Embed Size (px)
Citation preview
1
NationalInstituteonDrugAbuse(NIDA)
Cocaine
LastUpdatedMay2016
https://www.drugabuse.gov
2
TableofContents
Cocaine
Whatiscocaine?
WhatisthescopeofcocaineuseintheUnitedStates?
Howiscocaineused?
Howdoescocaineproduceitseffects?
Whataresomewaysthatcocainechangesthebrain?
Whataretheshort-termeffectsofcocaineuse?
Whatarethelong-termeffectsofcocaineuse?
WhyarecocaineusersatriskforcontractingHIV/AIDSandhepatitis?
Whataretheeffectsofmaternalcocaineuse?
Howiscocaineaddictiontreated?
Howiscutting-edgesciencehelpingusbetterunderstandaddiction?
References
WherecanIgetfurtherinformationaboutcocaine?
3
Whatiscocaine?
Cocaineisapowerfullyaddictivestimulantdrug.Forthousandsofyears,peopleinSouthAmericahavechewedandingestedcocaleaves(Erythroxyloncoca),thesourceofcocaine,fortheirstimulanteffects. Thepurifiedchemical,cocainehydrochloride,wasisolatedfromtheplantmorethan100yearsago.Intheearly1900s,purifiedcocainewasthemainactiveingredientinmanytonicsandelixirsdevelopedtotreatawidevarietyofillnessesandwasevenaningredientintheearlyformulationsofCoca-Cola .Beforethedevelopmentofsyntheticlocalanesthetic,surgeonsusedcocainetoblockpain. However,researchhassinceshownthatcocaineisapowerfullyaddictivesubstancethatcanalterbrainstructureandfunctionifusedrepeatedly.
Today,cocaineisaScheduleIIdrug,whichmeansthatithashighpotentialforabusebutcanbeadministeredbyadoctorforlegitimatemedicaluses,suchaslocalanesthesiaforsomeeye,ear,andthroatsurgeries.Asastreetdrug,cocaineappearsasafine,white,crystallinepowderandisalsoknownasCoke,C,Snow,Powder,orBlow.Streetdealersoftendilute(or“cut”)itwithnon-psychoactivesubstancessuchascornstarch,talcumpowder,flour,orbakingsodatoincreasetheirprofits.Theymayalsoadulteratecocainewithotherdrugslikeprocaine(achemicallyrelatedlocalanesthetic)oramphetamine(anotherpsychoactivestimulant). Someuserscombinecocainewithheroin—calledaSpeedball.
Photoby©iStock.com/RafalCichawa
1,2
®
1
2,3
2

4
Peopleabusetwochemicalformsofcocaine:thewater-solublehydrochloridesaltandthewater-insolublecocainebase(orfreebase).Usersinjectorsnortthehydrochloridesalt,whichisapowder.Thebaseformofcocaineiscreatedbyprocessingthedrugwithammoniaorsodiumbicarbonate(bakingsoda)andwater,thenheatingittoremovethehydrochloridetoproduceasmokablesubstance.Thetermcrack,whichisthestreetnamegiventofreebasecocaine,referstothecracklingsoundheardwhenthemixtureissmoked.2
5
WhatisthescopeofcocaineuseintheUnitedStates?
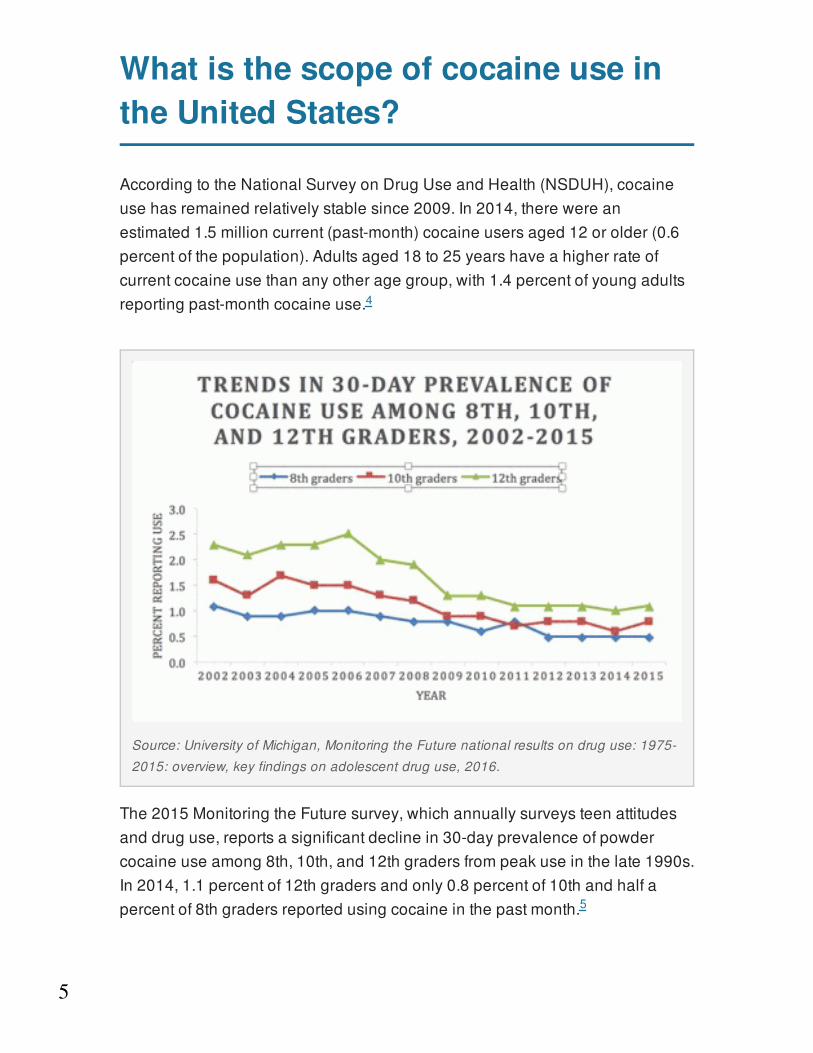
AccordingtotheNationalSurveyonDrugUseandHealth(NSDUH),cocaineusehasremainedrelativelystablesince2009.In2014,therewereanestimated1.5millioncurrent(past-month)cocaineusersaged12orolder(0.6percentofthepopulation).Adultsaged18to25yearshaveahigherrateofcurrentcocaineusethananyotheragegroup,with1.4percentofyoungadultsreportingpast-monthcocaineuse.
The2015MonitoringtheFuturesurvey,whichannuallysurveysteenattitudesanddruguse,reportsasignificantdeclinein30-dayprevalenceofpowdercocaineuseamong8th,10th,and12thgradersfrompeakuseinthelate1990s.In2014,1.1percentof12thgradersandonly0.8percentof10thandhalfapercentof8thgradersreportedusingcocaineinthepastmonth.
4
Source:UniversityofMichigan,MonitoringtheFuturenationalresultsondruguse:1975-
2015:overview,keyfindingsonadolescentdruguse,2016.
5
6
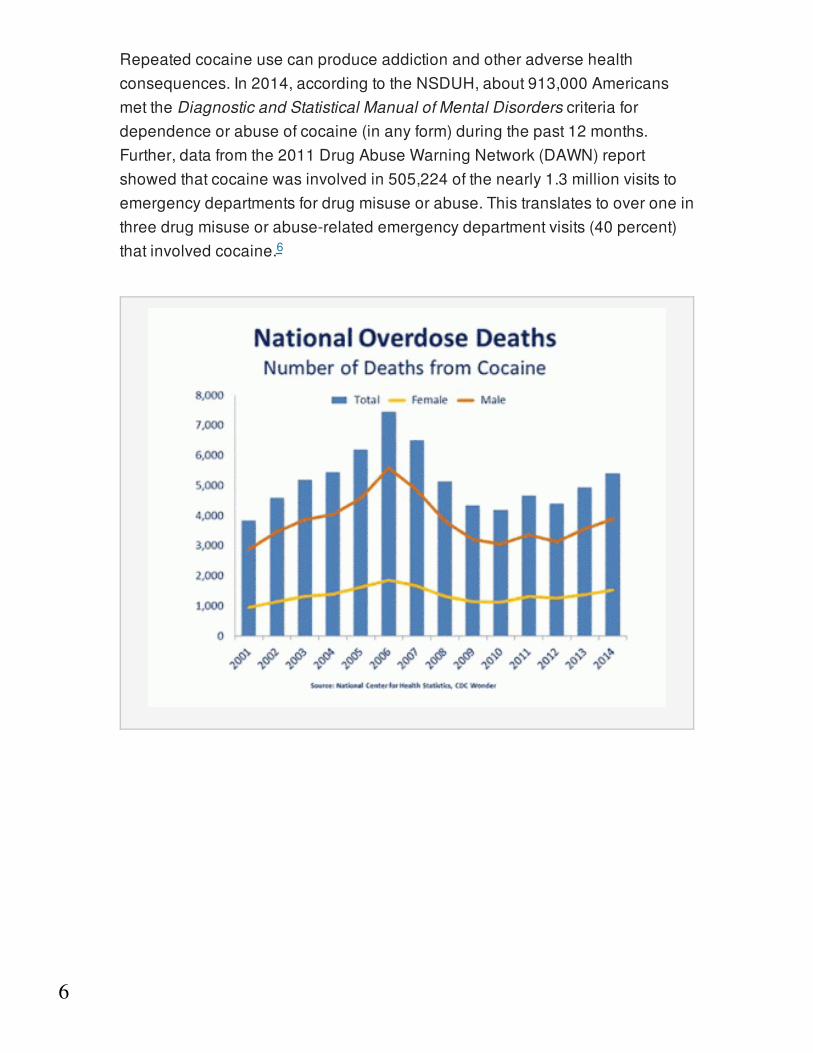
Repeatedcocaineusecanproduceaddictionandotheradversehealthconsequences.In2014,accordingtotheNSDUH,about913,000AmericansmettheDiagnosticandStatisticalManualofMentalDisorderscriteriafordependenceorabuseofcocaine(inanyform)duringthepast12months.Further,datafromthe2011DrugAbuseWarningNetwork(DAWN)reportshowedthatcocainewasinvolvedin505,224ofthenearly1.3millionvisitstoemergencydepartmentsfordrugmisuseorabuse.Thistranslatestooveroneinthreedrugmisuseorabuse-relatedemergencydepartmentvisits(40percent)thatinvolvedcocaine.6
7
Howiscocaineused?
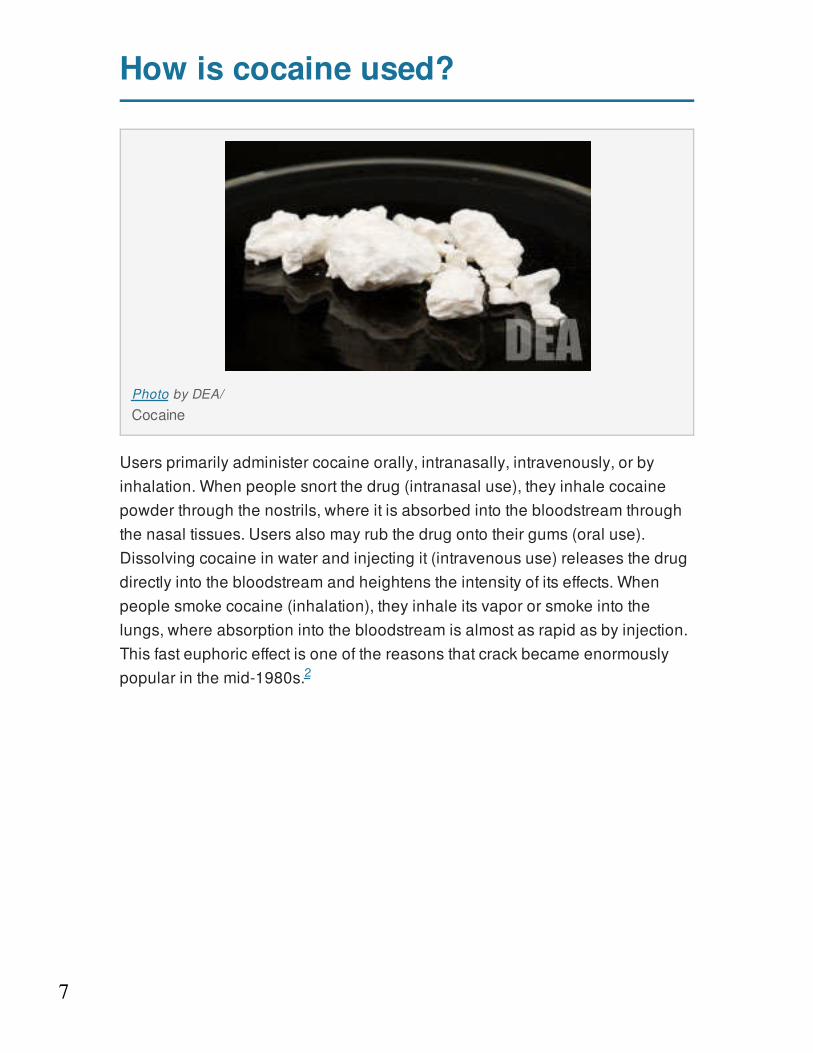
Usersprimarilyadministercocaineorally,intranasally,intravenously,orbyinhalation.Whenpeoplesnortthedrug(intranasaluse),theyinhalecocainepowderthroughthenostrils,whereitisabsorbedintothebloodstreamthroughthenasaltissues.Usersalsomayrubthedrugontotheirgums(oraluse).Dissolvingcocaineinwaterandinjectingit(intravenoususe)releasesthedrugdirectlyintothebloodstreamandheightenstheintensityofitseffects.Whenpeoplesmokecocaine(inhalation),theyinhaleitsvapororsmokeintothelungs,whereabsorptionintothebloodstreamisalmostasrapidasbyinjection.Thisfasteuphoriceffectisoneofthereasonsthatcrackbecameenormouslypopularinthemid-1980s.
PhotobyDEA/
Cocaine
2
8
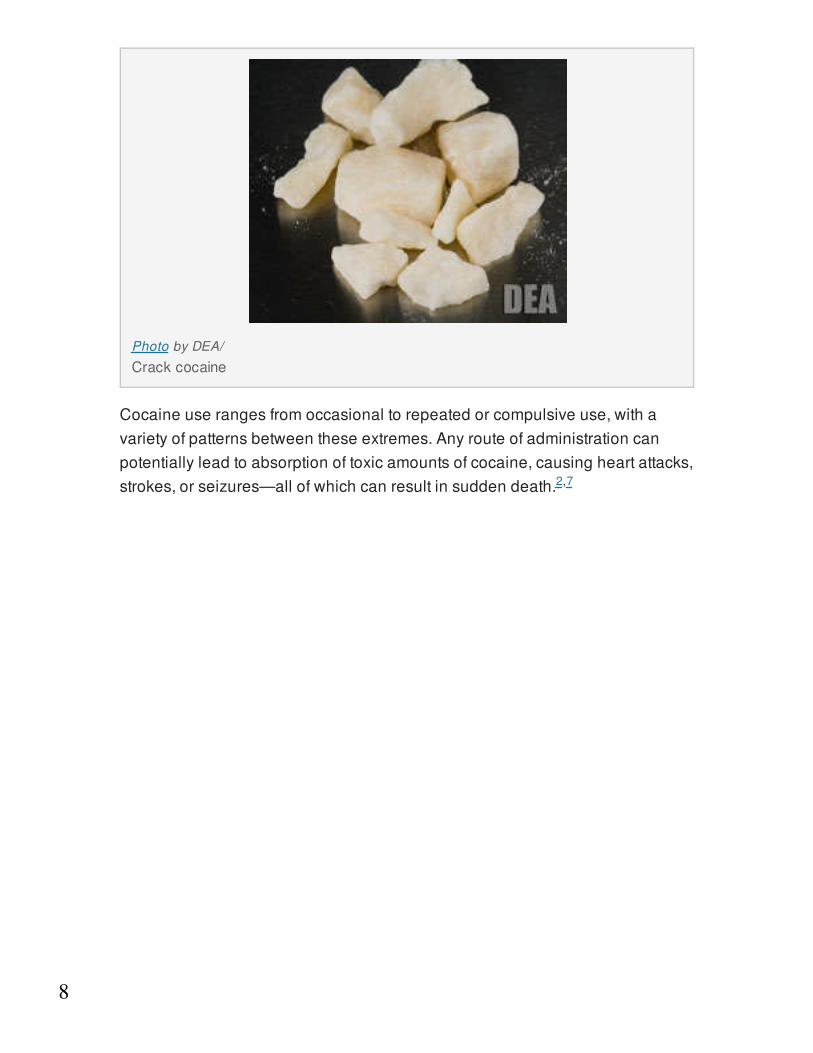
Cocaineuserangesfromoccasionaltorepeatedorcompulsiveuse,withavarietyofpatternsbetweentheseextremes.Anyrouteofadministrationcanpotentiallyleadtoabsorptionoftoxicamountsofcocaine,causingheartattacks,strokes,orseizures—allofwhichcanresultinsuddendeath.
PhotobyDEA/
Crackcocaine
2,7
9
Howdoescocaineproduceitseffects?
Thebrain’smesolimbicdopaminesystem,itsrewardpathway,isstimulatedbyalltypesofreinforcingstimuli,suchasfood,sex,andmanydrugsofabuse,includingcocaine. Thispathwayoriginatesinaregionofthemidbraincalledtheventraltegmentalareaandextendstothenucleusaccumbens,oneofthebrain’skeyrewardareas. Besidesreward,thiscircuitalsoregulatesemotionsandmotivation.
Inthenormalcommunicationprocess,dopamineisreleasedbyaneuronintothesynapse(thesmallgapbetweentwoneurons),whereitbindstospecializedproteinscalleddopaminereceptorsontheneighboringneuron.Bythisprocess,dopamineactsasachemicalmessenger,carryingasignalfromneurontoneuron.Anotherspecializedproteincalledatransporterremovesdopaminefromthesynapsetoberecycledforfurtheruse.
Drugsofabusecaninterferewiththisnormalcommunicationprocess.Forexample,cocaineactsbybindingtothedopaminetransporter,blockingtheremovalofdopaminefromthesynapse.Dopaminethenaccumulatesinthesynapsetoproduceanamplifiedsignaltothereceivingneurons.Thisiswhatcausestheeuphoriacommonlyexperiencedimmediatelyaftertakingthedrug(seethevideo"BrainReward:UnderstandingHowtheBrainRespondstoNaturalRewardsandDrugsofAbuse").
8
8
8
10
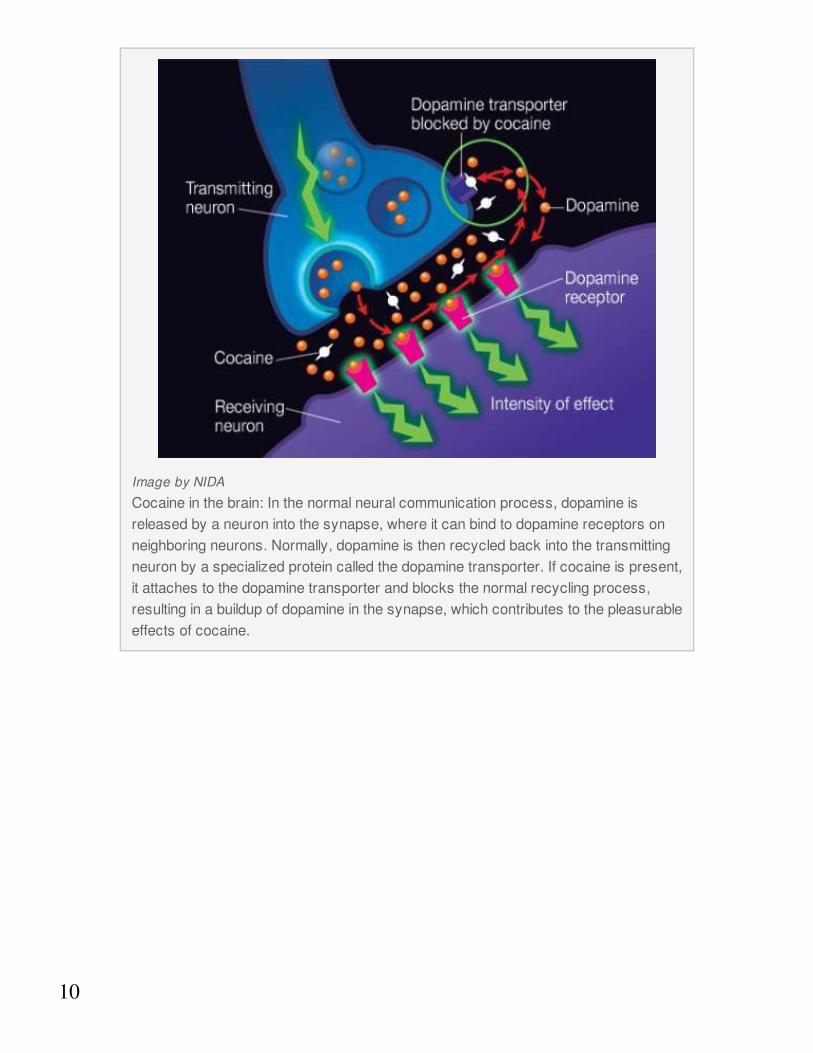
ImagebyNIDA
Cocaineinthebrain:Inthenormalneuralcommunicationprocess,dopamineisreleasedbyaneuronintothesynapse,whereitcanbindtodopaminereceptorsonneighboringneurons.Normally,dopamineisthenrecycledbackintothetransmittingneuronbyaspecializedproteincalledthedopaminetransporter.Ifcocaineispresent,itattachestothedopaminetransporterandblocksthenormalrecyclingprocess,resultinginabuildupofdopamineinthesynapse,whichcontributestothepleasurableeffectsofcocaine.
11
Whataresomewaysthatcocainechangesthebrain?
Useofcocaine,likeotherdrugsofabuse,induceslong-termchangesinthebrain.Animalstudiesshowthatcocaineexposurecancausesignificantneuroadaptationsinneuronsthatreleasetheexcitatoryneurotransmitterglutamate. Animalschronicallyexposedtococainedemonstrateprofoundchangesinglutamateneurotransmission—includinghowmuchisreleasedandthelevelofreceptorproteins—intherewardpathway,particularlythenucleusaccumbens.Theglutamatesystemmaybeanopportunetargetforanti-addictionmedicationdevelopment,withthegoalofreversingthecocaine-inducedneuroadaptationsthatcontributetothedrivetousethedrug.
Althoughaddictionresearchershavefocusedonadaptationsinthebrain’srewardsystem,drugsalsoaffectthebrainpathwaysthatrespondtostress.Stresscancontributetococainerelapse,andcocaineusedisordersfrequentlyco-occurwithstress-relateddisorders. Thestresscircuitsofthebrainaredistinctfromtherewardpathway,butresearchindicatesthatthereareimportantwaysthattheyoverlap.Theventraltegmentalareaseemstoactasacriticalintegrationsiteinthebrainthatrelaysinformationaboutbothstressanddrugcuestootherareasofthebrain,includingonesthatdrivecocaineseeking.Animalsthathavereceivedcocainerepeatedlyaremorelikelytoseekthedruginresponsetostress,andthemoreofthedrugtheyhavetaken,themorestressaffectsthisbehavior. Researchsuggeststhatcocaineelevatesstresshormones,inducingneuroadaptationsthatfurtherincreasesensitivitytothedrugandcuesassociatedwithit.
9,10
9
11
11
11
11
12
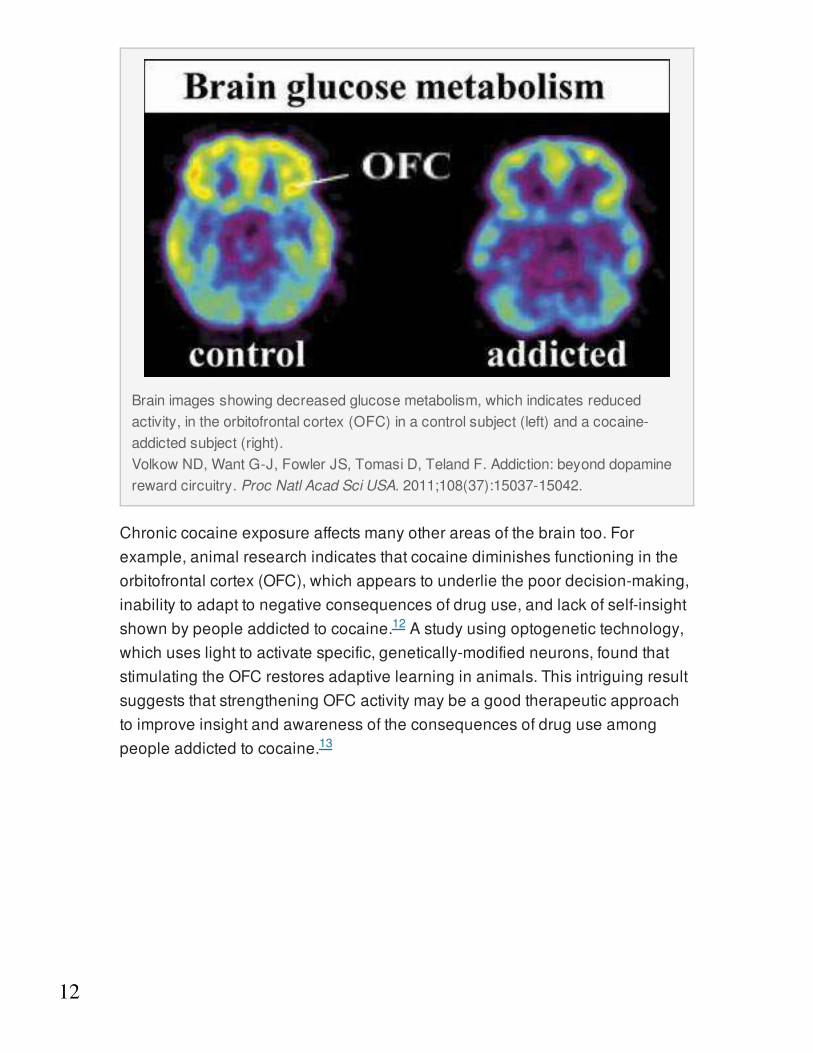
Chroniccocaineexposureaffectsmanyotherareasofthebraintoo.Forexample,animalresearchindicatesthatcocainediminishesfunctioningintheorbitofrontalcortex(OFC),whichappearstounderliethepoordecision-making,inabilitytoadapttonegativeconsequencesofdruguse,andlackofself-insightshownbypeopleaddictedtococaine. Astudyusingoptogenetictechnology,whichuseslighttoactivatespecific,genetically-modifiedneurons,foundthatstimulatingtheOFCrestoresadaptivelearninginanimals.ThisintriguingresultsuggeststhatstrengtheningOFCactivitymaybeagoodtherapeuticapproachtoimproveinsightandawarenessoftheconsequencesofdruguseamongpeopleaddictedtococaine.
Brainimagesshowingdecreasedglucosemetabolism,whichindicatesreducedactivity,intheorbitofrontalcortex(OFC)inacontrolsubject(left)andacocaine-addictedsubject(right).VolkowND,WantG-J,FowlerJS,TomasiD,TelandF.Addiction:beyonddopaminerewardcircuitry.ProcNatlAcadSciUSA.2011;108(37):15037-15042.
12
13
13
Whataretheshort-termeffectsofcocaineuse?
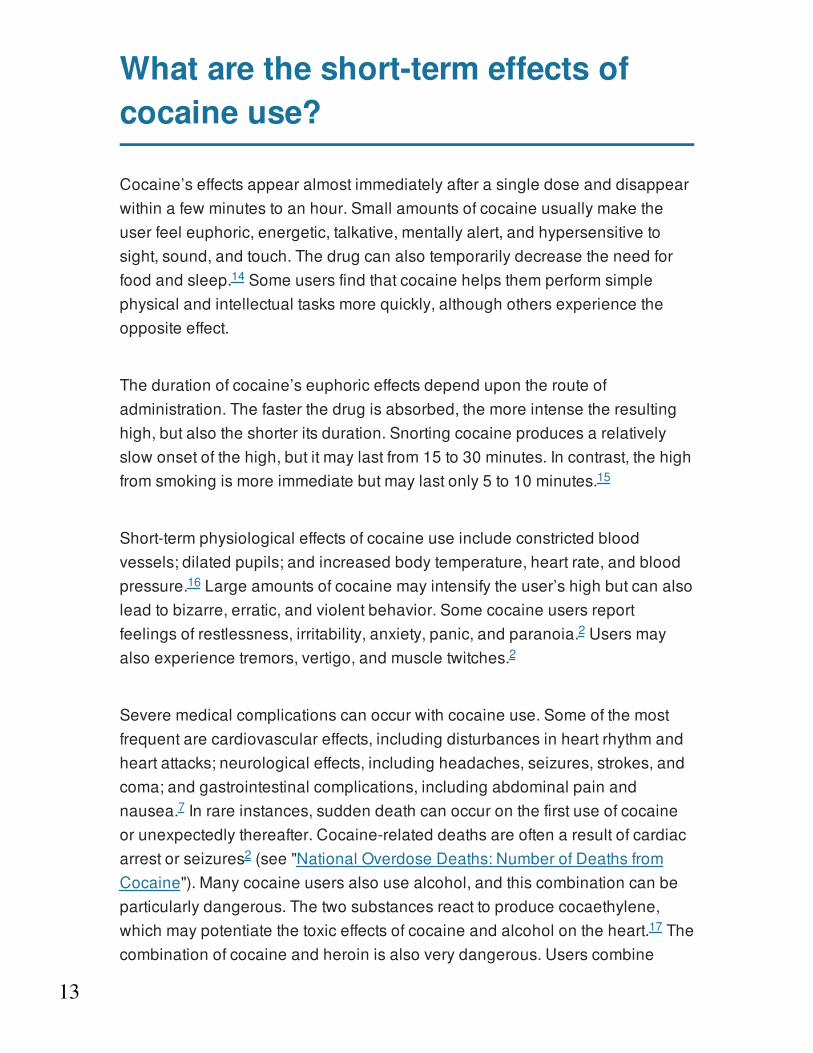
Cocaine’seffectsappearalmostimmediatelyafterasingledoseanddisappearwithinafewminutestoanhour.Smallamountsofcocaineusuallymaketheuserfeeleuphoric,energetic,talkative,mentallyalert,andhypersensitivetosight,sound,andtouch.Thedrugcanalsotemporarilydecreasetheneedforfoodandsleep. Someusersfindthatcocainehelpsthemperformsimplephysicalandintellectualtasksmorequickly,althoughothersexperiencetheoppositeeffect.
Thedurationofcocaine’seuphoriceffectsdependupontherouteofadministration.Thefasterthedrugisabsorbed,themoreintensetheresultinghigh,butalsotheshorteritsduration.Snortingcocaineproducesarelativelyslowonsetofthehigh,butitmaylastfrom15to30minutes.Incontrast,thehighfromsmokingismoreimmediatebutmaylastonly5to10minutes.
Short-termphysiologicaleffectsofcocaineuseincludeconstrictedbloodvessels;dilatedpupils;andincreasedbodytemperature,heartrate,andbloodpressure. Largeamountsofcocainemayintensifytheuser’shighbutcanalsoleadtobizarre,erratic,andviolentbehavior.Somecocaineusersreportfeelingsofrestlessness,irritability,anxiety,panic,andparanoia. Usersmayalsoexperiencetremors,vertigo,andmuscletwitches.
Severemedicalcomplicationscanoccurwithcocaineuse.Someofthemostfrequentarecardiovasculareffects,includingdisturbancesinheartrhythmandheartattacks;neurologicaleffects,includingheadaches,seizures,strokes,andcoma;andgastrointestinalcomplications,includingabdominalpainandnausea. Inrareinstances,suddendeathcanoccuronthefirstuseofcocaineorunexpectedlythereafter.Cocaine-relateddeathsareoftenaresultofcardiacarrestorseizures (see"NationalOverdoseDeaths:NumberofDeathsfromCocaine").Manycocaineusersalsousealcohol,andthiscombinationcanbeparticularlydangerous.Thetwosubstancesreacttoproducecocaethylene,whichmaypotentiatethetoxiceffectsofcocaineandalcoholontheheart. Thecombinationofcocaineandheroinisalsoverydangerous.Userscombine
14
15
16
2
2
7
2
17

14
thesedrugsbecausethestimulatingeffectsofcocaineareoffsetbythesedatingeffectsofheroin;however,thiscanleadtotakingahighdoseofheroinwithoutinitiallyrealizingit.Becausecocaine'seffectswearoffsooner,thiscanleadtoaheroinoverdose,inwhichtheuser'srespirationdangerouslyslowsdownorstops,possiblyfatally.
15
Whatarethelong-termeffectsofcocaineuse?
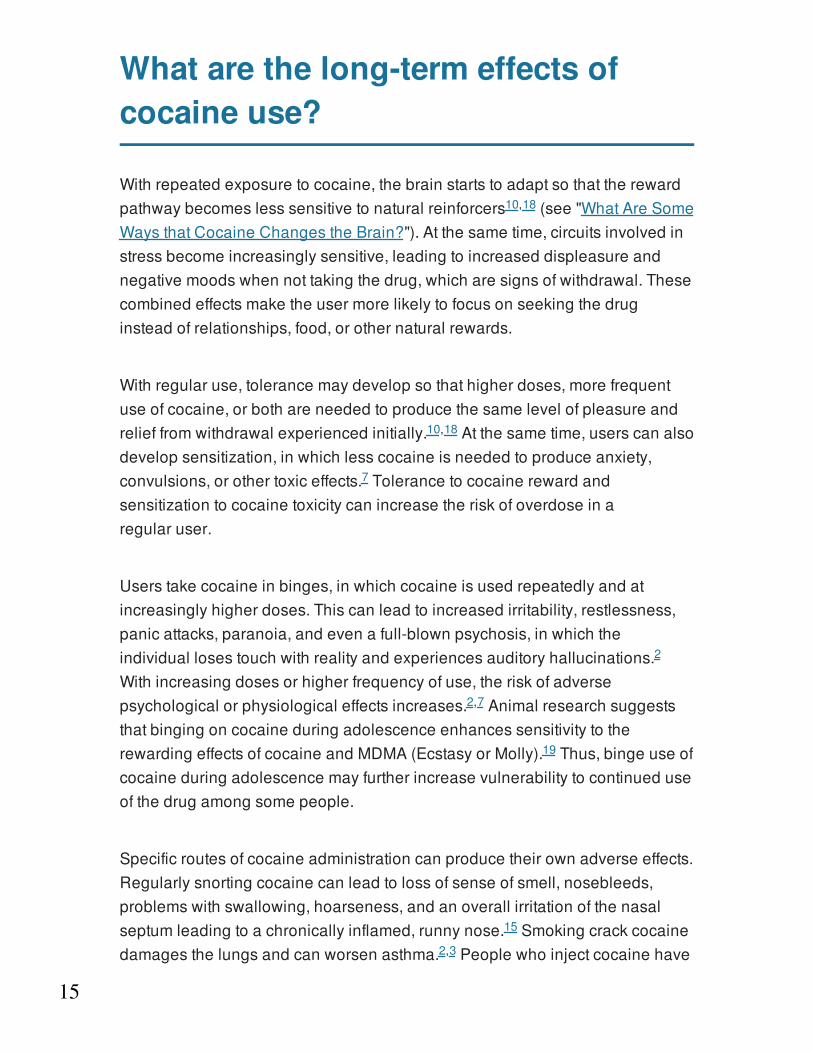
Withrepeatedexposuretococaine,thebrainstartstoadaptsothattherewardpathwaybecomeslesssensitivetonaturalreinforcers (see"WhatAreSomeWaysthatCocaineChangestheBrain?").Atthesametime,circuitsinvolvedinstressbecomeincreasinglysensitive,leadingtoincreaseddispleasureandnegativemoodswhennottakingthedrug,whicharesignsofwithdrawal.Thesecombinedeffectsmaketheusermorelikelytofocusonseekingthedruginsteadofrelationships,food,orothernaturalrewards.
Withregularuse,tolerancemaydevelopsothathigherdoses,morefrequentuseofcocaine,orbothareneededtoproducethesamelevelofpleasureandrelieffromwithdrawalexperiencedinitially. Atthesametime,userscanalsodevelopsensitization,inwhichlesscocaineisneededtoproduceanxiety,convulsions,orothertoxiceffects. Tolerancetococainerewardandsensitizationtococainetoxicitycanincreasetheriskofoverdoseinaregularuser.
Userstakecocaineinbinges,inwhichcocaineisusedrepeatedlyandatincreasinglyhigherdoses.Thiscanleadtoincreasedirritability,restlessness,panicattacks,paranoia,andevenafull-blownpsychosis,inwhichtheindividuallosestouchwithrealityandexperiencesauditoryhallucinations.Withincreasingdosesorhigherfrequencyofuse,theriskofadversepsychologicalorphysiologicaleffectsincreases. AnimalresearchsuggeststhatbingingoncocaineduringadolescenceenhancessensitivitytotherewardingeffectsofcocaineandMDMA(EcstasyorMolly). Thus,bingeuseofcocaineduringadolescencemayfurtherincreasevulnerabilitytocontinueduseofthedrugamongsomepeople.
Specificroutesofcocaineadministrationcanproducetheirownadverseeffects.Regularlysnortingcocainecanleadtolossofsenseofsmell,nosebleeds,problemswithswallowing,hoarseness,andanoverallirritationofthenasalseptumleadingtoachronicallyinflamed,runnynose. Smokingcrackcocainedamagesthelungsandcanworsenasthma. Peoplewhoinjectcocainehave
10,18
10,18
7
2
2,7
19
15
2,3
7
16
puncturemarkscalledtracks,mostcommonlyintheirforearms, andtheyareatriskofcontractinginfectiousdiseaseslikeHIVandhepatitisC(see"WhyAreCocaineUsersatRiskforContractingHIVandHepatitis?").Theyalsomayexperienceallergicreactions,eithertothedrugitselfortoadditivesinstreetcocaine,whichinseverecasescanresultindeath.
Cocainedamagesmanyotherorgansinthebody.Itreducesbloodflowinthegastrointestinaltract,whichcanleadtotearsandulcerations. Manychroniccocaineuserslosetheirappetiteandexperiencesignificantweightlossandmalnourishment.Cocainehassignificantandwell-recognizedtoxiceffectsontheheartandcardiovascularsystem. Chestpainthatfeelslikeaheartattackiscommonandsendsmanycocaineuserstotheemergencyroom.Cocaineuseislinkedwithincreasedriskofstroke, aswellasinflammationoftheheartmuscle,deteriorationoftheabilityofthehearttocontract,andaorticruptures.
Inadditiontotheincreasedriskforstrokeandseizures,otherneurologicalproblemscanoccurwithlong-termcocaineuse. Therehavebeenreportsofintracerebralhemorrhage,orbleedingwithinthebrain,andballoon-likebulgesinthewallsofcerebralbloodvessels. Movementdisorders,includingParkinson’sdisease,mayalsooccuraftermanyyearsofcocaineuse.Generally,studiessuggestthatawiderangeofcognitivefunctionsareimpairedwithlong-termcocaineuse—suchassustainingattention,impulseinhibition,memory,makingdecisionsinvolvingrewardsorpunishments,andperformingmotortasks.
Formercocaineusersareathighriskforrelapse,evenfollowinglongperiodsofabstinence.Researchindicatesthatduringperiodsofabstinence,thememoryofthecocaineexperienceorexposuretocuesassociatedwithdrugusecantriggerstrongcravings,whichcanleadtorelapse.
7
7
7,16,20
7,20
16
20
7,18
7,18
7
14
21
17
WhyarecocaineusersatriskforcontractingHIV/AIDSandhepatitis?
Drugintoxicationandaddictioncancompromisejudgmentanddecision-makingandpotentiallyleadtoriskysexualbehavior,includingtradingsexfordrugs,andneedlesharing.Thisincreasesacocaineuser’sriskforcontractinginfectiousdiseasessuchasHIVandhepatitisC(HCV). TherearenovaccinestopreventHIVorHCVinfections.
StudiesthatexaminepatternsofHIVinfectionandprogressionhavedemonstratedthatcocaineuseacceleratesHIVinfection. Researchindicatesthatcocaineimpairsimmunecellfunction, promotesreplicationoftheHIVvirus,andpotentiatesthedamagingeffectsofHIVondifferenttypesofcellsinthebrainandspinalcord,resultinginfurtherdamage. StudiesalsosuggestthatcocaineuseacceleratesthedevelopmentofNeuroAIDS,neurologicalconditionsassociatedwithHIVinfection.SymptomsofNeuroAIDSincludememoryloss,movementproblems,andvisionimpairment.
CocaineuserswithHIVoftenhaveadvancedprogressionofthedisease,withincreasedviralloadandaccelerateddecreasesinCD4+cellcounts.InfectionwithHIVincreasesriskforco-infectionwithHCV,avirusthataffectstheliver.Co-infectioncanleadtoseriousillnesses—includingproblemswiththeimmunesystemandneurologicconditions.Livercomplicationsareverycommon,withmanyco-infectedindividualsdyingofchronicliverdiseaseandcancer.AlthoughthelinkbetweeninjectiondruguseandHIV/HCViswellestablished,morestudiesareneededtounderstandthemolecularmechanismsunderlyingthisincreasedriskofco-infectioninnon-injectingsubstanceusers.
Theinteractionofsubstanceuse,HIV,andhepatitismayacceleratediseaseprogression.Forexample,HIVspeedsthecourseofHCVinfectionbyacceleratingtheprogressionofhepatitis-associatedliverdisease. ResearchhaslinkedHIV/HCVco-infectionwithincreasedmortalitywhencomparedtoeitherinfectionalone. Substanceuseandco-infectionlikelynegativelyinfluenceHIVdiseaseprogressionandtheabilityofthebodytomarshalanimmuneresponse.
22
23
24
23
23
24
22
24
24
24
24
18
PatientswithHIV/HCVco-infectioncanbenefitfromsubstanceabusetreatmentandantiretroviraltherapies,whencloselymonitored. Antiretroviraltreatmentisnoteffectiveforeveryoneandcanhavesignificantsideeffects,necessitatingclosemedicalsupervision.TestingforHIVandHCVisrecommendedforanyindividualwhohaseverinjecteddrugs,sincethediseaseishighlytransmissibleviainjection.
22
19
Whataretheeffectsofmaternalcocaineuse?
Mostwomenwhoareaddictedtococaineareofchildbearingage.Estimatessuggestthatabout5percentofpregnantwomenuseoneormoreaddictivesubstances, andtherearearound750,000cocaine-exposedpregnancieseveryyear. Althoughwomenmaybereluctanttoreportsubstanceusepatternsbecauseofsocialstigmaandfearoflosingcustodyoftheirchildren,theyshouldbeawarethatdrugusewhilepregnantisassociatedwithspecificrisksthatmaybereducedwithappropriatecare.
Cocaineuseduringpregnancyisassociatedwithmaternalmigrainesandseizures,prematuremembranerupture,andseparationoftheplacentalliningfromtheuteruspriortodelivery. Pregnancyisaccompaniedbynormalcardiovascularchanges,andcocaineuseexacerbatesthese—sometimesleadingtoseriousproblemswithhighbloodpressure(hypertensivecrises),spontaneousmiscarriage,pretermlabor,anddifficultdelivery. Cocaine-usingpregnantwomenmustreceiveappropriatemedicalandpsychologicalcare—includingaddictiontreatment—toreducetheserisks.
Sex-specificaddictiontreatmentandcomprehensiveservices—includingprenatalcare,mentalhealthcounseling,vocational/employmentassistance,andparentingskillstraining—canpromotedrugabstinenceandotherpositivehealthbehaviors. Motivationalincentives/contingencymanagement(see"BehavioralInterventions")asanadjuncttootheraddictiontreatmentisaparticularlypromisingstrategytoengagewomeninprenatalcareandcounselingforsubstanceuse.
Itisdifficulttoestimatethefullextentoftheconsequencesofmaternaldruguseandtodeterminethespecifichazardofaparticulardrugtotheunbornchild.Thisisbecausemultiplefactors—suchastheamountandnumberofalldrugsused,includingnicotineoralcohol;extentofprenatalcare;exposuretoviolenceintheenvironment;socioeconomicconditions;maternalnutrition;otherhealthconditions;andexposuretosexuallytransmitteddiseases—canallinteracttoinfluencematernalandchildoutcomes. Similarly,parentingstyles,
25
26
25
26
25
27
28
26,29,30
20
qualityofcareduringearlychildhood,exposuretoviolence,andcontinuedparentaldrugusearestrongenvironmentalfactorsinfluencingoutcomes.
Babiesborntomotherswhousecocaineduringpregnancyareoftenprematurelydelivered,havelowbirthweightsandsmallerheadcircumferences,andareshorterinlengththanbabiesborntomotherswhodonotusecocaine. Direpredictionsofreducedintelligenceandsocialskillsinbabiesborntomotherswhousedcrackcocainewhilepregnantduringthe1980s—so-called"crackbabies"—weregrosslyexaggerated.However,thefactthatmostofthesechildrendonotshowseriousovertdeficitsshouldnotbeoverinterpretedtoindicatethatthereisnocauseforconcern.
Usingsophisticatedtechnologies,scientistsarenowfindingthatexposuretococaineduringfetaldevelopmentmayleadtosubtle,yetsignificant,laterdeficitsinsomechildren. Theseincludebehaviorproblems(e.g.,difficultieswithself-regulation)anddeficitsinsomeaspectsofcognitiveperformance,informationprocessing,andsustainedattentiontotasks—abilitiesthatareimportantfortherealizationofachild’sfullpotential. Somedeficitspersistintothelateryears,withprenatallyexposedadolescentsshowingincreasedriskforsubtleproblemswithlanguageandmemory. Brainscansinteenssuggeststhatat-restfunctioningofsomebrainregions—includingareasinvolvedinattention,planning,andlanguage—maydifferfromthatofnon-exposedpeers. Moreresearchisneededonthelong-termeffectsofprenatalcocaineexposure.
31,32
26,29,30
31,32
32,33
34
35
21
Howiscocaineaddictiontreated?
In2013,cocaineaccountedforalmost6percentofalladmissionstodrugabusetreatmentprograms.Themajorityofindividuals(68percentin2013)whoseektreatmentforcocaineusesmokecrackandarelikelytobepolydrugusers,meaningtheyusemorethanonesubstance. Thosewhoprovidetreatmentforcocaineuseshouldrecognizethatdrugaddictionisacomplexdiseaseinvolvingchangesinthebrainaswellasawiderangeofsocial,familial,andotherenvironmentalfactors;therefore,treatmentofcocaineaddictionmustaddressthisbroadcontextaswellasanyotherco-occurringmentaldisordersthatrequireadditionalbehavioralorpharmacologicalinterventions.
PharmacologicalApproaches
Presently,therearenomedicationsapprovedbytheU.S.FoodandDrugAdministrationtotreatcocaineaddiction,thoughresearchersareexploringavarietyofneurobiologicaltargets.Pastresearchhasprimarilyfocusedondopamine,butscientistshavealsofoundthatcocaineuseinduceschangesinthebrainrelatedtootherneurotransmitters—includingserotonin,gamma-aminobutyricacid(GABA),norepinephrine,andglutamate. ResearchersarecurrentlytestingmedicationsthatactatthedopamineD receptor,asubtypeofdopaminereceptorthatisabundantintheemotionandrewardcentersofthebrain. Otherresearchistestingcompounds(e.g.,N-acetylcysteine)thatrestorethebalancebetweenexcitatory(glutamate)andinhibitory(GABA)neurotransmission,whichisdisruptedbylong-termcocaineuse. Researchinanimalsisalsolookingatmedications(e.g.,lorcaserin)thatactatserotoninreceptors.
Severalmedicationsmarketedforotherdiseasesshowpromiseinreducingcocaineusewithincontrolledclinicaltrials.Amongthese,disulfiram,whichisusedtotreatalcoholism,hasshownthemostpromise.Scientistsdonotyetknowexactlyhowdisulfiramreducescocaineuse,thoughitseffectsmayberelatedtoitsabilitytoinhibitanenzymethatconvertsdopaminetonorepinephrine.However,disulfiramdoesnotworkforeveryone.Pharmacogeneticstudiesarerevealingvariantsinthegenethatencodes
36
37
3
38
39
40
22
theDBHenzymeandseemstoinfluencedisulfiram’seffectivenessinreducingcocaineuse. Knowingapatient’sDBHgenotypecouldhelppredictwhetherdisulfiramwouldbeaneffectivepharmacotherapyforcocainedependenceinthatperson.
Finally,researchershavedevelopedandconductedearlytestsonacocainevaccinethatcouldhelpreducetheriskofrelapse.Thevaccinestimulatestheimmunesystemtocreatecocaine-specificantibodiesthatbindtococaine,preventingitfromgettingintothebrain. Inadditiontoshowingthevaccine’ssafety,aclinicaltrialfoundthatpatientswhoattainedhighantibodylevelssignificantlyreducedcocaineuse. However,only38percentofthevaccinatedsubjectsattainedsufficientantibodylevelsandforonly2months.
Researchersareworkingtoimprovethecocainevaccinebyenhancingthestrengthofbindingtococaineanditsabilitytoelicitantibodies. Newvaccinetechnologies,includinggenetransfertoboostthespecificityandlevelofantibodiesproducedorenhancethemetabolismofcocaine,mayalsoimprovetheeffectivenessofthistreatment. Apharmacogeneticsstudywithasmallnumberofpatientssuggeststhatindividualswithaparticulargenotyperespondwelltothecocainevaccine—anintriguingfindingthatrequiresmoreresearch.
Inadditiontotreatmentsforaddiction,researchersaredevelopingmedicalinterventionstoaddresstheacuteemergenciesthatresultfromcocaineoverdose.Oneapproachbeingexploredistheuseofgeneticallyengineeredhumanenzymesinvolvedinthebreakdownofcocaine,whichwouldcounterthebehavioralandtoxiceffectsofacocaineoverdose. Currently,researchersaretestingandrefiningtheseenzymesinanimalresearch,withtheultimategoalofmovingtoclinicaltrials.
BehavioralInterventions
Manybehavioraltreatmentsforcocaineaddictionhaveproventobeeffectiveinbothresidentialandoutpatientsettings.Indeed,behavioraltherapiesareoftentheonlyavailableandeffectivetreatmentsformanydrugproblems,includingstimulantaddictions.However,theintegrationofbehavioraland
41–43
41–43
44
45
45
44,46
47
48
49
49

23
pharmacologicaltreatmentsmayultimatelyprovetobethemosteffectiveapproach.
Oneformofbehavioraltherapythatisshowingpositiveresultsinpeoplewithcocaineusedisordersiscontingencymanagement(CM),alsocalledmotivationalincentives.Programsuseavoucherorprize-basedsystemthatrewardspatientswhoabstainfromcocaineandotherdrugs.Onthebasisofdrug-freeurinetests,thepatientsearnpoints,orchips,whichcanbeexchangedforitemsthatencouragehealthyliving,suchasagymmembership,movietickets,ordinneratalocalrestaurant.CMmaybeparticularlyusefulforhelpingpatientsachieveinitialabstinencefromcocaineandstayintreatment. Thisapproachhasrecentlybeenshowntobepracticalandeffectiveincommunitytreatmentprograms.
ResearchindicatesthatCMbenefitsdiversepopulationsofcocaineusers.Forexample,studiesshowthatcocaine-dependentpregnantwomenandwomenwithyoungchildrenwhoparticipatedinaCMprogramasanadjuncttoothersubstanceusedisordertreatmentwereabletostayabstinentlongerthanthosewhoreceivedanequivalentamountofvoucherswithnobehavioralrequirements. PatientsparticipatinginCMtreatmentforcocaineusewhoalsoexperiencedpsychiatricsymptoms—suchasdepression,emotionaldistress,andhostility—showedasignificantreductionintheseproblems,probablyrelatedtoreductionsincocaineuse.
Cognitive-behavioraltherapy(CBT)isaneffectiveapproachforpreventingrelapse.Thisapproachhelpspatientsdevelopcriticalskillsthatsupportlong-termabstinence—includingtheabilitytorecognizethesituationsinwhichtheyaremostlikelytousecocaine,avoidthesesituations,andcopemoreeffectivelywitharangeofproblemsassociatedwithdruguse.Thistherapycanalsobeusedinconjunctionwithothertreatments,therebymaximizingthebenefitsofboth.
Recently,researchersdevelopedacomputerizedformofCBT(CBT4CBT)thatpatientsuseinaprivateroomofaclinic. Thisinteractivemultimediaprogramcloselyfollowsthekeylessonsandskill-developmentactivitiesofin-personCBTinaseriesofmodules.Moviespresentexamplesandinformation
50
39,50–52
51
28
53
50
54–56
24
thatsupportthedevelopmentofcopingskills;quizzes,games,andhomeworkassignmentsreinforcethelessonsandprovideopportunitiestopracticeskills. StudieshaveshownthataddingCBT4CBTtoweeklycounselingboostedabstinence andincreasedtreatmentsuccessratesupto6monthsaftertreatment.
Therapeuticcommunities(TCs)—drug-freeresidencesinwhichpeopleinrecoveryfromsubstanceusedisordershelpeachothertounderstandandchangetheirbehaviors—canbeaneffectivetreatmentforpeoplewhousedrugs,includingcocaine. TCsmayrequirea6-to12-monthstayandcanincludeonsitevocationalrehabilitationandothersupportiveservicesthatfocusonsuccessfulre-integrationoftheindividualintosociety.TCscanalsoprovidesupportinotherimportantareas—improvinglegal,employment,andmentalhealthoutcomes.
Regardlessofthespecifictypeofsubstanceusedisordertreatment,itisimportantthatpatientsreceiveservicesthatmatchalloftheirtreatmentneeds.Forexample,anunemployedpatientwouldbenefitfromvocationalrehabilitationorcareercounselingalongwithaddictiontreatment.Patientswithmaritalproblemsmayneedcouplescounseling.Onceinpatienttreatmentends,ongoingsupport—alsocalledaftercare—canhelppeopleavoidrelapse.Researchindicatesthatpeoplewhoarecommittedtoabstinence,engageinself-helpbehaviors,andbelievethattheyhavetheabilitytorefrainfromusingcocaine(self-efficacy)aremorelikelytoabstain. Aftercareservestoreinforcethesetraitsandaddressproblemsthatmayincreasevulnerabilitytorelapse,includingdepressionanddecliningself-efficacy.
Scientistshavefoundpromisingresultsfromtelephone-basedcounselingasalow-costmethodtodeliveraftercare.Forexample,peoplewhomisusedstimulantswhoparticipatedinsevensessionsoftelephonecounselingshoweddecreasingdruguseduringthefirst3months,whereasthosewhodidnotreceivecallsincreasedtheiruse. Voucherincentivescanboostpatients'willingnesstoparticipateintelephoneaftercare,doublingthenumberofsessionsreceivedaccordingtoonestudy.
Community-basedrecoverygroups—suchasCocaineAnonymous—thatusea
54–56
54
55
57
57,58
59
59
60
61

25
12-stepprogramcanalsobehelpfulinmaintainingabstinence.Participantsmaybenefitfromthesupportivefellowshipandfromsharingwiththoseexperiencingcommonproblemsandissues.62

26
Howiscutting-edgesciencehelpingusbetterunderstandaddiction?
Twocutting-edgeareasofscience,geneticsandbrainimaging,aresignificantlyadvancingourunderstandingofcocaineaddiction.
Researchersestimatethatgeneticscontributes42to79percentoftheriskforcocaineuseanddependence. Ofcourse,withacomplexdiseasesuchasaddiction,manydifferentgenesareinvolved,andtheirexpressioncanbeinfluencedbytheenvironment.Thereappearstobesignificantoverlapinthegenesthatputpeopleatriskforalladdictivesubstances,perhapsindicatingacommonbiologicalpathwayforaddictionregardlessofthedrug.
Ingenome-wideassociationstudies(GWAS),researchersexaminewhethercertaingenevariantsaremorefrequentlyfoundinpeoplewithasubstanceusedisorder,whicheventuallymighthelpidentifythoseatincreasedriskfordrugaddiction. Identifyinggeneslinkedtoaddictionisonlythefirststep.Candidate-generesearchexaminesthelinksbetweensubstanceuseandspecificgenesthatencodeproteinsthatappeartoberelatedtoaddiction.Forexample,researchershavefoundconnectionsbetweenvariousaspectsofcocaineaddictionandthegenesthatencodeforparticulardopaminereceptorsandtheenzymesthatbreakdownthisneurotransmitter.
Becauseenvironmentalfactorstypicallyshapetheimpactofgenesondiseaserisk,researchersmustalsoidentifyhowparticulargene-by-environmentinteractionsinfluencethecourseofaddiction. Researchinthefieldofepigeneticsisuncoveringhowtheenvironmentinduceslong-termchangesingeneexpression—influencingthepatternofgeneexpression—withoutalteringtheDNAsequence.
Inanimalresearch,scientistsaredetermininghowlong-termcocaineexposurechangesgeneexpressioninthebrain,particularlyintherewardpathway.Studieshavelinkedspecificcocaine-inducedepigeneticchangestoneuroadaptations andbehavioralhallmarksofaddiction,suchassensitivityto
63
63
64,65
63
63
66
67
66,67
27
cocaine’srewardingeffects. Theepigeneticchangesinducedbycocainecanbepassedtothenextgeneration,evenifthedrugexposuredoesnotoccurprenatally. Althoughmuchmoregeneticandepigeneticresearchisneeded,understandingaddictionatthemolecularleveloffersgreatpromiseforimprovingdiagnosis,forexamplebydiscoveringbiomarkersfordiseaseseverityortreatmentresponse.
Althoughmoreresearchisneeded,brain-imagingmightbeusedtodetectbiomarkersfordrugaddictionvulnerability,asthesetechnologieshaveyieldedinsightsintotheprocessesunderlyingcravingandhowmedicationsmayquellthebrain’sresponsetococainecues. Arelativelynewneuroimagingtechnologycalleddefault-modeorresting-statefunctionalmagneticresonanceimaging(rs-fMRI)revealsbrainactivitywhenpeoplearealertbutnotperformingaparticulartask;researchersusethistechniquetocomparefunctionalbrainnetworksofpeoplewhohaveusedcocaineforalongtimeandthosewhohavenot.Thesestudiessuggestthatthereisreducedconnectivitybetweenvariousbraincircuits andbetweenthetwohemispheres amongpeoplewithcocainedependence.Researchershavealsocorrelatedreducedconnectivitybetweenparticularbraincircuitswithimportantaddiction-relatedbehaviors,includingriskforrelapse andimpulsivity.
Neuroimagingtechnologiesarealsodocumentinghowthebrainsofcocaineusersmayrecoverafterperiodsofabstinence.Forexample,thesetechniquesindicatethatyearsofcocaineuseareassociatedwithreducedgreymatterinparticularbrainregions.However,peoplewhomaintainedcocaineabstinenceforapproximately9monthsshowedgreymatterlevelssimilartoorgreaterthanthoseofpeoplewhohadneverusedthedrug. Furtheranalysisindicatedthattheincreasedgreymatteroccurredinregionsotherthantheonesalteredbycocaineuse,suggestingthattheneurobiologicalchangesinvolvedinrecoveryaremorecomplexthansimplyreversingthechangesrelatedtoaddiction. Theresearchersalsofoundthatincreasedgreymattervolumeinbrainregionsinvolvedwithbehavioralcontrolwereassociatedwithlongerdurationofabstinence.
fMRItechnologieshavealsorevealedthatabstinencefromcocainehasimportant,restorativeeffectsonthebrain.Althoughcurrentcocaineusersdemonstratedreducedbrainactivityinabraincircuitthatmediatesresponse
66,67
68
66
69
70–72 73
71 72
74
74
74

28
inhibitionduringamotorcontroltask,individualswhohadattainedabstinenceforanaverageof8monthsshowedsimilarpatternsofactivationandlevelsofperformancetothosewhohadneverusedthedrug. Theresultssuggestthatabstinencehelpsrestorethefunctioningofthisbraincircuit.
Researchersareengagedinseverallarge-scale,collaborativeprojectstomapthehumanconnectome,whichisthebrain’snetworkofinterconnectedcircuits.Forexample,theNationalInstitutesofHealthsupportstheHumanConnectomeProjecttogeneratemapsofthedeveloping,adult,andagingbrain.Byhavingamapofthetypicalbrain,scientistswillfurtherunderstandhowneuralfunctioningdiffersinbehavioraldisorders—knowledgethatwilldriveimproveddiagnosticsandtreatments.
75
29
References
1. CalatayudJ,GonzálezA.Historyofthedevelopmentandevolutionoflocalanesthesiasincethecocaleaf.Anesthesiology.2003;98(6):1503-1508.
2. GoldsteinRA,DesLauriersC,BurdaAM.Cocaine:history,socialimplications,andtoxicity–areview.Dis–MonDM.2009;55(1):6-38.doi:10.1016/j.disamonth.2008.10.002.
3. DrentM,WijnenP,BastA.Interstitiallungdamageduetococaineabuse:pathogenesis,pharmacogenomicsandtherapy.CurrMedChem.2012;19(33):5607-5611.
4. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).BehavioralHealthTrendsintheUnitedStates:Resultsfromthe2014NationalSurveyonDrugUseandHealth.Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration;2015.HHSPublicationNo.SMA15-4927,NSDUHSeriesH-50.
5. JohnstonL,O’MalleyP,MiechR,BachmanJ,SchulenbergJ.MonitoringtheFutureNationalSurveyResultsonDrugUse:1975-2015:Overview:KeyFindingsonAdolescentDrugUse.AnnArbor,MI:InstituteforSocialResearch,TheUniversityofMichigan;2015.
6. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).DrugAbuseWarningNetwork:2011:SelectedTablesofNationalEstimatesofDrug-RelatedEmergencyDepartmentVisits.Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration;2013.
7. RiezzoI,FioreC,DeCarloD,etal.Sideeffectsofcocaineabuse:multiorgantoxicityandpathologicalconsequences.CurrMedChem.2012;19(33):5624-5646.
8. BaikJ-H.Dopaminesignalinginreward-relatedbehaviors.FrontNeuralCircuits.2013;7.doi:10.3389/fncir.2013.00152.
9. SchmidtHD,PierceRC.Cocaine-inducedneuroadaptationsinglutamatetransmission:potentialtherapeutictargetsforcravingandaddiction.AnnNYAcadSci.2010;1187:35-75.doi:10.1111/j.1749-6632.2009.05144.x.
10. WolfME.TheBermudaTriangleofcocaine-inducedneuroadaptations.
30
TrendsNeurosci.2010;33(9):391-398.doi:10.1016/j.tins.2010.06.003.
11. MantschJR,VranjkovicO,TwiningRC,GasserPJ,McReynoldsJR,BlacktopJM.Neurobiologicalmechanismsthatcontributetostress-relatedcocaineuse.Neuropharmacology.2014;76,PartB:383-394.doi:10.1016/j.neuropharm.2013.07.021.
12. LucantonioF,StalnakerTA,ShahamY,NivY,SchoenbaumG.Theimpactoforbitofrontaldysfunctiononcocaineaddiction.NatNeurosci.2012;15(3):358-366.doi:10.1038/nn.3014.
13. LucantonioF,TakahashiYK,HoffmanAF,etal.Orbitofrontalactivationrestoresinsightlostaftercocaineuse.NatNeurosci.2014;17(8):1092-1099.doi:10.1038/nn.3763.
14. SpronkDB,vanWelJHP,RamaekersJG,VerkesRJ.Characterizingthecognitiveeffectsofcocaine:acomprehensivereview.NeurosciBiobehavRev.2013;37(8):1838-1859.doi:10.1016/j.neubiorev.2013.07.003.
15. AdvokatC,ComatyJ,JulienR.Julien’sPrimerofDrugAction.13thed.NewYork,NY:WorthPublishers;2014.
16. FonsecaAC,FerroJM.Drugabuseandstroke.CurrNeurolNeurosciRep.2013;13(2):325.doi:10.1007/s11910-012-0325-0.
17. PenningsEJM,LecceseAP,WolffFAde.Effectsofconcurrentuseofalcoholandcocaine.AddictAbingdonEngl.2002;97(7):773-783.
18. BüttnerA.Neuropathologicalalterationsincocaineabuse.CurrMedChem.2012;19(33):5597-5600.
19. Mateos-GarcíaA,Roger-SánchezC,Rodriguez-AriasM,etal.HighersensitivitytotheconditionedrewardingeffectsofcocaineandMDMAinHigh-Novelty-Seekersmiceexposedtoacocainebingeduringadolescence.Psychopharmacology(Berl).2015;232(1):101-113.doi:10.1007/s00213-014-3642-y.
20. MarajS,FigueredoVM,LynnMorrisD.Cocaineandtheheart.ClinCardiol.2010;33(5):264-269.doi:10.1002/clc.20746.
21. SinhaR.Theclinicalneurobiologyofdrugcraving.CurrOpinNeurobiol.2013;23(4):649-654.doi:10.1016/j.conb.2013.05.001.
31
22. KhalsaJH,ElkashefA.InterventionsforHIVandhepatitisCvirusinfectionsinrecreationaldrugusers.ClinInfectDis.2010;50(11):1505-1511.doi:10.1086/652447.
23. BuchS,YaoH,GuoM,etal.CocaineandHIV-1interplayinCNS:cellularandmolecularmechanisms.CurrHIVRes.2012;10(5):425-428.
24. ParikhN,NonnemacherMR,PirroneV,BlockT,MehtaA,WigdahlB.Substanceabuse,HIV-1andhepatitis.CurrHIVRes.2012;10(7):557-571.
25. WendellAD.Overviewandepidemiologyofsubstanceabuseinpregnancy.ClinObstetGynecol.2013;56(1):91-96.doi:10.1097/GRF.0b013e31827feeb9.
26. CainMA,BornickP,WhitemanV.Thematernal,fetal,andneonataleffectsofcocaineexposureinpregnancy.ClinObstetGynecol.2013;56(1):124-132.doi:10.1097/GRF.0b013e31827ae167.
27. HullL,MayJ,Farrell-MooreD,SvikisDS.Treatmentofcocaineabuseduringpregnancy:translatingresearchtoclinicalpractice.CurrPsychiatryRep.2010;12(5):454-461.doi:10.1007/s11920-010-0138-2.
28. SchottenfeldRS,MooreB,PantalonMV.Contingencymanagementwithcommunityreinforcementapproachortwelve-stepfacilitationdrugcounselingforcocainedependentpregnantwomenorwomenwithyoungchildren.DrugAlcoholDepend.2011;118(1):48-55.doi:10.1016/j.drugalcdep.2011.02.019.
29. BehnkeM,SmithVC,AbuseConS,NewbornConFA.Prenatalsubstanceabuse:short-andlong-termeffectsontheexposedfetus.Pediatrics.2013;131(3):e1009-e1024.doi:10.1542/peds.2012-3931.
30. GouinK,MurphyK,ShahPS,KnowledgeSynthesisgrouponDeterminantsofLowBirthWeightandPretermBirths.Effectsofcocaineuseduringpregnancyonlowbirthweightandpretermbirth:systematicreviewandmetaanalyses.AmJObstetGynecol.2011;204(4):340.e1-e12.doi:10.1016/j.ajog.2010.11.013.
31. LambertBL,BauerCR.Developmentalandbehavioralconsequencesofprenatalcocaineexposure:areview.JPerinatolOffJCalifPerinatAssoc.2012;32(11):819-828.doi:10.1038/jp.2012.90.
32
32. LesterBM,LagasseLL.Childrenofaddictedwomen.JAddictDis.2010;29(2):259-276.doi:10.1080/10550881003684921.
33. AckermanJP,RigginsT,BlackMM.Areviewoftheeffectsofprenatalcocaineexposureamongschool-agedchildren.Pediatrics.2010;125(3):554-565.doi:10.1542/peds.2009-0637.
34. Buckingham-HowesS,BergerSS,ScalettiLA,BlackMM.Systematicreviewofprenatalcocaineexposureandadolescentdevelopment.Pediatrics.2013;131(6):e1917-e1936.doi:10.1542/peds.2012-0945.
35. LiK,ZhuD,GuoL,etal.Connectomicssignaturesofprenatalcocaineexposureaffectedadolescentbrains.HumBrainMapp.2013;34(10):2494-2510.doi:10.1002/hbm.22082.
36. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).TreatmentEpisodeDataSet(TEDS):2003-2013.NationalAdmissionstoSubstanceAbuseTreatmentServices.Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration;2015.BHSISSeriesS-75,HHSPublicationNo.(SMA)15-4934.
37. ShorterD,DomingoCB,KostenTR.Emergingdrugsforthetreatmentofcocaineusedisorder:areviewofneurobiologicaltargetsandpharmacotherapy.ExpertOpinEmergDrugs.2015;20(1):15-29.doi:10.1517/14728214.2015.985203.
38. KarilaL,ReynaudM,AubinH-J,etal.Pharmacologicaltreatmentsforcocainedependence:istheresomethingnew?CurrPharmDes.2011;17(14):1359-1368.
39. KampmanKM.What’snewinthetreatmentofcocaineaddiction?CurrPsychiatryRep.2010;12(5):441-447.doi:10.1007/s11920-010-0143-5.
40. Harvey-LewisC,LiZ,HigginsGA,FletcherPJ.The5-HT2Creceptoragonistlorcaserinreducescocaineself-administration,reinstatementofcocaine-seekingandcocaineinducedlocomotoractivity.Neuropharmacology.2016;101:237-245.doi:10.1016/j.neuropharm.2015.09.028.
41. ShorterD,NielsenDA,HuangW,HardingMJ,HamonSC,KostenTR.Pharmacogeneticrandomizedtrialforcocaineabuse:disulfiramand1A-adrenoceptorgenevariation.EurNeuropsychopharmacolJEurCollNeuropsychopharmacol.2013;23(11):1401-1407.
33
doi:10.1016/j.euroneuro.2013.05.014.
42. SpellicyCJ,KostenTR,HamonSC,HardingMJ,NielsenDA.ANKK1andDRD2pharmacogeneticsofdisulfiramtreatmentforcocaineabuse.PharmacogenetGenomics.2013;23(7):333-340.doi:10.1097/FPC.0b013e328361c39d.
43. KostenTR,WuG,HuangW,etal.Pharmacogeneticrandomizedtrialforcocaineabuse:disulfiramanddopamine-hydroxylase. BiolPsychiatry.2013;73(3):219-224.doi:10.1016/j.biopsych.2012.07.011.
44. KostenTR,DomingoCB.Canyouvaccinateagainstsubstanceabuse?ExpertOpinBiolTher.2013;13(8):1093-1097.doi:10.1517/14712598.2013.791278.
45. MartellBA,OrsonFM,PolingJ,etal.Cocainevaccineforthetreatmentofcocainedependenceinmethadone-maintainedpatients:arandomized,double-blind,placebo-controlledefficacytrial.ArchGenPsychiatry.2009;66(10):1116-1123.doi:10.1001/archgenpsychiatry.2009.128.
46. CaiX,TsuchikamaK,JandaKD.Modulatingcocainevaccinepotencythroughhaptenfluorination.JAmChemSoc.2013;135(8):2971-2974.doi:10.1021/ja400356g.
47. BrimijoinS,ShenX,OrsonF,KostenT.Prospects,promiseandproblemsontheroadtoeffectivevaccinesandrelatedtherapiesforsubstanceabuse.ExpertRevVaccines.2013;12(3):323-332.doi:10.1586/erv.13.1.
48. NielsenDA,HamonSC,KostenTR.The-opioidreceptorgeneasapredictorofresponseinacocainevaccineclinicaltrial.PsychiatrGenet.2013;23(6):225-232.doi:10.1097/YPG.0000000000000008.
49. SchindlerCW,GoldbergSR.Acceleratingcocainemetabolismasanapproachtothetreatmentofcocaineabuseandtoxicity.FutureMedChem.2012;4(2):163-175.doi:10.4155/fmc.11.181.
50. PenberthyJK,Ait-DaoudN,VaughanM,FanningT.Reviewoftreatmentforcocainedependence.CurrDrugAbuseRev.2010;3(1):49-62.
51. PetryNM,BarryD,AlessiSM,RounsavilleBJ,CarrollKM.Arandomizedtrialadaptingcontingencymanagementtargetsbasedoninitialabstinencestatusofcocaine-dependentpatients.JConsultClinPsychol.
34
2012;80(2):276-285.doi:10.1037/a0026883.
52. SchierenbergA,vanAmsterdamJ,vandenBrinkW,GoudriaanAE.Efficacyofcontingencymanagementforcocainedependencetreatment:areviewoftheevidence.CurrDrugAbuseRev.2012;5(4):320-331.
53. PetryNM,AlessiSM,RashCJ.Contingencymanagementtreatmentsdecreasepsychiatricsymptoms.JConsultClinPsychol.2013;81(5):926-931.doi:10.1037/a0032499.
54. CarrollKM,BallSA,MartinoS,etal.Computer-assisteddeliveryofcognitive-behavioraltherapyforaddiction:arandomizedtrialofCBT4CBT.AmJPsychiatry.2008;165(7):881-888.doi:10.1176/appi.ajp.2008.07111835.
55. CarrollKM,BallSA,MartinoS,NichC,BabuscioTA,RounsavilleBJ.Enduringeffectsofacomputer-assistedtrainingprogramforcognitivebehavioraltherapy:a6-monthfollow-upofCBT4CBT.DrugAlcoholDepend.2009;100(1-2):178-181.doi:10.1016/j.drugalcdep.2008.09.015.
56. CarrollKM,KilukBD,NichC,etal.Computer-assisteddeliveryofcognitive-behavioraltherapy:efficacyanddurabilityofCBT4CBTamongcocaine-dependentindividualsmaintainedonmethadone.AmJPsychiatry.2014;171(4):436-444.doi:10.1176/appi.ajp.2013.13070987.
57. VanderplasschenW,ColpaertK,AutriqueM,etal.Therapeuticcommunitiesforaddictions:areviewoftheireffectivenessfromarecovery-orientedperspective.SciWorldJ.2013;2013,2013:e427817.doi:10.1155/2013/427817.
58. LeonGD.Isthetherapeuticcommunityanevidencebasedtreatment?Whattheevidencesays.TherCommunitiesIntJdournalTherSupportOrgan.2010;31(2):104-128.
59. McKayJR,VanHornD,RennertL,DrapkinM,IveyM,KoppenhaverJ.Factorsinsustainedrecoveryfromcocainedependence.JSubstAbuseTreat.2013;45(2):163-172.doi:10.1016/j.jsat.2013.02.007.
60. FarabeeD,CousinsSJ,BrechtM-L,etal.Acomparisonoffourtelephone-basedcounselingstylesforrecoveringstimulantusers.PsycholAddictBehav.2013;27(1):223-229.doi:10.1037/a0029572.
35
61. VanHornDHA,DrapkinM,IveyM,etal.Voucherincentivesincreasetreatmentparticipationintelephone-basedcontinuingcareforcocainedependence.DrugAlcoholDepend.2011;114(2-3):225-228.doi:10.1016/j.drugalcdep.2010.09.007.
62. DonovanDM,DaleyDC,BrighamGS,etal.Stimulantabusergroupstoengagein12-step:amultisitetrialintheNationalInstituteonDrugAbuseClinicalTrialsNetwork.JSubstAbuseTreat.2013;44(1):103-114.doi:10.1016/j.jsat.2012.04.004.
63. AgrawalA,VerweijKJH,GillespieNA,etal.Thegeneticsofaddiction-atranslationalperspective.TranslPsychiatry.2012;2:e140.doi:10.1038/tp.2012.54.
64. DrgonT,ZhangP-W,JohnsonC,etal.Genomewideassociationforaddiction:replicatedresultsandcomparisonsoftwoanalyticapproaches.PloSOne.2010;5(1):e8832.doi:10.1371/journal.pone.0008832.
65. KreekMJ,LevranO,ReedB,SchlussmanSD,ZhouY,ButelmanER.Opiateaddictionandcocaineaddiction:underlyingmolecularneurobiologyandgenetics.JClinInvest.2012;122(10):3387-3393.doi:10.1172/JCI60390.
66. NestlerEJ.Epigeneticmechanismsofdrugaddiction.Neuropharmacology.2014;76PtB:259-268.doi:10.1016/j.neuropharm.2013.04.004.
67. SchmidtHD,McGintyJF,WestAE,Sadri-VakiliG.Epigeneticsandpsychostimulantaddiction.ColdSpringHarbPerspectMed.2013;3(3):a012047.doi:10.1101/cshperspect.a012047.
68. VassolerFM,Sadri-VakiliG.Mechanismsoftransgenerationalinheritanceofaddictive-likebehaviors.Neuroscience.2014;264:198-206.doi:10.1016/j.neuroscience.2013.07.064.
69. YoungKA,FranklinTR,RobertsDCS,etal.Nippingcuereactivityinthebud:baclofenpreventslimbicactivationelicitedbysubliminaldrugcues.JNeurosciOffJSocNeurosci.2014;34(14):5038-5043.doi:10.1523/JNEUROSCI.4977-13.2014.
70. GuH,SalmeronBJ,RossTJ,etal.Mesocorticolimbiccircuitsareimpairedinchroniccocaineusersasdemonstratedbyresting-statefunctionalconnectivity.NeuroImage.2010;53(2):593-601.doi:10.1016/j.neuroimage.2010.06.066.
36
71. McHughMJ,DemersCH,SalmeronBJ,DevousMD,SteinEA,AdinoffB.Cortico-amygdalacouplingasamarkerofearlyrelapseriskincocaine-addictedindividuals.FrontPsychiatry.2014;5:16.doi:10.3389/fpsyt.2014.00016.
72. WisnerKM,PatzeltEH,LimKO,MacDonaldAW.Anintrinsicconnectivitynetworkapproachtoinsula-deriveddysfunctionsamongcocaineusers.AmJDrugAlcoholAbuse.2013;39(6):403-413.doi:10.3109/00952990.2013.848211.
73. KellyC,ZuoX-N,GotimerK,etal.Reducedinterhemisphericrestingstatefunctionalconnectivityincocaineaddiction.BiolPsychiatry.2011;69(7):684-692.doi:10.1016/j.biopsych.2010.11.022.
74. ConnollyCG,BellRP,FoxeJJ,GaravanH.Dissociatedgreymatterchangeswithprolongedaddictionandextendedabstinenceincocaineusers.PLoSONE.2013;8(3):e59645.doi:10.1371/journal.pone.0059645.
75. BellRP,FoxeJJ,RossLA,GaravanH.Intactinhibitorycontrolprocessesinabstinentdrugabusers(I):afunctionalneuroimagingstudyinformercocaineaddicts.Neuropharmacology.2014;82:143-150.doi:10.1016/j.neuropharm.2013.02.018.
37
WherecanIgetfurtherinformationaboutcocaine?
Tolearnmoreaboutcocaineandotherdrugsofabuse,visittheNIDAwebsiteatwww.drugabuse.govorcontactDrugPubsat877-NIDA-NIH(877-643-2644;TTY/TDD:240-645-0228).
NIDA'swebsiteincludes:
Informationondrugsofabuseandrelatedhealthconsequences
NIDApublications,news,andevents
Resourcesforhealthcareprofessionals,educators,andpatientsandfamilies
InformationonNIDAresearchstudiesandclinicaltrials
Fundinginformation(includingprogramannouncementsanddeadlines)
Internationalactivities
Linkstorelatedwebsites(accesstowebsitesofmanyotherorganizationsinthefield)
InformationinSpanish(enespañol)
NIDAwebsitesandwebpages
www.drugabuse.gov
www.teens.drugabuse.gov
www.easyread.drugabuse.gov
www.drugabuse.gov/drugs-abuse/cocaine
www.researchstudies.drugabuse.gov
www.irp.drugabuse.gov
38
Forphysicianinformation
NIDAMED:www.drugabuse.gov/nidamed
Otherwebsites
InformationoncocaineabuseisalsoavailablethroughthefollowingWebsite:
SubstanceAbuseandMentalHealthServicesAdministration:www.samhsa.gov
DrugEnforcementAdministration:www.dea.gov
MonitoringtheFuture:www.monitoringthefuture.org/
ThePartnershipatDrugFree.org:www.drugfree.org/drug-guide
ThispublicationisavailableforyouruseandmaybereproducedinitsentiretywithoutpermissionfromtheNIDA.Citationofthesourceisappreciated,usingthefollowinglanguage:Source:NationalInstituteonDrugAbuse;NationalInstitutesofHealth;U.S.DepartmentofHealthandHumanServices.