Embed Size (px)
Citation preview
The Changing Face of Primary Immune Deficiency Diseases: “Treatment Experiences and Preferences of Patientswith Primary Immune Deficiency Diseases: FirstNational Survey”
The face of primary immune deficiency diseases is changing. IDF recentlyreleased data from a comprehensive survey of Americans affected by primaryimmune deficiency diseases, and the results reveal that what was once consideredprimarily a pediatric disease now affects more adults than children. This is the only
T H E N A T I O N A L N E W S L E T T E R O F T H E I M M U N E D E F I C I E N C Y F O U N D A T I O N
SUMMER 2003 NUMBER 44
Immune Globulin, Intravenous,is a life-saving biologic agent usedby approximately 70% of thepatients served by the Immune Deficiency Foundation. IGIV is also known topatients and physicians as IVIG and gamma globulin. What makes IGIV so usefulis that it contains antibodies to fight bacteria, fungi, and viruses that may affectthose with primary immune deficiency diseases. The antibodies are present as aresult of the immunization and infectious disease histories of the donors whoseplasma is used to manufacture IGIV.
IGIV was first licensed in the United States in 1981. Prior to that time, only anintra-muscular preparation was available. The volume of the intra-muscular product
The Facts about IGIV
PAGE 1
The Changing Face of Primary
Immune DeficiencyDiseases
PAGE 1
SARS and WestNile Virus Risks
PAGE 6
This Newsletter is sponsored byan educational grant from BayerCorporation
IDF VolunteerKatharine AustinRemembered
PAGE 5
continued on page 2
continued on page 6
Immune Globulin Intravenous (IGIV)A Brief Primer for Patients and Families
w20410 6/19/03 2:16 PM Page 1

PAGE 2 I D F A D V O C A T E
I hope you enjoy this issue of the IDFAdvocate. As the new editor of ournational newsletter, I’d like to take thisopportunity to introduce myself.
With more than 10 years in marketingand communications, I bring to this position experience in media relations,copywriting, public relations, publishing,graphic design, and market research.
Aside from my responsibilities as editor, I will also be working on the overall marketing and communications program to advance IDF’s mission: to improve thediagnosis and treatment of primary immunodeficiency diseases throughresearch, education and advocacy.
I am very excited to be part of IDF and the primary immune deficiency patientcommunity, and I look forward to workingwith all of you.
Pamela Mooring
E D I T O RPamela Mooring
M E D I C A L E D I T O RJonathan Goldsmith, M.D.
IDF Advocate is published quarterly by theImmune Deficiency Foundation. To obtaina free subscription, please contact:
The EditorIDF AdvocateImmune Deficiency Foundation40 West Chesapeake Avenue, Suite 308Towson, Maryland 21204
Toll-Free 800-296-4433Direct 410-321-6647Fax 410-321-9165E-mail [email protected] Site www.primaryimmune.org
A MESSAGE FROM THE EDITOR
needed to help protect those with aprimary immune deficiency diseaseswas quite large, often painful to deliv-er in “shots,” had to be given severaltimes each month and did notachieve blood antibody levels thatphysicians were seeking. The licensureof the IGIV form of immunoglobulinallowed the administration of largerdoses of the product on a less frequentand less painful basis.
Several U.S. and European compa-nies have been granted licenses tomarket and distribute their IGIV prod-uct in the U.S. Prior to licensure, each company has to perform clinical trialsin a significant number of researchsubjects to prove that the formulationis safe and effective. The currentlylicensed products are listed in Table A.
Many of the IGIV manufacturershave performed additional clinical studies in disorders other than primaryimmune deficiency diseases. As a result,the Food and Drug Administrationhas approved IGIV for the treatmentof these disorders for some of theproducts. These additional indicationsinclude Idiopathic ThrombocytopenicPurpura (a low blood platelet disor-der), Kawasaki Disease (a multi-sys-tem inflammatory disorder affectingespecially the heart), ChronicLymphocytic Leukemia, pediatric HIVdisease, and Graft Versus Host Diseasefollowing bone marrow transplantation.However, about one-fourth of all theIGIV that is manufactured is pre-scribed for individuals with primaryimmune deficiency diseases.
Use of IGIV for Treatment of the Primary ImmuneDeficiency Diseases
Typically, patients with primary
immune deficiency diseases receive aninfusion of IGIV every three or fourweeks. Over half the patients areinfused every four weeks and morethan a quarter receive infusions everythree weeks. Some patients areinfused more frequently.
Doses are usually approximately 0.4grams per kilogram of body weight. This means that for a 25 kg (55 pound)child, 10.0 grams will be infused. As achild grows, the dose has to be recal-culated each year based on the cur-rent weight. This is an important partof management.
The time needed for the infusionvaries from patient to patient. If it isthe first infusion, it will be given moreslowly initially and then the rate ofthe infusion will be increased overtime. The infusion will probably takeseveral hours. Some patients experi-ence side effects like headache, fever,nausea, vomiting, and chills if theinfusion is given too fast for them.Hydration, slower rates of infusionand the use of pre-medications such asanti-histamines or steroid medicinesmay help alleviate these side effects.
Record keeping is critical. The product name, lot number (a uniqueidentifier), and date of expirationshould be recorded for each infusion.The doctor or hospital chart is a con-sistent and logical place to keep theinformation. In addition, some patientskeep this information in their personalmedical diary. This information is veryimportant if a manufacturer or theFood and Drug Administration decidethat there is a problem with a particu-lar brand or lot number. Knowing thename of the product and the lot num-bers can assist patients and families toCopyright © 2003 by the Immune Deficiency Foundation
The Immune Deficiency Foundation is a publicly supported tax-exempt organization as described under Section 501(C)(3)of the Internal Revenue Code of 1954, as amended.
continued on page 3
IGIV continued from page 1
w20410 6/19/03 2:16 PM Page 2
I D F A D V O C A T E PAGE 3
determine quickly if they may beaffected. An easy way to learn of these types of problems is to registerfor the National Notification System.This can be done online at www.notify1.com; by telephone at 1-888-UPDATE-U.
Safety InformationThe plasma that is the source of the
immunoglobulin is collected fromdonors who undergo questioning aboutrisk behaviors and medical problemsthat are associated with certain bloodborne diseases, who are examined medically, and whose donations areevaluated in the laboratory usingsophisticated techniques like NucleicAcid Testing (NAT). NAT actuallyidentifies whether or not a particularvirus is present in a plasma pool that is being considered for use in the
manufacture of IGIV.The purification process known as
Cohn-Oncley fractionation, or its modifications, uses alcohol, which caninactivate potentially contaminatingviruses. In addition, all manufacturersuse dedicated viral inactivation orremoval techniques that have beenshown to be very robust. These techniques include: Acidification,Caprylate, Nanofiltration,Pasteurization, PEG-Bentonite, Pepsin exposure, Solvent-DetergentTreatment, and Trypsin exposure.
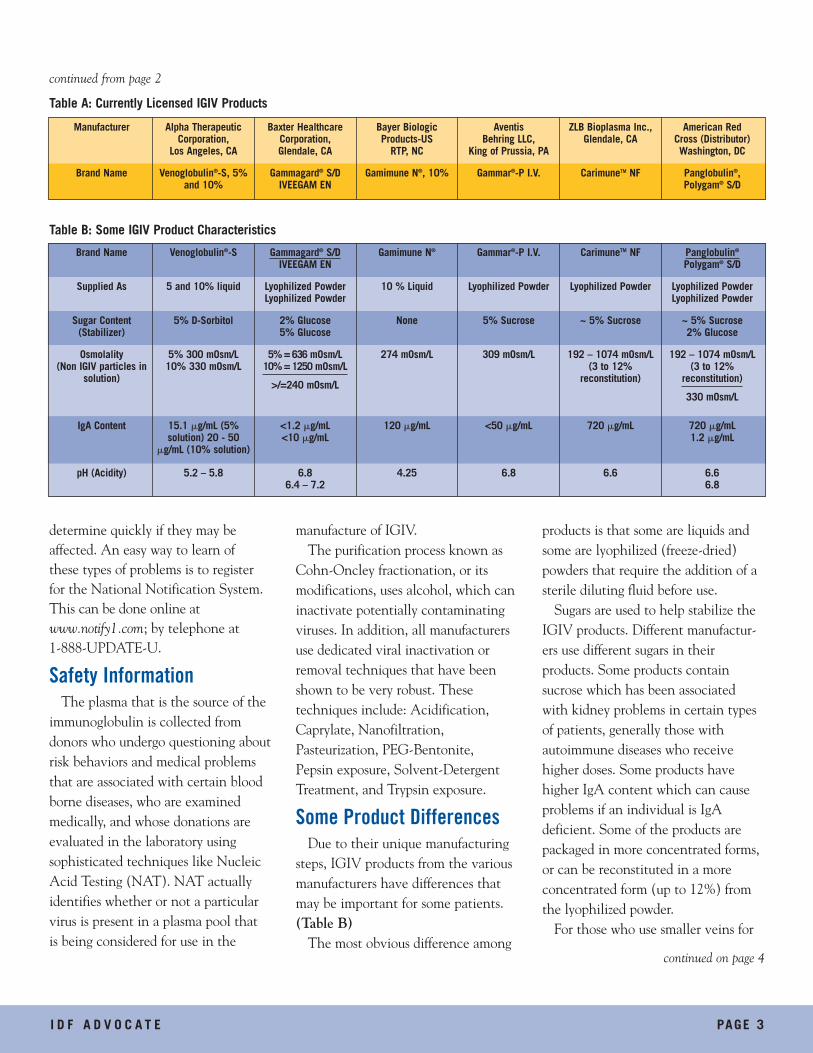
Some Product Differences Due to their unique manufacturing
steps, IGIV products from the variousmanufacturers have differences thatmay be important for some patients.(Table B)
The most obvious difference among
products is that some are liquids andsome are lyophilized (freeze-dried)powders that require the addition of asterile diluting fluid before use.
Sugars are used to help stabilize theIGIV products. Different manufactur-ers use different sugars in their products. Some products containsucrose which has been associatedwith kidney problems in certain typesof patients, generally those withautoimmune diseases who receivehigher doses. Some products havehigher IgA content which can causeproblems if an individual is IgA deficient. Some of the products arepackaged in more concentrated forms,or can be reconstituted in a more concentrated form (up to 12%) fromthe lyophilized powder.
For those who use smaller veins for
Manufacturer Alpha TherapeuticCorporation,
Los Angeles, CA
Baxter Healthcare Corporation,Glendale, CA
Bayer BiologicProducts-US
RTP, NC
Aventis Behring LLC,
King of Prussia, PA
ZLB Bioplasma Inc.,Glendale, CA
American Red Cross (Distributor)Washington, DC
Brand Name Venoglobulin®-S, 5%and 10%
Gammagard® S/DIVEEGAM EN
Gamimune N®, 10% Gammar®-P I.V. CarimuneTM NF Panglobulin®,Polygam® S/D
Table A: Currently Licensed IGIV Products
Brand Name Venoglobulin®-S Gammagard® S/DIVEEGAM EN
Gamimune N® Gammar®-P I.V. CarimuneTM NF Panglobulin®
Polygam® S/D
Supplied As 5 and 10% liquid Lyophilized PowderLyophilized Powder
10 % Liquid Lyophilized Powder Lyophilized Powder Lyophilized PowderLyophilized Powder
Sugar Content(Stabilizer)
5% D-Sorbitol 2% Glucose5% Glucose
None 5% Sucrose ~ 5% Sucrose ~ 5% Sucrose2% Glucose
Osmolality(Non IGIV particles in
solution)
5% 300 mOsm/L10% 330 mOsm/L
5% = 636 mOsm/L10% = 1250 mOsm/L
>/=240 mOsm/L
274 mOsm/L 309 mOsm/L 192 – 1074 mOsm/L (3 to 12%
reconstitution)
192 – 1074 mOsm/L(3 to 12%
reconstitution)
330 mOsm/L
IgA Content 15.1 �g/mL (5% solution) 20 - 50
�g/mL (10% solution)
<1.2 �g/mL<10 �g/mL
120 �g/mL <50 �g/mL 720 �g/mL 720 �g/mL1.2 �g/mL
pH (Acidity) 5.2 – 5.8 6.86.4 – 7.2
4.25 6.8 6.6 6.66.8
Table B: Some IGIV Product Characteristics
continued on page 4
continued from page 2
w20410 6/19/03 2:16 PM Page 3

PAGE 4 I D F A D V O C A T E
Check out www.primaryimmune.org! The Immune Deficiency
Foundation launched a new web site this spring to celebrate Primary
Immunodeficiency Awareness Week. The new web site features the most
up-to-date information on primary immune deficiency diseases and IDF’s
programs and services. The web site offers expanded information on
health insurance, a new section on genetics and inheritance of primary
immune deficiency diseases, and an “In the News” section highlighting
research, IDF events and initiatives and other important information.
While visiting www.primaryimmune.org you can make a charitable
contribution to the IDF, access and download all IDF publications includ-
ing the Patient and Family Handbook, learn about recent IGIV recalls and
sign up for the Patient Notification System. If you are looking to chat
with others affected by primary immune deficiency diseases, you can
enter one of five password protected discussion forums.
The current forum topics include:
• Living as an Adult with a Primary Immune Deficiency Disease
• Parenting a Child with a Primary
Immune Deficiency Disease
• Experiences with Immune
Globulin Therapy
• Coping with a New Diagnosis
• Teen Talk: Teens living with
a Primary Immune Deficiency
Disease.
IDF Launches New Web Sitecontinued from page 3
infusions, products that are moreacidic (lower pH) may be less well tolerated. Also some products mayhave more non-IGIV substances dis-solved in the solution such as sodium.For some patients, products with ahigher osmolality may cause problemsduring infusion. Normal serum osmo-lality, a measure of these particles insolution in blood, is 285-290 mOsm/L.Products range from 192 to 1074mOsm/L.
Recommended rates of infusion ofthe various products vary somewhat.All should be administered at the lowest rate of infusion for the initialinfusion and then at a faster rate basedon how well the patient tolerates theinfusion.
The differences in the IGIV products may be important for somepatients. Patients should consult withtheir treating physicians to see if thesedifferences are important for them.
IGIV products are a life-saving treat-ment for those with primary immunedeficiency diseases. Their availabilityhas helped thousands of affected indi-viduals to better health and a betterlife. The products currently availableand on the near horizon offer choicesas well as safety improvements. ■ We encourage you to log on today!
The IDF web site is sponsored by an educational grant from BayerCorporation.
www.primaryimmune.org
w20410 6/19/03 2:16 PM Page 4
I D F A D V O C A T E PAGE 5
1909-2003“The patient is first — and last always”
-Colonel Ogden C. Bruton, M.D.
Founder of Clinical Immunology RememberedThe Immune Deficiency Foundation is sad to acknowledge the death
of Colonel Ogden C. Bruton, M.D. earlier this year. Colonel Bruton was
widely respected in the medical community as a pediatrician, educator
and especially for the discovery and treatment of Agammaglobulinemia.
In 1952, Colonel Bruton first described X-Linked Agammaglobulinemia
(XLA). This disease is sometimes called Bruton’s Agammaglobulinemia, in
his honor, or Congenital Agammaglobulinemia. The disease is an inherited
immunodeficiency disease in which patients lack the ability to produce
antibodies that make up the gamma globulin fraction of blood plasma.
This monumental discovery became the stimulus for further studies in
fields such as infectious disease, immunology and genetics. He gained
recognition as a founder of clinical immunology which has impacted
medical fields as diverse as immunization practices and bone marrow
transplantation.
A native of North Carolina, Colonel Bruton received many military,
medical and humanitarian honors and medals including recognition from
the Immune Deficiency Foundation for his breakthrough discoveries in
the field of immunology. An ardent advocate for children, Dr. Bruton
will be remembered for his important contributions to medicine and his
caring nature.
Please watch your mailbox for the IDF Advocate Special Issue, which provides more information aboutIDF’s first endowment and capitalcampaign, For Today and FutureGenerations, chaired by Founder
Marcia Boyle. We encourage you to give serious consideration to the many benefits thecampaign will enable IDF to provide, today and in the future, and to make a commitmentto supporting IDF in this vital initiative.
w20410 6/19/03 2:16 PM Page 5
PAGE 6 I D F A D V O C A T E
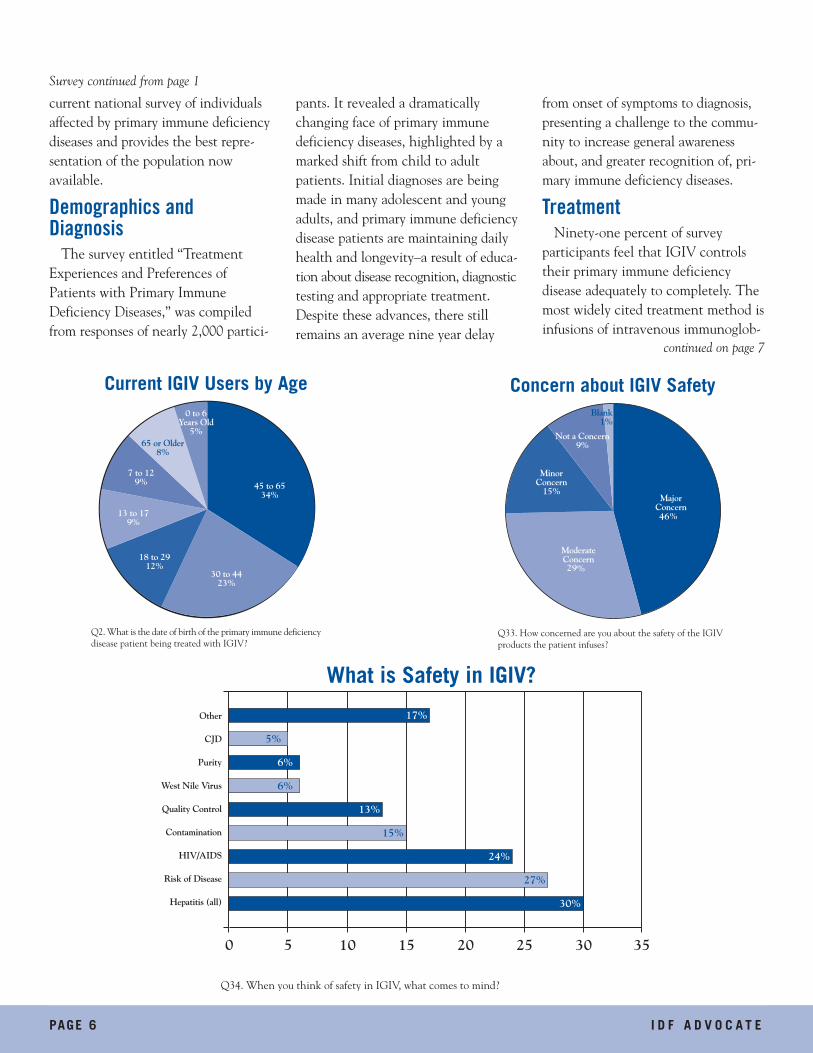
current national survey of individualsaffected by primary immune deficiencydiseases and provides the best repre-sentation of the population now available.
Demographics andDiagnosis
The survey entitled “TreatmentExperiences and Preferences ofPatients with Primary ImmuneDeficiency Diseases,” was compiledfrom responses of nearly 2,000 partici-
pants. It revealed a dramaticallychanging face of primary immunedeficiency diseases, highlighted by amarked shift from child to adultpatients. Initial diagnoses are beingmade in many adolescent and youngadults, and primary immune deficiencydisease patients are maintaining dailyhealth and longevity–a result of educa-tion about disease recognition, diagnostictesting and appropriate treatment.Despite these advances, there stillremains an average nine year delay
from onset of symptoms to diagnosis,presenting a challenge to the commu-nity to increase general awarenessabout, and greater recognition of, pri-mary immune deficiency diseases.
TreatmentNinety-one percent of survey
participants feel that IGIV controlstheir primary immune deficiency disease adequately to completely. Themost widely cited treatment method isinfusions of intravenous immunoglob-
Survey continued from page 1
29
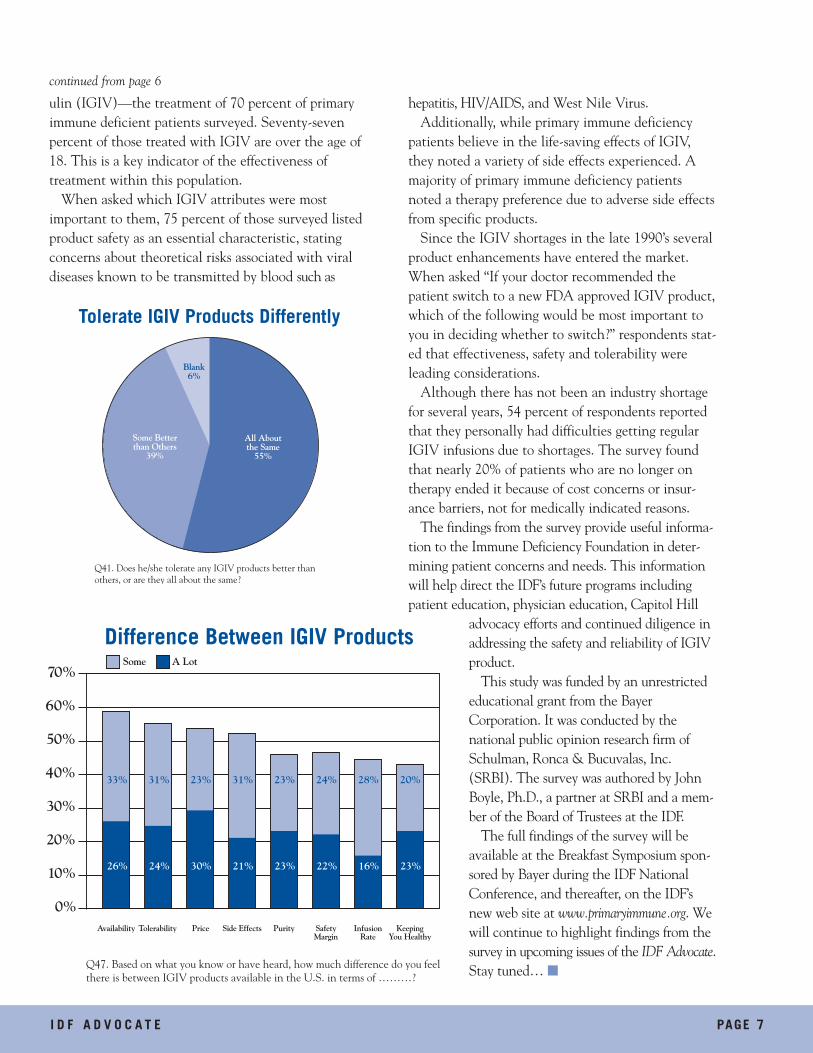
46
continued on page 7
w20410 6/19/03 2:16 PM Page 6
I D F A D V O C A T E PAGE 7
ulin (IGIV)—the treatment of 70 percent of primaryimmune deficient patients surveyed. Seventy-sevenpercent of those treated with IGIV are over the age of18. This is a key indicator of the effectiveness of treatment within this population.
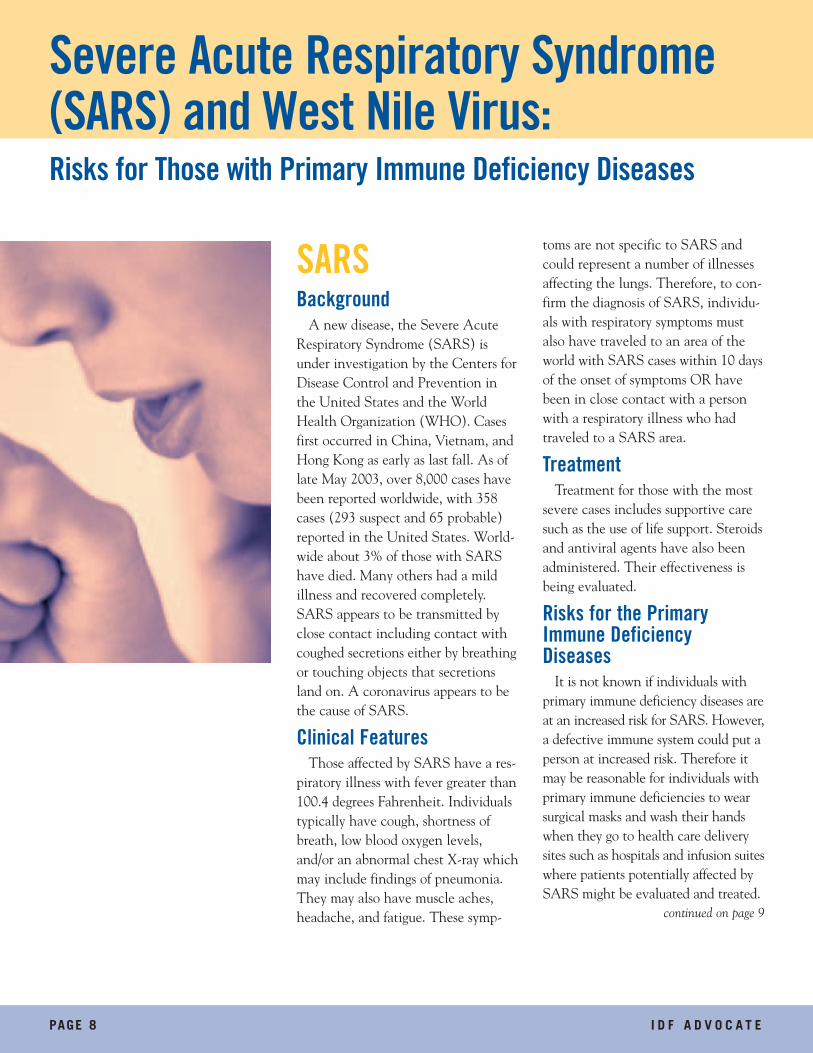
When asked which IGIV attributes were most important to them, 75 percent of those surveyed listedproduct safety as an essential characteristic, statingconcerns about theoretical risks associated with viraldiseases known to be transmitted by blood such as
hepatitis, HIV/AIDS, and West Nile Virus.Additionally, while primary immune deficiency
patients believe in the life-saving effects of IGIV,they noted a variety of side effects experienced. Amajority of primary immune deficiency patientsnoted a therapy preference due to adverse side effectsfrom specific products.
Since the IGIV shortages in the late 1990’s severalproduct enhancements have entered the market.When asked “If your doctor recommended thepatient switch to a new FDA approved IGIV product,which of the following would be most important toyou in deciding whether to switch?” respondents stat-ed that effectiveness, safety and tolerability wereleading considerations.
Although there has not been an industry shortagefor several years, 54 percent of respondents reportedthat they personally had difficulties getting regularIGIV infusions due to shortages. The survey foundthat nearly 20% of patients who are no longer ontherapy ended it because of cost concerns or insur-ance barriers, not for medically indicated reasons.
The findings from the survey provide useful informa-tion to the Immune Deficiency Foundation in deter-mining patient concerns and needs. This informationwill help direct the IDF’s future programs includingpatient education, physician education, Capitol Hill
advocacy efforts and continued diligence inaddressing the safety and reliability of IGIVproduct.
This study was funded by an unrestricted-educational grant from the BayerCorporation. It was conducted by thenational public opinion research firm ofSchulman, Ronca & Bucuvalas, Inc.(SRBI). The survey was authored by JohnBoyle, Ph.D., a partner at SRBI and a mem-ber of the Board of Trustees at the IDF.
The full findings of the survey will beavailable at the Breakfast Symposium spon-sored by Bayer during the IDF NationalConference, and thereafter, on the IDF’snew web site at www.primaryimmune.org. Wewill continue to highlight findings from thesurvey in upcoming issues of the IDF Advocate.Stay tuned… ■
continued from page 6
w20410 6/19/03 2:16 PM Page 7
PAGE 8 I D F A D V O C A T E
SARSBackground
A new disease, the Severe AcuteRespiratory Syndrome (SARS) isunder investigation by the Centers forDisease Control and Prevention inthe United States and the WorldHealth Organization (WHO). Casesfirst occurred in China, Vietnam, andHong Kong as early as last fall. As oflate May 2003, over 8,000 cases havebeen reported worldwide, with 358cases (293 suspect and 65 probable)reported in the United States. World-wide about 3% of those with SARShave died. Many others had a mild illness and recovered completely.SARS appears to be transmitted byclose contact including contact withcoughed secretions either by breathingor touching objects that secretionsland on. A coronavirus appears to bethe cause of SARS.
Clinical FeaturesThose affected by SARS have a res-
piratory illness with fever greater than100.4 degrees Fahrenheit. Individualstypically have cough, shortness ofbreath, low blood oxygen levels,and/or an abnormal chest X-ray whichmay include findings of pneumonia.They may also have muscle aches,headache, and fatigue. These symp-
toms are not specific to SARS andcould represent a number of illnessesaffecting the lungs. Therefore, to con-firm the diagnosis of SARS, individu-als with respiratory symptoms mustalso have traveled to an area of theworld with SARS cases within 10 daysof the onset of symptoms OR havebeen in close contact with a personwith a respiratory illness who hadtraveled to a SARS area.
TreatmentTreatment for those with the most
severe cases includes supportive caresuch as the use of life support. Steroidsand antiviral agents have also beenadministered. Their effectiveness isbeing evaluated.
Risks for the PrimaryImmune DeficiencyDiseases
It is not known if individuals with primary immune deficiency diseases areat an increased risk for SARS. However,a defective immune system could put aperson at increased risk. Therefore itmay be reasonable for individuals withprimary immune deficiencies to wearsurgical masks and wash their handswhen they go to health care deliverysites such as hospitals and infusion suiteswhere patients potentially affected bySARS might be evaluated and treated.
continued on page 9
Severe Acute Respiratory Syndrome(SARS) and West Nile Virus:Risks for Those with Primary Immune Deficiency Diseases
w20410 6/19/03 2:16 PM Page 8
I D F A D V O C A T E PAGE 9
West Nile VirusAs summer approaches, it is time to prepare for West Nile
Virus. West Nile Virus is spread by mosquitoes and infection with the virus can cause severe and sometimesfatal illness. Older individuals and those with underlying ill-nesses including immune deficiency seem to be at increasedrisk for the more severe complications of infection. Theseclinical signs of infection range from none to fever, nausea,vomiting, flu-like symptoms as well as meningitis andencephalitis (inflammations of the covering of the brain andof the brain itself). It has therefore become important toincrease our understanding of the virus and its potentialimpact on those with primary immune deficiency diseases.
Current CasesThe CDC reports over 4,000 cases of West Nile diseases in
the United States during 2002, including 284 deaths. It islikely that all mainland states in the United States will seeWest Nile Virus activity in 2003. As of May 2003, Alabama,Florida, Georgia, Louisiana, Michigan, Minnesota,Mississippi, North Carolina and Pennsylvania have reportedverified cases of avian, animal or mosquito infections ofWest Nile Virus.
Safety of IGIV An important question for those with primary immune
deficiency diseases is if IGIV could be contaminated with West Nile Virus. The good news is that there appears to belittle to no risk for transmission of West Nile Virus throughthe use of IGIV for several reasons:• Potential blood and plasma donors with West Nile Virus
may be ill with fever and would not be allowed to donate• There is only a small chance that an infected person would
have virus in the blood stream• Viral inactivation techniques used on all IGIV products
including pasteurization and solvent detergent treatmenthave been shown by manufacturers to inactivate the West Nile Virus.
Reducing the Risk of ExposureFor everyone including those with a primary immune defi-
ciency disease, the best way to avoid the West Nile Virus isto avoid exposure to mosquitoes. Some ways to accomplishthis are:• Reduce time outdoors, especially in the early evening hours• Wear long pants and long sleeved shirts• Apply mosquito repellent containing DEET
(N,N-diethyl-m-toluamide) to exposed skin areas following the manufacturer’s recommendations for dosing frequency, application, and clean-up.
Public health authorities have also undertaken measures to destroy mosquito habitats and to spray insecticides thatkill mosquitoes.
There seems to be little risk posed to individuals with primary immune deficiency disease from the West Nile Virusthrough the use of IGIV therapy. However, individuals face the same risks as the general population if bitten by aninfected mosquito. Those with severe signs of infection aretreated using supportive measures. There is active research inthe area of vaccine development.
For the latest information on SARS and West Nile Virus,visit the CDC’s web site at www.cdc.gov. ■
continued from page 8
w20410 6/19/03 2:16 PM Page 9

PAGE 10 I D F A D V O C A T E
When Katharine Austin’s grandsonMark was diagnosed with CD-5/CD-9primary immune deficiency at age three,she asked herself only one question:“How can I help?” Like many people,Katharine had no knowledge ofprimary immune deficiency diseases,their symptoms, or treatment options.Instinct told her that public knowledgeof these diseases would help lead toadvancements in treatment and a cure.Katharine decided the answer to howshe could help was by becoming aproactive part of her grandson’s treatment.
From the beginning, Katharine hada special relationship with Mark that
went beyond her role as a grandmother.She served as Mark’s confidant, helpinghim cope with his illness, school issues,and IGIV treatments. The two sharedspecial time together away from thestresses of primary immune deficiencydisease, when they ate fast food andtalked about his problems.
As Mark grew older and IGIV treat-ment became more frequent, Katharinededicated her time to learning aboutthe disease and helping the familycope with Mark’s illness. When hereceived his monthly IGIV therapy,Katharine brought dinner for the familyand for the nurses who administered
his treatment. Over the years, Katharine became
an advocate for raising awarenessabout the IDF and generating funds tohelp researchers find a cure for primaryimmune deficiency diseases, and forMark. She spoke with local reporters,urging them to write articles that wouldhelp raise awareness for these diseasesthat kept her grandson home fromschool for weeks at a time. At church,she encouraged fellow parishioners togive donations to the IDF.
Last spring Katharine unexpectedlypassed away. As her final wish sheinsisted that instead of sending flowersand food to her family, that loved onesdonate money to the IDF in her memory.The idea for the legacy fund was born.
Katharine’s family has dedicatedMay 19 as Katharine & Mark AustinLegacy Fund Day and every year on thisday her family will conduct a specialfundraising drive to raise money forprimary immune deficiency educationand awareness.
“Katharine was incredibly passionateabout primary immune deficiencydiseases. She gave in so many ways tohelp advance treatments and educatethe public about these diseases. Givingto a legacy fund became the mostappropriate way to honor her life, herspirit and her gifts to the primaryimmune deficiency community,” saidAutumn Austin, about her mother-in-law’s efforts.
“Katharine kept up to date on thelatest medical treatments; she stead-fastly believed that raising money tobenefit research for a cure was a vitalcomponent in helping my son lead a
“Happiness Starts Here”Family honors loved one through gift of hope for finding a cure
continued on page 11
w20410 6/19/03 2:16 PM Page 10
normal life,” continued Ms. Austin, “She would bepleased to have her love for Mark honored in this way.”
Mark, who is now 13, and his family further commemorated Katharine’s endless efforts to help the primary immune deficient community by planting agarden in her honor. A polished stone bears a plaque quotingKatharine’s life-long credo: “Happiness Starts Here.”
If you would like to set up a legacy fund in the name ofsomeone you love to benefit the primary immune deficiencycommunity, please contact the IDF.
I D F A D V O C A T E PAGE 11
Gifts In Memory OfKatharine AustinSophie ChaitJeannine ClineVincent GentilomaStanley LiebovitzEric MarderBruce MartinDonald MichaelPaula OdleDominick Passalacqua Jr.Arene Agnes RichardsonLawrence TrottiFlorence Wehrlin
Gifts In Honor OfMark AustinCamela Sue ColeMary FratantuonoJessica GrabowskiVictoria Alexandra HayesRyan Eric MarderLainey MeekinsMallory PaigeJeannette PuretzJasmine RaeMr. & Mrs. Wil RomanoffThomas SmithNeil SteinMatthew StoweJane Ulig
Philanthropy
Second National ConferenceThe Immune Deficiency Foundation will host its SecondNational Conference in Baltimore, Maryland on June 19-21,2003. We have reached our goal and more than 1,000 individuals affected by primary immune deficiency diseases, leading clinical immunologists, nursing professionals, andgovernment and industry resentatives have registered toattend the three-day conference. Event highlights will be post-ed on the IDF web site in the weeks following the conference.
IDF would like to acknowledge the generous sponsorship ofour industry partners:
Platinum SponsorsAventis BehringBaxter Healthcare CorporationBayer CorporationFFF Enterprises, Inc.Grifols
Gold SponsorsAlpha Therapeutic CorporationAmerican Red CrossOctapharma AGZLB Bioplasma Inc.
Specific Event SponsorshipsAmerican Red Cross Breakfast Symposium, June 21
Aventis Behring Badge Necklaces
Baxter Healthcare Corporation Box Lunches, June 20 & 21
Bayer Corporation IDF Extravaganza at Pier 6Breakfast Symposium, June 20
Dean Family Foundation Scholarships
Dyax Corporation Breakfast Symposium, June 21
First Union/Wachovia Bank Continental Breakfast, June 20 & 21
Grifols Opening ReceptionYouth ProgramCoffee Breaks
Infusion Systems, Inc. Scholarships
ZLB Bioplasma Inc. Registration BagsBreakfast Symposium, June 21
N A T I O N A LC O N F E R E N C E
Immune Deficiency Foundation
continued from page 10
w20410 6/19/03 2:16 PM Page 11
Mark your CalendarsIDF National Conference 2005
IDF is planning to hold its Third National Conference June 23-25, 2005 in Orlando, Florida.
Local ProgramsThe Immune Deficiency Foundation is planning educational andsupport meetings this summer in the following communities. Formore information on the meetings, call the IDF at 800-296-4433.
Madison, WisconsinJuly 12, 2003Chesire, ConnecticutJuly 13, 2003
Albuquerque, New MexicoAugust 9, 2003Cleveland, OhioAugust 9, 2003
IDF BOARD OF TRUSTEESG. Richard Barr, M.D. Chairman
Kathy Crews, Vice-Chairman
Marcia Boyle, FounderSecretary
Katherine AntillaBarbara BallardDouglas BellJohn Boyle, Ph.D.
Rebecca Buckley, M.D. Chairman, Medical Advisory Committee
Carol Ann DemaretRobert LeBienPatrick SchmidtJerry Winkelstein, M.D.
Thomas L. Moran, President
CHAMPIONS CIRCLE OF SUPPORTAlpha TherapeuticCorporation
American Red Cross
Aventis Behring
Baxter HealthcareCorporation
Bayer Corporation
FFF Enterprises, Inc.
ZLB Bioplasma Inc.
The Champions Circle consists of organizationscommitted to supporting IDF at the highestlevel. The Circle provides vital resources tofulfill the vision, mission, and core services ofthe Immune Deficiency Foundation.
Immune Deficiency Foundation40 West Chesapeake AvenueSuite 308Towson, Maryland 21204
Non-profit Org.U.S.Postage
PAIDBaltimore,MD
Permit No.6936
Address service requested
w20410 6/19/03 2:16 PM Page 12