Embed Size (px)
Citation preview

Neural Mobilization: A Systematic Review of Randomized ControlledTrials with an Analysis of Therapeutic Efficacy
Richard F. Ellis, B. Phly, Post Grad DipWat/ne A. Hing, PT, PhD
Abstract: Neural mobilization is a treatment modality used in relation to pathologies of the nervoussystem. It has been suggested that neural mobilization is an effective treatment modality, althoughsupport of this suggestion is primarily anecdotal. The purpose of this paper was to provide a systematicreview ofthe literature pertaining to the therapeutic efficacy of neural mobilization. A search to identifyrandomized controlled triais investigating neural mobilization was conducted using the key words neu-ral mobilisation/mobilization, nerve mobilisation/mobilization, neural manipulative physical therapy,physica (therapy, neurallnen>e glide, nerve glide exercises, nerve/neural treatment, nerve/neural stretch-ing, neurodynamics, and nemelneural physiotherapy. The titles and abstracts ofthe papers identifiedwere reviewed to select papers specifically detailing neural mobilization as a treatment modality. ThePEDro scale, a systematic tool used to critique RCTs and grade methodological quality, was used to as-sess these trials. Methodological assessment allowed an analysis of research investigating therapeuticefficacy of neural mobilization. Ten randomized clinical trials (discussed in 11 retrieved articles} wereidentified that discussed the therapeutic effect of neural mobilization. This review highlights the lackin quantity and quality of the available research. Qualitative analysis of these studies revealed that thereis only limited evidence to support the use of neura! mobilization. Future research needs to re-examinethe application of neural mobilization with use of more homogeneous study designs and pathologies:in addition, it should standardize the neural mobilization interventions used in the study.
Keywords: Neural Mobilization, Neurodynamics, Randomized Controlled Trial, Systematic Review,Therapeutic Efficacy.
In the past, neural tension was used to describe dysfunc-tion of the peripheral nervous system. More recently,tbere has been a shift away from a purely mecbanical
rationale to include physiological concepts sucb as structureand function of the nervous system. Neurodynamics is nowa more accepted term referring to tbe integrated biome-cbanical, physiological, and morphological functions ofthenervous system' . Regardless of the underlying construct,it is vital that the nervous system is able to adapt to mechani-
Address all correspondence and requests for reprints to:
Richard Ellis
Lecturer
School of Physiotherapy
Auckland University of Technology (AUT)
Private Bag 92006
Auckland New Zealand 1020E-mail: richard.ellisC'*aut.ac.nz
cal loads, and it must undergo distinct mechanical eventssucb as elongation, sliding, cross-sectional change, angula-tion. and compression. If these dynamic protective mecha-nisms fail, the nervous system is vulnerable to neural edema,ischaemia. fibrosis, and hypoxia. which may cause alteredneurodynamics'-.
When neura! mobilization is used for treatment of ad-verse neurodynamics, the primary theoretical objective is toattempt to restore the dynamic balance between the relativemovement of neural tissues and surrounding mechanicalinterfaces, thereby allowing reduced intrinsic pressures onthe neural tissue and thus promoting optimum physiologicfunction'-''. The hypothesized benefits from such tech-niques include facilitation of nerve gliding, reduction of nerveadherence, dispersion of noxious fluids, increased neural vas-cularity, and improvement of axoplasmic flow' -"". However,these etiological mechanisms for the clinically observed ef-fects of neural mobilization still require robust validation. Atpresent, the positive clinically observed effect of neural mo-
8 / The Journal of Manual & Manipulative Therapy, 2008The Journal of Manual & Manipulative TherapyVol. 16 No. I (2008), 8-22
biiization is mainly based on anecdotal evidence. Therefore,the purpose of this paper was to systematically review andassess the therapeutic efficacy of neural mobilization fortreatment of altered neurodynamics through evaluation ofappropriate randomized controlled trials (RCTs). It was hy-pothesized that the findings might guide evidence-basedpractice in the clinical application of neural mobilization.
Methods
Literature Search Strategy
A search to identify RCTs examining neural mobilization wasconducted in March 2007. The following electronic databaseswere searched: MEDLINE via PubMed (from 1966 onwards).Cumulative Index to Nursing and Allied Health Literature
(CINAHL) (from 1982 onwards), the Cochrane ControlledTrials Register in the Cochrane Library (latest edition),SPORT-Discus (from 1830 onwards). Allied and Complemen-tary Medicine Database (AMED) (from 1985 onwards).Physiotherapy Evidence Database (PEDro) (from 1953 on-wards). ProQuest 5000 International, ProQuest Healthand Medical Complete, EBSCO MegaFile Premier, ScienceDirect (from 1995 onwards) and Web of Science (from 1945onwards).
The search strategy of these databases included termsand keywords related to the intervention: neural mobilisa-tion/mobilization, nerve mobilisation/mobilization, neuralmanipulative physical therapy, physical therapy, neural/nerve glide, nerve glide exercises, nerve/neural treatment,nerve/neural stretching, neurodynamics and nerve/neuralphysiotherapy. Randomized controlled trial or RCT was thekey term used in relation to the methodology of the studies.
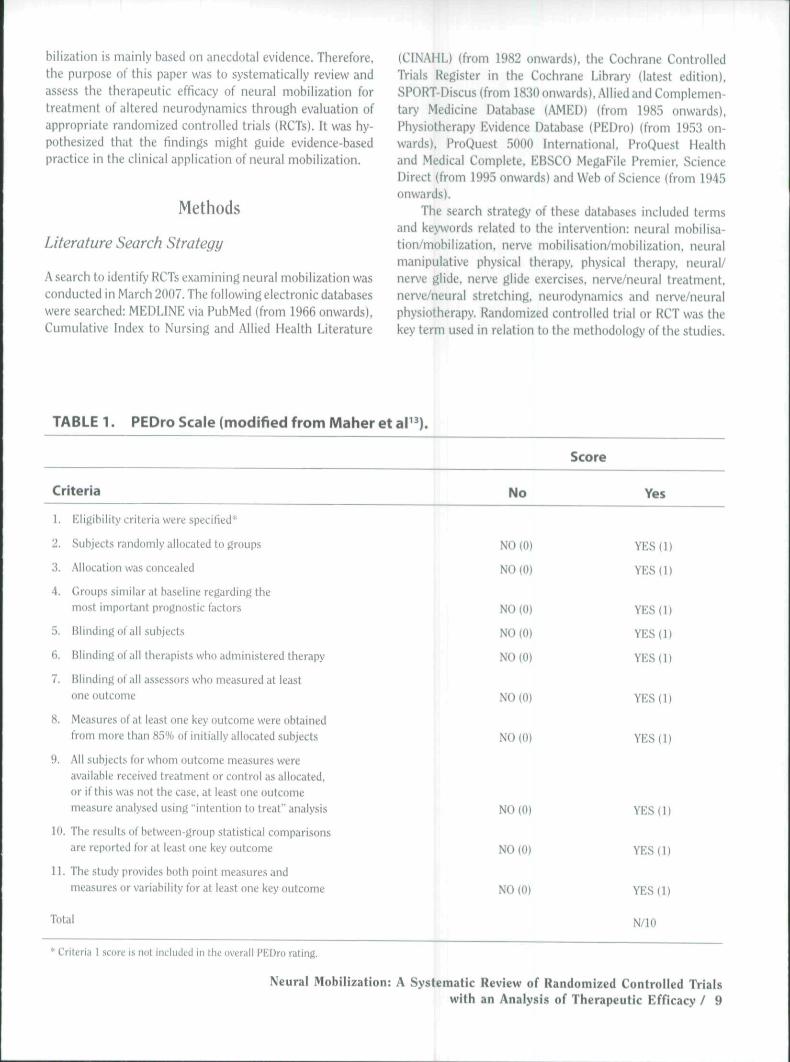
TABLE 1.
Criteria
PEDro Scale (modified from Maher et ar^).
No
Score
Y«s
1. Eligibility criteria were specified*
2. Subjects randomly allocated to groups
3. Allocation was concealed
4. Groups similar at baseline regarding tbemost important prognostic factors
5. Blinding of all subjects
fi. Blinding of all therapists wbo administered therapy
7. Blinding of all assessors who measured at leastone outcome
8. Measures of at least one key outcome were obtainedfrom more than 85% of initially allocated subjects
9. AM subjects for whom outcome measures wereavailable received treatment or control as allocated,or if this was not the case, at least one outcomemeasure analysed using "intention IQ treat" analysis
1(1. Tbe results of between-group statistical comparisonsare reported for at least one key outcome
U. The study provides botb point measures andmeasures or variability for at least one key outcome
Total
NO(0)
NO(0)
NO(0)
NO(0)
NO(0)
N0(0)
NOlO)
YES {11
YES (1)
YES(l)
YES(l)
YES(l)
YES(l)
YES(l)
NO(0)
NO(0}
NO (0)
YES{1)
YES(l)
YES(l)
N/10
* Criteria 1 score is not included in the overaii PEDro rating.
Neural Mobilization: A Systematic Review of Randomized Controlled Trialswith an Analysis of Therapeutic Efficacy / 9
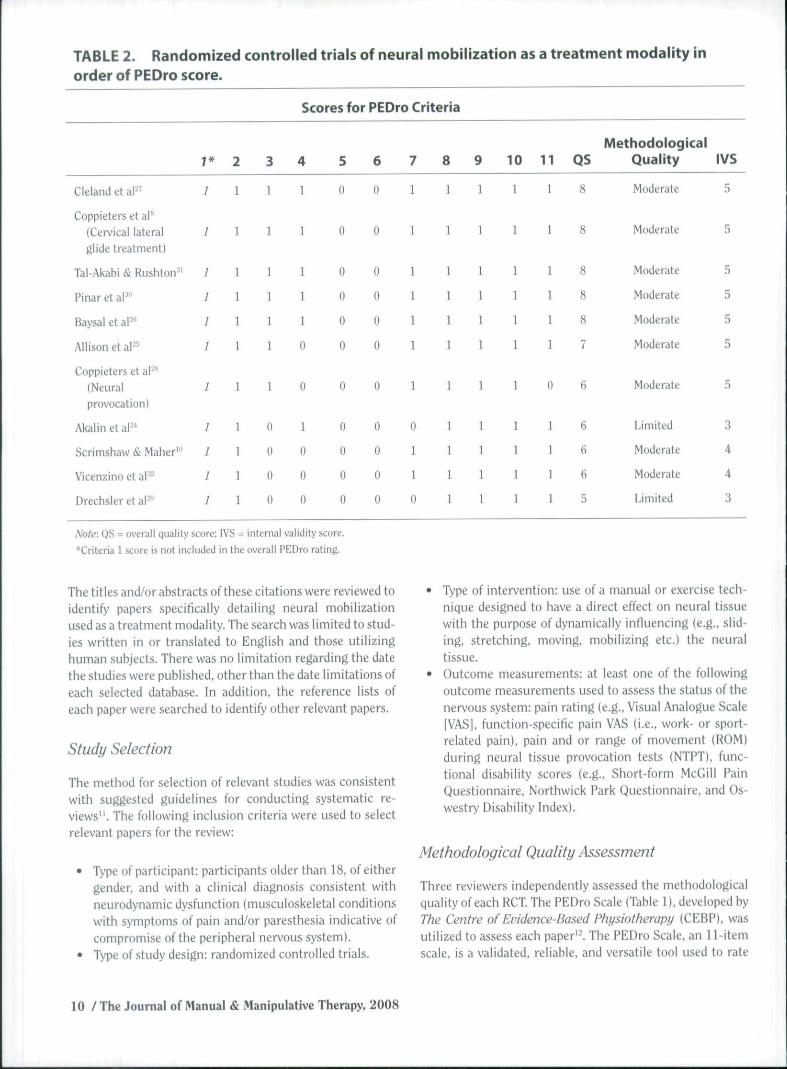
TABLE 2. Randomized controlled trials of neural mobilization as a treatment modality inorder of PEDro score.
Cleland et al-"
Coppieters et aP(Cervical lateralglide treatment)
Tal-Akabi & Rushton-"
Pinar et a P
Baysal et aP**
Allison et aP^
Coppieters et aP"(Neuralprovocation)
Akalin et al-
Scrimshaw & Maher'"
Vicenzino et al'-
Drechsler et aP^
7*
;
7
/
]
1
I
J
I
!
1
1
2
1
1
1
]
1
1
1
1
1
1
1
3
1
1
1
1
1
1
1
0
U
0
0
Scores for PEDro Criteria
4
1
1
1
1
1
0
0
1
0
0
0
5
0
0
0
0
0
0
0
0
0
0
0
6
0
u
0
0
0
0
0
0
0
0
0
7
1
1
1
1
1
1
1
0
1
1
0
8
1
1
1
1
1
1
1
1
1
1
1
9
1
1
1
1
1
1
1
1
1
1
1
10
1
1
1
1
1
1
1
1
1
1
1
11
1
1
1
1
1
1
0
1
1
1
1
QS
8
8
8
8
8
7
6
6
6
6
5
MethodologicalQuailty
Moderate
Moderate
Moderate
Moderate
Moderate
Moderate
Moderate
Limited
Moderate
Moderate
Limited
IVS
5
5
5
5
5
5
5
3
4
4
3
Note: QS = overall quality score: IVS = internal validity score.
*Criteria 1 score is not included in the overall PEDro rating.
The titles and/or abstracts of these citations were reviewed toidentify papers specifically detailing neural mobilizationused as a treatment modality. The search was limited to stud-ies written in or translated to English and those utilizinghuman subjects. There was no limitation regarding the datethe studies were published, other than the date limitations ofeach selected database. In addition, the reference lists ofeach paper were searched to identify other relevant papers.
Study Selection
The method for selection of relevant studies was consistentwith suggested guidelines for conducting systematic re-views". The following inclusion criteria were used to selectrelevant papers for the review:
• Type of participant: participants older than 18, of eithergender, and with a clinical diagnosis consistent withneurodynamic dysfunction (musculoskeletal conditionswith symptoms of pain and/or paresthesia indicative ofcompromise ofthe peripheral nervous system).
• Type of study design: randomized controlled trials.
• Type of intervention: use of a manual or exercise tech-nique designed to have a direct effect on neural tissuewith the purpose of dynamically influencing {e.g., slid-ing, stretching, moving, mobilizing etc.) the neuraltissue.
• Outcome measurements: at least one of the followingoutcome measurements used to assess the status of thenervous system: pain rating (e.g.. Visual Analogue Scale|VAS], function-specific pain VAS (i.e., work- or sport-related pain), pain and or range of movement (ROM)during neural tissue provocation tests (NTPT). func-tional disability scores (e,g., Short-form McGill PainQuestionnaire, Northwick Park Questionnaire, and Os-westry Disability Index).
Methodotogical Quality Assessment
Three reviewers independently assessed the methodologicalquality of each RCT. The PEDro Scale (Table 1). developed byThe Centre of Evidence-Based Physiotherapy (CEBP), wasutilized to assess each paper''. The PEDro Scale, an 11-itemscale, is a validated, reliable, and versatile tool used to rate
10 /The Journal of Manual & Manipulative Therapy, 2008
RCTs for the PEDro Database'^ ' I The PEDro scale has beenused as a measure of methodological quality in manysystematic literature reviews"'-".
An overall score of methodological quality, or qualityscore (QS), was determined for each paper by each of thethree reviewers as a total of positive scores for 10 of the 11items (i.e., N/10). Unlike the other items. Criterion One ofthe PEDro scale relates to external validity and was not usedin the final total PEDro score'"\ A consensus method wasused to discuss and resolve discrepancies between the mark-ings of each paper between the reviewers. The agreed QS foreach paper is included in Table 2.
The various items of the PEDro Score deal with differentaspects of RCT analysis including internal validity, externalvalidity, and statistics. In order to allow quantitative analysisof the methodological quality of a systematic review, van Tul-der et al" recommended the analysis of the internal validitycriteria of any rating tool. For the PEDro Scale, seven itemsrelating to internal validity were identified. These sevenitems include items 2, 3, and 5 through 9 (Table 1). An inter-nal validity score (IVS) has also been used in other system-atic reviews-' to allow calculation of the number of internalvalidity criteria met for that particular rating system and tothereby give an assessment of methodological quality. It wasdecided to calculate an IVS for this review based on the rele-vant internal validity criteria of the PEDro Scale. The posi-tive scores of each of these seven items were added togetherto calculate the IVS (Table 2).
To stratify methodological quality, the summated scoreof the 7-item IVS, calculated from the initial PEDro score(QS). was divided into three categories. A study of high meth-odological quality obtained IVS values of 6-7. a moderatequality obtained IVS values between 4-5, and a limited qual-ity was scored between 0-3. This decision was made based oneven cut-off points between 0 and 7.
Analysis of Therapeutic Efficacy
When RCTs are heterogeneous, there is no available methodto quantitatively assess the relative benefit (or lack thereoOof one intervention versus another because the studies com-pare dissimilar patient populations or interventions. In situ-ations where the heterogeneity of primary studies preventsuse of a quantitative meta-analysis to summarize the results,recommendations are typically made based on a qualitativeassessment of the strength of the evidence-'. The RCTs re-viewed for this paper were considered heterogeneous be-cause they explored a variety of pathologies and differenttypes of neural mobilization techniques. Consequently, aquantitative meta-analysis was not appropriate and resultswere analyzed in a qualitative fashion. The qualitative assess-ment involved the following categories scored specifically foreach type of intervention:
Level 1; Strong evidence: provided by generally consis-tent findings in multiple RCTs of high quality.Level 2: Moderate evidence: provided by generally con-sistent findings in one RCT of high quality and one ormore of lower quality.Level 3: Limited evidence: provided by generally consis-tent findings in one RCT of moderate quality and one ormore low-quality RCTs.Level 4: Insufficient evidence: provided by generallyconsistent findings of one or more RCTs of limited qual-ity, or when no RCTs were available, or when studiesprovided conflicting results.
Clinical Benefit
Lastly, to determine whether a clinical benefit for neuralmobilization could be concluded, a ranking system similar tothat used by Linton and van Tulder'' was used. A positive effectwas concluded if the intervention (i.e., neural mobilization)was statistically significantly more beneficial compared to thecontrol for at least one key outcome variable, a negative effectif the intervention was less effective than the control, and aneutral effect was concluded where the intervention andcontrol did not statistically differ significantly for any of theoutcome variables-'.
Results
Selection of Studies
Ten RCTs, represented by 11 published article5''•"'•^^^^ satis-fied the inclusion criteria following the electronic and man-ual reference list searches. The articles published by Cop-pieters et al -^ are from the same subject group and werethus classified as one RCT.
Methodological Quality
The methodological quality for each paper, represented bythe IVS, is detailed in Table 2. Nine of 11 studies'*'"-•'•'-""^reviewed were given an IVS of 4 or 5 and were of moderatemethodological quality. 1\vo of the studies^ ' ^ were given anIVS of 3, suggesting limited methodological quality. Table 3presents statistics relating to the percentage of each itemthat was satisfied for an IVS score.
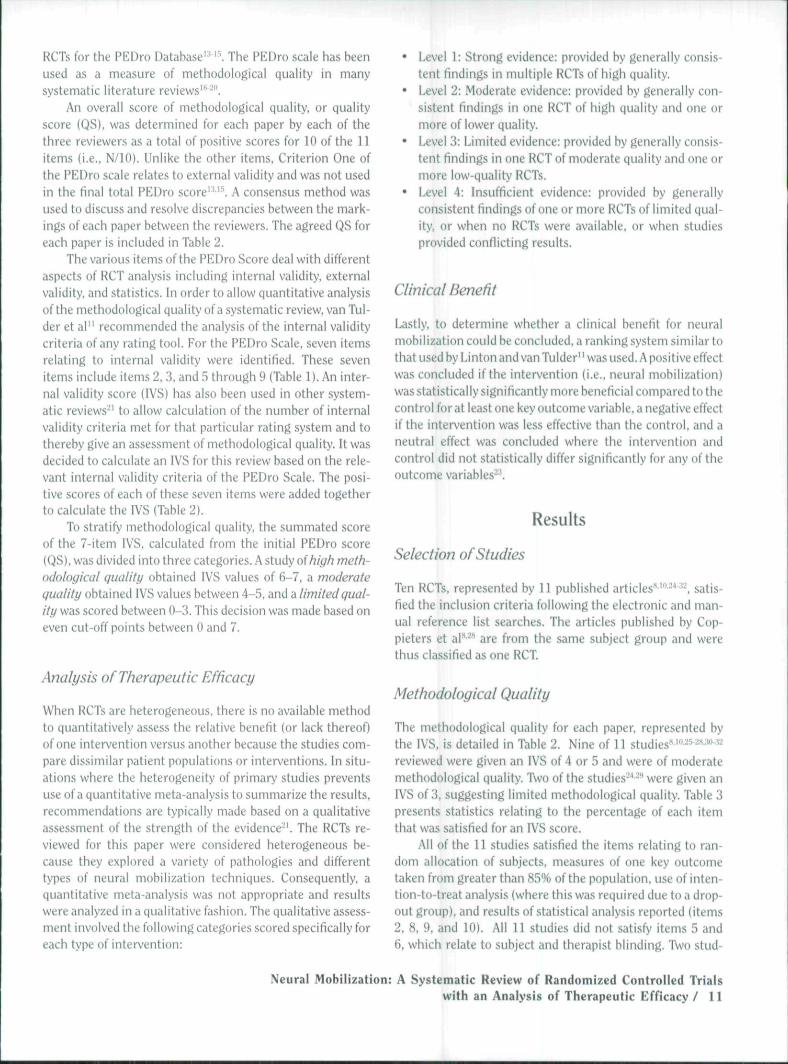
All of the 11 studies satisfied the items relating to ran-dom allocation of subjects, measures of one key outcometaken from greater than 85% of the population, use of inten-tion-to-treat analysis (where this was required due to a drop-out group), and results of statistical analysis reported (items2, 8, 9, and 10). All 11 studies did not satisfy items 5 and6, which relate to subject and therapist blinding. 1\vo stud-
Neural Mobilization: A Systematic Review of Randomized Controlled Trialswith an Analysis of Therapeutic Efficacy / 11
TABLE 3. Number and percentage of the studies meeting each PEDro criteria.
PEDro Criteria
Numbermeeting
criterion (N)
11
11
7
6
0
0
9
9
9
9
10
Percentmeeting
criterion (%)
100
100
64
55
0
0
82
100
100
100
91
1 Eligibility criteria specified (yes/no)
2. Subjects randomly allocated to groups (yes/no)
3. Allocation was concealed (yes/no)
4. Groups similar at baseline (yes/no)
5. Subjects were blinded to group allocation (yes/no)
6. Therapists who administered therapy were blinded (yes/no)
7. Assessors were blinded (yes/no)
8. Minimum 85% follow-up (yes/no)
9. Intent to treat analysis for at least 1 key variable (yes/no)
10. Results of statistical analysis between groups reported (yes/no)
11. Point measurements and variability reported (yes/no)
jggM. H jjj p(jf satisfy item 7, which relates to rater blinding.
This suggests that these t^o studies lacked all three forms ofblinding (subject, therapist, and rater). The other 9 studieswere single-blinded (rater-blinded) studies. There was noclear trend established for item 4, which relates to concealedallocation of subjects.
Study Characteristics
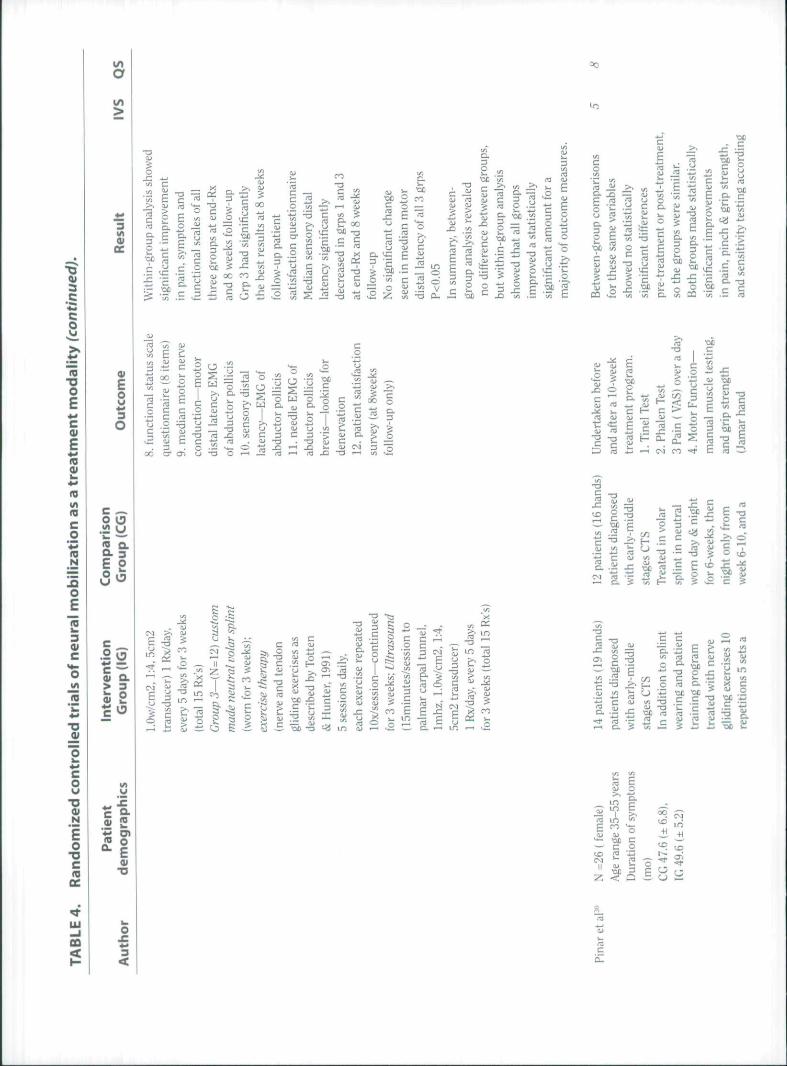
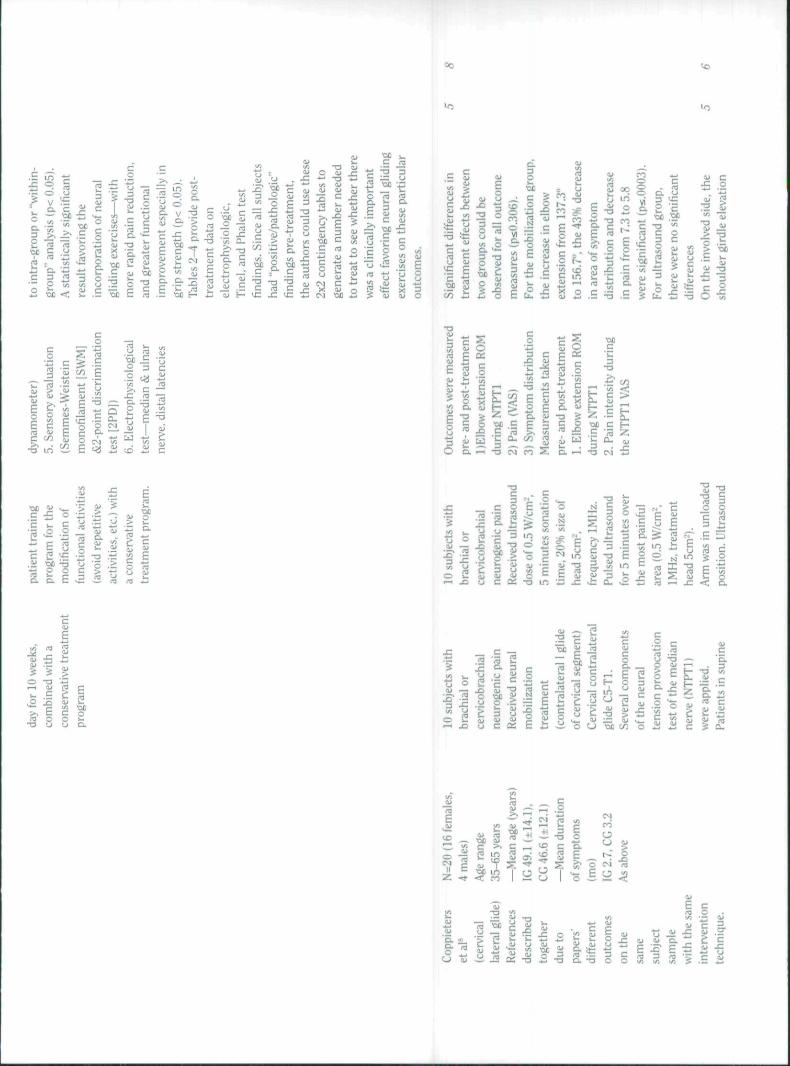
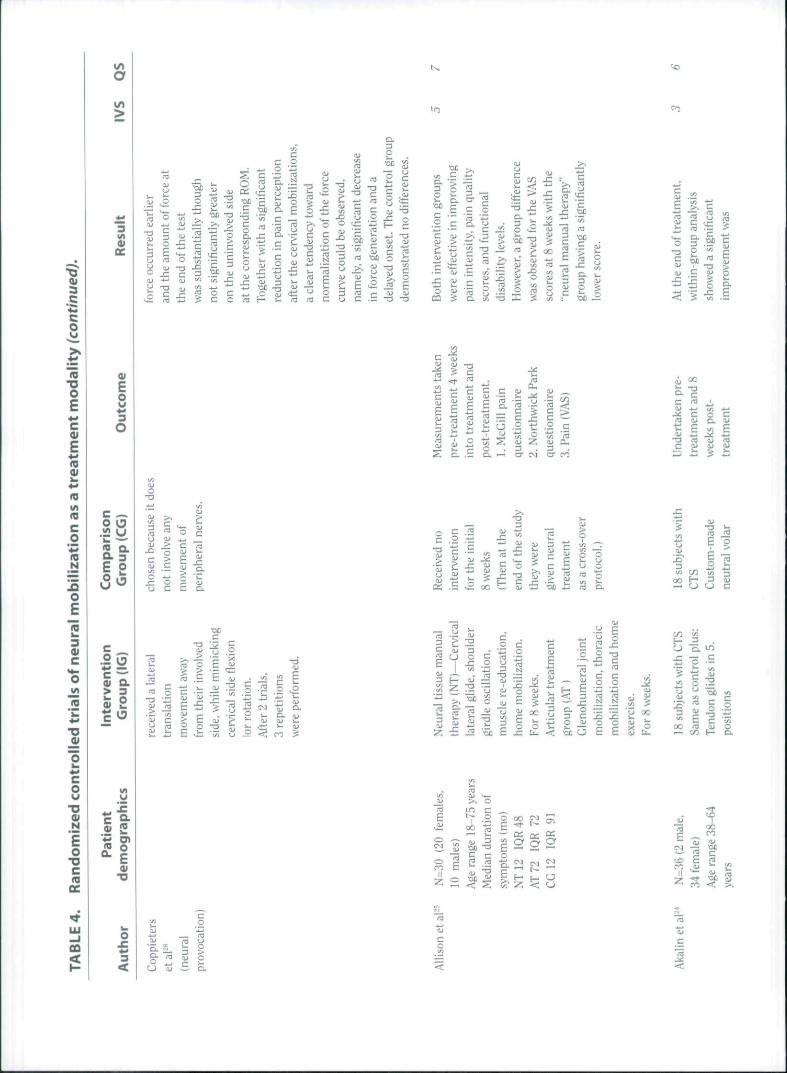
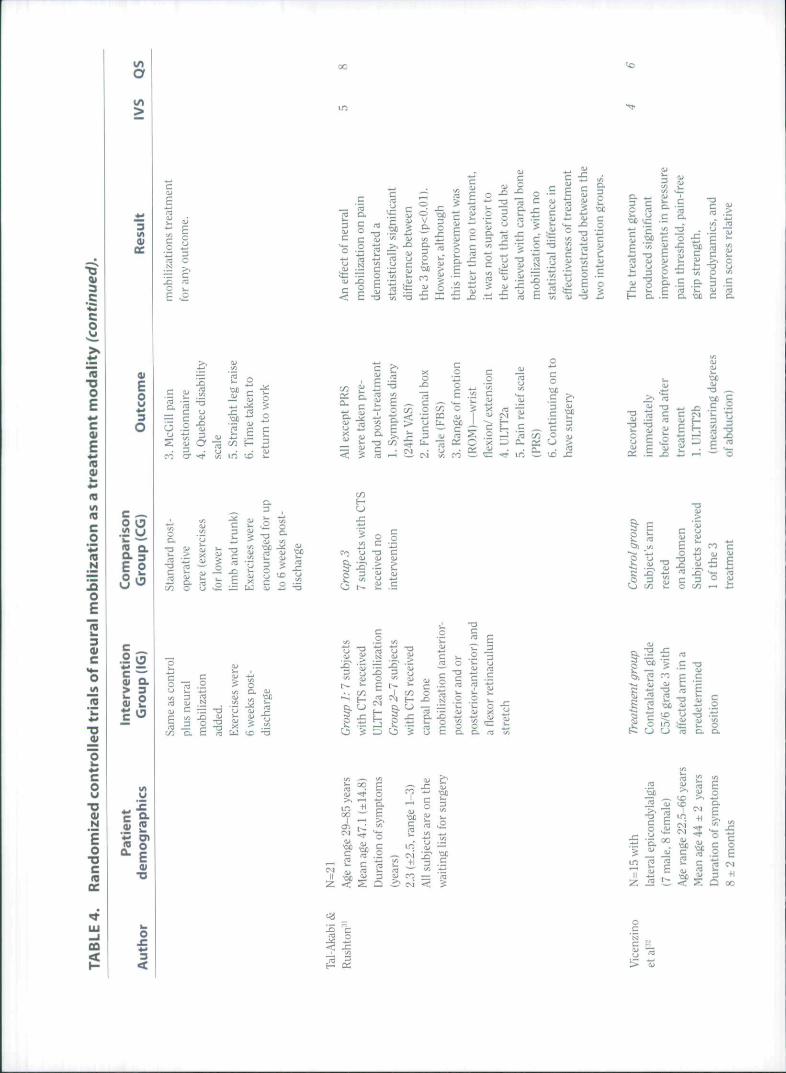
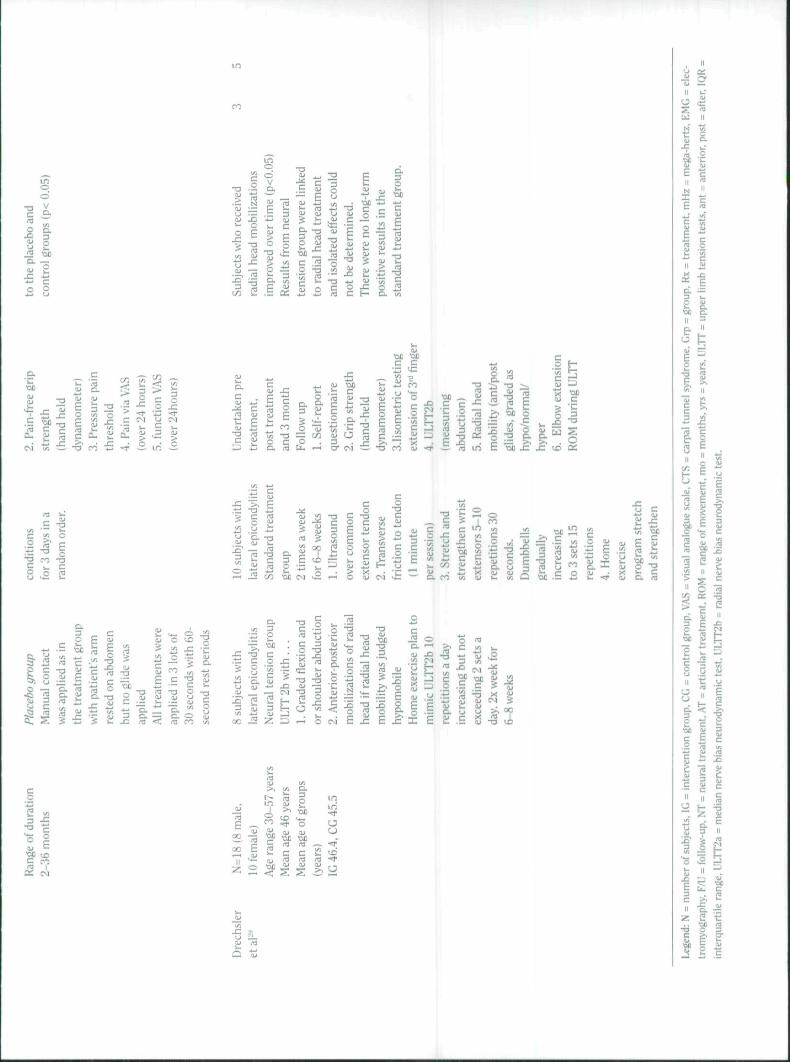
All ten RCTs used different methods of application of neuralmobilization (e.g.. cervical lateral glide, slump sliders, pe-ripheral nerve sliders, etc.), and some studies chose to com-bine these techniques with home-based neural mobilizationexercises. There were also differing neurodynamic dysfunc-tions examined, including lateral epicondylalgia, carpal tun-nel syndrome, post-operative spinal surgery, non-radicularlow back pain, and neurogenic cervico-brachial pain syn-drome. Therefore, all ten RCTs were clinically and therapeu-ticaliy heterogeneous, necessitating a qualitative analysis forsummarizing the results. Table 4 contains details of studycharacteristics.
Therapeutic Efficacy
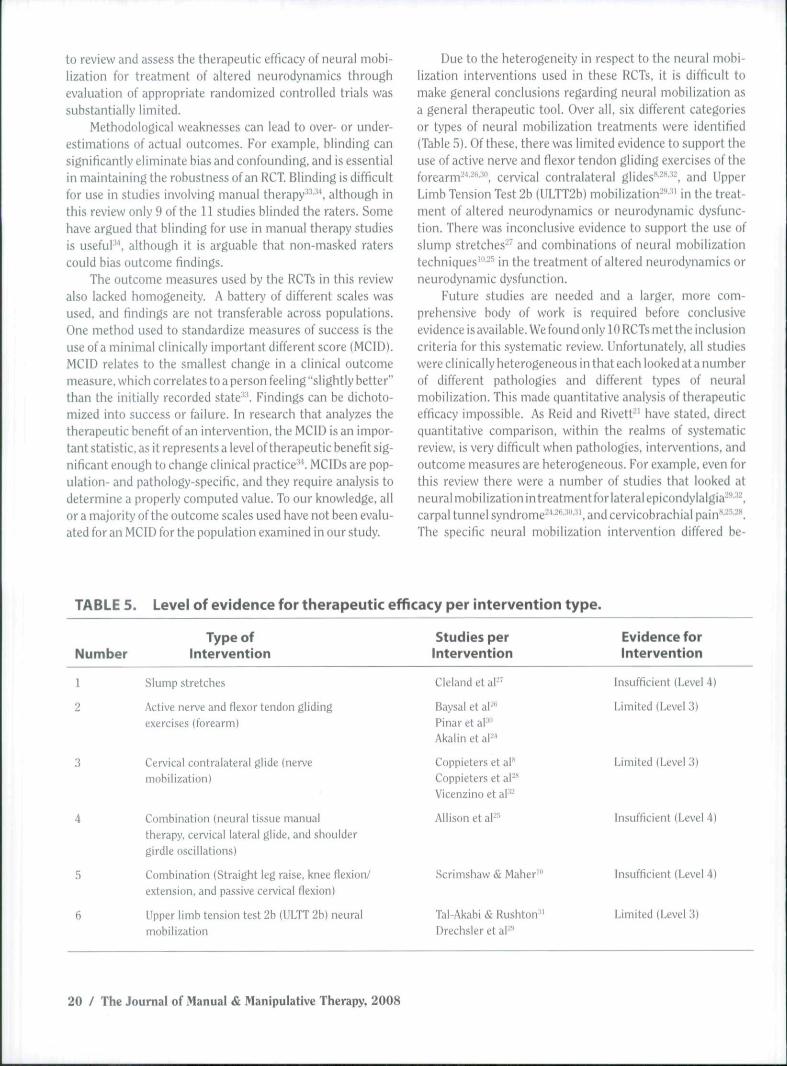
Of the 11 studies identified. 6 different categories or types oftreatment were identified (Tahle 5). Using the qualitative rat-ing system, as mentioned earlier, it appears there is limitedevidence (Level 3) to support the use of neural mobilizationthat involves active nerve and flexor tendon gliding exercisesof the forearm-'*-''''"', cervical contralateral glides"-"''-, and
Upper Limb Tension Test 2b (ULTT2b) mobilization-"' in thetreatment of altered neurodynamics or neurodynamic dys-function. There was inconclusive evidence (Level 4) to sup-port the use of neural mobilization involving slumpstretches^' and combinations of neural mobilization tech-niques'"-^' in the treatment of altered neurodynamics or neu-rodynamic dysfunction.
Clinical Benefit
Tahle 4 lists the study details of the 11 studies. More studiesfound a positive effect*-''' •^"'-' than a neutral effect'"• ••" .
Discussion
A search to identify RCTs investigating neural mobilizationyielded 11 studies that met the inclusion criteria for this re-view. Analyses of these studies, using the criteria of Lintonand van Tulder", indicated that 8 of the 11 studies'-'*-'"•"'•'-'concluded a positive benefit from using neural mobilizationin the treatment of altered neurodynamics or neurodynamicdysfunction. Three of the 11 studies'"-''•" concluded a neu-tral benefit, which suggests that neural mobilization was nomore beneficial than standard treatment or no treatment.Nine of the 11 studies^'"-"^-^'"'- reviewed demonstratedmoderate methodological quality; the two remaining stud-ies-* -" yielded limited methodological quality. Studies exhib-ited weaknesses in random allocation, intention to treat.concealed allocation, and blinding; consequently, our ability
12 / The Journal of Manual & Manipulative Therapy, 2008

I/)
a
01CC
"oco
•oOfN
Eo
•ac
LU
CQ
9t
Eo3
o
o o
E 2
> 3
5; s
=1E
"O
E -" —
o
c<uE.•aa.)
.^,
oCu
-ac
re-
c
>>.•
S""E'Ofl
.2*a-o'o
CQ
UIO
.
Q.
E>,moc
_o
istj
-T3
•onC
C
ra
3.-
EzCM
QO
c ^ O -gQ: -a • -
Z ^ .^— TD —^ O . ^
- - ; • ^ fO
— /u
a j
ao
rac
:ion
S Ec
'•OE-3
S. .£
I ? J J •£ J
I iiiii
T 33-o g ,;2
13C X
o oX ,— .—
t i .ii ro oj
E y -S G oin ^• ^ - = CM
o
E -H
E •OC -H ^
ood
c .rf ,iJ
55 aj 4)
isf=
c ra .2i 5a> j : : (Q X
•a Cc p
•3 raj ; tic
x: o
15 - -
• ^ " ^ ^
^ ^ I I -alu in C c P I
' i^ -a -^ -S w•OC 1 2 • « * - 'OB
^ a; x: C c
c o. i "z;
x: -c
•c
| |
I I
C o wO C "ii " IJ•r -a x:
2 £
£ re ra
^ ^ C ^ r. s 130 ra -oD .B
c-a
in ra m ^4J ^
fci E =3 >, caj 5 o -p • -S t j & o .E
-^ ]£ fi> o
x | J-fr- S i: o
n r% ^
X >i o> ra o4) X i I—I aJ "—'
II - O .^3C 3O O
t/S4j -a
1- CM
O•OC
c 'bb
ob ra
2 ^
ra
£ o S E8 § c ^^ C O —"
u
un+1
00
e
•H
r—1
OIT)CM
i n
i nCO
e-o
c:
.s3
T3Craw
Eo"D.E5^
t o^^+1
L O
•—'
£•
00
o+1
1—'
£•
oqo+
•*t•—1
o
I/I>
a;GC
3
CO
ra•DOEc
ECD
(D(A
racoreN
JDO
E
ou3O
c _O O
2- =E 2O in
01 Q.
I I
N
£oC
ot 2
w o**• E
CD<
a> , . , , ^
1/1 t C
re "E E aj o
•z; 5
I,-;s re .o c
3 . -
1= .2
? Si e-
3 "S
aj 00
1/3-TD
reSi1/3aJ
J3
D.C L
3
O
Co
re
O in • ^
'OC
-TD
c •^ 5 re E- T= . o
rere HI
B
00
C f-
X! = —• -t:OC
cH i
O.
_O .« T3
c; ^ ] ^
— ob •/! c .2 o
E 5
i sO . 4 - .
E =re °-o =
OC « •
•K E
o
co
c
loto
r
fcc.2^ i
E
o
cEco
t j3
-oC
o
enc
_re
"re
CLS
polli
] _
^ 3
.re
dist
a
£•o1/3
o
ou.
>.
0c0
Ilic
is
ot j3
O
O
HIo;C
Ilic
is
o
>_23
T3
dng
loot
tion
'•> HIaj C
Co
arti
latis
f
*
c
. a:—CM
z
" .^
B 3u -a
in
£-HI
OC
c
cr 're se
c3
X
S o
113C1LO
-TD _
£- 3
re s:
OC
OC ir
c R
E .2-— aj mre u o
cOC
re
Eret/5
1/3ajC<—1
(-1
re1/3
oC
-TDHI
o
^ > oo
^ ? -
(A
•a2 =3 E -o
c"S.o
c_o
- p
c.Si"re
cre
III
Ogr
ao.c
ini:
re
HI
HiC
-TD
"reHI
I—1
i f tH)irtU
HI
=J
OC.E.^
ret/3
HI1/3
inuo
cQ
H)Q
ale)
E•Si• — •
1X3CM
i-reHI
5-55
i
CO
oocre
Bc
sym
pl
co
3 +1
8 ^
= s ^
3 >, . i"O -1^ —
C 3 5
Ji OC <
si3 Sc IO QJ
S !5E oc
occ
o _ — o
3; '^ ra aj
CM
b -M E-.ra ^ ^ •=
oc
QJ ='OC ^c ra
o P
c'OC
co
IU
QJ
t u
x :co1 / :
ajt«fj> :
5
•A
Eouo
JJ
ra
ific
'OC
4 - "
(J-ua)
CQJ
E%QJ
C-a
OC ^^ "3O ,si
c o S £1 -E c t^ — -^
x: S— f^ L= ™
E
E S
?= r —
oc
a> ^ 3•a
3
13 j2 *r c T-< ' 7 i r
5 E 3 S S ' o p c HCO
^ - O CM CO
^ .s ra
occc
: tr
ai
c
raQ,
IU
•B
Era'OO
oi-a.
"oc.Srao
O
_>
inal
;
^^
C•2
^ 1 /
repe
'
'o
a j
'.3; >
ura
irva
t
«)
cora
X^ D.
II5i y
•o
c o E" 'Ix: ^ _5 -y 3 ; ; ;
U O .> o I ^£ 5
i n QJ "a
o E E 3 l - ic C £ : - a L n ' Z ! . r : ^ O -
• = W T3
T 3
)ine
Ec
1mC0
UIB.,
'OC0
.•t: 3 'ra 2J2 >- y bi c O•*-; r- ra = Uf .—
oh 3i «J— E "ra
'oc >-ra 4> • "I- irt C
w _ o^ 3 ^o oc ^ .N c
u o .£ — E
S s y I §X) u c ce E i;
rae
•a «j S -^ o —
co
- I"i— o
3 ^ —„_ o «
i n
— « .2
i=20
i
..<:.
</>
3ppi
i
CJ
t n
mal
e
QJ
gera
* ^
ervi
t5-
65
CO
'3?!2oc
tera
l
ra
c ,_,ra
1 —
in
c 1
G46
,
0
eeth
oa.B - :
o CM
a
>
3VI
ec
•ooEc
E
"D0)
cou
•o01N
1o
•ocm
CC
01
Eow• ^
O
c ...O O
c.2 KD(U O.> 3
o 9
c'^re0 .
aQO)0EOf
T3
a;tj
O
cI—^
c3O
B
<naj
aJ
•£
x:'OC3O
x ;_>.
iaI
cra
Oft:
'oc
o.1/5
ifi(
c'OJd
'i/i
ith
o.
a j
c.cracc
bil
c
rvii
3 ^
XI
3•u .2
aj 3'OC ^
-araco
•rs C 1/5•" aj cra 130 o
- e £ E -2 1
ra
>alA
Ul
"c
cQJ
I
aC
"rak -
x;c
Ili
oo
S 1.= E
a>
e.o
c
s §B ^
occ
> X
x; 5 'OC
II13 t
^ o
ra .^ "ra <= 5
.2 to
i ^^^ . i c4> ;Zi a>
o-T3
, >
Rec
(
o
rven
tiin
tei
• 2
he i
nifo
rt:e
ks
IU
ao
a)
x:
mat
t(T
he
"5!
ofth
een
dw
ere
they
ral
n ne
ugi
vetm
ent
treat
cros
s-ra
ocol
.)
oQ
2 O
I gto ^ •
^ ra ^ - "^c co oa j
is <! 3 ra raJ2 — __C N N3 o. o r= f=
. y 3 C XI X3< oc O E E
c:q
to
E _g. cra ^ 3 ;§
•B ^.§ S•o ° •" c= & « s<u c aj o
5 £ i ^
a.c
ra<u
-ac
• o
ra"c
EraOJ
•toOD.
a j
Ca>E"raOJ
X I
00 H
E 15O k.
CJ C
U "D. mx: -T; c
aj toOJ3 •/)
s g• E c 3)
00 ra oj o•-* en h- a.
CM
<OCOII
Z
tJc
a j
ra
a j
QJ
ang
1 M
raa>
^^•—. r- * ^ ' — • ^ ^ ' ^ ^
~ 3
•oc : = a j
.E E
Q. C
o -o•OC S
£ •£fO O
i/j
-o
Q. 4J
C.-«
tn (Jc .E•OD D.
-OB •OO - a
^
3 ^ J:
3 oj
><
•DC
c
a,
Isw •on
(U 4* —
•DC 41 ts <
COO iT3
cQ.3O1 -•OH
co
T3
cOl
-ac
Qo'OC
•T3<u
C
o.0)1 -
Q.fu
JZ
• - I
3ul<U
>
cot J
T3<U
^
3x :
c
IS s
igPh
ale
^^
sign
v)
Tin
el2-
poi
CO
lati
onsc
rim
i
'-B
reng
l
1 * ^
Gri
p:
• ^
stre
njPi
nch
m
Eo
Sym
p
t o
core
1 / :
veri
ty
i>1/1
3
onal
:F
und
ore
u
o
Cti
.<«
satis
fpa
tien
<:
tion
•op
ylU
C
ider
tai
3
.5)
T I
;8.3
(le
phor
_2
c1o£X
onth
s
E
Ul
Ca.t / 3
VI
C
tJ3inC
u l
5
c
p
_1 L
-a
_ ' ^- C • —
.— 3c -a
E
IS ^
3
E ^
C J*:
OE 13
^ J-a cj
PE
i .3 2
.E ro
3 — ^ ^ ^
O C
£, ^ * ^
o .E E<y o ^ o
- S V- 5 tj
in C !CO 3 -
wi
c g ctu
to __in 1/1
S :K
1--: ,_^
* . 5 '-^ Lri
o I -- o" " S- * • r l t-'
>.
S
I
IS
1
3
C
*OI/I
.2
•o
Iou
•oN
iocmae
^lij
CQ
a
>
«o
w
O
toM(0co*B(0N
15o
co
aE
c
nQ.
i nW
a(0
OlOIU
00
is.13 O
;= >.
IS «
fl .—
5 c, ^ a;
- S ^ f -
11 i= ^ E S 'O
fl
D
"H.
c
7^ "O
E ro
cu5m
ise
cuX
J—'
OC L
1/1
O)(U
'E•OC
=
stic
a
caj+->
renc
i
•—•o
D,
un
g-
Jgro
•£"rt
•eve
r,
3
rt
c
eme
o
impt
c
.rau•bjoc
rt
Q• ' - '
ior
uper
1/1
"oc•./3
• : >
11-Cl
3o'-J
ro-Ct j
CoroD.
UJZ
%
eved
• —
cc
x:
co
iliz
a'
caj
C
iffer
i
• a
stic
a
o
" Q t/3 " O 4-1
EM
^
O1/3
nes
a*>
C
5
<
11/)
CO
aDo•OC
co"c.
rve
o
3 ?i
rt I"
£; E"Si S-p ^
c . u. ^ a: o "><
ion
1 C
i x: rt
c _'ro u^
c
c"co
(«uifq
ns;
1o
rece
ivC
TSw
ith
jati
onlo
bili
;
c
1
1 JII •OC
3 .S^ rq — ro.^ ' c i <i >
co•ci
"ccu
_§"rt
a j
x:
rt^c
gni
-yi
•a
-aQo.
i,Q .
.E'"cOi
a>>cQ .
£
C' f l
a
old
sz
c*rtc
t/1
.9-•OC
-acV3
u
'Ert>.T 3O
a;C
ii>
%
rel
res
1/1
c'roo
« -a
o p =;« P aj
CC B su
•a _
C .2
I" i
E :: rn £o 4.: a, w
2 kJ £ E"5 X 3 • -= rt
a ^ ° Po cfl >—' —
T3 x;
C -3o _ ^ _a, rt ro c c--. ai cu E ' cJ: -a "o rt c^ -2 2 -a S c.§ S ^ a 1: .2
§ %^t=; u o
^ ^ E
"rt
• ^
oo
oi
I
22.5
cu
C
CM
+1
3:fl
Q .
E-./I
. 0
un
x:"c0E
2 .12 ' ^
> cu
Q cx
O O.
1 iJ2 •OOo . —
3 O
oV
"»LU
I1
k-
o
>O
impr
;ura
c
from
m^ ^
Res
u
c—
vere
.Q.
grou
co
tens
i
cHI
EHIkH
T3
Ihea
.2"5rtio
^ 33O
ated
o•yi
and
i
2 £OJ
c ^e § ^
OJ a;
•a 5
5i •«
o.3O
. IQC W .W
•a n _ c
-a
C E— a . m
Ii E
-y)
•OC
c
g
"3" --i in ----
a.c
I Iin "O
2 ^p. nJ
i I.fcj w •OJ]
•= ^ -r -o= CO 4* O
"00
c§ ^
E -K
I I.2 ro ^ts ^ ^3 J
•OC
c
13 CL. O
o-a
•B c
y? u
fu SJ
V
O. T3
a* «
ro ^
E -i- S CO •OC CM
c
c o c3 E 4J
I I ^u
oTJ
o HI
•a
cI So5 I m
O ^ H> I/I:7 --* -c •
<u _ ow* * - I—< ™
D. ro i/j "ij
QCi n
.2 "*j -o
c
=s ^ c
a. u 3k- i/i i-j
I 3E T3
b 1/)
c o•OC . t .S £ - t S
t r t •OC
^ c:o . ro
I E
c -:::;
S = - - E ^
C '/I . , -'r • - • . . _ .
'> o
' • /^ • 4 - '
oo -2
3
-a
o^ CN| ^
O m _ — 'O. c ra "V , ,
•g "I .£ ^ "o o .b c
E ^' X E
i n
« ^ fi S) ^00 E p !_ "
to review and assess the therapeutic efficacy of neural mobi-lization for treatment of altered neurodynamics throughevaluation of appropriate randomized controlled trials wassubstantially limited.
Methodological weaknesses can lead to over- or under-estimations of actual outcomes. For example, blinding cansignificantly eliminate bias and confounding, and is essentialin maintaining the robustness of an RCT. Blinding is difficultfor use in studies involving manual therapy"-'', although inthis review only 9 ofthe U studies blinded the raters. Somehave argued that blinding for use in manual therapy studiesis useful", although it is arguable that non-masked raterscould bias outcome findings.
The outcome measures used by the RCTs in this reviewalso lacked homogeneity. A battery of different scales wasused, and findings are not transferable across populations.One method used to standardize measures of success is theuse of a minimal clinically important different score (MCID).MOID relates to the smallest change in a clinical outcomemeasure, which correlates to a person feeling "slightly better"than the initially recorded state''. Findings can be dichoto-mized into success or failure. In research that analyzes thetherapeutic benefit of an intervention, the MCID is an impor-tant statistic, as it represents a level of therapeutic benefit sig-nificant enough to change clinical practice-'^ MCIDs are pop-ulation- and pathology-specific, and they require analysis todetermine a properly computed value. To our knowledge, allor a majority of the outcome scales used have not been evalu-ated for an MCID for the population examined in our study.
Due to the heterogeneity in respect to the neural mobi-lization interventions used in these RCTs, it is difficult tomake general conclusions regarding neural mobilization asa general therapeutic tool. Over all, six different categoriesor types of neural mobilization treatments were identified(Table 5). Of these, there was limited evidence to support theuse of active nerve and flexor tendon gliding exercises of theforearm-'"""', cervical contralateral glides*'' '*-' and UpperLimb Tension Test 2b (ULTT2b) mobilization-'''" in the treat-ment of altered neurodynamics or neurodynamic dysfunc-tion. There was inconclusive evidence to support the use ofslump stretches-' and combinations of neural mobilizationtechniques'"-^ in the treatment of altered neurodynamics orneurodynamic dysfunction.
Future studies are needed and a larger, more com-prehensive body of work is required before conclusiveevidence is available. We found only 10 RCTs met the inclusioncriteria for this systematic review. Unfortunately, all studieswere clinically heterogeneous in that each looked at a numberof different pathologies and different types of neuralmobilization. This made quantitative analysis of therapeuticefficacy impossible. As Reid and Rivett"' have stated, directquantitative comparison, within the realms of systematicreview, is very difficult when pathologies, interventions, andoutcome measures are heterogeneous. For example, even forthis review there were a number of studies that looked atneural mobilization intreatment for lateral epicondylalgia^'*''^carpal tunnel syndrome '-*^-'"- '. and cervicobrachial pain^•"•^^The specific neural mobilization intervention differed be-
TABLE 5. Level of evidence for therapeutic efficacy per intervention type.
Number
1
2
3
4
5
6
Type ofIntervention
Slump stretches
Active nerve and flexor tendon glidingexercises (forearm)
Cervical contralateral glide (nervemobilization)
Combination (neural tissue manualtherapy, cervical lateral glide, and shouldergirdle oscillations)
Combination (Straight leg raise, knee flexion/extension, and passive cervical flexion)
Upper limb tension test 2b (ULTT 2b) neuralmobilization
Studies perIntervention
Cleland et aF"
Baysa! et al '''Pinar et aP"Akalin et aF*
Coppieters etal**Coppieters et a PVicenzino et al''-
Allison et aF''
Scrimshaw & Maber'"
Tal-Akabi & Rushton-"Drech.sler et ai-''
Evidence forIntervention
Insufficient (Level 4)
Limited (Level 3)
Limited (Level 3)
Insufficient (Level 4)
insufficient (Level 4)
Limited (Level 3)
20 / The Journal of Manual & Manipulative Therapy, 2008

tween studies, making, in these cases, the treatments tooheterogeneous for statistical pooling.
With respect to the clinical implications of these find-ings, it is interesting to note that generally all the RCTs thatlooked at neural mobilization for upper quadrant (i.e., cervi-cal spine, shoulder girdle, and upper limb) problems, withthe exception of one study -'•, concluded that there was lim-ited evidence lor therapeutic efficacy. This is in direct con-trast to studies that examined neural mobilization for lowerquadrant (i.e., lumbar spine, pelvic girdle, and lower limb)problems'"- " ' ^ in that all provided inconclusive evidence fortherapeutic efficacy. From a more specific pathological per-spective, for neural mobilization of cervical nerve roots,three papers supported the use of cervical contralateral glidemobilization. For neural mobilization ofthe median nerve inpeople with carpal tunnel syndrome, three papers supportedthe use of active nerve and flexor tendon gliding exercises ofthe forearm-'"'''".
Future Research
Considering the results of the extensive literature searchcarried out for this review, there is an obvious paucity of re-search concerning the therapeutic use of neural mobiliza-tion. Not only is there a lack in quantity of such research,upon dissection ofthe scarce research that is available, thereis also a lack of quality. Future research should look not onlyat similar pathologies but also at similar neural mobilizationtechniques.
Another key feature of these studies is that only clinicaloutcome measures were used. In the introduction, we dis-cus.sed the biomechanical. physiological, and morphologicaltheories underlying neural mobilization. One of the key the-ories for using neural mobilization is to exploit the mechani-cal effect that this form of mobilization has on the neuraltissue and its mechanical interface. It is possible to use ob-
jective in-^vivo measurements of neural movement (i.e.,glide, slide, stretch, etc.) via real-time diagnostic ultrasound.It will be important to eventually substantiate clinical im-provements with objective measurement of neural move-ment. For example, recent unpublished data have demon-strated that it is possible to visualize and quantify, withreasonable reliability, sciatic nerve movement during neuralmobilization*''. As it has been postulated that an improve-ment in nerve mobility may explain any perceived benefits ofneural mobilization, it would be relevant to make a compari-son of clinical measures with objective measures (e.g., ROMand neural mobility) in an in-vivo situation in studies thatexamine neural mobilization. Such a comparison may giveclues as to whether neural mobilization is more likely to im-pose a mechanical effect or a neurophysiological effect onthe newous system.
Conclusion
Neural mobilization is advocated for treatment of neurody-namic dysfunction. To date, the primary justification forusing neural mobilization has been based on a few clinicaltrials and primarily anecdotal evidence. Following a sys-tematic review of the literature examining the therapeuticefficacy of neural mobilisation. 10 RCTs discussed in 11studies were retrieved. A majority of the.se studies con-cluded a positive therapeutic benefit from using neural mo-bilization. However, in consideration of their methodologi-cal quality, qualitative analysis of these studies revealedthat there is only limited evidence to support the use ofneural mobilization. Future research needs to examinemore homogeneous studies {with regard to design, pathol-ogy, and intervention), and we suggest that they combineclinical outcome measures with in-vivo objective assess-ment of neural movement. H
REFERENCES1. Butler DS. The Sensitive Newous System. Adelaide, Australia: Noi-
group Publications, 2000.2. Shacklock MO. Neurodynamics. Phy.-iiotherapy 1995:81:9-UJ.3. Shacklock MO. Clinical applications of neurodynamics. In: Shacklock
MO, ed, Moving in on Pain. Chatswood, UK: Butterworth-Heine-niann, 1995:123-131.
4. Shacklock MO. Clinical Neurodynamics: A New System ofNeuro-musculoskeletal TYeatment. Oxford, UK: Butterworth Heinemann,2005,
5. Butler DS. Shacklock MO, Slater H. Treatment of altered nervous.system mechanics. In: Boyling J. Palastanga N. eds. Grieves ModemManual Therapy: The Vertebral Column. 2nd ed, Edinburgh, UK:Livinjf.ston Churchill, 1994:693-703.
6. Gifford L. Neurodynamics, In: Pitt-Brooke J, Reid H. Lockwood J,Kerr K. eds. Rehabilitation of Movement. London. UK: WB SaundersCompany Ltd. 1998:159-195.
7. Kitteringham C. Tbe effect of straight leg raise exercises after lum-bar decompression surgery: A pilot study. Physiotherapy 1996:82:115-123.
8. Coppieters MW. Stappaerts KH. Wouters LL. Janssens K. The imme-diate effects of a cervical lateral glide treatment technique in patientswith neurogenic cervicohrachial pain. J Orthop Sports Phys Ther2003:33:369-378.
9. Rozmaryn LM. Dovelle S. Rothman ER, C.orman K. Olvey KM, BartkoJJ, Nerve and tendon gliding exercises and the conservative manage-ment of carpal tunnel syndrome. J Hand Ther 1998:11:171-179.
10. Scrimsbaw S. Maher C. Randomized controlleil trial of neural mo-bilization after spinal surgery. Spine 2001:26:2647-2652.
Neural Mobilization: A Systematic Review of Randomized Controlled Trialswith an Analysis of Therapeutic Efficacy / 21
11. van TuMer M. Furlan A. Bombardier C. Bouter L. Updated methodguidelines tor .systematic reviews in the Cochrane Collaboration BackReview Group. Spine 2003:28:1290-1299. 25.
12. CEBP. PEDro Scale. PEDro. Retrieved August 6, 2006 from http://w\vw.pedr<).fhs.usyd.edu.au/test/scale_item.htm!.
13. Maher C. Sherrington C, Herbert R. Moseley A. Elkins M. Reliability 26,ofthe FEDro Scale for rating quality of randomized controlled trials.Php Ther 2im-M7l3-72].
14. Clark HD, Wells GA. Huet C. et al. Assessing the quality of ran- 27.domized trials: Reliability of the Jadad scale. Control Clin TYials1999:20:448-452.
15. Overington M, Goddard D. Hing W. A critical appraisal and literature 28.critique on the effect of patellar taping: Is patellar taping effectivein the treatment of patellofemoral pain syndrome? New Zealand JPhysiother 2006:34:66-80.
16. Hakkennes S, Keating JL. Constraint-induced movement therapy 29.following stroke: A systematic review of randomised controlled trials.Aust J Physlnther 2005:51:221-231.
17. O'Siiea SD. Taylor NF, Faratz J. Peripheral muscle strength training 30.in COFD: A systematic review. Chest 2004:126:903-914.
18. Ackerman IN, Bennell KL, Does pre-operative physiotherapy improveoutcomes from lower limb joint replacement surger>'? A systematic 31.review. Aust J Physiother 2004:5(1:25-30.
19. Bieakley C. McDonough S. MacAuley D. The use of ice In the treatmentof acute soft-tissue injury: A systematic review of randomizedcontrolled trials. .4m J Sports Med 2004:32:251-261. 32.
20. Harvey L. Herbert R. Crosbie J. Does stretching induce lastingincreases in joint ROM? A systematic review. Physiother Researchfntemat 2002:7:1-13. 33.
21. Reid SA, Rivett DA. Manual therapy treatment of cervicogenicdizziness: A systematic review. Man Ther 2005:10:4-13.
22. Karjalainen K. Malmivaara A, van Tulder M. et al. Muitidisciplin-ary biopsychosociat rehabilitation for subacute low back pain in 34.working-age adults: A systematic review within the framework ofthe Cochrane Collaboration Back Review Group. Spine 2001:26:262-269. 35.
23. Linton SJ. van Tulder MW. Preventive interventions for back andneck pain problems. Spine 2001:26:778-787.
24. Akalin E. El 0. Peker 0. et a!. Treatment of carpal tunnel syndrome
with nerve and tendon gliding exercises. Am J Phys Med Rehabil2002:81:108-113.Allison GT Nagy BM. Hall T. A randomized clinical trial of manualtherapy for cervico-brachial pain syndrome; A pilot study. Man Ther2002:7:95-102.Baysal 0, Altay Z, Ozcan C. Ertem K. Yologlu S. Kayhan A. Comparisonof three conservative treatment protocols in carpal tunnel syndrome.intemutionalJ Clin Practice 2006:60:820-828.Cleland JA. Childs JD. Falmer JA, Eberhart S. Slump stretching inthe management of non-radicular low back pain: A pilot clinical trial./Van 7ft(?r 2007:11:279-286,Coppieters MW. Stappaerts KH. Wouters LL. Janssens K, Aberrantprotective force generation during neural provocation testing andthe effect of treatment in patients with neurogenic cervicobrachialpain. J Manipulative Physiological Therapeutics 2003:26:99-106.Drechsler WI. Knarr JF, Snyder-Mackler L A comparison of two treat-ment regimens for lateral epicondylitis: A randomized trial of clinicalinterventions. 7 Sport Rehabil 1997:6:226-234.Pinar L, Enhos A. Ada S, Cungor N, Can we use nerve gliding exer-cises in women with carpal tunnel syndrome? Advances in PhysicalTherapy 2005:22:467-475.Tal-Akabi A. Rushton A. An investigation to compare the effective-ness of carpal bone mobili.sation and neurodynamic mobilisationas methods of treatment for carpal tunnel syndrome, Man Ther2000:5:214-222.Vicenzino B. Collins D. Wright A. The initial effects of a cervical spinemanipulative physiotherapy treatment on the pain and dysfunctionof lateral epicondylalgia. Pain 1996:(i8:69-74.Salaffi F. Stancati A. Silvestri CA. Ciapetti A, Gra.ssi W. Minimalclinically Important changes in chronic muscuioskeietal pain in-tensity measured on a numerical rating scale, European J Pain2004:8:283-291.Beaton DE, Boers M, Weils GA. Many faces of the minimal clinicalimportant difference (MCID): A literature review and directions forfuture research. Curr Opin Rheiimatol 2002:14:109-114,Eliis RF. Hing W. DilleyA. McNair P, Diagnostic assessment of sciaticnerve movement during neural mobilisation: Quantitative assess-ment and reliability. Unpublished data. Auckland. AUT University:2007.
22 / The Journal of Manual & Manipulative Therapy. 2008













![[Draft] Malawi Joint Resource Mobilisation Strategy Web viewThis document provides focus to the joint resource mobilization efforts of ... and Disaster Risk Reduction ... Country Assessment](https://img.pdfslide.net/doc/110x75/5aa04f557f8b9a84178df5e7/draft-malawi-joint-resource-mobilisation-strategy-web-viewthis-document-provides.jpg)














