Embed Size (px)
Citation preview

66Med Genet 1997;34:666-669
Short reports
Neurogenic chronic idiopathic intestinalpseudo-obstruction, patent ductus arteriosus, andthrombocytopenia segregating as an X linkedrecessive disorder
D R FitzPatrick, L Strain, A E Thomas, D G D Barr, A Todd, N M Smith,W G Scobie
Department of ClinicalGenetics, MolecularMedicine Centre,Western GeneralHospital, EdinburghEH4 2XU, UKD R FitzPatrick
Department ofHumanGenetics, MolecularMedicine Centre,Western GeneralHospital, EdinburghEH4 2XU, UKD R FitzPatrickL Strain
Department ofPaediatricHaematology, RoyalHospital for SickChildren, EdinburghEH9 1LF, UKA E Thomas
Department ofMedicine, RoyalHospital for SickChildren, EdinburghEH9 1LF, UKD G D Barr
Scottish BloodTransfusion Service,Royal Infirmary,Edinburgh, UKA Todd
Department ofPathology, RoyalHospital for SickChildren, EdinburghEH9 1LF, UKN M Smith
Department ofSurgery, RoyalHospital for SickChildren, EdinburghEH9 1LF, UKW G Scobie
Correspondence to:Dr FitzPatrick.
Received 25 October 1996Revised version accepted forpublication 7 February 1997
AbstractWe present a family with three affectedmales in two generations with congenitalneurogenic chronic idiopathic intestinalpseudo-obstruction (CIIP), patent ductusarteriosus, and large platelet thrombocy-topenia apparently segregating as an Xlinked recessive disorder. The pattern ofsegregation of DNA markers within thefamily is consistent with linkage to thepreviously described neurogenic CIIP(CIIPX) locus at Xq28. This combinationmay represent a new contiguous gene dis-order and appears to have a good progno-sis with supportive therapy.(7Med Genet 1997;34:666-669)
Keywords: X chromosome; pseudo-obstruction; patentductus arteriosus; thrombocytopenia
Chronic idiopathic intestinal pseudo-obstruction (CIIP) may present at any age andis diagnosed by finding radiological, surgical,or manometric evidence of abnormal bowelmotility causing clinical features of intestinalobstruction with no mechanical aetiology.1 2Congenital CIIP is a rare, often fatal,3 cause ofabdominal distension in infancy and can becategorised, on the basis of histologicalexamination of a full thickness intestinalbiopsy, into three groups, neurogenic (28%),myopathic (36%), and unclassifiable (36%).4Recently, an X linked recessive neurogenicform of congenital CIIP (CIIPX) associatedwith pyloric hypertrophy and gut malrotationhas been shown to cosegregate with DNAmarkers at Xq28 in a large Italian family.5CIIPX is not associated with any othernon-gastrointestinal dysmorphic features. Herewe present a family with an apparently new Xlinked disorder characterised by congenitalneurogenic CIIP, patent ductus arteriosus(PDA), facial dysmorphism, and an unusuallarge platelet thrombocytopenia. We also dis-cuss similarities with three previously reportedmale infants6 7 and possible disease mecha-nisms in this family.
Case reportsCASE 1
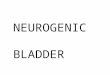
The proband is III.1 (fig 1), the first child ofhealthy, non-consanguineous Scottish parents.He was born at term weighing 3970 g after anuneventful pregnancy. At 4 days he wasassessed for bilious vomiting and abdominaldistension and a laparotomy performed at 10days showed malrotation with a narrow pedi-cle, which was corrected. He also requiredoperative ligation of a patent ductus arteriosus(PDA) at the age of 24 days. A post-laparotomybarium meal showed delayed passage with noobstruction. At 3 months he presented withchronic diarrhoea and vomiting and an intesti-nal biopsy at that time showed neuronal intes-tinal dysplasia (fig 2) suggestive of a diagnosisof neurogenic CIIP. His feeding problems wereprofound throughout the first year of life andhe initially required total parenteral nutritionwith subsequent nasogastric (NG) tube feed-ing. Chronic thrombocytopenia (32-104 x1 09/1) with no bleeding problem had also beennoted since birth. A bone marrow aspiration at6 months of age was normal with plentifulmegakaryocytes. He had further operations foran undescended right testis and infantileesotropia. When last reviewed at 6 years of age
1 1 2
1 2 311 4
III 1 2 3 4Figure 1 Family pedigree showing affected subjects 11.3,III. 1, and III. 4 related through a phenotypically normalfemale, 1. 2. .3 died in the neonatal period, but the causeof death is not known.
666

X linked syndromic intestinal pseudo-obstruction
t
.1
iO
w -.*-s t....... ..... i. t X
.*
- = iXs
_s @ .................. s -vmvi wsUL
>...i-QX Xq 8 w
B ^
. . a..iNV-Al
I1
Figure 2 Photomicrograph showing ileal mucosa withaberrant nerve fibres and ganglion cells in the laminapropria (small arrowheads). Large groups ofganglion cellsin normal submucosal location beneath muscularis mucosaeare also present (large arrowhead). Acetylcholinesterasestain.
(fig 3A) he was generally in good health withnear normal bowel function and doing well at a
normal school. He had mild craniofacialdysmorphism with a rather smooth philtrum, a
large jaw, and low set ears. Chromosomeanalysis was normal.
CASE 2
Case 2 (III.4) is the younger brother of case 1
and the fourth child of their parents. Case 2also has two older sisters (III.2, III.3) who are
both completely well. He was born at 38 weeks'gestation weighing 3827 g after a normal preg-nancy. He had early neonatal jaundice and was
noted to have feeding difficulties which neces-
sitated NG tube feeding. He was also noted tobe facially dysmorphic (fig 3B) with downwardslanting palpebral fissures, hypertelorism, andlow set ears. At 2 weeks of age he had an
episode of abdominal distension and visibleperistalsis. Barium studies showed slow pas-sage of the contrast media through the smallbowel with no evidence of mechanical obstruc-tion. A rectal biopsy at that time was too super-ficial to diagnose neuronal intestinal dysplasia;however, the clinical features were consistentwith the diagnosis of CIIP. He was also notedto have left sided hydronephrosis and a PDAwhich was ligated at 22 days. He has been per-sistently mildly thrombocytopenic (60-140 x
109/1) with large platelets noted on inspectionof the blood film (fig 4) but no bleeding prob-lems. His clinical picture over the first 9months of life has been very similar to his olderbrother with poor feeding (he continues to befed via nasogastric tube) and infrequentepisodes of abdominal distension and vomit-ing. His neurodevelopmental profile is normal.
C417j
Figure 3 Facial photographs of affected subjects andobligate carrier women. (A) Facial photograph of case 1 atthe age of 6 years. (B) Case 2 at the age of 8 months withdownward slanting palpebralfissures and hypertelorism; aNG tube is requiredforfeeding problems. (C) Mother (left)and maternal grandmother (right) of cases I and 2.
Figure 4 A peripheral blood film from case 2shows largebut not giant platelets with normal granulation inassociation with a mild thrombocytopenia. This is incontrast to Wiskott-Aldich syndrome where the platelets aresmall. A normal neutrophil and lymphocyte are also shown.
CASE 3Case 3 (11.3) is the maternal uncle of cases 1and 2 and was born in 1961 as the first child ofhealthy, non-consanguineous Scottish parents.He was born at term weighing 3800 g. He wasadmitted to hospital at the age of 3 days with a
667
I
-NW ,..

FitzPatrick et al
Markers AllelesDXS1108 1,2,3DXS15 1,2F8Cintron 13 1,2,3DXYS154 1, 2
11
III
Figure 5 Segregation ofXq28 hapl11.2, III. 1, and 11.4. The numbers (
are designated alleles at the (CA), mDXS15, F8C intron 13, and DXYS
history of poor feeding and blaparotomy at the age ofmalrotated, short midgut witsmall bowel. He died at the anecropsy showed a patentand atrial septal defect witdbowel and a microcolon. Intethat time was said to "exclu(Hirschprung's disease". Apartly calcified haemangiomEthe liver was also noted. Craphism was not mentioned an
graphs are available.
DNA studiesDNA MARKERSDNA samples were availabsubjects I.2, IL.2, III.1, and I]labelled primers were usedpolymorphic (CA)L repeat ir
DXS15, F8C intron 13, a
polymerase chain reaction (1ard methods. These marker162.261, 162.458, 163.59megabases from the Xp telc(Xq telomere is at 164.000the composite map at Genetbase, http://cedar.genetics.sproducts were analysed by a(
trophoresis with laser detectiusing the ALF system (Phar
RESULTSThese markers were chosen because they have
3 been linked to CIIPX in one large Italian2 family.5 No submicroscopic deletions were
1 detected in the affected boys using these mark-1 ers. However, a grandmaternal Xq28 haplotype
was found to cosegregate with the disease (fig5) giving a maximum lod score of 0.602 at
0=0.0.
3 2 Discussion2 2 The affected subjects in this family have an
unusual pattern of clinical features which showremarkable similarities to a previously reported
| _ ~~~~single case of a male child with congenital CIIP- and giant platelets6 (table 1). There are also4 similarities to a report of two brothers with
1 1 congenital CIIP and PDA which was thought3 3 to be an X linked disorder, although this report2 2 does not mention platelet abnormalities.7 No
oypes in subjects 2craniofacial dysmorphic features were de-
Yrom top to bottom) scribed in these cases. Interestingly, gut malro-arkers DXS1108, tation does not appear to be a common feature154, respectively. in congenital CIIP but is seen in 5/6 cases
..lious vomiting. A summarised in table 1 and several subjects inilious vomiting. A the Italian CIIPX kindred.5 This malformation16 days showed could, therefore, prove to be a useful pheno-
th dilatation of the typic marker for an X linked form of the
ige of 5 weeks and disease.
ductus arteriosus In the present family the affected subjects are
h distended small male and are related through a normal female
estinal histology at (fig 3C) suggesting X linked recessive inherit-de the presence of ance. In this respect it is interesting that I.2 had3 cm diameter an older brother who died in the late neonatal
a of the left lobe of period, although no clinical details are avail-iniofacial dysmor- able. Sex modified expression of an autosomalid no facial photo- dominant trait or a cryptic chromosomal
translocation could mimic this inheritance pat-tern. An X linked form of CIIP (CIIPX) asso-
ciated with bowel malrotation and pyloricstenosis has recently been mapped to Xq28
le for analysis on with a maximum lod score of 2.32 at 0=0.0II.4. Fluorescently with DXS 154. The DNA marker results in ourto amplify highly family are consistent with linkage to thisiarkers DXS 1108, marker although the lod score generated fromnd DXYS1 54 by such a small family is obviously non-significantPCR) using stand- (-4: 1 odds of linkage at the single locus tested) .
s map to Xq28 at The apparently disparate clinical features)6, and 163.669 seen in the affected subjects in this report mayDmere respectively be the result of a microdeletion in Xq28 whichmegabases using has inactivated CIIPX and neighbouring genes
tic Location Data- involved in platelet production and ductusoton.ac.uk). PCR arteriosus closure. Against this thought is thecrylamide gel elec- fact that there have been no families describedion of fluorescence with an X linked form of PDA, although PDAmacia). does occur as part of the spectrum of severe
Table 1 Comparison of clinicalfeatures of affected subjects
Harris et aP
Features Case I Case 2 Case 3 Case I Case 2 Pollock etal'
Sex M M M M M MCmIP + + + + + +
Malrotation + - + + + +
Pyloric stenosis - - - - - +
PDA + + + + + +
Thrombocytopenia + + +
Hydronephrosis - + - - -Esotropia + -?Undescended testes + - - -Normal intelligence + + ?
668

Xlinked syndromic intestinal pseudo-obstruction
malformations in the thoracoabdominal syn-drome (MIM 313850). Three different typesof X linked thrombocytopenia have beendescribed: X linked thrombocytopenia (MIM313900, maps to the same region of Xp asWiskott-Aldrich syndrome), thrombocytope-nia with raised serum IgA and renal disease(MIM 314000, single family), and thrombocy-topenia, platelet dysfunction, haemolysis, andimbalanced globin synthesis (MIM 314050,single family). None of these is associated withlarge platelets, indeed MIM 313900 causesreduced platelet volume, and all cause signifi-cant bleeding diatheses.Another possible explanation for the appar-
ently unrelated clinical features in thesechildren is that the CIIPX gene may have a rolein the developmental regulation of multiplesystems with different mutations causing a dif-ferent spectrum of abnormalities. The influ-ence of prostaglandin E on platelet functionand ductus closure is well known and it is pos-sible that mutations in the prostaglandinbiosynthetic or regulatory genes may result in a
phenotype similar to this family. However, nogenes in this pathway have been identified onthe X chromosome.
We would like to acknowledge the involvement and support ofthe family in this work, which was funded by the Western Gen-eral Hospital NHS Trust and the Edinburgh Sick Children'sNHS Trust. We also thank Dr Susan Holloway for help with lodscore calculation.
1 Miglioli M, Pironi L. Chronic intestinal pseudoobstruction.Clin Nutrit 1995;14:21-3.
2 Ghosh S, Eastwood MA. Primary chronic intestinalpseudoobstruction - an update. PostgradMedJt 1994;70:65-7.
3 Huang YC, Lee HG, Huang FY, et al. Neonatal-onsetchronic intestinal pseudoobstruction syndrome. Clin Pedi-atr 1995;34:241-7.
4 Fell JME, Smith W, Milla PJ. Infantile chronic idiopathicintestinal pseudoobstruction - the role of small-intestinalmanometry as a diagnostic-tool and prognostic indicator.Gut 1996;39:306-1 1.
5 Auricchio A, Brancolini V, Casari G, et al. The locus for anovel syndromal form of neuronal intestinal pseudoob-struction maps to Xq28. Am J Hum Genet 1996;58:743-8.
6 Pollock I, Holmes SJK, Patton MA, Hamilton PA, StaceyTE. Congenital intestinal pseudo-obstruction associatedwith a giant platelet disorder. J Med Genet 199 1;28:495-6.
7 Harris DJ, Ashkraft KW, Beatty EC, Holder TM, LeonidasJC. Natal teeth, patent ductus arteriosus and intestinalpseudo-obstruction: a lethal syndrome in the newborn.Clin Genet 1976;9:479-82.
669






![Neurogenic bladder [Dr. Edmond Wong]](https://img.pdfslide.net/doc/110x75/554af038b4c90559058b4779/neurogenic-bladder-dr-edmond-wong.jpg)