Embed Size (px)
Citation preview
Critical Reviews in Oncology/Hematology 42 (2002) 145–155
Oncology drug clinical development and approval in Japan:the role of the pharmaceuticals and medical devices
evaluation center (PMDEC)�
Yasuhiro Fujiwara a,*,1, Ken Kobayashi b
a E�aluation Di�ision II, Pharmaceuticals and Medical De�ices E�aluation Center, National Institute of Health Sciences, The Ministry of HealthLabour and Welfare, Toranomon 33 Mori Bldg, 10F, Toranomon 3-8-21 Minato-ku, Tokyo 105-8409, Japan
b Mansfield Center for Pacific Affairs, Washington, DC, USA
Accepted 25 January 2002
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
2. Regulatory agencies concerned with drug development in Japan . . . . . . . . . . . . . . . . 146
3. Development and approval requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147
4. Post-marketing evaluation system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1504.1. Drug reexamination (Sai-shinsa) system (post-approval phase III study) . . . . . . . . . 1504.2. Drug reevaluation (Sai-hyouka) system . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
5. Regulatory programs for expediting development and approval: priority review . . . . . . . 151
6. Off-label usage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1526.1. Non-sponsor-initiated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1526.2. Sponsor-initiated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
6.2.1. Prior approval overseas and clinical use experience overseas . . . . . . . . . . . . 1526.2.2. Preexisting overseas approval, clinical use experience overseas, and publicly
available clinical research data . . . . . . . . . . . . . . . . . . . . . . . . . . . 1526.2.3. Publicly-sponsored research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
7. ICH E5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
8. Impact of reforms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
9. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
www.elsevier.com/locate/critrevonc
� The views and opinions expressed in this work reflect the author’s personal opinions and do not necessarily represent the views of thePharmaceuticals and Medical Devices Evaluation Center, Japan and the US Food and Drug Administration.
* Corresponding author. Tel.: +81-3-5403-1411; fax: +81-3-5403-1417.E-mail addresses: [email protected] (Y. Fujiwara), [email protected] (K. Kobayashi).1 Present address: Division of Oncology Drug Products, Center for Drug Evaluation and Research, HFD-150, Food and Drug Administration,
5600 Fishers Lane, Rockville, MD 20857, USA.
1040-8428/02/$ - see front matter © 2002 Published by Elsevier Science Ireland Ltd.PII: S1040 -8428 (02 )00010 -0

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155146
Abstract
In 1996 the Japanese Diet amended the Pharmaceutical Affairs Law (PAL) and its related laws based on 1996 report of thead-hoc Committee for Drug Safety Ensuring Measures. Between 1996 and 2000, the drug approval system in Japan underwenta series of radical reforms. We describe in this paper the current system for drug approval, discuss the post-approvalreexamination and reevaluation system, conditions under which development and review may be expedited, and mechanisms forapproval of off-label usage. Finally, we discuss the impact of the International Conference on Harmonization (ICH) agreementon drug development and review in Japan. © 2002 Published by Elsevier Science Ireland Ltd.
Keywords: PMDEC; Drug development; Drug approval; Off-label usage; ICH-E5
1. Introduction
In 1996, the Japanese Diet amended the Pharmaceu-tical Affairs Law (PAL) and its related laws to providecomprehensive drug safety measures at each stage dur-ing drug development, from the pre-clinical and clinicalphases to the post-marketing surveillance phase, basedon the 1996 report of the Committee for Drug SafetyEnsuring Measures.
Based on this change in the law, between 1996 and2001 the Ministry of Health and Welfare (MHW, cur-rently MHLW) [1] revised the regulations implementingthe PAL. This resulted in a fundamental reform of themanufacturing (or import) approval application (com-parable to the New Drug Application (NDA) in theUS) review system (Table 1). One of the most impor-tant changes was the establishment of the Pharmaceuti-cals and Medical Devices Evaluation Center (PMDEC;‘Shinsa-center’) under the National Institute of HealthSciences (NIHS) of the MHLW in 1997 [2].
These changes came about as the result of two majorincidents related to the safety of prescription drugs thattriggered public outrage and enhanced MHW’s aware-
ness of the safety of pharmaceutical products. In thefall of 1993, 15 deaths were caused by use of ananti-viral agent named sorivudine and in combinationwith oral fluorouracil derivatives. Sorivudine, by in-hibiting the breakdown of 5-FU, decreased the clear-ance of 5-FU and raised its blood level, which in turnled to the development of severe drug toxicity anddeath. The Japanese public had already become con-cerned about the safety of prescription drugs as a resultof previous serious problems relating to thalidomideand chinoform. The sorivudine incident boosted publicconcern even more and led MHW to reflect on Japan’ssystem for controlling drugs. More recently, althoughthe well-known worldwide HIV infection issue causedby unheated blood products took place more than 10years ago, the Japanese courts only recently settled avery high-profile case brought by transfusion-associatedHIV disease sufferers against the manufactures of thecoagulants and the MHW. In court, delay in develop-ment of heated blood products, which would poten-tially have prevented transmission of HIV disease totransfusion recipients was a major issue in the case. Inboth the sorivudine and HIV incidents, the governmentcame under considerable public pressure to reform theold system of drug approval [3].
2. Regulatory agencies concerned with drugdevelopment in Japan
The primary law governing drug development inJapan is the PAL2 [2]. The PAL [4] and its attendantregulations [5,6] set forth the general principles govern-ing drug development and their specific implementingprocedures. Broad policy-level directives relating to theapplicability and implementation of the laws are issuedby the Cabinet as a whole and by Ministers of individ-ual ministries as Enforcement Ordinances (‘Sei-rei’) andEnforcement Regulations (‘Shou-rei’’’), respectively. Is-sues that require greater clarification, or that are con-
Table 1Key points of revision in the 1996 pharmaceutical affairs law
Strengthening of previous requirements fora
Good Clinical Practice (GCP)Good Laboratory Practice (GLP)Good Post-Marketing Surveillance Practice (GPMSP)
Introduction ofb
Standard compliance reviewsfor data attached to ‘manufacturing’ or ‘import’ approvalapplicationsfor data attached to Reexamination and Reevaluationapplications
obligation for sponsors (pharmaceutical companies)to report on adverse drug reactions and infections
obligation for sponsors to maintain confidentiality aboutsubjects
who were enrolled in the clinical trials for approvalapplications
Establishment of special pre-approval licensing system
a Previously published in the form of administrative guidances,which were replaced and incorporated into the law as of the 1996revision.
b Represented the introduction of completely new requirements.
2 In Japan, as in the United States, the legislature enacts laws,which are then interpreted with varying degrees of legal authority bythe appropriate government agency. The Cabinet issues EnforcementOrdinances, which provide broad policy-level explications.

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155 147
cerned with more technical issues are handled by sub-ministeral level (Bureau or Division) Notifications(‘Kyokuchou-tsuuchi’ or ‘Kacho-tsuuchi’, respectively).These Notifications (i.e. Kyokuchou-tsuuchi and Ka-cho-tsuuchi), which are sometimes translated into En-glish as ‘Guidelines’, are official governmentalregulations that have binding legal authority upon therelevant governmental agencies. In contrast, academicsocieties in Japan frequently issue documents that sug-gest or recommend preferred approaches to certainproblems, which are also frequently translated intoEnglish as ‘Guidelines’. These documents, however,originate from private, nongovernmental bodies, reflectthe collective opinions of these agencies, but are notlegally binding upon governmental agencies. The Eval-uation and Licensing Division of the Pharmaceuticaland Medical Safety Bureau (PMSB) [7] in MHLW,PMDEC, and the Organization for PharmaceuticalSafety and Research (OPSR; called ‘Kiko’ in Japanese)are jointly responsible for drug approval and for reviewof reexamination (‘Sai-shinsa’) and reevaluation (‘Sai-hyouka’) applications (Fig. 1).
The Evaluation and Licensing Division is responsiblefor integrating the PMDEC review into the final recom-mendation for approval (or non-approval) of an indi-vidual application, which is then forwarded to theMinister of Health, Labour, and Welfare for final ac-tion. It also has responsibility for other administrativematters, such as coordinating international affairs andformulating regulatory policy. OPSR is responsible forreviewing the ‘Initial Clinical Trial Protocol Notifica-tion’, conducting ‘Clinical Trial Consultations’ for reg-istration-directed clinical trials (industry-sponsored)(‘Chiken’) or reexamination- or reevaluation-directedclinical trials, for conducting compliance reviews of alldocuments contained within an NDA or application forreexamination or application for reevaluation, and fordomestic Good Clinical Practice (GCP) inspections.PMDEC assumes pivotal responsibility for reviewingNDA documents and is also responsible for followingon-going registration-directed clinical trials and forconducting overseas GCP inspections (Table 2).
Under PAL Article 80-2, the sponsor must submit a‘Clinical Trial Protocol Notification’ with the latestinvestigator’s brochure, clinical trial protocol, a samplecase report form, explanatory material and the consentform used in informed consent to PMDEC. The firsttime that a drug is studied in Japanese subjects, theprotocol, its supporting data, and other documents (asmentioned) are submitted to OPSR. OPSR then con-sults PMDEC, which assists in the review. However,this situation holds true for only the initial submission.Subsequent clinical trial protocol documents (and allamendments or changes to any ongoing clinical trial)are submitted and reviewed by PMDEC alone.
Article 80-2 also requires that the sponsor submitADR reports (Report of the Occurrence of AdverseDrug Reactions and Infections, etc) to the PMDECregarding a drug from all over the world if at least oneregistration-directed clinical development (until the ap-proval) using the drug is underway in Japan.
It should be noted here that, in Japan, GCP appliesonly to industry-sponsored research, i.e. registration-di-rected clinical trials and clinical trials intended to sup-port reexamination or reevaluation applications. Inother words, industry-independent, investigator-ini-tiated clinical trials are not legally bound by GCP. Inother words, Japanese law regards clinical research(except in the case of industry-sponsored research, asnoted above) to be an extension of medical practice,which has no GCP requirements. While many individ-ual investigators do abide by GCP requirements, this ison a voluntary and individual basis.
Separate but parallel Articles in the PAL governapprovals and licensing of drugs manufactured domes-tically and those imported into Japan from foreignsources. In the following paragraph, statements govern-ing domestic manufacturing are cited, with parallelstatements for import approvals or licenses indicated,as appropriate, in parentheses.
According to Article 14 (Article 23) only ‘‘… aperson intending to manufacture (import) it [a drug]…’’can submit an NDA, and according to Article 12(Article 22) ‘‘…any person who has not obtained alicense for manufacturing (importing) drugs shall notprofessionally manufacture (import) drugs…’’. In otherwords, Japan regards licensing for manufacture (im-port) and approval to manufacture (import) drugs astwo sides of the same coin. A license to manufacture(import) drugs is a business-oriented certification,granted on the basis of the applicant’s ability to con-duct such business in Japan, and upon the applicant’sability to secure appropriate facilities and personnel forsuch purpose. A license becomes invalid unless it isrenewed every 5 years. In contrast, appro�al is basedupon a scientific standard. Specifically, approval tomanufacture (import) drugs is granted upon demon-stration of appropriate safety and efficacy towards theclaimed indication and dosage.
3. Development and approval requirements
Registration-directed clinical trials of cytotoxic drugsshould be conducted in accordance with the ‘Guidelineon Clinical Evaluation Method of Anticancer Drugs’issued in 1991 [8]. In contrast to the US and the EU, inJapan, cytotoxic oncology drugs can be approved basedon tumor shrinkage. In other words, one of the princi-ples of the accelerated approval system in the US hasbeen applied to all cytotoxic oncology drugs for many
Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155148
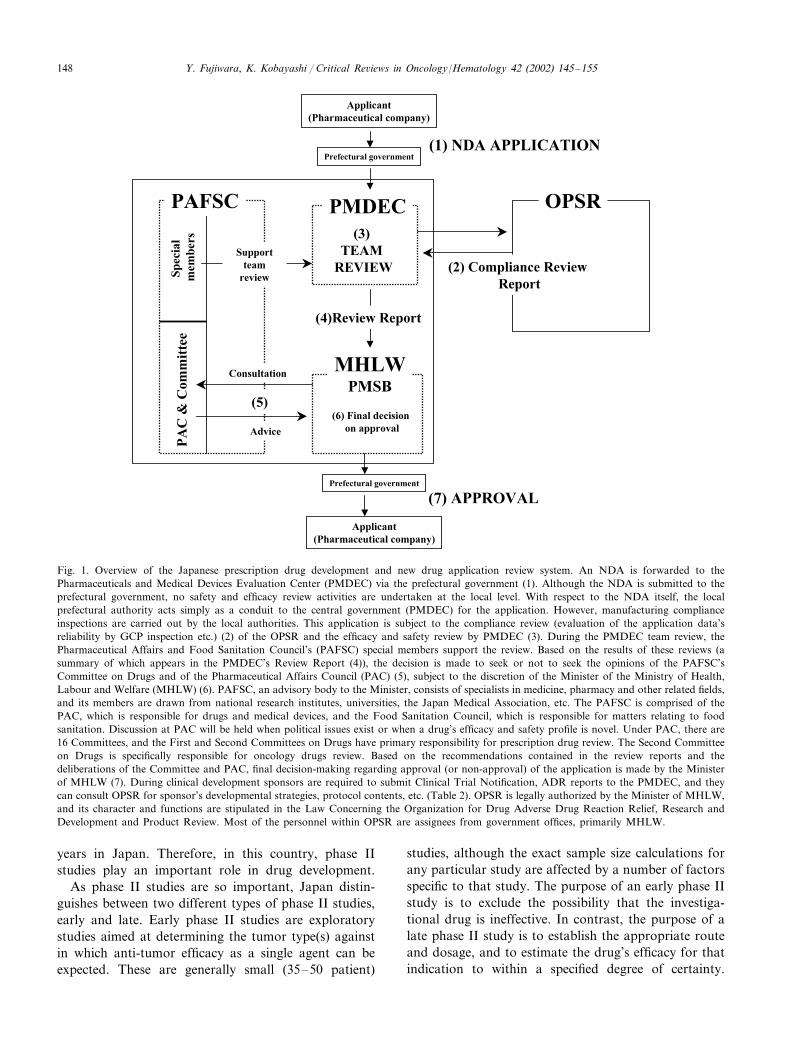
Fig. 1. Overview of the Japanese prescription drug development and new drug application review system. An NDA is forwarded to thePharmaceuticals and Medical Devices Evaluation Center (PMDEC) via the prefectural government (1). Although the NDA is submitted to theprefectural government, no safety and efficacy review activities are undertaken at the local level. With respect to the NDA itself, the localprefectural authority acts simply as a conduit to the central government (PMDEC) for the application. However, manufacturing complianceinspections are carried out by the local authorities. This application is subject to the compliance review (evaluation of the application data’sreliability by GCP inspection etc.) (2) of the OPSR and the efficacy and safety review by PMDEC (3). During the PMDEC team review, thePharmaceutical Affairs and Food Sanitation Council’s (PAFSC) special members support the review. Based on the results of these reviews (asummary of which appears in the PMDEC’s Review Report (4)), the decision is made to seek or not to seek the opinions of the PAFSC’sCommittee on Drugs and of the Pharmaceutical Affairs Council (PAC) (5), subject to the discretion of the Minister of the Ministry of Health,Labour and Welfare (MHLW) (6). PAFSC, an advisory body to the Minister, consists of specialists in medicine, pharmacy and other related fields,and its members are drawn from national research institutes, universities, the Japan Medical Association, etc. The PAFSC is comprised of thePAC, which is responsible for drugs and medical devices, and the Food Sanitation Council, which is responsible for matters relating to foodsanitation. Discussion at PAC will be held when political issues exist or when a drug’s efficacy and safety profile is novel. Under PAC, there are16 Committees, and the First and Second Committees on Drugs have primary responsibility for prescription drug review. The Second Committeeon Drugs is specifically responsible for oncology drugs review. Based on the recommendations contained in the review reports and thedeliberations of the Committee and PAC, final decision-making regarding approval (or non-approval) of the application is made by the Ministerof MHLW (7). During clinical development sponsors are required to submit Clinical Trial Notification, ADR reports to the PMDEC, and theycan consult OPSR for sponsor’s developmental strategies, protocol contents, etc. (Table 2). OPSR is legally authorized by the Minister of MHLW,and its character and functions are stipulated in the Law Concerning the Organization for Drug Adverse Drug Reaction Relief, Research andDevelopment and Product Review. Most of the personnel within OPSR are assignees from government offices, primarily MHLW.
years in Japan. Therefore, in this country, phase IIstudies play an important role in drug development.
As phase II studies are so important, Japan distin-guishes between two different types of phase II studies,early and late. Early phase II studies are exploratorystudies aimed at determining the tumor type(s) againstin which anti-tumor efficacy as a single agent can beexpected. These are generally small (35–50 patient)
studies, although the exact sample size calculations forany particular study are affected by a number of factorsspecific to that study. The purpose of an early phase IIstudy is to exclude the possibility that the investiga-tional drug is ineffective. In contrast, the purpose of alate phase II study is to establish the appropriate routeand dosage, and to estimate the drug’s efficacy for thatindication to within a specified degree of certainty.

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155 149
Generally, late phase II studies are to be conducted usingmonotherapy in previously untreated patients, but thisgeneral principle is interpreted broadly in the context ofexisting standard therapy. For instance, in the case ofbreast cancer, leukemia, malignant lymphoma, and otherdiseases in which well-accepted standard therapy exists,late phase II studies may be conducted in previously-treated patients. In cases where standard therapy calls forcombination regimens, monotherapy studies may beforegone in favor of including the investigational drug aspart of a combination regimen. However, should thisapproach be taken, a comparative study would beneeded.
In accordance with the aforementioned guideline,sponsors usually conduct several disease-oriented earlyphase II studies and more than two independent latePhase II studies. The two independent studies do notnecessarily have to be of identical design (although theyusually are), and any study design will be acceptable, aslong as consistency in drug efficacy and safety can bedemonstrated.
The guideline makes two noteworthy points regardingthe design of phase II trials. In the interest of maximizingefficiency, the guideline proposes the use of a multi-level-study method (i.e. two-stage design) for early phase IIstudies, enabling early stopping of the trial [9,10]. Theguideline requires that late phase II studies be conductedto determine the investigational drug’s efficacy (as mea-sured by response rate) to a specified degree of confi-dence, i.e. the width of the 95% confidence interval forthe desirable target level (response rate) should be at leastwithin 20%. For instance, the 95% CI should be within10–30% if the point estimate for response rate is 20%.Similarly, the 95% CI should be 40–60% if the pointestimate for response rate is 50%.
The guideline states that ‘‘… the desirable target levelis in general a partial response or above (PR or abovewhen using WHO criteria) with more than 20% …’’ foran early phase II study, and this statement has causedmany sponsors to mistakenly equate oncology drugapproval in Japan with a 20% response rate. However,
this is an erroneous assumption. To think that evaluationof a new anticancer treatment can be reduced to a singlenumerical value is a naı̈ve oversimplification. On thecontrary, final decisions regarding approvability of adrug are complex and require an integrated assessmentof many issues (Table 3).
Since Japanese oncology drug approvals for cytotoxicdrugs are based on tumor shrinkage, it is critical to assurethe reliability of these data. To that end, the responsiblemedical reviewers personally review all source data(radiographic material including X-ray and CT/MRIfilms, endoscopic records, ultrasonographic records,etc.). PMDEC and sponsor representatives then meet todiscuss discrepancies between the reviewer’s evaluationand the sponsor’s evaluation. Although the regulationsallow instances of significant remaining unresolved dis-crepancies in these individual response determinations tobe discussed before the PAFSC after this meeting, to datethere have been no instances in which the PAFSC hasbeen asked to do so.
At present sponsors are not required to use ResponseEvaluation Criteria in Solid Tumors (RECIST) [11,12] instudy protocols, but it is advised that sponsors adoptRECIST’s underlying concepts, especially in regard tomeasurability of tumor lesions. The choice of tumorimaging modalities must also be given careful consider-ation and must be clearly specified in the protocol.
Great emphasis has been placed in this section onresponse rates, because that is the efficacy endpoint thatis used most often in making approval decisions. Histor-ically, Japan has not approved drugs for oncologyindications based solely on relief of symptoms.
Sponsors, investigators, and patients can obtainPMDEC’s review reports (parts of which are masked forconfidentiality reasons), the sponsor’s overall summary,and other review-related documents from the Internet(http://www.pharmasys.gr.jp/shinyaku/shinyaku– index.html) and can see PMDEC’s current thinking about drugdevelopment or approval standards.
One of the characteristic features of Japanese oncologypractice is the widespread use of oral fluoropyrim-
Table 2Division of responsibility among the Japanese regulatory agencies regarding new drug application review, and reviews of applications forreexamination and for reevaluation
PMSB Evaluation and Licensing Division PMDEC OPSR
Reviews NDAIntegrates PMDEC review for final recommendation Reviews initial protocol notificationFollows ongoingCoordinates international affairs Conducts clinical trial consultationregistration-Directed trials
Formulates regulatory policy Conducts overseas GCP inspections Conducts domestic GCP inspectionsFollows post-marketing trials Conducts compliance reviewsReviews applications forReexaminationReviews applications forReevaluation

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155150
Table 3Points to consider in the review process of phase II studies of cytotoxic oncology drugs
What is the target population?In principle a clinical trial should be conducted using a homogeneous population of previously treated patients when standard
chemotherapy is available (e.g. certain leukemias and malignant lymphomas, small-cell lung cancer, ovarian cancer, testicular cancer andbreast cancer). However, the approved indication is not necessarily restricted to previously treated patients even when the NDA wasbased on phase II studies in previously treated patients
What is the meaning of the calculated value of response rate?The response rate must be interpreted carefully, taking into account the characteristics of the enrolled patients, especially the extent and
nature of the previous treatment and performance statusIs the safety profile appropriate?What is the state of the art of treatment regarding the concerned disease type?
idine derivatives [13]. When an investigational drug is achemical derivative of an already approved drug (mean-ing that the two drugs are structurally related), thesponsor is required to clearly demonstrate superiority(in efficacy or other characteristics) to the approveddrug in the late phase II setting by a randomizedcomparative study conducted in accordance with theaforementioned guideline [8].
4. Post-marketing evaluation system
4.1. Drug reexamination (Sai-shinsa) system(post-appro�al phase III study)
Data submitted for approval is of necessity limited inquantity, because a relatively small number of patients(e.g. on the order of 100–200 in case of oncologydrugs) are enrolled in the preapproval clinical trials,and interpatient variability is restricted by protocoleligibility criteria. Therefore, it is possible that unantic-ipated or new adverse drug reactions may be observedpostapproval, or that previously unknown effects maybe noted in specific patient subgroups, such as theelderly and pediatric populations. To address theseconcerns, Japan has instituted two systems for assessingthe safety and efficacy of drugs in a wider postmarket-ing setting.
The first system, called the Reexamination System,was established in order to provide a safety and efficacyreview based on large-scale marketing experience,rather than on controlled, highly limited clinical trialsexperience. Specifically, under its provisions, the initialapproval of a drug is considered to be tentative only,and subject to a subsequent review of efficacy andsafety at a specified future time point. This secondreview is based on investigations conducted by thesponsor over a 4–10-year-period following initial ap-proval and introduction into the marketplace (i.e. dur-ing ‘Period of Reexamination’. The law and thenotification specifies that the period of reexaminationshould be ‘‘4 years for supplemental NDA approvals, 6years for most drugs when they are approved for the
first time in Japan, and 10 years for orphan drugs’’[14,15]. Based on the outcome of this second review,three possible actions may be taken [16]:
(i) the initial approval may be canceled.(ii) Modifications to the initially approved items (e.g.
indications or dosing recommendations) may berequired.
(iii) No action will be required.In principle, regardless of the action taken at the time
of the reexamination, further reevaluation of a drugmay be requested (see below).
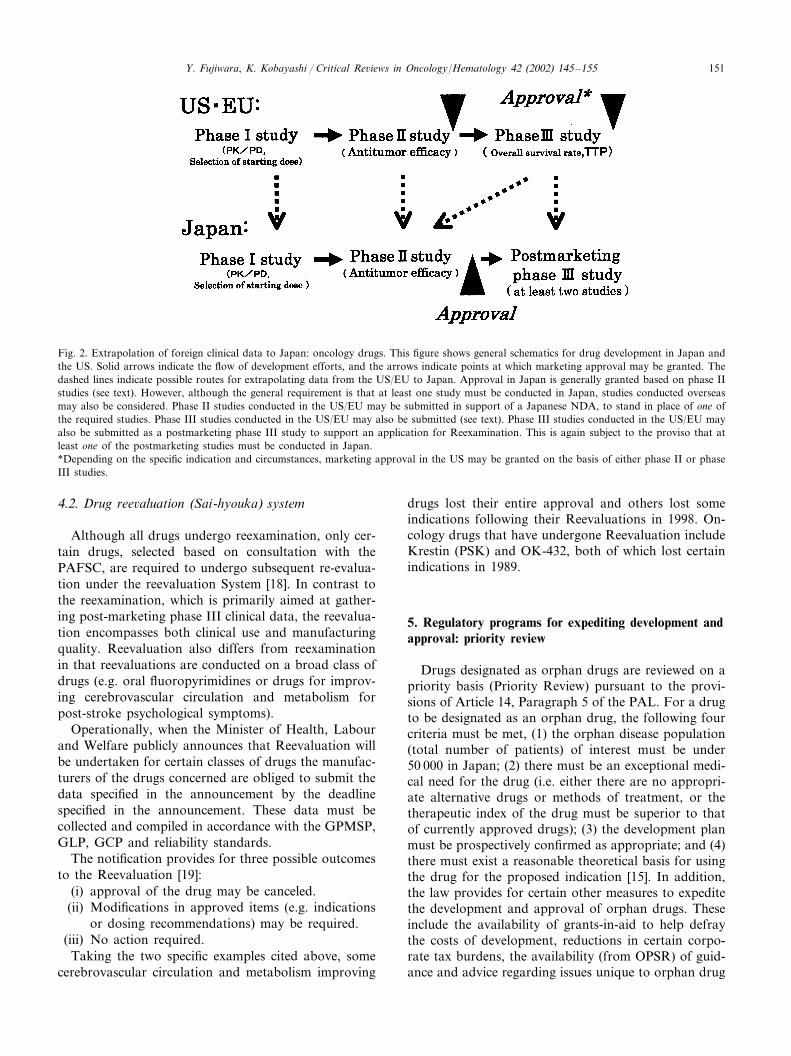
For oncology drugs, the sponsor is required to sub-mit the study plan for post-approval phase III study(e.g. a concept sheet) prior to approval. Since oncologydrugs in Japan are usually approved based on theresults of phase II studies (Fig. 2), at least two indepen-dently-conducted randomized comparative phase IIIstudies, with survival as an endpoint, are required inthe post-marketing setting [8]. It is strongly recom-mended that these studies be completed and the resultsbe submitted along with the application for reexamina-tion. The concerned phase III studies can be conductedeither by monotherapy or combination therapy. Asnoted previously in the case of phase II studies, thestudy designs need not be identical. Furthermore, con-siderable latitude is allowed in the specific details ofstudy design, as long as comparability of the expectedoutcomes can be maintained. In addition, the targetpopulations for the two phase III studies need not beidentical; for instance, if a drug is approved for morethan two indications, the sponsor may conduct twoindependent studies targeting two different diseaseindications.
As a result of the implementation of the ICH-E5guideline (Guidance on ethnic factors in the acceptabil-ity of foreign clinical data) in 1998 [17], the priorrequirement that both studies be conducted in Japanwas modified, however, sponsors are now required toconduct at least one post-approval phase III study inJapan. In other words, it is acceptable that one of thetwo prerequisite post-marketing phase III study beconducted overseas.
Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155 151
Fig. 2. Extrapolation of foreign clinical data to Japan: oncology drugs. This figure shows general schematics for drug development in Japan andthe US. Solid arrows indicate the flow of development efforts, and the arrows indicate points at which marketing approval may be granted. Thedashed lines indicate possible routes for extrapolating data from the US/EU to Japan. Approval in Japan is generally granted based on phase IIstudies (see text). However, although the general requirement is that at least one study must be conducted in Japan, studies conducted overseasmay also be considered. Phase II studies conducted in the US/EU may be submitted in support of a Japanese NDA, to stand in place of one ofthe required studies. Phase III studies conducted in the US/EU may also be submitted (see text). Phase III studies conducted in the US/EU mayalso be submitted as a postmarketing phase III study to support an application for Reexamination. This is again subject to the proviso that atleast one of the postmarketing studies must be conducted in Japan.*Depending on the specific indication and circumstances, marketing approval in the US may be granted on the basis of either phase II or phaseIII studies.
4.2. Drug ree�aluation (Sai-hyouka) system
Although all drugs undergo reexamination, only cer-tain drugs, selected based on consultation with thePAFSC, are required to undergo subsequent re-evalua-tion under the reevaluation System [18]. In contrast tothe reexamination, which is primarily aimed at gather-ing post-marketing phase III clinical data, the reevalua-tion encompasses both clinical use and manufacturingquality. Reevaluation also differs from reexaminationin that reevaluations are conducted on a broad class ofdrugs (e.g. oral fluoropyrimidines or drugs for improv-ing cerebrovascular circulation and metabolism forpost-stroke psychological symptoms).
Operationally, when the Minister of Health, Labourand Welfare publicly announces that Reevaluation willbe undertaken for certain classes of drugs the manufac-turers of the drugs concerned are obliged to submit thedata specified in the announcement by the deadlinespecified in the announcement. These data must becollected and compiled in accordance with the GPMSP,GLP, GCP and reliability standards.
The notification provides for three possible outcomesto the Reevaluation [19]:
(i) approval of the drug may be canceled.(ii) Modifications in approved items (e.g. indications
or dosing recommendations) may be required.(iii) No action required.
Taking the two specific examples cited above, somecerebrovascular circulation and metabolism improving
drugs lost their entire approval and others lost someindications following their Reevaluations in 1998. On-cology drugs that have undergone Reevaluation includeKrestin (PSK) and OK-432, both of which lost certainindications in 1989.
5. Regulatory programs for expediting development andapproval: priority review
Drugs designated as orphan drugs are reviewed on apriority basis (Priority Review) pursuant to the provi-sions of Article 14, Paragraph 5 of the PAL. For a drugto be designated as an orphan drug, the following fourcriteria must be met, (1) the orphan disease population(total number of patients) of interest must be under50 000 in Japan; (2) there must be an exceptional medi-cal need for the drug (i.e. either there are no appropri-ate alternative drugs or methods of treatment, or thetherapeutic index of the drug must be superior to thatof currently approved drugs); (3) the development planmust be prospectively confirmed as appropriate; and (4)there must exist a reasonable theoretical basis for usingthe drug for the proposed indication [15]. In addition,the law provides for certain other measures to expeditethe development and approval of orphan drugs. Theseinclude the availability of grants-in-aid to help defraythe costs of development, reductions in certain corpo-rate tax burdens, the availability (from OPSR) of guid-ance and advice regarding issues unique to orphan drug

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155152
development, and extensions of the reexaminationperiod.
In addition to orphan drug status, there is anotherroute for expediting approval of important drugs. Thisis the Priority Review mechanism [20]. Drugs meetingboth of the following requirements are eligible forPriority Review, (1) the indicated disease is severe; and(2) the drug under consideration has a therapeuticindex for the proposed indication that is clearly supe-rior to that of already approved drugs. An Applica-tion for Priority Review must be accompanied bydocuments demonstrating that the drug satisfies bothof the aforementioned two requirements. This Applica-tion must be submitted together with the Applicationfor New Drug Approval. Decisions regarding PriorityReview are made soon after the MHLW receives theapplication, and the decision is promptly communi-cated to the sponsor. At the time of approval, drugsapproved on a priority basis are noted as such inMHLW’s publicly available documents. To date, 11drugs have been approved on a priority basis in theoncology field. Ten received priority review by virtueof being designated an orphan drug. Only one drug[S-1, a combination oral agent for gastric cancer con-sisting of ftorafur, CDHP (5-chloro-2,4-dihydropyrim-idine, a DPD inhibitor), and oxonic acid (a mucosalprotective agent)] received priority review without alsobeing an orphan drug.
6. Off-label usage
For many years, off-label usage of prescriptiondrugs has been a serious problem in Japan [2,13]. On1 February 1999, an official notification describingprocedures for approval of off-label usages was issuedjointly by the Evaluation and Licensing Division,PMSB, and by the Research and Development Divi-sion, Health Policy Bureau [21]. This rule is intendedto apply to drugs for which there is a very large bodyof accumulated experience and clinical research in theproposed off-label indication.
Applications for approval to the off-labeled indica-tions and dosage are officially included in the categoryof applications for a partial change (‘Ichi-hen’) in ap-proved items (indication and dosage). Such applica-tions may be based on two different classes ofevidence.
6.1. Non-sponsor-initiated
In cases where there is a formal petition from anacademic society to consider an approval of off-labelindication AND a recognized medical necessity forsuch a use, the Research and Development Divisionwill encourage the company (sponsor) to consider pur-
suing a clinical development strategy for expansion ofthe already approved indications(s). In this case,prospectively-planned clinical trials may be necessary,and the merits of application will be evaluated basedon the outcomes of those studies. However, in certaincases, an alternative mechanism (see next section) isalso available.
6.2. Sponsor-initiated
When there is general recognition in the medicaland pharmaceutical communities that an off-labelusage is safe and effective (as defined below), it ispossible that literature-based applications, using al-ready existing studies, may suffice. In this case, consul-tation with the Evaluation and Licensing Division ofPMSB prior to submitting an application is advised.
The three situations in which the above-mentionedgeneral recognition of safety and effectiveness can beapplied are as follows.
6.2.1. Prior appro�al o�erseas and clinical useexperience o�erseas
(a) The proposed indication has already been ap-proved in a foreign country which has a drug ap-proval system (or its equivalent) that is recognized byMHLW to based on the same level of standards asJapan (e.g. the US and EU); (b) a sizable body ofdata from use in clinical practice has been accumu-lated in the country(ies) where approval has been ob-tained; and (c) the material submitted to the overseasapproving authority must be submitted to Japan (con-sistent with Japanese government requirement).
6.2.2. Preexisting o�erseas appro�al, clinical useexperience o�erseas, and publicly a�ailable clinicalresearch data
Cases in which overseas approval (according to theconditions previously stipulated) has been obtained, asizable body of data from use in clinical practice hasbeen accumulated, AND reliable results from clinicaltrials conducted by internationally-recognized clinicalresearch organizations have been published in rep-utable peer-reviewed journals. To meet this standard,such results should be of high scientific quality (e.g.high-level data as understood by evidence-based stan-dards).
6.2.3. Publicly-sponsored researchCases in which there exist scientifically reliable data
from studies conducted under the auspices of a pub-licly sponsored (e.g. Japanese governmental) organiza-tion. To meet this standard, such studies must havebeen conducted in accordance with currently acceptedinternational ethical standards.
Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155 153
Using this mechanism, two applications for partialchange in approved items have been approved in theoncology field: cisplatin for small cell lung cancer andosteosarcoma (approved, 21 December 1999), and car-boplatin for non-small cell lung cancer (approved, 27July 2000). Cisplatin had been marketed in Japan for 16years, and carboplatin for 10 years, prior to theirrespective approvals for the previously off-label indica-tions and dosages.
7. ICH E5
As of 1 December 2001, following implementation ofthe ICH-E5 guideline in 1998 [17], only one oncologydrug (anastrozole, approved 22 December 2000) hasbeen approved with a prospectively conceptualizedbridging strategy during clinical development. How-ever, it is likely that more oncology drugs will bedeveloped based on such strategies in the near future.In fact, several such proposals have been received bythe Japanese government. In addition to the examplementioned earlier (cf. Drug Reexamination System) ofa potential strategy for incorporating preexisting over-seas data into late-stage development in Japan, thefollowing scenarios are also possible (Fig. 2):1. If overseas Phase I study results are available,
starting dose estimation for Japanese Phase I stud-ies may be based on the overseas experience.Therefore, an abbreviated phase I study in Japanmay begin at a dose level that is below the MTD(as determined overseas) but above the overseasstarting dose.
2. Overseas phase II data from studies using the newdrug as a single agent may be substituted for oneof the two required late phase II studies. In thiscase, the other supporting Japanese phase II study(ies) must have been conducted in an acceptablemanner (in particular, sample size must have beensufficiently large) and the dose, route, and sched-ule of the overseas study should be the same asthose used in the Japanese study (ies). When thereis a difference between the doses used in the over-seas study and in the Japanese studies, the spon-sor must be able to demonstrate that thedifference in dosing will not result in a differencein clinical effect. Data to support such an asser-tion should be based on comparisons of the re-sults from appropriately designed andwell-conducted PK/PD studies conducted in cancerpatients both in Japan and elsewhere (countriesthose participate in ICH). These studies should besufficiently large that potential ethnic differencescan be meaningfully evaluated. Of note, however,PK studies must be conducted in Japanese sub-
jects, but may be undertaken at sites either inJapan or abroad [17].
3. Overseas phase III comparative study results mayprovide data regarding the safety of chronic dos-ing (e.g. studies of hormonal agents or of adjuvanttherapy) in the preapproval setting. In this setting,though, careful consideration should be given tothe potential impact upon the study outcomes(and the ability to extrapolate these results toJapan) of extrinsic factors, such as variation intreatment patterns, standards of care, etc. Thus,care should be taken when data from postmarket-ing phase III study results are used, as mentionedearlier.
8. Impact of reforms
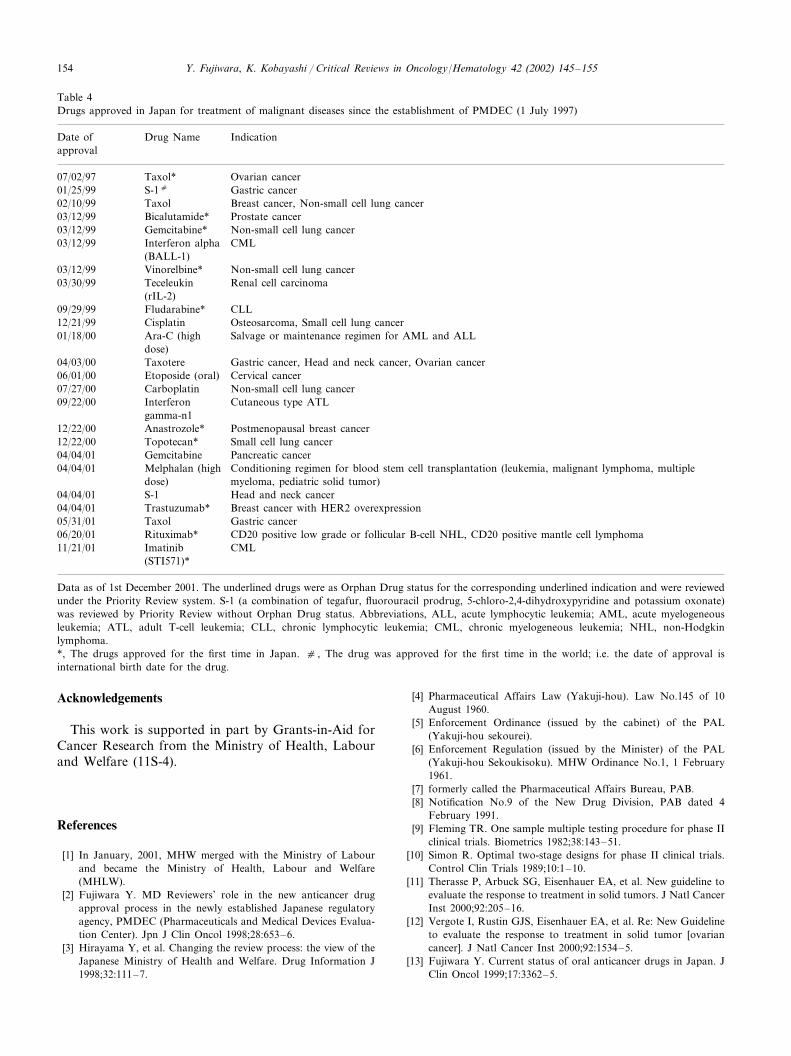
Between January 1993 and June 1997, 17 NDAs,including supplemental ones for primary therapeuticanticancer agents, were received. As of 1 December2001, 15 of these were approved by MHLW in amedian of 36.9 months (range, 19.3–77.0). Since theestablishment of PMDEC in July 1997 until 1 Decem-ber 2001, 34 NDAs for primary therapeutic anticanceragents were received. Sixteen of these were approved(as of 1 December 2001) in a median of 14.5 months(range, 3.9–26.5) (Table 4).
9. Conclusion
After the establishment of the PMDEC in 1997 andnumerous other changes, including those cited in thispaper, in the drug development and approval process,the speed of review for oncology drugs has greatlyimproved. At PMDEC, our sustaining motto is ‘‘Makegood drugs available more rapidly. Base approval on ademonstration of patient benefit that is commensurableto the probable risk. Make the review processtransparent’’.
Reviewers
Dr Francesco Pignatti, Evaluation of Medicines forHuman Use, The European Agency for the Evaluationof Medicinal Products, 7 Wetferry Circus, CanaryWharf, London E14 4HB, UK.
Steven Hirschfeld, Division of Oncology Drug Prod-ucts, Center for Drug Evaluation and Research, Foodand Drug Administration, Rockville, MD 20852, USA.
Charles A. Coltman Jr., Cancer Therapy ResearchCenter, 8122 Datapint Dr., Ste. 600, San Antonio, TX78229-3219.
Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155154
Table 4Drugs approved in Japan for treatment of malignant diseases since the establishment of PMDEC (1 July 1997)
Date of Drug Name Indicationapproval
07/02/97 Ovarian cancerTaxol*01/25/99 S-1c Gastric cancer
Breast cancer, Non-small cell lung cancerTaxol02/10/99Bicalutamide*03/12/99 Prostate cancerGemcitabine*03/12/99 Non-small cell lung cancerInterferon alpha CML03/12/99(BALL-1)Vinorelbine*03/12/99 Non-small cell lung cancerTeceleukin Renal cell carcinoma03/30/99(rIL-2)
09/29/99 Fludarabine* CLLCisplatin12/21/99 Osteosarcoma, Small cell lung cancerAra-C (high Salvage or maintenance regimen for AML and ALL01/18/00dose)
04/03/00 Gastric cancer, Head and neck cancer, Ovarian cancerTaxotereCervical cancerEtoposide (oral)06/01/00
Carboplatin07/27/00 Non-small cell lung cancerInterferon09/22/00 Cutaneous type ATLgamma-n1
12/22/00 Postmenopausal breast cancerAnastrozole*Topotecan*12/22/00 Small cell lung cancer
Pancreatic cancerGemcitabine04/04/01Melphalan (high04/04/01 Conditioning regimen for blood stem cell transplantation (leukemia, malignant lymphoma, multiple
myeloma, pediatric solid tumor)dose)04/04/01 Head and neck cancerS-1
Breast cancer with HER2 overexpressionTrastuzumab*04/04/01Taxol05/31/01 Gastric cancer
06/20/01 Rituximab* CD20 positive low grade or follicular B-cell NHL, CD20 positive mantle cell lymphomaImatinib CML11/21/01(STI571)*
Data as of 1st December 2001. The underlined drugs were as Orphan Drug status for the corresponding underlined indication and were reviewedunder the Priority Review system. S-1 (a combination of tegafur, fluorouracil prodrug, 5-chloro-2,4-dihydroxypyridine and potassium oxonate)was reviewed by Priority Review without Orphan Drug status. Abbreviations, ALL, acute lymphocytic leukemia; AML, acute myelogeneousleukemia; ATL, adult T-cell leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myelogeneous leukemia; NHL, non-Hodgkinlymphoma.*, The drugs approved for the first time in Japan. c , The drug was approved for the first time in the world; i.e. the date of approval isinternational birth date for the drug.
Acknowledgements
This work is supported in part by Grants-in-Aid forCancer Research from the Ministry of Health, Labourand Welfare (11S-4).
References
[1] In January, 2001, MHW merged with the Ministry of Labourand became the Ministry of Health, Labour and Welfare(MHLW).
[2] Fujiwara Y. MD Reviewers’ role in the new anticancer drugapproval process in the newly established Japanese regulatoryagency, PMDEC (Pharmaceuticals and Medical Devices Evalua-tion Center). Jpn J Clin Oncol 1998;28:653–6.
[3] Hirayama Y, et al. Changing the review process: the view of theJapanese Ministry of Health and Welfare. Drug Information J1998;32:111–7.
[4] Pharmaceutical Affairs Law (Yakuji-hou). Law No.145 of 10August 1960.
[5] Enforcement Ordinance (issued by the cabinet) of the PAL(Yakuji-hou sekourei).
[6] Enforcement Regulation (issued by the Minister) of the PAL(Yakuji-hou Sekoukisoku). MHW Ordinance No.1, 1 February1961.
[7] formerly called the Pharmaceutical Affairs Bureau, PAB.[8] Notification No.9 of the New Drug Division, PAB dated 4
February 1991.[9] Fleming TR. One sample multiple testing procedure for phase II
clinical trials. Biometrics 1982;38:143–51.[10] Simon R. Optimal two-stage designs for phase II clinical trials.
Control Clin Trials 1989;10:1–10.[11] Therasse P, Arbuck SG, Eisenhauer EA, et al. New guideline to
evaluate the response to treatment in solid tumors. J Natl CancerInst 2000;92:205–16.
[12] Vergote I, Rustin GJS, Eisenhauer EA, et al. Re: New Guidelineto evaluate the response to treatment in solid tumor [ovariancancer]. J Natl Cancer Inst 2000;92:1534–5.
[13] Fujiwara Y. Current status of oral anticancer drugs in Japan. JClin Oncol 1999;17:3362–5.

Y. Fujiwara, K. Kobayashi / Critical Re�iews in Oncology/Hematology 42 (2002) 145–155 155
[14] Article 14-4 of the PAL.[15] Notification No.725 of the PAB dated 25 August 1993.[16] Notification No. 82 of the PAB dated 29 January 1986.[17] Notification No. 739 of PMSB dated August 11, 1998 and
Notification No.672 of Evaluation and Licensing Division,PMSB dated 11 August 1998.
[18] Article 14-5 of the PAL.[19] Notification No. 592 of the PAB dated 11 July 1987.[20] Notification No. 92, New Drug Division, PAB, dated 1 October
1993.[21] Notification No.104 of Evaluation and Licensing Division,
PMSB and Notification No.4 of Research and DevelopmentDivision, Health Policy Bureau dated 1 February 1999.
Biographies
Dr Fujiwara graduated from Hiroshima UniversitySchool of Medicine in 1984. He completed a fellowship(thoracic oncology) at the National Cancer Center Hos-pital, Tokyo. Before joining PMDEC in 1997, he was astaff scientist at National Cancer Center Research Insti-tute, and was an assistant professor of medicine atHiroshima University School of Medicine, with a re-search focus on molecular and clinical pharmacological
mechanism of anticancer drug resistance. He was avisiting fellow at Dartmouth Medical School, UICCfellow at University of Chicago Medical Center andJohns Hopkins Oncology Center, and was Japan Soci-ety for the Promotion of Science fellow at Center ofExcellence Abroad at University of Maryland CancerCenter. He has been on the Editorial Board of CancerChemotherapy and Pharmacology since 2001.
Dr Kobayashi graduated from Northwestern UniversityMedical School and subsequently trained in generalsurgery at the Medical College of Wisconsin and inter-nal medicine at Northwestern Memorial Hospital. Hecompleted a joint fellowship in medical oncology andclinical pharmacology at the University of Chicago,with a research focus on phase I and population phar-macokinetic studies of suramin. He has been a medicalofficer at the US Food and Drug Administration since1996. From 1999 to 2001, he was seconded to theMansfield Center for Pacific Affairs and spent a yearassigned to the Ministry of Health and Welfare, thePharmaceutical and Medical Devices Evaluation Cen-ter, and the Japanese National Cancer Center as aMike Mansfield Fellow.





























