Embed Size (px)
Citation preview

Research in Nursing ond Heolth, 1979, 2, 61 -72
Nurses’ and Physicians’ Performance on Clinical Simulation Test:
Hypertension Frank E. McLaughlin, Thomas Cesa, Harold Johnson, Mary Lemons,
Sara Anderson, Patricia Larson, and Josephine Gibson
The purpose!, of this study were to determine whether nurse practitioners with a master’s degree (NPM), nurse practitioners with a certificate (NPC), and public health nurses (PHN) pc,rform as proficiently as family practice physicians (FPP) in assessing and managing essential hypertension and whether the four groups use a psychosocial or pathophysiological model in providing care. Subjects included 30 FPPs, 30 NPMs, 33 NPCs, and 40 F’HNs. A clinical simulation test required subjects to collect data, identify problems, interpret tests, and formulate care plans. Criterion test performance was es- tablished by eight expert nurses and physicians. Physicians and nurse practitioners were equally proficient, and public health nurses were significantly less proficient on only 3 of 1 1 test sections. Sharpest contrasts were in test interpretation, with FPPs clearly more expert. FPPs’ practice style was less psychosocial but not more pathophysiological than that of the nurse practitioners. The study suggests that, except for nurses’ greater use of a psychosocial model, expanded role nurses and physicians perform similarly in assessing and managing hypertension and that, with slightly more training, PHNs could perform com para b I y
The inability of the traditional health care system to meet the present high demand for health services is well known. Equally known are the contributing factors, including an increased life expectancy and the result- ing greater proportion of people who have chronic health problems, an increased number and variety of treatments because of technological advances, an increased public recognition that everyone has a right to health care, and a maldistribution of health practitioners.
During the past few years, expanding the role of the nurse has been viewed as one an- swer to the problenis of distribution and availability ofprimary health care (ANA, 1973; DHEW, 1972). In particular, the use of spe- cially prepared nurses in the management of long-term health problems has gained con- siderable support (DHEW, 1972: Kodadek, 1976: Spitzer, Harth, Goldsmith, Norman, Dickie, Bass, & Newell, 1976; Twaddle, 1968).
Since the first published reports on the
preparation of nurses to function in ex- panded roles (Ford, Seacat, & Silver, 1966; Ford & Silver, 1967; Lewis & Resnik, 1967; Silver, Ford, & Stearly, 1967), much has been written on the number of practitioners completing programs, their work locations, and the satisfaction of physicians, nurses, and patients with their services (Andrews, Yankauer, & Connelly, 1970: Day, Egli, & Silver, 1970: Hoekelman, 1972: Lewis, Res- nik, Schmidt, & Waxman, 1969; Pickard & Watkins, 1977; Sackett, Spitzer, Gent, & Robbins, 1974; Sultz, Zielezny, & Kinyon, I 976).
Reports in the literature support three gen- eral conclusions about nurse practitioners: (a) that patients are satisfied when nurses give primary care (Day et al., 1970: Hoekel- man, 1972; Lewis & Resnik, 1967; Lewis et al., 1969; Linn, 1975b); (b) that first contact decisions, preventative care, and manage- ment of stabilized long-term illnesses can be safely provided by nurses (Cheyovitch, Lewis, & Gortner, 1976; Moore, Barber,
This research was supported by Division of Nursing, DHEW, Grant NU00528
@ 1979 Wiley 0160-6891/79/020061-12 $01.00 61

62 RESEARCH IN NURSING AND HEALTH
Robinson, & Taylor, 1973; Sackett et al., 1974); and (c) that primary care given by nurses can be economically feasible for both the agency and the recipients (Baker, Soper, Kearnes, Farrisey, & Goldfinger, 1973; Spitzer, Sackett, & Sibley, 1974). In the Kaiser-Permanente health care system, cost comparisons showed that primary health services provided by nurse practitioners to patients with chronic disease were less ex- pensive than those provided by physicians (Feldman, Taller, Garfield, Collen, Richart, Cella, & Sender, 1977).
Investigators have also reported a detailed evaluation of the outcomes of clinical care rendered by physicians and nurse practition- ers in primary care practice (Sackett et al., 1974; Spitzer et al., 1974). These outcomes of effectiveness and safety, expressed in rela- tion to physical, emotional, and social func- tions, showed similar levels for two groups of patients who received care for 1 year from either a nurse practitioner or a physician.
Other investigators have proposed that be- cause of education and prior practice, the nurse brings to the practitioner role special nursing skills in patient education, psycho- social assessment, and caring for the patient as a whole. Because of these special skills, the nurse practitioner’s work should prove complementary, rather than just substitutive, to that of the physician (Linn, 1974, 1975a; Pritchard, 1974). Some researchers have stated that the public health nurse, who has long served in a similar complementary role, is the generalist best prepared to offer pri- mary care in a structured health care team (Brunetto & Birk, 1972).
At the time this study was initiated, around 1975, the literature on nurse practitioners consisted mainly of retrospective studies and anecdotal accounts. There had been no in- vestigation of the quality of care provided by nurse practitioners in relation to their per- formance as they participated in the primary care process. Therefore, it was believed that there was a need for an empirical study to examine the performance of nurse prac- titioners as they gather information, evaluate and interpret it, and make patient care deci- sions, as well as whether or not their care emphasizes psychosocial components and thus might be considered complementary.
In designing this study, the following as- sumptions were made: The sequence of be- haviors that are effective in diagnosing and managing chronic disease consists of data-
gathering, information-proce ssing , decision- making, and evaluating. To perform this se- quence of behaviors proficiently, one must have a knowledge base of both patho- physiological and psychosocial components of health and disease, and one must be capable of making decisions and taking risks. These qualifications are derived from syste- matic scientific education and clinical train- ing experiences.
Although physicians receive the neces- sary pathophysiological and decision-making training as a routine part of their basic education, nurses do not. Nurses, however, receive more training in psychosocial compo- nents of health and illness than do physi- cians. To prepare to function in the expanded role in primary health care, registered nurses need an educational program that increases both their pathophysiological knowledge and their ability to make decisions and take risks. After completing such a program, nurse practitioners may be equally well prepared in both areas of health care. Although they have not received formal training beyond their basic education to increase their sci- entific knowledge, public health nurses who have provided care to patients over time and who function somewhat independently may already possess the necessary decision- making and risk-taking capabilities.
The purposes of this study were to deter- mine (a) whether formal training programs prepare nurse practitioners to perform at a level comparable to that of family practice physicians in rendering primary care, (b) whether registered nurses who have not had practitioner training but who have been functioning as public health nurses perform at a level comparable to that of formally pre- pared nurse practitioners and family practice physicians, and (c) whether both nurse prac- titioners and public health nurses emphasize psychosocial aspects of care more than do physicians.
The study, therefore, was designed to measure and compare the performance of four groups of health professionals on a clini- cal simulation test based on a systems theory and problem-oriented model of the clinical process. The criterion performance on the test was derived from the performance of an expert panel. The four groups consisted of family practice physicians (FPPs), nurse practitioners with a master’s degree (NPMs), nurse practitioners with a certificate (NPCs), and public health nurses (PHNs). Essential

CllNlCAL SIMULATION TEST PERF1
hypertension was used as the simulated chronic disease problem.
Subject performance was determined ac- cording to three scales: (a) proficiency in providing primary care, (b) psychosocial scores, and (c) pathophysiological scores. It was evaluated on two dimensions: (a) how closely performance matched that of an ex- pert panel and (b) how much Performance reflected psychosocial versus pathophysio- logical emphasis. Hypotheses 1, 2, 5, and 7 were stated in terms of no differences because of the additional education of NPNs and NPCs (Keppel, 1973).
The hypotheses, as they pertain to the three scales, are given below.
ProJicirncy Sccrlr: H I : FPPs’ proficiencl, scores will not differ
from those of NPMs or from those of NPCs.
H2: NPMs’ proficiency scores will not differ from those of NPCs.
H3: PHNs’ proficiency scores will be significantly lower than those of FPPs, NPMs, and NPCs.
Psyclzosociril Sralr : H4: FPPs’ psychosocial scores will be
significantly lower than those of N P M s , NPCs, and PHNs.
H5: NPMs’ psychosocial scores will not differ from those of NPCs and PHNs .
Pii tlr o p h y siolog icii 1 Sc .d P : H6: FPPs‘ pathophysiological scores will be
significantly higher than those of NPMs, NHCs, and PHNs.
H7: NPMs’ pathophysiological scores will not differ from those of NPCs.
€18: PHNs’ pathophysiological scores will be significantly lower than those of NPMs and NPCs.
Definition of Key Terms
“Proficiency” in providing primary care was a measure of skill in performance as com- pared to expert performance. The subjects’ responses to a test requiring the gathering of data, the identification of problems, the interpretation of data and diagnostic tests, and the formulation of treatment plans were considered representative of performance.
“Psychosocial” refers to the patient’s relationships with people, family and job situations, financial considerations. and rec- reational and exercise patterns. Patient edu- cation was considered psychosocial even if
3RMANCE / McLAUGHLlN ET AL 63
the interaction concerned pathophysiological content.
“ Pathophysiological” refers to the disease process itself, including laboratory tests, physical examinations, the specification and alteration of medication strategies, and the performance of invasive or surgical proce- dures.
METHOD
lnstrumenf
Theoretical basis. Since no comprehen- sive clinical simulation test for the manage- ment of essential hypertension was available, it was necessary to construct one. The theoretical basis for development of this tool was a combination of systems theory and the problem-oriented approach described by Weed (1971). The work of Howland and McDowell (1964), who conceptualized pa- tient care in relation to a systems mode, and of Chow (1969), who developed a systems approach for identifying and categorizing nursing actions, provided background for this tool.
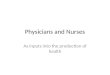
As the health practitioner uses knowledge of the physical and emotional components of the disease process in the systematic as- sessment and management of chronic dis- ease. the practitioner is thought to follow a model such as that depicted in Figure I (the Clinical Process Decision Model); this model includes the concepts of Weed (1971) and of Bailey and Claus (1975). The Clinical Process Decision Model incorporates a holistic view of man and a comprehensive approach to pa- tient management in which the results are continually evaluated and fed back into the system for adjustment. The model reflects a data-gathering, information-processing, deci- sion-making, and evaluating sequence of behaviors.
Also depicted in the model are constraints and capabilities that may hamper or facilitate the decision sequence. Constraints include legal. institutional, and environmental bar- riers: inadequate money and time; and in- hibiting patient characteristics. Capabilities include the influences. such as financial sup- port, practitioner expertise, and support systems, that enable the provision of care.
Content development. To operationalize the Clinical Process Decision Model into a clinically meaningful, relevant: and realistic testing device, several steps were taken.
First, baseline information on essential

Const
rain
ts a
Pre
sent
i ng
D
ata
pro
ble
m
colle
ctio
n
com
pla
int)
ob
i ect
i ve)
(s
ubie
ctiv
e,
(chie
f -
Ca
pa
bi I i
ties a
I
- P
lan
of c
are
z
of e
I e m
en
ts)
ed
uca
tion
) Z
psyc
hoso
cial
) p
rio
ritie
s)
0
Pro
ble
m
An
aly
sis
of
ide
ntif
ica
- a
ltern
ativ
es
Co
ntr
ol
tion
(p
ath
o-
- ph
ysio
log
ica
l, p
atie
nt
z (p
rob
lem
go
al, d
tre
atm
en
t, - (co
rre
ctio
n
Res
ults
5 v,
(dia
gn
osi
s,

CLINICAL SIMULATION TEST PERFORMANCE / McLAUGHLlN ET At. 65
hypertension, including its pathophysiologi- cal and emotional components, clinical problems, and management strategies, was culled from up-to-date medical and nursing texts, general health care literature, and symposia. Next, the project staff received special training in physical examination and clinical patient interview procedures.
After this preparation, the staff wrote a script for a patient interview that was to be videotaped, and developed the written test materials for a test booklet. The script and test booklet were revised several times, until they were ready for critique by expert local practitioners. Finally, 10 such practitioners, four physicians. and six nurse practitioners were asked to review the materials; their suggestions for additions and deletions were incorporated.
The final test materials were designed to approximate the actual sequence involved in assessing and managing health problems. These materials consisted of a 15-minute videotaped patient interview and a related test booklet containing about 600 possible items. The booklet covers three major areas: (a) data collection, (b) problem identification, and (c) care plans (treatment and manage- ment). These major areas include the fol- lowing 11 specific sections: Elicit Patient History, Assessment of Patient History, Physical Examination, Clinical Laboratory Studies, Tentative Problem List, Actual Problem List, and Patient Visits 1 Through 5.
The test’s sequence and content in brief are as follows:
Vitlrol(ipe--chie.f cornpictint. The first brief section of the videotape shows a patient and a health practitioner inan initialinterview. The patient is a 46-year-old Caucasian man who reports two recent episodes of chest pain associated with emotional upset.
The subject is re- quested to generate 10 pertinent questions to ask this patient and to rate each question’s importance on a scale of 1 to 7.
V ittoo trrlw -pn ti0 t i t his tory . The v id- eotaped interview continues with a review of body systems and the collection of data on pertinent negatives, family history, and life style. The intervie6, shows that the patient smokes cigarettes, leads a sedentary life, and has job-related stress.
The sub- ject is asked to summarize the patient’s sub- jective data and to rate the importance of each fact.
Elicit ptrtit.17t Iiistory.
Asscssrnrnt o f putirnt history.
Physicrrl esaminution. The subject re- ceives data on the patient’s initial visit vital signs, height, weight, and blood pressure. The data show that the patient is overweight and has an elevated blood pressure. The subject then receives a comprehensive list of physical examination procedures and is asked to select and rate the procedures most appropriate for this patient. Next, the subject receives a list of relevant physical examina- tion findings.
Firnditscopic examination. The subject receives a photographic reproduction of an eyeground and is asked for specific inter- pretative data about the eyeground.
Trntntive problPm l i s t . The subject is asked to list and rate the patient’s problems at this point.
Clinical luborritoiy stirdics. The subject is given a list of 37 possible diagnostic tests and is asked to select and rate those appro- priate for this patient. Then the subject re- ceives relevant clinical laboratory findings for the patient.
Chrst x-rrry crnd ECG. The subject is asked for specific interpretative data con- cerning a six-lead ECG recording and a photograph of a chest x-ray.
Actirtrl problem list. The subject is asked to list and rate the specific problems that he or she plans to manage.
Plun o j cur(’ (potirnt t9isits I throirgh 5) . The subject then manages the identified patient problems for a series of five simulated visits. Before each visit, the subject receives a summary of pertinent clinical findings, in- cluding diagnostic test results and interval history. For each visit, the subject is asked to select and rate appropriate treatment and management actions from a list of 51 possibte items and to decide on the time for the pa- tient’s next visit. After the fifth visit, the subject is asked for a narrative summary of follow-up plans and of the patient’s prog- nosis.
To establish the Proficiency Scale, which represents compe- tency of performance in primary care, and the Psychosocial and Pathophysiological Scales, which represent the mode of treat- ment characterized by each item, we se- lected a panel of four expert nurses and four expert physicians. These people were na- tionally known and were from the eastern, middle western, and western states.
We identified potential members of this panel by examining recent journals and
Development of scales.

66 RESEARCH IN NURSING AND HEALTH
textbooks for names of people who had pub- lished research or clinical papers on essential hypertension. A final list of 29 names was generated and all of these people were con- tacted by mail. The 12 people indicating willingness to participate were then asked to furnish curriculum vitae. These were exam- ined to determine each person’s degree of experience in the field, particularly in teach- ing and consultation, and to verify that each one had been providing primary care to pa- tients during the previous year. Final selec- tion was based on closeness of fit to criteria, geographic diversity, and mutually agreeable testing dates.
The expert panel participated in three pro- cedures. First, the panel members completed the clinical simulation tests as if they were study subjects. Each panelist selected test items and rated each item on a 1 (low) to 7 (high) scale of how beneficial the item would be for the simulated patient. Next, the panelists reviewed the test items. This time, they examined the items they had not se- lected during the test and rated each, on the same scale, for how detrimental the item would be for the patient. Finally, each panelist examined the test booklet a third time and, using the same scale, rated each item on the extent to which the item was psychosocial and the extent to which it was pathophysiological.
Mann-Whitney U statistical analysis showed that the expert nurses and physicians responded in a similar manner throughout the three procedures. Therefore, for the Proficiency Scale, their beneficial and det- rimental ratings were combined mathe- matically to provide a criterion score for each item. Their ratings of psychosocial and pathophysiological items were also com- bined mathematically to establish criterion- referenced items for the other two scales.
To assess reliabil- ity of the instrument, 33 of the study subjects ( 1 1 physicians and 22 nurses) were asked to take the test again 60 to 90 days after their initial testing. It was thought unlikely that these subjects would remember their initial responses to approximately 600 test items after this time lapse. Pearson Product- Moment Correlation coefficients obtained to measure reliability for two of the scales were relatively high considering that the test was in the initial stage of development. The coef- ficients were .67 for the psychosocial scale and .68 for the pathophysiological scale.
Reliability and validity.
A standard correlational coefficient was not calculated because of the lack of disper- sion of the proficiency scores. Instead, the average percent agreement was calculated as follows: If a subject gave the same score to an item on the first and second test, then the item was scored “agree”; the proportion of subjects who “agreed” was computed for each item; and the average of these “item proportions” was computed. Subject re- sponse was found to be consistent, with an average agreement of 78% (Marascuilo, 1971) for the entire test.
Content validity was established by the thorough inspection of all test items and the videotaped patient interview by 12 local ex- pert practitioners and by the eight nationally known expert panel members. Medical and nursing students are currently being tested with the instrument for additional assess- ment of its validity.
Subjects
Study participants were selected from among four groups of health practitioners, that is, FPPs, NPMs, NPCs, and PHNs, in the states of Arizona, California, Colorado, Montana, New Mexico, and Washington. Additional criteria for eligibility were (a) completion of an educational program within the past 7 years for their present professional role, (b) current provision of primary care to ambulatory patients with essential hyperten- sion, and (c) willingness to participate and travel to a test site.
Names and addresses of possible partici- pants were gathered from the six state health departments, planning councils, regional medical programs, the American Academy of Family Practice, and the 12 schools and agencies in those states that had programs preparing nurse practitioners. As a result, 9.440 health practitioners (5.300 FPPs. 320 NPMs, 570 NPCs, and 3,250 PHNs) were contacted by mail. Of these, 1,358 (540 FPPs, 92 NPMs, 222 NPCs, and 504 PHNs) expressed interest in participating by re- turning a completed demographic form to the project office.
Initially, a random sampling procedure was deemed appropriate to select subjects from those responding, but because only a small proportion met the eligibility criteria, all subjects who did so were accepted into the study. The final number of participants was 133: 30 FPPs, 30 NPMs, 33 NPCs, and

CLINICAL SIMULATION TEST PERFORMANCE / McLAUGHLlN ET AL. 67
40 PHNs (McLaughlin, Cesa, Johnson, Lem- ons, Anderson, Larson, & Gibson, 1978). All subjects were paid for their services.
All except four of the participating nurses had a bachelor’s degree, and NPMs also had a master’s degree. Both NPMs and NPCs had completed 12 to 18 months of prac- titioner training. NPMs were graduates of programs from seven universities, and NPCs had completed programs in seven universi- ties and two medical centers. PHNs had ex- perienced no formal practitioner training be- yond their basic nursing education program. Of the physicians, 18 had 2 or more years of residency training; 11 had a 1-year rotating internship; and one physician reported no internship or residency.
The NPCs were older and had considera- bly more years of working experience than the other three groups, as shown in Table 1 . Their average years of experience as nurse practitioners. however. were similar to the other groups’ years i n their specialties.
Procedures
The test was given to groups of up to 12 participants at eight test sites in central loca- tions in the six states. Subjects first signed an informed consent form that described study purposes and procedures for protecting anonymity. The general organization of the test instrument was discussed, and subjects were told that they would be asked to select a small number of items from a large list and then rate each selected item on its impor- tance. In addition, they were asked not to compete with each other since group scores were the central interest of the study.
Test booklets were then distributed, and the videotaped interview of the simulated patient was shown on a black-and-white, 19-inch television monitor. Participants gen- erally completed the test booklet in about 2 hours. During the session members of the project staff were available to answer ques-
tions, and before subjects left the testing area staff members checked the booklets for completeness.
To obtain a proficiency score for each study subject, the sub-ject’s test responses were compared with those of the expert panel. If the subject scored an item higher than the expert’s criterion score or selected an item not selected by the experts, a commis- sion error occurred. If a subject scored an item lower than the expert’s criterion score or did not select an item chosen by the ex- perts, an omission error occurred. Finally, to obtain the subject’s overall proficiency score, errors of commission and omission were algebraically combined according to a scoring system developed for this study by W. Michael Becker, Ph.D., an industrial so- cial psychologist at the University of San Francisco.
As noted, the test procedure contained re- productions of the patient’s funduscopic ex- amination, chest x-ray, and ECG recordings, which required the subject‘s interpretation. These items were scored as being either right or wrong and were treated separately, not as a part of the proficiency score.
To obtain the overall psychosocial and pathophysiological scores for each study subject, the procedure was simply to add the subject’s ratings of the items that the indi- vidual selected and that appeared on the Psychosocial and Pathophysiological Scales, respectively.
A series of one-way factorial analyses of variance (ANOVA) with planned a priori contrasts (Winer, 1962) were run for each of the 11 sections of the test instrument to es- tablish whether differences or similarities existed among the four groups in mean score on the Proficiency, Psychosocial, and Pathophysiological Scales. Planned contrasts ( p < .05) are shown on Tables 2, 3 , and 4, to clarify the specific hypotheses that were supported and rejected. A multivariate facto- rial MANOVA design (four groups by 11
Table 1 Demographic Characteristics of Physician and Nurse Groups ~ ~~~ ~
Sex Average Average Years Average Years
Group N Age M F of Experience in Specialty
FPP 30 31 a 26 4 4 8 yrs 2 5 yrs N PM 30 28 8 1 29 6 0 yrs 1 4 yrs N PC 33 36 7 1 32 14 7 yrs 2 6 yrs PHN 40 28 0 0 40 4 9 yrs 4 9 yrs

68 RESEARCH IN NURSING AND HEALTH
sections) was considered but not done be- cause individual test sections, rather than an overall summary statistic, were of major interest. In addition, a xz statistic (Maras- cuilo, 1971) was run for the test sections for which frequency data were obtained, as shown in Table 5.
RESULTS
Proficiency Scale Comparisons
The mean proficiency scores for the four groups on the 1 1 test sections were consis- tently high. with a range of 81% to 95%. as shown in Table 2. These scores reflect a high level of agreement with the expert panel.
Hypothesis 1 , which stated that FPPs’ proficiency scores would not differ from those of NPMs and NPCs, was supported. Hypothesis 2, which predicted that there would be no difference between the two nurse practitioner groups, was also sup- ported.
Hypothesis 3, which predicted that the PHN group would be less proficient than the other three groups, received support on only 3 of the 1 1 sections. PHNs were significantly less proficient than FPPs and NPMs on Physical Examination and on Plan of Care 1, and were significantly less proficient than FPPs on Plan of Care 2. However, there was no significant difference between the mean scores of PHNs and NPCs on any of the 11 test sections. Overall, the PHN group’s ac- tual mean scores were similar to those of the other three groups.
Psychosocial Scale Comparisons
Hypothesis 4, predicting that the FPPs’ psychosocial scores would be significantly lower than those of the three groups of nurses, was generally supported, as shown in Table 3. Significant contrasts between FPPs and at least one nurse-group were obtained for six of the nine appropriate sections; two test sections, Physical Examination and Clinical Laboratory Studies, contained no items that were judged psychosocial. Hy- pothesis 5, which predicted that there would be no significant differences between the three nurse groups, was also supported.
Although not predicted, PHNs had the highest mean psychological scores on seven of the nine test sections. The results also showed that in general the nurse-groups se- lected more psychosocial actions than did the physicians for all the sections.
Pathophysiological Scale Comparisons
The results from the pathophysiological scores were mixed and complex, as shown in Table 4. Hypothesis 6, which predicted that the FPPs’ scores would be significantly higher than the nurse-groups’ scores, was not supported. There were no significant differences among the four groups for 6 of the 11 test sections, and the only test section on which FPPs scored significantly higher than NPMs and NPCs was the Actual Prob- lems List.
FPPs scored significantly higher than the PHN group on only four sections: Elicit Pa-
Table 2 Mean Proficiency Scale Scores of Study Groups, with ANOVA Comparisons
CI i n ica I Simulation FPP NPM NPC PHN Significant Test Section (n=30) (n=30) (n=33) (n=40) Contrasts*
Elicit Patient History Assess Patient History Physica I Examination
CI i n ical Laboratory
Ten tat ive Problems Actual Problems Plan of Care 1 Plan of Care 2 Plan of Care 3 Plan of Care 4 Plan of Care 5
Studies
,827 .814 ,809 ,953 ,951 ,952 ,925 .906 ,897
.890 .888 .871
.932 .917 ,927
.932 ,917 ,927
.915 ,916 .904 ,887 ,879 ,872 ,898 .882 .878 ,889 ,891 ,878 ,895 ,893 ,879
.826 ,950 ,857
.869
.923 ,923 .886 ,862 .875 .892 ,888
ns
FPP>PHN, NPM>PHN, FPP>NPM+ NPC+ PHN
ns
ns
ns ns
FPP> PHN, N PM> PHN FPP>PHN
ns ns ns
* p < .05

C-INICAL SIMULATION TEST PERFORMANCE I McLAUGHLlN ET AL. 69
Table 3 Mean Psychosocial Scale Scores of Study Groups, with ANOVA Comparisons ~-
Cl i n ica I Simulation FPP NPM Test Section (n=30) (n=30)
Elicit Patient History Assess Patient Histwy
Tentative Problem:, Actual Problems Plan of Care 1 Plan of Core 2
Plan of Care 3
Plan of Care 4
Plan of Care 5
7.8 10.9 21.3 27.1
3 .5 6.2 3.7 5.6
19.6 21.8 23.6 32.1
18.8 28.5
17.8 24.5
17.0 22.2
9.9 24.3
5.2 4.0
25.8 32.0
27.7
24.5
22.2
NPC PHN Significant (n=33) (n=40) Con t rusts"
~~
12.8 FPP<PHN 26.9 FPP<<NPM, FPP<NPC,
FPP<PHN, FPP<NPM + NPC+ PHN
6.3 ns 4.6 ns
28.4 FPP<PHN 36.1 FPP<NPM+NPC,
FPP<PHN. FPP<NPM+ NPC+PHN
FPP<:NPM, F P P t NPC, FPP<PHN
FPP<NPM + NPC + PHN
29 8 FPP<NPM+NPC+PHN,
26 2 FPP<PHN,
23.1 ns
*p < 05
Table 4 Mean Pathophysiological Scale Scores of Study Groups, with ANOVA Comparisons
Clinical Simulatioii FPP NPM NPC PHN Sign i fica n i Test Section (n=30) (n=30) (n=33) (n-40) Contrasts*
Elicit Patient History 34.8
Assess Patient History 14.3 Physical Examinaiion 106.0 Clinical La borator 70.5
Tenfative Probiems 18.1 Actual Problems 24.2
Studies
Plan of Care 1 18 3 Plan of Care 2 22 4 Plan of Care 3 26 0 Plan of Care 4 29 6 Plan of Care 5 26 8
*p 05
~~~
__ 35.5
15.5 117.4 62.1
19.7 21.4
18.3 20.9 24.4 23 7 22.3
tient History. Clinical Laboratory Studies, Actual Problems List, and Plan of Care 4. Of special interest is that the PHN group scored significantly higher than the FPP group on Physical Examination.
Hypothesis 7, predicting that there would be no significant differences between the two nurse practitioner groups, was supported. Hypothesis 8, which predicted that PHNs would score lower than NPMs and NPCs, was supported in relation to both nurse prac- titioner groups for only three sections: Elicit Patient History, Clinical Laboratory Studies, and Actual Problems List.
_____
32 3
15 3 121 1 72 8
18 0 21 2
21 2 22 4 27 9 2 8 1 26 7
27.9
14.9 134.7 54.1
15.7 17.3
22.8 22.5 22.9 20.9 21.3
FPP>PHN, NPM>PHN, NPM+NPC>PHN
PHN>FPP FPP>PHN, NPC>PHN, NPM + NPC>PHN
FPP,NPM + NPC+ PHN, FPP>PHN NPM+NPC>PHN
n s
ns
ns ns ns
FPP>PHN, NPC>PHN ns
Interpretation of Diagnostic Tests
Table 5 shows the proportions of each group that correctly interpreted the simu- lated patient's funduscopic examination, chest x-ray, and ECG recordings.
With the exception of one item (focal spasm, on which a greater proportion of both NPMs and NPCs responded correctly), the FPP group scored highest in interpreting these diagnostic tests. However, on four other items the proportion of nurse prac- titioners, particularly NPMs, who responded correctly was no more than lo%> lower than

70 RESEARCH IN NURSING AND HEALTH
Table 5 Items, with xz Comparisons
Number and Proportion of Correct Responses of Study Groups on Diagnostic Test
Correct Responses by Group
FPP N PM NPC PHN (n=30) (n=30) (n=33) (n=40)
Diagnostic Test Item No. % No. % No. % No. % xz (df=3)
Funduscopic Focal spasm Hemorrhages Exudates Papilledema A N ratio K-W classification
Card io-thoracic ratio X-ray interpretation
Interpretation of ECG
X-ray
ECG
20 67 24 80 26 79 19 48 30 100 28 93 30 91 30 75 30 100 28 93 29 88 26 65 30 100 27 90 24 73 16 40
22 73 1 1 37 7 21 0 0 17 57 9 30 16 4a 2 5
22 73 10 33 12 37 4 10 22 73 20 67 10 58 18 45
28 93 1 1 37 12 36 4 10
1 1.23* 12.13* 19.65* 37.53* 25.45* 45.75*
29.94* 6.55
50.24*
* p < .05
that of FPPs. The PHN group had the lowest proportion of correct responses on all items.
DISCUSS10 N According to our findings for proficiency in
primary care, physicians and nurse prac- titioners perform at a comparable level in as- sessing and managing a simulated patient with essential hypertension. Although the type of training, whether in a master’s pro- gram or a certificated program, appears to make little difference in the nurse prac- titioner’s level of proficiency, the group of NPCs in this study did have about 8 more years of work experience than did NPMs.
In addition, the PHN group, which had no practitioner training and fewer years of work experience than either nurse practitioner group, performed at nearly the same level of proficiency on most test sections as the other three groups. This finding suggests that if public health nurses received special training in their few areas of weakness, such as physical examination procedures, diagnostic tests, and medication strategies, they could offer a greater range of primary health care services, particularly to the underserved populations that are part of their usual case load. Greater use of this group to provide periodic physical health assessments could wbstantially reduce health costs through early case-finding and treatment.
The sections of the test that most sharply
discriminated among the four groups were those requiring specific skills in interpreting a photograph of an eyeground, a chest x-ray, and ECG recordings. Because of their special preparation, the nurse practitioner groups might be expected to perform better than they did on these interpretations. It is suggested that if nurse practitioners are functioning as the principal source of pri- mary care in many rural and inner city ghetto areas, they should receive more thorough in- struction in these and other basic diagnostic procedures during their formal training pro- grams.
Our findings definitely support the view that the nurse groups emphasize psychoso- cia1 aspects of care more than physicians do. Of some surprise, perhaps, is the consistent pattern of the physicians’ scoring lowest on the Psychosocial Scale on all test sections. Because the majority of the physician group had completed a residency in family practice specialty programs, which ostensibly em- phasize psychosocial factors, one might ex- pect these physicians to score somewhat higher than they did on this scale.
Some authors have expressed concern that nurses who are trained to function in an ex- panded role might eventually de-emphasize their background in psychosocial approaches (Bates & Lynaugh, 1973). Our findings tend to refute such concerns and to suggest that, even after extensive education in the more physical aspects, nurse practitioners appear

71 CLII\IICAL SIMULATION TEST PERFORMANCE / McLAUGHLlN ET AL
to remain committed to placing emphasis on psychosocial factors.
Because of the nurse practitioners' com- petency in recognizing and using psychoso- cia1 factors. we propose that their practice can be considered complementary to the tra- ditional medical model. In addition, the nurse practitioners' demonstration of com- mitment to the importance of recognizing and treating emotional aspects of the patient might lead to the development of more hu- mane approaches in other health professions.
The picture of nurse practitioners that emerges from our findings on the Patho- physiological Scale is one of profession- als whose style of practice combines psychosocial and pat hophysiological ap- proaches. Perhaps their practice represents a desirable synthesis of the two approaches.
The unexpected finding that the PHN group scored significantly higher than the physician group did on the number of Physi- cal Examination items chosen may be ex- plained on the basis of the lack of training or experience of this group of nurses in adult physical assessment. Lt seems likely that these nurses were willing to select many nonessential physical examination proce- dures because of their possible worth and lack of potential harm to the patient. The generally higher than predicted scores of the PHN group appear to reflect considerably more use of the pathophysiological approach than was expected.
Finally. although the clinical simulation test instrument was used only as an assess- ment device in this study, we suggest that it could be an excellent teaching tool for medi- cal and nursing students. It also could be used as a model of a systems-oriented, problem-solving method for developing similar tests for other health problems.
By using such teaching instruments. stu- dents could "fail" without causing harm to an actual patient and could learn from feed- back directly related to the specific actions taken. In addition, they could experience the actual problem-solving, evaluating, and decision-making process that will be required of them in practicc.
REFERENCES
American Nurses' Associotmon. Accountability and the nurse. 1973.
Andrews, P., Yankouer, A., & Connelly, P. P. Changing the patterns of ombulatory pediatric
ca reta ki ng : An action-oriented training program for nurses. American Journal of Public Health, 1970,
Bailey, J T , & Claus, K. E. Derision making in nursing. St. Louis: Mosby, 1975.
Baker, A. S., Soper, M., Keolrnes, H., Farrisey, R., & Goldfinger, S. E. Expeditious training of nurse practitioners: Repeat of a program in Mossuchu- setts. Massachusetts Physician, 1973,32(9), 52-53, 55-56.
Bates, R , & Lynaugh, J. Laying the foundations for medical nursing practice. American Journal of Nursing, 1973, 73, 1375-1 379
Brunetto, E., & Birk, P. The primary care nurse: The generalist in a structured health care team. Ameri- can Journal of Public Health, 1972, 62, 785-794
Cheyovitch, T. D., Lewis, C. E., & Gortner, S. R. The nurse practitioner in an adult outpatient clinic (DHEW Publication No. HRA 76-29). Washington, D C : U.S. Government Printing Office, 1976
Chow, R . Postoperative cardiac nursing research. A method for identifying and categorizing nursing acrion. Nursing Research, 1969, J8( 1 ), 4- 13.
Day, L . R., Egli, R., & Silver, H. K. Acceptonce of pediatric nurse proctitioners: Parents' opinion of combined care by a pediatrician and o pediatric nurse practitioner in a private practice. Arnericon Jourriai of Diseases of Children, 1970, 199, 204- 208.
Department of Health, Education, and Welfare. Ex- tending the scope of nursing practice: Report of Secretary's Committee to Study Extended Roles for Nurses. Nursiriy Outlook, 1972, 20, 46-52.
Feldmnn, R., Taller, S. L., Garfield, S. R., Collen, R F., Richart, R. H., Cello, R , & Sender, A. J. Nurse practitioner multiphasic heolth checkups. Preveri- tive Medicine, 1977, 6, 391 -403.
Ford, L C., Seocat, M S , & Silver, G. G. Broadening roles of public heolth nurse and physician in pre-riatal and infant supervision Anierican Jour- nal of Public Health, 1966, 56, 1097-1 103.
Ford, L. C., & Silver, H. K. The expanded role of the nurse in child care. Nursing Outlook, 1967, 1.5, 43-45.
Hoekelman, R. A. Pediatric nurse practitioner: Analysis of potential troining and utilization in
New York State. N e w York State Journal of Medi- cine, 1972, 72( 15), 199 1-2000.
Howlond, D., & McDowell, W. E. The measure of patient cure: A conceptual framework Nursing Research, 1964, 13(1), 4-7.
Keppel, G. Desrgn and analysis: A researcher's hond- book Englewood Cliffs, N.J.: Prentice-Hall, 1973.
Kodadek, S. (Ed.). Analysis and planning for improved distribution of nursing personnel and services (DHEW Publication No. HRA 77-2). Washington, D.C.: U.S. Government Printing Office, 1976.
Lewis, C. E., & Resnik. B. A. Nurse clinics in am- bulatory care. New England Journal of Medicine, 1967, 277, 1236-1241.
Lewis, C. E., Resnik, 8. A., Schmidt, G., & Waxman. D. Activities, events and outcomes in ambulatory
60, 870-879.

72 RESEARCH IN NURSING AND HEALTH
patient care. New England Journal of Medicine,
Linn, L. S. Care vs. Cure: How the nurse practitioner 1974, 22,
Linn, L. S. Expectation vs. realization in the nurse practitioner role. Nursing Outlook, 1975,23, 166- 171. (a)
Linn, L. S. Factors associated with patient evaluation of health care. The Milbank Memorial fund Quar- terly, 1975,53, 531-548. (b)
Marascui lo, L. A. Statistical methods for behavioral sci- ence research. New York: McGraw-Hill, 1971.
McLaughlin, F. E., Cesa, T., Johnson, H., Lemons, M., Anderson, S., Larson, P., & Gibson, J. Primary care judgments of nurses and physicians: Report of the research, Vol. 1 (DHEW, Division of Nursing, Grant NU00528). Veterans Administration Hos- pital, San Francisco, 1978.
Moore, M. F., Barber, J. H., Robinson, E. T., & Taylor, T. R. First contact decisions in general practice: Comparisons between a nurse and three general practitioners. lancet, April 14, 1973, 81 7-819.
Pickard, C. G., Watkins, J. D. (Eds.). Current directions in family nurse practitioner curriculo (DHEW Publi- cation No. HRA 77-28). Washington, D.C.: U.S. Government Printing Office, 1977.
Pritchard, C. G. Family nurse practitioners: Prelimi- nary answers and new issues (editorial). Annals of Internal Medicine, 1974, 80, 267-268.
1969,280, 645-649.
views the patient. Nursing Outlook, 641 -644.
Sackett, D. L., Spitzer, W. O., Gent, M., & Robbins, R. S. The Burlington randomized trial of the nurse practitioners: Health outcomes of patients. Annals o f Internal Medicine, 1974, 80, 137-1 42.
Silver, H. K., Ford, L. C., &Steady, S. G. A program to increase health care for children: The pediatric nurse practitioner program. Pediatrics, 1967, 39,
Spitzer, W. O., Harth, M., Goldsmith, C. H., Norman, G. R., Dickie, G. L., Bass, M. J., & Newell, J. P. The arthritic complaint i n primary care: Prevalence, related disability and costs. Journal of Rheumotol-
Spitzer, W. O., Sackett, D. L., & Sibley, J. C. The Burlington randomized trial of the nurse prac- titioner. New England Journal of Medicine, 1974,
Sultz, H. A., Zielezny, M., & Kinyon, L. Longitudinal study of nurse practitioners: Phase I (DHEW Publica- tion No. HRA 7643). Washington, D.C.: U.S. Gov- ernment Printing Office, 1976.
Twaddle, A. C. Aging population growth and chronic illness: A projection, United States, 1960-1 985. Journal of Chronic Disease, 1968,21, 41 7-422.
Weed, L. W. Medical records, medical education, and patientcare. Chicago: Year Book Publishers, 1971.
Winer, 6. J. Statistical principles in experimental de- sign. New York: McGraw-Hill, 1962.
756-760.
~ g y , 1976,3( l), 88-99.
290, 25 1-256.
Dr. Frank E. Mctaughlin is chief of research in clinical nursing at the Veterons Administration Hospital, San Francisco. Mr. Thomas Cesa is an administrative analyst in the Office of Student Affairs Research, University of California at Berkeley. Dr. Harold Johnson is in private practice in San Bruno, California. Ms. Mary Lemons is associate hospital director at Texas A & M Hospital, Lubbock, Texas. Ms. Sara Anderson i s assistant professor at the College of Nursing, University of New Mexico. Ms. Patricia Larson is a D.N.Sc. candidate at the School of Nursing, University of California at San Francisco. Ms. Josephine Gibson i s director of the Nurse Practitioner Program, University of Arizona at Tucson.
Requests for reprints may be addressed to Dr. Frank E. Mctaughlin, Veterans Administration Hospital, 4150 Clement Street, Son Francisco, Colifornia 94121. The script far the videotape and clinical simulation test booklet for hypertension are available from United States Department of Commerce, NTIS, 5285 Port Royal Road, Springfield, Virginia 22161, Vol. 2-HRP0900605.
This paper was received September 11, 1978, was revised, and was accepted far publication February 21, 1979.