Embed Size (px)
Citation preview
Neonatal Surgical Emergencies James Moore, MD, PhD
Associate Professor of Pediatrics UT Southwestern Medical Center
Medical Director NICU Children’s Medical Center Dallas, Dallas, TX
The speaker has signed a disclosure form and indicated he has no significant financial interest or relationship with companies or the manufacturer(s) of any commercial product/service that will be discussed as part of this presentation.
Session Summary
During this session multiple neonatal anomalies and conditions that require emergent surgery will be presented in case format and discussed from a presentation/stabilization and management focus.
Session Objectives
Upon completion of this presentation, the participant will be able to:
discuss CDH in detail, as well as evidence for current treatment;
understand multiple GI emergencies in case-based format with emphasis on stabilization/treatment;
recognize airway/pulmonary emergencies and stabilization.
References
Boloker, J., Bateman, D., Wung, J. & Stolar, C. (2002). Congenital diaphragmatic hernia in 120 infants treated conservatively with permissive hypercapnea/spontaneous respiration/elective repair. Journal of Pediatric Surgery, 37: 357-366
Dillon, P.W., et al. (2004). The relationship of pulmonary artery pressure and survival in congenital diaphragmatic hernia. Journal of Pediatric Surgery, 39(3): 307-12.
Finer, N.N., et al. (1998). Congenital diaphragmatic hernia: Developing a protocolized approach. Journal of Pediatric Surgery, 33(9): 1331-7.
Grosfeld, J., O’Neill, J., Fonkalsrud, E. & Coran, A. (Eds.) (2006). Pediatric surgery ( 6th ed.). Philadelphia: Mosby-Elsevier.
Guarino, et al. (2000). Journal of Pediatric Surgery, 35: 1468-1473
Lally, K.P., et al. (2004). Surfactant does not improve survival rate in preterm infants with congenital diaphragmatic hernia. Journal of Pediatric Surgery, 39(6): 829-33.
Lally, K.P., et al. (2006). Corticosteroids for fetuses with congenital diaphragmatic hernia: Can we show benefit. Journal of Pediatric Surgery, 41(4): 668-74.
Millar, A., Rode, H. & Cywes, S. (2003). Malrotation and volvulus in infancy and childhood. Seminars in Pediatric Surgery, 12: 229-236.
Rowe, M., O’Neill, J., Grosfeld, J., Fonkalsrud, E., Coran, A. (Eds.) (1995). Essentials of pediatric surgery. St. Louis: Mosby-Year Book, Inc.
Van Meurs, K., et al. (2004). Is surfactant therapy beneficial in the treatment of the term newborn infant with congenital diaphragmatic hernia. Journal of Pediatrics, 145(3): 312-6.
Session Outline
See handout on the following pages.
A11a FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 1 of 12
FANNP’s 23rd National Neonatal Nurse Practitioner Symposium October 18, 2012
James Moore M.D, Ph.D.Associate Professor of PediatricsUT Southwestern Medical Center
Medical Director NICU: Children’s Medical Center Dallas
To discuss in detail CDH, and evidence for current treatment
Multiple GI emergencies in case based format with emphasis on stabilization/treatmentwith emphasis on stabilization/treatment
Airway/Pulmonary emergencies and stabilization
Should we use steroids prenatally?
Should we use Surfactant after birth?
D iNO h l i h h P l HTN f Does iNO help with the Pulmonary HTN of CDH?
What mode and strategy of ventilation should be employed?
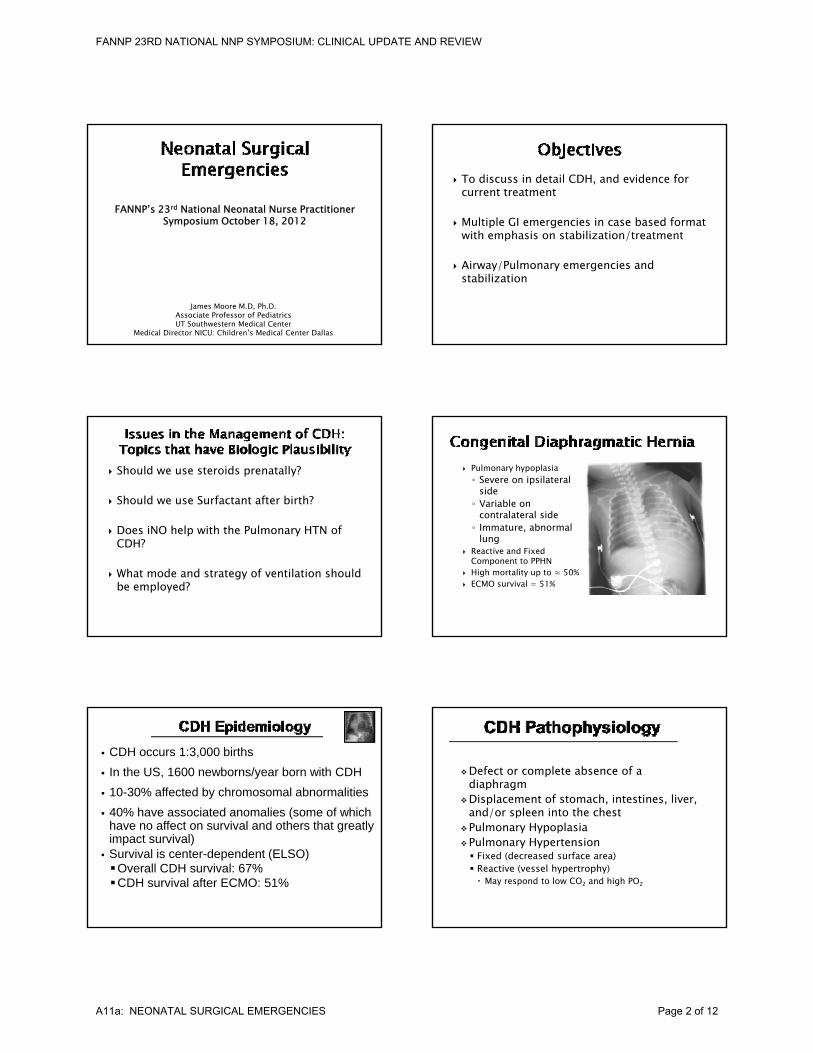
Pulmonary hypoplasia◦ Severe on ipsilateral
side◦ Variable on
contralateral sideImmature abnormal◦ Immature, abnormal lung
Reactive and Fixed Component to PPHN
High mortality up to ≈ 50% ECMO survival = 51%
CDH occurs 1:3,000 births In the US, 1600 newborns/year born with CDH 10-30% affected by chromosomal abnormalities 40% have associated anomalies (some of which (
have no affect on survival and others that greatly impact survival)
Survival is center-dependent (ELSO)Overall CDH survival: 67%CDH survival after ECMO: 51%
Defect or complete absence of a diaphragm
Displacement of stomach, intestines, liver, and/or spleen into the chest/ p
Pulmonary HypoplasiaPulmonary Hypertension Fixed (decreased surface area) Reactive (vessel hypertrophy) May respond to low CO2 and high PO2
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 2 of 12
Question #1
Do CDH infants exposed to antenatal steroids compared to placebo have improved
S i l?
Antenatal Steroid Use for CDH Infants
Survival? Need for ECMO? # Ventilator Days? Length of Stay?
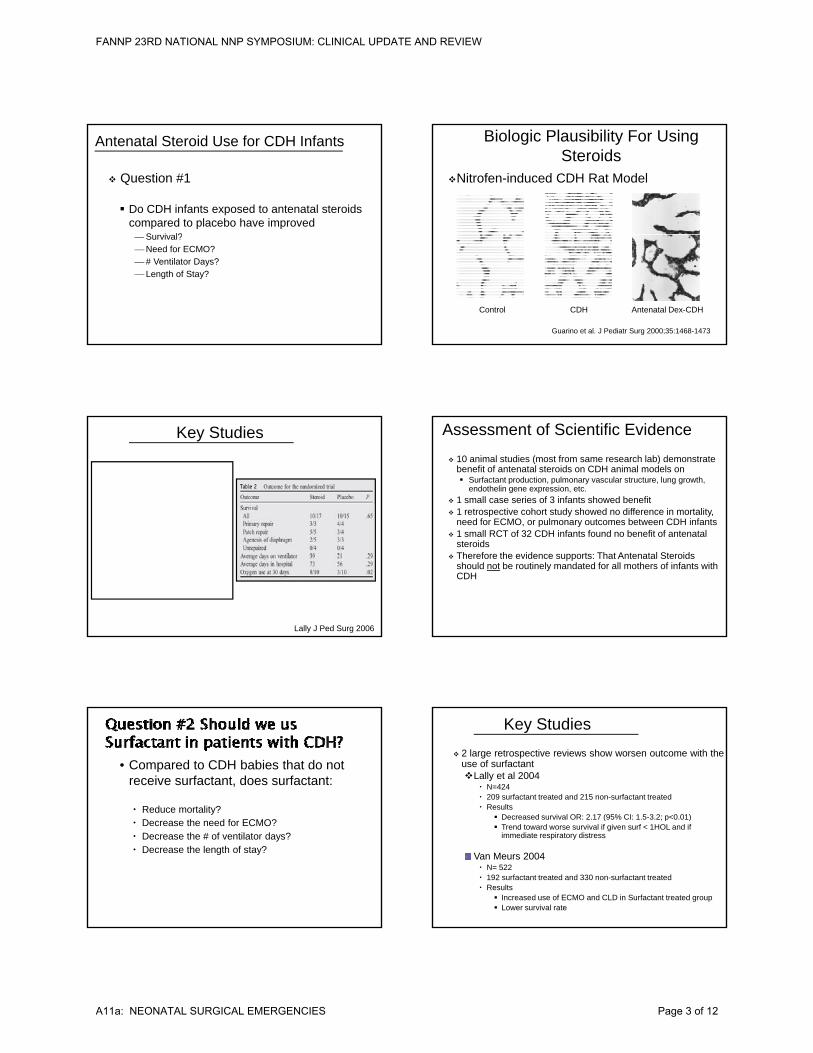
Nitrofen-induced CDH Rat Model
Biologic Plausibility For Using Steroids
Control CDH Antenatal Dex-CDH
Guarino et al. J Pediatr Surg 2000;35:1468-1473
Key Studies
Lally J Ped Surg 2006
10 animal studies (most from same research lab) demonstrate benefit of antenatal steroids on CDH animal models on Surfactant production, pulmonary vascular structure, lung growth,
endothelin gene expression, etc. 1 small case series of 3 infants showed benefit 1 retrospective cohort study showed no difference in mortality,
need for ECMO, or pulmonary outcomes between CDH infants
Assessment of Scientific Evidence
, p y 1 small RCT of 32 CDH infants found no benefit of antenatal
steroids Therefore the evidence supports: That Antenatal Steroids
should not be routinely mandated for all mothers of infants with CDH
• Compared to CDH babies that do not receive surfactant, does surfactant:
Reduce mortality? Decrease the need for ECMO? Decrease the # of ventilator days? Decrease the length of stay?
2 large retrospective reviews show worsen outcome with the use of surfactantLally et al 2004
N=424 209 surfactant treated and 215 non-surfactant treated Results
Decreased survival OR: 2 17 (95% CI: 1 5-3 2; p<0 01)
Key Studies
Decreased survival OR: 2.17 (95% CI: 1.5-3.2; p<0.01) Trend toward worse survival if given surf < 1HOL and if
immediate respiratory distress
Van Meurs 2004 N= 522 192 surfactant treated and 330 non-surfactant treated Results
Increased use of ECMO and CLD in Surfactant treated group Lower survival rate
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 3 of 12
Pulmonary arteries and veins of all sizes from CDH patients demonstrate increases in muscularization and wall thickness
Animal CDH models suggest that pulmonary Animal CDH models suggest that pulmonary vascular shows abnormal vasoconstrictor response
Alveolar capillary cross sectional area of CDH lungs is reduced predisposing to PAH
Presence of PAH confers a worse prognosis
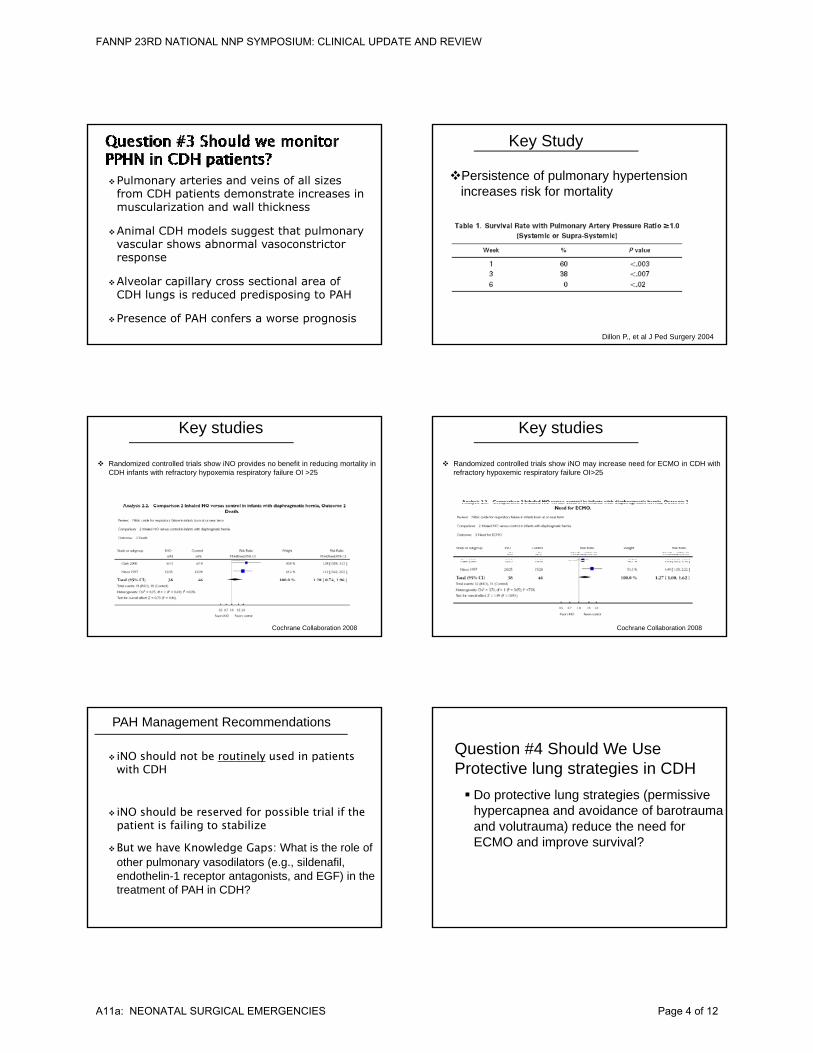
Persistence of pulmonary hypertension increases risk for mortality
Key Study
Dillon P., et al J Ped Surgery 2004
Randomized controlled trials show iNO provides no benefit in reducing mortality in CDH infants with refractory hypoxemia respiratory failure OI >25
Key studies
Lt CO
Cochrane Collaboration 2008
QuickTime™ and a decompressor
are needed to see this picture.
Randomized controlled trials show iNO may increase need for ECMO in CDH with refractory hypoxemic respiratory failure OI>25
Key studies
Lt CO
QuickTime™ and a decompressor
are needed to see this picture.
Cochrane Collaboration 2008
iNO should not be routinely used in patients with CDH
iNO should be reserved for possible trial if the
PAH Management Recommendations
ppatient is failing to stabilize
But we have Knowledge Gaps: What is the role of other pulmonary vasodilators (e.g., sildenafil, endothelin-1 receptor antagonists, and EGF) in the treatment of PAH in CDH?
Do protective lung strategies (permissive hypercapnea and avoidance of barotrauma
Question #4 Should We UseProtective lung strategies in CDH
and volutrauma) reduce the need for ECMO and improve survival?
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 4 of 12
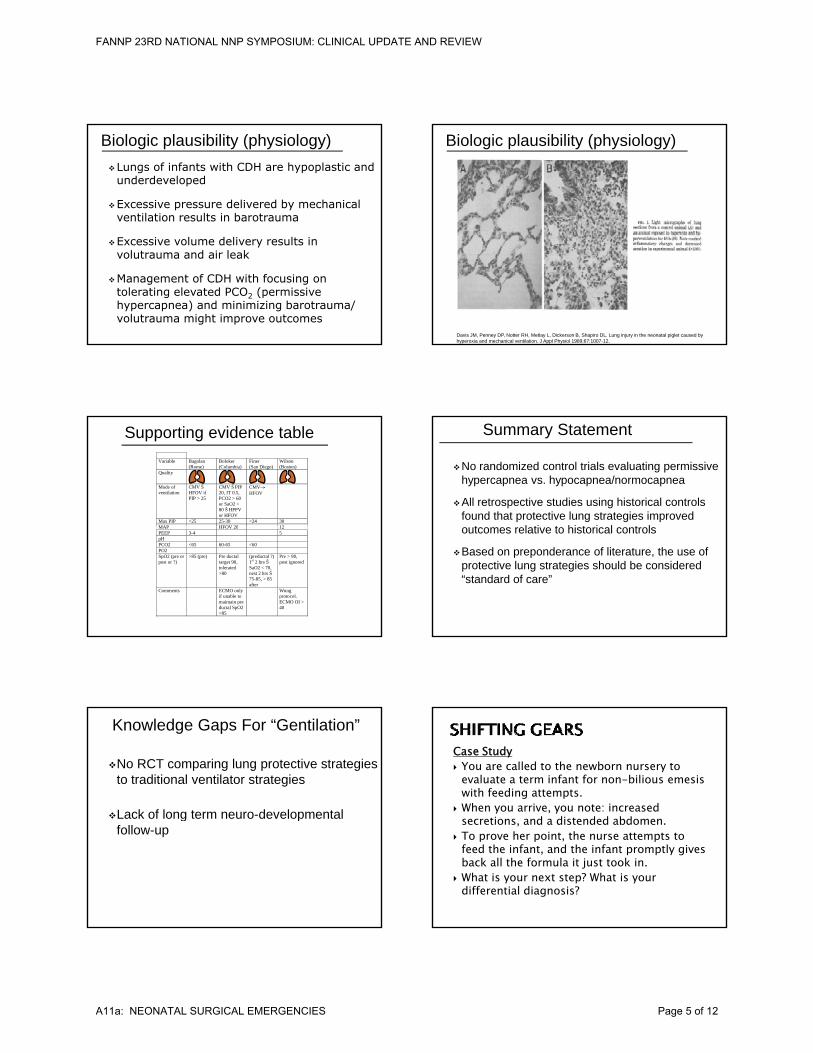
Lungs of infants with CDH are hypoplastic and underdeveloped
Excessive pressure delivered by mechanical ventilation results in barotrauma
Biologic plausibility (physiology)
Excessive volume delivery results in volutrauma and air leak
Management of CDH with focusing on tolerating elevated PCO2 (permissive hypercapnea) and minimizing barotrauma/ volutrauma might improve outcomes
Biologic plausibility (physiology)
Davis JM, Penney DP, Notter RH, Metlay L, Dickerson B, Shapiro DL. Lung injury in the neonatal piglet caused by hyperoxia and mechanical ventilation. J Appl Physiol 1989;67:1007-12.
Supporting evidence table Variable Bagolan
(Rome) Boloker (Columbia)
Finer (San Diego)
Wilson (Boston)
Quality
Mode of ventilation
CMV Š HFOV if PIP > 25
CMV Š PIP 20, IT 0.5, PCO2 > 60 or SaO2 < 80 Š HPPV or HFOV
CMV HFOV
Max PIP <25 25-30 <24 30 MAP HFOV 20 12MAP HFOV 20 12 PEEP 3-4 5 pH PCO2 <65 60-65 <60 PO2 SpO2 (pre or post or ?)
>85 (pre) Pre ductal target 90, tolerated >80
(preductal ?) 1st 2 hrs Š SaO2 < 70, nest 2 hrs Š 75-85, > 85 after
Pre > 90, post ignored
Comments ECMO only if unable to maintain pre ductal SpO2 >85
Wung protocol. ECMO OI > 40
No randomized control trials evaluating permissive hypercapnea vs. hypocapnea/normocapnea
All retrospective studies using historical controls found that protective lung strategies improved
t l ti t hi t i l t l
Summary Statement
outcomes relative to historical controls
Based on preponderance of literature, the use of protective lung strategies should be considered “standard of care”
No RCT comparing lung protective strategies to traditional ventilator strategies
Lack of long term neuro-developmental
Knowledge Gaps For “Gentilation”
Lack of long term neuro developmental follow-up
Case Study You are called to the newborn nursery to
evaluate a term infant for non-bilious emesis with feeding attempts.
When you arrive, you note: increased ti d di t d d bdsecretions, and a distended abdomen.
To prove her point, the nurse attempts to feed the infant, and the infant promptly gives back all the formula it just took in.
What is your next step? What is your differential diagnosis?
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 5 of 12
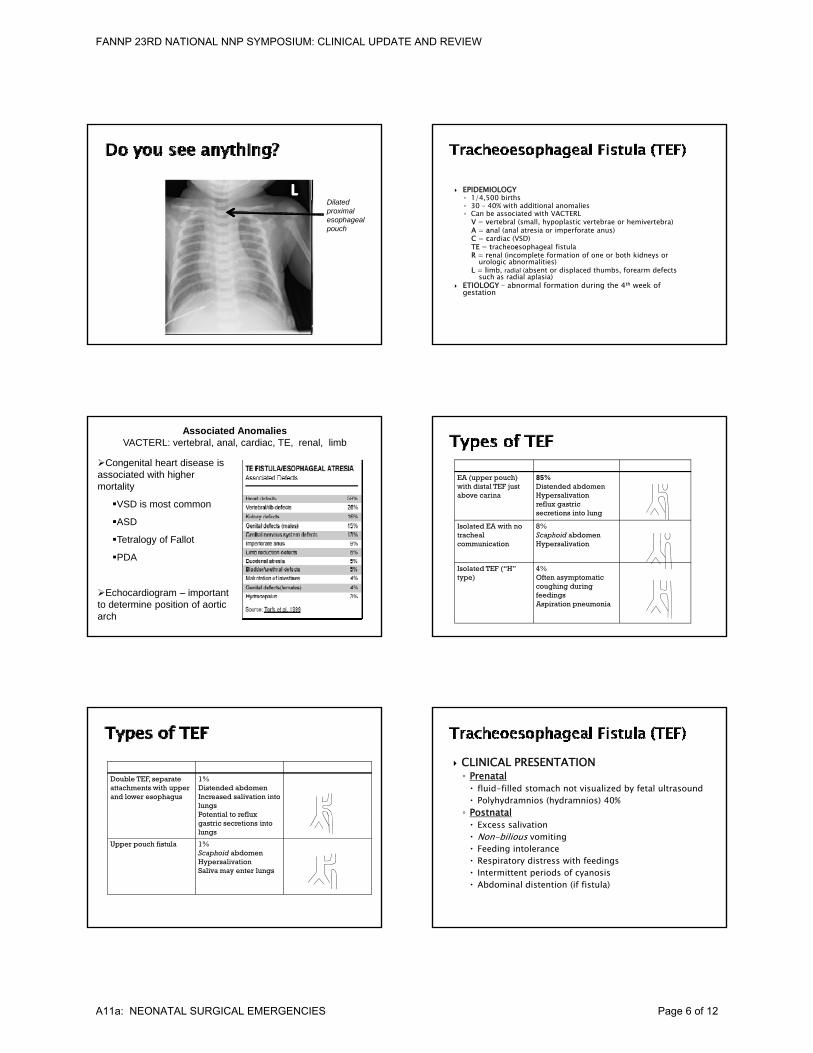
Dilated proximal esophageal pouch
EPIDEMIOLOGY◦ 1/4,500 births◦ 30 – 40% with additional anomalies◦ Can be associated with VACTERL
V = vertebral (small, hypoplastic vertebrae or hemivertebra) A = anal (anal atresia or imperforate anus) C = cardiac (VSD)TE = tracheoesophageal fistulaR = renal (incomplete formation of one or both kidneys or
urologic abnormalities)L = limb, radial (absent or displaced thumbs, forearm defects
such as radial aplasia) ETIOLOGY – abnormal formation during the 4th week of
gestation
Associated AnomaliesVACTERL: vertebral, anal, cardiac, TE, renal, limb
Congenital heart disease is associated with higher mortality
VSD is most common
ASD
Tetralogy of Fallot
PDA
Echocardiogram – important to determine position of aortic arch
EA (upper pouch) with distal TEF just above carina
85%Distended abdomenHypersalivationreflux gastric secretions into lung
Isolated EA with no 8%Isolated EA with no tracheal communication
8%Scaphoid abdomenHypersalivation
Isolated TEF (“H” type)
4%Often asymptomaticcoughing during feedings Aspiration pneumonia
Double TEF, separate attachments with upper and lower esophagus
1%Distended abdomenIncreased salivation into lungsPotential to reflux gastric secretions into lungs
Upper pouch fistula 1%Scaphoid abdomenHypersalivationSaliva may enter lungs
CLINICAL PRESENTATION◦ Prenatal fluid-filled stomach not visualized by fetal ultrasound Polyhydramnios (hydramnios) 40%◦ Postnatal Excess salivation Non-bilious vomiting Feeding intolerance Respiratory distress with feedings Intermittent periods of cyanosis Abdominal distention (if fistula)
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 6 of 12
TEF Outcome
PROGNOSIS
85% to 95% survival
Infants with increased risk of morbidity and mortality
•Low birth weight (>1500)
•Major CHD
•Severe associated anomalies
•Ventilator dependency
•Long gap atresia
You are called to evaluate an infant with bilious emesis.
Upon arrival you note that the infant has physical features that are consistent with Trisomy 21.
Green stains on blanket.
http://newborns.stanford.edu/PhotoGallery/Bile1.html
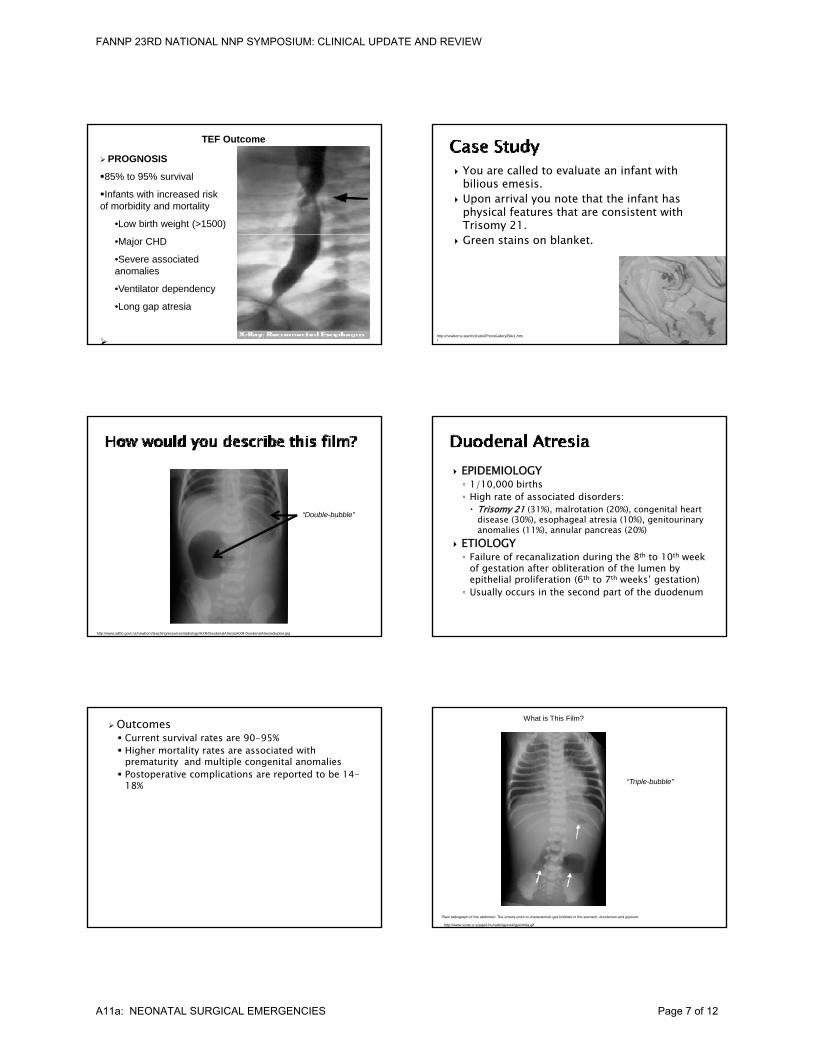
“Double-bubble”
http://www.adhb.govt.nz/newborn/teachingresources/radiology/AXR/DuodenalAtresia/AXR-DuodenalAtresiaSupine.jpg
EPIDEMIOLOGY◦ 1/10,000 births◦ High rate of associated disorders: Trisomy 21 (31%), malrotation (20%), congenital heart
disease (30%), esophageal atresia (10%), genitourinary anomalies (11%), annular pancreas (20%)
ETIOLOGY◦ Failure of recanalization during the 8th to 10th week
of gestation after obliteration of the lumen by epithelial proliferation (6th to 7th weeks’ gestation)◦ Usually occurs in the second part of the duodenum
Outcomes Current survival rates are 90-95% Higher mortality rates are associated with
prematurity and multiple congenital anomalies Postoperative complications are reported to be 14-
18% “Triple-bubble”
What is This Film?
Plain radiograph of the abdomen: The arrows point to characteristic gas bubbles in the stomach, duodenum and jejunum.
http://www.szote.u-szeged.hu/radio/gyerek/gyerm9a.gif
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 7 of 12
EPIDEMIOLOGY◦ Overall incidence greater than duodenal or colonic
atresias◦ Male = female◦ Usually single atresia (multiple atresias occur in 6%
to 20%)◦ Distal ileum: 36% ◦ Proximal jejunum: 31%◦ Distal jejunum: 20%◦ Proximal ileum: 13%
ETIOLOGY: In utero mesenteric vascular occlusion Operative photograph showing the distal apple-peel deformity
with extensive jejunal and ileal atresia.
http://www.virtualpediatrichospital.org/providers/CAP/Case23/Images/Case23.05.jpg
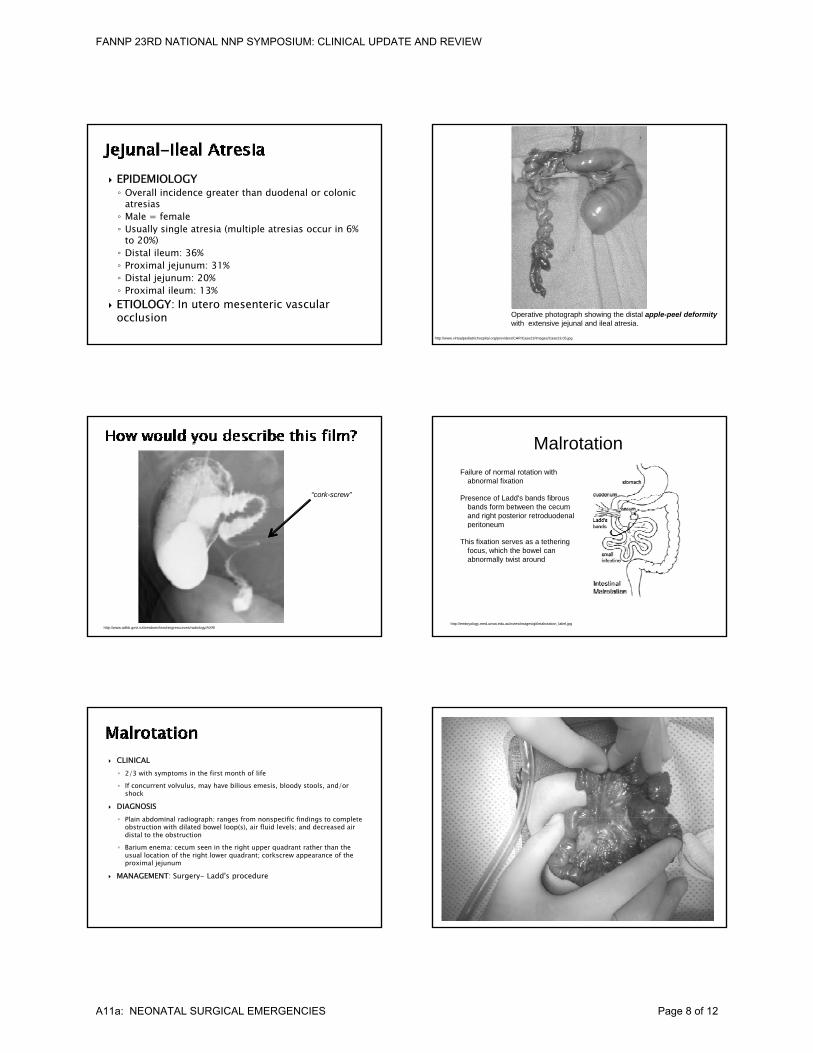
“cork-screw”
http://www.adhb.govt.nz/newborn/teachingresources/radiology/AXR/
Failure of normal rotation with abnormal fixation
Presence of Ladd's bands fibrous bands form between the cecum and right posterior retroduodenal peritoneum
Malrotation
http://embryology.med.unsw.edu.au/notes/images/git/malrotation_label.jpg
peritoneum
This fixation serves as a tethering focus, which the bowel can abnormally twist around
CLINICAL◦ 2/3 with symptoms in the first month of life◦ If concurrent volvulus, may have bilious emesis, bloody stools, and/or
shock
DIAGNOSISPl i bd i l di h f ifi fi di t l t◦ Plain abdominal radiograph: ranges from nonspecific findings to complete obstruction with dilated bowel loop(s), air fluid levels; and decreased air distal to the obstruction
◦ Barium enema: cecum seen in the right upper quadrant rather than the usual location of the right lower quadrant; corkscrew appearance of the proximal jejunum
MANAGEMENT: Surgery- Ladd's procedure
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 8 of 12
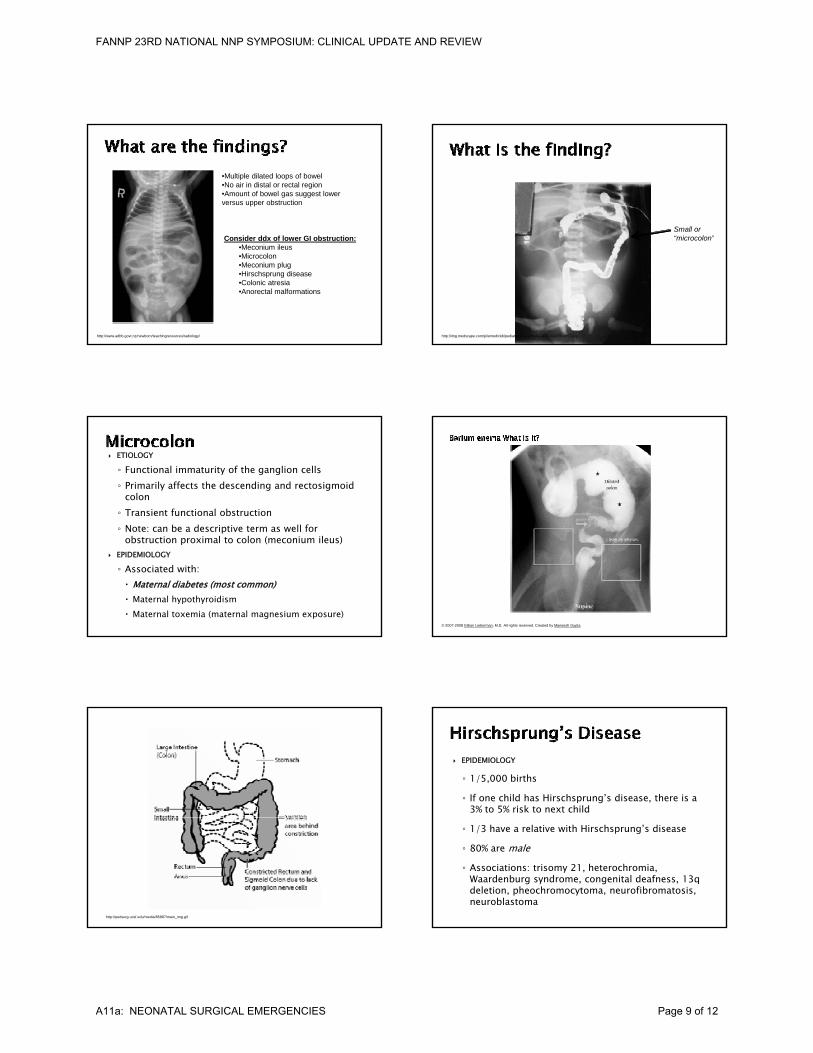
•Multiple dilated loops of bowel•No air in distal or rectal region•Amount of bowel gas suggest lower versus upper obstruction
http://www.adhb.govt.nz/newborn/teachingresources/radiology/
Consider ddx of lower GI obstruction:•Meconium ileus•Microcolon•Meconium plug•Hirschsprung disease•Colonic atresia•Anorectal malformations
Small or
http://img.medscape.com/pi/emed/ckb/pediatrics_surgery/933425-939258-2857.jpg
“microcolon”
ETIOLOGY
◦ Functional immaturity of the ganglion cells◦ Primarily affects the descending and rectosigmoid
colon ◦ Transient functional obstruction
N t b d i ti t ll f◦ Note: can be a descriptive term as well for obstruction proximal to colon (meconium ileus)
EPIDEMIOLOGY
◦ Associated with: Maternal diabetes (most common) Maternal hypothyroidism Maternal toxemia (maternal magnesium exposure)
© 2007-2008 Gillian Lieberman, M.D. All rights reserved. Created by Maneesh Gupta.
http://pedsurg.ucsf.edu/media/85887/main_img.gif
EPIDEMIOLOGY
◦ 1/5,000 births
◦ If one child has Hirschsprung’s disease, there is a 3% to 5% risk to next child
◦ 1/3 have a relative with Hirschsprung’s disease
◦ 80% are male◦ Associations: trisomy 21, heterochromia,
Waardenburg syndrome, congenital deafness, 13q deletion, pheochromocytoma, neurofibromatosis, neuroblastoma
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 9 of 12
MANAGEMENT◦ Diverting colostomy proximal to transition zone
with definitive treatment at age 1.0 to 1.5 years or weight > 10 kg
◦ Daily anal dilations followed by laparoscopy-soave pull-through of colon through anus
◦ Monitor for signs of enterocolitis
◦ Hearing screen (suggests syndromic etiology, ex. Waardenburg syndrome)
•Multiple dilated loops of bowel•No air in distal or rectal region•Amount of bowel gas suggest lower versus upper obstruction
www.uhrad.com/pedsarc/peds074.htm
Consider ddx of lower GI obstruction:
•Meconium ileus•Microcolon•Meconium plug•Hirschsprung disease•Colonic atresia•Anorectal malformations
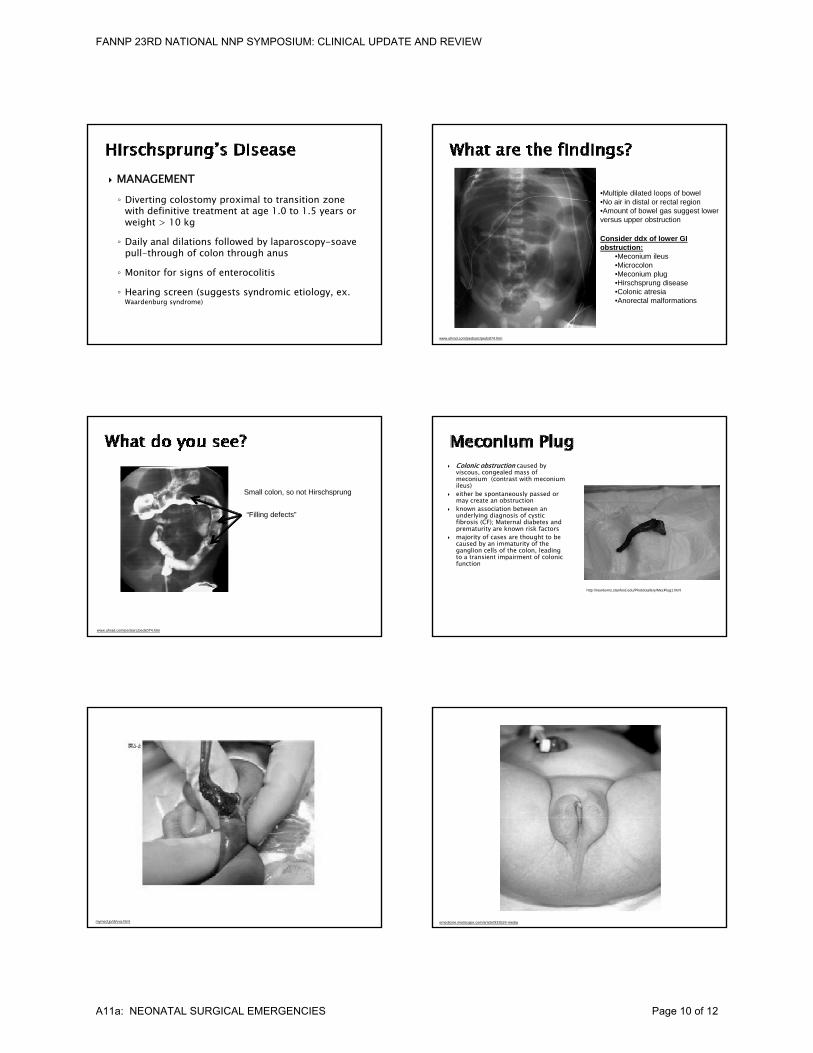
Small colon, so not Hirschsprung
“Filling defects”
www.uhrad.com/pedsarc/peds074.htm
Colonic obstruction caused by viscous, congealed mass of meconium (contrast with meconium ileus)
either be spontaneously passed or may create an obstruction
known association between an underlying diagnosis of cystic fibrosis (CF); Maternal diabetes and
k k f
http://newborns.stanford.edu/PhotoGallery/MecPlug1.html
prematurity are known risk factors majority of cases are thought to be
caused by an immaturity of the ganglion cells of the colon, leading to a transient impairment of colonic function
mymed.jp/di/vva.html emedicine.medscape.com/article/933524-media
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 10 of 12
EPIDEMIOLOGY
◦ 1/5,000 births◦ Includes wide spectrum of anorectal abnormalities
(anal stenosis, genitourinary abnormalities) ◦ Associated with other anomalies: genitourinary◦ Associated with other anomalies: genitourinary
(28% to 50% if high imperforate anus), gastrointestinal (13%), cardiac (7%), skeletal or central nervous system (6%), VACTERL◦ Usually no familial pattern, but there have been
reports of autosomal recessive or dominant inheritance
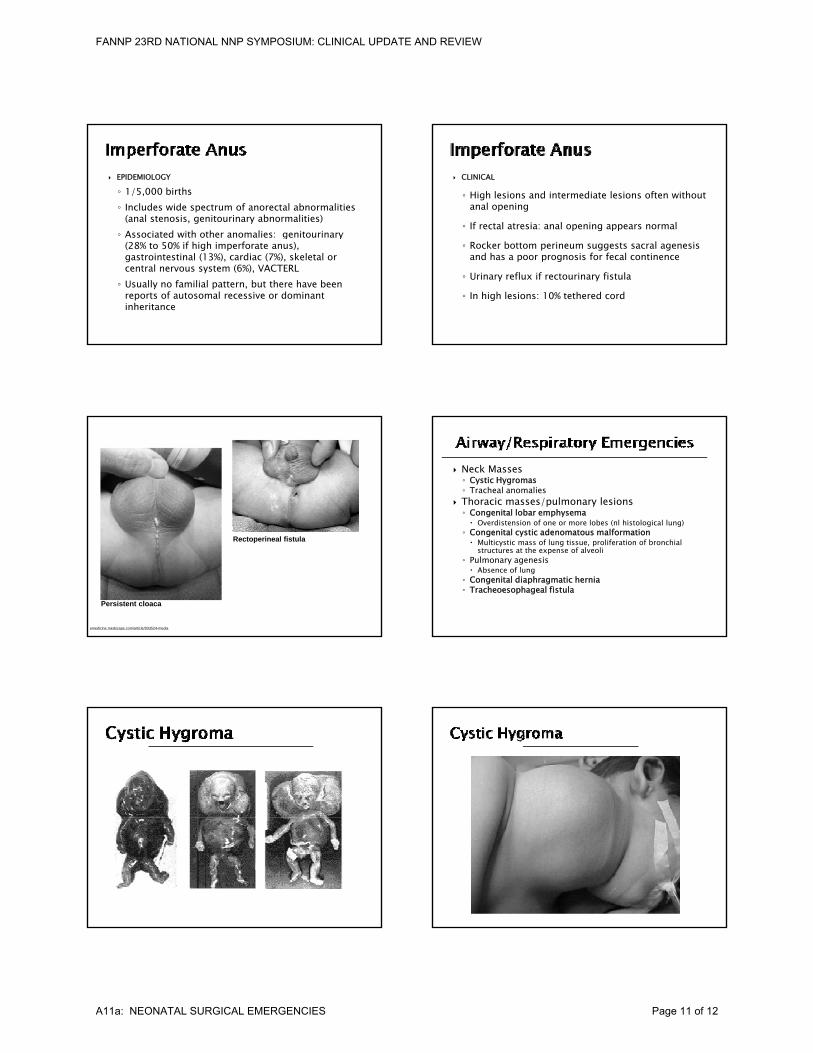
CLINICAL
◦ High lesions and intermediate lesions often without anal opening
◦ If rectal atresia: anal opening appears normal
◦ Rocker bottom perineum suggests sacral agenesis and has a poor prognosis for fecal continence
◦ Urinary reflux if rectourinary fistula
◦ In high lesions: 10% tethered cord
Persistent cloaca
emedicine.medscape.com/article/933524-media
Rectoperineal fistula
Neck Masses◦ Cystic Hygromas◦ Tracheal anomalies
Thoracic masses/pulmonary lesions◦ Congenital lobar emphysema Overdistension of one or more lobes (nl histological lung)( g g)
◦ Congenital cystic adenomatous malformation Multicystic mass of lung tissue, proliferation of bronchial
structures at the expense of alveoli◦ Pulmonary agenesis Absence of lung
◦ Congenital diaphragmatic hernia◦ Tracheoesophageal fistula
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 11 of 12
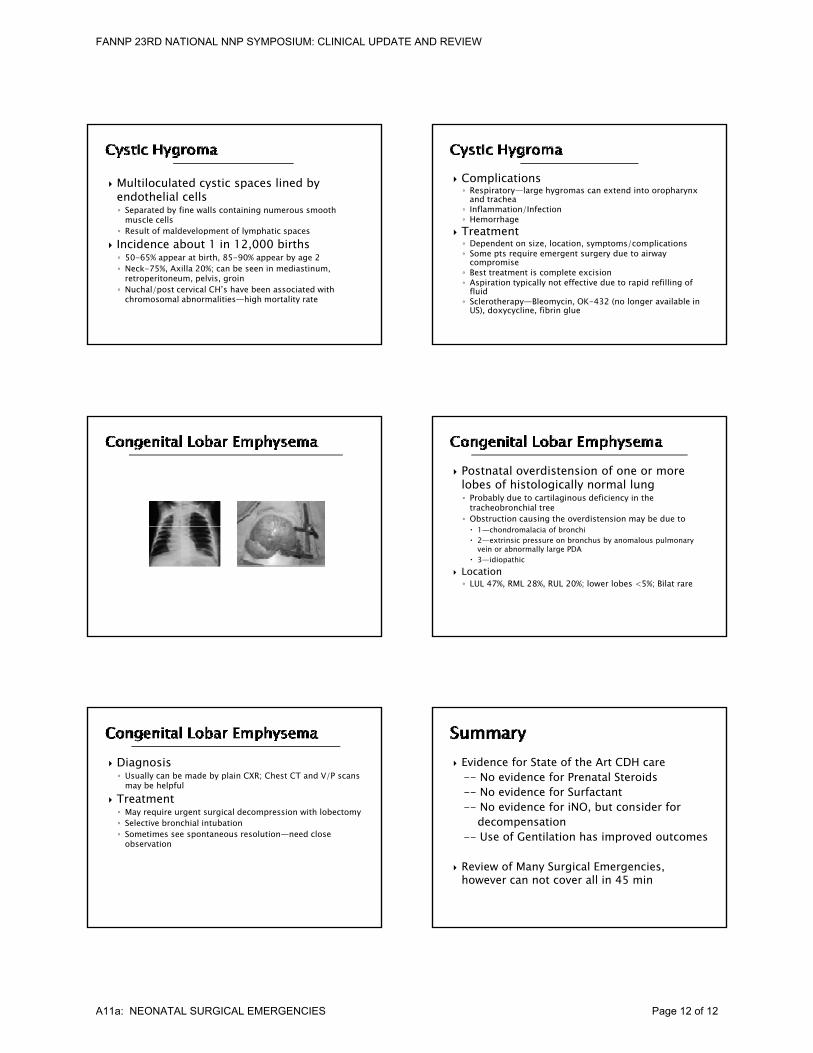
Multiloculated cystic spaces lined by endothelial cells◦ Separated by fine walls containing numerous smooth
muscle cells◦ Result of maldevelopment of lymphatic spacesp y p p
Incidence about 1 in 12,000 births◦ 50-65% appear at birth, 85-90% appear by age 2◦ Neck-75%, Axilla 20%; can be seen in mediastinum,
retroperitoneum, pelvis, groin◦ Nuchal/post cervical CH’s have been associated with
chromosomal abnormalities—high mortality rate
Complications◦ Respiratory—large hygromas can extend into oropharynx
and trachea◦ Inflammation/Infection◦ Hemorrhage
Treatment Treatment◦ Dependent on size, location, symptoms/complications◦ Some pts require emergent surgery due to airway
compromise◦ Best treatment is complete excision◦ Aspiration typically not effective due to rapid refilling of
fluid◦ Sclerotherapy—Bleomycin, OK-432 (no longer available in
US), doxycycline, fibrin glue
Postnatal overdistension of one or more lobes of histologically normal lung◦ Probably due to cartilaginous deficiency in the
tracheobronchial tree◦ Obstruction causing the overdistension may be due to 1—chondromalacia of bronchi 2—extrinsic pressure on bronchus by anomalous pulmonary
vein or abnormally large PDA 3—idiopathic
Location◦ LUL 47%, RML 28%, RUL 20%; lower lobes <5%; Bilat rare
Diagnosis◦ Usually can be made by plain CXR; Chest CT and V/P scans
may be helpful Treatment◦ May require urgent surgical decompression with lobectomy◦ Selective bronchial intubation◦ Sometimes see spontaneous resolution—need close
observation
Evidence for State of the Art CDH care-- No evidence for Prenatal Steroids-- No evidence for Surfactant-- No evidence for iNO, but consider for
d idecompensation-- Use of Gentilation has improved outcomes
Review of Many Surgical Emergencies, however can not cover all in 45 min
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
A11a: NEONATAL SURGICAL EMERGENCIES Page 12 of 12