Embed Size (px)
Citation preview

Journal of Neuroimmunology xxx (2014) xxx–xxx
JNI-475896; No of Pages 3
Contents lists available at ScienceDirect
Journal of Neuroimmunology
j ourna l homepage: www.e lsev ie r .com/ locate / jneuro im
Short communication
Opsoclonus–myoclonus syndrome and limbic encephalitis associatedwith GABAB receptor antibodies in CSF
Alicia DeFelipe-Mimbrera a,⁎, Jaime Masjuan a, Íñigo Corral a, Luisa Maria Villar b,Francesc Graus c, Nuria García-Barragán a
a Department of Neurology, IRYCIS (Health Research Institute), Madrid, Spainb Immunology Hospital Universitario Ramón y Cajal, IRYCIS (Health Research Institute), Madrid, Spainc Department of Neurology, Hospital Clínic, Universitat de Barcelona, Institut d'Investigació Biomèdica August Pi i Sunyer (IDIBAPS), Barcelona, Spain
⁎ Corresponding author at: Department of Neurology,Cajal, Carretera de Colmenar, km 9.100, 28034 Madrid, Sp+34 913369016.
E-mail address: [email protected] (A. DeFelipe-M
http://dx.doi.org/10.1016/j.jneuroim.2014.04.0090165-5728/© 2014 Published by Elsevier B.V.
Please cite this article as: DeFelipe-Mimbreraantibodies in CSF, J. Neuroimmunol. (2014),
a b s t r a c t
a r t i c l e i n f oArticle history:Received 24 March 2014Received in revised form 12 April 2014Accepted 16 April 2014Available online xxxx
Keywords:GABAB receptor antibodiesAutoimmune diseasesEncephalitisOpsoclonus–myoclonus
We report a case of a woman who had two consecutive autoimmune neurological disorders, including anopsoclonus–myoclonus syndrome (OMS) and limbic encephalitis (LE), with positive titers of GABAB receptor an-tibodies. The patient never developed seizures or had an underlying tumor after 4 years of follow-up.
© 2014 Published by Elsevier B.V.
1. Introduction
An increasing number of neuronal antibodies against different cellsurface antigens have been associated with autoimmune encephalitisand limbic encephalitis (LE). These include antibodies against NMDA,AMPA, mGluR5 and mGluR1 receptors, dipeptidyl-peptidase-likeprotein-6 (DPPX); leucine-rich glioma inactivated 1 protein (LGI1),contactin-associated protein-like 2 (CASPR2), and contactin-2 (thesethree proteins are components of voltage-gated potassium channels).Recently, antibodies against inhibitory γ-aminobutyric acid-B receptor(GABABR) have been described which are particularly relevant in LEwith epilepsy (Graus et al., 2010; Lancaster and Dalmau, 2012).
Indeed, most of the cases of LE due to GABABR antibodies describedto date developed seizures and around 50% of the patients had an un-derlying small-cell lung cancer (SCLC) (Höftberger et al., 2013;Lancaster et al., 2010).
Here, we report a case of a woman, previously mentioned in a caseseries (Höftberger et al., 2013) but not described, who had two consec-utive autoimmune neurological disorders, including an opsoclonus–myoclonus syndrome (OMS) and LE, with positive titers of GABABR
Hospital Universitario Ramón yain. Tel.: +34 913368895; fax:
imbrera).
, A., et al., Opsoclonus–myoclohttp://dx.doi.org/10.1016/j.jn
antibodies in serum and CSF. The patient did not develop seizures andhad no underlying tumor after 4 years of follow-up.
2. Case report
A33-year-oldwoman,who3 years earlier had aHashimoto thyroid-itis treated with levothyroxine, first consulted because of a three-weekcourse of gait instability. The initial neurologic examination revealedopsoclonus and generalized myoclonus. Past history of fever or infec-tious symptoms was negative.
Blood cell count, general chemistry and thyroid function wereunrevealing. Immunological and microbiological tests were negative.CSF analysis showed30 WBC/μl, predominantly lymphocytes; total pro-tein concentration, 0.76 g/l; normal glucose concentration and no cyto-logical or microbiological findings. Intrathecal immunoglobulinsynthesis was proved by elevated IgG index (1.03) and by the detectionof oligoclonal IgG and IgM bands restricted to CSF. Cranial CT and MRIwere normal. Mammography, body CT, gastrointestinal upper andlower endoscopy, and gynecological ultrasound, were negative.
The patient was diagnosed as idiopathic OMS and started treatmentwith 1 g methylprednisolone daily for 5 days and clonazepam (1 mgevery 8 h). The patient recovered progressively and was dischargedafter a month of hospitalization with a tapering dose of oral corticoste-roids (initial dose 120 mg methylprednisolone daily) and clonazepam(0.5 every 8 h). She regained stable gait and her OMS remitted.
nus syndrome and limbic encephalitis associatedwith GABAB receptoreuroim.2014.04.009

2 A. DeFelipe-Mimbrera et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
Three months later she was admitted because of a two-week courseof fever that reached 38 °C. Drowsiness, impairment of temporal andspatial orientation and auditory and visual hallucinations were presentover the 24-hour period prior to hospitalization. Neurologic examina-tion revealed inattentiveness, inconsistent language with perseverationand short- and long-term memory deficits. The patient presented pro-gressive deterioration of awareness and central hypoventilation that re-quired supportive treatment and mechanical ventilation in theintensive care unit. Considering the severity of the clinical picture andher past history, autoimmune encephalitis was suspected and empiricimmunotherapy was started on admission, which included, again, ste-roids (1 gmethylprednisolone daily for 5 days) and intravenous immu-noglobulins (0.4 g/kg daily for 5 days). Blood tests, microbiological andimmunological studies of CSF and serum including PCR for herpes sim-plex virus were unrevealing. CSF analysis showed lymphocyticpleocytosis (25 WBC/μl) with normal concentration of glucose and pro-teins. Immunological CSF analysis again revealed elevated IgG index(2.68) and oligoclonal IgG and IgM bands present in serum with addi-tional ones restricted to CSF. An MRI was performed on the day of ad-mission and was unremarkable. Continuous EEG monitoring showeddiffuse slow and disorganized activity with no epileptiform discharges.
After 10 days, she no longer requiredmechanical ventilation but stillpresented a fluctuating level of awareness and impaired language withperiods of mutism, visual and auditory hallucinations. EEGs lasting 12 hwere repeated daily, revealing diffuse slow activitywith no epileptiformdischarges, suggesting that these episodes were due to encephalopathyand temporal lobe impairment. Due to the poor treatment outcome,plasmapheresis was performed (a total of 6 courses)with no clinical re-sponse. Therefore, rituximab infusions (560 mg at an infusion rate of100 ml per hour) were scheduled every 1–2 weeks for two months. Atotal of 4 rituximab infusions were administered, after which clinicalimprovement in terms of awareness and languagewas observed. An ex-tent study (which included PET scan, body CT, gynecological ultrasound,
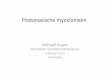
Fig. 1. Serial MRI studies. A, B, 15 days after hospital post-admission FLAIR sequencesshowed enhancement in white and gray matter of both temporal and frontal lobes andcingular gyrus. C, D, T2 (C) and FLAIR (D) sequences taken one year later show markedfrontal and temporal lobe atrophy and white matter hyperintensity.
Please cite this article as: DeFelipe-Mimbrera, A., et al., Opsoclonus–myocloantibodies in CSF, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/j.jn
and gastrointestinal upper and lower endoscopy) was repeated, and noevidence of underlying tumor was found.
The MRI was repeated 15 days post-admission and showed en-hancement in T2 and FLAIR sequences in white and gray matter ofboth temporal and frontal lobes and cingular gyrus (Fig. 1A, B).
Serumand CSFwere sent for analysis of autoantibodies to the Centerof Paraneoplastic Disorders at the University of Pennsylvania, Philadel-phia revealing positive titers of GABABR antibodies in CSF and serum.
The CSF analysis repeated one year later still detected IgG OCB re-stricted to CSF and raised IgG index (0.96). MRI one year after onsetshowed marked frontal and temporal lobe atrophy (Fig. 1C, D). The pa-tient received a progressive tapering dose of methylprednisolone for aperiod of 18 months after discharge. After 4 years of follow-up, thereis still evidence of temporal and frontal lobe affection, perseveration,short- and long-termmemory impairment, and temporal disorientationresulting in dependence formost activities. No relapsing events have oc-curred and screening for underlying tumor remains negative.
3. Discussion
Herein we present a case of a patient with special features; the pa-tient presented with two consecutive autoimmune neurological disor-ders, an unusual feature (Ducray et al., 2010) and, in addition, thepresence of an OMS syndrome extends the spectrum of neurologicaldisorders associated with GABABR antibodies.
GABAB receptors have been related to a variety of neurological disor-ders. These receptors modulate synaptic excitability and plasticity andarewidely distributed throughout the CNS but predominate in the cere-bral cortex, thalamic nuclei, cerebellum, and amygdala (Benarroch,2012).
The relationship between GABABR antibodies and LE was first de-scribed in a study which included 15 patients with LE and positive anti-body titers in serum or CSF. All these patients developed seizures,mostly as a presenting symptom. Almost half of the patients had an un-derlying tumor, with SCLC being the most common (Lancaster et al.,2010).
Another study showed that GABABR antibodies may be detected inpatients with SCLC and LE who are seronegative for other neuronal an-tibodies, and that the association of glutamic acid decarboxylase (GAD)antibodies is related to paraneoplastic syndromes (Boronat et al., 2011).The authors describe a patient with GAD and GABABR antibodies whopresentedwith reversible cerebellar ataxiawithout LE associated to car-cinoid of the thymus. In addition, there is a recent report of a case of cer-ebellar ataxia in a patientwithmalignantmelanoma (Jarius et al., 2013).However, few patients have been described to have cerebellar symp-toms associated with GABAB autoimmunity (Boronat et al., 2011;Höftberger et al., 2013; Jarius et al., 2013). Recently a series of 20 pa-tients with GABABR antibodies have been described. Most cases pre-sented with LE (17) and three patients presented with ataxia, statusepilepticus and OMS (the one described here), 2 of which developedLE (Höftberger et al., 2013).
OMS in our case extends the spectrum of neurological disorders as-sociated with GABABR antibodies. Furthermore, we cannot rule out theabsence of a relationship between both neurological disorders, asGABABR antibodies were not tested at the time of the OMS. However,both the growing number of cases described with cerebellar symptomsand the high expression of GABABR in the cerebellum support the impli-cation of GABABR antibodies in cerebellar symptoms as in our case.Moreover, intrathecal IgG synthesis adds to the argument for an immu-nological cause for both episodes. The patient had a poor functional out-come despite the fact that an autoimmune disorderwas suspected earlyand treated promptly. The patient never showed clinical or electroen-cephalographic evidence of seizure activity, nor didwe detect an under-lying malignant process after 4 years of follow-up, which seemsunusual for GABABR LE. Therefore, it is important to continue studying
nus syndrome and limbic encephalitis associatedwith GABAB receptoreuroim.2014.04.009

3A. DeFelipe-Mimbrera et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
patients with GABABR antibodies to determine their full clinicalspectrum.
References
Benarroch, E., 2012. GABAB receptors: structure, functions, and clinical implications. Neu-rology 78, 578–584.
Boronat, A., Sabater, L., Saiz, A., Dalmau, J., Graus, F., 2011. GABAB receptor antibodies inlimbic encephalitis and anti-GAD-associated neurologic disorders. Neurology 76,795–800.
Ducray, F., Graus, F., Vigliani, M.C., Antoine, J.C., Rogemond, V., Saiz, A., Honnorat, J., 2010.Delayed onset of a second paraneoplastic neurological syndrome in eight patients. J.Neurol. Neurosurg. Psychiatry 81, 937–939.
Graus, F., Saiz, A., Dalmau, J., 2010. Antibodies and neuronal autoimmune disorders of theCNS. J. Neurol. 257, 509–517.
Please cite this article as: DeFelipe-Mimbrera, A., et al., Opsoclonus–myocloantibodies in CSF, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/j.jn
Höftberger, R., Titulaer, M.J., Sabater, L., Dome, B., Rózsás, A., Hegedus, B., Hoda, M.A.,Laszlo, V., Ankersmit, H.J., Harms, L., Boyero, S., de Felipe, A., Saiz, A., Dalmau, J.,Graus, F., 2013. Encephalitis and GABAB receptor antibodies: novel findings in anew case series of 20 patients. Neurology 81, 1500–1506.
Jarius, S., Steinmeyer, F., Knobel, A., Streitberger, K., Hotter, B., Horn, S., Heuer, H.,Schreiber, S.J., Wilhelm, T., Trefzer, U., Wildemann, B., Ruprecht, K., 2013. GABAB re-ceptor antibodies in paraneoplastic cerebellar ataxia. J. Neuroimmunol. 256, 94–96.
Lancaster, E., Dalmau, J., 2012. Neuronal autoantigens: pathogenesis, associated disorders,and antibody testing. Nat. Rev. Neurol. 8, 380–390.
Lancaster, E., Lai, M., Peng, X., Hughes, E., Constantinescu, R., Raizer, J., Friedman, D., Skeen,M.B., Grisold, W., Kimura, A., Ohta, K., Iizuka, T., Guzman, M., Graus, F., Moss, S.J.,Balice-Gordon, R., Dalmau, J., 2010. Antibodies to the GABA(B) receptor in limbic en-cephalitis with seizures: case series and characterisation of the antigen. LancetNeurol. 9, 67–76.
nus syndrome and limbic encephalitis associatedwith GABAB receptoreuroim.2014.04.009