Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6www.nursingoutlook.org
Oncology nurses’ experiences with prognosis-relatedcommunication with patients who have advanced cancer
Susan M. McLennon, PhD, RNa,b,*, Sue Lasiter, PhD, RNa,Wendy R. Miller, PhD, RN, CCRNa, Kathryn Amlin, BSN, RNb,
Amy R. Chamness, BAb, Paul R. Helft, MDb,c
a Indiana University School of Nursing, Indianapolis, INbCharles Warren Fairbanks Center for Medical Ethics, Indiana University Health, Indianapolis, IN
c Indiana University School of Medicine, Indianapolis, IN
a r t i c l e i n f o
Article history:Received 30 July 2012Revised 8 November 2012Accepted 2 December 2012
Keywords:Advanced cancerCommunicationOncologyPrognosis
* Corresponding author: Susan M. McLennonDr., NU W 437, Indianapolis, IN 46202.
E-mail address: [email protected] (S.M
0029-6554/$ - see front matter � 2013 Elsevihttp://dx.doi.org/10.1016/j.outlook.2012.12.00
a b s t r a c t
Background: Oncology nurses have opportunities to engage in prognosis-relatedcommunication with patients who have advanced cancer but encounterbarriers that impede the patient’s understanding of prognosis, delay transitionsto end-of-life care, and contribute to nonbeneficial treatments.Purpose: To describe nurses’ experiences with prognosis-related communicationwith patients who have advanced cancer.Method: Thematic analysis of audio-recorded interviews with oncology nurses(n ¼ 27). After data coding, themes were identified, and a thematic map wasdeveloped. Methods to ensure trustworthiness of the findings were used.Results: Six themes were identified: being in the middle, assessing the situation,barriers to prognosis communication, nurse actions, benefits of prognosisunderstanding, and negative outcomes. Nurses managed barriers throughfacilitation, collaboration, or independent actions to help patients with prog-nosis understanding.Conclusions: Shortcomings in prognosis-related communication with patients whohave advanced cancer may contribute to negative outcomes for patients andnurses. Interventions that empower nurses to engage in prognosis communi-cations are needed. Interprofessional communication skills education also maybe beneficial.
Cite this article: McLennon, S. M., Lasiter, S., Miller, W. R., Amlin, K., Chamness, A. R., & Helft, P. R. (2013,
DECEMBER). Oncology nurses’ experiences with prognosis-related communication with patients who
have advanced cancer. Nursing Outlook, 61(6), 427-436. http://dx.doi.org/10.1016/j.outlook.2012.12.001.
Patients with life-ending cancer diagnoses (i.e.,advanced cancer) often receive intensive, disease-directed treatments that are neither beneficial norconsistent with their wishes. The administration ofchemotherapy in the last month of life has continuedto increase from 9% (Emanuel et al., 2003) to 16.4%
, Assistant Professor, Indi
. McLennon).
er Inc. All rights reserved1
(Sheffield et al., 2011). The critical need to improvecare for patients with advanced cancers extendsbeyond nonbeneficial chemotherapy administrationto excessive, nonbeneficial, and potentially harmfulmedical treatments given to patients at the end of life(EOL). In a recent study of older adults dying from
ana University School of Nursing, Indiana University, 1111 Middle
.

Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6428
cancer, 61% were hospitalized and 23.7% wereadmitted to the intensive care unit within 30 days ofdeath, whereas only 55% received care in a hospice(Miesfeldt et al., 2012).
Inadequacies in oncologists’ prognosis-relatedcommunication with patients, family members, andnurses contribute to overly intensive treatment at theEOL. In an ineffective effort to enhance physiciancommunication about prognosis and EOL options,patients with advanced cancer and their physicianswere enrolled in the SUPPORT study (Study to Under-stand Prognoses and Preferences for Outcomes andRisks of Treatments), a landmark clinical trial (Connorset al., 1995). Of importance, patients who did notunderstand their prognosis overestimated their lifeexpectancy (compared with physician estimates) andwere 2.6 times more likely to choose life-extendingtreatments (Weeks et al., 1998). Mack et al. (2012)found that 90% of patients with advanced cancerreceived EOL discussions, but half took place withina month of death and occurred with physicians otherthan oncologists.
Discussions with patients who have advancedcancer and their families about prognosis and tran-sitioning from disease-directed care to comfort-focused care are not easy, but evidence suggests thatunderstanding their prognosis influences patients’decisions. Temel et al. (2011) reported that patientswithadvanced cancer who received early palliative care,compared with usual care, had greater understandingof their prognosis and were less likely to be givenchemotherapy at EOL. In another study, communica-tion skills of the health care provider influenced patientreadiness to discuss prognosis and EOL care and wereassociated with the patient’s sense of control andfeeling able to move on (Walczak et al., 2011). The needto communicate about prognosis with patients whohave advanced cancer in an understandable, accurate,and timely way cannot be underestimated.
The American Nurses Association (ANA, 2010)offered guidance for nurses about their role in EOLcare that included providing counseling and initiatingearlier EOL discussions. Nurses have more opportuni-ties to initiate EOL discussions than other health careproviders because they spend more time with patientsat theEOLandengage in advocacybehaviors to improvethe quality of EOL care (Badger, 2005; Jablonski &Wyatt,2005; Thacker, 2008). Little is known about the nature ofnurses’ roles in prognosis-related communication, andtheir role is not well defined (Bradley et al., 2000; Helft,Chamness, Terry, Uhrich, 2011; McLennon, Uhrich,Lasiter, Chamness, & Helft, 2012).
Gutierrez (2012) observed that critical care nursesmade significant contributions to prognosis communi-cations by “stepping in to fill the gaps” (p. 176) andinterpreting physician’s language. Similarly, Krimshteinet al. (2011) reported improvements in critical care nurseself-efficacy for prognosis discussions after a communi-cation skills training program. In a mailed survey ofOncology Nursing Society members, authors found that
mostnursesperceived responsibility for helpingpreparepatients for EOL but encountered barriers, frequentlydescribed as ethical dilemmas, such as physicianavoidance of prognosis-related discussions, uncertaintyabout role boundaries, and the need for further educa-tion (Helft et al., 2011; McLennon et al., 2012).
In light of the importance of prognosis-relatedcommunication to improving EOL decision-making andour own research indicating uncertainty about nursesroles’ and underlying ethical dilemmas with suchcommunication, we undertook this qualitative study toobtain a better understanding of oncology nurses’experiences with prognosis-related communication.
Methods
Design
A qualitative descriptive design and thematic analysiswas used to analyze narrative interview data (Braun &Clark, 2006; Polit & Beck, 2012). The goal of a qualitativedescriptive design is to describe the phenomenon ofinterest in a realistically representative and useful way(Sandelowski, 2000). Thematic analysis is a systematicway to analyze and present the meaning of collectiveexperiences within a social context (Braun & Clark,2006). We used an inductive, semantic, experiential,and essentialist approach to thematic analysis todescribe the nurse’s experiences. An inductive,semantic approach indicates the codes are determinedfrom the data and themes reflect the surface meaningof the data (Braun & Clark, 2012; Patton, 2001). Experi-ential refers to an approach that is essentialist andconsiders the real motivations, experiences, andmeaning of the data directly (Braun & Clark, 2012). Inthematic analysis the process moves from descriptionof the organized data, to a depiction of the pattern ofthe semantic content, to a summary that theorizes thesignificance of the patterns, their meanings, andimplications (Braun & Clark, 2012; Patton, 2001).
Procedure
After approval by the Institutional Review Board, regis-tered nurses who provided care for patients withadvanced cancerwere sought. Informational flyersweredistributed by unit managers and educators. All poten-tial participants who phoned or e-mailed the researcherwere screened for eligibility, and none were excluded.Inclusion criteria were (1) registered nurseswith at least1 year of oncology nursing experience and (2) currentlyworking in an oncology setting. Participants wereinterviewed once, and all interviews were audio-tapedand held in a private location near their work area.
Purposive sampling using both maximum variationand opportunistic sampling strategies were used torecruit a diverse group of oncology nurses withcommon experiences (Patton, 2001). The characteristics

Nur s Ou t l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6 429
of the desired oncology nurse sample were: (1) a rangeof years of experience, (2) minorities and males, (3)from rural and urban hospitals, and (4) from inpatientand outpatient oncology settings. Early in the recruit-ment process, all interested nurses (participants 1 to16) whomet the inclusion criteria were enrolled. Later,nurse managers and educators were again contactedto assist with targeted recruitment (participants 16 to27). There also were two opportunities to enrollparticipants who volunteered for the study and fit theinclusion criteria when the researcher was present fora prescheduled interview.
Study details were provided to interested nurses anda date, time, and location for the interview weredecided. Before the scheduled interview, participantswere provided an explanation that interviews wouldfocus on “prognosis-related communication” withpatients who had advanced cancer. “Prognosis-relatedcommunication” was defined as when patients refer tothe possibility of dying from cancer, hospice or pallia-tive care, hope for the future, disease trajectory andoutcomes, or estimates of life expectancy. Patientswith advanced cancer were patients with incurable,terminal, or life-ending cancer diagnoses.
At the meeting, the study was explained to theparticipants and informed consent obtained. Theinterview guide, used during all interviews, consistedof questions about nurses’ experiences with prognosis-related communication such as “Tell me about a timewhen you discussed prognosis with an advancedcancer patient,” “Tell me about a time when youwanted to discuss prognosis with a patient withadvanced cancer, but did not for some reason,” and“Tell me about a time when you had a conversationabout prognosis with a patient with advanced cancerthat you felt went especially well, or did not go well.”Probes and conversational interview techniques werealso used (Patton, 2001).
Demographic and contextual information, includingaverage number of ethical dilemmas encountered permonth and how often in the room during prognosisdiscussions, was collected last to reduce the influenceon information offered by participants during inter-views. Recruitment continued until the sample con-sisted of nurses who met the predetermined samplingcriteria, and data saturation was reached, meaning nonew information related to prognosis communicationswere noted in the transcripts (Sandelowski, 1995).A mix of redundancy and new concepts were notedduring the initial interviews. Data saturation wasachieved when no new concepts were noted deter-mined by “evaluating the quality of the informationcollected against the uses to which it will be put”Sandelowski (1995, p. 179).
Data Analysis
Data from the audio-recorded interviews, which aver-aged 36 minutes in length, were transcribed verbatim,including all spoken words and sounds, and checked
for accuracy. Three nurse researchers (S.M., S.L., W.M.)with experience in qualitative analysis took part in thethematic analysis that followed the six phases outlinedby Braun and Clark (2012). In phase 1, we familiarizedourselves with the data. Initially one researcher (S.M.)read the entire dataset of transcripts, which were thenevenly divided among the three researchers for coding.Guided by the overarching research goal “to describeoncology nurses experiences with prognosis relatedcommunication,” we read over the transcripts andthen re-read them, noting aspects of interest. In phase2, each researcher generated a list of codes, defined asphrases or words obtained from the data that reflecta basic element of the phenomenon (Boyatzis, 1998;Braun & Clark, 2006). As coding proceeded, additionalresearch questions were generated, discussed, andagreed upon as important features of the mainresearch question (Braun & Clark, 2012). Examples ofthese questions were as follows:
“What were the barriers encountered by thenurses?”
“How did they manage difficult situations related toprognosis discussions?”
“What were the outcomes of their actions, orinactions?”
Each researcher used a computer software programto record the extracted chunks of data and associatedcodes. We then combined our code lists into onedocument and compared and discussed the codes,noting overlap and duplications, until consensus wasreached on a final list of unique codes. Each codeincluded a label and a description of qualifications orexclusions (Boyatzis, 1998; Braun & Clark, 2006). Inphase 3, related codes were sorted, grouped, andlabeled as preliminary themes by drawing compari-sons across the data. This process was first performedindividually and, later, results were compared asa group until consensus was reached. A theme wasdefined as capturing something significant or note-worthy in the data related to nurses’ experiences,determined by prevalence in the data or whether itcaptured an important aspect relative to the researchgoal (Braun & Clark, 2012). After the completion ofthese steps, we developed a thematic map (Boyatzis,1998; Braun & Clark, 2006).
In phase 4, to check for quality, the themes were re-reviewed in relation to the coded data and to the entiredataset. This process revealed that some themeslacked conceptual clarity and were related to commu-nications around EOL issues as well as prognosisdiscussions. The full dataset was then reduced toa subset specific to nurses’ experiences with prognosiscommunications. Coding was again performed,yielding many of the previous codes and some newcodes. In phase 5, this process was repeated iterativelyuntil a final code list was agreed upon, themes were

Table 1 e Sample Demographics
Characteristic(n ¼ 27)
Range Mean/n SD/%
Experience as RN, y 2e34 11.98 10.04Experience in oncology, y 2e25 8.67 6.58Ethical conflict (timesper month)
0e6 1.68 1.54
Age, y21e31 8 29.6332e41 5 18.5242e51 9 33.3352e61 5 18.52
SexFemale 25 92.60Male 2 7.40
RaceWhite or Caucasian 24 88.88African American 1 3.70Hispanic or Latino 1 3.70Asian 1 3.70
Education (nursing)Master’s degree 0 0Bachelor’s degree 22 81.48Associate’s degree 4 14.81Diploma program 1 3.70
Present during prognosisdiscussionsRarely 3 11.11Sometimes 11 40.74
Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6430
identified and named, and a final thematic map wasdeveloped. Each theme and subtheme describeda unique aspect of the data, themes were directlyrelated to the research goal, and together offered anoverall picture of the nurses’ experiences with prog-nosis discussions (Braun & Clark, 2012).
Credibility, transferability, dependability, andconfirmability refer to criteria to evaluate the trust-worthiness of the findings in qualitative research(Lincoln & Guba, 1985). Regarding credibility, we usedmember checks, independent analysis by more thanone researcher, and verbatim quotes. Transferabilitywas supported by using purposive sampling methodsand preset criteria to obtain a heterogeneous sample,providing detailed demographic and backgroundinformation, and a complete description of the inter-view process and tools. For dependability, researcherskept audit trails to account for the processes used ineach phase of analysis. Analytical methods were clear,logical, and outlined in the Methods section. Confirm-ability was maintained by providing the audit trail tothe other reviewers and final results were reviewed byclinician experts (P.H., K.A.). Demographic data wereanalyzed with descriptive statistical analyses(frequencies, percentages, means, SD, and ranges)using statistical software IBM SPSS Statistics-Version19. The sixth phase, reporting the results, follows next.
Most of the time 11 40.74All of the time 2 7.41
Adult oncology settingInpatient 18 67.0Bone marrow 6 22.0
Results
transplantationOutpatient clinics 3 11.0
Note. RN, registered nurse.
Sample
The sample consisted of both female (n ¼ 25) and male(n ¼ 2) oncology nurses with a range of years of expe-rience (M ¼ 8.67; SD ¼ 6.58) who were employed inseven adult oncology hospital units within an urbanacademic medical center or one of three affiliatedregional hospitals in a Midwestern region. Of the 27nurses, 18 were employed in four different inpatientoncology units, six were from a bone marrow trans-plant unit, three from outpatient clinics, and providedcare in rural and urban hospitals (see Table 1 fordemographics).
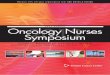
Ninety-six codes were grouped into six mainthemes: the contextual environmentdbeing in themiddle, assessing the situation, barriers to prognosiscommunication, nurse actions, benefits of prognosisunderstanding, and negative outcomes. A thematicmap (see Figure 1) depicts the themes and subthemes.
Contextual Environment: Being in the Middle
The overarching theme from the nurses’ narrativeswas the sense of “being in the middle” between thephysician and patient/family and formed the contex-tual environment for the nurses’ experiences withprognosis-related discussions. Sometimes “being inthe middle” was an advantageous position from which
the nurses advocated for patients with the physiciansto clarify prognoses and plans of care. One nurseexplained advocacy saying, “Nurses have a big role inbeing able to talk to the doctors and say, ‘what’s theplan of care’? Oncology patients. need advocates.they get to know, are they at the end of their rope?”
At other times nurses felt “stuck in the middle,” notknowing the patient’s prognosis, their own role inprognosis discussions, or whether communicationabout prognosis took place. Caring for a patient whoseprognosis was unknownwas typical in the nurses’ day-to-day work environment and represented the experi-ences of several nurses. “We just feel like we’re left outof the loop, yet we’re having to deal with the patients,families, and they will quite frankly ask us, do we thinkthe patient’s going to survive.so we feel like we’restuck.” The following sections include nurses’ methodsfor assessing the situationdrecognizing the need forprognosis discussions, gathering additional informa-tion, and reflecting. They described barriers toprognosis-related communication and strategies fornegotiating the barriers. When barriers were notovercome, prognosis discussions were overlooked,causing moral distress.

•
Figure 1 e Nurses’ experiences with prognosis communication
Nur s Ou t l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6 431
Assessing the SituationStudy nurses explained the process of how they iden-tified the need for prognosis discussiondby recog-nizing patient cues and knowing when it was time,gathering additional information to gain a betterunderstanding of the full picture, and reflecting onrisks and benefits.
Recognizing ReadinessPatients indicated readiness for prognosis informationor for transitioning from a focus on disease-directedtreatment to comfort care in different ways. Nursesdescribed cues used to time the initiation of prognosis-related communication. One nurse said, “I don’t bringit up until I see a cue from them, like ‘am I going to getbetter from this’?” Sometimes patients simply asked“howmuch time do I have?” In other situations, nursesdescribed oblique references such as “The person willsay to you, ‘you know, I really need some new tennisshoes but I just wonder should I invest in them, youknow, they’re not going to do me any good in a fewmonths’.” Nurses recognized subtle signs anddescribed them as intuitive knowing:
I think when their determination to fight the illnessstarts lagging.and they know they’re not gettingbetter. I think theycometoapoint, a crossroad,whereyoucan just tell. It’s likethe, the little light intheireyesgoes away, their smile, I’m not smiling on the inside,I’mmiserable on the inside and no one is listening tome kind of thing so.emotionally, physically.
Gaining InsightSeveral nurses described methods they used such asfurther assessment or just listening to gather moreinformation about a specific patient or family
situation. Often their initial response was to deter-mine what the patient already understood. “I find itvery helpful to ask my patients what their physicianhas told them about their prognosis before answeringtheir questions.” Another nurse found “all informationpossible and then ask the patient what they under-stand.” It was important to listen to the patient’sresponses and one nurse offered this advice: “Youreally have to be a good listener. That will tell youmore than enough” and “They’ll tell you, you just haveto listen to what they’re saying and take it fromthere.”
Patient characteristics such as educational level,spirituality, and cultural beliefs determined individualneeds. One nurse described assessing for a patient’sability to understand and level of education, “In thefirst few minutes, I gauge how to converse with them.They might be a person who’s not very well educa-ted.and then I just sort of try to, make it so that wecan connect somehow?” Several of the nurses relatedstories of cultural or religious beliefs that impactedprognosis-related communication. A nurse recalleda situation in which a patient’s angry wife said “shedidn’t think we understood her religion, that oneperson did not make a decision, and she consulted allthe different family members.”
ReflectingIn many cases the nurses deliberated, weighing themajor issues; they wondered about the extent ofinformation that should be given and the potential forinflicting additional pain or removing hope. Many ofthe nurses described situations of caring for patientsthat they knew or suspected didn’t want to continuewith cancer treatments and then weighed the optionsfor or against intervening. In this example a nursereflected:

Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6432
Sometimes I wondered if the patient didn’t feel likethey would let down the doctor if they told him, ‘Idon’t want to do this anymore’.and I’m feeling like‘you know, you don’t have to do this.’ And in reality,I potentially would be doing him a favor, you know,by offering the other side, but also feeling like, is thatbeing negative?
Another nurse reflected on taking away hope andwhether it was the right action to take.
I don’t want to stop them fromhaving hope, and so, Idon’t know if that’s right or wrong, I mean, becauseif I have to I can just come right out and say, but I’mtrying to balance what they need, and a lot of timesit is never the right time.
After gaining a better understanding of the mainissues, nurses often encountered barriers thatimpacted whether prognosis-related communicationcould take place. These additional factors groupedtogether to create the theme “barriers to prognosiscommunication.”
Barriers to Prognosis Communication
Most of the oncology nurses described one or morebarriers that were encountered when patients indi-cated readiness for prognosis related information.Barriers were grouped into four subthemes: uncer-tainty, discomfort, disconnect, and perceived risk.
UncertaintyWhen patients asked about their prognosis, nursesdescribed being unclear about what to say because ofa lack of knowledge, education, or the perceived needfor “secret keeping.” One relatively new nurse said, “Idon’t feel like I know enough, I’ve had two years’experience, but I’m terrified that they’re going to startasking me questions I can’t answer. I would just feelhorrible if I told them the wrong information.” Incontrast, an experienced nurse said, “What you don’trealize.working in this setting, it’s not always abouta cure. Sometimes it’s about hope and sometimes it’sabout hitting milestones.” This quote is an example ofhow several nurses would respond when asked bya patient ‘do you think I’m going to live?’ It reflectsoverlap of the subthemes of uncertainty and discom-fort, “she talked to me about, and I hate those kinds ofquestions because I don’t know, I can’t predict thefuture, it was hard to talk to her about that and I woulddeflect, try to talk about something else.” Severalnurses felt ethically conflicted in circumstances inwhich they had knowledge about the patient’s prog-nosis and were uncertain about disclosing that infor-mation to the patient, “It feels like you’re keepinga secret.the doctors aren’t saying, and there you arein the room as a nurse, what do you do with.thosedynamics?”
DiscomfortFor some nurses, personal feelings of distress andsadness about the topic blocked prognosis-relatedcommunication. They preferred not to speak aboutimminent death or “be the bad guy. I just hate givingbad news, I really do, so, in all honesty a lot times Iavoid it.” Several nurses explained “I feel like we needto be honest with them so they can get their life inorder.but then I don’t want to be the one to do it.”Some nurses worried about patients’ reactions, “it’sjust so sad, I don’t want to see her cry,” and werehesitant to potentially influence a patient’s decision. “Iguess I don’t want them tomake a decision based uponan opinion dmy opinion.” This nurse told a story thatexemplifies the theme of discomfort.
She was young, maybe 21, some sort of advancedcancer, when they diagnosed her and I had herthe day before she was discharged, the day thedoctors came in and told everybody that it wasinoperable and that she had like months, evenweeks to live, and there was nothing she could do.I had her that day and it was really hard, I keptthinking ‘I don’t want to go in the room, I don’twant to look at her, I don’t want to’.it was justa weird conflict, but somebody that young, younever really got a chance to do anything, it wasunfair and sad, and that’s probably why, why Iwas so uncomfortable.
DisconnectA number of nurses commented about communicationgaps between the physician, nurse, and patient aroundprognosis-related information and treatment goals.The term disconnect was described as nurses andphysicians working tangentially, in contact but notintersecting, rather than in tandem. A disconnect, orgap, between the physician and nurse resulted fromdifferent ways of caring for and evaluating patients.“Sometimes the families have false hope. I think it’sjust a disconnect between physicians and their plan ofaction and what their thinking is.compared tonursing and their experience with the patients. Wedon’t have a close enough connection with physi-cians.” Disconnect also was reflected in situations inwhich nurses explained not knowing the informationthat had been disclosed to the patient, “I think some-times I’m afraid to bring it up just because I don’t knowhow much they know,” and by this statement,“Sometimes I don’t even know when they’re in theroom. So if they would just tell that they’re going inthere, then I could be with them and understand whatthe whole plan is.”
Disconnect was noted when physicians did notdiscuss prognosis and nurses were willing but unableto do so. “Oncologists don’t like to tell people they aredying. Nurses are more likely to discuss it but its hardwhen you’re the only one talking about it and theirdoctor, who is determining their treatment, is notwilling or not accepting.”

Nur s Ou t l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6 433
Perceived RiskPerceived risk wasmost often related to role ambiguityand the potential for negative consequences, primarilyfrom physicians, and impeded nurse willingness todiscuss prognosis and related information withpatients or families. “I worry if I will be oversteppingmy boundaries by telling them something he has notdiscussed” and also “I guess there’s a little bit of a grayarea on how much autonomy you can have when youtalk to patients about stuff like that.” Nurses in thestudy had experienced or anticipated conflict withphysicians that restricted their willingness to partici-pate in prognosis related communication, “and thenthat unapproachable doctor I was talking about, Imean, I don’t think he would appreciate it if I told themsomething that he hadn’t already told them.”
In summary, there weremany barriers to prognosis-related communication embedded in the nurse’snarratives. Next, nurses’ actions to overcome barrierswill be described. When barriers were overcome orwere not problematic, prognosis discussions took placeand were described by nurses as experiences that“went well” meaning the patient benefited. In contrast,if barriers blocked patient prognosis understanding,patient preferences were overlooked and nursesexperienced moral distress.
Nurse Actions
Nurses engaged in prognosis-related communicationwith patients and families in three ways. Commonlythey facilitated these types of discussions; otherwise,they either teamed with physicians or independentlyproceeded with a prognosis-related discussion on theirown. At times, nurses were not able to engage inprognosis-related discussions.
FacilitatingNurses described advocacy behaviors that were used toovercome disconnect. “I think the nurses have a bigrole in being able to talk to the physicians and just ask‘what are we going to do about this?’” Sometimes theyoffered to partner with the patient or family, instructedthem about what to ask the physician, or offered to setup a meeting. “I do inquire with patients if they wouldlike a discussion with the physician regarding prog-nosis. I will also educate patients about questions theyshould ask their physicians, what symptoms and labvalues they need to focus on, etc.”
To overcome perceived risk, another nurse enlistedfamily assistance, “and I kind of told him [the son] that‘you’re just going to have to tell that doctor that youdon’t want any more done’.I don’t think that doctorwas going to listen to me.” Nurses used caution andcareful language, “I would go.and explain why I thinkthey [the patient] need to know. I would explain thenecessity and ask how could you help me take care ofthis patient?” Also, “With this particular physician, I tryto be very careful inmywording, ‘would you consider’?A nurse explained how, at times, it is not possible to
facilitate prognosis-related communication because ofpower differentials, “I think it would have been hard tosay ‘no we’re done’ when somebody in a position ofauthority is telling you that you need to keep going.”
CollaboratingStudy nurses teamed with physicians to work intandem. One nurse explained that a physician initiatedthe team approach to a prognosis conversation, “Wehave a really good relationship, so the doctor came in,and he was like, ‘let’s go talk to him and tell himeverything’.” An example of a nurse overcomingdiscomfort follows here:
I didn’t want to go in the room (laugh) but I figured,you know, I need to do it, I was a part of the medicalteam, and the person that is going to be cleaning upthe aftermath when everybody leaves the room, youneed to sort of be in there and hear what they haveto say. I was proud of myself because I had myselfface it and sit down and talk to her.
The role of the nurse in collaborating with thephysician was described as “filling in the gaps.” “I thinkthat it really helps for the nurse to be involved in thetalkwith the patient, thenwe hear it and understand it,and know what they were told.[and can] fill in thegaps.” By teaming with physicians, nurses overcomesome of the uncertainty and discomfort associatedwith not knowing what to say and giving bad news.There were a few comments from nurses aboutprognosis-related conversations that did not go well orwhen nurses were not present, “It depends on thephysician, some are very good, some it makes themnervous.they kind of jump around, don’t reallyexplain what palliative care or hospice is. A nurseshould be involved in those discussions but we getbusy.”
IndependentIn a few cases, nurses offered their own experiences ofanswering patient prognosis questions directly andmatter-of-factly, “given my experience with otherpatients in your situation.I’d say weeks-to-monthsand likely less than a year.” Sometimes nurses werehesitant to carry out prognosis-related discussions butdid so out of a sense of obligation and desire todo what was best for the patient, to tell them “whatthey needed to hear,” despite the perceived risks. Inthis instance, a nurse explained that she first spokewith the physicians prior to talking about prognosiswith the patient, “I felt a responsibility to my patientand the family to tell them that the prognosis was notgood and he probably only had a matter of days.” Inanother situation, the nurse described feelingconflicted, “I am always torndbut if I don’t open upthe conversation, the patient will continue on to deathwithout the benefit of having made a plan.” This nurseexperienced regret for not communicating honestlyabout prognosis with patients at times, “There have

Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6434
been several cases where I’m mad at myself for notbeing more honest with them when I leave at the endof the day. ‘Why did you take the chicken route andnot deal with it?’”
In summary, nurses’ contributed to prognosis-related communication by facilitating, collaborating,or acting independently to overcome communicationbarriers. Theseexamples illustrated thecomplexity andskills required to negotiate these diverse and oftenchallenging circumstances. At times, barriers blockedprognosis-related communication and led to nursemoral distress and overlooked patient preferences forEOL care, illustrated next. With improved prognosisunderstanding, nurses expressed satisfaction primarilybecause they perceived that patients’ actual prefer-ences were being respected.
Benefits of Patients’ Understanding of Their Prognosis
Nurses discussed how patients’ understanding ofprognosis, symptom management, and quality of lifewere positively impacted by transitions to palliativecare or hospice, “I’ve noticed a huge difference if we getpalliative care involved, and how early they getinvolved.” Nurses described the satisfaction of helpingpatients during a difficult time, “You feel like you’reactually making a difference. You’re helping themcope.you’re answering questions and directing themto resources that will actually help them.” Anothernurse described the benefit of palliative care:
There was a patient.in so much pain, woundseverywhere, anythingyoudidhurt her and she’d startcrying. Thenextnight [I cameback towork] therewasjust like a weight lifted off, there’s 20 people in theroom,muchbetter spirits, the patient looked somuchmorecomfortable.helpedthequalityofwhatshedidhave left. I thinkpartofmy job is tomake themrealizethat their quality of life is important.
Negative Outcomes
Nurses described more cases of negative outcomesthan positive outcomes. They witnessed patient pref-erences that were ignored or not assessed whichresulted in moral distress.
Patient Preferences OverlookedNurses perceived that patients experienced detri-mental effects from missed opportunities forprognosis-related communication such as unrealizedpatient preferences for place of death and treatmentchoices. This example demonstrates the disconnectbetween the patients’ preferences and the physiciansdirecting care, “so, I don’t know if we could have star-ted the conversation earlier, we didn’t have enoughtime, he ended up dying here, which wasn’t what theywanted.” Many nurses described stories of patientsreceiving cancer treatments that were not wanted. At
times, nurses met resistance from physicians whenexplaining patients’ preferences. “It’s difficult tocommunicate for your patient and say, ‘no, this is thedirection she wants to go’ when the doctors are saying,‘no, I’m the oncologist.we still have another round oftreatment.’ We were shut down.”
Nurse Moral DistressNurses reported experiencing ethical dilemmasprimarily related to perceived lack of full disclosureabout prognosis and treatment options. When physi-cians refused or blocked prognosis-related communi-cation, nurses felt “stuck in the middle” with no wayout. For example, “I know it’s not our place to tell themthe diagnosis but it is our place to care for them.and Idon’t think we should be keeping information likethat.” When nurses were unable to bridge thecommunication barriers to do what they thought bestfor the patient, they experienced feelings of regret,anger, and frustration. For example, this nurse’s frus-tration with a physician who refused to talk aboutprognosis with patients was expressed here, “I thought‘he’s got kids, how can he not know that this cancer isgoing to take his life?’ It makes me angry that thephysicians haven’t been upfront and honest.we’restringing them along.”
Another nurse recalled a patient she had cared forwho did not want aggressive measures, “I didn’tprepare him for what could happen and then I find outthat he ended up getting transferred [intensive care],coding and dying.it’s a very hard thing for me.”Frustration was also evident in this nurse’s story:
Pancreatic cancer with metastasis to the liver andelsewhere, she was jaundiced, glowing yellow. TheGI doctors came in and told her, ‘There’s nothingmore we can do. We want you to go home onhospice.’ Then our oncologist came in and told her,‘well we can do this chemotherapy,’ I just got soangry because, no she can’t, her liver is obliterated.It’s very frustrating because, you know, why wouldanyone listen to me, the nurse?
Discussion and Implications
Practicing oncology nurses described their experi-ences with prognosis-related communication fromtheir position of “being in the middle.” They reportedhaving the opportunity and the motivation to helppatients and families understand their health situa-tion but encountered barriers to prognosis-relatedcommunication that interfered with transitions fromdisease directed therapies to palliative and EOL care.They shared experiences with barriers, methods usedto manage them, and perceptions of how patientoutcomes were affected. Barriers often resulted inmoral distress about their perceived inability toadvocate for the patients. Despite the desire to

Nur s Ou t l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6 435
collaborate with oncologists, nurses felt excluded,discounted, and unable to obtain information neededto provide optimal patient care. Physicians and nurseshave little spare time but nurses thought that round-ing together would be more efficient particularly whenprognostic discussions and critical conversations tookplace.
Aspects of the oncology nurses’ experiences wereparticularly striking and have important implications.Participants discussed witnessing patients undergononbeneficial and unwanted treatments such aschemotherapy in very advanced disease, late or absentreferrals to palliative care and hospice, and theperceived lack of full disclosure by physicians aboutprognoses and treatment. They described working inan environment of uncertainty in which they observedgaps in care that required risk-taking to achieve posi-tive outcomes for patients and their families. Fromtheir vantage point “in the middle,” oncology nursesare poised to have a substantial impact on the qualityof care for advanced cancer patients through newinitiatives focused on care coordination, patient-centered care, and collaborative prognosis relatedcommunication (US Department of Health and HumanServices, 2011). However, it will become increasinglyimportant for nurses to ensure that roles are“measured, recognized, and fully integrated” (Lamb &Donaldson, 2011).
National priorities designed to improve clinicaloutcomes from a patient-centered perspective offerways for oncology nurses to improve the quality of carefor patients with advanced cancer. The need for orga-nized and clear communication with patients is key inmaking timely health care decisions. This is a futurepriority set out by the National Quality Strategy, USDepartment of Health and Human Services. Oncologynurses must continue to advocate on behalf of theirpatients and families to ensure that they receivequality cancer care that is consistent with their pref-erences. Research designed to clarify nurses’ rolesconcerning prognosis-related communication isurgent. Interprofessional communication skillstraining and collaborative practices (nurseephysician)may also reduce communication barriers and theassociated “disconnect.”
Oncology nurses need an institutional culture thatsupports and facilitates collaboration with physiciancolleagues, particularly when patients and familiessuggest a lack of understanding and/or a readiness toengage in prognosis related communication. In thepast, quality improvement measures and educationalefforts (Connors et al., 1995) have had limitedsuccess, creating a need for robust external pres-sures from patients and health care institutions tochange physicians’ practices. Together, the nationalimperatives to transform health care, the focus onpatient-centered care, and research and discussionto clarify nurses’ roles in prognosis-related commu-nication may provide the needed impetus forchange.
Limitations
Our goal was to attain an in-depth understanding ofthe experiences of oncology nurses and to present thefindings in a meaningful way and not to quantify thecategories and themes. Although we intentionallysought to recruit many diverse oncology nurses, wewere limited by the relatively homogeneousmakeup ofnurses from a single Midwestern region therefore,these finding may not be transferable to other pop-ulations of oncology nurses. Quotes illustrated herewere not selected to represent recommendedcommunication techniques but as exemplars of thecategories and themes.
Conclusion
Evidence from these nurses’ experiences suggests thatoncology nurses are positioned to improve the qualityof prognosis-related communication and EOL care forpatients with advanced cancer and their families byfacilitating, collaborating, or independently partici-pating in prognosis discussions. Areas in whichoncology nurses can make substantial contributionsinclude assessing the needs of the patient and family;overcoming communication barriers to facilitateunderstanding of the prognosis; opening up avenues ofcommunication about treatment options and EOLwishes between patients, families, and the health careteam; and enabling patients (or their surrogates) tomake informed choices. More research aimed atempowering oncology nurses to overcome the barriersthey face in aiding patients and families during crucialEOL transitions is needed.
Acknowledgments
Research supported, in part, by the Walther CancerFoundation, Inc., Indianapolis, IN (to S.M.M., A.R.C.,and P.R.H.).
r e f e r e n c e s
American Nurses Association. (2010). Position statement:Registered nurses’ roles and responsibilities in providingexpert care and counseling at the end of life. Retrieved from:http://nursingworld.org/MainMenuCategories/EthicsStandards/Ethics-Position-Statements/etpain14426.pdf.
Badger, J. M. (2005). Factors that enable or complicate end-of-lifetransitions in critical care. American Journal of Critical Care,14(6), 513e521.
Boyatzis, R. E. (1998). Transforming Qualitative Information: ThematicAnalysis and Code Development. Thousand Oaks, CA: Sage.
Bradley, E. H., Fried, T. R., Kasl, S. V., Cicchetti, D. V., Johnson-Hurzeler, R., & Horwitz, S. M. (2000). Referral of terminally ill

Nur s Out l o o k 6 1 ( 2 0 1 3 ) 4 2 7e 4 3 6436
patients for hospice: Frequency and correlates. Journal ofPalliative Care, 16(4), 20e26.
Braun, V., & Clark, V. (2012). Thematic analysis. In H. Cooper (Ed.),APA Handbook of Research Methods in Psychology: Vol. 2. ResearchDesigns (pp. 57e71). Washington, DC: American PsychologicalAssociation.
Braun, V., & Clark, V. (2006). Using thematic analysis inpsychology. Qualitative Research in Psychology, 3, 77e101.
Connors, A. F., Dawson, N. V., Desbiens, N. A., Fulkerson, W. J.,Goldman, L., Knaus, W. A., ., & Ransohoff, D. (1995).A controlled trial to improve care for seriously ill hospitalizedpatients. The study to understand prognoses and preferencesfor outcomes and risks of treatments (SUPPORT). Journal of theAmerican Medical Association, 274(20), 1591e1598.
Emmanuel, E. J., Young-Xu, Y., Levinsky, N. G., Gazelle, G.,Saynina, L., & Ash, A. S. (2003). Chemotherapy use amongMedicare beneficiaries at the end of life. Annals of InternalMedicine, 138(8), 639e643.
Gutierrez, K. M. (2012). Prognostic communication of critical carenurses and physicians at the end of life. Dimensions of CriticalCare Nursing, 31(3), 170e182.
Helft, P. R., Chamness, A., Terry, C., & Ulrich, M. (2011). Oncologynurses’ attitudes toward prognosis related communication: Apilot mailed survey of Oncology Nursing Society members.Oncology Nursing Forum, 38(4), 468e474.
Jablonski, A., & Wyatt, G. K. (2005). A model for identifyingbarriers to effective symptom management at the end-of-life.Journal of Hospice & Palliative Nursing, 7(1), 23e36.
Lamb, G., & Donaldson, N. (2011). Performance measurementdAstrategic imperative and a call to action. Nursing Outlook, 59,336e338.
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic Inquiry. BeverlyHills, CA: Sage Publications, Inc.
Krimshtein, N. S., Luhrs, C. A., Puntillo, K. A., Cortez, T. B.,Livote, E. E., Penrod, J. D., & Nelson, J. E. (2011). Training nursesfor interdisciplinary communication with families in theintensive care unit: An intervention. Journal of Palliative CareMedicine, 14(12), 1325e1332.
Mack, J. W., Cronin, A., Taback, N., Huskamp, H. A., Keating, N. L.,Malin, J. L., ., & Weeks, J. C. (2012). End-of-life carediscussions among patients with advanced cancer: A cohortstudy. Annals of Internal Medicine, 12(156), 204e210.
McLennon, S. M., Uhrich, M., Lasiter, S., Chamness, A. R., &Helft, P. R. (2013). Oncology nurses narratives about ethicaldilemmas and prognosis related communication in advancedcancer patients. Cancer Nursing, 36(2), 114e121.
Miesfeldt, S., Murray, K., Lucas, L., Chang, C. H., Goodman, D., &Morden, N. E. (2012). Association of age, gender, and race withintensity of end-of-life care for Medicare beneficiaries withcancer. Journal of Palliative Medicine, 15(5), 548e554.
Patton, M. (2001). Qualitative Research and Evaluation Methods (3rded.). Thousand Oaks, CA: Sage.
Polit, D., & Beck, C. (2012). Nursing Research; Generating andAssessing Evidence for Nursing Practice. Philadelphia: WoltersKluwer Health/Lippincott Williams & Wilkins.
Sandelowski, M. (2000). Whatever happened to qualitativedescription? Research in Nursing and Health, 23(3), 334e340.
Sandelowski, M. (1995). Sample size in qualitative research.Research in Nursing and Health, 18(2), 179e183.
Sheffield, K. M., Boyd, C. A., Benarroch-Gampel, J., Kuo, Y. F.,Cooksley, C. D., & Riall, T. S. (2011). End-of-life care inMedicare beneficiaries dying of pancreatic cancer. Cancer,117(21), 5003e5012.
Temel, J. S., Greer, J. A., Admane, S., Gallagher, E. R.,Jackson, V. A., Lynch, T. J., ., & Pirl, W. F. (2011).Longitudinal perceptions of prognosis and goal of therapy inpatients with metastatic non-small-cell lung cancer: Resultsof a randomized study of early palliative care. Journal ofClinical Oncology, 29, 2319e2326.
Thacker, K. S. (2008). Nurses’ advocacy behaviors in end-of-lifenursing care. Nursing Ethics, 15(2), 174e185.
US Department of Health and Human Services. (2011). Nationalquality strategy. Retrieved from http://www.healthcare.gov/law/resources/reports/quality03212011a.html.
Walczak, A., Butow, P. N., Davidson, P. M., Bellemore, F. A.,Tattersall, M. H. N., Clayton, J. M. & Epstein, R. M. (2011).Patient perspectives regarding communication aboutprognosis and end-of-life issues: How can it be optimised?Patient Education and Counseling, doi:10.1016/j.pec.2011.08.009.
Weeks, J. C., Cook, E. F., O’Day, S. J., Peterson, L. M., Wenger, N.,Reding, D., ., & Phillips, R. S. (1998). Relationship betweencancer patients’ predictions of prognosis and their treatmentpreferences. Journal of the American Medical Association, 279(21),1709e1714. http://dx.doi.org/10.1001/jama.279.21.1709.