Embed Size (px)
Citation preview

Nursing Home–Acquired Bloodstream Infection • Author(s): Joseph M. Mylotte , MDSource: Infection Control and Hospital Epidemiology, Vol. 26, No. 10 (October 2005), pp. 833-837Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/502502 .
Accessed: 15/05/2014 15:38
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions
Vol. 26 No. 10 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY 833
Topics in Long-Term CareEDITED BY PHILIP W. SMITH, MD
Dr. Mylotte is from the Departments of Medicine and Microbiology, School of Medicine and Biomedical Sciences, University at Buffalo; and the Department of Medicine, Division of Infectious Diseases, Erie County Medical Center, Buffalo, New York.
Address reprint requests to Joseph M. Mylotte, MD, Infectious Diseases, Erie County Medical Center, 462 Grider St., Buffalo, NY 14215. [email protected]
Nursing Home–Acquired Bloodstream InfectionJoseph M. Mylotte, MD
Septicemia or bloodstream infection (BSI) is a major cause of morbidity and mortality among the U.S. population despite the use of potent antimicrobial therapy and inten-sive supportive measures. Among the 15 leading causes of death between 1950 and 1997, septicemia was associated with the greatest increase in death rate.1 In addition, rates of hospitalization due to BSI increased by 10.5% per year between 1980 and 19942 and increased more than twofold in the elderly population between 1986 and 1997.3 Despite these findings, BSI has been infrequently studied in the nursing home population, currently the most frail and de-bilitated elderly population in the United States. There are only seven published studies that have specifically evalu-ated BSI in the nursing home population in North America in the past 20 years.4-10
The objective of this article is to provide a review of the epidemiology of nursing home–acquired BSI, empha-sizing some of the limitations of the published studies. This review addresses nursing home residents who received long-term care only and does not apply to those who re-
ceived short-term rehabilitation and returned to living in-dependently.
USE OF BLOOD CULTURES IN THE NURSING HOME SETTING
To the best of the author’s knowledge, only one study7 provided data on the frequency of use of blood cultures in the nursing home setting. In this study,7 performed during a 7.5-year period from 1984 to 1991 in one facility in Winnipeg, Manitoba, Canada, there was 24-hour physician coverage and an on-site laboratory. The number of blood cultures pro-cessed each year varied from 26 to 126, and the proportion of positive cultures varied from 2.9% to 11.9%; overall, 29 (6.3%) of 459 cultures processed during the study period were posi-tive. Because of the level of physician coverage and the capa-bility of the on-site laboratory, this study may be a reasonable estimate of what blood culture use might be in the nursing home setting if such cultures were generally available. How-ever, it has been the author’s experience that blood cultures are rarely performed in the community nursing home setting
OBJECTIVES: This article reviews published studies of nursing home–acquired BSI in North America to determine whether there have been changes in the epidemiology of this infection in the past 20 years and to define indications for blood cultures in the nursing home setting.
METHODS: A Medline search was conducted for the pe-riod from 1980 to August 2003.
RESULTS: Seven studies of nursing home–acquired BSI were identified. The incidence of nursing home–acquired BSI was low (0.3 episode per 1,000 resident care–days). Sources of BSI changed little during the past two decades, with urinary tract infection representing approximately 50% of the episodes. The bacteriology also did not change substantially during the past 20 years; gram-negative bacilli were isolated in approxi-mately 50% of the episodes and Escherichia coli was the most
commonly isolated organism. In the most recent study, covering the period 1997–2000, resistance to fluoroquinolones and broad-spectrum penicillins and cephalosporins was uncommon among gram-negative blood isolates; MRSA was the most common re-sistant organism causing nursing home–acquired BSI. Case-fa-tality rates changed little during the past 20 years; urinary tract infection was associated with the lowest mortality and pneumo-nia had the highest case-fatality rate.
CONCLUSION: There has been little change in the epi-demiology of nursing home–acquired BSI in the past 20 years. Given the low incidence of BSI and the low overall yield of posi-tive results of blood cultures (probably 6%), there is currently no support for the routine use of blood cultures in the nursing home setting (Infect Control Hosp Epidemiol 2005;26:833-837).
ABSTRACT
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions
834 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY October 2005
because of lack of staff training. In a study of nursing home pneumonia, for example, 75% of 378 episodes were treated in the nursing home11 and no blood cultures were performed in those treated. In a hospital-based or Veterans Affairs nursing home, it is possible that blood cultures may be used more frequently because of the presence of an on-site laboratory or good physician coverage.
LIMITATIONS OF STUDIES OF NURSING HOME–ACQUIRED BSI
Before the epidemiology of nursing home–acquired BSI is reviewed, it is useful to consider some of the limi-tations of the published studies to put the findings in per-spective. Richardson and Hricz8 performed a case–control
study to define risk factors for bacteremia in nursing home patients. This study was done in a long-term–care hospital in Baltimore, Maryland, that provided both intermediate-level and long-term care. The authors did not distinguish between the two groups in their analysis; therefore, their findings may not be relevant to the typical community nurs-ing home population. Sinclair et al.9 found that 10 (8.8%) of 113 nursing home residents evaluated in the emergency department of a hospital in Halifax, Nova Scotia, Canada, during an 8-month period had positive blood cultures. All but one episode were due to gram-negative bacilli, the uri-nary tract was the source in six episodes, and there were two deaths. Because of their design limitations, these two studies8,9 will not be considered further in this review.
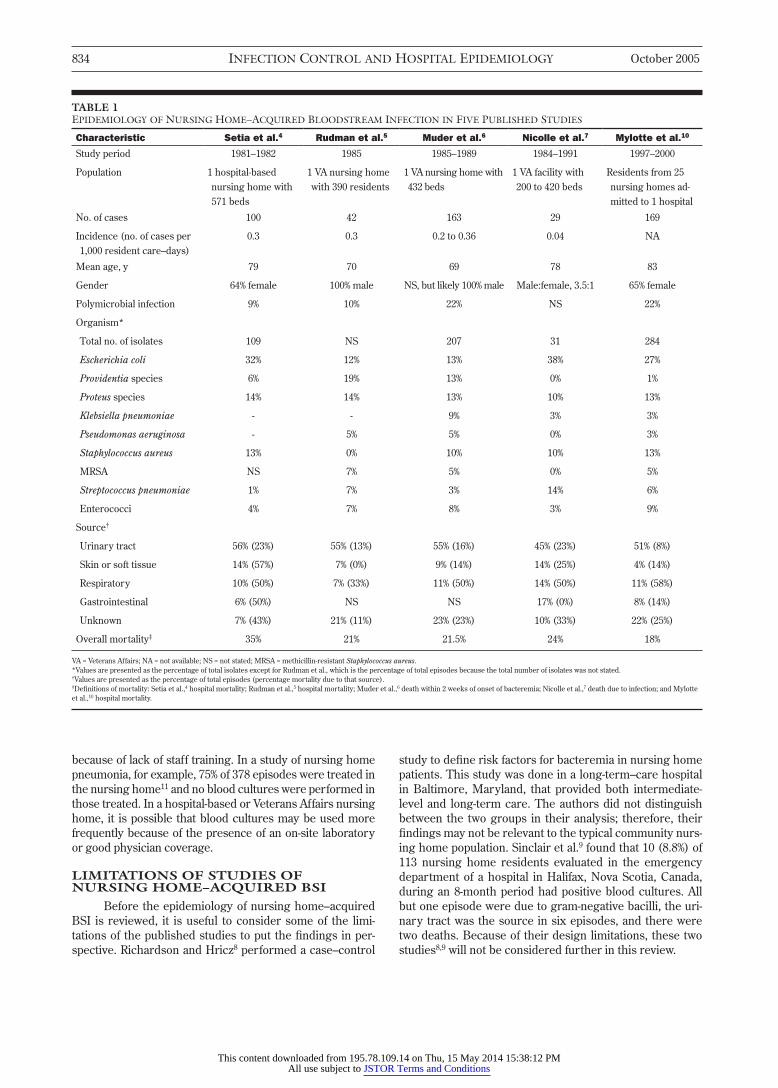
TABLE 1EPIDEMIOLOGY OF NURSING HOME–ACQUIRED BLOODSTREAM INFECTION IN FIVE PUBLISHED STUDIES
Characteristic Setia et al.4 Rudman et al.5 Muder et al.6 Nicolle et al.7 Mylotte et al.10
Study period 1981–1982 1985 1985–1989 1984–1991 1997–2000
Population 1 hospital-based nursing home with 571 beds
1 VA nursing home with 390 residents
1 VA nursing home with 432 beds
1 VA facility with 200 to 420 beds
Residents from 25 nursing homes ad-mitted to 1 hospital
No. of cases 100 42 163 29 169
Incidence (no. of cases per 1,000 resident care–days)
0.3 0.3 0.2 to 0.36 0.04 NA
Mean age, y 79 70 69 78 83
Gender 64% female 100% male NS, but likely 100% male Male:female, 3.5:1 65% female
Polymicrobial infection 9% 10% 22% NS 22%
Organism*
Total no. of isolates 109 NS 207 31 284
Escherichia coli 32% 12% 13% 38% 27%
Providentia species 6% 19% 13% 0% 1%
Proteus species 14% 14% 13% 10% 13%
Klebsiella pneumoniae - - 9% 3% 3%
Pseudomonas aeruginosa - 5% 5% 0% 3%
Staphylococcus aureus 13% 0% 10% 10% 13%
MRSA NS 7% 5% 0% 5%
Streptococcus pneumoniae 1% 7% 3% 14% 6%
Enterococci 4% 7% 8% 3% 9%
Source†
Urinary tract 56% (23%) 55% (13%) 55% (16%) 45% (23%) 51% (8%)
Skin or soft tissue 14% (57%) 7% (0%) 9% (14%) 14% (25%) 4% (14%)
Respiratory 10% (50%) 7% (33%) 11% (50%) 14% (50%) 11% (58%)
Gastrointestinal 6% (50%) NS NS 17% (0%) 8% (14%)
Unknown 7% (43%) 21% (11%) 23% (23%) 10% (33%) 22% (25%)
Overall mortality‡ 35% 21% 21.5% 24% 18%
VA = Veterans Affairs; NA = not available; NS = not stated; MRSA = methicillin-resistant Staphylococcus aureus. *Values are presented as the percentage of total isolates except for Rudman et al., which is the percentage of total episodes because the total number of isolates was not stated. †Values are presented as the percentage of total episodes (percentage mortality due to that source). ‡Definitions of mortality: Setia et al.,4 hospital mortality; Rudman et al.,5 hospital mortality; Muder et al.,6 death within 2 weeks of onset of bacteremia; Nicolle et al.,7 death due to infection; and Mylotte et al.,10 hospital mortality.
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions

Vol. 26 No. 10 TOPICS IN LONG-TERM CARE 835
Three5-7 of the remaining five studies of nursing home–acquired BSI were done in a single Veterans Affairs facility, one4 was done in a single hospital-based facility, and one10 was done among nursing home residents admitted to one hospital from multiple community homes in a metro-politan area. The studies done in Veterans Affairs facilities may not be representative of the epidemiology of BSI in community nursing homes for several reasons. Almost all of the residents in the Veterans Affairs facilities were male, whereas the community nursing homes had a majority (65% to 70%) of female residents (Table 1). The residents in the Veterans Affairs facilities were younger, on average, com-pared with those in community nursing homes. The dif-ferences in gender and age distribution between these two groups have some significance in terms of the frequency of various underlying diseases and risk for infection. For ex-ample, Mulhausen et al.12 evaluated the prevalence of meth-icillin-resistant Staphylococcus aureus (MRSA) colonization of the nares and rate of MRSA infection in a Veterans Affairs facility compared with those in three community nursing homes in the same region. They found that the residents of the community nursing homes were significantly older, had significantly poorer functional status, and were more likely to have a history of dementia than the residents of the Veterans Affairs facility. Although the prevalence of MRSA colonization of the nares was significantly higher in the Vet-erans Affairs facility, the rate of MRSA infection was higher (4.7-fold) in the community nursing homes. The study by Mulhausen et al.12 illustrates the potential impact of differ-ences in underlying disease, gender, and age between the populations of Veterans Affairs nursing homes and commu-nity nursing homes on infection rates and outcome.
EPIDEMIOLOGYThe findings of five studies4-7,10 of nursing home–ac-
quired BSI are summarized and compared in Table 1. These studies span approximately 20 years, with three of them eval-uating this infection exclusively in the 1980s. Only one of the studies10 evaluated nursing home residents from multiple nursing homes. Despite the fact that there were differences in the study populations, the incidences of BSI reported by three of the studies4-6 were remarkably similar, approximate-ly 0.3 episode per 1,000 resident care–days, whereas the inci-dence was 10-fold lower in one study.7
SourcesUrinary tract infection was the most common source
in all five studies and represented 45% to 56% of the infec-tions (Table 1). Skin or soft tissue infections appeared to decline in frequency during the 20-year period covered by these five studies, whereas respiratory tract infection (pneumonia) demonstrated less variation, ranging from 7% to 14% of episodes. The frequency of an unknown focus of infection varied from 7% to 23%. Overall, there was little change in the distribution of sources of BSI among these five studies spanning two decades. Intravenous catheters were rarely a source of BSI in these five studies,4,6 but four of these studies were done primarily in the 1980s, when in-
travenous therapy was not common in the nursing home setting.
BacteriologyThere are some interesting differences in the fre-
quency of isolation of organisms among these five studies that should be emphasized (Table 1). Escherichia coli, Prov-identia species, and Proteus species were the most common gram-negative isolates in all five studies and were usually associated with urinary tract infection (data not shown). However, the distribution of these three gram-negative organisms varied between the Veterans Affairs facilities and the non–Veterans Affairs facilities. Escherichia coli was more than twice as common a cause of BSI in the studies by Setia et al.,4 Nicolle et al.,7 and Mylotte et al.10 compared with the two Veterans Affairs studies. On the other hand, Providentia species were isolated more than threefold as often in the Veterans Affairs studies5,6 compared with the other three studies.4,7,10 It has been observed that Providen-tia species are a common cause of urinary tract infection in association with long-term use of invasive urinary devices.13 As indicated in Table 2, an invasive urinary device was pres-ent much more commonly in the populations of the Veter-ans Affairs studies4,5 as compared with those of the other three studies. It is therefore likely that the high level of use of invasive urinary devices among the residents of the Vet-erans Affairs facilities explains the more frequent isolation of Providentia species in this population. There did not ap-pear to be much change in the frequency of gram-positive organisms causing BSI among these five studies during the 20-year period.
There has been increasing concern about antibiotic-resistant organisms in the nursing home setting, especially resistant gram-negative bacilli.14 However, as pointed out recently by two authors,15,16 studies reporting high rates of antibiotic resistance among gram-negative bacilli isolated from nursing home residents have primarily come from single, large tertiary-care centers or Veterans Affairs nurs-ing homes. Studies of community nursing home residents have not found high prevalence rates of antibiotic resistance
TABLE 2RELATIONSHIP BETWEEN THE PRESENCE OF A URINARY DEVICE AND BLOODSTREAM INFECTION AMONG NURSING HOME RESIDENTS
Study
No. of Residents With a Device/
Total No. With BSI
No. of Residents With a Device/ Total
No. With UTI
Setia et al.4 NS 12/56 (21%)
Rudman et al.5 NS 16/34 (47%)
Muder et al.6 136/162 (84%) 84/90 (93%)
Nicolle et al.7 4/29 (14%) NS
Mylotte et al.10 37/162 (23%) 29/85 (34%)*
BSI = bloodstream infection; UTI = urinary tract infection; NS = not stated. *This information was not provided but was extracted by the author from the database used for the study.
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions

836 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY October 2005
among gram-negative bacilli, and MRSA appears to be the most common resistant organism.17,18 Only two studies6,10 provided information about the antibiotic susceptibility of bacteria causing nursing home–acquired BSI. However, it is difficult to compare the findings of these two studies re-garding antibiotic susceptibility because one study was done in the mid to late 1980s6 and the other in the late 1990s.10 In addition, the study by Muder et al.6 was done in a single Veterans Affairs facility, whereas Mylotte et al.10 studied a group of residents admitted to one hospital from multiple community nursing homes. Nevertheless, there are some comparisons that can be made. First, in the study by Muder et al.,6 43% of 23 Escherichia coli blood isolates were resis-tant to trimethoprim–sulfamethoxazole compared with 25% of 52 isolates in the study by Mylotte et al.10 Muder et al.6 reported that 40% to 50% of Proteus species were resistant to ampicillin and trimethoprim–sulfamethoxazole, whereas Mylotte et al.10 found that 91% of Proteus strains were sus-ceptible to all antibiotics tested. These differences in antibi-otic susceptibility patterns likely reflect variation in the use of invasive urinary devices and antibiotics between the two study populations as well as demographic differences be-tween the populations of Veterans Affairs facilities and com-munity nursing homes. In the most recent study,10 none of the blood isolates of Pseudomonas aeruginosa and Klebsiella pneumoniae were resistant to ciprofloxacin, piperacillin–tazobactam, or a third-generation cephalosporin.
The frequency of BSI due to MRSA did not change during the period covered by the studies listed in Table 1. Two studies4,7 did not report MRSA as a cause of BSI. However, MRSA was not a problem in nursing homes in the United States in the early 1980s when the study of Setia et al.4 was done nor in Canada19 during the time of the study by Nicolle et al.7 Nevertheless, recent studies20-22 have found that among nursing home residents with Staphylococcus aureus bacteremia at the time of hospital admission, 75% to 88% of the episodes were due to methicillin-resistant strains. This indicates that the epidemiology of MRSA may be chang-ing in the nursing home setting in the United States, with an apparent increase in invasive infections. Further study of the epidemiology of MRSA BSI in the nursing home setting is clearly warranted.
MortalityThe reported mortality related to nursing home–ac-
quired BSI in each of five studies is provided in Table 1. One must be aware of the definition of mortality used in each of these studies before making any comparisons. Three stud-ies4,5,10 reported hospital mortality or “all-cause” mortality, whereas Muder et al.6 defined mortality as death within 2 weeks of onset of bacteremia and Nicolle et al.7 reported death directly due to infection. Mylotte et al.10 reported that of the 30 hospital deaths in their study, 50% occurred within 3 days of admission, 75% within 7 days of admission, and all but 2 within 14 days of admission. These findings regard-ing timing of death suggest that it is probably valid to make direct comparisons of the case-fatality rates among the five studies listed in Table 1. The highest case-fatality rate was
reported by Setia et al.,4 which is the oldest of the five stud-ies, whereas the case-fatality rate ranged from 18% to 24% in the other four studies. Trends in mortality by source of the BSI are also apparent (Table 1). Skin or soft tissue and uri-nary tract sources were usually associated with the lowest case-fatality rate, whereas a respiratory (pneumonia) source was associated with the highest case-fatality rate (approxi-mately 50%). Using multivariate analysis and controlling for acute severity of illness, Mylotte et al.10 found the following factors to be independent predictors of hospital mortality in nursing home residents with BSI: a pulmonary focus of infection (P < .001), a systolic blood pressure lower than 90 mm Hg at the time of admission (P = .034), and a white blood cell count greater than 20,000 cells/mm3 (P = .01).
INDICATIONS FOR BLOOD CULTURES IN THE NURSING HOME SETTING
It is difficult to formulate indications for blood cul-tures in the nursing home setting because there are no established guidelines for evaluation of suspected infection in this setting.23 As pointed out in a recently published con-sensus guideline for the evaluation of fever and infection in the nursing home setting,23 the presentation of infection in residents can be subtle and fever may be absent. In the nursing home setting, the incidence of BSI appears to be low ( 0.3 episode per 1,000 resident care–days).4-7 Based on this information and expert opinion, blood cultures were not recommended in the evaluation of fever or suspected infection in nursing home residents23 and transfer to the hospital was recommended if BSI was suspected. However, the recommendation to transfer residents with suspected BSI to the hospital begs the question as to who should be suspected to have this severe complication of bacterial in-fection. However, until methods become available that are accurate and feasible for predicting BSI in nursing home residents, I would agree with the expert panel23 that blood cultures should not be part of the diagnostic work-up of sus-pected infection in the nursing home resident who is not hospitalized.
It is also not clear whether results of blood cultures impact the outcome of nursing home residents with BSI ad-mitted to the hospital. As reported by Mylotte et al.,10 50% of deaths occurred within the first 3 days of admission among nursing home residents with positive blood cultures. It would be unlikely for positive blood cultures to substantially impact that mortality as it often takes 48 hours for antibiotic susceptibility data to be become available.
CONCLUSIONSThe incidence of nursing home–acquired BSI has
been consistently low in the few studies that have evalu-ated this parameter. The overall yield of positive results of blood cultures is also low (probably 6%) in the nursing home population. Therefore, there is currently no sup-port for the routine use of blood cultures in the evalua-tion of nursing home residents with suspected infection who are not hospitalized. Sources of BSI in the nursing home setting have changed little during the past two de-
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions

Vol. 26 No. 10 TOPICS IN LONG-TERM CARE 837
cades, with urinary tract infection representing approxi-mately 50% of the episodes. The bacteriology of nursing home–acquired BSI also has not changed substantially during the past 20 years; gram-negative bacilli are isolated in approximately 50% of the episodes and Escherichia coli is the most commonly isolated organism overall. In the most recent study,10 resistance to fluoroquinolones and broad-spectrum penicillins and cephalosporins was un-common among gram-negative blood isolates and MRSA was the most common resistant organism causing BSI. Case-fatality rates showed little change during the past 20 years, but urinary tract infection was associated with the lowest mortality and pneumonia had the highest case-fa-tality rate. Future research considerations should include determining the benefit, if any, of hospitalizing residents with BSI and evaluating the epidemiology of MRSA BSI in nursing home residents.
REFERENCES 1. Hoyert KL, Kochanek KD, Murphy SL. Deaths: final data for 1997.
Vl 47. In: National Center for Health Statistics. National Vital Statis-tics Report 19. Hyattsville, MD: National Center for Health Statistics; 1999.
2. Simonsen L, Conn LA, Pinner RW, Teutsch S. Trends in infectious dis-ease hospitalizations in the United States, 1980-1994. Arch Intern Med 1998;158:1923-1928.
3. McBean M, Rajamani S. Increasing rates of hospitalization due to septicemia in the US elderly population, 1986-1997. Clin Infect Dis 2001;183:596-603.
4. Setia U, Serventi I, Lorenz P. Bacteremia in a long-term care facility: spectrum and mortality. Arch Intern Med 1984;144:1633-1635.
5. Rudman D, Hontanosas A, Cohen Z, Mattson DE. Clinical correlates of bacteremia in a Veterans Administration extended care facility. J Am Geriatr Soc 1988;36:726-732.
6. Muder RR, Brennen C, Wagener MM, Goetz AM. Bacteremia in a long-term care facility: a five-year prospective study of 163 consecutive episodes. Clin Infect Dis 1992;14:647-654.
7. Nicolle LE, McIntyre M, Hoban D, Murray D. Bacteremia in a long term care facility. Canadian Journal of Infectious Diseases 1994;5:130-132.
8. Richardson JP, Hricz L. Risk factors for the development of bacteremia in nursing home patients. Archives of Family Practice 1995;4:785-789.
9. Sinclair D, Svendsen A, Marrie T. Bacteremia in nursing home patients: prevalence among patients presenting to an emergency de-partment. Can Fam Physician 1998;44:317-322.
10. Mylotte JM, Tayara A, Goodnough S. Epidemiology of bloodstream infection in nursing home residents: evaluation in a large cohort from multiple homes. Clin Infect Dis 2002;35:1484-1490.
11. Naughton BJ, Mylotte JM, Tayara A. Outcome of nursing home-ac-quired pneumonia: derivation and application of a practical model to predict 30 day mortality. J Am Geriatr Soc 2000;48:1292-1299.
12. Mulhausen PL, Harrell LJ, Weinberger M, Kochersberger GG, Feuss-ner JR. Contrasting methicillin-resistant Staphylococcus aureus in Vet-erans Affairs and community nursing homes. Am J Med 1996;100:24-31.
13. Warren JW. Providentia stuartii: a common cause of antibiotic-resis-tant bacteriuria in patients with long-term indwelling catheters. Rev Infect Dis 1986;8:61-67.
14. Bonomo RA. Multiple antibiotic-resistant bacteria in long-term care facilities: an emerging problem in the practice of infectious diseases. Clin Infect Dis 2000;31:1414-1422.
15. Bradley SF. Issues in the management of resistant bacteria in long-term–care facilities. Infect Control Hosp Epidemiol 1999;20:362-366.
16. Loeb M. Antibiotic use in long-term care facilities: many unanswered questions. Infect Control Hosp Epidemiol 2000;21:680-683.
17. Smith PW, Seip CW, Schaefer SC, Bell-Dixon C. Microbiologic survey of long-term care facilities. Am J Infect Control 2000;28:8-13.
18. Mylotte JM, Goodnough S, Tayara A. Antibiotic-resistant organisms among long-term care facility residents on admission to an inpatient geriatrics unit: retrospective and prospective surveillance. Am J Infect Control 2001;29:139-144.
19. Embil J, Ramaotar K, Romance L, et al. Methicillin-resistant Staphylococcus aureus in tertiary care institutions on the Canadian prairies, 1990-1992. Infect Control Hosp Epidemiol 1994;15:646-651.
20. Rezende NA, Blumberg HM, Metzger BS, Larsen NM, Ray SM, McGowan JE. Risk factors for methicillin-resistance among patients with Staphylococcus aureus bacteremia at the time of hospital admis-sion. Am J Med Sci 2002;323:117-123.
21. Johnson LB, Bhan A, Pawlak J, Manzor O, Saravolatz LD. Changing epidemiology of community-onset methicillin-resistant Staphylococcus aureus bacteremia. Infect Control Hosp Epidemiol 2003;24:431-435.
22. Lodise TP, McKinnon PS, Rybak M. Prediction model to identify patients with Staphylococcus aureus bacteremia at risk for methicillin resistance. Infect Control Hosp Epidemiol 2003;24:655-661.
23. Bentley DW, Bradley S, High K, Schoenbaum S, Taler G, Yoshikawa TT. Practice guideline for evaluation of fever and infection in long-term care facilities. Clin Infect Dis 2000;31:640-645.
This content downloaded from 195.78.109.14 on Thu, 15 May 2014 15:38:12 PMAll use subject to JSTOR Terms and Conditions















![N Hospital infection Control. n Nosocomial infections (hospital –acquired infection): An infection acquired in [a] hospital by a patient who was admitted](https://img.pdfslide.net/doc/110x75/5697c0071a28abf838cc627a/n-hospital-infection-control-n-nosocomial-infections-hospital-acquired.jpg)













