigators as Lima et al. (2006), they most probably acquired necessary skills during the first procedure.
NOTES viscerotomy closure NOTES gastrotomy closure
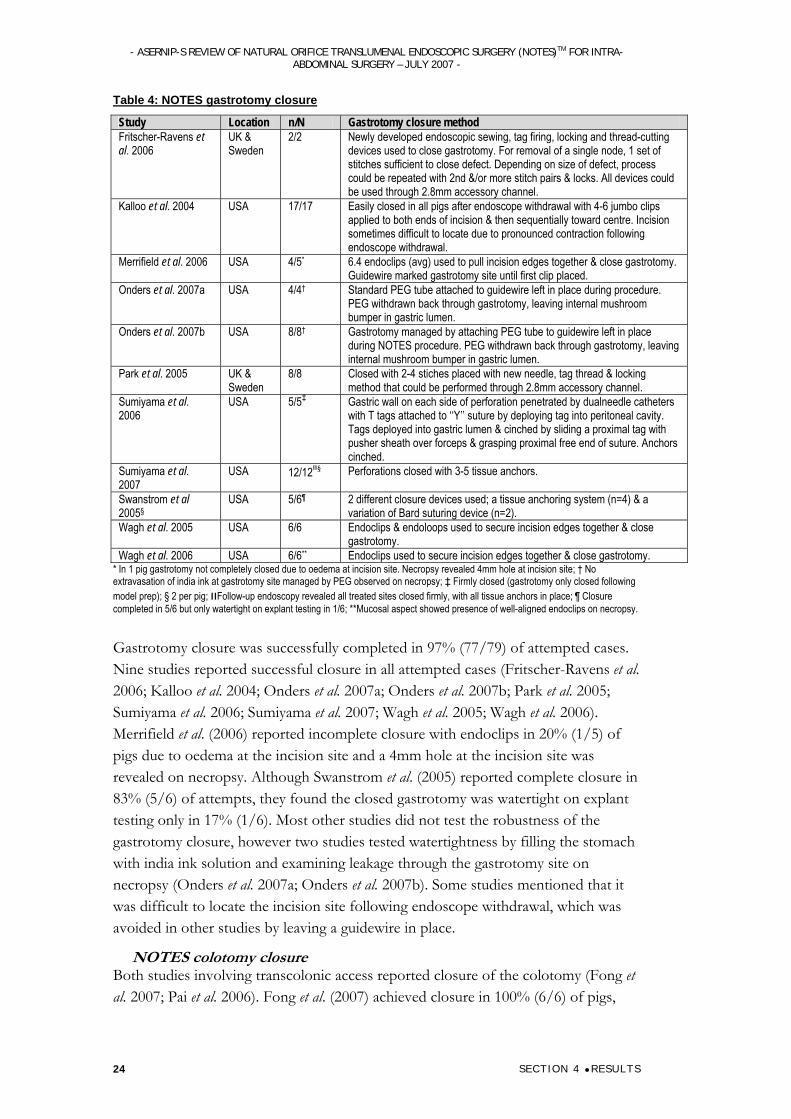
Gastrotomy closure was attempted in 11 studies, using various devices including endoclips, jumbo clips, endoloops, mushroom bumper from PEG tube and tissue anchor/tag systems (Fritscher-Ravens et al. 2006; Kalloo et al. 2004; Merrifield et al. 2006; Onders et al. 2007a; Onders et al. 2007b; Park et al. 2005; Sumiyama et al. 2006; Sumiyama et al. 2007; Swanstrom et al. 2005; Wagh et al. 2005; Wagh et al. 2006) (Table 4). Transgastric procedures where a gastrojejunal or cholecystogastric anastomosis was created did not require gastrotomy closure, as the incision formed part of the anastomosis (Bergstrom et al. 2006; Fritscher-Ravens et al. 2003; Kantsevoy et al. 2005; Kantsevoy et al. 2006b; Park et al. 2005). Three articles did not report gastrotomy closure, often because gastrotomy closure was unnecessary in non-survival feasibility studies where the animal was euthanized immediately following surgery (Jagannath et al. 2005; Kantsevoy et al. 2006a; McGee et al. 2007d; Rolanda et al. 2007). Rolanda et al. (2007) stated that no attempt was made to close the gastrotomy, as in preliminary experiments (n=9), gastrostomy closure with endoscopic clips was unreliable.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 24
Table 4: NOTES gastrotomy closure
Study Location n/N Gastrotomy closure method Fritscher-Ravens et al. 2006
UK & Sweden
2/2 Newly developed endoscopic sewing, tag firing, locking and thread-cutting devices used to close gastrotomy. For removal of a single node, 1 set of stitches sufficient to close defect. Depending on size of defect, process could be repeated with 2nd &/or more stitch pairs & locks. All devices could be used through 2.8mm accessory channel.
Kalloo et al. 2004 USA 17/17 Easily closed in all pigs after endoscope withdrawal with 4-6 jumbo clips applied to both ends of incision & then sequentially toward centre. Incision sometimes difficult to locate due to pronounced contraction following endoscope withdrawal.
Merrifield et al. 2006 USA 4/5* 6.4 endoclips (avg) used to pull incision edges together & close gastrotomy. Guidewire marked gastrotomy site until first clip placed.
Onders et al. 2007a USA 4/4† Standard PEG tube attached to guidewire left in place during procedure. PEG withdrawn back through gastrotomy, leaving internal mushroom bumper in gastric lumen.
Onders et al. 2007b USA 8/8† Gastrotomy managed by attaching PEG tube to guidewire left in place during NOTES procedure. PEG withdrawn back through gastrotomy, leaving internal mushroom bumper in gastric lumen.
Park et al. 2005 UK & Sweden
8/8 Closed with 2-4 stiches placed with new needle, tag thread & locking method that could be performed through 2.8mm accessory channel.
Sumiyama et al. 2006
USA 5/5‡ Gastric wall on each side of perforation penetrated by dualneedle catheters with T tags attached to ‘‘Y’’ suture by deploying tag into peritoneal cavity. Tags deployed into gastric lumen & cinched by sliding a proximal tag with pusher sheath over forceps & grasping proximal free end of suture. Anchors cinched.
Sumiyama et al. 2007
USA 12/12װ§ Perforations closed with 3-5 tissue anchors.
Swanstrom et al 2005§
USA 5/6¶ 2 different closure devices used; a tissue anchoring system (n=4) & a variation of Bard suturing device (n=2).
Wagh et al. 2005 USA 6/6 Endoclips & endoloops used to secure incision edges together & close gastrotomy.
Wagh et al. 2006 USA 6/6** Endoclips used to secure incision edges together & close gastrotomy. * In 1 pig gastrotomy not completely closed due to oedema at incision site. Necropsy revealed 4mm hole at incision site; † No extravasation of india ink at gastrotomy site managed by PEG observed on necropsy; ‡ Firmly closed (gastrotomy only closed following model prep); § 2 per pig; װFollow-up endoscopy revealed all treated sites closed firmly, with all tissue anchors in place; ¶ Closure completed in 5/6 but only watertight on explant testing in 1/6; **Mucosal aspect showed presence of well-aligned endoclips on necropsy.
Gastrotomy closure was successfully completed in 97% (77/79) of attempted cases. Nine studies reported successful closure in all attempted cases (Fritscher-Ravens et al. 2006; Kalloo et al. 2004; Onders et al. 2007a; Onders et al. 2007b; Park et al. 2005; Sumiyama et al. 2006; Sumiyama et al. 2007; Wagh et al. 2005; Wagh et al. 2006). Merrifield et al. (2006) reported incomplete closure with endoclips in 20% (1/5) of pigs due to oedema at the incision site and a 4mm hole at the incision site was revealed on necropsy. Although Swanstrom et al. (2005) reported complete closure in 83% (5/6) of attempts, they found the closed gastrotomy was watertight on explant testing only in 17% (1/6). Most other studies did not test the robustness of the gastrotomy closure, however two studies tested watertightness by filling the stomach with india ink solution and examining leakage through the gastrotomy site on necropsy (Onders et al. 2007a; Onders et al. 2007b). Some studies mentioned that it was difficult to locate the incision site following endoscope withdrawal, which was avoided in other studies by leaving a guidewire in place.
NOTES colotomy closure Both studies involving transcolonic access reported closure of the colotomy (Fong et al. 2007; Pai et al. 2006). Fong et al. (2007) achieved closure in 100% (6/6) of pigs,
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 25
using different closure methods. In one pig, endoscopic clips were sequentially deployed along the incision from the superior margin to the inferior margin until complete closure was achieved. In another pig, forceps were used to pull margins of the incision into an open endoloop before subsequent closure and approximation of incision margins. Both of these closure methods were technically demanding and endoscope withdrawal from the peritoneal cavity caused air leakage into the abdomen and affected luminal distention and colotomy visualization. In four of the six pigs, a prototype closure device was trialled, in which a titanium knot was deployed to secure previously placed purse string suture and close the incision. Closure with this prototype device was easily achieved.
Pai et al. (2006) used a single endoloop to close the colonic incision in one of their five pigs and in the other four pigs they used 3-8 endoclips. Incision edges were secured together using one or both devices and residual air was evacuated from the peritoneum via an external percutaneous catheter. Closure was achieved in only 80% (4/5) of pigs. In one pig (closure method not reported), complete closure of the colonic incision site not possible and a 4mm residual defect remained at the conclusion of surgery.
NOTES Vesicotomy Closure Lima et al. (2006) reported that the cystoscope showed obvious signs of contraction following ureteroscope withdrawal, making the vesicotomy appear like a puncture hole, so it was left unclosed without any apparent adverse effect. There is no mention of any vesicotomy closure in the other study involving transvesical access, but this was a non-survival study and the gastrotomy made during this procedure was not closed either (Rolanda et al. 2007).
Pneumoperitoneum creation during NOTES In the majority of studies, a CO2 pneumoperitoneum was created up to 12mmHg, to lift the abdominal wall away from the viscera and thus aid visualisation and manoeuvrability. This was usually created using a laparoscopic insufflation port and moderated with venting catheters to avoid complications such as respiratory compromise and multisystem organ failure that can occur with high pressure. Although some studies reported monitoring of vital signs to avoid complications, these were not reported in detail and no pneumoperitoneum-related complications were reported. No pneumoperitoneum was created in procedures using a prototype endoscopic firing device (Fritscher-Ravens et al. 2003; Fritscher-Ravens et al. 2006), thus avoiding any related complications.
Reliability of intra-abdominal pressure monitoring during NOTES One study investigated the reliability of various methods for monitoring intra-abdominal pressure during NOTES (McGee et al. 2007d). Following insufflation, intra-abdominal pressures were recorded simultaneously from the insufflator output (point A), RLQ transabdominal 12-gauge catheter (point B), Tygon tubing fastened alongside endoscope (point C), and the biopsy port at headset of endoscope (point D). A first-order least-squares fit was calculated to determine correlation of pressures

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 26
across all measurement points. The Pearson coefficient of correlation and coefficient of determination between biopsy port pressures (at point D) and the actual intra-abdominal pressures (at point B) were, respectively, 0.99 and 0.98, therefore biopsy port pressures were quite accurate in recording actual intra-abdominal pressures.
Success of visualisation using NOTES Only studies reporting or commenting on the success or quality of visualisation (Table 5), manoeuvrability or grasping are discussed in the following sections.
Standard endoscopic techniques such as rotation, torque and retroflection were usually adequate for visualisation in most studies, but were sometimes aided by external transillumination. Various measures were undertaken to improve visualisation in the peritoneal cavity such as the creation of a pneumoperitoneum (see above) and positional changes of the animal to move obstructive organs away from others. Such positional changes when using transgastric access, include a 15 head-down position to shift the bowel away from the uterus (Merrifield et al. 2006), Reverse Trendelenburg position to ‘‘retract’’ the spleen downward (Swanstrom et al. 2005), head-low, left or right lateral position for examining some parts of the small intestine and colon or a 45 degree head-low position used to displace intestinal loops and enable assessment of pelvic structures (Wagh et al. 2005). When using transcolonic access, positional changes included the ‘Reverse Trendelenburg’ position and right and left lateral rotation used to gain additional exposure of upper abdominal structures or ‘Trendelenburg’ position, which was used to examine the right and left lower quadrants (Fong et al. 2007).
Complications such as bleeding hindered visualisation. For example, during cholecystectomy Swanstrom et al. (2005) found that uncontrolled bleeding from a cystic artery caused loss of visualisation in one pig, while gallbladder perforation made identification of gallbladder dissection planes impossible in another.
Visualisation appeared to vary depending of the access port used. When the transgastric port was used, visualisation was generally good (Table 5). Visualisation using transcolonic access was not as reliable and many organs were unable to be identified (Fong et al. 2007; Pai et al. 2006). Rolanda et al. (2007) utilised both transvesical and transgastric ports to monitor all procedures, with a scope positioned through the transvesical port.
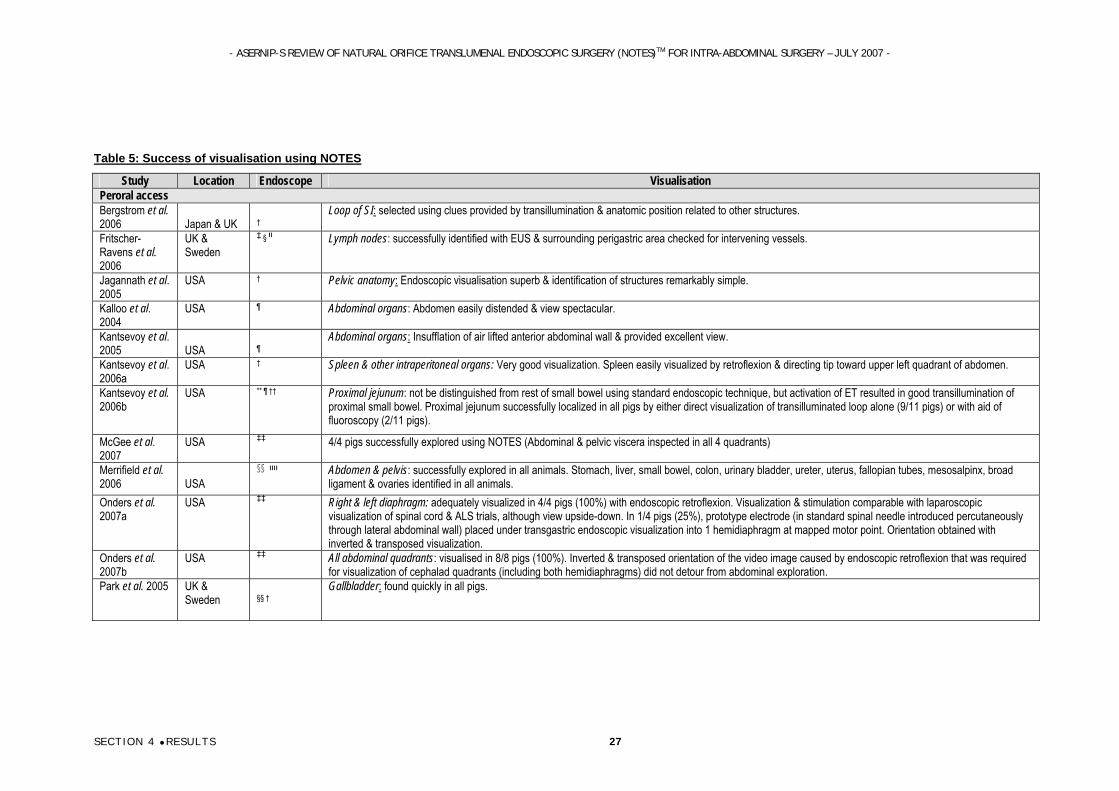
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 27
Table 5: Success of visualisation using NOTES
Study Location Endoscope Visualisation Peroral access Bergstrom et al. 2006
Japan & UK
†
Loop of SI: selected using clues provided by transillumination & anatomic position related to other structures.
Fritscher-Ravens et al. 2006
UK & Sweden
.Lymph nodes: successfully identified with EUS & surrounding perigastric area checked for intervening vessels װ § ‡
Jagannath et al. 2005
USA † Pelvic anatomy: Endoscopic visualisation superb & identification of structures remarkably simple.
Kalloo et al. 2004
USA ¶ Abdominal organs: Abdomen easily distended & view spectacular.
Kantsevoy et al. 2005
USA
¶
Abdominal organs: Insufflation of air lifted anterior abdominal wall & provided excellent view.
Kantsevoy et al. 2006a
USA † Spleen & other intraperitoneal organs: Very good visualization. Spleen easily visualized by retroflexion & directing tip toward upper left quadrant of abdomen.
Kantsevoy et al. 2006b
USA ** ¶ †† Proximal jejunum: not be distinguished from rest of small bowel using standard endoscopic technique, but activation of ET resulted in good transillumination of proximal small bowel. Proximal jejunum successfully localized in all pigs by either direct visualization of transilluminated loop alone (9/11 pigs) or with aid of fluoroscopy (2/11 pigs).
McGee et al. 2007
USA ‡‡ 4/4 pigs successfully explored using NOTES (Abdominal & pelvic viscera inspected in all 4 quadrants)
Merrifield et al. 2006
USA
װװ §§
Abdomen & pelvis: successfully explored in all animals. Stomach, liver, small bowel, colon, urinary bladder, ureter, uterus, fallopian tubes, mesosalpinx, broad ligament & ovaries identified in all animals.
Onders et al. 2007a
USA ‡‡ Right & left diaphragm: adequately visualized in 4/4 pigs (100%) with endoscopic retroflexion. Visualization & stimulation comparable with laparoscopic visualization of spinal cord & ALS trials, although view upside-down. In 1/4 pigs (25%), prototype electrode (in standard spinal needle introduced percutaneously through lateral abdominal wall) placed under transgastric endoscopic visualization into 1 hemidiaphragm at mapped motor point. Orientation obtained with inverted & transposed visualization.
Onders et al. 2007b
USA ‡‡ All abdominal quadrants: visualised in 8/8 pigs (100%). Inverted & transposed orientation of the video image caused by endoscopic retroflexion that was required for visualization of cephalad quadrants (including both hemidiaphragms) did not detour from abdominal exploration.
Park et al. 2005 UK & Sweden
§§ †
Gallbladder: found quickly in all pigs.
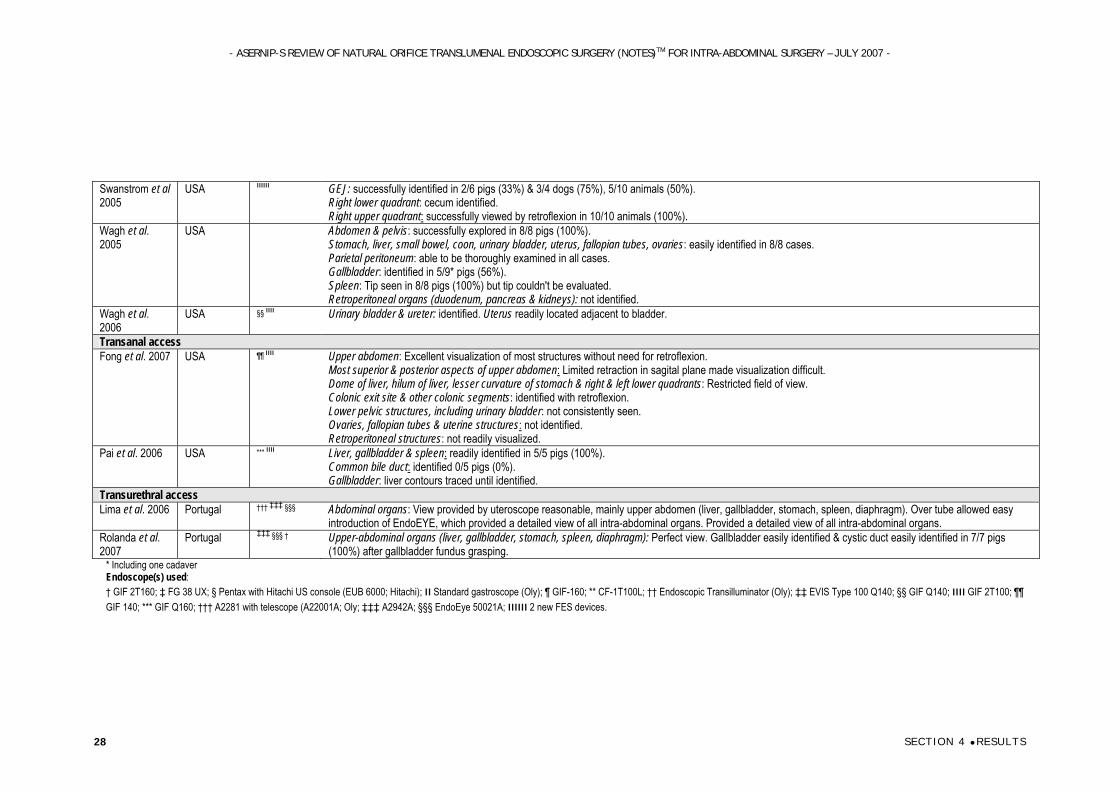
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 28
Swanstrom et al 2005
USA װװװ GEJ: successfully identified in 2/6 pigs (33%) & 3/4 dogs (75%), 5/10 animals (50%). Right lower quadrant: cecum identified. Right upper quadrant: successfully viewed by retroflexion in 10/10 animals (100%).
Wagh et al. 2005
USA Abdomen & pelvis: successfully explored in 8/8 pigs (100%). Stomach, liver, small bowel, coon, urinary bladder, uterus, fallopian tubes, ovaries: easily identified in 8/8 cases. Parietal peritoneum: able to be thoroughly examined in all cases. Gallbladder: identified in 5/9* pigs (56%). Spleen: Tip seen in 8/8 pigs (100%) but tip couldn't be evaluated. Retroperitoneal organs (duodenum, pancreas & kidneys): not identified.
Wagh et al. 2006
USA §§ װװ Urinary bladder & ureter: identified. Uterus readily located adjacent to bladder.
Transanal access Fong et al. 2007 USA ¶¶ װװ Upper abdomen: Excellent visualization of most structures without need for retroflexion.
Most superior & posterior aspects of upper abdomen: Limited retraction in sagital plane made visualization difficult. Dome of liver, hilum of liver, lesser curvature of stomach & right & left lower quadrants: Restricted field of view. Colonic exit site & other colonic segments: identified with retroflexion. Lower pelvic structures, including urinary bladder: not consistently seen. Ovaries, fallopian tubes & uterine structures: not identified. Retroperitoneal structures: not readily visualized.
Pai et al. 2006 USA *** װװ Liver, gallbladder & spleen: readily identified in 5/5 pigs (100%). Common bile duct: identified 0/5 pigs (0%). Gallbladder: liver contours traced until identified.
Transurethral access Lima et al. 2006 Portugal ††† ‡‡‡ §§§ Abdominal organs: View provided by uteroscope reasonable, mainly upper abdomen (liver, gallbladder, stomach, spleen, diaphragm). Over tube allowed easy
introduction of EndoEYE, which provided a detailed view of all intra-abdominal organs. Provided a detailed view of all intra-abdominal organs. Rolanda et al. 2007
Portugal ‡‡‡ §§§ † Upper-abdominal organs (liver, gallbladder, stomach, spleen, diaphragm): Perfect view. Gallbladder easily identified & cystic duct easily identified in 7/7 pigs (100%) after gallbladder fundus grasping.
* Including one cadaver Endoscope(s) used: † GIF 2T160; ‡ FG 38 UX; § Pentax with Hitachi US console (EUB 6000; Hitachi); װ Standard gastroscope (Oly); ¶ GIF-160; ** CF-1T100L; †† Endoscopic Transilluminator (Oly); ‡‡ EVIS Type 100 Q140; §§ GIF Q140; װװ GIF 2T100; ¶¶ GIF 140; *** GIF Q160; ††† A2281 with telescope (A22001A; Oly; ‡‡‡ A2942A; §§§ EndoEye 50021A; 2 װװװ new FES devices.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 29
Fritscher-Ravens et al. (2006) reported success using endoscopic ultrasound (EUS) for visualisation of lymph nodes to be selected for removal. This was useful to identify blood vessels in surrounding areas and avoided the requirement for an endoscope in the peritoneal cavity, thus minimising leakage, negating the need for a pneumoperitoneum and allowing the lymph node to be targeted and pulled back to the gastric wall without gastric incision.
Kantsevoy et al. (2006c) used an endoscopic transilluminator (ET) to direct the endoscope to proximal jejunum and reported that ET placement was completed without any technical problems in 100% (11/11) of pigs.
Success of manoeuvrability of equipment during NOTES Standard endoscopic techniques (torquing, retroflexion, rotation, scope reduction, tip deflection) were adequate in many cases but in others, movement was limited, making completion of procedures difficult. Creation of pneumoperitoneum appears to aid manoeuvrability in the peritoneal cavity by providing more space in which to move. Various endoscopes were used to perform NOTES procedures including standard endoscopes as well as specially designed prototypes and equipment such as overtube was often used to assist endoscope passage and increase stability.
Manoeuvrability in the upper abdominal quadrants posed few problems when using transgastric access, however a few more difficulties were encountered when manoeuvring endoscopic devices through a transcolonic port. In a study using transcolonic access, limited retraction in the sagital plane made scope control in the most superior and posterior aspects of the upper abdomen difficult (Fong et al. 2007). Scope control near the dome of liver, hilum of liver, lesser curvature of stomach and right and left lower quadrants were also restricted (Fong et al. 2007). Using a transvesical port, Lima et al. (2006) reported that the length of their ureteroscope allowed liver biopsy and falciform ligament section to be performed in all animals without difficulty and the use of an overtube allowed easy introduction of the EndoEye.
Success of grasping and organ manipulation during NOTES Although most procedures required grasping to manipulate organs/tissue at some stage, the difficulty and problems depended on the specific procedure and factors such as location of the organ, as organs which were situated further away, or were obstructed, were difficult to grasp. Most of the difficulties with grasping were reported during cholecystectomy or cholecystogastric anastomosis (Fritscher-Ravens et al. 2003; Pai et al. 2006; Park et al. 2005; Rolanda et al. 2007; Swanstrom et al. 2005) and techniques were often described in detail. Grasping and organ manipulation during anastomosis creation and other procedures including hysterectomy was also challenging, but achievable (Merrifield et al. 2006; Wagh et al. 2005). Grasping the cystic duct during cholecystectomy and grasping the jejunum or gallbladder firmly enough to pull it into the stomach for anastomosis creation also presented considerable challenges, which were solved in all cases (Pai et al. 2006; Park et al. 2005; Rolanda et al. 2007; Swanstrom et al. 2005).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 30
Wagh et al. (2006) found that grasping uterine horns with grasping forceps could be aided by the use of an endoloop. Grasping forceps were popular for grasping in most studies, but snares and endoscopes were also commonly used in combination. Most articles reported trial and error with different grasping techniques and equipment, however optimal methods have not yet been determined. Equipment was mostly passed through endoscopic accessory ports, which allowed greater stability and space to work. The access point appeared to effect grasping, as did the proximity of the organ to the access point.
Transgastric grasping and organ manipulation As with manoeuvrability, positional changes aided grasping by moving obstructing organs away from the target organ, such as a 15 degree head-down position used by Merrifield et al (2006) to shift the bowel away from the uterus.
A common challenge in organ manipulation was exposure of the cystic duct for cholecystectomy, as retraction of the floppy porcine hepatic lobes was difficult with most flexible endoscopic instruments (Park et al. 2005; Swanstrom et al. 2005). Park et al. (2005) were able to expose the cystic duct and artery by placing an endoscope as close as possible to the gallbladder and grasping it with two pairs of forceps, sometime aided by a grasper. They found that forceps were reasonably effective for grasping the gallbladder and did not cause bile leaks, but occasionally slipped off the gallbladder, necessitating repositioning. Manipulation of the gallbladder with snares was especially effective for pulling the gallbladder into the stomach to form cholecystogastric anastomoses but was less useful for dissection. Exposure of the gallbladder was performed by Swanstrom et al. (2005) with the endoscopic device in retroflexion, the locking body was used to hold up the liver while aggressive graspers were used to retract the infundibulum.
Swanstrom et al. (2005) achieved exposure of the oesophageal hiatus to identify the gastroesophageal junction in 50% (5/10) of animals by manoeuvring a retroflexed scope under the left liver lobe and using Reverse Trendelenburg position to retract the spleen downward.
The small bowel was easily grasped and run for several centimetres using two endoscopically-placed graspers by Swanstrom et al. (2005), Wagh et al. (2005) and Onders et al. (2007b). Following this, Onders et al. (2007b) also used two 2mm percutaneous needlescopic suture graspers (passed transabdominally) to enable complete evaluation of all intestines.
The caecum was successfully grasped and raised anteriorly in 100% (10/10) of animals by Swanstrom et al. (2005). They also reported that that tissue retraction in the stomach was best achieved either with the most aggressive (4mm) grasper trialled, or with a 2mm ‘corkscrew’ device.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 31
Transcolonic grasping and organ manipulation Positional changes were also useful in exposing organs for transcolonic grasping. Fong et al. (2007) achieved additional exposure of the gallbladder and cystic duct using blunt-tip probing and retraction of the overlying liver lobes with two forceps. Positional changes, including the Reverse Trendelenburg position and right and left lateral rotation were used to gain additional exposure of the upper abdominal structures. Using two forceps, segments of the small bowel and associated mesentery were traced for several centimetres along their length.
Pai et al. (2006) readily exposed the cystic duct and artery in three pigs using grasping forceps to pull the gallbladder away from the fossa, however in the other two pigs, the duct and artery were only identified after careful dissection of the organ from the fossa. Complete removal of the gallbladder was achieved with snare cautery.
Transgastric and transvesical grasping and organ manipulation Rolanda et al. (2007) transvesically grasped the gallbladder fundus and upwardly retracted it to expose the gallbladder infundibulum and the cystic duct. Transvesical gallbladder grasping allowed quick identification of the cystic duct and significant manipulation of the gallbladder, such as retraction of the gallbladder body in the major axis (up & down; right & left). This was particularly useful in selecting the best position for gastroscope-guided dissection. Small positional adjustments were also possible when using forceps introduced by the gastroscope. Coordination of gallbladder transvesical-transgastric manipulation proved feasible, with rapid progress during the experiments. After gallbladder fundus grasping with transvesical instruments, the gastroscope easily identified the cystic duct in all seven pigs. Gallbladder withdrawal was easily achieved with a grasper inserted through the gastroscope.
Success of NOTES intervention and techniques Success of NOTES anastomosis Anastomosis creation was successful in 100% (44/44) of reported cases, regardless of method (Table 6). Nine of the reported anastomoses were cholecystogastric (Fritscher-Ravens et al. 2003; Park et al. 2005) and the other 31 were gastrojejunal (Bergstrom et al. 2006; Fritscher-Ravens et al. 2003; Kantsevoy et al. 2005; Kantsevoy et al. 2006b). Kantsevoy et al. (2005), Fritscher-Ravens et al. (2003) and Bergstrom et al. reported that 100% (26/26) of anastomoses were patent on necropsy and no leakage was observed by these groups in 100% (20/20) of gastrojejunal anastomoses. Fritscher-Ravens et al. (2003) also reported that anastomoses withstood balloon dilation in 50% (6/12) of pigs, with bursting pressures ranging from 180-230mm Hg.
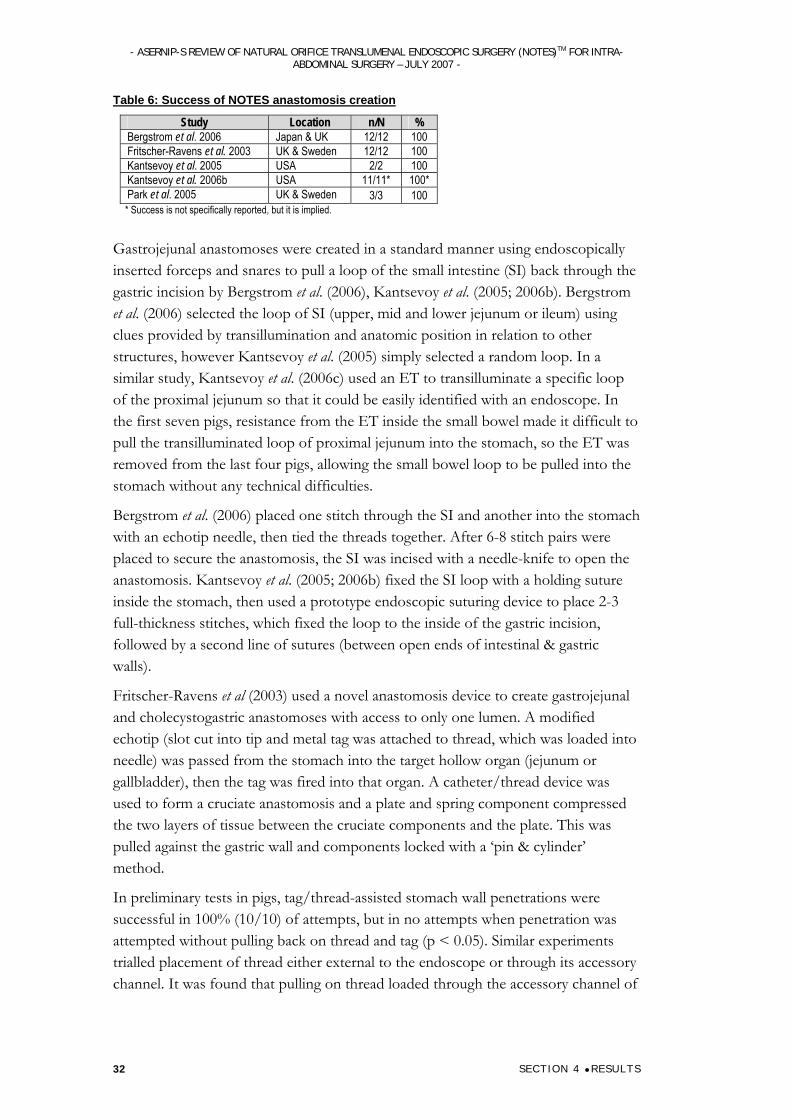
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 32
Table 6: Success of NOTES anastomosis creation
Study Location n/N % Bergstrom et al. 2006 Japan & UK 12/12 100 Fritscher-Ravens et al. 2003 UK & Sweden 12/12 100 Kantsevoy et al. 2005 USA 2/2 100 Kantsevoy et al. 2006b USA 11/11* 100* Park et al. 2005 UK & Sweden 3/3 100 * Success is not specifically reported, but it is implied.
Gastrojejunal anastomoses were created in a standard manner using endoscopically inserted forceps and snares to pull a loop of the small intestine (SI) back through the gastric incision by Bergstrom et al. (2006), Kantsevoy et al. (2005; 2006b). Bergstrom et al. (2006) selected the loop of SI (upper, mid and lower jejunum or ileum) using clues provided by transillumination and anatomic position in relation to other structures, however Kantsevoy et al. (2005) simply selected a random loop. In a similar study, Kantsevoy et al. (2006c) used an ET to transilluminate a specific loop of the proximal jejunum so that it could be easily identified with an endoscope. In the first seven pigs, resistance from the ET inside the small bowel made it difficult to pull the transilluminated loop of proximal jejunum into the stomach, so the ET was removed from the last four pigs, allowing the small bowel loop to be pulled into the stomach without any technical difficulties.
Bergstrom et al. (2006) placed one stitch through the SI and another into the stomach with an echotip needle, then tied the threads together. After 6-8 stitch pairs were placed to secure the anastomosis, the SI was incised with a needle-knife to open the anastomosis. Kantsevoy et al. (2005; 2006b) fixed the SI loop with a holding suture inside the stomach, then used a prototype endoscopic suturing device to place 2-3 full-thickness stitches, which fixed the loop to the inside of the gastric incision, followed by a second line of sutures (between open ends of intestinal & gastric walls).
Fritscher-Ravens et al (2003) used a novel anastomosis device to create gastrojejunal and cholecystogastric anastomoses with access to only one lumen. A modified echotip (slot cut into tip and metal tag was attached to thread, which was loaded into needle) was passed from the stomach into the target hollow organ (jejunum or gallbladder), then the tag was fired into that organ. A catheter/thread device was used to form a cruciate anastomosis and a plate and spring component compressed the two layers of tissue between the cruciate components and the plate. This was pulled against the gastric wall and components locked with a ‘pin & cylinder’ method.
In preliminary tests in pigs, tag/thread-assisted stomach wall penetrations were successful in 100% (10/10) of attempts, but in no attempts when penetration was attempted without pulling back on thread and tag (p < 0.05). Similar experiments trialled placement of thread either external to the endoscope or through its accessory channel. It was found that pulling on thread loaded through the accessory channel of

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 33
the retroflexed endoscope pulled tissue toward the endoscope, but pulling on thread loaded outside the endoscope pulled tissue away.
In subsequent experiments, the device was used to create anastomosis in live pigs. Firstly, the devices were successfully tested in four pigs after being surgically inserted into the SI or gallbladder. In another 12 pigs, the devices were placed entirely endoscopically without surgical assistance in the gallbladder (n=6) and the jejunum (n=6) to create cholecystogastric and gastrojejunal anastomosis, respectively. Upon inspection four days after surgery, the device had left the stomach in 50% (6/12) pigs, was found in the fundus of the stomach in 17% (2/12) of pigs, but had not completely eroded through in the last 33% (4/12) of pigs.
Park et al. (2005) successfully created cholecystogastric anastomoses via a transgastric port in 100% (3/3) of pigs. The gallbladder was securely grasped and pulled through the gastric incision, then stitched to the stomach wall in two of the pigs, or attached to the stomach wall with clips in the other pig. The anastomosis was completed by incising the intragastric portion of the gallbladder with a needle-knife.
Success of NOTES cholecystectomy NOTES cholecystectomy was attempted in four articles, using transgastric access in two (Park et al. 2005; Swanstrom et al. 2005), transcolonic access in one (Pai et al. 2006), and a combination of transvesical and transgastric access in the other (Rolanda et al. 2007). Cholecystectomy was successful in 33%-100% (median=100%) of cases. All cholecystectomies essentially involved exposure, clipping and ligation of the cystic duct and artery, followed by mobilisation of the gallbladder from the fossa and removal through the NOTES access point.
Table 7: Success of NOTES cholecystectomy
Study Location n/N % Pai et al. 2006 USA 5/5 100 Park et al. 2005 UK & Sweden 5/5 100 Rolanda et al. 2007 Portugal 7/7 100 Swanstrom et al. 2005 USA 1/3 33
Cholecystectomy was challenging due to difficulties in grasping and manipulating the gallbladder with the flexible endoscopic devices used to access the gallbladder via a natural orifice. Differences in pig anatomy to human anatomy also posed some challenges (i.e. large, floppy hepatic lobes and the gallbladder body is commonly hidden in liver parenchyma in pigs). The combined transvesical and transgastric approach allowed Rolanda et al. (2007) to co-ordinate grasping across these two ports to achieve more complex manipulations.
Endoscopic clips were used to control the cystic duct and artery in all studies, but Swanstrom et al. (2005) reported that in one animal, bleeding from the cystic artery was unable to be controlled, causing loss of visualisation and the attempt was abandoned. The other unsuccessful attempt reported by Swanstrom et al. (2005) was
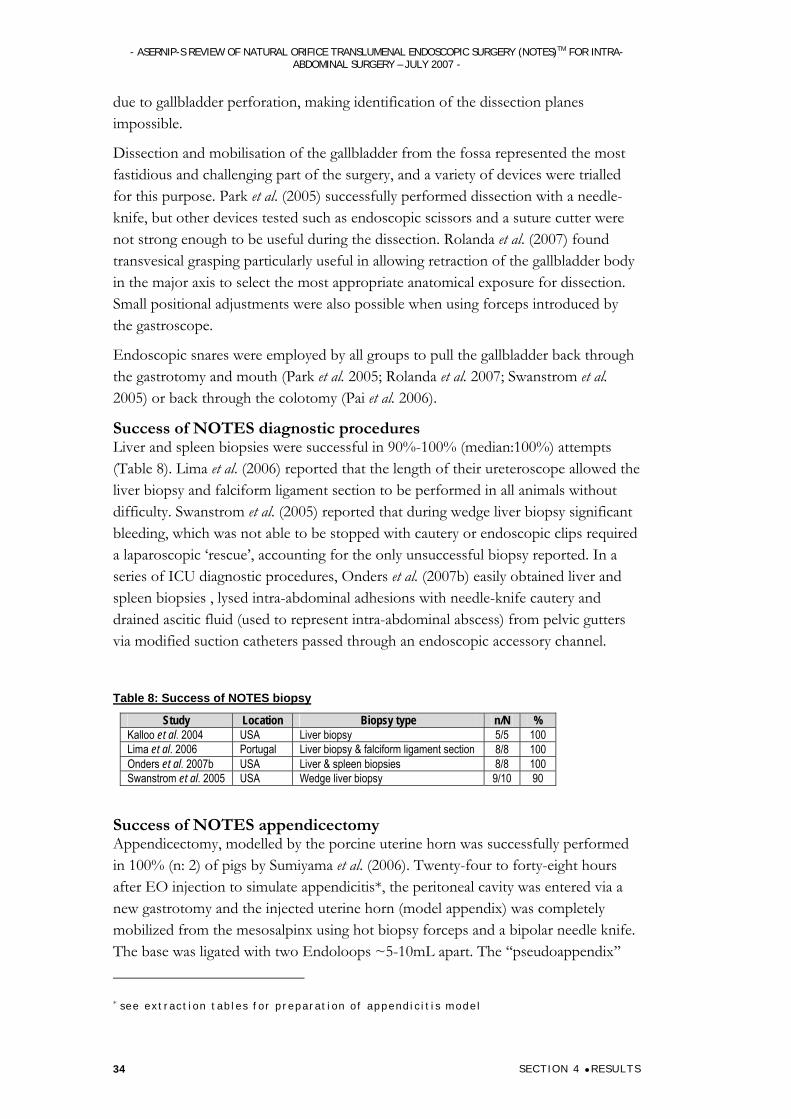
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 34
due to gallbladder perforation, making identification of the dissection planes impossible.
Dissection and mobilisation of the gallbladder from the fossa represented the most fastidious and challenging part of the surgery, and a variety of devices were trialled for this purpose. Park et al. (2005) successfully performed dissection with a needle-knife, but other devices tested such as endoscopic scissors and a suture cutter were not strong enough to be useful during the dissection. Rolanda et al. (2007) found transvesical grasping particularly useful in allowing retraction of the gallbladder body in the major axis to select the most appropriate anatomical exposure for dissection. Small positional adjustments were also possible when using forceps introduced by the gastroscope.
Endoscopic snares were employed by all groups to pull the gallbladder back through the gastrotomy and mouth (Park et al. 2005; Rolanda et al. 2007; Swanstrom et al. 2005) or back through the colotomy (Pai et al. 2006).
Success of NOTES diagnostic procedures Liver and spleen biopsies were successful in 90%-100% (median:100%) attempts (Table 8). Lima et al. (2006) reported that the length of their ureteroscope allowed the liver biopsy and falciform ligament section to be performed in all animals without difficulty. Swanstrom et al. (2005) reported that during wedge liver biopsy significant bleeding, which was not able to be stopped with cautery or endoscopic clips required a laparoscopic ‘rescue’, accounting for the only unsuccessful biopsy reported. In a series of ICU diagnostic procedures, Onders et al. (2007b) easily obtained liver and spleen biopsies , lysed intra-abdominal adhesions with needle-knife cautery and drained ascitic fluid (used to represent intra-abdominal abscess) from pelvic gutters via modified suction catheters passed through an endoscopic accessory channel.
Table 8: Success of NOTES biopsy
Study Location Biopsy type n/N % Kalloo et al. 2004 USA Liver biopsy 5/5 100 Lima et al. 2006 Portugal Liver biopsy & falciform ligament section 8/8 100 Onders et al. 2007b USA Liver & spleen biopsies 8/8 100 Swanstrom et al. 2005 USA Wedge liver biopsy 9/10 90
Success of NOTES appendicectomy Appendicectomy, modelled by the porcine uterine horn was successfully performed in 100% (n: 2) of pigs by Sumiyama et al. (2006). Twenty-four to forty-eight hours after EO injection to simulate appendicitis*, the peritoneal cavity was entered via a new gastrotomy and the injected uterine horn (model appendix) was completely mobilized from the mesosalpinx using hot biopsy forceps and a bipolar needle knife. The base was ligated with two Endoloops ~5-10mL apart. The ‘‘pseudoappendix’’ * see extract ion tab les for p reparat ion o f append ic i t i s mode l

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 35
was then excised using an electrosurgical bipolar snare placed between two endoloops. On necropsy, the right uterine horn was successfully resected up to uterine bifurcation and an endoloop firmly sealed the uterine horn stump.
Success of NOTES splenectomy Peroral splenectomy performed by Kantsevoy et al. (2006a) was successful in 100% (6/6) of pigs. Using grasping forceps and a needle knife or polypectomy snare, the omentum was cauterised and separated from the spleen. Both sets of the pigs' splenic vessels were ligated with two detachable endoloops and in addition, the mesenteric (remaining) portion of the vessel was secured with an endoscopic clip and then cut by a polypectomy snare. After the spleen was mobilized, the gastric incision was enlarged with a sphincterotome to allow the spleen to be pulled into the stomach.
Success of NOTES Lymphadenectomy Peroral lymphadenectomy was performed by Fritscher-Ravens et al. (2006), using a novel tag and thread firing system. EUS (before gastrotomy) was used to select a lymph node suitable for removal. An Echotip needle with back-loaded tag and thread (used unmodified in two cases, or with a slot cut into the needle tip hosting thread attached to a T-bar anchor in four) was passed through the gastric wall then fired into and through the entire lymph node. All nodes could be punctured with the needle in two to four attempts. In the first two procedures, using an unmodified needle, the tag-holding thread led out of the needle tip, hindering easy puncture of the node. In the last four procedures, the thread led out through the slot beyond the needle tip and kept the tip sharp enough to puncture through the node without resistance. The captured lymph node was easily pulled to the gastric wall using gentle traction on the thread. This part of the procedure was performed successfully in 100% (6/6) of pigs. Subsequent gastric incision and lymph node removal, followed by gastrotomy closure was only performed in the final two pigs. A needle-knife was used to make the gastric incision at the site the thread penetrated the gastric wall, so a pull would reveal foreign tissue within the incision, which was then enlarged. Further tension exerted via the thread on the T-bar anchor tended to pull the lymph node into the gastric lumen and hence out of the pig.
In 33% (2/6) of cases, threads fired alongside the gastric laceration became tangled, making locking impossible (caused by lack of care taken to keep threads under tension). The threads were cut and this part of procedure was repeated. In 33% (2/6) of cases (the metal tag would not turn into its horizontal position to capture nodes after firing and had to be replaced by another anchor (subsequent bench experiments showed it necessary for the thread to be fixed at the exact middle point of the anchor to enable reliable turnaround). None of these problems resulted in a failed procedure but necessitated repeating a small sequence of the procedure.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 36
Success of NOTES fallopian tube ligation Peroral fallopian tube ligation using NOTES was performed by Jagannath et al. (2005) to test the feasibility of NOTES procedures. Female reproductive procedure was chosen for the sake of simplicity to test the feasibility of NOTES, rather than their potential application in a clinical setting. The procedure was performed successfully in all six pigs (100%), measured using the nonligated fallopian tube as a control and a follow-up hysterosalpingogram performed to reveal complete obstruction at point of ligation. No complications were experienced relating to deployment and/or placement of Endoloops.
Success of NOTES oophorectomy and tubectomy Peroral oophorectomy and tubectomy using NOTES was undertaken by Wagh et al. (2005; 2006). In both studies, it was successfully performed in 100% (12/12 total) of animals, which was confirmed by necropsy with histopathologic assessment. The uterus was readily located adjacent to the bladder and the uterine horns were followed with grasping forceps inserted through an endoscopic port to reveal the body of the uterus (medial) and ovaries (lateral). A left or right lateral position was used to display the ovary for resection. An endoloop was placed around the ovary, ipsilateral tube and mesosalpinx. Tubectomy with ipsilateral oophorectomy was performed using a snare cautery above the endoloop, with no reported complications.
Success of partial hysterectomy NOTES partial hysterectomy was successful in 100% (13/13) of attempted cases by Merrifield et al. (n: 5), Sumiyama et al. (2006)(n: 2) and Wagh et al. (2005)(n: 6). The model appendicectomy performed by Sumiyama et al. (2006) was essentially a partial hysterectomy, but is described in the appendicectomy section. Merrifield et al. (2006) placed their pigs in a 15 head-down position to shift the bowel away from the uterus, then used forceps to move aside any remaining overlying small bowel. The uterus was grasped with forceps and pulled into an endoloop, which was subsequently tightened around the tissue. The forceps were pushed through an open snare and used to pull the uterus into it. The uterine horn and body were resected above the endoloop using snare cautery. The resected portion of uterus was secured in the snare and withdrawn via an overtube. No complications were encountered during the procedure and necropsy confirmed partial hysterectomy in 100% (5/5) of pigs.
Wagh et al. (2005) followed the uterine horns with grasping forceps inserted through an endoscope to the reveal the body of the uterus (medial). Snare cautery was then used to remove the uterine horn and body after endoloop placement. Partial hysterectomy was successfully performed in six animals and confirmed by necropsy. The uterine lumen was secured by placing an endoloop before restriction and by snare cautery, thereby minimising complications such as bleeding and infection. The complete uterine horn and body were resected in two cases, but the body was transected with removal of the proximal segment and one horn in four cases. No complications were noted.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 37
Success of NOTES diaphragm pacing A prototype NOTES diaphragm mapping system was designed by Onders et al. (2007a) and a chronic diaphragm pacing system (DPS) was modified to provide temporary (several days-weeks) diaphragm pacing. The diaphragm mapping system was transgastrically inserted into the diaphragm muscle using NOTES and the electrode attached to the DPS stimulator and the diaphragm paced synchronously with a ventilator. The prototype endoscopic mapping device allowed stimulation of the diaphragm with qualitative assessment of diaphragm contraction in 100% (4/4) of pigs. Visualisation and stimulation was comparable with laparoscopic visualization of the spinal cord and ALS (amyotrophic lateral sclerosis) trials, although the view was upside-down.
Duration of surgery Operative times were recorded for different procedures or for different stages of individual procedures and therefore were not comparable between studies (Table 9). Even for similar procedures, duration of surgery varied greatly, due to differing surgical techniques and partially due to the developmental stage of NOTES procedures, which have a very steep learning curve. One trend that could be observed is that operating times generally decreased with experience.
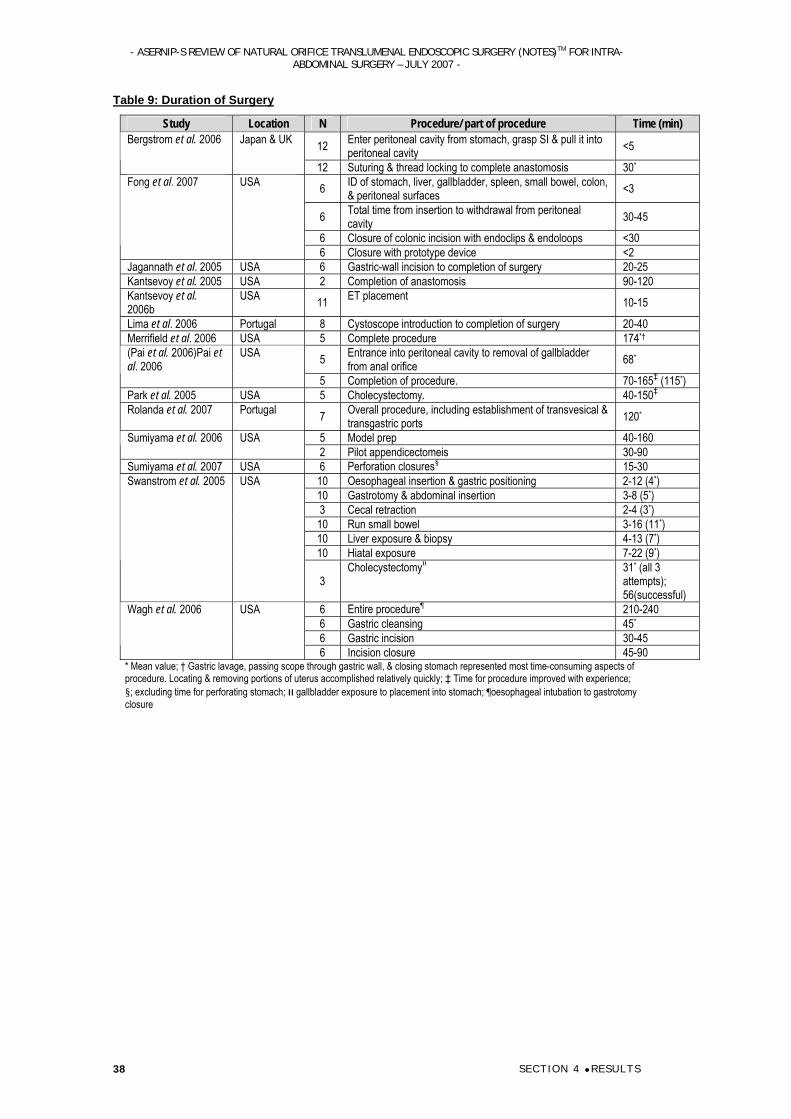
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 38
Table 9: Duration of Surgery
Study Location N Procedure/ part of procedure Time (min)
12 Enter peritoneal cavity from stomach, grasp SI & pull it into peritoneal cavity <5 Bergstrom et al. 2006 Japan & UK
12 Suturing & thread locking to complete anastomosis 30*
6 ID of stomach, liver, gallbladder, spleen, small bowel, colon, & peritoneal surfaces <3
6 Total time from insertion to withdrawal from peritoneal cavity 30-45
6 Closure of colonic incision with endoclips & endoloops <30
Fong et al. 2007 USA
6 Closure with prototype device <2 Jagannath et al. 2005 USA 6 Gastric-wall incision to completion of surgery 20-25 Kantsevoy et al. 2005 USA 2 Completion of anastomosis 90-120 Kantsevoy et al. 2006b
USA 11 ET placement 10-15
Lima et al. 2006 Portugal 8 Cystoscope introduction to completion of surgery 20-40 Merrifield et al. 2006 USA 5 Complete procedure 174*†
5 Entrance into peritoneal cavity to removal of gallbladder from anal orifice 68* (Pai et al. 2006)Pai et
al. 2006 USA
5 Completion of procedure. 70-165‡ (115*) Park et al. 2005 USA 5 Cholecystectomy. 40-150‡ Rolanda et al. 2007 Portugal 7 Overall procedure, including establishment of transvesical &
transgastric ports 120*
5 Model prep 40-160 Sumiyama et al. 2006 USA 2 Pilot appendicectomeis 30-90
Sumiyama et al. 2007 USA 6 Perforation closures§ 15-30 10 Oesophageal insertion & gastric positioning 2-12 (4*) 10 Gastrotomy & abdominal insertion 3-8 (5*) 3 Cecal retraction 2-4 (3*) 10 Run small bowel 3-16 (11*) 10 Liver exposure & biopsy 4-13 (7*) 10 Hiatal exposure 7-22 (9*)
Swanstrom et al. 2005 USA
3 Cholecystectomy31 װ* (all 3
attempts); 56(successful)
6 Entire procedure¶ 210-240 6 Gastric cleansing 45* 6 Gastric incision 30-45
Wagh et al. 2006 USA
6 Incision closure 45-90 * Mean value; † Gastric lavage, passing scope through gastric wall, & closing stomach represented most time-consuming aspects of procedure. Locating & removing portions of uterus accomplished relatively quickly; ‡ Time for procedure improved with experience; §; excluding time for perforating stomach; װ gallbladder exposure to placement into stomach; ¶oesophageal intubation to gastrotomy closure
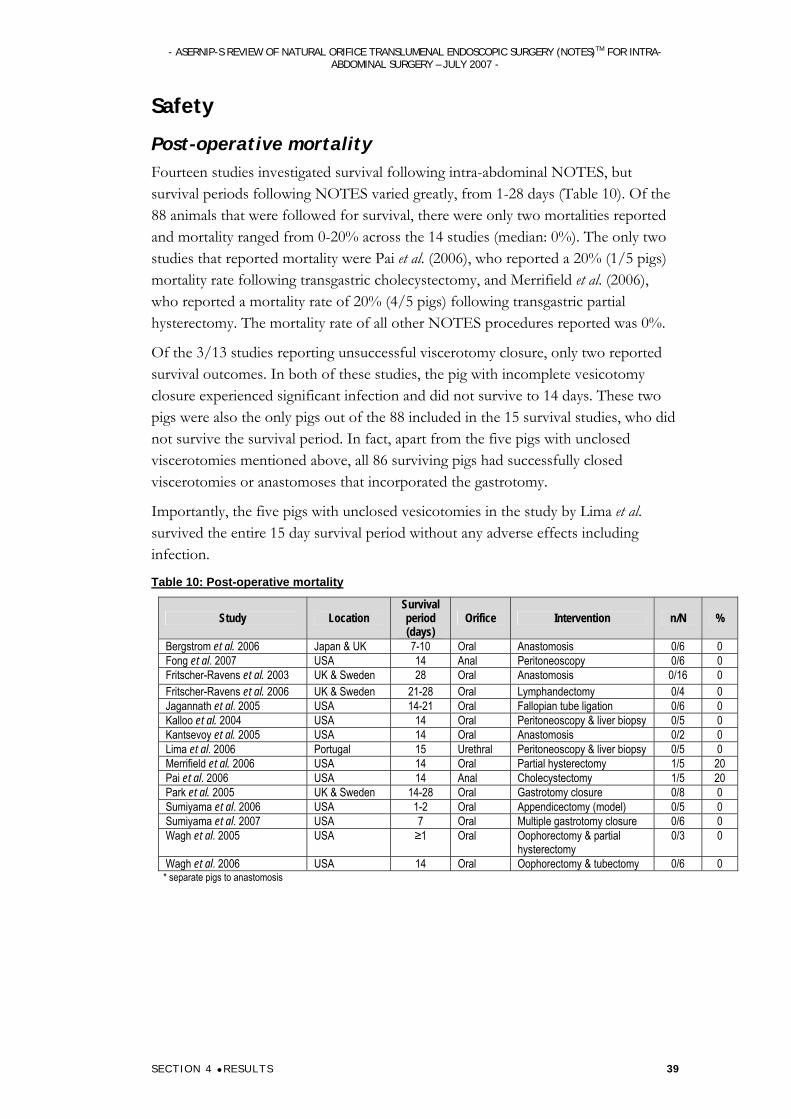
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 39
Safety
Post-operative mortality Fourteen studies investigated survival following intra-abdominal NOTES, but survival periods following NOTES varied greatly, from 1-28 days (Table 10). Of the 88 animals that were followed for survival, there were only two mortalities reported and mortality ranged from 0-20% across the 14 studies (median: 0%). The only two studies that reported mortality were Pai et al. (2006), who reported a 20% (1/5 pigs) mortality rate following transgastric cholecystectomy, and Merrifield et al. (2006), who reported a mortality rate of 20% (4/5 pigs) following transgastric partial hysterectomy. The mortality rate of all other NOTES procedures reported was 0%.
Of the 3/13 studies reporting unsuccessful viscerotomy closure, only two reported survival outcomes. In both of these studies, the pig with incomplete vesicotomy closure experienced significant infection and did not survive to 14 days. These two pigs were also the only pigs out of the 88 included in the 15 survival studies, who did not survive the survival period. In fact, apart from the five pigs with unclosed viscerotomies mentioned above, all 86 surviving pigs had successfully closed viscerotomies or anastomoses that incorporated the gastrotomy.
Importantly, the five pigs with unclosed vesicotomies in the study by Lima et al. survived the entire 15 day survival period without any adverse effects including infection.
Table 10: Post-operative mortality
Study Location Survival period (days)
Orifice Intervention n/N %
Bergstrom et al. 2006 Japan & UK 7-10 Oral Anastomosis 0/6 0 Fong et al. 2007 USA 14 Anal Peritoneoscopy 0/6 0 Fritscher-Ravens et al. 2003 UK & Sweden 28 Oral Anastomosis 0/16 0 Fritscher-Ravens et al. 2006 UK & Sweden 21-28 Oral Lymphandectomy 0/4 0 Jagannath et al. 2005 USA 14-21 Oral Fallopian tube ligation 0/6 0 Kalloo et al. 2004 USA 14 Oral Peritoneoscopy & liver biopsy 0/5 0 Kantsevoy et al. 2005 USA 14 Oral Anastomosis 0/2 0 Lima et al. 2006 Portugal 15 Urethral Peritoneoscopy & liver biopsy 0/5 0 Merrifield et al. 2006 USA 14 Oral Partial hysterectomy 1/5 20 Pai et al. 2006 USA 14 Anal Cholecystectomy 1/5 20 Park et al. 2005 UK & Sweden 14-28 Oral Gastrotomy closure 0/8 0 Sumiyama et al. 2006 USA 1-2 Oral Appendicectomy (model) 0/5 0 Sumiyama et al. 2007 USA 7 Oral Multiple gastrotomy closure 0/6 0 Wagh et al. 2005 USA ≥1 Oral Oophorectomy & partial
hysterectomy 0/3 0
Wagh et al. 2006 USA 14 Oral Oophorectomy & tubectomy 0/6 0 * separate pigs to anastomosis
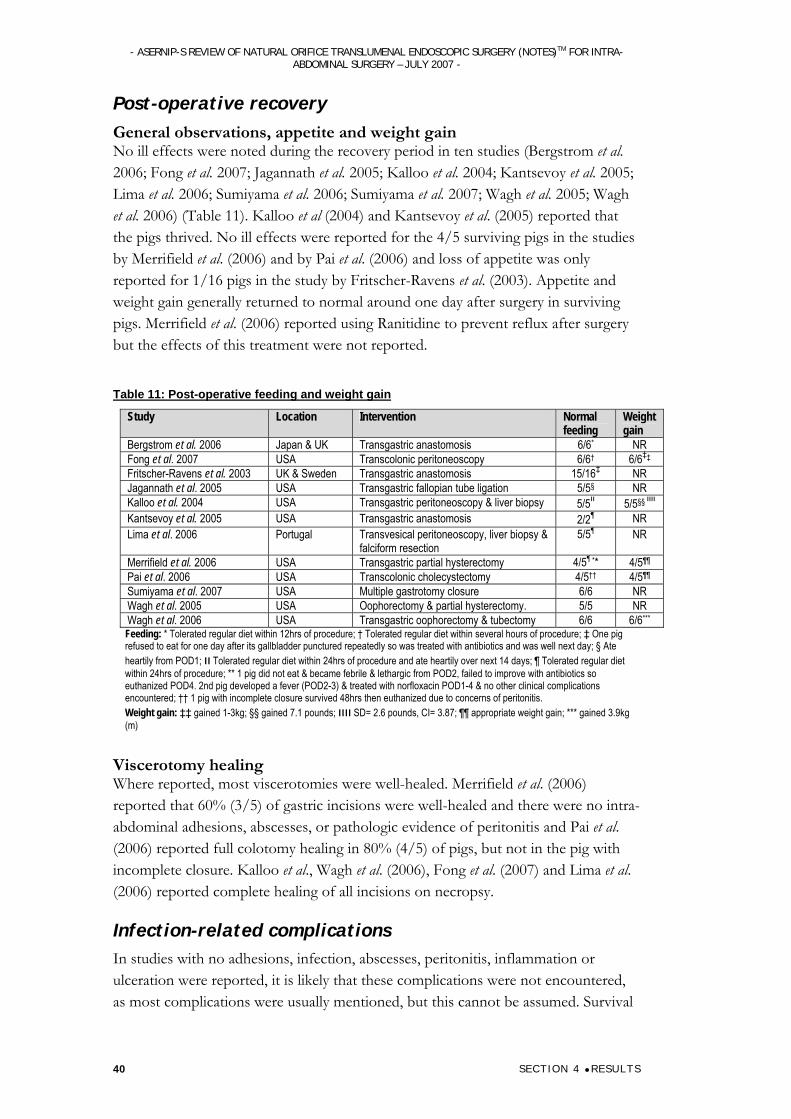
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 40
Post-operative recovery General observations, appetite and weight gain No ill effects were noted during the recovery period in ten studies (Bergstrom et al. 2006; Fong et al. 2007; Jagannath et al. 2005; Kalloo et al. 2004; Kantsevoy et al. 2005; Lima et al. 2006; Sumiyama et al. 2006; Sumiyama et al. 2007; Wagh et al. 2005; Wagh et al. 2006) (Table 11). Kalloo et al (2004) and Kantsevoy et al. (2005) reported that the pigs thrived. No ill effects were reported for the 4/5 surviving pigs in the studies by Merrifield et al. (2006) and by Pai et al. (2006) and loss of appetite was only reported for 1/16 pigs in the study by Fritscher-Ravens et al. (2003). Appetite and weight gain generally returned to normal around one day after surgery in surviving pigs. Merrifield et al. (2006) reported using Ranitidine to prevent reflux after surgery but the effects of this treatment were not reported.
Table 11: Post-operative feeding and weight gain
Study Location Intervention Normal feeding
Weight gain
Bergstrom et al. 2006 Japan & UK Transgastric anastomosis 6/6* NR Fong et al. 2007 USA Transcolonic peritoneoscopy 6/6† 6/6‡‡ Fritscher-Ravens et al. 2003 UK & Sweden Transgastric anastomosis 15/16‡ NR Jagannath et al. 2005 USA Transgastric fallopian tube ligation 5/5§ NR Kalloo et al. 2004 USA Transgastric peritoneoscopy & liver biopsy 5/5װװ §§5/5 װ Kantsevoy et al. 2005 USA Transgastric anastomosis 2/2¶ NR Lima et al. 2006 Portugal Transvesical peritoneoscopy, liver biopsy &
falciform resection 5/5¶ NR
Merrifield et al. 2006 USA Transgastric partial hysterectomy 4/5¶ ** 4/5¶¶ Pai et al. 2006 USA Transcolonic cholecystectomy 4/5†† 4/5¶¶ Sumiyama et al. 2007 USA Multiple gastrotomy closure 6/6 NR Wagh et al. 2005 USA Oophorectomy & partial hysterectomy. 5/5 NR Wagh et al. 2006 USA Transgastric oophorectomy & tubectomy 6/6 6/6*** Feeding: * Tolerated regular diet within 12hrs of procedure; † Tolerated regular diet within several hours of procedure; ‡ One pig refused to eat for one day after its gallbladder punctured repeatedly so was treated with antibiotics and was well next day; § Ate heartily from POD1; װ Tolerated regular diet within 24hrs of procedure and ate heartily over next 14 days; ¶ Tolerated regular diet within 24hrs of procedure; ** 1 pig did not eat & became febrile & lethargic from POD2, failed to improve with antibiotics so euthanized POD4. 2nd pig developed a fever (POD2-3) & treated with norfloxacin POD1-4 & no other clinical complications encountered; †† 1 pig with incomplete closure survived 48hrs then euthanized due to concerns of peritonitis. Weight gain: ‡‡ gained 1-3kg; §§ gained 7.1 pounds; װװ SD= 2.6 pounds, CI= 3.87; ¶¶ appropriate weight gain; *** gained 3.9kg (m)
Viscerotomy healing Where reported, most viscerotomies were well-healed. Merrifield et al. (2006) reported that 60% (3/5) of gastric incisions were well-healed and there were no intra-abdominal adhesions, abscesses, or pathologic evidence of peritonitis and Pai et al. (2006) reported full colotomy healing in 80% (4/5) of pigs, but not in the pig with incomplete closure. Kalloo et al., Wagh et al. (2006), Fong et al. (2007) and Lima et al. (2006) reported complete healing of all incisions on necropsy.
Infection-related complications In studies with no adhesions, infection, abscesses, peritonitis, inflammation or ulceration were reported, it is likely that these complications were not encountered, as most complications were usually mentioned, but this cannot be assumed. Survival
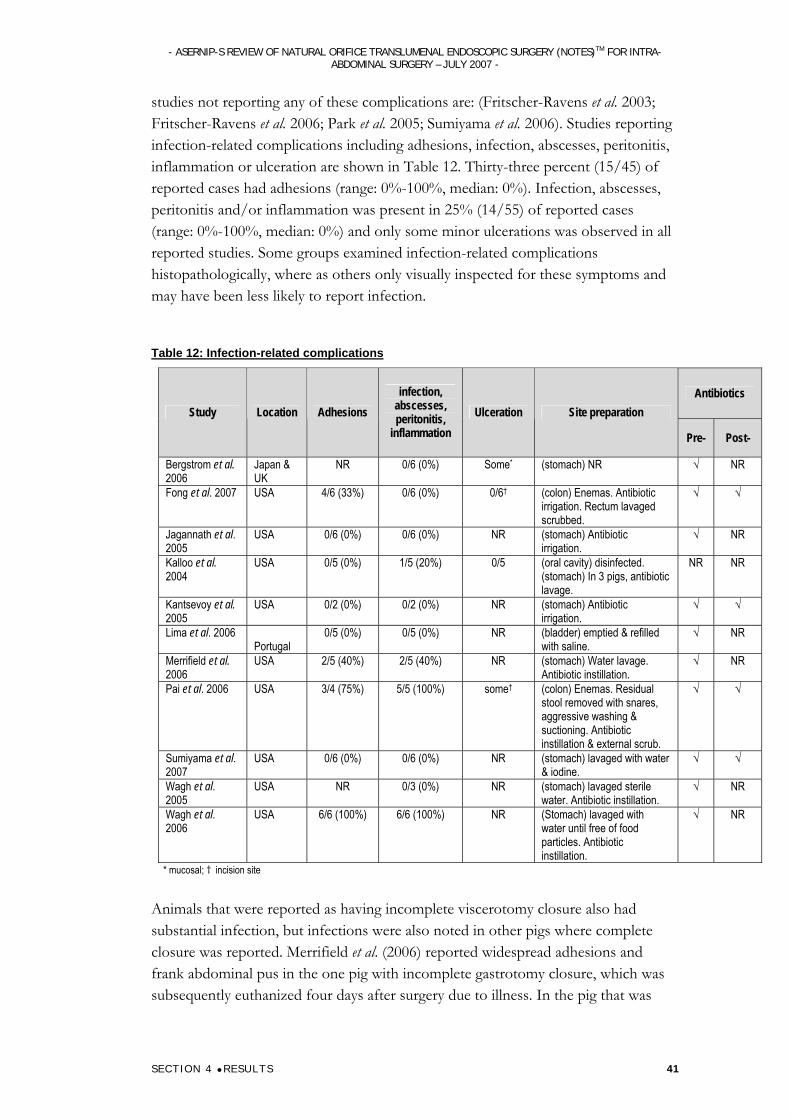
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 41
studies not reporting any of these complications are: (Fritscher-Ravens et al. 2003; Fritscher-Ravens et al. 2006; Park et al. 2005; Sumiyama et al. 2006). Studies reporting infection-related complications including adhesions, infection, abscesses, peritonitis, inflammation or ulceration are shown in Table 12. Thirty-three percent (15/45) of reported cases had adhesions (range: 0%-100%, median: 0%). Infection, abscesses, peritonitis and/or inflammation was present in 25% (14/55) of reported cases (range: 0%-100%, median: 0%) and only some minor ulcerations was observed in all reported studies. Some groups examined infection-related complications histopathologically, where as others only visually inspected for these symptoms and may have been less likely to report infection.
Table 12: Infection-related complications
Antibiotics Study Location Adhesions
infection, abscesses, peritonitis,
inflammation Ulceration Site preparation
Pre- Post-
Bergstrom et al. 2006
Japan & UK
NR 0/6 (0%) Some* (stomach) NR √ NR
Fong et al. 2007 USA 4/6 (33%) 0/6 (0%) 0/6†
(colon) Enemas. Antibiotic irrigation. Rectum lavaged scrubbed.
√ √
Jagannath et al. 2005
USA 0/6 (0%) 0/6 (0%) NR (stomach) Antibiotic irrigation.
√ NR
Kalloo et al. 2004
USA 0/5 (0%) 1/5 (20%) 0/5 (oral cavity) disinfected. (stomach) In 3 pigs, antibiotic lavage.
NR NR
Kantsevoy et al. 2005
USA 0/2 (0%) 0/2 (0%) NR (stomach) Antibiotic irrigation.
√ √
Lima et al. 2006 Portugal
0/5 (0%) 0/5 (0%) NR (bladder) emptied & refilled with saline.
√ NR
Merrifield et al. 2006
USA 2/5 (40%) 2/5 (40%) NR (stomach) Water lavage. Antibiotic instillation.
√ NR
Pai et al. 2006 USA 3/4 (75%) 5/5 (100%) some† (colon) Enemas. Residual stool removed with snares, aggressive washing & suctioning. Antibiotic instillation & external scrub.
√ √
Sumiyama et al. 2007
USA 0/6 (0%) 0/6 (0%) NR (stomach) lavaged with water & iodine.
√ √
Wagh et al. 2005
USA NR 0/3 (0%) NR (stomach) lavaged sterile water. Antibiotic instillation.
√ NR
Wagh et al. 2006
USA 6/6 (100%) 6/6 (100%) NR (Stomach) lavaged with water until free of food particles. Antibiotic instillation.
√ NR
* mucosal; † incision site
Animals that were reported as having incomplete viscerotomy closure also had substantial infection, but infections were also noted in other pigs where complete closure was reported. Merrifield et al. (2006) reported widespread adhesions and frank abdominal pus in the one pig with incomplete gastrotomy closure, which was subsequently euthanized four days after surgery due to illness. In the pig that was
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 42
febrile from 2-3 days after surgery, copious adhesions and a 1mm abscess were observed at the gastric incision site and small collections of pus were seen in the remaining portion of the uterus and scattered throughout the abdominal cavity. No intra-abdominal adhesions, abscesses or pathologic evidence of peritonitis were observed in the other three pigs in this study.
Pai et al. (2006) also reported substantial infection in 20% (1/5) of pigs, which was the pig with incomplete colotomy closure. This pig had acute peritonitis, with seepage of bowel contents from the colonic perforation and necrotising granulomas. External adhesions were observed in 75% (3/4) of pigs: salpingocolonic attachments in two pigs and colovesical attachments the third. Submucosal and/or serosal microabscesses and ulceration and necrosis at the incision site were seen in 100% (5/5) of pigs.
Only one study did not report any site preparation (Bergstrom et al. 2006), but only minor ulceration was reported in these pigs and no other complications. Kalloo et al. (2004) noted intraperitoneal microabscesses in the two pigs not pre-treated with antibiotic, so gave prophylactic antibiotics to the subsequent three pigs and found no intraperitoneal microabscesses on necropsy. Only 17% (1/6) of pigs in that study showed signs of infection on necropsy. That pig was one of the two not given prophylactic antibiotics and culture from that pig grew a Proteus species.
Fong et al. 2007 reported salpingocolonic and colovesicular adhesions in 67% (4/6) of pigs. No adhesions were seen in 25% (1/4) of pigs where a prototype closure device was used in the pig closed with endoscopic clips. Incision-related adhesions and inflammatory changes restricted to colonic closure sites were observed in 100% (6/6) of pigs. Inflammatory infiltrates, microscopic abscesses, microscopic, mucosal ulcerations and serositis were seen in all pigs on histopathologic examination, but could not be picked up by visual examination on necropsy. Similarly, although Jagannath et al. (2005) did not find any infection-related complications upon visual examination, they found chronic inflammatory infiltrates without abscesses on histopathologic examination.
Although Wagh et al. (2006) did not report any major infection, they did observe follicular hyperplasia of mesenteric and pelvic lymph nodes in 100% (6/6) of pigs as well as a body giant-cell reaction secondary to the endoclips and chronic inflammatory changes at the gastrotomy site.
Procedure-Related Complications Bleeding Although minor bleeding during surgery occurred in many cases, it was generally self-limiting or was controlled by methods including electrocauterisation, clamping & tissue anchors. Studies generally reported bleeding narratively so it is difficult to compare bleeding across studies because some groups have reported minor bleeding (Kalloo et al. 2004), but others have not reported numbers for non-significant or
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 4 RESULTS 43
minor bleeding. Five studies reported no significant bleeding (Bergstrom et al. 2006; Fong et al. 2007; Kalloo et al. 2004; Merrifield et al. 2006; Onders et al. 2007a). Kalloo et al. (2004) reported minor bleeding in 40% (2/5) of pigs, which was stopped with electrocoagulation. Kantsevoy et al. (2005) noted minor bleeding of an intestinal loop stopped with electrocautery and Park et al. (2005) encountered occasional manageable bleeding from the cystic artery during dissection. Rolanda et al. (2007) reported liver-surface bleeding in 14% (1/7) of pigs that did not obscure endoscopic visualization and Sumiyama et al. (2007) managed arterial bleeding at the perforation site in 17% (1/6) of pigs. Bleeding which was not able to be controlled was experienced by Swanstrom et al. (2005). During liver resection they encountered significant bleeding that not able to be stopped with cautery or endoscopic clips in 10% (1/10) of animals and laparoscopic ‘rescue’ was required. During cholecystectomy bleeding from cystic artery unable to be controlled and visualization lost in the first animal of three.
Organ Injury Of the studies that examined organ injury, most studies reported no injury to surrounding organs and vessels (Bergstrom et al. 2006; Fong et al. 2007; Fritscher-Ravens et al. 2003; Kalloo et al. 2004; Kantsevoy et al. 2005; Kantsevoy et al. 2006a; Merrifield et al. 2006; Pai et al. 2006; Rolanda et al. 2007; Wagh et al. 2005; Wagh et al. 2006), but organ injury was not thoroughly examined in all cases so may have been unnoticed. Although no organ injury was reported, Rolanda et al. (2007) reported secondary bile leakage during cholecystectomy in one pig (of 7), which seriously disturbed endoscopic view and Wagh et al. (2006) reported that trauma to the liver during gastric exit may have occurred and in one pig the anterior abdominal wall was punctured during gastrotomy. Kantsevoy et al. (2006c) reported no injuries as the result of ET use, but did not mention injuries associated with any other part of procedure.
Sumiyama et al. (2007) reported penetration of surrounding organs by 12.5% (3/24) of tissue anchors used. Swanstrom et al. (2005) reported that during cholecystectomy in the second animal (of three), perforation of the gallbladder made identification of dissection planes impossible so the cholecystectomy was abandoned and in the third animal some gallbladder perforations occurred.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 44
Discussion
Limitations of the evidence Our search of the literature failed to identify any studies of NOTES procedures performed in humans. There were numerous references in the literature to peroral transgastric appendicectomeis performed in humans in India, but these were cited as personal communications and no published data could be obtained. Additionally, there have been a number of news reports of a transvaginal cholecystectomy that was successfully performed in a human at the Columbia University Medical Center (Grady 2007; The Age 2007; USGI Medical 2007). The reports state that Bessler presented the procedure at the 2007 SAGES meeting, but the abstract only describes the procedure in pigs (Bessler et al. 2007) and the human trial is yet to be published in peer-reviewed literature.
Thus, in each of the 22 articles included in this review, NOTES procedures were performed in animals, reflecting the developmental stage of these procedures. Some of these studies may have subject overlap as different aspects of NOTES procedures in the same cohort of animals were sometime reported in more than one paper. None of the included studies compared NOTES procedures with current intra-abdominal surgical procedures, and most focused primarily on the ability to successfully complete the procedure, rather than on how effective the procedure was nor a comprehensive safety evaluation.
In many studies, the first few animals were used to optimise methods and gain experience with performing various aspects of the procedure, however outcomes for these animals were often pooled with those of subsequent animals. Additionally, as these procedures were novel, the learning curve was significant and ability to successfully perform the technique generally increased greatly with experience, which has an obvious impact on outcomes. With the exception of one study which used four dogs, all procedures were performed in pigs, which may respond differently to surgical procedures than humans, in addition to the obvious differences in surgical technique due to pig anatomy.
Safety and efficacy outcomes It was apparent that although technically possible to perform many of the procedures using NOTES, they have not yet been optimised for maximum effectiveness and minimisation of risk. Substantial refinement is required before they can be compared with established procedures in a clinical setting.
Although many interventions could be successfully performed using different approaches and orifices (oral, anal or urethral), these methods were not directly compared. Therefore optimal methods for performing NOTES could not be determined. Transvaginal access was also used in studies presented at the 2007 SAGES meeting, indicating the potential of using this access site for NOTES. The
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 45
combination of transgastric and transvesical access appeared to be advantageous when performing NOTES cholecystectomies, particularly in manipulating the gallbladder, however this needs further investigation to be substantiated. Similarly, combining transgastric and transcolonic access was shown to be advantageous for organ manipulation and visualisation in studies presented at the 2007 SAGES meeting.
In all accounts, cholecystectomy performed using NOTES was challenging, but could be successfully performed. News reports state that this procedure was successfully performed in a 66 year old woman by Bessler at the Columbia University Medical Center, New York, as part of an ongoing trial, with no complications reported (Grady 2007; The Age 2007; USGI Medical 2007). This suggests that the procedure is potentially transferable to humans, but peer-reviewed data will need to be produced before any conclusions may be drawn.
Although the 100% success rate for peroral transgastric appendicectomeis is testament to the procedure’s feasibility, both the small sample size and the fact that it was a model appendicectomy indicate the need for further studies. Similarly, the small sample size for transgastric splenectomies does not indicate much more than the feasibility of the procedure. The 100% success rate of 31 NOTES procedures involving female reproductive organs indicates the potential for the use of NOTES for the performance of intra-abdominal surgery. NOTES female reproductive procedures are not likely to be adopted and were chosen for study due to their simplicity.
The reported success of using NOTES to provide temporary diaphragm pacing in one study shows definite potential for this developmental procedure. The advantages of using NOTES to perform this intervention are more apparent than for most of the other interventions tested. When used in ICU patients with a PEG tube, there is no need to create a new gastrotomy, so the procedure is truly minimally invasive. The importance of minimising invasive procedures is higher for ICU patients, for whom even a small laparoscopic wound can pose potentially dangerous complications.
The efficacy of specific aspects of NOTES procedures such as viscerotomy creation and closure, was more easily measurable than the efficacy of the interventions. The development of NOTES has attracted the attention of many prominent surgeons and gastroenterologists, who have formed collaborations to identify concerns and challenges in the development of NOTES. A working group established at the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) leadership meeting in Chicago in 2005 developed guidelines for the implementation of NOTES, which were outlined in a resulting ‘NOTES White Paper’ (Rattner and Kalloo 2006).
The challenges include:
peritoneal access
viscerotomy closure
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 46
prevention of infection
suturing and anastomotic devices
maintenance of spatial orientation
development of a multitasking platform
management of intraperitoneal complications and haemorrhage
adverse events caused by NOTES
education and training
Some of these challenges have been investigated in the included studies, but have not been satisfactorily resolved at this stage. Many of the studies presented at the SAGES 2007 meeting investigated these issues in more detail, but further research is still required.
As proposed in the NOTES White paper (Rattner and Kalloo 2006), peritoneal access was easily achieved in all studies without significant complication, via oral, anal or urethral orifices. Although no complications appeared to be related to viscerotomy creation, it is likely that further optimisation may yield better surgical results overall. Using the sphincterotome method to dilate initial needle-knife gastric incisions has the advantage of allowing quick and repeated endoscope passage but the disadvantage that complete gastrotomy closure must be assured, whereas the muscle layers spring back together following the balloon method, making closure easier. No dilation was required for transcolonic incisions. Viscerotomy site location may also have a significant impact on the surgical intervention, as suggested by Park et al. (2005), who reported that a gastrotomy site a few centimetres away from the gallbladder, rather than immediately adjacent, aided gallbladder manipulation and anastomosis creation. Most groups agree that optimisation of viscerotomy creation method and site must be determined (Ellsmere et al. 2006; McGee et al. 2006b; Rattner and Kalloo 2006; Sclabas et al. 2006), but this has not been achieved in all included studies.
Although it was proposed in the NOTES White Paper that a 100% reliable means of viscerotomy closure must be ensured (Rattner and Kalloo 2006), this remains to be proven. In total, two were deaths reported in of all the included studies. Each occurred after infections from unclosed procedures: one after an unclosed gastrotomy and the other after an unclosed colotomy. This is suggestive of a relationship between unclosed viscerotomy with poor outcome, however in one study, five pigs with unclosed vesicotomies survived the post-procedural observation period without complication in one study, as did six pigs with unclosed gastrotomies in another. This suggests that vesicotomy closure may not always be crucial for a good outcome, however this finding may be different in a human model.
Viscerotomy closure was completed in the majority of cases where it was attempted, using a variety of devices, with incomplete closure not consistent for any device. The reliability of the various closure methods in achieving successful closure cannot be

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 47
properly assessed due to the very small sample size and lack of comparison between methods. The developmental stage of the studies included in this review also prevents measuring the reliability of closure, as closure was only assessed in a very controlled environment where time was not an issue and closure was performed by expert surgeons. Additionally, it is not appropriate to pool results for success of closure to measure reliability as many of the studies were investigating how to perform various closure techniques that have not yet been optimised. Another concern is that while the closure of one viscerotomy is considered to be relatively simple, ensuring the closure of multiple punctures created for multiple working ports is more difficult (McGee et al. 2006b; Rattner and Kalloo 2006). In one of the studies, two gastrotomies per animal were successfully closed, and no subsequent infection-related complications reported, but the closure of multiple viscerotomies needs to be further tested. The novel closure devices presented at the SAGES 2007 meeting such as the Power Medical SurgASSIST and the NDO plicator may help to provide solutions to achieving simple and reliable closure, but again, these devices will need to be further tested.
Although the gastric puncture is expected to heal quickly and cause little ill effect due to good vascularisation and the thick stomach wall (Lamade et al. 2006), it is important to measure the robustness of viscerotomy closure when determining reliability of closure. The fact not all successfully closed gastrotomies were watertight on explant testing, indicates that ensuring viscerotomy closure does not necessarily ensure that the viscerotomy will stay closed. This means that while closed gastrotomies did not pose significant problems in the carefully controlled animals included in this review, in a clinical setting closed viscerotomies could reopen if placed under any stress such as food consumption or physical activity. The use of bioprosthetic plugs for viscerotomy closure, as presented at the SAGES 2007 meeting, may speed the viscerotomy healing process.
The reports of peritoneal infection, experienced by pigs with closed viscerotomies, although not major, suggest that complete viscerotomy closure is not the only important factor determining susceptibility to infection following NOTES. This could be explained by the above theory, that although closure was completed, it may not be completely reliable. It is also likely that pathogens were introduced into the peritoneal cavity during surgery as all natural orifices are not sterile (Rattner and Kalloo 2006). Intestinal pathogens may have leaked into the peritoneal cavity following viscerotomy or may have been introduced by equipment passing through pathogen-containing lumens. Studies have revealed that peritoneal exposure to low levels of bacteria appear to be well tolerated (Lamade et al. 2006; Rattner and Kalloo 2006) and it has been observed during bowel surgery that leakage of small amounts of bacteria into the peritoneal cavity has been well tolerated if prophylactic antibiotics were given (Rattner and Kalloo 2006). Additionally, the study presented by Hazey et al. at the SAGES 2007 meeting demonstrated that transgastric equipment
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 48
does contaminate the peritoneal cavity, but pathogens are clinically insignificant due to species or bacterial load’.
Although many studies reported cleaning and disinfection of the viscerotomy site (stomach, colon or bladder), the use of sterile overtubes and administration of prophylactic antibiotics pre- and post-surgery to prevent infection, outcomes for these treatments have not been compared (Hochberger and Lamade 2005; Lamade et al. 2006). Additionally, it is expected that very low gastric pH (3-4) limits bacterial growth and thus contamination (Lamade et al. 2006). Thus, excessive cleansing of the stomach or the administration of prophylactic antacids, as was undertaken in some of the included studies, may in fact increase the risk of peritoneal contamination. A study presented at the SAGES 2007 meeting by McGee at al. indicated that pre-procedural gastric lavage was not effective in eliminating infection. It is important to note that although peritoneal contamination may be minimised in highly controlled animal studies, it is another issue to determine if this may be achieved reliably in practice.
Although gastroenterologists are used to working in line with their light source and camera, laparoscopic and open surgery allows a wider, three dimensional view which is necessary to perform complex surgery in larger spaces such as the peritoneal cavity (Rattner and Kalloo 2006). Visualisation was good in many cases and was adequate to allow the completion of many procedures. The inability to identify numerous organs and structures is not really acceptable if NOTES is to be performed in the range of intra-abdominal interventions possible with current surgical techniques including diagnostics. A better field of view using two ports with the combined transvesical and transgastric approach, rather than a single port, is helpful to capture the whole procedure due to the better angles and illumination possible with present flexible endoscopic technology. This would help to reduce adverse events such as organ laceration and if such events do occur, they are more likely to be visualised so that consequences could be minimised. With more advanced technology a better field of view may be achievable using a multi-tasking platform, such as the incorporation of cameras on separate arms of endoscopic devices (Rattner and Kalloo 2006; Swanstrom 2006).
The flexibility of endoscopic equipment that is required to transverse long luminal spaces does not allow for adequate traction and counter-traction to be achieved, making organ and tissue manipulation difficult. (McGee et al. 2006b; Rattner and Kalloo 2006). Additionally, most endoscopic devices have limited degrees of freedom, with the lack of manoeuvrability further hindering tissue manipulation (McGee et al. 2006b). Manoeuvrability of flexible endoscopic devices through the peritoneal cavity was generally achievable with current devices, but was often tedious and cumbersome. The mini-robot described by Rentschler et al. at the SAGES 2006 meeting was easily able to traverse the peritoneal cavity and with further development holds great potential for use in NOTES. Grasping and organ manipulation was very variable, depending on the target organ/tissue, equipment and
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 49
access port used and distance of the target organ from that port. Adequate grasping could be achieved to perform all included procedures, but was often difficult and unreliable. Using a combination of transvesical and transgastric ports helped with organ manipulation and should be explored as a possibility, as should the development of new devices which include a multitasking platform (Rattner and Kalloo 2006). The development of a multitasking platform and physically stable work environment is perhaps not essential for performing very simple procedures, but will be critical to the use of NOTES for more complex procedures. Other methods to address these manoeuvrability and grasping issues include the use of overtubes to stabilise positioning of equipment, the development of surgical robots with flexible arms attached to the end of an endoscope (Saltzman 2004) and voice activation technology (Falcone and Steiner 2002; Rattner and Kalloo 2006).
Bleeding and organ injury was easily managed in most cases, but in some cases where it could not be controlled, this led to the failure of the procedure. While the risk of these complications may be minimised with better equipment and NOTES experience, they may never be completely eliminated, especially during more complicated procedures. If management methods such as electrocautery and suturing fail, laparoscopic backup may be used and will be necessary in early trials until more experience is gained and better devices are developed. Additionally, the consequences of bleeding and organ injury during NOTES were not followed up and this may be important for human studies.
The normal appetite and weight gain observed the day after surgery in non-infected animals indicated very fast recovery following NOTES procedures, however the recovery times may not be transferable to humans. An important consideration is the physiologic effects of pneumoperitoneum creation during NOTES, which may be different to those studies for laparotomy (Rattner and Kalloo 2006). No outcomes were reported in the included studies, however in a SAGES presentation by Bingener (2007), it was demonstrated that there were significant cardiopulmonary differences between NOTES and laparoscopy in pigs, however the meaning of these differences is unknown. Although one study found that biopsy port pressures were quite accurate in recording actual intra-abdominal pressures during NOTES, this finding will need to be repeated and tested in other NOTES procedures where intra-abdominal pressure may vary more greatly.
NOTES devices Many of the challenges that have been identified are related to the capacity of devices used to reliably perform procedures with such limited access (long confined distances with low visibility). Rapidly advancing surgical technology makes this a technical possibility, yet it is unclear if current technology is adequately advanced and if surgeons’ skills in using these novel devices may keep up with the technology (Kalloo et al. 2004; Ko and Kalloo 2006). Flexible video endoscopes and devices which enable suturing, dissecting, grasping, ligating and anastomosis are being perfected to
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 50
address issues such as flexibility vs. strength/traction, visualisation and lack of tactile feedback (Ellsmere et al. 2006; Kalloo et al. 2004; Ko and Kalloo 2006; Lehman et al. 2006; Rattner and Kalloo 2006; Swanstrom 2006). The novel 4-channel flexible endoscopic device presented by Swanstrom et al. at the SAGES 2007 meeting represents a new generation of endoscopic devices which may solve some of these challenges. The MAGS technology used in SAGES 2007 studies also addresses these challenges in providing a stable platform, providing triangulation and rigidity. These devices clearly show potential to address challenges experienced in NOTES development, but will need to be further tested and developed.
The NOTES White Paper (2006) also indicated the need for advanced endoscopic suturing devices during NOTES procedures as most current devices are cumbersome and back-up is needed in case mechanical closure and anastomoses devices fail, especially for use during complex procedures (Rattner and Kalloo 2006). Additionally, many novel devices were used to perform other parts of procedures, such as the novel anastomosis creation devices described in the included studies. The novel tag/thread firing devices used by Fritscher-Ravens et al (2003) and Fritscher-Ravens et al (2006) could potentially reduce complications by eliminating the need for a pneumoperitoneum, and also to minimise peritoneal infection because the gastric incision is only made after the target organ (gallbladder, jejunum or lymph node) has been dragged to the stomach, reducing the possibility of leakage and need to probe endoscopic devices around the peritoneal cavity. A number of prototype suturing, anastomoses and closure devices were successfully used in the included studies and in SAGES presentations, however their efficiency will have to be further tested and the devices further developed.
Other considerations As with any new technology, the cost of NOTES will probably be high when it is first adopted, but will decrease with more widespread implementation and the development of more effective and cost-effective technologies. At present, the cost of NOTES procedures is high because they are still in the early stages of development and are being optimised by expert surgeons, while the cost of the specialised equipment is also high. Eventually, the adoption of NOTES may reduce the societal costs of intra-abdominal surgery due to reduced hospital stays and surgical site complications (McGee et al. 2006b; Rattner and Kalloo 2006; Richards and Rattner 2005; Vitale et al. 2005).
The trend for considerable decreases in operative times with increased experience is a further indication of the developmental stage of NOTES at present and suggests even more improvements are possible once procedures have been optimised and their techniques mastered. Past experience, especially with the introduction of laparoscopy, has revealed the need for adequate and regulated training. The problems that occurred with the rapid adoption of laparoscopic surgery, such as complications associated with laparoscopic cholecystectomies (Osborne et al. 2006) definitely want
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 51
to be avoided with the introduction of NOTES. This signifies a need for good research into NOTES with adequate and transparent reporting to ensure surgeons are provided with up-to-date information on optimal methods of performing the procedures, handling of the latest devices, and potential complications to be aware of (Rattner and Kalloo 2006).
Considering the developmental stage of NOTES at present, there would be significant ethical issues surrounding its use in patients, given that many of these procedures are still novel and relatively unrefined (Lamade et al. 2006). The cosmetic/aesthetic benefits of such procedures would need to be carefully weighted against the risk of potential complications. Surveys presented at the SAGES 2007 meeting where patients were asked their perceptions of NOTES technology indicate what risks are considered acceptable. Complications, recovery time and post operative pain were considered to be more important than cosmesis, cost and length of hospital stay, and there was no tolerance for higher risk or worse outcomes for NOTES, regardless of expected benefits. This indicates that safety and efficacy need to be adequately addressed before it is acceptable to perform NOTES in a clinical setting.
Future research At the SAGES 2005 meeting it was acknowledged that NOTES has blurred the boundaries between traditional disciplines such as gastroenteroscopy and endoscopic and laparoscopic surgery. A general consensus was reached, however, that NOTES is truly surgery and should be developed and promoted by surgeons knowledgeable in suturing, wound healing, anatomy, and other surgical options (Rattner and Kalloo 2006; Richards and Rattner 2005; Soper 2005). This group went on to form the Natural Orifice Surgery Consortium for Assessment and Research* (NOSCAR), whose goal is to conduct research into this emerging field and to guide the responsible development of NOTES. NOSCAR have identified the following membership criteria, which should be applied to all those developing NOTES:
must have a multidisciplinary (i.e. possesses advanced endoscopic and laparoscopic skills)
should be SAGES and/or ASGE members
must have animal laboratory facilities to perform research and training
must agree to share laboratory results with other NOSCAR members
must agree that any and all human procedures be performed only after obtaining Institutional Review Board approval (Rattner and Kalloo 2006)
Further optimisation and refinement of NOTES procedures is required and it is critical that future studies compare the outcomes of these procedures with those of current intra-abdominal surgical procedures, in order to evaluate the advantages and
* h t tp://www.noscar .org/
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 52
disadvantages of each. Challenges including achieving adequate visualisation/spatial orientation, manoeuvrability, grasping and organ manipulation still need to be addressed and will be aided by further development of the many promising devices outlined in the literature (Bardaro and Swanstrom 2006; Lehman et al. 2006; McGee et al. 2006b; Rattner and Kalloo 2006; Saltzman 2004; Swanstrom 2006; Wolf, Jr. 2005). The method of Failure Mode and Effect Analysis to survey technical problems of NOTES, as presented by Shinohara at the SAGES 2007 meeting, may assist in this development.
Optimisation of peritoneal access and a reliable closure method will need to be determined in future studies comparing viscerotomy creation and closure with important outcomes such as organ injury, bleeding, infection, recovery and survival. Longer and more comprehensive survival studies may help to determine adverse events caused by NOTES and it has also been suggested that better animal models need to be used to account for physiologic differences before moving into human trials (McGee et al. 2006b).
Detailed randomised control trials will need to be performed in humans to compare optimised intra-abdominal NOTES procedures with currently available intra-abdominal surgical techniques. Hybrid studies in humans (i.e. laparoscopic/transgastric) could be used in early human procedures (Rattner and Kalloo 2006), although the risk seems unnecessary as they would be greater than those for laparoscopy with none of the benefits of NOTES. Alternatively, laparoscopic and laparotomic backup may be enlisted to ensure patient safety when performing NOTES in early human trials.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 6 CONCLUS IONS AND RECOMMENDATIONS 53
Conclusions As NOTES is still in a developmental stage and no human studies have been published, is difficult to compare the safety and efficacy of using NOTES to perform intra-abdominal surgery with current intra-abdominal surgical interventions, however current NOTES procedures do not appear as safe or effective as alternative surgical options. The outcomes obtained from the 22 studies included in this review indicate that NOTES can in fact be used to perform some intra-abdominal procedures in animal models. What is more apparent is the need for the further development of these procedures, as well as studies comparing NOTES to current intra-abdominal surgical procedures before it can seriously be considered for use in a clinical setting. The development of new devices will speed the development of NOTES and improve outcomes. There is a definite need for further studies to compare surgical methodology of NOTES procedures and aspects thereof, to determine optimal methods of performing intra-abdominal surgery via a natural orifice. The safety and efficacy of these optimised procedures will then need to be carefully evaluated and compared with existing surgical interventions.
Classification and Recommendations On the basis of the evidence presented in this systematic review, the ASERNIP-S Review Group agreed on the following classifications and recommendations concerning the safety and efficacy of NOTES for intra-abdominal surgery:
Classifications Evidence rating The available evidence was assessed as being poor.
Safety At this point in time, NOTES for intra-abdominal surgery is less safe than laparoscopic and laparotomic alternatives.
Efficacy Presently, NOTES for intra-abdominal surgery is currently less efficacious than laparoscopic and laparotomic alternatives.
Clinical and Research Recommendations NOTES is still in early stages of development and more robust technologies will be needed to achieve reliable closure and overcome technical challenges. Well-managed human studies need to be conducted to determine the safety and efficacy of NOTES in a clinical setting. This may be approached by performing hybrid NOTES/laparoscopic procedures, which may help to evaluate the safety of NOTES in a human model, before moving into larger trials. NOTES procedures and studies should be performed under strict guidelines, such as the membership criteria developed by NOSCAR.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
SECT ION 5 D ISCUSS ION 54
Acknowledgments The authors wish to acknowledge Dr Karen Facey, Dr Wendy Babidge and Ms Prema Thavaneswaran for their assistance during the preparation of this review. The ASERNIP-S project is funded by the Australian Government Department of Health and Ageing and the South Australian Department of Health.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
REFERENCES 55
References
Aletti GD, Dowdy S, Podratz KC, Cliby WA. Role of lymphadenectomy in the management of grossly apparent advanced stage epithelial ovarian cancer. Am J Obstet Gynecol 2006; 195(6): 1862-1868.
Barbare JC, Boige V, Boudjema K, Lescesne R, Trinchet JC. Hepatocellular carcinoma (primary cancer of the liver). Gastroenterol Clin Biol 2006; 30 Spec No 2: 2S57-2S61.
Bardaro SJ and Swanstrom L. Development of advanced endoscopes for natural orifice transluminal endoscopic surgery (NOTES). Minimally Invasive Therapy & Allied Technologies: Mitat 2006; . 15(6)
Bengmark S. Aggressive management of surgical emergencies. Ann R Coll Surg Engl 2006; 88(7): 624-629.
Bergstrom M, Ikeda K, Swain P, Park P-O. Transgastric anastomosis by using flexible endoscopy in a porcine model (with video). Gastrointestinal Endoscopy 2006; . 63(2)
Bessler M, Stevens PD, Milone L, Hogle NJ, Durak E, Fowler D. Transvaginal laparoscopic cholecystectomy: Laparoscopically assisted (V029). SAGES 2007 Meeting. 2007.
Bingener J, Winston J, Haines V, Michalek J, Van Sickle K, Saha A, Lopez P, Wayne Schwesinger W. The physiologic effects of NOTES in a porcine model: comparison with standard laparoscopy (P502). SAGES 2007 Meeting. 2007.
Boni L, Benevento A, Rovera F, Dionigi G, Di Giuseppe M, Bertoglio C, Dionigi R. Infective complications in laparoscopic surgery. Surg Infect (Larchmt.) 2006; 7 Suppl 2: S109-S111.
Bunyavejchevin S and Phupong V. Laparoscopic surgery for presumed benign ovarian tumor during pregnancy. Cochrane Database Syst Rev 2006;(4): CD005459.
Calland JF, Tanaka K, Foley E, Bovbjerg VE, Markey DW, Blome S, Minasi JS, Hanks JB, Moore MM, Young JS, Jones RS, Schirmer BD, Adams RB. Outpatient laparoscopic cholecystectomy: patient outcomes after implementation of a clinical pathway. Ann Surg 2001; 233(5): 704-715.
Cameron AM and Busuttil RW. The status of liver transplantation for hepatitis C. Expert Opin Biol Ther 2006; 6(10): 993-1002.
Cios TJ, Reavis KM, Renton DR, Hazey JW, Mikami DJ, Allemang MT, Davis SS, Paul CM, Melvin WS. Successful closure of gastrotomy using bioabsorbable plugs in a canine model (S047). SAGES 2007 Meeting. 2007.
Eckel F, Schneider G, Schmid RM. Pancreatic cancer: a review of recent advances. Expert Opin Investig.Drugs 2006; 15(11): 1395-1410.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
56 REFERENCES
Ellsmere J, Jones D, Pleskow D, Chuttani R. Endoluminal instrumentation is changing gastrointestinal surgery. Surgical Endoscopy 2006; 13(2): 145-151.
Falcone T and Steiner CP. Robotically assisted gynaecological surgery. Hum Fertil.(Camb.) 2002; 5(2): 72-74.
Fong DG, Pai RD, Thompson CC. Transcolonic endoscopic abdominal exploration: a NOTES survival study in a porcine model. Gastrointest Endosc 2007; 65(2): 312-318.
Forsythe RM, Harbrecht BG, Peitzman AB. Blunt splenic trauma. Scand J Surg 2006; 95(3): 146-151.
Fritscher-Ravens A, Mosse CA, Ikeda K, Swain P. Endoscopic transgastric lymphadenectomy by using EUS for selection and guidance. Gastrointest Endosc 2006; 63(2): 302-306.
Fritscher-Ravens A, Mosse CA, Mukherjee D, Mills T, Park PO, Swain CP. Transluminal endosurgery: single lumen access anastomotic device for flexible endoscopy. Gastrointest Endos 2003; 58(4): 585-591.
Fu Louis Kuo Tai. The origins of surgery: 1. From prehistory to Renaissance. Ann College Surg HK 1999; 3(4): 127-136.
Grady D. Doctors Try New Surgery for Gallbladder Removal. The New York Times 2007; 20 April 2007
Greenhalf W. An unfavourable prognosis for pancreatic cancer indicates fields of opportunity. Gut 2006; 55(11): 1533-1535.
Hawn MT, Bian J, Leeth RR, Ritchie G, Allen N, Bland KI, Vickers SM. Impact of obesity on resource utilization for general surgical procedures. - Annals of Surgery 2005; 241(5): 821-826.
Hayes C, Ambazidis S, Gani JS. Intensive care unit admissions following laparoscopic surgery: what lessons can be learned? Aust N Z J Surg 1996; 66(4): 206-209.
Hazey JW, Needleman BJ, Melvin WS, Mikami DJ, Narula VR. Transgastric instrumentation and bacterial contamination of the peritoneal cavity (S044). SAGES 2007 Meeting. 2007.
Hilger WS, Magrina JF, Magtibay PM. Laparoscopic management of the adnexal mass. Clin Obstet Gynecol 2006; 49(3): 535-548.
Hochberger J and Lamade W. Transgastric surgery in the abdomen: The dawn of a new era? Gastrointest Endosc 2005; 62(2): 293-296.
Humes DJ and Simpson J. Acute appendicitis. BMJ 2006; 333(7567): 530-534.
Jagannath SB, Kantsevoy SV, Vaughn CA, Chung SSC, Cotton PB, Gostout CJ, Hawes RH, Pasricha PJ, Scorpio DG, Magee CA, Pipitone LJ, Kalloo AN.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
REFERENCES 57
Peroral transgastric endoscopic ligation of fallopian tubes with long-term survival in a porcine model. Gastrointest Endosc 2005; . 61(3)
Johnson WR. Laparoscopic surgery: time for re-evaluation. Med J Aust 1996; 165(7): 355-356.
Kaido T. Recent randomized controlled trials in pancreaticoduodenectomy. Pancreas 2006; 33(3): 228-232.
Kalloo AN, Singh VK, Jagannath SB, Niiyama H, Hill SL, Vaughn CA, Magee CA, Kantsevoy SV. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc 2004; 60(1): 114-117.
Kantsevoy SV, Hu B, Jagannath SB, Vaughn CA, Beitler DM, Chung SSC, Cotton PB, Gostout CJ, Hawes RH, Pasricha PJ, Magee CA, Pipitone LJ, Talamini MA, Kalloo AN. Transgastric endoscopic splenectomy - Is it possible? Surgical Endoscopy 2006a; 20(3): 522-525.
Kantsevoy SV, Jagannath SB, Niiyama H, Chung SS, Cotton PB, Gostout CJ, Hawes RH, Pasricha PJ, Magee CA, Vaughn CA, Barlow D, Shimonaka H, Kalloo AN. Endoscopic gastrojejunostomy with survival in a porcine model. Gastrointest Endosc 2005; 62(2): 287-292.
Kantsevoy SV, Niiyama H, Jagannath SB, Chung SS, Cotton PB, Gostout CJ, Hawes RH, Pasricha PJ, Magee CA, Vaughn CA, Barlow D, Kawano H, Shimonaka H, Kalloo AN. The endoscopic transilluminator: an endoscopic device for identification of the proximal jejunum for transgastric endoscopic gastrojejunostomy. Gastrointest Endosc 2006b; 63(7): 1055-1058.
Kapischke M, Caliebe A, Tepel J, Schulz T, Hedderich J. Open versus laparoscopic appendicectomy: a critical review. Surg Endosc 2006; 20(7): 1060-1068.
Katz SC and Pachter HL. Indications for splenectomy. Am Surg 2006; 72(7): 565-580.
Kemmer H, Siemer S, Stockle M. Nephrectomy, Work Bench Surgery, and Autotransplantation: A Case of a Solitary Left Kidney with an Extensive Centrally Located Renal Cell Carcinoma and a Tumour Thrombus Entering the Vena Cava. Eur Urol 2007;
Keus F, de Jong JA, Gooszen HG, van Laarhoven CJ. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev 2006;(4): CD006231.
King J. Polycystic ovary syndrome. J Midwifery Womens Health 2006; 51(6): 415-422.
Ko C-W and Kalloo AN. Per-oral transgastric abdominal surgery. Chinese Journal of Digestive Diseases. 2006; 7(2): 67-70.
Koene HR. Critical issues of current and future developments in the treatment of immune thrombocytopenic purpura. Pediatr Blood Cancer 2006; 47(5 Suppl): 703-705.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
58 REFERENCES
Kulier R, Boulvain M, Walker D, Candolle G, Campana A. Minilaparotomy and endoscopic techniques for tubal sterilisation. Cochrane Database Syst Rev 2004;(3): CD001328.
Lamade W, Hochberger J, Lamade W, Hochberger J. Transgastric surgery: avoiding pitfalls in the development of a new technique. Gastrointest Endosc 2006; 63(4): 698-700.
Larson SD, Nealon WH, Evers BM. Management of gallstone pancreatitis. Adv Surg 2006; 40: 265-284.
Lehman AC, Rentschler ME, Farritor SM, Oleynikov D. Endoluminal minirobots for transgastric peritoneoscopy. Minimally Invasive Therapy & Allied Technologies 2006; 15(6): 384-388.
Liao JC, Breda A, Schulam PG. Laparoscopic renal surgery for benign disease. Curr Urol Rep 2007; 8(1): 12-18.
Lima E, Rolanda C, Pego JM, Henriques-Coelho T, Silva D, Carvalho JL, Correia-Pinto J. Transvesical endoscopic peritoneoscopy: a novel 5 mm port for intra-abdominal scarless surgery. J Urol 2006; 176(2): 802-805.
Malik A, Mellinger JD, Hazey JW, Dunkin BJ, MacFadyen BV. Endoluminal and transluminal surgery: current status and future possibilities. Surgical Endoscopy and Other Interventional Techniques 2006; 20(8): 1179-1192.
Marks J. A novel technique for management of endoscopic gastrotomy following NOTES (P013). SAGES 2006 Meeting. 2006.
Marks J, McGee M, Onders R, Chak A, Williams C, Jin J, Schomisch S, Ponsky J. Complete endoscopic closure of gastrotomy following NOTES utilizing the NDO plicator (S049). SAGES 2007 Meeting. 2007a.
Marks J, McGee M, Raymond Onders R, Chak A, Williams C, Jin J, Schomisch S, Ponsky J. Complete endoscopic closure of gastrotomy following NOTES utilizing the NDO plicator (V024). SAGES 2007 Meeting. 2007b.
Marks J, McGee M, Rosem M, Onders R, Chak A, Faulx A, Ignagni A, Schomisch S, Ponsky J. NOTES (V001). SAGES 2006 Meeting. 2006.
Martin I. Bariatric surgery: folly or the future? N Z Med J 2004; 117(1207): U1209.
Mastorakos G, Lambrinoudaki I, Creatsas G. Polycystic ovary syndrome in adolescents: current and future treatment options. Paediatr Drugs 2006; 8(5): 311-318.
Matthes K, Yusuf TE, Mino-Kenudson M, Rattner DW, Brugge WR. Feasibility of endoscopic transgastric distal pancreatectomy (EDTP) (P505). SAGES 2007 Meeting. 2007a.
Matthes K, Yusuf TE, Mino-Kenudson M, Rattner DW, Brugge WR. Feasibility of endoscopic transgastric distal pancreatectomy (EDTP) (resident session). SAGES 2007 Meeting. 2007b.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
REFERENCES 59
McGee MF, Marks JM, Amitabh Chak A, Onders RP, Schomisch SJ, Andrews JM, Delaney CP. Combined transrectal and transgastric NOTES in the porcine model (V028). SAGES 2007 Meeting. 2007a.
McGee MF, Marks JM, Chak A, Onders RP, Schomisch SJ, Andrews JM, Delaney CPP. Feasibility of transrectal NOTES in the porcine model (P018). SAGES 2007 Abstracts. 2007b.
McGee MF, Marks JM, Onders RP, Chak A, Rosen MJ, Williams CP, Judy Jin J, Schomisch SJ, Ponsky JL. Transrectal endoscopic surgery (NOTES) with percutaneous endoscopic gastrotomy (PEG) tube closure: A quantitative bacteriologic study in the porcine model (S045). SAGES 2007 Meeting. 2007c.
McGee MF, Rosen MJ, Marks J, Chak A, Onders R, Faulx A, Ignagni A, Schomisch S, Ponsky J. A reliable method for monitoring intraabdominal pressure during natural orifice translumenal endoscopic surgery. Surgical Endoscopy 2007d;
McGee MF, Rosen MJ, Marks J, Chak A, Onders RP, Faulx A, Ignagni A, Schomisch S, Ponsky J. A reliable method for intra-abdominal pressure monitoring during NOTES (S013). 2006a.
McGee MF, Rosen MJ, Marks J, Onders RP, Chak A, Faulx A, Chen VK, Ponsky J. A primer on natural orifice transluminal endoscopic surgery: building a new paradigm. Surg Innov. 2006b; 13(2): 86-93.
Mehrabi A, Kashfi A, Fonouni H, Schemmer P, Schmied BM, Hallscheidt P, Schirmacher P, Weitz J, Friess H, Buchler MW, Schmidt J. Primary malignant hepatic epithelioid hemangioendothelioma: a comprehensive review of the literature with emphasis on the surgical therapy. Cancer 2006; 107(9): 2108-2121.
Meireles OR, Kantsevoy S, Assumpcao LR, Hanly EJ, Kalloo AN, Marohn MR. Reliable gastric closure after NOTES using a novel per-oral felxible stapling device (S048). SAGES 2007 Meeting. 2007.
Merrifield BF, Wagh MS, Thompson CC. Peroral transgastric organ resection: A feasibility study in pigs. Gastrointest Endosc 2006; 63(4): 693-697.
Mintz Y, Cullen J, Falor E, Talamini MA. Dual lumen NOTES: A new method for performing a safe anastomosis (S046). SAGES 2007 Meeting. 2007a.
Mintz Y, Cullen J, Stuart D, Falor E, Talamini MA. NOTES: Technical problems and solutions (V023). SAGES 2007 Meeting. 2007b.
Moscatiello S, Manini R, Marchesini G. Diabetes and liver disease: an ominous association. Nutr Metab Cardiovasc Dis 2007; 17(1): 63-70.
Neto MG, Ramos A, Campos J, Amaral P, Moura E, Galvao MCA, Falcao M. Transgastric salpingectomy in a porcine animal. A NOTES procedure (V027). SAGES 2007 Meeting. 2007.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
60 REFERENCES
Nezhat C, Saberi NS, Shahmohamady B, Nezhat F. Robotic-assisted laparoscopy in gynecological surgery. JSLS 2006; 10(3): 317-320.
O'Grady JG and Williams R. Liver transplantation for viral hepatitis. Br Med Bull 1990; 46(2): 481-491.
O'Rourke NA FAU and Fielding GA. - Laparoscopic cholecystectomy for acute cholecystitis. - Aust N Z J Surg 1992 Dec;62(12): 944-946.
Onders R, Marks J, Ignagni A, McGee MS, Rosen M, Chak A, Faulx A. Diaphragm pacing with NOTES: Potential for difficult to wean ICU patients (S050). SAGES 2006 Meeting. 2006a.
Onders R, Marks J, Ignagni A, McGee MS, Rosen M, Chak A, Faulx A, Schilz R, Schomisch S, Ponsky J. NOTES as a diagnostic tool in the ICU (S015). SAGES 2006 Meeting. 2006b.
Onders R, Mcgee M, Marks J, Chak A, Schilz R, Rosen M, Ignagni A, Faulx A, Elmo M, Schomisch S, Ponsky J, Schauer P, Chand B, Brethauer S. Diaphragm pacing with natural orifice transluminal endoscopic surgery: potential for difficult-to-wean intensive care unit patients. Surgical Endoscopy 2007a; 3: 475-479.
Onders RP, McGee MF, Marks J, Chak A, Rosen MJ, Ignagni A, Faulx A, Schomisch S, Ponsky J. Natural orifice transluminal endoscopic surgery (NOTES) as a diagnostic tool in the intensive care unit. Surgical Endoscopy 2007b; 21(4): 681-683.
Osborne DA, Alexander G, Boe B, Zervos EE. Laparoscopic cholecystectomy: past, present, and future. Surg Technol Int 2006; 15: 81-85.
Osborne EK, Shear MA, Lederman AB, Ritter M, Robert D Fanelli RD. Endoscopy-assisted laparoscopic transluminal resection of a GE junction tumor: A case report (P507). SAGES 2007 Meeting. 2007.
Pai RD, Fong DG, Bundga ME, Odze RD, Rattner DW, Thompson CC. Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model. Gastrointest Endosc 2006; 64(3): 428-434.
Park PO, Bergstrom M, Ikeda K, Fritscher-Ravens A, Swain P. Experimental studies of transgastric gallbladder surgery: cholecystectomy and cholecystogastric anastomosis. Gastrointest Endosc 2005; 61(4): 601-606.
Park PO, Bergström M, Ikeda K, Mosse S, Fritcher-Ravens A, Swain P. The flexible development and testing of a new simple flexible endoscopic suturing method for intraluminal and transgastric surgery (NOTES), with early clinical experience (S020). SAGES 2007 Meeting. 2007.
Power RE, Preston JM, Griffin A, Martin I, Wall DR, Nicol DL. Laparoscopic vs open living donor nephrectomy: a contemporary series from one centre. BJU Int 2006; 98(1): 133-136.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
REFERENCES 61
Rattner D and Kalloo A. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. October 2005. Surg Endosc 2006; 20(2): 329-333.
Rentschler ME, Dumpert J, Platt S, Farritor SM, Oleynikov D. NOTES with a wireless endoluminal mobile robot (S011). SAGES 2006 Meeting. 2006.
Rhodes MF, Rudd MF, O'Rourke NF, Nathanson LF, Fielding G. - Laparoscopic splenectomy and lymph node biopsy for hematologic disorders. - Ann Surg 1995 Jul;222(1): 43-46.
Richards WO and Rattner DW. Endoluminal and transluminal surgery: No longer if, but when. Surgical Endoscopy 2005; 19(4): 461-463.
Rolanda C, Lima E, Pego JM, Henriques-Coelho T, Silva D, Moreira I, Macedo G, Carvalho JL, Correia-Pinto J. Third-generation cholecystectomy by natural orifices: transgastric and transvesical combined approach. Gastrointest Endosc 2007; . 65(1)
Romanelli JR, Desilets DJ, Surti VC, Earle DB. Early experience with visceral closure in NOTES procedures in a porcine model (P508). SAGES 2007 Meeting. 2007.
Romero FR, Rais-Bahrami S, Permpongkosol S, Fine SW, Kohanim S, Jarrett TW. Primary carcinoid tumors of the kidney. J Urol 2006; 176(6 Pt 1): 2359-2366.
Rongey C and Kaplowitz N. Current concepts and controversies in the treatment of alcoholic hepatitis. World J Gastroenterol 2006; 12(43): 6909-6921.
Rosen M. Optimizing peritoneal access for NOTES (P321). SAGES 2006 Meeting. 2006.
Ryou M. A novel trans-colonic endoscopic approach to intra-abdominal surgery in the porcine model (P439). SAGES 2006 Meeting. 2006.
Ryou M, Fong D, Thompson CC. Transgastric ventral hernia mesh repair in a porcine model using a new endosurgical operating system (P509). SAGES 2007 Meeting. 2007a.
Ryou M, G Fong DG, Pai R, Rattner DW, Sauer JS, Thompson CC. New automated Technology for NOTES Transmural Access (V025). SAGES 2007 Meeting. 2007b.
Saltzman JR. The Future of Endoscopic Technology. Medscape coverage of: Digestive Disease Week 2004. Last updated 2004. http://www.medscape.com/viewarticle/478425
Sarmiento R, V.J.Villaflor, Duque G, Villaflor V, Navarro NS. NOTES and laparocopy: A documentation on endoscope orientation, manipulation and instrumentation in a porcine model: A labaratory work by an independent endoscopic and laparosocpy center (P510). SAGES 2007 Meeting. 2007.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
62 REFERENCES
Sauerland S, Lefering R, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev 2004;(4): CD001546.
Sclabas GM, Swain P, Swanstrom LL, Sclabas GM, Swain P, Swanstrom LL. Endoluminal methods for gastrotomy closure in natural orifice transenteric surgery (NOTES). Surg Innov 2006; 13(1): 23-30.
Scott DJ, Tang SJ, Fernandez R, Bergs R, Cadeddu JA. Transgastric, transcolonic and transvaginal cholecystectomy using magnetically anchored instruments (P511). SAGES 2007 Meeting. 2007a.
Scott DJ, Tang SJ, Fernandez R, Bergs R, Goova MT, I., Cadeddu JA. Completely transvaginal cholecystectomy using magnetically anchored instruments (S002). SAGES 2007 Meeting. 2007b.
Sereno S, Forgione A, Simone M, Perretta S, Alzahrani A, Dallemagne B, Marescaux J. Transgastric left adenalectomy in a survived porcine model after transgastric cholecystectomy (V03). SAGES 2007 Meeting. 2007.
Shih SP, Meireles OR, Kantsevoy SV, Hanly EJ, Kalloo AN, Jagganath SB, Beitler DM, Marohn MR. Hybrid minimally invasive surgery - a bridge between laparoscopic and translumenal surgery. SAGES 2006 Meeting. 2006.
Shinohara K. Investigation of the technical problems for the development of NOTES assisting system (P512). SAGES 2007 Meeting. 2007.
Soper N. Natural Orifice Surgery -- The Next "Big Thing"? ACS Surgery: Principles & Practice 2005;
Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Deters JL, Knipschield MA. Endoscopic full-thickness closure of large gastric perforations by use of tissue anchors. Gastrointest Endosc 2007; 65(1): 134-139.
Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Deters JL, Knipschield MA, Hawes RH, Kalloo AN, Pasricha PJ, Chung S, Kantsevoy SV, Cotton PB. Pilot study of the porcine uterine horn as an in vivo appendicitis model for development of endoscopic transgastric appendectomy. Gastrointest Endosc 2006; 64(5): 808-812.
Swanstrom LL. Current technology development for natural orifice transluminal endoscopic surgery. Cir Esp 2006; 80(5): 283-288.
Swanstrom LL, Kozarek R, Pasricha PJ, Gross S, Birkett D, Park PO, Saadat V, Ewers R, Swain P. Development of a new access device for transgastric surgery. J Gastrointest Surg 2005; 9(8): 1129-1136.
Swanstrom LL, Kozarek RA, Soper ND. A new generation of flexible endoscope and instrumentation for advanced endoscopy and NOTES (S021). SAGES 2007 Meeting. 2007.
Tchana-Sato V, Detry O, Polus M, Thiry A, Detroz B, Maweja S, Hamoir E, Defechereux T, Coimbra C, De Roover A, Meurisse M, Honore P. Carcinoid
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
REFERENCES 63
tumor of the appendix: a consecutive series from 1237 appendectomies. World J Gastroenterol 2006; 12(41): 6699-6701.
The Age. Cutting Away Pain. The Age 2007;
USGI Medical. USGI Medical Announces First US NOTES Cholecystectomy Procedure . USGI News 2007;
Vitale GC, Davis BR, Tran TC. The advancing art and science of endoscopy. Am J Surg 2005; 190(2)
Volckmann ET, Hungness ES, Soper NJ, Swanstrom LL. Patient perceptions of NOTES (P033). SAGES 2007 Meeting. 2007.
Volk ML, Marrero JA, Lok AS, Ubel PA. Who decides? Living donor liver transplantation for advanced hepatocellular carcinoma. Transplantation 2006; 82(9): 1136-1139.
Wagh MS, Merrifield BF, Thompson CC. Survival studies after endoscopic transgastric oophorectomy and tubectomy in a porcine model. Gastrointest Endosc 2006; 63(3): 473-478.
Wagh MS, Merrifield BF, Thompson CC, Wagh MS. Endoscopic transgastric abdominal exploration and organ resection: initial experience in a porcine model. Clin Gastroenterol Hepatol 2005; 3(9): 892-896.
Wakeman CJ, Martin IG, Robertson RW, Dobbs BR, Frizelle FA. Pancreatic cancer: management and survival. ANZ J Surg 2004; 74(11): 941-944.
Wolf JS, Jr. Devices for hand-assisted laparoscopic surgery. Expert Rev Med Devices 2005; 2(6): 725-730.
Zehetner J, Shamiyeh A, Wayand W. Lost gallstones in laparoscopic cholecystectomy: all possible complications. Am J Surg 2007; 193(1): 73-78.


- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
APPENDIX A – HIERARCHY OF EVIDENCE
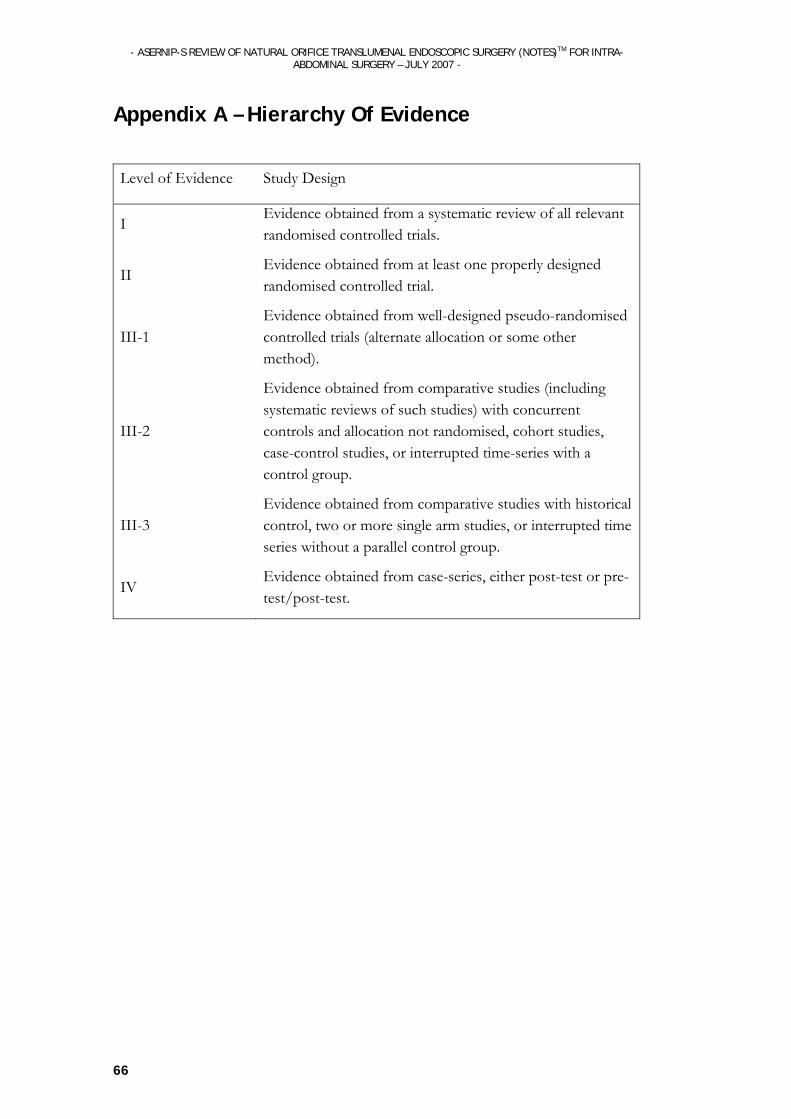
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
66
Appendix A – Hierarchy Of Evidence
Level of Evidence Study Design
I Evidence obtained from a systematic review of all relevant randomised controlled trials.
II Evidence obtained from at least one properly designed randomised controlled trial.
III-1 Evidence obtained from well-designed pseudo-randomised controlled trials (alternate allocation or some other method).
III-2
Evidence obtained from comparative studies (including systematic reviews of such studies) with concurrent controls and allocation not randomised, cohort studies, case-control studies, or interrupted time-series with a control group.
III-3 Evidence obtained from comparative studies with historical control, two or more single arm studies, or interrupted time series without a parallel control group.
IV Evidence obtained from case-series, either post-test or pre-test/post-test.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
67
APPENDIX B – CONFERENCE PROCEEDINGS

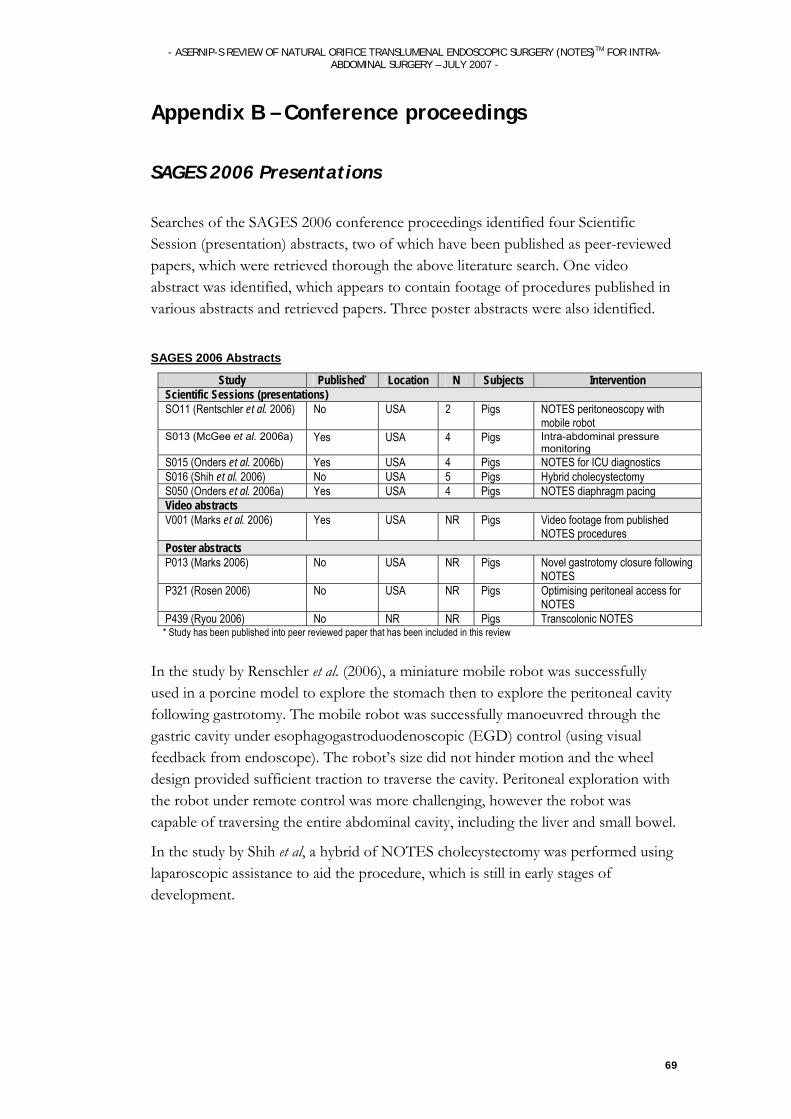
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
69
Appendix B – Conference proceedings
SAGES 2006 Presentations
Searches of the SAGES 2006 conference proceedings identified four Scientific Session (presentation) abstracts, two of which have been published as peer-reviewed papers, which were retrieved thorough the above literature search. One video abstract was identified, which appears to contain footage of procedures published in various abstracts and retrieved papers. Three poster abstracts were also identified.
SAGES 2006 Abstracts
Study Published* Location N Subjects Intervention Scientific Sessions (presentations) SO11 (Rentschler et al. 2006) No USA 2 Pigs NOTES peritoneoscopy with
mobile robot S013 (McGee et al. 2006a) Yes USA 4 Pigs Intra-abdominal pressure
monitoring S015 (Onders et al. 2006b) Yes USA 4 Pigs NOTES for ICU diagnostics S016 (Shih et al. 2006) No USA 5 Pigs Hybrid cholecystectomy S050 (Onders et al. 2006a) Yes USA 4 Pigs NOTES diaphragm pacing Video abstracts V001 (Marks et al. 2006) Yes USA NR Pigs Video footage from published
NOTES procedures Poster abstracts P013 (Marks 2006) No USA NR Pigs Novel gastrotomy closure following
NOTES P321 (Rosen 2006) No USA NR Pigs Optimising peritoneal access for
NOTES P439 (Ryou 2006) No NR NR Pigs Transcolonic NOTES * Study has been published into peer reviewed paper that has been included in this review
In the study by Renschler et al. (2006), a miniature mobile robot was successfully used in a porcine model to explore the stomach then to explore the peritoneal cavity following gastrotomy. The mobile robot was successfully manoeuvred through the gastric cavity under esophagogastroduodenoscopic (EGD) control (using visual feedback from endoscope). The robot’s size did not hinder motion and the wheel design provided sufficient traction to traverse the cavity. Peritoneal exploration with the robot under remote control was more challenging, however the robot was capable of traversing the entire abdominal cavity, including the liver and small bowel.
In the study by Shih et al, a hybrid of NOTES cholecystectomy was performed using laparoscopic assistance to aid the procedure, which is still in early stages of development.
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
70
SAGES 2007 presentations Twenty-seven presentations at the SAGES meeting in April 2007 were related to the development of NOTES. Many of the issues that were not adequately addressed in the included studies have been investigated more recently in studies. Searches of the SAGES 2007 ten Scientific Session (presentation) abstracts, nine video abstracts and ten poster abstracts that were relevant to NOTES development, none of which have been subsequently published in peer-reviewed literature, although some groups presented both a video and a poster or scientific session on the same topic. The issues that were addressed were:
Closure
Infections
device development
feasibility of different NOTES intra-abdominal interventions
feasibility of using different access routes for NOTES
physiologic effects of NOTES compared to laparoscopy
patient perceptions of NOTES.
Interventions Successful transvaginal cholecystectomies in pigs were reported in three presentations (Bessler et al. 2007; Scott et al. 2007b), indicating the feasibility of using the vaginal orifice for NOTES. A number of news reports have announced that Bessler has recently performed this procedure on a human, in the first human NOTES procedure in the US (Grady 2007; The Age 2007; USGI Medical 2007), but the SAGES video abstract only describes the procedure in pigs. Although the news reports stated that the transvaginal cholecystectomy in a 66 year old New York woman was performed successfully with USGI devices (Grady 2007; The Age 2007; USGI Medical 2007), no further clinical trial data or peer-reviewed information could be obtained.
Transrectal cholecystectomy was also reported in one study, where it was successfully performed in 6 pigs (McGee et al. 2007b). Matthes et al. reported successfully performing pancreatectomy using NOTES (EDTP) (Matthes et al. 2007a; Matthes et al. 2007b). One scientific session reported successful bowel anastomosis in pigs using both the upper and lower GI tract as entry points and stapling devices designed for laparoscopic surgery (Mintz et al. 2007a). In a video presentation, Sereno et al. reported the feasibility of multiple transgastric operations by successfully performing transgastric cholecystectomy followed by adrenalectomy in a pig model (Sereno et al. 2007). Another video presentation reported successful and reliable transgastric salpingectomy using five pigs (Neto et al. 2007). In one poster, Ryou et al. reported successfully performing transgastric ventral hernia mesh repair in one pig using an

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
71
EndoSurgical Operating System (EOS) featuring ShapeLock technology from USGI Medical. This group will be performing further porcine survival studies (Ryou et al. 2007a). Neto et al. (2007) demonstrated that transgastric salpingectomy in a porcine model is reliable and achievable and could help develop NOTES procedures.
Instrumentation Magnetic Anchoring and Guidance System (MAGS) instruments were used by Scott et al. to perform transvaginal cholecystectomies. The procedure involved inserting a rigid access port with integrated instrument tethers (electric, mechanical, and pneumatic power supplies) into the peritoneal cavity. This allowed a CO2 pneumoperitoneum to be maintained and enabled instruments to be held in place on the peritoneal surface using magnetic coupling. Some problems encountered with this system included inadvertent magnetic coupling between instruments, preventing cholecystectomies from being performed in the first two animals. Problems were overcome using new instrumentation with a longer access port to provide easier deployment of instruments and suitable reach, which allowed transvaginal cholecystectomy to be successfully completed in the third animal. Thus, MAGS may facilitate a NOTES approach while alleviating shortcomings of a flexible platform by offering triangulation and rigidity.
A novel suturing device employed by Park et al. allowed simple and easy to use endoscopic suturing almost anywhere in the GI-tract that can be reached by a flexible endoscope. The potential of this suturing technique was demonstrated in clinical results reported in three patients, where it was used to successfully close gastric ulcers. Swanstrom et al. reported the development of a novel 4 channel rigidizing endoscopic access device that will define the next generation of operating endoscopes. The device was successfully used in human cadavers, but will need to be further developed in live animal and human trials.
Peritoneal contamination For the first time, the bacterial load and contamination of the peritoneal cavity due to gastrotomy and transgastric instrumentation was reported by Hazey et al. In patients (humans), who requited a gastrotomy for gastric bypass, it was reported that transgastric instrumentation does contaminate the abdominal cavity, however pathogens are clinically insignificant due to species or bacterial load.
Viscerotomy closure McGee explored the use of PEG tubes to manage NOTES gastrotomies while providing chronic enteral access. They reported that 94.7% (18/19) of animals survived the entire 14 day period without observable sequelae, however one animal died on post-operative day two after the PEG tube dislodged. At 14 days, 27.8% (5/19) of animals demonstrated intra-abdominal abscesses, 38.9% (7/19) had positive peritoneal wash cultures, and 55.6% (10/19) of wires were contaminated on culture. Seventy-five percent (12/19) of animals had either abscess, positive peritoneal, or positive wire culture at the end of the study. Pre-procedural lavage was
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
72
not effective in completely evacuating gastric succus, as 38.5% (8/13) of animals had intra-operative NOTES peritoneal fluid cultures growth in excess of 103 CFU/ml of bacteria. Infectious complications may represent failure of PEG gastrotomy management or intra-operative seeding and deposition of succus during NOTES. Alternatively, complications may be caused by conditions unique to the pig such as inability to evacuate bezoars, dependent positioning of the PEG, and quadrupedism, necessitating further studies to determine if porcine models are appropriate and applicable to human subjects in the NOTES setting.
Sereno et al. reported that successful closure of gastrotomies with endoscopic clips is possible but challenging and difficult to reproduce, thus a more reliable closure method needs to be used for NOTES. A more reliable device was the Power Medical SurgASSIST device, used by Meireles et al., which may provide a simple, secure, reliable, technique for gastric closure following NOTES. Marks et al. reported that the NDO Plicator was successfully used for gastrotomy closure in pigs and may be a particularly useful tool in obtaining complete closure of gastric perforations, anastomotic leaks, and performing stomal reduction following gastric bypass procedures. Durable closure of the gastric perforation with physiologic healing of the injury site was reported by Cios et al., when using a bioabsorbable device to plug gastrotomies.
Physiologic effects of NOTES In a study comparing the physiologic effects of NOTES with laparotomy in a pig model, Bingener et al. reported significant cardiopulmonary differences between the NOTES and laparoscopic group. However no clear evidence of detrimental changes was encountered so far.
Patient perceptions of NOTES In a survey of patients’ perceptions, Volckmann et al. reported that when offered a choice, the majority of patients prefer cholecystectomy by NOTES to laparoscopy, but in a study of bariatric patients, Osborne et al. reported that laparoscopy was clearly preferred by patients over NOTES. Discrepancies may have resulted from the information on the procedures that was presented to survey participants, so care must be taken when using these results. Osborne et al. also reported that
Acceptability of various orifices depended strongly on the distance from the entry site to the target organ and the oral route was generally preferred. When comparing operations, procedure related risks, pain, and recovery time are more important than cosmesis, cost, length of hospital stay, or anaesthesia type. Patients are willing to accept some increased risk for NOTES, but are less willing to accept NOTES as the risks and cost increase and as surgeon experience and procedure availability decrease.
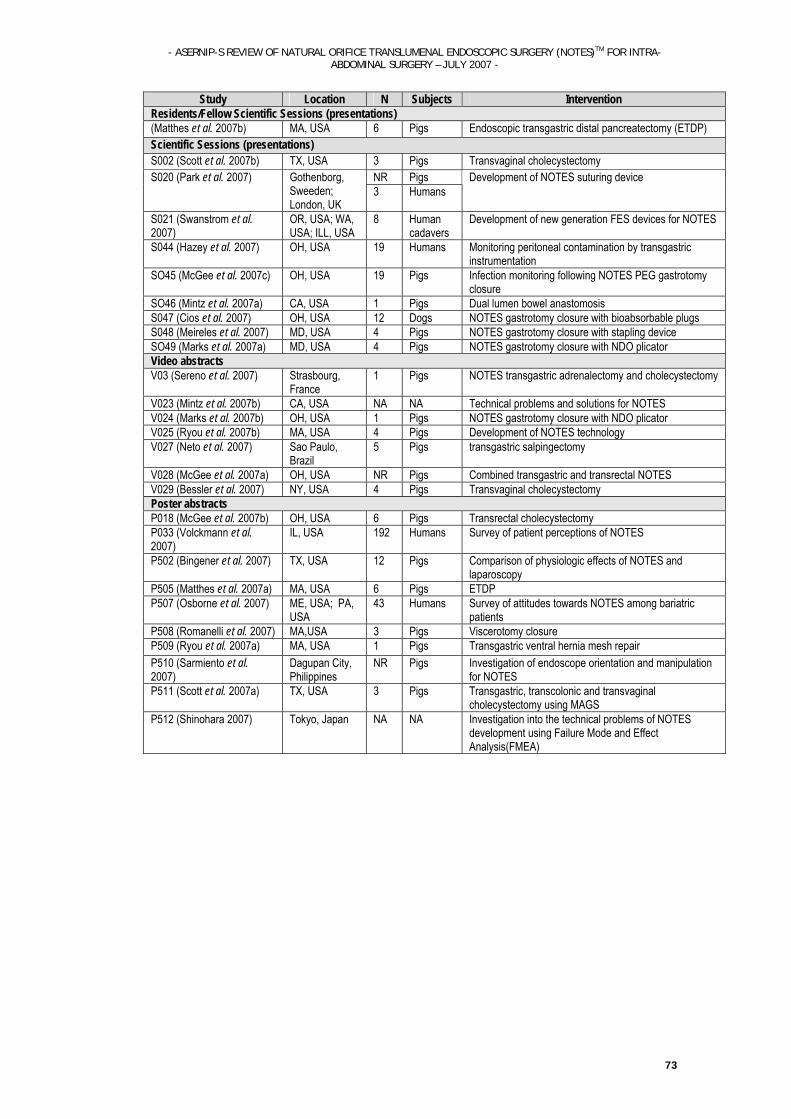
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
73
Study Location N Subjects Intervention Residents/Fellow Scientific Sessions (presentations) (Matthes et al. 2007b) MA, USA 6 Pigs Endoscopic transgastric distal pancreatectomy (ETDP) Scientific Sessions (presentations) S002 (Scott et al. 2007b) TX, USA 3 Pigs Transvaginal cholecystectomy
NR Pigs S020 (Park et al. 2007) Gothenborg, Sweeden; London, UK
3 Humans Development of NOTES suturing device
S021 (Swanstrom et al. 2007)
OR, USA; WA, USA; ILL, USA
8 Human cadavers
Development of new generation FES devices for NOTES
S044 (Hazey et al. 2007) OH, USA 19 Humans Monitoring peritoneal contamination by transgastric instrumentation
SO45 (McGee et al. 2007c) OH, USA 19 Pigs Infection monitoring following NOTES PEG gastrotomy closure
SO46 (Mintz et al. 2007a) CA, USA 1 Pigs Dual lumen bowel anastomosis S047 (Cios et al. 2007) OH, USA 12 Dogs NOTES gastrotomy closure with bioabsorbable plugs S048 (Meireles et al. 2007) MD, USA 4 Pigs NOTES gastrotomy closure with stapling device SO49 (Marks et al. 2007a) MD, USA 4 Pigs NOTES gastrotomy closure with NDO plicator Video abstracts V03 (Sereno et al. 2007) Strasbourg,
France 1 Pigs NOTES transgastric adrenalectomy and cholecystectomy
V023 (Mintz et al. 2007b) CA, USA NA NA Technical problems and solutions for NOTES V024 (Marks et al. 2007b) OH, USA 1 Pigs NOTES gastrotomy closure with NDO plicator V025 (Ryou et al. 2007b) MA, USA 4 Pigs Development of NOTES technology V027 (Neto et al. 2007) Sao Paulo,
Brazil 5 Pigs transgastric salpingectomy
V028 (McGee et al. 2007a) OH, USA NR Pigs Combined transgastric and transrectal NOTES V029 (Bessler et al. 2007) NY, USA 4 Pigs Transvaginal cholecystectomy Poster abstracts P018 (McGee et al. 2007b) OH, USA 6 Pigs Transrectal cholecystectomy P033 (Volckmann et al. 2007)
IL, USA 192 Humans Survey of patient perceptions of NOTES
P502 (Bingener et al. 2007) TX, USA 12 Pigs Comparison of physiologic effects of NOTES and laparoscopy
P505 (Matthes et al. 2007a) MA, USA 6 Pigs ETDP P507 (Osborne et al. 2007) ME, USA; PA,
USA 43 Humans Survey of attitudes towards NOTES among bariatric
patients P508 (Romanelli et al. 2007) MA,USA 3 Pigs Viscerotomy closure P509 (Ryou et al. 2007a) MA, USA 1 Pigs Transgastric ventral hernia mesh repair P510 (Sarmiento et al. 2007)
Dagupan City, Philippines
NR Pigs Investigation of endoscope orientation and manipulation for NOTES
P511 (Scott et al. 2007a) TX, USA 3 Pigs Transgastric, transcolonic and transvaginal cholecystectomy using MAGS
P512 (Shinohara 2007) Tokyo, Japan NA NA Investigation into the technical problems of NOTES development using Failure Mode and Effect Analysis(FMEA)

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
74
APPENDIX C – EXCLUDED STUDIES
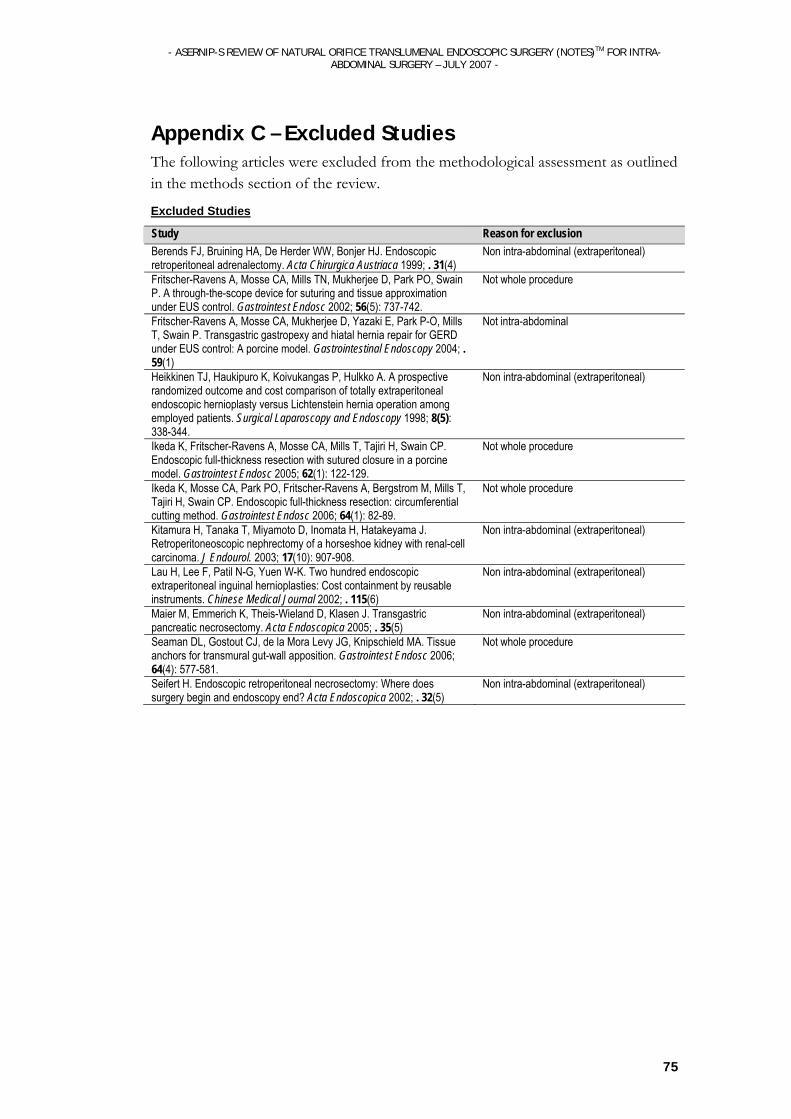
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
75
Appendix C – Excluded Studies The following articles were excluded from the methodological assessment as outlined in the methods section of the review.
Excluded Studies
Study Reason for exclusion Berends FJ, Bruining HA, De Herder WW, Bonjer HJ. Endoscopic retroperitoneal adrenalectomy. Acta Chirurgica Austriaca 1999; . 31(4)
Non intra-abdominal (extraperitoneal)
Fritscher-Ravens A, Mosse CA, Mills TN, Mukherjee D, Park PO, Swain P. A through-the-scope device for suturing and tissue approximation under EUS control. Gastrointest Endosc 2002; 56(5): 737-742.
Not whole procedure
Fritscher-Ravens A, Mosse CA, Mukherjee D, Yazaki E, Park P-O, Mills T, Swain P. Transgastric gastropexy and hiatal hernia repair for GERD under EUS control: A porcine model. Gastrointestinal Endoscopy 2004; . 59(1)
Not intra-abdominal
Heikkinen TJ, Haukipuro K, Koivukangas P, Hulkko A. A prospective randomized outcome and cost comparison of totally extraperitoneal endoscopic hernioplasty versus Lichtenstein hernia operation among employed patients. Surgical Laparoscopy and Endoscopy 1998; 8(5): 338-344.
Non intra-abdominal (extraperitoneal)
Ikeda K, Fritscher-Ravens A, Mosse CA, Mills T, Tajiri H, Swain CP. Endoscopic full-thickness resection with sutured closure in a porcine model. Gastrointest Endosc 2005; 62(1): 122-129.
Not whole procedure
Ikeda K, Mosse CA, Park PO, Fritscher-Ravens A, Bergstrom M, Mills T, Tajiri H, Swain CP. Endoscopic full-thickness resection: circumferential cutting method. Gastrointest Endosc 2006; 64(1): 82-89.
Not whole procedure
Kitamura H, Tanaka T, Miyamoto D, Inomata H, Hatakeyama J. Retroperitoneoscopic nephrectomy of a horseshoe kidney with renal-cell carcinoma. J Endourol. 2003; 17(10): 907-908.
Non intra-abdominal (extraperitoneal)
Lau H, Lee F, Patil N-G, Yuen W-K. Two hundred endoscopic extraperitoneal inguinal hernioplasties: Cost containment by reusable instruments. Chinese Medical Journal 2002; . 115(6)
Non intra-abdominal (extraperitoneal)
Maier M, Emmerich K, Theis-Wieland D, Klasen J. Transgastric pancreatic necrosectomy. Acta Endoscopica 2005; . 35(5)
Non intra-abdominal (extraperitoneal)
Seaman DL, Gostout CJ, de la Mora Levy JG, Knipschield MA. Tissue anchors for transmural gut-wall apposition. Gastrointest Endosc 2006; 64(4): 577-581.
Not whole procedure
Seifert H. Endoscopic retroperitoneal necrosectomy: Where does surgery begin and endoscopy end? Acta Endoscopica 2002; . 32(5)
Non intra-abdominal (extraperitoneal)

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
76
APPENDIX D – GLOSSARY OF TERMS AND ABBREVIATIONS
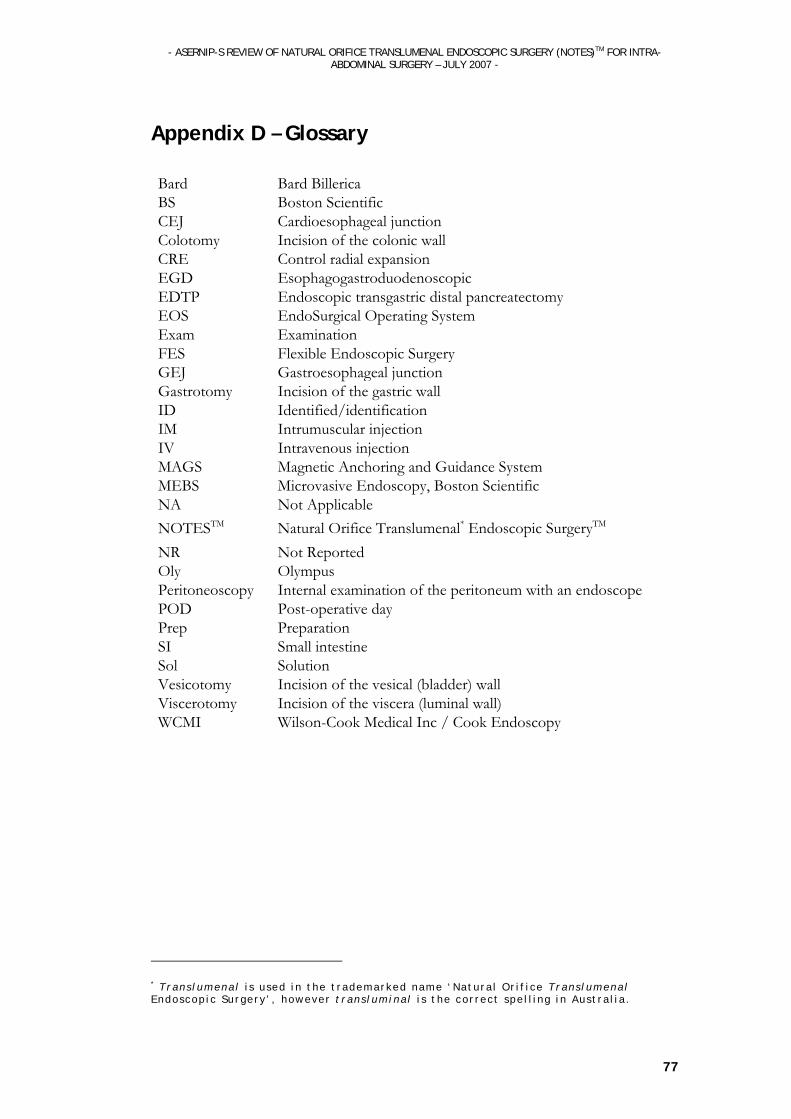
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
77
Appendix D – Glossary
Bard Bard BillericaBS Boston ScientificCEJ Cardioesophageal junctionColotomy Incision of the colonic wallCRE Control radial expansionEGD EsophagogastroduodenoscopicEDTP Endoscopic transgastric distal pancreatectomy EOS EndoSurgical Operating SystemExam ExaminationFES Flexible Endoscopic SurgeryGEJ Gastroesophageal junctionGastrotomy Incision of the gastric wallID Identified/identificationIM Intrumuscular injectionIV Intravenous injectionMAGS Magnetic Anchoring and Guidance SystemMEBS Microvasive Endoscopy, Boston ScientificNA Not ApplicableNOTESTM Natural Orifice Translumenal* Endoscopic SurgeryTM NR Not ReportedOly OlympusPeritoneoscopy Internal examination of the peritoneum with an endoscope POD Post-operative dayPrep PreparationSI Small intestineSol SolutionVesicotomy Incision of the vesical (bladder) wallViscerotomy Incision of the viscera (luminal wall)WCMI Wilson-Cook Medical Inc / Cook Endoscopy
* Trans lumenal i s used in the t rademarked name ‘Natura l Or i f i ce Trans lumenal Endoscop ic Surgery ’ , however t rans luminal i s the cor rect spe l l ing in Aus tra l ia .

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
78
APPENDIX E – EQUIPMENT DESCRPITIONS
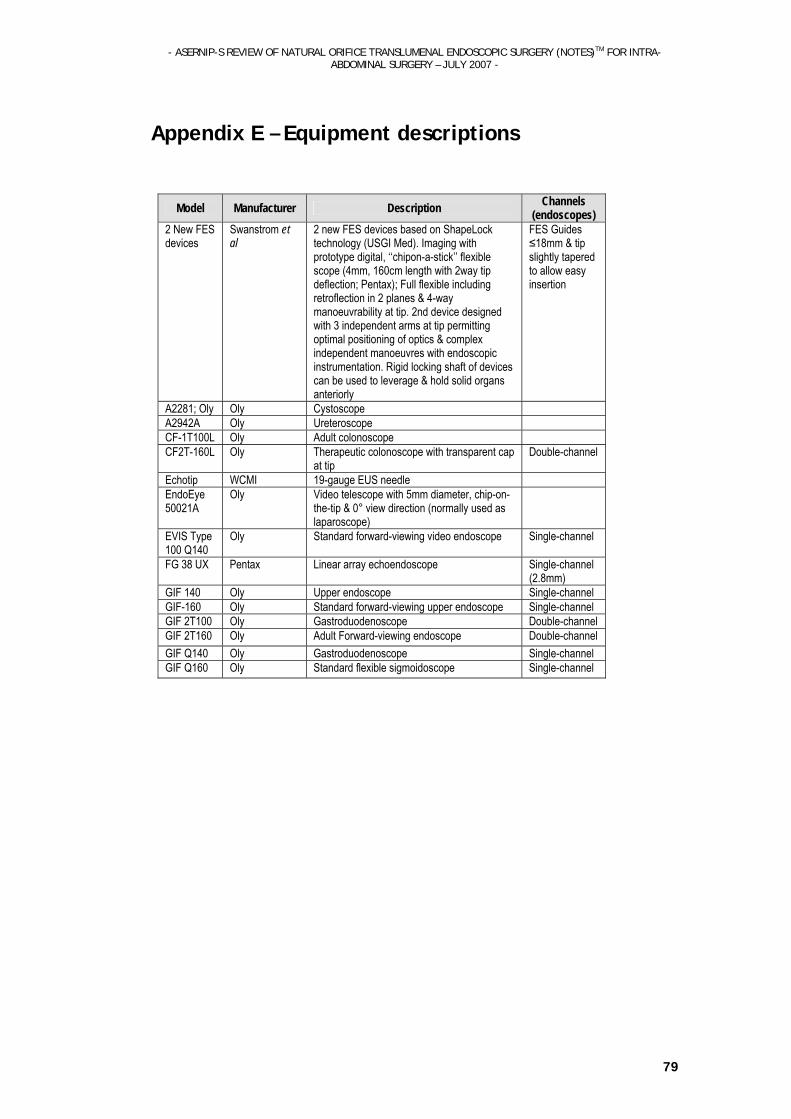
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
79
Appendix E – Equipment descriptions
Model Manufacturer Description Channels
(endoscopes) 2 New FES devices
Swanstrom et al
2 new FES devices based on ShapeLock technology (USGI Med). Imaging with prototype digital, ‘‘chipon-a-stick’’ flexible scope (4mm, 160cm length with 2way tip deflection; Pentax); Full flexible including retroflection in 2 planes & 4-way manoeuvrability at tip. 2nd device designed with 3 independent arms at tip permitting optimal positioning of optics & complex independent manoeuvres with endoscopic instrumentation. Rigid locking shaft of devices can be used to leverage & hold solid organs anteriorly
FES Guides ≤18mm & tip slightly tapered to allow easy insertion
A2281; Oly Oly Cystoscope A2942A Oly Ureteroscope CF-1T100L Oly Adult colonoscope CF2T-160L Oly Therapeutic colonoscope with transparent cap
at tip Double-channel
Echotip WCMI 19-gauge EUS needle EndoEye 50021A
Oly Video telescope with 5mm diameter, chip-on-the-tip & 0° view direction (normally used as laparoscope)
EVIS Type 100 Q140
Oly Standard forward-viewing video endoscope Single-channel
FG 38 UX Pentax Linear array echoendoscope Single-channel (2.8mm)
GIF 140 Oly Upper endoscope Single-channel GIF-160 Oly Standard forward-viewing upper endoscope Single-channel GIF 2T100 Oly Gastroduodenoscope Double-channel GIF 2T160 Oly Adult Forward-viewing endoscope Double-channel GIF Q140 Oly Gastroduodenoscope Single-channel GIF Q160 Oly Standard flexible sigmoidoscope Single-channel

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
80
APPENDIX F – STUDY DESIGN, SAFETY & EFFICACY TABLES
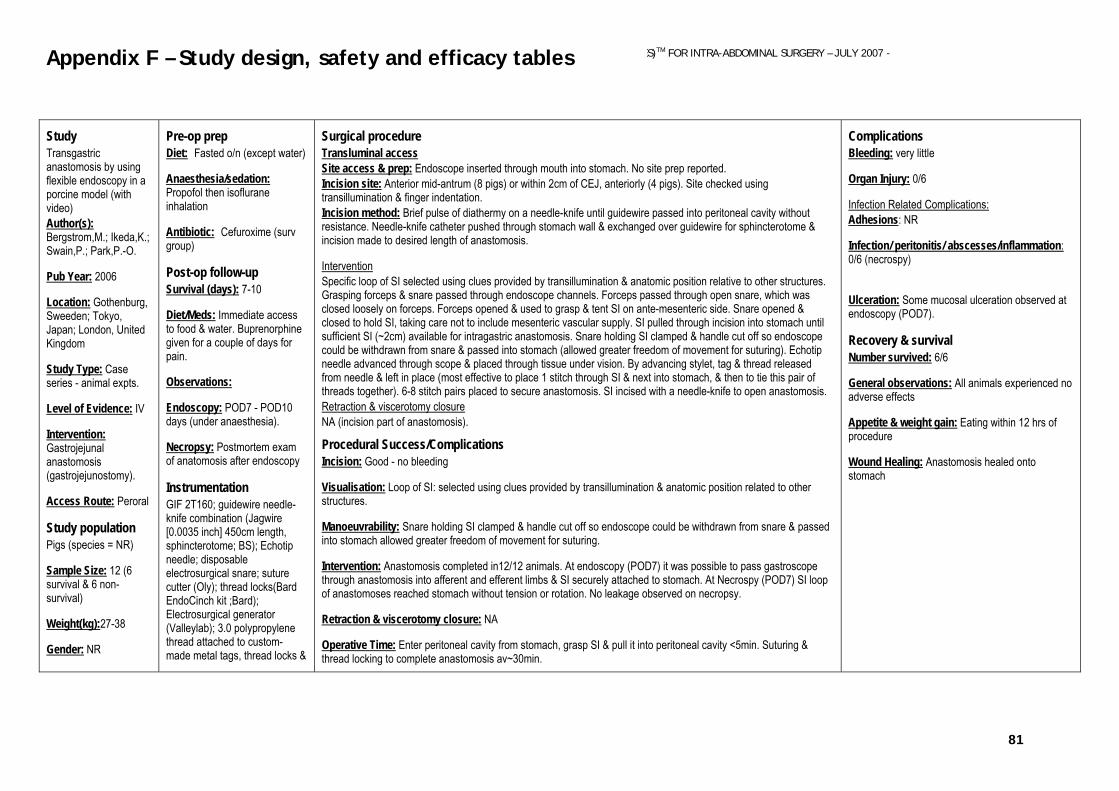
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
81
Study Transgastric anastomosis by using flexible endoscopy in a porcine model (with video) Author(s): Bergstrom,M.; Ikeda,K.; Swain,P.; Park,P.-O.
Pub Year: 2006
Location: Gothenburg, Sweeden; Tokyo, Japan; London, United Kingdom
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Gastrojejunal anastomosis (gastrojejunostomy).
Access Route: Peroral
Study population Pigs (species = NR)
Sample Size: 12 (6 survival & 6 non-survival)
Weight(kg):27-38
Gender: NR
Pre-op prep Diet: Fasted o/n (except water)
Anaesthesia/sedation: Propofol then isoflurane inhalation
Antibiotic: Cefuroxime (surv group)
Post-op follow-up
Survival (days): 7-10
Diet/Meds: Immediate access to food & water. Buprenorphine given for a couple of days for pain.
Observations:
Endoscopy: POD7 - POD10 days (under anaesthesia).
Necropsy: Postmortem exam of anatomosis after endoscopy
Instrumentation
GIF 2T160; guidewire needle-knife combination (Jagwire [0.0035 inch] 450cm length, sphincterotome; BS); Echotip needle; disposable electrosurgical snare; suture cutter (Oly); thread locks(Bard EndoCinch kit ;Bard); Electrosurgical generator (Valleylab); 3.0 polypropylene thread attached to custom-made metal tags, thread locks &
Surgical procedure Transluminal access Site access & prep: Endoscope inserted through mouth into stomach. No site prep reported. Incision site: Anterior mid-antrum (8 pigs) or within 2cm of CEJ, anteriorly (4 pigs). Site checked using transillumination & finger indentation. Incision method: Brief pulse of diathermy on a needle-knife until guidewire passed into peritoneal cavity without resistance. Needle-knife catheter pushed through stomach wall & exchanged over guidewire for sphincterotome & incision made to desired length of anastomosis.
Intervention Specific loop of SI selected using clues provided by transillumination & anatomic position relative to other structures. Grasping forceps & snare passed through endoscope channels. Forceps passed through open snare, which was closed loosely on forceps. Forceps opened & used to grasp & tent SI on ante-mesenteric side. Snare opened & closed to hold SI, taking care not to include mesenteric vascular supply. SI pulled through incision into stomach until sufficient SI (~2cm) available for intragastric anastomosis. Snare holding SI clamped & handle cut off so endoscope could be withdrawn from snare & passed into stomach (allowed greater freedom of movement for suturing). Echotip needle advanced through scope & placed through tissue under vision. By advancing stylet, tag & thread released from needle & left in place (most effective to place 1 stitch through SI & next into stomach, & then to tie this pair of threads together). 6-8 stitch pairs placed to secure anastomosis. SI incised with a needle-knife to open anastomosis. Retraction & viscerotomy closure NA (incision part of anastomosis).
Procedural Success/Complications Incision: Good - no bleeding
Visualisation: Loop of SI: selected using clues provided by transillumination & anatomic position related to other structures.
Manoeuvrability: Snare holding SI clamped & handle cut off so endoscope could be withdrawn from snare & passed into stomach allowed greater freedom of movement for suturing.
Intervention: Anastomosis completed in12/12 animals. At endoscopy (POD7) it was possible to pass gastroscope through anastomosis into afferent and efferent limbs & SI securely attached to stomach. At Necrospy (POD7) SI loop of anastomoses reached stomach without tension or rotation. No leakage observed on necropsy.
Retraction & viscerotomy closure: NA
Operative Time: Enter peritoneal cavity from stomach, grasp SI & pull it into peritoneal cavity <5min. Suturing & thread locking to complete anastomosis av~30min.
Complications Bleeding: very little
Organ Injury: 0/6
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: 0/6 (necrospy)
Ulceration: Some mucosal ulceration observed at endoscopy (POD7).
Recovery & survival Number survived: 6/6
General observations: All animals experienced no adverse effects
Appetite & weight gain: Eating within 12 hrs of procedure
Wound Healing: Anastomosis healed onto stomach
Appendix F – Study design, safety and efficacy tables

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
82
needles. Instrument Prep:
NR
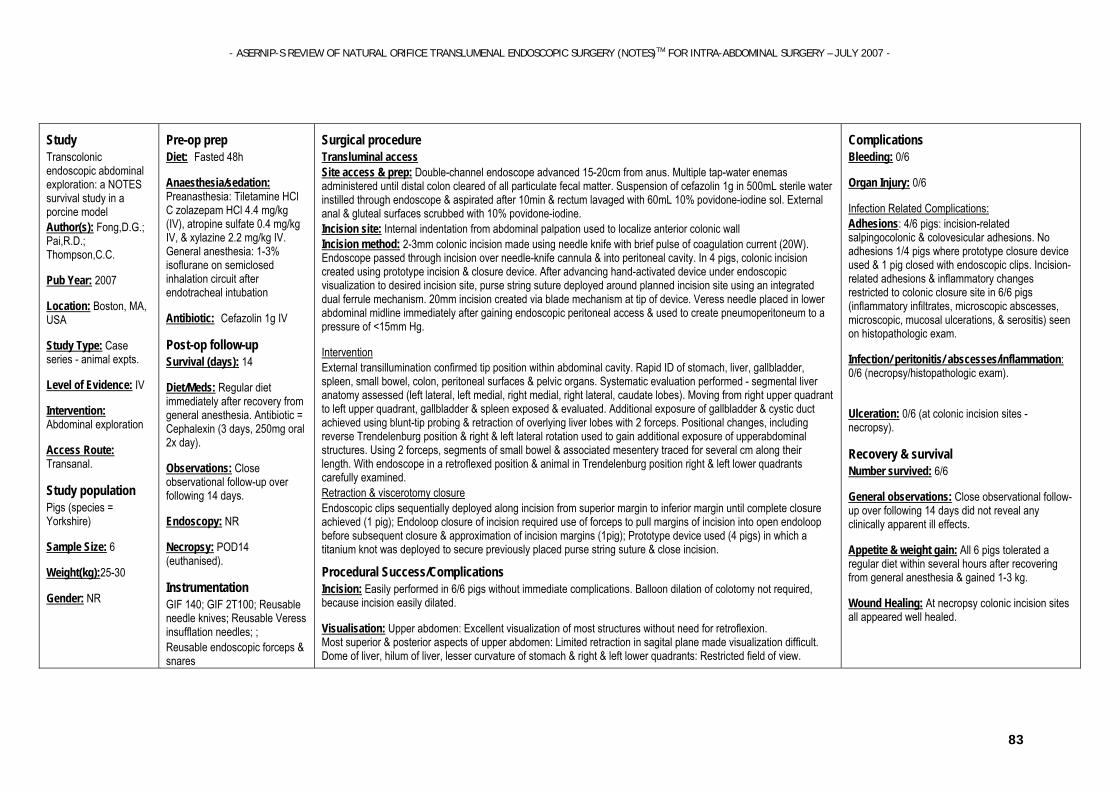
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
83
Study Transcolonic endoscopic abdominal exploration: a NOTES survival study in a porcine model Author(s): Fong,D.G.; Pai,R.D.; Thompson,C.C.
Pub Year: 2007
Location: Boston, MA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Abdominal exploration
Access Route: Transanal.
Study population Pigs (species = Yorkshire)
Sample Size: 6
Weight(kg):25-30
Gender: NR
Pre-op prep Diet: Fasted 48h
Anaesthesia/sedation: Preanasthesia: Tiletamine HCl C zolazepam HCl 4.4 mg/kg (IV), atropine sulfate 0.4 mg/kg IV, & xylazine 2.2 mg/kg IV. General anesthesia: 1-3% isoflurane on semiclosed inhalation circuit after endotracheal intubation
Antibiotic: Cefazolin 1g IV
Post-op follow-up
Survival (days): 14
Diet/Meds: Regular diet immediately after recovery from general anesthesia. Antibiotic = Cephalexin (3 days, 250mg oral 2x day).
Observations: Close observational follow-up over following 14 days.
Endoscopy: NR
Necropsy: POD14 (euthanised).
Instrumentation
GIF 140; GIF 2T100; Reusable needle knives; Reusable Veress insufflation needles; ; Reusable endoscopic forceps & snares
Surgical procedure Transluminal access Site access & prep: Double-channel endoscope advanced 15-20cm from anus. Multiple tap-water enemas administered until distal colon cleared of all particulate fecal matter. Suspension of cefazolin 1g in 500mL sterile water instilled through endoscope & aspirated after 10min & rectum lavaged with 60mL 10% povidone-iodine sol. External anal & gluteal surfaces scrubbed with 10% povidone-iodine. Incision site: Internal indentation from abdominal palpation used to localize anterior colonic wall Incision method: 2-3mm colonic incision made using needle knife with brief pulse of coagulation current (20W). Endoscope passed through incision over needle-knife cannula & into peritoneal cavity. In 4 pigs, colonic incision created using prototype incision & closure device. After advancing hand-activated device under endoscopic visualization to desired incision site, purse string suture deployed around planned incision site using an integrated dual ferrule mechanism. 20mm incision created via blade mechanism at tip of device. Veress needle placed in lower abdominal midline immediately after gaining endoscopic peritoneal access & used to create pneumoperitoneum to a pressure of <15mm Hg.
Intervention External transillumination confirmed tip position within abdominal cavity. Rapid ID of stomach, liver, gallbladder, spleen, small bowel, colon, peritoneal surfaces & pelvic organs. Systematic evaluation performed - segmental liver anatomy assessed (left lateral, left medial, right medial, right lateral, caudate lobes). Moving from right upper quadrant to left upper quadrant, gallbladder & spleen exposed & evaluated. Additional exposure of gallbladder & cystic duct achieved using blunt-tip probing & retraction of overlying liver lobes with 2 forceps. Positional changes, including reverse Trendelenburg position & right & left lateral rotation used to gain additional exposure of upperabdominal structures. Using 2 forceps, segments of small bowel & associated mesentery traced for several cm along their length. With endoscope in a retroflexed position & animal in Trendelenburg position right & left lower quadrants carefully examined. Retraction & viscerotomy closure Endoscopic clips sequentially deployed along incision from superior margin to inferior margin until complete closure achieved (1 pig); Endoloop closure of incision required use of forceps to pull margins of incision into open endoloop before subsequent closure & approximation of incision margins (1pig); Prototype device used (4 pigs) in which a titanium knot was deployed to secure previously placed purse string suture & close incision.
Procedural Success/Complications Incision: Easily performed in 6/6 pigs without immediate complications. Balloon dilation of colotomy not required, because incision easily dilated.
Visualisation: Upper abdomen: Excellent visualization of most structures without need for retroflexion. Most superior & posterior aspects of upper abdomen: Limited retraction in sagital plane made visualization difficult. Dome of liver, hilum of liver, lesser curvature of stomach & right & left lower quadrants: Restricted field of view.
Complications Bleeding: 0/6
Organ Injury: 0/6
Infection Related Complications: Adhesions: 4/6 pigs: incision-related salpingocolonic & colovesicular adhesions. No adhesions 1/4 pigs where prototype closure device used & 1 pig closed with endoscopic clips. Incision-related adhesions & inflammatory changes restricted to colonic closure site in 6/6 pigs (inflammatory infiltrates, microscopic abscesses, microscopic, mucosal ulcerations, & serositis) seen on histopathologic exam.
Infection/ peritonitis/ abscesses/inflammation: 0/6 (necropsy/histopathologic exam).
Ulceration: 0/6 (at colonic incision sites - necropsy).
Recovery & survival Number survived: 6/6
General observations: Close observational follow-up over following 14 days did not reveal any clinically apparent ill effects.
Appetite & weight gain: All 6 pigs tolerated a regular diet within several hours after recovering from general anesthesia & gained 1-3 kg.
Wound Healing: At necropsy colonic incision sites all appeared well healed.
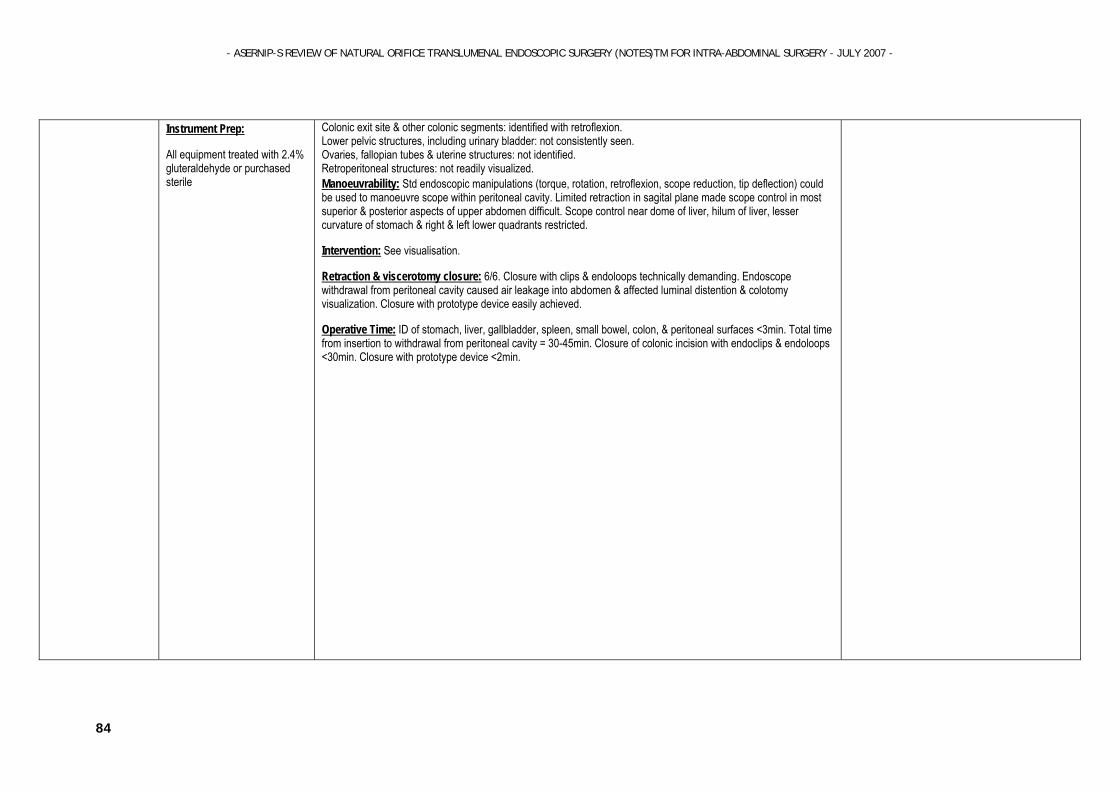
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
84
Instrument Prep:
All equipment treated with 2.4% gluteraldehyde or purchased sterile
Colonic exit site & other colonic segments: identified with retroflexion. Lower pelvic structures, including urinary bladder: not consistently seen. Ovaries, fallopian tubes & uterine structures: not identified. Retroperitoneal structures: not readily visualized. Manoeuvrability: Std endoscopic manipulations (torque, rotation, retroflexion, scope reduction, tip deflection) could be used to manoeuvre scope within peritoneal cavity. Limited retraction in sagital plane made scope control in most superior & posterior aspects of upper abdomen difficult. Scope control near dome of liver, hilum of liver, lesser curvature of stomach & right & left lower quadrants restricted.
Intervention: See visualisation.
Retraction & viscerotomy closure: 6/6. Closure with clips & endoloops technically demanding. Endoscope withdrawal from peritoneal cavity caused air leakage into abdomen & affected luminal distention & colotomy visualization. Closure with prototype device easily achieved.
Operative Time: ID of stomach, liver, gallbladder, spleen, small bowel, colon, & peritoneal surfaces <3min. Total time from insertion to withdrawal from peritoneal cavity = 30-45min. Closure of colonic incision with endoclips & endoloops <30min. Closure with prototype device <2min.
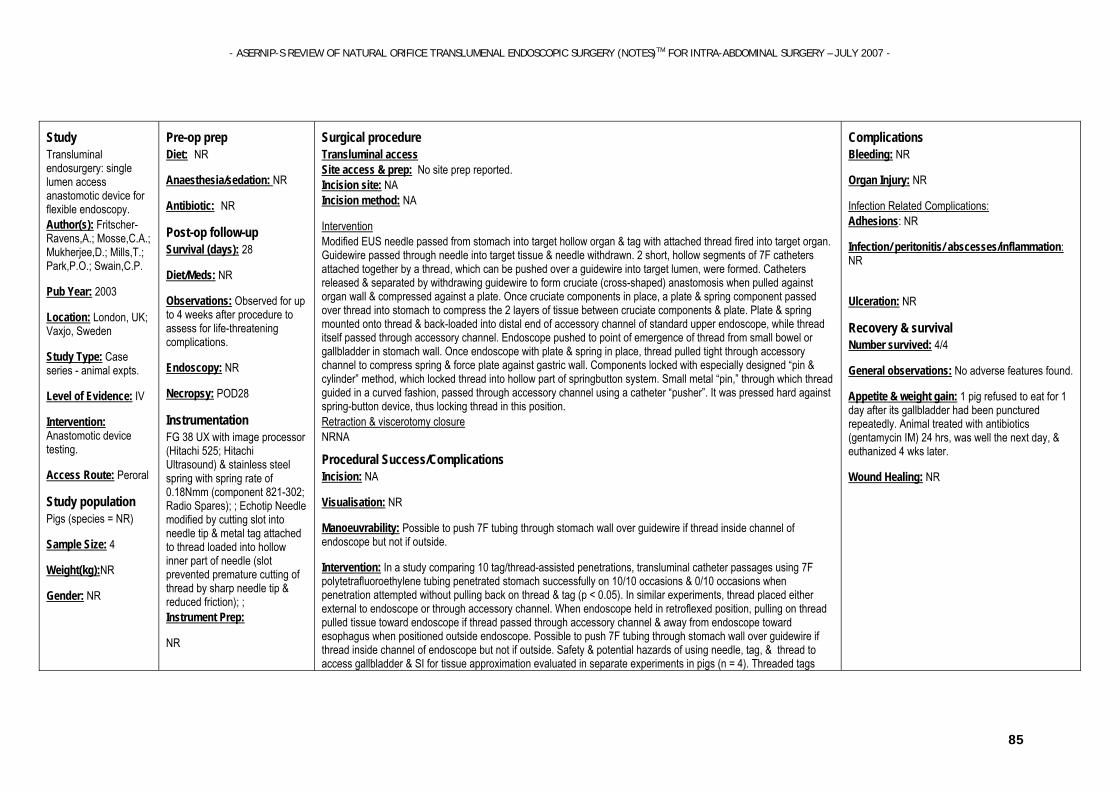
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
85
Study Transluminal endosurgery: single lumen access anastomotic device for flexible endoscopy. Author(s): Fritscher-Ravens,A.; Mosse,C.A.; Mukherjee,D.; Mills,T.; Park,P.O.; Swain,C.P.
Pub Year: 2003
Location: London, UK; Vaxjo, Sweden
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Anastomotic device testing.
Access Route: Peroral
Study population Pigs (species = NR)
Sample Size: 4
Weight(kg):NR
Gender: NR
Pre-op prep Diet: NR
Anaesthesia/sedation: NR
Antibiotic: NR
Post-op follow-up
Survival (days): 28
Diet/Meds: NR
Observations: Observed for up to 4 weeks after procedure to assess for life-threatening complications.
Endoscopy: NR
Necropsy: POD28
Instrumentation
FG 38 UX with image processor (Hitachi 525; Hitachi Ultrasound) & stainless steel spring with spring rate of 0.18Nmm (component 821-302; Radio Spares); ; Echotip Needle modified by cutting slot into needle tip & metal tag attached to thread loaded into hollow inner part of needle (slot prevented premature cutting of thread by sharp needle tip & reduced friction); ; Instrument Prep:
NR
Surgical procedure Transluminal access Site access & prep: No site prep reported. Incision site: NA Incision method: NA
Intervention Modified EUS needle passed from stomach into target hollow organ & tag with attached thread fired into target organ. Guidewire passed through needle into target tissue & needle withdrawn. 2 short, hollow segments of 7F catheters attached together by a thread, which can be pushed over a guidewire into target lumen, were formed. Catheters released & separated by withdrawing guidewire to form cruciate (cross-shaped) anastomosis when pulled against organ wall & compressed against a plate. Once cruciate components in place, a plate & spring component passed over thread into stomach to compress the 2 layers of tissue between cruciate components & plate. Plate & spring mounted onto thread & back-loaded into distal end of accessory channel of standard upper endoscope, while thread itself passed through accessory channel. Endoscope pushed to point of emergence of thread from small bowel or gallbladder in stomach wall. Once endoscope with plate & spring in place, thread pulled tight through accessory channel to compress spring & force plate against gastric wall. Components locked with especially designed “pin & cylinder” method, which locked thread into hollow part of springbutton system. Small metal “pin,” through which thread guided in a curved fashion, passed through accessory channel using a catheter “pusher”. It was pressed hard against spring-button device, thus locking thread in this position. Retraction & viscerotomy closure NRNA
Procedural Success/Complications Incision: NA
Visualisation: NR
Manoeuvrability: Possible to push 7F tubing through stomach wall over guidewire if thread inside channel of endoscope but not if outside.
Intervention: In a study comparing 10 tag/thread-assisted penetrations, transluminal catheter passages using 7F polytetrafluoroethylene tubing penetrated stomach successfully on 10/10 occasions & 0/10 occasions when penetration attempted without pulling back on thread & tag (p < 0.05). In similar experiments, thread placed either external to endoscope or through accessory channel. When endoscope held in retroflexed position, pulling on thread pulled tissue toward endoscope if thread passed through accessory channel & away from endoscope toward esophagus when positioned outside endoscope. Possible to push 7F tubing through stomach wall over guidewire if thread inside channel of endoscope but not if outside. Safety & potential hazards of using needle, tag, & thread to access gallbladder & SI for tissue approximation evaluated in separate experiments in pigs (n = 4). Threaded tags
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: NR
Ulceration: NR
Recovery & survival Number survived: 4/4
General observations: No adverse features found.
Appetite & weight gain: 1 pig refused to eat for 1 day after its gallbladder had been punctured repeatedly. Animal treated with antibiotics (gentamycin IM) 24 hrs, was well the next day, & euthanized 4 wks later.
Wound Healing: NR

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
86
fired 61 times (small bowel 28, gallbladder 33).
Retraction & viscerotomy closure: NR
Operative Time: NR
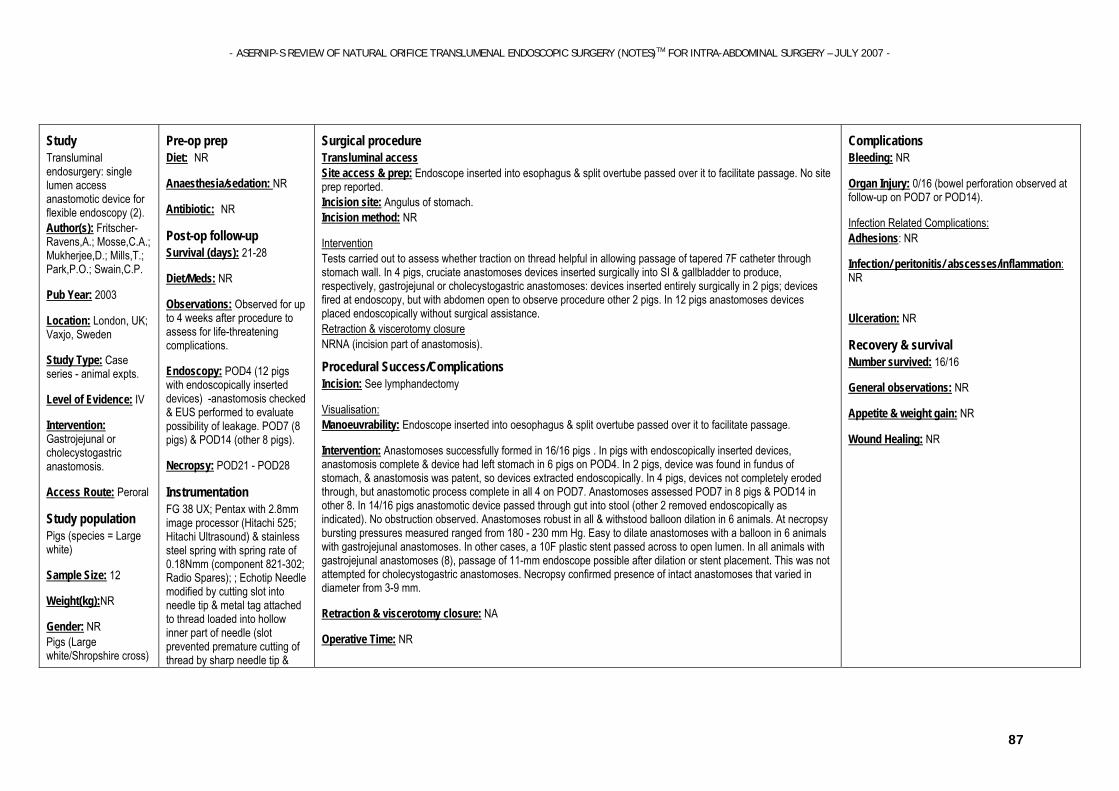
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
87
Study Transluminal endosurgery: single lumen access anastomotic device for flexible endoscopy (2). Author(s): Fritscher-Ravens,A.; Mosse,C.A.; Mukherjee,D.; Mills,T.; Park,P.O.; Swain,C.P.
Pub Year: 2003
Location: London, UK; Vaxjo, Sweden
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Gastrojejunal or cholecystogastric anastomosis.
Access Route: Peroral
Study population Pigs (species = Large white)
Sample Size: 12
Weight(kg):NR
Gender: NR Pigs (Large white/Shropshire cross)
Pre-op prep Diet: NR
Anaesthesia/sedation: NR
Antibiotic: NR
Post-op follow-up
Survival (days): 21-28
Diet/Meds: NR
Observations: Observed for up to 4 weeks after procedure to assess for life-threatening complications.
Endoscopy: POD4 (12 pigs with endoscopically inserted devices) -anastomosis checked & EUS performed to evaluate possibility of leakage. POD7 (8 pigs) & POD14 (other 8 pigs).
Necropsy: POD21 - POD28
Instrumentation
FG 38 UX; Pentax with 2.8mm image processor (Hitachi 525; Hitachi Ultrasound) & stainless steel spring with spring rate of 0.18Nmm (component 821-302; Radio Spares); ; Echotip Needle modified by cutting slot into needle tip & metal tag attached to thread loaded into hollow inner part of needle (slot prevented premature cutting of thread by sharp needle tip &
Surgical procedure Transluminal access Site access & prep: Endoscope inserted into esophagus & split overtube passed over it to facilitate passage. No site prep reported. Incision site: Angulus of stomach. Incision method: NR
Intervention Tests carried out to assess whether traction on thread helpful in allowing passage of tapered 7F catheter through stomach wall. In 4 pigs, cruciate anastomoses devices inserted surgically into SI & gallbladder to produce, respectively, gastrojejunal or cholecystogastric anastomoses: devices inserted entirely surgically in 2 pigs; devices fired at endoscopy, but with abdomen open to observe procedure other 2 pigs. In 12 pigs anastomoses devices placed endoscopically without surgical assistance. Retraction & viscerotomy closure NRNA (incision part of anastomosis).
Procedural Success/Complications Incision: See lymphandectomy
Visualisation: Manoeuvrability: Endoscope inserted into oesophagus & split overtube passed over it to facilitate passage.
Intervention: Anastomoses successfully formed in 16/16 pigs . In pigs with endoscopically inserted devices, anastomosis complete & device had left stomach in 6 pigs on POD4. In 2 pigs, device was found in fundus of stomach, & anastomosis was patent, so devices extracted endoscopically. In 4 pigs, devices not completely eroded through, but anastomotic process complete in all 4 on POD7. Anastomoses assessed POD7 in 8 pigs & POD14 in other 8. In 14/16 pigs anastomotic device passed through gut into stool (other 2 removed endoscopically as indicated). No obstruction observed. Anastomoses robust in all & withstood balloon dilation in 6 animals. At necropsy bursting pressures measured ranged from 180 - 230 mm Hg. Easy to dilate anastomoses with a balloon in 6 animals with gastrojejunal anastomoses. In other cases, a 10F plastic stent passed across to open lumen. In all animals with gastrojejunal anastomoses (8), passage of 11-mm endoscope possible after dilation or stent placement. This was not attempted for cholecystogastric anastomoses. Necropsy confirmed presence of intact anastomoses that varied in diameter from 3-9 mm.
Retraction & viscerotomy closure: NA
Operative Time: NR
Complications Bleeding: NR
Organ Injury: 0/16 (bowel perforation observed at follow-up on POD7 or POD14).
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: NR
Ulceration: NR
Recovery & survival Number survived: 16/16
General observations: NR
Appetite & weight gain: NR
Wound Healing: NR

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
88
Weight = NR Sample size = 4 Gender = NR
reduced friction); Split overtube (KeyMed); Instrument Prep:
NR
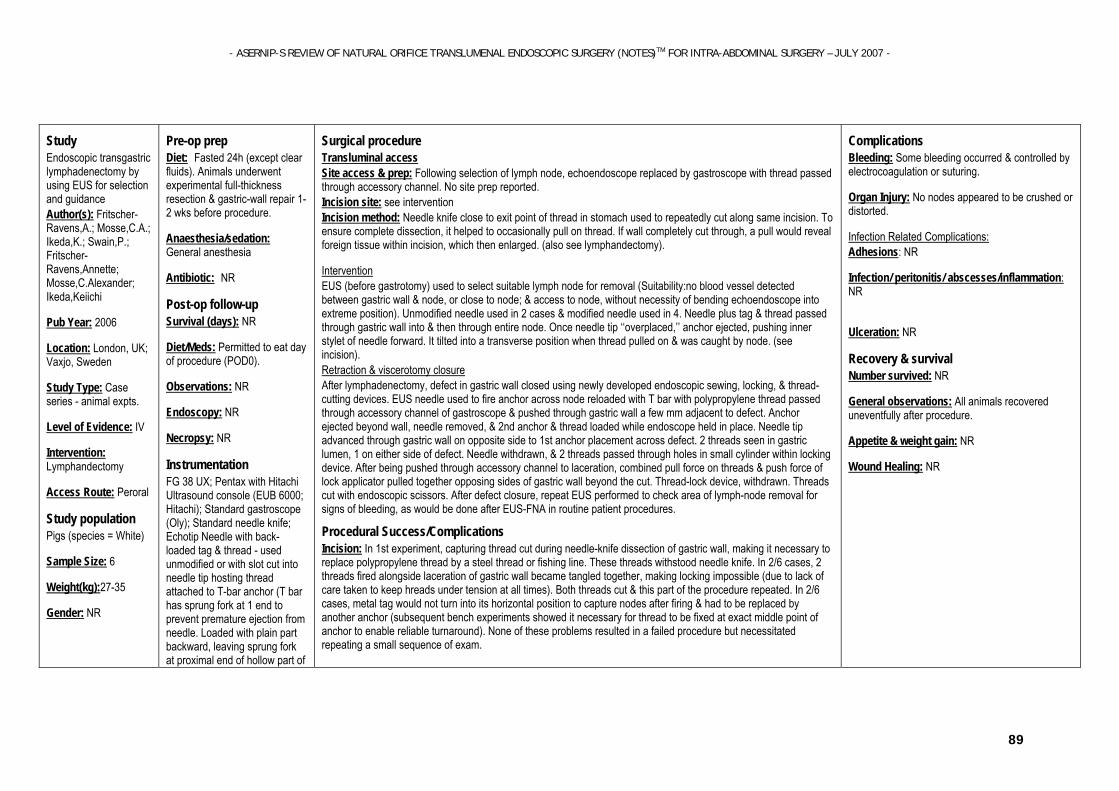
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
89
Study Endoscopic transgastric lymphadenectomy by using EUS for selection and guidance Author(s): Fritscher-Ravens,A.; Mosse,C.A.; Ikeda,K.; Swain,P.; Fritscher-Ravens,Annette; Mosse,C.Alexander; Ikeda,Keiichi
Pub Year: 2006
Location: London, UK; Vaxjo, Sweden
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Lymphandectomy
Access Route: Peroral
Study population Pigs (species = White)
Sample Size: 6
Weight(kg):27-35
Gender: NR
Pre-op prep Diet: Fasted 24h (except clear fluids). Animals underwent experimental full-thickness resection & gastric-wall repair 1-2 wks before procedure.
Anaesthesia/sedation: General anesthesia
Antibiotic: NR
Post-op follow-up
Survival (days): NR
Diet/Meds: Permitted to eat day of procedure (POD0).
Observations: NR
Endoscopy: NR
Necropsy: NR
Instrumentation
FG 38 UX; Pentax with Hitachi Ultrasound console (EUB 6000; Hitachi); Standard gastroscope (Oly); Standard needle knife; Echotip Needle with back-loaded tag & thread - used unmodified or with slot cut into needle tip hosting thread attached to T-bar anchor (T bar has sprung fork at 1 end to prevent premature ejection from needle. Loaded with plain part backward, leaving sprung fork at proximal end of hollow part of
Surgical procedure Transluminal access Site access & prep: Following selection of lymph node, echoendoscope replaced by gastroscope with thread passed through accessory channel. No site prep reported. Incision site: see intervention Incision method: Needle knife close to exit point of thread in stomach used to repeatedly cut along same incision. To ensure complete dissection, it helped to occasionally pull on thread. If wall completely cut through, a pull would reveal foreign tissue within incision, which then enlarged. (also see lymphandectomy).
Intervention EUS (before gastrotomy) used to select suitable lymph node for removal (Suitability:no blood vessel detected between gastric wall & node, or close to node; & access to node, without necessity of bending echoendoscope into extreme position). Unmodified needle used in 2 cases & modified needle used in 4. Needle plus tag & thread passed through gastric wall into & then through entire node. Once needle tip ‘‘overplaced,’’ anchor ejected, pushing inner stylet of needle forward. It tilted into a transverse position when thread pulled on & was caught by node. (see incision). Retraction & viscerotomy closure After lymphadenectomy, defect in gastric wall closed using newly developed endoscopic sewing, locking, & thread-cutting devices. EUS needle used to fire anchor across node reloaded with T bar with polypropylene thread passed through accessory channel of gastroscope & pushed through gastric wall a few mm adjacent to defect. Anchor ejected beyond wall, needle removed, & 2nd anchor & thread loaded while endoscope held in place. Needle tip advanced through gastric wall on opposite side to 1st anchor placement across defect. 2 threads seen in gastric lumen, 1 on either side of defect. Needle withdrawn, & 2 threads passed through holes in small cylinder within locking device. After being pushed through accessory channel to laceration, combined pull force on threads & push force of lock applicator pulled together opposing sides of gastric wall beyond the cut. Thread-lock device, withdrawn. Threads cut with endoscopic scissors. After defect closure, repeat EUS performed to check area of lymph-node removal for signs of bleeding, as would be done after EUS-FNA in routine patient procedures.
Procedural Success/Complications Incision: In 1st experiment, capturing thread cut during needle-knife dissection of gastric wall, making it necessary to replace polypropylene thread by a steel thread or fishing line. These threads withstood needle knife. In 2/6 cases, 2 threads fired alongside laceration of gastric wall became tangled together, making locking impossible (due to lack of care taken to keep hreads under tension at all times). Both threads cut & this part of the procedure repeated. In 2/6 cases, metal tag would not turn into its horizontal position to capture nodes after firing & had to be replaced by another anchor (subsequent bench experiments showed it necessary for thread to be fixed at exact middle point of anchor to enable reliable turnaround). None of these problems resulted in a failed procedure but necessitated repeating a small sequence of exam.
Complications Bleeding: Some bleeding occurred & controlled by electrocoagulation or suturing.
Organ Injury: No nodes appeared to be crushed or distorted.
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: NR
Ulceration: NR
Recovery & survival Number survived: NR
General observations: All animals recovered uneventfully after procedure.
Appetite & weight gain: NR
Wound Healing: NR
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
90
the needle to hold it securely within); ; thread = polypropylene or Steelthread (Ethicon Endosurgery) or Berkeley Fishing Line (Pure Fishing America) Instrument Prep:
NR
Visualisation: Lymph nodes ID with EUS & surrounding perigastric area checked for intervening vessels.
Manoeuvrability: NR
Intervention: Suitable nodes, measured 0.8-1.5cm (diameter) & hyperechoic or isoechoic. Although slippery nature of targets & thread alongside needle made puncture difficult (tip appeared rather blunt & nodes appeared very soft & compressible & would move away from tip), all nodes could be punctured by EUS needle. 2-4 attempts necessary to pass needle with anchor through selected node. In 1st 2 procedures, using unmodified needle, tag-holding thread led out of needle tip, hindering easy puncture of node. In last 4 procedures, using slotted needle, the thread led out through slot beyond needle tip & kept tip sharp enough to puncture through node without resistance.
Firing of metal anchor across node & ability to pull target node toward gastric wall using gentle traction on thread proved easy. Only targeting, puncturing, tagging & pulling node to gastric wall was performed successfully in 1st 4/6 pigs (focus of study). In remaining 2, complete sequence of examination, consisting of puncturing, tagging & removing target lymph node, with subsequent defect closure, successfully performed.
Retraction & viscerotomy closure: Depending on size of defect, process could be repeated with 2nd &/or more stitch pairs & locks. For removal of a single node, 1 set of stitches sufficient to close defect. All devices could be used through accessory channel of 2.8mm in diameter.
Operative Time: NR
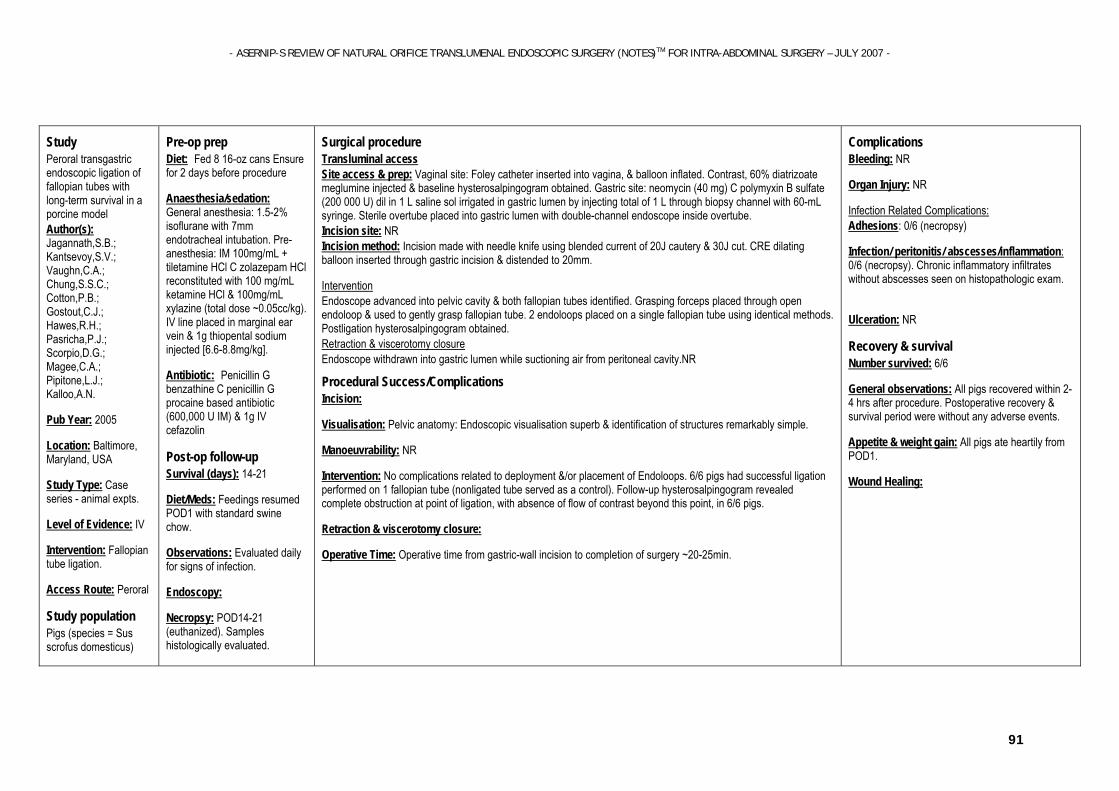
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
91
Study Peroral transgastric endoscopic ligation of fallopian tubes with long-term survival in a porcine model Author(s): Jagannath,S.B.; Kantsevoy,S.V.; Vaughn,C.A.; Chung,S.S.C.; Cotton,P.B.; Gostout,C.J.; Hawes,R.H.; Pasricha,P.J.; Scorpio,D.G.; Magee,C.A.; Pipitone,L.J.; Kalloo,A.N.
Pub Year: 2005
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Fallopian tube ligation.
Access Route: Peroral
Study population Pigs (species = Sus scrofus domesticus)
Pre-op prep Diet: Fed 8 16-oz cans Ensure for 2 days before procedure
Anaesthesia/sedation: General anesthesia: 1.5-2% isoflurane with 7mm endotracheal intubation. Pre-anesthesia: IM 100mg/mL + tiletamine HCl C zolazepam HCl reconstituted with 100 mg/mL ketamine HCl & 100mg/mL xylazine (total dose ~0.05cc/kg). IV line placed in marginal ear vein & 1g thiopental sodium injected [6.6-8.8mg/kg].
Antibiotic: Penicillin G benzathine C penicillin G procaine based antibiotic (600,000 U IM) & 1g IV cefazolin
Post-op follow-up
Survival (days): 14-21
Diet/Meds: Feedings resumed POD1 with standard swine chow.
Observations: Evaluated daily for signs of infection.
Endoscopy:
Necropsy: POD14-21 (euthanized). Samples histologically evaluated.
Surgical procedure Transluminal access Site access & prep: Vaginal site: Foley catheter inserted into vagina, & balloon inflated. Contrast, 60% diatrizoate meglumine injected & baseline hysterosalpingogram obtained. Gastric site: neomycin (40 mg) C polymyxin B sulfate (200 000 U) dil in 1 L saline sol irrigated in gastric lumen by injecting total of 1 L through biopsy channel with 60-mL syringe. Sterile overtube placed into gastric lumen with double-channel endoscope inside overtube. Incision site: NR Incision method: Incision made with needle knife using blended current of 20J cautery & 30J cut. CRE dilating balloon inserted through gastric incision & distended to 20mm.
Intervention Endoscope advanced into pelvic cavity & both fallopian tubes identified. Grasping forceps placed through open endoloop & used to gently grasp fallopian tube. 2 endoloops placed on a single fallopian tube using identical methods. Postligation hysterosalpingogram obtained. Retraction & viscerotomy closure Endoscope withdrawn into gastric lumen while suctioning air from peritoneal cavity.NR
Procedural Success/Complications Incision:
Visualisation: Pelvic anatomy: Endoscopic visualisation superb & identification of structures remarkably simple.
Manoeuvrability: NR
Intervention: No complications related to deployment &/or placement of Endoloops. 6/6 pigs had successful ligation performed on 1 fallopian tube (nonligated tube served as a control). Follow-up hysterosalpingogram revealed complete obstruction at point of ligation, with absence of flow of contrast beyond this point, in 6/6 pigs.
Retraction & viscerotomy closure:
Operative Time: Operative time from gastric-wall incision to completion of surgery ~20-25min.
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: 0/6 (necropsy)
Infection/ peritonitis/ abscesses/inflammation: 0/6 (necropsy). Chronic inflammatory infiltrates without abscesses seen on histopathologic exam.
Ulceration: NR
Recovery & survival Number survived: 6/6
General observations: All pigs recovered within 2-4 hrs after procedure. Postoperative recovery & survival period were without any adverse events.
Appetite & weight gain: All pigs ate heartily from POD1.
Wound Healing:

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
92
Sample Size: 6
Weight(kg):50
Gender: All female
Instrumentation
GIF-2T160; Triplelumen, 4mm, cutting-wire needle knife (WCMI) with blended current of 20J cautery & 30J cut (Valleylab SSE2L; TycoHealthcare); ; Sterile overtube (Oly); 16F Foley catheter with 30cc balloon (Rusch Inc); Contrast, 60% diatrizoate meglumine (Hypaque; Amersham); CRE dilating balloon (MEBS); Grasping forceps (FG-47L-1; Oly); Endoloop (Olympus Loop; Oly) Instrument Prep:
All equipment underwent high-level disinfection (Cidex) & gas sterilization with ethylene oxide.
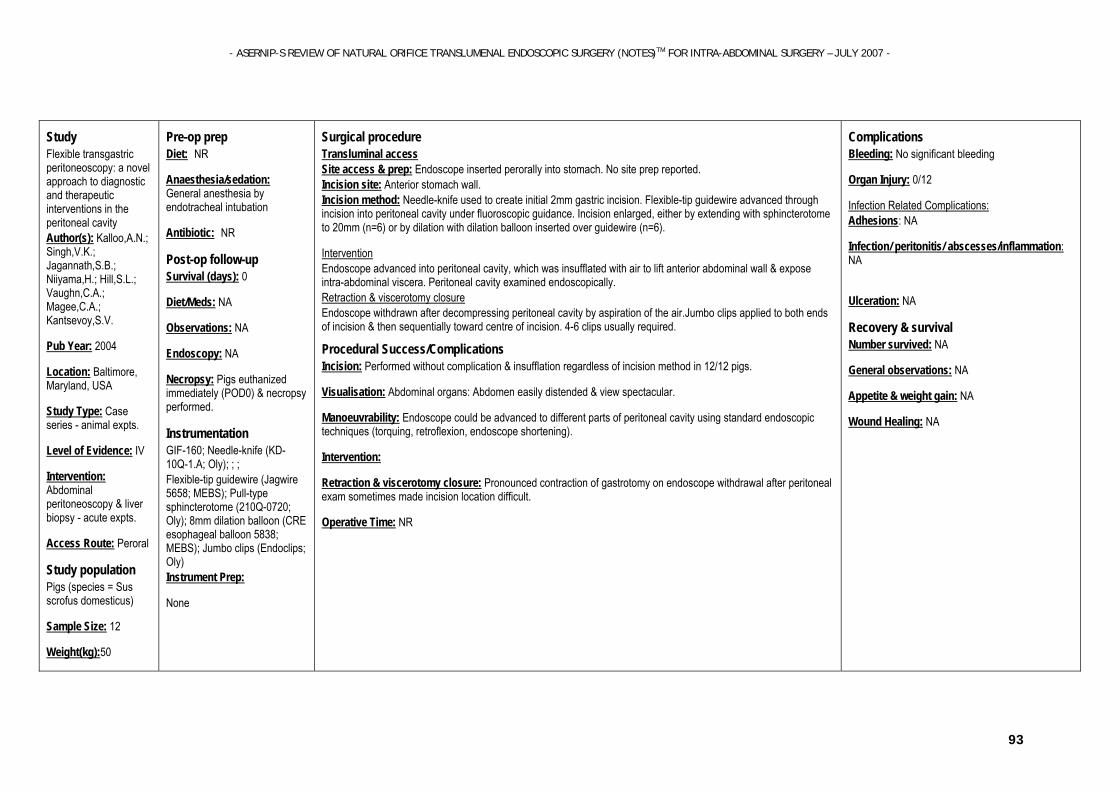
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
93
Study Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity Author(s): Kalloo,A.N.; Singh,V.K.; Jagannath,S.B.; Niiyama,H.; Hill,S.L.; Vaughn,C.A.; Magee,C.A.; Kantsevoy,S.V.
Pub Year: 2004
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Abdominal peritoneoscopy & liver biopsy - acute expts.
Access Route: Peroral
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 12
Weight(kg):50
Pre-op prep Diet: NR
Anaesthesia/sedation: General anesthesia by endotracheal intubation
Antibiotic: NR
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NA
Necropsy: Pigs euthanized immediately (POD0) & necropsy performed.
Instrumentation
GIF-160; Needle-knife (KD-10Q-1.A; Oly); ; ; Flexible-tip guidewire (Jagwire 5658; MEBS); Pull-type sphincterotome (210Q-0720; Oly); 8mm dilation balloon (CRE esophageal balloon 5838; MEBS); Jumbo clips (Endoclips; Oly) Instrument Prep:
None
Surgical procedure Transluminal access Site access & prep: Endoscope inserted perorally into stomach. No site prep reported. Incision site: Anterior stomach wall. Incision method: Needle-knife used to create initial 2mm gastric incision. Flexible-tip guidewire advanced through incision into peritoneal cavity under fluoroscopic guidance. Incision enlarged, either by extending with sphincterotome to 20mm (n=6) or by dilation with dilation balloon inserted over guidewire (n=6).
Intervention Endoscope advanced into peritoneal cavity, which was insufflated with air to lift anterior abdominal wall & expose intra-abdominal viscera. Peritoneal cavity examined endoscopically. Retraction & viscerotomy closure Endoscope withdrawn after decompressing peritoneal cavity by aspiration of the air.Jumbo clips applied to both ends of incision & then sequentially toward centre of incision. 4-6 clips usually required.
Procedural Success/Complications Incision: Performed without complication & insufflation regardless of incision method in 12/12 pigs.
Visualisation: Abdominal organs: Abdomen easily distended & view spectacular.
Manoeuvrability: Endoscope could be advanced to different parts of peritoneal cavity using standard endoscopic techniques (torquing, retroflexion, endoscope shortening).
Intervention:
Retraction & viscerotomy closure: Pronounced contraction of gastrotomy on endoscope withdrawal after peritoneal exam sometimes made incision location difficult.
Operative Time: NR
Complications Bleeding: No significant bleeding
Organ Injury: 0/12
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
94
Gender: NR
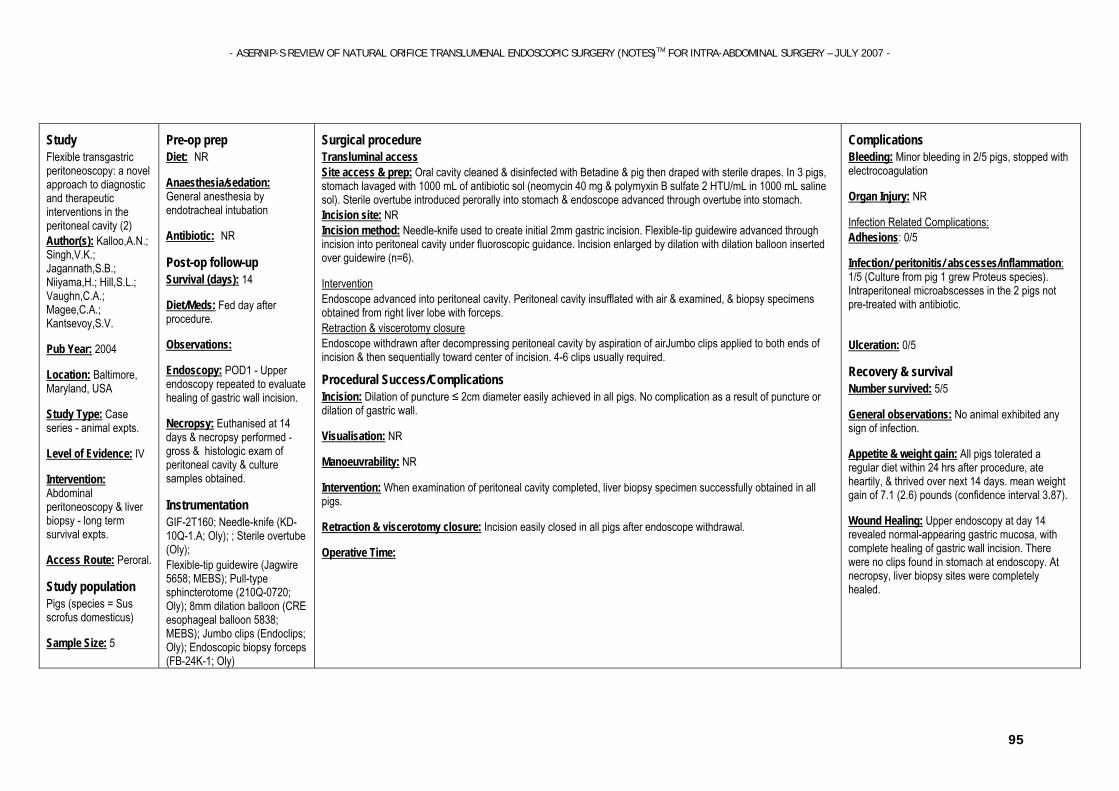
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
95
Study Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity (2) Author(s): Kalloo,A.N.; Singh,V.K.; Jagannath,S.B.; Niiyama,H.; Hill,S.L.; Vaughn,C.A.; Magee,C.A.; Kantsevoy,S.V.
Pub Year: 2004
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Abdominal peritoneoscopy & liver biopsy - long term survival expts.
Access Route: Peroral.
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 5
Pre-op prep Diet: NR
Anaesthesia/sedation: General anesthesia by endotracheal intubation
Antibiotic: NR
Post-op follow-up
Survival (days): 14
Diet/Meds: Fed day after procedure.
Observations:
Endoscopy: POD1 - Upper endoscopy repeated to evaluate healing of gastric wall incision.
Necropsy: Euthanised at 14 days & necropsy performed - gross & histologic exam of peritoneal cavity & culture samples obtained.
Instrumentation
GIF-2T160; Needle-knife (KD-10Q-1.A; Oly); ; Sterile overtube (Oly); Flexible-tip guidewire (Jagwire 5658; MEBS); Pull-type sphincterotome (210Q-0720; Oly); 8mm dilation balloon (CRE esophageal balloon 5838; MEBS); Jumbo clips (Endoclips; Oly); Endoscopic biopsy forceps (FB-24K-1; Oly)
Surgical procedure Transluminal access Site access & prep: Oral cavity cleaned & disinfected with Betadine & pig then draped with sterile drapes. In 3 pigs, stomach lavaged with 1000 mL of antibiotic sol (neomycin 40 mg & polymyxin B sulfate 2 HTU/mL in 1000 mL saline sol). Sterile overtube introduced perorally into stomach & endoscope advanced through overtube into stomach. Incision site: NR Incision method: Needle-knife used to create initial 2mm gastric incision. Flexible-tip guidewire advanced through incision into peritoneal cavity under fluoroscopic guidance. Incision enlarged by dilation with dilation balloon inserted over guidewire (n=6).
Intervention Endoscope advanced into peritoneal cavity. Peritoneal cavity insufflated with air & examined, & biopsy specimens obtained from right liver lobe with forceps. Retraction & viscerotomy closure Endoscope withdrawn after decompressing peritoneal cavity by aspiration of airJumbo clips applied to both ends of incision & then sequentially toward center of incision. 4-6 clips usually required.
Procedural Success/Complications Incision: Dilation of puncture ≤ 2cm diameter easily achieved in all pigs. No complication as a result of puncture or dilation of gastric wall.
Visualisation: NR
Manoeuvrability: NR
Intervention: When examination of peritoneal cavity completed, liver biopsy specimen successfully obtained in all pigs.
Retraction & viscerotomy closure: Incision easily closed in all pigs after endoscope withdrawal.
Operative Time:
Complications Bleeding: Minor bleeding in 2/5 pigs, stopped with electrocoagulation
Organ Injury: NR
Infection Related Complications: Adhesions: 0/5
Infection/ peritonitis/ abscesses/inflammation: 1/5 (Culture from pig 1 grew Proteus species). Intraperitoneal microabscesses in the 2 pigs not pre-treated with antibiotic.
Ulceration: 0/5
Recovery & survival Number survived: 5/5
General observations: No animal exhibited any sign of infection.
Appetite & weight gain: All pigs tolerated a regular diet within 24 hrs after procedure, ate heartily, & thrived over next 14 days. mean weight gain of 7.1 (2.6) pounds (confidence interval 3.87).
Wound Healing: Upper endoscopy at day 14 revealed normal-appearing gastric mucosa, with complete healing of gastric wall incision. There were no clips found in stomach at endoscopy. At necropsy, liver biopsy sites were completely healed.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
96
Weight(kg):50
Gender: NR
Instrument Prep:
All equipment underwent high-level disinfection followed by gas sterilization.
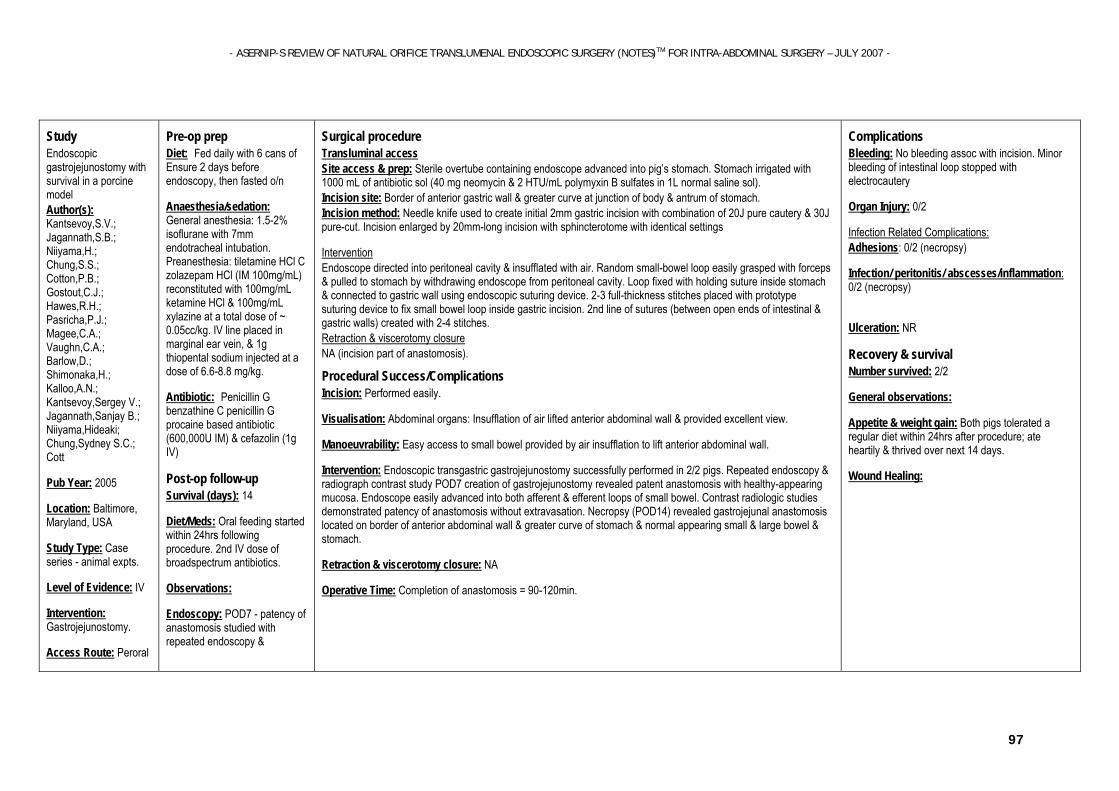
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
97
Study Endoscopic gastrojejunostomy with survival in a porcine model Author(s): Kantsevoy,S.V.; Jagannath,S.B.; Niiyama,H.; Chung,S.S.; Cotton,P.B.; Gostout,C.J.; Hawes,R.H.; Pasricha,P.J.; Magee,C.A.; Vaughn,C.A.; Barlow,D.; Shimonaka,H.; Kalloo,A.N.; Kantsevoy,Sergey V.; Jagannath,Sanjay B.; Niiyama,Hideaki; Chung,Sydney S.C.; Cott
Pub Year: 2005
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Gastrojejunostomy.
Access Route: Peroral
Pre-op prep Diet: Fed daily with 6 cans of Ensure 2 days before endoscopy, then fasted o/n
Anaesthesia/sedation: General anesthesia: 1.5-2% isoflurane with 7mm endotracheal intubation. Preanesthesia: tiletamine HCl C zolazepam HCl (IM 100mg/mL) reconstituted with 100mg/mL ketamine HCl & 100mg/mL xylazine at a total dose of ~ 0.05cc/kg. IV line placed in marginal ear vein, & 1g thiopental sodium injected at a dose of 6.6-8.8 mg/kg.
Antibiotic: Penicillin G benzathine C penicillin G procaine based antibiotic (600,000U IM) & cefazolin (1g IV)
Post-op follow-up
Survival (days): 14
Diet/Meds: Oral feeding started within 24hrs following procedure. 2nd IV dose of broadspectrum antibiotics.
Observations:
Endoscopy: POD7 - patency of anastomosis studied with repeated endoscopy &
Surgical procedure Transluminal access Site access & prep: Sterile overtube containing endoscope advanced into pig’s stomach. Stomach irrigated with 1000 mL of antibiotic sol (40 mg neomycin & 2 HTU/mL polymyxin B sulfates in 1L normal saline sol). Incision site: Border of anterior gastric wall & greater curve at junction of body & antrum of stomach. Incision method: Needle knife used to create initial 2mm gastric incision with combination of 20J pure cautery & 30J pure-cut. Incision enlarged by 20mm-long incision with sphincterotome with identical settings
Intervention Endoscope directed into peritoneal cavity & insufflated with air. Random small-bowel loop easily grasped with forceps & pulled to stomach by withdrawing endoscope from peritoneal cavity. Loop fixed with holding suture inside stomach & connected to gastric wall using endoscopic suturing device. 2-3 full-thickness stitches placed with prototype suturing device to fix small bowel loop inside gastric incision. 2nd line of sutures (between open ends of intestinal & gastric walls) created with 2-4 stitches. Retraction & viscerotomy closure NA (incision part of anastomosis).
Procedural Success/Complications Incision: Performed easily.
Visualisation: Abdominal organs: Insufflation of air lifted anterior abdominal wall & provided excellent view.
Manoeuvrability: Easy access to small bowel provided by air insufflation to lift anterior abdominal wall.
Intervention: Endoscopic transgastric gastrojejunostomy successfully performed in 2/2 pigs. Repeated endoscopy & radiograph contrast study POD7 creation of gastrojejunostomy revealed patent anastomosis with healthy-appearing mucosa. Endoscope easily advanced into both afferent & efferent loops of small bowel. Contrast radiologic studies demonstrated patency of anastomosis without extravasation. Necropsy (POD14) revealed gastrojejunal anastomosis located on border of anterior abdominal wall & greater curve of stomach & normal appearing small & large bowel & stomach.
Retraction & viscerotomy closure: NA
Operative Time: Completion of anastomosis = 90-120min.
Complications Bleeding: No bleeding assoc with incision. Minor bleeding of intestinal loop stopped with electrocautery
Organ Injury: 0/2
Infection Related Complications: Adhesions: 0/2 (necropsy)
Infection/ peritonitis/ abscesses/inflammation: 0/2 (necropsy)
Ulceration: NR
Recovery & survival Number survived: 2/2
General observations:
Appetite & weight gain: Both pigs tolerated a regular diet within 24hrs after procedure; ate heartily & thrived over next 14 days.
Wound Healing:

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
98
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 2
Weight(kg):50
Gender: NR
radiographic contrast studies.
Necropsy: POD14 (euthanized).
Instrumentation
GIF-160; Endoscopic needle knife (KD-10Q-1.A; Oly) with a combination of 20J pure cautery & 30J pure-cut (Valleylab SSE2L); ; Sterile overtube (Oly); Pull-type sphincterotome (210Q-0720; Oly); Endoscopic forceps (FG-47L-1; Oly); prototype endoscopic suturing device (Eagle Claw; Oly); radiographic contrast (60% Hypaque contrast; Amersham) Instrument Prep:
All equipment underwent high-level disinfection (Cidex OPA) followed by gas sterilization with ethylene oxide.
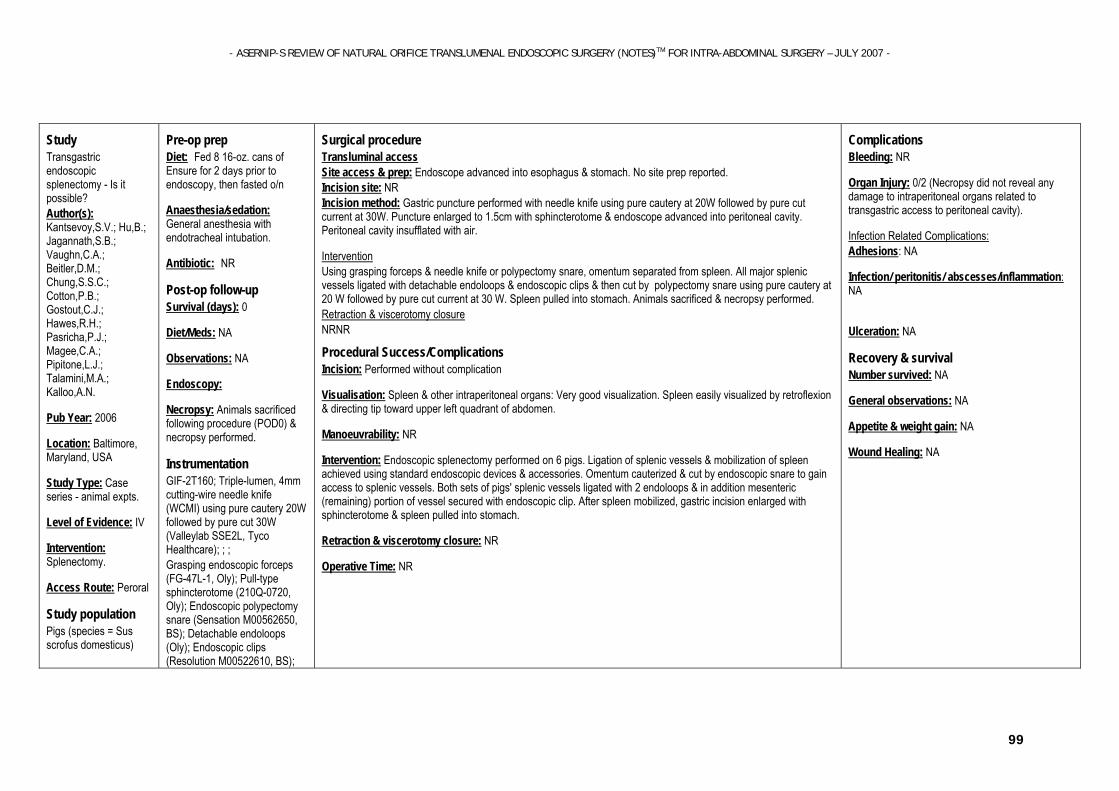
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
99
Study Transgastric endoscopic splenectomy - Is it possible? Author(s): Kantsevoy,S.V.; Hu,B.; Jagannath,S.B.; Vaughn,C.A.; Beitler,D.M.; Chung,S.S.C.; Cotton,P.B.; Gostout,C.J.; Hawes,R.H.; Pasricha,P.J.; Magee,C.A.; Pipitone,L.J.; Talamini,M.A.; Kalloo,A.N.
Pub Year: 2006
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Splenectomy.
Access Route: Peroral
Study population Pigs (species = Sus scrofus domesticus)
Pre-op prep Diet: Fed 8 16-oz. cans of Ensure for 2 days prior to endoscopy, then fasted o/n
Anaesthesia/sedation: General anesthesia with endotracheal intubation.
Antibiotic: NR
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy:
Necropsy: Animals sacrificed following procedure (POD0) & necropsy performed.
Instrumentation
GIF-2T160; Triple-lumen, 4mm cutting-wire needle knife (WCMI) using pure cautery 20W followed by pure cut 30W (Valleylab SSE2L, Tyco Healthcare); ; ; Grasping endoscopic forceps (FG-47L-1, Oly); Pull-type sphincterotome (210Q-0720, Oly); Endoscopic polypectomy snare (Sensation M00562650, BS); Detachable endoloops (Oly); Endoscopic clips (Resolution M00522610, BS);
Surgical procedure Transluminal access Site access & prep: Endoscope advanced into esophagus & stomach. No site prep reported. Incision site: NR Incision method: Gastric puncture performed with needle knife using pure cautery at 20W followed by pure cut current at 30W. Puncture enlarged to 1.5cm with sphincterotome & endoscope advanced into peritoneal cavity. Peritoneal cavity insufflated with air.
Intervention Using grasping forceps & needle knife or polypectomy snare, omentum separated from spleen. All major splenic vessels ligated with detachable endoloops & endoscopic clips & then cut by polypectomy snare using pure cautery at 20 W followed by pure cut current at 30 W. Spleen pulled into stomach. Animals sacrificed & necropsy performed. Retraction & viscerotomy closure NRNR
Procedural Success/Complications Incision: Performed without complication
Visualisation: Spleen & other intraperitoneal organs: Very good visualization. Spleen easily visualized by retroflexion & directing tip toward upper left quadrant of abdomen.
Manoeuvrability: NR
Intervention: Endoscopic splenectomy performed on 6 pigs. Ligation of splenic vessels & mobilization of spleen achieved using standard endoscopic devices & accessories. Omentum cauterized & cut by endoscopic snare to gain access to splenic vessels. Both sets of pigs' splenic vessels ligated with 2 endoloops & in addition mesenteric (remaining) portion of vessel secured with endoscopic clip. After spleen mobilized, gastric incision enlarged with sphincterotome & spleen pulled into stomach.
Retraction & viscerotomy closure: NR
Operative Time: NR
Complications Bleeding: NR
Organ Injury: 0/2 (Necropsy did not reveal any damage to intraperitoneal organs related to transgastric access to peritoneal cavity).
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
100
Sample Size: 6
Weight(kg):50
Gender: NR
Endoscopic polypectomy snare (Sensatio Instrument Prep:
NR
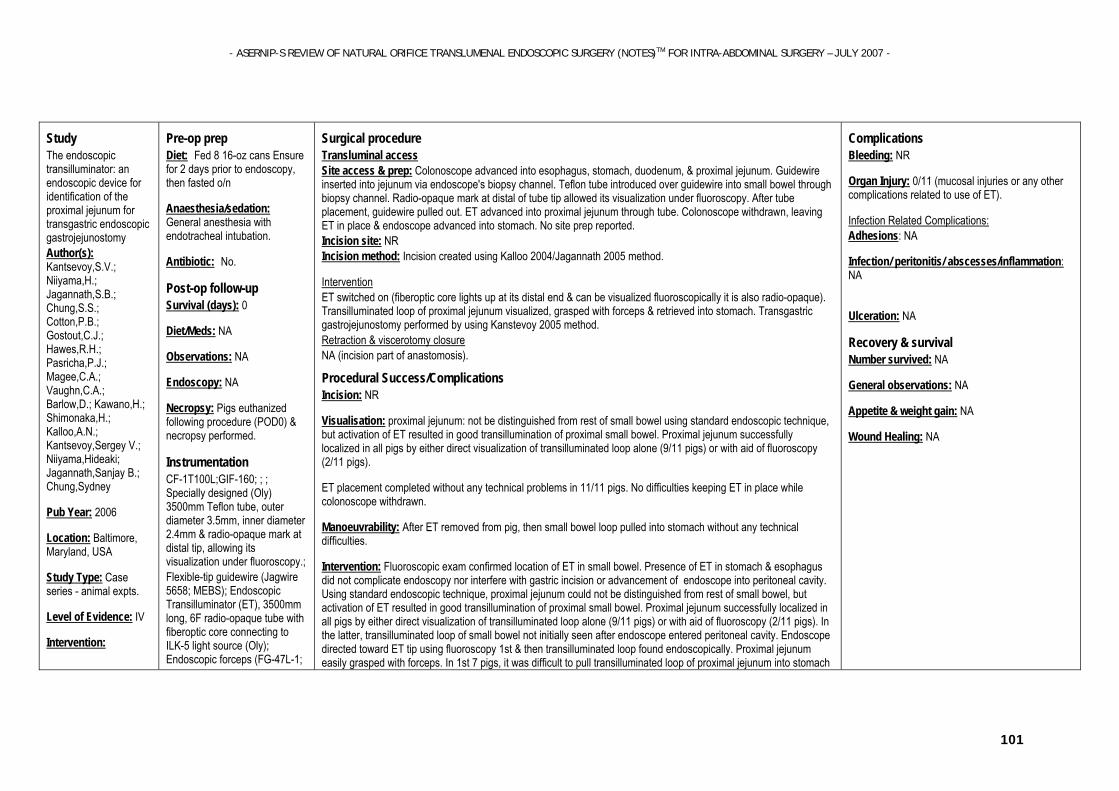
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
101
Study The endoscopic transilluminator: an endoscopic device for identification of the proximal jejunum for transgastric endoscopic gastrojejunostomy Author(s): Kantsevoy,S.V.; Niiyama,H.; Jagannath,S.B.; Chung,S.S.; Cotton,P.B.; Gostout,C.J.; Hawes,R.H.; Pasricha,P.J.; Magee,C.A.; Vaughn,C.A.; Barlow,D.; Kawano,H.; Shimonaka,H.; Kalloo,A.N.; Kantsevoy,Sergey V.; Niiyama,Hideaki; Jagannath,Sanjay B.; Chung,Sydney
Pub Year: 2006
Location: Baltimore, Maryland, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention:
Pre-op prep Diet: Fed 8 16-oz cans Ensure for 2 days prior to endoscopy, then fasted o/n
Anaesthesia/sedation: General anesthesia with endotracheal intubation.
Antibiotic: No.
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NA
Necropsy: Pigs euthanized following procedure (POD0) & necropsy performed.
Instrumentation
CF-1T100L;GIF-160; ; ; Specially designed (Oly) 3500mm Teflon tube, outer diameter 3.5mm, inner diameter 2.4mm & radio-opaque mark at distal tip, allowing its visualization under fluoroscopy.; Flexible-tip guidewire (Jagwire 5658; MEBS); Endoscopic Transilluminator (ET), 3500mm long, 6F radio-opaque tube with fiberoptic core connecting to ILK-5 light source (Oly); Endoscopic forceps (FG-47L-1;
Surgical procedure Transluminal access Site access & prep: Colonoscope advanced into esophagus, stomach, duodenum, & proximal jejunum. Guidewire inserted into jejunum via endoscope's biopsy channel. Teflon tube introduced over guidewire into small bowel through biopsy channel. Radio-opaque mark at distal of tube tip allowed its visualization under fluoroscopy. After tube placement, guidewire pulled out. ET advanced into proximal jejunum through tube. Colonoscope withdrawn, leaving ET in place & endoscope advanced into stomach. No site prep reported. Incision site: NR Incision method: Incision created using Kalloo 2004/Jagannath 2005 method.
Intervention ET switched on (fiberoptic core lights up at its distal end & can be visualized fluoroscopically it is also radio-opaque). Transilluminated loop of proximal jejunum visualized, grasped with forceps & retrieved into stomach. Transgastric gastrojejunostomy performed by using Kanstevoy 2005 method. Retraction & viscerotomy closure NA (incision part of anastomosis).
Procedural Success/Complications Incision: NR
Visualisation: proximal jejunum: not be distinguished from rest of small bowel using standard endoscopic technique, but activation of ET resulted in good transillumination of proximal small bowel. Proximal jejunum successfully localized in all pigs by either direct visualization of transilluminated loop alone (9/11 pigs) or with aid of fluoroscopy (2/11 pigs).
ET placement completed without any technical problems in 11/11 pigs. No difficulties keeping ET in place while colonoscope withdrawn.
Manoeuvrability: After ET removed from pig, then small bowel loop pulled into stomach without any technical difficulties.
Intervention: Fluoroscopic exam confirmed location of ET in small bowel. Presence of ET in stomach & esophagus did not complicate endoscopy nor interfere with gastric incision or advancement of endoscope into peritoneal cavity. Using standard endoscopic technique, proximal jejunum could not be distinguished from rest of small bowel, but activation of ET resulted in good transillumination of proximal small bowel. Proximal jejunum successfully localized in all pigs by either direct visualization of transilluminated loop alone (9/11 pigs) or with aid of fluoroscopy (2/11 pigs). In the latter, transilluminated loop of small bowel not initially seen after endoscope entered peritoneal cavity. Endoscope directed toward ET tip using fluoroscopy 1st & then transilluminated loop found endoscopically. Proximal jejunum easily grasped with forceps. In 1st 7 pigs, it was difficult to pull transilluminated loop of proximal jejunum into stomach
Complications Bleeding: NR
Organ Injury: 0/11 (mucosal injuries or any other complications related to use of ET).
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA
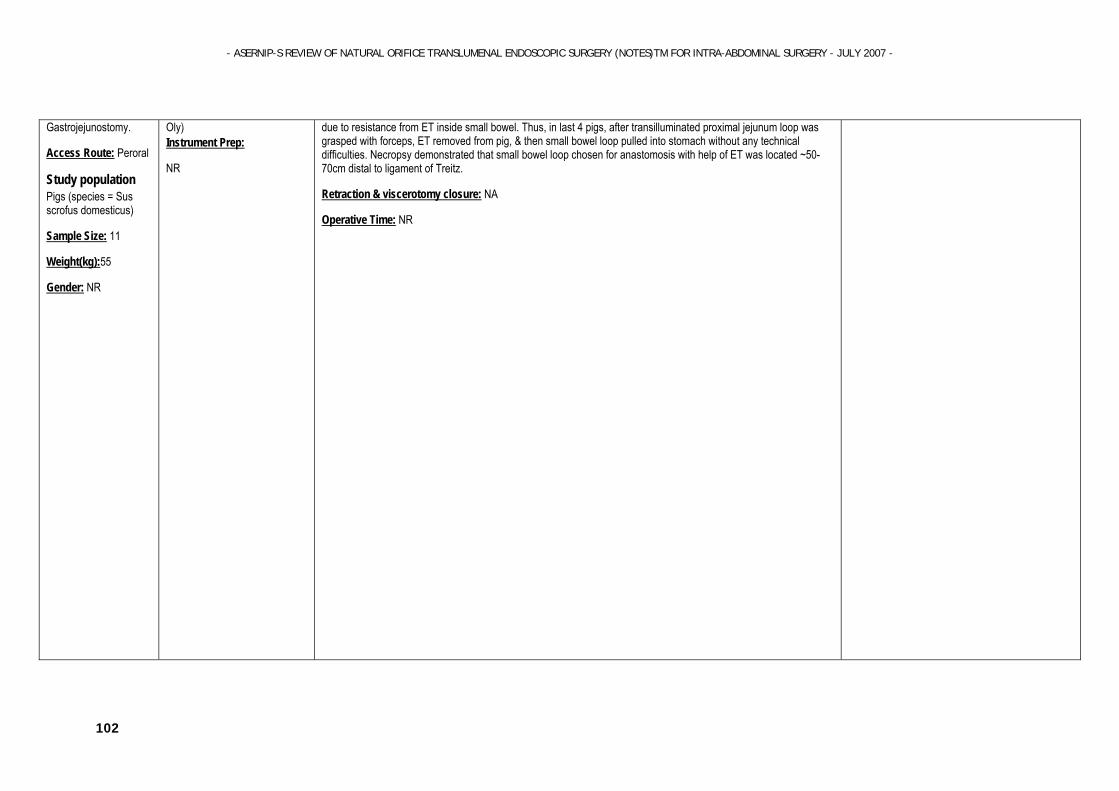
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
102
Gastrojejunostomy.
Access Route: Peroral
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 11
Weight(kg):55
Gender: NR
Oly) Instrument Prep:
NR
due to resistance from ET inside small bowel. Thus, in last 4 pigs, after transilluminated proximal jejunum loop was grasped with forceps, ET removed from pig, & then small bowel loop pulled into stomach without any technical difficulties. Necropsy demonstrated that small bowel loop chosen for anastomosis with help of ET was located ~50-70cm distal to ligament of Treitz.
Retraction & viscerotomy closure: NA
Operative Time: NR
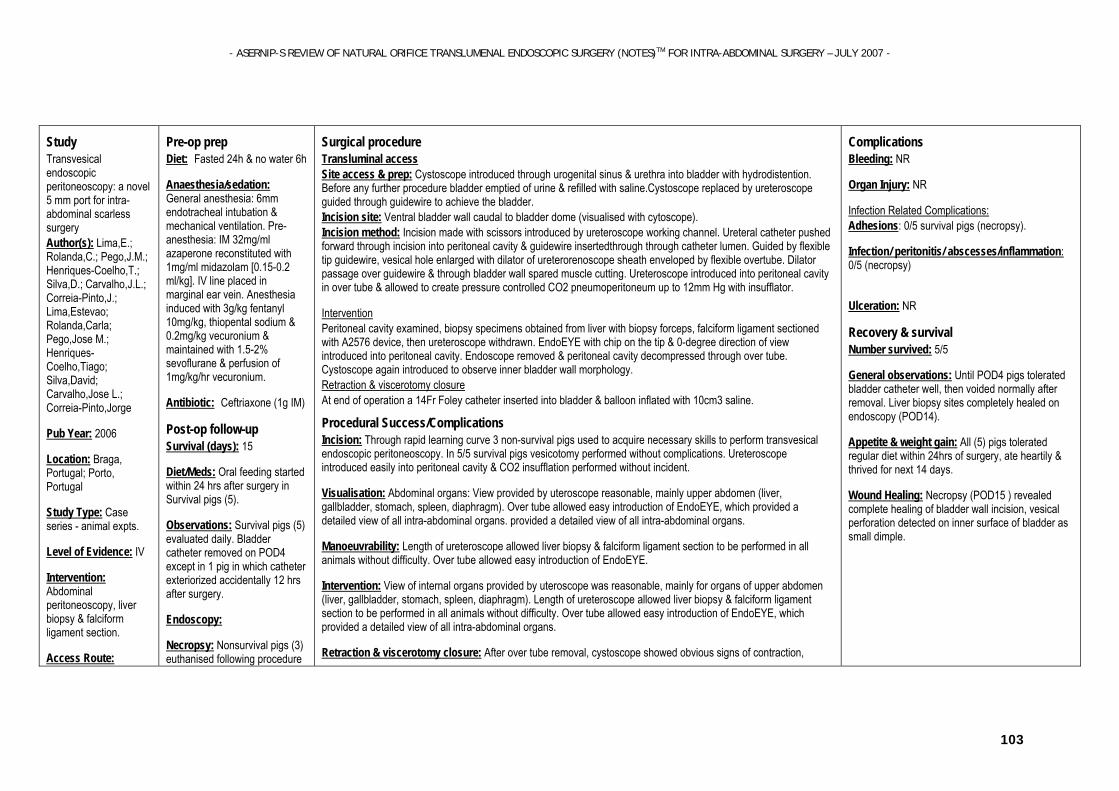
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
103
Study Transvesical endoscopic peritoneoscopy: a novel 5 mm port for intra-abdominal scarless surgery Author(s): Lima,E.; Rolanda,C.; Pego,J.M.; Henriques-Coelho,T.; Silva,D.; Carvalho,J.L.; Correia-Pinto,J.; Lima,Estevao; Rolanda,Carla; Pego,Jose M.; Henriques-Coelho,Tiago; Silva,David; Carvalho,Jose L.; Correia-Pinto,Jorge
Pub Year: 2006
Location: Braga, Portugal; Porto, Portugal
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Abdominal peritoneoscopy, liver biopsy & falciform ligament section.
Access Route:
Pre-op prep Diet: Fasted 24h & no water 6h
Anaesthesia/sedation: General anesthesia: 6mm endotracheal intubation & mechanical ventilation. Pre-anesthesia: IM 32mg/ml azaperone reconstituted with 1mg/ml midazolam [0.15-0.2 ml/kg]. IV line placed in marginal ear vein. Anesthesia induced with 3g/kg fentanyl 10mg/kg, thiopental sodium & 0.2mg/kg vecuronium & maintained with 1.5-2% sevoflurane & perfusion of 1mg/kg/hr vecuronium.
Antibiotic: Ceftriaxone (1g IM)
Post-op follow-up
Survival (days): 15
Diet/Meds: Oral feeding started within 24 hrs after surgery in Survival pigs (5).
Observations: Survival pigs (5) evaluated daily. Bladder catheter removed on POD4 except in 1 pig in which catheter exteriorized accidentally 12 hrs after surgery.
Endoscopy:
Necropsy: Nonsurvival pigs (3) euthanised following procedure
Surgical procedure Transluminal access Site access & prep: Cystoscope introduced through urogenital sinus & urethra into bladder with hydrodistention. Before any further procedure bladder emptied of urine & refilled with saline.Cystoscope replaced by ureteroscope guided through guidewire to achieve the bladder. Incision site: Ventral bladder wall caudal to bladder dome (visualised with cytoscope). Incision method: Incision made with scissors introduced by ureteroscope working channel. Ureteral catheter pushed forward through incision into peritoneal cavity & guidewire insertedthrough through catheter lumen. Guided by flexible tip guidewire, vesical hole enlarged with dilator of ureterorenoscope sheath enveloped by flexible overtube. Dilator passage over guidewire & through bladder wall spared muscle cutting. Ureteroscope introduced into peritoneal cavity in over tube & allowed to create pressure controlled CO2 pneumoperitoneum up to 12mm Hg with insufflator.
Intervention Peritoneal cavity examined, biopsy specimens obtained from liver with biopsy forceps, falciform ligament sectioned with A2576 device, then ureteroscope withdrawn. EndoEYE with chip on the tip & 0-degree direction of view introduced into peritoneal cavity. Endoscope removed & peritoneal cavity decompressed through over tube. Cystoscope again introduced to observe inner bladder wall morphology. Retraction & viscerotomy closure At end of operation a 14Fr Foley catheter inserted into bladder & balloon inflated with 10cm3 saline.
Procedural Success/Complications Incision: Through rapid learning curve 3 non-survival pigs used to acquire necessary skills to perform transvesical endoscopic peritoneoscopy. In 5/5 survival pigs vesicotomy performed without complications. Ureteroscope introduced easily into peritoneal cavity & CO2 insufflation performed without incident.
Visualisation: Abdominal organs: View provided by uteroscope reasonable, mainly upper abdomen (liver, gallbladder, stomach, spleen, diaphragm). Over tube allowed easy introduction of EndoEYE, which provided a detailed view of all intra-abdominal organs. provided a detailed view of all intra-abdominal organs.
Manoeuvrability: Length of ureteroscope allowed liver biopsy & falciform ligament section to be performed in all animals without difficulty. Over tube allowed easy introduction of EndoEYE.
Intervention: View of internal organs provided by uteroscope was reasonable, mainly for organs of upper abdomen (liver, gallbladder, stomach, spleen, diaphragm). Length of ureteroscope allowed liver biopsy & falciform ligament section to be performed in all animals without difficulty. Over tube allowed easy introduction of EndoEYE, which provided a detailed view of all intra-abdominal organs.
Retraction & viscerotomy closure: After over tube removal, cystoscope showed obvious signs of contraction,
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: 0/5 survival pigs (necropsy).
Infection/ peritonitis/ abscesses/inflammation: 0/5 (necropsy)
Ulceration: NR
Recovery & survival Number survived: 5/5
General observations: Until POD4 pigs tolerated bladder catheter well, then voided normally after removal. Liver biopsy sites completely healed on endoscopy (POD14).
Appetite & weight gain: All (5) pigs tolerated regular diet within 24hrs of surgery, ate heartily & thrived for next 14 days.
Wound Healing: Necropsy (POD15 ) revealed complete healing of bladder wall incision, vesical perforation detected on inner surface of bladder as small dimple.
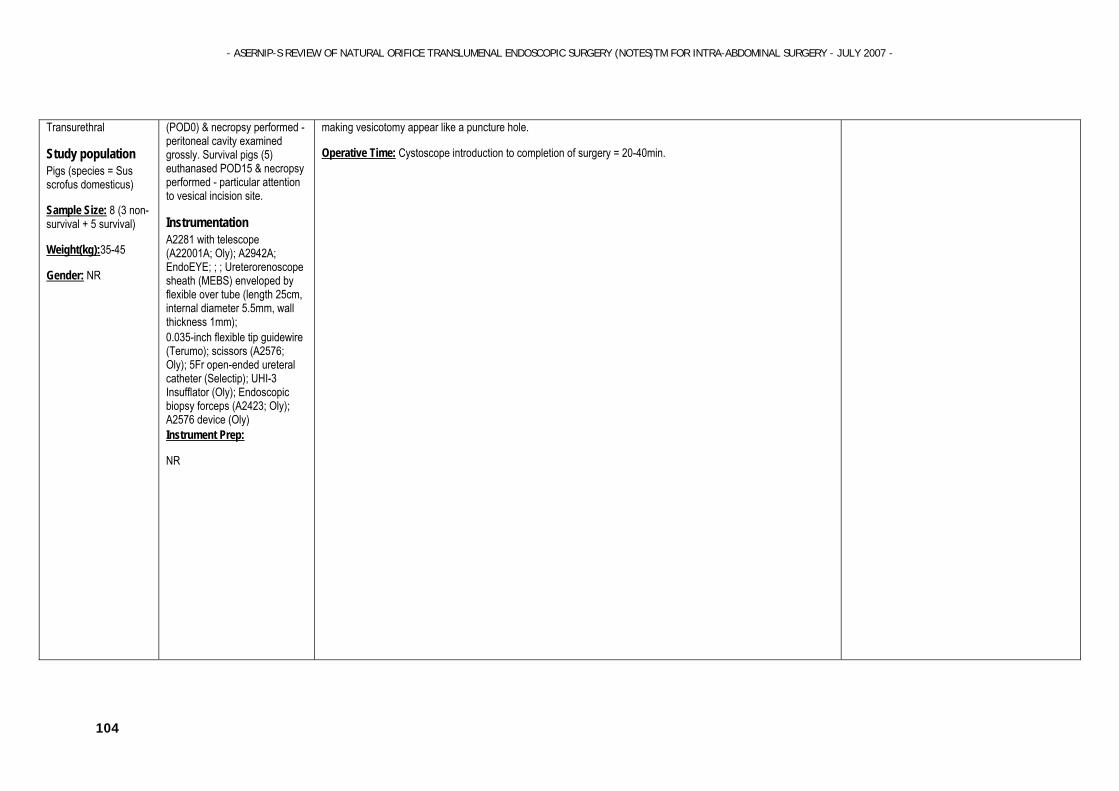
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
104
Transurethral
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 8 (3 non-survival + 5 survival)
Weight(kg):35-45
Gender: NR
(POD0) & necropsy performed - peritoneal cavity examined grossly. Survival pigs (5) euthanased POD15 & necropsy performed - particular attention to vesical incision site.
Instrumentation
A2281 with telescope (A22001A; Oly); A2942A; EndoEYE; ; ; Ureterorenoscope sheath (MEBS) enveloped by flexible over tube (length 25cm, internal diameter 5.5mm, wall thickness 1mm); 0.035-inch flexible tip guidewire (Terumo); scissors (A2576; Oly); 5Fr open-ended ureteral catheter (Selectip); UHI-3 Insufflator (Oly); Endoscopic biopsy forceps (A2423; Oly); A2576 device (Oly) Instrument Prep:
NR
making vesicotomy appear like a puncture hole.
Operative Time: Cystoscope introduction to completion of surgery = 20-40min.
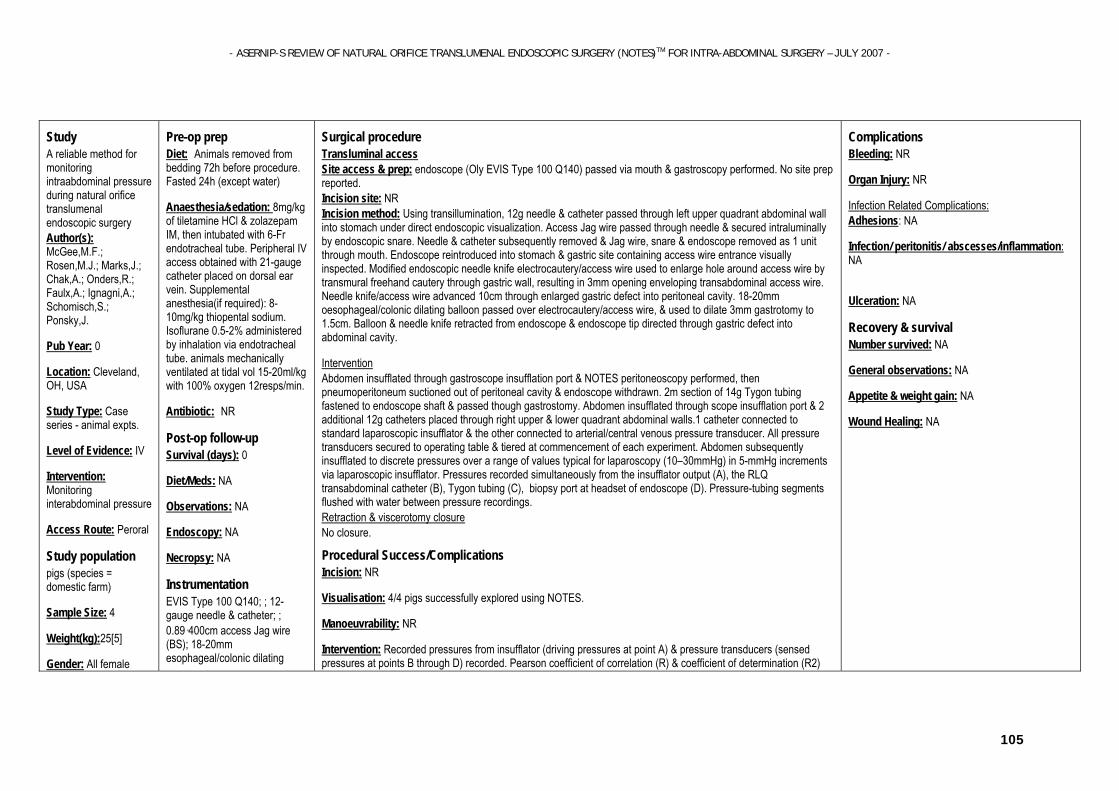
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
105
Study A reliable method for monitoring intraabdominal pressure during natural orifice translumenal endoscopic surgery Author(s): McGee,M.F.; Rosen,M.J.; Marks,J.; Chak,A.; Onders,R.; Faulx,A.; Ignagni,A.; Schomisch,S.; Ponsky,J.
Pub Year: 0
Location: Cleveland, OH, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Monitoring interabdominal pressure
Access Route: Peroral
Study population pigs (species = domestic farm)
Sample Size: 4
Weight(kg):25[5]
Gender: All female
Pre-op prep Diet: Animals removed from bedding 72h before procedure. Fasted 24h (except water)
Anaesthesia/sedation: 8mg/kg of tiletamine HCl & zolazepam IM, then intubated with 6-Fr endotracheal tube. Peripheral IV access obtained with 21-gauge catheter placed on dorsal ear vein. Supplemental anesthesia(if required): 8-10mg/kg thiopental sodium. Isoflurane 0.5-2% administered by inhalation via endotracheal tube. animals mechanically ventilated at tidal vol 15-20ml/kg with 100% oxygen 12resps/min.
Antibiotic: NR
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NA
Necropsy: NA
Instrumentation
EVIS Type 100 Q140; ; 12-gauge needle & catheter; ; 0.89·400cm access Jag wire (BS); 18-20mm esophageal/colonic dilating
Surgical procedure Transluminal access Site access & prep: endoscope (Oly EVIS Type 100 Q140) passed via mouth & gastroscopy performed. No site prep reported. Incision site: NR Incision method: Using transillumination, 12g needle & catheter passed through left upper quadrant abdominal wall into stomach under direct endoscopic visualization. Access Jag wire passed through needle & secured intraluminally by endoscopic snare. Needle & catheter subsequently removed & Jag wire, snare & endoscope removed as 1 unit through mouth. Endoscope reintroduced into stomach & gastric site containing access wire entrance visually inspected. Modified endoscopic needle knife electrocautery/access wire used to enlarge hole around access wire by transmural freehand cautery through gastric wall, resulting in 3mm opening enveloping transabdominal access wire. Needle knife/access wire advanced 10cm through enlarged gastric defect into peritoneal cavity. 18-20mm oesophageal/colonic dilating balloon passed over electrocautery/access wire, & used to dilate 3mm gastrotomy to 1.5cm. Balloon & needle knife retracted from endoscope & endoscope tip directed through gastric defect into abdominal cavity.
Intervention Abdomen insufflated through gastroscope insufflation port & NOTES peritoneoscopy performed, then pneumoperitoneum suctioned out of peritoneal cavity & endoscope withdrawn. 2m section of 14g Tygon tubing fastened to endoscope shaft & passed though gastrostomy. Abdomen insufflated through scope insufflation port & 2 additional 12g catheters placed through right upper & lower quadrant abdominal walls.1 catheter connected to standard laparoscopic insufflator & the other connected to arterial/central venous pressure transducer. All pressure transducers secured to operating table & tiered at commencement of each experiment. Abdomen subsequently insufflated to discrete pressures over a range of values typical for laparoscopy (10–30mmHg) in 5-mmHg increments via laparoscopic insufflator. Pressures recorded simultaneously from the insufflator output (A), the RLQ transabdominal catheter (B), Tygon tubing (C), biopsy port at headset of endoscope (D). Pressure-tubing segments flushed with water between pressure recordings. Retraction & viscerotomy closure No closure.
Procedural Success/Complications Incision: NR
Visualisation: 4/4 pigs successfully explored using NOTES.
Manoeuvrability: NR
Intervention: Recorded pressures from insufflator (driving pressures at point A) & pressure transducers (sensed pressures at points B through D) recorded. Pearson coefficient of correlation (R) & coefficient of determination (R2)
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA
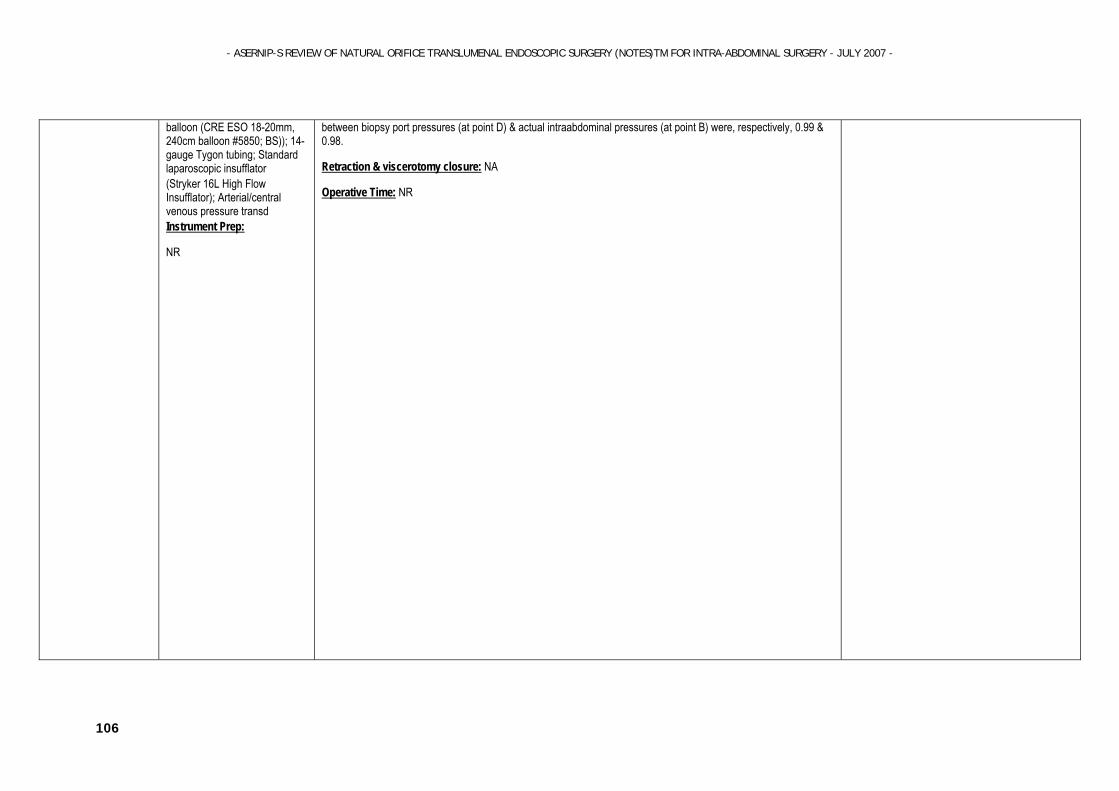
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
106
balloon (CRE ESO 18-20mm, 240cm balloon #5850; BS)); 14-gauge Tygon tubing; Standard laparoscopic insufflator (Stryker 16L High Flow Insufflator); Arterial/central venous pressure transd Instrument Prep:
NR
between biopsy port pressures (at point D) & actual intraabdominal pressures (at point B) were, respectively, 0.99 & 0.98.
Retraction & viscerotomy closure: NA
Operative Time: NR
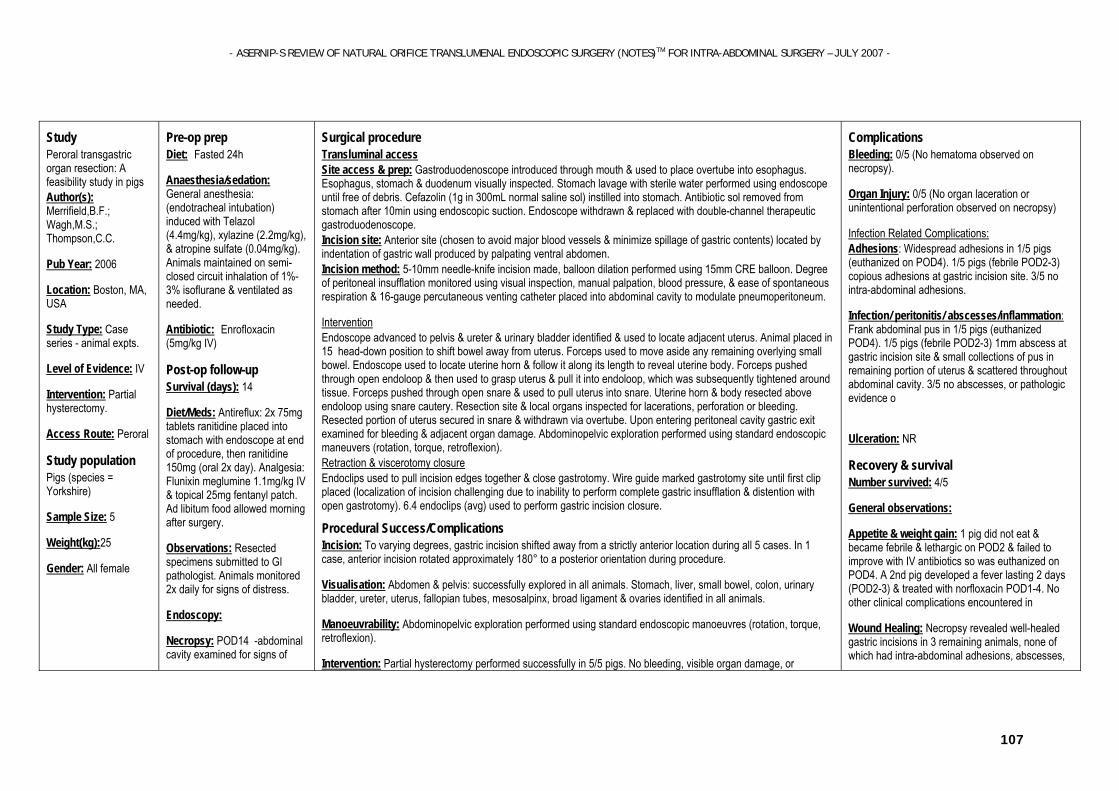
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
107
Study Peroral transgastric organ resection: A feasibility study in pigs Author(s): Merrifield,B.F.; Wagh,M.S.; Thompson,C.C.
Pub Year: 2006
Location: Boston, MA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Partial hysterectomy.
Access Route: Peroral
Study population Pigs (species = Yorkshire)
Sample Size: 5
Weight(kg):25
Gender: All female
Pre-op prep Diet: Fasted 24h
Anaesthesia/sedation: General anesthesia: (endotracheal intubation) induced with Telazol (4.4mg/kg), xylazine (2.2mg/kg), & atropine sulfate (0.04mg/kg). Animals maintained on semi-closed circuit inhalation of 1%-3% isoflurane & ventilated as needed.
Antibiotic: Enrofloxacin (5mg/kg IV)
Post-op follow-up
Survival (days): 14
Diet/Meds: Antireflux: 2x 75mg tablets ranitidine placed into stomach with endoscope at end of procedure, then ranitidine 150mg (oral 2x day). Analgesia: Flunixin meglumine 1.1mg/kg IV & topical 25mg fentanyl patch. Ad libitum food allowed morning after surgery.
Observations: Resected specimens submitted to GI pathologist. Animals monitored 2x daily for signs of distress.
Endoscopy:
Necropsy: POD14 -abdominal cavity examined for signs of
Surgical procedure Transluminal access Site access & prep: Gastroduodenoscope introduced through mouth & used to place overtube into esophagus. Esophagus, stomach & duodenum visually inspected. Stomach lavage with sterile water performed using endoscope until free of debris. Cefazolin (1g in 300mL normal saline sol) instilled into stomach. Antibiotic sol removed from stomach after 10min using endoscopic suction. Endoscope withdrawn & replaced with double-channel therapeutic gastroduodenoscope. Incision site: Anterior site (chosen to avoid major blood vessels & minimize spillage of gastric contents) located by indentation of gastric wall produced by palpating ventral abdomen. Incision method: 5-10mm needle-knife incision made, balloon dilation performed using 15mm CRE balloon. Degree of peritoneal insufflation monitored using visual inspection, manual palpation, blood pressure, & ease of spontaneous respiration & 16-gauge percutaneous venting catheter placed into abdominal cavity to modulate pneumoperitoneum.
Intervention Endoscope advanced to pelvis & ureter & urinary bladder identified & used to locate adjacent uterus. Animal placed in 15 head-down position to shift bowel away from uterus. Forceps used to move aside any remaining overlying small bowel. Endoscope used to locate uterine horn & follow it along its length to reveal uterine body. Forceps pushed through open endoloop & then used to grasp uterus & pull it into endoloop, which was subsequently tightened around tissue. Forceps pushed through open snare & used to pull uterus into snare. Uterine horn & body resected above endoloop using snare cautery. Resection site & local organs inspected for lacerations, perforation or bleeding. Resected portion of uterus secured in snare & withdrawn via overtube. Upon entering peritoneal cavity gastric exit examined for bleeding & adjacent organ damage. Abdominopelvic exploration performed using standard endoscopic maneuvers (rotation, torque, retroflexion). Retraction & viscerotomy closure Endoclips used to pull incision edges together & close gastrotomy. Wire guide marked gastrotomy site until first clip placed (localization of incision challenging due to inability to perform complete gastric insufflation & distention with open gastrotomy). 6.4 endoclips (avg) used to perform gastric incision closure.
Procedural Success/Complications Incision: To varying degrees, gastric incision shifted away from a strictly anterior location during all 5 cases. In 1 case, anterior incision rotated approximately 180° to a posterior orientation during procedure.
Visualisation: Abdomen & pelvis: successfully explored in all animals. Stomach, liver, small bowel, colon, urinary bladder, ureter, uterus, fallopian tubes, mesosalpinx, broad ligament & ovaries identified in all animals.
Manoeuvrability: Abdominopelvic exploration performed using standard endoscopic manoeuvres (rotation, torque, retroflexion).
Intervention: Partial hysterectomy performed successfully in 5/5 pigs. No bleeding, visible organ damage, or
Complications Bleeding: 0/5 (No hematoma observed on necropsy).
Organ Injury: 0/5 (No organ laceration or unintentional perforation observed on necropsy)
Infection Related Complications: Adhesions: Widespread adhesions in 1/5 pigs (euthanized on POD4). 1/5 pigs (febrile POD2-3) copious adhesions at gastric incision site. 3/5 no intra-abdominal adhesions.
Infection/ peritonitis/ abscesses/inflammation: Frank abdominal pus in 1/5 pigs (euthanized POD4). 1/5 pigs (febrile POD2-3) 1mm abscess at gastric incision site & small collections of pus in remaining portion of uterus & scattered throughout abdominal cavity. 3/5 no abscesses, or pathologic evidence o
Ulceration: NR
Recovery & survival Number survived: 4/5
General observations:
Appetite & weight gain: 1 pig did not eat & became febrile & lethargic on POD2 & failed to improve with IV antibiotics so was euthanized on POD4. A 2nd pig developed a fever lasting 2 days (POD2-3) & treated with norfloxacin POD1-4. No other clinical complications encountered in
Wound Healing: Necropsy revealed well-healed gastric incisions in 3 remaining animals, none of which had intra-abdominal adhesions, abscesses,

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
108
peritonitis, abscess, bleeding, perforation. Gastrotomy site, resection bed, & peritoneal biopsies submitted for histologic examination.
Instrumentation
GIF Q140; GIF 2T100; ; ; Oesophageal overtube (CE); Needle-knife (Huibregtse RAMP; CE); CRE dilatation balloon (MEBS); Reusable endoscopic jumbo forceps; Polypectomy snare; disposable endoclips & endoloops (Oly) Instrument Prep:
Endoscopes immersed & flushed with 2.4% glutaraldehyde & air-dried before use. Sterile disposable endoclips & endoloops were used.Other instruments chemically sterilized in 2.4% glutaraldehyde bath before surgery.
hemodynamic instability encountered during procedure. Abdomen & pelvis successfully explored in all animals. Stomach, liver, small bowel, colon, urinary bladder, ureter, uterus, fallopian tubes, mesosalpinx, broad ligament, & ovaries identified in all animals. Necropsy confirmed partial hysterectomy in 5/5 pigs.
Retraction & viscerotomy closure: In 1 pig gastrotomy not completely closed with endoclips due to oedema at incision site. Necropsy revealed 4mm hole at incision site.
Operative Time: Complete procedure =2.9hrs (avg). Gastric lavage, passing scope through gastric wall, & closing stomach represented most time-consuming aspects of procedure. Locating & removing portions of uterus accomplished relatively quickly.
or pathologic evidence of peritonitis.
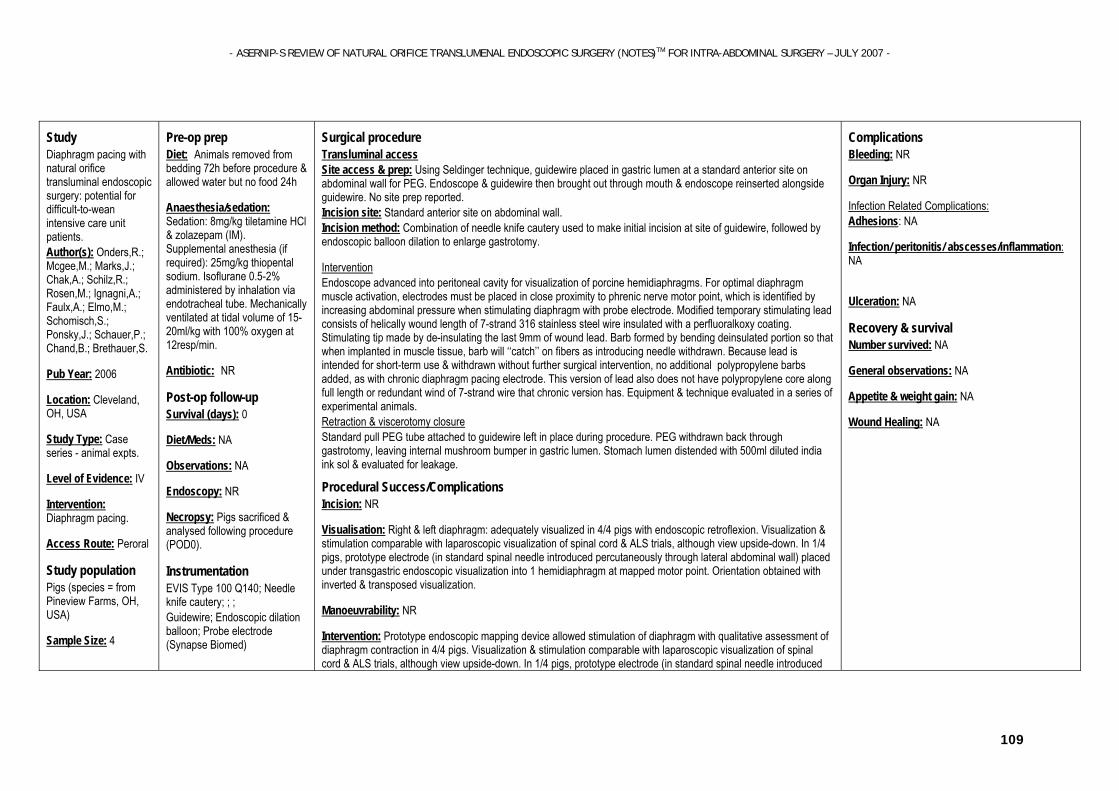
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
109
Study Diaphragm pacing with natural orifice transluminal endoscopic surgery: potential for difficult-to-wean intensive care unit patients. Author(s): Onders,R.; Mcgee,M.; Marks,J.; Chak,A.; Schilz,R.; Rosen,M.; Ignagni,A.; Faulx,A.; Elmo,M.; Schomisch,S.; Ponsky,J.; Schauer,P.; Chand,B.; Brethauer,S.
Pub Year: 2006
Location: Cleveland, OH, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Diaphragm pacing.
Access Route: Peroral
Study population Pigs (species = from Pineview Farms, OH, USA)
Sample Size: 4
Pre-op prep Diet: Animals removed from bedding 72h before procedure & allowed water but no food 24h
Anaesthesia/sedation: Sedation: 8mg/kg tiletamine HCl & zolazepam (IM). Supplemental anesthesia (if required): 25mg/kg thiopental sodium. Isoflurane 0.5-2% administered by inhalation via endotracheal tube. Mechanically ventilated at tidal volume of 15-20ml/kg with 100% oxygen at 12resp/min.
Antibiotic: NR
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NR
Necropsy: Pigs sacrificed & analysed following procedure (POD0).
Instrumentation
EVIS Type 100 Q140; Needle knife cautery; ; ; Guidewire; Endoscopic dilation balloon; Probe electrode (Synapse Biomed)
Surgical procedure Transluminal access Site access & prep: Using Seldinger technique, guidewire placed in gastric lumen at a standard anterior site on abdominal wall for PEG. Endoscope & guidewire then brought out through mouth & endoscope reinserted alongside guidewire. No site prep reported. Incision site: Standard anterior site on abdominal wall. Incision method: Combination of needle knife cautery used to make initial incision at site of guidewire, followed by endoscopic balloon dilation to enlarge gastrotomy.
Intervention Endoscope advanced into peritoneal cavity for visualization of porcine hemidiaphragms. For optimal diaphragm muscle activation, electrodes must be placed in close proximity to phrenic nerve motor point, which is identified by increasing abdominal pressure when stimulating diaphragm with probe electrode. Modified temporary stimulating lead consists of helically wound length of 7-strand 316 stainless steel wire insulated with a perfluoralkoxy coating. Stimulating tip made by de-insulating the last 9mm of wound lead. Barb formed by bending deinsulated portion so that when implanted in muscle tissue, barb will ‘‘catch’’ on fibers as introducing needle withdrawn. Because lead is intended for short-term use & withdrawn without further surgical intervention, no additional polypropylene barbs added, as with chronic diaphragm pacing electrode. This version of lead also does not have polypropylene core along full length or redundant wind of 7-strand wire that chronic version has. Equipment & technique evaluated in a series of experimental animals. Retraction & viscerotomy closure Standard pull PEG tube attached to guidewire left in place during procedure. PEG withdrawn back through gastrotomy, leaving internal mushroom bumper in gastric lumen. Stomach lumen distended with 500ml diluted india ink sol & evaluated for leakage.
Procedural Success/Complications Incision: NR
Visualisation: Right & left diaphragm: adequately visualized in 4/4 pigs with endoscopic retroflexion. Visualization & stimulation comparable with laparoscopic visualization of spinal cord & ALS trials, although view upside-down. In 1/4 pigs, prototype electrode (in standard spinal needle introduced percutaneously through lateral abdominal wall) placed under transgastric endoscopic visualization into 1 hemidiaphragm at mapped motor point. Orientation obtained with inverted & transposed visualization.
Manoeuvrability: NR
Intervention: Prototype endoscopic mapping device allowed stimulation of diaphragm with qualitative assessment of diaphragm contraction in 4/4 pigs. Visualization & stimulation comparable with laparoscopic visualization of spinal cord & ALS trials, although view upside-down. In 1/4 pigs, prototype electrode (in standard spinal needle introduced
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA
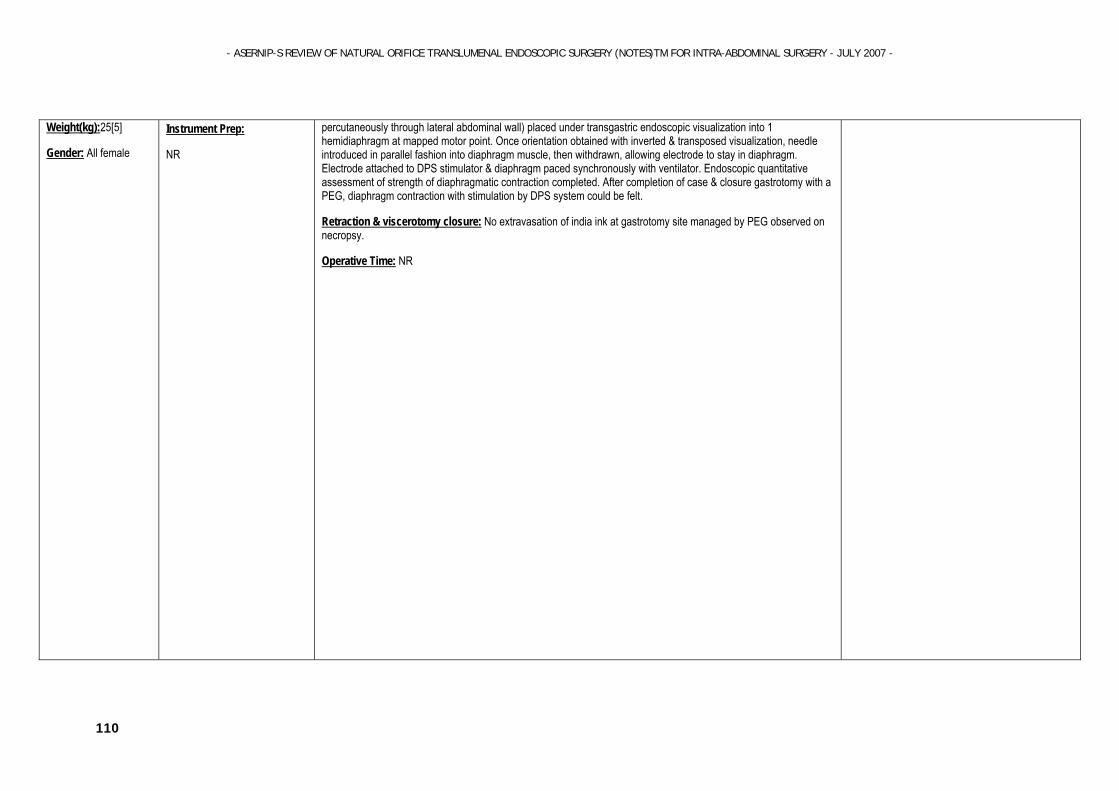
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
110
Weight(kg):25[5]
Gender: All female
Instrument Prep:
NR
percutaneously through lateral abdominal wall) placed under transgastric endoscopic visualization into 1 hemidiaphragm at mapped motor point. Once orientation obtained with inverted & transposed visualization, needle introduced in parallel fashion into diaphragm muscle, then withdrawn, allowing electrode to stay in diaphragm. Electrode attached to DPS stimulator & diaphragm paced synchronously with ventilator. Endoscopic quantitative assessment of strength of diaphragmatic contraction completed. After completion of case & closure gastrotomy with a PEG, diaphragm contraction with stimulation by DPS system could be felt.
Retraction & viscerotomy closure: No extravasation of india ink at gastrotomy site managed by PEG observed on necropsy.
Operative Time: NR
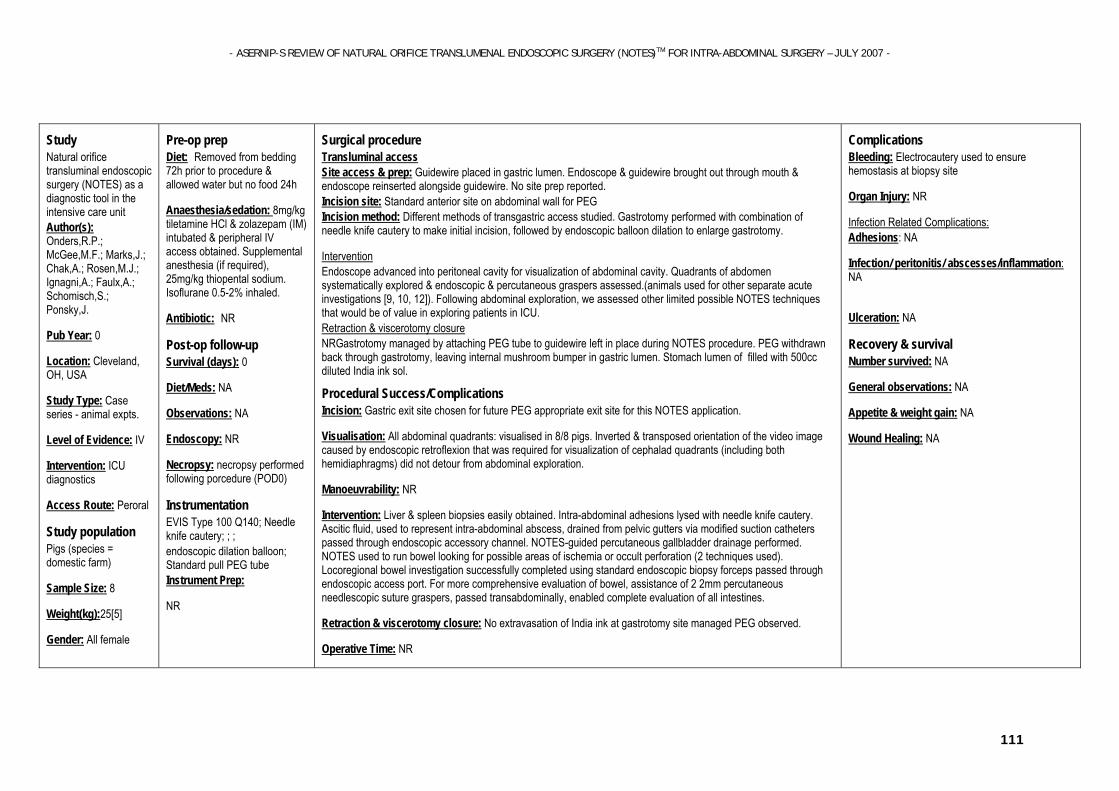
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
111
Study Natural orifice transluminal endoscopic surgery (NOTES) as a diagnostic tool in the intensive care unit Author(s): Onders,R.P.; McGee,M.F.; Marks,J.; Chak,A.; Rosen,M.J.; Ignagni,A.; Faulx,A.; Schomisch,S.; Ponsky,J.
Pub Year: 0
Location: Cleveland, OH, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: ICU diagnostics
Access Route: Peroral
Study population Pigs (species = domestic farm)
Sample Size: 8
Weight(kg):25[5]
Gender: All female
Pre-op prep Diet: Removed from bedding 72h prior to procedure & allowed water but no food 24h
Anaesthesia/sedation: 8mg/kg tiletamine HCl & zolazepam (IM) intubated & peripheral IV access obtained. Supplemental anesthesia (if required), 25mg/kg thiopental sodium. Isoflurane 0.5-2% inhaled.
Antibiotic: NR
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NR
Necropsy: necropsy performed following porcedure (POD0)
Instrumentation
EVIS Type 100 Q140; Needle knife cautery; ; ; endoscopic dilation balloon; Standard pull PEG tube Instrument Prep:
NR
Surgical procedure Transluminal access Site access & prep: Guidewire placed in gastric lumen. Endoscope & guidewire brought out through mouth & endoscope reinserted alongside guidewire. No site prep reported. Incision site: Standard anterior site on abdominal wall for PEG Incision method: Different methods of transgastric access studied. Gastrotomy performed with combination of needle knife cautery to make initial incision, followed by endoscopic balloon dilation to enlarge gastrotomy.
Intervention Endoscope advanced into peritoneal cavity for visualization of abdominal cavity. Quadrants of abdomen systematically explored & endoscopic & percutaneous graspers assessed.(animals used for other separate acute investigations [9, 10, 12]). Following abdominal exploration, we assessed other limited possible NOTES techniques that would be of value in exploring patients in ICU. Retraction & viscerotomy closure NRGastrotomy managed by attaching PEG tube to guidewire left in place during NOTES procedure. PEG withdrawn back through gastrotomy, leaving internal mushroom bumper in gastric lumen. Stomach lumen of filled with 500cc diluted India ink sol.
Procedural Success/Complications Incision: Gastric exit site chosen for future PEG appropriate exit site for this NOTES application.
Visualisation: All abdominal quadrants: visualised in 8/8 pigs. Inverted & transposed orientation of the video image caused by endoscopic retroflexion that was required for visualization of cephalad quadrants (including both hemidiaphragms) did not detour from abdominal exploration.
Manoeuvrability: NR
Intervention: Liver & spleen biopsies easily obtained. Intra-abdominal adhesions lysed with needle knife cautery. Ascitic fluid, used to represent intra-abdominal abscess, drained from pelvic gutters via modified suction catheters passed through endoscopic accessory channel. NOTES-guided percutaneous gallbladder drainage performed. NOTES used to run bowel looking for possible areas of ischemia or occult perforation (2 techniques used). Locoregional bowel investigation successfully completed using standard endoscopic biopsy forceps passed through endoscopic access port. For more comprehensive evaluation of bowel, assistance of 2 2mm percutaneous needlescopic suture graspers, passed transabdominally, enabled complete evaluation of all intestines.
Retraction & viscerotomy closure: No extravasation of India ink at gastrotomy site managed PEG observed.
Operative Time: NR
Complications Bleeding: Electrocautery used to ensure hemostasis at biopsy site
Organ Injury: NR
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA
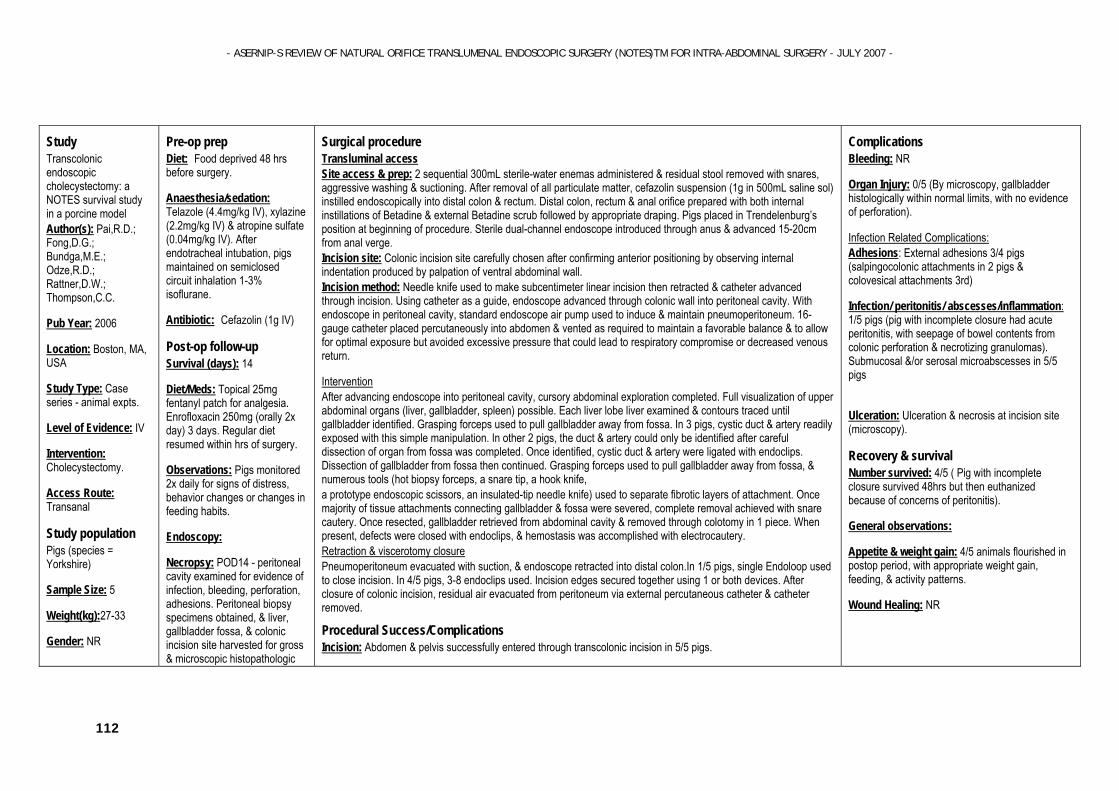
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
112
Study Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model Author(s): Pai,R.D.; Fong,D.G.; Bundga,M.E.; Odze,R.D.; Rattner,D.W.; Thompson,C.C.
Pub Year: 2006
Location: Boston, MA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Cholecystectomy.
Access Route: Transanal
Study population Pigs (species = Yorkshire)
Sample Size: 5
Weight(kg):27-33
Gender: NR
Pre-op prep Diet: Food deprived 48 hrs before surgery.
Anaesthesia/sedation: Telazole (4.4mg/kg IV), xylazine (2.2mg/kg IV) & atropine sulfate (0.04mg/kg IV). After endotracheal intubation, pigs maintained on semiclosed circuit inhalation 1-3% isoflurane.
Antibiotic: Cefazolin (1g IV)
Post-op follow-up
Survival (days): 14
Diet/Meds: Topical 25mg fentanyl patch for analgesia. Enrofloxacin 250mg (orally 2x day) 3 days. Regular diet resumed within hrs of surgery.
Observations: Pigs monitored 2x daily for signs of distress, behavior changes or changes in feeding habits.
Endoscopy:
Necropsy: POD14 - peritoneal cavity examined for evidence of infection, bleeding, perforation, adhesions. Peritoneal biopsy specimens obtained, & liver, gallbladder fossa, & colonic incision site harvested for gross & microscopic histopathologic
Surgical procedure Transluminal access Site access & prep: 2 sequential 300mL sterile-water enemas administered & residual stool removed with snares, aggressive washing & suctioning. After removal of all particulate matter, cefazolin suspension (1g in 500mL saline sol) instilled endoscopically into distal colon & rectum. Distal colon, rectum & anal orifice prepared with both internal instillations of Betadine & external Betadine scrub followed by appropriate draping. Pigs placed in Trendelenburg’s position at beginning of procedure. Sterile dual-channel endoscope introduced through anus & advanced 15-20cm from anal verge. Incision site: Colonic incision site carefully chosen after confirming anterior positioning by observing internal indentation produced by palpation of ventral abdominal wall. Incision method: Needle knife used to make subcentimeter linear incision then retracted & catheter advanced through incision. Using catheter as a guide, endoscope advanced through colonic wall into peritoneal cavity. With endoscope in peritoneal cavity, standard endoscope air pump used to induce & maintain pneumoperitoneum. 16-gauge catheter placed percutaneously into abdomen & vented as required to maintain a favorable balance & to allow for optimal exposure but avoided excessive pressure that could lead to respiratory compromise or decreased venous return.
Intervention After advancing endoscope into peritoneal cavity, cursory abdominal exploration completed. Full visualization of upper abdominal organs (liver, gallbladder, spleen) possible. Each liver lobe liver examined & contours traced until gallbladder identified. Grasping forceps used to pull gallbladder away from fossa. In 3 pigs, cystic duct & artery readily exposed with this simple manipulation. In other 2 pigs, the duct & artery could only be identified after careful dissection of organ from fossa was completed. Once identified, cystic duct & artery were ligated with endoclips. Dissection of gallbladder from fossa then continued. Grasping forceps used to pull gallbladder away from fossa, & numerous tools (hot biopsy forceps, a snare tip, a hook knife, a prototype endoscopic scissors, an insulated-tip needle knife) used to separate fibrotic layers of attachment. Once majority of tissue attachments connecting gallbladder & fossa were severed, complete removal achieved with snare cautery. Once resected, gallbladder retrieved from abdominal cavity & removed through colotomy in 1 piece. When present, defects were closed with endoclips, & hemostasis was accomplished with electrocautery. Retraction & viscerotomy closure Pneumoperitoneum evacuated with suction, & endoscope retracted into distal colon.In 1/5 pigs, single Endoloop used to close incision. In 4/5 pigs, 3-8 endoclips used. Incision edges secured together using 1 or both devices. After closure of colonic incision, residual air evacuated from peritoneum via external percutaneous catheter & catheter removed.
Procedural Success/Complications Incision: Abdomen & pelvis successfully entered through transcolonic incision in 5/5 pigs.
Complications Bleeding: NR
Organ Injury: 0/5 (By microscopy, gallbladder histologically within normal limits, with no evidence of perforation).
Infection Related Complications: Adhesions: External adhesions 3/4 pigs (salpingocolonic attachments in 2 pigs & colovesical attachments 3rd)
Infection/ peritonitis/ abscesses/inflammation: 1/5 pigs (pig with incomplete closure had acute peritonitis, with seepage of bowel contents from colonic perforation & necrotizing granulomas). Submucosal &/or serosal microabscesses in 5/5 pigs
Ulceration: Ulceration & necrosis at incision site (microscopy).
Recovery & survival Number survived: 4/5 ( Pig with incomplete closure survived 48hrs but then euthanized because of concerns of peritonitis).
General observations:
Appetite & weight gain: 4/5 animals flourished in postop period, with appropriate weight gain, feeding, & activity patterns.
Wound Healing: NR

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
113
exam.
Instrumentation
GIF Q160; GIF 2T100; Cold & hot biopsy forceps; Snares; Endoloops (Oly); Prototype endoscopic scissors (MEBS); Hook knife: Insulated-tip & regular needle knives Instrument Prep: Disposable endoclips & Endoloops used. Other equipment cleaned using high-level chemical disinfection in 2.4% glutaraldehyde.
Visualisation: Liver, gallbladder & spleen: readily identified in 5/5 pigs.
Common bile duct: identified 0/5 pigs.
Gallbladder: liver contours traced until identified.
Manoeuvrability: NR
Intervention: Complete gallbladder resection with ligation of cystic duct & artery completed & gallbladder removed in 1 piece in 5/5 pigs.
Retraction & viscerotomy closure: Appeared closed & fully healed from luminal aspect in 4/5 pigs. In 1/5 pigs, complete closure of colonic incision site not possible & 4mm residual defect remained at conclusion of surgery.
Operative Time: Entrance into peritoneal cavity to removal of gallbladder from anal orifice = 68min(avg). Completion of procedure = 70-165min (mean=115min). Time for procedure improved with experience.
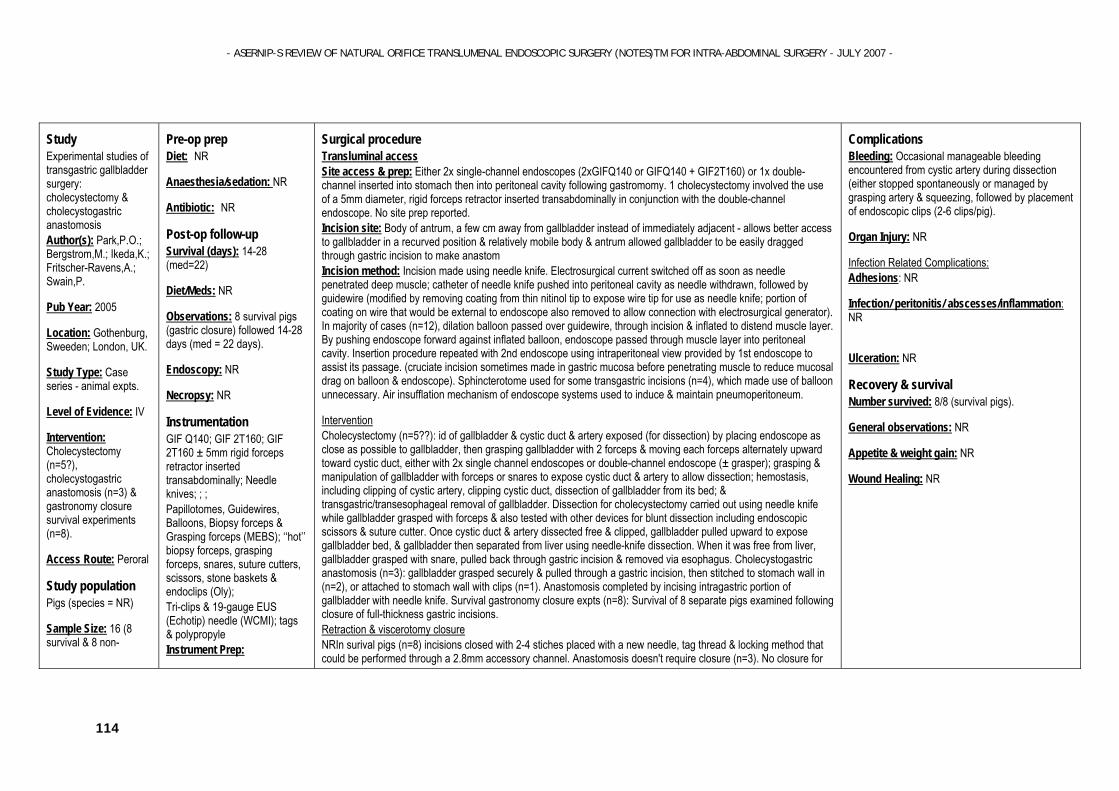
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
114
Study Experimental studies of transgastric gallbladder surgery: cholecystectomy & cholecystogastric anastomosis Author(s): Park,P.O.; Bergstrom,M.; Ikeda,K.; Fritscher-Ravens,A.; Swain,P.
Pub Year: 2005
Location: Gothenburg, Sweeden; London, UK.
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Cholecystectomy (n=5?), cholecystogastric anastomosis (n=3) & gastronomy closure survival experiments (n=8).
Access Route: Peroral
Study population Pigs (species = NR)
Sample Size: 16 (8 survival & 8 non-
Pre-op prep Diet: NR
Anaesthesia/sedation: NR
Antibiotic: NR
Post-op follow-up
Survival (days): 14-28 (med=22)
Diet/Meds: NR
Observations: 8 survival pigs (gastric closure) followed 14-28 days (med = 22 days).
Endoscopy: NR
Necropsy: NR
Instrumentation
GIF Q140; GIF 2T160; GIF 2T160 ± 5mm rigid forceps retractor inserted transabdominally; Needle knives; ; ; Papillotomes, Guidewires, Balloons, Biopsy forceps & Grasping forceps (MEBS); ‘‘hot’’ biopsy forceps, grasping forceps, snares, suture cutters, scissors, stone baskets & endoclips (Oly); Tri-clips & 19-gauge EUS (Echotip) needle (WCMI); tags & polypropyle Instrument Prep:
Surgical procedure Transluminal access Site access & prep: Either 2x single-channel endoscopes (2xGIFQ140 or GIFQ140 + GIF2T160) or 1x double-channel inserted into stomach then into peritoneal cavity following gastromomy. 1 cholecystectomy involved the use of a 5mm diameter, rigid forceps retractor inserted transabdominally in conjunction with the double-channel endoscope. No site prep reported. Incision site: Body of antrum, a few cm away from gallbladder instead of immediately adjacent - allows better access to gallbladder in a recurved position & relatively mobile body & antrum allowed gallbladder to be easily dragged through gastric incision to make anastom Incision method: Incision made using needle knife. Electrosurgical current switched off as soon as needle penetrated deep muscle; catheter of needle knife pushed into peritoneal cavity as needle withdrawn, followed by guidewire (modified by removing coating from thin nitinol tip to expose wire tip for use as needle knife; portion of coating on wire that would be external to endoscope also removed to allow connection with electrosurgical generator). In majority of cases (n=12), dilation balloon passed over guidewire, through incision & inflated to distend muscle layer. By pushing endoscope forward against inflated balloon, endoscope passed through muscle layer into peritoneal cavity. Insertion procedure repeated with 2nd endoscope using intraperitoneal view provided by 1st endoscope to assist its passage. (cruciate incision sometimes made in gastric mucosa before penetrating muscle to reduce mucosal drag on balloon & endoscope). Sphincterotome used for some transgastric incisions (n=4), which made use of balloon unnecessary. Air insufflation mechanism of endoscope systems used to induce & maintain pneumoperitoneum.
Intervention Cholecystectomy (n=5??): id of gallbladder & cystic duct & artery exposed (for dissection) by placing endoscope as close as possible to gallbladder, then grasping gallbladder with 2 forceps & moving each forceps alternately upward toward cystic duct, either with 2x single channel endoscopes or double-channel endoscope (± grasper); grasping & manipulation of gallbladder with forceps or snares to expose cystic duct & artery to allow dissection; hemostasis, including clipping of cystic artery, clipping cystic duct, dissection of gallbladder from its bed; & transgastric/transesophageal removal of gallbladder. Dissection for cholecystectomy carried out using needle knife while gallbladder grasped with forceps & also tested with other devices for blunt dissection including endoscopic scissors & suture cutter. Once cystic duct & artery dissected free & clipped, gallbladder pulled upward to expose gallbladder bed, & gallbladder then separated from liver using needle-knife dissection. When it was free from liver, gallbladder grasped with snare, pulled back through gastric incision & removed via esophagus. Cholecystogastric anastomosis (n=3): gallbladder grasped securely & pulled through a gastric incision, then stitched to stomach wall in (n=2), or attached to stomach wall with clips (n=1). Anastomosis completed by incising intragastric portion of gallbladder with needle knife. Survival gastronomy closure expts (n=8): Survival of 8 separate pigs examined following closure of full-thickness gastric incisions. Retraction & viscerotomy closure NRIn surival pigs (n=8) incisions closed with 2-4 stiches placed with a new needle, tag thread & locking method that could be performed through a 2.8mm accessory channel. Anastomosis doesn't require closure (n=3). No closure for
Complications Bleeding: Occasional manageable bleeding encountered from cystic artery during dissection (either stopped spontaneously or managed by grasping artery & squeezing, followed by placement of endoscopic clips (2-6 clips/pig).
Organ Injury: NR
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: NR
Ulceration: NR
Recovery & survival Number survived: 8/8 (survival pigs).
General observations: NR
Appetite & weight gain: NR
Wound Healing: NR
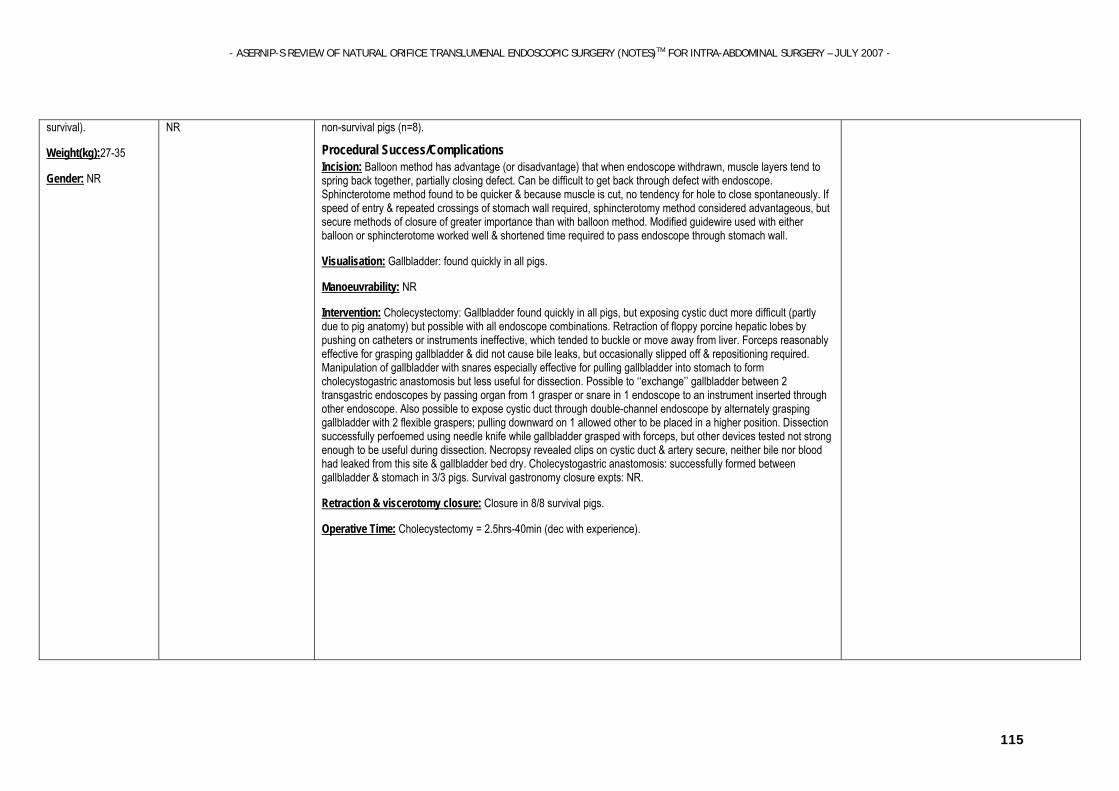
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
115
survival).
Weight(kg):27-35
Gender: NR
NR non-survival pigs (n=8).
Procedural Success/Complications Incision: Balloon method has advantage (or disadvantage) that when endoscope withdrawn, muscle layers tend to spring back together, partially closing defect. Can be difficult to get back through defect with endoscope. Sphincterotome method found to be quicker & because muscle is cut, no tendency for hole to close spontaneously. If speed of entry & repeated crossings of stomach wall required, sphincterotomy method considered advantageous, but secure methods of closure of greater importance than with balloon method. Modified guidewire used with either balloon or sphincterotome worked well & shortened time required to pass endoscope through stomach wall.
Visualisation: Gallbladder: found quickly in all pigs.
Manoeuvrability: NR
Intervention: Cholecystectomy: Gallbladder found quickly in all pigs, but exposing cystic duct more difficult (partly due to pig anatomy) but possible with all endoscope combinations. Retraction of floppy porcine hepatic lobes by pushing on catheters or instruments ineffective, which tended to buckle or move away from liver. Forceps reasonably effective for grasping gallbladder & did not cause bile leaks, but occasionally slipped off & repositioning required. Manipulation of gallbladder with snares especially effective for pulling gallbladder into stomach to form cholecystogastric anastomosis but less useful for dissection. Possible to ‘‘exchange’’ gallbladder between 2 transgastric endoscopes by passing organ from 1 grasper or snare in 1 endoscope to an instrument inserted through other endoscope. Also possible to expose cystic duct through double-channel endoscope by alternately grasping gallbladder with 2 flexible graspers; pulling downward on 1 allowed other to be placed in a higher position. Dissection successfully perfoemed using needle knife while gallbladder grasped with forceps, but other devices tested not strong enough to be useful during dissection. Necropsy revealed clips on cystic duct & artery secure, neither bile nor blood had leaked from this site & gallbladder bed dry. Cholecystogastric anastomosis: successfully formed between gallbladder & stomach in 3/3 pigs. Survival gastronomy closure expts: NR.
Retraction & viscerotomy closure: Closure in 8/8 survival pigs.
Operative Time: Cholecystectomy = 2.5hrs-40min (dec with experience).
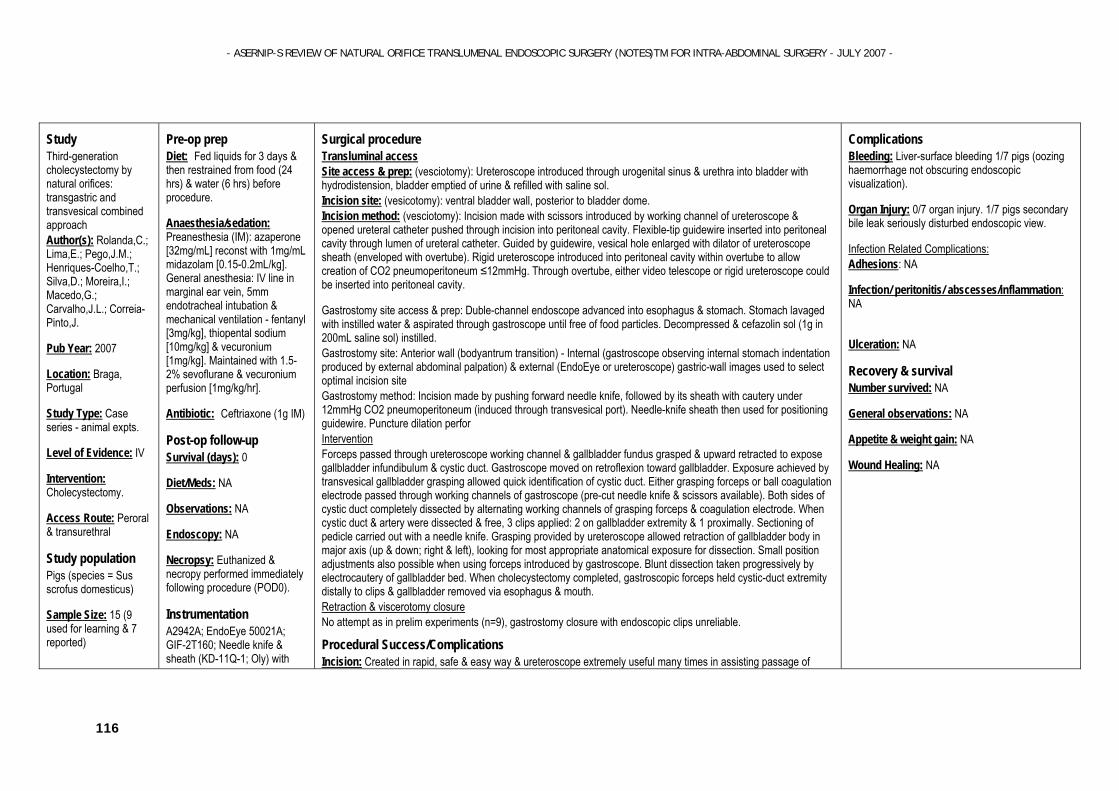
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
116
Study Third-generation cholecystectomy by natural orifices: transgastric and transvesical combined approach Author(s): Rolanda,C.; Lima,E.; Pego,J.M.; Henriques-Coelho,T.; Silva,D.; Moreira,I.; Macedo,G.; Carvalho,J.L.; Correia-Pinto,J.
Pub Year: 2007
Location: Braga, Portugal
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Cholecystectomy.
Access Route: Peroral & transurethral
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 15 (9 used for learning & 7 reported)
Pre-op prep Diet: Fed liquids for 3 days & then restrained from food (24 hrs) & water (6 hrs) before procedure.
Anaesthesia/sedation: Preanesthesia (IM): azaperone [32mg/mL] reconst with 1mg/mL midazolam [0.15-0.2mL/kg]. General anesthesia: IV line in marginal ear vein, 5mm endotracheal intubation & mechanical ventilation - fentanyl [3mg/kg], thiopental sodium [10mg/kg] & vecuronium [1mg/kg]. Maintained with 1.5-2% sevoflurane & vecuronium perfusion [1mg/kg/hr].
Antibiotic: Ceftriaxone (1g IM)
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NA
Necropsy: Euthanized & necropy performed immediately following procedure (POD0).
Instrumentation
A2942A; EndoEye 50021A; GIF-2T160; Needle knife & sheath (KD-11Q-1; Oly) with
Surgical procedure Transluminal access Site access & prep: (vesciotomy): Ureteroscope introduced through urogenital sinus & urethra into bladder with hydrodistension, bladder emptied of urine & refilled with saline sol. Incision site: (vesicotomy): ventral bladder wall, posterior to bladder dome. Incision method: (vesciotomy): Incision made with scissors introduced by working channel of ureteroscope & opened ureteral catheter pushed through incision into peritoneal cavity. Flexible-tip guidewire inserted into peritoneal cavity through lumen of ureteral catheter. Guided by guidewire, vesical hole enlarged with dilator of ureteroscope sheath (enveloped with overtube). Rigid ureteroscope introduced into peritoneal cavity within overtube to allow creation of CO2 pneumoperitoneum ≤12mmHg. Through overtube, either video telescope or rigid ureteroscope could be inserted into peritoneal cavity.
Gastrostomy site access & prep: Duble-channel endoscope advanced into esophagus & stomach. Stomach lavaged with instilled water & aspirated through gastroscope until free of food particles. Decompressed & cefazolin sol (1g in 200mL saline sol) instilled. Gastrostomy site: Anterior wall (bodyantrum transition) - Internal (gastroscope observing internal stomach indentation produced by external abdominal palpation) & external (EndoEye or ureteroscope) gastric-wall images used to select optimal incision site Gastrostomy method: Incision made by pushing forward needle knife, followed by its sheath with cautery under 12mmHg CO2 pneumoperitoneum (induced through transvesical port). Needle-knife sheath then used for positioning guidewire. Puncture dilation perfor Intervention Forceps passed through ureteroscope working channel & gallbladder fundus grasped & upward retracted to expose gallbladder infundibulum & cystic duct. Gastroscope moved on retroflexion toward gallbladder. Exposure achieved by transvesical gallbladder grasping allowed quick identification of cystic duct. Either grasping forceps or ball coagulation electrode passed through working channels of gastroscope (pre-cut needle knife & scissors available). Both sides of cystic duct completely dissected by alternating working channels of grasping forceps & coagulation electrode. When cystic duct & artery were dissected & free, 3 clips applied: 2 on gallbladder extremity & 1 proximally. Sectioning of pedicle carried out with a needle knife. Grasping provided by ureteroscope allowed retraction of gallbladder body in major axis (up & down; right & left), looking for most appropriate anatomical exposure for dissection. Small position adjustments also possible when using forceps introduced by gastroscope. Blunt dissection taken progressively by electrocautery of gallbladder bed. When cholecystectomy completed, gastroscopic forceps held cystic-duct extremity distally to clips & gallbladder removed via esophagus & mouth. Retraction & viscerotomy closure No attempt as in prelim experiments (n=9), gastrostomy closure with endoscopic clips unreliable.
Procedural Success/Complications Incision: Created in rapid, safe & easy way & ureteroscope extremely useful many times in assisting passage of
Complications Bleeding: Liver-surface bleeding 1/7 pigs (oozing haemorrhage not obscuring endoscopic visualization).
Organ Injury: 0/7 organ injury. 1/7 pigs secondary bile leak seriously disturbed endoscopic view.
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA
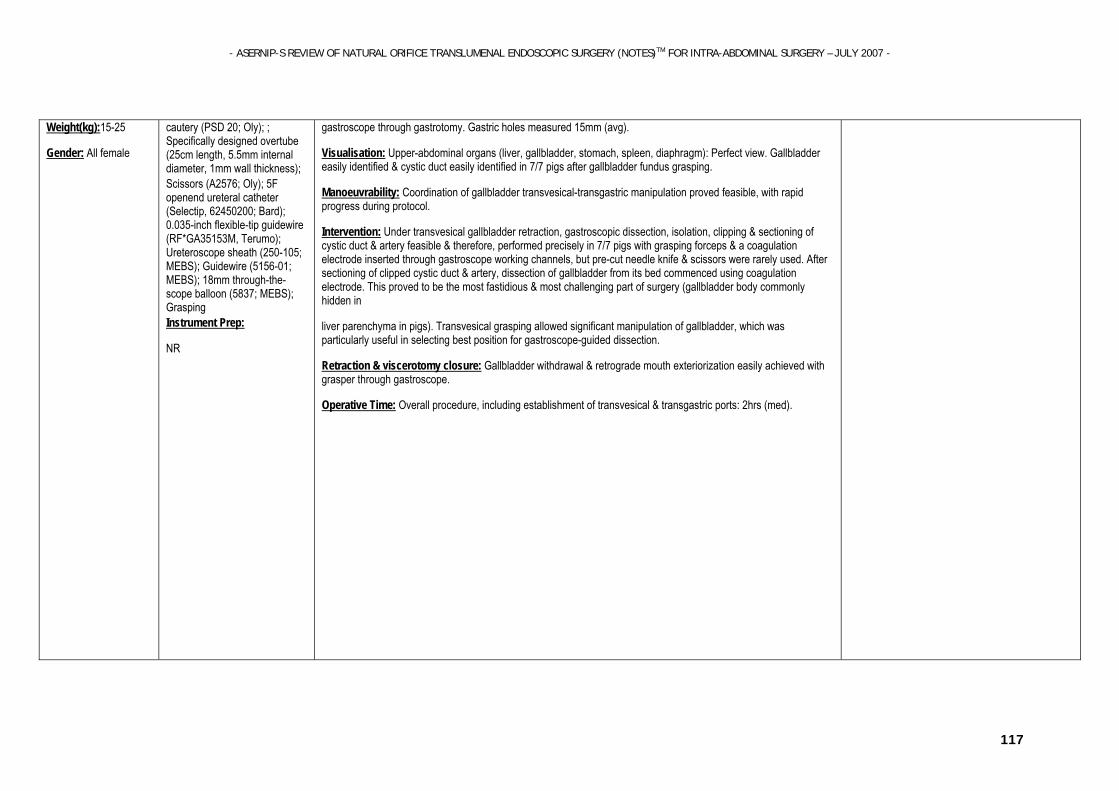
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
117
Weight(kg):15-25
Gender: All female
cautery (PSD 20; Oly); ; Specifically designed overtube (25cm length, 5.5mm internal diameter, 1mm wall thickness); Scissors (A2576; Oly); 5F openend ureteral catheter (Selectip, 62450200; Bard); 0.035-inch flexible-tip guidewire (RF*GA35153M, Terumo); Ureteroscope sheath (250-105; MEBS); Guidewire (5156-01; MEBS); 18mm through-the-scope balloon (5837; MEBS); Grasping Instrument Prep:
NR
gastroscope through gastrotomy. Gastric holes measured 15mm (avg).
Visualisation: Upper-abdominal organs (liver, gallbladder, stomach, spleen, diaphragm): Perfect view. Gallbladder easily identified & cystic duct easily identified in 7/7 pigs after gallbladder fundus grasping.
Manoeuvrability: Coordination of gallbladder transvesical-transgastric manipulation proved feasible, with rapid progress during protocol.
Intervention: Under transvesical gallbladder retraction, gastroscopic dissection, isolation, clipping & sectioning of cystic duct & artery feasible & therefore, performed precisely in 7/7 pigs with grasping forceps & a coagulation electrode inserted through gastroscope working channels, but pre-cut needle knife & scissors were rarely used. After sectioning of clipped cystic duct & artery, dissection of gallbladder from its bed commenced using coagulation electrode. This proved to be the most fastidious & most challenging part of surgery (gallbladder body commonly hidden in
liver parenchyma in pigs). Transvesical grasping allowed significant manipulation of gallbladder, which was particularly useful in selecting best position for gastroscope-guided dissection.
Retraction & viscerotomy closure: Gallbladder withdrawal & retrograde mouth exteriorization easily achieved with grasper through gastroscope.
Operative Time: Overall procedure, including establishment of transvesical & transgastric ports: 2hrs (med).
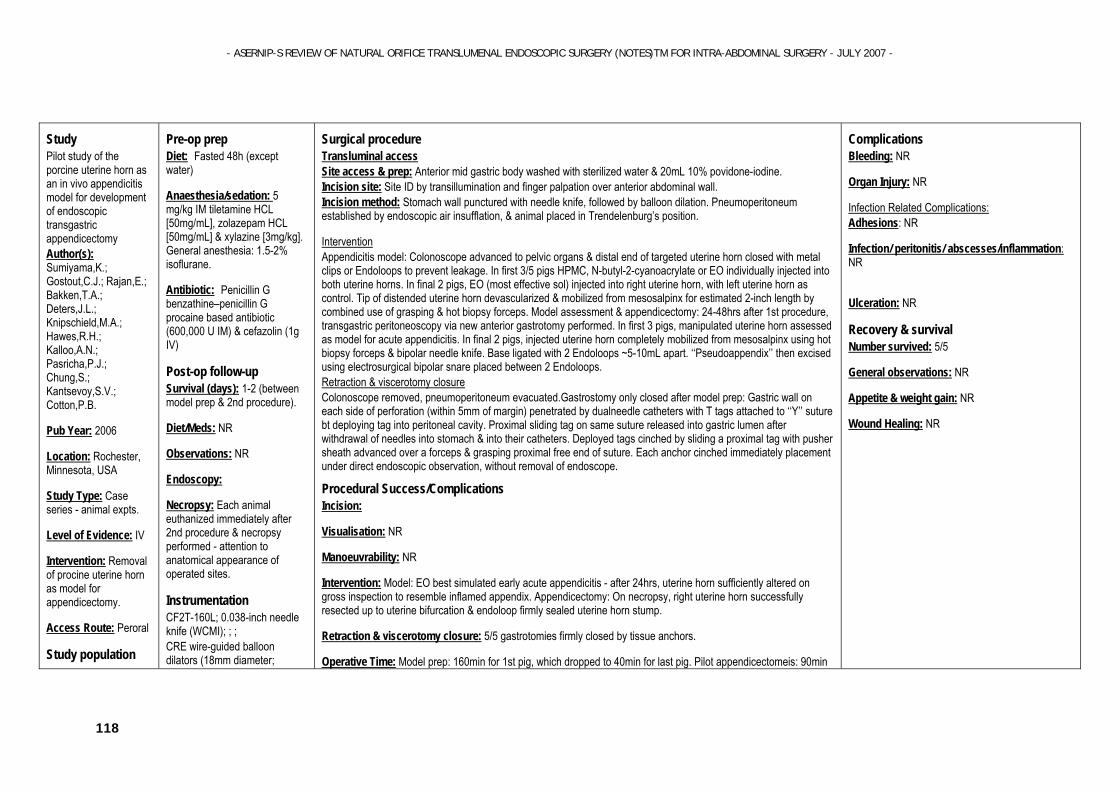
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
118
Study Pilot study of the porcine uterine horn as an in vivo appendicitis model for development of endoscopic transgastric appendicectomy Author(s): Sumiyama,K.; Gostout,C.J.; Rajan,E.; Bakken,T.A.; Deters,J.L.; Knipschield,M.A.; Hawes,R.H.; Kalloo,A.N.; Pasricha,P.J.; Chung,S.; Kantsevoy,S.V.; Cotton,P.B.
Pub Year: 2006
Location: Rochester, Minnesota, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Removal of procine uterine horn as model for appendicectomy.
Access Route: Peroral
Study population
Pre-op prep Diet: Fasted 48h (except water)
Anaesthesia/sedation: 5 mg/kg IM tiletamine HCL [50mg/mL], zolazepam HCL [50mg/mL] & xylazine [3mg/kg]. General anesthesia: 1.5-2% isoflurane.
Antibiotic: Penicillin G benzathine–penicillin G procaine based antibiotic (600,000 U IM) & cefazolin (1g IV)
Post-op follow-up
Survival (days): 1-2 (between model prep & 2nd procedure).
Diet/Meds: NR
Observations: NR
Endoscopy:
Necropsy: Each animal euthanized immediately after 2nd procedure & necropsy performed - attention to anatomical appearance of operated sites.
Instrumentation
CF2T-160L; 0.038-inch needle knife (WCMI); ; ; CRE wire-guided balloon dilators (18mm diameter;
Surgical procedure Transluminal access Site access & prep: Anterior mid gastric body washed with sterilized water & 20mL 10% povidone-iodine. Incision site: Site ID by transillumination and finger palpation over anterior abdominal wall. Incision method: Stomach wall punctured with needle knife, followed by balloon dilation. Pneumoperitoneum established by endoscopic air insufflation, & animal placed in Trendelenburg’s position.
Intervention Appendicitis model: Colonoscope advanced to pelvic organs & distal end of targeted uterine horn closed with metal clips or Endoloops to prevent leakage. In first 3/5 pigs HPMC, N-butyl-2-cyanoacrylate or EO individually injected into both uterine horns. In final 2 pigs, EO (most effective sol) injected into right uterine horn, with left uterine horn as control. Tip of distended uterine horn devascularized & mobilized from mesosalpinx for estimated 2-inch length by combined use of grasping & hot biopsy forceps. Model assessment & appendicectomy: 24-48hrs after 1st procedure, transgastric peritoneoscopy via new anterior gastrotomy performed. In first 3 pigs, manipulated uterine horn assessed as model for acute appendicitis. In final 2 pigs, injected uterine horn completely mobilized from mesosalpinx using hot biopsy forceps & bipolar needle knife. Base ligated with 2 Endoloops ~5-10mL apart. ‘‘Pseudoappendix’’ then excised using electrosurgical bipolar snare placed between 2 Endoloops. Retraction & viscerotomy closure Colonoscope removed, pneumoperitoneum evacuated.Gastrostomy only closed after model prep: Gastric wall on each side of perforation (within 5mm of margin) penetrated by dualneedle catheters with T tags attached to ‘‘Y’’ suture bt deploying tag into peritoneal cavity. Proximal sliding tag on same suture released into gastric lumen after withdrawal of needles into stomach & into their catheters. Deployed tags cinched by sliding a proximal tag with pusher sheath advanced over a forceps & grasping proximal free end of suture. Each anchor cinched immediately placement under direct endoscopic observation, without removal of endoscope.
Procedural Success/Complications Incision:
Visualisation: NR
Manoeuvrability: NR
Intervention: Model: EO best simulated early acute appendicitis - after 24hrs, uterine horn sufficiently altered on gross inspection to resemble inflamed appendix. Appendicectomy: On necropsy, right uterine horn successfully resected up to uterine bifurcation & endoloop firmly sealed uterine horn stump.
Retraction & viscerotomy closure: 5/5 gastrotomies firmly closed by tissue anchors.
Operative Time: Model prep: 160min for 1st pig, which dropped to 40min for last pig. Pilot appendicectomeis: 90min
Complications Bleeding: NR
Organ Injury: NR
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: NR
Ulceration: NR
Recovery & survival Number survived: 5/5
General observations: NR
Appetite & weight gain: NR
Wound Healing: NR
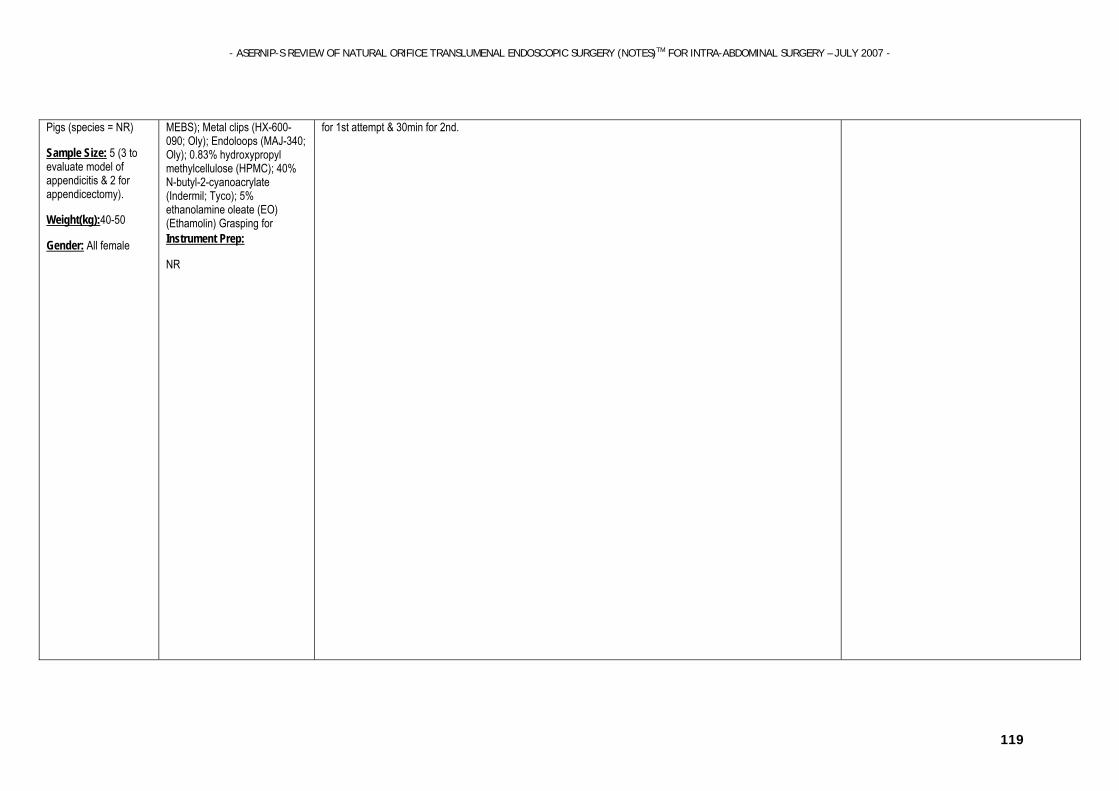
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
119
Pigs (species = NR)
Sample Size: 5 (3 to evaluate model of appendicitis & 2 for appendicectomy).
Weight(kg):40-50
Gender: All female
MEBS); Metal clips (HX-600-090; Oly); Endoloops (MAJ-340; Oly); 0.83% hydroxypropyl methylcellulose (HPMC); 40% N-butyl-2-cyanoacrylate (Indermil; Tyco); 5% ethanolamine oleate (EO) (Ethamolin) Grasping for Instrument Prep:
NR
for 1st attempt & 30min for 2nd.
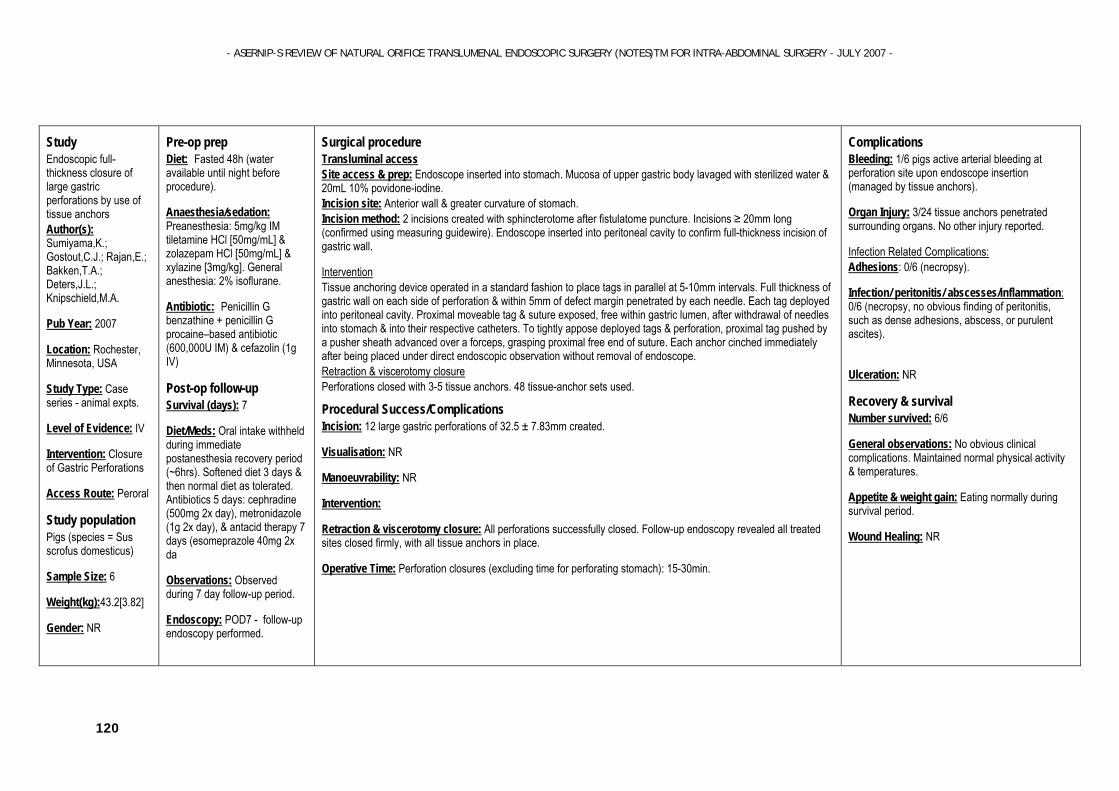
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
120
Study Endoscopic full-thickness closure of large gastric perforations by use of tissue anchors Author(s): Sumiyama,K.; Gostout,C.J.; Rajan,E.; Bakken,T.A.; Deters,J.L.; Knipschield,M.A.
Pub Year: 2007
Location: Rochester, Minnesota, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Closure of Gastric Perforations
Access Route: Peroral
Study population Pigs (species = Sus scrofus domesticus)
Sample Size: 6
Weight(kg):43.2[3.82]
Gender: NR
Pre-op prep Diet: Fasted 48h (water available until night before procedure).
Anaesthesia/sedation: Preanesthesia: 5mg/kg IM tiletamine HCl [50mg/mL] & zolazepam HCl [50mg/mL] & xylazine [3mg/kg]. General anesthesia: 2% isoflurane.
Antibiotic: Penicillin G benzathine + penicillin G procaine–based antibiotic (600,000U IM) & cefazolin (1g IV)
Post-op follow-up
Survival (days): 7
Diet/Meds: Oral intake withheld during immediate postanesthesia recovery period (~6hrs). Softened diet 3 days & then normal diet as tolerated. Antibiotics 5 days: cephradine (500mg 2x day), metronidazole (1g 2x day), & antacid therapy 7 days (esomeprazole 40mg 2x da
Observations: Observed during 7 day follow-up period.
Endoscopy: POD7 - follow-up endoscopy performed.
Surgical procedure Transluminal access Site access & prep: Endoscope inserted into stomach. Mucosa of upper gastric body lavaged with sterilized water & 20mL 10% povidone-iodine. Incision site: Anterior wall & greater curvature of stomach. Incision method: 2 incisions created with sphincterotome after fistulatome puncture. Incisions ≥ 20mm long (confirmed using measuring guidewire). Endoscope inserted into peritoneal cavity to confirm full-thickness incision of gastric wall.
Intervention Tissue anchoring device operated in a standard fashion to place tags in parallel at 5-10mm intervals. Full thickness of gastric wall on each side of perforation & within 5mm of defect margin penetrated by each needle. Each tag deployed into peritoneal cavity. Proximal moveable tag & suture exposed, free within gastric lumen, after withdrawal of needles into stomach & into their respective catheters. To tightly appose deployed tags & perforation, proximal tag pushed by a pusher sheath advanced over a forceps, grasping proximal free end of suture. Each anchor cinched immediately after being placed under direct endoscopic observation without removal of endoscope. Retraction & viscerotomy closure Perforations closed with 3-5 tissue anchors. 48 tissue-anchor sets used.
Procedural Success/Complications Incision: 12 large gastric perforations of 32.5 ± 7.83mm created.
Visualisation: NR
Manoeuvrability: NR
Intervention:
Retraction & viscerotomy closure: All perforations successfully closed. Follow-up endoscopy revealed all treated sites closed firmly, with all tissue anchors in place.
Operative Time: Perforation closures (excluding time for perforating stomach): 15-30min.
Complications Bleeding: 1/6 pigs active arterial bleeding at perforation site upon endoscope insertion (managed by tissue anchors).
Organ Injury: 3/24 tissue anchors penetrated surrounding organs. No other injury reported.
Infection Related Complications: Adhesions: 0/6 (necropsy).
Infection/ peritonitis/ abscesses/inflammation: 0/6 (necropsy, no obvious finding of peritonitis, such as dense adhesions, abscess, or purulent ascites).
Ulceration: NR
Recovery & survival Number survived: 6/6
General observations: No obvious clinical complications. Maintained normal physical activity & temperatures.
Appetite & weight gain: Eating normally during survival period.
Wound Healing: NR
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
121
Necropsy:
Instrumentation
CF2T-160L; ; ; ; Prototype tissue-anchoring–device prototype consisting of 2 18-gauge, flexible, retractable, needle catheters (7.5F outer sheath, 1660mm length) & bifurcated nylon thread (‘‘Y’’ shaped) with 3 small t tags (2 tags fixed at bifurcated distal ends & other t Instrument Prep:
NR
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
122
Study Development of a new access device for transgastric surgery Author(s): Swanstrom,L.L.; Kozarek,R.; Pasricha,P.J.; Gross,S.; Birkett,D.; Park,P.O.; Saadat,V.; Ewers,R.; Swain,P.; Swanstrom,Lee L.; Kozarek,Richard; Pasricha,Pankaj J.; Gross,Steven; Birkett,Desmond; Park,Per Ola; Saadat,Vahid; Ewers,Richard; Swain,Paul
Pub Year: 2005
Location: Portland, Oregon, USA; San Clemente, CA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Development of 2 new flexible ensoscopic devices & testing in endoscopic staging, peritonoscopy, appendicectomy &
Pre-op prep Diet: NR
Anaesthesia/sedation: Anesthetised.
Antibiotic: Prophylactic antibiotics
Post-op follow-up
Survival (days): 0
Diet/Meds: NA
Observations: NA
Endoscopy: NR
Necropsy: NR
Instrumentation
2 new FES devices*; Needle knife; ; ; Cautery snare; Various endoscopic suturing devices including Bard Endocynch (Conmed Medl) & tissue anchoring system; 4mm grasper; 2mm ‘‘corkscrew’’ device Needle-knife cautery (BS) Endoscopic clips (BS) Instrument Prep:
NR
Surgical procedure Transluminal access Site access & prep: In pigs, flexible endoscopic devices inserted directly via esophagotomy. Devices inserted per os in canine model. All animals had a 5mm laparoscope port inserted into gastric fundus to record intragastric movements of FES scopes & instruments. Laparoscopic ports also placed in low abdomen to allow FES devices to be viewed & their movements recorded. FES devices advanced into stomach & configured into both antegrade & retroflexed positions. Ability of different grasper designs tested by attempting to grasp & imbricate stomach wall. Gastric prep to ensure no solid contaminants in stomach & topical antibiotic lavage. Incision site: Anterior wall. Various tissue approximation devices tested by approximating adjacent folds of gastric fundus & approximating lesser & greater gastric curvature at GEJ. Incision method: Gastrotomy created using standard energy sources & FES devices advanced into peritoneal cavity once it was insufflated.
Intervention Peritonoscopy modeled by positioning FES devices in each abdominal quadrant. In left upper quadrant, exposure of esophageal hiatus to ID GEJ attempted by retroflexing scope, maneuvering it under left liver lobe & using reverse Trendelenburg position to ‘‘retract’’ spleen downward. Various manipulations performed including, bowel manipulation, cecal retraction. In 3 animals, gallbladder exposed & retracted, cystic artery & duct dissected & divided, & removal of gallbladder attempted in a standard retrograde fashion. Wedge liver biopsy attempted using a grasper & monopolar cautery (n=10). Exposure & dissection of gallbladder (cholecystectomy) attempted in 3 pigs in retroflexion with locking body of device used to hold up liver. Aggressive graspers used to retract infundibulum & needle-knife cautery used to dissect cystic duct & artery as well as mobilize gallbladder off liver bed. Cystic arteries controlled with endoscopic clips. Mobilized gallbladder withdrawn back into stomach as device withdrawn. Retraction & viscerotomy closure Device withdrawn into stomach. Gastrotomy closure attempted in 6 animals. 2 different closure devices used; a tissue anchoring system in 4 & a variation of Bard suturing device in 2.
Procedural Success/Complications Incision: Tissue retraction best achieved either with most aggressive 4mm grasper or with 2mm ‘‘corkscrew’’ device. Gastrotomy created without bleeding 10/10 animals, & device & scope successfully advanced into abdomen.
Visualisation: GEJ: successfully identified in 2/6 pigs & 3/4 dogs.
Right lower quadrant: cecum identified.
Right upper quadrant: successfully viewed by retroflexion in 10/10 animals. During cholecystectomy: In 1/3 pigs, uncontrolled bleeding from cystic artery caused loss of visualisation in 1 animal & gallbladder perforation & made ID of dissection planes impossible in another.
Complications Bleeding: During liver resection, significant bleeding, not able to be stopped with cautery or endoscopic clips in 1/10 animal required laparoscopic ‘‘rescue". During cholecystectomy bleeding from cystic artery unable to be controlled & visualization lost in 1st an
Organ Injury: During cholecystectomy in 2nd animal (of 3), perforation of gallbladder made ID of dissection planes impossible so attempt abandoned. In 3rd animal some gallbladder perforations occurred.
Infection Related Complications: Adhesions: NA
Infection/ peritonitis/ abscesses/inflammation: NA
Ulceration: NA
Recovery & survival Number survived: NA
General observations: NA
Appetite & weight gain: NA
Wound Healing: NA

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
123
cholecystectomy.
Access Route: Peroral
Study population Pigs (species = NR)
Sample Size: 6
Weight(kg):50
Gender: NR Dogs (mongrel) Weight = NR Sample size = 4 Gender = NR
Manoeuvrability: Both FES devices successfully inserted in 10/10 animals without mucosal injury & able to be positioned in stomach, in antegrade & retrograde positions & locked into place. Device able to be directed to all 4 abdominal quadrants & locked into place using Shapelock technology. Right upper quadrant successfully viewed by retroflexion in all animals.
Intervention: Wedge liver biopsy accomplished in 9/10 animals, but in 1 animal, significant bleeding, which was not able to be stopped with cautery or endoscopic clips required a laparoscopic ‘‘rescue". Cholecystectomy successfully accomplished in 1/3 animals: In 1 animal, bleeding from cystic artery was unable to be controlled & visualization lost; In 2nd, perforation of gallbladder occurred & made ID of dissection planes impossible so attempt was abandoned. In 3rd animal, gallbladder successfully removed, although perforations occurred, & was withdrawn into stomach.
Retraction & viscerotomy closure: Closure completed in 5/6 attempts but was watertight on explant testing only in 1/6.
Operative Time: Esophagael insertion & gastric positioning: 4min (range=(2-12min). Gastrotomy & abdominal insertion: 5min(range=3-8min). Cecal retraction: 3min(2-4min). Run small bowel: 11min(range=3-16min). Liver exposure & biopsy: 7min(range=4-13min). Hiatal exposure: 9min(7-22min). Cholecystectomy (gallbladder exposure to placement into stomach): 31min (av for all 3 attempts. successful cholecystectomy took 56min).
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
124
Study Endoscopic transgastric abdominal exploration and organ resection: initial experience in a porcine model Author(s): Wagh,M.S.; Merrifield,B.F.; Thompson,C.C.; Wagh,Mihir S.; Merrifield,Benjamin F.; Thompson,Christopher C.
Pub Year: 2005
Location: Boston, MA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Ipsilateral ophorectomy & partial hysterectomy (transgastric).
Access Route: Peroral
Study population Pigs (species = Yorkshire)
Sample Size: 8
Weight(kg):25-30
Gender: All female
Pre-op prep Diet: Fasted 48h
Anaesthesia/sedation: General anasthesia:Telazol (4.4mg/kg IV), xylazine (2.2mg/kg IV), atropine sulphate (0.04mg/kg IV). Maintained on semi-closed circuit inhalation of 1-3% isoflurane.
Antibiotic: Enrofloxacin (5mg/kg IV, surv group)
Post-op follow-up
Survival (days): ≥ 1
Diet/Meds: Regular diet from POD1. Flunixin meglumine 1.1mg/kg IV & topical 25μg fentanly patch following surgery. Ranitidine 150mg (2xday orally).
Observations: Monitored closely 2x day.
Endoscopy: No 'second-look' peritoneal endoscopy to minimise contamination.
Necropsy: 5 euthanised immediately & 3
Instrumentation
GIF Q140; GIF 2T100; Needle knives (Huibregtse RAMP needle-knife; WCMI); ; oesophageal overtube (Oly); Endoscopic forceps, Snares,
Surgical procedure Transluminal access Site access & prep: Orally inserted gastroscope used to insert overtube into oesophagus. Stomach lavaged with sterile water until free of food particels, then decompressed & instilled with cefazoliln (1g in 200mL saline) for 10min then aspirated. Incision site: Anterior wall (minimise spillage of gastric contents & provide optimal visualisation of peritoneal cavity). Incision method: Needle-knife used to make 5-10mm gastrotomy. If required, incision dilated with 15mm through-the-scope balloon. Pneumoperitomeum created with endoscope insufflation port & moderated with 16-gauge venting catheter.
Intervention Abdominal exploration performed using standard endoscopic techniques (rotation, torque, retroflection) aided by external transillumination. Omentum pierced with needle-knife as needed & exploration begun with tight retroflection. Gastric site, parietal peritoneum & small bowel examined. Pig placed in head-low, left or right lateral position for examining some parts of SI & colon. 45° head-low position used to displace intestinal loops & enable assessment of pelvic structures. Urinary bladded & uterus ID'd. Uterine horns followed with grasping forceps inserted through endoscope to reveal body of uterus (medial) & ovaries (lateral). Left or right lateral position used to display ovary for resection. Endoloop placed around ovary, ipsilateral tube & mesosalpinx. Tubectomy with oophorectomy performed using snare cautery above endoloop. Snare caurtery then used to remove uterine horn & body after endoloop placement. Retraction & viscerotomy closure Guidewire placed through gastrotomy, pneumoperitoneum evacuated & specimins & endoscope withdrawn through mouth.Endoclips & endoloops used to secure incision edges together & close gastrotomy.
Procedural Success/Complications Incision: Proximal anterior gastric wall provided most reliable peritoneal access.
Visualisation: Abdomen & pelvis: successfully explored in 8/8 pigs. Stomach, liver, small bowel, coon, urinary bladder, uterus, fallopian tubes, ovaries: easily identified in 8/8 cases. Parietal peritomeum: able to be thoroughly examined in all cases. Gallbladder: identified in 5/9 pigs*. Spleen: Tip seen in 8/8 pigs but tip couldn't be evaluated. Retroperitonel organs (duodenum, pancreas & kidneys): not identified.
Manoeuvrability: NR
Intervention: Partial hysterectomy & ipsilateral oophorectomy successfully performed in 6 animals & confirmed by necropsy. Uterine lumen secured by placing endoloop before restriction & by snare cautery, thereby minimising complications such as bleeding & infection. Complete uterine horn & body resected in 2 cases, but body transected with removal of proximal segment & 1 horn in 4. No complications noted.
Complications Bleeding: 0/8
Organ Injury: 0/8 (no damage to abdominal viscera)
Infection Related Complications: Adhesions: NR
Infection/ peritonitis/ abscesses/inflammation: 0/3
Ulceration: NR
Recovery & survival Number survived: 3/3
General observations: Ambulated freely & exhibited normal behaviour without signs of distress.
Appetite & weight gain: Tolerated regular diet.
Wound Healing: NR
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
125
Endoloops, Endoclips (Oly); Dilatation balloons (CRE, MEBS) Instrument Prep:
Sterilised with 2.4% gluteraldehyde & air-dried.
Retraction & viscerotomy closure: 6/6
Operative Time: NR
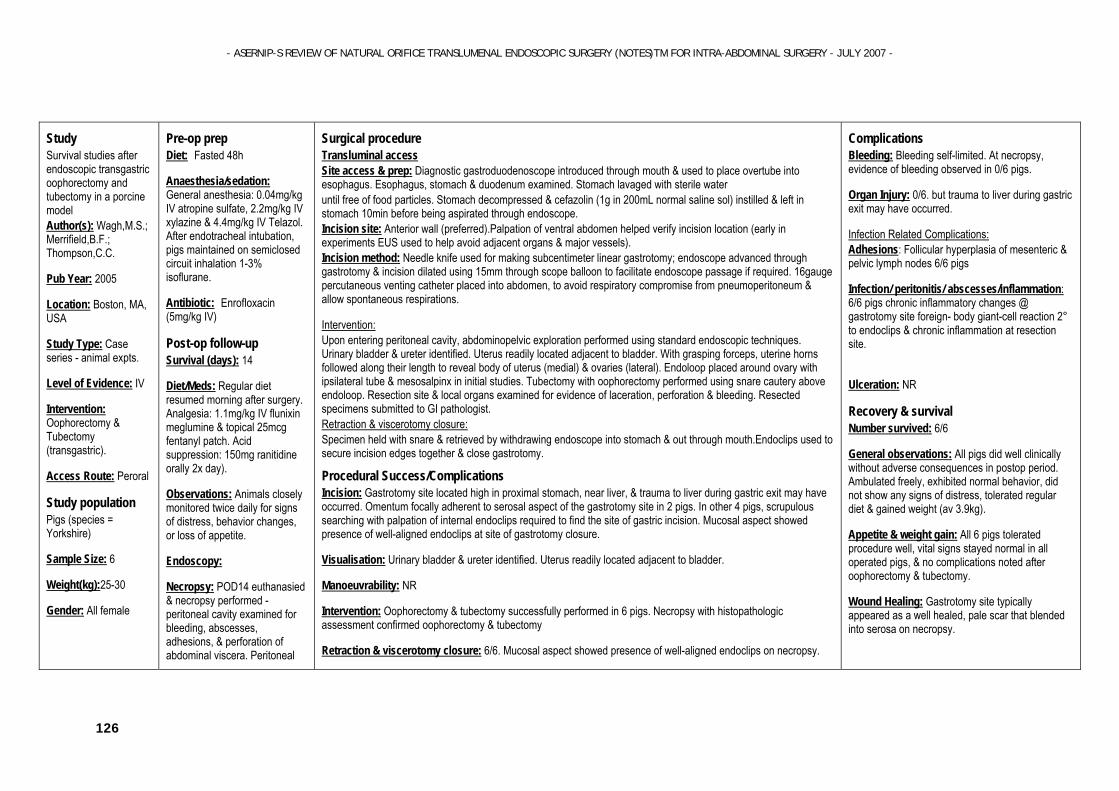
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
126
Study Survival studies after endoscopic transgastric oophorectomy and tubectomy in a porcine model Author(s): Wagh,M.S.; Merrifield,B.F.; Thompson,C.C.
Pub Year: 2005
Location: Boston, MA, USA
Study Type: Case series - animal expts.
Level of Evidence: IV
Intervention: Oophorectomy & Tubectomy (transgastric).
Access Route: Peroral
Study population Pigs (species = Yorkshire)
Sample Size: 6
Weight(kg):25-30
Gender: All female
Pre-op prep Diet: Fasted 48h
Anaesthesia/sedation: General anesthesia: 0.04mg/kg IV atropine sulfate, 2.2mg/kg IV xylazine & 4.4mg/kg IV Telazol. After endotracheal intubation, pigs maintained on semiclosed circuit inhalation 1-3% isoflurane.
Antibiotic: Enrofloxacin (5mg/kg IV)
Post-op follow-up
Survival (days): 14
Diet/Meds: Regular diet resumed morning after surgery. Analgesia: 1.1mg/kg IV flunixin meglumine & topical 25mcg fentanyl patch. Acid suppression: 150mg ranitidine orally 2x day).
Observations: Animals closely monitored twice daily for signs of distress, behavior changes, or loss of appetite.
Endoscopy:
Necropsy: POD14 euthanasied & necropsy performed - peritoneal cavity examined for bleeding, abscesses, adhesions, & perforation of abdominal viscera. Peritoneal
Surgical procedure Transluminal access Site access & prep: Diagnostic gastroduodenoscope introduced through mouth & used to place overtube into esophagus. Esophagus, stomach & duodenum examined. Stomach lavaged with sterile water until free of food particles. Stomach decompressed & cefazolin (1g in 200mL normal saline sol) instilled & left in stomach 10min before being aspirated through endoscope. Incision site: Anterior wall (preferred).Palpation of ventral abdomen helped verify incision location (early in experiments EUS used to help avoid adjacent organs & major vessels). Incision method: Needle knife used for making subcentimeter linear gastrotomy; endoscope advanced through gastrotomy & incision dilated using 15mm through scope balloon to facilitate endoscope passage if required. 16gauge percutaneous venting catheter placed into abdomen, to avoid respiratory compromise from pneumoperitoneum & allow spontaneous respirations.
Intervention: Upon entering peritoneal cavity, abdominopelvic exploration performed using standard endoscopic techniques. Urinary bladder & ureter identified. Uterus readily located adjacent to bladder. With grasping forceps, uterine horns followed along their length to reveal body of uterus (medial) & ovaries (lateral). Endoloop placed around ovary with ipsilateral tube & mesosalpinx in initial studies. Tubectomy with oophorectomy performed using snare cautery above endoloop. Resection site & local organs examined for evidence of laceration, perforation & bleeding. Resected specimens submitted to GI pathologist. Retraction & viscerotomy closure: Specimen held with snare & retrieved by withdrawing endoscope into stomach & out through mouth.Endoclips used to secure incision edges together & close gastrotomy.
Procedural Success/Complications Incision: Gastrotomy site located high in proximal stomach, near liver, & trauma to liver during gastric exit may have occurred. Omentum focally adherent to serosal aspect of the gastrotomy site in 2 pigs. In other 4 pigs, scrupulous searching with palpation of internal endoclips required to find the site of gastric incision. Mucosal aspect showed presence of well-aligned endoclips at site of gastrotomy closure.
Visualisation: Urinary bladder & ureter identified. Uterus readily located adjacent to bladder.
Manoeuvrability: NR
Intervention: Oophorectomy & tubectomy successfully performed in 6 pigs. Necropsy with histopathologic assessment confirmed oophorectomy & tubectomy
Retraction & viscerotomy closure: 6/6. Mucosal aspect showed presence of well-aligned endoclips on necropsy.
Complications Bleeding: Bleeding self-limited. At necropsy, evidence of bleeding observed in 0/6 pigs.
Organ Injury: 0/6. but trauma to liver during gastric exit may have occurred.
Infection Related Complications: Adhesions: Follicular hyperplasia of mesenteric & pelvic lymph nodes 6/6 pigs
Infection/ peritonitis/ abscesses/inflammation: 6/6 pigs chronic inflammatory changes @ gastrotomy site foreign- body giant-cell reaction 2° to endoclips & chronic inflammation at resection site.
Ulceration: NR
Recovery & survival Number survived: 6/6
General observations: All pigs did well clinically without adverse consequences in postop period. Ambulated freely, exhibited normal behavior, did not show any signs of distress, tolerated regular diet & gained weight (av 3.9kg).
Appetite & weight gain: All 6 pigs tolerated procedure well, vital signs stayed normal in all operated pigs, & no complications noted after oophorectomy & tubectomy.
Wound Healing: Gastrotomy site typically appeared as a well healed, pale scar that blended into serosa on necropsy.
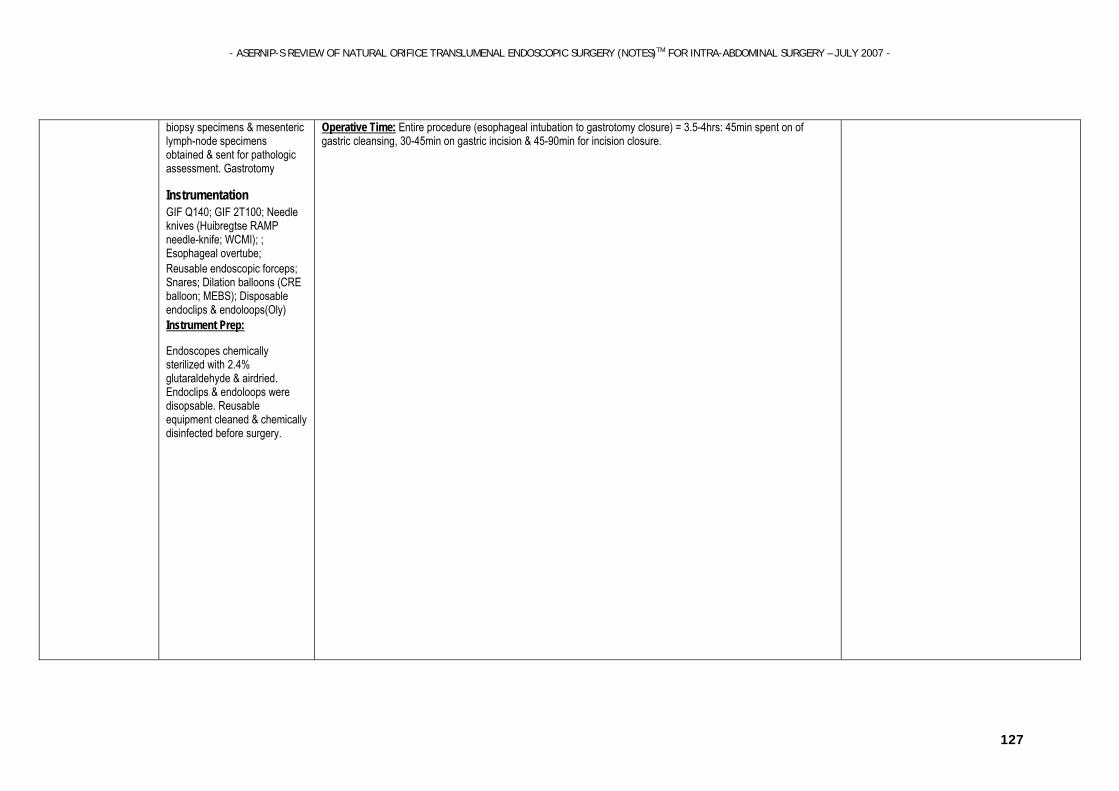
- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY – JULY 2007 -
127
biopsy specimens & mesenteric lymph-node specimens obtained & sent for pathologic assessment. Gastrotomy
Instrumentation
GIF Q140; GIF 2T100; Needle knives (Huibregtse RAMP needle-knife; WCMI); ; Esophageal overtube; Reusable endoscopic forceps; Snares; Dilation balloons (CRE balloon; MEBS); Disposable endoclips & endoloops(Oly) Instrument Prep:
Endoscopes chemically sterilized with 2.4% glutaraldehyde & airdried. Endoclips & endoloops were disopsable. Reusable equipment cleaned & chemically disinfected before surgery.
Operative Time: Entire procedure (esophageal intubation to gastrotomy closure) = 3.5-4hrs: 45min spent on of gastric cleansing, 30-45min on gastric incision & 45-90min for incision closure.

- ASERNIP-S REVIEW OF NATURAL ORIFICE TRANSLUMENAL ENDOSCOPIC SURGERY (NOTES)TM FOR INTRA-ABDOMINAL SURGERY - JULY 2007 -
128