Embed Size (px)
Citation preview

Table of Contents
Neonatal Abstinence Syndrome: 2019 Report
Bureau of Epidemiology
June 2021

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 2
Table of Contents 2
Introduction 3
Methods 3
Findings 5
Data Limitations 18
Discussion 19
Citations 23

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 3
Introduction
Neonatal Abstinence Syndrome (NAS) is a newborn withdrawal syndrome due to prenatal exposure to opioids, benzodiazepines, and barbiturates. It can cause a range of symptoms including body tremors, increased muscle tone, gastrointestinal dysfunction, poor feeding, and more. In addition to having withdrawal signs, babies with NAS are at increased risk of low birth weight, jaundice, seizures, and sudden infant death syndrome.1 The national NAS incidence rate increased approximately 433% from 1.5 per 1000 live births in 2004 to 8.0 per 1000 live births in 2014.2 NAS surveillance, including in Pennsylvania, has typically relied on the retrospective review of hospital discharge data. This results in a delay in the prompt allocation of public health resources to high burden areas. Although several states have implemented mandated reporting of NAS from medical facilities to state health departments, differences in reporting methods and case definitions limit interstate data comparisons.2 Neonatal Abstinence Syndrome in Pennsylvania On January 10, 2018, Governor Wolf declared a 90-day disaster emergency for the opioid epidemic. With this declaration, NAS related to opioid use became a reportable condition to the Pennsylvania Department of Health (Department) per Chapter 27 of the Pennsylvania Health and Safety code, and rapid case ascertainment was requested. The purpose of the NAS surveillance initiative was to provide de-identified aggregated data for state and local responders to identify high incidence areas for targeted intervention to reduce the burden of NAS in the state. Since the initial emergency declaration, 13 subsequent renewals have been issued to continue the overall efforts towards preventing new addictions and improving outcomes for those affected by the opioid epidemic. The most recent extension occurred on May 7, 2021. This report summarizes the second calendar year of this initiative and includes data from NAS infants born between January 1 and December 31, 2019. Data from the first calendar year of NAS reporting (infants born January 10 through December 31, 2018) is available in the 2018 NAS annual report on the Department’s “Opioid Epidemic” webpage within the “Providers and Prescribers” weblink.3
Methods
To achieve rapid case ascertainment, the Bureau of Epidemiology instituted a web-based reporting system (REDCap Cloud) so employees within birthing facilities and pediatric hospitals could report NAS cases electronically to the Department in near real-time. To standardize reporting, a NAS surveillance case definition was developed after a thorough literature review and consultation with other state health departments.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 4
Due to the limited authority under the governor’s opioid emergency declaration, the NAS case definition was limited to those infants with opioid exposure and did not include infants who may experience NAS due to exposure to other drugs. Only symptomatic infants were included in this case definition; asymptomatic infants were excluded. The final case definition used in Pennsylvania was established as:
• A newborn with a clinical diagnosis in the neonatal period (birth up to 28 days of life) who has symptoms of withdrawal because of prenatal exposure to opiate drugs, either via prescription, medical therapy (MAT), or illegal use (ICD-10 codes P96.1 and P04.49 only, if available);
• A resident of Pennsylvania (only infants born to mothers who resided in Pennsylvania before the baby's birth); and
• An infant born on or after 1/10/2018. A one-page case report form was developed and implemented in REDCap Cloud in January 2018. The variables required for report on the case report form were limited to the most vital demographic and clinical information to facilitate hospitals’ abilities to comply with the reporting guidelines and to provide more timely and consistent reporting. Therefore, data collection were centered upon infant health parameters, and parameters about the maternal characteristics were limited. Variables like length of stay, cost, and types of treatment over the duration of a stay were not collected due to the rapid case ascertainment process and desire to receive the report form early in the birth hospitalization process. Concurrent with the development of the case report form, a Department of Health team contacted all target facilities via phone call to confirm names and contact information of managers within all newborn nurseries or neonatal intensive care units (NICU), and these managers became the initial contact points for the dissemination of the new reporting information. Using these contacts, the case reporting guidance and a frequently asked questions (FAQs) document were provided via email in February 2018 to 93 birthing facilities. Two additional facilities were added shortly after the initial guidance release. In addition to the direct contact with facility staff, information was distributed via The Hospital and Healthsystem Association of Pennsylvania (HAP) to help disseminate reporting details to other potentially relevant staff. Case reporters and nursery managers were contacted via email approximately every 90 days to provide updated reporting periods, data summaries, and updated FAQs, as previous emergency declaration renewals expired and new emergency declaration periods began. On January 1, 2020, NAS case reporting changed from the REDCap Cloud weblink to a new NAS module in the existing newborn screening data collection system. Due to the time lag between an infant’s birth and NAS reporting, infants with NAS born at the end of 2019 were reported into the new system. All 2019 cases entered into the new system were combined with 2019 cases stored in REDCap for analysis after processing for variable and response agreement. Descriptive analysis by race and by geographic region were performed on all NAS cases. Analyses by geographic region were performed by county of the facility of birth and by county

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 5
of maternal residence to assess corresponding county needs. Statewide data for comparison was obtained from the latest available vital statistics data (2018). SAS Enterprise Guide 7.1 was used for data processing, and ArcGIS 10.4.1 for Desktop (ArcMap) was used for geocoding and map generation.
Findings
A total of 1,608 NAS cases were reported in 2019. Out of 94 birthing facilities and pediatric hospitals that received direct communication from the Department, 76 facilities (81%) attempted to report NAS cases, although some cases were excluded due to duplicate reporting or not meeting the inclusion criteria. In total, 75 facilities (80%) reported cases to the Department that met the case definition and were included in the final case count. There were 13 facilities that reported a total of 39 cases in 2018 but did not report any cases in 2019, including one facility that closed in 2018. In addition, three facilities which reported a total of five cases in 2019 did not report any cases in 2018. Reasons for facilities not reporting is unknown. These facilities may have had cases and not reported, or they may have had zero cases to report. Stratifying by race, 1321 (77%) cases were born to white non-Hispanic mothers, 112 (7%) to Black non-Hispanic mothers, 211 (13%) to other/unknown race/ethnicity, and 54 (3.4%) to Hispanic mothers. In total, 52% of infants with NAS were male (slightly higher than females at 48%), and 77% were born to mothers with race reported as being white non-Hispanic. Mothers of infants with NAS were 2.5 times more likely to have Medicaid as the primary payor for delivery than among statewide births (86% versus 35%).4 Infants with NAS were more than twice as likely to have low birthweight (less than 2,500 grams) compared to all infants born statewide in 2018 (19% versus 8%).4 While 18% of NAS cases were born prematurely (less than 37 weeks gestation), only 10% of 2018 statewide infants were born premature.4 Ninety-one percent of mothers of infants with NAS were reported to have received any prenatal care versus 98% statewide,4 more than half (51%) of NAS cases received care in a NICU, and 91% of infants with NAS had 3 or more symptoms of NAS. A greater percentage of infants born with NAS to mothers who were Hispanic or Black non-Hispanic were low birthweight and early gestational age (low birthweight: 30% and 28%, respectively; preterm: 28% and 30%, respectively) compared to infants born to mothers of white non-Hispanic or other/unknown race/ethnicity (low birthweight: 17% and 22%, respectively; preterm: 16% and 21%, respectively). Black non-Hispanic and Hispanic mothers less often received any prenatal care compared with white non-Hispanic and other/unknown race/ethnicity mothers. The percentage of infants receiving care in a NICU was approximately 41% higher for infants born to Hispanic or Black non-Hispanic mothers compared to infants of white non-Hispanic or other/unknown race/ethnicity mothers. Despite

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 6
infants born to Hispanic mothers more often receiving care in the NICU, these infants more often had a “normal” Apgar score (7 or greater) at one minute and at five minutes compared with infants born to white non-Hispanic mothers. An Apgar score is a test given to infants shortly after birth to evaluate specific health parameters and determine whether extra medical care is needed. Infants born to mothers of other/unknown race/ethnicity less often had normal Apgar scores and less often received care in the NICU in comparison to infants born to white or black non-Hispanic mothers. Table 1 shows characteristics of infants with NAS and their mothers. Table 1 – Demographic Characteristics and Birth Parameters of Infants with NAS Born in 2019
Parameter White Non-
Hispanic
Black Non-
Hispanic
Other/ Multiracial/
Unknown Race/
Ethnicity
Hispanic Total Cases
Statewide Births (2018)4
% Difference (NAS Cases vs Statewide)a
Population (n) 1231 112 211 54 1608 135 677 --
Percent of all NAS cases 77% 7% 13% 3% 100% -- --
Male infants 51% 54% 40% 63% 52% 51% 2%
Medicaid 86% 88% 83% 94% 86% 35% 146%
Low birthweight (<2500 grams) 17% 29% 21% 30% 19% 8% 138%
Preterm (<37 weeks) 16% 29% 21% 28% 18% 10% 80%
Received prenatal care 92% 85% 90% 83% 91% 98% -7%
Received care in NICU 49% 67% 46% 67% 50% -- --
Apgar 1 minute (≥ 7) 88% 88% 73% 93% 87% -- --
Apgar 5 minute (≥ 7) 94% 93% 89% 98% 93% -- --
3 or more NAS symptoms 90% 90% 92% 98% 91% -- --
SOURCE: Vital Statistics (Division of Health Informatics, Pennsylvania Department of Health, 2018);4 NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Reviewing infant testing and withdrawal assessment parameters, 88% percent of NAS cases were tested for laboratory evidence of prenatal drug exposure. Of those tested, 80% had a positive laboratory result indicating substance exposure. Non-positive test results in a child with NAS indicate that the mother’s opioid use is known through other means (self-report or other documented history). Non-positive results with known exposure often indicate that the drug of exposure was not included in the drug panel used for testing. Among infants with a positive lab result, 82% tested positive for opioids; 69% tested positive for drugs commonly associated with Medication Assisted Treatment (MAT); and 20% tested positive for opiates,
a Percent difference was obtained as ([percent NAS cases]-[percent statewide])/[percent statewide].

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 7
oxycodone, or fentanyl. Most infants (92%) were evaluated using a Finnegan or Modified Finnegan scoring method to assess the severity of withdrawal. Table 2 shows a summary of clinical assessment and laboratory testing data for infants with NAS. Of all infants with NAS who were tested for laboratory evidence of exposure, infants born to Black non-Hispanic mothers less frequently tested positive for opioids (72%) and for MAT-associated drugs (41%) than infants born to white non-Hispanic mothers (82% and 71% positive for opioids and MAT-associated drugs, respectively), other/unknown race/ethnicity mothers (90% and 78% positive for opioids and MAT-associated drugs, respectively), or Hispanic mothers (92% and 58% positive for opioids and MAT-associated drugs, respectively). Infants born to white non-Hispanic mothers less often tested positive for opiates, oxycodone, and fentanyl (17%) than infants born to Black non-Hispanic, other/unknown race/ethnicity, or Hispanic mothers respectively (32%, 23%, and 40%, respectively). Table 2 – NAS Assessment and Testing Characteristics
Testing or Assessment All NAS Cases
White Non-
Hispanic
Black Non-
Hispanic
Other/ Multiracial/
Unknown Race/
Ethnicity
Hispanic
Population (n) 1608 1231 112 211 54
Tested for laboratory evidence of substance exposure
Yes, results known 80% 77% 87% 87% 83%
Yes, results pending 9% 10% 5% 6% 7%
No, not tested 12% 13% 8% 7% 9%
Positive laboratory result (if tested and known)
82% 82% 84% 81% 84%
Of those testing positive, % positive for any form of opioid
83% 82% 72% 90% 92%
Of those testing positive, % positive for addiction treatment drugs
69% 71% 41% 78% 58%
Of those testing positive, % positive for opiates, oxycodone, or fentanyl
20% 17% 32% 23% 40%
Used Finnegan or Modified Finnegan scoring
92% 92% 96% 94% 98%
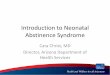
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Ninety-one percent of infants with NAS exhibited three or more NAS-related symptoms. The most commonly reported symptom was “overactive reflexes (twitching) and tight muscle tone” in 85% of infants followed by “body shakes (tremors)” (77%) and “trouble sleeping and lots of yawning” (57%). Seizures were reported in less than 1% of total cases, and although seizure rates appear to vary by race, case counts are low and rates are therefore unstable. Figure 1 displays symptoms observed in infants with NAS.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 8
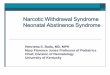
Infants with NAS may receive one or more types of treatment. The most commonly reported treatment was morphine (38% of infants). The second most common treatment reported was non-pharmacologic treatment, which may include breastfeeding and skin-to-skin care (35% of infants). Twenty-seven percent of infants were reported to have received no care specifically for NAS, and 12% of infants were reported as receiving pharmacologic treatment with a drug other than morphine. Figure 2 displays types of treatment received by infants with NAS. Figure 1 – Percent of NAS Infants Exhibiting Specific Symptoms by Race
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Figure 2 – Treatment Type for NAS Infants by Race
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019)

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 9
The percent of infants receiving non-pharmacologic treatments was 45% lower in infants born to other/unknown race/ethnicity mothers (20%) compared to other groups (36%, 44%, and 37% in white, Black non-Hispanic and Hispanic, respectively). While non-pharmacologic treatment was the most commonly used treatment in infants with Black non-Hispanic mothers, morphine was the most commonly used treatment in infants born to white non-Hispanic, other/unknown race/ethnicity, andHispanic mothers. “Other drug” was more often used for infants born to Black non-Hispanic mothers in comparison to other groups. Case Counts and Incidence Rates NAS case counts and incidence rates were aggregated or calculated by the county of reporting facility and by the county of maternal residence. NAS case counts and incidence rates were also aggregated by region using Pennsylvania’s community health districts (northcentral, northwest, northeast, southcentral, southwest, and southeast).b
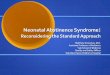
Case Counts by County of Facility Maps 1 and 2 depict the NAS cases by the location of the reporting facility. Map 1 shows NAS cases by location of the reporting facility at the county level. Map 2 shows NAS cases by location of the reporting facility at the regional level. Darker colored regions represent greater case counts, and larger red circles represent a greater number of facilities within the county or region. Facility counts on the map include facilities that received NAS reporting guidance regardless of whether they reported NAS cases. Case counts by county of facility ranged from zero to 338 cases in Allegheny County. A total of 25 (37%) counties had zero cases reported. Eighteen of the 25 counties did not have birthing hospitals or pediatric hospitals in 2019. Most counties with higher reported case counts also had more reporting facilities, although some, like Fayette, Washington, and Beaver in the southwest, had higher reported case counts with only one reporting facility in each county. Case counts by region ranged from 99 cases in the northcentral region to 501 cases in the southeast where the greatest number of facilities are located.
b Region Counties: Northcentral (NC): Bradford, Centre, Clinton, Columbia, Lycoming, Montour, Northumberland,
Potter, Snyder, Sullivan, Tioga, Union. Northeast (NE): Carbon, Lackawanna, Lehigh, Luzerne, Monroe, Northampton,
Pike, Susquehanna, Wayne, Wyoming. Northwest (NW): Cameron, Clarion, Clearfield, Crawford, Elk, Erie, Forest,
Jefferson, Lawrence, McKean, Mercer, Venango, Warren. Southcentral (SC): Adams, Bedford, Blair, Cumberland,
Dauphin, Franklin, Fulton, Huntingdon, Juniata, Lebanon, Mifflin, Perry, York. Southeast (SE): Berks, Bucks, Chester,
Delaware, Lancaster, Montgomery, Philadelphia, Schuylkill. Southwest (SW): Allegheny, Armstrong, Beaver, Butler,
Cambria, Fayette, Greene, Indiana, Somerset, Washington, Westmoreland.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 10
Map 1 – Neonatal Abstinence Syndrome Case and Facility Counts by County of Facility
NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Map 2 – Neonatal Abstinence Syndrome Case and Facility Counts by Region of Facility
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019)

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 11
Case Counts and Incidence Rates by County of Maternal Residence The overall NAS incidence rate in Pennsylvania is 11.9 cases per 1000 live births.c Maps 3 and 4 show case counts and incidence rates by location of maternal residence. Darker colored areas represent higher incidence rates while larger red dots represent greater case counts. Map 3 shows case counts and incidence rates by location of maternal residence at the county level. County case counts ranged from zero cases in Forest, Potter,and Bradford counties to-221 in Philadelphia County. Incidence rates ranged from zero (in counties with zero cases) to 61.6 cases per 1000 live births in Fayette County. Map 4 shows case counts and incidence rates by location of maternal residence at the regional level. Case counts by region ranged from 85 in the northcentral region to 500 in the southeast. The highest incidence rate in the northwest was nearly three times the lowest rate in the northeast (23.7 versus 8.2 NAS cases per 1000 births). Map 3 – Neonatal Abstinence Syndrome Case Counts and Incidence Rates by County of Residenced
SOURCE: Vital Statistics (Division of Health Informatics, Pennsylvania Department of Health, 2018);4 NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019)
c Incidence rate is calculated using Pennsylvania 2018 live birth counts.3 d Two cases are excluded from this map due to address being listed as “homeless.”

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 12
Map 4 – Neonatal Abstinence Syndrome Case Counts and Incidence Rates by Region of Residencee
SOURCE: Vital Statistics (Division of Health Informatics, Pennsylvania Department of Health, 2018);4 NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Case counts by county of residence ranged from zero cases (reported by 3 counties) to 221 in Philadelphia County. Table 3 shows case counts by county of facility and county of residence, and case counts from 2018 are included for comparison. Table 4 shows 2019 incidence rates by region. Confidence intervals were generated to better compare 2019 rates to 2018 rates. Overlapping confidence intervals indicate that differences in rate are more likely to occur by chance, while non-overlapping intervals indicate that the rates are considered statistically different and are less likely to occur by chance. All regions but one (northcentral) had a decrease in incidence rate in 2019. The rates in three regions were statistically lower in 2019 than 2018, and no regions showed a statistically significant increase in rate. The southwest saw the largest decrease in rate (38%), while the rate in northcentral increased by 5%.
e Two cases are excluded from this map due to address being listed as “homeless.”

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 13
Table 3 – 2018 and 2019 Neonatal Abstinence Syndrome Case Counts by County of Facility and by County of Maternal Residence
Cases (n) Cases (n) Cases (n) Cases (n)
County Facilities
(n) By Facility
County By Resident
County County
Facilities (n)
By Facility County
By Resident County
(2019) 2018 2019 2018 2019 (2019) 2018 2019 2018 2019 Adams 1 2 1 15 7 Lackawanna 1 36 22 32 24 Allegheny 9 470 338 249 158 Lancaster 4 67 44 61 41 Armstrong 1 0 0 21 19 Lawrence 0 0 0 37 36 Beaver 1 20 41 29 39 Lebanon 1 2 1 16 11 Bedford 0 0 0 8 10 Lehigh 3 50 12 27 3 Berks 2 19 35 20 32 Luzerne 3 79 92 65 78 Blair 2 40 33 29 28 Lycoming 1 21 8 24 14 Bradford 1 0 0 2 0 McKean 1 1 2 2 4 Bucks 3 118 88 122 82 Mercer 2 44 38 33 33 Butler 1 6 6 40 17 Mifflin 1 21 25 18 21 Cambria 1 74 28 52 18 Monroe 1 18 2 21 3 Cameron 0 0 0 3 1 Montgomery 6 81 62 48 57 Carbon 0 0 0 11 2 Montour 1 75 77 4 1 Centre 1 6 10 11 10 Northampton 2 4 0 12 5 Chester 3 38 30 38 31 Northumberland 0 0 0 16 26
Clarion 1 0 2 12 10 Perry 0 0 0 11 15 Clearfield 1 44 47 29 29 Philadelphia 8 255 230 263 221 Clinton 0 0 0 14 17 Pike 0 0 0 4 1 Columbia 1 1 0 9 8 Potter 1 2 1 1 0 Crawford 1 11 7 39 24 Schuylkill 1 4 4 14 11 Cumberland 2 20 16 27 21 Snyder 0 0 0 1 3 Dauphin 2 79 61 39 32 Somerset 0 0 0 18 7 Delaware 4 49 8 52 25 Sullivan 0 0 0 1 1 Elk 1 8 0 17 8 Susquehanna 0 0 0 10 6 Erie 3 72 30 39 18 Tioga 1 1 0 3 1 Fayette 1 87 33 106 61 Union 1 2 3 4 4 Forest 0 0 0 0 0 Venango 1 34 39 34 29 Franklin 2 41 26 32 25 Warren 1 0 2 1 4 Fulton 0 0 0 4 1 Washington 1 52 32 59 52 Greene 0 0 0 29 18 Wayne 1 6 1 5 2
Huntingdon 0 2 0 10 5 Westmoreland 1 7 5 51 42 Indiana 1 0 0 16 7 Wyoming 0 0 0 11 8 Jefferson 1 3 1 5 11 York 3 68 65 64 65 Juniata 0 0 0 7 3 Total 94 2140 1608 2107f 1606g
SOURCE: Vital Statistics (Division of Health Informatics, Pennsylvania Department of Health, 2018);4 NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019)
f Count totals less than the total case count due to unknown resident address. g Count totals less than the total case count due to 2 resident addresses being listed as “homeless.”

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 14
Table 4 – 2018 and 2019 Neonatal Abstinence Syndrome Incidence Rates per 1000 Births by Region of Maternal Residenceh
2018 2019
Region
Incidence Rate
95% CI Incidence
Rate 95% CI
NW 28 (24.8, 31.7) 23.7 (20.5, 26.9)
SW 26 (24.1, 28.0) 16* (15.2, 18.4)
NC 14.3 (11.7, 17.6) 15.0 (11.8, 18.2)
SC 15.4 (13.7, 17.3) 13.1 (11.5, 14.7)
NE 12.7 (11.0, 14.6) 8.2* (6.8, 9.6)
SE 10.4 (9.6, 11.3) 8.4* (7.7, 9.1)
*2019 rates are statistically different from 2018 rates within the same region.
SOURCE: 2019 incidence rates were obtained using 2019 NAS cases (Bureau of Epidemiology, Pennsylvania Department of Health) and 2018 births from Vital Statistics (Division of Health Statistics, Pennsylvania Department of Health).4 Rates for 2018 were obtained from reported rates (Bureau of Epidemiology, Pennsylvania Department of Health).3
Table 5 provides county-level incidence rates by maternal residence. For comparison, 2018 rates and percent change in rate between 2018 to 2019 are included. Negative rate changes indicate a decrease in rate within the county, and these decreases are denoted with bold text. Table 5 – 2018 and 2019 Neonatal Abstinence Syndrome Incidence Rates per 1000 Births by County of Maternal Residence
County Cases
(n) Births
(n)
2018 Rate per
1000 Births
2019 Rate per
1000 Births
Rate Change
(%)
County Cases
(n) Births
(n)
2018 Rate per
1000 Births
2019 Rate per
1000 Births
Rate Change
(%)
Adams 7 934 16.8 7.5 -55.4 Lackawanna 24 2,027 15.5 11.8 -23.6
Allegheny 158 12,872 19.4 12.3 -36.7 Lancaster 41 6,954 8.4 5.9 -29.8
Armstrong 19 560 31 33.9 9.4 Lawrence 36 879 43 41.0 -4.8
Beaver 39 1,584 18.8 24.6 31.0 Lebanon 11 1,555 10.1 7.1 -30.0
Bedford 10 468 18.4 21.4 16.1 Lehigh 3 4,375 6.3 0.7 -89.1
Berks 32 4,608 4.2 6.9 65.3 Luzerne 78 3,317 20 23.5 17.6
Blair 28 1,210 24.1 23.1 -4.0 Lycoming 14 1,210 20.5 11.6 -43.6
Bradford 0 672 3.6 0.0 -100.0 McKean 4 365 6.5 11.0 68.6
Bucks 82 5,712 25 14.4 -42.6 Mercer 33 1,062 31 31.1 0.2
Butler 17 1,784 23 9.5 -58.6 Mifflin 21 610 30.5 34.4 12.9
Cambria 18 1,209 41.1 14.9 -63.8 Monroe 3 1,521 14.5 2.0 -86.4
Cameron 1 37 68.2 27.0 -60.4 Montgomery 57 8,538 5.6 6.7 19.2
Carbon 2 547 18.6 3.7 -80.3 Montour 1 197 18.4 5.1 -72.4
Centre 10 1,173 9.5 8.5 -10.3 Northampton 5 2,885 4.4 1.7 -60.6
h 2019 incidence rates were obtained using 2019 NAS cases and 2018 births from vital statistics. Rates for 2018 were
obtained from reported rates, which were calculated using 2018 NAS cases and 2017 vital statistics births.4

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 15
County Cases
(n) Births
(n)
2018 Rate per
1000 Births
2019 Rate per
1000 Births
Rate Change
(%)
County Cases
(n) Births
(n)
2018 Rate per
1000 Births
2019 Rate per
1000 Births
Rate Change
(%)
Chester 31 5,378 7.5 5.8 -23.1 Northumberland 26 895 17.2 29.1 68.9
Clarion 10 370 31.3 27.0 -13.7 Perry 15 506 21.6 29.6 37.2
Clearfield 29 700 38.6 41.4 7.3 Philadelphia 221 20,654 12.5 10.7 -14.4
Clinton 17 419 36.5 40.6 11.2 Pike 1 413 14.1 2.4 -82.8
Columbia 8 522 17 15.3 -9.8 Potter 0 168 7.6 0.0 -100.0
Crawford 24 913 41.5 26.3 -36.7 Schuylkill 11 1,275 10.7 8.6 -19.4
Cumberland 21 2,598 10.4 8.1 -22.3 Snyder 3 432 2.2 6.9 215.7
Dauphin 32 3,402 11.5 9.4 -18.2 Somerset 7 738 28.1 9.5 -66.2
Delaware 25 6,470 8.1 3.9 -52.3 Sullivan 1 42 22.7 23.8 4.9
Elk 8 263 62.7 30.4 -51.5 Susquehanna 6 388 37.2 15.5 -58.4
Erie 18 2,785 13.1 6.5 -50.7 Tioga 1 394 10.3 2.5 -75.4
Fayette 61 1,301 92.3 46.9 -49.2 Union 4 401 9.8 10.0 1.8
Forest 0 19 0 0.0 0.0 Venango 29 471 71.1 61.6 0.0
Franklin 25 1,728 19.8 14.5 -26.9 Warren 4 417 2.6 9.6 268.9
Fulton 1 141 33.1 7.1 -78.6 Washington 52 2,017 30.7 25.8 -16.0
Greene 18 335 111.1 53.7 -51.6 Wayne 2 396 13.4 5.1 -62.3
Huntingdon 5 417 27.1 12.0 -55.8 Westmoreland 42 2,914 17.3 14.4 -16.7
Indiana 7 809 20.5 8.7 -57.8 Wyoming 8 240 40.3 33.3 -17.3
Jefferson 11 477 10.5 23.1 119.6 York 65 4,711 13.9 13.8 -0.7
Juniata 3 293 25.7 10.2 -60.2 Total 1606 135,677 16 11.9 -25.6
SOURCE: 2019 incidence rates were obtained using 2019 NAS cases (Bureau of Epidemiology, Pennsylvania Department of Health) and 2018 births from Vital Statistics (Division of Health Statistics, Pennsylvania Department of Health).4 Rates for 2018 were obtained from reported rates (Neonatal Abstinence Syndrome: 2018 Report).3
Map 5 shows where statewide NAS cases are concentrated. Cities with populations of approximately 10,000 or greater were included. Darker colors represent a higher case density, and larger red dots indicate larger city populations.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 16
Map 5 – Neonatal Abstinence Syndrome Case Densityi
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019). The city map is sourced from ArcGIS Data & Maps.5 City populations are sourced from 2019 U.S. Census Bureau projected populations.6 Multiple NAS Births We additionally aimed to calculate the proportion of infants born with NAS to a mother who had previously birthed an infant with NAS , according to the 2018-2019 reported case data. To calculate this percentage, all reported cases of NAS (born between January 10, 2018 j -December 31, 2019) were analyzed. Mothers with two or more births at least eight months apart, indicating different pregnancies, were identified. In total, 58 mothers had two discrete births involving a diagnosis of NAS in an infant, with births separated by eight or more months. Each of the 58 mothers had one birth in 2018 and one birth in 2019, and all births were singleton births. In total, 4% of infants born with NAS in 2019 had a mother who previously gave birth to an infant with NAS. Characteristics of mothers with a repeat NAS birth were analyzed in comparison to characteristics of mothers who did not have a repeat birth to an infant with NAS (Tables 6 and 7). Reported drug exposure was determined using a variable in which reporters selected drugs from listed choices. Evidence of drug exposure could include a laboratory test of the mother or infant, self-report by the mother, or other evidence of drug exposure in the mother’s medical chart. Drugs of exposure were obtained per birth event, so mothers with multiple NAS-related birthsare represented up to two times: one time for each birth with drug exposure reported. In
i A city map with populations of approximately 10 000 or greater was obtained from ArcGIS Data & Maps. Population
estimates were based on 2019 U.S. Census Bureau projected population data. j January 10, 2018, is the date that NAS became reportable in Pennsylvania.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 17
analysis, MAT-associated drugs include buprenorphine and methadone. Although our data do not distinguish between mothers using these drugs via prescription versus diverted use of another person’s medication, prescribed use of these drugs indicate that mothers are pursuing care and treatment for an opioid use disorder, and a longer duration of opioid medication use during pregnancy is associated with improved maternal and perinatal outcomes.7 It is a safer alternative for both mothers and babies compared to ongoing opioid misuse. “Non-MAT” drugs (i.e., drugs not associated with MAT) include oxycodone, tramadol, fentanyl, heroin, alcohol, tobacco, opiates, cocaine, and “other” drugs, where “other” drug is not specified by reporters. Mothers with multiple NAS-related births (MMB) were statistically more likely to have reported use of buprenorphine or methadone (MAT drugs) than mothers with a single NAS-related birth (MSB) using Pearson’s chi-squared test. They were also less often reported as using non-MAT associated drugs, although this difference was not statistically significant. Race and ethnicity were similar across the two populations. Table 6 – Characteristics of Mothers with Two Known NAS Births Compared to Mothers with One Known NAS Birth: Drugs of Exposure and Race/Ethnicity, by Birth Event
Reported Drug Exposure Race
n
Reported
Use of Drugs
Associated
with MAT
Reported
Use of Drugs
Not
Associated
with MAT n
White
Non-
Hispanic
Black
Non-
Hispanic
Other/
Multiracial/
Unknown
Race/
Ethnicity Hispanic
Mothers with multiple NAS-related
births (MMB) 109 93% 60% 109 72% 8% 17% 3%
Mothers with single NAS-related
birth (MSB) 3103 83% 65% 3146 72% 6% 18% 3%
p-value 0.002* 0.31 0.56
*The difference between populations is statistically significant.
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) The median and mean maternal ages of MMB were slightly lower than those of MSB, although the minimum age of MMB was higher. In total, 69% of MMB were age 30 or less, while 55% of MSB were 30 or less. However, most of the population difference is due to a higher percentage of “MMB that are closer to age 30 (ages 26-30: 46% and 37% in MMB and and MSB, respectively) versus younger (ages 17-25: 22% and 18% in MMB and MSB, respectively). It is important to note that counts of MMB are small and rates are therefore unstable. No differences in race/ethnicity were seen among mothers regarding repeat vs. non-repeat NAS births.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 18
Table 7 – Maternal Age Comparison Between Mothers with Two or More Known NAS Births and Mothers with One Known NAS Birth
n Median Mean Minimum Maximum
% Mothers
Age 30 or Less
Repeat mothers 54 28 29 20 39 69%
Non-repeat mothers 3147 30 30 17 47 55%
SOURCE: NAS surveillance database (Bureau of Epidemiology, Pennsylvania Department of Health, 2019) Data Limitations The case data used in this report were obtained from facilities that submitted cases of NAS. A simple case verification process was performed on the reported cases, but full medical record abstraction for case confirmation was not performed. Therefore, the quality of case data, including race and ethnicity, relies upon the reporters’ access to requested information, especially for transferred infants, and upon reporters consistently and accurately reporting the information. Further, infants are often transferred to a different facility to receive a higher level of care, to transition to a step-down facility, or for other reasons. Regardless of transfer status, the Department asked all facilities to report a case, so duplicate reports for the same infant were received. Where multiple records on the same infant were received, a hierarchical logic was used in automated case processing to select the most appropriate record to retain. Infants with testing performed and a positive result were prioritized, followed by infants with testing performed and a negative result, infants with testing pending, and infants with no testing performed. If there were no distinctions in testing, the most recent record was retained. If infants were transferred to neighboring counties for care, case counts by county of facility will be underestimated due to select records being discarded. Similarly, statistics on variables like percentage of infants in the NICU or mothers receiving prenatal care are based upon retained records, so these percentages may be underestimated. All 2018 statewide birth data used for relative comparisons to NAS case data were obtained from the Pennsylvania Department of Health Enterprise Data Dissemination Information Exchange (EDDIE). This data represents Pennsylvania resident live births occurring in state and out of state. It also includes births that occurred outside of birthing facilities and pediatric hospitals, including at home or at smaller birthing clinics. However, multiple smaller facilities reported that they would immediately transfer any suspected infants with NAS to a larger facility that is better prepared to care for these infants. For this reason, it’s unlikely that many NAS infants were missed from this report. Additionally, there were 18 facilities that did not attempt to report any NAS cases to the Department in 2019, so there is a possibility that some cases were not reported. The reason for not reporting cases is unknown; it is possible they had zero cases to report, or they may have had cases but did not report. There is also potential that some facilities with limited capacity were only intermittently reporting cases and therefore also underreporting. Further, in October of 2018, the Philadelphia Department of Public Health (PDPH) released guidance

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 19
for reporting cases to PDPH using a different case definition than the state definitionk. This guidance was distributed to all Philadelphia facilities and also three neighboring county facilities. Although the Department of Health and PDPH have made efforts to collaborate on case reporting and messaging to facilities, there is potential that misinterpretation or burden of reporting to both PDPH and the state could have inadvertently reduced case reporting. The determination of mothers that had repeat NAS births is limited by the period of time used for analysis. The calendar years referenced are arbitrary; mothers having a birth in 2018 or 2019 in our dataset may have had additional births prior to 2018 or first births in 2019, and they may have repeat NAS-related births in 2020 or later years. The inclusion of additional years of data in future analyses will improve classification of mothers into the respective groups and may provide more insight for education and intervention efforts. In analysis of MMB and MSB and drug exposure, reporters were not asked to specify drugs used when “other” drug was indicated. Therefore, it cannot be determined whether “other” drug represents use of a single drug or multiple drugs. In total, 17 mothers had “other” drug listed as the only drug of exposure. All of these mothers were “non-repeat mothers,” and they were analyzed as if “other” drug represented a single drug despite this data limitation. This report is therefore intended to provide a reasonable estimation and means for future comparisons. Discussion This report presents findings from Pennsylvania’s second year of real-time NAS reporting. NAS burden in Pennsylvania remained high in 2019, with 11.9 cases per 1000 births. This is higher than the 2014 reported national incidence of eight per 1000 live births, although differences in case definitions could account for some of this variation.2 Overall, infants with NAS in Pennsylvania were typically born to mothers reported as being white non-Hispanic and using Medicaid as a primary payor. Infants born with NAS were more likely to be born with low birthweight and premature compared to statewide births. Both prematurity and low birthweight are associated with poorer health outcomes in a newborn.9 More than one out of every four infants with NAS born to a Hispanic or Black non-Hispanic mother were born prematurely or with low birthweight. Correspondingly, 50% of infants with NAS received care in a NICU, although a greater percentage of infants with Hispanic or Black non-Hispanic mothers (approximately 40% more) were treated in a NICU than infants born to other/unknown race/ethnicity mothers and white non-Hispanic mothers. This high rate of NICU care for infants born to Black non-Hispanic or Hispanic mothers may be related to the high rates of low birthweight and prematurity in the population. Although low birthweight and prematurity are often associated with lower frequency of normal Apgar scores,10,11 infants born with NAS to Hispanic mothers had the highest rate of normal Apgar scores (98%) and infants
k The Pennsylvania NAS case definition required any infant diagnosed with NAS having at least one NAS-related symptom
to be reported. In contrast, the PDPH case criteria included any infant with known or suspected drug use, at least one NAS-
related symptom, and at least one Finnegan score of 8 or higher.8

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 20
born to Black non-Hispanic mothers had a frequency similar to infants born to white non-Hispanic mothers (93% vs 94%). A lower percentage of Hispanic and Black non-Hispanic mothers were reported as receiving prenatal care than white non-Hispanic mothers. Additionally, the percentage of infants born to Hispanic and Black non-Hispanic mothers testing positive for MAT-associated drugs was lower than other races, providing further indication that these mothers may have been receiving less medical care during pregnancy than other groups. Infants born with NAS to white non-Hispanic mothers were less likely to receive any pharmacologic treatment (49%) than infants born to mothers of other races (54%, 65%, and 54% in Black non-Hispanic, Hispanic, and other/unknown race/ethnicity mothers, respectively). Although the proportion of infants exhibiting specific symptoms did not differ greatly across races, a greater percentage of infants born to Black non-Hispanic mothers had trouble breathing in comparison to other races, while infants with Hispanic mothers more often experienced trouble sleeping, seizures, and fever, sweating, or blotchy skin compared to other groups. However, the comparison are based on low case counts of infants with Hispanic mothers, so the rates are unstable. Infants born with NAS to mothers of other/unknown race/ethnicity were more often born with low birthweight and prematurely than infants born to white mothers. They had the lowest frequency of normal Apgar scores at five minutes (89%) but appeared to least often receive care in a NICU (46%). They were most likely to receive morphine treatment and less than half as likely to receive non-pharmacologic treatment compared to other NAS infants. Although a comparatively high proportion of infants tested positive for MAT-associated drugs, a comparatively high proportion also tested positive for opiates, oxycodone, or fentanyl, and the combination of infants testing positive totaled more than 100%, indicating that mothers appeared to be using multiple types of opioids. Infants born with NAS to white non-Hispanic mothers were less often born with low birthweight and prematurely than infants born to Black non-Hispanic, other/unknown race/ethnicity, or Hispanic mothers. The lowered rates of prematurity and low birthweight are consistent with statewide race and ethnicity trends, although the rate of prematurity and low birthweight is disproportionately elevated in infants with NAS born to Hispanic mothers.4 Although infants with NAS are predominately born to white, non-Hispanic mothers, at least 11% of the NAS population is born to Black non-Hispanic or Hispanic mothers. . Mothers of infants with NAS in these minority populations appear to use opiates, oxycodone, or fentanyl at approximately twice the rate of white non-Hispanic mothers of infants with NAS. This data shows the importance of directing resources and interventions to the populations with the most significant need for comprehensive prenatal care and substance use treatment. Maps 1 and 3 showing case counts by county of facility versus county of residence highlight differences in county-level cases. Counties with large discrepancies between number of NAS cases by facility location and by maternal residence demonstrate the variability in resource needs across the state. Counties with a higher case count by maternal residence indicate a greater need for community services and resources like substance use treatment and early interventionservices. Counties with larger facilities receiving an in-migration of patients for care, like Montour County with Geisinger Medical Center, highlight the need for facilities to

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 21
provide location-appropriate referrals to services for patients living in neighboring counties in order to make treatment accessible. Map 3 concurrently shows counties with high case counts and counties with high incidence rates. Counties with both high case counts and high rates indicate a more stable incidence rate and represent regions with a large population of infants with NAS affecting a disproportionately high percentage of the population compared to statewide populations. For example, although Allegheny and Philadelphia counties have the largest case counts, they have lower incidence rates than neighboring counties. Counties like Luzerne and Fayette have high case counts and high incidence rates in comparison to their neighboring counties. More targeted intervention efforts should be made to areas with larger case counts and higher incidence rates. Map 4 displays an increase in the rate of NAS moving from east to west across the state. For the regions with lower rates, there is no evidence to suggest that the statistically lowered rates were due to fewer facilities reporting in 2019 than 2018. Only three of the 13 newly non-reporting facilities were in one of these three regions, and they reported a total of seven cases in 2018. The total number of births was included in Table 4 with incidence rates by county to show the denominator used to calculate the NAS incidence rate. Forty-eight (72%) counties experienced a decrease in the NAS incidence rate in 2019. For the two counties that had the highest NAS rates in 2018 (Fayette and Greene counties at 9% and 11% of live births, respectively), the rates dropped approximately 50%. Both counties had an increase in resident births in 2019 and a decrease in NAS cases. Fayette County had a reporting facility in 2018 that closed its obstetrics and inpatient pediatric services in June 2019, and Greene did not have a reporting facility in either year. Map 5 shows areas with high density of NAS cases. It is expected that higher case densities would center upon the cities with the higher population density. However, the map shows some areas with lower population density that had higher case density, and it highlights some cities with a lower-than-expected case density compared to the local population density. In these areas, NAS prevention or management appears to be well-managed compared to higher case density areas. For example, Allentown has a lower case density than Pittsburgh and Wilkes-Barre despite having a higher population density. Demographics and other factors could be explored further to better understand this difference and opportunities for services in higher density areas. Despite the NAS incidence rate being higher than the national average, the statewide rate dropped approximately 26% from the 2018 state rate (16.0 cases per 1000 births). This may be a result of multiple contributing factors. One factor may be that fewer facilities attempted to report cases in 2019 than in 2018, and this potentially resulted in underreporting. Further, in comparison to incidence rates calculated in 2018 that excluded resident births occurring out of state, all 2019 incidence rates were calculated with resident births occurring out of state included. This would not affect case counts, but could slightly decrease the 2019 incidence rate in comparison to the 2018 rate because of a slightly larger denominator.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 22
However, it is important to note that claims data from newborn hospitalizations also noted a decrease in the rate of NAS-related stays. According to the Pennsylvania Health Care Cost Containment Council (PHC4), there were 1,610 NAS-related newborn hospital stays in 2019, which was a 12% decrease from 1,879 NAS-related stays in 2017.12 The rate of NAS-related stays dropped 10%, from 14.3 NAS-related stays per 1000 newborn stays in 2018 to 12.9 per 1000 stays in 2019.12 Overall, data indicates that, in addition to fewer NAS cases being reported to the Department in 2019, fewer infants were being diagnosed with NAS or were being assigned a billing code associated with NAS in 2019. The reason for this decrease in NAS-related billing codes is unclear, but one potential reason is that some facilities began adopting a different method for assessing the severity of withdrawal in infants with substance exposure. In 2019, a small number of facilities changed from using the Finnegan method of scoring to using the “Eat, Sleep, Console” (ESC) method. (Reported use of the Finnegan or modified Finnegan scoring methods dropped by approximately 5% in 2019.) The ESC method uses fewer and more focused infant health indicators to assess an infant’s symptom severity, and the method is commonly used to determine whether an infant requires pharmacologic intervention. The method has been shown to reduce the use of pharmacologic treatment for infants with NAS and to reduce infant length of stay in comparison to the use of the Finnegan scoring method.13 Related to this, some facilities indicated the use of minimum severity scores or the use of pharmacologic treatment as standards for diagnosing NAS or for assigning a NAS-related billing code. If select facilities have adopted a method of assessing infants with a scoring system that results in a lower severity score and less frequent use of pharmacologic treatment, these facilities may be less often diagnosing infants with NAS, assigning NAS-related billing codes, or both. The analysis of mothers with a second birth to a NAS infant has important limitations, as described above. Based on the data available, it appears that births to mothers with more than one NAS birth more often involved MAT-associated substance exposure. Again, it is not possible to determine whether these substances were prescribed to the mother or diverted for use from another person’s prescription medication. MMB also appeared to have a slightly lower rate of non-MAT drug exposure than MSB (60% vs 64%). Of mothers using a non-MAT associated drug, MMB more often had only one non-MAT drug reported (versus multiple non-MAT drugs) than MSB (62% versus 49%), and they less often had illicit drug exposure reported than MSB (22% vs 32%). Of “repeat mothers,” the proportion of mothers that were reported as using illicit drugs was higher in the first birth than in the second birth (27% vs 16%). It is important to note that 2019 NAS data corresponds only to NAS related to opioid exposure during pregnancy and does not include NAS caused by exposure to other substances. It also does not include infants that were exposed to opioids prenatally but did not exhibit signs of withdrawal. The total case counts and corresponding rates of infants affected by substance use during pregnancy would likely increase with the inclusion of these criteria. Accordingly, a nationally standardized case definition was published by the Council for State and Territorial Epidemiologists (CSTE) in July 2019, and it included exposure to barbiturates and benzodiazepines as causes of NAS. The inclusion of other exposure substances was adopted for NAS surveillance by the Department beginning on January 1, 2020.

NEONATAL ABSTINENCE SYNDROME PENNSYLVANIA DEPARTMENT OF HEALTH 23
Citations
1. March of Dimes. Neonatal Abstinence Syndrome. March of Dimes.
https://www.marchofdimes.org/complications/neonatal-abstinence-syndrome-(nas).aspx. Accessed March 11, 2021.
2. Jilani, SM, Frey, MT, Pepin, D, Jewell, T, Jordan, M, Miller, AM, … Reefhuis, J. Evaluation of State-Mandated Reporting of Neonatal Abstinence syndrome – Six States, 2013-2017. Morbidity and Mortality Weekly Report. 2019 Jan 11; pp. 6-10.
3. Bureau of Epidemiology, Pennsylvania Department of Health. Neonatal Abstinence Syndrome: 2018 Report.
Pennsylvania Department of Health. https://www.health.pa.gov/topics/Documents/Diseases%20and%20Conditions/2018%20NAS%20REPORT.pdf. Published August 2019. Accessed February 22, 2021.
4. Division of Health Informatics, Pennsylvania Department of Health. Pennsylvania Births: Crude/Age-Specific
Birth Rates per 1,000 females of specified age group. Enterprise Data Dissemination Informatics Exchange. https://www.phaim1.health.pa.gov/EDD/. Accessed February 18, 2021.
5. Esri Inc. ArcGIS Data and Maps. ArcGIS Online.
https://www.arcgis.com/home/item.html?id=872b352dfd1d4f6e942e8e0208321ced. Accessed February 11, 2021.
6. QuickFacts. United States Census Bureau. https://www.census.gov/quickfacts/fact/table/US/PST045219.
Accessed February 11, 2021.
7. Krans EE, Kim JY, Chen Q, Rothenberger SD, James AE, Kelley D, Jarlenski MP. Outcomes associated with the use of medications for opioid use disorder during pregnancy. Addiction. 2021 May 25.
8. Philadelphia Department of Public Health. (2019). Health Notification: Neonatal Abstinence Syndrome Reporting Requirement in Philadelphia February 26, 2019.
9. March of Dimes. Preterm Labor and Premature Birth. March of Dimes.
https://www.marchofdimes.org/complications/preterm-labor-and-premature-baby.aspx. Accessed February 17, 2021.
10. Hegyi T, Carone T, Anwar M, Ostfeld B, Hiatt M, Koons A, Pinto-Martin J, Paneth N. (1998). The Apgar
Score and Its Components in the Preterm Infant. Pediatrics, 101(1), 77-81.
11. Cnattinguis S, Johansson S, Razaz N. (2020). Apgar Score and Risk of Neonatal Death among Preterm Infants. N Engl J Med, 383, 49-57.
12. Pennsylvania Health Care Cost Containment Council. Three-Year Hospitalization Trends: Maternal Stays
with Opioid Use and Newborn Stays with Neonatal Abstinence Syndrome. Research Briefs. https://www.phc4.org/reports/researchbriefs/substanceuse/19/docs/researchbrief_substanceuse19_maternal.pdf. Published October 2020. Accessed March 1, 2021.
13. Blount, T, Painter, A, Freeman, E, Grossman, M, Sutton, AG. Reduction in Length of Stay and Morphine
Use for NAS With the “Eat, Sleep, Console” Method. Hosp Pediatr. 2019 Aug; 9(8): 615-623.