Embed Size (px)
Citation preview

Noroviruses
Duncan Steele
Bill & Melinda Gates Foundation
Acknowledgements:
Ben Lopman and Umesh Parashar, CDC
Megan Carey and Julia Bosch, BMGF
1

Global norovirus burden
• Globally, norovirus is associated with 18% (95% CI: 17-20%) of diarrhoeal disease
• Estimated to cause approximately:
– 1 billion episodes annually
– 200,000 deaths annually, about >70,000 of which are among children in developing countries.
• Disease occurs across the age range in all settings, but incidence is highest in young children.
• Noroviruses are transmitted by multiple routes
– Person-to-person spread predominates
– Foodborne transmission is estimated to account for approximately 15% of disease
2

0
1
2
3
4
5
1980 1985 1990 1995 2000 2005 2010 2015
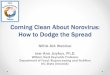
877,000 25%
1980
440,000 22%
1994
527,000 29%
2004
453,000 37%
2008
ROTAVIRUS DEATH ESTIMATES
90,000 13%
2010
NOROVIRUS DEATH ESTIMATES
212,000 12%
2004
71,000 9.9%
2011
197,000 28%
2010
173,000 26%
2011
To
tal
dia
rrh
ea d
eath
s (M
illi
on
s)
Mid-point of Study Period
Deaths % of diarrheal deaths
Year
Deaths % of diarrheal deaths
Year
3
Estimates of norovirus mortality

Norovirus detection is common amongst
healthy controls
1) True asymptomatic infection
2) Shedding of virus in stool continues long after the resolution of symptoms
3) Ingested virus may even transit the gut without replicating
• For this combination of reasons, norovirus can frequently be detected using RT-qPCR in stools from healthy individuals.
• However, norovirus is clearly a pathogen
• Complicates interpretation of etiological studies including MAL-ED or GEMS
4

Norovirus illness and infection rates in children
in community based cohort studies
5

Sapovirus (not previously tested)
Shigella (PCR vs. culture)
LT-ETEC (PCR vs. culture)
tEPEC (PCR vs. culture)
Adenovirus 40/41 (PCR vs. EIA)
ST-ETEC (PCR vs. culture)
Cryptosporidium (PCR vs. EIA)
Astrovirus (PCR vs. EIA)
C. jejuni/coli (PCR vs. EIA)
Rotavirus (PCR vs. EIA)
Norovirus GII (both PCR) MAL-ED WorkupTAC
0% 2% 4% 6% 8% 10% 12% 14% 16% 18%
Sapovirus (not previously tested)Salmonella (PCR vs. culture)
E. histolytica(PCR vs. EIA)EIEC (PCR vs. culture)
Adenovirus 40/41 (PCR vs. EIA)LT-ETEC (PCR vs. culture)
Cryptosporidium(PCR vs. EIA)ST-ETEC (PCR vs. culture)Shigella (PCR vs. culture)
Astrovirus (PCR vs. EIA)Rotavirus (PCR vs. EIA)
Norovirus GII (both PCR)C. jejuni/coli (PCR vs. EIA)
Attributable Fraction (%)
1-2
yea
rs o
f ag
e
0-1
yea
rs o
f ag
e
0% 2% 4% 6% 8% 10% 12% 14% 16% 18%
Sapovirus (not previously tested)Salmonella (PCR vs. culture)
E. histolytica(PCR vs. EIA)EIEC (PCR vs. culture)
Adenovirus 40/41 (PCR vs. EIA)LT-ETEC (PCR vs. culture)
Cryptosporidium(PCR vs. EIA)ST-ETEC (PCR vs. culture)Shigella (PCR vs. culture)
Astrovirus (PCR vs. EIA)Rotavirus (PCR vs. EIA)
Norovirus GII (both PCR)C. jejuni/coli (PCR vs. EIA)
Attributable Fraction (%)
POSTER TEMPL ATE BY:
www.PosterPresentations.com
▪ Studies of childhood diarrhea in
developing countries have traditionally
employed a wide range of diagnostic
modalities including culture, microscopy,
enzyme immunoassay, and polymerase chain
reaction.
▪ Molecular diagnostics offer more consistent
diagnostic performance, however they
substantially increase the background rate of
pathogen detection.
▪ Quantitative analysis of molecular testing
can help identify the subset of clinically
significant molecular detections.
Molecular re-analysis of community burdens of diarrhea in children
in developing countries in the multisite MAL-ED cohort study
James A. Platts-Mills1*, Jie Liu1*, Jean Gratz1,2, Darwin Operario1, Amidou Samie3, Ira Praharaj4, Gagandeep Kang4, Carl Mason5, Ladaporn Bodhidatta5, Sadia Shakoor6,
Furqan Kabir6, Shahida Qureshi6, Rashidul Haque7, Mami Taniuchi1,7, Margaret Kosek8.9, Mery S. Salas9, Alexandre Havt10, Aldo A. Lima10, Eric R. Houpt1
1Division of Infectious Diseases and International Health, University of Virginia, Charlottesville, Virginia, USA, 2Haydom Lutheran Hospital, Haydom, Tanzania, 3University of Venda, Thohoyandou, South Africa, 4Christian Medical College, Vellore, India, 5Armed Forces Research Institute of Medical
Sciences, Bangkok, Thailand, 6Aga Khan University, Karachi, Pakistan, 7International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh, 8Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA, 9Asociación Benéfica PRISMA, Iquitos, Peru, 10Clinical
Research Unit and Institute of Biomedicine, Federal University of Ceara, Fortaleza, Brazil, *Contributed equally
BACKGROUND
STUDY DEISGN AND STOOL TESTING
RESULTS ANALYSIS METHODS
CONCLUSIONS
CONTACT INFORMATION
James A. Platts-Mills, Assistant Professor
Infectious Diseases and International Health, University of Virginia
MAL-ED Study: http://mal-ed.fnih.org/
REFERENCES
1. Platts-Mills JA, Babji S, Bodhidatta L, Gratz J, Haque R, Havt A,
et al. Pathogen-specific burdens of community diarrhoea in
developing countries (MAL-ED): a multisite birth cohort study.
Lancet Global Health 2015, in press.
2. Liu J, Kabir F, Manneh J, Lertsethtakarn P, Begum S, Gratz J,
Becker SM, Operario DJ, Taniuchi M, Janaki L, Platts-Mills JA,
et al. Development and assessment of molecular diagnostic
tests for 15 enteropathogens causing childhood diarrhoea: a
multicentre study. Lancet Infect Dis 2014;8:716-24.
▪ We re-analyzed stool specimens from a
community-based multisite birth cohort study,
involving a total of 2086 children from 8 sites.1
▪ Diarrhea was defined as 3 or more loose
stools in 24 hours or presence of blood in stool.
Asymptomatic control specimens were
collected monthly; specimens collected within 7
days of an episode of diarrhea were excluded
from the analysis
▪ We re-tested diarrheal as well as quarterly
surveillance stools from the first two years of
life from a subset of approximately 60 children
per site with singleplex, quantitative PCR for a
broad range of enteropathogens using TaqMan
Array Cards (TAC).
▪ A total of 8508 diarrheal and 24238 control
stools were tested for a broad range of
enteropathogens in the primary analysis; 2182
diarrheal and 3244 control stools from
approximately 60 children per site were re-
analyzed by TAC.
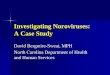
▪ The total AF for all pathogens increased from
24.7% to 34.9% in the first year of life and 38.0%
to 57.6% in the second year of life.
▪ In comparison to conventional detection
methods, the AF for Shigella, ST-ETEC, and
adenovirus 40/41 increased substantially.
Sapovirus was not previously assayed for in the
study and is revealed to have a substantial
burden of disease in these settings.
▪ This re-analysis substantially revises prior
estimates of pathogen-specific burdens of
diarrhea in children in developing countries and
can help refine priorities for development of
pathogen-specific interventions.
Figure 2. Overall adjusted attributable fractions derived for conventional diagnostic work-up (red) and TAC re-analysis (blue)
▪ Generalized estimating equations were used to
fit logistic regression models to calculate odds
ratios for the association between the detection
of each pathogen and diarrhea.
▪ Attributable fractions (AF) were calculated as
where N = total number of cases of diarrhea,
ORi = odds ratio from the fitted model for each
case i in which the pathogen was detected.
Sapovirus*(not*previously*tested)*
Shigella*(PCR*vs.*culture)*
LT<ETEC*(PCR*vs.*culture)*
tEPEC*(PCR*vs.*culture)*
Adenovirus*40/41*(PCR*vs.*EIA)*
ST<ETEC*(PCR*vs.*culture)*
Cryptosporidium*(PCR*vs.*EIA)*
Astrovirus*(PCR*vs.*EIA)*
C.*jejuni/coli*(PCR*vs.*EIA)*
Rotavirus*(PCR*vs.*EIA)*
Norovirus*GII*(both*PCR)* MAL<ED*Workup*TAC*
0%* 2%* 4%* 6%* 8%* 10%* 12%* 14%* 16%* 18%*
Sapovirus*(not*previously*tested)*
Salmonella*(PCR*vs.*culture)*
E.*histolyQca(PCR*vs.*EIA)*
EIEC*(PCR*vs.*culture)*
Adenovirus*40/41*(PCR*vs.*EIA)*
LT<ETEC*(PCR*vs.*culture)*
Cryptosporidium(PCR*vs.*EIA)*
ST<ETEC*(PCR*vs.*culture)*
Shigella*(PCR*vs.*culture)*
Astrovirus*(PCR*vs.*EIA)*
Rotavirus*(PCR*vs.*EIA)*
Norovirus*GII*(both*PCR)*
C.*jejuni/coli*(PCR*vs.*EIA)*
A" ributable+Frac. on+(%)+
1<2*years*of*age
**********************************0<1*years*of*a
ge*
Figure 1. Sensitivity (blue) and specificity (red) of comparator methods vs. TAC
! " =( 1/& )∑*↑▒( - . ↓* −1)/ - . ↓*
A total of 8,508 diarrhoeal and 24,238 control stools were tested for a broad range of enteropathogens in the primary analysis; 2,182 diarrhoeal and 3,244 control stools from approximately 60 children per site were re-analyzed by qPCR assays in TAC
6
Molecular re-analysis of MAL-ED

Challenges to Estimating Global
Norovirus Burden
• Little routine testing performed in ongoing surveillance platforms; or in developing countries
• Sensitive assays have only recently been widely available, and are not available for most settings
• Community-based studies are expensive and challenging
• Some norovirus acute gastroenteritis cases do not present with diarrhoea, only vomiting
• Challenges in interpretation of diagnostic results
Birth cohort study in Vellore, India
Leveraging the global rotavirus networks with TAC assays
8

Norovirus: basic virology
• Noroviruses are a highly diverse group of ssRNA viruses.
• GII.4 norovirus: – is the most common genotype causing cases
and outbreaks across the age range – evolves in a boom-and-bust cycling of
epochal evolution and escape population immunity with new variants emerge every 2-4 years
– cause more severe disease and affect both young and elderly vulnerable populations.
• Real time RT-PCR is – the gold standard for norovirus diagnostics – exquisitely sensitive and frequently detects
virus in the stool of healthy individuals • Uncultivable, but there has been important
recent progress in in vitro cell culture for norovirus.
9

Norovirus vaccines
• A number of noroviruses vaccines being developed.
• Based on the expression of VP1 leading to the production of VLPs or P particle subunit in various expression systems.
• Preclinical and early human studies of various concentrations of monovalent or bivalent norovirus antigens, with and without adjuvants, and various routes of immunization have shown safety and immunogenicity.
10

Transgenic plant-based
norovirus vaccine
Norovirus P particle and
combination vaccines
Trivalent norovirus/ rotavirus
combination vaccine
Bivalent norovirus VLP
vaccine
Principal
inventor
Charles Arntzen, PhD
Arizona State University
Xi Jason Jiang, PhD
Cincinnati Children's Hospital
Timo Vesikari, MD PhD
University of Tampere, Finland
Mary K. Estes, Ph.D.
Baylor College of Medicine
Norovirus
antigen(s)
(all based on
VP1)
Norwalk virus (GI.1) VLP Two to three noroviruses P
domains representing
different GI and GII strains
GII-4 and GI-3 VLP GI.1 and GII.4 consensus
VLP
Other
antigen(s)
None Chimeric norovirus P-
rotavirus VP8* particle,
experimental formulations
include influenza, Hepatitis E
Rotavirus VP6 None
Adjuvant(s) gardiquimod or none when
delivered with GelVac
5 mg chitosan, 50 μg MPL,
and TNC buffer 24920797
None, but some evidence that the
RV VP6 component adjuvant effect
alum and MPL (3-O-
desacyl-4’ monophosphoryl
lipid A)
Route of
administrati
on
Intranasal by GelVac dry
powder and oral by ingestion
of raw potato
Intranasal Intramuscular and intranasal Intramuscular, previously
intranasal and oral
Commercial
partner
UMN Pharma (Japan). Takeda Pharmaceuticals
Norovirus vaccine candidates
11

Human efficacy data from challenge studies
• The only products with human efficacy data are being developed by Takeda Pharmaceuticals. – An intranasal monovalent formulation was shown to be effective against
infection and disease following GI.1 challenge. • 47% (95% CI, 15%–67%) against AGE
• Norwalk virus infection by 26% (95% CI, 1%–45%)
– An IM bivalent formulation showed a degree of protection against disease
following GII.4 challenge sufficient to warrant further clinical development. • Non-significant reduction in AGE (26.0% among vaccinees ; 33.3% among
placebo recipients)
• Reductions of more severe disease and diarrhoea and vomiting in vaccine recipients following GII.4 challenge
12

Critical questions for a norovirus vaccine
• Can a vaccine elicit broad protection against multiple genotypes?
• What will be the duration of protection from vaccination?
• Will a norovirus vaccine have to be regularly updated in order to keep up with natural evolution of the virus?
• How will prior norovirus infection history affect vaccine immunogenicity and effectiveness?
• Will the same vaccine formulation be effective in all population groups, including in infants or low-income settings?
• How will the variation in human genetic susceptibility affect vaccine outcomes?
13

Target groups for vaccination strategies
Inci
de
nce
He
alth
car
e
uti
lizat
ion
1
Ho
spit
aliz
atio
n
De
ath
s
Soci
etal
co
sts
He
alth
care
cost
s
Ro
le/r
isk
in
tran
smis
sio
n
Ch
alle
nge
s in
vacc
inat
ing:
imm
un
olo
gica
l
Ch
alle
nge
s in
vacc
inat
ing:
pro
gram
mat
ic
Children
(<5 years)
High
High High
Med
.
High High High Naïve: may
need multiple
doses
Interaction with
other routine
immunizations
Older children
(5-14 years)
Med Low Low Low Med Low Med History of
exposure
Younger
adults
(15-64 years)
Med Low Low Low Med Low Med History of
exposure
Generally low
coverage
Older adults
(≥65 years)
Low Med High High
Low High Low History of
exposure
immune
senescence
Generally low
coverage
Top priority?
14

Specific sub-population target groups for
vaccination
• Healthcare workers
• Travelers
• Military personnel
• Immunocompromised patients
• Food service workers
Each group has unique epidemiological, economic and programmatic considerations
15

Specific roles for WHO in 2016-2017
• Study design to help quantify incidence and burden , particularly in developing countries
• Call for better epidemiology data on norovirus – Birth cohort studies
– Regional norovirus surveillance networks with standardized protocols
– Development / optimization of diagnostics for use in etiology and clinical studies
• Development of preferred product characteristics; TPPs – Different population targets will likely have different TPPs
• Confirmation of currently proposed immune correlates of protection; validation in different populations
16

THE WORK IS COMPLICATED. WHY WE DO IT, IS NOT