Embed Size (px)
Citation preview
Campus Innenstadt | Campus Großhadern
Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe
Prof. Dr. Nadia HarbeckLeitung Brustzentrum der Universität München
Klinik und Poliklinik für Frauenheilkunde und Geburtshilfe Ludwig-Maximilians-Universität München
Direktor: Prof. Dr. Klaus Friese
Neues aus San Antonio2013
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
NEUES AUS SAN ANTONIO 2013: PRIMÄRES MAMMAKARZINOM
LokaltherapieAdjuvante Therapie
BisphosphonateHER2-positiv
…
26.01.20142
San Antonio 2013 | Prof. Harbeck
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
Effects Of Bisphosphonate Treatment OnRecurrence And Cause-specific Mortality
In Women With Early Breast Cancer:A Meta-analysis Of Individual Patient Data
From Randomised Trials
R Coleman, M Gnant, A Paterson, T Powles, G von Minckwitz,K Pritchard, J Bergh, J Bliss, J Gralow, S Anderson, D Cameron,
V Evans, H Pan, R Bradley, C Davies, R Gray.Early Breast Cancer Trialists’ Collaborative Group
(EBCTCG)’s Bisphosphonate Working Group.
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
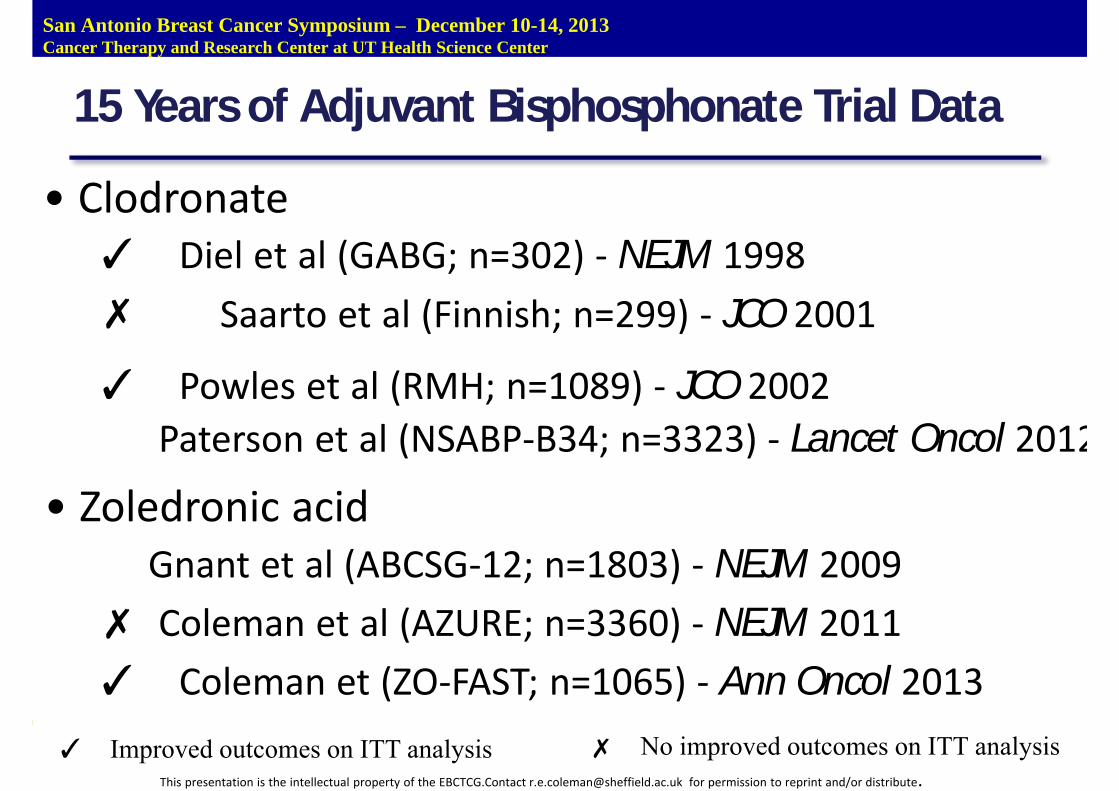
15 Years of Adjuvant Bisphosphonate Trial Data
• Clodronate✓ Diel et al (GABG; n=302) ‐ NEJM 1998✗ Saarto et al (Finnish; n=299) ‐ JCO 2001
✓ Powles et al (RMH; n=1089) ‐ JCO 2002Paterson et al (NSABP‐B34; n=3323) ‐ Lancet Oncol 2012
• Zoledronic acidGnant et al (ABCSG‐12; n=1803) ‐ NEJM 2009
✗ Coleman et al (AZURE; n=3360) ‐ NEJM 2011✓ Coleman et (ZO‐FAST; n=1065) ‐ Ann Oncol 2013
✓ Improved outcomes on ITT analysis ✗ No improved outcomes on ITT analysis
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
Bisphosphonate Analysis Outcomes
Primary outcomesTime to recurrence: includes distant recurrence, localrecurrence and new second primary breast cancer (ipsilateralor contralateral).
Time to first distant recurrence: includes distant recurrenceand ignores any prior loco-regional or contralateralrecurrences.
Breast cancer mortality.
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
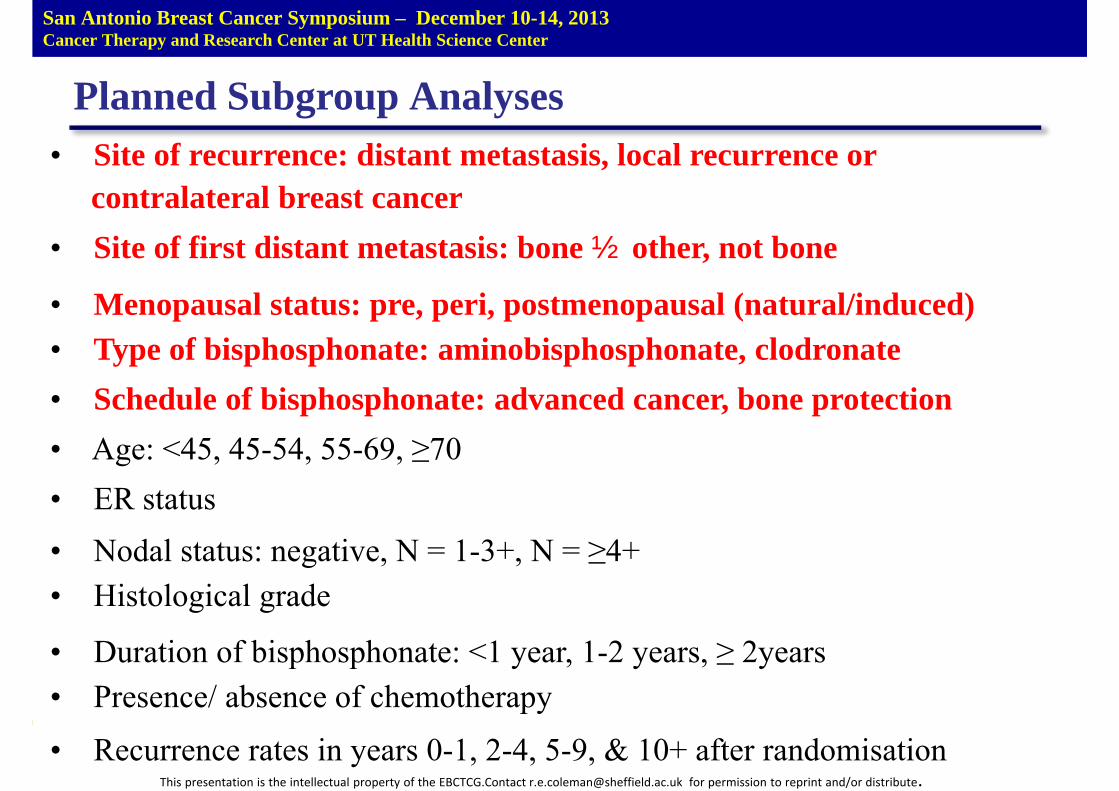
Planned Subgroup Analyses• Site of recurrence: distant metastasis, local recurrence or
contralateral breast cancer• Site of first distant metastasis: bone± other, not bone
• Menopausal status: pre, peri, postmenopausal (natural/induced)• Type of bisphosphonate: aminobisphosphonate, clodronate• Schedule of bisphosphonate: advanced cancer, bone protection• Age: <45, 45-54, 55-69, ≥70• ER status• Nodal status: negative, N = 1-3+, N = ≥4+• Histological grade
• Duration of bisphosphonate: <1 year, 1-2 years, ≥ 2years• Presence/ absence of chemotherapy
• Recurrence rates in years 0-1, 2-4, 5-9, & 10+ after randomisation
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
Number
trials
Numberpatients
Trialsreceived
Patientsreceived
Percentreceived
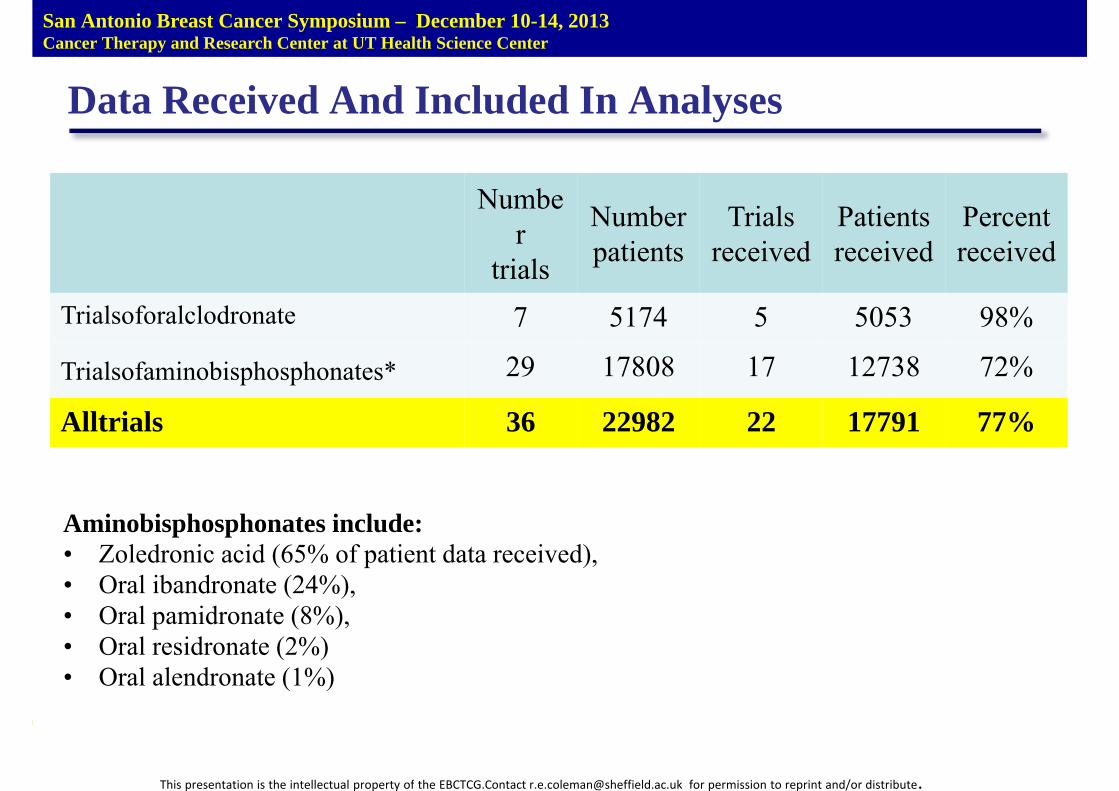
Trialsoforalclodronate 7 5174 5 5053 98%
Trialsofaminobisphosphonates* 29 17808 17 12738 72%
Alltrials 36 22982 22 17791 77%
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
Data Received And Included In Analyses
Aminobisphosphonates include:• Zoledronic acid (65% of patient data received),• Oral ibandronate (24%),• Oral pamidronate (8%),• Oral residronate (2%)• Oral alendronate (1%)
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
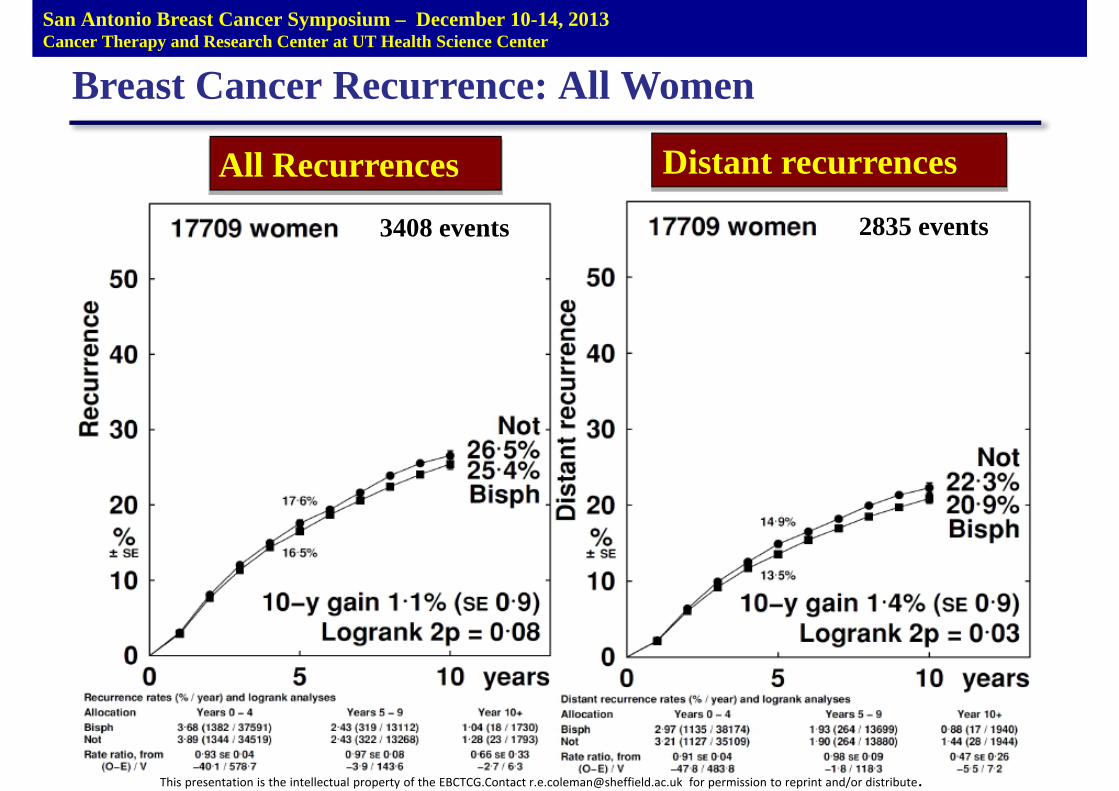
Breast Cancer Recurrence: All Women
All Recurrences
3408 events
Distant recurrences
2835 events
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
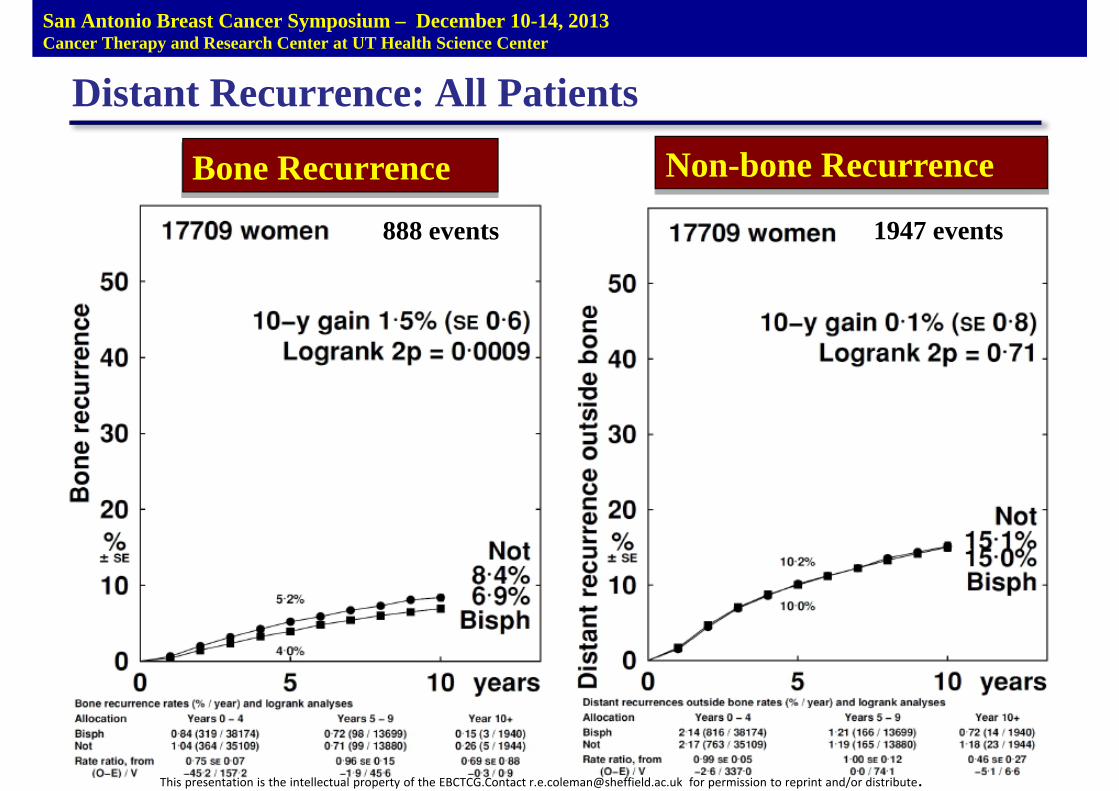
Distant Recurrence: All Patients
Bone Recurrence
888 events
Non-bone Recurrence
1947 events
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
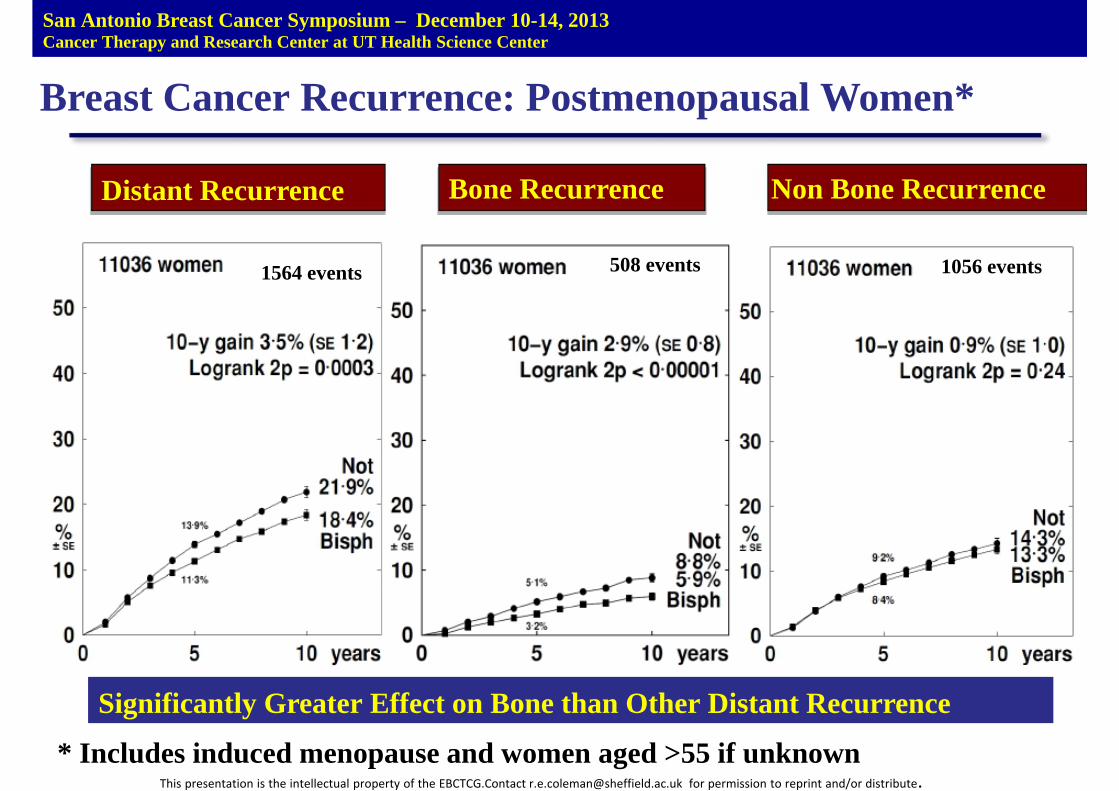
Breast Cancer Recurrence: Postmenopausal Women*
Distant Recurrence
1564 events
Bone Recurrence
508 events
Non Bone Recurrence
1056 events
Significantly Greater Effect on Bone than Other Distant Recurrence
* Includes induced menopause and women aged >55 if unknownThis presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
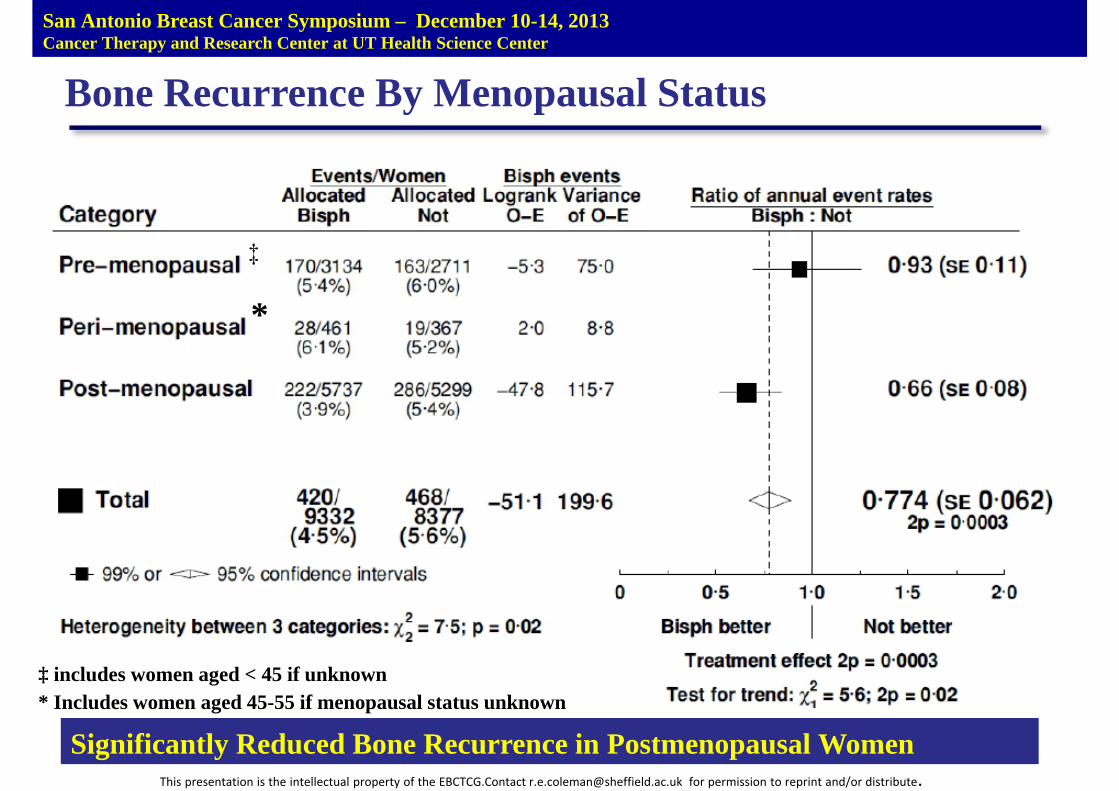
Bone Recurrence By Menopausal Status
‡
*
‡ includes women aged < 45 if unknown* Includes women aged 45-55 if menopausal status unknown
Significantly Reduced Bone Recurrence in Postmenopausal WomenThis presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
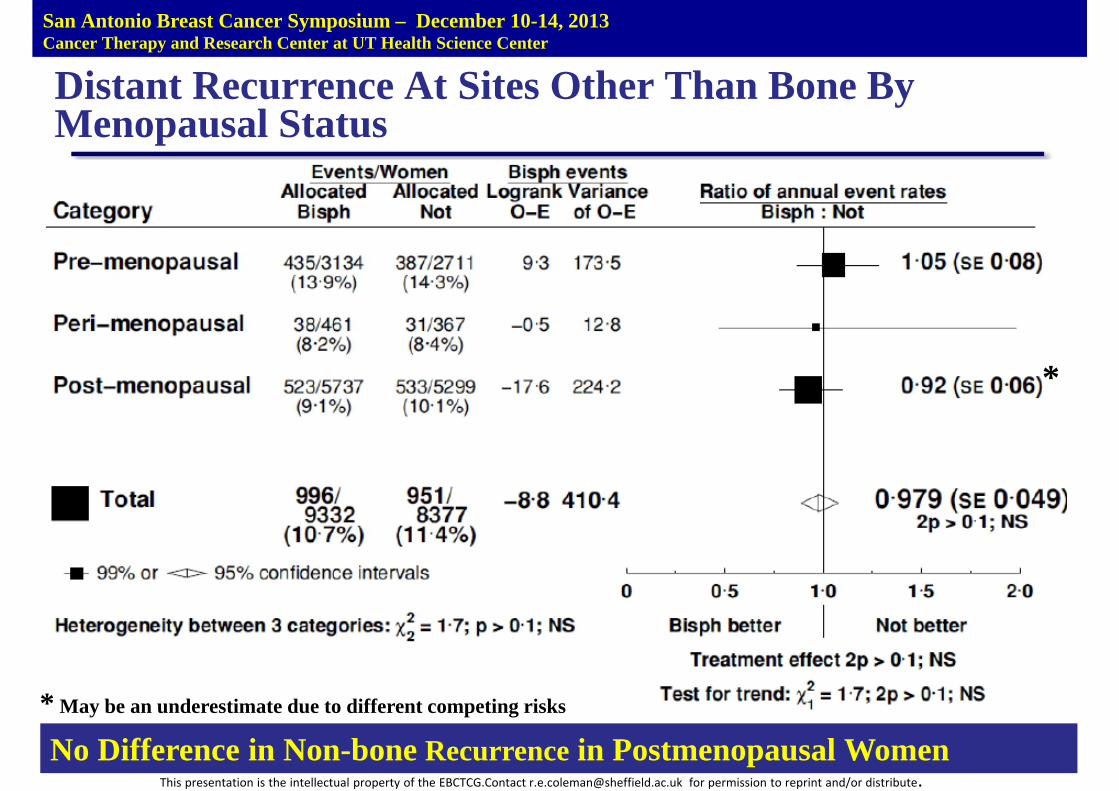
Distant Recurrence At Sites Other Than Bone ByMenopausal Status
*
* May be an underestimate due to different competing risks
No Difference in Non-bone Recurrence in Postmenopausal WomenThis presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
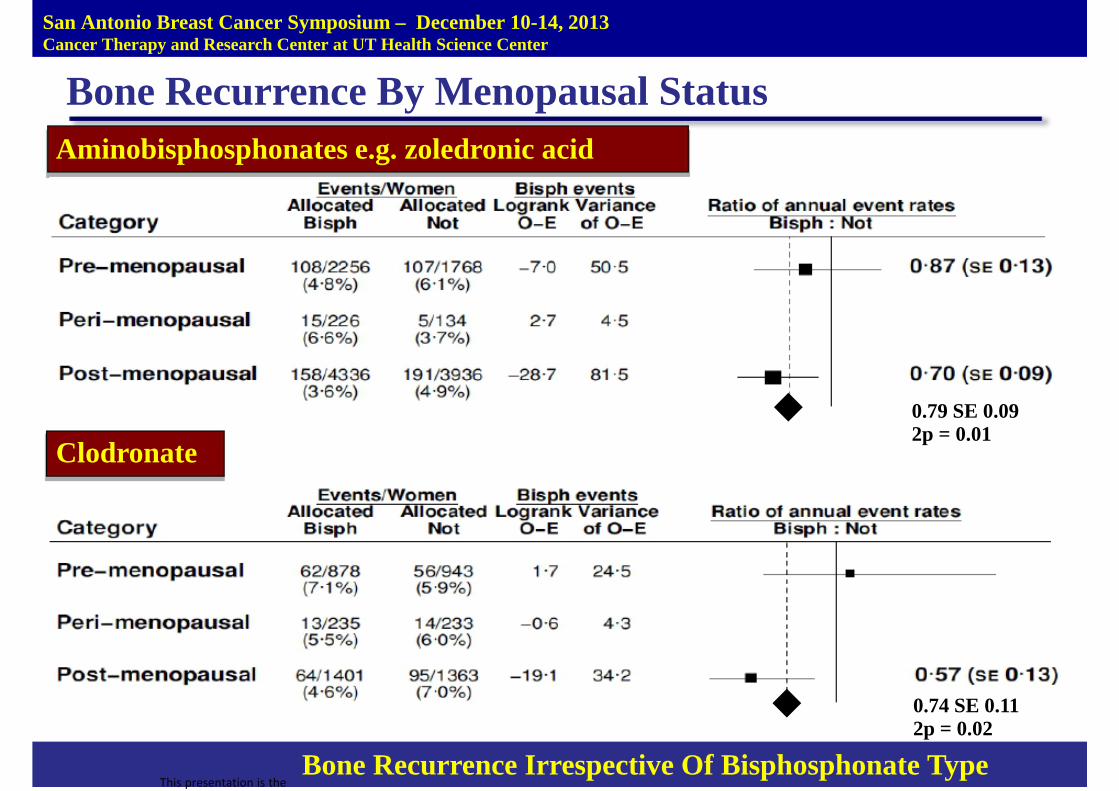
Bone Recurrence By Menopausal StatusAminobisphosphonates e.g. zoledronic acid
Clodronate
Bone Recurrence Irrespective Of Bisphosphonate TypeThis presentation is the
0.79 SE 0.092p = 0.01
0.74 SE 0.112p = 0.02
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
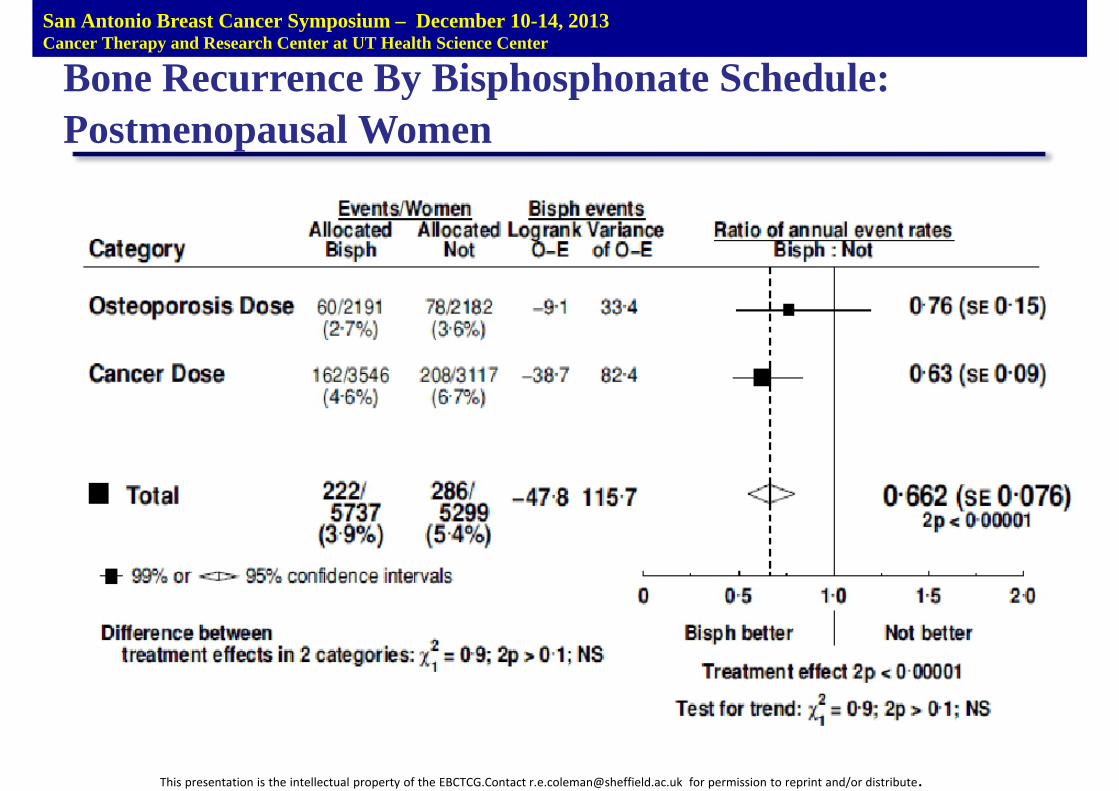
Bone Recurrence By Bisphosphonate Schedule:Postmenopausal Women
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
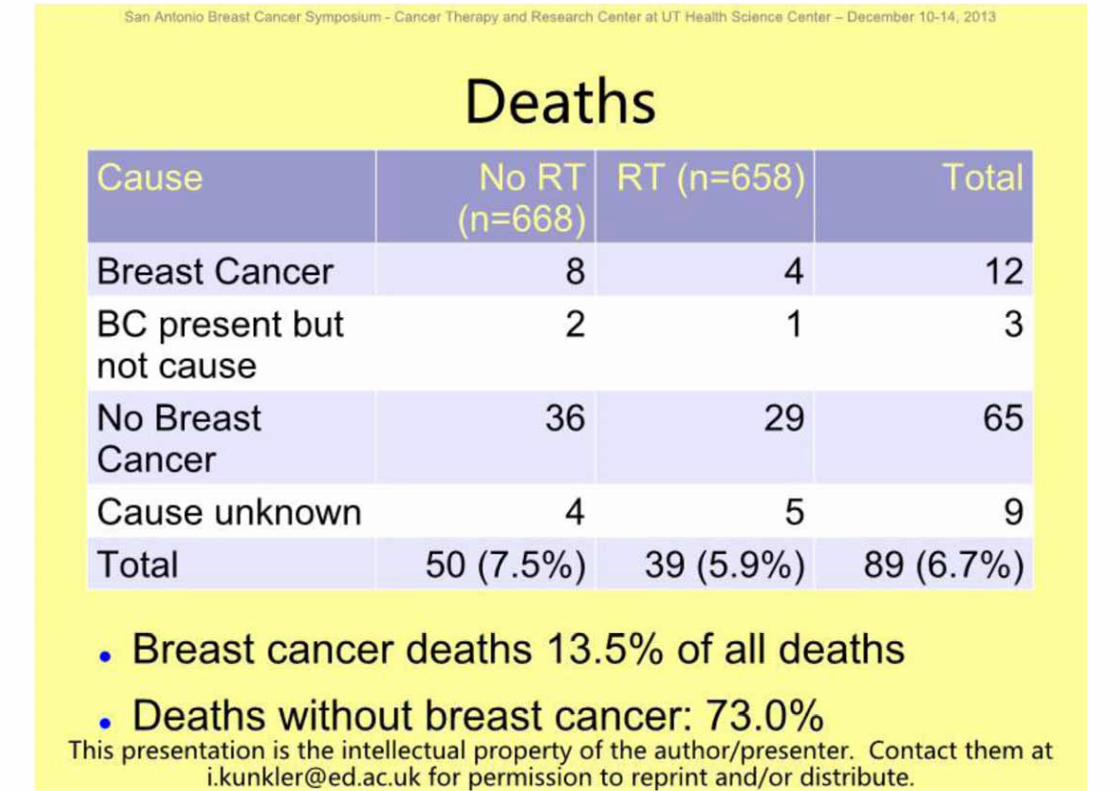
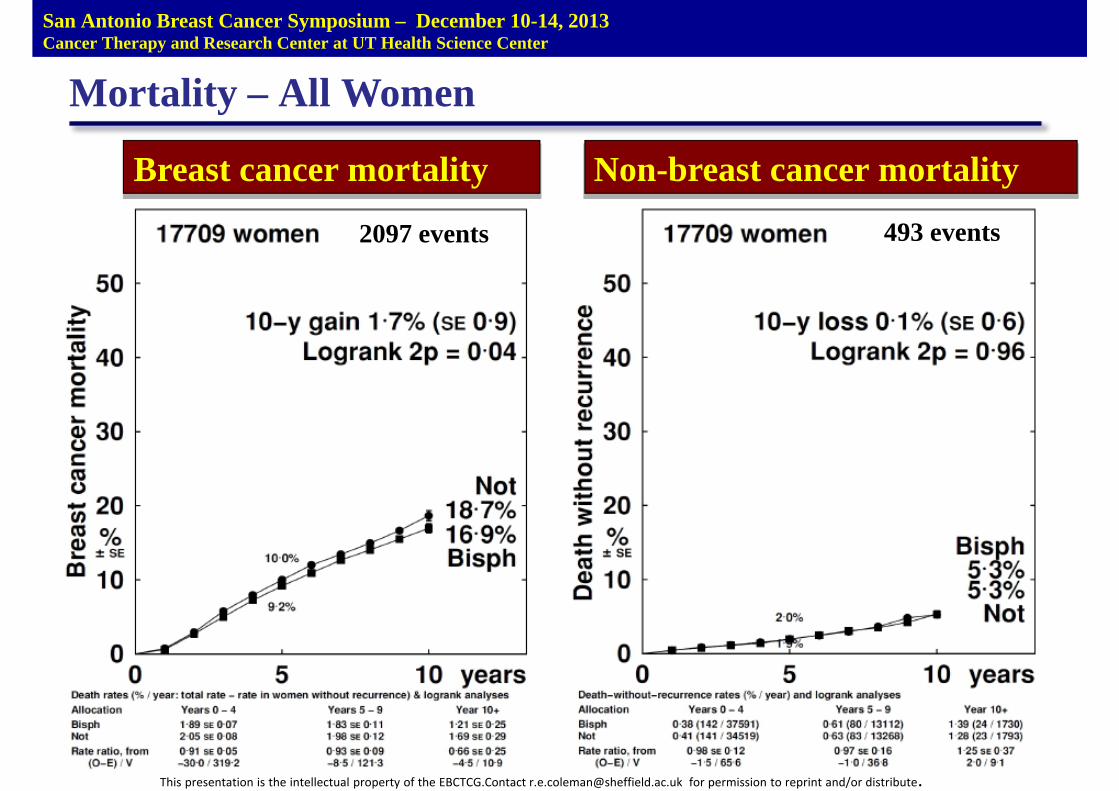
Mortality – All Women
Breast cancer mortality
2097 events
Non-breast cancer mortality
493 events
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
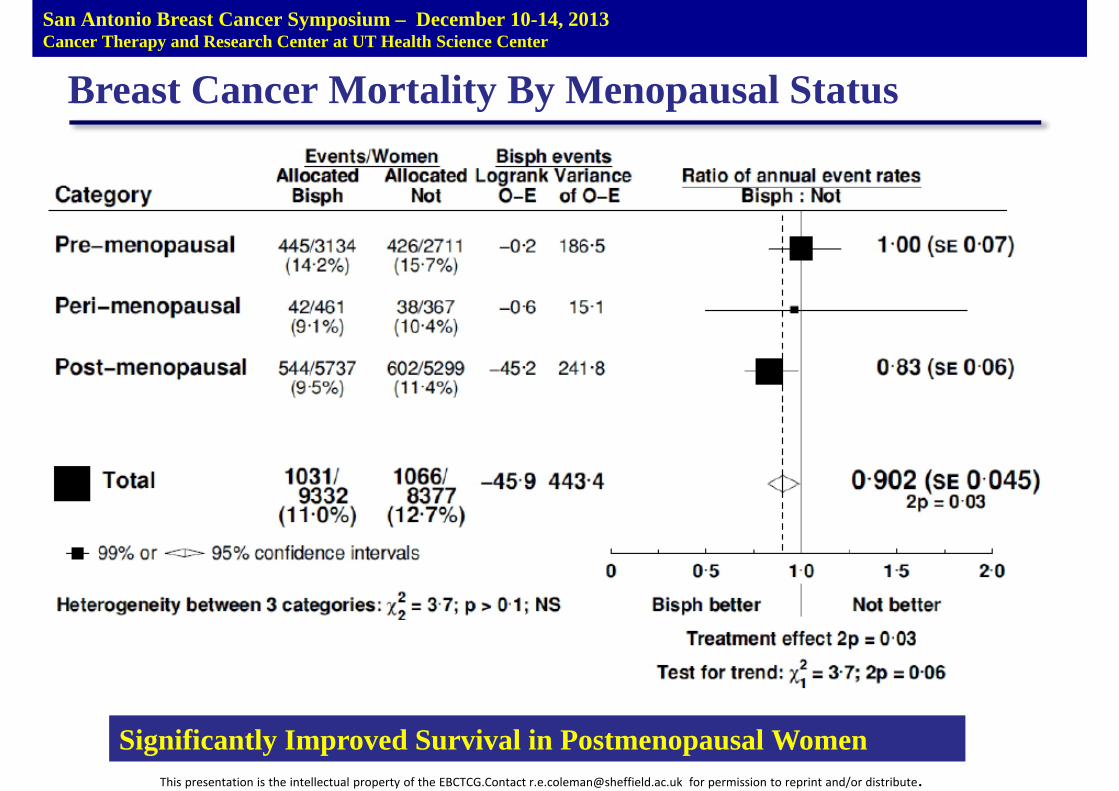
Breast Cancer Mortality By Menopausal Status
Significantly Improved Survival in Postmenopausal WomenThis presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
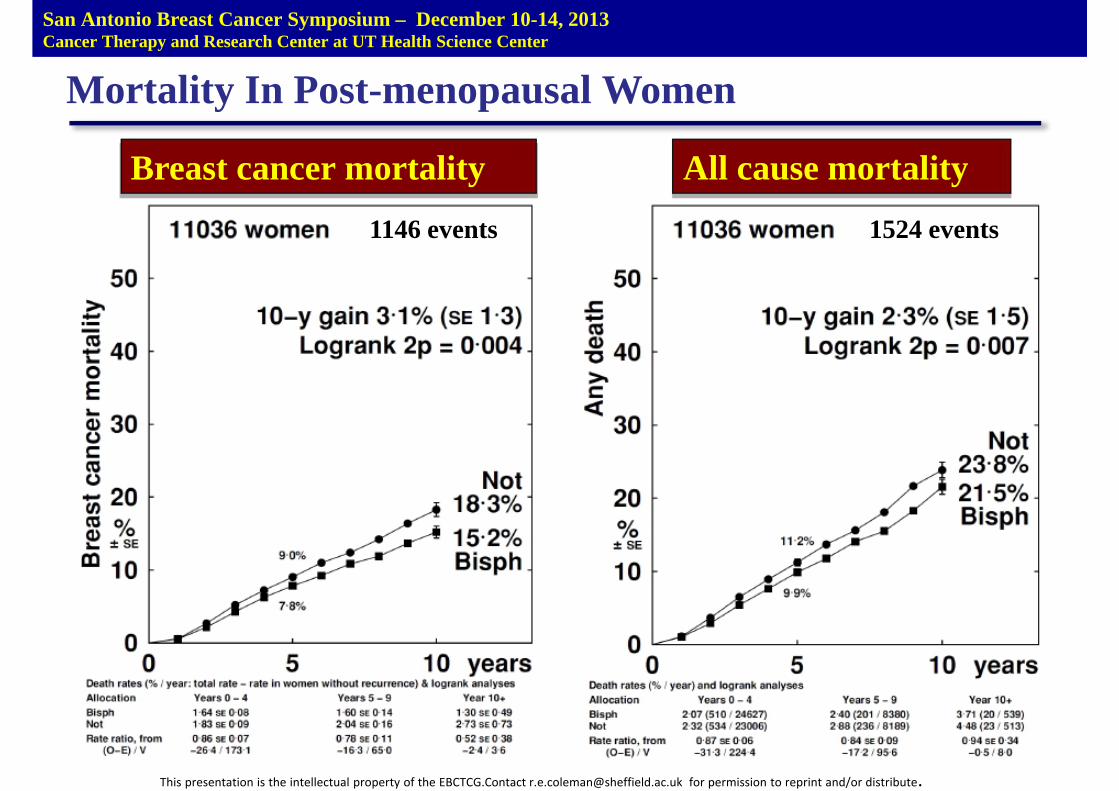
Mortality In Post-menopausal Women
Breast cancer mortality
1146 events
All cause mortality
1524 events
San Antonio Breast Cancer Symposium – December 10-14, 2013Cancer Therapy and Research Center at UT Health Science Center
This presentation is the intellectual property of the EBCTCG.Contact [email protected] for permission to reprint and/or distribute.
Conclusions
• Adjuvant bisphosphonates reduce bone metastases andimprove survival in post-menopausal women.– 34% reduction in risk of bone recurrence (p=0.00001).
– 17% reduction in risk of breast cancer death (p=0.004).
– No significant reduction in first distant recurrence outside bone
– Risk reductions similar irrespective of ER, node status, use/non useof chemotherapy.
– Benefits similar for aminobisphosphonates and clodronate.
• No effects apparent on disease outcomes in pre-menopausalwomen.
• No significant effects on non breast cancer deaths,contralateral breast cancer or loco-regional recurrence.
Postneoadjuvant treatment with zoledronate in patients with tumor residuals
after anthracycline-taxane-based chemotherapy for primary breast cancer – the
phase III NATAN study (GBG 36/ABCSG 29)
Gunter von Minckwitz, Mahdi Rezai, Holger Eidtmann, Hans Tesch, Jens Huober, Bernd Gerber, Dirk Michael
Zahm, Jörn Hilfrich, Serban Costa, Michael Gnant, Jens Uwe Blohmer, Carsten Denkert, Claus Hanusch,
Christian Jackisch, Sherko Kümmel, Peter A. Fasching, Andreas Schneeweiß, Stefan Paepke, Michael Untch,
Valentina Nekljudova, Keyur Mehta, Sibylle Loibl
for the
GBG / AGO-B / ABCSG study groups
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center – December 10-14, 2013
This presentation is the intellectual property of GBG and AGO-B. Contact them at [email protected] for permission to reprint and/or distribute.
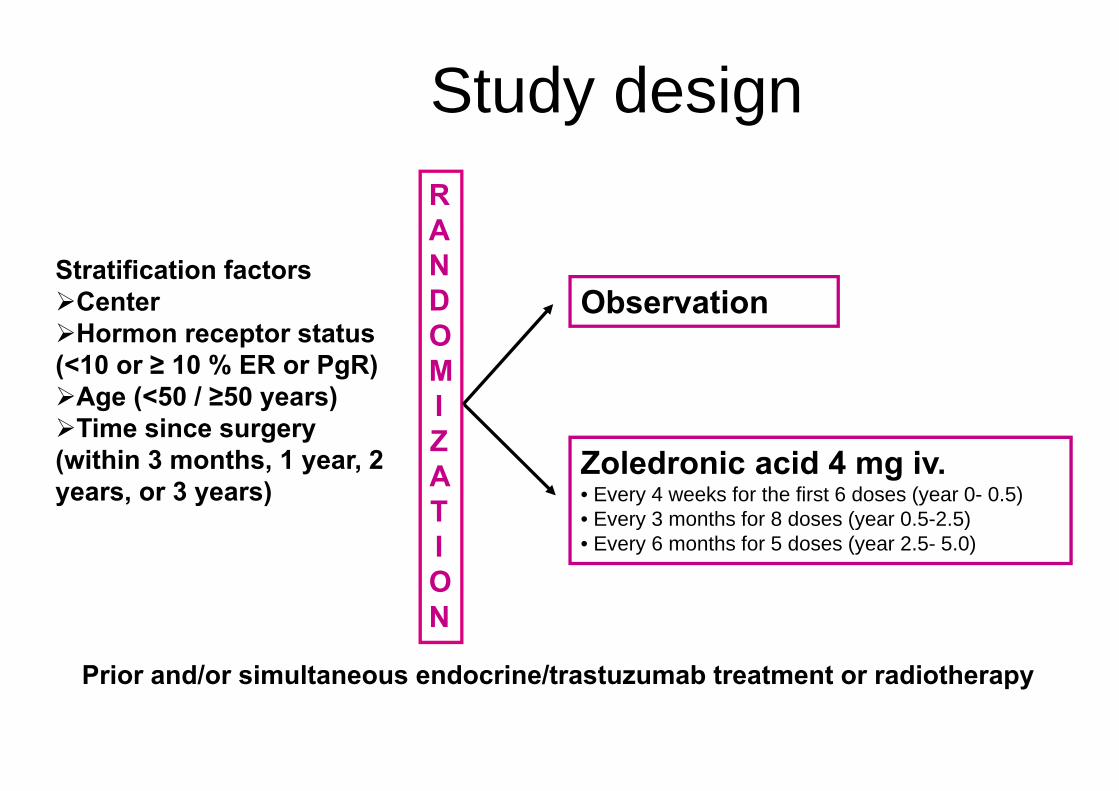
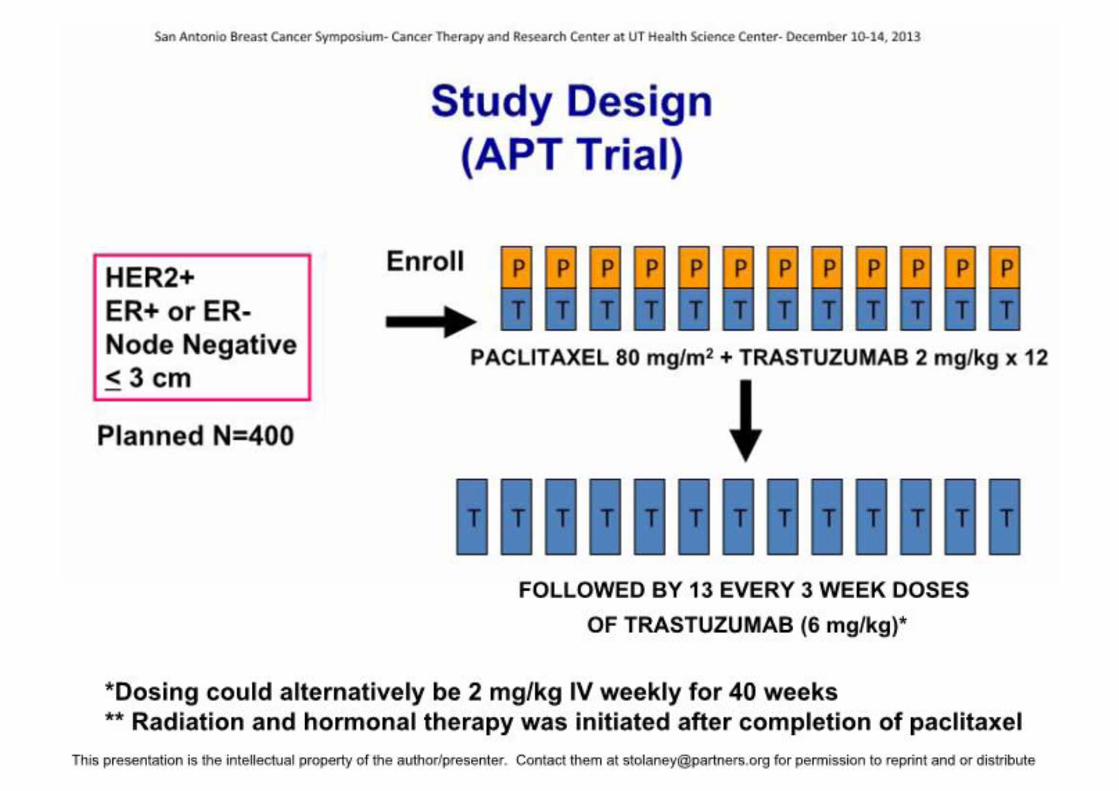
Study design
Observation
RANDOMIZATION
Prior and/or simultaneous endocrine/trastuzumab treatment or radiotherapy
Stratification factorsCenterHormon receptor status
(<10 or ≥ 10 % ER or PgR)Age (<50 / ≥50 years) Time since surgery
(within 3 months, 1 year, 2 years, or 3 years)
Zoledronic acid 4 mg iv.• Every 4 weeks for the first 6 doses (year 0- 0.5)• Every 3 months for 8 doses (year 0.5-2.5)• Every 6 months for 5 doses (year 2.5- 5.0)
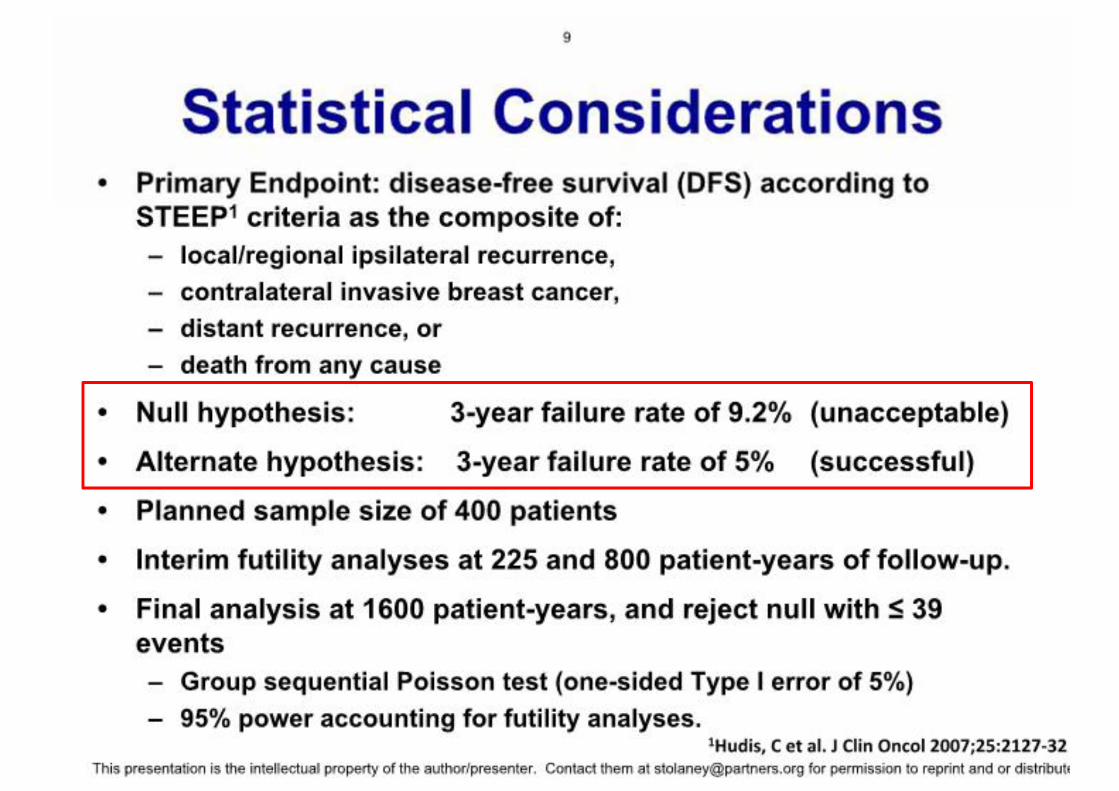
Primary objective• To determine disease-free survival (DFS) after
zoledronic acid for 5 years vs. observation in patients with chemo-insensitive breast cancer after preoperative anthracycline/taxane containing chemotherapy
Event definition: any invasive or non-invasive ipsilateral locoregional, contralateral, distant recurrence, secondary primaries or death due to any cause (corresponding to DFS-DCIS1)
1 Hudis C, JCO 2007
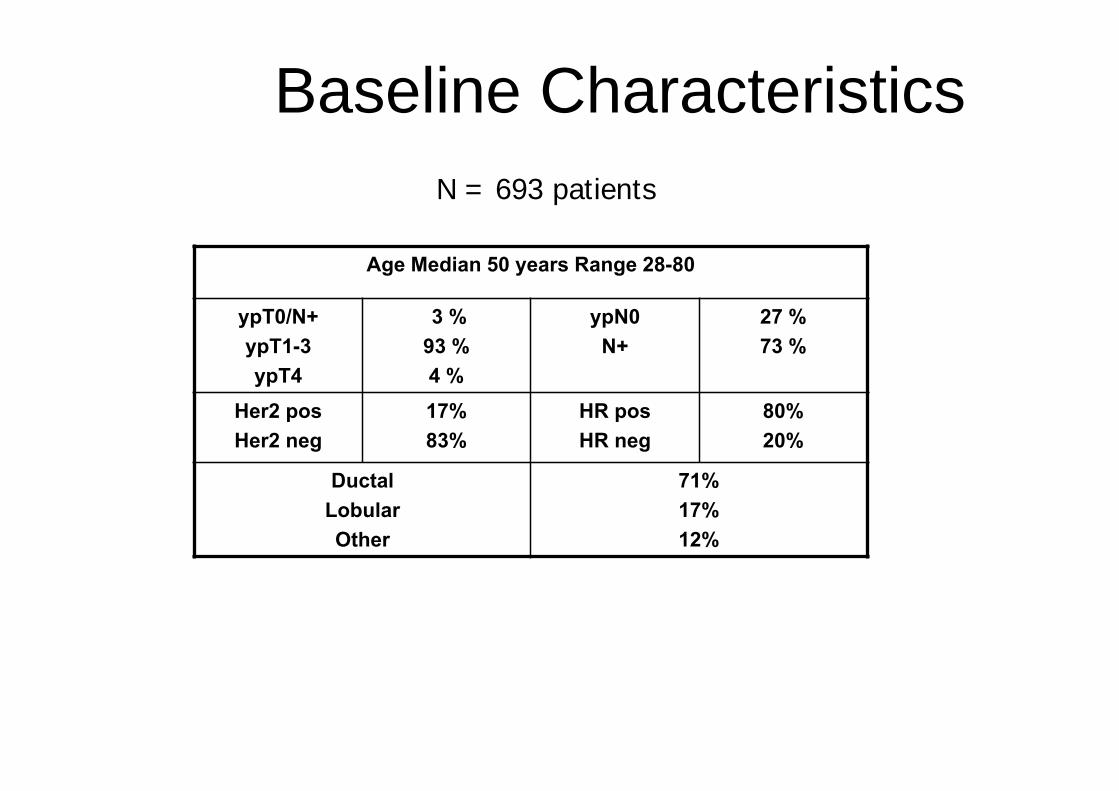
Baseline Characteristics
Age Median 50 years Range 28-80
ypT0/N+ypT1-3ypT4
3 %93 %4 %
ypN0N+
27 %73 %
Her2 posHer2 neg
17%83%
HR posHR neg
80%20%
Ductal Lobular Other
71%17%12%
N = 693 patients
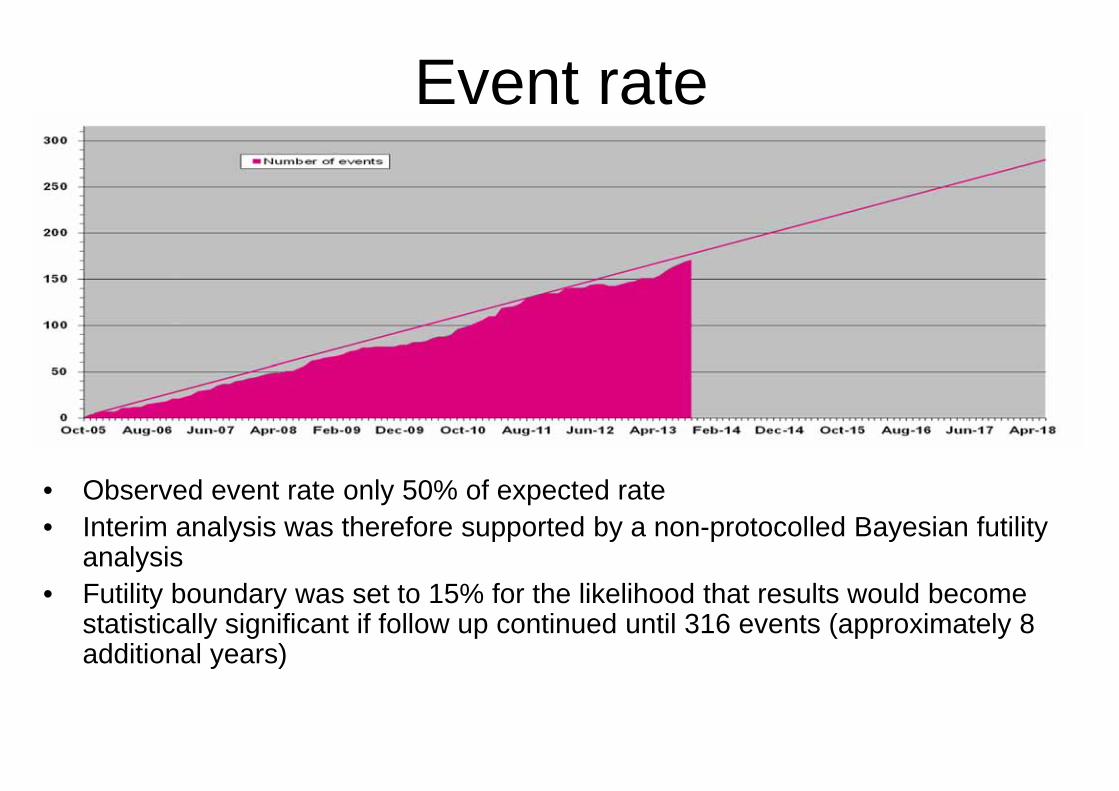
Event rate
• Observed event rate only 50% of expected rate• Interim analysis was therefore supported by a non-protocolled Bayesian futility
analysis• Futility boundary was set to 15% for the likelihood that results would become
statistically significant if follow up continued until 316 events (approximately 8 additional years)
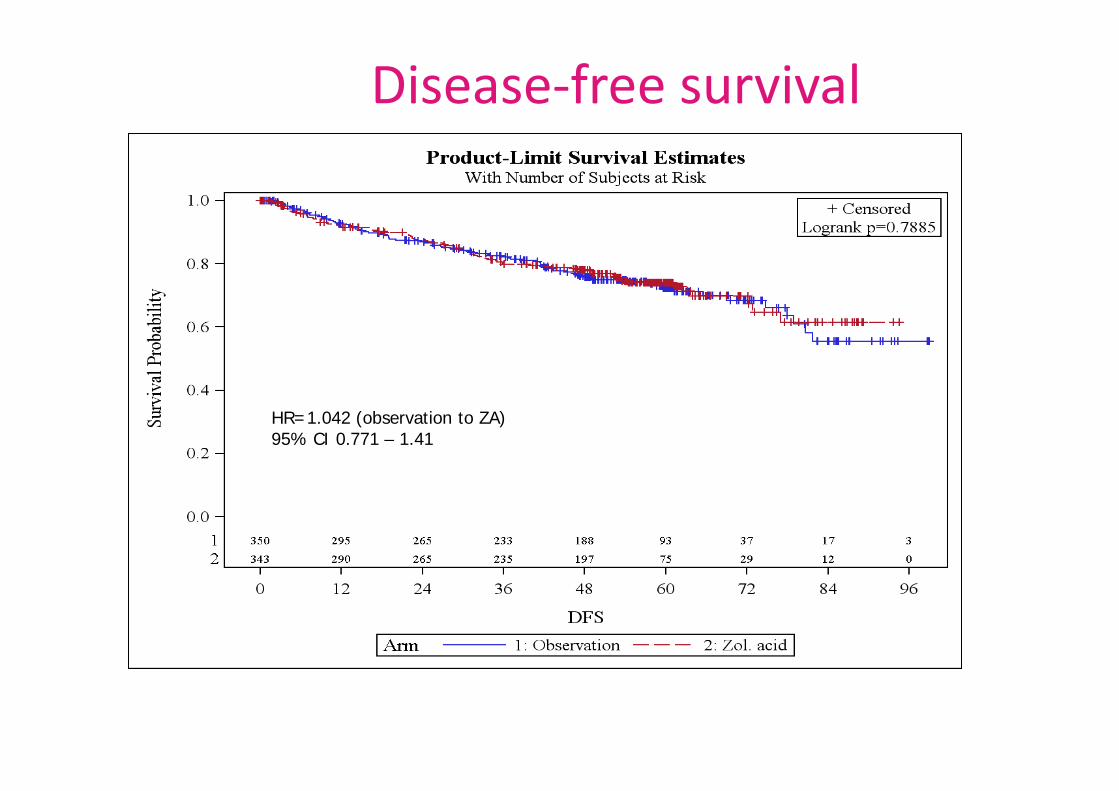
Disease‐free survival
HR=1.042 (observation to ZA)95% CI 0.771 – 1.41
Conclusions• Postneoadjuvant treatment of zoledronate does not
improve outcome in patients without pCR after neoadjuvant anthracycline-taxane-based chemotherapy for early breast cancer.
• No subgroup effect observed• No new safety signal for zoledronate observed• Other options are currently investigated in this setting,
e.g. – Rucaparib (PARP-inh.) in TNBC (BRE09-146)– Trastuzumab emtansine in HER2+ disease (Katherine) – palbociclib in HR+/HER2- disease (Penelope)
BETH: A Randomized Phase III Study Evaluating Adjuvant Bevacizumab Added
to Trastuzumab/Chemotherapy for Treatment of HER2+ Early Breast Cancer
TRIO -011 / NSABP B-44-1 / BO20906
D.Slamon, S.Swain, M.Buyse, M.Martin, C.Geyer, Y-H.Im, T.Pienkowski, S-B.Kim, N.Robert, G.Steger, J.Crown, S.Verma, W.Eiermann,
J.Costantino, SA.Im, E.Mamounas, L.Schwartzberg, A.Paterson, J.Mackey, L.Provencher, M.Press, M.Thirlwell, V.Bee-Munteanu,
V.Henschel, A.Crepelle-Flechais, N.Wolmark
Slamon et al, SABCS 2013
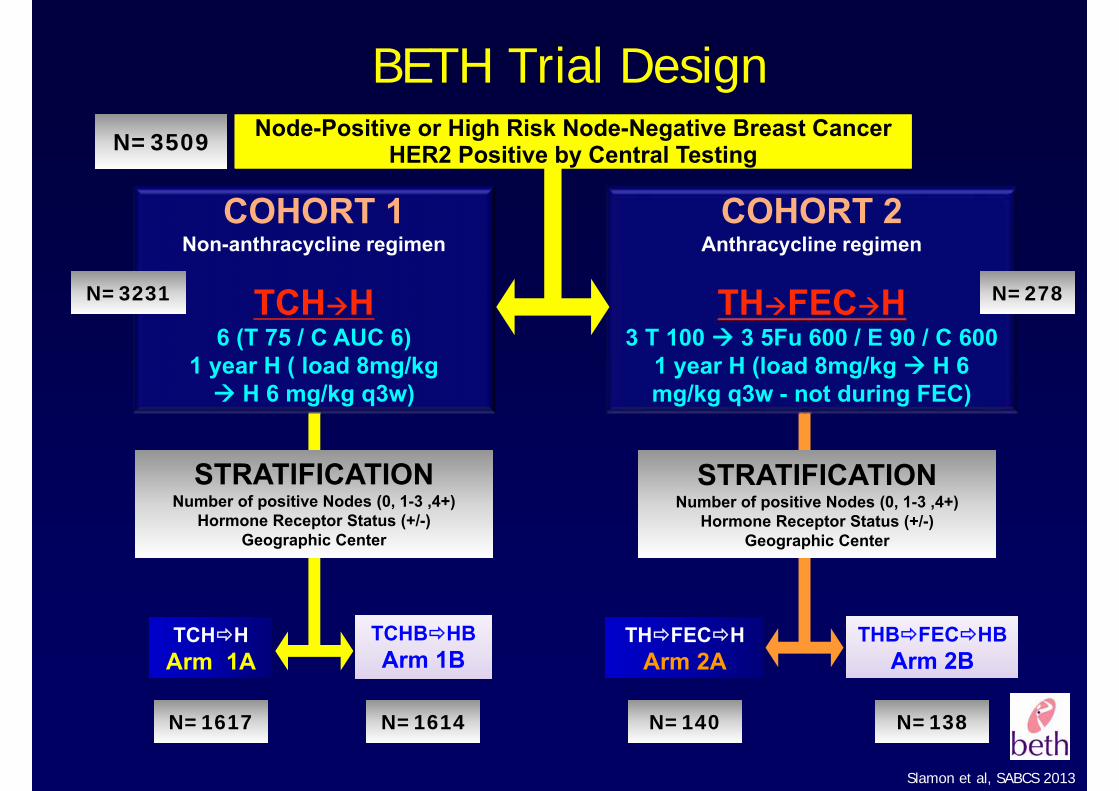
BETH Trial Design
STRATIFICATIONNumber of positive Nodes (0, 1-3 ,4+)
Hormone Receptor Status (+/-)Geographic Center
COHORT 1Non-anthracycline regimen
TCH H6 (T 75 / C AUC 6)
1 year H ( load 8mg/kgH 6 mg/kg q3w)
COHORT 2Anthracycline regimen
TH FEC H3 T 100 3 5Fu 600 / E 90 / C 600
1 year H (load 8mg/kg H 6 mg/kg q3w - not during FEC)
TCH HArm 1A
TCHB HBArm 1B
TCHB HBArm 1B
TH FEC HArm 2A
THB FEC HBArm 2B
THB FEC HBArm 2B
N=3509
N=3231 N=278
N=1617 N=1614 N=140 N=138
STRATIFICATIONNumber of positive Nodes (0, 1-3 ,4+)
Hormone Receptor Status (+/-)Geographic Center
Node-Positive or High Risk Node-Negative Breast Cancer HER2 Positive by Central Testing
Node-Positive or High Risk Node-Negative Breast Cancer HER2 Positive by Central Testing
Slamon et al, SABCS 2013
BETH Assumptions
BETH: Assumptions based on results of BCIRG-006 (AC→T vs AC→TH vs TCH) at 3-year follow-up:
• 86% DFS on TCH arm
• 87% DFS on AC→TH arm
Slamon et al, SABCS 2013
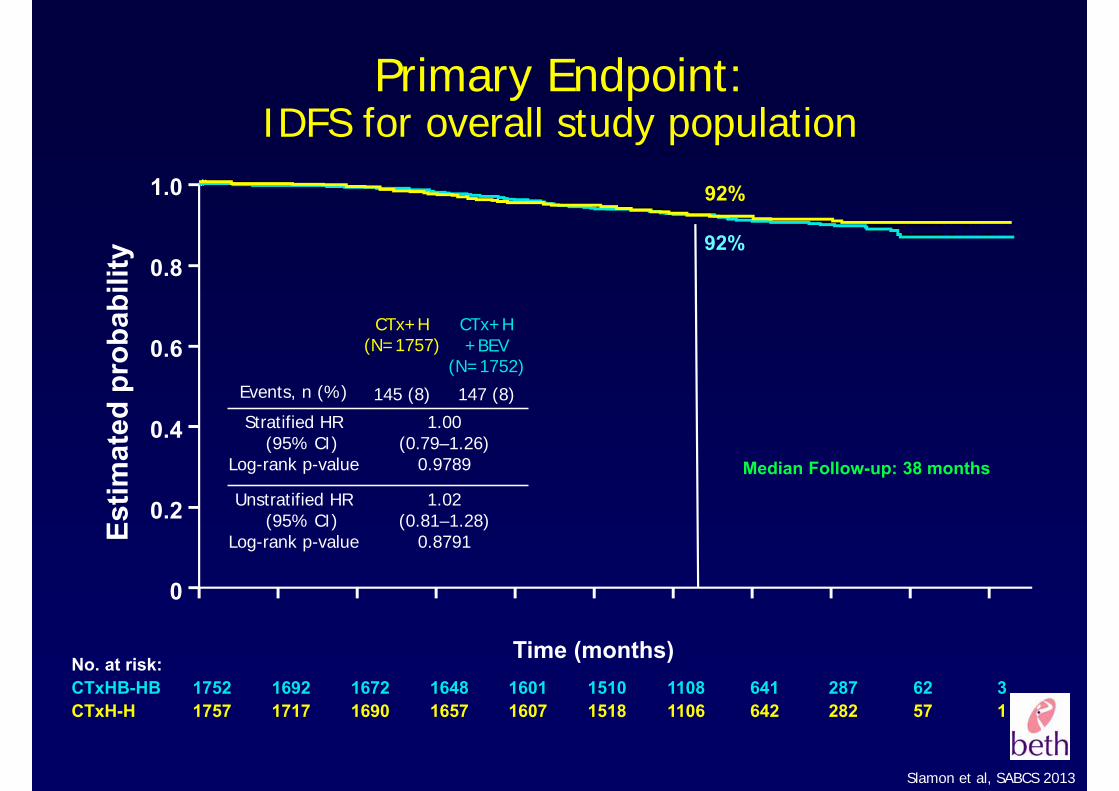
Primary Endpoint: IDFS for overall study population
1.0
0.8
0.6
0.4
0.2
0
No. at risk:CTxHB-HB 1752 1692 1672 1648 1601 1510 1108 641 287 62 3CTxH-H 1757 1717 1690 1657 1607 1518 1106 642 282 57 1
Time (months)
Estim
ated
pro
babi
lity
92%
92%
Median Follow-up: 38 months
CTx+H(N=1757)
CTx+H+BEV
(N=1752)Events, n (%) 145 (8) 147 (8)
Stratified HR (95% CI)
Log-rank p-value
1.00(0.79–1.26)
0.9789
Unstratified HR (95% CI)
Log-rank p-value
1.02(0.81–1.28)
0.8791
Slamon et al, SABCS 2013
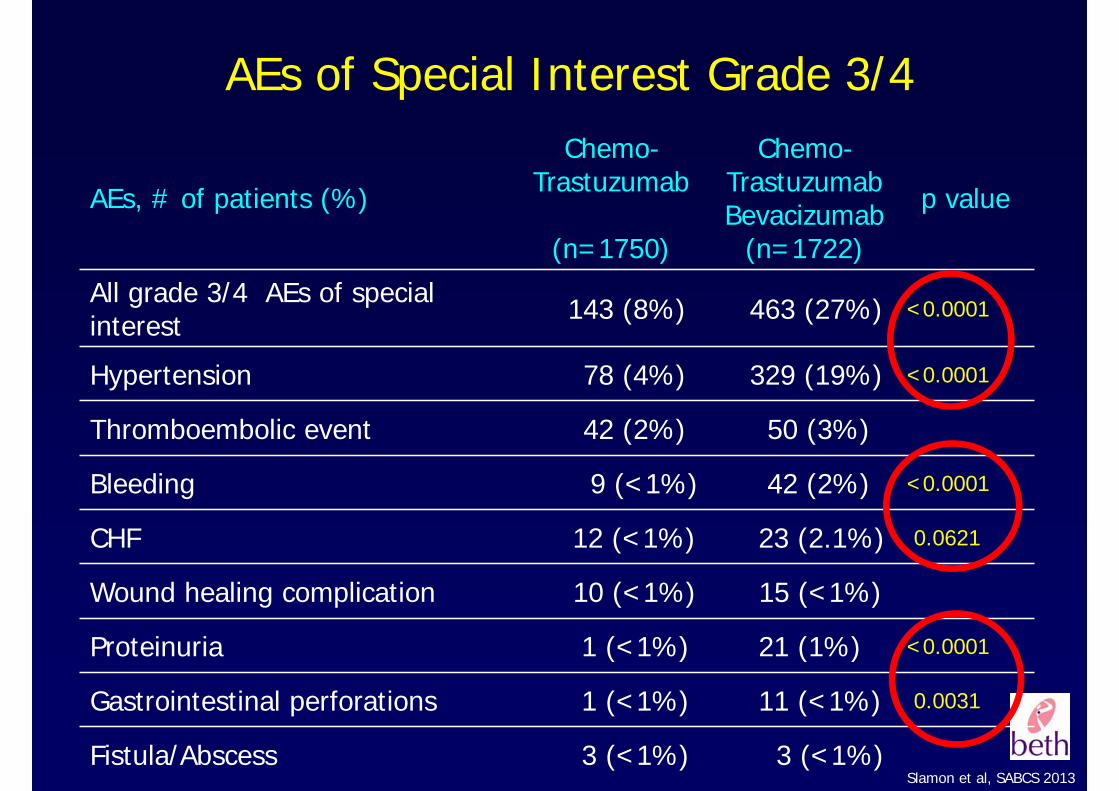
AEs of Special Interest Grade 3/4
AEs, # of patients (%)
Chemo-Trastuzumab
(n=1750)
Chemo-TrastuzumabBevacizumab
(n=1722)
p value
All grade 3/4 AEs of special interest 143 (8%) 463 (27%) <0.0001
Hypertension 78 (4%) 329 (19%) <0.0001
Thromboembolic event 42 (2%) 50 (3%)
Bleeding 9 (<1%) 42 (2%) <0.0001
CHF 12 (<1%) 23 (2.1%) 0.0621
Wound healing complication 10 (<1%) 15 (<1%)
Proteinuria 1 (<1%) 21 (1%) <0.0001
Gastrointestinal perforations 1 (<1%) 11 (<1%) 0.0031
Fistula/Abscess 3 (<1%) 3 (<1%)
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
26.01.201453
San Antonio 2013 | Prof. Harbeck
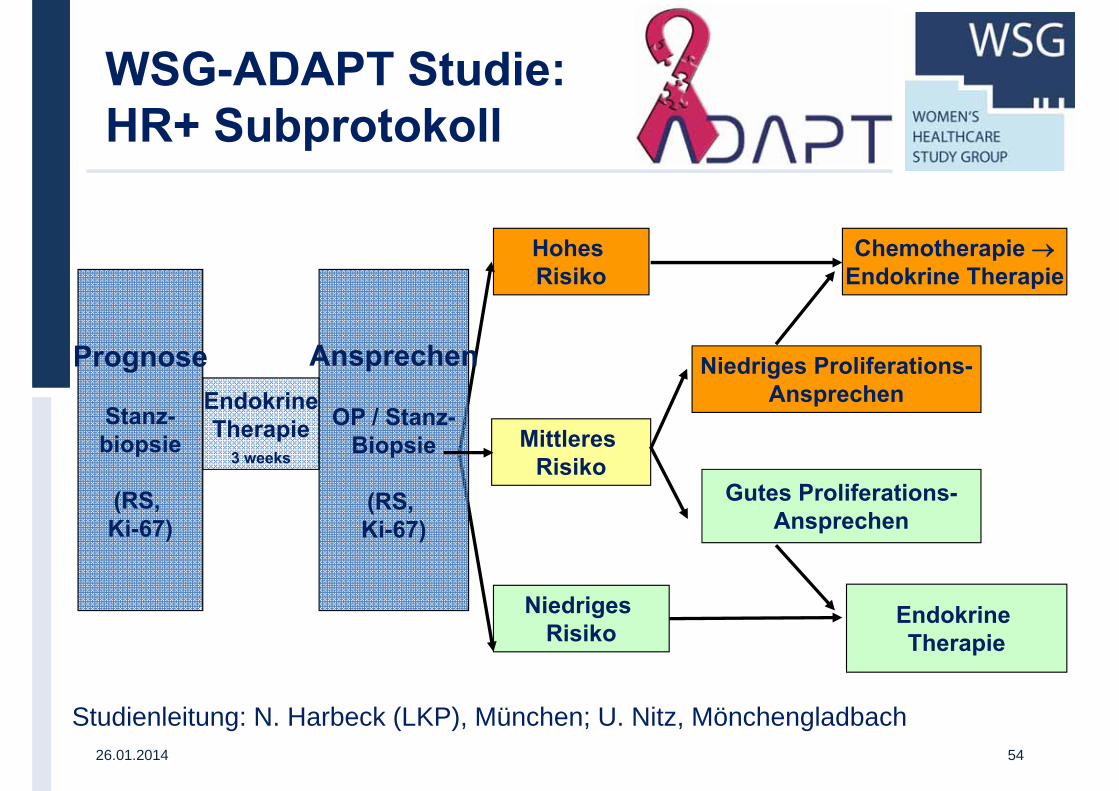
Prognose
Stanz-biopsie
(RS, Ki-67)
EndokrineTherapie
3 weeks
Hohes Risiko
Mittleres Risiko
Niedriges Risiko
Endokrine Therapie
Ansprechen
OP / Stanz-Biopsie
(RS, Ki-67)
Gutes Proliferations-Ansprechen
Niedriges Proliferations-Ansprechen
Chemotherapie →Endokrine Therapie
Studienleitung: N. Harbeck (LKP), München; U. Nitz, Mönchengladbach
WSG-ADAPT Studie: HR+ Subprotokoll
26.01.2014 54
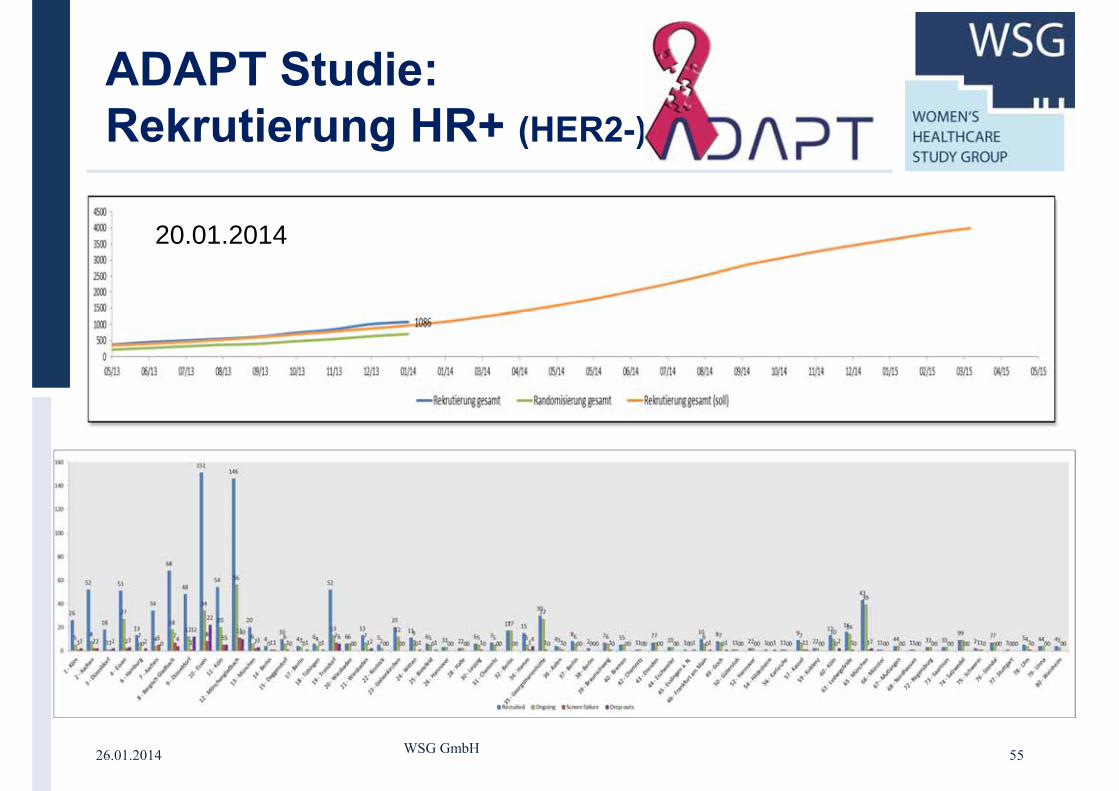
26.01.2014 WSG GmbH 55
20.01.2014
ADAPT Studie: Rekrutierung HR+ (HER2-)
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
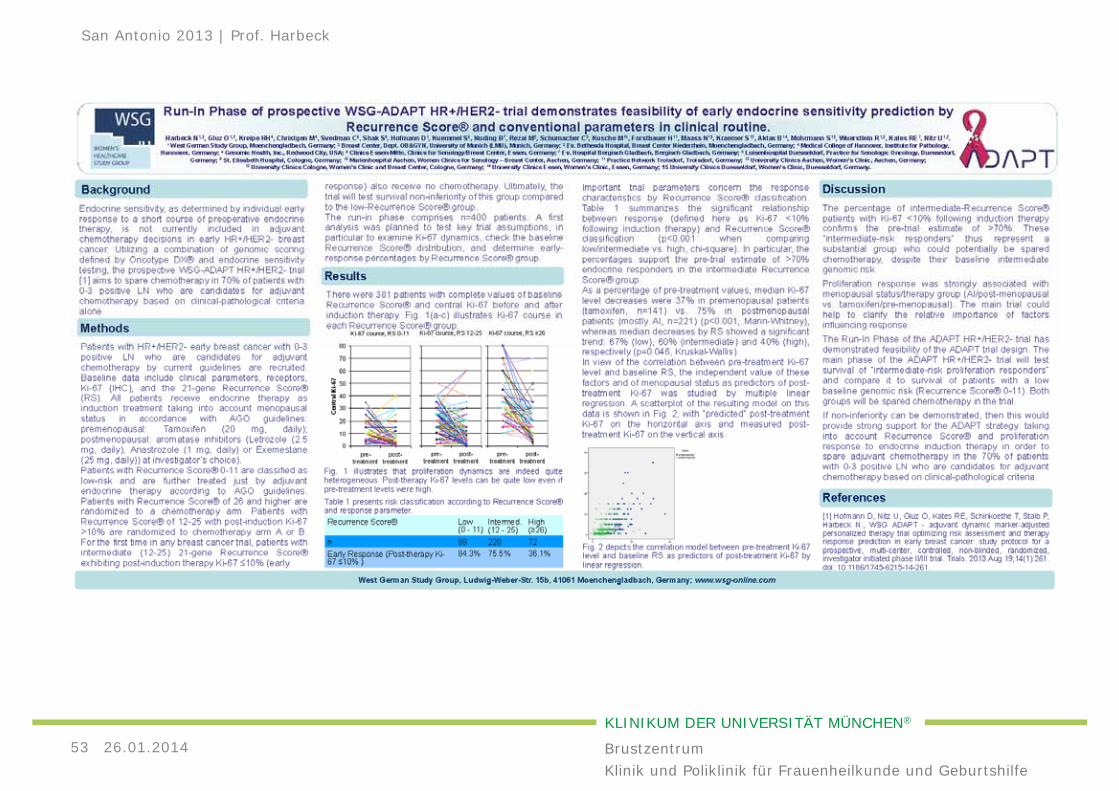
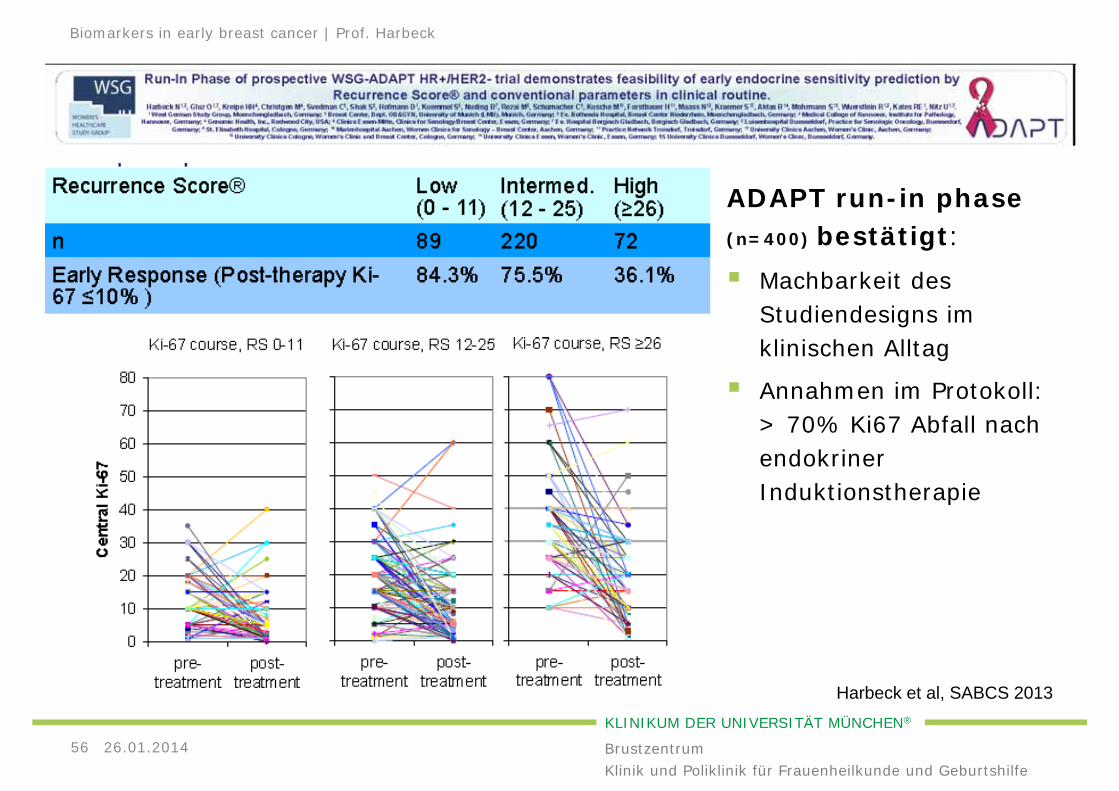
ADAPT run-in phase(n=400) bestätigt:
Machbarkeit des Studiendesigns im klinischen Alltag
Annahmen im Protokoll: > 70% Ki67 Abfall nach endokriner Induktionstherapie
26.01.201456
Biomarkers in early breast cancer | Prof. Harbeck
Harbeck et al, SABCS 2013
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
26.01.201457
San Antonio 2013 | Prof. Harbeck
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
PRIMÄRES MAMMAKARZINOMNACH SAN ANTONIO 2013:
26.01.201458
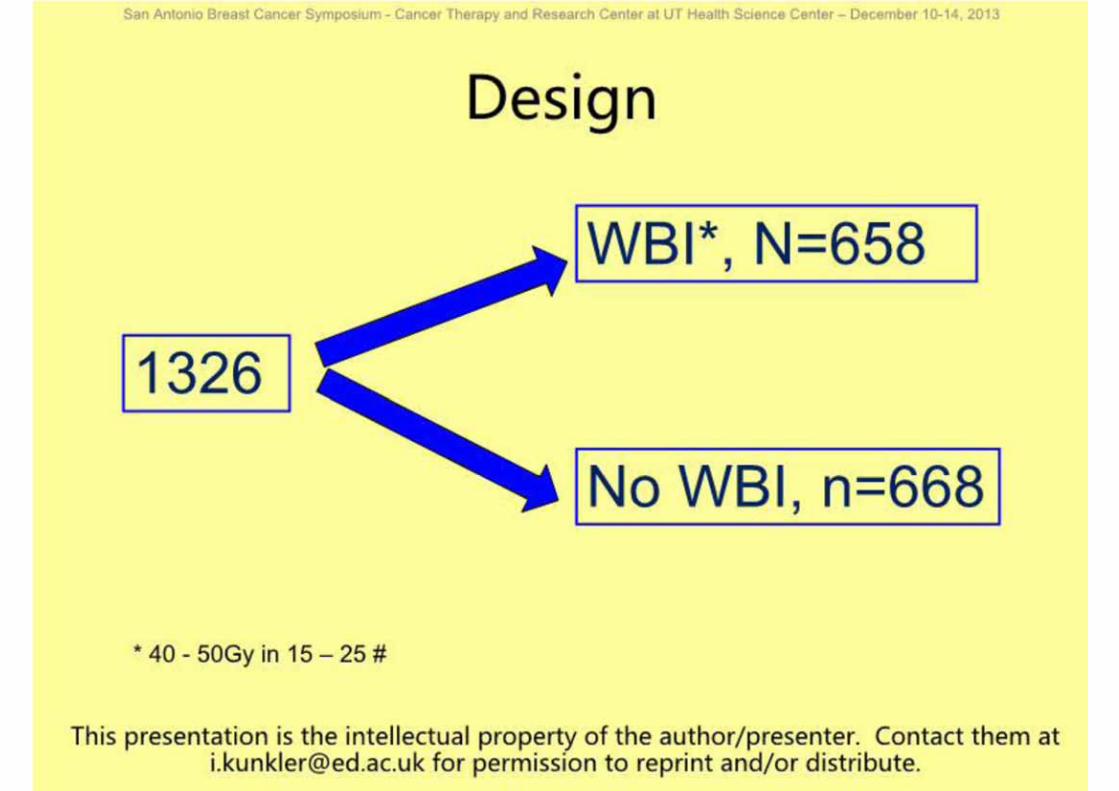
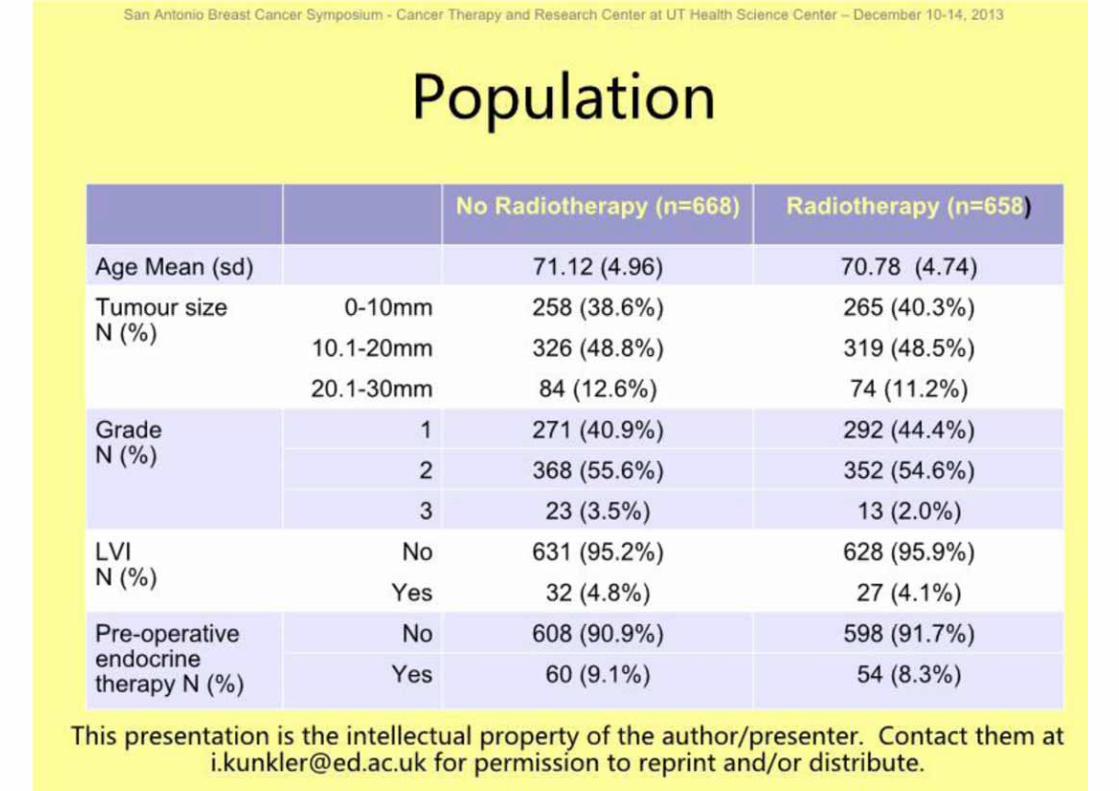
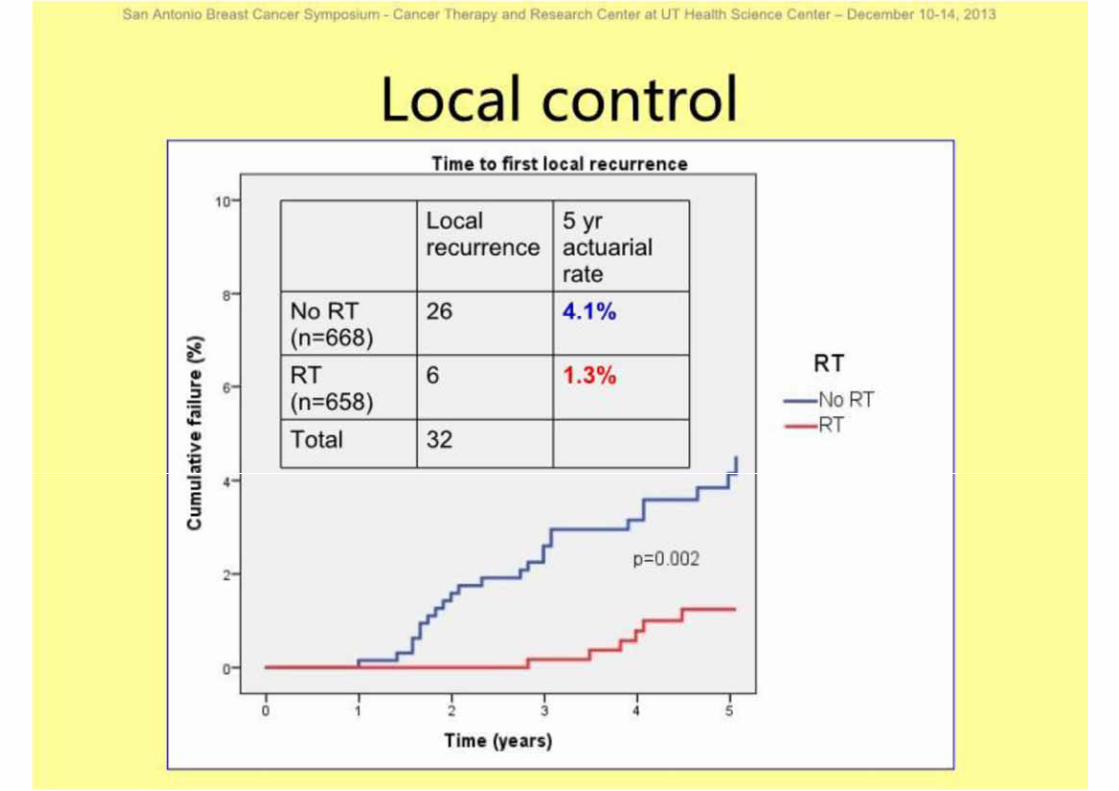
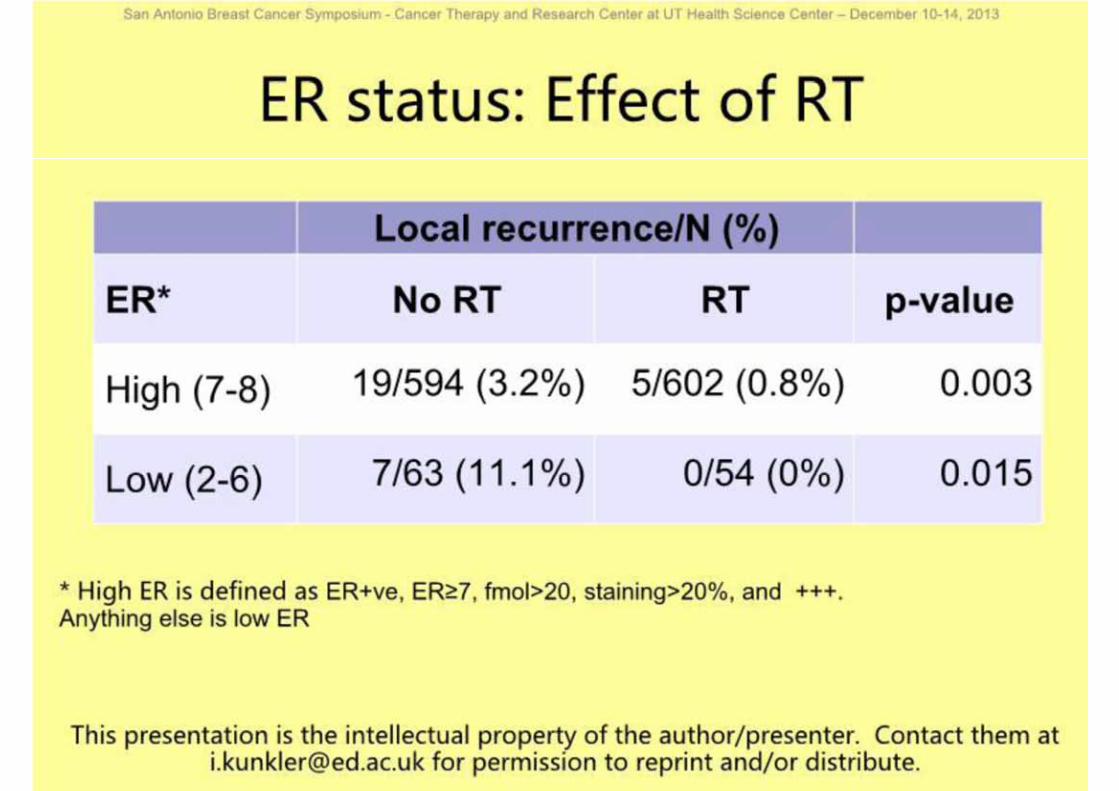
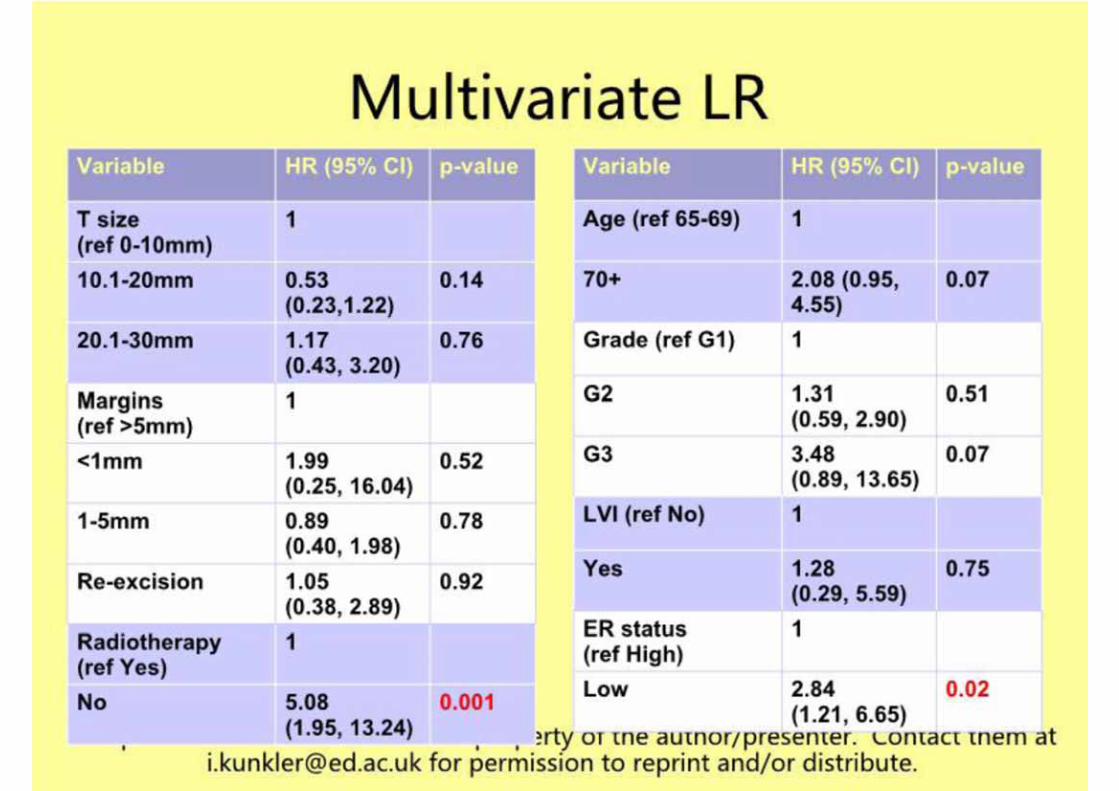
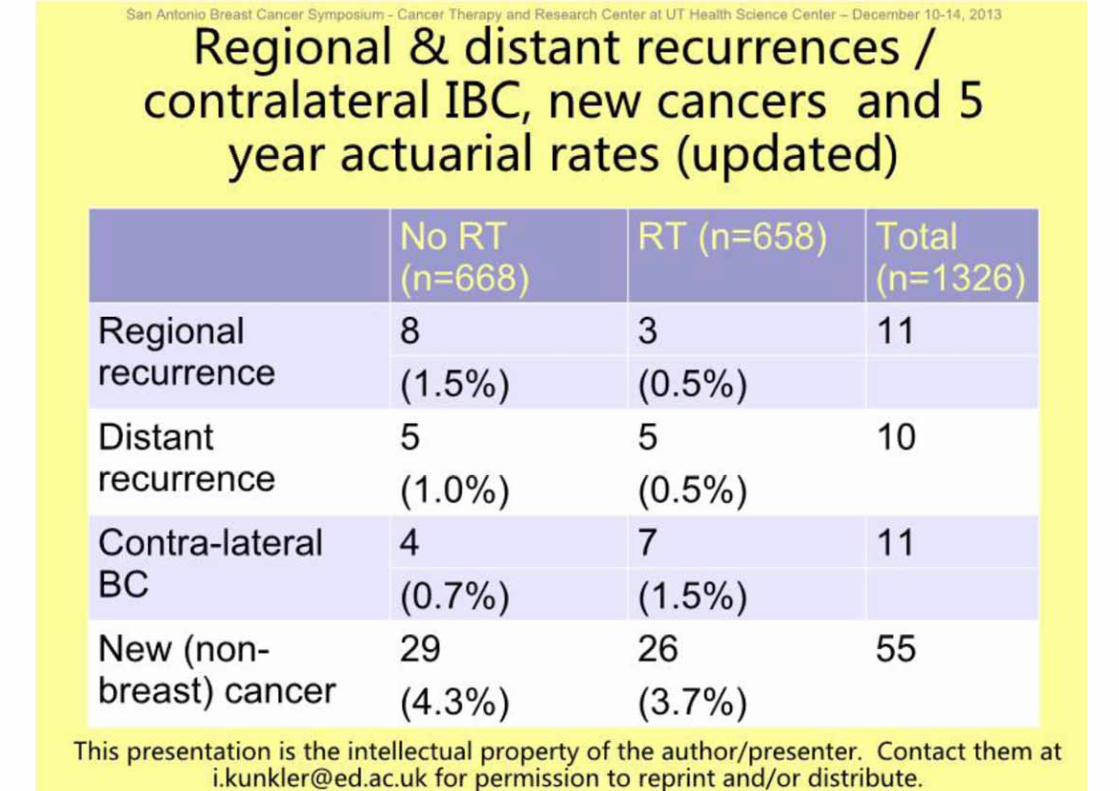
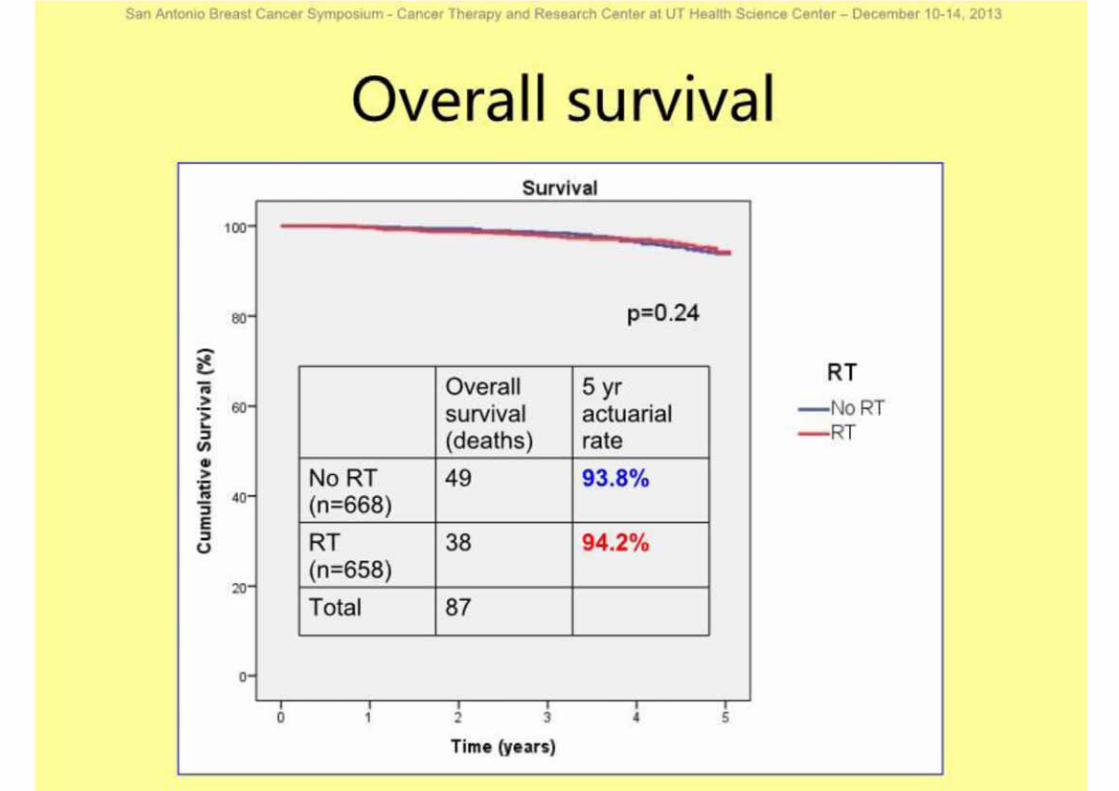
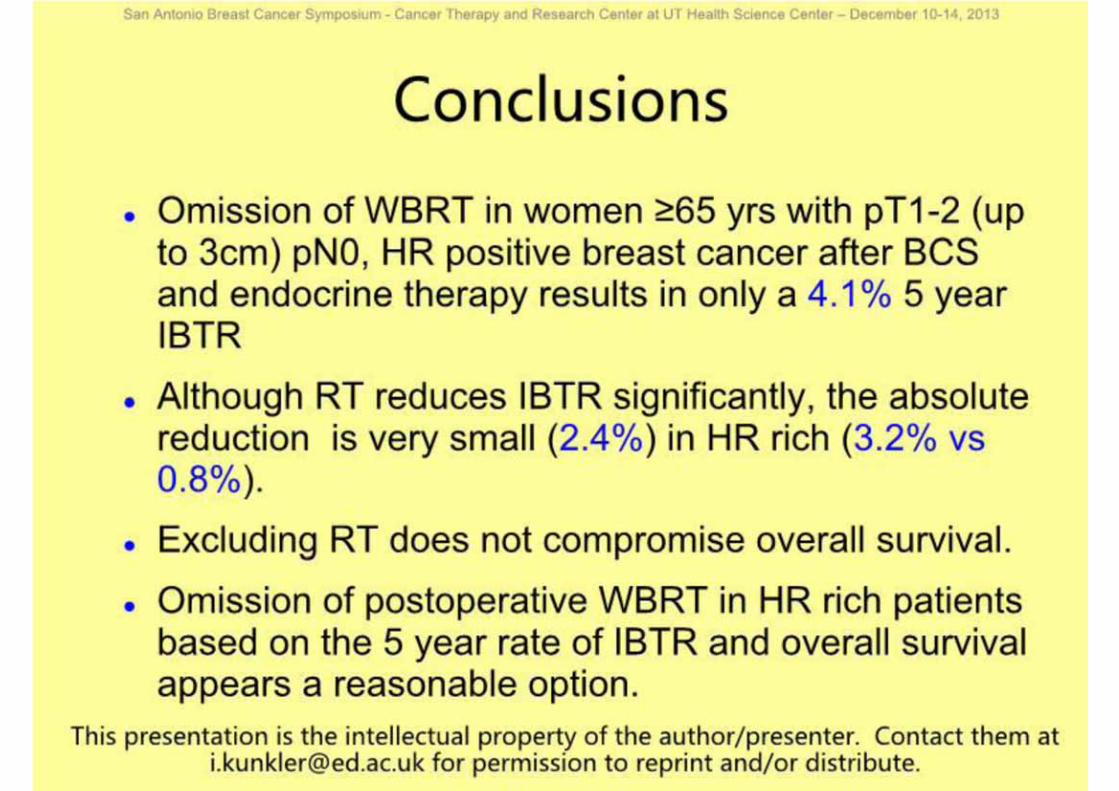
Adjuvante Strahlentherapie: Strahlentherapie verbessert lokale Kontrolle nicht aber Gesamtüberleben bei älteren Patientinnen mit low riskhormonempfindlichen TumorenDifferenzierte Aufklärung auch über Alternativen (z.B. IORT, Hypofraktionierung) erforderlich
San Antonio 2013 | Prof. Harbeck
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
PRIMÄRES MAMMAKARZINOMNACH SAN ANTONIO 2013:
26.01.201459
Adjuvante Bisphosphonat-therapie: Signifikanter Effekt auf Knochenmetastasen und Brustkrebs-bedingte Mortalität nur bei POSTmenopausalen Frauen:unabhängig von ER Status oder Bisphosphonat-Regime (oral vs. i.v.)
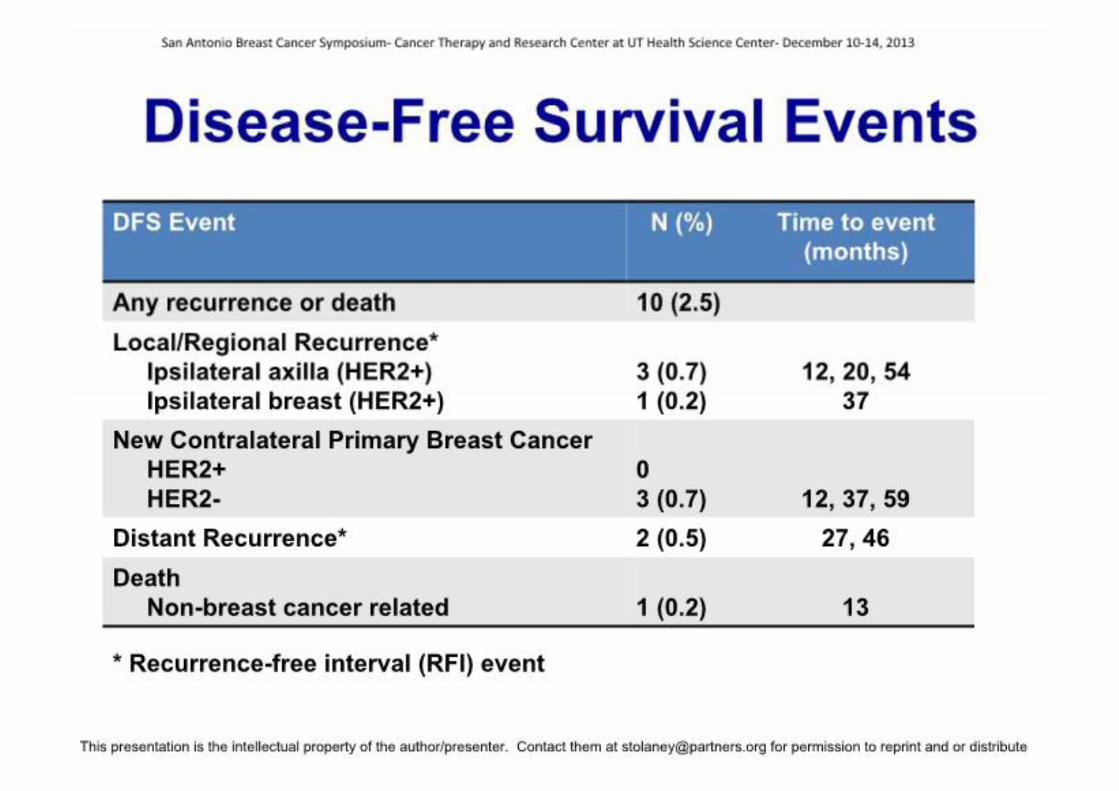
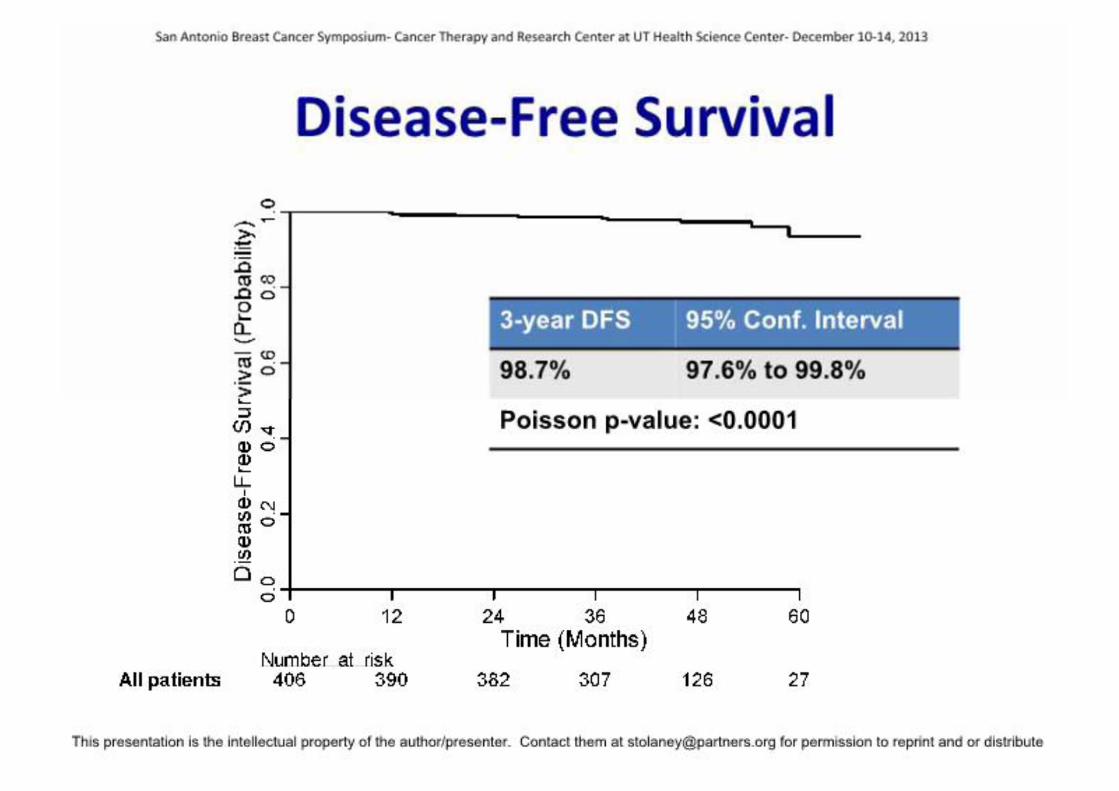
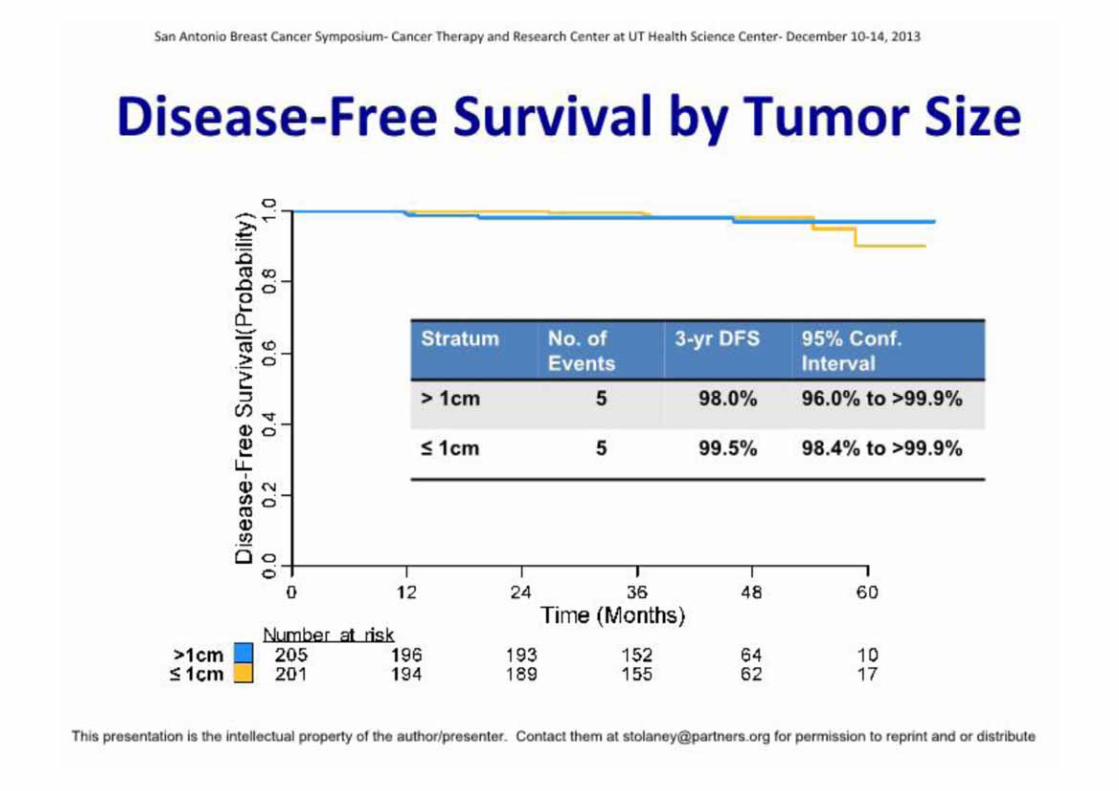
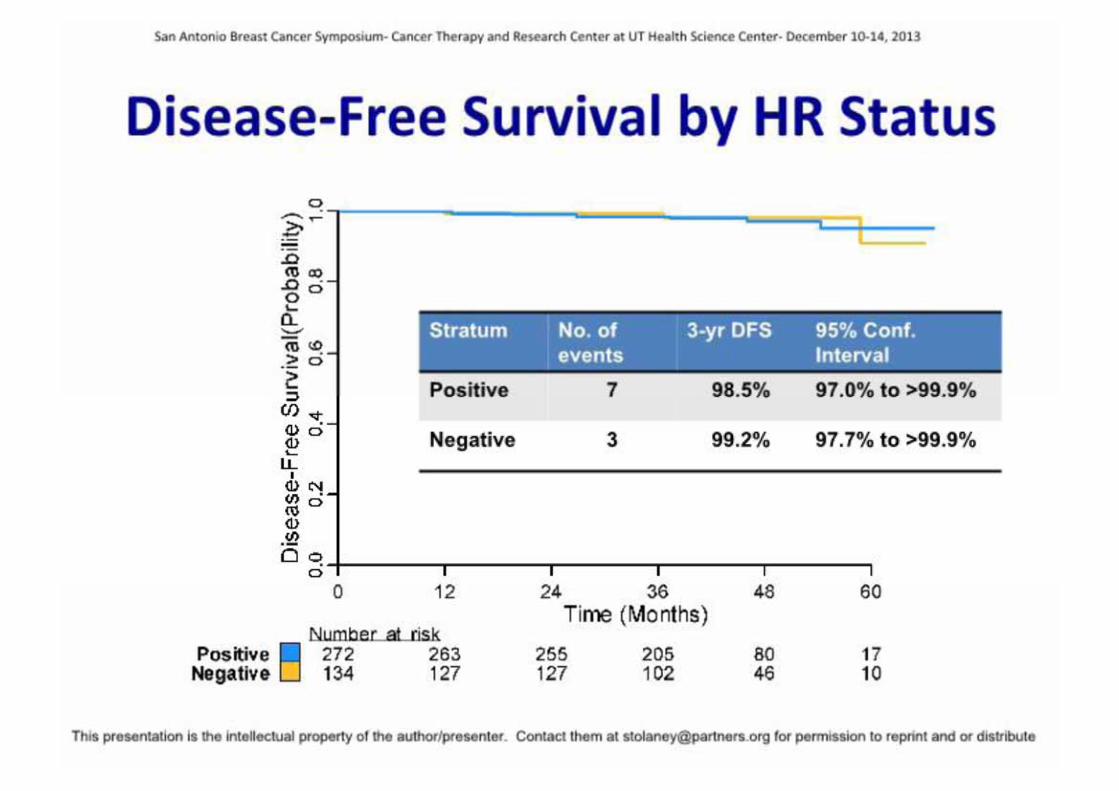
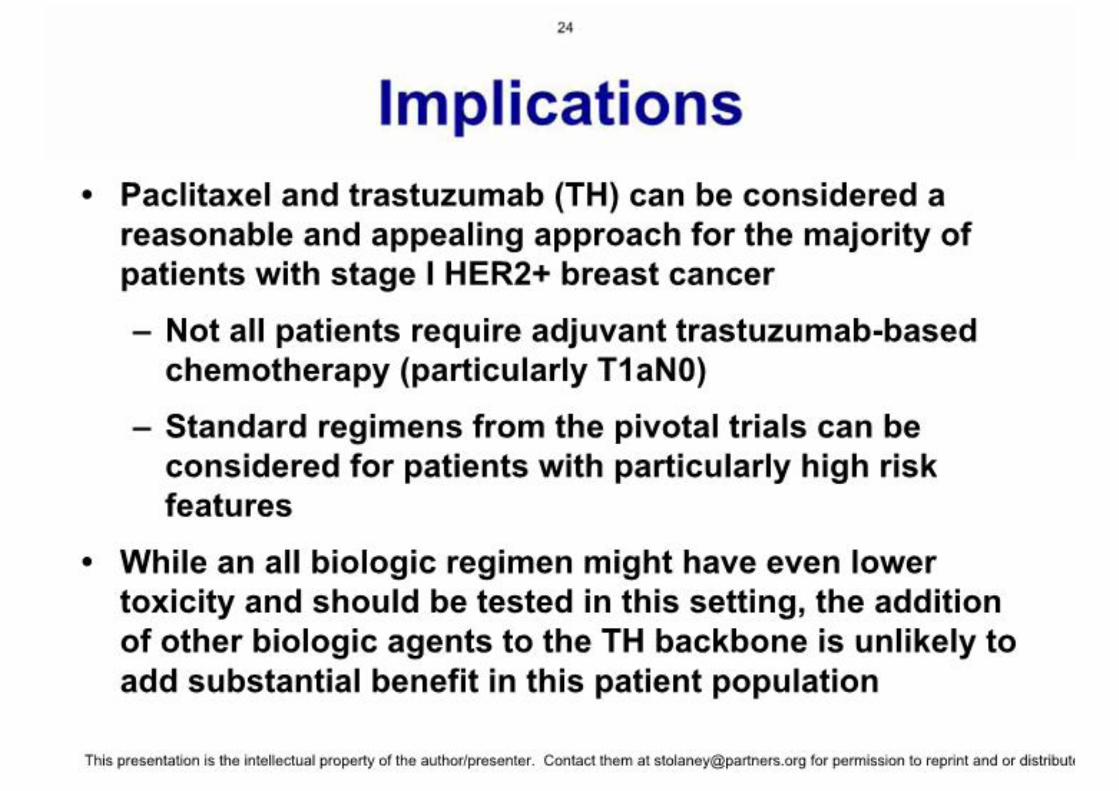
HER2-positiv:Frühes Mammakarzinom (Stadium I):Exzellentes Outcome nach Paclitaxel und Trastuzumab (3 Jahres DFS 98,7%)Studie beantwortet nicht die Frage, welche Pat. KEINE Chemotherapie mit Trastuzumab benötigt
BETH-Studie: keine Rolle für Bevacizumab
San Antonio 2013 | Prof. Harbeck

KLINIKUM DER UNIVERSITÄT MÜNCHEN®
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
26.01.201460
www.karger.com/brc
EVIDENZBASIERTE BRUSTKREBS-THERAPIE
AGO (DKG, DGGG) www.ago-online.de
Jährlich aktualisierte, evidenzbasierte Empfehlungen zur Diagnostik und Therapie
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
26.01.201461
San Antonio 2013 | Prof. Harbeck
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
26.01.201462
San Antonio 2013 | Prof. Harbeck
BrustzentrumKlinik und Poliklinik für Frauenheilkunde und Geburtshilfe
KLINIKUM DER UNIVERSITÄT MÜNCHEN®
26.01.201463
San Antonio 2013 | Prof. Harbeck



![Neues aus der Stadtverwaltung DA[L]HEIM · Neues aus der Stadtverwaltung Neues aus der Stadtverwaltung Sozialausschuss tagt in Dalheim Bereits zum zweiten Mal seit seinem Bestehen](https://img.pdfslide.net/doc/110x75/5ccd90d988c9932b558df865/neues-aus-der-stadtverwaltung-dal-neues-aus-der-stadtverwaltung-neues-aus.jpg)
![Neues aus der Vergangenheit - IslamHouse.com · 2000. 3. 26. · Neues aus der Vergangenheit [ Deutsch – German – ﺎﻟﻤ ] Quelle : 2012 - 1434](https://img.pdfslide.net/doc/110x75/5feec8ae166a2f0c7f62795d/neues-aus-der-vergangenheit-2000-3-26-neues-aus-der-vergangenheit-deutsch.jpg)
























