Embed Size (px)
Citation preview

Case SeriesNiemann-Pick Disease An Underdiagnosed LysosomalStorage Disorder
Inusha Panigrahi 1 Manoj Dhanorkar1 Renu Suthar1 Chanchal Kumar1
Mullai Baalaaji1 Babu Ram Thapa2 and Jasvinder Kalra 3
1Department of Pediatrics PGIMER Chandigarh India2Department of Gastroenterology PGIMER Chandigarh India3Department of Obstetrics and Gynecology PGIMER Chandigarh India
Correspondence should be addressed to Inusha Panigrahi inupanyahoocom
Received 26 February 2019 Accepted 20 March 2019 Published 21 April 2019
Academic Editor Balraj Mittal
Copyright copy 2019 Inusha Panigrahi et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Lysosomal storage disorders (LSDs) collectively constitute a significant public health burden in developing countries CommonerLSDs include Gaucher Fabry and Niemann-Pick disease (NPD) but many cases remain undiagnosed With the high incidenceof consanguineous marriages South East Asian countries are expected to have high prevalence of these LSDs Here we report4 cases of NPD type AB in 3 families presenting with hepatosplenomegaly and cytopenias including one family with two sibshaving hypertension and mitral valve prolapse The diagnosis of NPD was proven by mutation analysis with identification of novelmutations including a novel 4 bp insertion mutation (CgtCCTGG) in exon 2 of the SMPD1 gene We also had two cases of NPDtype C confirmed on mutation analysis
1 Introduction
High prevalence of LSDs has been reported from some SouthEast Asian populations [1ndash5] and Saudi Arabia possiblybecause of increased frequency of consanguineous matingsNiemann-Pick disease (NPD) is a lysosomal storage disor-der which presents with hepatosplenomegaly jaundice andcytopenia In the severe form of disease patient can presentearly with failure to thrive hepatosplenomegaly or pul-monary manifestations [6] The clinical manifestations havebeen classified into type A type B and type C disease presen-tations Mutations in types A and B are seen in SMPD1 genebut in type C disease are seen inNPC1 andNPC2 genes TypesA and B result from the deficient activity of sphingomyelinaseand the SMPD1 gene located on bands 11p151-p154 [7] andare referred to as acid sphingomyelinase deficiency (ASMD)The enzymatic defect results in pathologic accumulation ofsphingomyelin a ceramide phospholipid and other lipidsin the monocyte-macrophage system [8 9] Type A is mostsevere form of the disorder resulting in early death [10] In
many cases the diagnosis rests on identification of cherryred spots in fundus on ophthalmic evaluation or presence ofstorage cells in the bone marrow [11] The enzyme analysis isavailable only in selected laboratories for sphingomyelinaseand may not be accessible in all suspected cases For type Cdisease the diagnosis traditionally required a liver biopsy andfilipin staining Nowadays biomarker studies and moleculartesting for NPC1C2 genes have helped in better diagnosisSmall molecule therapy has been tried in NPD but furtherresearch is needed to devise better treatment modalities forthe disorder
This is a retrospective analysis of cases of Niemann-Pick disease detected on follow-up in Genetic Clinic of atertiary care centre Earlier bone marrow evaluation wasroutinely done for diagnosis of storage disorder of whichcommonest is Gaucher disease in patients presenting withhepatosplenomegaly and cytopenias Nowadays with betterexpertise and availability of good laboratory facilities some-times enzyme analysis is done upfront for diagnosis of storagedisorder
HindawiCase Reports in GeneticsVolume 2019 Article ID 3108093 5 pageshttpsdoiorg10115520193108093
2 Case Reports in Genetics
2 Case Presentation
In retrospective analysis of children undergoing bone mar-row evaluation for suspected storage disorder (Nov 1998-October 2008) we found oldest child of 12-year age (range1 month to 12 years) There were 21 were typical Gauchercells having cytoplasm with crumpledcrinkled tissue paperappearance and 27 were diagnosed as non-Gaucher storagedisorder Four cases with ASMD-Niemann-Pick disease typeAB and 2 cases ofNiemann-Pick disease typeC are describedbelow
Enzyme analysis was done by fluorimetric assay usingstandard protocols and use of control enzyme for increasingreliability of the result Normal value of acid sphingomyeli-nase taken was 10-32 nmolhrmg and chitotriosidase nor-mal level was 2866-6294 nmolmlhr Mutation analysis wasdone by Sanger sequencing or by next generation sequencing(NGS) with targeted analysis for storage disorder genes InSanger sequencing all the six exons were amplified andsequenced bidirectionally on ABI DNA Sequencer For NGS-Clinical Exome test 5000 genes were amplified using Illu-mina platforms and target genes were analysed by standardbioinformatics databases Consent for testing was takenfrom the parentscouple who came for genetic counseling ormolecular testing
In family 1 the 27-year-old female presented for antenatalcounseling in the fetal medicine clinic She had history of2 previous children who had expired in early childhoodwith seizures and hepatosplenomegaly The enzyme analysisdone in the second child was available and was consistentwith NPD The prenatal diagnosis was done on CVS samplewhich was borderline low (N range-72-210 nmolhrmg) andthe parents decided to continue the pregnancy Subsequentanalysis of SMPD1 gene was performed by Sanger sequenc-ing Two heterozygote mutations in the SMPD1 gene weredetected One was the R542 X mutation resulting fromC997888rarrT substitution at nucleotide position C1624 in exon 6 ofSMPD1TheothermutationwasC387F resulting fromG997888rarrTsubstitution at nucleotide position C1160 in exon 3 of SMPD1The mother carried the C387F mutation and the father hadthe R542X mutation The family was recalled and coun-seled accordingly The database search showed two knownmutations -R542X and mutation C387F or pCys287Phe inSMPD1
In family 2 the 5-month-old male child resident ofMuzaffarnagar UP state presented with episodic loose stoolsand progressive abdominal distension since birth Child wasborn at term with birth weight of 225 kg and no historyof neonatal encephalopathy Child was on top feeds sincebirth As the child was growing parents started noticingepisodic loose stools in child which was unrelated to thechanges in the type of feeds Parents also started noticingprogressive abdominal distension onset since first month oflife which was involving the whole abdomen This was notassociated with waxing and waning phenomenon unrelatedto feed and bowel habit not in form of isolated palpablemass in abdominal quadrant This time he presented with15-day history of fever associated with respiratory distressand irritability for last 2 days prior to admission no history
suggestive of jaundice high colored urine clay coloredstool seizure and bleeding manifestation In developmentalhistory he was having mild delay in motor and cognitionsectors He was born to third degree consanguineous couplewith no family history of similar illness At presentation tothe hospital he was having respiratory distress otherwisehemodynamically stable He was having coarse facies gradeII malnutrition according to IAP classification and severewasting according to WHO classification with small headHe also had firm hepatosplenomegaly liver of 4 cm belowright costal margin with span of 9 cm firm in consistencyand being with palpable left lobe Spleen was 3 cm alongsplenic axis below left costal margin Child had right sidedreducible inguinal On central nervous system examinationchild was found to have generalized hypotonia The possi-bilities considered were intrauterine infectionmetabolic orstorage disorder with acute presentation with communityacquired pneumonia Complete blood count was suggestiveof microcytic and hypochromic anemia with normal plateletsand leukocytosis Biochemical parameters were suggestive ofelevated transaminases-AST-229 and ALT-489 units Toxo-plasma and CMV serology were negative and HIV ELISAwas nonreactiveThe tubercular work-up includingMantouxtest and 3 gastric aspirates for AFB were negative Ultra-sound abdomen showed hepatosplenomegaly with normalechotexture of liver and normal kidneys and cranium Fundusexamination showed bilateral cherry red spots Radiologicalevaluation did not show any dysostosis in the spine andhand radiographs Bonemarrow examination revealed foamyvacuolated large sized macrophages with size of 25-30 timesthe size of mature lymphocytes or foam cells consistent withstorage disorder As per the next step of investigation enzymeanalysis was done for NPD which was suggestive of lowsphingomyelinase level Hence a diagnosis of Niemann-Pickdisease likely type A was made in the index child Howeverunfortunately child succumbed to an illness three monthslater at 8 months of age
The familywas initially counseled regarding enzyme anal-ysis on amniotic fluidHowever in the subsequent pregnancythey did not come for prenatal diagnosis and a girl child wasborn She was also similarly affected and expired due to anillness at 4 month of age The parents came to the geneticsclinic again after death of the second child DNA mutationanalysis was done for SMPD1 gene by Sanger sequencing andboth parents were heterozygous for the same 4 bp insertionmutation (CgtCCTGG) in exon 2 of the gene (Figure 1)
In family 3 a 9-year-old male child a case presentingwith short stature and hepatosplenomegaly with suspectedNPD type B homozygosity for a novel missense variantc1566TgtG in exon 6 of the SMPD1 gene was NGS andconfirmed by bidirectional Sanger sequencing He had hep-atosplenomegaly and recurrent respiratory problems Themale child was admitted in pediatric ICU for left focalmotor seizures and also had features of acute on chronicmalnutrition facial dysmorphism (mild coarse facies promi-nent ears) and large hepatosplenomegaly and hypertensiverecords at admission Otherwise his neurological examina-tion was essentially normal MRI brain done was suggestiveof T2 hyperintensities in left side of pons and medulla
Case Reports in Genetics 3
GAAAGGAAGGAGCCTGATTGTTTG
380
470 480
SMPD1exon2 -MUTATION CONTEXT
CTTGGGAGCCCTGGCTGGCTGCCT370
GGAGCCCTGGCT
GGAGCCCTGGCTGGCT
Figure 1 Representation of the novel 4 bp insertion mutation inSMPD1 gene in exon 2 in family 2 in parental sample
with patchy contrast enhancement He also had hypertensiveemergency during hospital stay with seizure pulmonaryedema and grade 4 hypertensive changes in retinal vesselsand nonoliguric acute kidney injury which responded topharmacological management He subsequently developedpancytopenia coagulopathy and sudden onset hypotensiveshock nonresponsive to fluid bolus and dopamine infusionand succumbed to the illness His enzyme assay revealednormal beta-glucosidase level for Gaucher disease and a lowlevel of sphingomyelinase consistent with NPD
His older sibling had similar features and was admittedin PGE ward at 12 years of age with periorbital puffinessaround 8 months earlier and had expired in hospital Shehad wasting and stunting hypertension encephalopathyseizures and shock Ultrasonography of abdomen showedliver of 21 cm normal echotexture normal outline and adistended gall bladder spleen of 22 cm normal echotextureand normal kidneys Echocardiography revealed mitral valvemildly thickened with prolapse of postmitral leaflet moder-ate mitral regurgitation and eccentric jet anteriorly directedand normal left ventricular ejection fraction The parentswere tested by Sanger sequencing of SMPD1 gene and wereheterozygous for the identified variant in child and werecounseled accordingly for future pregnancies
In family 4 a female child was brought with regression ofmilestones from 2 12-year age She had history of neonatalcholestasis At 4-year age she presented with fever andrespiratory complaints Examination revealed microcephalygrowth failure hepatosplenomegaly and upward gaze restric-tion Fundus examination did not show any cherry redspot and X-rays did not reveal any dysostosis Keepinga possibility of Niemann-Pick disease a sphingomyelinaseassay was done which showed normal sphingomyelinaseenzyme in the blood lymphocytes However further testingby targeted DNA analysis was done for storage disordersby next generation sequencing (NGS) and two variants inNPC1 gene were identified One was an exon 3 variant c275AgtG (pGln92Arg) and an exon 22 variant c3246 TgtA(pSer1082Arg) confirming diagnosis of NPD type C Thefamily was counseled for subsequent prenatal diagnosis
Family 5 A 9-month male child presented with devel-opmental delay respiratory problems failure to gain weightHe was born full term by LSCS (indicationoligohydramnios)with birth weight of 22 kg He had jaundice on day 2 of liferequiring phototherapy for 3 days From 4 months age he
developed on and off cough without significant fever Locallyhe was admitted for 2 months and given antibiotics andoxygen For positive CMV IgM he received also ganciclovirfor 2 weeks Thereafter he developed increasing respira-tory distress and perioral cyanosis Examination revealedlengthheight of 56 cm (-085 Z score) and head circum-ference of 375 cm (-183 Z score) and hepatosplenomegalyThe liver was 4 cm below RCM and 5 cm below the xiphoidspleen was 4 cm below LCM with notch present He hadhypotonia with scarf sign crossing midline He had anemiaduring hospital stay but X-rays did not show any dysostosisChest X-ray was suggestive of interstitial pneumonia andCECT chest revealed multifocal areas of patchy consolidationwith ground glass opacity and reduced volume of thymusThe transaminases levels were 191 and 133 UL with normalserum creatinine Stool for fat globules were 30-40HPF andflow cytometry for chronic granulomatous disease (CGD)was negative Keeping a clinical diagnosis of Niemann-Pickdisease enzyme analysis was performed which showed nor-mal sphingomyelinase level-18 units (N-18-85 nmolhrmgprotein) However chitotriosidase was elevated (2041 units)above normal values (287-63 nmolmlhr) and bone marrowshowed scattered histiocytes with eccentric nuclei and mul-tivacuolated cytoplasm suggestive of non-Gaucher storagedisorder Thus NPC was not ruled out Vit D level was lowand he was given replacement therapy Further DNA testingwas done by targeted NGS and identified homozygosity foran insertion variant in NPC2 gene c82 +2 -gtG which wasfound to affect splicing on bioinformatics analysis Geneticcounseling was done and feasibility of prenatal diagnosis wasdiscussed
3 Discussion
Mucopolysaccharidosis disorders and Gaucher disease arecommoner lysosomal storage disorders (LSDs) Recently sph-ingolipidoses have been reported to be common metabolicdisorders from Saudi Arabia [12] Early diagnosis and earlyinitiation of treatment including enzyme replacement ther-apy (ERT) in selected disorders can enable the affected chil-dren to have near normal life Because of the variable clinicalpresentation and limited availability of diagnostic testingthese disorders are missed out during routine evaluation InNiemann-Pick disease (NPD) the incidence for carrier of thegene-SMPD1 causing ASMD is 1120 in the general popula-tion and increases to 160 for individuals of Ashkenazi Jewishdescent [13] NPD type A disease manifests with persistentearly jaundice enlarging abdomen hepatosplenomegaly andpoor developmental progress and failure to thrive [10] Deathusually occurs by 3 years of age
In a Nepalese boy 13-year-old presenting with gait abnor-malities and supranuclear gaze palsy bone marrow revealedabundant foamy cytoplasm suggestive of storage disorderMutation analysis revealed two variants in the NPC1 genec302TgtG F101C in exon 4 and another IVS 24+1GgtA muta-tion [14] This confirmed the diagnosis of NPC NPD type Coften present with prolonged neonatal jaundice may remainnormal for 1-2 years ultimately leading to slowly progressiveand variable neurodegenerative course Hepatosplenomegaly
4 Case Reports in Genetics
in type C is less severe than type A or B and they maysurvive into adulthoodThe underlying biochemical defect intype C is abnormal cholesterol transport which leads to sph-ingomyelin and cholesterol accumulation in the lysosomesand a secondary partial reduction in acid sphingomyelinaseactivity NPC1 and NPC2 are the genes underlying NPD typeC Few cases of NPC are reported compared to NPD [15ndash17] In present study we found one case with NPC1 witha likely deleterious variant in homozygous state She hadhepatosplenomegaly and gaze palsy and presented at 4 yearsof age A high index of suspicion is needed for the diagnosisSometimes it is difficult to do filipin staining in hepatic cellsby biopsy but increased level of chitotriosidase as a surrogatemarker helps in giving a clue to underlying diagnosisChitotriosidase is more elevated especially in ASMD casesthan in NPC cases Mutation studies are now available forNPC and can be done in individual cases However if VUSis identified pathogenicity confirmation can only be donewhen another similar case is reported in another family In themale infant with respiratory problems we found an insertionmutation in the NPC2 gene Lung involvement is a dominantfeature in NPD and this may also lead to persistent oxygenrequirement
Small deletions or nonsensemutations in the SMPD1 geneusually lead to NPD type A whereas missense mutationsthat produce a defective enzyme cause a milder NPD typeB phenotype [15 18] ] Levran et al identified single basedeletion in Ashkenazi Jews causing the pro330FS mutationcausing a frameshift leading to premature chain termination[7] Most (65) SMPD1 mutations are accounted for bythree mutations R496L L302P and pro330FS mutation inAshkenazi Jewish NPD cases
In the family 2 we found a 4 bp insertion variation(CgtCCTGG) in exon 2 leading to a premature stop codonThismutation is 35 amino acids from the amino acid position355 in the SMPD1 gene On database analysis this mutationwas predicted to disrupt protein function Family 3 alsoshowed novel missense variant c1566TgtG in exon 6 ofthe SMPD1 gene identified on NGS This was predictedto be deleterious on analysis in available mutation specificdatabases and not reported in general population
In family 3 the siblings showed growth retardationhypertension and mitral valve prolapse in addition to hep-atosplenomegaly Cardiomyopathy and MVP are commonlyreported in mucopolysaccharidoses but can also be seenin NPD Mutation analysis also showed novel missensemutation in this family in exon 6 of SMPD1 gene
Various treatment modalities tried with no or littlesuccess are orthotopic liver transplantation in type A andcord blood transplantation in several type B A phase Itrial of enzyme replacement therapy for type B has beencompleted Clinical trials of the drug Miglustat (substratereduction therapy SRT) have been performed and the drughas been approved in Europe for the treatment of type Cdisease [6] SRT has emerged as promising form of treatmentas single therapy or in addition to ERT for ASMD Olipudasealfa is the recombinant enzyme the human acid sphin-gomyelinase which has been found beneficial in treatment ofASMD [19] There are only mild adverse events like nausea
abdominal pain and headache and no severe reactions werereported
Chitotriosidase is a surrogate marker for diagnosis ofGaucher and Niemann-Pick disease and is significantlyincreased in these disorders However 6 of the populationis deficient for chitotriosidase protein In case the enzymelevels are inconclusive the further mutation analysis cangive a confirmatory diagnosis New biomarkers are beingdeveloped to make diagnosis easier One of these is plasmalysosphingomyelin which can of potential use in diagnosis ofNiemann-Pick type B and also NPC [20 21] Recently bileacid B has also been found to detect NPC1 related diseaseon newborn dried blood spots [22] Chitotriosidase andlysosphingomyelin levels have also been found to be helpfulinmonitoring response to therapy [19] Recent research is alsoon to find new therapeutic options for NPC and one of thestudied molecules is 6-O-120572-maltosyl-120573-cyclodextrin (G2-120573-CD) in treatment ofNPC1disease [23] Promising results havebeen demonstrated in NPC1 deficient mice models
In countries like India and nearby South Asian countrieswith low GDP the numbers of diagnosed cases actuallyrepresent a minority of the actual number of cases in view ofthe large population base There is discrepancy in resourcesand availability of diagnosis and treatment facilities for raredisorders [2 3] NPD also present with nonimmune hydropsfetalis (NIHF) and should be considered in pregnancies withrecurrent hydrops The availability of enzyme analysis andmutation analysis has made early prenatal diagnosis of NPDpossible in selected families at risk of child with severe NPDThere is also a need to increase awareness regarding earlydiagnosis of these disorders Till the treatment of NPD ismade widely available the focus lies on timely detection ofindex child with NPD and provision of genetic counselingand planned prenatal diagnosis in some families
Additional Points
KeyMessage Niemann-Pick disease can have variable clinicalpresentations and suspicion is the key to early diagnosis Highincidence is expected in South East Asia region A completeevaluation including DNA analysis can help in reaching anappropriate diagnosis
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] I C Verma and D Kumar ldquoEpidemiology of genetic diseasesrdquoin Genetic Disorders of the Indian Subcontinent D Kumar Edpp 81ndash87 Springer Dordrecht Netherlands 2004
[2] J Sheth M Mistri F Sheth et al ldquoBurden of lysosomal storagedisorders in India experience of 387 affected children from asingle diagnostic facilityrdquo JIMD Reports vol 12 pp 51ndash63 2014
[3] X Chen W Qiu J Ye L Han X Gu and H ZhangldquoDemographic characteristics and distribution of lysosomalstorage disorder subtypes in Eastern Chinardquo Journal of HumanGenetics vol 61 no 4 pp 345ndash349 2016
Case Reports in Genetics 5
[4] J Sheth R Bhavsar M Mistri et al ldquoGaucher disease sin-gle gene molecular characterization of one-hundred Indianpatients reveals novel variants and the most prevalent muta-tionrdquo BMC Medical Genetics vol 20 no 1 p 31 2019
[5] P J Meikle J J Hopwood A E Clague and W F CareyldquoPrevalence of lysosomal storage disordersrdquo Journal of theAmericanMedical Association vol 281 no 3 pp 249ndash254 1999
[6] R M Kliegman B M D Stanton J S Geme and N F SchorNelson Textbook of Pediatrics Elsevier Health Sciences 2015
[7] O Levran R J Desnick and E H Schuchman ldquoType A Nie-mann-Pick disease A frameshift mutation in the acid sphingo-myelinase gene (fsP330) occurs in Ashkenazi Jewish patientsrdquoHuman Mutation vol 2 no 4 pp 317ndash319 1993
[8] R W Jenkins D Canals and Y A Hannun ldquoRoles andregulation of secretory and lysosomal acid sphingomyelinaserdquoCellular Signalling vol 21 no 6 pp 836ndash846 2009
[9] P G Camoletto H Vara L Morando et al ldquoSynaptic vesi-cle docking Sphingosine regulates syntaxin1 interaction withMunc18rdquo PLoS ONE vol 4 no 4 Article ID e5310 2009
[10] J Aicardi M Bax and C Gillberg Diseases of the NervousSystem in Childhood Mac Keith Press London UK 2009
[11] Y-U Cho J D ChaeW M Lee et al ldquoA case of a Korean adultaffected by type B Niemann-Pick disease Secondary sea-bluehistiocytosis andmolecular characterizationrdquoKorean Journal ofLaboratory Medicine vol 29 no 2 pp 97ndash103 2009
[12] M Alfadhel M Benmeakel M A Hossain et al ldquoThirteenyear retrospective review of the spectrum of inborn errors ofmetabolism presenting in a tertiary center in Saudi ArabiardquoOrphanet Journal of Rare Diseases vol 11 no 1 p 126 2016
[13] S R Pupecki Focus on Genetic Screening Research NovaScience Publishers 2006
[14] P Jain S Sharma P Poudel J Reunert T Marquardt and SAneja ldquoNiemann-Pick type C disease in a 13-year-old boy fromNepal a genetically confirmed caserdquo Neurology India vol 63no 4 pp 626ndash628 2015
[15] H Ida O M Rennert K Maekawa and Y Eto ldquoIdentificationof three novel mutations in the acid sphingomyelinase gene ofJapanese patients with Niemann-Pick disease type A and BrdquoHuman Mutation vol 7 no 1 pp 65ndash67 1996
[16] J Sheth J J Joseph K Shah M Muranjan M Mistri andF Sheth ldquoPulmonary manifestations in Niemann-Pick type Cdisease with mutations in NPC2 gene case report and review ofliteraturerdquo BMC Medical Genetics vol 18 no 1 p 5 2017
[17] M Hebbar H Prasada L A D Bhowmik et al ldquoHomozygousdeletion of exons 2 and 3 of NPC2 associated with Niemann-Pick disease type Crdquo American Journal of Medical Genetics PartA vol 170 no 9 pp 2486ndash2489 2016
[18] T Takahashi M Suchi R J Desnick G Takada and E HSchuchman ldquoIdentification and expression of five mutations inthe human acid sphingomyelinase gene causing types A and BNiemann-Pick disease Molecular evidence for genetic heter-ogeneity in the neuronopathic and non-neuronopathic formsrdquoThe Journal of Biological Chemistry vol 267 no 18 pp 12552ndash12558 1992
[19] M PWassersteinG ADiaz R H Lachmann et al ldquoOlipudasealfa for treatment of acid sphingomyelinase deficiency (ASMD)safety and efficacy in adults treated for 30 monthsrdquo Journal ofInherited Metabolic Disease vol 41 no 5 pp 829ndash838 2018
[20] R W D Welford M Garzotti C M Lourenco et al ldquoPlasmalysosphingomyelin demonstrates great potential as a diagnosticbiomarker for niemann-pick disease type C in a retrospectivestudyrdquo PLoS ONE vol 9 no 12 Article ID e114669 2014
[21] W-L Chuang J Pacheco S Cooper et al ldquoLyso-sphingomyelinis elevated in dried blood spots of Niemann-Pick B patientsrdquoMolecular Genetics and Metabolism vol 111 no 2 pp 209ndash2112014
[22] X Jiang R Sidhu J J Orsini et al ldquoDiagnosis of niemann-pickC1 by measurement of bile acid biomarkers in archived new-born dried blood spotsrdquo Molecular Genetics and Metabolismvol 126 no 2 pp 183ndash187 2019
[23] N Yasmin Y Ishitsuka M Fukaura et al ldquoIn vitro and invivo evaluation of 6-O-120572-maltosyl-120573-cyclodextrin as a potentialtherapeutic agent against niemann-pick disease type Crdquo Inter-national Journal of Molecular Sciences vol 20 no 5 Article IDE1152 2019
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

2 Case Reports in Genetics
2 Case Presentation
In retrospective analysis of children undergoing bone mar-row evaluation for suspected storage disorder (Nov 1998-October 2008) we found oldest child of 12-year age (range1 month to 12 years) There were 21 were typical Gauchercells having cytoplasm with crumpledcrinkled tissue paperappearance and 27 were diagnosed as non-Gaucher storagedisorder Four cases with ASMD-Niemann-Pick disease typeAB and 2 cases ofNiemann-Pick disease typeC are describedbelow
Enzyme analysis was done by fluorimetric assay usingstandard protocols and use of control enzyme for increasingreliability of the result Normal value of acid sphingomyeli-nase taken was 10-32 nmolhrmg and chitotriosidase nor-mal level was 2866-6294 nmolmlhr Mutation analysis wasdone by Sanger sequencing or by next generation sequencing(NGS) with targeted analysis for storage disorder genes InSanger sequencing all the six exons were amplified andsequenced bidirectionally on ABI DNA Sequencer For NGS-Clinical Exome test 5000 genes were amplified using Illu-mina platforms and target genes were analysed by standardbioinformatics databases Consent for testing was takenfrom the parentscouple who came for genetic counseling ormolecular testing
In family 1 the 27-year-old female presented for antenatalcounseling in the fetal medicine clinic She had history of2 previous children who had expired in early childhoodwith seizures and hepatosplenomegaly The enzyme analysisdone in the second child was available and was consistentwith NPD The prenatal diagnosis was done on CVS samplewhich was borderline low (N range-72-210 nmolhrmg) andthe parents decided to continue the pregnancy Subsequentanalysis of SMPD1 gene was performed by Sanger sequenc-ing Two heterozygote mutations in the SMPD1 gene weredetected One was the R542 X mutation resulting fromC997888rarrT substitution at nucleotide position C1624 in exon 6 ofSMPD1TheothermutationwasC387F resulting fromG997888rarrTsubstitution at nucleotide position C1160 in exon 3 of SMPD1The mother carried the C387F mutation and the father hadthe R542X mutation The family was recalled and coun-seled accordingly The database search showed two knownmutations -R542X and mutation C387F or pCys287Phe inSMPD1
In family 2 the 5-month-old male child resident ofMuzaffarnagar UP state presented with episodic loose stoolsand progressive abdominal distension since birth Child wasborn at term with birth weight of 225 kg and no historyof neonatal encephalopathy Child was on top feeds sincebirth As the child was growing parents started noticingepisodic loose stools in child which was unrelated to thechanges in the type of feeds Parents also started noticingprogressive abdominal distension onset since first month oflife which was involving the whole abdomen This was notassociated with waxing and waning phenomenon unrelatedto feed and bowel habit not in form of isolated palpablemass in abdominal quadrant This time he presented with15-day history of fever associated with respiratory distressand irritability for last 2 days prior to admission no history
suggestive of jaundice high colored urine clay coloredstool seizure and bleeding manifestation In developmentalhistory he was having mild delay in motor and cognitionsectors He was born to third degree consanguineous couplewith no family history of similar illness At presentation tothe hospital he was having respiratory distress otherwisehemodynamically stable He was having coarse facies gradeII malnutrition according to IAP classification and severewasting according to WHO classification with small headHe also had firm hepatosplenomegaly liver of 4 cm belowright costal margin with span of 9 cm firm in consistencyand being with palpable left lobe Spleen was 3 cm alongsplenic axis below left costal margin Child had right sidedreducible inguinal On central nervous system examinationchild was found to have generalized hypotonia The possi-bilities considered were intrauterine infectionmetabolic orstorage disorder with acute presentation with communityacquired pneumonia Complete blood count was suggestiveof microcytic and hypochromic anemia with normal plateletsand leukocytosis Biochemical parameters were suggestive ofelevated transaminases-AST-229 and ALT-489 units Toxo-plasma and CMV serology were negative and HIV ELISAwas nonreactiveThe tubercular work-up includingMantouxtest and 3 gastric aspirates for AFB were negative Ultra-sound abdomen showed hepatosplenomegaly with normalechotexture of liver and normal kidneys and cranium Fundusexamination showed bilateral cherry red spots Radiologicalevaluation did not show any dysostosis in the spine andhand radiographs Bonemarrow examination revealed foamyvacuolated large sized macrophages with size of 25-30 timesthe size of mature lymphocytes or foam cells consistent withstorage disorder As per the next step of investigation enzymeanalysis was done for NPD which was suggestive of lowsphingomyelinase level Hence a diagnosis of Niemann-Pickdisease likely type A was made in the index child Howeverunfortunately child succumbed to an illness three monthslater at 8 months of age
The familywas initially counseled regarding enzyme anal-ysis on amniotic fluidHowever in the subsequent pregnancythey did not come for prenatal diagnosis and a girl child wasborn She was also similarly affected and expired due to anillness at 4 month of age The parents came to the geneticsclinic again after death of the second child DNA mutationanalysis was done for SMPD1 gene by Sanger sequencing andboth parents were heterozygous for the same 4 bp insertionmutation (CgtCCTGG) in exon 2 of the gene (Figure 1)
In family 3 a 9-year-old male child a case presentingwith short stature and hepatosplenomegaly with suspectedNPD type B homozygosity for a novel missense variantc1566TgtG in exon 6 of the SMPD1 gene was NGS andconfirmed by bidirectional Sanger sequencing He had hep-atosplenomegaly and recurrent respiratory problems Themale child was admitted in pediatric ICU for left focalmotor seizures and also had features of acute on chronicmalnutrition facial dysmorphism (mild coarse facies promi-nent ears) and large hepatosplenomegaly and hypertensiverecords at admission Otherwise his neurological examina-tion was essentially normal MRI brain done was suggestiveof T2 hyperintensities in left side of pons and medulla
Case Reports in Genetics 3
GAAAGGAAGGAGCCTGATTGTTTG
380
470 480
SMPD1exon2 -MUTATION CONTEXT
CTTGGGAGCCCTGGCTGGCTGCCT370
GGAGCCCTGGCT
GGAGCCCTGGCTGGCT
Figure 1 Representation of the novel 4 bp insertion mutation inSMPD1 gene in exon 2 in family 2 in parental sample
with patchy contrast enhancement He also had hypertensiveemergency during hospital stay with seizure pulmonaryedema and grade 4 hypertensive changes in retinal vesselsand nonoliguric acute kidney injury which responded topharmacological management He subsequently developedpancytopenia coagulopathy and sudden onset hypotensiveshock nonresponsive to fluid bolus and dopamine infusionand succumbed to the illness His enzyme assay revealednormal beta-glucosidase level for Gaucher disease and a lowlevel of sphingomyelinase consistent with NPD
His older sibling had similar features and was admittedin PGE ward at 12 years of age with periorbital puffinessaround 8 months earlier and had expired in hospital Shehad wasting and stunting hypertension encephalopathyseizures and shock Ultrasonography of abdomen showedliver of 21 cm normal echotexture normal outline and adistended gall bladder spleen of 22 cm normal echotextureand normal kidneys Echocardiography revealed mitral valvemildly thickened with prolapse of postmitral leaflet moder-ate mitral regurgitation and eccentric jet anteriorly directedand normal left ventricular ejection fraction The parentswere tested by Sanger sequencing of SMPD1 gene and wereheterozygous for the identified variant in child and werecounseled accordingly for future pregnancies
In family 4 a female child was brought with regression ofmilestones from 2 12-year age She had history of neonatalcholestasis At 4-year age she presented with fever andrespiratory complaints Examination revealed microcephalygrowth failure hepatosplenomegaly and upward gaze restric-tion Fundus examination did not show any cherry redspot and X-rays did not reveal any dysostosis Keepinga possibility of Niemann-Pick disease a sphingomyelinaseassay was done which showed normal sphingomyelinaseenzyme in the blood lymphocytes However further testingby targeted DNA analysis was done for storage disordersby next generation sequencing (NGS) and two variants inNPC1 gene were identified One was an exon 3 variant c275AgtG (pGln92Arg) and an exon 22 variant c3246 TgtA(pSer1082Arg) confirming diagnosis of NPD type C Thefamily was counseled for subsequent prenatal diagnosis
Family 5 A 9-month male child presented with devel-opmental delay respiratory problems failure to gain weightHe was born full term by LSCS (indicationoligohydramnios)with birth weight of 22 kg He had jaundice on day 2 of liferequiring phototherapy for 3 days From 4 months age he
developed on and off cough without significant fever Locallyhe was admitted for 2 months and given antibiotics andoxygen For positive CMV IgM he received also ganciclovirfor 2 weeks Thereafter he developed increasing respira-tory distress and perioral cyanosis Examination revealedlengthheight of 56 cm (-085 Z score) and head circum-ference of 375 cm (-183 Z score) and hepatosplenomegalyThe liver was 4 cm below RCM and 5 cm below the xiphoidspleen was 4 cm below LCM with notch present He hadhypotonia with scarf sign crossing midline He had anemiaduring hospital stay but X-rays did not show any dysostosisChest X-ray was suggestive of interstitial pneumonia andCECT chest revealed multifocal areas of patchy consolidationwith ground glass opacity and reduced volume of thymusThe transaminases levels were 191 and 133 UL with normalserum creatinine Stool for fat globules were 30-40HPF andflow cytometry for chronic granulomatous disease (CGD)was negative Keeping a clinical diagnosis of Niemann-Pickdisease enzyme analysis was performed which showed nor-mal sphingomyelinase level-18 units (N-18-85 nmolhrmgprotein) However chitotriosidase was elevated (2041 units)above normal values (287-63 nmolmlhr) and bone marrowshowed scattered histiocytes with eccentric nuclei and mul-tivacuolated cytoplasm suggestive of non-Gaucher storagedisorder Thus NPC was not ruled out Vit D level was lowand he was given replacement therapy Further DNA testingwas done by targeted NGS and identified homozygosity foran insertion variant in NPC2 gene c82 +2 -gtG which wasfound to affect splicing on bioinformatics analysis Geneticcounseling was done and feasibility of prenatal diagnosis wasdiscussed
3 Discussion
Mucopolysaccharidosis disorders and Gaucher disease arecommoner lysosomal storage disorders (LSDs) Recently sph-ingolipidoses have been reported to be common metabolicdisorders from Saudi Arabia [12] Early diagnosis and earlyinitiation of treatment including enzyme replacement ther-apy (ERT) in selected disorders can enable the affected chil-dren to have near normal life Because of the variable clinicalpresentation and limited availability of diagnostic testingthese disorders are missed out during routine evaluation InNiemann-Pick disease (NPD) the incidence for carrier of thegene-SMPD1 causing ASMD is 1120 in the general popula-tion and increases to 160 for individuals of Ashkenazi Jewishdescent [13] NPD type A disease manifests with persistentearly jaundice enlarging abdomen hepatosplenomegaly andpoor developmental progress and failure to thrive [10] Deathusually occurs by 3 years of age
In a Nepalese boy 13-year-old presenting with gait abnor-malities and supranuclear gaze palsy bone marrow revealedabundant foamy cytoplasm suggestive of storage disorderMutation analysis revealed two variants in the NPC1 genec302TgtG F101C in exon 4 and another IVS 24+1GgtA muta-tion [14] This confirmed the diagnosis of NPC NPD type Coften present with prolonged neonatal jaundice may remainnormal for 1-2 years ultimately leading to slowly progressiveand variable neurodegenerative course Hepatosplenomegaly
4 Case Reports in Genetics
in type C is less severe than type A or B and they maysurvive into adulthoodThe underlying biochemical defect intype C is abnormal cholesterol transport which leads to sph-ingomyelin and cholesterol accumulation in the lysosomesand a secondary partial reduction in acid sphingomyelinaseactivity NPC1 and NPC2 are the genes underlying NPD typeC Few cases of NPC are reported compared to NPD [15ndash17] In present study we found one case with NPC1 witha likely deleterious variant in homozygous state She hadhepatosplenomegaly and gaze palsy and presented at 4 yearsof age A high index of suspicion is needed for the diagnosisSometimes it is difficult to do filipin staining in hepatic cellsby biopsy but increased level of chitotriosidase as a surrogatemarker helps in giving a clue to underlying diagnosisChitotriosidase is more elevated especially in ASMD casesthan in NPC cases Mutation studies are now available forNPC and can be done in individual cases However if VUSis identified pathogenicity confirmation can only be donewhen another similar case is reported in another family In themale infant with respiratory problems we found an insertionmutation in the NPC2 gene Lung involvement is a dominantfeature in NPD and this may also lead to persistent oxygenrequirement
Small deletions or nonsensemutations in the SMPD1 geneusually lead to NPD type A whereas missense mutationsthat produce a defective enzyme cause a milder NPD typeB phenotype [15 18] ] Levran et al identified single basedeletion in Ashkenazi Jews causing the pro330FS mutationcausing a frameshift leading to premature chain termination[7] Most (65) SMPD1 mutations are accounted for bythree mutations R496L L302P and pro330FS mutation inAshkenazi Jewish NPD cases
In the family 2 we found a 4 bp insertion variation(CgtCCTGG) in exon 2 leading to a premature stop codonThismutation is 35 amino acids from the amino acid position355 in the SMPD1 gene On database analysis this mutationwas predicted to disrupt protein function Family 3 alsoshowed novel missense variant c1566TgtG in exon 6 ofthe SMPD1 gene identified on NGS This was predictedto be deleterious on analysis in available mutation specificdatabases and not reported in general population
In family 3 the siblings showed growth retardationhypertension and mitral valve prolapse in addition to hep-atosplenomegaly Cardiomyopathy and MVP are commonlyreported in mucopolysaccharidoses but can also be seenin NPD Mutation analysis also showed novel missensemutation in this family in exon 6 of SMPD1 gene
Various treatment modalities tried with no or littlesuccess are orthotopic liver transplantation in type A andcord blood transplantation in several type B A phase Itrial of enzyme replacement therapy for type B has beencompleted Clinical trials of the drug Miglustat (substratereduction therapy SRT) have been performed and the drughas been approved in Europe for the treatment of type Cdisease [6] SRT has emerged as promising form of treatmentas single therapy or in addition to ERT for ASMD Olipudasealfa is the recombinant enzyme the human acid sphin-gomyelinase which has been found beneficial in treatment ofASMD [19] There are only mild adverse events like nausea
abdominal pain and headache and no severe reactions werereported
Chitotriosidase is a surrogate marker for diagnosis ofGaucher and Niemann-Pick disease and is significantlyincreased in these disorders However 6 of the populationis deficient for chitotriosidase protein In case the enzymelevels are inconclusive the further mutation analysis cangive a confirmatory diagnosis New biomarkers are beingdeveloped to make diagnosis easier One of these is plasmalysosphingomyelin which can of potential use in diagnosis ofNiemann-Pick type B and also NPC [20 21] Recently bileacid B has also been found to detect NPC1 related diseaseon newborn dried blood spots [22] Chitotriosidase andlysosphingomyelin levels have also been found to be helpfulinmonitoring response to therapy [19] Recent research is alsoon to find new therapeutic options for NPC and one of thestudied molecules is 6-O-120572-maltosyl-120573-cyclodextrin (G2-120573-CD) in treatment ofNPC1disease [23] Promising results havebeen demonstrated in NPC1 deficient mice models
In countries like India and nearby South Asian countrieswith low GDP the numbers of diagnosed cases actuallyrepresent a minority of the actual number of cases in view ofthe large population base There is discrepancy in resourcesand availability of diagnosis and treatment facilities for raredisorders [2 3] NPD also present with nonimmune hydropsfetalis (NIHF) and should be considered in pregnancies withrecurrent hydrops The availability of enzyme analysis andmutation analysis has made early prenatal diagnosis of NPDpossible in selected families at risk of child with severe NPDThere is also a need to increase awareness regarding earlydiagnosis of these disorders Till the treatment of NPD ismade widely available the focus lies on timely detection ofindex child with NPD and provision of genetic counselingand planned prenatal diagnosis in some families
Additional Points
KeyMessage Niemann-Pick disease can have variable clinicalpresentations and suspicion is the key to early diagnosis Highincidence is expected in South East Asia region A completeevaluation including DNA analysis can help in reaching anappropriate diagnosis
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] I C Verma and D Kumar ldquoEpidemiology of genetic diseasesrdquoin Genetic Disorders of the Indian Subcontinent D Kumar Edpp 81ndash87 Springer Dordrecht Netherlands 2004
[2] J Sheth M Mistri F Sheth et al ldquoBurden of lysosomal storagedisorders in India experience of 387 affected children from asingle diagnostic facilityrdquo JIMD Reports vol 12 pp 51ndash63 2014
[3] X Chen W Qiu J Ye L Han X Gu and H ZhangldquoDemographic characteristics and distribution of lysosomalstorage disorder subtypes in Eastern Chinardquo Journal of HumanGenetics vol 61 no 4 pp 345ndash349 2016
Case Reports in Genetics 5
[4] J Sheth R Bhavsar M Mistri et al ldquoGaucher disease sin-gle gene molecular characterization of one-hundred Indianpatients reveals novel variants and the most prevalent muta-tionrdquo BMC Medical Genetics vol 20 no 1 p 31 2019
[5] P J Meikle J J Hopwood A E Clague and W F CareyldquoPrevalence of lysosomal storage disordersrdquo Journal of theAmericanMedical Association vol 281 no 3 pp 249ndash254 1999
[6] R M Kliegman B M D Stanton J S Geme and N F SchorNelson Textbook of Pediatrics Elsevier Health Sciences 2015
[7] O Levran R J Desnick and E H Schuchman ldquoType A Nie-mann-Pick disease A frameshift mutation in the acid sphingo-myelinase gene (fsP330) occurs in Ashkenazi Jewish patientsrdquoHuman Mutation vol 2 no 4 pp 317ndash319 1993
[8] R W Jenkins D Canals and Y A Hannun ldquoRoles andregulation of secretory and lysosomal acid sphingomyelinaserdquoCellular Signalling vol 21 no 6 pp 836ndash846 2009
[9] P G Camoletto H Vara L Morando et al ldquoSynaptic vesi-cle docking Sphingosine regulates syntaxin1 interaction withMunc18rdquo PLoS ONE vol 4 no 4 Article ID e5310 2009
[10] J Aicardi M Bax and C Gillberg Diseases of the NervousSystem in Childhood Mac Keith Press London UK 2009
[11] Y-U Cho J D ChaeW M Lee et al ldquoA case of a Korean adultaffected by type B Niemann-Pick disease Secondary sea-bluehistiocytosis andmolecular characterizationrdquoKorean Journal ofLaboratory Medicine vol 29 no 2 pp 97ndash103 2009
[12] M Alfadhel M Benmeakel M A Hossain et al ldquoThirteenyear retrospective review of the spectrum of inborn errors ofmetabolism presenting in a tertiary center in Saudi ArabiardquoOrphanet Journal of Rare Diseases vol 11 no 1 p 126 2016
[13] S R Pupecki Focus on Genetic Screening Research NovaScience Publishers 2006
[14] P Jain S Sharma P Poudel J Reunert T Marquardt and SAneja ldquoNiemann-Pick type C disease in a 13-year-old boy fromNepal a genetically confirmed caserdquo Neurology India vol 63no 4 pp 626ndash628 2015
[15] H Ida O M Rennert K Maekawa and Y Eto ldquoIdentificationof three novel mutations in the acid sphingomyelinase gene ofJapanese patients with Niemann-Pick disease type A and BrdquoHuman Mutation vol 7 no 1 pp 65ndash67 1996
[16] J Sheth J J Joseph K Shah M Muranjan M Mistri andF Sheth ldquoPulmonary manifestations in Niemann-Pick type Cdisease with mutations in NPC2 gene case report and review ofliteraturerdquo BMC Medical Genetics vol 18 no 1 p 5 2017
[17] M Hebbar H Prasada L A D Bhowmik et al ldquoHomozygousdeletion of exons 2 and 3 of NPC2 associated with Niemann-Pick disease type Crdquo American Journal of Medical Genetics PartA vol 170 no 9 pp 2486ndash2489 2016
[18] T Takahashi M Suchi R J Desnick G Takada and E HSchuchman ldquoIdentification and expression of five mutations inthe human acid sphingomyelinase gene causing types A and BNiemann-Pick disease Molecular evidence for genetic heter-ogeneity in the neuronopathic and non-neuronopathic formsrdquoThe Journal of Biological Chemistry vol 267 no 18 pp 12552ndash12558 1992
[19] M PWassersteinG ADiaz R H Lachmann et al ldquoOlipudasealfa for treatment of acid sphingomyelinase deficiency (ASMD)safety and efficacy in adults treated for 30 monthsrdquo Journal ofInherited Metabolic Disease vol 41 no 5 pp 829ndash838 2018
[20] R W D Welford M Garzotti C M Lourenco et al ldquoPlasmalysosphingomyelin demonstrates great potential as a diagnosticbiomarker for niemann-pick disease type C in a retrospectivestudyrdquo PLoS ONE vol 9 no 12 Article ID e114669 2014
[21] W-L Chuang J Pacheco S Cooper et al ldquoLyso-sphingomyelinis elevated in dried blood spots of Niemann-Pick B patientsrdquoMolecular Genetics and Metabolism vol 111 no 2 pp 209ndash2112014
[22] X Jiang R Sidhu J J Orsini et al ldquoDiagnosis of niemann-pickC1 by measurement of bile acid biomarkers in archived new-born dried blood spotsrdquo Molecular Genetics and Metabolismvol 126 no 2 pp 183ndash187 2019
[23] N Yasmin Y Ishitsuka M Fukaura et al ldquoIn vitro and invivo evaluation of 6-O-120572-maltosyl-120573-cyclodextrin as a potentialtherapeutic agent against niemann-pick disease type Crdquo Inter-national Journal of Molecular Sciences vol 20 no 5 Article IDE1152 2019
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Case Reports in Genetics 3
GAAAGGAAGGAGCCTGATTGTTTG
380
470 480
SMPD1exon2 -MUTATION CONTEXT
CTTGGGAGCCCTGGCTGGCTGCCT370
GGAGCCCTGGCT
GGAGCCCTGGCTGGCT
Figure 1 Representation of the novel 4 bp insertion mutation inSMPD1 gene in exon 2 in family 2 in parental sample
with patchy contrast enhancement He also had hypertensiveemergency during hospital stay with seizure pulmonaryedema and grade 4 hypertensive changes in retinal vesselsand nonoliguric acute kidney injury which responded topharmacological management He subsequently developedpancytopenia coagulopathy and sudden onset hypotensiveshock nonresponsive to fluid bolus and dopamine infusionand succumbed to the illness His enzyme assay revealednormal beta-glucosidase level for Gaucher disease and a lowlevel of sphingomyelinase consistent with NPD
His older sibling had similar features and was admittedin PGE ward at 12 years of age with periorbital puffinessaround 8 months earlier and had expired in hospital Shehad wasting and stunting hypertension encephalopathyseizures and shock Ultrasonography of abdomen showedliver of 21 cm normal echotexture normal outline and adistended gall bladder spleen of 22 cm normal echotextureand normal kidneys Echocardiography revealed mitral valvemildly thickened with prolapse of postmitral leaflet moder-ate mitral regurgitation and eccentric jet anteriorly directedand normal left ventricular ejection fraction The parentswere tested by Sanger sequencing of SMPD1 gene and wereheterozygous for the identified variant in child and werecounseled accordingly for future pregnancies
In family 4 a female child was brought with regression ofmilestones from 2 12-year age She had history of neonatalcholestasis At 4-year age she presented with fever andrespiratory complaints Examination revealed microcephalygrowth failure hepatosplenomegaly and upward gaze restric-tion Fundus examination did not show any cherry redspot and X-rays did not reveal any dysostosis Keepinga possibility of Niemann-Pick disease a sphingomyelinaseassay was done which showed normal sphingomyelinaseenzyme in the blood lymphocytes However further testingby targeted DNA analysis was done for storage disordersby next generation sequencing (NGS) and two variants inNPC1 gene were identified One was an exon 3 variant c275AgtG (pGln92Arg) and an exon 22 variant c3246 TgtA(pSer1082Arg) confirming diagnosis of NPD type C Thefamily was counseled for subsequent prenatal diagnosis
Family 5 A 9-month male child presented with devel-opmental delay respiratory problems failure to gain weightHe was born full term by LSCS (indicationoligohydramnios)with birth weight of 22 kg He had jaundice on day 2 of liferequiring phototherapy for 3 days From 4 months age he
developed on and off cough without significant fever Locallyhe was admitted for 2 months and given antibiotics andoxygen For positive CMV IgM he received also ganciclovirfor 2 weeks Thereafter he developed increasing respira-tory distress and perioral cyanosis Examination revealedlengthheight of 56 cm (-085 Z score) and head circum-ference of 375 cm (-183 Z score) and hepatosplenomegalyThe liver was 4 cm below RCM and 5 cm below the xiphoidspleen was 4 cm below LCM with notch present He hadhypotonia with scarf sign crossing midline He had anemiaduring hospital stay but X-rays did not show any dysostosisChest X-ray was suggestive of interstitial pneumonia andCECT chest revealed multifocal areas of patchy consolidationwith ground glass opacity and reduced volume of thymusThe transaminases levels were 191 and 133 UL with normalserum creatinine Stool for fat globules were 30-40HPF andflow cytometry for chronic granulomatous disease (CGD)was negative Keeping a clinical diagnosis of Niemann-Pickdisease enzyme analysis was performed which showed nor-mal sphingomyelinase level-18 units (N-18-85 nmolhrmgprotein) However chitotriosidase was elevated (2041 units)above normal values (287-63 nmolmlhr) and bone marrowshowed scattered histiocytes with eccentric nuclei and mul-tivacuolated cytoplasm suggestive of non-Gaucher storagedisorder Thus NPC was not ruled out Vit D level was lowand he was given replacement therapy Further DNA testingwas done by targeted NGS and identified homozygosity foran insertion variant in NPC2 gene c82 +2 -gtG which wasfound to affect splicing on bioinformatics analysis Geneticcounseling was done and feasibility of prenatal diagnosis wasdiscussed
3 Discussion
Mucopolysaccharidosis disorders and Gaucher disease arecommoner lysosomal storage disorders (LSDs) Recently sph-ingolipidoses have been reported to be common metabolicdisorders from Saudi Arabia [12] Early diagnosis and earlyinitiation of treatment including enzyme replacement ther-apy (ERT) in selected disorders can enable the affected chil-dren to have near normal life Because of the variable clinicalpresentation and limited availability of diagnostic testingthese disorders are missed out during routine evaluation InNiemann-Pick disease (NPD) the incidence for carrier of thegene-SMPD1 causing ASMD is 1120 in the general popula-tion and increases to 160 for individuals of Ashkenazi Jewishdescent [13] NPD type A disease manifests with persistentearly jaundice enlarging abdomen hepatosplenomegaly andpoor developmental progress and failure to thrive [10] Deathusually occurs by 3 years of age
In a Nepalese boy 13-year-old presenting with gait abnor-malities and supranuclear gaze palsy bone marrow revealedabundant foamy cytoplasm suggestive of storage disorderMutation analysis revealed two variants in the NPC1 genec302TgtG F101C in exon 4 and another IVS 24+1GgtA muta-tion [14] This confirmed the diagnosis of NPC NPD type Coften present with prolonged neonatal jaundice may remainnormal for 1-2 years ultimately leading to slowly progressiveand variable neurodegenerative course Hepatosplenomegaly
4 Case Reports in Genetics
in type C is less severe than type A or B and they maysurvive into adulthoodThe underlying biochemical defect intype C is abnormal cholesterol transport which leads to sph-ingomyelin and cholesterol accumulation in the lysosomesand a secondary partial reduction in acid sphingomyelinaseactivity NPC1 and NPC2 are the genes underlying NPD typeC Few cases of NPC are reported compared to NPD [15ndash17] In present study we found one case with NPC1 witha likely deleterious variant in homozygous state She hadhepatosplenomegaly and gaze palsy and presented at 4 yearsof age A high index of suspicion is needed for the diagnosisSometimes it is difficult to do filipin staining in hepatic cellsby biopsy but increased level of chitotriosidase as a surrogatemarker helps in giving a clue to underlying diagnosisChitotriosidase is more elevated especially in ASMD casesthan in NPC cases Mutation studies are now available forNPC and can be done in individual cases However if VUSis identified pathogenicity confirmation can only be donewhen another similar case is reported in another family In themale infant with respiratory problems we found an insertionmutation in the NPC2 gene Lung involvement is a dominantfeature in NPD and this may also lead to persistent oxygenrequirement
Small deletions or nonsensemutations in the SMPD1 geneusually lead to NPD type A whereas missense mutationsthat produce a defective enzyme cause a milder NPD typeB phenotype [15 18] ] Levran et al identified single basedeletion in Ashkenazi Jews causing the pro330FS mutationcausing a frameshift leading to premature chain termination[7] Most (65) SMPD1 mutations are accounted for bythree mutations R496L L302P and pro330FS mutation inAshkenazi Jewish NPD cases
In the family 2 we found a 4 bp insertion variation(CgtCCTGG) in exon 2 leading to a premature stop codonThismutation is 35 amino acids from the amino acid position355 in the SMPD1 gene On database analysis this mutationwas predicted to disrupt protein function Family 3 alsoshowed novel missense variant c1566TgtG in exon 6 ofthe SMPD1 gene identified on NGS This was predictedto be deleterious on analysis in available mutation specificdatabases and not reported in general population
In family 3 the siblings showed growth retardationhypertension and mitral valve prolapse in addition to hep-atosplenomegaly Cardiomyopathy and MVP are commonlyreported in mucopolysaccharidoses but can also be seenin NPD Mutation analysis also showed novel missensemutation in this family in exon 6 of SMPD1 gene
Various treatment modalities tried with no or littlesuccess are orthotopic liver transplantation in type A andcord blood transplantation in several type B A phase Itrial of enzyme replacement therapy for type B has beencompleted Clinical trials of the drug Miglustat (substratereduction therapy SRT) have been performed and the drughas been approved in Europe for the treatment of type Cdisease [6] SRT has emerged as promising form of treatmentas single therapy or in addition to ERT for ASMD Olipudasealfa is the recombinant enzyme the human acid sphin-gomyelinase which has been found beneficial in treatment ofASMD [19] There are only mild adverse events like nausea
abdominal pain and headache and no severe reactions werereported
Chitotriosidase is a surrogate marker for diagnosis ofGaucher and Niemann-Pick disease and is significantlyincreased in these disorders However 6 of the populationis deficient for chitotriosidase protein In case the enzymelevels are inconclusive the further mutation analysis cangive a confirmatory diagnosis New biomarkers are beingdeveloped to make diagnosis easier One of these is plasmalysosphingomyelin which can of potential use in diagnosis ofNiemann-Pick type B and also NPC [20 21] Recently bileacid B has also been found to detect NPC1 related diseaseon newborn dried blood spots [22] Chitotriosidase andlysosphingomyelin levels have also been found to be helpfulinmonitoring response to therapy [19] Recent research is alsoon to find new therapeutic options for NPC and one of thestudied molecules is 6-O-120572-maltosyl-120573-cyclodextrin (G2-120573-CD) in treatment ofNPC1disease [23] Promising results havebeen demonstrated in NPC1 deficient mice models
In countries like India and nearby South Asian countrieswith low GDP the numbers of diagnosed cases actuallyrepresent a minority of the actual number of cases in view ofthe large population base There is discrepancy in resourcesand availability of diagnosis and treatment facilities for raredisorders [2 3] NPD also present with nonimmune hydropsfetalis (NIHF) and should be considered in pregnancies withrecurrent hydrops The availability of enzyme analysis andmutation analysis has made early prenatal diagnosis of NPDpossible in selected families at risk of child with severe NPDThere is also a need to increase awareness regarding earlydiagnosis of these disorders Till the treatment of NPD ismade widely available the focus lies on timely detection ofindex child with NPD and provision of genetic counselingand planned prenatal diagnosis in some families
Additional Points
KeyMessage Niemann-Pick disease can have variable clinicalpresentations and suspicion is the key to early diagnosis Highincidence is expected in South East Asia region A completeevaluation including DNA analysis can help in reaching anappropriate diagnosis
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] I C Verma and D Kumar ldquoEpidemiology of genetic diseasesrdquoin Genetic Disorders of the Indian Subcontinent D Kumar Edpp 81ndash87 Springer Dordrecht Netherlands 2004
[2] J Sheth M Mistri F Sheth et al ldquoBurden of lysosomal storagedisorders in India experience of 387 affected children from asingle diagnostic facilityrdquo JIMD Reports vol 12 pp 51ndash63 2014
[3] X Chen W Qiu J Ye L Han X Gu and H ZhangldquoDemographic characteristics and distribution of lysosomalstorage disorder subtypes in Eastern Chinardquo Journal of HumanGenetics vol 61 no 4 pp 345ndash349 2016
Case Reports in Genetics 5
[4] J Sheth R Bhavsar M Mistri et al ldquoGaucher disease sin-gle gene molecular characterization of one-hundred Indianpatients reveals novel variants and the most prevalent muta-tionrdquo BMC Medical Genetics vol 20 no 1 p 31 2019
[5] P J Meikle J J Hopwood A E Clague and W F CareyldquoPrevalence of lysosomal storage disordersrdquo Journal of theAmericanMedical Association vol 281 no 3 pp 249ndash254 1999
[6] R M Kliegman B M D Stanton J S Geme and N F SchorNelson Textbook of Pediatrics Elsevier Health Sciences 2015
[7] O Levran R J Desnick and E H Schuchman ldquoType A Nie-mann-Pick disease A frameshift mutation in the acid sphingo-myelinase gene (fsP330) occurs in Ashkenazi Jewish patientsrdquoHuman Mutation vol 2 no 4 pp 317ndash319 1993
[8] R W Jenkins D Canals and Y A Hannun ldquoRoles andregulation of secretory and lysosomal acid sphingomyelinaserdquoCellular Signalling vol 21 no 6 pp 836ndash846 2009
[9] P G Camoletto H Vara L Morando et al ldquoSynaptic vesi-cle docking Sphingosine regulates syntaxin1 interaction withMunc18rdquo PLoS ONE vol 4 no 4 Article ID e5310 2009
[10] J Aicardi M Bax and C Gillberg Diseases of the NervousSystem in Childhood Mac Keith Press London UK 2009
[11] Y-U Cho J D ChaeW M Lee et al ldquoA case of a Korean adultaffected by type B Niemann-Pick disease Secondary sea-bluehistiocytosis andmolecular characterizationrdquoKorean Journal ofLaboratory Medicine vol 29 no 2 pp 97ndash103 2009
[12] M Alfadhel M Benmeakel M A Hossain et al ldquoThirteenyear retrospective review of the spectrum of inborn errors ofmetabolism presenting in a tertiary center in Saudi ArabiardquoOrphanet Journal of Rare Diseases vol 11 no 1 p 126 2016
[13] S R Pupecki Focus on Genetic Screening Research NovaScience Publishers 2006
[14] P Jain S Sharma P Poudel J Reunert T Marquardt and SAneja ldquoNiemann-Pick type C disease in a 13-year-old boy fromNepal a genetically confirmed caserdquo Neurology India vol 63no 4 pp 626ndash628 2015
[15] H Ida O M Rennert K Maekawa and Y Eto ldquoIdentificationof three novel mutations in the acid sphingomyelinase gene ofJapanese patients with Niemann-Pick disease type A and BrdquoHuman Mutation vol 7 no 1 pp 65ndash67 1996
[16] J Sheth J J Joseph K Shah M Muranjan M Mistri andF Sheth ldquoPulmonary manifestations in Niemann-Pick type Cdisease with mutations in NPC2 gene case report and review ofliteraturerdquo BMC Medical Genetics vol 18 no 1 p 5 2017
[17] M Hebbar H Prasada L A D Bhowmik et al ldquoHomozygousdeletion of exons 2 and 3 of NPC2 associated with Niemann-Pick disease type Crdquo American Journal of Medical Genetics PartA vol 170 no 9 pp 2486ndash2489 2016
[18] T Takahashi M Suchi R J Desnick G Takada and E HSchuchman ldquoIdentification and expression of five mutations inthe human acid sphingomyelinase gene causing types A and BNiemann-Pick disease Molecular evidence for genetic heter-ogeneity in the neuronopathic and non-neuronopathic formsrdquoThe Journal of Biological Chemistry vol 267 no 18 pp 12552ndash12558 1992
[19] M PWassersteinG ADiaz R H Lachmann et al ldquoOlipudasealfa for treatment of acid sphingomyelinase deficiency (ASMD)safety and efficacy in adults treated for 30 monthsrdquo Journal ofInherited Metabolic Disease vol 41 no 5 pp 829ndash838 2018
[20] R W D Welford M Garzotti C M Lourenco et al ldquoPlasmalysosphingomyelin demonstrates great potential as a diagnosticbiomarker for niemann-pick disease type C in a retrospectivestudyrdquo PLoS ONE vol 9 no 12 Article ID e114669 2014
[21] W-L Chuang J Pacheco S Cooper et al ldquoLyso-sphingomyelinis elevated in dried blood spots of Niemann-Pick B patientsrdquoMolecular Genetics and Metabolism vol 111 no 2 pp 209ndash2112014
[22] X Jiang R Sidhu J J Orsini et al ldquoDiagnosis of niemann-pickC1 by measurement of bile acid biomarkers in archived new-born dried blood spotsrdquo Molecular Genetics and Metabolismvol 126 no 2 pp 183ndash187 2019
[23] N Yasmin Y Ishitsuka M Fukaura et al ldquoIn vitro and invivo evaluation of 6-O-120572-maltosyl-120573-cyclodextrin as a potentialtherapeutic agent against niemann-pick disease type Crdquo Inter-national Journal of Molecular Sciences vol 20 no 5 Article IDE1152 2019
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

4 Case Reports in Genetics
in type C is less severe than type A or B and they maysurvive into adulthoodThe underlying biochemical defect intype C is abnormal cholesterol transport which leads to sph-ingomyelin and cholesterol accumulation in the lysosomesand a secondary partial reduction in acid sphingomyelinaseactivity NPC1 and NPC2 are the genes underlying NPD typeC Few cases of NPC are reported compared to NPD [15ndash17] In present study we found one case with NPC1 witha likely deleterious variant in homozygous state She hadhepatosplenomegaly and gaze palsy and presented at 4 yearsof age A high index of suspicion is needed for the diagnosisSometimes it is difficult to do filipin staining in hepatic cellsby biopsy but increased level of chitotriosidase as a surrogatemarker helps in giving a clue to underlying diagnosisChitotriosidase is more elevated especially in ASMD casesthan in NPC cases Mutation studies are now available forNPC and can be done in individual cases However if VUSis identified pathogenicity confirmation can only be donewhen another similar case is reported in another family In themale infant with respiratory problems we found an insertionmutation in the NPC2 gene Lung involvement is a dominantfeature in NPD and this may also lead to persistent oxygenrequirement
Small deletions or nonsensemutations in the SMPD1 geneusually lead to NPD type A whereas missense mutationsthat produce a defective enzyme cause a milder NPD typeB phenotype [15 18] ] Levran et al identified single basedeletion in Ashkenazi Jews causing the pro330FS mutationcausing a frameshift leading to premature chain termination[7] Most (65) SMPD1 mutations are accounted for bythree mutations R496L L302P and pro330FS mutation inAshkenazi Jewish NPD cases
In the family 2 we found a 4 bp insertion variation(CgtCCTGG) in exon 2 leading to a premature stop codonThismutation is 35 amino acids from the amino acid position355 in the SMPD1 gene On database analysis this mutationwas predicted to disrupt protein function Family 3 alsoshowed novel missense variant c1566TgtG in exon 6 ofthe SMPD1 gene identified on NGS This was predictedto be deleterious on analysis in available mutation specificdatabases and not reported in general population
In family 3 the siblings showed growth retardationhypertension and mitral valve prolapse in addition to hep-atosplenomegaly Cardiomyopathy and MVP are commonlyreported in mucopolysaccharidoses but can also be seenin NPD Mutation analysis also showed novel missensemutation in this family in exon 6 of SMPD1 gene
Various treatment modalities tried with no or littlesuccess are orthotopic liver transplantation in type A andcord blood transplantation in several type B A phase Itrial of enzyme replacement therapy for type B has beencompleted Clinical trials of the drug Miglustat (substratereduction therapy SRT) have been performed and the drughas been approved in Europe for the treatment of type Cdisease [6] SRT has emerged as promising form of treatmentas single therapy or in addition to ERT for ASMD Olipudasealfa is the recombinant enzyme the human acid sphin-gomyelinase which has been found beneficial in treatment ofASMD [19] There are only mild adverse events like nausea
abdominal pain and headache and no severe reactions werereported
Chitotriosidase is a surrogate marker for diagnosis ofGaucher and Niemann-Pick disease and is significantlyincreased in these disorders However 6 of the populationis deficient for chitotriosidase protein In case the enzymelevels are inconclusive the further mutation analysis cangive a confirmatory diagnosis New biomarkers are beingdeveloped to make diagnosis easier One of these is plasmalysosphingomyelin which can of potential use in diagnosis ofNiemann-Pick type B and also NPC [20 21] Recently bileacid B has also been found to detect NPC1 related diseaseon newborn dried blood spots [22] Chitotriosidase andlysosphingomyelin levels have also been found to be helpfulinmonitoring response to therapy [19] Recent research is alsoon to find new therapeutic options for NPC and one of thestudied molecules is 6-O-120572-maltosyl-120573-cyclodextrin (G2-120573-CD) in treatment ofNPC1disease [23] Promising results havebeen demonstrated in NPC1 deficient mice models
In countries like India and nearby South Asian countrieswith low GDP the numbers of diagnosed cases actuallyrepresent a minority of the actual number of cases in view ofthe large population base There is discrepancy in resourcesand availability of diagnosis and treatment facilities for raredisorders [2 3] NPD also present with nonimmune hydropsfetalis (NIHF) and should be considered in pregnancies withrecurrent hydrops The availability of enzyme analysis andmutation analysis has made early prenatal diagnosis of NPDpossible in selected families at risk of child with severe NPDThere is also a need to increase awareness regarding earlydiagnosis of these disorders Till the treatment of NPD ismade widely available the focus lies on timely detection ofindex child with NPD and provision of genetic counselingand planned prenatal diagnosis in some families
Additional Points
KeyMessage Niemann-Pick disease can have variable clinicalpresentations and suspicion is the key to early diagnosis Highincidence is expected in South East Asia region A completeevaluation including DNA analysis can help in reaching anappropriate diagnosis
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] I C Verma and D Kumar ldquoEpidemiology of genetic diseasesrdquoin Genetic Disorders of the Indian Subcontinent D Kumar Edpp 81ndash87 Springer Dordrecht Netherlands 2004
[2] J Sheth M Mistri F Sheth et al ldquoBurden of lysosomal storagedisorders in India experience of 387 affected children from asingle diagnostic facilityrdquo JIMD Reports vol 12 pp 51ndash63 2014
[3] X Chen W Qiu J Ye L Han X Gu and H ZhangldquoDemographic characteristics and distribution of lysosomalstorage disorder subtypes in Eastern Chinardquo Journal of HumanGenetics vol 61 no 4 pp 345ndash349 2016
Case Reports in Genetics 5
[4] J Sheth R Bhavsar M Mistri et al ldquoGaucher disease sin-gle gene molecular characterization of one-hundred Indianpatients reveals novel variants and the most prevalent muta-tionrdquo BMC Medical Genetics vol 20 no 1 p 31 2019
[5] P J Meikle J J Hopwood A E Clague and W F CareyldquoPrevalence of lysosomal storage disordersrdquo Journal of theAmericanMedical Association vol 281 no 3 pp 249ndash254 1999
[6] R M Kliegman B M D Stanton J S Geme and N F SchorNelson Textbook of Pediatrics Elsevier Health Sciences 2015
[7] O Levran R J Desnick and E H Schuchman ldquoType A Nie-mann-Pick disease A frameshift mutation in the acid sphingo-myelinase gene (fsP330) occurs in Ashkenazi Jewish patientsrdquoHuman Mutation vol 2 no 4 pp 317ndash319 1993
[8] R W Jenkins D Canals and Y A Hannun ldquoRoles andregulation of secretory and lysosomal acid sphingomyelinaserdquoCellular Signalling vol 21 no 6 pp 836ndash846 2009
[9] P G Camoletto H Vara L Morando et al ldquoSynaptic vesi-cle docking Sphingosine regulates syntaxin1 interaction withMunc18rdquo PLoS ONE vol 4 no 4 Article ID e5310 2009
[10] J Aicardi M Bax and C Gillberg Diseases of the NervousSystem in Childhood Mac Keith Press London UK 2009
[11] Y-U Cho J D ChaeW M Lee et al ldquoA case of a Korean adultaffected by type B Niemann-Pick disease Secondary sea-bluehistiocytosis andmolecular characterizationrdquoKorean Journal ofLaboratory Medicine vol 29 no 2 pp 97ndash103 2009
[12] M Alfadhel M Benmeakel M A Hossain et al ldquoThirteenyear retrospective review of the spectrum of inborn errors ofmetabolism presenting in a tertiary center in Saudi ArabiardquoOrphanet Journal of Rare Diseases vol 11 no 1 p 126 2016
[13] S R Pupecki Focus on Genetic Screening Research NovaScience Publishers 2006
[14] P Jain S Sharma P Poudel J Reunert T Marquardt and SAneja ldquoNiemann-Pick type C disease in a 13-year-old boy fromNepal a genetically confirmed caserdquo Neurology India vol 63no 4 pp 626ndash628 2015
[15] H Ida O M Rennert K Maekawa and Y Eto ldquoIdentificationof three novel mutations in the acid sphingomyelinase gene ofJapanese patients with Niemann-Pick disease type A and BrdquoHuman Mutation vol 7 no 1 pp 65ndash67 1996
[16] J Sheth J J Joseph K Shah M Muranjan M Mistri andF Sheth ldquoPulmonary manifestations in Niemann-Pick type Cdisease with mutations in NPC2 gene case report and review ofliteraturerdquo BMC Medical Genetics vol 18 no 1 p 5 2017
[17] M Hebbar H Prasada L A D Bhowmik et al ldquoHomozygousdeletion of exons 2 and 3 of NPC2 associated with Niemann-Pick disease type Crdquo American Journal of Medical Genetics PartA vol 170 no 9 pp 2486ndash2489 2016
[18] T Takahashi M Suchi R J Desnick G Takada and E HSchuchman ldquoIdentification and expression of five mutations inthe human acid sphingomyelinase gene causing types A and BNiemann-Pick disease Molecular evidence for genetic heter-ogeneity in the neuronopathic and non-neuronopathic formsrdquoThe Journal of Biological Chemistry vol 267 no 18 pp 12552ndash12558 1992
[19] M PWassersteinG ADiaz R H Lachmann et al ldquoOlipudasealfa for treatment of acid sphingomyelinase deficiency (ASMD)safety and efficacy in adults treated for 30 monthsrdquo Journal ofInherited Metabolic Disease vol 41 no 5 pp 829ndash838 2018
[20] R W D Welford M Garzotti C M Lourenco et al ldquoPlasmalysosphingomyelin demonstrates great potential as a diagnosticbiomarker for niemann-pick disease type C in a retrospectivestudyrdquo PLoS ONE vol 9 no 12 Article ID e114669 2014
[21] W-L Chuang J Pacheco S Cooper et al ldquoLyso-sphingomyelinis elevated in dried blood spots of Niemann-Pick B patientsrdquoMolecular Genetics and Metabolism vol 111 no 2 pp 209ndash2112014
[22] X Jiang R Sidhu J J Orsini et al ldquoDiagnosis of niemann-pickC1 by measurement of bile acid biomarkers in archived new-born dried blood spotsrdquo Molecular Genetics and Metabolismvol 126 no 2 pp 183ndash187 2019
[23] N Yasmin Y Ishitsuka M Fukaura et al ldquoIn vitro and invivo evaluation of 6-O-120572-maltosyl-120573-cyclodextrin as a potentialtherapeutic agent against niemann-pick disease type Crdquo Inter-national Journal of Molecular Sciences vol 20 no 5 Article IDE1152 2019
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Case Reports in Genetics 5
[4] J Sheth R Bhavsar M Mistri et al ldquoGaucher disease sin-gle gene molecular characterization of one-hundred Indianpatients reveals novel variants and the most prevalent muta-tionrdquo BMC Medical Genetics vol 20 no 1 p 31 2019
[5] P J Meikle J J Hopwood A E Clague and W F CareyldquoPrevalence of lysosomal storage disordersrdquo Journal of theAmericanMedical Association vol 281 no 3 pp 249ndash254 1999
[6] R M Kliegman B M D Stanton J S Geme and N F SchorNelson Textbook of Pediatrics Elsevier Health Sciences 2015
[7] O Levran R J Desnick and E H Schuchman ldquoType A Nie-mann-Pick disease A frameshift mutation in the acid sphingo-myelinase gene (fsP330) occurs in Ashkenazi Jewish patientsrdquoHuman Mutation vol 2 no 4 pp 317ndash319 1993
[8] R W Jenkins D Canals and Y A Hannun ldquoRoles andregulation of secretory and lysosomal acid sphingomyelinaserdquoCellular Signalling vol 21 no 6 pp 836ndash846 2009
[9] P G Camoletto H Vara L Morando et al ldquoSynaptic vesi-cle docking Sphingosine regulates syntaxin1 interaction withMunc18rdquo PLoS ONE vol 4 no 4 Article ID e5310 2009
[10] J Aicardi M Bax and C Gillberg Diseases of the NervousSystem in Childhood Mac Keith Press London UK 2009
[11] Y-U Cho J D ChaeW M Lee et al ldquoA case of a Korean adultaffected by type B Niemann-Pick disease Secondary sea-bluehistiocytosis andmolecular characterizationrdquoKorean Journal ofLaboratory Medicine vol 29 no 2 pp 97ndash103 2009
[12] M Alfadhel M Benmeakel M A Hossain et al ldquoThirteenyear retrospective review of the spectrum of inborn errors ofmetabolism presenting in a tertiary center in Saudi ArabiardquoOrphanet Journal of Rare Diseases vol 11 no 1 p 126 2016
[13] S R Pupecki Focus on Genetic Screening Research NovaScience Publishers 2006
[14] P Jain S Sharma P Poudel J Reunert T Marquardt and SAneja ldquoNiemann-Pick type C disease in a 13-year-old boy fromNepal a genetically confirmed caserdquo Neurology India vol 63no 4 pp 626ndash628 2015
[15] H Ida O M Rennert K Maekawa and Y Eto ldquoIdentificationof three novel mutations in the acid sphingomyelinase gene ofJapanese patients with Niemann-Pick disease type A and BrdquoHuman Mutation vol 7 no 1 pp 65ndash67 1996
[16] J Sheth J J Joseph K Shah M Muranjan M Mistri andF Sheth ldquoPulmonary manifestations in Niemann-Pick type Cdisease with mutations in NPC2 gene case report and review ofliteraturerdquo BMC Medical Genetics vol 18 no 1 p 5 2017
[17] M Hebbar H Prasada L A D Bhowmik et al ldquoHomozygousdeletion of exons 2 and 3 of NPC2 associated with Niemann-Pick disease type Crdquo American Journal of Medical Genetics PartA vol 170 no 9 pp 2486ndash2489 2016
[18] T Takahashi M Suchi R J Desnick G Takada and E HSchuchman ldquoIdentification and expression of five mutations inthe human acid sphingomyelinase gene causing types A and BNiemann-Pick disease Molecular evidence for genetic heter-ogeneity in the neuronopathic and non-neuronopathic formsrdquoThe Journal of Biological Chemistry vol 267 no 18 pp 12552ndash12558 1992
[19] M PWassersteinG ADiaz R H Lachmann et al ldquoOlipudasealfa for treatment of acid sphingomyelinase deficiency (ASMD)safety and efficacy in adults treated for 30 monthsrdquo Journal ofInherited Metabolic Disease vol 41 no 5 pp 829ndash838 2018
[20] R W D Welford M Garzotti C M Lourenco et al ldquoPlasmalysosphingomyelin demonstrates great potential as a diagnosticbiomarker for niemann-pick disease type C in a retrospectivestudyrdquo PLoS ONE vol 9 no 12 Article ID e114669 2014
[21] W-L Chuang J Pacheco S Cooper et al ldquoLyso-sphingomyelinis elevated in dried blood spots of Niemann-Pick B patientsrdquoMolecular Genetics and Metabolism vol 111 no 2 pp 209ndash2112014
[22] X Jiang R Sidhu J J Orsini et al ldquoDiagnosis of niemann-pickC1 by measurement of bile acid biomarkers in archived new-born dried blood spotsrdquo Molecular Genetics and Metabolismvol 126 no 2 pp 183ndash187 2019
[23] N Yasmin Y Ishitsuka M Fukaura et al ldquoIn vitro and invivo evaluation of 6-O-120572-maltosyl-120573-cyclodextrin as a potentialtherapeutic agent against niemann-pick disease type Crdquo Inter-national Journal of Molecular Sciences vol 20 no 5 Article IDE1152 2019
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom








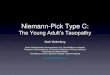



![GÖQ - tip.kocaeli.edu.trtip.kocaeli.edu.tr/.../NIEMANN-PICKTIPC.pdf · x Genetik inceleme Niemann Pick d] Z ofRfvf }R µo v fX. Niemann Pick , ofRf (NPH) Niemann Pick , ofRfV ol](https://img.pdfslide.net/doc/110x75/5c6c994f09d3f2fe088b4cea/goeq-tip-x-genetik-inceleme-niemann-pick-d-z-ofrfvf-r-o-v-fx-niemann.jpg)