Embed Size (px)
Citation preview
Opinions and Clinical Practices Related to Diagnosing andManaging Patients with Psychogenic Movement Disorders: AnInternational Survey of Movement Disorder Society Members
Alberto J. Espay, MD, MSc,1* Linda M. Goldenhar, PhD,2 Valerie Voon, MD,3 Anette Schrag, MD,PhD,4 Noel Burton, MA,1 and Anthony E. Lang, MD, FRCPC5
1Movement Disorders Center, Department of Neurology, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA2Office of Medical Education Evaluation and Research, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA
3National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland, USA4Department of Clinical Neurosciences, Royal Free and University College Medical School, London, United Kingdom
5Movement Disorders Division, Division of Neurology, University of Toronto, Toronto, Canada
Abstract: Five hundred and nineteen members of theMovement Disorder Society completed a 22-item question-naire probing diagnostic and management issues in psycho-genic movement disorders (PMD). When patients showeddefinite evidence of PMD with no other unexplained clinicalfeatures, approximately 20% said they informed patients ofthe diagnosis and requested no further neurological testing.The 51% who reported conducting standard neurologicalinvestigations to rule out organic causes before presentingthe diagnosis to such patients had fewer years of fellowshiptraining and fewer PMD patients seen per month. A non-PMD diagnosis was correlated with patients’ normal social orpersonal functioning, little or no employment disruption, lackof non-physiologic findings, and lack of psychiatric history.Ongoing litigation was more predictive of the PMD diagnosisfor US compared to non-US respondents. Two thirds ofrespondents, more commonly younger and academic clinician
researchers, refer PMD patients to a psychiatrist or mentalhealth specialist while also providing personal follow up.Physician reimbursement, insurability of PMD patients, andongoing litigation interfered with managing PMD patients toa greater extent in the US compared to non-US countries.Acceptance of the diagnosis by the patient and identificationand management of psychological stressors and concurrentpsychiatric disorders were considered most important for pre-dicting a favorable prognosis. These findings suggest thatexpert opinions and practices related to diagnosing and man-aging PMD patients differ among movement disorders neu-rologists. Some of the discrepancies may be accounted for byfactors such as training, type of practice, volume of patients,and country of practice, but may also reflect absence of prac-tice guidelines. � 2009 Movement Disorder SocietyKey words: psychogenic movement disorders; medically
unexplained symptoms; survey
Psychogenic movement disorders (PMD) are invol-
untary movements that cannot be attributed to known
organic causes, and which have a significant psycho-
logical or psychiatric contribution.1 The number of
patients with PMD is substantial, estimated to be as
high as 25% in specialized movement disorders clin-
ics.2 Although criteria for diagnosing PMD have been
published,3–5 little is known about neurologists’ acqui-
sition and delivery of diagnosis, extent of testing, use
of ancillary services, as well as treatment and long-
term follow up practices. Physician-related factors such
as training and gender; patient-related factors such as
type of movement disorder and degree of disability;
and ecological factors such as type of practice and
medico-legal environment may introduce substantial
variability in practice behaviors. We sought the opin-
ions of practicing neurologists experienced in PMD
Potential conflict of interest: None reported.The Movement Disorder Society helped distribute the survey to its
members but did not participate as sponsor.
Additional Supporting Information may be found in the onlineversion of this article.
*Correspondence to: Dr. Alberto J. Espay, University of Cincin-nati, 260 Stetson St., Suite 2300, Cincinnati, OH 45267-0525.E-mail: [email protected]
Received 6 November 2008; Revised 26 February 2009; Accepted25 March 2009
Published online 7 May 2009 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.22618
1366
Movement DisordersVol. 24, No. 9, 2009, pp. 1366–1374� 2009 Movement Disorder Society

and other movement disorders to understand their
beliefs and practices related to diagnosing and manag-
ing patients with PMD.
METHODS
A small group of PMD experts met to identify
knowledge gaps (Supporting Table 1, available online),
develop research questions related to caring for PMD
patients, and create a preliminary questionnaire to col-
lect valid data to address these. After multiple itera-
tions, the questionnaire underwent independent external
expert review to assure content and face validity. Final
changes were made based on feedback received. An
e-mail message from the Movement Disorder Society
(MDS) requesting participation in this study was sent
to all 2,106 MDS members. A hyperlink to Survey
Monkey embedded within the e-mail, when clicked
took the respondents to the final 22-item online ques-
tionnaire (Supporting Table 2, available online), which
they completed anonymously. Survey Monkey (http://www.surveymonkey.com/) is an internet-based tool to
gather information quickly and inexpensively from tar-
geted groups. Only practicing neurologists experienced
in evaluating patients with PMD and other movement
disorders were asked to complete the survey. Members
were asked to complete the questionnaire within 2
weeks and a reminder was sent after 1 week.
Statistical Analyses
The survey data were downloaded into SPSS statisti-
cal program (SPSS v. 11.5). Responses were examined
with descriptive statistics including frequencies, corre-
lations, difference between proportions, and chi-square
analysis and to assess the degree to which the results
varied by demographic factors (i.e., gender, age, train-
ing length, patient load, type of practice, location of
practice, and years of practice). We also investigated if
there were response differences depending on whether
the respondents practiced in the US or in other coun-
tries (‘‘non-US’’), limited to Europe and Canada given
the small number of respondents from other countries.
RESULTS
Five hundred and nineteen members completed the
on-line anonymous survey. The response rate was 25%
of all MDS member recipients; we estimate they repre-
sent approximately 40 to 50% of all practicing move-
ment disorders neurologists experienced in PMD. De-
mographic features are listed in Table 1.
On a per-month basis, approximately 30% reported
seeing more than 80 patients with any movement disor-
der, and 20% reported seeing more than three patients
with a PMD. The number of patients seen with any
movement disorder was directly correlated with the
number of PMD diagnoses per month (Kendall’s Tau 50.184; P 5 0.01). Tremor was the most common PMD
reported. Sixty-eight percent of respondents reported an
underlying organic MD or an underlying neurologic dis-
order in 1 to 10% of cases seen (Table 2).
Reaching the Diagnosis
Only a very small number of respondents believed
that their role in caring for patients with PMD was re-
stricted to diagnosis (3%) or diagnosis and personal
management of patient care (5%). A majority believed
their role was to diagnose and coordinate interdiscipli-
nary long-term management (40%) or diagnose and
attempt to secure expert management (52%). Most
respondents (71%) involve psychiatrists or other men-
TABLE 1. Demographics of respondents
Demographic variables N %
GenderMale 313 68Female 150 32
Age25–35 72 1636–45 172 3746–55 144 3156–65 59 13‡66 16 4
CountryUS 199 43Europe 1 Canada 149 32Others in sample (combined) 118 25(South America, Russia, Oceania,
Middle East, Asia, and other)Years in practice (Post-Residency)�5 yr 110 246–10 yr 88 1911–15 yr 85 1816–20 yr 67 14>21 yr 114 25
Length of fellowship trainingNone 92 201 yr 100 222 yr 126 283 yr 52 114 yr 89 19
Type of practiceAcademic clinician 133 29Academic clinician/researcher 255 55Community practice 77 17
Practice settingSmall center 14 3City – Population > 50K 161 35City – Population > 1 million 285 62
1367PSYCHOGENIC MOVEMENT DISORDERS
Movement Disorders, Vol. 24, No. 9, 2009

tal health specialists to assess underlying psychopathol-
ogy before discussing the diagnosis directly with the
patient.
An electrophysiology laboratory is not available to
one fourth of all respondents (24%) to confirm the
myoclonus or tremor forms of PMD; an additional
9% do not believe it useful for this purpose. For the
remaining two thirds with access to electrophysiology
testing, most use it only to confirm the diagnosis
when clinical examination alone is insufficient (i.e., in
uncertain cases) and almost 40% say they never or
rarely use the test results to explain the diagnosis to
the patient while 21% say they use it often or
always.
While close to 70% of respondents indicated that
incongruity with a classical movement disorder and
presence of psychogenic signs on neurologic examina-
tion were ‘essential or absolutely necessary’ findings to
establish a clinically definite diagnosis of PMD, only
18% needed evidence of an emotional disturbance and
substantially fewer, an obvious psychiatric disturbance
(8%) (Supporting Fig. 1, available online). Respond-
ents reported using suggestion (guiding or encouraging
a change in the movement) sometimes (34%), often
(30%), or always (17%) to document and diagnose
PMD; almost as many said they would never (51%) or
rarely (24%) use placebo (using an inert intravenous or
oral drug to resolve or worsen a movement) to do so.
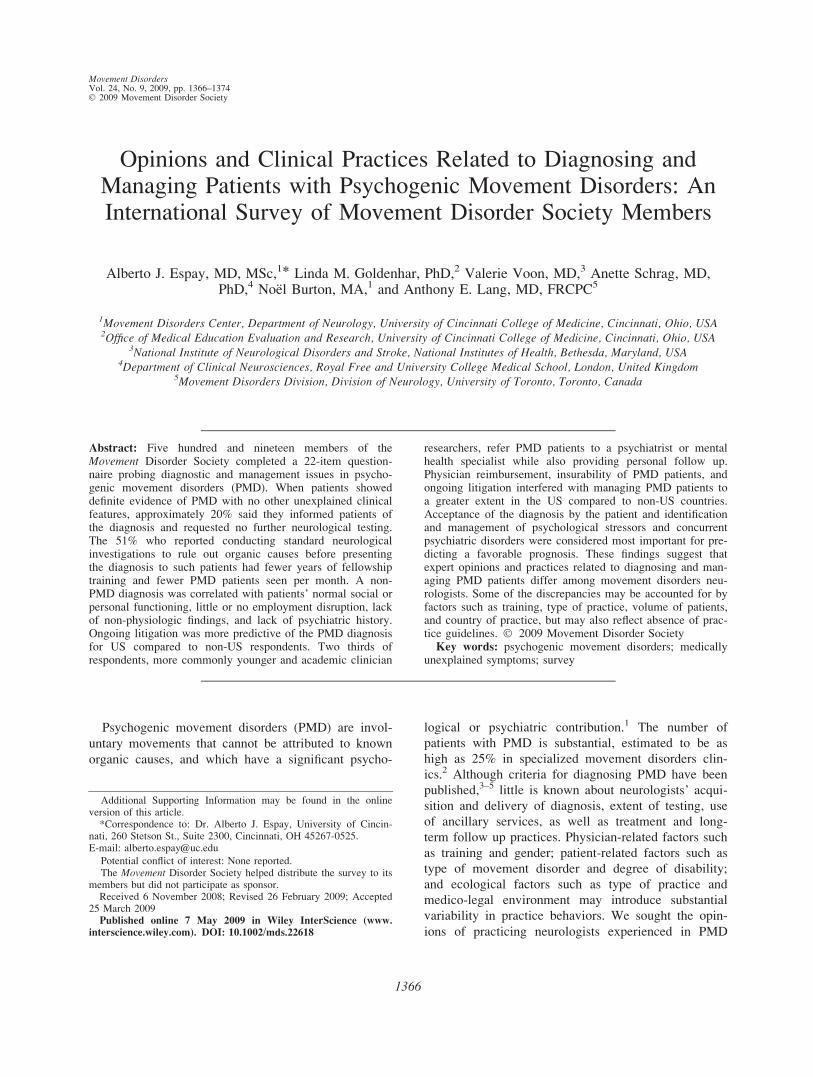
Half of all participants (51.3%) request further standard
neurological investigations to rule out organic causes
in patients already fulfilling criteria for clinically defi-
nite PMD (with no other unexplained clinical features)
before informing the patients of the diagnosis. This
practice was associated with shorter fellowship training
(v2, 12.3, P 5 0.02) and fewer PMD patients seen per
month (v2, 10.2, P 5 0.04) but not with type or years
of post-residency practice. The reduction of diagnostic
certainty from clinically definite to clinically probable
did not substantially influence this behavior, although
the proportion of neurologists that disclose the diagno-
sis without standard investigations fell from almost 20
to 2% (Fig. 1).
There were also differences in diagnostic approach
between countries. Compared with non-US countries,
US respondents more frequently inform patients of the
definite diagnosis at the initial evaluation without
requesting neurological investigations (30 vs. 15%;
P < 0.001).
Predictors of the Diagnosis
Most respondents rated excessive loss of function or
disability relative to examination findings as ‘very pre-
dictive’ (45%) or ‘extremely predictive’ (16%) of a
PMD diagnosis. This observation correlated with
extensive normal or inconclusive neurological investi-
gations (r 5 0.36; P < 0.001) and the presence of
other medically unexplained symptoms (r 5 0.31; P <0.001) in predicting a PMD diagnosis. Normal investi-
gations were reported as more common among those
with non-physiologic findings on exam (e.g., give-
away weakness) (r 5 0.37; P < 0.001). In contrast,
extremes of age were ‘very influential’ for a non-PMD
diagnosis, which correlated with lack of non-physio-
logic findings and lack of psychiatric history (r 50.51, P < 0.001) as well as little or no employment
disruption and normal social or personal function (r 50.69; P < 0.001).
The degree of how predictive certain diagnostic cri-
teria were for PMD differed between practicing neurol-
ogists in the US versus non-US countries. Specifically,
to a greater extent for US respondents ongoing litiga-
tion (83/191 5 92% vs. 44/143 5 31%; P 5 0.02),
TABLE 2. Distribution and nature of patients seen
N %
Number of patients with PMD seen per month<1 148 321–3 220 484–6 63 147–10 26 5>11 6 1
Number of all MD patients seen per month<30 63 1431–45 100 2246–60 82 1861–80 82 18>80 133 29
Frequency of PMD reported in practiceTremor 237 50.5Gait disorder 123 26.2Dystonia 51 10.9Myoclonus 38 8.1Tics 8 1.7Parkinsonism 7 1.5Chorea 5 1.1
Coexistent organic movement disorderNever 27 61–5% 175 386–10% 136 3011–20% 91 2021–40% 26 6>40% 4 1
Coexistent organic neurologic disorderNever 56 121–5% 198 436–10% 115 2511–20% 70 1521–40% 17 4>40% 5 1
1368 A.J. ESPAY ET AL.
Movement Disorders, Vol. 24, No. 9, 2009
spontaneous remissions/cures (173/195 5 89% vs.
117/147 5 80%; P 5 0.02), non-physiologic deficits
(173/193 5 90% vs. 117/146 5 80%; P 5 0.01), and
history of mental health problems or psychological
stressors (73/195 5 37% vs. 35/148 5 24%; P 50.006) were ‘somewhat,’ ‘very,’ or ‘extremely’ predic-
tive of PMD.
Approach to Management
Two thirds of respondents refer PMD patients to a
psychiatrist or mental health specialist while also pro-
viding personal follow up. This practice was similarly
frequent among those who request neurological investi-
gations before disclosing the diagnosis (67%) and those
who do not (63%), in the context of clinically definite
PMD. The pattern of referral and personal follow up
was associated with age (younger respondents provid-
ing follow-up; v2, 10.7; P 5 0.03) and type of practice
(academic clinician researchers vs. community practice
neurologists providing follow-up; v2, 16.6; P < 0.001)
but not with other demographic factors. Of interest,
50% of respondents reported that psychiatrists, psy-
chologists, or rehabilitation specialists ‘sometimes’
(35%), ‘often’ (14%) or ‘always’ (1%) question the
neurologists’ original diagnosis and recommend the
neurological basis for the disorder be reconsidered.
Perceived Effectiveness of Treatment Strategies
Only two management modalities were believed to
be ‘very’ or ‘extremely effective’ by approximately 1/3
or more of respondents: avoiding iatrogenic harm
(46%) and educating the patient (29%) (Table 3). A
majority of respondents ranked as ‘mostly not effec-
tive’ or ‘not at all effective’ pharmacological treatment
and alternative or complementary therapies. ‘Educating
the patient about PMD’ was the only strategy per-
ceived by US respondents it to be more effective com-
pared non-US respondents (v2, 10.21, P 5 0.037).
Limitations in Ability to Manage PMD Patients
Cultural beliefs about psychological illnesses (40%),
ongoing litigation (37%), and availability of referral
services (33%) were selected as ‘often’ or ‘always’
limiting the ability to manage patients. The largest
consensus for ‘never’ affecting PMD management was
for physician reimbursement (50%) and insurability of
PMD patients (42%) (Supplementary Table 3).
There were between-country differences about per-
ceptions related to treatment and management factors.
Compared to non-US countries, US respondents
believe that reimbursement (22/195 5 11% vs. 5/143
5 3%; P < 0.0001), insurability (29/193 5 15% vs.
7/143 5 5%; P < 0.003), availability of referral serv-
FIG. 1. Approach to delivering the diagnosis in clinically definite (black bars) and clinically probable (gray bars) PMD.
1369PSYCHOGENIC MOVEMENT DISORDERS
Movement Disorders, Vol. 24, No. 9, 2009
ices (82/195 5 42% vs. 38/144 5 26%; P 5 0.003),
ongoing litigation by the patient (93/196 5 47% vs.
38/144 5 26%; P < 0.0002), and potential for litiga-
tion involvement of the physician (40/195 5 21% vs.
16/145 5 8%; P 5 0.02) were ‘often’ or ‘always’
likely to affect physicians’ ability to treat and manage
patients with PMD.
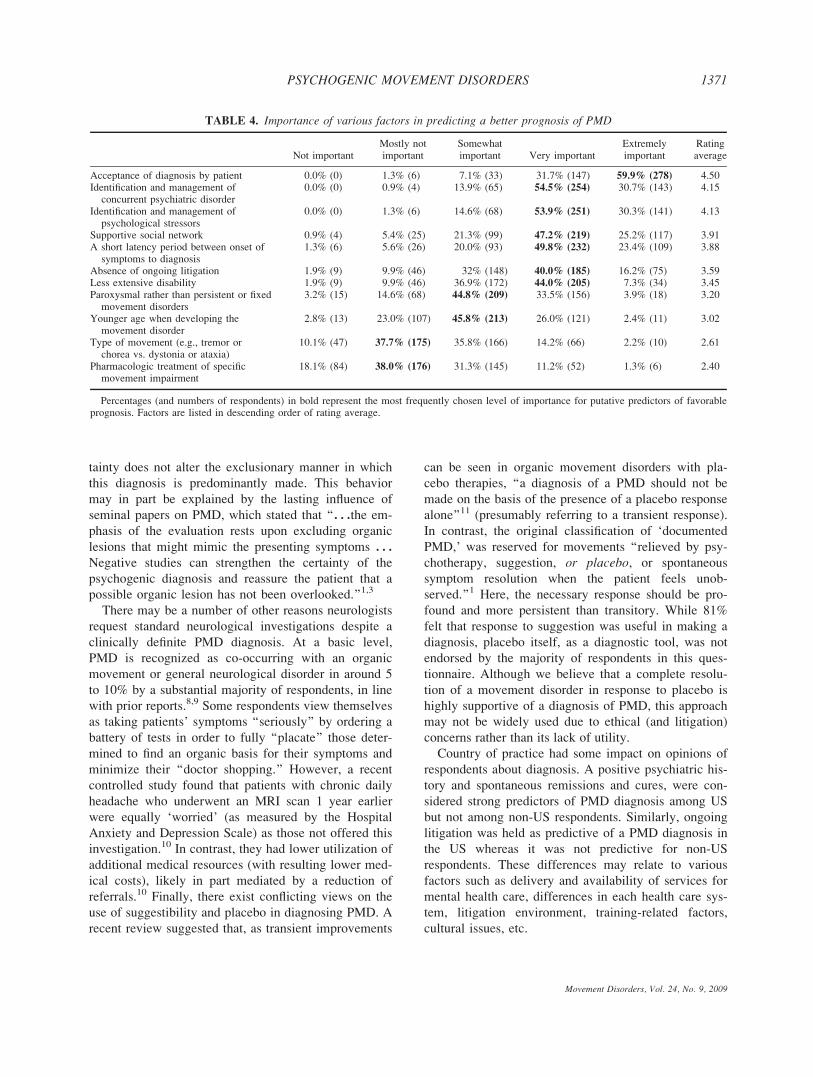
Predictors of Prognosis
Acceptance of the diagnosis by the patient was the
only variable endorsed as ‘extremely important’ (60%)
in predicting a favorable prognosis. Identification and
management of psychological stressors (54%) and con-
current psychiatric disorders (55%) were rated as ‘very
important.’ (Table 4). There were between-country dif-
ferences in perceptions of prognostic predictors. Com-
pared to non-US countries, a greater percentage of US
respondents believe that the absence of ongoing litiga-
tion (v2 5 9.6; P < 0.05) as well as the identification
and management of psychological stressors (v2 511.4; P < 0.01) and associated psychiatric disorders
(v2 5 13.8; P 5 0.003) were important for predicting
a favorable prognosis.
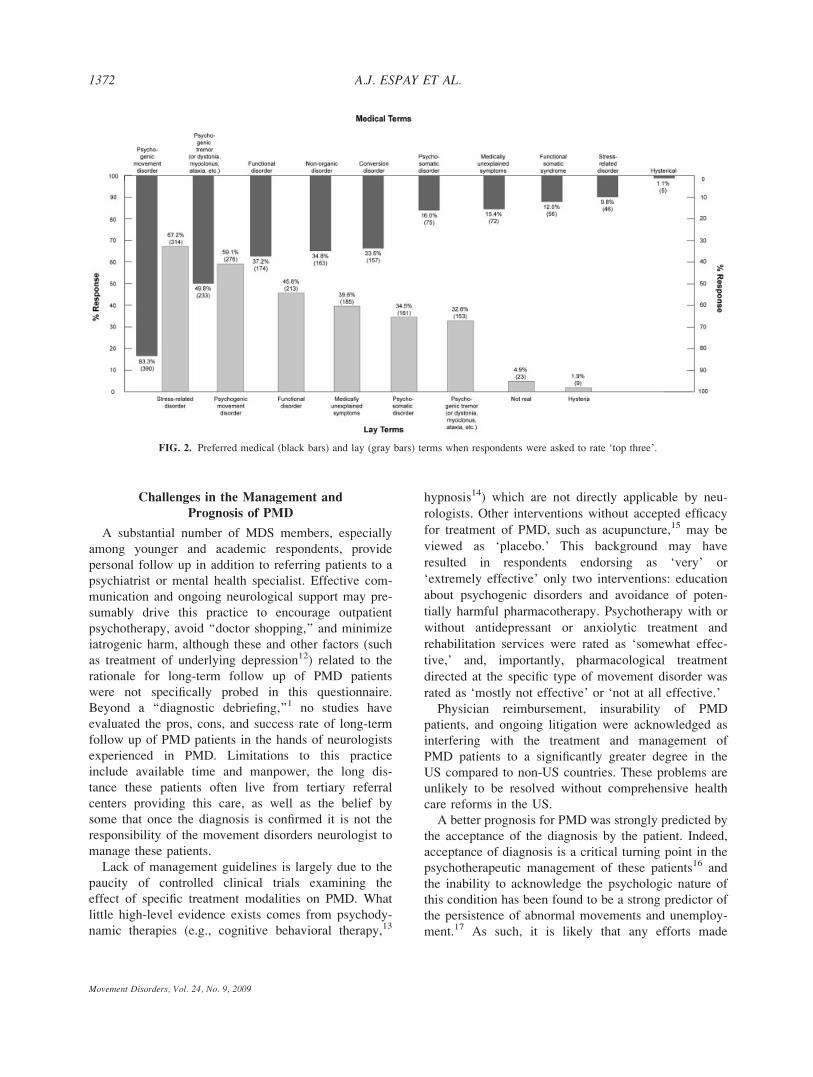
Although ‘‘psychogenic movement disorder’’ was the
preferred medical term (84%), other terminologies
were variably endorsed by respondents (Fig. 2). These
and relevant open-ended responses related to diagnos-
tic, management and prognosis issues are listed in the
Supplemental Table 4 (available online).
DISCUSSION
Expert opinions and practices regarding diagnosis
and management of PMD patients differed among neu-
rologists with movement disorders expertise. Some of
the discrepancies were partly accounted for by length
of training (e.g., investigations prior to diagnosis), type
of practice (e.g., referral pattern to psychiatrists or
mental health specialists), and country, but also
reflected absence of uniform practice guidelines. Psy-
chiatric history, a classic component of the diagnostic
background, was held as neither sensitive nor specific
for the diagnosis of PMD: it wasn’t necessary to estab-
lish the diagnosis for the vast majority of respondents
but its absence discouraged it. Added difficulty comes
from the findings that some features typically associ-
ated with recognized movement disorders may be seen
in patients with otherwise definite PMD (e.g., geste
antagoniste),6 classic diagnostic electrophysiologic
findings may be lacking (e.g., psychogenic tremor may
not always be associated with complete coherence),
and overt psychiatric problems are often absent.7 Per-
haps these factors may partly explain the limited reli-
ance of movement disorders neurologists on emotional
disturbances and neurophysiological methods to make
or confirm the PMD diagnosis.
Challenges in Reaching a Diagnosis of PMD
Despite efforts at making definite PMD a diagnosis
of inclusion by following previously published diag-
nostic criteria, a majority of respondents confirm the
diagnosis only after excluding a range of organic neu-
rological conditions. Only one fifth of respondents acts
on the clinical diagnostic criteria and inform the
patients of the definite PMD diagnosis during the ini-
tial assessment without requesting additional investiga-
tions. Importantly, the frequency with which neurolo-
gists request standard neurological investigations is
similar for clinically definite and probable categories
of PMD, suggesting that the level of diagnostic cer-
TABLE 3. Perceived effectiveness of specific treatment strategies
Not effectiveMostly noteffective
Somewhateffective
Veryeffective
Extremelyeffective
Ratingaverage
Avoiding iatrogenic harm 4.0% (18) 15.9% (72) 34.4% (156) 30.5% (138) 15.2% (69) 3.37Educating the patient 2.4% (11) 17.5% (81) 51.1% (237) 23.9% (111) 5.2% (24) 3.12Psychotherapy with
antidepressant/anxiolytic treatment1.7% (8) 14.9% (69) 60.7% (281) 20.1% (93) 2.6% (12) 3.07
Rehabilitation services(physiotherapy, biofeedback, etc.)
4.3% (20) 16.8% (78) 58.4% (271) 19.2% (89) 1.3% (6) 2.96
Psychotherapy withoutantidepressant/anxiolytic treatment
2.6% (12) 23.1% (106) 63.1% (289) 10.7% (49) 0.4% (2) 2.83
Alternative or complementary medicine 18.3% (84) 42.8% (196) 34.1% (156) 4.4% (20) 0.4% (2) 2.26Pharmacologic treatment of specific
movement impairment30.8% (143) 52.4% (243) 15.1% (70) 1.7% (8) 0.0% (0) 1.88
Percentages (and numbers of respondents) in bold represent the most frequently chosen levels of efficacy per treatment category. Factors arelisted in descending order of rating average.
1370 A.J. ESPAY ET AL.
Movement Disorders, Vol. 24, No. 9, 2009
tainty does not alter the exclusionary manner in which
this diagnosis is predominantly made. This behavior
may in part be explained by the lasting influence of
seminal papers on PMD, which stated that ‘‘. . .the em-
phasis of the evaluation rests upon excluding organic
lesions that might mimic the presenting symptoms . . .Negative studies can strengthen the certainty of the
psychogenic diagnosis and reassure the patient that a
possible organic lesion has not been overlooked.’’1,3
There may be a number of other reasons neurologists
request standard neurological investigations despite a
clinically definite PMD diagnosis. At a basic level,
PMD is recognized as co-occurring with an organic
movement or general neurological disorder in around 5
to 10% by a substantial majority of respondents, in line
with prior reports.8,9 Some respondents view themselves
as taking patients’ symptoms ‘‘seriously’’ by ordering a
battery of tests in order to fully ‘‘placate’’ those deter-
mined to find an organic basis for their symptoms and
minimize their ‘‘doctor shopping.’’ However, a recent
controlled study found that patients with chronic daily
headache who underwent an MRI scan 1 year earlier
were equally ‘worried’ (as measured by the Hospital
Anxiety and Depression Scale) as those not offered this
investigation.10 In contrast, they had lower utilization of
additional medical resources (with resulting lower med-
ical costs), likely in part mediated by a reduction of
referrals.10 Finally, there exist conflicting views on the
use of suggestibility and placebo in diagnosing PMD. A
recent review suggested that, as transient improvements
can be seen in organic movement disorders with pla-
cebo therapies, ‘‘a diagnosis of a PMD should not be
made on the basis of the presence of a placebo response
alone’’11 (presumably referring to a transient response).
In contrast, the original classification of ‘documented
PMD,’ was reserved for movements ‘‘relieved by psy-
chotherapy, suggestion, or placebo, or spontaneous
symptom resolution when the patient feels unob-
served.’’1 Here, the necessary response should be pro-
found and more persistent than transitory. While 81%
felt that response to suggestion was useful in making a
diagnosis, placebo itself, as a diagnostic tool, was not
endorsed by the majority of respondents in this ques-
tionnaire. Although we believe that a complete resolu-
tion of a movement disorder in response to placebo is
highly supportive of a diagnosis of PMD, this approach
may not be widely used due to ethical (and litigation)
concerns rather than its lack of utility.
Country of practice had some impact on opinions of
respondents about diagnosis. A positive psychiatric his-
tory and spontaneous remissions and cures, were con-
sidered strong predictors of PMD diagnosis among US
but not among non-US respondents. Similarly, ongoing
litigation was held as predictive of a PMD diagnosis in
the US whereas it was not predictive for non-US
respondents. These differences may relate to various
factors such as delivery and availability of services for
mental health care, differences in each health care sys-
tem, litigation environment, training-related factors,
cultural issues, etc.
TABLE 4. Importance of various factors in predicting a better prognosis of PMD
Not importantMostly notimportant
Somewhatimportant Very important
Extremelyimportant
Ratingaverage
Acceptance of diagnosis by patient 0.0% (0) 1.3% (6) 7.1% (33) 31.7% (147) 59.9% (278) 4.50Identification and management of
concurrent psychiatric disorder0.0% (0) 0.9% (4) 13.9% (65) 54.5% (254) 30.7% (143) 4.15
Identification and management ofpsychological stressors
0.0% (0) 1.3% (6) 14.6% (68) 53.9% (251) 30.3% (141) 4.13
Supportive social network 0.9% (4) 5.4% (25) 21.3% (99) 47.2% (219) 25.2% (117) 3.91A short latency period between onset of
symptoms to diagnosis1.3% (6) 5.6% (26) 20.0% (93) 49.8% (232) 23.4% (109) 3.88
Absence of ongoing litigation 1.9% (9) 9.9% (46) 32% (148) 40.0% (185) 16.2% (75) 3.59Less extensive disability 1.9% (9) 9.9% (46) 36.9% (172) 44.0% (205) 7.3% (34) 3.45Paroxysmal rather than persistent or fixed
movement disorders3.2% (15) 14.6% (68) 44.8% (209) 33.5% (156) 3.9% (18) 3.20
Younger age when developing themovement disorder
2.8% (13) 23.0% (107) 45.8% (213) 26.0% (121) 2.4% (11) 3.02
Type of movement (e.g., tremor orchorea vs. dystonia or ataxia)
10.1% (47) 37.7% (175) 35.8% (166) 14.2% (66) 2.2% (10) 2.61
Pharmacologic treatment of specificmovement impairment
18.1% (84) 38.0% (176) 31.3% (145) 11.2% (52) 1.3% (6) 2.40
Percentages (and numbers of respondents) in bold represent the most frequently chosen level of importance for putative predictors of favorableprognosis. Factors are listed in descending order of rating average.
1371PSYCHOGENIC MOVEMENT DISORDERS
Movement Disorders, Vol. 24, No. 9, 2009
Challenges in the Management and
Prognosis of PMD
A substantial number of MDS members, especially
among younger and academic respondents, provide
personal follow up in addition to referring patients to a
psychiatrist or mental health specialist. Effective com-
munication and ongoing neurological support may pre-
sumably drive this practice to encourage outpatient
psychotherapy, avoid ‘‘doctor shopping,’’ and minimize
iatrogenic harm, although these and other factors (such
as treatment of underlying depression12) related to the
rationale for long-term follow up of PMD patients
were not specifically probed in this questionnaire.
Beyond a ‘‘diagnostic debriefing,’’1 no studies have
evaluated the pros, cons, and success rate of long-term
follow up of PMD patients in the hands of neurologists
experienced in PMD. Limitations to this practice
include available time and manpower, the long dis-
tance these patients often live from tertiary referral
centers providing this care, as well as the belief by
some that once the diagnosis is confirmed it is not the
responsibility of the movement disorders neurologist to
manage these patients.
Lack of management guidelines is largely due to the
paucity of controlled clinical trials examining the
effect of specific treatment modalities on PMD. What
little high-level evidence exists comes from psychody-
namic therapies (e.g., cognitive behavioral therapy,13
hypnosis14) which are not directly applicable by neu-
rologists. Other interventions without accepted efficacy
for treatment of PMD, such as acupuncture,15 may be
viewed as ‘placebo.’ This background may have
resulted in respondents endorsing as ‘very’ or
‘extremely effective’ only two interventions: education
about psychogenic disorders and avoidance of poten-
tially harmful pharmacotherapy. Psychotherapy with or
without antidepressant or anxiolytic treatment and
rehabilitation services were rated as ‘somewhat effec-
tive,’ and, importantly, pharmacological treatment
directed at the specific type of movement disorder was
rated as ‘mostly not effective’ or ‘not at all effective.’
Physician reimbursement, insurability of PMD
patients, and ongoing litigation were acknowledged as
interfering with the treatment and management of
PMD patients to a significantly greater degree in the
US compared to non-US countries. These problems are
unlikely to be resolved without comprehensive health
care reforms in the US.
A better prognosis for PMD was strongly predicted by
the acceptance of the diagnosis by the patient. Indeed,
acceptance of diagnosis is a critical turning point in the
psychotherapeutic management of these patients16 and
the inability to acknowledge the psychologic nature of
this condition has been found to be a strong predictor of
the persistence of abnormal movements and unemploy-
ment.17 As such, it is likely that any efforts made
FIG. 2. Preferred medical (black bars) and lay (gray bars) terms when respondents were asked to rate ‘top three’.
1372 A.J. ESPAY ET AL.
Movement Disorders, Vol. 24, No. 9, 2009

towards making patients fully embrace the diagnosis and
‘take the lead’ in the subsequent identification of psy-
chological stressors and mental and physical rehabilita-
tion will greatly improve the prognosis.
CONCLUSIONS AND RECOMMENDATIONS
Limitations notwithstanding (mainly, a survey
response rate that may not be fully representative of
the entire community of experts and our inability to
fully interpret differences in diagnostic and therapeutic
behaviors between countries), the opinions and clinical
practices summarized above highlight the need to fos-
ter research that may assist in the eventual creation of
diagnostic and management guidelines. In planning
further steps in the understanding and treatment of
PMD, the following areas may require the greatest
attention:
1. An MDS-driven effort is needed to encourage a
positive rather than exclusionary diagnosis for PMD
by adding operational elements per movement ab-
normality (tremor, myoclonus, dystonia, etc.) to the
currently available diagnostic criteria. This may dis-
regard the ‘clinically probable’ category of PMD,
for which ancillary testing to exclude underlying or-
ganic disorders are warranted.
2. Neurologists need to embrace PMD as a complex
neurobehavioral disorder for which they have a pri-
mary role in establishing the diagnosis and coordi-
nating management. The delivery of diagnosis by
the neurologist should not reject the reality of the
symptoms but explain them in a way that is tangible
(that is, makes sense), exculpating (removed from
any blame), and involving (generating ideas about
how the patients can manage their symptoms) to
satisfy and empower patients.18 Clinicians that
engage in the discussion of patients’ psychosocial
problems are less likely to request investigations,
refer patients elsewhere, or offer a drug treatment.19
3. A proactive role of clinician researchers is important
to further examine the therapeutic value in PMD of
therapeutic interventions without currently accepted
efficacy such as acupuncture, yoga or meditation.
4. The functional and biochemical brain abnormalities
that underlie specific PMD behaviors, receiving be-
lated attention in other psychogenic disorders,20–22
need to be explored and may also serve as surrogate
markers to measure the success of future therapeutic
efforts.
5. ‘‘PMD’’ or any alternative nomenclature should be
officially recognized and endorsed by other special-
ties, particularly psychiatrists and physiotherapists,
ideally with the help of relevant task forces for
DSM-V, to ensure successful multidisciplinary con-
tinuity of care.
Acknowledgments: We thank Joseph Jankovic, GuentherDeuschl, Christopher Goetz, Mark Hallett, Stanley Fahn, andStephen Reich for serving as external reviewers to ensurecontent and face validity of the survey. We also thank MaryKemper, medical editor, and Martha Headworth, medicalillustrator, of the UC Neuroscience Institute for assisting inthe editing and figure design for this manuscript.
Author Roles: Research project: A. Conception: Espay,Lang; B. Organization: Espay, Lang, Goldenhar, Burton,Schrag, Voon; C. Execution: Espay, Lang, Goldenhar;Statistical Analysis: A. Design: Goldenhar; B. Execution:Goldenhar C. Review and Critique: Lang, Espay, Schrag;Manuscript: A. Writing of the first draft: Espay; B. Reviewand Critique: Lang, Goldenhar, Schrag, Voon.
REFERENCES
1. Williams DT, Ford B, Fahn S. Phenomenology and psychopa-thology related to psychogenic movement disorders. In: WeinerWJ, Lang AE, editors. Behavioral neurology of movement disor-ders. New York, NY: Raven Press, 1995. p 231–257.
2. Miyasaki JM, Sa DS, Galvez-Jimenez N, Lang AE. Psychogenicmovement disorders. Can J Neurol Sci 2003;30 (Suppl 1):S94–S100.
3. Fahn S, Williams DT. Psychogenic dystonia. Adv Neurol 1988;50:431–455.
4. Koller W, Lang A, Vetere-Overfield B, et al. Psychogenic trem-ors. Neurology 1989;39:1094–1099.
5. Marjama J, Troster AI, Koller WC. Psychogenic movement dis-orders. Neurol Clin 1995;13:283–297.
6. Munhoz RP, Lang AE. Gestes antagonistes in psychogenic dysto-nia. Mov Disord 2004;19:331–332.
7. Schrag A, Lang AE. Psychogenic movement disorders. CurrOpin Neurol 2005;18:399–404.
8. Ranawaya R, Riley D, Lang A. Psychogenic dyskinesias inpatients with organic movement disorders. Mov Disord 1990;5:127–133.
9. Stone J, Smyth R, Carson A, et al. Systematic review of misdiag-nosis of conversion symptoms and ‘‘hysteria’’. BMJ 2005;331:989.
10. Howard L, Wessely S, Leese M, et al. Are investigations anxio-lytic or anxiogenic? A randomised controlled trial of neuroimag-ing to provide reassurance in chronic daily headache. J NeurolNeurosurg Psychiatry 2005;76:1558–1564.
11. Hinson VK, Haren WB. Psychogenic movement disorders. Lan-cet Neurol 2006;5:695–700.
12. Voon V, Lang AE. Antidepressant treatment outcomes of psy-chogenic movement disorder. J Clin Psychiatry 2005;66:1529–1534.
13. Speckens AE, van Hemert AM, Spinhoven P, et al. Cognitivebehavioural therapy for medically unexplained physical symp-toms: a randomised controlled trial. BMJ 1995;311:1328–1332.
14. Moene FC, Spinhoven P, Hoogduin KA, van Dyck R. A rando-mised controlled clinical trial on the additional effect of hypnosisin a comprehensive treatment programme for in-patients withconversion disorder of the motor type. Psychother Psychosom2002;71:66–76.
1373PSYCHOGENIC MOVEMENT DISORDERS
Movement Disorders, Vol. 24, No. 9, 2009

15. Van Nuenen BF, Wohlgemuth M, Wong Chung RE, et al. Acu-puncture for psychogenic movement disorders: treatment or diag-nostic tool? Mov Disord 2007;22:1353–1355.
16. Hinson VK, Weinstein S, Bernard B, et al. Single-blind clinicaltrial of psychotherapy for treatment of psychogenic movementdisorders. Parkinsonism Relat Disord 2006;12:177–180.
17. Feinstein A, Stergiopoulos V, Fine J, Lang AE. Psychiatric out-come in patients with a psychogenic movement disorder: a pro-spective study. Neuropsychiatry Neuropsychol Behav Neurol2001;14:169–176.
18. Salmon P, Peters S, Stanley I. Patients’ perceptions of medicalexplanations for somatisation disorders: qualitative analysis. BMJ1999;318:372–376.
19. Salmon P, Humphris GM, Ring A, et al. Primary careconsultations about medically unexplained symptoms: patientpresentations and doctor responses that influence theprobability of somatic intervention. Psychosom Med 2007;69:571–577.
20. Vuilleumier P. Hysterical conversion and brain function. ProgBrain Res 2005;150:309–329.
21. Mailis-Gagnon A, Giannoylis I, Downar J, et al. Altered centralsomatosensory processing in chronic pain patients with ‘‘hysteri-cal’’ anesthesia. Neurology 2003;60:1501–1507.
22. Ghaffar O, Staines WR, Feinstein A. Unexplained neurologicsymptoms: an fMRI study of sensory conversion disorder. Neu-rology 2006;67:2036–2038.
1374 A.J. ESPAY ET AL.
Movement Disorders, Vol. 24, No. 9, 2009