Embed Size (px)
Citation preview

ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 12, No. 3 Copyright © 1982, Institute for Clinical Science, Inc.
Necrotizing Enterocolitis of the NewbornLAURENCE E. BRISKI, M.D.,* VOLLRAD VON BERG,
and JAMES J. HUMES, M.D.*Departments of *Pathology and f Surgery,
St. John Hospital, Detroit, MI 48236
ABSTRACTThe clinical presentation, diagnostic features, therapeutic measures, and
results of treatm ent of 29 infants with the firmly established diagnosis of necrotizing enterocolitis are reviewed. A cohort of control patients are studied in an attempt to identify risk factors which may predispose infants to develope this serious complication of the newborn period. The incidence of necrotizing enterocolitis in our series is 1.2 per 1000 live births, similar to that reported by other investigators. The prognosis is particularly grave in infants of very low birth weight and among those who exhibit radiographic evidence of portal venous air or who develop disseminated intravascular coagulation.
IntroductionSince its original description in 1891
by Genersich,6 necrotizing enterocolitis (NEC) has gained recognition as a serious and frequently fatal disorder affecting newborn infants. The first comprehensive reports on NEC appeared in 1965 from Babies Hospital, New York10 with the first significant surgical experience recorded from that same institution in 1967.15 With the advent of neonatology and the institution of neonatal intensive care units, NEC has come to the forefront among problems afflicting young infants, as evidenced by the plethora of articles appearing in the pediatric and surgical literature by the mid-1970’s.
The purpose of this paper is to describe our experience with the diagnosis, clinical manifestations, management, and outcome of NEC, the pathogenesis of which is poorly understood. In order to gain insight into the etiology and obtain information about possible predisposing factors, clinical data from affected infants and from a control group are compared.Patients and Methods
St. John Hospital is a 550 bed acute care hospital, with a 26 unit neonatal intensive care facility serving northeast Detroit and its neighboring suburbs. From January, 1975 through December, 1980,2,861 neonates were admitted to our intensive care unit. All charts with a discharge diagnosis
1860091-7370/82/0500-0186 $01.20 © Institute for Clinical Science, Inc.

NECROTIZING EN TEROCOLITIS O F TH E NEW BORN 187of necrotizing enterocolitis during this study period were reviewed. A case was accepted as NEC if there was (1) pathologic conformation of NEC from surgical or autopsy specimens, or (2) radiographic evidence of pneumatosis intestinalis and one or more of the following: (a) abdominal distention, (b) vomiting or regurgitation, (c) guaiac positive or grossly bloody stools. Forty charts were reviewed and utilizing the previously mentioned criteria, 29 cases were accepted as NEC. It should be emphasized that the 11 patients rejected for the purpose of this study have shown all or part of the clinical picture of NEC, but they failed to demonstrate roentgen evidence of pneumatosis intestinalis. This group represents an important and significant num ber of infants in whom the diagnosis was suspected and medical therapy instituted before the full blown syndrome developed. However, without more objective evidence of NEC, it is difficult to assess accurately these patients; therefore, they were omitted from this review.
A control group was developed by selecting infants admitted to our neonatal intensive care unit (NICU), in whom the diagnosis of NEC was never entertained, within one month of each patient with NEC, providing their birthweight was within 75 grams of the patient under study. This created a control group comparable in weight, gestational age, and sex to the study group and obviated any changes in the nursery or house staff environment. Wherever possible, two controls were selected for each patient w ith NEC. However, in some instances only one control could be found, resulting in a control group of 44 patients.12
ResultsP a t i e n t P o p u l a t i o n
There were 19 males and 10 females with NEC among the 2,861 infants, repre
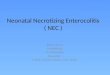
46004400420040003800360034003200
£j 3000 O —h co 2800 U E¡3 2 2600O' ~ 2400 « 2 2 0 0
2000
1800 1600 1400 1200
1000
800 600 400 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44
GESTATIONAL AGE (weeks)
• Definite necrotizing enterocolitis ▲ Suspect necrotizing enterocolitis
F i g u r e 1. A g e -w e ig h t re la t io n s h ip o f in fa n ts w ith n e c ro tiz in g e n te ro c o l it is .
senting 1.0 percent of the total admissions to our NICU during the half-decade from 1975 through 1980. During the same period, there were 9,916 live births at St. John Hospital, including 12 of the patients with NEC, yielding an incidence of1.2 cases per 1000 live births. This is identical to the projected annual incidence in the U.S. based on an informal survey of 31 neonatal intensive care units in the U.S. and Canada from 1975 through 1977.
Twenty-four patients (82.8 percent) were "born prematurely (less than 38 weeks gestation) and were of low birthweight; only five infants weighed more
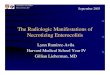
F ig u r e 2. A ge a t o n s e t o f n e c ro tiz in g e n te ro c o l it is .

188 B R IS K I, V O N B E R G , A N D H U M E S
T A B L E I
Perinatal Complications
Percent of Patients Statistical NEC Controls Significance
Complication (n=29) (n=44) (p)
Rupture of membranes > 24 hours
34.5 22.7 NS
Breech delivery 10.3 20.4 NSCesarian section 17.2 13.6 NSPlacenta praevia 6.9 11.4 NSAbruptio placenta 6.9 11.4 NSBirth asphyxia 48.3 52.3 NSApgar < 7 at 48.3 56.8 NS
1 minute
NEC = Necrotizing enterocolitis NS = Not significant
than 2,500 grams (figure 1). This did not differ significantly from the control group. The mean age at onset of NEC was 7.3 days (range 1 to 37), with nearly two- thirds occurring during the first week of life (figure 2).
P e r i n a t a l C o m p l i c a t i o n s
The incidence of perinatal complications was high; in only six patients was the delivery and immediate postpartum pe-
T A B L E II
Postnatal Complications
Percent of Patients Statistical NEC Controls Significance
Complication (n=29) (n=44) (P)
RDS 79.3 90.9 NSHeadbox < 40 per 41.3 40.9 NScent FIO2Keadbox > 40 per 17.2 22.7 NScent FIO2CPAP 24.1 20.5 NSVentilator 18.2 15.9 NS
Apnea 44.8 40.9 NSPatent ductuc 37.9 20.5 NS
arteriosusExchange trans 6.9 2.3 NS
fusionUAC 48.3 36.4 NS
Above renal 42.9 43.7 NSartery
Enteric feedings 79.3 78.1 NS
NEC = Necrotizing enterocolitis RDS = Respiratory distress syndrome NS = Not significantCPAP - Continuous positive airway pressure UAC = Umbilical artery catheterization
riod recorded as normal. Birth asphyxia, requiring bagging and resuscitation in the delivery room, occurred in 14 patients (48.3 percent). Low apgar ratings were also recorded in 14 patients, 11 of whom required immediate resuscitation. Premature rupture of membranes more than 24 hrs prior to delivery occurred in 10 patients (34.5 percent). Other complications included a relatively high percentage of Cesarean sections (17.2 percent), breech deliveries (10.3 percent), placenta praevia (6.9 percent), and abruptio placenta (6.9 percent). However, when compared to the control group, no signficant difference was recorded among these perinatal risk factors (table I).P o s t n a t a l C o m p l i c a t i o n s
Postnatal complications were commonly encountered (table II). Respiratory distress syndrome of sufficient severity to require various degrees of ventilatory support and recurrent apnea occurred with similar frequency in both groups. Although the incidence of patent ductus arteriosus (37.9 percent) and umbilical artery catheterization (48.3 percent) was greater in the NEC group as compared to the control group (20.5 percent and 36.4 percent, respectively), this difference was not statistically significant (p > 0.05). Twenty-three patients (79.3 percent) were receiving oral feedings until the onset of NEC. On the same day of life that symptoms developed, 78.1 percent of the age weight matched control group were also receiving oral feedings. Most of the infants in both groups were fed 20 calories per ounce of standard commercial formula averaging 12 ml per kg every three hours.C l i n i c a l P i c t u r e
The disease was characterized by a pattern of poor feeding, recurrent apnea, and lethargy, associated frequently with abdominal distention and occult blood loss from the gastrointestinal tract in an infant apparently recovering from a stressful

N E C R O T IZ IN G E N T E R O C O L IT IS O F T H E N E W B O R N 189perinatal period (table III). Clinical signs of perforation with or w ithout peritonitis, sepsis, and disseminated intravascular coagulation (DIC) developed in infants with advanced disease (table IV).
Routine antemortum cultures of the stool were performed in all patients and were consistently negative for pathogens. Blood cultures were positive in 11 infants (37.9 percent) with Klebsiella pneumoniae recorded in five, E. coli in three, Enterobacter cloace in one, Streptococcus bovis in one, and Micrococcus in one. However, in no instance did septicemia precede the onset of abdominal symptoms in patients with NEC. Peritoneal fluid cultures had a similar distribution of organisms. The DIC occurred in seven patients, as evidenced by worsening anemia, thrombocytopenia, prolonged prothrombin time, and partial thromboplastin time. This event had ominous portent as six of the infants expired.R o e n t g e n F i n d i n g s
In order of decreasing frequency, the radiographic findings included: (1) pneumatosis intestinalis, (2) pneumoperitoneum, and (3) portal venous gas (table III).
Pneumatosis intestinalis is a pathognomic sign of NEC, particularly in the clinical setting described, and occurred in86.2 percent of patients. The radiographic pattern consisted of bubble-like collections of gas or diffuse linear stripes along distended loops of bowel. In most instances, this finding was localized to the region of the terminal ileum and cecum, but on occasion, the entire small intestine and/or colon was involved.
Pneumoperitoneum occurred with much less frequency, but is an important finding and is indicative of intestinal perforation. In some instances, it was demonstrated on the first roentgen examination, while in others, it followed the development of pneumatosis intestinalis.
Portal venous gas is a serious sign, usually seen in the most seriously affected
T A B L E III
Clinical and Radiographic Manifestations of 29 Infants with Necrotizing Enterocolitis
Number Percent
Abdominal distention 22 75.9GI blood loss 1 2 41.4Emesis/regurgitation 8 27.6Abdominal X-ray
Pneumatosis intestinalis 25 8 6 . 2
Pneumoperitoneum 8 21.6Portal venous air 7 24.1Obstructive pattern 1 3.4
infants, and is easily identified by its arborizing pattern over the liver. This finding was demonstrated in seven patients, five of whom died.P a t h o l o g y
There is considerable variability in both the distribution and severity of the pathologic lesions characteristic of NEC. Lesions have been reported in all parts of the gastrointestinal tract with the exception of the duodenum .13 In our series, as in others, the most common sites of involvem ent were the terminal ileum, cecum and ascending colon (table V).
Grossly, the involved intestine appeared dilated and hemorrhagic, dusky gray to frankly necrotic, depending upon the severity of involvement. The adjacent segments of bowel, which seemed well perfused and viable in many instances, demonstrated variable degrees of friabil-
T A B L E IV
Complications of Necrotizing Enterocolitis in 29 Infants
Complication Number Percent
Intestinal perforation 12 41.4Peritonitis 1 2 41.4Sepsis 1 1 37.9DIC 7 24.1Shock 5 17.2Pneumonitis 2 6.9Intestinal obstruction 1 3.4Death 1 0 34.5
DIC = Disseminated intravascular coagulation

190 B R IS K I, V O N B E R G , A N D H U M E S
TABLE VSites of Involvement*
Site Number Percent
Esophagus 0 0 . 0Stomach 1 5.3Duodenum 0 0 . 0
Jejunum 3 15.8Ileum 17 89.5Appendix 4 2 1 . 0
Cecum 15 78.9Ascending colon 1 1 57.9Transverse colon 5 26.2Descending colon 2 10.5Rectum 0 0 . 0
*Based on surgical/autopsy findings in 19 cases.
ity, making it difficult to judge the extent of involvement at the time of surgery. Perforations were encountered most commonly in the terminal ileum, where the intestinal wall is extremely thin. The serosa and mesentary in the areas of perforation were covered by a fibrinopurulent exudate.
The earliest microscopically recognizable lesion was bland necrosis of the superficial mucosa, in some cases associated with mucosal and submucosal hemorrhage. With increasing severity and duration of the disease, there was evidence of mucosal ulceration, with involved areas often covered by a meshwork of fibrin, necrotic debri and bacteria (figure 3), ultimately progressing to transmural infarction (figure 4). In addition, intramural
TABLE V ISurgical Complications in 17 Infants With
Necrotizing Enterocolitis
Complication Number Percent
Intestinal obstruction Adhesions 3 17.6Stomal stenosis 2 1 1 . 8Stricture 1 5.9
Short bowel syndrome 3 17.6Incisional abscess 6 35.3Peritoneal abscess 1 5.9Evisceration 1 5.9
gas filled cysts (pneumatosis) were commonly encountered within the necrotic regions (figure 5) as well as the submucosa beneath more viable mucosa. Occasionally, reactive fibrosis of the submucosa was seen beneath areas of active mucosal degeneration, suggestive of early healing and repair.
T r e a t m e n t a n d Su r v iv a l
All 29 patients received intensive supportive and medical therapy, which included cessation of oral feedings as soon as the diagnosis was suspected, nasogastric decompression, intravenous fluids, careful attention to acid base and electrolyte balance, and parenteral broad-spec- trum antibiotics. Some infants also required hyperalimentation to maintain body weight and positive nitrogen balance.
An important and essential part of the management included repeated gentle abdominal examination and frequent radio- graphic studies with the aim of initiating operative intervention at the earliest sign of peritonitis or localized disease. Persistent and unexplained hypoglycemia, apnea and/or bradycardia often antecede the development of frank NEC. Radiographic or clinical evidence of perforation in most cases mandates immediate surgery. Other indications for surgery included gastrointestinal hemorrhage and obstruction.
Six patients responded to medical management and did not require surgery. Another infant, successfully managed medically, developed an intestinal stricture as a late sequelae, necessitating operation. Five patients died without benefit of surgery, four of whom were deem ed too ill to subject to operation prior to their deaths. If one includes these four infants in the medical-treatment-only group, the survival would be 58.3 percent.
Seventeen patients were operated upon during the acute phase of their illness. There were five postoperative deaths, resulting in a survival rate of 70.6 percent.

N E C R O T IZ IN G E N T E R O C O L IT IS O F T H E N E W B O R N 191
F ig u r e 3. Cross-section through small intestine (6- day-old infant) shows mucosal ulceration and dense polymorphonuclear leukocytic infiltrate adjacent to more viable mucosa (32 x ).
F ig u r e 4. Cross-section through small intestine (7-day-old infant) shows transmural infarct. Necrotic, ulcerated mucosa covered by fibrinopurulent exudate, composed of fibrin, necrotic cell debri and bacteria. Dense infiltrate of polymorphonuclear leukocytes involves entire thickness of bowel wall (32 x).

192 B R IS K I, V O N B E R G , A N D H U M E S
F ig u r e 5. C ro ss-sec tio n th ro u g h sm all in te s t in e (7- d a y -o ld in fa n t) re v e a ls is c h e m ic n e c ro s is a n d h e m orrh ag e in v o lv in g m ucosa. Sm all a re a of p n e u m a to s is is s e e n in th e su b m u c o sa (3 2 x ) .
The operative procedure in all 17 infants included resection of visably diseased intestine and peritoneal lavage in those patients with perforation. A proximal decompressing enterostomy or colostomy with a distal mucus fistula was created in all infants. Continuity of the bowel was reestablished at a later date, after all signs and symptoms of disease disappeared.
Six survivors went on to develop intestinal obstruction,—three secondary to intra-abdominal adhesions, one due to stricture (all required reoperation) and two because of stromal stenosis. Short bowel syndrome occurred in three patients, one of whom died because of failure to thrive. Other complications included incisional abscess in six patients, peritoneal abscess in one, and evisceration in another (table VI).
Overall, 19 of 29 patients or 65.5 percent survived. The results related to birthweight are summarized in table VII. Eighty percent of deaths occurred in infants under 1,500 g, and there were no
survivors among patients under 1,000 g in either group.Conclusion
Necrotizing enterocolitis is recognized as a serious and frequently fatal condition affecting the newborn infant. Premature infants of low birthweight experiencing significant stress during the perinatal and immediate postpartum period appear to be particularly prone to develop this disease. An acute awareness of the symptom complex mentioned previously with prompt institution of therapy is essential for survival.
The pathogenesis of NEC is poorly understood. A variety of factors have been implicated in the etiology of this disease, including a congential defect in the intestinal wall,4 bacterial enteritis resulting from ingestion of infected amniotic fluid,2 lysozyme deficient diet,10 or a localized Schwartzman reaction related to the formation of endotoxins by gram-negative

N E C R O T IZ IN G E N T E R O C O L IT IS O F T H E N E W B O R N 193TABLE V I I
R e s u lts R e la ted to B ir th w e ig h t
Birthweight (gm) No.Survived
Operation No Operation
< 1 0 0 0 3 0 of 2 0 of 1
1000 - 1500 13 5 of 8 3 of 51501 - 2500 8 5 of 5 3 of 3> 2500 5 2 of 2 1 of 3Total 29 12 of 17 7 of 12Percent survived 65.5 70.6 58.3
bacteria in the intestine.5 Theories implicating these factors have been abandoned in favor of more recent hypothesis suggesting “selective circulatory ischemia,” 3,7’8’9’16 deficient secretory IgA in formula-fed infants,1,11 and bacerial col- onziation of the bowel in the presence of a nutrative substrate.1
This study neither supports or disproves the current theories as to the etiology of NEC. The cause appears to be multifaceted. Why some infants develop NEC and others experiencing similar perinatal and postnatal complications do not, remains an enigma to those devoted to the treatm ent and management of the newborn infant.
References1. B a r l o w , B ., Sa n t u l l i , T. V., H e i r d , W. C., e t
AL: An Experimental study of acute necrotizing enterocolitis—The importance of breast milk. J. Pediatr. Surg. 9:587, 1974.
2. B l a n e , W. A.: Amniotic infection syndrome: Pathogenesis, morphology, and significance in circumnatal mortality. Clin. Obstet. Gynecol. 2:705, 1959.
3. B u r t o n , G. L., D u r b i n , M . G., M c I n t o s h , N., ET AL: Necrotizing enterocolitis, controlled
study of 3 years’ experience in a neonatal intensive care unit. Arch. Dis. Child. 52:772, 1977.
4. F i s c h e r , A. E.: Fetal peritonitis: Report of a case following spontaneous rupture of the large intestine. Amer. J. Dis. Child. 36:774, 1928.
5. H e r m a n , R. E.: Perforation of the colon from necrotizing colitis in the newborn: Report of a survival and a new etiologic concept. Surgery 58:436, 1965.
6. G e n e r s i CH, A.: Bauchfellent ziindung beim Neugebornen in Folge von Perforation des Ileums. Arch. f. Path. Anat. Berlin cxxvi:485- 494, 1891.
7. Jo s h i , V. V., D r a p e r , D . A., and B a t e s , R. D.-. Neonatal necrotizing enterocolitis, occurrence secondary to thrombosis of abdominal aorta following umbilical arterial catheterization. Arch. Pathol. 99:540, 1975.
8. K i t t e r m a n , J. A.: R oss Conference on Pediatric Research: Necrotizing enterocolitis in the newborn infant. Ross Labs., Columbus, O H , 1975, p. 38.
9. L l y o d , J. R.: The etiology of gastrointestinal perforation in the newborn. J. Pediatr. Surg. 4:77, 1969.
10. M i z r a h i , A ., B a r l o w , O ., B e r d o n , W., e t a l : Necrotizing enterocolitis in premature infants. J. Pediatr. 66:697, 1965.
11. P i t t , J., B a r l o w , B ., and H e i r d , W. C.: Macrophages and the protective action of breast milk in necrotizing enterocolitis. Pediatr. Res. 8:384,1974.
12. R o b a c k , S. A., F o k e r , J., F r a n t z , I. F ., e t a l : Necrotizing enterocolitis. An emerging entity in the regional infant intensive care facility. Arch. Surg. i09:314, 1974.
13. S a n t u l l i , T. V., S c h u l l i n g e r , J. N., H e i r d , W. C., ET AL: Acute necrotizing enterocolitis in infancy: A review of 64 cases. Pediatrics 55 :376,1975.
14. S w e e t , A. Y.: Epidemiology. Monographs in Neonatology, Necrotizing Enterocolitis. Brown, E. G. and Sweet, A. Y., eds. New York, Grune and Stratton, 1980, p. 11.
15. T o u l o u k ia n , R. J., B e r d o n , W. E., A m o u r y , R. A ., and Sa n t u l l i , T. V.: Surgical experience with necrotizing enterocolitis in the infant. J. Pediatr. Surg. 2:389, 1967.
16. T o u l o u k ia n , R. J., P o s c h , J. N., a n d Sp e n c e r , R. P .: T h e p a th o g e n e s i s o f i s c h e m ic g a s tro - e n te r o c o l i t i s o f t h e n e o n a te ; s e le c t iv e g u t m u c o s a l i s c h e m ia in a s p h y x ia te d n e o n a ta l p ig le t s . J. P e d ia t r . S u rg . 7:194, 1972.