Embed Size (px)
Citation preview

Oncologypatients’and oncology nurses’perceptions of nurse caringbehaviours
Kimberly A.Christopher,KathrynHegedus
Previous research on patients’andnurses’perceptions of nurse caring behaviours hasdocumentedsignificantdifferences intherankingof importantbehaviours.However, thesesamples have included avariety ofmedical-surgical patients andnurses anddifferent typesof institutional settings, allofwhichmayhave affectedtheresults.Thepresent study soughtto determine if patients andnurses fromone subspecialty area and one institutionwouldhavemore concordant perceptions of caring.Forty-fouroncology patients and 49 oncologynurses completed the Respondents Perceptions of Caring Behaviour Scale (RPCBS).Results showedthatoverallmeanpatient rankingswerehighlycorrelatedwithmeannurserankings (Spearman’s correlations coefficient 0.94, P50.0001).TheWilcoxon two-samplerank sumtest was used to test the difference in rankof the 20 items between the patientsand nurses.Therewas a significant difference in rank in only sixof the 20 items.These datasuggestthatoncologypatients andnurseshavemore concordantperceptionsofcaring thanpreviously investigated groups. Implications for practice and further research arediscussed. # 2000 Harcourt Publishers Ltd
Keywords: care, caring, caring perceptions, nursing
DieWahrnehmung von Krebspatientenund Krebspflegekraº ften der Verhaltensweise von Krebspflegekraº ften in ihrer ArbeitFruº here Studien uº ber dieWahrenehmung seitens Patienten und Pflegekraº ften in bezug auf dasVerhalten derPflegekraº fte in ihrer Arbeit hast grobe Unterschiede in der Rangordnung der wichtigenVerhaltensweinsenaufgezeigt.DieseTestgruppen umfassten jedoch unterschiedlichemedizinsch-chirurgische Patienten undPflegekraº fte und unterschiedliche Arten von Institutionen, was die Ergebnisse vielleicht beeinflusst hat.Das Zieldieser Studiewar, herauszufinden, ob Patienten und Pflegekraº fte einer spezifischen Untergruppe und aus einerInstitution uº bereinstimmendeWahrnehmungenmachten.Vierundvierzig Krebspatienten und 49Krebspflegekraº fte fuº llten einen Fragebogen Respondents Perceptions of Caring Behaviour Scale (RPCBS) aus.Das Resultat Zeigte, dass allgemein diemittleren Benotungen der Patientenweitgehendmit denen derPflegekraº fte uº bereinstimmten, (Spearmans Korrelationskoeffizient 0.94, P50.0001).Der Wilcoxon zwei Proben-Bewertungssummen-Test wurde Fuº r die unterschiedliche Benotung Zwischen Patienten und Pflegepersonal von20 Fragen angewandt.Nur bei sechs der 20 Fragenwar ein deutlicher Unterschied zu erkennen.Dies Ergebniszeigt, dass Patienten und Pflegekraº fe in dieser Studie uº bereinstimmendereWahrnehmung in bezug auf die Pflegehaben, als in fruº her untersuchten Gruppen.Die Konsequenzen fuº r die Praxis und fuº r weitere Untersuchungenwerden in diesemArtikel diskutiert.
Percepciones de las conductas de atencioŁ n de enfermer|¤a de pacientes oncolo¤ gicos y enfermeros oncolo¤ gicosLas investigaciones anteriores sobre las percepciones que tienen los pacientes y los enfermeros con respecto a laatencioŁ n han documentado diferencias significativas en la clasificatioŁ n de conductas importantes. Sin embargo,estasmuestras han incluido una variedad de pacientes y enfermerosmeŁ dicos/quiruŁ rgicos y diferentes tipos deentornos institucionales, todo lo cual puede haber afectado los resultados. Este estudio intentoŁ determinar si lospacientes y enfermeros de un a¤ rea de subespecialidad y una institucio¤ n tendr|¤an percepcionesmaŁ s concordantesde la atencioŁ n.Cuarenta y cuatro pacientes oncoloŁ gicos y 49 enfermeros oncoloŁ gicos rellenaron la Escala dePercepciones de Entrevistados sobre laConducta de laAtencioŁ n (RPCBS).Los resultados indicaron que engenerallas clasificaciones de los pacientes estabanmuy correlaciones de Spearman 0.94, P50,0001). Se utilizoŁ el test desumatoria de clasificacioŁ n de dosmuestras deWilcoxon para someter a prueba la diferencia en la classificatioŁ n delos 20 elementos entre los pacientes y los enfermeros. Se observoŁ una diferencia significativa en la clasificacioŁ nsoŁ lo en seis de los 20 elementos. Estos datos sugieren que los pacientes y enfermeros oncolo¤ gicos tienenpercepciones de la atencio¤ n ma¤ s concordantes que otros grupos previamente estudiados. Se tratan lasrepercusiones para la praŁ ctica e investigaciones posteriores.
Kimberly A.ChristopherPhD, RN,OCNAssistant Professor,College of Nursing,University ofMassachusetts,Dartmouth,OldWestport Road,North Dartmouth MA02747,USAE-mail: [email protected] HegedusDNS, RN, AssociateProfessor,University of Connecticut,Storrs,CT 06269,USACorrespondence ando¡print requests to:Kimberly A.Christopher
European Journal of Oncology Nursing 4 (4),196^204 # 2000 Harcourt Publishers Ltddoi:10.1054/ejon.2000.0108, available online at http://www.idealibrary.com on

Patients’ and nurses’ perceptions of nurse caring behaviours 197
INTRODUCTION
In an attempt to meet the ongoing challenge of
demonstrating and articulating the nature of
nursing’s contribution to health care, various
nurse scholars have argued that caring is the
central focus or ‘essence’ of nursing (Benner &
Wrubel 1989, Crowden 1994, Leininger 1984,
Watson 1985). However, if caring is the ‘central,
dominating, and unifying feature of nursing’
then this must be demonstrated in a manner
relevant to practice and the patient (Morse et al.
1990). This research study measured and de-
scribed the extent to which a sample of oncology
patients and nurses in a comprehensive cancer
center agreed on the importance of selected nurse
caring behaviours. Although concordance of
perceptions has been measured in a variety of
nurse and patient samples, no investigation has
focused specifically on cancer patients and nurses
in a comprehensive cancer center setting. Such
data increases knowledge on the caring nature of
oncology nursing, identifies the degree to which
this sample of oncology patients and nurses
agree on priority caring behaviours and facil-
itates a plan of nursing care based on priority
caring behaviours identified by oncology pa-
tients.
REVIEWOF THELITERATURE
Previous research with nurses and patients has
concluded that the concept of caring is a critical
component of high-quality nursing care (Benner
& Wrubel 1989, Gadow 1985, Watson 1985,
Williams 1997). Today’s health-care environ-
ment with its emphasis on market competition,
cost containment, shorter hospital stays and
expanding use of high technology increases the
necessity to identify nursing behaviours that
make patients feel that they are being cared
for. The literature indicates that congruency of
patient-nurse perceptions and goals is important
for the patients to profit from their care (von
Essen & Sjoden 1991a). For example, investiga-
tions have documented a positive relationship
between patients’ overall satisfaction with the
hospitalization experience and their recovery,
comfort, health behaviours and compliance
(Gardener & Wheeler 1979, Keane-McDermott
et al. 1987, Kovner 1989, Lauer et al. 1982,
Valentine 1989, Williams 1997). More specifi-
cally, research has concluded that recovery
outcomes are enhanced when patients encounter
satisfying ‘nurse caring experiences’ (Valentine
1989).
Professional interest in nurse caring beha-
viours has existed since the Nightingale era
(Donahue 1995). However, over the last 25 years
an increasing number of nurse scholars have
focused on the phenomenon of caring and
systematic inquiries into the philosophical (Grif-
fin 1983, Leininger 1980, 1988, Roach 1987),
ethical (Fry 1988, Gadow 1985, Watson 1985),
professional (Benner & Wrubel 1989, Knowlden
1988, Weiss 1988) and clinical relevance (Larson
1984, Orem 1985) of caring have ensued. The
overall goal of nursing research on caring is to
identify and measure the impact that caring has
on patient health outcomes. More specifically,
the aims are to measure the extent to which
nursing care contributes to patient well-being,
quality of life, the recovery process and length of
hospitalization. However, research to date has
focused on identifying specific caring behaviours
from the perspective of patients and nurses,
developing a systematic classification of caring
behaviours and measuring the extent to which
patients and nurses agree on the importance of
nurse caring behaviours.
Classification of caring behaviours
Based on a review of the research literature,
‘affective’ and ‘instrumental’ categories of caring
behaviour are most frequently identified (Benner
1984, Clifford 1995, Komorita et al. 1991,
Larson 1984, Lea et al. 1998, Mayer 1986, von
Essen & Sjoden 1991a, 1991b, Watson 1985).
Both categories include two types of activities.
Affective caring behaviours include 1) those
activites which establish a relationship with the
patient based on qualities such as trust, sensitiv-
ity and empathy and 2) activities that offer
support, for example, surveillance, comfort and
privacy (Watson et al. 1979). Instrumental caring
behaviours include 1) physical activities or tasks
such as medication administration, hygiene care
and equipment management and 2) cognitive-
oriented activities such as teaching programmes,
advising and problem solving (Watson et al.
1979). To date, research findings have generally
demonstrated significant differences in patient
and nurse perceptions of nurse caring behaviour
(Kyle 1995, Larson 1984, Mayer 1986, von Essen
& Sjoden 1991a, Widmark-Petersson et al. 1998,
White 1972) This dichotomy requires further
investigation if nurse clinicians are to consider
such perceptual differences as they plan and
implement their nursing care.
Patient perceptions of caring
Research with medical, surgical, rehabilitation,
home-care and elderly patients has consistently
demonstrated that patients are most concerned
with instrumental caring behaviours (task-
oriented). Rehabilitation patients perceived
clinical expertise, for example knowing how to
administer an injection, how to manage the
equipment and when to call the doctor as the
European Journal of Oncology Nursing 4 (4),196^204

198 European Journalof Oncology Nursing
most important nurse caring behaviours (Keane-
McDermott et al. 1987). Caring by ‘doing extra
things’ was the most frequent response of a
sample of home-care patients receiving home-
visiting nurse services (Henry 1975). White
(1972) evaluated the responses of 300 hospita-
lized patients on the importance of 50 nursing
activities and concluded that patients were
primarily concerned with their physical care.
Brown (1986) asked a sample of 80 hospitalized
medical-surgical patients which nursing beha-
viours were perceived as indicators of care by the
nurse. Two response categories were identified:
what the nurse does (for example, assessment
and nursing procedures) and the nurses’ personal
and professional qualities. Brown concluded
that the affective and instrumental dimensions
of caring were equally important in this sample.
Using the Caring Assessment Instrument
(CARE-Q Instrument), which employs a Q-sort
methodology, Larson (1984) had 57 adult cancer
patients who were hospitalized in three acute
care hospitals prioritize 50 nurse-caring beha-
viours on a seven-point scale. The 10 most
important behaviours identified were again con-
cerned with the instrumental or task-oriented
aspects of care and included knowing how to
give injections, manage equipment and giving
medications on time. Mayer (1986) replicated
Larson’s study (1984) with a group of 54
oncology patients and found that patients again
selected instrumental behaviours as most indica-
tive of caring.
Scandinavian investigators (von Essen &
Sjoden 1991a, 1991b) used a Swedish version of
the CARE-Q Instrument to determine how
medical-surgical patients and nurses ranked
caring behaviours. Both studies identified sig-
nificant differences in perceptions of caring.
Again patients consistently ranked competent
clinical expertise as most important. Some
investigators have assumed that the differences
in patient and nurse perceptions resulted from
differences in the content of patients’ and nurses’
cognitive associations with caring behaviour
(von Essen & Sjoden 1991a, 1991b, Larson
1984, Mayer 1987). Recenly, Widmark-Petersson
et al. (1998) explored this possibility with a group
of cancer patients and cancer nurses. Subjects
were asked open-ended questions about their
cognitive associations with nine preselected
CARE-Q behaviours. Content analysis revealed
similar representations of the nine caring beha-
viours. However, patients described physical,
medical and technical aspects of caring to a
greater extent than nursing staff (Widmark-
Petersson et al. 1998).
Focusing on a maternity clinical population,
a sample of antepartum and postpartum patients
rated the importance of 65 caring behaviours
identified on the Caring Behaviour Assessment
European Journal of Oncology Nursing 4 (4),196^204
instrument (CBA) (Schultz et al. 1998). Investi-
gators hypothesized that uncomplicated mater-
nity patients would focus less on the clinical
aspects of care and more on the teaching and
emotional support aspects of care. However, this
was not the case. Again, all subjects indicated
that the most important aspects of caring were
continuous monitoring of their condition and
demonstrable clinical competency.
Nurse perceptions of caring
Nurses select caring behaviours from the affec-
tive category (emotional) as the most important.
Nurses reported satisfying psychosocial
needs rather than physical care as the priority
(White 1972). Gardner and Wheelers’ (1979)
sample of 74 nurses identified three behaviours
as most caring: interest in the patient, creating an
environment where the patient is free to express
feelings and listening to the patient. Nurses
identified ‘listening’ as the single most important
caring behaviour in several studies (Ford
1981, Gardener & Wheeler 1979, Larson 1986,
Mayer 1987). Using the Care-Q Instrument
with oncology nurses, Larson (1986, 1987) and
Mayer (1986) determined that the most impor-
tant nurse caring behaviours were listening to the
patient, touching the patient in order to comfort,
allowing patients to express their feelings, being
perceptive of patients’ needs and planning for
such needs and realizing that patients know
themselves best. Swedish investigators (von
Essen & Sjoden 1991a, 1991b, Widmark-Peters-
son et al. 1998) administered a Swedish version
of the Care-Q Instrument and obtained results
similar to Larson and Mayer. As an exception to
this pattern, the Keane-McDermott et al. (1987)
study also using the Care-Q Instrument, reported
that rehabilitation nurses identified competent
clinical expertise as the most important nurse
caring behaviour. Prioritizing physical needs
before affective needs is, according to Keane-
McDermott et al. (1987), congruent with reha-
bilitative nursing philosophy. Lea et al. (1998)
conducted a large postal survey of nurses and
student nurses (n¼1452) in order to examine the
potential existence of an underlying structure of
caring. Factor analysis of data from the Caring
Dimensions Inventory resulted in the first factor
focusing on the psychosocial aspects of care and
the second on the technical. Again, this nurse
sample’s priority was the affective aspects of
care.
These studies clearly demonstrate differences
in perceptions of caring by patients and nurses.
Patients valued activities associated with being
‘cared for’. When considered in light of the fact
that patients enter the hospital to have a problem
eliminated or improved, it is not surprising
that they focus on interventions related to the

Patients’ and nurses’ perceptions of nurse caring behaviours 199
problem (Komorita et al. 1991). Nurses, on the
other hand, emphasize behaviours indicative of
the cognitive process of ‘caring about’ (Komorita
et al. 1991). When ranking behaviours, nurses
may assume a level of technical competence
as fundamental to their practice (Mayer 1986).
However, previous research that measured
nurses’ assessment of the extent to which patients
were experiencing stress, discomfort, anxiety and
depression demonstrated that nurses’ misper-
ceived and overrated patients’ emotional distress
(Farrell 1991, Holmes & Eburn 1989, Johnston
1976, Mason & Muhlenkamp 1976). Therefore,
nurses cannot assume that patients perceive
caring efforts as they are intended. To avoid
poor communication and dissatisfied patients it
is imperative that nurses validate with patients
that their care needs are being met.
Limitations of previous research
Differences in patient-nurse perceptions may be
attributable to methodological limitations; for
example, the study sample and size, the setting in
which the nurse–patient interaction takes place
and the data collection instruments. Sample sizes
in the previously described studies are generally
small. With one exception (Lea et al. 1998) all
samples had less than 110 participants
(range¼ 30–105). Perceptions of caring are
influenced by the setting in which the nurse and
patient interact (Fealy 1995, Larson 1987, Mayer
1987). Therefore, studies that drew samples from
a variety of settings (Larson 1984, 1986, von
Essen & Sjoden 1991b) may not consider the
importance of the context of the nurse–patient
interaction and the extent to which this influ-
ences perception. Moreover, combining multiple
types of patients (for example, medical, surgical
and oncology (Brown 1986, von Essen & Sjoden
1991b)) and different types of institutions (for
example, university and community hospitals
(Larson 1987, von Essen & Sjoden, 1991b)) may
contribute to perceptual differences.
In addition, data collection instruments may
limit the application of findings. Specifically,
those studies using the forced choice Q-technique
(Larson 1986, 1987, Lea & Watson 1996, Mayer
1987, von Essen & Sjoden 1991a, 1991b) may
inadvertently bias results because the technique
limits the number of responses per category
(Polit & Hungler 1995, von Essen & Sjoden
1991a, Widmark-Petersson 1998). Also those
data collected with the CBA instrument may
not distinguish between more caring and less
caring behaviour because responses tend to be
positively skewed (Schultz 1998). Finally, instru-
ments that merely request the ranking of specific
items do not provide any information on the
meaning of caring for patients (Kyle 1995, Morse
et al. 1990).
Previous research that combined multiple
types of patients, nurses and institutions demon-
strated a lack of agreement with important
caring behaviours. The current study was de-
signed to determine if patients’ and nurses’
perceptions of caring behaviours were more
concordant when the sample was selected from
one subspecialty area and one institution.
PURPOSEOF THESTUDY
This descriptive exploratory study focused on the
caring perceptions of oncology patients and
oncology nurses in a comprehensive cancer
center in northeast USA.
Specific objectives were:
1. To measure the oncology patients’ and
oncology nurses’ perceptions of nurse caring
behaviours.
2. To describe the extent to which oncology
patients and oncology nurses agree on their
perceptions of nurse caring behaviours.
3. To identify those caring behaviours on
which patients and nurses disagree.
METHODOLOGY
Design
This was a descriptive exploratory study. All
subjects completed a brief demographic form
and the self-administered Respondents Percep-
tions of Caring Scale (RPCS) that rank ordered
20 caring behaviours (Hegedus 1999, Hegedus &
Neuberg 1994).
Setting
Comprehensive cancer center in northeast USA.
Recruitment
Approval to conduct the study was obtained
from the Institutional Review Board at the
comprehensive cancer center. Participation was
voluntary and subjects were assured of confiden-
tiality. English-speaking oncology patients who
were hospitalized for cancer therapy including
chemotherapy, bone marrow transplantation,
febrile neutropenia, spinal cord compression,
dehydration and pain control were potentially
eligible to participate in this study. Each patient
was determined by their primary medical and
nursing staff to be through the acute phase of
their admission, to be clinically stable and
psychologically appropriate to participate in the
study. Patients were not receiving pharmacolo-
gical therapies in doses that impaired cognition.
European Journal of Oncology Nursing 4 (4),196^204

200 European Journal of Oncology Nursing
In addition, patients must have had a least one
prior admission to the institution. This criteria
was included because the facility was a tertiary
cancer center and many patients, newly referred
to the institution, were unfamiliar with the daily
hospitalization routine. The investigators felt
that as a common minimum among the study
subjects, two hospitalizations would provide the
subjects with an adequate frame of reference and
interactions with the nursing staff to successfully
evaluate caring behaviours.
All English-speaking registered nurses em-
ployed on the in-patient clinical units who
worked at least 20 hours per week were eligible
to participate in the study.
Three times per week the nurse researcher
reviewed the in-patient admission list and
identified potential study subjects. Once it was
determined that the patient met the eligibility
requirements, the nurse researcher approached
the patient with an explanation of the study. The
instrument packet materials were reviewed and
written consent to participate in the research was
obtained from each patient who agreed to
complete the instrument.
Nurses were informed of the study at a staff
meeting and through a letter sent to each eligible
nurse. The letter explained the study and also
included a postcard which the nurse returned if
she/he was interested in participating. The nurse
researcher met with each interested nurse,
explained the purpose of the study and the
instrument packet materials, and obtained
written informed consent to participate in the
study.
Respondents Perceptions of CaringScale (RPCS)
Based on the literature, clinical observations and
discussions with nurses, 45 items representing
a wide range of nurse caring behaviours were
initially selected (Hegedus 1999). Ten nurses with
expertise in either the substantive area of caring
or instrument development evaluated the 45
items (Davis 1992). The content experts were
asked to assign each item to one of Benner’s
(1984) seven domains of nursing practice and
to indicate how strongly they felt this was the
appropriate domain using Gable’s (1986) scoring
procedure, 1¼ not very sure, 2¼ strongly agree,
3¼ no question about agreement.
Two criteria were used to retain items: a
minimum of 80% agreement of assignment of
items to a domain and a minimum comfort level
of 2. The final scale had 20 items that reflected
two of Benner’s domains, the helping role and
the teaching-coaching function (Hegedus 1999).
Results of the instrument pilot test are reported
separately (Hegedus 1999).
European Journal of Oncology Nursing 4 (4),196^204
Procedure
The study packet included the following materi-
als: instructions for completing the RPCS, the 20
caring items typed on individual self-adhering
labels and three sheets of paper – one each titled
‘Most Caring’, ‘Average Caring’ and ‘Least
Caring’. The papers were divided into 20
consecutively numbered lines on which the
caring labels were placed. Information on
how to contact the nurse researcher was pro-
vided.
Previous research experiences at the facility
that required study subjects to rank order
preselected items were not successful. Investiga-
tors noted that once the first few items were
prioritized, subjects were unable to discriminate
between the remaining items. The investigators
determined that providing the subjects with a
more structured process, for example sorting
into specific subgroups then ranking within the
subgroups, was easier for the subjects to
complete (D.S. Neuberg, personal communica-
tion, September 14 1995). Pilot testing of the
RPCBS also determined that subjects had
difficulty with sorting and ranking the items
(Hegedus 1999). Based on these experiences, the
RPCS was revised to a two-step process.
First the subjects sorted the 20 items into one
of three subgroups – ‘Most Caring’, ‘Average
Caring’ and ‘Least Caring’. Then in the second
step, subjects rank ordered the items from most
to least within each subgroup. To further
facilitate the ranking process, the caring item
‘The nurse treats me as an individual’ was
selected as the starting point. During the item
selection phase of developing the instrument, the
content reviewers concurred that ‘The nurse
treats me as an individual’ was a very caring
behaviour and would serve as an appropriate
anchor against which the other caring items
could be compared (Hegedus 1999). Subjects
began by determining which of the three
subgroups they would place the item ‘The nurse
treats me as an individual’. The remaining 19
items were then sorted into the subgroups by
comparing the specific item to ‘The nurse treats
me as an individual’ and deciding if the item
was more caring, less caring, or equally as caring
as this.
After the items were sorted into the subgroups,
the subject took each subgroup and ranked the
items from most caring to least caring within that
subgroup. Once the ranking was completed the
self-adhering labels were attached to the appro-
priately designated paper so that the ‘most
caring’ item was placed in the space labeled #1,
the next item in space #2 and so forth.
The directions were reviewed with the study
subjects when the packets were distributed.
Questions were answered as needed. Two

Patients’ and nurses’ perceptions of nurse caring behaviours 201
patients and one nurse returned incomplete
packets that were not included in the analysis.
Data analysis
Overall correlation of mean rankings was deter-
mined by Spearman’s Rho. Mean rankings for
individual items were calculated using a Wilcox-
on rank sum test comparing two groups. No
correction for multiple comparisons was in-
cluded in the P-values reported.
RESULTS
A total of 44 patients completed the instrument
(26 female, 18 male). Of those patients recruited,
six refused to participate. The median age was 50
(range 22–71). Patients were being treated for a
variety of oncological malignancies and approxi-
mately one third were admitted for a bone
marrow or stem call transplantation. Forty-nine
nurses (48 female, 1 male) out of a possible total
of 78 completed the instrument (62% participa-
tion rate). The median age of the nurses was 36
(range 26–51). The median length of time work-
ing at the institution was 8.75 years (range of
6 months–19 years), indicating that the vast
majority of nurse participants were very experi-
enced in caring for oncology patients.
Overall patients’ mean rankings were highly
correlated with nurses’ rankings (r¼ 0.94,
P50.0001). Patients ranked several items as
significantly less caring than the nurses’ ranking
and several additional items as more caring than
the nurses. Specifically, the patients and nurses
assessment of 14 out of the 20 caring behaviours
were concordant (Table 1). Both groups selected
and ranked the same top five caring items – the
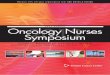
Table1 Mean Rank Score for Patients andNurses, and
Caring Behavior Item
The nurses treatme as an individualThe nurses speak tome in angry tonesThe nurses respectmy rightsThe nurses did not talk about howmy illnessmight a¡ectmy liThe nurses encourageme to expressmy frustration and angerWhen I’m sad and cry the nurses stay withmeThe nurses coachme through bad experiencesThe nurses comfortme by their silent presenceWhen I am fearful the nurses try to easemy fearsThe nurses do not individualizemy careThe nurses know how tomakeme laughThe nurses provide soothing reassurance through their touchThe nurses are always honest withmeThe nurses know when I need a smileThe nurses are in toomuch of a hurryThe nurses know when I need a hugThe nurses do not explain procedures to meThe nursesmakeme feel importantThe nurses did not tellmewhat to expectThe nurses do not listen to themembers ofmy family
nurses treat me as an individual, the nurses
respect my rights, the nurses are always honest
with me, when I am fearful the nurses try to ease
my fears, and the nurses coach me through bad
experiences. Of the three least caring behaviours,
both groups identified being in a hurry and
speaking in an angry tone of voice as uncaring.
Patients identified failing to listen to family
members and nurses identified failing to explain
procedures as the third least caring behaviour.
Six items had significantly different mean
rankings. Specifically, the nurses perceived re-
spect for patient rights, expression of anger and
fear, staying with a sad and crying patient, and
providing soothing reassurance through touch as
more caring behaviours than patients. Patients
did not consider the absence of a discussion of
how illness might affect their life and failure to
individualize care to be as uncaring as the nurses
reported.
Interestingly, the last seven items were the
same for both groups; however, they were not
ranked in the same order. In the nurse group 6 of
the 7 items had just about the same rank score
(range¼ 16.2–16.7), suggesting that the nurses
had a clear sense of what were not considered to
be caring behaviours. In the patient group the
rank scores were spread out. This lack of
uniformity in the patients’ scores suggested that
patients were able to discriminate between caring
items and determine that certain behaviours were
less caring than other behaviours. This lack of
uniformity may also indicate that cancer patients
and nurses have different perceptions of caring.
However, out of the seven least caring items only
two (the nurses did not talk about how my illness
might affect my life and the nurses did not
individualize my care) actually had statistically
significant different mean rankings.
P-value less than 0.05 by theWilcoxon test
Patients Nurses P-value
3.3 2.517.0 19.05.2 3.6 0.01
fe 13.9 16.2 0.0111.1 7.1 0.00019.2 6.7 0.0036.9 6.610.6 9.55.6 6.314.2 16.6 0.029.0 10.39.2 7.1 0.025.2 4.59.4 10.315.5 16.711.1 10.215.2 17.07.3 6.914.9 16.616.0 16.5
European Journal of Oncology Nursing 4 (4),196^204

202 European Journalof Oncology Nursing
Limitations of the current study
Findings from the current study must be
considered in light of several methodological
limitations. A small convenience sample (n¼ 93)
was used. Therefore, the findings cannot be
extrapolated to other cancer patients, nurses or
cancer institutions. Also, because the sample was
small, the investigator provided each subject with
an individual explanation of the study instru-
ment directions. It must be determined whether
or not the sorting and ranking procedure can be
successfully completed without a verbal explana-
tion. Otherwise, this scale will not be feasible for
use with large samples.
DISCUSSION
The ultimate goal of nursing research on caring
is to identify and measure the impact that caring
has on patient health outcomes. The first step
towards achieving this goal is to systematically
determine the extent to which patients and
nurses agree on important nurse caring beha-
viours. The lack of perceptual agreement in
previous studies has been attributed to samples
that combined different types of patients and
different types of hospital settings and thereby
disregarded the possibility that perceptions of
caring were influenced by the context in which
the interaction occurred. Previous studies that
included some oncology patients and nurses
determined that there was no perceptual agree-
ment on caring behaviours (Larson 1987, Mayer
1986, Widmark-Petersson et al. 1998). The
current study comprising oncology patients and
nurses from one cancer institute determined that
perceptions of caring were very highly correlated
in this sample. It supports the position that
perceptions are influenced by the context of the
interaction (Fealy 1995, Larson 1984, 1987, von
Esson & Sjoden 1991b). Therefore, future caring
research must carefully select the study sample
and setting if the best measures of perceptual
agreement are to be determined.
Although there was concordance between
oncology patients’ and nurses’ views of most of
the nurse caring behaviour items, there were
some differences between the two groups. It is
important for oncology nurses to recognize that
differences exist and not to assume that nursing
efforts are always perceived as caring. For
example, in this sample, nurses and patients did
not agree on the extent to which touch as
a form of reassurance was a caring behaviour.
Nurses ranked touch as more caring than
patients. Perhaps patients do not want to be
touched or perhaps touching was merely not a
reassuring action. However, this is an interesting
patient–nurse discrepancy in light of the current
European Journal of Oncology Nursing 4 (4),196^204
emphasis on alternative/complementary thera-
pies, many of which involve some form of touch
healing. Based on study findings, alternative
ways of providing patients with reassurance
should be identified. Oncology nurses must ask
their patients about the values they associate
with caring. Results from this study demon-
strated that these oncology patients were capable
of distinguishing between caring items and
assigning a priority ranking to the individual
items. Patients were actually more discriminating
than nurses when assigning importance to the
least caring behaviours. Of note, von Essen and
Sjoden (1991b) also found that patients were
more discriminating in their evaluation of items.
Clearly patients have beliefs and expectations
about caring which nurses need to identify.
These beliefs influence patients’ attitudes toward
nursing care and the potential benefits or out-
comes from such care. Nurses want to use their
time to best benefit the patient (Schultz et al.
1998). Clear communication will identify desired
behaviors, facilitate appropriate plans of care
and increase the likelihood that ‘patients feel
cared for’ (Widmark-Petersson et al. 1998)
Moreover, identifying agreement and disagree-
ment with specific caring behaviours provides
nurses with information on specific aspects of
their practice that should be reinforced and those
that need to be changed.
Although measuring caring behaviours can be
a challenge, it is possible. The present study
adds to our knowledge of the caring nature of
oncology nursing practice by specifically identi-
fying the most important caring behaviours. This
sample of oncology patients and nurses were in
strong agreement on priority behaviours and this
information should be incorporated into plans of
nursing care. Further evaluation of the instru-
ment using larger samples and other oncology
settings will add to our understanding of priority
caring behaviours in this particular group of
patients and nurses.
ACKNOWLEDGEMENT
Thank you to Susan M. Grant MS, RN, OCN for
supporting this research.
REFERENCES
Benner P (1984) From Novice to Expert: Excellence and
Power in Clinical Nursing Practice. Addison Wesley,
Menlo Park, CA
Benner P, Wrubel J (1989) The Primacy of Caring: Stress
and Coping in Health and Illness, 2nd edn. Addison
Wesley, Menlo Park
Brown L (1986) The experience of care: patient perspec-
tives. Topics of Clinical Nursing 8(2): 56–62
Clifford C (1995) Caring: fitting the concept to nursing
practice. Journal of Clinical Nursing 4: 37–41

Patients’ and nurses’ perceptions of nurse caring behaviours 203
Crowden A (1994) On the moral nature of nursing
practice. Journal of Advanced Nursing 20: 1104–1110
Dans LL (1992) Instrument review: getting the most from
a panel of experts. Applied Nursing Research 5:
194–197
Donahue MP (1995) Nursing the Finest Art, 2nd edn.
Mosby-Year Book, Inc., St. Louis
Farrell G (1991) How accurately do nurses perceive
patients’ needs? A comparison of general and
psychiatric settings. Journal of Advanced Nursing 16:
1062–1070
Fealy G (1995) Professional caring: the moral dimension.
Journal of Advanced Nursing 22: 1135–1140
Ford M (1981) Nurse professionals and the caring process.
Doctoral Dissertation, University of Northern
Colorado. Dissertation Abstracts International 42:
967b–968b.
Fry S (1988) The ethic of caring: can it survive in nursing?
Nursing Outlook 36(1): 48
Gadow S (1985) Nurse and patient: the caring relation-
ship. In: Bishop A & Scudder J (Eds) Caring, Curing,
Coping. University of Alabama Press, Birmingham
AL
Gable RK (1986) Instrument Development in the Affec-
tive Domain. Kluwer Nijhoff, Boston
Gardner KG, Wheeler E (1979) Patients and staff nurses’
perceptions of supportive nursing behaviours: a
preliminary analysis. In: Leininger E (Ed.) Caring.
An Essential Human Need. Charles B. Slacks,
Thorofare, NJ
Griffin A (1983) A philosophical analysis of caring
in nursing. Journal of Advanced Nursing 5:
261–272
Hegedus K (1999) Provider’s and consumer’s perspectives
of nurses’ caring behaviours. Journal of Advanced
Nursing 30(3): 1090–1096
Hegedus K, Neuberg D (1994) Nursing carative beha-
viours: devising a scale to measure. In: Imagination
and Creativity, 6th Annual Nurses Research
Conference. Eastern Nursing Research Society,
Binghamton, NY
Henry D (1975) Nurse behaviors perceived by patients as
indicators of caring. Doctoral Dissertation, Catholic
University, Washington DC. Dissertation Abstracts
International 36: 02652 B.
Holmes S, Eburn E (1989) Patients’ and nurses’ percep-
tions of symptom distress in cancer. Journal of
Advanced Nursing 14: 840–846
Johnston M (1976) Communication of patients’ feelings
in hospital. In: Bennet AE (Ed.) Communication
between doctors and patients. Nuffield Hospital
Trust, London, UK
Keane-McDermott S, Chastain B, Rudisill K (1987)
Caring nurse–patient perceptions. Rehabilitative
Nursing 12: 182–187
Kovner C (1989) Nurse–patient agreement on outcomes
after surgery. Western Journal of Nursing Research 1:
7–19
Knowlden V (1988) Nurse caring as constructed knowl-
edge. In: Caring and Nursing Explorations in the
Feminist Perspectives. School of Nursing, University
of Colorado Health Sciences Center, Denver,
Colorado
Komorita N, Doehring K, Hirchert P (1991) Perceptions
of caring by nurse educators. Journal of Nursing
Education 30(1): 23–29
Kyle TV (1995) The concept of caring: a review of
the literature. Journal of Advanced Nursing 21:
506–514
Lauer P, Murphy S, Powers M (1982) Learning needs of
cancer patients: a comparison of nursing and patients
perceptions. Nursing Research 31: 11–16
Larson P (1984) Important nurse caring behaviours
perceived by patients with cancer. Oncology Nursing
Forum 11(6): 46–50
Larson P (1986) Cancer nurses’ perceptions of caring.
Cancer Nursing 9(2): 86–91
Larson P (1987) Comparison of cancer patients’ and
professional nurses’ perceptions of important
nurse caring behaviours. Heart & Lung 16(2):
187–192
Lauer P, Murphy A, Powers M (1982) Learning needs of
cancer patients: a comparison of nursing and patient
perceptions. Nursing Research 31: 11–16
Lea A, Watson R (1996) Caring research and concepts: a
selected review of the literature. Journal of Clinical
Nursing 5: 71–77
Lea A, Watson R, Deary I (1998) Caring in nursing: a
multivariate analysis. Journal of Advanced Nursing
28(3): 662–671
Leininger M (1980) Caring: A central focus of nursing and
health care services. In: Leininger M (Ed.) Care: The
Essence of Nursing and Health. Charles B. Slack,
Thorofare, NJ
Leininger M (1981) Caring: An Essential Human Need.
Charles B. Slack, Thorofare, NJ
Leininger M (1984) Care: the Essence of Nursing
and Health. Wayne State University Press,
Detroit
Leininger M (1988) Leininger’s theory of nursing: cultural
care diversity and universality. Nursing Science
Quarterly 1: 152–160
Mason L, Muhlenkamp A (1976) Patients’ self-reported
affective states following loss and caregivers’ expec-
tations of patients’ affective states. Rehabilitation
Psychology 23(30): 72–76
Mayer D (1986) Cancer patients’ and families perceptions
of nurse caring behaviours: a replication study.
Topics in Clinical Nursing 8(2): 63–69
Mayer D (1987) Oncology nurses versus cancer
patients’ perceptions of nurse caring behaviours: a
replication study. Oncology Nursing Forum 14(3):
48–52
Morse J, Solberg S, Neander W, Bottorff J, Johnson J
(1990) Concepts of caring and caring as a concept.
Advances in Nursing Science 13(1): 1–19
Orem D (1985) Nursing: Concepts of Practice, 3rd edn.
McGraw-Hill, New York
Polit H, Hungler B (1995) Nursing Research: Principles
and Methods, 5th edn.
Roach M (1987) The human act of caring: A blueprint for
health professions. Canadian Hospital Association,
Toronto, Canada
Schultz A, Bridgham C, Smith M, Higgins D (1998)
Perceptions of Caring. Clinical Nursing Research
7(4): 363–378
Valentine K (1991) Comprehensive assessment of
caring and its relationship to outcome measures.
Journal of Nursing Quality Assurance 5(2): 59–68
Valentine K (1989) Caring is more than kindness:
modeling its complexities. Journal of Nursing Ad-
ministration 19(11): 28–34
von Essen L, Sjoden P (1991a) The importance of nurse
caring behaviours as perceived by Swedish hospital
patients and nursing staff. International Journal of
Nursing Studies 28(3): 267–281
von Essen L, Sjoden P (1991b) Patient and staff
perceptions of caring: review and replication. Journal
of Advanced Nursing 16: 1363–1374
Watson J, Burckhardt C, Brown L, Bloch D, Nester N
(1979) A Model of Caring: An Alternative Health
Care Model for Nursing Practice and Research.
In: Clinical and Scientific Sessions, ANA, Kansas
City
European Journal of Oncology Nursing 4 (4),196^204

204 European Journal of Oncology Nursing
Watson J (1985) Nursing: Human Science and Human
Care, A Theory of Nursing. Appleton-Century-
Crofts, Norwalk, CN
Weiss C (1988) Model to discover, validate, and use care
in nursing. In: Leininger M (Ed.). Care, Discovery
and Uses in Clinical and Community Nursing. Wayne
State University Press, Detroit
White M (1972) Importance of selected nursing activities.
Nursing Research 21: 4–14
Widmark-Petersson V, von Essen L, Sjoden P (1998)
Perceptions of caring: patients’ and staffs’ associa-
European Journal of Oncology Nursing 4 (4),196^204
tions to CARE-Q behaviours. Journal of Psychoso-
cial Oncology 16 (1): 75–96
Williams SA (1997) Caring in patient-focused care: the
relationship of patients’ perceptions of holistic nurse
caring to their levels of anxiety. Holistic Nursing
Practice 11 (3): 61–68
Williams SA (1997) The relationship of patients’ percep-
tion of holistic nurse caring to satisfaction with
nursing care. Journal of Nursing Care Quality 11(5):
15–29