-
8/10/2019 NTP Presentation
1/40
Introduction to the National TB
program in Georgia:
current status, challenges and
future prospective
National Center for TB and Lung
Diseases
-
8/10/2019 NTP Presentation
2/40
TB Epi-Snapshot
Georgia is one among 27 high MDR-TB burden countries
In 2013:
TB prevalence: 96 cases per 100,000
TB incidence (new and relapse): 76 cases per 100,000
Case detection rate (all forms) 78%
Laboratory-confirmed MDR-TBprevalence 11.2%among new and
38%among retreatment cases
Treatment success rate in 2012 for new and relapse cases
excluding
those moved SLD treatment - 85%
Treatment success rate for M/XDR-TB in 2011 cohort50%
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
3/40
Notified TB cases(absolute numbers)
66126435
5926
63656073
5862
6448 6311
5911 5836 5982
57965536
4975
43204476 4393
3900
43784096
3819
4244 42834063 4148
4458 43834226
3779
3133
2136 2042 2026 1987 1977 2043 2204
20281848
16881524 1413 1310 1196 1187
0
1000
2000
3000
4000
5000
6000
7000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
2012 2013
All cases New cases Re-treated cases
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
4/40
TB in adults (15+ age-group) and children (0-14 age-
group)(per 100,000)
142,1153,6 159
170,3154,6 155,7 150
127,7
111
88,8
61,849
60,2
43,6 45,335,838,1 33,6
27,128,2
24,50
20
40
60
80
100
120
140
160
180
Adults Children
4NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
5/40
new
cases, 1.0
all cases, 2.3
0
1
2
3
4
5
6
%
TB in prisons(per 100 prisoner)
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
6/40
84
6,1 4,4 2,2 3,3
0
1020
30
40
50
60
70
80
90
Treatment success
Lost to follow-up
Failure
Died
Unknown
1stline treatment outcomes of the new pulmonary
bacteriologically confirmed TB cases
(2012 cohort, %)
-
8/10/2019 NTP Presentation
7/40
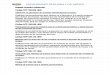
6,8% 6,8% 6,4%
11,3% 10,2% 9,5% 10,9% 9,2% 11,2%
27,4% 26,4%
32,0%
40,3%
31,1% 31,4% 31,7% 31,2%
38,1%
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
DRS 2006 2007 2008 2009 2010 2011 2012 2013
New TB Cases Re-treated TB Cases
Drug Resistance Surveillance(DRSDrug Resistance Survey conducted
between July 2005 and June 2006)
MDR-TB prevalence, pulmonary cases
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
8/40
DRSStudy (2005-2006)
revealed that:
6.8%among new and
27.4% among re-
treatment TB cases hadMDR-TB;
Independent Risk
Factors for MDR-TB:
Previous TB Treatment
OR=5.47 (95%CI, 3.86-
7.72), p
-
8/10/2019 NTP Presentation
9/40
Co-infectionTB/HIV
(%)
3,2 2,82,1
3,8
3,1
1,9
2,6
3,4
1,3
2,31,7
21,7
2,1
0
1
23
4
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
20
13
TB-HIV %
3,9
2,5
5,3 5,3
0
1
2
3
4
5
6
2010 2011 2012 2013
MDR-TB/HIV %
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
10/40
Co-infectionTB/HCV
-
8/10/2019 NTP Presentation
11/40
XDR-TB
10% 10%9%
6%
9%
20%
0%
5%
10%
15%
20%
25%
2008 2009 2010 2011 2012 2013
XDR-TB among MDR-TB cases (%)
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
12/40
Cases enrolled in 2ndline treatment
(absolute numbers)
466
636 633
741
666
526
400
500
600
700
800
2008 2009 2010 2011 2012 2013
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
13/40
M/XDR-TB (2ndline) TOM
54%
20%
13%
8%
5%
Success Lost to follow-up Died Failure Not evaluated
52%
27%
10%
4%7%
54%
27%
8%
6% 5%
2008
20092010
50%
34%
6%3%
7%
2011
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
14/40
Treatment Outcomes of MDR vs XDR
2011
50%
3%5%
36%
6%11%
21%
26% 26%
16%
0%
10%
20%
30%
40%
50%
60%
Cured or
treatment
completed
Treatment
failed
Died Lost to
follow-up
Not
evaluated*
MDR-TB
XDR-TB
NTP Data Base. Global TB Reports
-
8/10/2019 NTP Presentation
15/40
1stline treatment outcomes of nonMDR-
TB/HIV co-infected cases(86 cases, 2009-2011, %)
58.1
17.4
9.3
8.1
7
nonMDR-HIV
Success
Failure
Default
Death
Not evaluated
-
8/10/2019 NTP Presentation
16/40
2ndline treatment outcomes of MDR-TB/HIV
co-infected cases(65 cases, 2009-2011, %)
30.8
4.6
29.2
26.2
9.2
MDR-HIV
Success
Failure
Default
Death
Not evaluated
-
8/10/2019 NTP Presentation
17/40
2ndline treatment outcomes of XDR-TB/HIV
co-infected cases(5 cases, 2009-2011, %)
00
40
60
0
XDR-HIV
Success
Failure
Default
Death
Not evaluated
-
8/10/2019 NTP Presentation
18/40
MDR-TB cases managed and generated XDR-TB
(N and cumulative N)
2555
90135 175
225
466
636 633
741
666
526
0
100
200
300
400
500
600
700
800
2008 2009 2010 2011 2012 2013
XDR-TB among MDR-TB cases (cum. N) MDR-TB cases put on treatment
(N)
-
8/10/2019 NTP Presentation
19/40
Impact of MDR-TB management on XDR-TB
Georgia example
54% 54%52%
Treatment
success rate %,
50%
20%
27% 27%
Default rate %,
34%
10% 10% 9%6%
9%
XDR-TB %, 20%
0%
10%
20%
30%
40%
50%
60%
2008 2009 2010 2011 2012 2013
Treatment success rate % Default rate % XDR-TB %
-
8/10/2019 NTP Presentation
20/40
Can MDR-TB case management generate additional XDR-TB?
Message: the higher the % of MDR-TBmanaged with current poor
outcomes,the higher the % of XDR-TB generated
Blower S, Supervie V. Predicting the future of XDR tuberculosis.
Lancet 2007
-
8/10/2019 NTP Presentation
21/40
Programmatic Management of M/XDR-TB
Process Summary
Treatment Success Rate
Treatment Strengthening
Universal Access to Quality TB and MDR-TB DiagnosisCase
Detection
Smear Microscopy
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
2014
DRS LJ + MGIT + HAIN + GeneXpert
First-line anti-TB Treatment / Pilot SLD Universal Access to SLD
Treatment
Action is Needed
-
8/10/2019 NTP Presentation
22/40
3. Effective governance, adequate financing and monitoring of
Georgias
TB response;
4. Human resources available at each level with the
professional
competence and support to meet GeorgiasTB Response
planstargets;
5. Prevent TB transmission in health facilities and prisons
through
strengthening IC measures;
6. Empower TB patients and communities;7. Enhance TB/HIV
collaboration to reduce the burden of TB in people
living with HIV and the burden of HIV in TB patients.
1. Universal coverage with qualityTB diagnostic services
2. Universal access to TB treatmentand patient support
services
Georgia TB Response
Strategic Plan 2013-2015
Source:
NCDC, Overview of NTP, US-Georgia Pro gram -Developm ent Work
sho p On HIV/TB/Hepatit is, June 17, 2014
Gl b l F d d S TB P Gl
-
8/10/2019 NTP Presentation
23/40
Global Fund and State TB Program at a Glance
Goal:
- To reduce TB prevalence,
mortality and transmission
- To prevent drug resistance
Beneficiaries: citizens of
Georgia who have symptoms
of TB and is defined as a
presumptive TB case by
physician
Objectives:
Coordinate the national TB
Surveillance system
Collect , analyze and report
the data on TB contact tracing Contribute to TB State
Program
Development
Participate in TB State Program
and GF Program M&E
Activities with NCTBLD
Goal:
To reduce the burden of
tuberculosis in Georgia by
sustaining universal access
to quality diagnosis and
treatment of all forms oftuberculosis including
M/XDR-TB
Four mainobjectives:
To strengthen National TB
Control Program management, monitoring and
To improve diagnosis of TB including M/XDR-
TB.
To ensure quality treatment of all forms of TB
To ensure adherence to TB
treatment by intensive support and follow up
Global Fund Program
Implementation Unit
TB Surveillance UnitState Program Unit
State and GFATM funds
under one umbrella-NCDC
Source:
NCDC, Overview of NTP, US-Georgia Pro gram -Developm ent Work
sho p On HIV/TB/Hepatit is, June 17, 2014
-
8/10/2019 NTP Presentation
24/40
TB Service Model in Georgia
Screening for Presumptive TB and referral
DOT locally under supervision of district TBteams
PHC/PrivateSector
Confirming TB diagnosis
Initiating in patient or outpatient treatment
Provide ongoing DOT monitoring and follow-up
DOT and DOT plus
NCTBLD &Specialized TB
services
Sputum microscopy, bacteriology, Gene Xpert
9 laboratories in the civilian and 2 inpenitentiary sector
Reference laboratory at National Center for TBand Lung Diseases
(NCTBLD)
Laboratoryservices
Contact tracing and referral to furtherinvestigation in TB
sites
NCDC and PublicHealth Services
www.ncdc.geSource:
NCDC, Overview of NTP, US-Georgia Pro gram -Developm ent Work
sho p On HIV/TB/Hepatit is, June 17, 2014
-
8/10/2019 NTP Presentation
25/40
USAID URC TPPMdecins
Sans Frontires
(MSF)
FIND
Source:
NCDC, Overview of NTP, US-Georgia Pro gram -Developm ent Work
sho p On HIV/TB/Hepatit is, June 17, 2014
-
8/10/2019 NTP Presentation
26/40
National Center forDisease Control and Public
HealthNCDCPH
Data Collection Information
System (IS)
State level
Central level Monthly reports
Samegrelo/
Zemo Svaneti
9 TB units
Imereti
13 units
Guria
3 units
Racha/Kvemo
Svaneti
4 TB units
Kakheti
8 TB units
Samckhe-
Javakheti
6 TB units
Adjara
6 TB units
Shida Kartli
4 TB units
Tbilisi 5 TB unitsNational Center of TB
and Lung Disease (NCTBLD)
PR PIU
Penitentiarysystem
16 prisons
Samegrelo
DB Manager
Imereti
DB Manager
Kakheti
DB Manager
Samckhe-
Javakheti
DB Manager
AdjaraDB Manager
Shida KartliDB Manager
Poti
DB Manager
Prison
DB Manager
Tbilisi
4 DB Managers
HIV/AIDS, Hepatitis, STI &
TB surveillance division
Primary datacollectionsites
First aggregationlevel (IAL)
Second aggregationlevel (central)
Electroni c data entry directly into the IS
Hardcopies: Weekly- TB-10/12, Hospital Admission Forms; Monthly
- HI V data; Quarterl y - aggregate reports on case notif ication
(Form TB-07)
and treatment outcomes (TB-08)
Sputum collection, transferr ing for smear microscopy and
receiving the result s
Kutaisi
ZDL
Batumi
ZDL
Telavi
LSS
Akhaltsikhe
LSS
Reference
Lab
Ozurgeti
LSS
Gori
LSS
Poti
LSS
Zugdidi
LSS
Kvemo Kartli
7 TB units
Mckheta
4 TB units
Kvemo Kartli
DB Manager
Mckheta
DB Manager
Data Flow Diagram
Source:
NCDC, Overview of NTP, US-Georgia Pro gram -Developm ent Work
sho p On HIV/TB/Hepatit is, June 17, 2014
-
8/10/2019 NTP Presentation
27/40
SWOT Analysis
Strengths:1. Universal countrywide access to TB and
M/XDR TB Diagnosis using conventionaland rapid WHO approved
diagnostic
testsGF & FIND support;
2. Universal Access to 1stand 2ndline anti-
TB treatmentGF support;
3. Electronic web based TB data collection
system under NCTBLD.
Weaknesses:1. Weak legislative environment;
2. No lead agency responsible for TB response inthe country is
identified;
3. State vs donor funding is 46% / 54%;
4. Ineffective funding model for TB services;
5. Infrastructure development;
6. Private service providers with suboptimal
funding;
7. High MDR TB default rate;
8. Stigma and low motivation to be treated;9.
Pharmacovigilance.
10. Side effects management
11. Lack of medical equipment
12. Human resources!!!
Opportunities:
1. Minister of health recognizes TB as a
priority health problem;
2. New drugs and new treatment
guidelines and protocolsTA with USAID
support, Drugs GF and MSF France;
3. TB Program review planned for 6-14
November, 2014.
Threats:
1. Substantial decrease of donor (GF and
USAID) funding starting 2016;
2. Suboptimal implementation of new
drugs because of systematic challenges
as mentioned above;
3. Critical lack of new generation coming to
the field;
4. Unwillingness of the private sector toparticipate in the TB
service delivery.
C t N ti l G id li d WHO iti
-
8/10/2019 NTP Presentation
28/40
Current National Guidelines and WHO position on new
drugs
National TB treatment guidelines updated in 2012 based on WHO
2011 update
and endorsed by ministerial decree in 2013 includes all
recommendationsprovided;
Recent GLC mission (July 2014) recommended introduction of new
drugs and
treatment regimens for X/MDR-TB patients that are in line with
the
recommendations provided in 2014 Companion handbook to the
WHO
guidelines for the programmatic management of drug-resistant
tuberculosis;
Global Fund responded to the new recommendations effectively and
approved
the new order prepared based on the new GLC
recommendationscountry
will receive the drugs by April 2015;
Otherwise Georgian NTP shares WHOs position on new drugs: the
regimens
which are markedly different from the ones which represent
current norm andhave undergone GRADE review, should only be used
within the context of
research and under close monitoring for a period of at least 12
months beyond
the end of treatment.
C t N ti l G id li
-
8/10/2019 NTP Presentation
29/40
Current National Guidelines
Treatment Regimens
-
8/10/2019 NTP Presentation
30/40
30
Current National Guidelines
Treatment Regimens
Proteonamide
-
8/10/2019 NTP Presentation
31/40
31
Current National Guidelines
Treatment Regimens
-
8/10/2019 NTP Presentation
32/40
Ongoing MSF France Approach
Mdecins Sans Frontires (MSF)-France
treatment project Implementation of new
Drug-Resistant Tuberculosis Treatments
started in Summer 2014;
MOU between MoLHSA, the NCTBLD and MSF to
was signed on September 4, 2014;
-
8/10/2019 NTP Presentation
33/40
MSF New DR-TB Treatment Approach
Main objective is to offer quality treatment to DR-TB patients
with the
introduction of new regimens;Specific Objectives are to support
NCTBLD Georgia with:
the identification of the DR-TB cases eligible and with their
preparation for
the new regimen;
the introduction of new TB drugs through the CU mechanism;
the start and follow up treatment with new regimen;
the pharmacovigilance;
the implementation of a system of reporting compatible with the
data
collection system;
registration of the new TB drugs (Bedaquiline, Delamanid and
other drugswhich may become available);
the procurement of a secure and affordable supply of new TB
drugs;
updating TB guideline/protocols as needed;
training corresponding staff on the use of side effects of new
treatments
and other topics related to new DR-TB regimen.
-
8/10/2019 NTP Presentation
34/40
MSF New DR-TB Treatment Approach
Who is Eligible?
XDR-TB
Pre-XDR - Fluoroquinolone
Pre-XDR- both injectables
Failures of MDR TBCurrently on MDR TB treatment and not
clinically
improving after 4 months or
a failure by WHO 2013 definitions
Household Contact of patients with XDRTB or Pre-XDRTB, orwho
have failed MDR TB treatment
Previous failure of MDRTB/XDRTB treatment, not currently on
treatment for whom a regimen could be constructed with
drugs not previously used
-
8/10/2019 NTP Presentation
35/40
MSF New DR-TB Treatment Approach
What is new and different for those eligible?
Addition of new drugs through compassionate use
(Bedaquiline)
Addition of other 3rd line drugs
Linezolid
Imipenem
Other first and secondline drugs that are still active
Goal is to make up a strong regimen of at least 4 drugs
for whom the effectiveness is sure (or as sure as
possible).
-
8/10/2019 NTP Presentation
36/40
MSF New DR-TB Treatment Approach
What are the Principles of constructing a new regimen? Extension
of treatment
duration, a minimum of 24 months is recommended;
Extension of the period of injectable to 12 months or
possibly the whole treatment
Must include the maximum number of effective drugs possible;
Effectiveness of drugs should be assessed using:
DST for those with reliableDST ( Injectables, FQ, H, R, Z)
History of past use
Response to treatment (if a drug has been included in a
regimen that has failed and with not enough effective drugs
then its effectiveness must be put in question
-
8/10/2019 NTP Presentation
37/40
MSF New DR-TB Treatment Approach
Optimization of pre-treatment status of patient is very
important: Nutition
Nutritional assessment (height and weight but not only)
Nutritional supplements - vitamins (D, B1, B6, Mg, Fe)
Attention to protein
Nausea, vomiting, diarrhoea, annorexia, etc
Co-mobidities
Diabetes, hypertension etc, HIV
Consent, patient education and adherence support
Program Vision: Implementing new M/XDR-TB
-
8/10/2019 NTP Presentation
38/40
g p gtreatment regimens and new drugs in Georgia
Complex preparatory work must take place where all
stakeholder
support is essential:
Develop framework for introduction of new drugs in Georgia;
Establish a coordinating group that will develop a National
Implementation Plan of Bedaquiline and other new drugs
(Delamanid) introduction; update guidelines/protocols and
conduct
training with an uptake of international expertise and TA, and
have
oversight for the new recommendations; Improve NRL capacity in
SLDST (Protheonamide, Moxifloxacin
testing);
Establish a system for effective Pharmacovigilance (PV) in
the
country and improve management capacity of AEs;
Revise/update the M/XDR-TB treatment monitoring standard
andschedule in line with current requirements (ECG, lipase
test,
electrolytes);
Improve overall patient support for PMDT through HSS
(including
patient-centered DOT, cash incentives, etc.) and nutritional
support;
-
8/10/2019 NTP Presentation
39/40
Room for Considerations
o Will this MSF approach or routine implementation of
new drugs/regimens be enough to reach the targets?
o With current high loss to follow-up rate what are
cross-cutting systematic interventions that needs to
be addressed?o Establishing effective pharmacovigilance system
in
the country?
o
Establishing flexible patient centered care throughHSS?
o Changing the TB funding model?
o Who should and will advocate for those changes?
Time to move from being Rationale
-
8/10/2019 NTP Presentation
40/40
Time to move from being Rationale
to being (com)Passionate