Embed Size (px)
DESCRIPTION
Case study
Citation preview
Liceo de Cagayan UniversityCollege Of Nursing
NCM501-205 Related Learning Experience
Case Presentation
Bronchial Asthma in Acute Exacerbation
January 26, 2011Group B6
Clinical InstructorMr. Andy Roy Salabas RN, MN
Overview of the Case
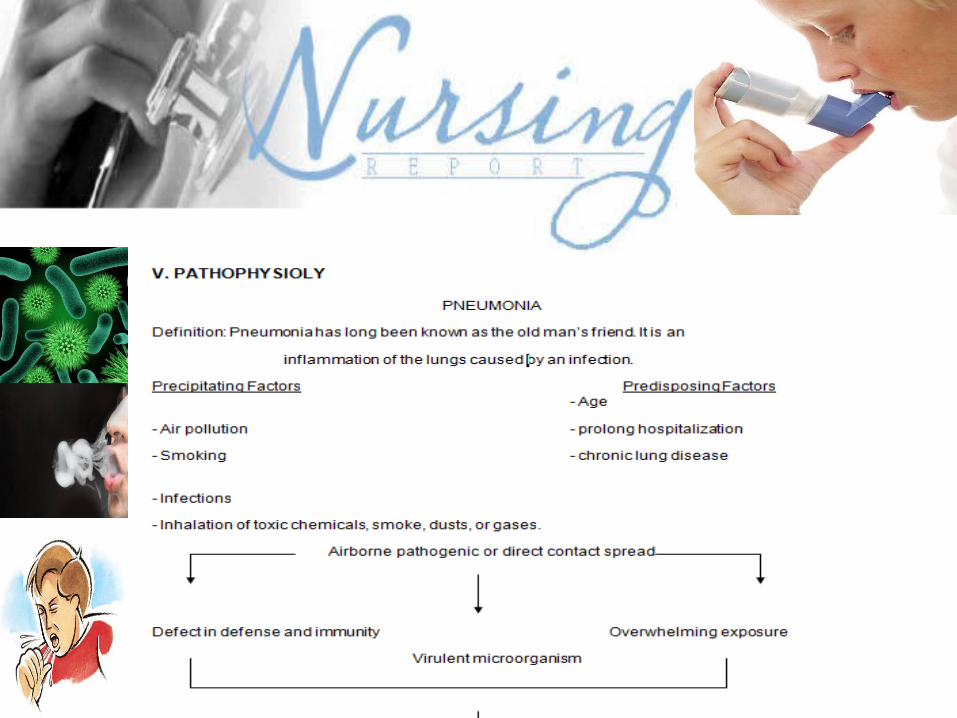
Pneumonia is an inflammation of the lungs usually caused by infection with bacteria, viruses, fungi or other organism. Pneumonitis is a more general term that describes an inflammatory process in the lung tissue that may predispose a patient to or a place at risk of microbial invasion. Spread by infected respiratory droplets thru person-person contact. According to UNICEF, Pneumonia rank as the number 5 top most leading cause of death in the Philippines and it comprises 1, 521, 912 persons being affected.(www.UNICEF.org-infobycountry-Philippines)
Pneumonia is a particular concern for older adults and people with chronic illnesses or impaired immune systems, but it also can strike young, healthy people. Worldwide, it's a leading cause of death in children, many of them younger than a year old.
There are more than 50 kinds of pneumonia ranging in seriousness from mild to life-threatening. Although signs and symptoms vary, many cases of pneumonia develop suddenly, with chest pain, fever, chills, cough and shortness of breath. Infection often follows a cold or the flu, but it also can be associated with other illnesses or occur on its own.
We choose patient X our client because the other patients we chose for this study unfortunately died and the group didn’t give care to the patient for the first choice due to her few days of staying.
Objective of the Study
The objective of the study is to bestow quality-nursing care to assigned patient, utilizing the knowledge based on the nursing process and critical thinking skills. This care study aims to guide the student nurses in providing client-centered nursing care while applying critical thinking in all phases of nursing care from assessment to evaluation.
Also, awareness and knowledge of the patient’s disease condition and its corresponding pathophysiology is vital in providing suitable intervention to the client. Thus, with accurate application of physical assessment, actual and potential health problems are being detected and resolved through the nursing care plan.
After completing the care for the patient with Pneumonia the student nurses will be able to:
Utilize the nursing process in the management of patient’s health condition and in giving quality nursing care.
Obtain a complete health data that can be used in the follow-up care.
Impart health teachings about necessary information pertaining to the disease condition.
Understand the course and essence of the chosen care study.
Add up additional knowledge and understanding in the Nursing profession
Scope and Limitation of the Study
The primary concern of the study is health maintenance and detection of actual and potential health problem that could further exacerbate the client’s disease.Nevertheless, the client’s history of present illness including family history is being scrutinized to detect any possible health problem or knowledge deficit regarding family care.
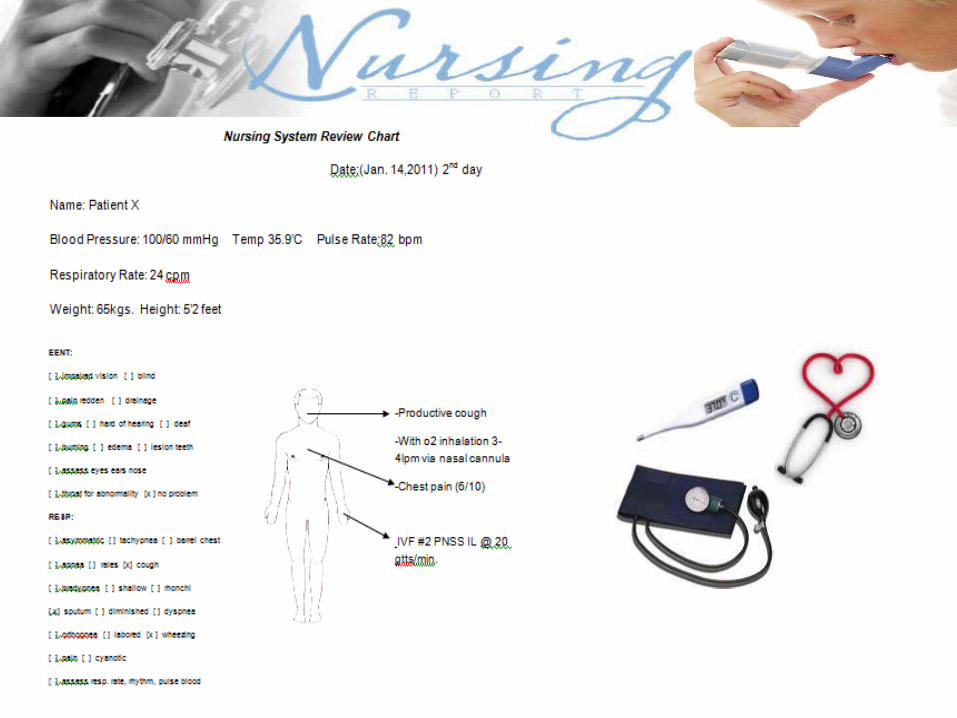
This study will include the effort of the student nurses and the assigned patient in the male ward at Sabal Hospital. The study was directed towards the aforementioned objectives. The study includes the overview of the case, health history of the patient, developmental data, medical management, pathophysiology with anatomy and physiology, nursing assessment, nursing management, referrals and follow-up and evaluation and implication. Attributes like the health history and honesty of the response to the questions asked were the limits of the study. The data gathering for the study is limited from January 13-15 & 19, 2011.
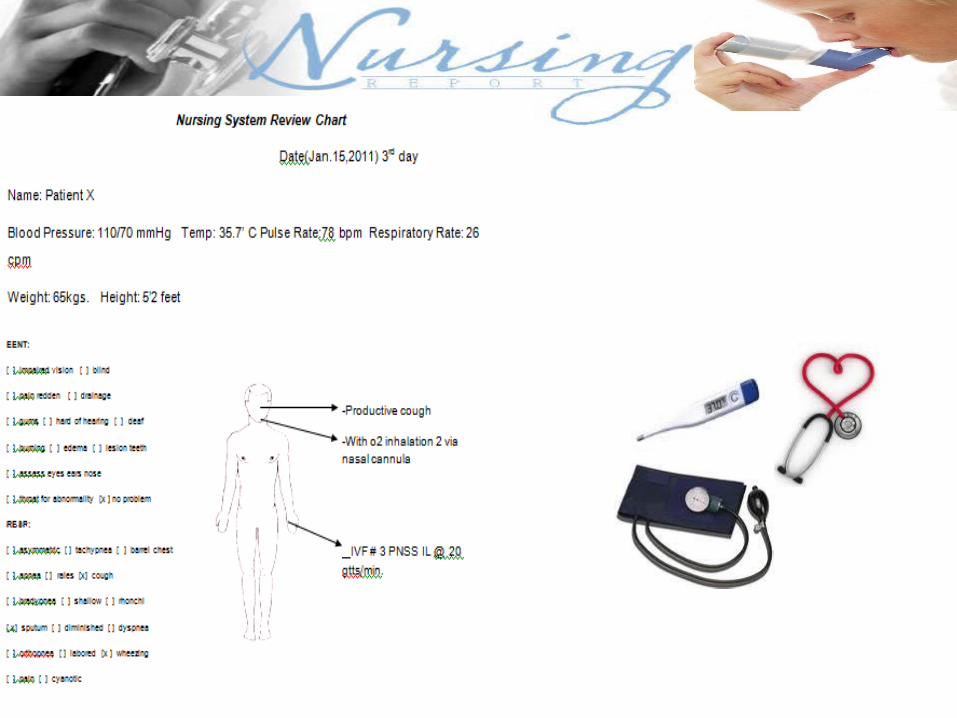
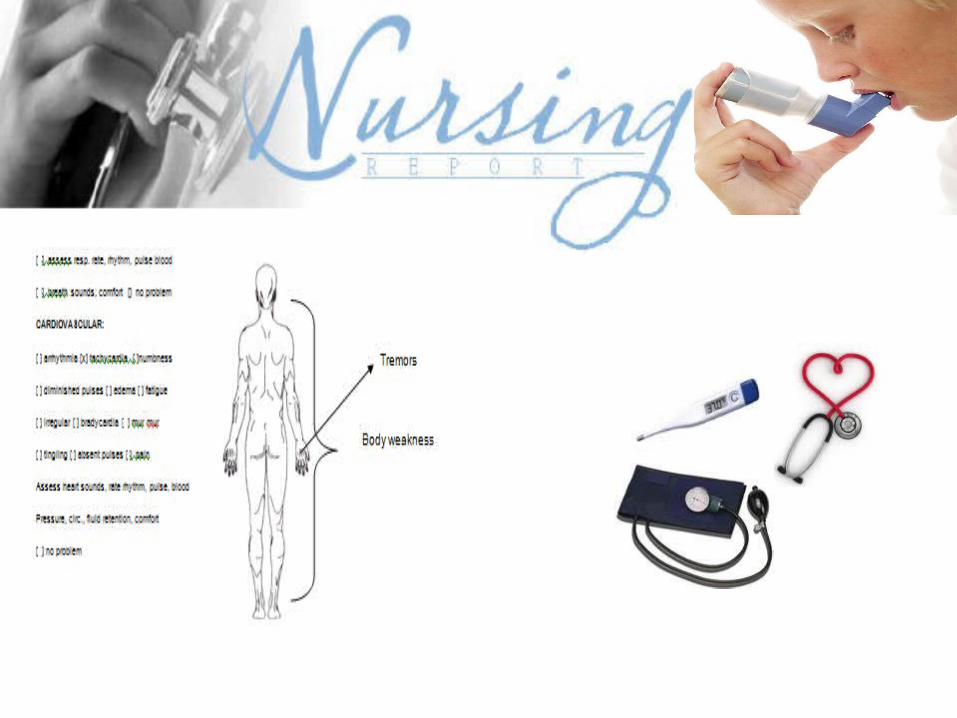
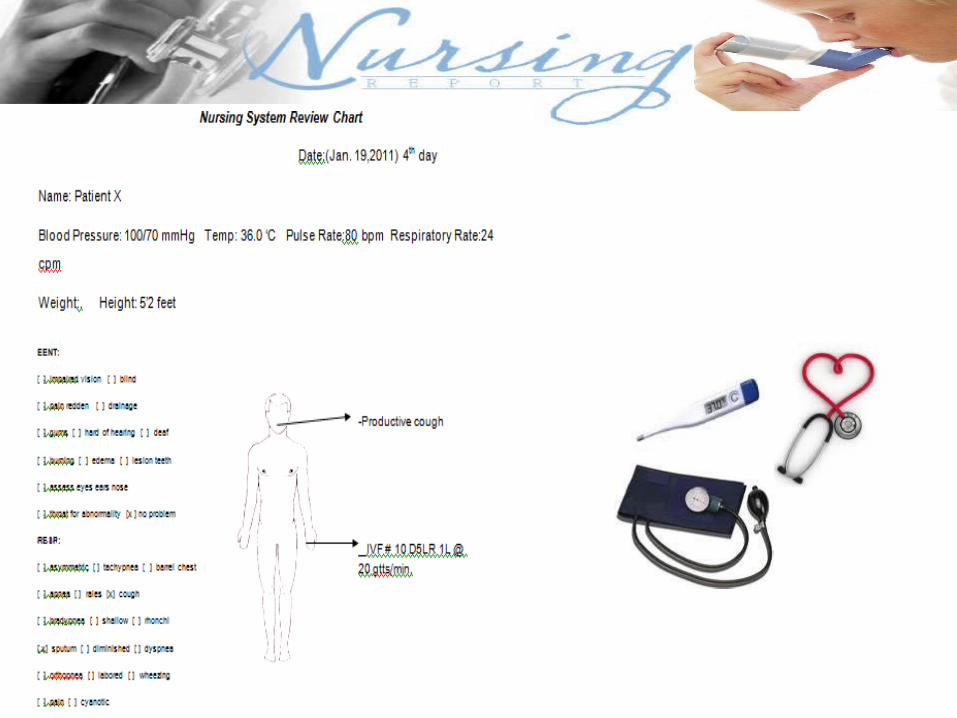
PATIENT PROFILE Name: Patient XAge: 73 years oldAddress: Lugait, Misamis OrientalGender: MaleCivil Status: MarriedDate of Birth: September 3, 1983Place of Birth: Cagayan de Oro CityReligion: Roman CatholicNationality: FilipinoOccupation: FarmerEducational Attainment: Grade 6Height: 5’2”Name of Hospital: Sabal HospitalWeight: 65 kgs.
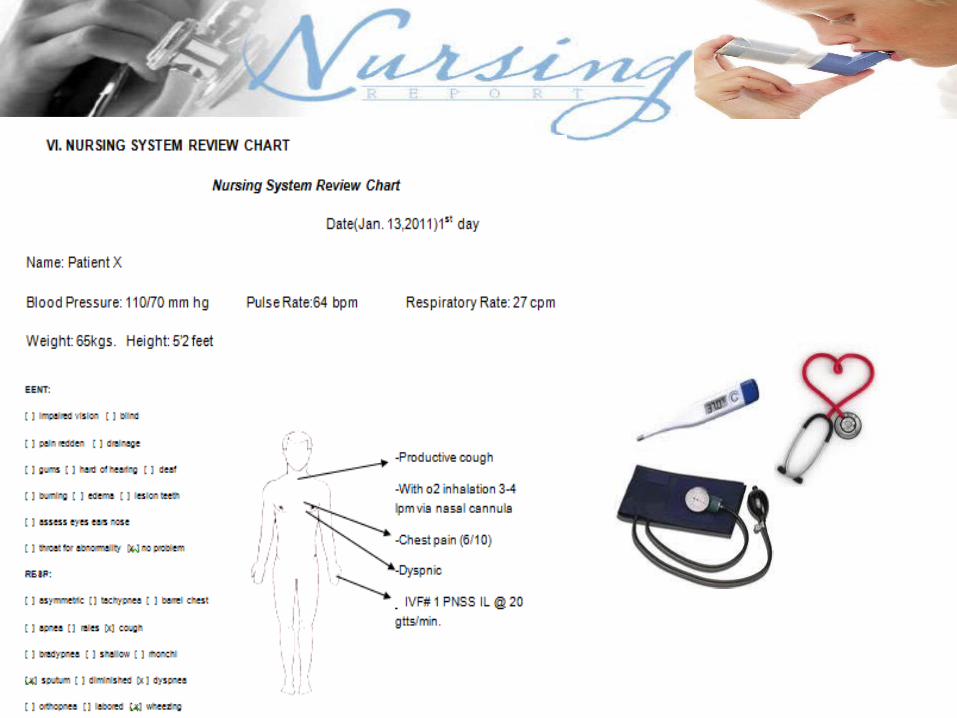
Date of Admission: January 13, 2011Time Admitted: 9:10 pmChief Complaint: Cough and Shortness of BreathAdmitting Physician: Dr. Arthur TanAdmitting Diagnosis: Bronchial Asthma in Acute ExacerbationIncome: 2,500/monthTemperature: 36.2 CPulse: 64 bpmRespiration Rate: 28 cpmBlood Pressure: 110/70 mmHg
HEALTH HISTORY
The informant mentioned that both families had no history of asthma. He also mentioned that his mother side had hypertension.
Patient X is known to be asthmatic since he was 10 years old. At age of 59, patient was admitted for the first time in Bega, Lugait Misamis Oriental for 15 days due to over fatigue.
He is maintaining medications such as cetirizine 10 mg, salbutamol 500mg, doxofylline 400 g, methyl prednisolone 4 g. A known smoker, he is able to consumed two packs of cigarette a day. He also consumed alcohol almost thrice a week. For the past 6 months, our patient was able to experience these conditions:Headache ColdsProductive cough – Occurred on January 10, 2011
HISTORY OF PRESENT ILLNESS A case of 73 years old, Male, Roman Catholic, a farmer from Lugait, Misamis Oriental, admitted for the second time due to shortness of breath.Three days prior to admission, patient felt and complained about cough associated with shortness of breath. Patient was referred to Dr. Arthur Tan.One day prior to admission, patient had washed dishes and was wet under the rain.
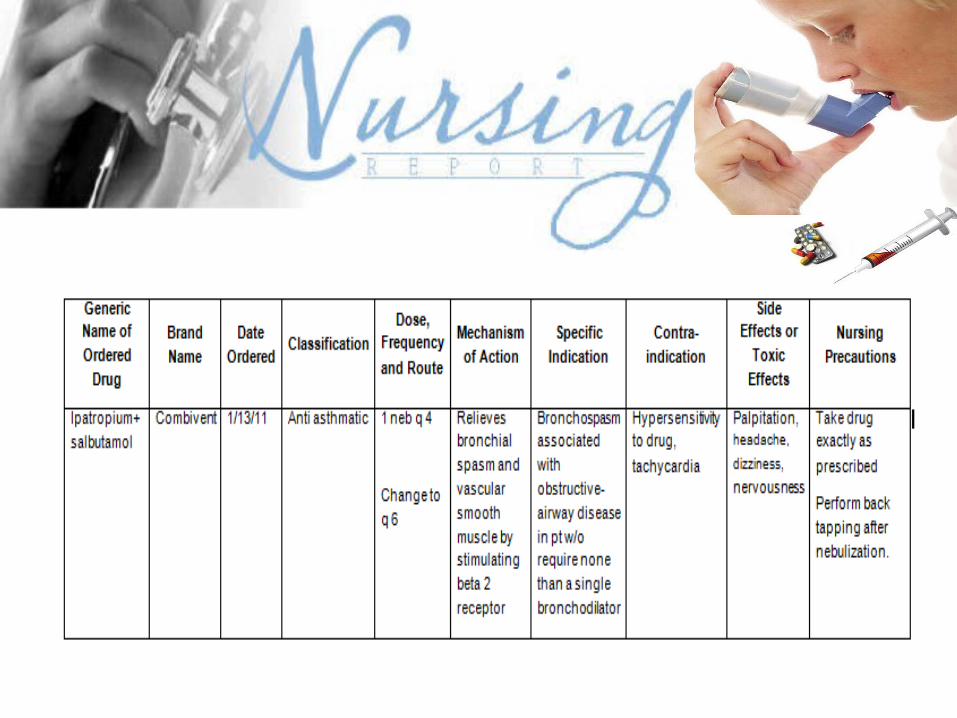
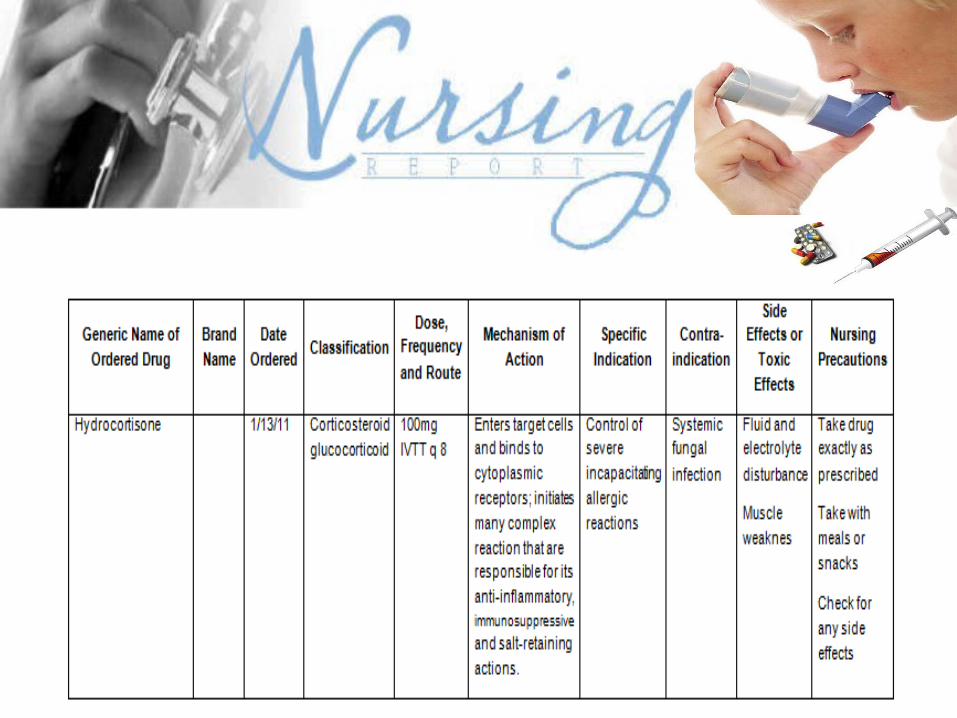
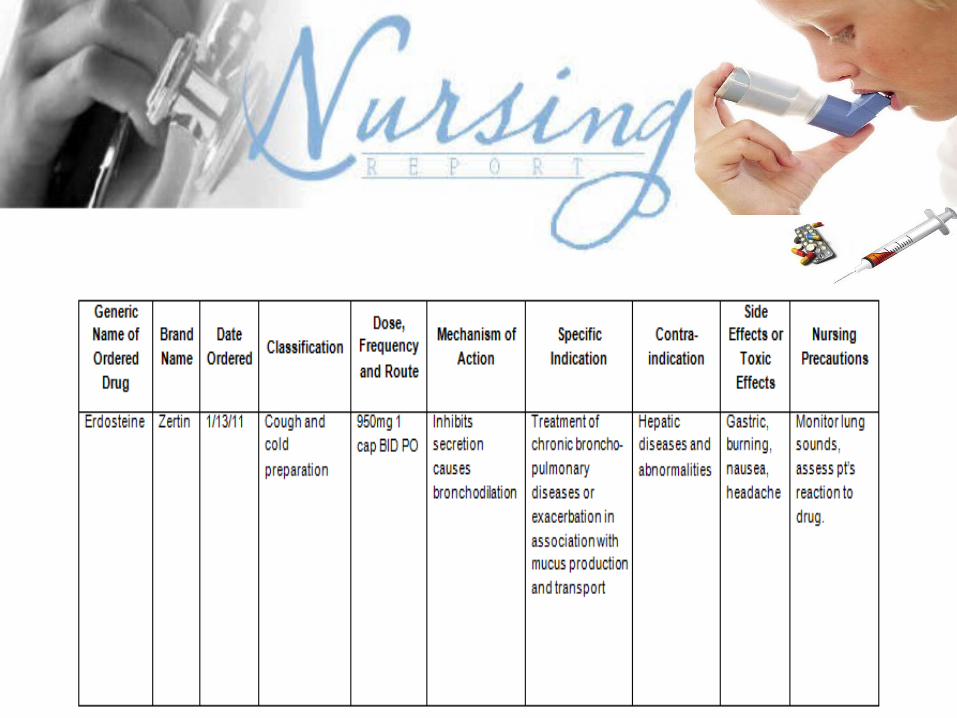
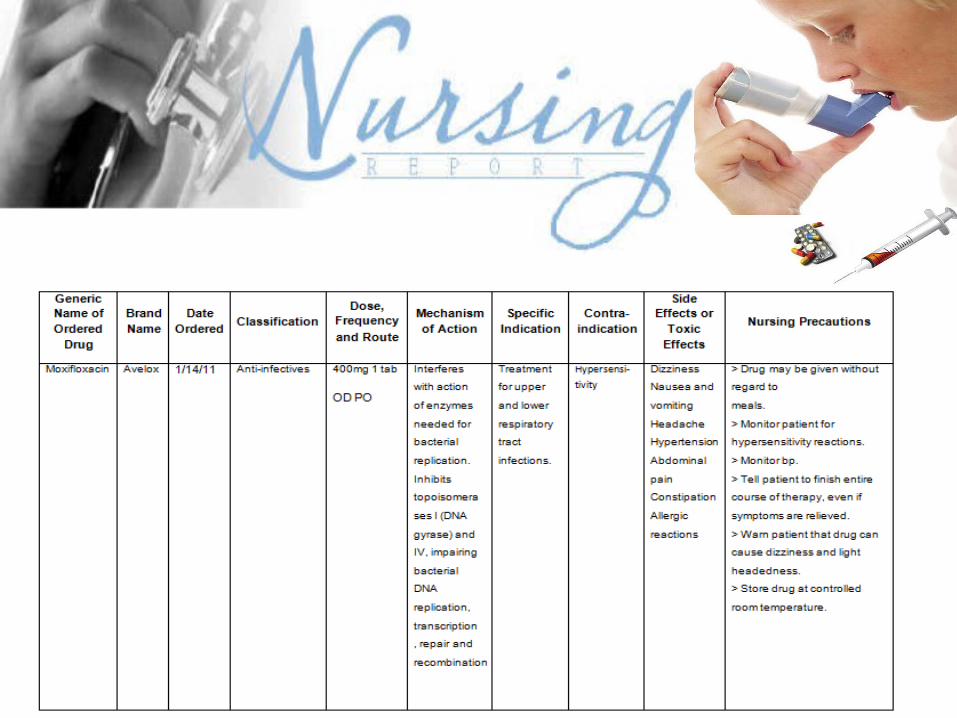
The night prior to admission, patient complained of weakness, coughing and shortnes of breath from too much worked. Then was immediately rushed to Sabal hospital Incorporated, where Blood Pressure was taken and was recorded 110/70mmHg, respiratory rate 28 cpm, pulse rate 64 bpm.Patient was prescribed with erdosteine 750 mg,hydrocortisone 100mg, combivent 1 nebule, sulperazone 1.5 gm and avelox 400mg. Patient was subsequently admitted at 01:10 in the morning.
DEVELOPMENTAL DATA
A.Erik Erikson’s Psychosocial Development Theory Erik Erickson envisioned life as a sequence of levels of achievement. Each stage signals a task that must be achieved. He believed that the greater that task achievement, the healthier the personality of the person. Failure to achieve a task influences the person’s ability to achieve the next task. Stages of Erikson’s Psychosocial Theory are as follows: Infancy Birth – 18 months Trust vs. Mistrust Early Childhood 18 months – 3 years Autonomy vs. Shame & Doubt Late Childhood 3 – 5 years Initiative vs. Guilt School Age 6 – 12 years Industry vs. Inferiority Adolescence 12 – 20 years Identity vs. Role Confusion Young Adulthood18 – 25 years Intimacy vs. Isolation Adulthood 25 – 65 years Generativity vs. Stagnation Maturity 65 years to death Integrity vs. Despair
Basing on this theory, our patient belongs to maturity. The development task at this time is ego integrity versus despair. People who attain ego integrity view life with a sense of wholeness and derive satisfaction from past accomplishments. They view death as an acceptable completion of life. According to Erikson (1963), people who develop integrity accept “one’s one and only life cycle”. By contrast, people who despair often believe they have made poor choices during life and wish they could live life over.
B.Sigmund Freud’s Psychosexual Development Theory
The psychosexual stages of Sigmund Freud are five different developmental periods during which the individual seeks pleasure from different areas of the body associated with sexual feelings.
Our patient falls under Genital Stage of Freud’s theory. It is the fifth and last stage of psychosexual development, the genital stage, from puberty onwards. It actually continues until development stops. This stage represents the major portion of life, and the basic task for the individual is the detachment from the parents. It is also the time when the individual tries to come in terms with unresolved residues of the early childhood. These stages are as follows: Oral Birth to 1 yearAnal 2 – 3 yearsPhallic 4 – 5 yearsLatency 6 – 12 yearsGenital 13 – Up
C.Robert Havighurst’s Developmental Task Theory
A developmental task is a task which arises at or about a certain period in the life of an individual. Havighurst has identified six major age periods: infancy and early childhood (0-5 years), middle childhood (6-12 years), adolescence (13-18 years), early adulthood (19-29 years), middle adulthood (30-60 years), and later maturity (61+). Basing on Havighurst’s Theory, our patient belongs in the later maturity stage.
D. Jean Piaget’s Cognitive Theory of Development
Cognitive development refers to how a person perceives, thinks, and gains understanding of his or her world through the interaction and influence of genetic and learning factors. This is divided into five major phases:
Sensorimotor Phase Birth to 2 yearsPre-conceptual Phase 2 – 3 yearsIntuitive Thought Phase 4 – 6 yearsConcrete Operations Phase 7 – 11 yearsFormal Operational Phase 12 – adulthood
Basing on this theory, our patient belongs to the Formal operational stage. Changes in the cognitive structures occur as a person ages. It is believed that progressive loss of neurons occurs, decreased of blood flow in the brain, the meninges appear to thicken, and brain metabolism slows. In older adults, changes in cognitive abilities are more often a difference in speed than in ability.
Overall the older adult maintains intelligence, problem solving, judgment, creativity, and other well – practiced cognitive skills. Intellectual loss generally reflects a disease process such as atherosclerosis, which causes the blood vessels to narrow and diminishes perfusion of nutrients to the brain. Most older adults do not experience cognitive impairments.
Older people need additional time for learning, largely because of the problem of retrieving information. Motivation is also important. It is suggested that the older person should remain mentally active to maintain cognitive ability at the highest possible level.
Lifelong mental activity, particularly verbal activity, helps the older person retain a high level of cognitive function and may help maintain long-term memory. Cognitive impairment that interferes with normal life is not considered part of normal aging.
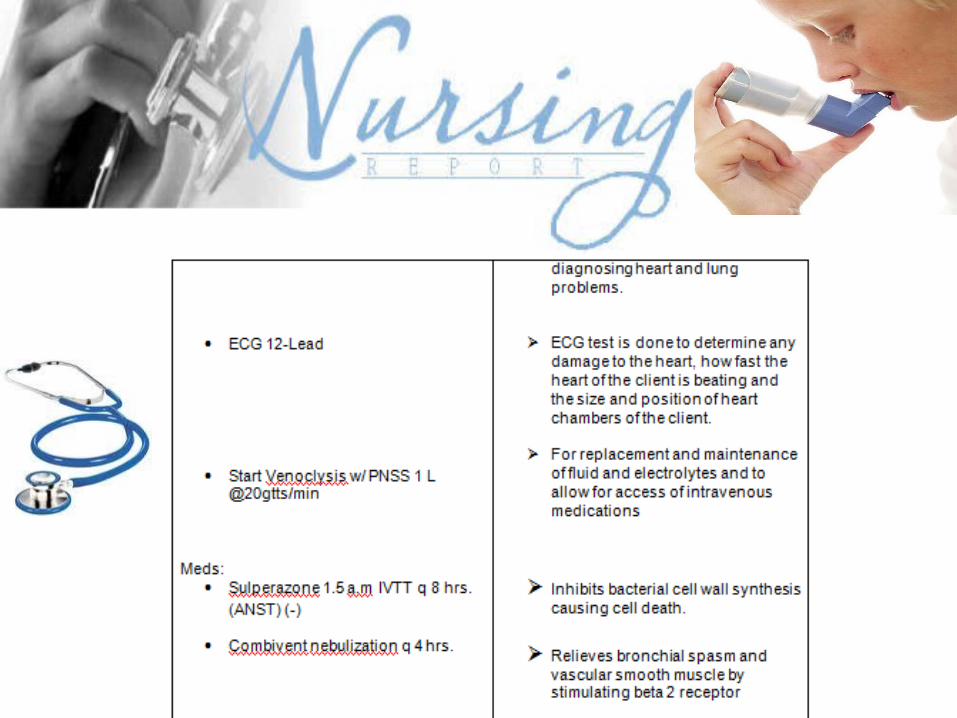
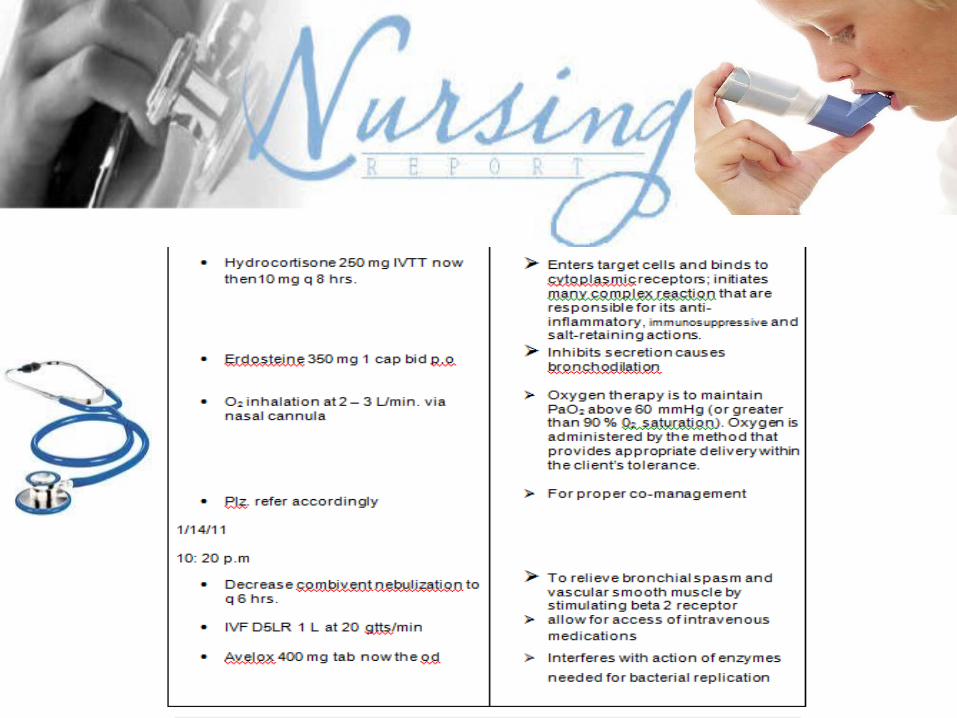
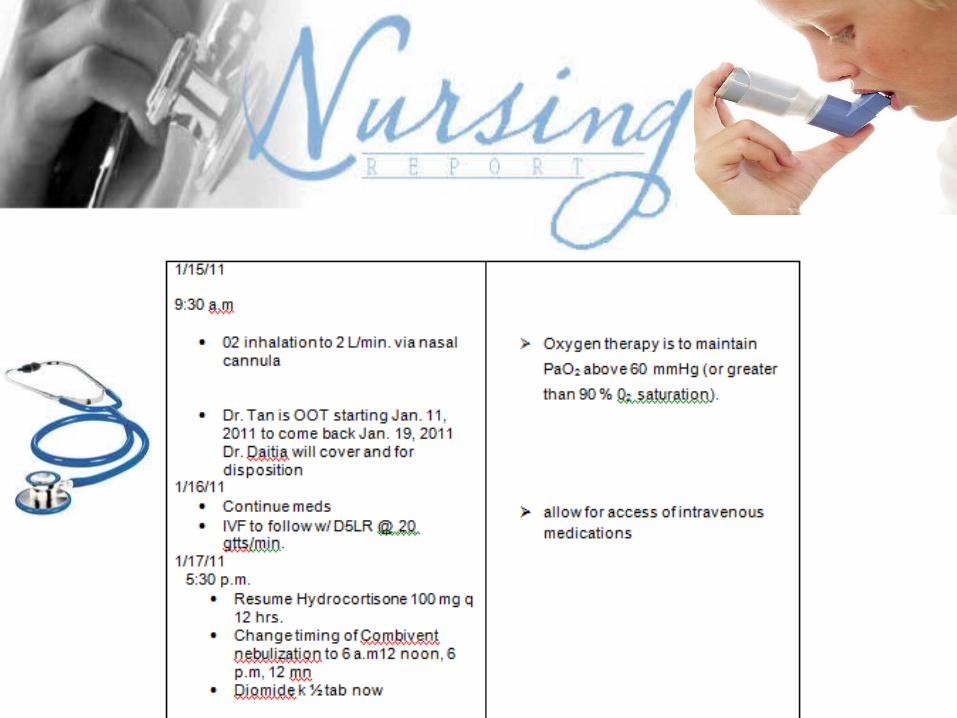
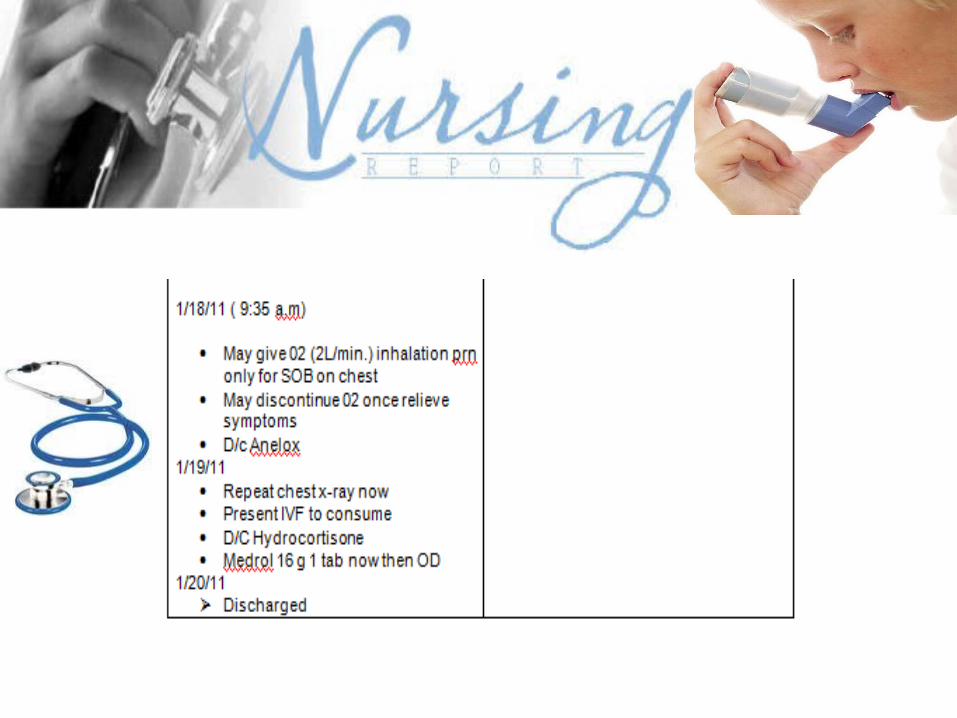
MEDICAL MANAGEMENT A. Medical Orders with Rationale
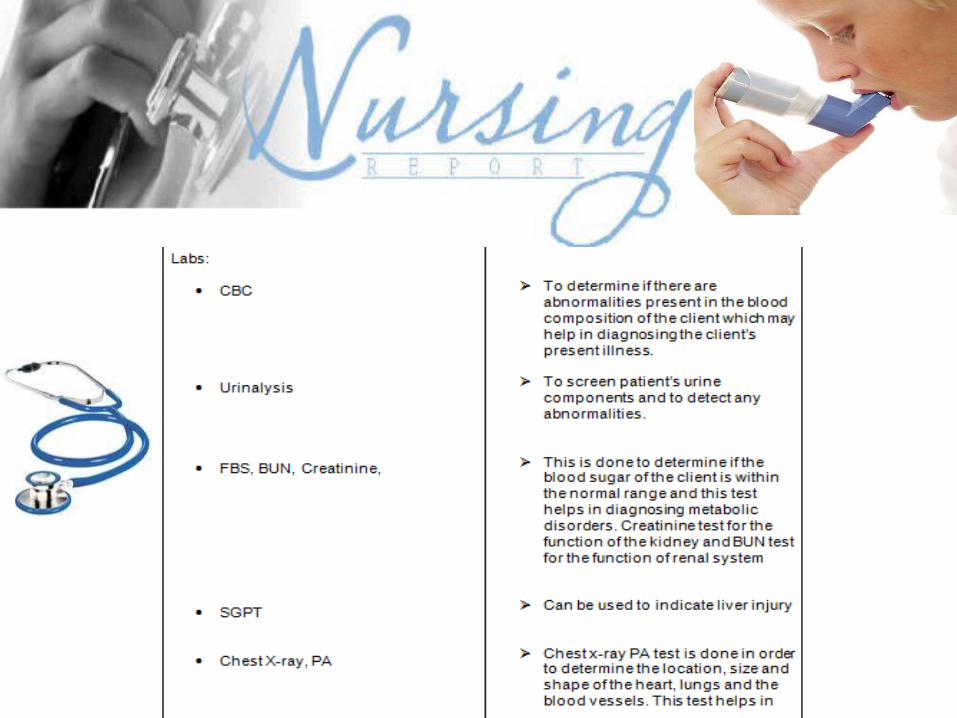
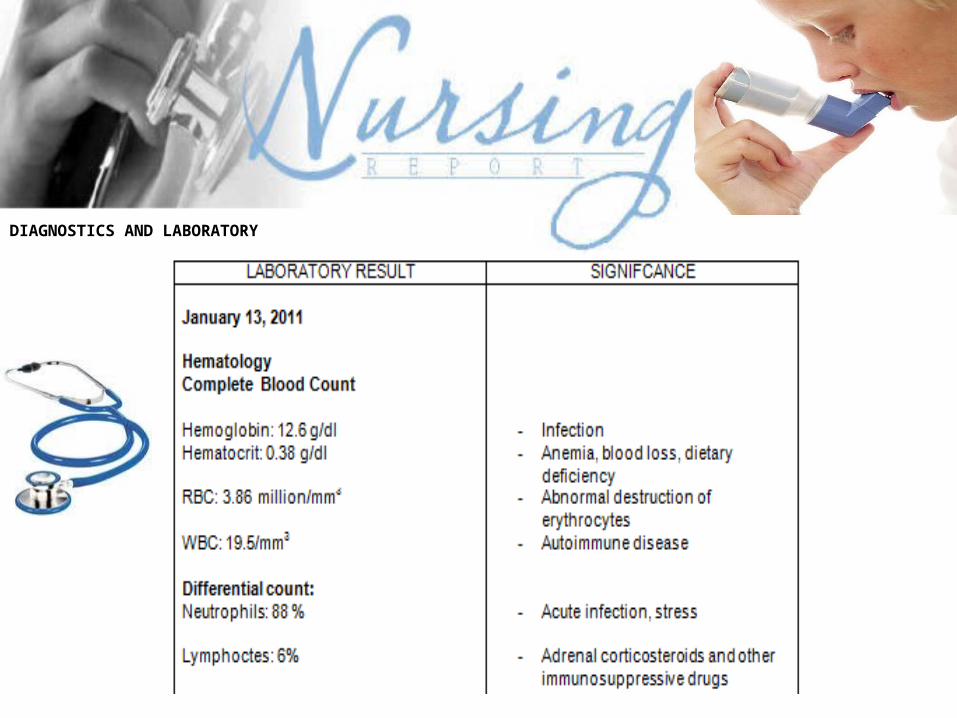
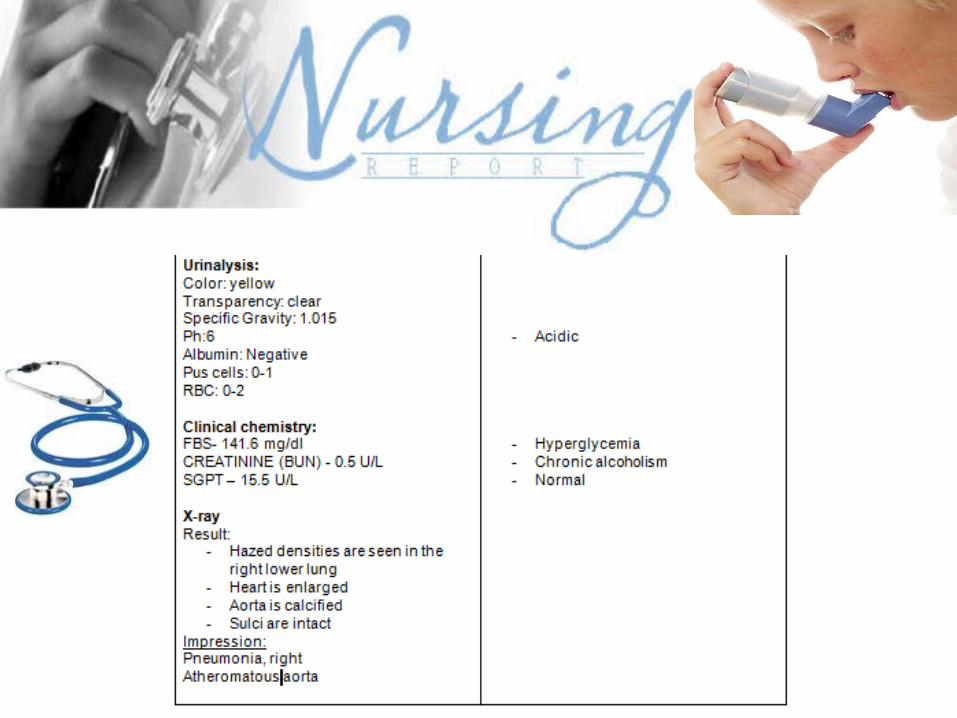
DIAGNOSTICS AND LABORATORY
ANATOMY AND PHYSIOLOGY
The respiratory system is an integrated network of organs and tubes that coordinates the exchange of oxygen and carbon dioxide between an organism and its environment. Harmony is seen in the fact that the respiratory system in animals involves the consumption of oxygen and contribution of carbon dioxide to the environment, while in plants the respiratory system involves the consumption of carbon dioxide and contribution of oxygen to the environment.
In humans, air enters the nose or mouth and travels down different tubes to the lungs, where gas exchange takes place. The diaphragm pulls air in and pushes it out. However, there are many different respiratory systems found across various organisms, including amphibians, many of which can breathe through their skin.
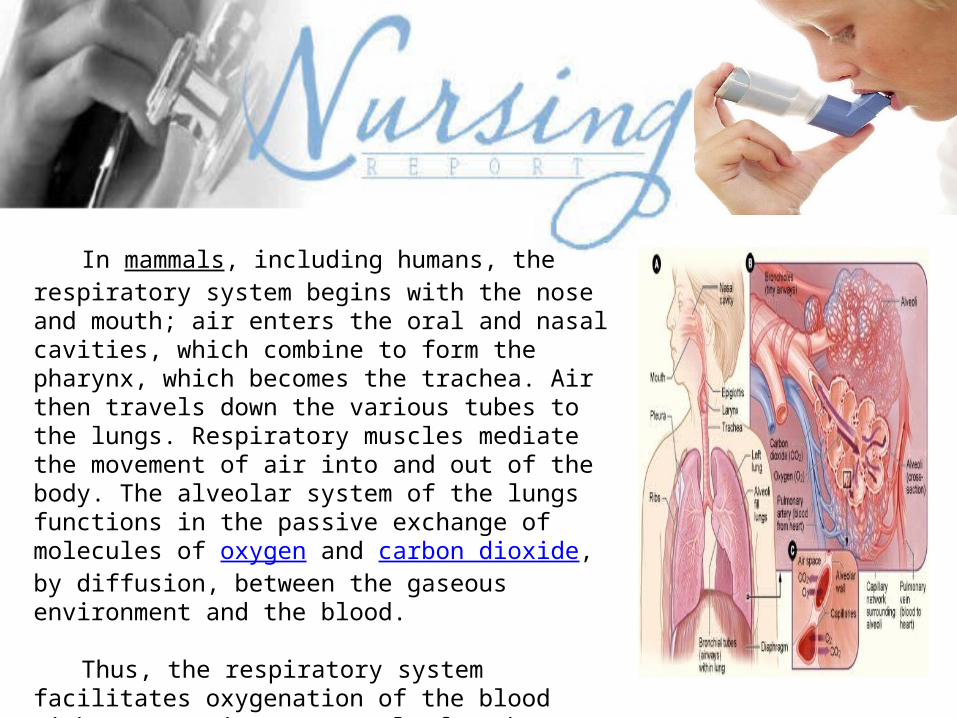
In mammals, including humans, the respiratory system begins with the nose and mouth; air enters the oral and nasal cavities, which combine to form the pharynx, which becomes the trachea. Air then travels down the various tubes to the lungs. Respiratory muscles mediate the movement of air into and out of the body. The alveolar system of the lungs functions in the passive exchange of molecules of oxygen and carbon dioxide, by diffusion, between the gaseous environment and the blood.
Thus, the respiratory system facilitates oxygenation of the blood with a concomitant removal of carbon dioxide and other gaseous metabolic wastes from the circulation. The system also helps to maintain the acid-base balance of the body through the efficient removal of carbon dioxide from the blood.
Anatomy
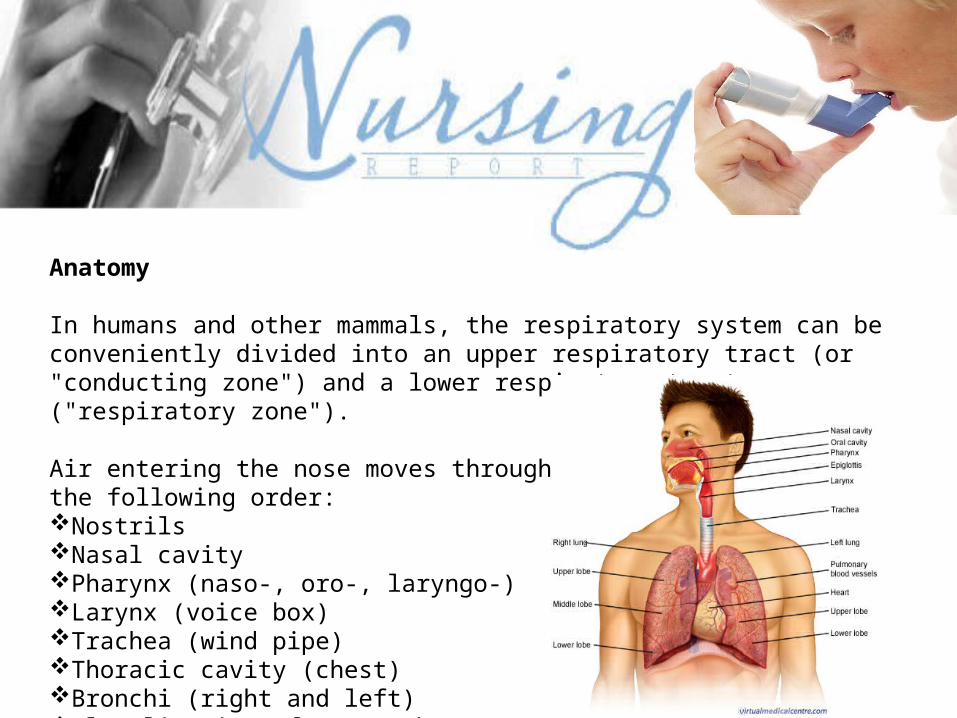
In humans and other mammals, the respiratory system can be conveniently divided into an upper respiratory tract (or "conducting zone") and a lower respiratory tract ("respiratory zone").
Air entering the nose moves through the body in the following order: Nostrils Nasal cavity Pharynx (naso-, oro-, laryngo-) Larynx (voice box) Trachea (wind pipe) Thoracic cavity (chest) Bronchi (right and left) Alveoli (site of gas exchange)
Upper respiratory tract/conducting zone
The upper respiratory tract begins with the nares (nostrils) of the nose, which open into the nasopharynx (nasal cavity). The primary functions of the nasal passages are to: 1) filter, 2) warm, 3) moisten, and 4) provide resonance in speech. Dust and other air impurities can be very harmful to the body, as can extremely cold or dry air. The nasopharnyx opens into the oropharynx (behind the oral cavity). During inhalation, air entering the oropharynx passes into the laryngopharynx and empties into the larynx (voicebox), which contains the vocal cords. Air then continues past the glottis down into the trachea (wind pipe).
Lower respiratory tract/respiratory zone
The trachea leads down to the chest, where it divides into the right and left "main stem" bronchi. The subdivisions of the bronchus are: Primary, secondary, and tertiary divisions (first, second, and third levels). In total, the bronchi divide 16 times into even smaller bronchioles. The bronchioles lead to the respiratory zone of the lungs, which consists of respiratory bronchioles, alveolar ducts, and the alveoli, the multi-lobulated sacs in which most of the gas exchange occurs.
Physiology:
VentilationVentilation of the lungs in humans is carried out by the muscles of respiration, which include intercostal muscles.
ControlVentilation is controlled by the autonomic nervous system. The breathing regulatory center is in the medulla oblongata and the pons, parts of the brain stem containing a series of interconnected neurons that coordinate respiratory movements. The sections are the pneumotaxic center, the apneustic center, and the dorsal and ventral respiratory groups (CRISP 2007). This section of the brain is especially sensitive during infancy, and the neurons can be destroyed if the infant is dropped or shaken violently. The result can be early death due to "shaken baby syndrome" (SIPH 2006).
Inhalation
Inhalation is driven primarily by the diaphragm with help from the intercostal muscles. When the diaphragm contracts, the ribcage expands and the contents of the abdomen are moved downward. The expansion of the ribs results in a greater chest volume, which in turn causes a decrease in intrathoracic pressure, according to Boyle’s Law. When the pressure inside the lungs is lower than the atmospheric pressure outside the body, air moves into the respiratory tract in an attempt to equalize the pressures. At rest, normal respiration is about 10 to 18 breaths per minute, with each inhalation lasting about 2 seconds. Rates of breathing can increase during exercise, fever, or illness. During vigorous inhalation (at rates exceeding 35 breaths per minute), or when approaching respiratory failure, other accessory muscles are recruited for support. During forced inhalation, as when taking a deep breath, the external intercostal muscles and accessory muscles further expand the thoracic cavity and more air moves into the lungs at a greater velocity.
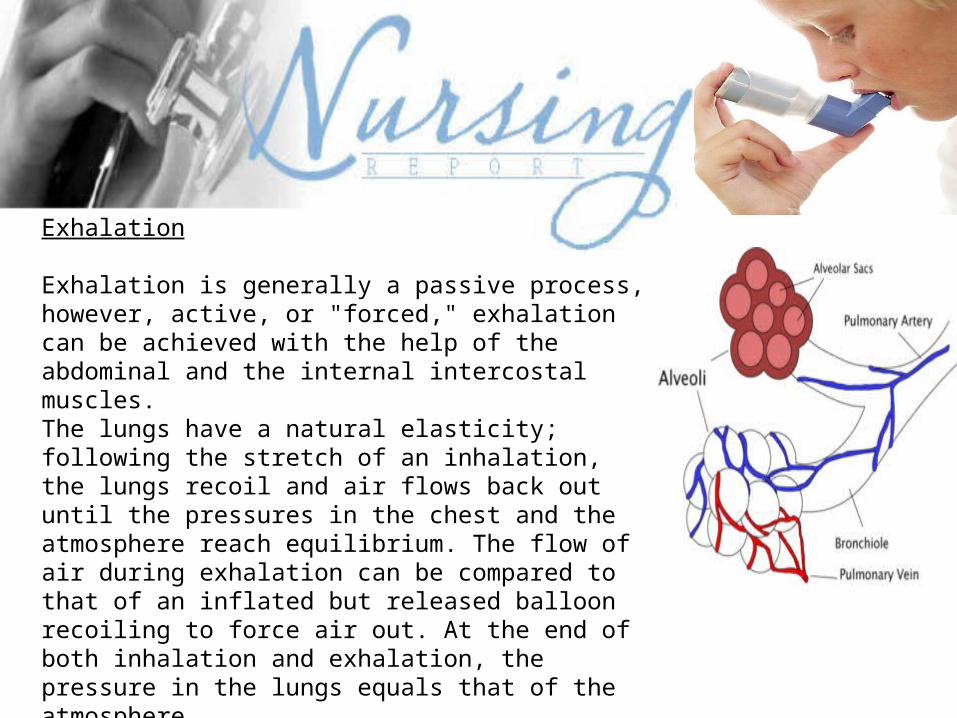
Exhalation
Exhalation is generally a passive process, however, active, or "forced," exhalation can be achieved with the help of the abdominal and the internal intercostal muscles. The lungs have a natural elasticity; following the stretch of an inhalation, the lungs recoil and air flows back out until the pressures in the chest and the atmosphere reach equilibrium. The flow of air during exhalation can be compared to that of an inflated but released balloon recoiling to force air out. At the end of both inhalation and exhalation, the pressure in the lungs equals that of the atmosphere. During forced exhalation, as when blowing out a candle, the abdominal muscles and internal intercostal muscles generate extra abdominal and thoracic pressure, which forces air out of the lungs with greater volume and with greater velocity.
Gas exchangeThe major function of the respiratory system is gas exchange. As gas exchange occurs in humans, the acid-base balance of the body is maintained as a component of homeostasis. In the absence of proper ventilation, two conditions could occur: 1)respiratory acidosis, a life threatening condition caused by a deficiency of ventilation, or 2)respiratory alkalosis, caused by an excess of ventilation, or hyperventilation. The actual gas exchange occurs at the alveoli, the basic functional component of the lungs. The alveolar walls are extremely thin (approx. 0.2 micrometers), and are permeable to gases. Pulmonary capillaries line the alveoli; the walls of these capillaries are also thin enough to permit gas exchange.
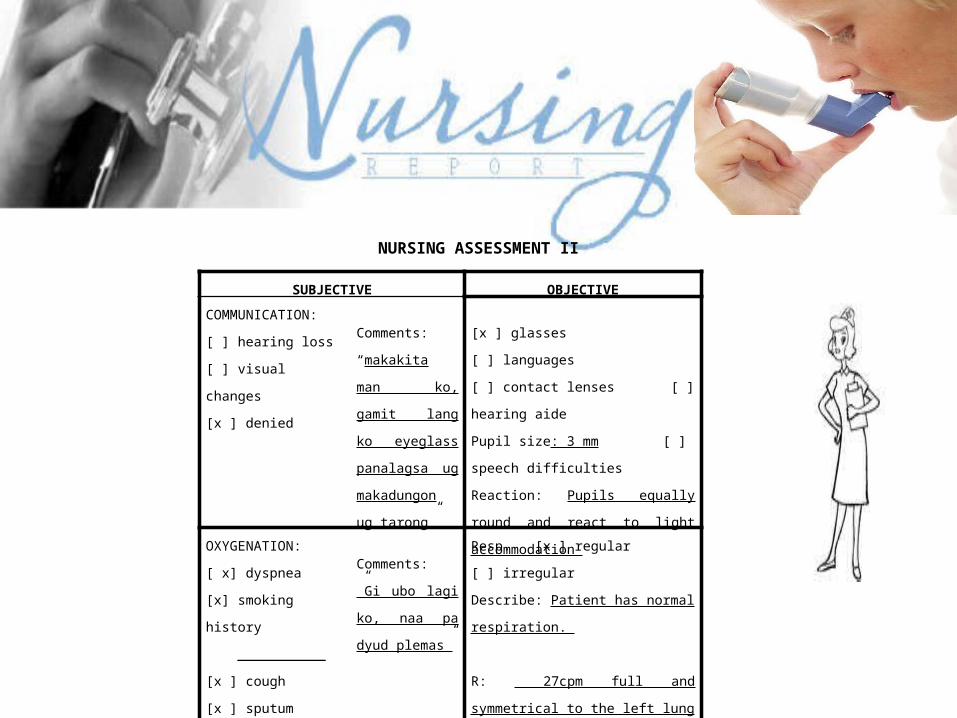
NURSING ASSESSMENT II
SUBJECTIVE OBJECTIVE
COMMUNICATION:
[ ] hearing loss
[ ] visual changes
[x ] denied
Comments:
“makakita man
ko, gamit lang ko
eyeglass
panalagsa ug
makadungon ug
tarong”
[x ] glasses [ ] languages
[ ] contact lenses [ ] hearing aide
Pupil size: 3 mm [ ] speech
difficulties
Reaction: Pupils equally round and
react to light accommodation
OXYGENATION:
[ x] dyspnea
[x] smoking history
___________
[x ] cough
[x ] sputum
[ ] denied
Comments: ”Gi
ubo lagi ko, naa
pa dyud plemas”
Resp. [x ] regular [ ] irregular
Describe: Patient has normal
respiration.
R: 27cpm full and symmetrical to the
left lung
L: 27cpm full and symmetrical to the
right lung
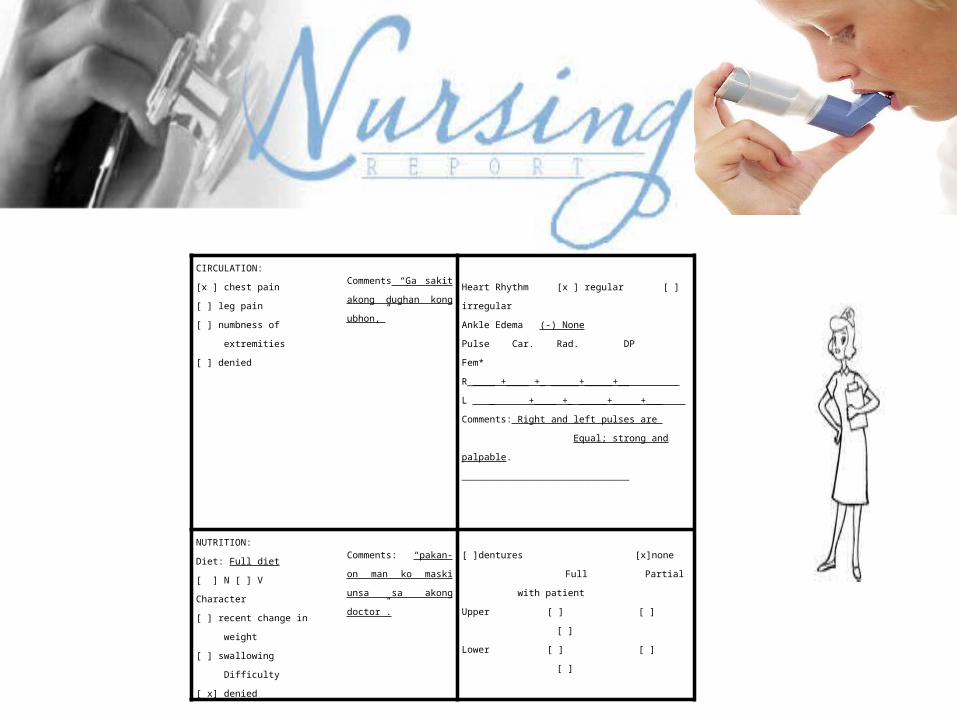
CIRCULATION:
[x ] chest pain
[ ] leg pain
[ ] numbness of
extremities
[ ] denied
Comments “Ga sakit
akong dughan kong
ubhon,”
Heart Rhythm [x ] regular [ ] irregular
Ankle Edema (-) None
Pulse Car. Rad. DP Fem*
R_____ +____ +_ _____+_____+__
L _ +____ +_ _____+_____+___
Comments: Right and left pulses are
Equal; strong and palpable.
______________________________
NUTRITION:
Diet: Full diet
[ ] N [ ] V
Character
[ ] recent change in
weight
[ ] swallowing
Difficulty
[ x] denied
Comments: “pakan-on
man ko maski unsa sa
akong doctor”.
[ ]dentures [x]none
Full Partial with patient
Upper [ ] [ ] [ ]
Lower [ ] [ ] [ ]
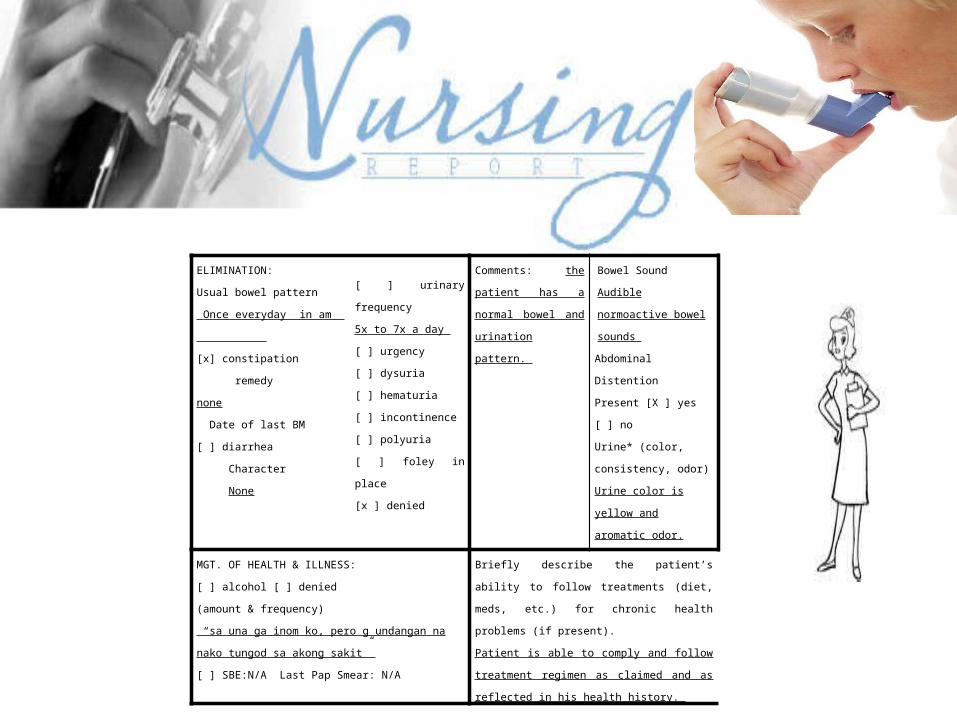
ELIMINATION:
Usual bowel pattern
Once everyday in am
[x] constipation
remedy
none
Date of last BM
[ ] diarrhea
Character
None
[ ] urinary frequency
5x to 7x a day
[ ] urgency
[ ] dysuria
[ ] hematuria
[ ] incontinence
[ ] polyuria
[ ] foley in place
[x ] denied
Comments: the patient
has a normal bowel
and urination pattern.
Bowel Sound
Audible normoactive
bowel sounds
Abdominal Distention
Present [X ] yes [ ] no
Urine* (color,
consistency, odor)
Urine color is yellow and
aromatic odor.
MGT. OF HEALTH & ILLNESS:
[ ] alcohol [ ] denied
(amount & frequency)
“sa una ga inom ko, pero g undangan na nako tungod
sa akong sakit”
[ ] SBE:N/A Last Pap Smear: N/A
Briefly describe the patient’s ability to follow
treatments (diet, meds, etc.) for chronic health
problems (if present).
Patient is able to comply and follow treatment
regimen as claimed and as reflected in his health
history.
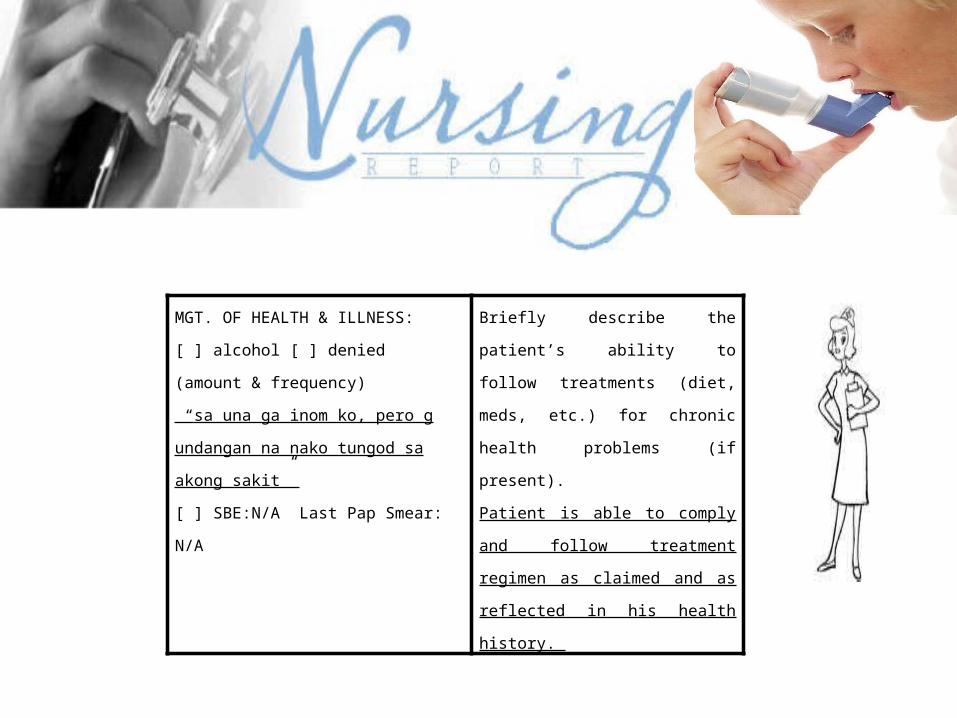
MGT. OF HEALTH & ILLNESS:
[ ] alcohol [ ] denied
(amount & frequency)
“sa una ga inom ko, pero g undangan
na nako tungod sa akong sakit”
[ ] SBE:N/A Last Pap Smear: N/A
Briefly describe the patient’s ability
to follow treatments (diet, meds,
etc.) for chronic health problems (if
present).
Patient is able to comply and follow
treatment regimen as claimed and
as reflected in his health history.
SUBJECTIVE
OBJECTIVE
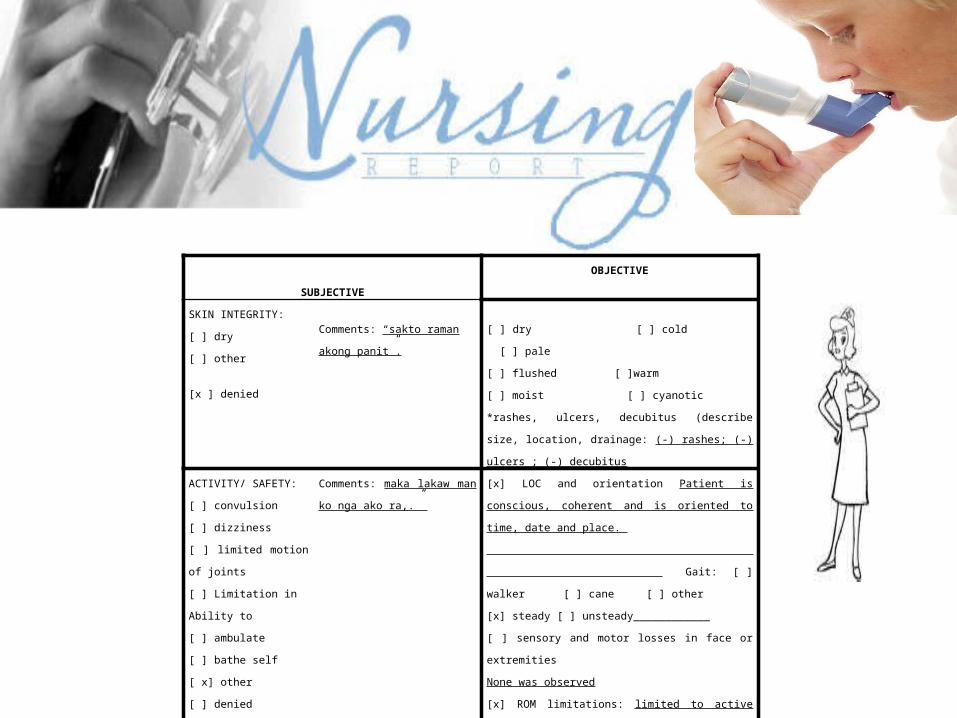
SKIN INTEGRITY:
[ ] dry
[ ] other
[x ] denied
Comments: “sakto raman akong
panit”.
[ ] dry [ ] cold [ ] pale
[ ] flushed [ ]warm
[ ] moist [ ] cyanotic
*rashes, ulcers, decubitus (describe size, location,
drainage: (-) rashes; (-) ulcers ; (-) decubitus
ACTIVITY/ SAFETY:
[ ] convulsion
[ ] dizziness
[ ] limited motion of joints
[ ] Limitation in
Ability to
[ ] ambulate
[ ] bathe self
[ x] other
[ ] denied
Comments: maka lakaw man ko
nga ako ra,.”
[x] LOC and orientation Patient is conscious, coherent
and is oriented to time, date and place.
Gait: [ ]
walker [ ] cane [ ] other
[x] steady [ ] unsteady____________
[ ] sensory and motor losses in face or extremities
None was observed
[x] ROM limitations: limited to active ROM.
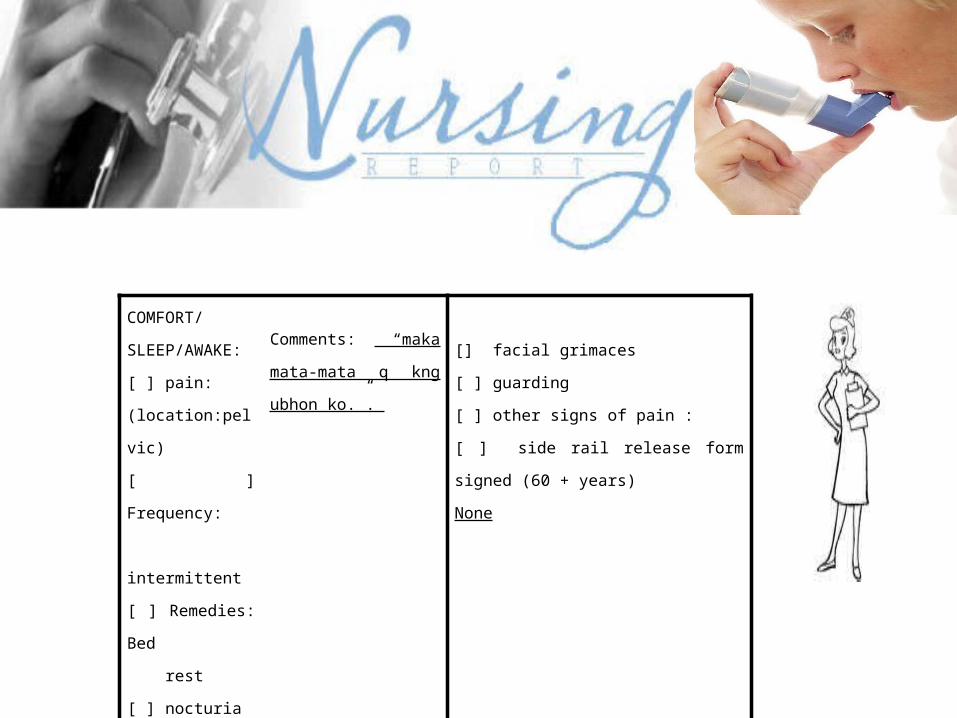
COMFORT/
SLEEP/AWAKE:
[ ] pain:
(location:pelvic)
[ ] Frequency:
intermittent
[ ] Remedies: Bed
rest
[ ] nocturia
[ x] sleep
difficulties
[ ] denied
Comments: “maka
mata-mata q kng ubhon
ko.”.
[] facial grimaces
[ ] guarding
[ ] other signs of pain :
[ ] side rail release form signed (60 +
years)
None
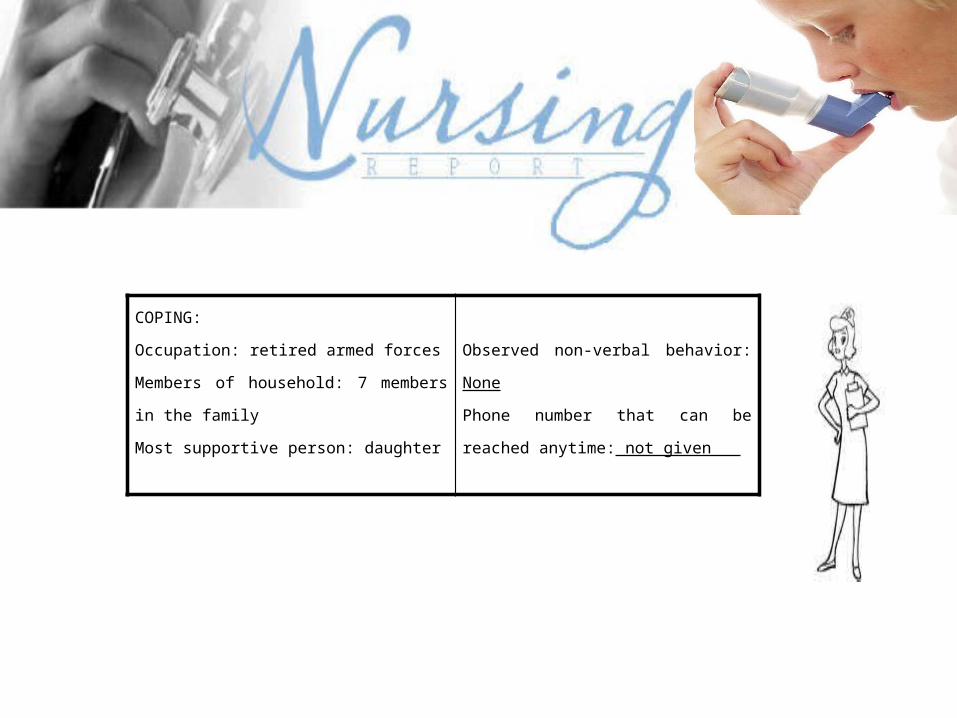
COPING:
Occupation: retired armed forces
Members of household: 7 members in the
family
Most supportive person: daughter
Observed non-verbal behavior: None
Phone number that can be reached
anytime: not given
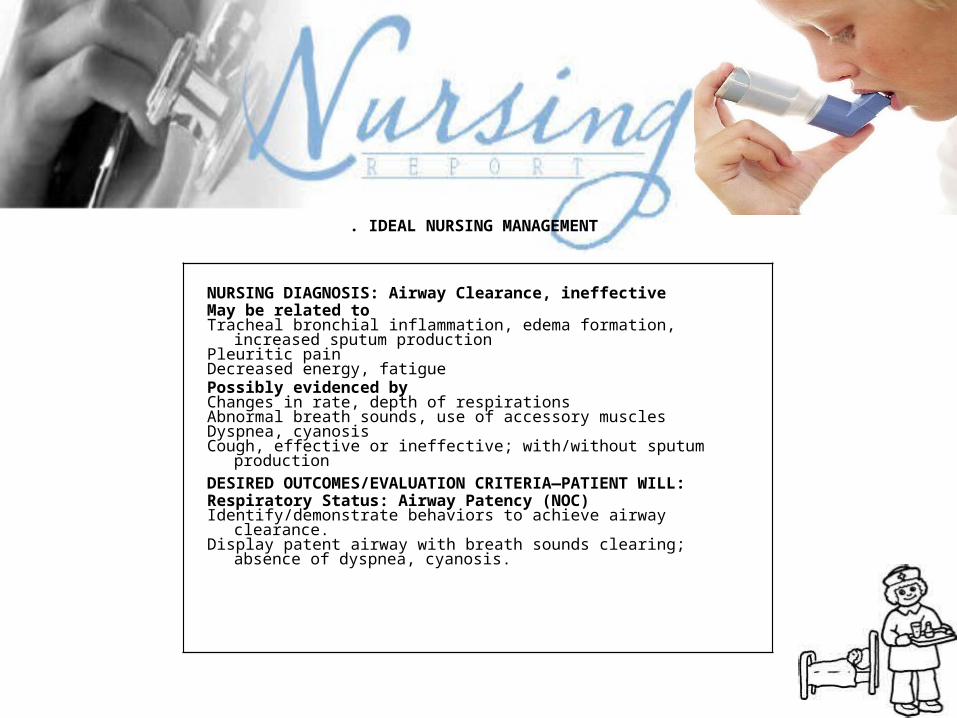
NURSING DIAGNOSIS: Airway Clearance, ineffectiveMay be related toTracheal bronchial inflammation, edema formation, increased
sputum productionPleuritic painDecreased energy, fatiguePossibly evidenced byChanges in rate, depth of respirationsAbnormal breath sounds, use of accessory musclesDyspnea, cyanosisCough, effective or ineffective; with/without sputum productionDESIRED OUTCOMES/EVALUATION CRITERIA—PATIENT WILL:Respiratory Status: Airway Patency (NOC)Identify/demonstrate behaviors to achieve airway clearance.Display patent airway with breath sounds clearing; absence of
dyspnea, cyanosis.
. IDEAL NURSING MANAGEMENT
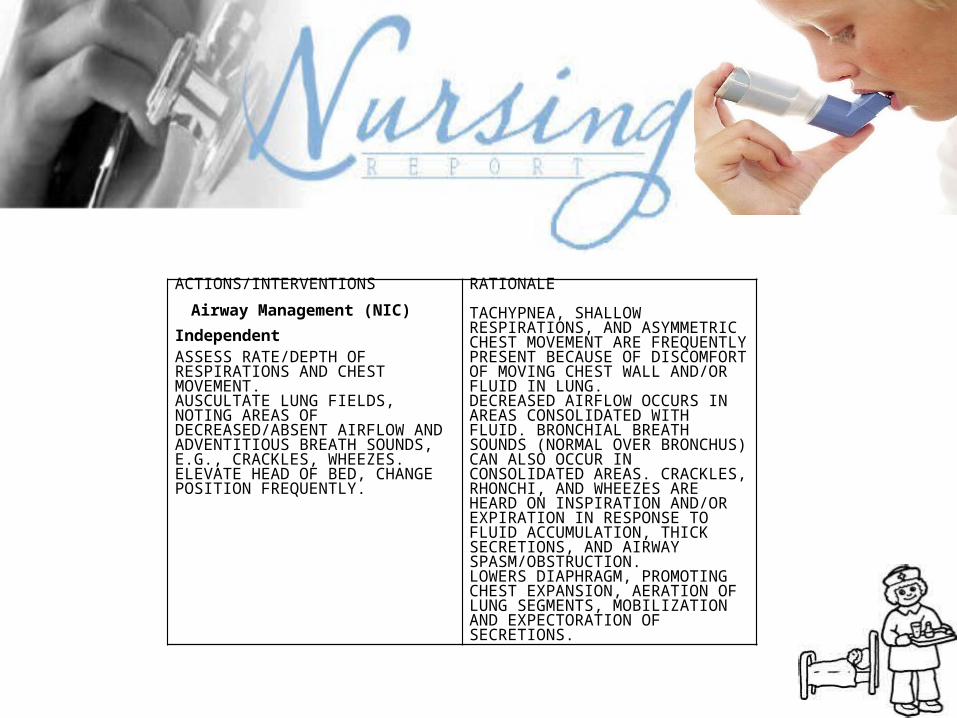
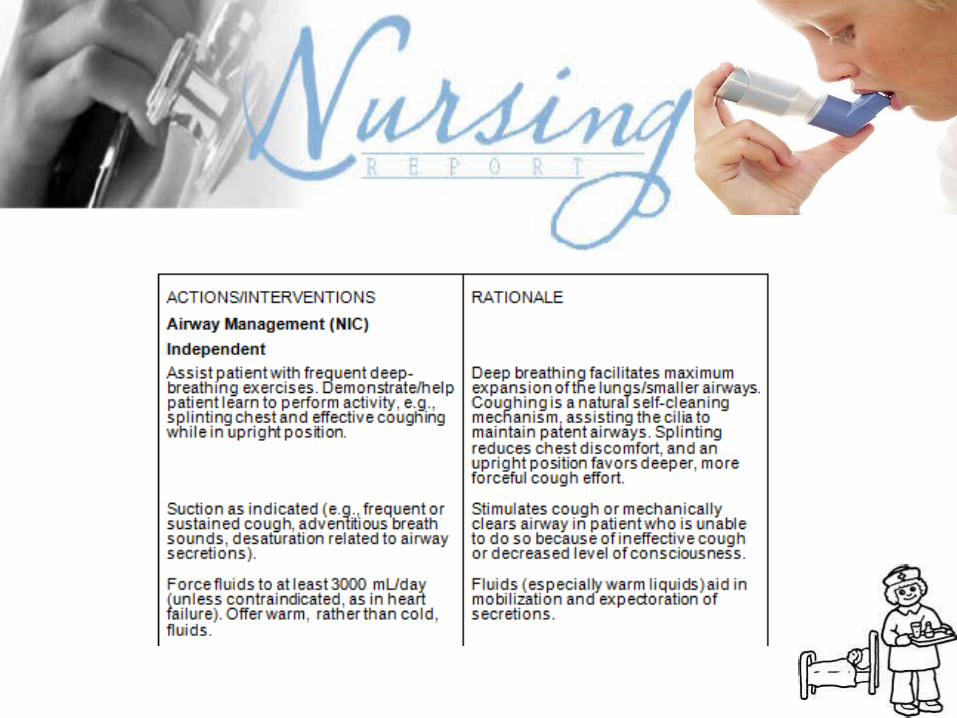
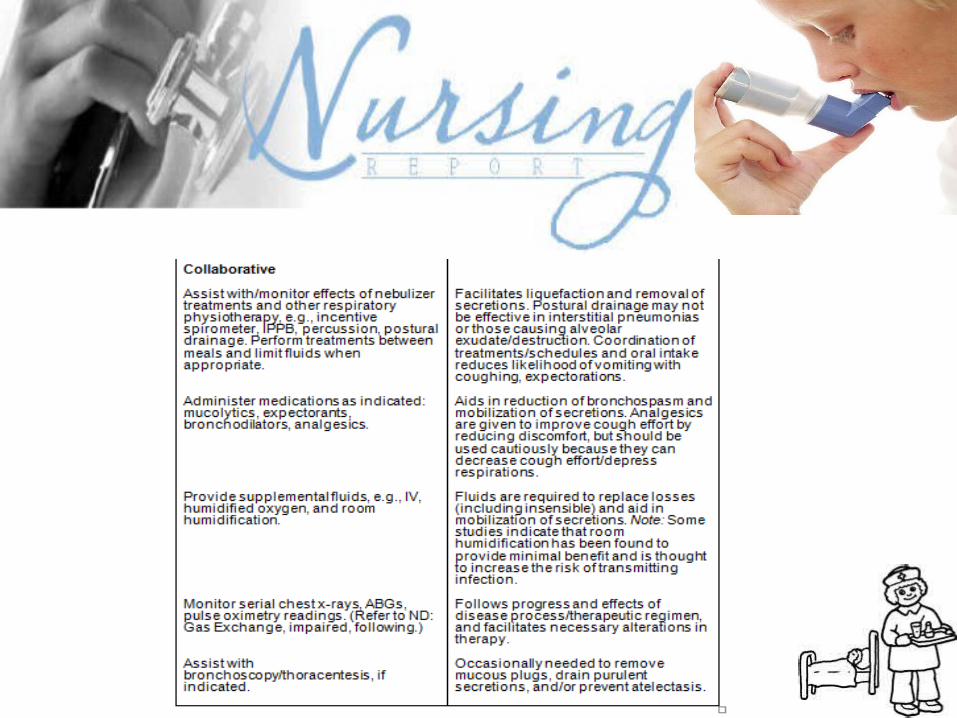
ACTIONS/INTERVENTIONS
Airway Management (NIC)
IndependentASSESS RATE/DEPTH OF RESPIRATIONS AND CHEST MOVEMENT.AUSCULTATE LUNG FIELDS, NOTING AREAS OF DECREASED/ABSENT AIRFLOW AND ADVENTITIOUS BREATH SOUNDS, E.G., CRACKLES, WHEEZES.ELEVATE HEAD OF BED, CHANGE POSITION FREQUENTLY.
RATIONALE
TACHYPNEA, SHALLOW RESPIRATIONS, AND ASYMMETRIC CHEST MOVEMENT ARE FREQUENTLY PRESENT BECAUSE OF DISCOMFORT OF MOVING CHEST WALL AND/OR FLUID IN LUNG.DECREASED AIRFLOW OCCURS IN AREAS CONSOLIDATED WITH FLUID. BRONCHIAL BREATH SOUNDS (NORMAL OVER BRONCHUS) CAN ALSO OCCUR IN CONSOLIDATED AREAS. CRACKLES, RHONCHI, AND WHEEZES ARE HEARD ON INSPIRATION AND/OR EXPIRATION IN RESPONSE TO FLUID ACCUMULATION, THICK SECRETIONS, AND AIRWAY SPASM/OBSTRUCTION.LOWERS DIAPHRAGM, PROMOTING CHEST EXPANSION, AERATION OF LUNG SEGMENTS, MOBILIZATION AND EXPECTORATION OF SECRETIONS.
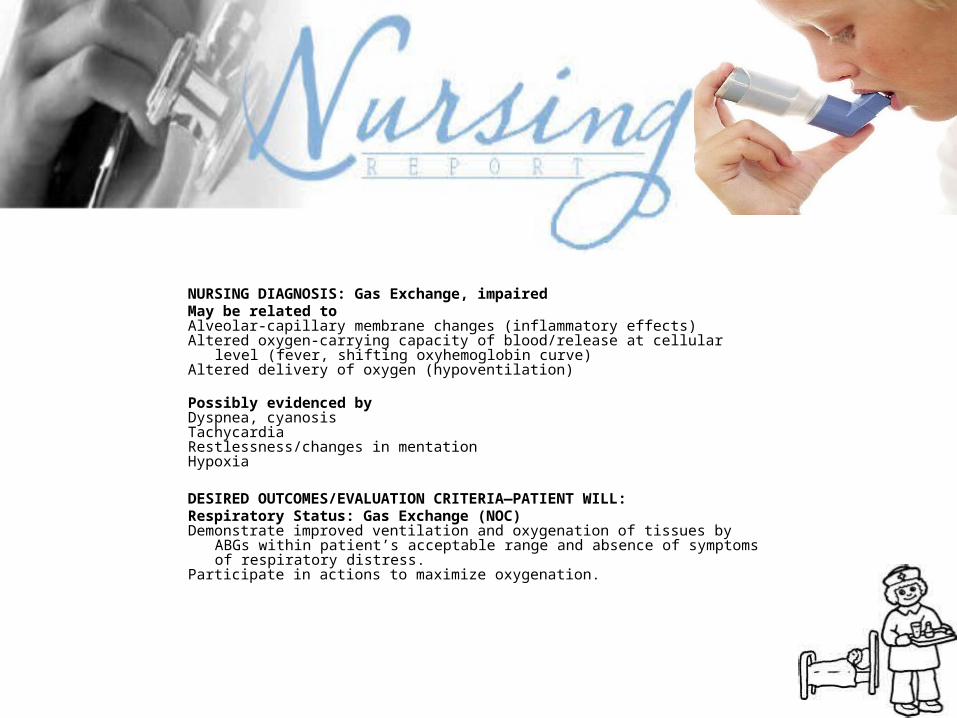
NURSING DIAGNOSIS: Gas Exchange, impairedMay be related toAlveolar-capillary membrane changes (inflammatory effects)Altered oxygen-carrying capacity of blood/release at cellular level (fever,
shifting oxyhemoglobin curve)Altered delivery of oxygen (hypoventilation)
Possibly evidenced byDyspnea, cyanosisTachycardiaRestlessness/changes in mentationHypoxia
DESIRED OUTCOMES/EVALUATION CRITERIA—PATIENT WILL:Respiratory Status: Gas Exchange (NOC)Demonstrate improved ventilation and oxygenation of tissues by ABGs within
patient’s acceptable range and absence of symptoms of respiratory distress.
Participate in actions to maximize oxygenation.
ACTIONS/INTERVENTIONS
Respiratory Monitoring (NIC)
IndependentASSESS RESPIRATORY RATE, DEPTH, AND EASE.OBSERVE COLOR OF SKIN, MUCOUS MEMBRANES, AND NAILBEDS, NOTING PRESENCE OF PERIPHERAL CYANOSIS (NAILBEDS) OR CENTRAL CYANOSIS (CIRCUMORAL).ASSESS MENTAL STATUS.MONITOR HEART RATE/RHYTHM.MONITOR BODY TEMPERATURE, AS INDICATED. ASSIST WITH COMFORT MEASURES TO REDUCE FEVER AND CHILLS, E.G., ADDITION/REMOVAL OF BEDCOVERS, COMFORTABLE ROOM TEMPERATURE, TEPID OR COOL WATER SPONGE BATH.MAINTAIN BEDREST. ENCOURAGE USE OF RELAXATION TECHNIQUES AND DIVERSIONAL ACTIVITIES.
RATIONALE
MANIFESTATIONS OF RESPIRATORY DISTRESS ARE DEPENDENT ON/AND INDICATIVE OF THE DEGREE OF LUNG INVOLVEMENT AND UNDERLYING GENERAL HEALTH STATUS.CYANOSIS OF NAILBEDS MAY REPRESENT VASOCONSTRICTION OR THE BODY’S RESPONSE TO FEVER/CHILLS; HOWEVER, CYANOSIS OF EARLOBES, MUCOUS MEMBRANES, AND SKIN AROUND THE MOUTH (“WARM MEMBRANES”) IS INDICATIVE OF SYSTEMIC HYPOXEMIA.RESTLESSNESS, IRRITATION, CONFUSION, AND SOMNOLENCE MAY REFLECT HYPOXEMIA/ DECREASED CEREBRAL OXYGENATION.TACHYCARDIA IS USUALLY PRESENT AS A RESULT OF FEVER/DEHYDRATION BUT MAY REPRESENT A RESPONSE TO HYPOXEMIA.HIGH FEVER (COMMON IN BACTERIAL PNEUMONIA AND INFLUENZA) GREATLY INCREASES METABOLIC DEMANDS AND OXYGEN CONSUMPTION AND ALTERS CELLULAR OXYGENATION.PREVENTS OVEREXHAUSTION AND REDUCES OXYGEN CONSUMPTION/DEMANDS TO FACILITATE RESOLUTION OF INFECTION.
ACTIONS/INTERVENTIONS
Respiratory Monitoring (NIC)
IndependentElevate head and encourage frequent position changes, deep breathing, and effective coughing.Assess level of anxiety. Encourage verbalization of concerns/feelings. Answer questions honestly. Visit frequently, arrange for SO/visitors to stay with patient as indicated.Observe for deterioration in condition, noting hypotension, copious amounts of pink/bloody sputum, pallor, cyanosis, change in level of consciousness, severe dyspnea, restlessness.CollaborativeMonitor ABGs, pulse oximetry.Oxygen Therapy (NIC)Administer oxygen therapy by appropriate means, e.g., nasal prongs, mask, Venturi mask.Prepare for/transfer to critical care setting if indicated.
RATIONALE
These measures promote maximal inspiration, enhance expectoration of secretions to improve ventilation. (Refer to ND: Airway Clearance, ineffective.)Anxiety is a manifestation of psychological concerns and physiological responses to hypoxia. Providing reassurance and enhancing sense of security can reduce the psychological component, thereby decreasing oxygen demand and adverse physiological responses.Shock and pulmonary edema are the most common causes of death in pneumonia and require immediate medical intervention.Follows progress of disease process and facilitates alterations in pulmonary therapy.The purpose of oxygen therapy is to maintain PaO2 above 60 mm Hg. Oxygen is administered by the method that provides appropriate delivery within the patient’s tolerance.Intubation and mechanical ventilation may be required in the event of severe respiratory insufficiency. (Refer to CP: Mechanical Ventilation.)
NURSING DIAGNOSIS: Infection, risk for [spread]Risk factors may includeInadequate primary defenses (decreased ciliary action, stasis of respiratory secretions)Inadequate secondary defenses (presence of existing infection, immunosuppression), chronic disease, malnutrition]Possibly evidenced by[Not applicable; presence of signs and symptoms establishes an actual diagnosis.]
DESIRED OUTCOMES/EVALUATION CRITERIA—PATIENT WILL:Infection Status (NOC)Achieve timely resolution of current infection without complications.Knowledge: Infection Control (NOC)Identify interventions to prevent/reduce risk/spread of/secondary infection.
ACTIONS/INTERVENTIONS
Infection Control (NIC)
IndependentMONITOR VITAL SIGNS CLOSELY, ESPECIALLY DURING INITIATION OF THERAPY.INSTRUCT PATIENT CONCERNING THE DISPOSITION OF SECRETIONS (E.G., RAISING AND EXPECTORATING VERSUS SWALLOWING) AND REPORTING CHANGES IN COLOR, AMOUNT, ODOR OF SECRETIONS.DEMONSTRATE/ENCOURAGE GOOD HANDWASHING TECHNIQUE.CHANGE POSITION FREQUENTLY AND PROVIDE GOOD PULMONARY TOILET.LIMIT VISITORS AS INDICATED.INSTITUTE ISOLATION PRECAUTIONS AS INDIVIDUALLY APPROPRIATE.ENCOURAGE ADEQUATE REST BALANCED WITH MODERATE ACTIVITY. PROMOTE ADEQUATE NUTRITIONAL INTAKE.MONITOR EFFECTIVENESS OF ANTIMICROBIAL THERAPY.INVESTIGATE SUDDEN CHANGES/DETERIORATION IN CONDITION, SUCH AS INCREASING CHEST PAIN, EXTRA HEART SOUNDS, ALTERED SENSORIUM, RECURRING FEVER, CHANGES IN SPUTUM CHARACTERISTICS.COLLABORATIVEADMINISTER ANTIMICROBIALS AS INDICATED BY RESULTS OF SPUTUM/BLOOD CULTURES: E.G., PENICILLINS: ERYTHROMYCIN (E-MYCIN), TETRACYCLINE (ACHROMYCIN), DOXYCYCLINE HYCLATE (VIBRAMYCIN), AMIKACIN (AMIKIN); CEPHALOSPORINS: CEFTRIAXONE (ROCEPHIN); AMANTADINE (SYMMETREL); SPARFLOXACIN (ZAGAM); MACROLIDE DERIVATIVES, E.G, AZITHROMYCIN (ZITHROMAX).
RATIONALE
DURING THIS PERIOD OF TIME, POTENTIALLY FATAL COMPLICATIONS (HYPOTENSION/SHOCK) MAY DEVELOP.ALTHOUGH PATIENT MAY FIND EXPECTORATION OFFENSIVE AND ATTEMPT TO LIMIT OR AVOID IT, IT IS ESSENTIAL THAT SPUTUM BE DISPOSED OF IN A SAFE MANNER. CHANGES IN CHARACTERISTICS OF SPUTUM REFLECT RESOLUTION OF PNEUMONIA OR DEVELOPMENT OF SECONDARY INFECTION.EFFECTIVE MEANS OF REDUCING SPREAD OR ACQUISITION OF INFECTION.PROMOTES EXPECTORATION, CLEARING OF INFECTION.REDUCES LIKELIHOOD OF EXPOSURE TO OTHER INFECTIOUS PATHOGENS.DEPENDENT ON TYPE OF INFECTION, RESPONSE TO ANTIBIOTICS, PATIENT’S GENERAL HEALTH, AND DEVELOPMENT OF COMPLICATIONS, ISOLATION TECHNIQUES MAY BE DESIRED TO PREVENT SPREAD/PROTECT PATIENT FROM OTHER INFECTIOUS PROCESSES.FACILITATES HEALING PROCESS AND ENHANCES NATURAL RESISTANCE.SIGNS OF IMPROVEMENT IN CONDITION SHOULD OCCUR WITHIN 24–48 HR.DELAYED RECOVERY OR INCREASE IN SEVERITY OF SYMPTOMS SUGGESTS RESISTANCE TO ANTIBIOTICS OR SECONDARY INFECTION. COMPLICATIONS AFFECTING ANY/ALL ORGAN SYSTEMS INCLUDE LUNG ABSCESS/EMPYEMA, BACTEREMIA, PERICARDITIS/ENDOCARDITIS, MENINGITIS/ENCEPHALITIS, AND SUPERINFECTIONS.THESE DRUGS ARE USED TO COMBAT MOST OF THE MICROBIAL PNEUMONIAS. COMBINATIONS OF ANTIVIRAL AND ANTIFUNGAL AGENTS MAY BE USED WHEN THE PNEUMONIA IS A RESULT OF MIXED ORGANISMS. NOTE: VANCOMYCIN AND THIRD-GENERATION CEPHALOSPORINS ARE THE TREATMENT OF CHOICE FOR PENICILLIN-RESISTANT STREPTOCOCCAL PNEUMONIA.
ACTIONS/INTERVENTIONS
Infection Control (NIC)
Collaborative
Prepare for/assist with diagnostic studies as indicated.
RATIONALE
Fiberoptic bronchoscopy (FOB) may be done in patients who do not respond rapidly (within 1–3 days) to antimicrobial therapy to clarify diagnosis and therapy needs.
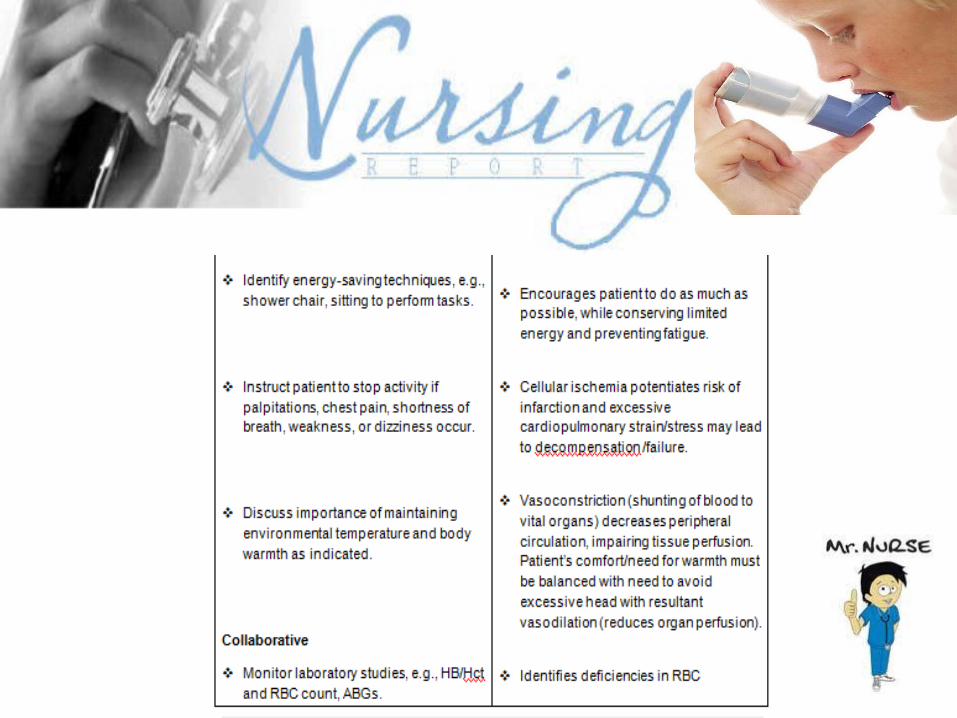
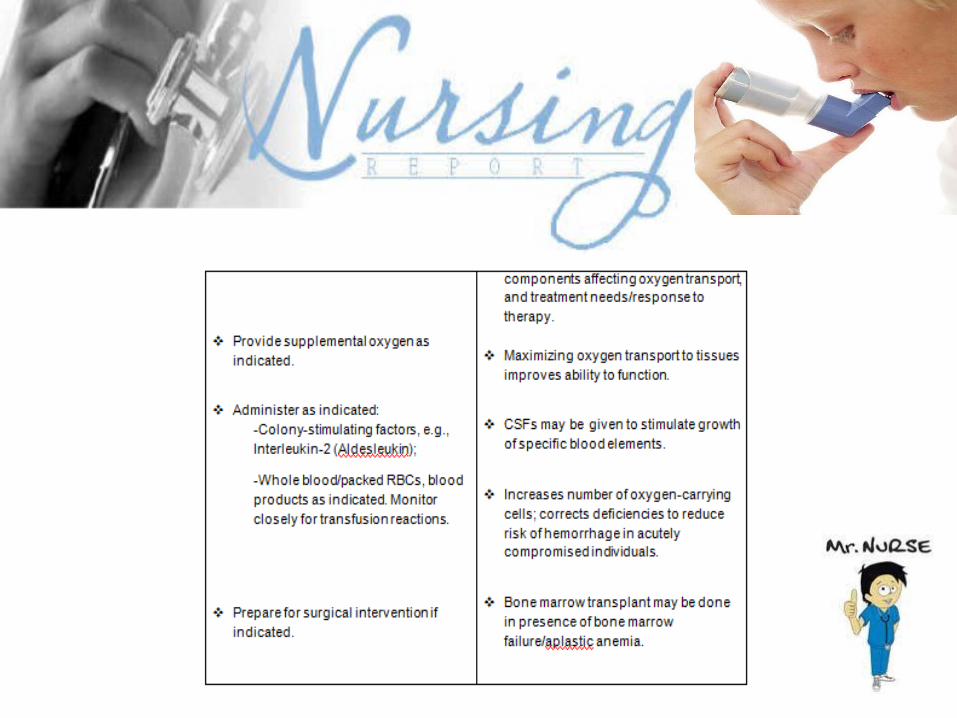
NURSING DIAGNOSIS: Activity intolerance
Risk factors may include
Imbalance between oxygen supply (delivery) and demand
Possibly evidenced by
Weakness and fatigue
Reports of decreased exercise/activity tolerance
Greater need for sleep/rest
Palpitations, tachycardia, increased BP/respiratory response with minor exertion
DESIRED OUTCOMES/EVALUATION CRITERIA – PATIENT WILL:
Report an increase in activity tolerance (including ADLs).
Demonstrate a decrease in physiologic signs of intolerance, e.g., pulse, respirations, and BP remain within patient’s normal range.
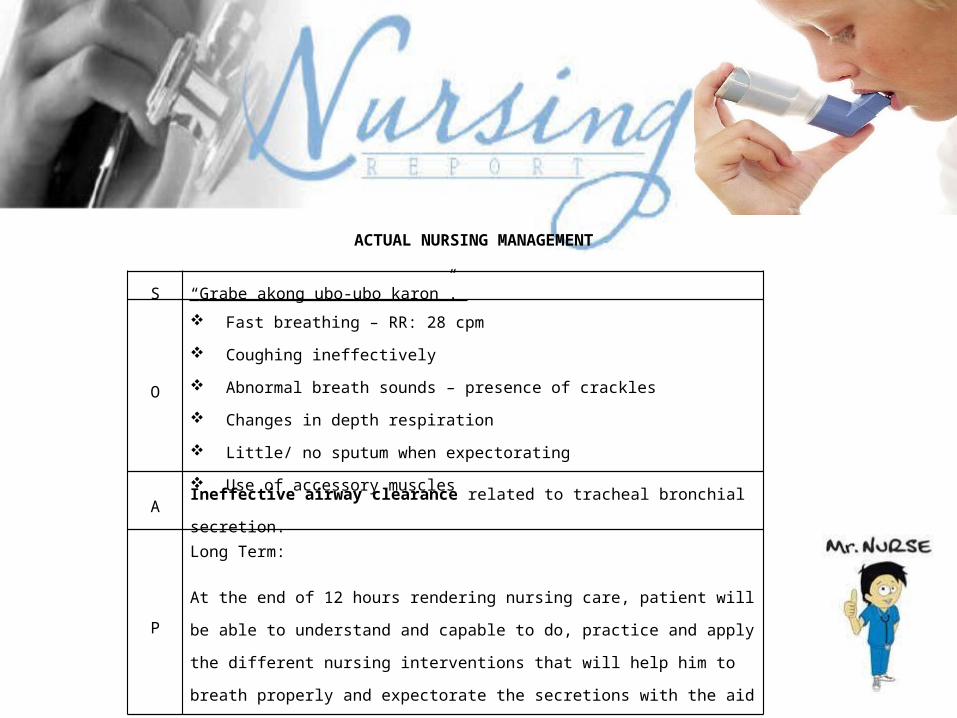
ACTUAL NURSING MANAGEMENT
S “Grabe akong ubo-ubo karon”.
O
Fast breathing – RR: 28 cpm
Coughing ineffectively
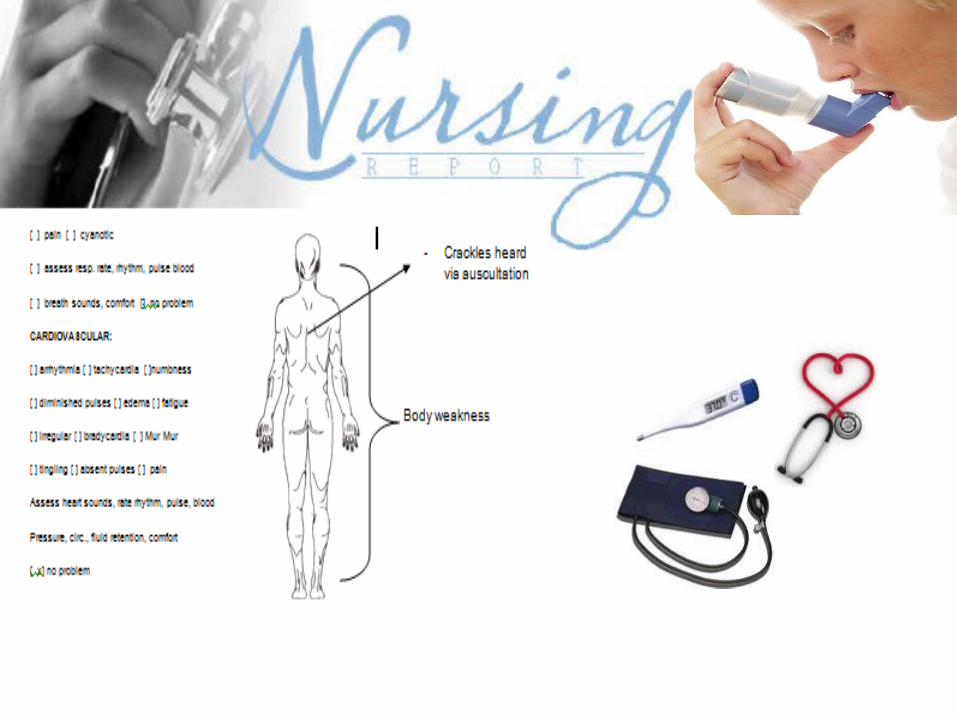
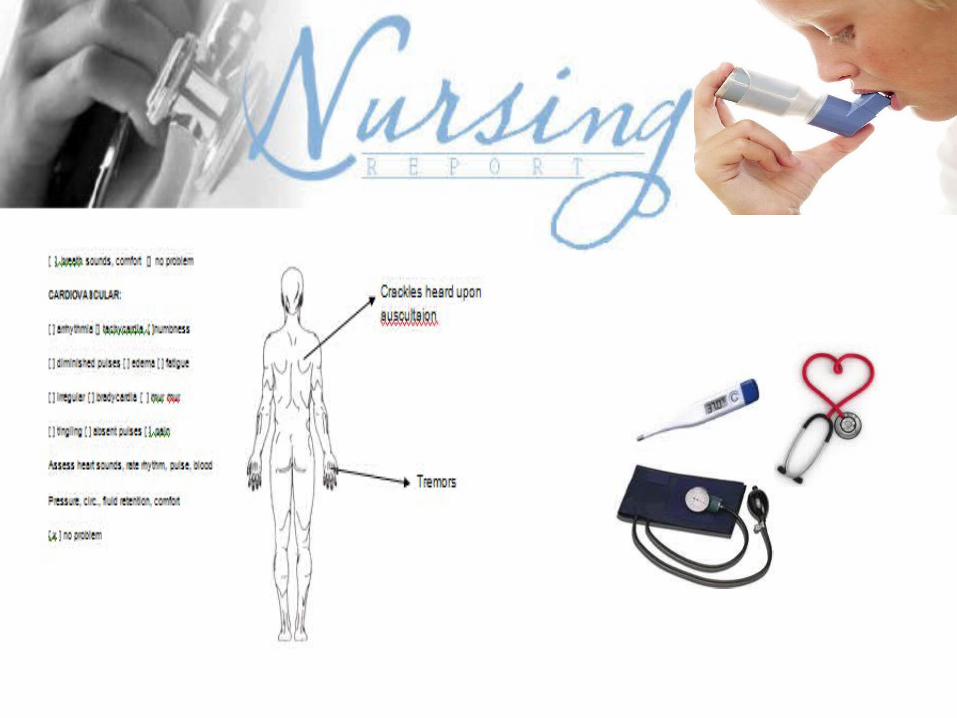
Abnormal breath sounds – presence of crackles
Changes in depth respiration
Little/ no sputum when expectorating
Use of accessory muscles
A Ineffective airway clearance related to tracheal bronchial secretion.
P
Long Term:
At the end of 12 hours rendering nursing care, patient will be able to understand
and capable to do, practice and apply the different nursing interventions that will
help him to breath properly and expectorate the secretions with the aid of
coughing effectively.
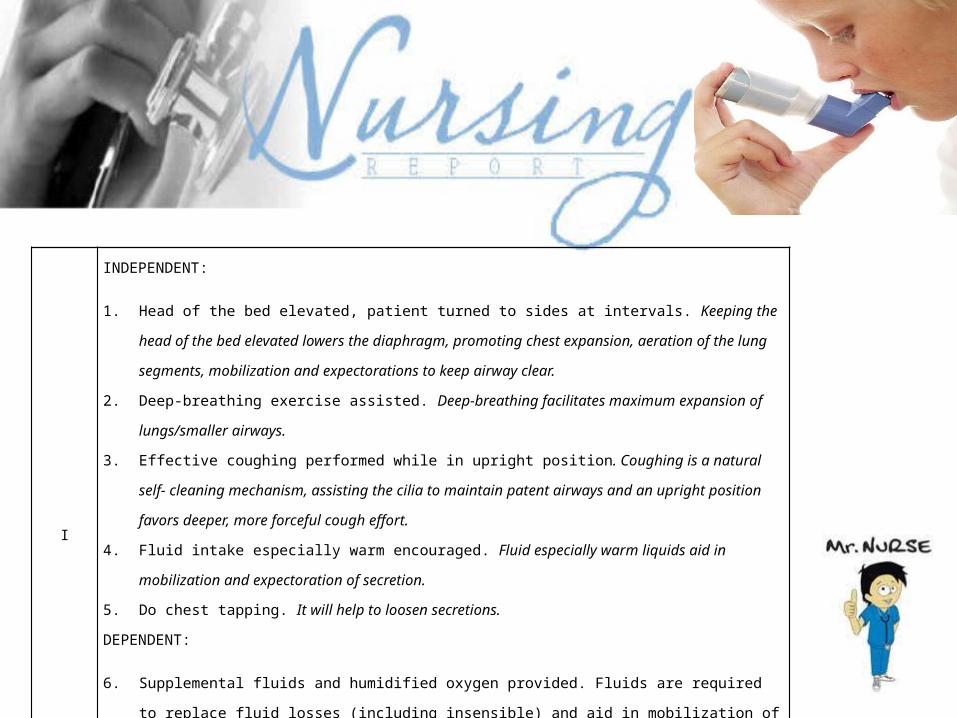
I
INDEPENDENT:
1. Head of the bed elevated, patient turned to sides at intervals. Keeping the head of the
bed elevated lowers the diaphragm, promoting chest expansion, aeration of the lung
segments, mobilization and expectorations to keep airway clear.
2. Deep-breathing exercise assisted. Deep-breathing facilitates maximum expansion of
lungs/smaller airways.
3. Effective coughing performed while in upright position. Coughing is a natural self-
cleaning mechanism, assisting the cilia to maintain patent airways and an upright
position favors deeper, more forceful cough effort.
4. Fluid intake especially warm encouraged. Fluid especially warm liquids aid in
mobilization and expectoration of secretion.
5. Do chest tapping. It will help to loosen secretions.
DEPENDENT:
6. Supplemental fluids and humidified oxygen provided. Fluids are required to replace
fluid losses (including insensible) and aid in mobilization of secretions.
7. Administered combivent nebulization q 4 hrs. A bronchodilator relaxes the smooth
muscle.
E
At the end of 12 hours of rendering nursing care, patient was able to do,
practice and apply the different nursing interventions that will help him to
breathe properly and expectorate the secretions with the aid of coughing
effectively.
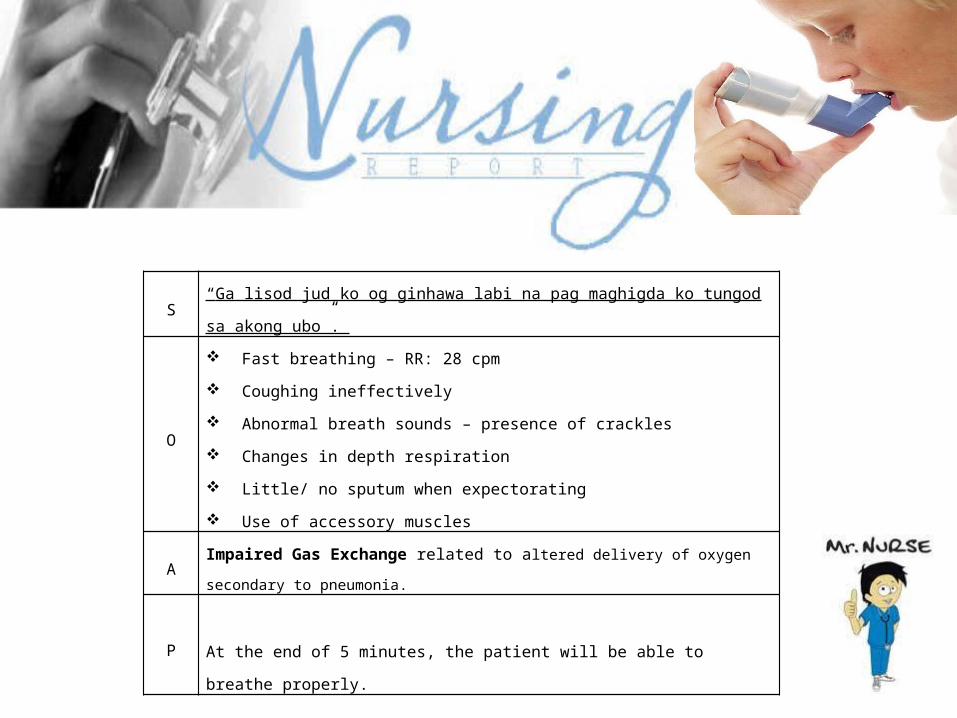
S “Ga lisod jud ko og ginhawa labi na pag maghigda ko tungod sa akong ubo”.
O
Fast breathing – RR: 28 cpm
Coughing ineffectively
Abnormal breath sounds – presence of crackles
Changes in depth respiration
Little/ no sputum when expectorating
Use of accessory muscles
AImpaired Gas Exchange related to altered delivery of oxygen secondary to
pneumonia.
PAt the end of 5 minutes, the patient will be able to breathe properly.
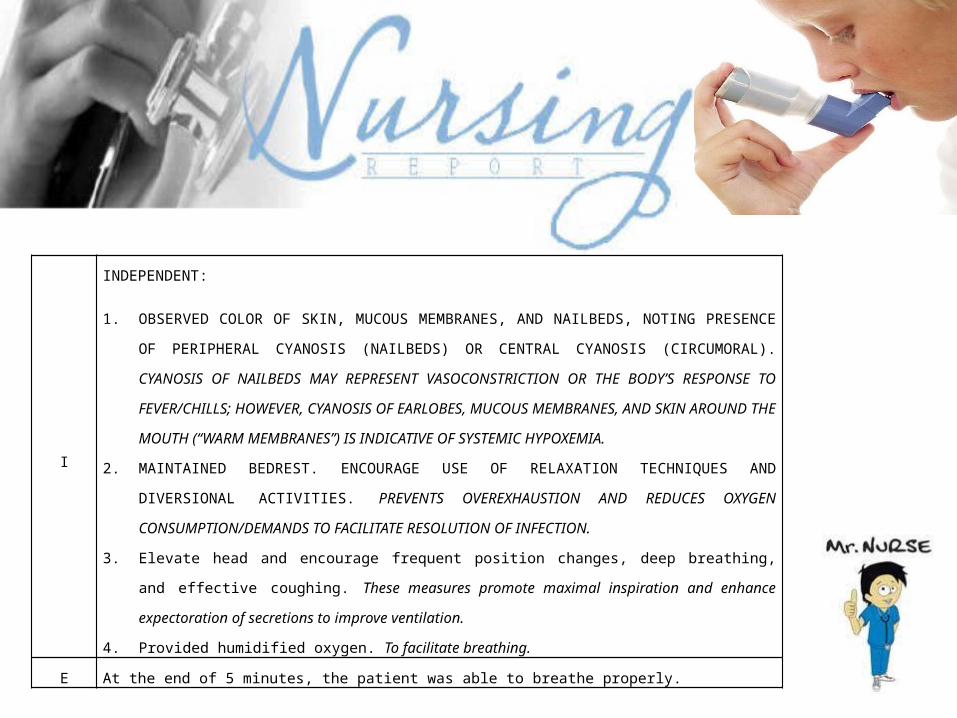
I
INDEPENDENT:
1. OBSERVED COLOR OF SKIN, MUCOUS MEMBRANES, AND NAILBEDS, NOTING
PRESENCE OF PERIPHERAL CYANOSIS (NAILBEDS) OR CENTRAL CYANOSIS
(CIRCUMORAL). CYANOSIS OF NAILBEDS MAY REPRESENT VASOCONSTRICTION OR THE
BODY’S RESPONSE TO FEVER/CHILLS; HOWEVER, CYANOSIS OF EARLOBES, MUCOUS
MEMBRANES, AND SKIN AROUND THE MOUTH (“WARM MEMBRANES”) IS INDICATIVE
OF SYSTEMIC HYPOXEMIA.
2. MAINTAINED BEDREST. ENCOURAGE USE OF RELAXATION TECHNIQUES AND
DIVERSIONAL ACTIVITIES. PREVENTS OVEREXHAUSTION AND REDUCES OXYGEN
CONSUMPTION/DEMANDS TO FACILITATE RESOLUTION OF INFECTION.
3. Elevate head and encourage frequent position changes, deep breathing, and effective
coughing. These measures promote maximal inspiration and enhance expectoration
of secretions to improve ventilation.
4. Provided humidified oxygen. To facilitate breathing.
E At the end of 5 minutes, the patient was able to breathe properly.
VIII. HEALTH TEACHINGS
A. MEDICATION The patient and his significant other are instructed to
follow the medication ordered by the doctor to be taken
at home. This medication is prescribed to help her to
promote wellness. Patient teachings are also imparted,
regarding on precaution and side effects of the
medications.
B. EXERCISES Encouraged the patient to perform passive range of
motion exercises and to perform chest physiotherapy in
order to help loosen secretions and promote lung
expansion.
C. TREATMENT Encouraged the patient to provide adequate rest periods
and observe and promote proper personal hygiene
Encouraged to practice relaxation technique such as deep
breathing, to help control airway clearance.
D. OUTPATIENT Encouraged the patient to return to the hospital a week
after discharge for a follow-up check-up from Monday to
Friday, from 8:00am to 5:00pm for a follow-up check-up.
E. DIET The patient is also instructed to take in nutritious food rich in vitamins and minerals like fruits and vegetables; have a balanced diet; increased fluid intake, like drinking milk rich in calcium and water. She is also instructed to increased fluid intake.
REFERRALS AND FOLLOW-UP
Our further Inpatient care includes monitoring of changes in vital signs, assessment of effectiveness of treatment regimen, reinforcement of dietary advice, facilitate deep breathing exercise while in sitting position, cough effectively, practice energy-saving techniques and do simple activity with rest. Provide ongoing education and reinforcement while monitoring the patient’s progress.
Our further Outpatient care includes instructions of our patient’s dietary modification, compliance with treatment regimen, and patient’s participation through reporting of adverse effects of medications to his physician. The patient as well as its significant others was also instructed to have a regular check-up at the nearest hospital in their place in order to monitor his current condition.
EVALUATION AND IMPLICATION
Within the span of 4 days of rendering care to our patient we were able to identify potential problems and a specific nursing intervention was provided. With the help of our health teachings and other interventions, our patient as well as to his significant others were able to learn how to recognize signs and symptoms and other risk factors of his condition.
Significant others were able to verbalize the importance of avoiding too much exposure to environmental allergens, restricting too much salt in his diet and were encouraged to increase fluid consumption of their family member. They had also recognized the importance of compliance to treatment regimen in order to manage his condition. Significant others were able to learn and verbalized some concerns regarding to the condition of the patient. They were now knowledgeable and are able to comprehend better.
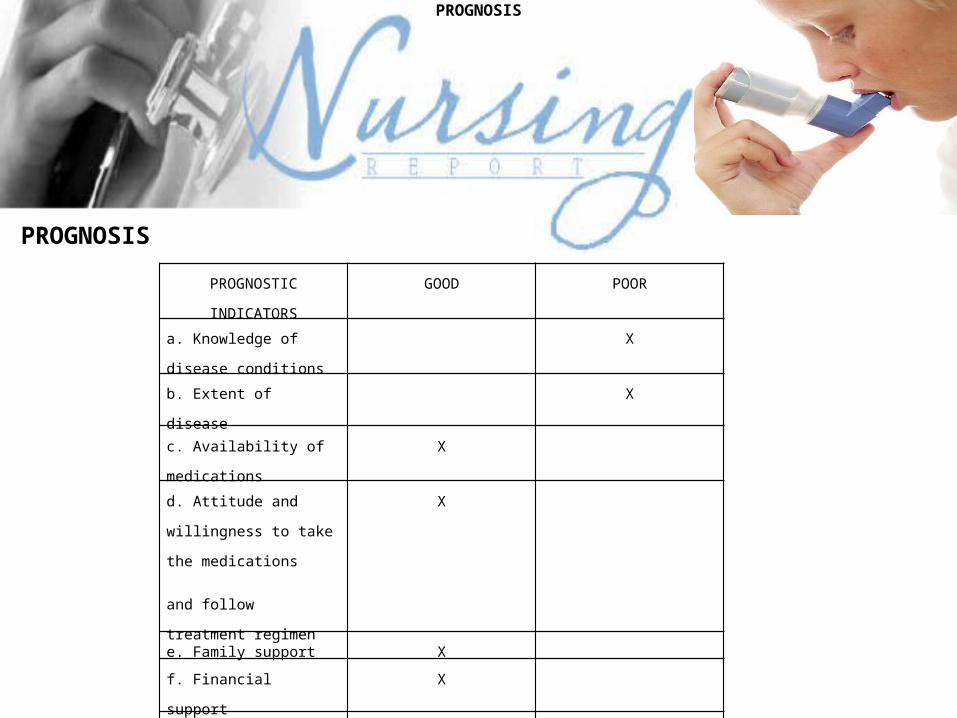
PROGNOSIS
PROGNOSTIC
INDICATORS
GOOD POOR
a. Knowledge of disease
conditions
X
b. Extent of disease X
c. Availability of
medications
X
d. Attitude and willingness
to take the medications
and follow treatment
regimen
X
e. Family support X
f. Financial support X
g. Family history X
PROGNOSIS
Knowledge of disease conditions The patient doesn’t have enough knowledge regarding his condition and its possible complication
Extent of disease Complications would greatly arise if medication and care would have pitfalls. And also, the willingness of the patient to participate in the treatment regimen would greatly help to improve his well being.
Availability of medicationsThe availability of medications was good because they can provide and respond to the prescription of the physician.
Attitude and willingness to take the medications and follow treatment regimenThe patient takes all his medications and follows all treatment regimens given to him.
Family supportFamily support was good because significant others were there to care and assist him in the hospital.
Financial supportFinancial support was good because the family can afford since some of his siblings were financially able and her nephews were employees.
Family historyThe present condition of the patient is not influence by heteredo-familial disease.

DOCUMENTATION
PROGNOSIS
XIII. BIBLIOGRAPHY
Nursing2003 DRUG HANDBOOK. 23rd EditionBrunner & Suddarth’s Textbook of MEDICAL-SURGICAL NURSING by Suzanne C. Smeltzer and Brenda G. Bare. 11 th EditionFUNDAMENTALS OF NURSING concepts, process, and practice by Barbara Kozier, Glenora Erb, Audrey Berman, and Shirlee Snyder. 8th EditionWebsite:(www.UNICEF.org-infobycountry-Philippines)
END
God Bless Everyone..
Liceo de Cagayan UniversityCollege Of Nursing
NCM501-205 Related Learning Experience
Case Presentation
Bronchial Asthma in Acute Exacerbation
January 26, 2011Group B6
Clinical InstructorMr. Andy Roy Salabas RN, MN









![[PPT]PowerPoint Presentation - Faculty Web Pages - Cape …faculty.cbu.ca/.../Safety_Basic_Body_Mechanics.ppt · Web viewSafety; Basic Body Mechanics; Moving & Positioning Nursing](https://img.pdfslide.net/doc/110x75/5aa2d2997f8b9ac67a8d976b/pptpowerpoint-presentation-faculty-web-pages-cape-viewsafety-basic-body.jpg)