Embed Size (px)
Citation preview
Operation of Choice for Resectable Carcinoma of the Head of the Pancreas
Ryoichi Tsuchiya, * Tsukasa Tsunoda, and Takashi Yamaguchi
Second Department of Surgery, Nagasaki University School of Medicine, 7-1 Sakamoto-Machi, Nagasaki 852, Japan
Received April 17, 1989; Revised August 31, 1989; Accepted September 5, 1989
Summary
What is the best procedure for resectable carcinoma of the head of the pancreas? In order to respond to the question, a retrospective study was performed based on 5 I0 cases with carcinoma of the head of the pancreas that were experienced from 1975 to 1984 at nine major surgical institutions in Japan. Laparotomized cases (504) were divided into four groups accord- ing to operative procedures: pancreatoduodenectomy (PD), total pancrea- tectomy (TP), regional pancreatectomy (RP), and palliative operation (PO). The postoperative cumulative survival rate (PCSR) was calculated on each group. Although the five year survival rate of PO was 0, those of PD, TP, and RP were 11.2, 4.6, and 4.5070, respectively. There was a sig- nificant difference between PD and TP (p < 0o01) according to generalized Wilcoxon's test. TNM stage grouping was applied to 447 cases that had adequate descriptions on T, N, and M categories. PCSR was calculated on PD, TP, and RP at each stage. It was found in Stage III that survival curve of PD was significantly higher than TP (p < 0.01), according to generalized Wilcoxon's test. It seems that PD is the best procedure, but it should be accompanied by extensive lymph node and retroperitoneal tissue dissection.
Key Words: Resectional surgery; postoperative survival period; postopera- tive cumulative survival rate; TNM stage grouping.
INTRODUCTION
Most general surgeons in the world feel pessimistic when they deal with a patient with carcinoma of the pancreas since even the most extensive and aggressive operations, such as regional pancreatectomy, could not improve the operative results (1). On the other hand, there have been reports that em-
*Author to whom all correspondence and reprint requests should be addressed.
International Journal of Oancreatology �9 1990 The Humana Press Inc.
International Journal of Pancreatology 295 Volume 6, 1990
296 Tsuchiya, Tsunoda, and Yarnaguchi
phasized that total pancreatectomy was a operation of choice, and the opera- tive results were much better than pancreatoduodenectomy (2,3).
Most surgeons in Japan have tried to cure the disease by surgery, and they have performed more and more aggressive procedures. It seemed that it was the time to evaluate which procedure was the best for treatment of resectable carcinoma of the head of the pancreas, and the retrospective study was done.
MATERIAL AND METHODS
An individual case report on carcinoma of the head of the pancreas, ex- perienced during the past 10 year period from January I, 1975 to December 31, 1984, was collected from nine major surgical institutions in Japan that participated in the National Pancreatic Cancer Project Team, supported by Ministry of Health and Welfare of our government. A case report consisted of the following items: age, sex, data of operation, operative procedure, T, N, and M categories during laparotomy, histopathology of the tumor, and outcome. Case reports on 510 patients with carcinoma of the head of the pancreas were collected. Cystadenocarcinoma, islet cell tumor, and ampullary carcinoma were excluded from this study.
It has been our general strategy that even if a tumor involves regional lymph nodes or major vascular vessels and invades the pancreatic capsule or retro- peritoneal tissues, whenever it is pOssible to do en bloc resection, the tumor may be regarded as a resectable one and a resectional procedure should be performed. Operative procedures were divided into pancreatoduodenectomy (PD), total pancreatectomy (TP), regional pancreatectomy (RP), and pallia~ tive operation (PO).
Regional pancreatectomy was defined as a procedure that was either pan- creatoduodenectomy, or total pancreatectomy accompanied with resection of major vessels, mostly the main t runk of the portal vein. TNM classifica- tion in exocrine pancreatic carcinoma, proposed by the UICC in 1987 (4), was used for stage grouping of the laparotomized patients.
The letter " T " means primary tumor. T is divided into To, TI, T2, and T3. To is "no evidence of primary tumor . " TI means " tumor limited to the pan- creas." T2 is " tumors extending beyond the confines of the pancreas, involv- ing one or more of the following: duodenum, bite duct, peripancreatic fat, and /or nerves." T3 means " tumors extending beyond the confines of the pancreas, involving one or more of the following: stomach, spleen, colon, or adjacent large vessels."
The symbol " N " means lymph nodes and is divided into No and N1. No is "no evidence of regional lymph node involvement." N1 means "evidence of involvement of regional lymph nodes related to the primary t umor . "
The letter " M " means distant metastasis, which is divided into M0 and M~. M0 is "no evidence of distant metastasis." MI means "presence of dis- tant metastases."
The stages of the disease can be grouped by T, N, and M categories, as shown in Table 1. Stage I is a tumor that exhibits relatively limited disease.
International Journal o f Pancreatology Volume 6, 1990
Pancreatic Cancer Resection 297
Table 1 Stage Grouping Proposed by the UICC in 1987
Stage I T1, T2 No M0 Stage II T3 No M0 Stage III Any T N1 Mo Stage IV Any T Any N MI
Stage II is a tumor that is more advanced than Stage I, but has no lymph node involvement or distant metastases. Stage III is a tumor, regardless of T, where regional lymph node involvement is evident, but there is no distant metastasis. Stage IV means that, regardless of T and N, distant metastasis is evident.
The cumulative survival rate after surgery was calculated by Kaplan-Meier's method, and statistical significance was evaluated by generalized Wilcoxon's test. Student's t-test was used for statistical comparison of the data on opera- tive mortality rates and average survival periods. Chi-squared test was used for comparisons of sex ratio in each procedure and the number of cases (in stages) in each procedure.
RESULTS
Sex and Age
Of 5 I0 patients with carcinoma of the head of the pancreas, 334 were males and 176 were females. The male to female ratio was 1.9:1. Ages ranged from 30- to 85-yr-old with an average of 61.3 yr.
Operation
Among 510 patients, six received no surgery because of the terminal ill- ness. Out of 504 patients, 284 or 56.3~ did not receive resectional surgery but a palliative one, and resection was performed on 220 patients. Therefore, the resectability rate was 43.7~
Out of 220 patients who underwent ablative surgery, PD was performed on 107 or 48.6%. TP and RP were done on 47 or 21.4~ and 66 or 30.0o/0, respectively.
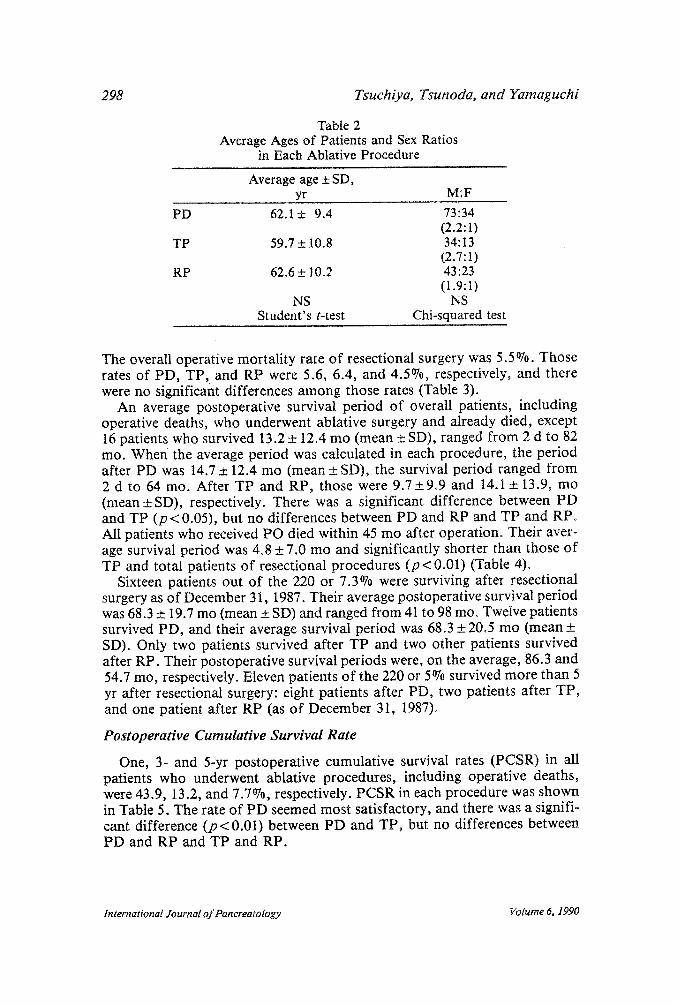
Average ages of patients and sex ratio in each ablative procedure were shown in Table 2. There were no significant differences among these procedures. The numbers of patients in each Stage of each resectional procedure were shown. Statistically, there were no differences among resectional procedures.
Operative Results
Of 504 patients who underwent laparotomy, 50 died within one month after the operation. Overall operative mortality was 9.9%. However, the highest mortality rate of 13.4~ was seen in cases of PO. Out of 220 patients who received resectional procedures, 12 operative deaths were encountered.
International Journal o f Pancreatology Volume 6, 1990
298 Tsuchiya, Tsunoda, and Yamaguchi
PD
TP
RP
Table 2 Average Ages of Patients and Sex Ratios
in Each Ablative Procedure
Average age _+ SD, yr M:F
62.1 + 9.4 73:34 (2.2:1)
59.7 _+ 10.8 34:13 (2.7:1)
62.6 +_ 10.2 43:23 (1.9:1)
NS NS Student's t-test Chi-squared test
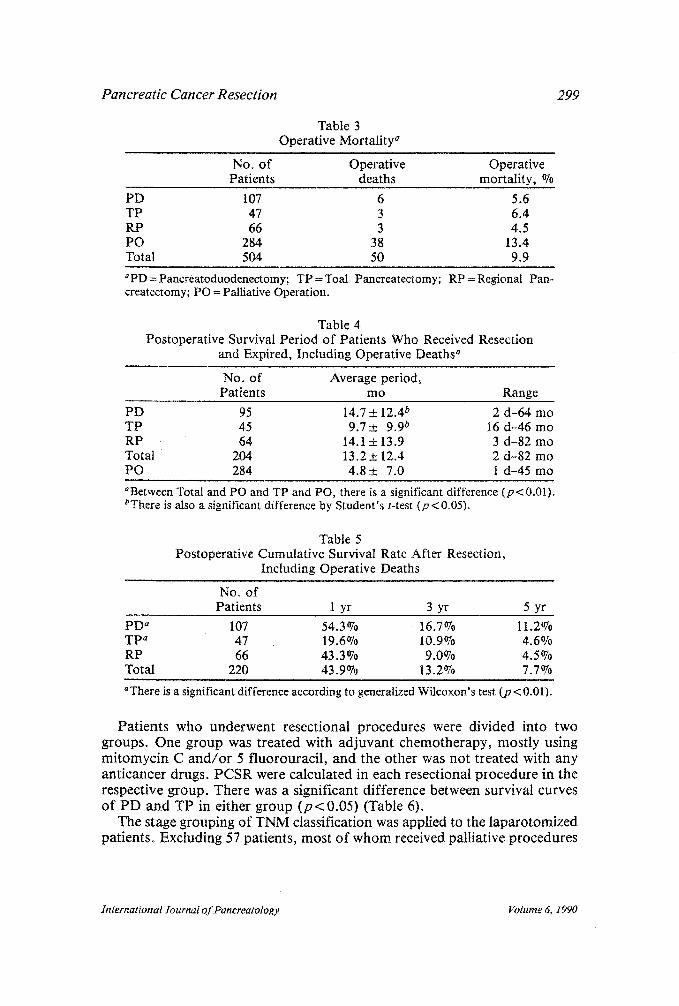
The overall operative mortality rate of resectional surgery was 5.5%. Those rates of PD, TP, and RP were 5.6, 6.4, and 4.5%, respectively, and there were no significant differences among those rates (Table 3).
An average postoperative survival period of overall patients, including operative deaths, who underwent ablative surgery and already died, except 16 patients who survived 13.2 + 12.4 mo (mean • SD), ranged from 2 d to 82 mo. When the average period was calculated in each procedure, the period after PD was 14.7 +__ 12.4 mo (mean ___ SD), the survival period ranged from 2 d to 64 mo. After TP and RP, those were 9.7+9.9 and 14.1 + 13.9, mo (mean +SD), respectively. There was a significant difference between PD and TP (p < 0.05), but no differences between PD and RP and TP and RP. All patients who received PO died within 45 mo after operation. Their aver- age survival period was 4.8 + 7.0 mo and significantly shorter than those of TP and total patients of resectional procedures ( p < 0.01) (Table 4).
Sixteen patients out of the 220 or 7.3% were surviving after resectional surgery as of December 31, 1987. Their average postoperative survival period was 68.3 +__ 19.7 mo (mean • SD) and ranged from 41 to 98 mo~ Twelve patients survived PD, and their average survival period was 68.3 • 20.5 mo (mean • SD). Only two patients survived after TP and two other patients survived after RP. Their postoperative survival periods were, on the average, 86.3 and 54.7 mo, respectively. Eleven patients of the 220 or 5% survived more than 5 yr after resectional surgery: eight patients after PD, two patients after TP, and one patient after RP (as of December 31, 1987).
Postoperative Cumulative Survival Rate
One, 3- and 5-yr postoperative cumulative survival rates (PCSR) in all patients who underwent ablative procedures, including operative deaths, were 43.9, 13.2, and 7.7%, respectively. PCSR in each procedure was shown in Table 5. The rate of PD seemed most satisfactory, and there was a signifi- cant difference ( p < 0.01) between PD and TP, but no differences between PD and RP and TP and RP.
International Journal of Pancreatology Volume 6, 1990
P a n c r e a t i c C a n c e r R e s e c t i o n
Table 3 Operative Mortality a
299
NO o of Operative Operative Patients deaths mortality, %
PD 107 6 5.6 TP 47 3 6.4 RP 66 3 4.5 PO 284 38 13.4 Total 504 50 9.9
~PD=Pancreatoduodenectomy; TP=Toal Pancreatectomy; RP=Regional Pan- createctomy; PO = Palliative Operation.
Table 4 Postoperative Survival Period of Patients Who Received Resection
and Expired, Including Operative Deaths a
No. of Average period, Patients mo Range
PD 95 14.7 _+ 12.4 b 2 d-64 mo TP 45 9.7_+ 9.9 b 16 d-46 mo RP 64 14.1 + 13.9 3 d-82 mo Total 204 13.2 _+ 12.4 2 d-82 mo PO 284 4 .8+ 7.0 1 d-45 mo
aBetween Total and PO and TP and PO, there is a significant difference (p<0.01). bThere is also a significant difference by Student's t-test (p < 0.05).
Table 5 Postoperative Cumulative Survival Rate After Resection,
Including Operative Deaths
No. of Patients 1 yr 3 yr 5 yr
PD ~ 107 54.3 0/o 16.7~ 11.2~ TP a 47 19.6070 10.9070 4.6% RP 66 43.3~ 9.0% 4.5% Total 220 43.9% 13.2~ 7.7%
aThere is a significant difference according to generalized Wilcoxon's test (p < 0.01).
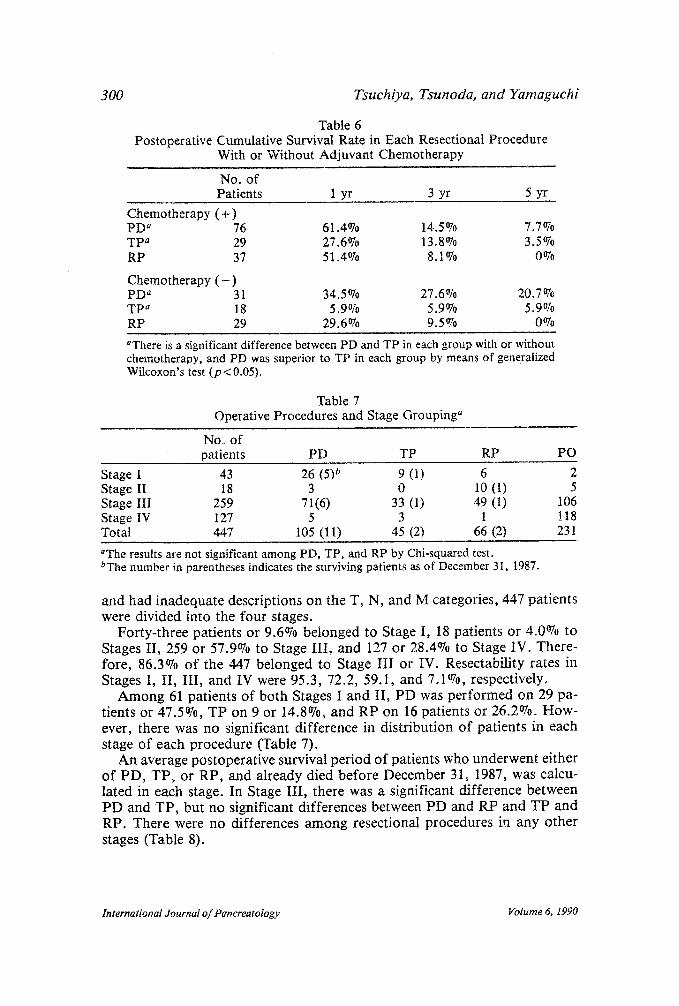
Pa t i en t s who unde rwen t resect ional p rocedures were divided into two groups . One g roup was t rea ted with a d j u v a n t ch em o th e rap y , mos t ly using m i t o m y c i n C a n d / o r 5 f luorourac i l , and the o the r was no t t r ea t ed with any an t i cancer drugs. P C S R were ca lcula ted in each resect ional p r o c e d u r e in the respect ive g roup . The re was a s ignif icant d i f fe rence between survival curves o f P D a n d T P in e i ther g roup ( p < 0.05) (Table 6).
The stage grouping o f T N M classification was applied to the l apa ro tomized pat ients . Excluding 57 pat ients , mos t o f w h o m received pall iat ive p rocedu re s
International Journal of Pancreatology Volume 6, 1990
300 Tsuchiya, Tsunoda, and Yarnaguchi
Table 6 Postoperative Cumulative Survival Rate in Each Resectional Procedure
With or Without Adjuvant Chemotherapy
No. of Patients 1 yr 3 yr 5 yr
Chemotherapy ( + ) PD a 76 61.4070 14.5~ 7.7070 TP a 29 27.6o70 13.807o 3.5% RP 37 51.4o/0 8.1% 0070
Chemotherapy ( - ) PD a 31 34.5070 27.6 o70 20.7o/0 TP a 18 5.907o 5.9o7o 5.9% RP 29 29.6o/0 9.5o70 0070
aThere is a significant difference between PD and TP in each group with or without chemotherapy, and PD was superior to TP in each group by means of generalized Wilcoxon's test (p < 0.05).
Table 7 Operative Procedures and Stage Grouping a
No. of patients PD TP RP PO
Stage I 43 26 (5) ~ 9 (1) 6 2 Stage II 18 3 0 10 (1) 5 Stage III 259 71(6) 33 (1) 49 (1) 106 Stage IV 127 5 3 1 118 Total 447 105 (11) 45 (2) 66 (2) 231
~ results are not significant among PD, TP, and RP by Chi-squared test. bThe number in parentheses indicates the surviving patients as of December 31, 1987.
and had inadequate descriptions on the T, N, and M categories, 447 patients were divided into the four stages.
Forty-three patients or 9.6~ belonged to Stage I, 18 patients or 4.0~ to Stages II, 259 or 57.9070 to Stage III, and 127 or 28.4070 to Stage IV. There- fore, 86.3% of the 447 belonged to Stage III or IV. Resectability rates in Stages I, II, III, and IV were 95.3, 72.2, 59.1, and 7.1~ respectively.
Among 61 patients o f both Stages I and II, PD was performed on 29 pa- tients or 47.5%, TP on 9 or 14.8~ and RP on 16 patients or 26.2%. How- ever, there was no significant difference in distribution of patients in each stage of each procedure (Table 7).
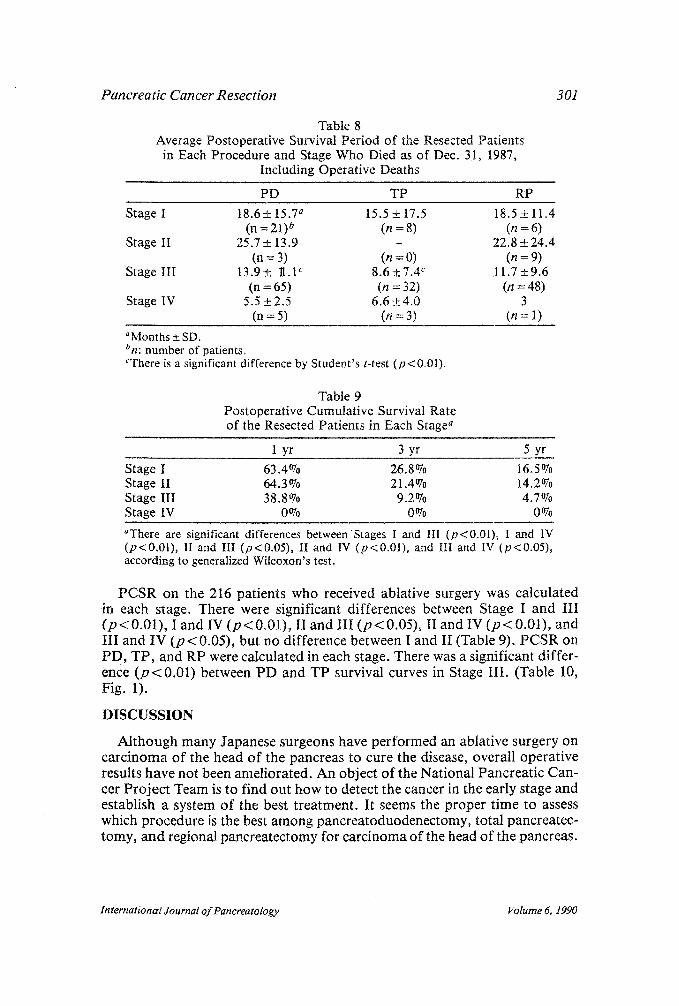
An average postoperative survival period of patients who underwent either of PD, TP, or RP, and already died before December 31, 1987, was calcu- lated in each stage. In Stage III, there was a significant difference between P D and TP, but no significant differences between PD and RP and TP and RP. There were no differences among resectional procedures in any other stages (Table 8).
International Journal of Pancreatology Volume 6, I990
Pancreatic Cancer Resection 301
Table 8 Average Postoperative Survival Period of the Resected Patients
in Each Procedure and Stage Who Died as of Dec. 31, 1987, Including Operative Deaths
PD TP RP
Stage I 18.6 _+ 15.7 a 15.5 +_ 17.5 18.5 + 11.4 (n = 21) a (n = 8) (n = 6)
Stage II 25.7 _+ 13.9 - 22.8 _ 24~ (n = 3) (n = 0) (n = 9)
Stage III 13.9_+ I1.1 c 8.6 _+ 7.4 c 11.7 +9.6 (n = 65) (n = 32) (n = 48)
Stage IV 5.5 +2.5 6.6+_4.0 3 (n = 5) (n = 3) (n = 1)
aMonths +_ SD. bn: number of patients. eThere is a significant difference by Student's t-test (p<0.01).
Table 9 Postoperative Cumulative Survival Rate of the Resected Patients in Each Stage a
1 yr 3 yr 5 yr
Stage I 63.4% 26.8% 16.5% Stage II 64.3% 21.4~ 14.2% Stage III 38.8~ 9.2% 4.7~ Stage IV 0070 0070 0070
aThere are significant differences betweenStages I and III (p<0.01), I and IV (p<0.01), II and III (p<0.05), II and IV (p<0.01), and III and IV (p<0.05), according to generalized Wilcoxon's test.
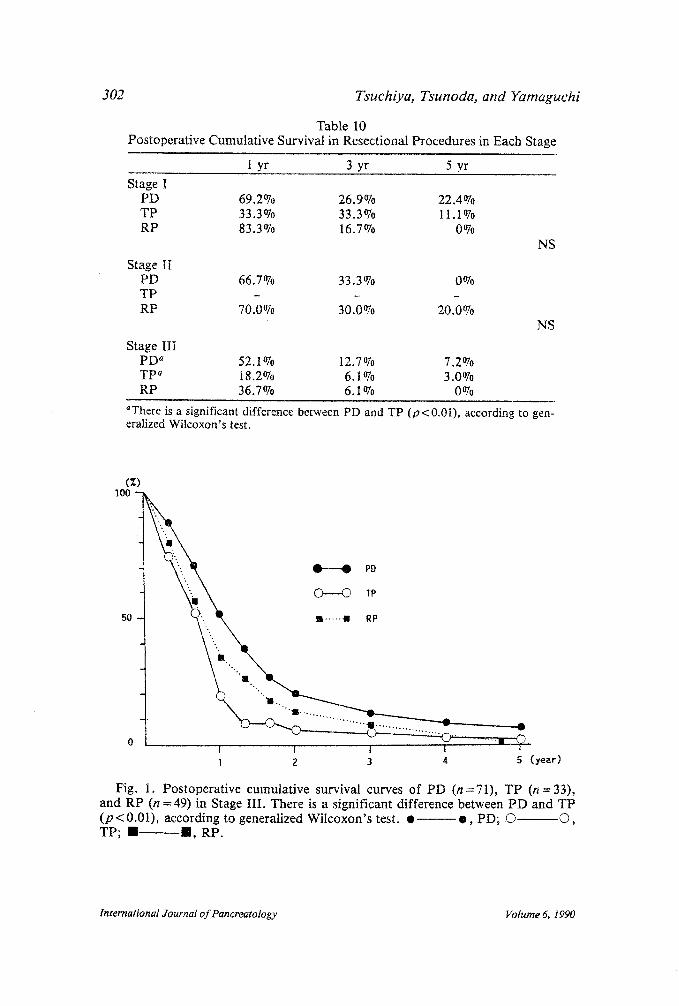
PCSR on the 216 patients who received ablative surgery was calculated in each stage. There were significant differences between Stage I and III (p<0 .01) , I and IV (p<0 .01) , II and III ( p < 0.05), II and IV (p < 0.01), and III and IV (p < 0.05), but no difference between I and II (Table 9). PCSR on PD, TP, and RP were calculated in each stage. There was a significant differ- ence (p<0 .01 ) between PD and TP survival curves in Stage III. (Table 10, Fig. 1).
DISCUSSION
Although many Japanese surgeons have performed an ablative surgery on carcinoma of the head of the pancreas to cure the disease, overall operative results have not been ameliorated. An object of the National Pancreatic Can- cer Project Team is to find out how to detect the cancer in the early stage and establish a system of the best treatment. It seems the proper time to assess which procedure is the best among pancreatoduodenectomy, total pancreatec- tomy, and regional pancreatectomy for carcinoma of the head of the pancreas.
International Journal of Pancreatology Volume 6, 1990
302 Tsuchiya, Tsunoda, and Yamaguchi
Table 10 Postoperative Cumulative Survival in Resectional Procedures in Each Stage
1 yr 3 yr 5 yr
Stage I PD 69.2% 26.9070 22.407o TP 33.3% 33.3% 11.1% RP 83.3% 16.7% 0%
Stage II PD 66.7% 33.3% 0% TP - - - RP 70.0% 30.0% 20.0%
Stage III PD a 52.1~ 12.707o 7.2% TP ~ 18.2% 6.1% 3.0070 RP 36.7% 6.1% 0%
NS
NS
~Tbere is a significant difference between PD and TP (p< 0.01), according to gen- eralized Wilcoxon's test~
(z) Ioo
50
i i i i z
1 2 3 4 5 (year)
Fig. 1. Postoperative cumulative survival curves of PD (n=71), TP (n=33) , and RP (n = 49) in Stage III. There is a significant difference between PD and TP (p<0 .01) , according to generalized Wilcoxon's test. �9 o , PD; (3 (D, TP; !1 ......... I I , RP.
International Journal of Pancreatology Volume 6, 1990

Pancreatic Cancer Resection
Table 11 Pancreatic Cancer Registry Ca. the Head of the Pancreas
303
1981 1982 1983 1984 1985 Total
Total no. 598 340 437 443 455 2273 No. of laparotomy 564 316 411 413 419 2123 No. of resection 221 148 220 189 242 1020 Resectability 39.2~ 46.8~ 53.5~ 45.8~ 57.8~ 48.0~
The resectability rate out of 504 laparotomized cases was 43.7~ This is not a surprisingly high rate at all. Pancreatic cancer registry in Japan (5) from 1981-1985 shows that the overall resectability rate of laparotomized cases with carcinoma of the head of the pancreas (48.0%) ranged from 39.207o in 1981 to 57.8% in 1985, as shown in Table 11.
The present study showed that an average operative mortality rate within one month postoperative was 5.5% in the resectional surgery, and even that of RP was 4.5%. These facts simply reflect the developments of operative and postoperative managements in Japan.
The average postoperative survival period of patients who underwent ablative surgery and already died was significantly longer than the period of patients who received PO. Among patients receiving a resectional procedure, patients of PD had a significantly longer survival period than patients of TPo As of December 31, 1987, 12 patients were surviving PD, 2 patients surviving TP, and 2 RP~ Besides, 8 patients after PD, 2 patients after TP, and 1 after RP survived more than 5 yr, as of December 31, 1987. As for the postopera- tive cumulative survival curve, again there was a significant difference be= tween PD and TP, and PD was better than TP. Therefore, it seemed that PD is the most satisfactory procedure among resectional procedures.
Some patients who underwent ablative surgery were treated by postopera- tive chemotherapy and others not, but without any intention. It was suspected that there might have been some influence on the prognosis of patients who received a resectional procedure.
The patients were divided into two groups: one with postoperative adju- vant chemotherapy, the other without it, and the postoperative cumulative survival curve was calculated in each procedure of each group. A significant difference was found between PD and TP in each group, and the postopera- tive survival rate of PD was better than TP.
Yet, there was a question whether PD was performed mostly on younger stages of the disease. Therefore, stage grouping of TNM classification, pro- posed by the UICC (4) in 1987, was applied. It seemed that PD was done mostly on patients of the early stages, that is, on 29 of 61 patients with Stage I and II or 47.5~ However, the proportion of the 29 to the number of pa- tients who received PD was 27.6%. Those proportions of Stages I and II to the numbers of patients who underwent TP and RP were 20 and 24.2%, respectively. There seemed no significant difference among them. Statisti-
International Journal o f Pancreatology Volume 6~ 1990
304 Tsuchiya, Tsunoda, and Yamaguchi
cally, there were no significant differences among the numbers of patients in each procedure of the stages.
Stage grouping proposed by the UICC seemed useful for the assessment of the disease prognosis. There were significant differences among postopera- tive cumulative survival curves of Stages I, III, and IV and among Stages II, III, and IV although there was no significant difference between Stages I and II. It also may be concluded that a prognosis of patients in Stage IV cannot be improved by any resectional procedures, and we must give up to perform ablative surgery on Stage IV patients.
Average postoperative survival periods of each resectional procedure were calculated in each stage. In Stages I, II, and IV, there were no significant dif- ferences among PD, TP, and RP, but in Stage III, an average survival period after PD was significantly longer than TP.
Finally, postoperative cumulative survival curves were calculated on each resectional procedure in each stage. In Stages I, II, and IV, there was no sig- nificant difference among PD, TP, and RP. However, in Stage III, the post~ operative cumulative survival curve of PD was significantly better than TP. Postoperative, 5-yr survivals in this series were four patients in Stage I and four patients in Stage III after receiving PD, one patient in Stage I, and one patient in Stage III after TP, and one patient in Stage II after RP.
As mentioned earlier, most Japanese surgeons have tried to cure the dis- ease by operation, and they have performed more aggressive resectional pro- cedures. Although their operative results have not been ameliorated, as shown in this study, that is the postoperative cumulative 5-yr survival rate of the patients who received ablative surgery, was merely 7.7O7o. However, they have become knowledgeable on the pathology of the carcinoma, that is, ex- tensions of the cancerous invasion, favorite site of lymph node metastasis, popular places of recurrence, and so on, and they have considered that it is important to do extensive dissection of lymph nodes and retroperitoneal tissues whenever they performed resectional surgery on pancreatic cancer.
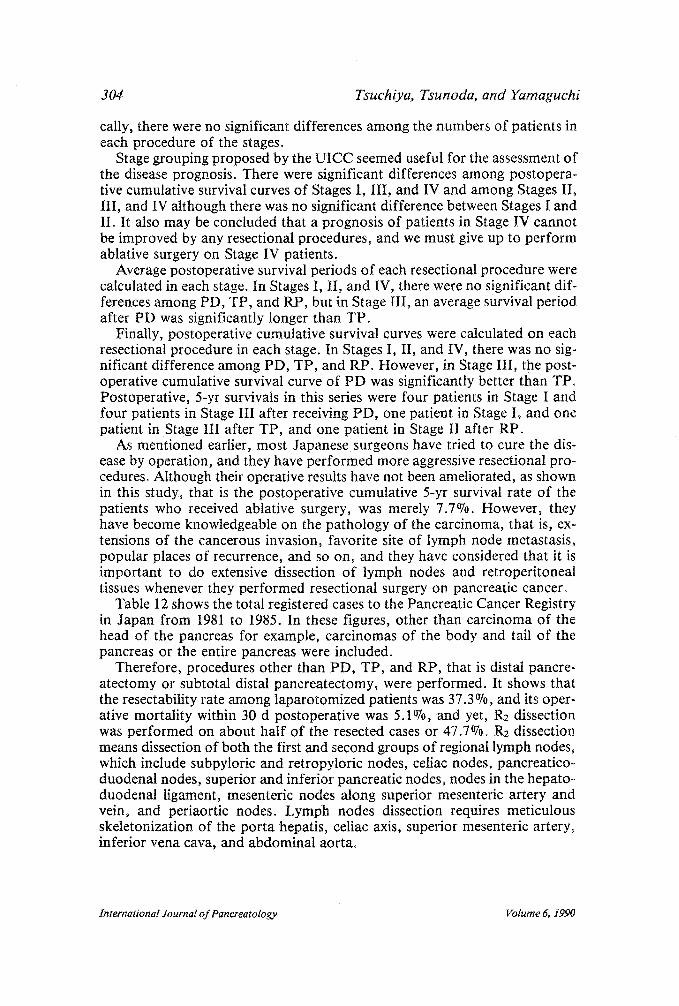
Table 12 shows the total registered cases to the Pancreatic Cancer Registry in Japan from 1981 to 1985. In these figures, other than carcinoma of the head of the pancreas for example, carcinomas of the body and tail of the pancreas or the entire pancreas were included.
Therefore, procedures other than PD, TP, and RP, that is distal pancre- atectomy or subtotal distal pancreatectomy, were performed. It shows that the resectability rate among laparotomized patients was 37.3O70, and its oper- ative mortality within 30 d postoperative was 5.1O70, and yet, R2 dissection was performed on about half of the resected cases or 47.7~ Rz dissection means dissection of both the first and second groups of regional lymph nodes, which include subpyloric and retropylofic nodes, celiac nodes, pancreatico- duodenal nodes, superior and inferior pancreatic nodes, nodes in the hepato- duodenal ligament, mesenteric nodes along superior mesenteric artery and vein, and periaortic nodes. Lymph nodes dissection requires meticulous skeletonization of the porta hepatis, celiac axis, superior mesenteric artery, inferior vena cava, and abdominal aorta.
International Journal of Pancreatology Volume 6, 1990
Pancreatic Cancer Resection
Table Pancreatic Cancer Registry of
305
12 the Japan Pancreas Society
1981 1982 1983 1984 1985 Total
Total no. 1191 814 1075 1067 1070 5217 No. of laparotomy 941 617 818 790 782 3948 Rate of laparotomy, ~ 79.0 75.8 76.1 74.0 73.1 75.7 No. of resection 292 211 318 295 355 1471 No. of PD 137 97 148 137 176 695 No. of TP 57 32 47 35 43 214 No. of RP 56 45 73 55 80 309 No. of others 42 37 50 68 56 253 Resectability rate, % 31.0 34.2 38.9 37.3 45.4 37.3 No. of op. deaths 19 16 24 5 11 75 Op. mortality rate, % 6.5 7.6 7.5 1.7 3.1 5.1 No. of R2 118 112 156 135 181 702 Rate of R2, %a 40.4 53.1 49.1 45.8 51.0 47.7
aR2: Extension of lymph node dissection of the second group of regional lymph nodes, includ- ing subpyloric and retropyloric nodes, celiac nodes, pancreaticoduodenal nodes, superior and inferior pancreatic nodes, nodes in the hepatoduodenal ligament, mesenteric nodes along superior mesenteric artery and vein, and periaortic nodes.
Therefore, it shoiuld be considered that, in the present study, about half the patients who received a resectional procedure may have undergone R2 dissection, and on this assumption, PD is thought to be the best procedure for carcinoma of the head of the pancreas from Stages I to III. However, the results are not satisfactory at all. In order to improve a postoperative 5-yr survival rate, adjuvant chemotherapy and/or radiotherapy should be com- bined with resectional surgery.
Of 66 patients who received RP, one patient survived more than 5 years after surgery, and two others were surviving more than 4 years postoperatively at the closing day of the study. In these three patients, cancerous involvement on the portal vein was suspected at the time of operation, but no invasion to the wall of the portal vein was microscopically found by the histopathological examination of the resected specimen in two patients, and the adventitial in- vasion was detected in one. Even if the portal vein involvement is suspected at the time of surgery, there is a possibility of survival for a long period of time postoperatively when it is removed.
ACKNOWLEDGMENTS
The authors deeply appreciate the cordial cooperation of the following members of the National Cancer Project Team who submitted their valuable case reports: T. Hiraoka, 1st Department of Surgery, Kumamoto University Hospital; R. Mizumoto, 1 st Department of Surgery, Mie University Hospital; T. Nagakawa, 2nd Department of Surgery, Kanazawa University Hospital; Y. Ogata, Department of Surgery, Keio University Hospital; H. Ozaki, De- partment of Surgery, National Cancer Center; Y. Saitoh, 1st Department of
International Journal of Pancreatology Volume 6, 1990
306 Tsuchiya, Tsunoda, and Yamaguchi
Surgery, Kobe University Hospital; T. Sato, 1st Department of Surgery, Tohoku University Hospital; and K. Sugawara, 1st Department of Surgery, Yamanashi Medical College.
This work was supported, in part, by a Grant in Aid for Cancer Research (60-5) from the Ministry of Health and Welfare of the Japanese Government~
REFERENCES
1 Fortner JG. Regional pancreatectomy for cancer of the pancreas, ampulla and other related sites. Tumor staging and results. Ann. Surg. 1984; 199: 418-425.
2 Brooks JR, Culebras JM. Cancer of the pancreas. Palliative operation, Whipple proce- dure, or total pancreatectomy? Am. J. Surg. 1976; 131: 516-520.
3 Moossa AR, Scott MH, Lavelle-Jones M. The place of total and extended total pancre- atectomy in pancreatic cancer. World J. Surg. 1984; 895-899.
4 UICC. TNM classification of malignant tumours, 4th edition, Springer-Verlag, 1987. 5 Japan Pancreas Society. Report of pancreatic cancer registry, 1981-1985 (in Japanese).
International Journal o f Pancreatology Volume 6, 1990