Embed Size (px)
Citation preview

NUTRITIONAL NUTRITIONAL DISORDERSDISORDERS
Myrna DC San Pedro, MD, FPPSMyrna DC San Pedro, MD, FPPS

MALNUTRITIONMALNUTRITIONA pathological state resulting fromA pathological state resulting from Relative or absolute deficiency Relative or absolute deficiency Or excess of one or more nutrients Or excess of one or more nutrients
andand Clinically detected only by Clinically detected only by
biochemical, anthropometric or biochemical, anthropometric or physiological testsphysiological tests

Forms of MalnutritionForms of Malnutrition
1.1. Undernutrition:Undernutrition: Marasmus Marasmus
2.2. Overnutrition:Overnutrition: Obesity, Obesity, HypervitaminosesHypervitaminoses
3.3. Specific Deficiency:Specific Deficiency: Kwashiorkor, Kwashiorkor, Hypovitaminoses, Mineral Hypovitaminoses, Mineral DeficienciesDeficiencies
4.4. Imbalance:Imbalance: Electrolyte Imbalance Electrolyte Imbalance

EtiologyEtiology



Protein Energy Protein Energy MalnutritionMalnutrition
(PEM)(PEM)

Classification of Classification of UndernutritionUndernutrition
1.1. Gomez ClassificationGomez ClassificationUses weight-for-age Uses weight-for-age
measurementsmeasurementsProvides prognosisProvides prognosisWeight-for-Age%Weight-for-Age% StatusStatus
91-10091-100 NormalNormal76-9076-90 11stst degree degree61-7561-75 22ndnd degree degree<60<60 33rdrd degree degree

2.2. Wellcome ClassificationWellcome ClassificationBased on 2 criteria only: weight loss Based on 2 criteria only: weight loss
(wt-for-age%) & edema (present or (wt-for-age%) & edema (present or absent)absent)
Wt-for-Age%Wt-for-Age% EdemaEdema No EdemaNo Edema80-6080-60 KwashiorkorKwashiorkor UndernutritionUndernutrition<60<60 Marasmic-Marasmic- MarasmusMarasmus
KwashiorkorKwashiorkor

3.3. Waterlow ClassificationWaterlow ClassificationDistinguishes between deficits of Distinguishes between deficits of
weight-for-height% (wasting*) & weight-for-height% (wasting*) & height-for-age% (stunting*)height-for-age% (stunting*)
Adopted by WHOAdopted by WHONN MildMild ModMod
SevereSevereWt-for-Ht%Wt-for-Ht%>90>90 89-80 79-70 <70 89-80 79-70 <70Ht-for-Age%Ht-for-Age% >95>95 95-90 95-90 90-80 <8090-80 <80

A 6-yr-old boy has an actual weight of A 6-yr-old boy has an actual weight of 15 kg & height of 105 cm. Compute for 15 kg & height of 105 cm. Compute for the wt-for-ht%.the wt-for-ht%.
Actual Wt = 15 kgActual Ht = 105 cmIBW based on actual age (6 yr) = 20 kgIBW based on plotted Ht = 17 kg
Wt-for-Ht% = 15/17 = 0.88Wt-for-age% = 15/20 = 0.75Ht-for-age% = 105/110 = 0.95

MarasmusMarasmus
Common in the Common in the 1st year of life1st year of life
Etiology:Etiology:““Balanced Balanced
starvation”starvation”Insufficient Insufficient
breastmilkbreastmilkDilute milk Dilute milk
mixture or lack mixture or lack of hygieneof hygiene

MarasmusMarasmusClinical Manifestations:Clinical Manifestations:1.1. WastingWasting2.2. Muscle wastingMuscle wasting3.3. Growth retardationGrowth retardation4.4. Mental changesMental changes5.5. No edemaNo edema6.6. Variable-subnormal Variable-subnormal
temp, slow PR, good temp, slow PR, good appetite, often with appetite, often with diarrhea, etc.diarrhea, etc.
Laboratory Data:Laboratory Data:1.1. Serum albumin NSerum albumin N2.2. Urinary urea/g Urinary urea/g
creatinine N or lowcreatinine N or low
3.3. Urinary hydroxyproline/g Urinary hydroxyproline/g creatinine low, earlycreatinine low, early
4.4. Serum essential amino Serum essential amino acid index Nacid index N
5.5. Anemia uncommonAnemia uncommon6.6. Glucose tolerance Glucose tolerance
curves diabetic typecurves diabetic type7.7. KK+ + deficiency presentdeficiency present8.8. Serum cholesterol lowSerum cholesterol low9.9. Diminished enzyme Diminished enzyme
activityactivity10.10. Bone growth delayedBone growth delayed11.11. Liver biopsy N or Liver biopsy N or
atrophicatrophic

MarasmusMarasmus

KwashiorkorKwashiorkorBetween 1-3 yrs oldBetween 1-3 yrs old
Etiology:Etiology:Very low protein but Very low protein but
with calories from with calories from CHOCHO
In places where In places where starchy foods main starchy foods main staplestaple
Never exclusively Never exclusively dietary*dietary*

KwashiorkorKwashiorkorClinical Manifestations:Clinical Manifestations:A.A. Diagnostic SignsDiagnostic Signs
1.1. EdemaEdema2.2. Muscle wastingMuscle wasting3.3. Psychomotor Psychomotor
changeschangesB.B. Common SignsCommon Signs
1.1. Hair changesHair changes2.2. Diffuse Diffuse
depigmentation of depigmentation of skinskin
3.3. MoonfaceMoonface4.4. AnemiaAnemia
C.C. Occasional Signs:Occasional Signs:1.1. Flaky-paint rashFlaky-paint rash2.2. NomaNoma3.3. HepatomegalyHepatomegaly4.4. AssociatedAssociated
Laboratory:Laboratory:1.1. Decreased serum Decreased serum
albuminalbumin2.2. EEG abnormalitiesEEG abnormalities3.3. Iron & folic acid Iron & folic acid
deficienciesdeficiencies4.4. Liver biopsy fatty or Liver biopsy fatty or
fibrosis may occurfibrosis may occur

KwashiorkorKwashiorkor

Treatment of PEMTreatment of PEM1.1. Severe PEM is an emergency, 1-3 months Severe PEM is an emergency, 1-3 months
hospitalization desirablehospitalization desirable2.2. On admission, treat dehydration, infections On admission, treat dehydration, infections
& vitamin deficiencies& vitamin deficiencies3.3. During 1During 1stst wk, the acute phase, stabilize & wk, the acute phase, stabilize &
start feeding as soon as rehydratedstart feeding as soon as rehydrated4.4. When edema subsides, give full-strength When edema subsides, give full-strength
feeds of maintenance calories & protein, feeds of maintenance calories & protein, recovery after 2-3 wkrecovery after 2-3 wk
5.5. Once full-strength feeds tolerated, start Once full-strength feeds tolerated, start rehabilitation with high energy feeds (150-rehabilitation with high energy feeds (150-200 kcal/kg/day), recovery expected within 200 kcal/kg/day), recovery expected within 4-6 wk4-6 wk

Prognosis of PEMPrognosis of PEM If severe & early, <6 months old, If severe & early, <6 months old,
permanent impairment of physical & permanent impairment of physical & mental growthmental growth
First 48 hours critical, with poor First 48 hours critical, with poor treatment mortality may be >50%treatment mortality may be >50%
Even with thorough treatment, 10% Even with thorough treatment, 10% mortality may still occurmortality may still occur
Some mortality causes: endocrine, Some mortality causes: endocrine, cardiac or liver failure, electrolyte cardiac or liver failure, electrolyte imbalance, hypoglycemia & hypothermiaimbalance, hypoglycemia & hypothermia

ObesityObesity

ObesityObesity1.1. Definition:Definition: Generalized, excessive accumulation of Generalized, excessive accumulation of
fat in subcutaneous & other tissuesfat in subcutaneous & other tissues2.2. Classification according to “desirable” weight Classification according to “desirable” weight
standard:standard: Overweight = Overweight = >>10% IBW or “desirable” weight10% IBW or “desirable” weight Obese = Obese = >>20% IBW or “desirable” weight20% IBW or “desirable” weight
3.3. The Centers for Disease Control (CDC)The Centers for Disease Control (CDC) avoids using avoids using "obesity" instead suggest "obesity" instead suggest two levels of overweight:two levels of overweight: ““At risk" level = BMI 85At risk" level = BMI 85thth%% More severe level = BMI 95More severe level = BMI 95thth%%
4.4. The American Obesity Association:The American Obesity Association: Overweight = BMI 85Overweight = BMI 85thth% because ~ BMI of 25, % because ~ BMI of 25,
overweight for adultsoverweight for adults Obesity = BMI 95Obesity = BMI 95thth% because ~ BMI of 30, obesity % because ~ BMI of 30, obesity
in adultsin adults

ObesityObesityAppears most frequently in the 1Appears most frequently in the 1stst yr, 5-6 yr, 5-6
yr & adolescenceyr & adolescenceEtiology:Etiology: Excessive food intake compared with Excessive food intake compared with
useuse Genetic constitutionGenetic constitution Psychic disturbance Psychic disturbance Endocrine & metabolic disturbances rareEndocrine & metabolic disturbances rare Insufficient exercise or lack of activity Insufficient exercise or lack of activity

ObesityObesityClinical Manifestations:Clinical Manifestations:1.1. Fine facial features on a heavy-looking taller Fine facial features on a heavy-looking taller
childchild2.2. Larger upper arms & thighsLarger upper arms & thighs3.3. Genu valgum commonGenu valgum common4.4. Relatively small hands & fingers taperingRelatively small hands & fingers tapering5.5. Adiposity in mammary regionsAdiposity in mammary regions6.6. Pendulous abdomen with striaePendulous abdomen with striae7.7. In boys, external genitalia appears small but In boys, external genitalia appears small but
actually average in sizeactually average in size8.8. In girls, external genitalia normal & menarche In girls, external genitalia normal & menarche
not delayednot delayed9.9. Psychologic disturbances commonPsychologic disturbances common10.10. Bone age advancedBone age advanced

ObesityObesity

Treatment of ObesityTreatment of ObesityA.A. 11stst principle: Decrease energy intake principle: Decrease energy intake
1.1. Initial med exam to R/O pathological causesInitial med exam to R/O pathological causes2.2. 3-day food recall to itemize child’s diet3-day food recall to itemize child’s diet3.3. Plan right dietPlan right diet
a.a. Avoid all sweets, fried foods & fatsAvoid all sweets, fried foods & fatsb.b. Limit milk intake to not >2 glasses/dayLimit milk intake to not >2 glasses/dayc.c. For 10-14 yrs, limit to 1,100-1300 kcal diet For 10-14 yrs, limit to 1,100-1300 kcal diet
for several monthsfor several months4.4. Child must be properly motivated & family Child must be properly motivated & family
involvement essentialinvolvement essentialB.B. 22ndnd principle: Increase energy output principle: Increase energy output
1.1. Obtain an activity historyObtain an activity history2.2. Increase physical activityIncrease physical activity3.3. Involve in hobbies to prevent boredomInvolve in hobbies to prevent boredom

Complication of ObesityComplication of ObesityPickwickian SyndromePickwickian SyndromeRare complication of extreme Rare complication of extreme
exogenous obesityexogenous obesitySevere cardiorespiratory distress & Severe cardiorespiratory distress &
alveolar hypoventilationalveolar hypoventilationIncludes polycythemia, hypoxemia, Includes polycythemia, hypoxemia,
cyanosis, CHF & somnolencecyanosis, CHF & somnolenceHigh OHigh O22 dangerous in cyanosis dangerous in cyanosisWeight reduction ASAP & quickWeight reduction ASAP & quick

TheTheFat-Soluble Fat-Soluble
VitaminsVitamins

Vitamin A (Retinol)Vitamin A (Retinol) Active forms: retinol, retinaldehyde & retinoic Active forms: retinol, retinaldehyde & retinoic
acidacid Plants synthesize Plants synthesize carotenoidscarotenoids cleaved to cleaved to
retinolretinol by most animals by most animals stored in liver as stored in liver as retinyl palmitateretinyl palmitate
Retinol,Retinol, alcohol form of vitamin A: N plasma alcohol form of vitamin A: N plasma values = 20–50 μg/dl in infants & 30–225 values = 20–50 μg/dl in infants & 30–225 μg/dL in older children & adultsμg/dL in older children & adults
RetinalRetinal, the aldehyde form, functions in , the aldehyde form, functions in visionvision
Retinoic acidRetinoic acid, the physiologically most , the physiologically most important vitamin A metabolite, regulates important vitamin A metabolite, regulates many genes involved in fundamental biologic many genes involved in fundamental biologic activities of cells*activities of cells*

Vitamin A (Retinol) Vitamin A (Retinol) DeficiencyDeficiency
Functions:Functions:1.1. Retinal is in photosensitive pigment in both rods Retinal is in photosensitive pigment in both rods
(rhodopsin) & cones (iodopsin)(rhodopsin) & cones (iodopsin)2.2. Needed in lysosomal membrane stabilityNeeded in lysosomal membrane stability3.3. Involved in keratinization, cornification, bone Involved in keratinization, cornification, bone
development & cell growth & reproductiondevelopment & cell growth & reproduction
Absence in the diet common by 2-3 yrs oldAbsence in the diet common by 2-3 yrs oldEtiology:Etiology:1.1. Poor fetal storagePoor fetal storage2.2. Poor absorption as in low-fat diet, malabsorption Poor absorption as in low-fat diet, malabsorption
syndromes, etc.syndromes, etc.3.3. Low protein intake resulting in deficient carriersLow protein intake resulting in deficient carriers4.4. Increased excretion as in cancer & UTIIncreased excretion as in cancer & UTI

Hypovitaminosis AHypovitaminosis AA.A. Eye signs & symptomsEye signs & symptoms
1.1. Nyctalopia or night blindness, an early Nyctalopia or night blindness, an early symptomsymptom photophobia photophobia pain pain insensitivityinsensitivity
2.2. Xerosis conjunctivae, 1Xerosis conjunctivae, 1stst clinical sign clinical sign
3.3. Bitot’s spotsBitot’s spots
4.4. Corneal xerosis or xeropthalmiaCorneal xerosis or xeropthalmia
5.5. Corneal ulcersCorneal ulcers
6.6. KeratomalaciaKeratomalacia
7.7. Blindness Blindness

Hypovitaminosis AHypovitaminosis AB.B. Skin signs:Skin signs: Xerosis of the skin & follicular Xerosis of the skin & follicular
hyperkeratosis or phrynodermahyperkeratosis or phrynodermaC.C. Others:Others: Apathy, physical & mental growth Apathy, physical & mental growth
retardation, faulty epiphyseal bone retardation, faulty epiphyseal bone formation, defective teeth enamel & signs formation, defective teeth enamel & signs of benign increased ICPof benign increased ICP
Diagnosis:Diagnosis:1.1. Routine PERoutine PE2.2. Dark adaptation test to detect nyctalopiaDark adaptation test to detect nyctalopia3.3. Absorption test for vitamin AAbsorption test for vitamin A4.4. Conjunctival impression cytology to Conjunctival impression cytology to
evaluate early xeropthalmiaevaluate early xeropthalmia

Hypovitaminosis AHypovitaminosis ARDA: RDA: 1800 IU/day (1 IU vitamin A = 0.3 mcg retinol)1800 IU/day (1 IU vitamin A = 0.3 mcg retinol)Prevention:Prevention:1.1. Pregnant in last trimester be given 5000 IU p. o.Pregnant in last trimester be given 5000 IU p. o.2.2. Every 6 months, infants <1 yr retinol palmitate 55mg or 33mg Every 6 months, infants <1 yr retinol palmitate 55mg or 33mg
retinol acetate (100,000 IU) p. o.retinol acetate (100,000 IU) p. o.3.3. Every 4-6 months, older children 110mg retinol palmitate or 66 Every 4-6 months, older children 110mg retinol palmitate or 66
mg retinol acetate (200,000 IU) p. o.mg retinol acetate (200,000 IU) p. o.4.4. In prevalent areas, 100,000 IU p. o. q 3 moIn prevalent areas, 100,000 IU p. o. q 3 mo5.5. For malnourished children 1-6 yrs, 250,000 IU p. o. q 6 moFor malnourished children 1-6 yrs, 250,000 IU p. o. q 6 moTreatment:Treatment:1.1. >>1 yr: 110mg retinol palmitate or 66mg retinol acetate (200,000 1 yr: 110mg retinol palmitate or 66mg retinol acetate (200,000
IU) orally or preferably 33mg (100,000 IU) of retinyl palmitate by IU) orally or preferably 33mg (100,000 IU) of retinyl palmitate by IMIM
2.2. The oral dose should be repeated on 2nd day and on discharge The oral dose should be repeated on 2nd day and on discharge from hospital 7-30 days after 1st dosefrom hospital 7-30 days after 1st dose
3.3. Above doses halved for infantsAbove doses halved for infants4.4. For corneal involvement, apply antibiotic ointment like topical For corneal involvement, apply antibiotic ointment like topical
bacitracinbacitracin to both eyes 6x/day and give also systemic to both eyes 6x/day and give also systemic antibioticsantibiotics

Hypovitaminosis AHypovitaminosis A

Hypervitaminosis AHypervitaminosis AAcute Intoxication:Acute Intoxication:1.1. Excessively Excessively large large
single doses single doses >>300,000 IU300,000 IU
2.2. Infants: nausea & Infants: nausea & vomiting, vomiting, drowsiness or drowsiness or irritability w/ signs irritability w/ signs of increased ICPof increased ICP
3.3. Adults: drowsiness, Adults: drowsiness, irritability, headache irritability, headache & vomiting& vomiting
4.4. Serum vitamin A Serum vitamin A values = 200-1000 values = 200-1000 IU/dl (N: 50-100 IU/dl (N: 50-100 IU/dl)IU/dl)
Chronic Intoxication:Chronic Intoxication:1.1. >>50,000 IU/day for several wk50,000 IU/day for several wk2.2. Signs & symptoms in infants:Signs & symptoms in infants:
a.a. Early: anorexia, pruritus, Early: anorexia, pruritus, irritability, tender swollen irritability, tender swollen bones w/ motion limitationbones w/ motion limitation
b.b. Alopecia, seborrhea, Alopecia, seborrhea, cheilosis & peeling palms cheilosis & peeling palms & soles& soles
c.c. Hepatomegaly & Hepatomegaly & hypercalcemiahypercalcemia
d.d. Craniotabes & Craniotabes & hyperostosis of long bones hyperostosis of long bones (differentiate from Caffey’s (differentiate from Caffey’s disease)disease)
3.3. Elevated serum vitamin AElevated serum vitamin A4.4. Reversible manifestations Reversible manifestations
when vitamin A discontinuedwhen vitamin A discontinued

Vitamin D (Cholecalciferol) Vitamin D (Cholecalciferol)
90% 90% Vitamin DVitamin D33, , cholecalciferolcholecalciferol, produced in skin , produced in skin by UV irradiation of 7-dehydrocholesterol (mainly by UV irradiation of 7-dehydrocholesterol (mainly an animal sterol) an animal sterol) blood blood 25 hydroxylation to 25 hydroxylation to calcidiol in liver + PTH calcidiol in liver + PTH di-hydroxylation in di-hydroxylation in kidney to calcitriol 1,25 (OH) 2-cholecalciferolkidney to calcitriol 1,25 (OH) 2-cholecalciferol
1,25-dihydroxycholecalciferol1,25-dihydroxycholecalciferol most active form most active form Vitamin DVitamin D22, , ergocalciferolergocalciferol, taken orally from , taken orally from
plants (ergosterol) then irradiated as aboveplants (ergosterol) then irradiated as above Animal derived vitamin DAnimal derived vitamin D3 3 and plant derived and plant derived
vitamin Dvitamin D22 biologically equal biologically equal

Vitamin D (Cholecalciferol) Vitamin D (Cholecalciferol) DeficiencyDeficiency
Functions:Functions: Vitamin D enhances Ca Vitamin D enhances Ca+2+2 absorption absorption from gut, removal of Cafrom gut, removal of Ca+2+2 from bone & PO from bone & PO44
-3-3 reabsorption in kidneyreabsorption in kidney
Rickets appear towards end of 1-2 yrRickets appear towards end of 1-2 yrEtiology:Etiology:1.1. Lack in diet or lack of sunlight exposureLack in diet or lack of sunlight exposure2.2. Rapid growth as in prematures & adolescentsRapid growth as in prematures & adolescents3.3. Disorders of absorption such as celiac Disorders of absorption such as celiac
disease, steatorrhea or cystic fibrosisdisease, steatorrhea or cystic fibrosis4.4. In children with hepatic diseaseIn children with hepatic disease5.5. Maternal malnutritionMaternal malnutrition6.6. Poverty or ignorancePoverty or ignorance

Hypovitaminosis D (Rickets)Hypovitaminosis D (Rickets)
A.A. Rickets:Rickets: Deficient calcification or softening bones in Deficient calcification or softening bones in a growing child resulting in deformation of bonesa growing child resulting in deformation of bones1.1. Head manifestationsHead manifestations
a.a. Craniotabes: Thinning of skull outer table & Craniotabes: Thinning of skull outer table & feeling ping-pong ball sensation over occiput feeling ping-pong ball sensation over occiput or posterior parietal bones or posterior parietal bones may disappear may disappear before end 1 yr before end 1 yr continues as flattening & continues as flattening & at times permanent head asymmetryat times permanent head asymmetry
b.b. Anterior fontanel larger & closure delayedAnterior fontanel larger & closure delayedc.c. Caput quadratum: Box-like head due to Caput quadratum: Box-like head due to
thickened & prominent central parts of thickened & prominent central parts of parietal & frontal bonesparietal & frontal bones
d.d. Delayed eruption of temporary teeth while Delayed eruption of temporary teeth while permanent with enamel defectspermanent with enamel defects

Hypovitaminosis D Hypovitaminosis D (Rickets)(Rickets)
2.2. Thorax signsThorax signsa.a. Palpable enlargement of costochondral Palpable enlargement of costochondral
junctions called “rachitic rosary”junctions called “rachitic rosary”b.b. Flattened sides of the thorax with posterior Flattened sides of the thorax with posterior
longitudinal grooveslongitudinal groovesc.c. Pigeon-breast deformityPigeon-breast deformityd.d. Harrison grooveHarrison groove
3.3. Spinal column signsSpinal column signsa.a. Scoliosis commonScoliosis commonb.b. Kyphosis when sittingKyphosis when sittingc.c. Lordosis in the erect positionLordosis in the erect position
4.4. Pelvis narrowed Pelvis narrowed due to changes in promontory, due to changes in promontory, sacrum & coccyx which if permanent, add to sacrum & coccyx which if permanent, add to hazards of childbirth in femalehazards of childbirth in female

Hypovitaminosis D Hypovitaminosis D (Rickets)(Rickets)
5.5. Extremities in children >2 yearsExtremities in children >2 yearsa.a. Thickened & enlarged wrists & anklesThickened & enlarged wrists & anklesb.b. Bowlegs or knock-knees as a result of the Bowlegs or knock-knees as a result of the
bending of the softened shafts of the femur, bending of the softened shafts of the femur, tibia & fibulatibia & fibula
c.c. Coxa vara or pronated feetCoxa vara or pronated feetd.d. Greenstick fracturesGreenstick fractures
6.6. MusclesMuscles poorly developed & lack tone poorly developed & lack tonea.a. Delay in sitting, standing & walkingDelay in sitting, standing & walkingb.b. Potbelly due to weakness of abdominal musclesPotbelly due to weakness of abdominal muscles
7.7. Other manifestationsOther manifestationsa.a. UnderweightUnderweightb.b. Mental retardationMental retardation

RicketsRickets

RicketsRickets

RicketsRickets

RicketsRickets
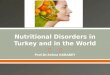
A teenage male w/ A teenage male w/ rickets. Note bow legs & rickets. Note bow legs & compromised height. compromised height.
Distal femur, proximal Distal femur, proximal tibia and fibula in tibia and fibula in rickets. Note widening rickets. Note widening epiphysis, resorption of epiphysis, resorption of provisional zone of provisional zone of calcification, flaring calcification, flaring metaphysis & bone metaphysis & bone deformity. deformity.

Hypovitaminosis D Hypovitaminosis D (Osteomalacia)(Osteomalacia)
B.B. Osteomalacia:Osteomalacia: Accumulation of uncalcified osteoid Accumulation of uncalcified osteoid tissue in rib joints of an adult resulting intissue in rib joints of an adult resulting in
1.1. Pain in pelvis, lower back and legsPain in pelvis, lower back and legs
2.2. Tenderness in shins and in other bonesTenderness in shins and in other bones
3.3. Waddling gaitWaddling gait
4.4. Deformities of pelvisDeformities of pelvis
5.5. Tetany may occur manifested by involuntary Tetany may occur manifested by involuntary twitching of facial muscles or by carpopedal twitching of facial muscles or by carpopedal spasmspasm
6.6. Spontaneous fractures may occurSpontaneous fractures may occur
C.C. Osteomalacia should not be confused with Osteomalacia should not be confused with osteoporosisosteoporosis, a disease of ageing, in which , a disease of ageing, in which decalcification is also a feature decalcification is also a feature

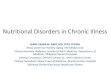
OsteomalaciaOsteomalaciaA young male w/ osteomalacia. Note a pseudofracture in the medial edge of the upper femoral shaft (arrow).
Xray showing a pseudofracture (red arrow) from an adult who has x-linked hypophosphatemic rickets. This sign is seen only in osteomalacia, but not in many of the cases.
AP pelvis in a patient w/ osteomalacia. The film shows diffuse osteopenia, & a Looser zone (arrow) in the superior ramus of the right obturator ring.

Hypovitaminosis DHypovitaminosis DDiagnosis:Diagnosis:
1.1. History & clinical observationHistory & clinical observation
2.2. Laboratory findings:Laboratory findings:
a.a. Serum CaSerum Ca+2+2 may be normal or low may be normal or low
b.b. Serum phosphorus level <4 mg/dl (N serum Serum phosphorus level <4 mg/dl (N serum phosphorus 4.5-6.5 mg/dl but in rachitic infants phosphorus 4.5-6.5 mg/dl but in rachitic infants reduced to reduced to <<1.5-3.5 mg/dl)1.5-3.5 mg/dl)
c.c. Serum alkaline phosphatase elevated (N serum Serum alkaline phosphatase elevated (N serum phosphatase 5-15 Bodansky units per 100 ml but phosphatase 5-15 Bodansky units per 100 ml but elevated to 20-30 in mild rickets & to elevated to 20-30 in mild rickets & to >>60 in 60 in severe)severe)
d.d. Serum 25-hydroxycholecalciferol decreasedSerum 25-hydroxycholecalciferol decreased
e.e. Urinary cyclic AMP elevatedUrinary cyclic AMP elevated

Hypovitaminosis DHypovitaminosis D3.3. Roentgenographic changesRoentgenographic changes
a.a. X-ray of wrist, cupping & fraying of proximal X-ray of wrist, cupping & fraying of proximal ends of ulna & radius, best for early diagnosisends of ulna & radius, best for early diagnosis
b.b. Humeral ossification centers barely visualizedHumeral ossification centers barely visualized
c.c. Shafts osteoporotic or density decreasedShafts osteoporotic or density decreased
d.d. Rosary beading of sternal ends of the ribs due Rosary beading of sternal ends of the ribs due to deposited uncalcified osteoid tissue to deposited uncalcified osteoid tissue becoming compressed & bulges laterally becoming compressed & bulges laterally
e.e. Initial healing indicated by appearance of line Initial healing indicated by appearance of line of preparatory calcificationof preparatory calcification

Hypovitaminosis DHypovitaminosis DDifferential Diagnosis:Differential Diagnosis:1.1. Craniotabes in hydrocephalus & Craniotabes in hydrocephalus &
osteogenesis imperfectaosteogenesis imperfecta2.2. ““Rosary” at costochondral junctions in scurvy Rosary” at costochondral junctions in scurvy
& chondrodystrophy& chondrodystrophy3.3. Epiphyseal lesions in congenital epiphyseal Epiphyseal lesions in congenital epiphyseal
dysplasia, cytomegalic inclusion disease, dysplasia, cytomegalic inclusion disease, syphilis, rubella & copper deficiencysyphilis, rubella & copper deficiency
4.4. Congenital pigeon breast deformityCongenital pigeon breast deformity5.5. Familial bowlegsFamilial bowlegs6.6. Metabolic disturbances with osseous lesionsMetabolic disturbances with osseous lesionsComplications:Complications:1.1. Respiratory infectionsRespiratory infections2.2. Chronic gastroenteritisChronic gastroenteritis3.3. Iron deficiency anemiaIron deficiency anemia

Hypovitaminosis DHypovitaminosis DPrognosis:Prognosis:1.1. In tropics, usually has tendency to heal In tropics, usually has tendency to heal
spontaneouslyspontaneously2.2. A possibly deforming disorderA possibly deforming disorder3.3. Not fatal but complications & intercurrent infections Not fatal but complications & intercurrent infections
may cause deathmay cause deathRDA:RDA: 400 IU (1 IU vitamin D = 0.025 mcg 400 IU (1 IU vitamin D = 0.025 mcg
cholecalciferol/ ergocalciferol)cholecalciferol/ ergocalciferol)Prevention:Prevention:1.1. Sunlight prophylaxis effective only in temperate Sunlight prophylaxis effective only in temperate
zones during summer months in haze-free areaszones during summer months in haze-free areas2.2. Daily requirement of vitamin D in 1 quart of fresh Daily requirement of vitamin D in 1 quart of fresh
whole milk or a can of evaporated milkwhole milk or a can of evaporated milk3.3. Natural vitamin D present only in animal foods like Natural vitamin D present only in animal foods like
egg yolk, liver, cod-liver & other fish-liver oils & egg yolk, liver, cod-liver & other fish-liver oils & fishbody oilsfishbody oils

Hypovitaminosis DHypovitaminosis D4.4. Prematures or breast-fed infants should receive Prematures or breast-fed infants should receive
supplemental vitamin D daily because milk is a supplemental vitamin D daily because milk is a poor source unless fortifiedpoor source unless fortified
5.5. Vitamin D should also be administered to Vitamin D should also be administered to pregnant & lactating motherspregnant & lactating mothers
Treatment:Treatment:1.1. Daily administration of 50-150 mcg of vitamin DDaily administration of 50-150 mcg of vitamin D33
or 0.5-2 mcg of 1,25-dihydroxycholecalciferol will or 0.5-2 mcg of 1,25-dihydroxycholecalciferol will produce healing seen on X-ray within 2-4 wksproduce healing seen on X-ray within 2-4 wks
2.2. Vitamin D 15,000 mcg in a single dose w/o Vitamin D 15,000 mcg in a single dose w/o further therapy for several months may be further therapy for several months may be advantageousadvantageous
3.3. After healing is complete, the dose of vitamin D After healing is complete, the dose of vitamin D should be lowered to 10 mcg/dayshould be lowered to 10 mcg/day
4.4. If no healing occurs, rickets is probably resistant If no healing occurs, rickets is probably resistant to vitamin D or non-nutritional ricketsto vitamin D or non-nutritional rickets

Hypervitaminosis DHypervitaminosis DEtiology: Etiology: Excessive intakes from Excessive intakes from 1.1. Inadvertently substituting concentrated form for diluteInadvertently substituting concentrated form for dilute2.2. Parents’ increasing prescribed doseParents’ increasing prescribed dose3.3. Inadequately controlling dosages for children receiving Inadequately controlling dosages for children receiving
large amounts of vitamin D for chronic large amounts of vitamin D for chronic hyperphosphatemiahyperphosphatemia
Clinical Manifestations: Clinical Manifestations: Symptoms after 1-3 monthsSymptoms after 1-3 months1.1. Anorexia, irritability, hypotonia & constipationAnorexia, irritability, hypotonia & constipation2.2. Polydipsia, polyuria & pallorPolydipsia, polyuria & pallor3.3. Dehydration usually presentDehydration usually present4.4. Aortic valvular stenosis, vomiting & hypertensionAortic valvular stenosis, vomiting & hypertension5.5. Retinopathy & clouding of cornea & conjunctiva may Retinopathy & clouding of cornea & conjunctiva may
occuroccur

Hypervitaminosis DHypervitaminosis DLaboratory Data:Laboratory Data:1.1. ProteinuriaProteinuria2.2. Hypercalcemia & hypercalciuriaHypercalcemia & hypercalciuria3.3. With continued excess, renal damage & With continued excess, renal damage &
metastatic calcifications may occurmetastatic calcifications may occur4.4. Roentgenograms of long bones reveal metastatic Roentgenograms of long bones reveal metastatic
calcification & generalized osteoporosiscalcification & generalized osteoporosisDifferential Diagnosis:Differential Diagnosis:1.1. Chronic nephritisChronic nephritis2.2. HyperparathyroidismHyperparathyroidism3.3. Idiopathic HypercalcemiaIdiopathic HypercalcemiaTreatment:Treatment:1.1. Discontinue vitamin D & decrease CaDiscontinue vitamin D & decrease Ca+2+2 intake intake2.2. For severe: Al(OH)3 p. o., cortisone or sodium For severe: Al(OH)3 p. o., cortisone or sodium
versenate may be usedversenate may be used

Vitamin KVitamin K Naturally occurring vitamin K abundant in Naturally occurring vitamin K abundant in
pork, liver, soybeans & green leafy pork, liver, soybeans & green leafy vegetablesvegetables
Synthesize by intestinal microorganismsSynthesize by intestinal microorganisms Required for normal clotting of bloodRequired for normal clotting of blood Vitamin K-dependent clotting factors:Vitamin K-dependent clotting factors:
• Prothrombin (Factor II)Prothrombin (Factor II)• Proconvertin (Factor VII)Proconvertin (Factor VII)• Plasma thromboplastin component or PTC Plasma thromboplastin component or PTC
(Factor IX)(Factor IX)• Stuart-Prower factor (Factor X)Stuart-Prower factor (Factor X)

Vitamin K Deficiency Vitamin K Deficiency (Hypoprothrombinemia)(Hypoprothrombinemia)
Etiology:Etiology:1.1. The fetus depends on mother for supply & at birth, The fetus depends on mother for supply & at birth,
bacterial flora of GIT not yet producebacterial flora of GIT not yet produce2.2. Exclusively breast-fed infants lower vitamin K Exclusively breast-fed infants lower vitamin K
compared to formula-fedcompared to formula-fed3.3. Faulty intestinal absorption as in diarrhea, celiac Faulty intestinal absorption as in diarrhea, celiac
disease, gastrointestinal malformation & disease, gastrointestinal malformation & steatorrheasteatorrhea
4.4. Obstructive jaundice, biliary fistula, insufficient Obstructive jaundice, biliary fistula, insufficient production of bile acids or pancreatic insufficiency production of bile acids or pancreatic insufficiency lead to inadequate intestinal absorptionlead to inadequate intestinal absorption
5.5. Administration of antibiotics inhibit intestinal Administration of antibiotics inhibit intestinal bacteriabacteria
6.6. In sepsis, deficiency from disease affecting In sepsis, deficiency from disease affecting hepatobiliary functions & therapyhepatobiliary functions & therapy
7.7. Drugs like coumarin, salicylates & anticonvulsantsDrugs like coumarin, salicylates & anticonvulsants

HypoprothrombinemiaHypoprothrombinemia
Clinical Manifestations:Clinical Manifestations:1.1. Hemorrhagic manifestations are the hallmarkHemorrhagic manifestations are the hallmark2.2. Bleeding in the newborn from the cord or Bleeding in the newborn from the cord or
circumcision sitecircumcision site3.3. GIT bleeding, hematuria & intracranial GIT bleeding, hematuria & intracranial
hemorrhagehemorrhage4.4. Anemia & shock may ensue from severe blood Anemia & shock may ensue from severe blood
losslossLaboratory Test: Laboratory Test: Most useful test is Most useful test is 1-stage 1-stage
prothrombin time test (Quick)prothrombin time test (Quick), prolongation , prolongation presumptive evidence deficiencypresumptive evidence deficiency

HypoprothrombinemiaHypoprothrombinemiaPrevention and Treatment:Prevention and Treatment:
A.A. 4 requirements to prevent & control a potentially fatal 4 requirements to prevent & control a potentially fatal hemorrhagic state:hemorrhagic state:
1.1. Bile of normal composition in the GITBile of normal composition in the GIT
2.2. Adequate dietAdequate diet
3.3. Normal absorptive surface in the small intestinesNormal absorptive surface in the small intestines
4.4. Functioning liver capable of synthesizingFunctioning liver capable of synthesizing
B.B. In the newborn, vitamin KIn the newborn, vitamin K11 is being used because: is being used because:
1.1. Greater margin of safety Greater margin of safety
2.2. Acts rapidly with therapeutic levels within 2-4 hoursActs rapidly with therapeutic levels within 2-4 hours

HypoprothrombinemiaHypoprothrombinemiaPrevention and Treatment:Prevention and Treatment:C.C. The AAP Committee on Nutrition recommends:The AAP Committee on Nutrition recommends:
1.1. Prophylactic dose: Vitamin K 0.5-1 mg as single Prophylactic dose: Vitamin K 0.5-1 mg as single parenteral dose or 1-2 mg single p. o. doseparenteral dose or 1-2 mg single p. o. dose
2.2. Mild prothrombin deficiency: Vitamin K 1-2 mg p. o. Mild prothrombin deficiency: Vitamin K 1-2 mg p. o. ODOD
3.3. In severe cases with hemorrhages:In severe cases with hemorrhages: Vitamin KVitamin K11 5 mg daily parenterally 5 mg daily parenterally Whole blood if due to liver damageWhole blood if due to liver damage
D.D. Avoid excessive doses in prematures & G-6-PD deficient Avoid excessive doses in prematures & G-6-PD deficient newborns due to hemolytic action & hyperbilirubinemianewborns due to hemolytic action & hyperbilirubinemia
E.E. Vitamin K prophylaxis to woman in labor may be Vitamin K prophylaxis to woman in labor may be followed by hemolytic anemia, hyperbilirubinemia, followed by hemolytic anemia, hyperbilirubinemia, kernicterus & death in infantkernicterus & death in infant

HypoprothrombinemiaHypoprothrombinemia

Vitamin E (Tocopherol)Vitamin E (Tocopherol) Denotes a group of 8 compounds with Denotes a group of 8 compounds with
similar structures and antioxidant activitysimilar structures and antioxidant activity The most potent member is The most potent member is tocopheroltocopherol, ,
the main form in humansthe main form in humans Functions as antioxidant mainly located Functions as antioxidant mainly located
within cell membranes where it prevents within cell membranes where it prevents lipid peroxidation and formation of free lipid peroxidation and formation of free radicalsradicals
Best dietary sources: vegetable oils, seeds, Best dietary sources: vegetable oils, seeds, nuts, green leafy vegetables and margarine nuts, green leafy vegetables and margarine

Hypovitaminosis EHypovitaminosis EEtiology:Etiology:1.1. Poor absorption in premature infants*Poor absorption in premature infants*2.2. In children with fat malabsorption, most common in cholestatic In children with fat malabsorption, most common in cholestatic
liver disease & a complication of autosomal recessive liver disease & a complication of autosomal recessive abetalipoproteinemia abetalipoproteinemia
3.3. Other malabsorptive states such as cystic fibrosis, Other malabsorptive states such as cystic fibrosis, acanthocytosis, celiac disease, short-bowel syndrome or Crohn acanthocytosis, celiac disease, short-bowel syndrome or Crohn diseasedisease
4.4. In a rare autosomal recessive disorder, Ataxia with isolated In a rare autosomal recessive disorder, Ataxia with isolated Vitamin E Deficiency (AVED), that affects vitamin E transportVitamin E Deficiency (AVED), that affects vitamin E transport
Clinical Manifestations:Clinical Manifestations:1.1. Appear after 1 yr of age in prolonged deficiency: degenerative Appear after 1 yr of age in prolonged deficiency: degenerative
neurologic syndrome of cerebellar disease, posterior column neurologic syndrome of cerebellar disease, posterior column dysfunction and retinal disease**dysfunction and retinal disease**
2.2. In premature infants, hemolysis typically develops during 2In premature infants, hemolysis typically develops during 2ndnd mo with edema and thrombocytosis potentially causing anemiamo with edema and thrombocytosis potentially causing anemia
Diagnosis:Diagnosis:1.1. Best by measuring ratio of vitamin E to serum lipids: abnormal Best by measuring ratio of vitamin E to serum lipids: abnormal
ratio <0.8 mg/gratio <0.8 mg/g

Hypovitaminosis EHypovitaminosis E2.2. Electroretinography abnormalities may precede PE findings in Electroretinography abnormalities may precede PE findings in
those with retinal involvementthose with retinal involvement3.3. Premature infants with unexplained hemolytic anemia after 1Premature infants with unexplained hemolytic anemia after 1 stst
mo, especially if thrombocytosis presentmo, especially if thrombocytosis presentPrognosis:Prognosis:
Hemolytic anemia in infants resolves with correction of deficiencyHemolytic anemia in infants resolves with correction of deficiency Treatment prevents progression of neurologic manifestationsTreatment prevents progression of neurologic manifestations
Prevention & Treatment:Prevention & Treatment: 1.1. Prevention in premature infants: sufficient vitamin E, 7mg/g of Prevention in premature infants: sufficient vitamin E, 7mg/g of
unsaturated fat in the diet, and formula without high content unsaturated fat in the diet, and formula without high content PUFAsPUFAs
2.2. Treatment dose in neonates: 25–50 units/day for 1 wk, follow Treatment dose in neonates: 25–50 units/day for 1 wk, follow with adequate dietary intakewith adequate dietary intake
3.3. Severe malabsorption: Severe malabsorption: -Tocopheryl polyethylene glycol -Tocopheryl polyethylene glycol succinate (TPGS), a water-soluble preparation absorbed in succinate (TPGS), a water-soluble preparation absorbed in absence of bile salts 20–25 units/kg/dayabsence of bile salts 20–25 units/kg/day
4.4. Children with AVED: high doses of vitamin EChildren with AVED: high doses of vitamin E

The The Energy-Releasing Energy-Releasing
VitaminsVitamins

Thiamine (Vitamin B1) Thiamine (Vitamin B1) Deficiency BeriberiDeficiency Beriberi
Pathology: Pathology: Biochemical accumulation of pyruvic Biochemical accumulation of pyruvic and lactic acid in body fluids causing:and lactic acid in body fluids causing:
1.1. Cardiac dysfunction such as cardiac Cardiac dysfunction such as cardiac enlargement esp. right side, edema of enlargement esp. right side, edema of interstitial tissue & fatty degeneration of interstitial tissue & fatty degeneration of myocardiummyocardium
2.2. Degeneration of myelin & axon cylinders Degeneration of myelin & axon cylinders resulting in peripheral neuropathy resulting in peripheral neuropathy
3.3. In chronic deficiency states, vascular dilatation In chronic deficiency states, vascular dilatation & brain hemorrhages of Wernicke’s Disease & brain hemorrhages of Wernicke’s Disease resulting in weakness of eye movement, resulting in weakness of eye movement, ataxia of gait and mental disturbanceataxia of gait and mental disturbance

BeriberiBeriberiThree forms:Three forms:1.1. Wet beriberi:Wet beriberi: generalized edema, acute cardiac generalized edema, acute cardiac
symptoms and prompt response to thiamine symptoms and prompt response to thiamine administrationadministration
2.2. Dry beriberi:Dry beriberi: edema not present, condition similar to edema not present, condition similar to peripheral neuritis w/ neurological disorders presentperipheral neuritis w/ neurological disorders present
3.3. Infantile beriberiInfantile beriberi divided into: divided into:a.a. Acute cardiac:Acute cardiac: Ages 2-4 months; sudden onset of Ages 2-4 months; sudden onset of
cardiac s/sx such as cyanosis, dyspnea, systolic cardiac s/sx such as cyanosis, dyspnea, systolic murmur & pulmonary edema w/ ralesmurmur & pulmonary edema w/ rales
b.b. Aphonic:Aphonic: Ages 5-7 months; insidious onset of Ages 5-7 months; insidious onset of hoarseness, dysphonia or aphoniahoarseness, dysphonia or aphonia
c.c. Pseudomeningeal:Pseudomeningeal: Ages 8-10 months; signs of Ages 8-10 months; signs of meningeal irritation w/ apathy, drowsiness & meningeal irritation w/ apathy, drowsiness & even unconsciousness; occurs more ofteneven unconsciousness; occurs more often

BeriberiBeriberiDiagnosis:Diagnosis:1.1. Clinical manifestations not Clinical manifestations not
conclusiveconclusive2.2. Therapeutic test, parenteral Therapeutic test, parenteral
thiamine = dramatic thiamine = dramatic improvementimprovement
3.3. Blood lactic & pyruvic acid Blood lactic & pyruvic acid levels elevated after oral levels elevated after oral glucose loadglucose load
4.4. Decreased red cell Decreased red cell hemolysate transketolasehemolysate transketolase
RDA:RDA: Infants 0.4mg Infants 0.4mg Older children 0.6-Older children 0.6-
1.2mg1.2mgNursing mothers Nursing mothers
1.5mg1.5mgAdults 1-1.3mgAdults 1-1.3mg
Prevention:Prevention:1.1. Richest sources: pork, whole Richest sources: pork, whole
grain, enriched cereal grains grain, enriched cereal grains and legumesand legumes
2.2. Improved milling of rice Improved milling of rice conserve thiamineconserve thiamine
3.3. Excessive cooking of Excessive cooking of vegetables or polishing of vegetables or polishing of cereals destroy itcereals destroy it
4.4. In breast-fed infants, In breast-fed infants, prevention achieved by prevention achieved by maternal diet w/ sufficient maternal diet w/ sufficient amountsamounts
Treatment:Treatment:1.1. Children: 10mg p. o. daily Children: 10mg p. o. daily
for several weeksfor several weeks2.2. Adults: 50mg Adults: 50mg

BeriberiBeriberi

BeriberiBeriberi

Riboflavin (Vitamin B2) Riboflavin (Vitamin B2) DeficiencyDeficiency
Functions:Functions:
1.1. Coenzyme of flavoprotein important in a. a., f. a. & Coenzyme of flavoprotein important in a. a., f. a. & CHO metabolism & cellular respirationCHO metabolism & cellular respiration
2.2. Needed also by retinal eye pigments for light Needed also by retinal eye pigments for light adaptationadaptation
Clinical Manifestations:Clinical Manifestations:
1.1. Lesions of the lips characteristic, most common are Lesions of the lips characteristic, most common are angular stomatitis and cheilosis angular stomatitis and cheilosis
2.2. Localized seborrheic dermatitis of the face such as Localized seborrheic dermatitis of the face such as nasolabial seborrhea or dyssebacia & angular nasolabial seborrhea or dyssebacia & angular palpebritispalpebritis
3.3. Scrotal or vulvar dermatosis may also occurScrotal or vulvar dermatosis may also occur
4.4. Ocular s/sx are photophobia, blurred vision, itching of Ocular s/sx are photophobia, blurred vision, itching of eyes, lacrimation & corneal vascularizationeyes, lacrimation & corneal vascularization

Riboflavin DeficiencyRiboflavin DeficiencyDiagnosis:Diagnosis:1.1. Urinary riboflavin determinationUrinary riboflavin determination2.2. RBC riboflavin load testRBC riboflavin load testRDA:RDA: Infants & children <10yrs 0.6-1.4mgInfants & children <10yrs 0.6-1.4mg
Children >10yrs 1.4-2mgChildren >10yrs 1.4-2mgAdults 0.025mg/gm dietary proteinAdults 0.025mg/gm dietary protein
Prevention:Prevention:1.1. Best sources: eggs, liver, meat, fish, milk, whole or Best sources: eggs, liver, meat, fish, milk, whole or
enriched ground cereals, legumes, green leafy enriched ground cereals, legumes, green leafy vegetablesvegetables
2.2. Also present in beerAlso present in beer3.3. Impaired absorption in achlorhydria, diarrhea & Impaired absorption in achlorhydria, diarrhea &
vomitingvomitingTreatment:Treatment:1.1. Riboflavin 2-5mg p. o. daily w/ increased B complexRiboflavin 2-5mg p. o. daily w/ increased B complex2.2. Parenteral administration Parenteral administration ifif relief not obtained relief not obtained

Riboflavin DeficiencyRiboflavin Deficiency

Niacin (Vitamin B3) Niacin (Vitamin B3) Deficiency PellagraDeficiency Pellagra
Etiology:Etiology:1.1. Diets low in niacin &/or tryptophanDiets low in niacin &/or tryptophan2.2. Amino acid imbalance or as result of malabsorptionAmino acid imbalance or as result of malabsorption3.3. Excessive corn consumptionExcessive corn consumptionClinical Manifestations:Clinical Manifestations:1.1. Starts w/ anorexia, weakness, irritability, numbness & dizzinessStarts w/ anorexia, weakness, irritability, numbness & dizziness2.2. Classical triad of dermatitis, diarrhea & dementiaClassical triad of dermatitis, diarrhea & dementia3.3. Dermatitis may develop insidiously to sunlight or heatDermatitis may develop insidiously to sunlight or heat
a.a. First as symmetrical erythemaFirst as symmetrical erythemab.b. Followed by drying, scaling & pigmentation w/ vesicles or Followed by drying, scaling & pigmentation w/ vesicles or
bullaebullaec.c. Predilection for back of hands, wrists, forearms (pellagrous Predilection for back of hands, wrists, forearms (pellagrous
glove), neck (Casal’s necklace) & lower legs (pellagrous boot)glove), neck (Casal’s necklace) & lower legs (pellagrous boot)4.4. GIT s/sx are stomatitis, glossitis or diarrhea w/ feces pale, foul GIT s/sx are stomatitis, glossitis or diarrhea w/ feces pale, foul
milky, soapy or at times steatorrheicmilky, soapy or at times steatorrheic5.5. Mental changes include depression, irritability, disorientation, Mental changes include depression, irritability, disorientation,
insomnia & deliriuminsomnia & delirium

PellagraPellagraDiagnosis:Diagnosis:1.1. History & manifestations of diet poor in niacin or tryptophanHistory & manifestations of diet poor in niacin or tryptophan2.2. In niacin deficiency, urinary levels of N-methyl-nicotinamide In niacin deficiency, urinary levels of N-methyl-nicotinamide
low or absentlow or absentDifferential diagnoses:Differential diagnoses: Kwashiorkor, Infantile Eczema, Kwashiorkor, Infantile Eczema,
Combination deficiencies of amino acids & trace minerals Combination deficiencies of amino acids & trace minerals such as zincsuch as zinc
RDA:RDA: Infants & children <10yrs 6-10mgInfants & children <10yrs 6-10mgOlder individuals 10-20mgOlder individuals 10-20mg
Prevention:Prevention:1.1. Rich sources include meat, peanuts and legumes, whole Rich sources include meat, peanuts and legumes, whole
grain and enriched breads and cerealsgrain and enriched breads and cereals2.2. Avoid too large a proportion of cornAvoid too large a proportion of cornTreatment:Treatment:1.1. Niacin 50-300mg daily may be taken for a long timeNiacin 50-300mg daily may be taken for a long time2.2. Skin lesions may be covered w/ soothing lotionsSkin lesions may be covered w/ soothing lotions

PellagraPellagra

Pyridoxine (Vitamin B6) Pyridoxine (Vitamin B6) DeficiencyDeficiency
Functions: Functions:
1.1. In the synthesis and catabolism of a. a., synthesis In the synthesis and catabolism of a. a., synthesis of neurotransmitters, porphyrins and niacinof neurotransmitters, porphyrins and niacin
2.2. Important role in clinical conditions such as Important role in clinical conditions such as anemia, hyperemesis gravidarum, cardiac anemia, hyperemesis gravidarum, cardiac decompensation, radiation effects, skin grafting, decompensation, radiation effects, skin grafting, INH therapy & seborrheic dermatitisINH therapy & seborrheic dermatitis
Etiology:Etiology:
1.1. Losses from refining, processing, cooking & Losses from refining, processing, cooking & storingstoring
2.2. Malabsorptive diseases such as celiac diseaseMalabsorptive diseases such as celiac disease
3.3. Direct antagonism between INH & pyridoxal Direct antagonism between INH & pyridoxal phosphate at the apoenzyme levelphosphate at the apoenzyme level

Pyridoxine DeficiencyPyridoxine DeficiencyClinical Manifestations:Clinical Manifestations:
1.1. Three different typesThree different types
a.a. NeuropathicNeuropathic, due to insufficient neurotransmitter , due to insufficient neurotransmitter synthesis such as irritability, depression & synthesis such as irritability, depression & somnolencesomnolence
b.b. PellagrousPellagrous, due to low endogenous niacin , due to low endogenous niacin synthesis such as seborrheic dermatitis, intertrigo, synthesis such as seborrheic dermatitis, intertrigo, angular stomatitis & glossitisangular stomatitis & glossitis
c.c. AnemicAnemic, due to low porphyrin synthesis such as , due to low porphyrin synthesis such as microcytic anemia & lymphopenia microcytic anemia & lymphopenia
2.2. In genetic diseases involving pyridoxal phosphate In genetic diseases involving pyridoxal phosphate enzymes: xanthurenic aciduria, cystathioninuria & enzymes: xanthurenic aciduria, cystathioninuria & homocystinuriahomocystinuria

Pyridoxine DeficiencyPyridoxine DeficiencyDiagnosis:Diagnosis: As screening test, tryptophan load test -100mg/kg BW As screening test, tryptophan load test -100mg/kg BW
tryptophan gives large amount of xanthurenic acid in urinetryptophan gives large amount of xanthurenic acid in urine
Prevention:Prevention:
1.1. Firm requirement not established but usual recommendation: Firm requirement not established but usual recommendation: Infant 0.1-0.5mg, Child 0.5-1.5mg & Adult 1.5-2mgInfant 0.1-0.5mg, Child 0.5-1.5mg & Adult 1.5-2mg
2.2. Rich sources: yeast, whole wheat, corn, egg yolk, liver and Rich sources: yeast, whole wheat, corn, egg yolk, liver and lean meatlean meat
3.3. Toxicity at extremely high doses described; infants whose Toxicity at extremely high doses described; infants whose mothers received large doses during pregnancy should be mothers received large doses during pregnancy should be observed for seizures due to dependencyobserved for seizures due to dependency
4.4. Children receiving INH therapy should be observed for Children receiving INH therapy should be observed for neurologic s/sx in w/c case pyridoxine should be givenneurologic s/sx in w/c case pyridoxine should be given
Treatment:Treatment:
1.1. Pyridoxine 100mg IM injection for seizures due to deficiencyPyridoxine 100mg IM injection for seizures due to deficiency
2.2. Children w/ pyridoxine dependency 2-10mg IM injection or 10-Children w/ pyridoxine dependency 2-10mg IM injection or 10-100mg oral vitamin B6 100mg oral vitamin B6

The The Hematopoietic Hematopoietic
VitaminsVitamins

Folic Acid (Vitamin B9) Folic Acid (Vitamin B9) DeficiencyDeficiencyFunctions:Functions:
1.1. Needed for RBC & DNA formation & cell multiplication esp. GI cellsNeeded for RBC & DNA formation & cell multiplication esp. GI cells2.2. Newly discovered functions:Newly discovered functions:
a.a. Prevents neural tube defectsPrevents neural tube defectsb.b. Prevents heart disease (reduces homocysteine levels)Prevents heart disease (reduces homocysteine levels)c.c. Prevents colon cancerPrevents colon cancer
Peak incidence 4-7 monthsPeak incidence 4-7 monthsEtiology:Etiology:1.1. Deficient dietary intake:Deficient dietary intake: goat’s milk deficient & powdered milk goat’s milk deficient & powdered milk
poor sourcepoor source2.2. Deficient absorptionDeficient absorption in celiac disease, achlorhydria, w/ in celiac disease, achlorhydria, w/
anticonvulsant drugs, zinc deficiency & bacterial overgrowthanticonvulsant drugs, zinc deficiency & bacterial overgrowth3.3. Impaired metabolismImpaired metabolism in ascorbic acid deficiency, hypothyroidism, in ascorbic acid deficiency, hypothyroidism,
w/ drugs like trimethoprimw/ drugs like trimethoprim4.4. Increased requirementIncreased requirement during rapid growth & infection during rapid growth & infection5.5. Increased excretion/lossIncreased excretion/loss may occur due to vitamin B12 deficiency may occur due to vitamin B12 deficiency

Folic Acid DeficiencyFolic Acid DeficiencyClinical Manifestations:Clinical Manifestations:1.1. Megaloblastic anemia w/ Megaloblastic anemia w/
irritability, failure to gain wt irritability, failure to gain wt & chronic diarrhea& chronic diarrhea
2.2. Thrombocytopenic Thrombocytopenic hemorrhages advanced hemorrhages advanced casescases
3.3. Scurvy may be presentScurvy may be presentLaboratory Findings:Laboratory Findings:1.1. Anemia macrocytic Anemia macrocytic 2.2. Serum folic acid <3ng/ml Serum folic acid <3ng/ml
(Normal = 5-20ng/ml)(Normal = 5-20ng/ml)3.3. RBC folate levels indicator RBC folate levels indicator
of chronic deficiency of chronic deficiency (Normal = 150-600ng/ml)(Normal = 150-600ng/ml)
4.4. Serum iron & vitamin B12 Serum iron & vitamin B12 normal or elevated normal or elevated
6.6. Formiminoglutamic acid in Formiminoglutamic acid in urine esp after oral histidineurine esp after oral histidine
7.7. Serum LDH markedly highSerum LDH markedly high8.8. Bone marrow hypercellularBone marrow hypercellularRDA:RDA: 20-50mcg/24 hrs 20-50mcg/24 hrsTreatment:Treatment:1.1. Parenteral folic acid Parenteral folic acid
2-5mg/24 hr response in 72 2-5mg/24 hr response in 72 hrs, for 3-4 wkshrs, for 3-4 wks
2.2. Transfusions only if anemia Transfusions only if anemia severesevere
3.3. Satisfactory responses even Satisfactory responses even w/ low doses of 50mcg/24 w/ low doses of 50mcg/24 hr, no effect on primary hr, no effect on primary vitamin B12 deficiencyvitamin B12 deficiency
4.4. If pernicious anemia present, If pernicious anemia present, prolonged use of folic acid prolonged use of folic acid should be avoidedshould be avoided

Folic Acid DeficiencyFolic Acid Deficiency

Cobalamine (Vitamin B12) Cobalamine (Vitamin B12) DeficiencyDeficiency
Absorption:Absorption: Vitamin B12 + glycoprotein (intrinsic factor) from Vitamin B12 + glycoprotein (intrinsic factor) from parietal cells of gastric fundus parietal cells of gastric fundus terminal ileum absorption + terminal ileum absorption + intrinsic factor + Ca++ intrinsic factor + Ca++ blood blood
Function: Function: Needed in reactions affecting production of methyl Needed in reactions affecting production of methyl groupsgroups
Etiology:Etiology:1.1. Congenital Pernicious AnemiaCongenital Pernicious Anemia: Lack of secretion of intrinsic : Lack of secretion of intrinsic
factor by stomach manifest at factor by stomach manifest at 9 mo-10 yr9 mo-10 yr as uterine stores as uterine stores become exhaustedbecome exhausted
2.2. Inadequate intake or dietary deficiency rareInadequate intake or dietary deficiency rarea.a. Strict vegetarian dietStrict vegetarian dietb.b. Not commonly seen in kwashiorkor or marasmusNot commonly seen in kwashiorkor or marasmusc.c. Breast-fed infants whose mothers had deficient diets or Breast-fed infants whose mothers had deficient diets or
pernicious anemiapernicious anemia3.3. Consumption or inhibition of B12-intrinsic factor complexConsumption or inhibition of B12-intrinsic factor complex4.4. Vitamin B12 malabsorption from disease of ileal receptor sites Vitamin B12 malabsorption from disease of ileal receptor sites
or other intestinal causesor other intestinal causes

Cobalamine DeficiencyCobalamine DeficiencyClinical Manifestations:Clinical Manifestations:
1.1. Megaloblastic anemia that becomes severe*Megaloblastic anemia that becomes severe*
2.2. Neurological includes ataxia, paresthesias, Neurological includes ataxia, paresthesias, hyporeflexia, Babinski responses, clonus & hyporeflexia, Babinski responses, clonus & coma**coma**
3.3. Tongue smooth, red & painfulTongue smooth, red & painful
Laboratory Findings:Laboratory Findings:
1.1. Anemia macrocyticAnemia macrocytic
2.2. Serum vitamin B12 <100pg/ml but serum iron & Serum vitamin B12 <100pg/ml but serum iron & folic acid normal or elevatedfolic acid normal or elevated
3.3. Serum LDH activity markedly increasedSerum LDH activity markedly increased
4.4. Urinary excess of methylmalonic acid, a reliable & Urinary excess of methylmalonic acid, a reliable & sensitive indexsensitive index

Cobalamine DeficiencyCobalamine Deficiency5.5. Schilling testSchilling test to assess the absorption of vitamin B12: to assess the absorption of vitamin B12:
a.a. Normal person ingests small amount of radioactive vitamin Normal person ingests small amount of radioactive vitamin B12 B12 none in urine **If flushing dose injected parenterally, none in urine **If flushing dose injected parenterally, 1000mcg of non-radioactive vitamin B12 1000mcg of non-radioactive vitamin B12 10-30% of 10-30% of previous radioactive vitamin B12 appears in urineprevious radioactive vitamin B12 appears in urine
b.b. Pernicious anemia Pernicious anemia 2% or less **If modified: 30 mg 2% or less **If modified: 30 mg intrinsic factor administered along intrinsic factor administered along normal amounts normal amounts
c.c. Disease of ileal receptor sites or other intestinal causes Disease of ileal receptor sites or other intestinal causes no improvement even w/ intrinsic factorno improvement even w/ intrinsic factor
RDA: RDA: Infants 0.5 mcg/dayInfants 0.5 mcg/dayOlder children & adults 3mcg/dayOlder children & adults 3mcg/day
Treatment:Treatment:1.1. Prompt hematological response w/ parenteral vitamin B12 1-Prompt hematological response w/ parenteral vitamin B12 1-
5mcg /24hr5mcg /24hr2.2. If there is neurological involvement 1mg IM daily for at least If there is neurological involvement 1mg IM daily for at least
2wks2wks3.3. Pernicious Anemia: Monthly vitamin B12 1mg IM necessary Pernicious Anemia: Monthly vitamin B12 1mg IM necessary
throughout patient’s lifethroughout patient’s life

Cobalamine DeficiencyCobalamine Deficiency

Ascorbic AcidAscorbic Acid(Vitamin C) Deficiency(Vitamin C) Deficiency
ScurvyScurvyFunctions:Functions:1.1. Hydroxyproline, found only in collagen, major connective Hydroxyproline, found only in collagen, major connective
tissue in body, forms from proline requiring ascorbic acidtissue in body, forms from proline requiring ascorbic acid2.2. If defective collagen formation, endochondral bone If defective collagen formation, endochondral bone
formation stops since oste, intercellular substance, not formation stops since oste, intercellular substance, not formedformed
3.3. In hydroxylation reactions in synthesis of steroids and In hydroxylation reactions in synthesis of steroids and epinephrineepinephrine
4.4. Aids iron absorption by reducing it to ferrous state in Aids iron absorption by reducing it to ferrous state in stomachstomach
5.5. Spares vitamin A, vitamin E and some B vitamins by Spares vitamin A, vitamin E and some B vitamins by protecting them from oxidationprotecting them from oxidation
6.6. Enhances utilization of folic acid by aiding conversion of Enhances utilization of folic acid by aiding conversion of folate to tetrahydrofolatefolate to tetrahydrofolate

Ascorbic AcidAscorbic Acid(Vitamin C) Deficiency(Vitamin C) Deficiency
ScurvyScurvy More common 6-24 monthsMore common 6-24 months
Etiology:Etiology:
1.1. May develop in breastfed infant if mother’s diet deficientMay develop in breastfed infant if mother’s diet deficient
2.2. Improper cooking practices produce significant lossesImproper cooking practices produce significant losses
Clinical Manifestations:Clinical Manifestations:
1.1. Early: irritability, digestive disturbances & anorexiaEarly: irritability, digestive disturbances & anorexia
2.2. Mild deficiency: ecchymoses, corkscrew hairs & Mild deficiency: ecchymoses, corkscrew hairs & petechiae due to increased capillary fragility from petechiae due to increased capillary fragility from weakened collagenweakened collagen
3.3. Severe deficiency: decreased wound healing, Severe deficiency: decreased wound healing, osteoporosis, hemorrhaging, bleeding into skin and osteoporosis, hemorrhaging, bleeding into skin and friable bleeding gums with loosened teethfriable bleeding gums with loosened teeth

ScurvyScurvyClinical Manifestations:Clinical Manifestations:4.4. A presenting feature: an infant w/ painful, immobile A presenting feature: an infant w/ painful, immobile
legs (pseudoparalysis), in “frog position” & legs (pseudoparalysis), in “frog position” & occasionally w/ massoccasionally w/ mass
5.5. Depression of sternum w/ a “rosary of scorbutic Depression of sternum w/ a “rosary of scorbutic beads” at costochondral junction due to subluxation beads” at costochondral junction due to subluxation of sternal plateof sternal plate
6.6. Orbital or subdural hemorrhages, melena & Orbital or subdural hemorrhages, melena & hematuriahematuria
7.7. Low grade fever & anemia usually presentLow grade fever & anemia usually present8.8. Impairment of growth & developmentImpairment of growth & developmentDiagnosis:Diagnosis:1.1. History of vitamin C-deficient dietHistory of vitamin C-deficient diet2.2. Clinical pictureClinical picture3.3. Therapeutic testTherapeutic test

ScurvyScurvyDiagnosis:Diagnosis:
4.4. X-ray findings in long bones:X-ray findings in long bones:
a.a. Most prominent & early change: knee atrophyMost prominent & early change: knee atrophy
b.b. Shaft trabeculae cannot be distinguished Shaft trabeculae cannot be distinguished giving “ground glass appearance”giving “ground glass appearance”
c.c. Cortex reduced to “pencil-point thinness”Cortex reduced to “pencil-point thinness”
d.d. Zone of well-calcified cartilage, white line of Zone of well-calcified cartilage, white line of Fraenkel irregular & thickened white lineFraenkel irregular & thickened white line
e.e. Zone of rarefaction, a linear break in bone Zone of rarefaction, a linear break in bone proximal & parallel to white line under at proximal & parallel to white line under at metaphysismetaphysis
f.f. Calcifying subperiosteal hemorrhages cause Calcifying subperiosteal hemorrhages cause bone to assume a dumb-bell shapebone to assume a dumb-bell shape

ScurvyScurvy5.5. Laboratory tests not helpful:Laboratory tests not helpful:
a.a. Ascorbic acid concentrate of buffy layer of Ascorbic acid concentrate of buffy layer of centrifuged oxalated blood = zero in latent centrifuged oxalated blood = zero in latent scurvyscurvy
b.b. Diminished urinary excretion of vitamin C after Diminished urinary excretion of vitamin C after loadingloading
Differential Diagnosis:Differential Diagnosis:1.1. Bleeding, swollen gums: Chronic gingivitis & Bleeding, swollen gums: Chronic gingivitis &
pyorrhea w/ pus & respond to good dental pyorrhea w/ pus & respond to good dental hygienehygiene
2.2. Pseudoparalysis: Syphilis negative x-ray; Pseudoparalysis: Syphilis negative x-ray; Poliomyelitis absent tenderness of extremitiesPoliomyelitis absent tenderness of extremities
3.3. Tenderness of limbs: RF age >2 yrs; Suppurative Tenderness of limbs: RF age >2 yrs; Suppurative arthritis & osteomyelitis positive blood culturesarthritis & osteomyelitis positive blood cultures
4.4. Bleeding manifestations: Blood dyscracias Bleeding manifestations: Blood dyscracias positive blood examspositive blood exams
5.5. ““Rosary of scorbutic beads”: RicketsRosary of scorbutic beads”: Rickets

ScurvyScurvyPrognosis:Prognosis: 1.1. Recovery rapid w/ adequate treatment & permanent Recovery rapid w/ adequate treatment & permanent
deformity raredeformity rare2.2. Pain ceases in a few days but swelling may last monthsPain ceases in a few days but swelling may last monthsPrevention :Prevention :1.1. Minimum daily intake 30mg as recommended by WHO Minimum daily intake 30mg as recommended by WHO
for all agesfor all ages2.2. Every infant should receive supplement starting 2nd wk Every infant should receive supplement starting 2nd wk 3.3. Lactating mothers at least 50mg vitamin C dailyLactating mothers at least 50mg vitamin C daily4.4. Guava & papaya richer than citrus fruits, also in most Guava & papaya richer than citrus fruits, also in most
green leafy vegetables, tomatoes & fresh tubers but green leafy vegetables, tomatoes & fresh tubers but absent in cereals, most animal products & canned milkabsent in cereals, most animal products & canned milk
Treatment: Treatment: Ascorbic acid 200-500mg daily or 100-150ml of fruit Ascorbic acid 200-500mg daily or 100-150ml of fruit juicejuice

ScurvyScurvy

ScurvyScurvy

Be master of your Be master of your habits, habits, Or they will master Or they will master you.you.