Embed Size (px)
Citation preview
Thorax (1971), 26, 55.
Opacities of the middle and upper lobes incombinationB. T. LE ROUX
Thoracic Unit, Wentworth Hospital, Durban, and the Department of Surgery, University of Natal
The diagnosis of bronchial carcinoma was confirmed in 8 of 17 patients who presented withthe radiographic appearances of a combination of right upper and middle lobar opacification.In 9 patients the cause of the combination of lobar shadows was inflammatory, in 2 destructive.This experience serves to emphasize that the investigation of lobar and segmental shadows,j;nwhatever combination, must, at an early stage, include bronchoscopy.
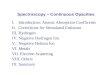
In certain combinations, shrinkage of more thanone lobe, or of segments separated by aeratedlung, diminishes the likelihood of a commonbronchus-obstructing lesion, such as bronchialcarcinoma of central type, as the cause of pul-monary shrinkage. Thus, while shrinkage of themiddle and right lower lobes together is commonand usually diagnostic of a bronchus-obstructingagent in the intermediate (lower part of rightmain) bronchus-whether this be mucus, a foreignbody, carcinoma or other lesions-shrinkage ofthe middle and right upper lobes together withoutshrinkage of the lower lobe should not denote acommon bronchus-obstructing lesion because ofthe length of the intermediate bronchus betweenthe bronchi which serve the shrunken lobe (Fig. 1).Exceptions to this rule-called by Felson (1960)the 'double lesion sign'-are common, andbronchoscopy remains an early requisite in theinvestigation of all lobar and segmental shadowsin whatever combination. Exceptions are commonbecause, in the circumstances in which relativelywidely separated lobes or segments are opaqueand shrunken, the bronchus-obstructing lesionsmay be dissimilar. Thus, bronchial carcinomawhich obstructs the right upper bronchus may beassociated with mucus obstruction or externalcompression of the middle bronchus by medi-astinal glandular metastasis.The purpose of this paper is to illustrate and
outline the pathology in 17 examples of shrinkageand opacification of the right upper and middlelobes in combination. The patients were all adultmen of an age which made likely bronchial car-cinoma as the cause of a pulmonary lesion. In allbut four patients the upper and middle lobestogether occupied a volume of the right hemi-
FIG. 1. A right lateral bronchogram shows why a commonbronchus-obstructing lesion is unlikely to be the cause ofacombination of a middle and upper lobar shadow on theright, while the lower lobe is spared. Middle and upperbronchial orifices are separated by the length of inter-mediate (lower part of main) bronchus through which airmust pass to reach the lower lobe.The bronchogram was made in late convalescence for theyoungest patient in the series who had shrinkage of themiddle and upper lobes together, and in whom the causewas an evanescent infection.
55
*| l:
I.
F
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
I;S. {l)
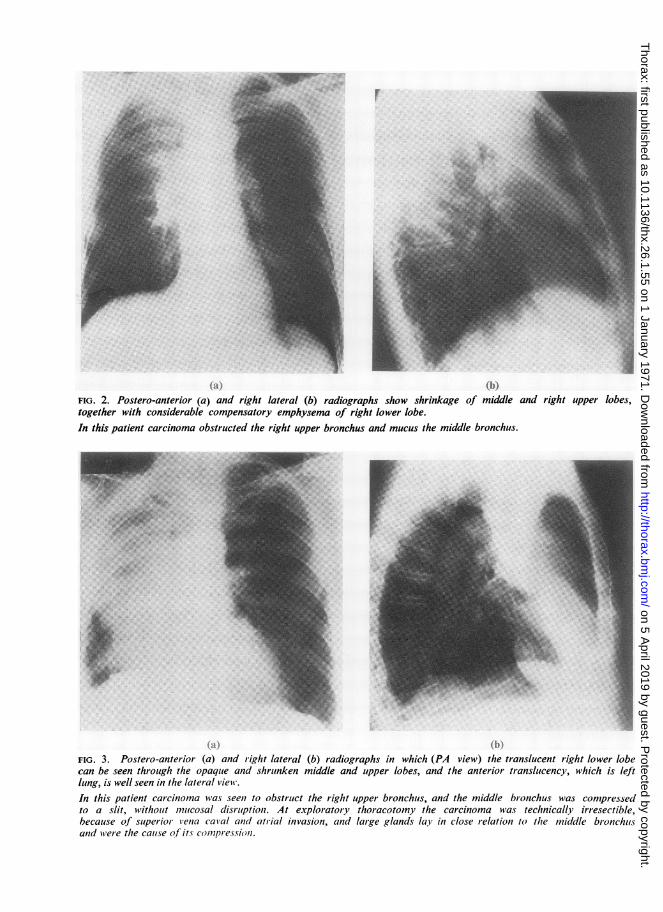
FIG. 2. Postero-anterior (a) and right lateral (b) radiographs show shrinkage of middle and right upper lobes,together with considerable compensatory emphysema of right lower lobe.In this patient carcinoma obstructed the right upper bronchus and mucus the middle bronchus.
*1FIG. 3. Postero-anterior (a) and right lateral (b) radiographs in which (PA view) the translucent right lower lobecan be seen through the opaqlue and shrunken middle and upper lobes, and the anterior translucency, which is leftlung, is well seen in the lateral view.In this patient carcinoma was seen to obstruct the right upper bronchus, and the middle bronchus was compressedto a slit, without mulcosal disruption. At exploratory thoracotomy the carcinoma was technically irresectible,because of superior *iena caval anbd atrial invasion, and large glands lay in close relation to the middle bronchutsand were the caiuse of its compression.
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
Opacities of the middle and upper lobes in combination
thorax smaller than normal. In one, shrinkagewas gross (Fig. 2), and in the others it varied fromconsiderable (Fig. 3) to minor (Fig. 4). The degreeof compensatory emphysema of the right lowerlobe varied appropriately with the extent of rightupper and middle lobar shrinkage. Left-sided pul-monary translucency was visible behind thesternum in most, but the depth and extent of thisvaried over a wide range, as shown in the lateralfilms (Figs 2b, 3b and 4b).
In four patients the radiographic opacity inter-preted as middle and right upper lobar was asso-ciated with caudally and posteriorly directed con-vexity of the oblique fissure, which suggested thatat least part of the opaque lobes was of largerthan normal size, whether from bulk of tumour ordistension in relation to infection with suppura-tion (Fig. 5). In two with middle and upper lobar'distension' there was, in early radiographs, afluid level (Fig. 5).
BRONCHOSCOPIC FINDINGS
In nine patients the only abnormality at broncho-scopy was pus in the bronchi, which, in the twopatients with fluid levels, was of large volume. Ineight patients there was bronchoscopic evidence oftumour. In three of these eight, the tumouroccluded the right upper bronchus and mucus orpus occluded the middle bronchial orifice, which,after aspiration of the foreign material, lookednormal. In these three patients, at exploratorythoracotomy which included pneumonectomy, thetransverse fissure was absent or vestigeal. Thecarcinoma was of central type and in none largerthan a golf ball, and in each there was airless,shrunken, solid lung distal to the tumour which,because of absence of the transverse fissure, madeupper and middle lobes appear as one. Histologic-ally, the inflammatory changes distal to the tumourwere evenly distributed between middle and upperlobes, as if these behaved as a single functioningunit. The bronchial anatomy was normal.
In three others of the eight patients with middleand upper lobar opacities and pulmonary carci-noma, the tumour was seen at bronchoscopy toobstruct the right upper bronchus and the middlebronchus was compressed to a horizontal slit.Exploratory thoracotomy was undertaken in twoof these patients and completed by pneumon-ectomy in one; in each, it could be demonstratedthat compression of the middle bronchus was con-sequent upon enlargement of related nodes inwhich there was metastatic tumour. In one ofthese two patients the transverse fissure was com-
plete; in the other it was incomplete but easilyrecognizable. In the third patient in this groupthere was gross oesophageal displacement pre-sumed to be from mediastinal glandular meta-stasis, and a thoracotomy was not made. In thispatient it is presumed that middle bronchialcompression was consequent upon relatedtumorous glands.
In one of the eight patients with middle andupper lobar opacities and bronchial carcinoma,tumour was visible in the right main bronchusand a bougie could be passed distally as far as thebasal bronchi, a fact confirmed radiographically.In this patient the main carina was widely invadedby tumour and there was oesophageal displace-ment and phrenic paresis. It is presumed that thecarcinoma obstructed both the middle and theupper bronchi and it was confirmed that there wasan air passage from the trachea to the basalbronchi.
In the last patient in this group of eight, rightupper bronchial carcinoma was associated with amiddle bronchus that looked in every respectnormal. At exploratory thoracotomy, whichincluded pneumonectomy, the middle lobe was atiny, shrunken wedge and the transverse fissurewas obliterated by adhesions. This is the onlypatient in the series with two unrelated diseases-right upper bronchial carcinoma and bronchi-ectasis of a shrunken middle lobe, the latter pre-sumably of long standing.
AETIOLOGY
The cause of combined middle and upper lobarpulmonary opacities in eight patients was bron-chial carcinoma: in three, with distal inflam-matory changes in the upper and middle lobeswhich were anatomically inseparable, although thebronchial anatomy was normal, and in these threepatients the tumour was in the right upperbronchus; in three patients, right upper bronchialcarcinoma was associated with compression of themiddle bronchus by mediastinal glands; in onepatient, carcinomatous involvement of the middleand upper bronchi was associated with retentionof an air passage to the basal bronchi; and in thelast of this group, right upper bronchial carcinomawas associated with bronchiectasis in a shrunkenmiddle lobe.
In seven of the nine patients in whom thebronchoscopic appearances, apart from thepresence of pus, were normal, the middle andupper radiographic opacities cleared slowly duringa period of physiotherapy and with the exhibition
57
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
M.~~~~~~~~I
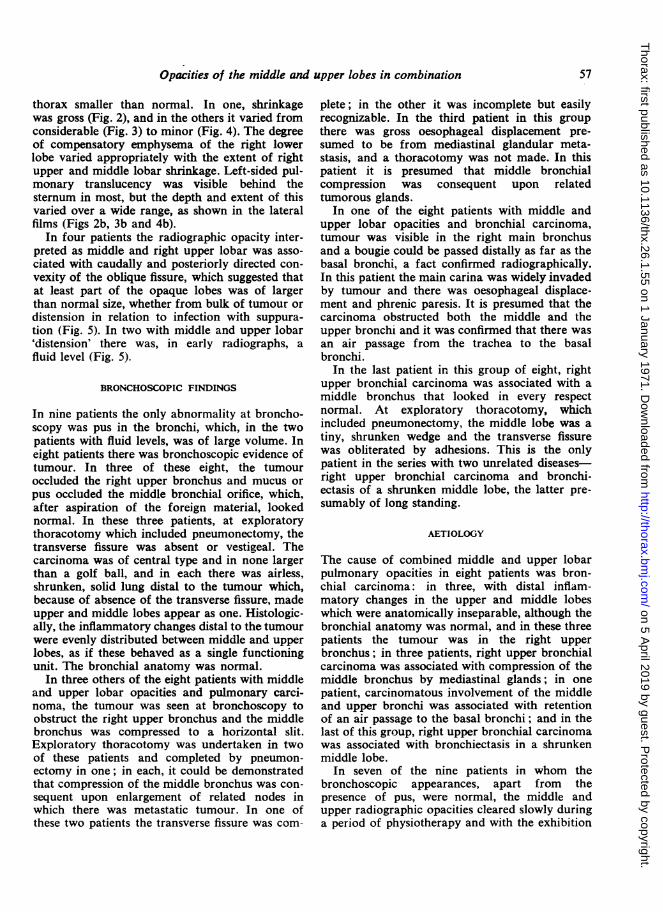
FIG. 4. Postero-anterior (a) and right lateral (b) radiographs of a patient in whom carcinoma obstructed theright upper bronchus and mucus the middle bronchus.
..
..1 {Ii)}
FIG. 5. Postero-anterior (a) and right lateral (b) radiographs of a patient who had a carcinoma obstructing theright upper bronchus. The middle bronchus looked normal and a bougie passed distally into both divisions for aconsiderable distance. At exploratory thoracotomy, the transverse fissure was obliterated by adhesions, the rightupper lobe was distended with pus distal to a quite small central carcinoma, and the middle lobe was a shrunkenwedge, the seat of chronic non-specific inflammatory changes, presumably of long standing, and with saccularbronchiectasis of the middle lobe.
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
Opacities of the middle and upper lobes in combination
of an appropriate antibiotic-determined on theground of sensitivity of organisms in the sputum.Bronchography was undertaken in these sevenpatients at a late stage in convalescence and thebronchographic appearances were normal, as wasthe bronchial anatomy. Friedlander's bacillus wasisolated from one of the two patients with 'dis-
.0~~. .:
F
(a)
(c)
tension' of the upper and middle lobes. From onepatient pneumococci were isolated, and from theothers staphylococci.
In the two patients in whom middle and upperlobar shadows included a fluid level, the course ofthe illness was prolonged, the opacities clearedslowly, and there was clear radiographic evidence
(b)
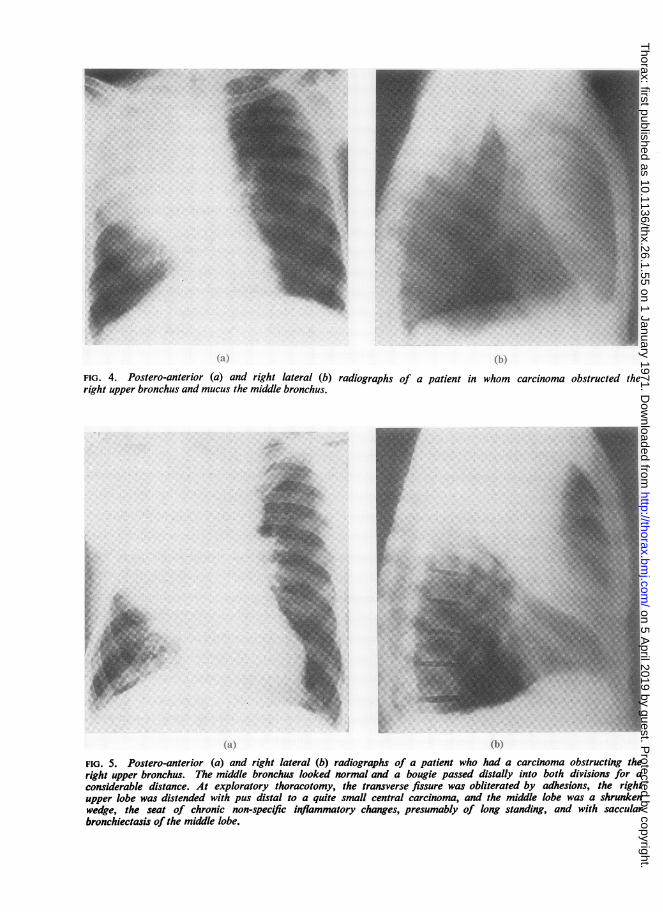
(d)FIG. 6. Legend on page 60.
.1...
59
A4.
;lw:..4.......
i...N.A
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
B. T. Le Roux
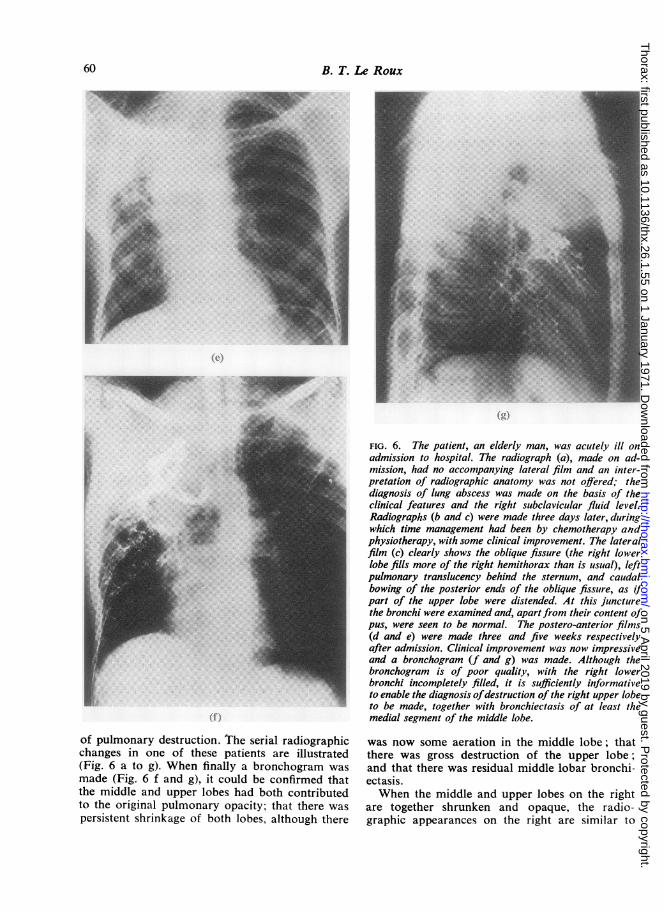
of pulmonary destruction. The serial radiographicchanges in one of these patients are illustrated(Fig. 6 a to g). When finally a bronchogram wasmade (Fig. 6 f and g), it could be confirmed thatthe middle and upper lobes had both contributedto the original pulmonary opacity; that there was
persistent shrinkage of both lobes, although there
FIG. 6. The patient, an elderly man, was acutely ill onadmission to hospital. The radiograph (a), made on ad-mission, had no accompanying lateral film and an inter-pretation of radiographic anatomy was not offered; thediagnosis of lung abscess was made on the basis of theclinical features and the right subclavicular fluid level.Radiographs (b and c) were made three days later, duringwhich time management had been by chemotherapy andphysiotherapy, with some clinical improvement. The lateralfilm (c) clearly shows the oblique fissure (the right lowerlobe fills more of the right hemithorax than is usual), leftpulmonary translucency behind the sternum, and caudalbowing of the posterior ends of the oblique fissure, as ifpart of the upper lobe were distended. At this juncturethe bronchi were examined and, apart from their content ofpus, were seen to be normal. The postero-anterior films(d and e) were made three and five weeks respectivelyafter admission. Clinical improvement was now impressiveand a bronchogram (f and g) was made. Although thebronchogram is of poor quality, with the right lowerbronchi incompletely filled, it is sufficiently informativeto enable the diagnosis ofdestruction of the right upper lobeto be made, together with bronchiectasis of at least themedial segment of the middle lobe.
was now some aeration in the middle lobe; thatthere was gross destruction of the upper lobe;and that there was residual middle lobar bronchi-ectasis.When the middle and upper lobes on the right
are together shrunken and opaque, the radio-graphic appearances on the right are similar to
ge'..
.;..
60
M.
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from
Opacities of the middle and upper lobes in combination
those on the left when the left upper lobe isshrunken and opaque.
COMMENT
In his original description of the 'double lesionsign' Felson (1960) stresses that 'one should notbe dogmatic in interpreting the double lesion sign.I have, myself, been guilty of overselling this signand, after encountering four failures in the pastfew years, have lost a little of my original faithin it.' Two of the failures were cases of bronchialcarcinoma, in one of which the tumour was in theupper lobe and there was an apparently unrelatedpneumonia of the middle lobe; and in the other,the carcinoma involved the stem bronchus with anairway to the basal bronchi. Other reasons for'failure' of the double lesion sign to make unlikelythe diagnosis of a common bronchus-obstructinglesion include multicentric neoplasm; separateareas of collapse produced by the primaryneoplasm and its metastases; extension of atumour through a fissure to involve another large
bronchus; a tumour in one location and anunrelated lesion in another; and anatomicalvariations in the distribution of bronchi. In 8 outof 17 cases the invalidity of the double lesion signas an exclusion of bronchial carcinoma servesonly to emphasize that the investigation of lobaror segmental shadows, in whatever combination,demands, at an early stage, bronchoscopy. Thatthere is bias in the selection of these cases isundeniable-all were referred to a thoracicsurgical unit from medical wards where, during aperiod of observation, the lobar opacities hadfailed to clear, and it was the chronicity of thepulmonary pathology which prompted referral. Itis not known how many quickly clearing com-bined middle and right upper lobar lesions weretreated during the period when nearly half ofthose referred for a surgical opinion were shownto be related to pulmonary carcinoma.
REFERENCE
Felson, B. (1960). Fundamentals of Chest Roen tgenology. SaundersPhiladelphia and London.
61
on 5 April 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.26.1.55 on 1 January 1971. D
ownloaded from