Embed Size (px)
Citation preview

OPTIMIZATION MODELS FOR RADIATION THERAPY: TREATMENT PLANNINGAND PATIENT SCHEDULING
By
CHUNHUA MEN
A DISSERTATION PRESENTED TO THE GRADUATE SCHOOLOF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OFDOCTOR OF PHILOSOPHY
UNIVERSITY OF FLORIDA
2009
1

c© 2009 Chunhua Men
2

To my wonderful family
3

ACKNOWLEDGMENTS
I would like to thank all of those people who helped make this dissertation possible.
First, I wish to thank my advisor, Dr. H. Edwin Romeijn for all his guidance, encouragement,
support, and patience. Also, I would like to thank my committee members Dr. James F.
Dempsey, Dr. Joseph P. Geunes, Dr. Stanislav Uryasev, and Dr. Fazil T. Najafi for their
very helpful insights, comments and suggestions. Additionally, I would like to acknowledge
Z. Caner Taskın and Ehsan Salari who provided technical support and assistance with my
projects.
4

TABLE OF CONTENTS
page
ACKNOWLEDGMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
LIST OF TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
LIST OF FIGURES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
CHAPTER
1 INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2 AN EXACT APPROACH TO DIRECT APERTURE OPTIMIZATION IN IMRTTREATMENT PLANNING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.2 Direct Aperture Optimization . . . . . . . . . . . . . . . . . . . . . . . . . 202.3 Column Generation Algorithm . . . . . . . . . . . . . . . . . . . . . . . . . 22
2.3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.3.2 Derivation of the Pricing Problem . . . . . . . . . . . . . . . . . . . 232.3.3 Solving the Pricing Problem . . . . . . . . . . . . . . . . . . . . . . 25
2.4 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292.4.1 Clinical Problem Instances . . . . . . . . . . . . . . . . . . . . . . . 292.4.2 Dose-Volume Histogram (DVH) Criteria . . . . . . . . . . . . . . . 322.4.3 Stopping Rules . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332.4.4 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
2.4.4.1 Delivery efficiency . . . . . . . . . . . . . . . . . . . . . . 362.4.4.2 Transmission effects . . . . . . . . . . . . . . . . . . . . . 37
2.5 Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
3 NEW MODELS FOR INCORPORATING INTERFRACTION MOTION INFLUENCE MAP OPTIMIZATION . . . . . . . . . . . . . . . . . . . . . . . . . 46
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 463.2 Beamlet-based Stochastic Optimization Models . . . . . . . . . . . . . . . 48
3.2.1 Beamlet-based Deterministic Model . . . . . . . . . . . . . . . . . . 483.2.2 First New Stochastic Optimization Model . . . . . . . . . . . . . . . 493.2.3 Second New Stochastic Optimization Model . . . . . . . . . . . . . 503.2.4 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
3.2.4.1 Clinical problem instances . . . . . . . . . . . . . . . . . . 523.2.4.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
3.3 Aperture-based Stochastic Optimization Models . . . . . . . . . . . . . . . 65
5

3.3.1 Aperture-based Stochastic Optimization Models . . . . . . . . . . . 653.3.2 Derivation of the Pricing Problem . . . . . . . . . . . . . . . . . . . 663.3.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
3.4 Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
4 OPTIMIZATION MODELS FOR PATIENT SCHEDULING PROBLEMS INPROTON THERAPY DELIVERY . . . . . . . . . . . . . . . . . . . . . . . . . 73
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 734.2 Building the Strategic Models . . . . . . . . . . . . . . . . . . . . . . . . . 75
4.2.1 The Objective Function . . . . . . . . . . . . . . . . . . . . . . . . . 754.2.2 The Constraints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
4.2.2.1 The capacity . . . . . . . . . . . . . . . . . . . . . . . . . 764.2.2.2 The patient mix . . . . . . . . . . . . . . . . . . . . . . . . 774.2.2.3 New patients’ treatment starting-time . . . . . . . . . . . 774.2.2.4 Anesthesia cases and twice-a-day fractions . . . . . . . . . 774.2.2.5 Gantry specialization and gantry switching . . . . . . . . . 78
4.2.3 The Optimization Model . . . . . . . . . . . . . . . . . . . . . . . . 794.2.4 The Model with Penalty Function . . . . . . . . . . . . . . . . . . . 814.2.5 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
4.2.5.1 Input data . . . . . . . . . . . . . . . . . . . . . . . . . . . 824.2.5.2 Results for the basic scenario . . . . . . . . . . . . . . . . 834.2.5.3 Sensitivity analysis . . . . . . . . . . . . . . . . . . . . . . 83
4.2.6 Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . 884.3 A Heuristic Approach to On-line Patient (Re-)scheduling . . . . . . . . . . 95
4.3.1 Problem Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . 954.3.2 Model Description . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
4.3.2.1 Sequence and timing decomposition . . . . . . . . . . . . . 964.3.2.2 Union sequence . . . . . . . . . . . . . . . . . . . . . . . . 974.3.2.3 Restricted and desired time windows . . . . . . . . . . . . 984.3.2.4 Evaluation criteria for the union sequence . . . . . . . . . 98
4.3.3 Solution Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . 994.3.3.1 Timing optimizer for a single day . . . . . . . . . . . . . . 994.3.3.2 Snout change index (SCI) . . . . . . . . . . . . . . . . . . 1024.3.3.3 Patient dissatisfaction index (PDI) . . . . . . . . . . . . . 1024.3.3.4 Sequence optimizer . . . . . . . . . . . . . . . . . . . . . . 1034.3.3.5 Fitting a new patient . . . . . . . . . . . . . . . . . . . . . 1064.3.3.6 Numerical example . . . . . . . . . . . . . . . . . . . . . . 107
4.3.4 Concluding Remarks . . . . . . . . . . . . . . . . . . . . . . . . . . 108
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
BIOGRAPHICAL SKETCH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
6

LIST OF TABLES
Table page
2-1 Model dimensions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
2-2 Number of apertures without transmission effects. . . . . . . . . . . . . . . . . . 41
2-3 Beam-on time without transmission effects. . . . . . . . . . . . . . . . . . . . . . 41
2-4 Aperture-based FMO: number of apertures with transmission effects. . . . . . . 42
2-5 Aperture-based FMO: beam-on time with transmission effects. . . . . . . . . . . 42
2-6 Aperture-based FMO: DVH criteria under C1 without transmission effects. . . . 42
2-7 Aperture-based FMO: DVH criteria under C1 with transmission effects addedafter optimization. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
2-8 Aperture-based FMO: DVH criteria under C1 with transmission effects. . . . . . 43
2-9 Beamlet-based FMO: DVH criteria under C1 without transmission effects. . . . 43
2-10 Beamlet-based FMO: DVH criteria under C1 with transmission effects. . . . . . 44
3-1 Model dimensions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
3-2 Radiation Therapy Oncology Group (RTOG P0126) criteria for prostate cancer. 53
3-3 Hotspots (%) for three models. . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3-4 DVH criteria for critical structures (%). . . . . . . . . . . . . . . . . . . . . . . 63
3-5 CPU running time (seconds) for three models (%). . . . . . . . . . . . . . . . . 63
3-6 C1: Number of apertures and beam-on time. . . . . . . . . . . . . . . . . . . . . 71
3-7 C2: Number of apertures and beam-on time. . . . . . . . . . . . . . . . . . . . . 71
3-8 C3: Number of apertures and beam-on time. . . . . . . . . . . . . . . . . . . . . 71
3-9 C4: Number of apertures and beam-on time. . . . . . . . . . . . . . . . . . . . . 71
4-1 Patients Classification. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
4-2 The results for the basic scenario model. . . . . . . . . . . . . . . . . . . . . . . 89
4-3 Gantry utilization per day using IP model (%). . . . . . . . . . . . . . . . . . . 89
4-4 The definitions of scenarios. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
7

4-5 Sensitivity analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
4-6 Patient mix scenarios (%). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
4-7 Scenarios 17–19: Gantry available time (minutes). . . . . . . . . . . . . . . . . . 92
4-8 Scenario 17–19: Gantry utilization (%). . . . . . . . . . . . . . . . . . . . . . . . 92
4-9 Scenario 20: Revenue per fraction. . . . . . . . . . . . . . . . . . . . . . . . . . 93
4-10 Results for Scenario 21. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
4-11 Scenario 22: Patient mix for different anesthesia availabilities. . . . . . . . . . . 93
4-12 Scenario 22: Other statistics for different anesthesia availabilities. . . . . . . . . 93
4-13 Scenario 23: Patient mix for different anesthesia availabilities. . . . . . . . . . . 93
4-14 Scenario 23: Other statistics for different anesthesia availabilities. . . . . . . . . 93
4-15 Scenario 24: Patient mix for different anesthesia availabilities. . . . . . . . . . . 94
4-16 Scenario 24: Other statistics for different anesthesia availabilities. . . . . . . . . 94
4-17 Scenario 25: Patient mix for different anesthesia availabilities. . . . . . . . . . . 94
4-18 Scenario 25: Other statistics for different anesthesia availabilities. . . . . . . . . 94
4-19 Scenario 26: Patient mix for different anesthesia availabilities. . . . . . . . . . . 94
4-20 Scenario 26: Other statistics for different anesthesia availabilities. . . . . . . . . 95
4-21 Results for scheduling a new patient on different gantries. . . . . . . . . . . . . . 107
8

LIST OF FIGURES
Figure page
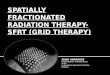
1-1 (a) Targets and critical structures delineated on a slice of a CT scan; (b) Radiationbeams passing through a patient. . . . . . . . . . . . . . . . . . . . . . . . . . . 14
1-2 (a) A multileaf collimator system1 ; (b) the projection of an aperture onto apatient. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
2-1 A typical CT slice illustrating target and critical structure deliniation. In particular,the targets PTV1 and PTV2 are shown, as well as the right parotid gland (RPG),the spinal cord (SC), and normal tissue (Tissue). . . . . . . . . . . . . . . . . . 31
2-2 DVHs of the optimal treatment plan obtained for Case 5 with C1 aperture constraintsand the Convergence stopping rule. . . . . . . . . . . . . . . . . . . . . . . . . . 35
2-3 Isodose curves for 73.8 Gy, 54 Gy, and 30 Gy on a typical CT slice, correspondingto the optimal treatment plan obtained for Case 5 with C1 aperture constraintsand the Convergence stopping rule. . . . . . . . . . . . . . . . . . . . . . . . . . 35
2-4 Case 5: The relative volume of (a) PTV1 and (b) PTV2 that receives in excessof its prescription dose. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
2-5 The relative volume of (a) LSG and (b) RSG that receives in excess of 30 Gy. . 45
3-1 The probability that a specified percentage of the target received the prescriptiondose for Case 1 (first stochastic model). . . . . . . . . . . . . . . . . . . . . . . . 55
3-2 The probability that a specified percentage of the target received the prescriptiondose for Case 1 (second stochastic model). . . . . . . . . . . . . . . . . . . . . . 56
3-3 The probability that a specified percentage of the target received the prescriptiondose for Case 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
3-4 The probability that a specified percentage of the target received the prescriptiondose for Case 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
3-5 The probability that a specified percentage of the target received the prescriptiondose for Case 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
3-6 The probability that a specified percentage of the target received the prescriptiondose for Case 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3-7 The probability that a specified percentage of the target received the prescriptiondose for Case 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3-8 DVHs for critical structures (first stochastic model vs. traditional model). . . . 60
9

3-9 DVHs for critical structures (second stochastic model vs. traditional model). . . 61
3-10 DVHs for Case 1 in Scenario 135 (first model vs. traditional model). . . . . . . 62
3-11 DVHs for Case 1 in Scenario 135 (second model vs. traditional model). . . . . . 62
3-12 Perceived and actual DVHs for critical structures for Case 1 and Case 2 . . . . . 63
3-13 Perceived and actual DVHs for target. . . . . . . . . . . . . . . . . . . . . . . . 64
3-14 Target dose coverage for two models with two stopping rules. . . . . . . . . . . . 72
10

Abstract of Dissertation Presented to the Graduate Schoolof the University of Florida in Partial Fulfillment of theRequirements for the Degree of Doctor of Philosophy
OPTIMIZATION MODELS FOR RADIATION THERAPY: TREATMENT PLANNINGAND PATIENT SCHEDULING
By
Chunhua Men
December 2009
Chair: H. Edwin RomeijnMajor: Industrial and Systems Engineering
My research addressed optimization models for radiation therapy treatment planning
and patient scheduling. In intensity modulated radiation therapy (IMRT) treatment
planning problems, I use direct aperture optimization (DAO) that explicitly formulates the
fluence map optimization (FMO) problem as a convex optimization problem in terms of
all multileaf collimator (MLC) deliverable apertures and their associated intensities and
solve it using column generation method. In addition, the interfraction motion has been
incorporated to the stochastic-programming based FMO and DAO models. Optimization
models for patient scheduling problems in proton therapy delivery have also been studied
in this research.
11

CHAPTER 1INTRODUCTION
Every year, approximately 300,000 people in the U.S. that are newly diagnosed with
cancer may benefit from radiation therapy (American Cancer Society [2]). With this
treatment modality, external beams of radiation pass through a patient with the aim
of killing cancerous cells and thereby curing the patient. However, radiation kills both
cancerous and normal cells. Many patients who are initially considered curable die of their
disease and others may suffer unintended side effects from radiation therapy. The major
reason is that radiation therapy treatment plans often deliver too little radiation dose
to the cancerous cells, too much radiation dose to healthy organs, or both. The goal of
radiation therapy treatment planning is therefore to design a treatment plan that delivers
a prescribed dose to regions in the patient that contain (or are suspected to contain)
cancerous cells (often called targets), while sparing nearby functional organs (often called
critical structures). Figure 1-1(a) shows a slice of a CT scan on which several targets
(PTV1 and PTV2) and critical structures (spinal cord (SC), right parotid gland (RPG)),
and tissue are delineated. Typically, there are several clinical targets that we wish to
irradiate and several critical structures that we wish to spare.
It may be possible to eradicate the disease with a single beam of radiation. However,
such a treatment may significantly damage normal cells in critical structures located along
the path of the beam. Hence, multiple beams (usually 3–9) are used, whose intersection
provides a high dose, whereas regions covered by a single beam or only a few beams
receive much lower radiation doses (see Figure 1-1(b)). In particular, patients receiving
radiation therapy are typically treated on a clinical radiation-delivery device called a linear
accelerator, which can rotate around the patient. Conformal radiation therapy seeks to
conform the geometric shape of the delivered radiation dose as closely as possible to that
of the intended targets. In conventional conformal radiation therapy, this usually means
12

(a) (b)
Figure 1-1. (a) Targets and critical structures delineated on a slice of a CT scan; (b)Radiation beams passing through a patient.
that from each beam direction we deliver a single beam with uniform intensity level whose
shape conforms to the beam’s eye view of the targets in the patient as seen from that
beam. Since the geometry of the targets and critical structure is different in each patient,
customized apertures have to be manufactured for each patient. A relatively recent
radiation therapy treatment delivery technique is Intensity Modulated Radiation Therapy
(IMRT). With this technique, which has been employed in clinics since 1994, the linear
accelerator is equipped with a so-called multileaf collimator (MLC) system. This system is
able to block different parts of the beam, so that it can dynamically form a large number
of different apertures (see Figure 1-2). IMRT thus allows for the delivery of a treatment
plan that uses a much larger number of different apertures than conventional conformal
radiation therapy, and thus the creation of very complex nonuniform dose distributions
that deliver sufficiently high radiation doses to targets while limiting the radiation dose
1 Varian Medical Systems; http://www.varian.com/orad/prd056.html.
13

(a) (b)
Figure 1-2. (a) A multileaf collimator system1 ; (b) the projection of an aperture onto apatient.
delivered to healthy tissues. The advent of IMRT has dramatically improved treatment
efficiency and quality.
Traditionally, IMRT treatment plans are developed using a two-stage process. In
particular, we model each beam as a collection of hundreds of small beamlets (or bixels),
and consider the intensities of each of these beamlets to be controllable on an individual
basis. The problem of finding an optimal intensity profile (also called fluence map) for
each beam is called the (beamlet-based) fluence map optimization (FMO) problem.
The goal of this problem is to develop a treatment plan that satisfies and/or optimizes
several clinical treatment plan evaluation criteria. However, this fluence map must then
be followed by a leaf-sequencing stage in which the fluence maps are decomposed into
a manageable number of apertures that are deliverable using a multileaf collimator
(MLC) system. The objective of this second stage problem is to accurately reproduce
the ideal fluence map while limiting the total treatment time. More formally, in this
second stage it is desirable to limit both the total time that radiation is delivered, i.e.,
the total beam-on-time, and the total number of apertures used. In Chapter 2, we
consider the problem of IMRT treatment planning using an approach which integrates
14

the beamlet-based FMO and leaf-sequencing problem into a single optimization model,
which is usually referred to as a direct aperture optimization approach to FMO.We extend
such a model to account for so-called transmission effects that have previously been dealt
with in a post-processing phase, and we perform an extensive clinical evaluation of the
approach and of different MLC delivery constraints.
In general, the IMRT treatment plans are delivered during 5-7 weeks and a daily
treatment is called a fraction. During a course of fractionated radiation therapy and
between the fractions the organs of the patients’ body may move. Organ movements
are divided into two general categories: interfraction motion and intrafraction motion
([36]). Interfraction organ motion consists of day-to-day changes, such as set-up errors,
tumor shrinkage, weight lost, etc. Intrafraction motion refers to the internal organ
motion occurring during the actual radiation treatment due to breathing, swallowing, etc.
Traditionally, the IMRT treatment systems are based on a static patient model, which
relies on a single static planning computed tomography (CT) image for treatment planning
and evaluation. To account for organ motion, the conventional method is to add a margin
around the clinical tumor volume (CTV) to get a planning target volume (PTV)([26, 27]).
Instead of using a margin, in Chapter 3, we introduce new stochastic-programming based
models for incorporating interfraction motion in FMO.
Finally, a challenge of radiation therapy has been to efficiently deliver high quality
treatment using limited and expensive resources. Effective scheduling systems have the
conflicting goals of maximizing the utilization of resources and the number of patients,
and minimizing the patient waiting time. The treatment providers are under pressure
to reduce the cost and improve treatment quality. In recent years, patient scheduling is
gradually becoming an essential component in medical care. However, little attention has
focused on patient scheduling in radiation therapy. In Chapter 4, we develop optimization
15

models for strategic and operational patient scheduling problems in proton therapy
delivery and test them using the data from the University of Florida Proton Therapy
Institute (UFPTI). The overall goals of the strategic models are to analyze the treatment
capacity and determine potential ways in which operations can be streamlined to increase
this capacity. In addition, a new heuristic method has been developed and implemented
to schedule patients for treatment delivery and the results indicate that we can obtain
high-quality schedules in real-time.
16

CHAPTER 2AN EXACT APPROACH TO DIRECT APERTURE OPTIMIZATION IN IMRT
TREATMENT PLANNING
2.1 Introduction
Traditionally, IMRT treatment plans are developed using a two-stage process: fluence
map optimization is followed by a leaf-sequencing problem. Both the beamlet-based FMO
problem and the leaf-sequencing problem are well-studied in the literature. For modeling
and solution approaches to the FMO problem we refer to the review paper by Shepard et
al. [64]. More recently, Lee et al. [40, 41] studied mixed-integer programming approaches,
Romeijn et al. [61] proposed new convex programming models, and Hamacher and Kufer
[24] and Kufer et al. [37] considered a multi-criteria approach to the problem. The
problem of leaf-sequencing while minimizing total beam-on-time is very efficiently solvable
in general. We refer in particular to Ahuja and Hamacher [1], Bortfeld [11], Kamath et
al. [31], and Siochi [66]; in addition, Baatar et al. [5], Boland et al. [10], Kamath et al.
[32, 33, 34, 35], Lenzen [42], and Siochi [66] study the problem under additional MLC
hardware constraints, while Kalinowski [30] studies the benefits of allowing rotation of
the MLC head. The problem of decomposing a fluence map into the minimum number of
apertures has been shown to be strongly NP-hard (see Baatar et al. [5]), leading to the
development of a large number of heuristics for solving this problem. Notable examples
are the heuristics proposed by Baatar et al. [5] (who also identify some polynomially
solvable special cases), Dai and Zhu [20], Que [54], Siochi [66], and Xia and Verhey [70].
In addition, Engel [23], Kalinowski [29], and Lim and Choi [43] developed heuristics
to minimize the number of apertures while constraining the total beam-on-time to be
minimal. Langer et al. [39] developed a mixed-integer programming formulation of the
problem, while Kalinowski [28] proposed an exact dynamic programming approach.
17

Finally, Taskın et al. [68] propose a new exact optimization approach to the problem of
minimizing total treatment time.
A major drawback of the decoupling of the treatment planning problem into a
beamlet-based FMO problem and a MLC leaf sequencing problem is that there is a
potential loss of treatment quality. This has led to the development of approaches that
integrate the beamlet-based FMO and leaf-sequencing problems into a single optimization
model, which are usually referred to as direct aperture optimization approaches to FMO.
In this approach, we explicitly solve for a set of apertures and corresponding intensities in
a single aperture-based FMO problem. For examples of integrated approaches to fluence
map optimization, sometimes also called aperture modulation or aperture-based fluence
map optimization, we refer to Preciado-Walters et al. [52], Shepard et al. [63], Siebers et
al. [65], Bednarz et al. [8] and Romeijn et al. [60]. The way the dose distribution received
by the patient is modeled in a beamlet-based FMO model is necessarily an approximation
since this distribution depends not only on the intensity profile but also on the actual
apertures used to deliver this profile. The current literature on aperture modulation has,
however, has not yet exploited the ability of aperture modulation to take into account
such effects. In particular, while the leaves in the MLC system do block most of the
radiation beam, there is some small but not insignificant amount of dose (on the order of
1.5–2%, see Arnfield et al. [4]) that is transmitted through the leaves in the MLC system.
Finally, while several aperture-based FMO approaches attempt to limit total treatment
time by limiting the number of apertures used, these models do not explicitly incorporate
total beam-on-time as a measure of treatment plan efficiency.
In this chapter, we extend the approach developed by Romeijn et al. [60] by (i)
allowing for the incorporation of more general treatment plan evaluation criteria and
treatment plan constraints; (ii) accounting for transmission effects. In addition, we also
18

extend the method to MLC systems that can only deliver apertures that are rectangular in
shape. Our goals are to
• evaluate the ability of our approach to efficiently find high-quality treatment planswith a limited number of apertures;
• evaluate the effect of MLC deliverability constraints on the required number ofapertures and beam-on-time;
• evaluate the importance of explicitly incorporating transmission effects.
2.2 Direct Aperture Optimization
With most forms of external-beam radiation therapy, a patient is irradiated from
several different directions, which we assume are chosen based on experience by a
physician or clinician. We will denote the set of beam directions by B. Each beam
b ∈ B is discretized into a matrix of bixels, indicated by the set Nb. For convenience we let
N ≡ ∪b∈BNb denote the set of all bixels. We will denote the set of apertures that can be
delivered by a MLC system from beam direction b ∈ B by Kb and the set of all deliverable
apertures by K ≡ ∪b∈BKb. For convenience, we let bk denote the beam that contains
aperture k, i.e., k ∈ Kbkfor all k ∈ K. Clearly, each aperture can then be viewed as a
subset of bixels in a beam, so we will denote a particular aperture k ∈ Kb by the set of
beamlets Ak ⊆ Nb. With each aperture k ∈ K we associate a decision variable yk that
indicates the intensity of that aperture.
The dose distribution in a patient is evaluated on a discretization of the 3-dimensional
geometry of the patient, obtained via a CT scan, into a number of voxels. We denote the
set of all voxels by V , and associate a decision variable zj with each voxel j ∈ V that
indicates the dose received by that voxel. The vector of voxel doses can be expressed as
a linear function of the intensities of the apertures through the so-called dose deposition
coefficients Dkj, the dose received by voxel j ∈ V from aperture k ∈ K at unit intensity.
19

Finally, we assume that a collection, say L, of treatment plan evaluation criteria has
been identified that measure clinical treatment plan quality and are expressed as functions
of the dose distribution: G` : RV → R for ` ∈ L. Each of these criteria is usually, but not
necessarily, a function of the dose distribution in a particular structure only. Without loss
of generality we assume that the criteria are expressed in such a way that smaller values
are preferred to larger values. Finally, we assume that all criteria are convex. This is
justified by the fact that most criteria proposed in the literature to date are indeed convex
or can be replaced by a convex criterion that has the property that the Pareto-efficient
frontier associated with all criteria is unchanged (see Romeijn et al. [62]). Examples of
such criteria are tumor control probability (TCP), normal tissue complication probability
(NTCP), equivalent uniform dose (EUD), conditional value-at-risk (CVaR), voxel-based
penalty functions, etc. (see, e.g., Niemierko [49] and [50], Lu and Chin [45], Kutcher and
Burman [38], Rockafellar and Uryasev [58]).
Our aperture-based FMO model can now be formulated as follows:
minimize∑
`∈L
G`(z)
subject to (A)
zj =∑
k∈K
Dkjyk for all j ∈ V (2–1)
yk ≥ 0 for all k ∈ K. (2–2)
Here z ∈ R|V | and y ∈ R|K| are the vectors containing the voxel doses and aperture
intensities, respectively. Many other aperture-based FMO models that have been proposed
in the literature are heuristics that are based on deterministic or stochastic search, such as
simulated annealing, for which it often cannot be guaranteed that all deliverable apertures
20

are (explicitly or implicitly) considered. In contrast, our approach explicitly incorporates
all deliverable apertures and corresponding intensities.
Traditional beamlet-based FMO models as well as all aperture-based FMO models to
date have assumed that the dose deposition coefficients can be written as
Dkj =∑i∈Ak
Dij (2–3)
where Dij is the dose received by voxel j from bixel i at unit intensity. However, this
definition ignores any transmission and scatter effects that are due to the shape of the
apertures used. Both of these effects cannot be modeled in a beamlet-based FMO model.
We will explicitly incorporate the transmission effect. In particular, the expression for
the dose deposition coefficients given in (2–3) assumes that any bixel that is blocked
in an aperture does not transmit any radiation. If we denote the fraction of dose that
is transmitted by ε ∈ [0, 1], we obtain the following expression for the dose deposition
coefficients:
Dkj =∑i∈Ak
Dij + ε∑
i∈Nbk\Ak
Dij
= (1− ε)∑i∈Ak
Dij + ε∑
i∈Nbk
Dij
= (1− ε)∑i∈Ak
Dij + εDbkj
where Dbj =∑
i∈NbDij. Clearly, the traditional expression (2–3) corresponds to the special
case where ε = 0.
2.3 Column Generation Algorithm
2.3.1 Introduction
It is clear that the number of allowable apertures (i.e., the cardinality of K) is
typically enormous. For example, consider an MLC that allows all combinations of left and
21

right leaf settings. Even with a coarse 10 × 10 bixel grid and 5 beams, this would yield
more than 1018 deliverable apertures to consider. However, it is reasonable to expect that
in the optimal solution to (A) only a relatively small number of apertures will actually
have positive intensity. The challenge is therefore to identify a small but judiciously chosen
set of apertures that yield a high-quality treatment plan. Since it does not seem possible
to intuitively identify or characterize such a set of apertures for each individual patient,
we use a formal column generation approach to solving the aperture-based FMO problem.
This method starts by choosing a limited number of apertures, for example corresponding
to a conformal plan, given by a set K ⊆ K. It then solves a restricted version of (A) using
only that set of apertures. Next, an optimization subproblem, called the pricing problem,
is solved. This
(i) identifies one or more promising apertures that will improve the current solutionwhen added to the collection of considered apertures; or
(ii) concludes that no such apertures exist, and therefore the current solution is optimal.
In case (i), we add the identified apertures to K, re-optimize the new aperture-based
FMO problem, and repeat the procedure. Intuitively, the pricing problem identifies those
apertures for which the improvement of the objective function per unit intensity is largest
(and therefore show promise for significantly improving the treatment plan). The very
nature of our approach thus allows us to study the effect of adding apertures on the
quality of the treatment plan, thereby enabling a sound trade-off between the number of
apertures and treatment plan quality.
2.3.2 Derivation of the Pricing Problem
Let us denote the dual multipliers associated with constraints (2–1) and (2–2) by πj
(j ∈ V ) and ρk (k ∈ K). The Karush-Kuhn-Tucker (KKT) optimality conditions (see, e.g.,
Bazaraa et al. [7]) for (A), which are necessary and sufficient for optimality because of the
22

convexity of the objective function and the linearity of the constraints, can be written as
follows:
πj =∑
`∈L
γ`∂G`(z)
∂zj
for all j ∈ V
ρk =∑j∈V
Dkjπj for all k ∈ K
zj =∑
k∈K
Dkjyk for all j ∈ V
ykρk = 0 for all k ∈ K
yk, ρk ≥ 0 for all k ∈ K.
Any solution to this system can be characterized by y ≥ 0 only: this vector then
determines, in turn, z, π, and ρ. Let (y; π, ρ) be an optimal pair of primal and dual
solutions to a subproblem problem in which only apertures in the set K ⊂ K are
considered, where we have set yk = 0 for k ∈ K\K. We can then conclude that this
solution is in fact optimal for (A) if and only if ρk ≥ 0 for all k ∈ K (note that this
inequality is satisfied for k ∈ K by construction). In other words, if and only if the
optimal solution to the following so-called pricing problem is nonnegative:
minimizek∈K
∑j∈V
Dkjπj.
Since each aperture contains beamlets in a single beam only, we may alternatively solve a
pricing problem for each individual beam b ∈ B:
minimizek∈Kb
∑j∈V
Dkjπj.
23

Now note that if k ∈ Kb we have
∑j∈V
Dkjπj =∑j∈V
((1− ε)
∑i∈Ak
Dij + εDbj
)πj
= (1− ε)∑j∈V
∑i∈Ak
Dijπj + ε∑j∈V
Dbjπj.
This then means that the current solution is optimal for (A) if and only if, for all b ∈ B,
the optimal solution to the following optimization problem
minimizek∈Kb
∑i∈Ak
(∑j∈V
Dijπj
)
exceeds the threshold value
− ε
1− ε
∑j∈V
Dbjπj. (2–4)
We can now justify the intuition behind the pricing problem and the column generation
algorithm that was provided earlier: realizing that∑
j∈V Dijπj measures the per-unit
change in objective function value if the intensity of beamlet i is increased, it follows
that the pricing problem for a given beam identifies the aperture with the property that
the rate of improvement in objective function value, as the intensity of the aperture is
increased, is largest among all deliverable apertures. Furthermore, this aperture is added
to the model only if increasing the intensity of that aperture actually corresponds to an
improvement in objective function value.
2.3.3 Solving the Pricing Problem
We will consider the following four common sets of hardware constraints on the set of
deliverable apertures:
C1. Consecutiveness constraintThis constraint simply corresponds to the fact that apertures are shaped by pairsof leaves, which means that, in each given bixel row, the exposed bixels should beconsecutive.
24

C2. Interdigitation constraintThis constraint says that, in addition to C1, the left leaf of a row cannot overlapwith the right leaf of an adjacent row.
C3. Connectedness constraintThis constraint says that, in addition to C2, the bixel rows that contain at least oneexposed bixel should be consecutive.
C4. Rectangle constraintThis constraint says that only rectangular apertures may be formed.
Note that constraint C4 corresponds to the use of conventional jaws only. Recently, the
viability of this delivery technique has been shown by Kim et al. [71] for treating prostate
cancer and by Earl et al. [21] for treating pancreas, breast, and prostate cancer.
Romeijn et al. [60] provide polynomial-time algorithms for solving the pricing problem
corresponding to C1–C3. In particular, suppose that each beam is discretized into an
m × n matrix of bixels. They then show that the pricing problem for a particular beam
can be solved in O(mn) time for C1 and in O(mn4) time for C2 and C3. For completeness
sake, we will briefly describe these algorithms below. Next, we will develop an efficient
algorithm for solving the pricing problem under C4.
It is easy to see that, under C1, the pricing problem decomposes by bixel row, i.e.,
we may find the optimal leaf settings for each row individually and then form the optimal
aperture by simply combining these leaf settings. We are thus interested in finding, for
each bixel row, a consecutive set of bixels for which the sum of their coefficients in the
objective function of the pricing problem is minimal. We can find such a set of bixels by
making a single pass, from left to right, through the n bixels in a given row and beam. In
doing so, we should keeping track of (i) the sum of the coefficients for all bixels considered
so far, and (ii) the maximum value of these sums encountered so far. Now note that, at
any point in this procedure, the difference between these two is a candidate for the best
25

solution value found so far, so we simply identify the leaf setting that corresponds to the
minimum value of this difference. (See also Bates and Constable [6] and Bentley [9].)
The algorithm for identifying the optimal aperture to add under C2 and C3 is
somewhat more complicated. For these two situations, we formulate the pricing problem
as the shortest path problem in an appropriately defined network. In particular, we define
a node corresponding to each potential leaf setting in each bixel row, i.e., (r; c1, c2) for
r = 1, . . . ,m and c1, c2 = 1, . . . , n with c1 < c2, where c1 and c2 denote the rightmost
and leftmost blocked bixel in row r, respectively. In addition, we define so-called source
and sink nodes representing the “top” and “bottom” of the aperture. We then create arcs
between nodes that correspond to feasible combinations of leaf settings in adjacent bixel
rows, and assign to any arc leading to a particular node a cost equal to the sum of all
coefficients corresponding to exposed bixels. That is, under C2 we create arcs between a
pair of nodes if the interdigitation constraint is satisfied. Under C3, we ignore all nodes
that correspond to bixel rows in which all bixels are blocked; then, in addition to the arcs
created for C2, we also create arcs from the source node to all other nodes and from all
nodes to the sink node, representing the fact that leaf settings that block all bixels are
allowed at the “top” and “bottom” of the aperture.
We will next develop a polynomial-time algorithm for the pricing problem associated
with C4. For convenience, let (b, r, c) denote the bixel in row r and column c of beam
b (r = 1, . . . , m; c = 1, . . . , n; and b ∈ B). Moreover, let (b, r1, r2, c1, c2) represent a
rectangular aperture in which r1 and r2 denote the first and the last row, while c1 and c2
denote the leftmost and rightmost column of bixels which form the rectangular aperture in
beam b. We can then formulate the pricing problem for beam b under C4 as follows:
minimize
r2∑r=r1
c2∑c=c1
(∑j∈V
D(b,r,c)jπj
)
26

subject to
r1 < r2
c1 < c2
r1, r2 ∈ {1, . . . , m}
c1, c2 ∈ {1, . . . , n}.
It is easy to see that we can employ the algorithm for C1 to construct an algorithm for
C4. In particular, suppose that we fix the range of rows in the rectangular aperture as r1
and r2 (with, of course, r1 < r2). Then the problem reduces to
minimize
c2∑c=c1
(r2∑
r=r1
∑j∈V
D(b,r,c)jπj
)
subject to
c1 < c2
c1, c2 ∈ {1, . . . , n}
which is precisely a pricing problem of the form as for C1 with respect to the sum of
rows r1, . . . , r2 in the matrix of objective function coefficients. Therefore, given these
aggregate objective coefficients we can solve the pricing problem for C4 in O(m2n) time
by enumerating all O(m2) possible collections of consecutive rows and selecting the best
solution among these candidates. Now note that we can, for each value of r1, determine
all aggregate objective function coefficients in O(mn) time. This means that all objective
function coefficients can be determined in O(m2n) time, and the running time of the entire
algorithm is O(m2n).
Clearly, if, for each beam b ∈ B, the best solution found has an objective function
value that exceeds the corresponding threshold value (2–4) derived in Section 2.3.2, no
27

aperture can improve the current solution, which is therefore optimal for (A). Otherwise,
adding the optimal aperture, say (b∗, r∗1, r∗2, c
∗1, c
∗2), to the set K can improve the current
solution.
2.4 Results
2.4.1 Clinical Problem Instances
To test our models, three-dimensional treatment planning data for ten head-and-neck
cancer patients was exported from a commercial patient imaging and anatomy segmentation
system at the University of Florida Department of Radiation Oncology. This data was
then imported into the University of Florida Optimized Radiation Therapy (UFORT)
treatment planning system and used to generate the data required by the models
described above.
For all ten cases, we designed plans using five equispaced 60Co-beams. Note that
this does not affect the optimization algorithm, which is, without modification, applicable
to high-energy X-ray beams as well (for example, see Romeijn et al. [60] for results with
6MV photon beams). The five beams are evenly distributed around the patient with
angles 0◦, 72◦, 144◦, 216◦, 288◦, respectively. The nominal size of each beam is 40 × 40 cm2.
The beams are discretized into bixels of size 1 × 1 cm2, yielding on the order of 1,600
bixels. However, we reduce the set of beamlets that actually need to be considered in the
optimization by using the fact that the actual volume to be treated is usually significantly
smaller. That is, for each beam, we identify a “mask” consisting of only those bixels
that can help treat the targets, i.e., we identify the bixels for which the dose deposition
coefficient Dij associated with at least one target voxel is nonzero. We then extend the
mask to a rectangle of minimum size to ensure that all deliverable apertures from C1–C4
that can help treat the targets are considered. For all cases we generate a voxel grid
with voxels of size 4 × 4 × 4 mm3. To decrease the size of problems, we use a voxel size
28

8 × 8 × 8 mm3 for unspecified tissue in the optimization models. But when we evaluate
the treatment quality, we take the size 4 × 4 × 4 mm3 for all voxels. Table 2-1 shows the
problem dimensions for the ten cases.
Table 2-1. Model dimensions.
case # structures total # voxels # voxels in the models # bixels1 14 85,017 17,576 9902 13 104,298 24,300 1,6373 8 189,234 36,414 1,6584 11 195,113 38,680 2,0065 12 86,255 15,985 1,1136 13 58,636 13,878 7657 10 102,262 21,386 1,2478 10 84,369 18,661 1,1499 10 71,837 14,664 938
10 12 148,294 40,202 2,183
Each case contained two targets, which are referred to as Planning Target Volume 1
(PTV1) and Planning Target Volume 2 (PTV2). PTV1 consists the Gross Tumor Volume
(GTV, which refers to the best clinical estimation of the exact areas of the primary tumor
volume) expanded to account for both sub-clinical disease as well as daily setup errors and
internal organ motion; PTV2 is a larger target that also contains high-risk nodal regions,
again expanded to account for sub-clinical disease and setup errors and organ motion.
PTV1 and PTV2 have prescription doses of 73.8 Gy and 54 Gy, respectively. Figure 2-1
shows an example of target deliniation.
Our FMO model employed treatment plan evaluation criteria that are quadratic
one-sided voxel-based penalties. In particular, denoting the set of targets by T the set of
critical structures by C, the set of all structures by S = T ∪ C, and the set of voxels in
29

Figure 2-1. A typical CT slice illustrating target and critical structure deliniation. Inparticular, the targets PTV1 and PTV2 are shown, as well as the right parotidgland (RPG), the spinal cord (SC), and normal tissue (Tissue).
structure s ∈ S by Vs, we use the following treatment plan evaluation criteria:
Gs−(z) =αs
|Vs|∑j∈Vs
(max{0, T−
s − zj})2
s ∈ T (2–5)
Gs+(z) =βs
|Vs|∑j∈Vs
(max{0, zj − T+
s })2
s ∈ S. (2–6)
(Clearly, this means that the set of treatment plan evaluation criteria can be expressed as
L = {s− : s ∈ T} ∪ {s+ : s ∈ S}.) The coefficients αs and βs (s ∈ S) are nonnegative
weights associated with the clinical treatment plan evaluation criteria. Criteria (2–5)
penalize underdosing below the underdosing threshold T−s in all targets s ∈ T , while
criteria (2–6) penalize overdosing above the overdosing threshold T+s in all structures
s ∈ S. We choose this model based on the fact that it, in our experience, can be solved
very efficiently and yields high-quality treatment plans. However, recall that our algorithm
can easily be applied to models that include other convex treatment plan evaluation
criteria, such as voxel-based penalty functions with higher powers, or EUD. The resulting
30

model (A) was solved by our in-house primal-dual interior point algorithm. We tuned the
problem parameters (underdose and overdose thresholds and criteria weights) by manual
adjustment based on two of the ten patient cases and a beamlet-based FMO model. We
then used this set of parameters to solve different variants of the beamlet-based and
aperture-based FMO problem for all ten patient cases. Finally, all of our experiments
were performed on a PC with a 3.4 GHz Intel Pentium IV processor and 2 GB of RAM,
running under Windows XP. Our algorithms were implemented in Matlab 7.
2.4.2 Dose-Volume Histogram (DVH) Criteria
A tool that is most commonly employed by physicians to judge the quality of a
treatment plan is the so-called (cumulative) dose-volume histogram (DVH). This
histogram specifies, for a given target or critical structure, the fraction of its volume
that receives at least a certain amount of dose. Using the finite representation of all
structures using voxels, the value of the DVH at dose d is precisely the fraction of voxels
in a structure who receive a dose of at least d units. Our approach is to employ a convex,
and therefore efficiently solvable, formulation of the FMO problem. However, we use
clinical DVH criteria to objectively verify both the ability of our models to create clinically
acceptable treatment plans as well as the robustness of the problem parameters (which,
as mentioned above, are not tuned for individual patients). We use the DVH criteria used
in the Department of Radiation Oncology at the University of Florida. These criteria are
based on the current clinical guidelines formulated by the Radiation Therapy Oncology
Group ([55], [56]):
• PTV1
– At least 99% should receive 93% of the prescribed dose (0.93× 73.8 Gy)
– At least 95% should receive the prescribed dose (73.8 Gy)
– No more than 10% should be overdosed by more than 10% of prescribed dose(1.1× 73.8 Gy)
31

– No more than 1% of PTV1 should be overdosed by more than 20% ofprescribed dose (1.2× 73.8 Gy)
• PTV2
– At least 99% should receive 93% of the prescribed dose (0.93× 54 Gy)
– At least 95% should receive the prescribed dose (54 Gy)
• Salivary glands (right and left parotid glands, right and left submandibular glands)
– No more than 50% of each gland should receive more than 30 Gy
• Other structures
– Tissue should receive less than 60 Gy
– Spinal cord should receive less than 45 Gy
– Mandible should receive less than 70 Gy
– Brain stem should receive less than 54 Gy
– Eye should receive less than 45 Gy
– Optic nerve should receive less than 50 Gy
– Optic chiasm should receive less than 55 Gy
2.4.3 Stopping Rules
We use the column generation algorithm to solve the aperture-based FMO problem.
In our implementation, we identify in each iteration the best aperture (among all beams)
that could improve the treatment plan quality, and add this aperture to the set of
apertures currently under consideration. This approach allows us to make a trade-off
between the number of apertures and the treatment plan quality. As the number of
apertures increases, at some point the improvement in treatment plan quality may not
be clinically significant anymore. Moreover, a high number of apertures in general leads
to a high beam-on time. Hence, rather than allowing the column generation algorithm
to formally converge, we propose to terminate the algorithm based on the observed
32

development of the clinical DVH criteria. In particular, we investigate the merits of the
following two stopping rules:
• Convergence:This stopping rule is based on observing that treatment plan quality, with respect toa particular criterion, has not improved markedly in recent iterations. More formally,we say that we are satisfied with the solution with respect to a particular criterionif, in the last 5 iterations, the range of observed criterion values spans less than δ(where we use δ = 0.5% for target criteria and δ = 2% for critical structure criteria).
• Clinical:This stopping rule is based on observing that the treatment plan performance withrespect to a clinical criterion has been satisfactory in the last 5 iterations. Moreformally, we say that we are satisfied with the solution with respect to a particularcriterion if either the first stopping rule is satisfied or, in the last 5 iterations, theclinical DVH criterion is satisfied, allowing for a 1% error bar in all but one of thoseiterations. (Note that we allow for the clinical stopping rule to be “satisfied” if theconvergence stopping rule is satisfied to account for the fact that certain clinicalcriteria cannot be achieved. This may, for example, be the case if a critical structureis wholly or partially contained in a target.)
In either case, we say that the algorithm has converged if the stopping rule has been
satisfied for all convergence (resp. clinical) criteria. Moreover, we report the solution
obtained in the first iteration of the last sequence of 5 iterations.
2.4.4 Results
We divide the discussion of our results into two parts according to the goals that we
formulated in Section 1. First, we evaluate the ability of our approach to efficiently find
high-quality treatment plans with a limited number of apertures, as well as the effect of
MLC deliverability constraints on the required number of apertures and beam-on-time.
Next, we evaluate the importance of explicitly incorporating transmission effects into the
optimization model. However, before we do so, in Figures 2-2 and 2-3 we illustrate the
behavior of our FMO model by showing the DVHs and isodose curves superimposed on a
typical CT slice, both corresponding to an optimal treatment plan found for Case 5. The
33

isodose curves show both the conformality of the plan with respect to the two targets and
the sparing of the spinal cord and saliva glands.
Figure 2-2. DVHs of the optimal treatment plan obtained for Case 5 with C1 apertureconstraints and the Convergence stopping rule.
Figure 2-3. Isodose curves for 73.8 Gy, 54 Gy, and 30 Gy on a typical CT slice,corresponding to the optimal treatment plan obtained for Case 5 with C1aperture constraints and the Convergence stopping rule.
34

2.4.4.1 Delivery efficiency
Tables 2-2 and 2-3 show the number of apertures and beam-on-time (in minutes) for
the ten cases obtained with our aperture-based approach. We used the two stopping
rules described in Section 2.4.3. For these experiments, we have not incorporated
any transmission effects. For comparison purposes, the tables also show the results of
traditional beamlet-based FMO where the optimal fluence maps were first discretized to
integer multiples of 5% of the maximum beamlet intensity in each beam, and subsequently
decomposed into apertures with the objective function of minimizing the beam-on time.
We used the algorithms by Kamath et al. [31, 32] to minimize the beam-on-time under C1
and C2, respectively. Furthermore, we applied a modification of the approach by Boland
et al. [10] to minimize the beam-on-time under C3, while we used a linear programming
model for the case of C4. (Note that there are, in general, many decompositions that
attain the minimum beam-on-time; the number of apertures that is given is for a
particular solution that the so-called leaf-sequencing algorithm found, but that number is
not minimized explicitly.)
Our main conclusions are:
• With our direct aperture optimization approach and based on our stopping rules, weconclude that the number of apertures required under aperture constraints C1–C3 is,on average, on the order of 30–45, increasing to 60–85 with jaws-only delivery.
• The direct aperture optimization approach leads to a reduction of the requirednumber of apertures by, on average, more than 75% of the number obtained with thetraditional two-phase approach. Moreover, the required beam-on-time is reduced by,on average, more than 50%.
• There is very little effect on the required number of apertures and beam-on-timewhen interdigitation or connectedness constraints are imposed; however, the requirednumber of apertures and beam-on-time increases by, on average, approximately 50%when only rectangular apertures are considered.
35

It is interesting to see that in some cases fewer apertures are required when the deliverability
constraints are strengthened. This is caused by a combination of the fact that our
approach does not explicitly minimize the number of apertures and the fact that the
effect of some constraints (in particular, the added constraint in C3 as compared to C2) is
apparently negligible in practice.
The amount of time required, on average, by our optimization algorithm to find
the aperture based solutions ranges from about 1–3 minutes of CPU time for the case of
consecutiveness constraints only. The required time increases to up to 4 minutes when
interdigitation and connectedness are imposed, while it further increases to up to about
12 minutes when only rectangular apertures are allowed. This is in comparison with
an average of a little over 1 minute of CPU time required for the traditional two-phase
approach. Note that these times do not include the time required to read the DICOM
data and compute the dose deposition constraints, which took about 10–25 minutes of
CPU time depending on the size of the case. However, note that these tasks only need to
be performed once for each patient.
To illustrate how our approach may be used to make a trade-off between treatment
plan quality and delivery efficiency, Figures 2-4–2-5 show the behavior of target coverage
and submandibular gland sparing as a function of the number of apertures used for C1–C4
for a typical example, Case 5.
2.4.4.2 Transmission effects
We have also studied the effect of incorporating transmission effects into the FMO
problem. First, Tables 2-4 and 2-5 show the number of apertures and beam-on-time with
incorporation of transmission effects. We have used ε = 1.7% as the transmission rate (see
Arnfield et al. [4]). A comparison with Tables 2-2 and 2-3 reveals that the incorporation of
transmission effects has very little effect on the treatment delivery efficiency.
36

Next, Tables 2-6–2-8 show the results of the aperture-based FMO problem under C1
without and with transmission effects using the convergence stopping rule. In particular,
the tables show values of the DVH criteria for the targets and main critical structures
for all ten cases. For example, the data in the column labeled PTV2@93% represents the
fraction of volume (in %) of PTV2 receiving 0.93× 54 Gy. The labels of the other columns
follow a similar format, where the acronyms correspond to the left parotid gland (LPG),
right parotid gland (RPG), left submandibular gland (LSG), and right submandibular
gland (RSG). Comparing Tables 2-6 and 2-8 suggests that treatment plans of very similar
quality can be found with and without incorporation of transmission effects. However,
the results of Table 2-6 neither incorporate transmission in the optimization problem nor
account for transmission in the presentation of the actual results, so that the treatment
plan quality in that table is a perceived rather than an actual one. Table 2-7 shows the
actual quality of the treatment plan that was obtained when solving an optimization
model that does not take transmission effects into account, i.e., for the results in Table 2-7
transmission effects were added a posteriori to the plan.
Finally, we analyzed the results of using a beamlet-based FMO approach followed by
a leaf sequencing phase, under C1. Table 2-9 shows the perceived quality of the obtained
treatment plan (in which transmission effects are ignored), while Table 2-10 shows the
actual quality of the treatment plan (in which transmission effects are added to the final
treatment plan).
From the latter two tables, it is clear that using a beamlet-based FMO optimization
approach may severely underestimate target hotspots (overdosing) and effects on
critical structures. The direct aperture optimization approach with transmission effects
incorporated, however, provides a high-quality treatment plan with, on average, a
comparable number of apertures and beam-on-time. Taking Case 5 as an example, a
37

treatment plan that ignored transmission effects appeared to spare all four saliva glands,
while less than 10% of PTV1 received in excess of 110% of its the prescription dose.
Adding transmission effects to the plan found using beamlet-based FMO showed that in
fact only two saliva glands were spared with the PTV1 hotspot increasing to over 80%.
Incorporating transmission effects into the aperture-based FMO model showed that it was
possible to spare all saliva glands and that keep the dose to PTV1 in excess of 110% of its
prescribed dose to about 3%.
2.5 Concluding Remarks
In this chapter, we consider the problem of IMRT treatment planning using direct
aperture optimization. We use an exact approach that explicitly formulates the FMO
problem as a convex optimization problem in terms of all MLC deliverable apertures
and their associated intensities. However, the number of deliverable apertures, and
therefore the number of decision variables and constraints in the new problem formulation,
is typically enormous. To overcome this, we use an iterative approach that employs a
subproblem whose optimal solution either provides a suitable aperture to add to a given
pool of allowable apertures or concludes that the current solution is optimal. We are able
to handle standard consecutiveness, interdigitation, and connectedness constraints that
may be imposed by the particular MLC system used, as well as jaws-only delivery. Our
approach has the additional advantage that it can explicitly account for transmission
of dose through the part of an aperture that is blocked by the MLC system, yielding a
more precise assessment of the treatment plan than what is possible using a traditional
beamlet-based FMO problem. Finally, we develop and test two stopping rules that can be
used to identify treatment plans of high clinical quality that are deliverable very efficiently.
Tests on clinical head-and-neck cancer cases showed the efficacy of our approach, yielding
treatment plans comparable in quality to plans obtained by the traditional method with
38

a reduction of more than 75% in the number of apertures and a reduction of more than
50% in beam-on-time, with only a modest increase in computational effort. The results
also show that delivery efficiency is very insensitive to the addition of traditional MLC
constraints; however, jaws-only treatment requires about a doubling in beam-on-time
and number of apertures used. Finally, we showed the importance of accounting for
transmission effects when assessing or, preferably, optimizing treatment plan quality.
39

Table 2-2. Number of apertures without transmission effects.
Aperture-based Beamlet-basedcase Clinical Convergence
C1 C2 C3 C4 C1 C2 C3 C4 C1 C2 C3 C41 17 29 22 59 57 48 51 142 170 189 329 3342 35 45 33 115 47 47 33 132 213 230 390 6503 19 19 20 33 35 31 33 39 212 252 384 5924 23 24 24 51 29 29 24 52 262 293 449 6365 32 19 26 42 39 37 64 55 185 227 348 3786 18 29 42 52 54 65 93 83 183 211 285 3217 18 18 19 32 49 22 30 55 196 219 357 4458 50 72 86 137 77 100 86 137 173 198 327 3949 19 20 23 38 30 30 27 66 181 203 312 38410 17 19 19 47 24 27 34 59 248 295 418 611
Average 24.8 29.4 31.4 60.6 44.1 43.6 47.5 82.0 202.3 231.7 359.9 474.5
Table 2-3. Beam-on time without transmission effects.
Aperture-based Beamlet-basedcase Clinical Convergence
C1 C2 C3 C4 C1 C2 C3 C4 C1 C2 C3 C41 2.56 2.90 2.70 6.59 3.98 3.52 3.56 12.43 7.43 8.23 14.51 14.672 2.98 3.09 2.77 9.14 3.21 3.12 2.77 9.84 8.46 9.16 15.65 26.003 2.92 2.72 2.70 4.66 3.30 3.08 3.06 4.98 8.07 9.43 14.48 22.864 2.73 2.68 2.65 6.26 2.89 2.82 2.65 6.30 10.35 11.68 18.85 27.195 3.24 2.60 2.78 5.05 3.49 3.09 3.89 6.13 8.94 10.95 17.52 19.456 2.56 2.72 3.26 5.00 3.54 3.69 4.06 6.91 6.81 7.81 10.70 12.117 2.56 2.52 2.49 3.98 3.30 2.62 2.82 5.77 7.98 8.79 14.11 18.008 4.04 4.42 4.68 12.12 4.48 4.92 4.68 12.12 7.31 8.35 13.92 16.819 2.65 2.56 2.69 4.42 3.12 2.96 2.82 6.29 7.09 7.70 12.51 17.1810 2.72 2.76 2.70 6.86 2.97 2.97 3.25 7.99 10.71 12.81 18.33 26.79
Average 2.89 2.89 2.94 6.41 3.42 3.28 3.36 7.87 8.31 9.50 15.05 20.10
40

Table 2-4. Aperture-based FMO: number of apertures with transmission effects.
Clinical Convergencecase C1 C2 C3 C4 C1 C2 C3 C41 26 25 29 87 44 32 102 1062 32 31 38 79 35 62 59 1403 17 18 16 36 37 23 23 514 28 32 20 39 28 32 29 635 23 24 24 68 60 68 31 686 24 31 27 49 79 76 43 557 24 17 22 24 41 41 30 688 68 74 66 138 70 74 66 1389 18 19 20 23 56 68 55 8110 16 21 22 33 27 36 34 51
Average 27.6 29.2 28.4 57.6 47.7 51.2 47.2 82.1
Table 2-5. Aperture-based FMO: beam-on time with transmission effects.
Clinical Convergencecase C1 C2 C3 C4 C1 C2 C3 C41 2.84 2.80 2.89 7.17 3.44 2.97 4.04 7.652 2.84 2.68 2.78 6.62 2.92 3.25 3.18 8.913 2.70 2.65 2.58 4.70 3.24 2.74 2.76 5.554 2.78 2.81 2.53 5.05 2.78 2.81 2.72 6.105 2.72 2.64 2.65 6.83 3.69 3.81 2.96 6.836 2.65 2.82 2.60 4.65 3.69 3.65 2.94 4.707 2.65 2.46 2.53 3.42 3.08 3.02 2.72 5.258 4.04 4.09 3.78 8.23 4.06 4.09 3.78 8.239 2.56 2.50 2.52 3.36 3.68 3.76 3.56 6.4710 2.61 2.78 2.90 4.85 2.96 3.22 3.16 6.11
Average 2.84 2.82 2.78 5.49 3.36 3.33 3.18 6.58
Table 2-6. Aperture-based FMO: DVH criteria under C1 without transmission effects.
PTV2 PTV2 PTV1 PTV1 PTV1 PTV1 LPG RPG LSG RSGcase @93% @100% @93% @100% @110% @120% @30Gy @30Gy @30Gy @30Gy
1 99.4 98.7 100.0 99.0 4.5 0.0 21.8 18.5 33.1 100.02 99.1 98.9 99.7 97.9 9.9 0.0 49.3 100.0 100.0 100.03 99.8 99.6 100.0 99.3 2.7 0.0 20.4 18.3 n/a n/a4 98.8 98.0 100.0 100.0 2.7 0.0 10.3 4.1 54.1 17.75 98.6 97.7 100.0 100.0 8.1 0.0 42.2 0.0 44.4 34.66 99.5 99.0 100.0 98.6 6.7 0.0 26.2 36.2 n/a n/a7 99.1 98.6 100.0 99.2 2.4 0.0 0.5 46.7 24.6 100.08 99.2 98.9 100.0 98.6 9.9 0.0 28.6 4.9 100.0 52.39 99.2 98.1 100.0 99.6 2.1 0.0 5.9 39.8 36.4 100.0
10 100.0 100.0 100.0 100.0 4.3 0.0 0.2 25.4 7.7 100.0
41

Table 2-7. Aperture-based FMO: DVH criteria under C1 with transmission effects addedafter optimization.
PTV2 PTV2 PTV1 PTV1 PTV1 PTV1 LPG RPG LSG RSGcase @93% @100% @93% @100% @110% @120% @30Gy @30Gy @30Gy @30Gy
1 99.6 99.2 100.0 99.9 19.5 0.0 23.8 21.4 38.6 100.02 99.3 99.0 99.9 99.0 34.0 0.0 51.0 100.0 100.0 100.03 99.8 99.7 100.0 100.0 24.3 0.0 21.8 19.1 n/a n/a4 98.8 98.1 100.0 100.0 20.9 0.0 10.5 4.1 55.7 17.75 98.8 98.1 100.0 100.0 30.6 0.0 43.0 0.0 46.8 39.56 99.6 99.2 100.0 99.2 25.7 0.0 28.2 38.4 n/a n/a7 99.2 98.8 100.0 99.8 15.0 0.0 0.7 48.2 29.8 100.08 99.3 99.0 100.0 100.0 41.6 0.0 29.5 5.5 100.0 58.19 99.5 98.8 100.0 99.9 18.9 0.0 7.2 46.1 40.2 100.0
10 100.0 100.0 100.0 100.0 11.2 0.0 0.2 25.4 9.1 100.0
Table 2-8. Aperture-based FMO: DVH criteria under C1 with transmission effects.
PTV2 PTV2 PTV1 PTV1 PTV1 PTV1 LPG RPG LSG RSGcase @93% @100% @93% @100% @110% @120% @30Gy @30Gy @30Gy @30Gy
1 99.3 98.4 99.7 96.9 4.9 0.0 22.9 20.2 33.1 100.02 99.0 98.6 99.9 97.5 6.7 0.0 44.6 100.0 100.0 100.03 99.7 99.6 100.0 99.3 1.3 0.0 20.0 18.1 n/a n/a4 98.4 97.5 100.0 100.0 2.4 0.0 9.5 1.4 53.0 15.65 98.5 97.7 100.0 99.4 3.1 0.0 38.9 0.0 42.7 33.36 99.3 98.9 100.0 97.4 4.0 0.0 24.8 35.7 n/a n/a7 99.0 98.4 100.0 99.1 0.5 0.0 0.5 47.5 17.5 100.08 98.9 98.6 100.0 97.7 8.8 0.0 26.9 3.9 100.0 48.99 99.1 98.3 100.0 99.2 1.2 0.0 2.6 35.1 33.6 100.0
10 100.0 100.0 100.0 100.0 8.6 0.0 0.2 23.1 1.4 100.0
Table 2-9. Beamlet-based FMO: DVH criteria under C1 without transmission effects.
PTV2 PTV2 PTV1 PTV1 PTV1 PTV1 LPG RPG LSG RSGcase @93% @100% @93% @100% @110% @120% @30Gy @30Gy @30Gy @30Gy
1 99.4 99.0 99.9 98.3 5.0 0.0 19.4 17.5 32.3 100.02 99.2 98.8 99.9 98.7 3.8 0.0 43.0 96.7 100.0 100.03 99.8 99.7 100.0 99.7 2.6 0.0 19.3 17.8 n/a n/a4 98.8 98.3 100.0 100.0 1.1 0.0 9.0 1.6 53.0 16.75 98.8 98.1 100.0 100.0 3.1 0.0 37.7 0.0 39.5 32.16 99.9 98.9 100.0 98.3 8.4 0.0 24.2 34.3 n/a n/a7 99.2 98.8 100.0 99.1 1.8 0.0 0.3 46.5 14.9 100.08 99.2 98.9 100.0 99.3 14.1 0.0 28.3 4.4 100.0 51.79 99.3 98.6 100.0 98.6 0.5 0.0 2.1 34.6 33.6 100.0
10 100.0 100.0 100.0 100.0 3.7 0.0 0.2 22.8 0.0 100.0
42

(a)
(b)
Figure 2-4. Case 5: The relative volume of (a) PTV1 and (b) PTV2 that receives in excessof its prescription dose.
Table 2-10. Beamlet-based FMO: DVH criteria under C1 with transmission effects.
PTV2 PTV2 PTV1 PTV1 PTV1 PTV1 LPG RPG LSG RSGcase @93% @100% @93% @100% @110% @120% @30Gy @30Gy @30Gy @30Gy
1 99.9 99.8 100.0 100.0 69.1 1.3 32.5 27.2 55.1 100.02 99.6 99.5 100.0 99.9 96.5 0.4 59.1 99.3 100.0 100.03 99.9 99.9 100.0 100.0 94.3 0.1 25.8 21.0 n/a n/a4 99.7 99.5 100.0 100.0 100.0 6.8 17.7 10.4 74.6 40.35 99.6 99.3 100.0 100.0 83.1 1.3 48.0 2.1 56.5 56.86 99.9 99.4 100.0 100.0 75.8 0.0 33.6 41.7 n/a n/a7 99.7 99.5 100.0 100.0 96.7 1.8 4.4 59.3 42.1 100.08 99.7 99.5 100.0 100.0 86.9 1.4 40.2 18.5 100.0 70.699 99.8 99.7 100.0 100.0 72.7 0.0 9.4 54.5 51.4 100.0
10 100.0 100.0 100.0 100.0 100.0 70.6 4.7 41.7 16.1 100.0
43

(a)
(b)
Figure 2-5. The relative volume of (a) LSG and (b) RSG that receives in excess of 30 Gy.
44

CHAPTER 3NEW MODELS FOR INCORPORATING INTERFRACTION MOTION IN FLUENCE
MAP OPTIMIZATION
3.1 Introduction
Geometrical uncertainties (interfraction and intrafraction motion) in radiotherapy
treatments are likely to cause significant differences between the intended and actually
delivered dose distribution in the patient. To account for these uncertainties, the
conventional method is to add a margin to the so-called clinical target volume (CTV)
to form the so-called planning target volume (PTV). CTV refers to the specific zone
surrounding the gross tumor volume at high risk for clinical extension of the tumor and
PTV refers to the specific zone surrounding the CTV with a margin accounting for the
interfraction and intrafraction motion. Many studies (Antolak and Rosen[3], Stroom et
al. [67], Herk et al. [25] and Parker et al. [51]) derived expressions for the size of margin.
However, these margin-based methods have some theoretical and practical problems: the
prescribed dose is applied to the entire PTV (rather than the CTV only), and the margin
may not adequately model the changes in dose distributions due to the random deviations
of organ motion: the CTV may only have a very small chance to reach some of the edges
of this high dose area but in other directions it may extend beyond this area. Therefore,
the CTV may not receive adequate dose while organs close to the CTV (critical structures
or organs at-risk) may not be spared due to overdosing; moreover, the dose distribution
of PTV cannot be used to accurately evaluate the treatment plan quality; finally, the
planning dose is delivered over a number of fractions so the dose received by PTV is an
accumulated dose. Hence, the actual dose received in each fraction may significantly differ
from the planned one and the total dose may be badly estimated as well.
Because of these problems of margin-based methods, attention has recently shifted to
the development of alternative methods. The most common methods are to process the
45

static planned dose distribution by convolving it with a probability density function
(PDF) which describes the motion uncertainties (Lujan et al. [46] and Carter and
Beckham [47]). This dose-convolution method assumes shift invariance of the dose
distribution. However, internal inhomogeneities and surface curvature may lead to
violations of this assumption (Craig et al. [18]); In addition, this method assumes that the
patient is treated with an infinite number of fractions, each delivering an infinitesimally
small dose. The effect of finite fractionation appears to have a greater impact on the dose
distribution than plan evaluation parameters (Craig et al. [19]). Recently, Lu et al. [44]
showed that the motion effects can be accounted for by modifying the fluence maps. After
such modification, dose calculation is the same as those based on a static planning image.
However, this method is only suitable for the cases when the patient motion is small (Lu
et al. [44]). Chan et al. [15] introduced a robust methodology for dealing with IMRT
optimization problems under intrafractional uncertainty induced by breathing motion.
They used the idea of a motion probability mass function (PMF) along with an associated
set describing the uncertainty of this PMF as their model of data uncertainty.
In Chapter 2, we introduced an aperture-based deterministic FMO model which
is actually a margin-based model. In this chapter, we will first focus on beamlet-based
stochastic models and then move to aperture-based stochastic models and both stochastic
models account for interfraction motion. We will not consider intrafraction motion which
need to be analyzed separately. Our goals in this chapter are to
• build new beamlet-based stochastic optimization models accounting for interfractionmotion (especially due to set-up errors);
• evaluate the ability of our models to find high-quality treatment plans;
• build and solve aperture-based stochastic models by direct aperture optimizationapproach.
46

3.2 Beamlet-based Stochastic Optimization Models
3.2.1 Beamlet-based Deterministic Model
Our beamlet-based stochastic optimization models were derived from the traditional
beamlet-based deterministic FMO model, we therefore first introduce the traditional
one. The related notation can be found in Chapter 2. Beamlet-based FMO is to find
the optimal intensity (fluence map) for each beamlet and we will denote the intensity of
beamlet i ∈ N by xi, then the vector of voxel doses can be expressed as a linear function
of the intensities of the beamlets through dose deposition coefficients Dij. Then the
beamlet-based deterministic model can be written as
minimize∑
`∈L
G`(z)
subject to
zj =∑i∈N
Dijxi for j ∈ V
xi ≥ 0 for i ∈ N.
Our FMO models employ treatment plan evaluation criteria that are quadratic
one-sided voxel-based penalties (see equations 2–5 and 2–6). If we denote the set of target
voxels by VT and the set of critical structure voxels by VC (VT ∪ VC = V ), then we can
rewrite the criteria as (2–5) and (2–6) as
Fj(zj) =αs
|Vs|(max{0, T−
s − zj})2
s ∈ T, j ∈ VT
Fj(zj) =βs
|Vs|(max{0, zj − T+
s })2
s ∈ S, j ∈ V
47

where
Gs−(z) =∑j∈Vs
Fj(zj) s ∈ T, j ∈ VT
Gs+(z) =∑j∈Vs
Fj(zj) s ∈ S, j ∈ V.
Then the objective function can be re-formulated to
minimize∑j∈V
Fj(zj)
zj =∑i∈N
Dijxi for j ∈ V
xi ≥ 0 for i ∈ N.
3.2.2 First New Stochastic Optimization Model
If we could account for the uncertainties of interfraction motion in the FMO model,
much more effective treatment plans may be obtained and implicit patient-dependent
margins can be created to optimally hedge against geometry changes. Hence, we would
be able to much more effectively balance the conflicting goals of tumor dose coverage
and critical structure sparing. Integrating the interfraction motion into the FMO model
essentially transforms the deterministic optimization problem into a stochastic one since
Dij, the dose receive by each voxel at unit intensity, is no longer known with certainty.
Since the current optimization models are already challenging large-scale optimization
problems, models that explicitly account for motion may quickly become intractable. To
simplify the model, we could (since the number of fractions is relatively large) consider
replacing the coefficients Dij in the original model by their expected values E(Dij).
Implicitly, this assumes that the relevant quantity is the total dose received by each
voxel over the course of the treatment. This assumption may be appropriate for critical
48

structures but it is inappropriate for targets, where a more important measure is the
amount of dose received in each individual fraction. Hence, our model is to apply the
simplifying assumption to the critical structures, but penalize the dose to targets in each
fraction via the incorporation of a large number of scenarios. Since the number of critical
structure voxels in general is much more than that of target voxels, our assumption could
implicitly decrease the size of the stochastic model. The following new notation has been
introduced: Dij denotes the expected (or average) dose received by voxel j from beamlet
i at unit intensity; S denotes the number of scenarios; Dsij denotes the dose received by
voxel j from beamlet i at unit intensity in scenario s = 1, . . . , S and zsj denotes the dose
received by voxel j ∈ VT in scenario s = 1, . . . , S. Since the target in the traditional model
(i.e., PTV) contains interfraction motion margin but the target in our new model does
not (instead of adding margin, our model accounts for interfraction motion by generating
scenarios), the target in our model is a subset of the PTV.
Our stochastic FMO model is then formulated as follows:
minimize1
S
S∑s=1
∑j∈VT
Fj(zsj ) +
∑j∈VC
Fj(zj)
subject to
zsj =
∑i∈N
Dsijxi for j ∈ VT , s = 1, . . . , S
zj =∑i∈N
Dijxi for j ∈ VC
xi ≥ 0 for i ∈ N.
3.2.3 Second New Stochastic Optimization Model
The target cannot be severely overdosed because (i) the critical structures around the
target may be overdosed too; (ii) the tumor cannot be accurately specified and the target
may contain health tissues and/or critical structures and (iii) traditionally, the prescribed
49

dose is applied to the entire PTV which contain very high volume of normal tissues and/or
critical structures because a margin is added to the CTV. However, the target in our
stochastic model is a subset of PTV and it potentially decreases the volume of heath
organs inside of the target and then we can slightly loosen the the treatment criteria for
the overdosing to target, and therefore we can deliver adequate dose to the tumor. In the
first stochastic model, we penalize dose for both overdosing and underdosing to targets
in each fraction, then in the second model, we separate the objective function into two
parts: one is for measuring the treatment plan quality for all voxels which receive the
averaged dose over all scenarios exceeding the prescribed one (denoted by F+j ); another is
for measuring the treatment plan quality for the target voxels which receive the dose in
each scenario less than the prescribed one (denoted by F−j ). The model is a potentially
better representation of the biological considerations. The new model can be formulated as
follows:
minimize1
S
S∑s=1
∑j∈VT
F−j (zs
j ) +∑j∈V
F+j (zj)
subject to
zsj =
∑i∈N
Dsijxi for j ∈ VT , s = 1, . . . , S
zj =∑i∈N
Dijxi for j ∈ V
xi ≥ 0 for i ∈ N.
Note that this method implicitly decreases the size of the problem because instead of
evaluating the treatment quality for the overdosed target voxels for each scenario, the new
model evaluates the overdosed target voxels based on averaged doses. Since this model put
penalty for the underdosing target voxels in each scenario, most likely, adequate doses can
be delivered to the target.
50

3.2.4 Results
3.2.4.1 Clinical problem instances
To test our models, we use five clinical cases of prostate cancer. Please refer to
Chapter 2 for detail information about the sizes of bixes and voxels, how to import data,
etc. For all five cases, we design plans using nine equispaced 60Co-beams. The nine beams
are evenly distributed around the patient with angles 0◦, 40◦, 80◦, 120◦, 160◦, 200◦, 240◦,
280◦, 320◦, respectively. There are one target (prostate) with prescription dose 73.8 Gy
and three critical structures: bladder, rectum and femoral head. Table 3-1 shows the
problem dimensions for the five cases.
Table 3-1. Model dimensions.
Case total # voxels # voxels in the models # bixels1 205,911 35,988 2,0552 131,216 22,330 2,2533 226,324 38,731 2,6534 162,628 29,828 2,4135 262,184 40,636 2,736
Since our model could account for the interfraction motion, the target in the
optimization model is the CTV with the intrafraction motion margin. Empirically, the
standard deviation of set-up errors in each direction has been found to be approximately
3 mm (El-Bassiouni et al. [22], Britton et al. [12], Price [53] and Wang et al. [69]) and
we therefore generated 200 scenarios by perturbing the location of the patient according
to a normal distribution with a mean of 0 and a standard deviation of 3 mm in each
coordinate direction for each case. For target, we test the dose coverage for individual
scenarios; for critical structures, we check the averaged dose distribution over all scenarios.
Dose-volume criteria and constraints have been established to keep toxicity at acceptable
levels. However, PTV is the CTV with interfraction and intrafraction motion margins
and the target in our model is CTV with intrafraction motion margin so the traditional
51

DVH criteria for PTV are not suitable for the target in our models. We therefore evaluate
the target dose coverage for each individual scenario: we estimate the probability that a
fraction β of the target receives the prescription dose, for different values of β. For critical
structures, specifically for prostate radiation therapy, we use the Radiation Therapy
Oncology Group criteria ([57]) (in Table 3-2) which are commonly used by physicians and
researchers (Moiseenko et al. [48], Rodrigues et al. [59] and Chen et al. [16]). Finally, we
compare our solutions with the ones obtained from the traditional method. The width of
the set-up error margin is set to be about 1.65 times the standard deviation (see Antolak
and Rosen [3]). Hence, 5 mm of margin in each direction has been added to the target for
the traditional method.
Table 3-2. Radiation Therapy Oncology Group (RTOG P0126) criteria for prostate cancer.
Rectum Bladder≤ 15% to receive ≥ 75 Gy ≤ 15% to receive ≥ 80 Gy≤ 25% to receive ≥ 70 Gy ≤ 25% to receive ≥ 75 Gy≤ 35% to receive ≥ 65 Gy ≤ 35% to receive ≥ 70 Gy≤ 50% to receive ≥ 60 Gy ≤ 50% to receive ≥ 65 Gy
Our FMO models employ treatment plan evaluation criteria that are quadratic
one-sided voxel-based penalties. We tuned the problem parameters (underdose and
overdose thresholds and criteria weights) by manual adjustment. In general, compared
to the traditional model, we increase the penalty weights to the target dose distributions
while decrease the penalty weights to the critical structures dose distributions. The models
were solved by our in-house primal-dual interior point algorithm. All experiments were
performed on a PC with 2.66 GHz Intel Quad CPU and 4 GB of RAM, running under
Windows Vista. Our algorithms were implemented in Matlab 7.
3.2.4.2 Results
We first test the effects of varying the number of scenarios that is included in
the optimization models. A large number of scenarios will lead to unacceptable CPU
52

running time while a small number of scenarios may be insufficient to capture the actual
uncertainties and may therefore result in unacceptable treatment quality. By testing
different number of scenarios included in the models, we could find a balance between the
computation effort and the treatment quality. We include 25, 50, 75 and 100 scenarios
in the two optimization models and test the treatment qualities for scenarios which
are in and out of the optimization models. Taking Case 1 as an example, Figure 3-1
and 3-2 estimate the probability that a specified percentage of the target received the
prescription dose for two models, respectively. We observe that the treatment qualities
from the scenarios out of the optimization models are not as good as ones included in the
optimization models if we only include 25, 50 or 75 scenarios in the models. For instance,
if we include 25 scenarios in the first optimization model, for all these 25 scenarios, at
least 95% of target volume could receive the prescription dose, however, there are only
21 out of 25 scenarios (i.e., 84%) out of the optimization model in which at least 95%
of target volume could receive the prescription dose. If we include 100 scenarios in the
models, the treatment qualities obtained from the scenarios out of the optimization models
are very similar with the ones obtained from the scenarios in the optimization models
(see Figure 3-1 and 3-2). By testing all five cases, we conclude that 100 is the (estimated)
minimal number of scenarios which should include in both optimization models in order to
obtain the stable treatment quality for all available scenarios.
Figures 3-3 to 3-7 estimate the probability that a specified percentage of the target
received the prescription dose for Scenarios 1-100 and 101-200, respectively, for the five
cases. No remarkable differences are observed between the scenarios in and out of the
optimization models. We observe that, in general, our stochastic models obtain better
target dose coverage than the traditional model does. Taking Case 1 as an example, the
probability of 95% target coverage is 98% for the first stochastic model; the probability
53

(a) (b)
(c) (d)
Figure 3-1. The probability that a specified percentage of the target received theprescription dose for Case 1 (first stochastic model).
is 99% for the second stochastic model; while by solving the traditional model, that
probability is only 91%. In particular, the second stochastic model obtain slightly better
target dose coverage than the first one. Figure 3-8 and 3-9 show the DVHs for the critical
structures for the two stochastic models compared to the traditional method, respectively.
Table 3-4 lists the corresponding DVH values based on the criteria. We conclude from
Figure 3-8, 3-9 and Table 3-4 that our methods could obtain better target dose coverage
with (almost) no additional dose to the critical structures.
Besides estimating the probability that a specified percentage of the target receive
the prescription dose for the two models, we would like to check another two important
54

(a) (b)
(c) (d)
Figure 3-2. The probability that a specified percentage of the target received theprescription dose for Case 1 (second stochastic model).
criteria: target coldspots (underdosing) and hotspots (overdosing) which refer to the
volume of target which receives less than 93% and more than 110% of prescription dose,
respectively. Table 3-3 shows the averaged hotspots for all five cases. We observe that
even though the second stochastic model obtain better target dose coverage than the
traditional and the first stochastic model, in general, it does not have higher hotspots. In
most of scenarios, 100% of target receive at least 93% of prescription dose for all five cases
so there are almost no coldspots for all models.
Our stochastic optimization models take individual dose distributions for target into
account and robust treatment plans can be obtained while the traditional method does not
55

have this merit: in some extreme scenarios, the treatment quality may be very bad using
the traditional method. We would like to take Case 1 as an example to check the target
dose coverage for Scenario 135. Note that this scenario is not included in the optimization
models. Figure 3-10 and 3-11 show the DVHs for first and second stochastic models
compared to the traditional method, respectively. We can see that about 96% and 98%
of target receive the prescription dose (73.8 Gy) by solving the first and second stochastic
models, respectively, while for the traditional method, that volume is only 92%.
The amount of time required, on average, by our optimization algorithms to find the
solutions ranges from about 3–7 minutes of CPU time for two models while it takes less
than 2 minutes to solve the traditional model. Moreover, the time required by the second
stochastic model is less than the first model due to the smaller size of the model. Table
3-5 records the CPU time for these three methods.
Finally, recall that the traditional method does not account for interfraction motion
in either the optimization model or its reporting of the treatment plan quality. Hence,
the perceived treatment plan quality may differ from the actual one. To assess this effect,
we compared the perceived DVHs reported from the traditional model with the actual
DVHs that take into account the uncertainty using the 200 scenarios from the interfraction
motion model. The results indicate that the perceived DVHs for critical structures are
very close to the actual ones (see examples in Figure 3-12). However, the perceived
DVHs overestimate the dose distribution to the targets (see results in Figure 3-13). This
further underscores the importance of taking interfraction motion uncertainty into account
explicitly.
56

(a) (b)
Figure 3-3. The probability that a specified percentage of the target received theprescription dose for Case 1.
(a) (b)
Figure 3-4. The probability that a specified percentage of the target received theprescription dose for Case 2.
(a) (b)
Figure 3-5. The probability that a specified percentage of the target received theprescription dose for Case 3.
57

(a) (b)
Figure 3-6. The probability that a specified percentage of the target received theprescription dose for Case 4.
(a) (b)
Figure 3-7. The probability that a specified percentage of the target received theprescription dose for Case 5.
Table 3-3. Hotspots (%) for three models.
Case traditional model stochastic model 1 stochastic model 21 1.65 2.59 2.072 3.63 4.55 4.753 6.41 4.36 4.704 1.97 4.61 1.465 3.00 4.01 2.17
58

(a) (b)
(c) (d)
(e)
Figure 3-8. DVHs for critical structures (first stochastic model vs. traditional model).
59

(a) (b)
(c) (d)
(e)
Figure 3-9. DVHs for critical structures (second stochastic model vs. traditional model).
60

(a)
Figure 3-10. DVHs for Case 1 in Scenario 135 (first model vs. traditional model).
(a)
Figure 3-11. DVHs for Case 1 in Scenario 135 (second model vs. traditional model).
61

Table 3-4. DVH criteria for critical structures (%).
Rectum BladderCase @75 Gy @70 Gy @65 Gy @60 Gy @80 Gy @75 Gy @70 Gy @65 Gy
(≤ 15%) (≤ 25%) (≤ 35%) (≤ 50%) (≤ 15%) (≤ 25%) (≤ 35%) (≤ 50%)1 Trad. 8.37 11.91 14.78 17.40 0.57 6.09 9.51 12.30
Stoch. 1 7.05 10.25 13.25 15.32 0.74 5.88 9.97 13.32Stoch. 2 9.29 12.35 15.16 16.92 0.68 10.47 15.06 17.97
2 Trad. 3.99 6.22 8.45 11.09 0.82 6.88 8.45 10.09Stoch. 1 5.53 8.09 11.11 14.41 4.11 8.79 10.63 13.63Stoch. 2 10.65 13.43 16.64 20.08 7.70 13.12 16.57 20.16
3 Trad. 2.70 14.13 17.17 22.85 0.79 11.36 16.82 24.95Stoch. 1 0.00 13.57 18.83 25.76 0.00 3.77 13.29 17.06Stoch. 2 2.77 9.69 16.06 20.49 0.00 2.58 9.52 14.48
4 Trad. 13.79 20.15 25.82 30.86 0.42 4.65 6.87 8.71Stoch. 1 13.64 20.50 25.33 30.02 0.95 4.40 6.83 8.65Stoch. 2 10.56 17.98 22.95 27.40 0.54 3.21 5.60 7.13
5 Trad. 11.20 19.52 25.41 29.57 0.29 4.45 6.93 8.99Stoch. 1 11.20 18.07 24.64 28.88 0.08 3.82 6.39 8.38Stoch. 2 8.21 15.46 20.29 25.60 0.14 2.63 4.90 6.96
Table 3-5. CPU running time (seconds) for three models (%).
Case traditional model stochastic model 1 stochastic model 21 45 312 2712 42 201 1493 71 467 3754 67 308 2465 89 301 251
(a) (b)
Figure 3-12. Perceived and actual DVHs for critical structures for Case 1 and Case 2
62

(a) (b)
(c) (d)
(e)
Figure 3-13. Perceived and actual DVHs for target.
63

3.3 Aperture-based Stochastic Optimization Models
3.3.1 Aperture-based Stochastic Optimization Models
In Chapter 2, we used a direct aperture optimization approach to design radiation
therapy treatment plans for individual patients which integrates the beamlet-based
FMO and leaf-sequencing problems into a single optimization model. We can apply this
approach to our beamlet-based stochastic optimization models. The related notation can
be found in Chapter 2. The first aperture-based stochastic FMO model can be formulated
as follows:
minimize1
S
S∑s=1
∑j∈VT
Fj(zsj ) +
∑j∈VC
Fj(zj)
subject to
zsj =
∑
k∈K
Dskjyk for j ∈ VT , s = 1, . . . , S (3–1)
zj =∑
k∈K
Dkjyk for j ∈ VC (3–2)
yk ≥ 0 for all k ∈ K (3–3)
where
Dskj =
∑i∈Ak
Dsij for j ∈ VT , s = 1, . . . , S
Dkj =∑i∈Ak
Dij for j ∈ VC .
If we incorporate the transmission effect, we obtain the following expression for the dose
deposition coefficients:
Dskj = (1− ε)
∑i∈Ak
Dsij + ε
∑i∈Nbk
Dsij for j ∈ VT , s = 1, . . . , S
Dkj = (1− ε)∑i∈Ak
Dij + ε∑
i∈Nbk
Dij for j ∈ VC .
64

The second aperture-based stochastic FMO model can be formulated as follows:
minimize1
S
S∑s=1
∑j∈VT
F−j (zs
j ) +∑j∈V
F+j (zj)
subject to
zsj =
∑
k∈K
Dskjyk for j ∈ VT , s = 1, . . . , S (3–4)
zj =∑
k∈K
Dkjyk for j ∈ V (3–5)
yk ≥ 0 for all k ∈ K. (3–6)
3.3.2 Derivation of the Pricing Problem
In Chapter 2, we derived the pricing problem for the aperture-based static FMO
model. Similarly, we can derive the pricing problem for these two aperture-based
stochastic models. Note that the Karush-Kuhn-Tucker (KKT) optimality conditions
are still necessary and sufficient for optimality because of the convexity of the objective
function and the linearity of the constraints for the two models. In our two stochastic
models, we check the target dose for each scenario with additional constraints (3–1) and
(3–4), respectively, therefore we need to denote new dual multipliers associated with them
to derive the KKT conditions. We first derive the pricing problem for the first model: let
us denote the dual multipliers associated with constraints (3–1), (3–2)and (3–3) by πsj
(j ∈ VT , s = 1, . . . , S), ωj (j ∈ VC) and ρk (k ∈ K), then the KKT conditions can be
written as follows:
πsj =
1
S
∂F (zs)
∂zsj
for j ∈ VT , s = 1, . . . , S
ωj =∂F (z)
∂zj
for j ∈ VC
ρk =S∑
s=1
∑j∈VT
Dskjπ
sj +
∑j∈VC
Dkjωj for k ∈ K
65

zsj =
∑
k∈K
Dskjyk for j ∈ VT , s = 1, . . . , S
zj =∑
k∈K
Dkjyk for j ∈ VC
ykρk = 0 for k ∈ K
yk, ρk ≥ 0 for k ∈ K.
Similar with previous chapter, any solution to this system can be characterized by
y ≥ 0 only: this vector then determines zs, z, πs, ω, and ρ. Let (y; πs, ω, ρ) be an optimal
pair of primal and dual solutions to a subproblem problem in which only apertures in
the set K ⊂ K are considered, where we have set yk = 0 for k ∈ K\K. Using the same
method in Chapter 2, we conclude that the current solution is optimal if and only if the
optimal solution to the following optimization problem
minimizek∈Kb
∑i∈Ak
(S∑
s=1
∑j∈VT
Dsijπ
sj +
∑j∈VC
Dijωj
)
exceeds the threshold value (A)
− ε
1− ε
∑i∈Nbk
(S∑
s=1
∑j∈VT
Dsijπ
sj +
∑j∈VC
Dijωj
).
In the second stochastic model let us denote the dual multipliers associated with
constraints (3–4), (3–5)and (3–6) by πsj (j ∈ VT , s = 1, . . . , S), ωj (j ∈ V ) and ρk (k ∈ K),
then the KKT conditions can be written as follows:
πsj =
1
S
∂F−(zs)
∂zsj
for j ∈ VT , s = 1, . . . , S
ωj =∂F+(z)
∂zj
for j ∈ V
ρk =S∑
s=1
∑j∈VT
Dskjπ
sj +
∑j∈V
Dkjωj for k ∈ K
66

zsj =
∑
k∈K
Dskjyk for j ∈ VT , s = 1, . . . , S
zj =∑
k∈K
Dkjyk for j ∈ V
ykρk = 0 for k ∈ K
yk, ρk ≥ 0 for k ∈ K.
Finally we conclude that the current solution is optimal if and only if the optimal solution
to the following optimization problem
minimizek∈Kb
∑i∈Ak
(S∑
s=1
∑j∈VT
Dsijπ
sj +
∑j∈V
Dijωj
)
exceeds the threshold value (B)
− ε
1− ε
∑i∈Nbk
(S∑
s=1
∑j∈VT
Dsijπ
sj +
∑j∈V
Dijωj
).
Note that we obtained the same form of expressions (A) and (B) as in Chapter 2:∑S
s=1
∑j∈VT
Dsijπ
sj +
∑j∈VC
Dijωj and∑S
s=1
∑j∈VT
Dsijπ
sj +
∑j∈V Dijωj measure the
per-unit change in objective function value if the intensity of beamlet i is increased for the
two models, respectively.
3.3.3 Results
In Chapter 2, by testing on clinical head-and-neck cancer cases, we showed the
efficacy of this approach compared to the traditional method. The results indicate that
delivery efficiency is very insensitive to the addition of traditional MLC constraints;
however, jaws-only treatment requires about a doubling in beam-on time and number of
apertures used. We also showed the importance of accounting for transmission effects. In
this chapter, we focus on the effects of these two stochastic models where the transmission
effects are taken into account.
67

In Chapter 2, we developed convergence and clinical stopping rules based on the
treatment quality (in particular, we checked the DVHs in each iteration). Note the
traditional DVH criteria for PTV are not suitable for the target in our stochastic models,
we therefore check the target dose coverage (by estimating the probability that a fraction
β of the target receives some certain dose, for different values of β) in each iteration in the
convergence stopping rule. Our new two stopping rules are:
• Convergence:This stopping rule is based on observing that treatment plan quality, with respect toa particular criterion, has not improved markedly in recent iterations. In particular,in each iteration, we check the probabilities that at least 95%, 97% and 99% oftarget receive the prescription dose; the probabilities that at most 10% of targetreceive dose at hotspot; the average volume of bladder received doses at 65 Gy, 70Gy, 75 Gy and 80 Gy over all scenarios; the average volume of rectum received dosesat 60 Gy, 65 Gy, 70 Gy and 75 Gy over all scenarios. More formally, we say that weare satisfied with the solution with respect to a particular criterion if, in the last 5iterations, the range of observed criterion values spans less than δ = 2%.
• Clinical:This stopping rule is based on observing that the treatment plan performance withrespect to a clinical criterion has been satisfactory in the last 5 iterations. Moreformally, we say that we are satisfied with the solution with respect to a particularcriterion if either the first stopping rule is satisfied or, in the last 5 iterations, forcritical structures, the clinical DVH criteria are satisfied based on the average dosesover all scenarios; for target, the average volume of target received prescription doseover all scenarios is more than 95% and the average volume of target received doseat hotspot over all scenarios is less than 10%.
Tables 3-6 to 3-9 show the number of apertures and beam-on time for the two
stochastic models according to four different MLC constraints, respectively. No big
differences are observed with these two stochastic models. Taking Case 1 as an example,
Figure 3-14 shows the target dose coverage for two stochastic models with two stopping
rules. By observing all five cases, we conclude that in general, the second stochastic model
yields slightly better target dose coverage.
68

3.4 Concluding Remarks
Our stochastic optimization models take individual dose distributions for target
into account and robust treatment plans can be obtained with only a modest number
of scenarios. The target dose coverage improves not only for the scenarios included
in the model but also in other scenarios. In general, the treatment plans obtained by
our approach are better than that of the traditional method. The CPU time required
for solving the beamlet-based models ranges about 3–7 minutes and for solving the
aperture-based models ranges about 3–20 minutes for the 100-scenario models, and
therefore feasible in a clinical setting. In addition, the second stochastic model obtained
slightly better target dose coverage than the the first one while the CPU time required
is relatively low (3-6 minutes for the beamlet-based model and 3-12 minutes for the
aperture-based model). As a by product, we conclude that the traditional model
overestimates the dose distribution to the target.
69

Table 3-6. C1: Number of apertures and beam-on time.
Number of apertures Beam-on timeStochastic model 1 Stochastic model 2 Stochastic model 1 Stochastic model 2
case Clinical Convergence Clinical Convergence Clinical Convergence Clinical Convergence1 17 51 20 42 2.47 3.22 2.54 3.152 19 59 40 68 2.37 3.49 3.93 5.153 37 46 50 50 2.95 3.14 3.22 3.224 16 47 21 39 2.12 2.96 2.25 2.785 17 50 22 41 2.33 3.18 2.50 2.91
Average 21.2 50.6 30.6 48.0 2.45 3.20 2.89 3.44
Table 3-7. C2: Number of apertures and beam-on time.
Number of apertures Beam-on timeStochastic model 1 Stochastic model 2 Stochastic model 1 Stochastic model 2
case Clinical Convergence Clinical Convergence Clinical Convergence Clinical Convergence1 17 45 19 34 2.39 3.05 2.43 2.752 16 45 22 37 2.29 3.09 2.37 2.773 20 34 20 31 2.63 2.85 2.52 2.984 19 43 20 36 2.36 2.77 2.26 2.645 21 37 24 45 2.10 2.74 2.54 2.84
Average 18.6 40.8 21.0 36.4 2.35 2.90 2.42 2.90
Table 3-8. C3: Number of apertures and beam-on time.
Number of apertures Beam-on timeStochastic model 1 Stochastic model 2 Stochastic model 1 Stochastic model 2
case Clinical Convergence Clinical Convergence Clinical Convergence Clinical Convergence1 17 29 17 33 2.49 2.76 2.41 2.972 17 46 27 50 2.22 2.98 2.63 3.063 23 37 22 36 2.52 2.80 2.78 3.424 28 52 32 59 2.39 2.89 2.24 2.935 29 44 33 40 2.56 2.73 2.59 2.90
Average 22.8 41.6 26.2 45.6 2.43 2.83 2.53 3.05
Table 3-9. C4: Number of apertures and beam-on time.
Number of apertures Beam-on timeStochastic model 1 Stochastic model 2 Stochastic model 1 Stochastic model 2
case Clinical Convergence Clinical Convergence Clinical Convergence Clinical Convergence1 21 56 37 75 2.77 5.37 3.91 6.092 18 37 25 41 2.40 4.68 3.08 4.843 27 59 27 58 2.33 5.87 3.10 5.124 22 42 24 57 2.70 3.92 2.90 5.145 25 63 33 63 2.83 5.37 3.48 5.29
Average 22.6 51.4 29.2 58.8 2.60 5.04 3.29 5.30
70

Figure 3-14. Target dose coverage for two models with two stopping rules.
71

CHAPTER 4OPTIMIZATION MODELS FOR PATIENT SCHEDULING PROBLEMS IN PROTON
THERAPY DELIVERY
4.1 Introduction
Patient scheduling problems are well-studied in the literature and most of the studies
have been focused on outpatient scheduling. The objective of outpatient scheduling is to
find an appointment system for which a particular measure of performance is optimized
in a clinical environment. Well-designed appointment systems have the potential to
increase the utilization of expensive personnel and equipment-based medical resources
as well as reducing waiting times for patients. An excellent comprehensive survey of
research on appointment scheduling in outpatient services can be found in Cayirli and
Veral [13] and Cayirli et al. [14]. However, there are only a few studies (e.g., Conforti et
al. [17]) concerning patient scheduling in the area of radiation therapy treatment patient
scheduling which has the following special concerns (but not limited to):
• Treatment continuity. In general, the treatment plans are delivered during 5-7 weeksand the treatment can not be terminated until all fractions have been delivered;
• Multi-daily-fraction treatments. Due to the medical necessity, some patients needto be treated twice or even more fractions per day. The minimum number of hoursbetween fractions in the same day is required;
• The first treatment fraction. In general, the new patients have to be started in somespecified day/time when the certified physicians or doctors are available; moreover,additional time is needed for the first fraction treatment;
• Anesthesia cases. The anesthesia patients also have to be treated in some specifiedday/time when certified physicians or doctors are available.
1 This chapter is joint work with Ehsan Salari
72

Improper patient scheduling may have a severer impact on the treatment quality or even
reduce the survival rate: the patients may miss the best treatment time due to a long
waiting time; some fractions may not be delivered at the right time or even be missed.
In this chapter, we first develop and implement strategic optimization models and test
them using data from the University of Florida Proton Therapy Institute (UFPTI) and
the main goals are to:
• analyze the treatment capacity;
• determine potential ways in which operations can be streamlined in order to increasethe utilization of the available resources.
Moreover, we have defined and modeled the on-line patient scheduling problem for
proton therapy treatments at the UFPTI, and proposed a local search heuristic for solving
this problem. The main contribution of this study lies in its precise and unique modeling
approach which has captured all operational details of the problem. Furthermore, on the
solution side, the local search heuristic developed allows for an efficient, real-time solution
of the problem.
The UFPTI is the newest proton facility in the US, performing its first patient
treatment in August 2006. It is one of only several proton therapy facilities operating
in the nation, and the only proton therapy facility in the Southeast. Due to the fact
that the technology is novel and scarce, efficient patient scheduling is essential. To date,
the UFPTI has delivered more than 21,000 proton therapy treatments, to patients with
head-and-neck, skull-base, sarcoma, prostate, pancreas and pituitary cancers. It is under
great pressure to increase the capacity due to the large number of patients requiring
or desiring treatment. Currently, the UFPTI has three proton treatment rooms, each
equipped with one gantry, and treats the patients from 6:00 am to 9:00 pm for each
business day. Since most of these patients (about 80%) suffer from prostate cancer, the
Gantry 3 is commissioned for these patients only. Due to clinical reasons and limitations
73

of physicians, new patients only start their first treatment from Monday to Wednesday
during prime hours (9:00 am to 4:00 pm) and anesthesia patients can only be treated
within 4 hours in Gantry 1.
4.2 Building the Strategic Models
4.2.1 The Objective Function
Based on treatment site, treatment time per fraction, total number of fractions,
number of fractions per day, snout size, etc., patients are classified into several categories
reflecting the various disease sites and levels of treatment complexity, or patient mix. The
objective of the first model is to maximize the number of fractions treated in the facility
under certain operational conditions and the desired patient mix. We denote the number
of patient categories by K (indexed by k) and the number of gantries by G (indexed by g).
For each patient in Category k, we let nk denote the total number of treatment days, fk
denote the number of fractions per day, ck denote the number of time units consumed per
fraction, and ck denote the number of additional time units consumed in the first fraction.
In addition, we let T denote the planning horizon (indexed by t). There are two sets of
decision variables: xtkg and ytkg which denote the number of patients in Category k who
start the treatment on day t in gantry g and the total number of patients in Category k
who are treated on day t in gantry g, respectively. Then the objective function can be
formulated as follows:
maximize1
T
T∑t=1
K∑
k=1
G∑g=1
fkytkg.
Note that a patient in Category k who starts the treatment on day t is treated on
days t, . . . , t + nk − 1 (k = 1, . . . , K; t = 1, . . . , T ); a patient in Category k that is treated
on day t must have started on one of the following days: t − nk + 1, . . . , t (k = 1, . . . , K;
t = 1, . . . , T ). Therefore, the following relationship between the sets of decision variables
74

has to hold:
ytkg =
nk∑n=1
xt−n+1,kg k = 1, . . . , K; t = 1, . . . , T ; g = 1, . . . , G.
4.2.2 The Constraints
4.2.2.1 The capacity
The patients in the same Category use the same snout size (then the snout changing
is not necessary). Let Ks denote the set of categories using snout size s, S denote the total
number of snout sizes, and α denote the snout changing time. Moreover, let Istg denote
an indicator variable showing if snout size s is used on gantry g on day t or not, in other
words:
Itsg =
1∑
k∈Ksytkg > 0
0 otherwise.
In general, the snout has been set up every morning before the treatment starts, so the
snout changing time is not counted for the first patient. If we denote the available time
per day for gantry g by Cg, then the gantry capacity constraints and the additional
constraints required are:
K∑
k=1
ckxtkg +K∑
k=1
ckfkytkg ≤ Cg − α(S∑
s=1
Itsg − 1) t = 1, . . . , T ; g = 1, . . . , G
∑
k∈Ks
ytkg ≤ MItsg t = 1, . . . , T ; s = 1, . . . , S; g = 1, . . . , G
Itsg ∈ {0, 1} t = 1, . . . , T ; s = 1, . . . , S; g = 1, . . . , G.
Note that α(∑S
s=1 Itsg − 1) is a lower bound of the snout changing time on day t for gantry
g.
75

4.2.2.2 The patient mix
The desired patient mix can be implemented either as a set of constraints or as a
penalty term in the objective function. First, assume the desired patient mix is given as a
number, say dk for k ∈ K (with∑
k∈K dk = 1). Then, in a continuous model, the patient
mix constraints are
T∑t=1
G∑g=1
xtk′g = dk′
T∑t=1
K∑
k=1
G∑g=1
xtkg k′ = 1, . . . , K.
For the integral model, these constraints could be replaced by
dk′
T∑t=1
K∑
k=1
G∑g=1
xtkg − 1
2≤
T∑t=1
G∑g=1
xtk′g ≤ dk′
T∑t=1
K∑
k=1
G∑g=1
xtkg +1
2k′ = 1, . . . , K.
Second, if we denote the penalty for deviating from the desired patient mix by Fk for
Category k, then the objective function containing the penalty term can be formulated as
follows:
maximizeT∑
t=1
K∑
k=1
G∑g=1
fkytkg −K∑
k=1
Fk
(T∑
t=1
G∑g=1
xtkg − dk
T∑t=1
K∑
k′=1
G∑g=1
xtk′g
).
4.2.2.3 New patients’ treatment starting-time
We can impose the constraint that new patients should start their treatment only on
particular days. Let TNA denote the set of non authorized days to start new patients, in
this case the set of constraints to ensure that new patients only start their treatment in
authorized days are:
xtkg = 0 t ∈ TNA; k = 1, . . . , K; g = 1, . . . , G.
4.2.2.4 Anesthesia cases and twice-a-day fractions
Let Ka denote the set of categories for anesthesia patients and C ′g is the maximal
amount of time each day in gantry g for anesthesia patients. let I ′tsg denote an indicator
76

variable showing if snout size s is used on gantry g on day t by anesthesia patients or not,
in other words:
I ′tsg =
1∑
k∈Ks⋂
Ka ytkg > 0
0 otherwise.
Then the capacity constraints for anesthesia patients are
∑
k∈Ka
(ckxtkg + ckfkytkg) ≤ C ′g − α
S∑s=1
I ′tsg t = 1, . . . , T ; g = 1, . . . , G
∑
k∈Ks⋃
Ka
ytkg ≤ MI ′tsg t = 1, . . . , T ; s = 1, . . . , S; g = 1, . . . , G
I ′tsg ∈ {0, 1} t = 1, . . . , T ; s = 1, . . . , S; g = 1, . . . , G.
Suppose that K2 is the set of categories for patients with twice-a-day fractions, and
let the minimal time between 2 fractions be equal to τ . If these patients are treated in
the same order and on the same gantry on a particular day, then we in principle only
need to make sure that the second set of fractions for these patients starts at least τ time
units after the start of the day. We also need to take into account that for some of these
patients the current day may be the first day, we should add in the additional time for this
in the morning as well. The constraints then can be formulated as follows:
∑
k∈K2
(ckxtkg + ckytkg) ≤ Cg − τ t = 1, . . . , T ; g = 1, . . . , G.
4.2.2.5 Gantry specialization and gantry switching
Constraints related to specializing a gantry to a certain patient category can be
defined as follows: if gantry g is specialized to treat patients in categories in the set Kg
only (g = 1, . . . , G), we should impose
ytkg = 0 t = 1, . . . , T ; k 6∈ Kg; g = 1, . . . , G.
77

Similarly, if patients in Category k can only be treated on gantries in the set Gk (k =
1, . . . , K) we should impose
ytkg = 0 t = 1, . . . , T ; k = 1, . . . , K; g 6∈ Gk.
Note that the formula
ytkg =
nk∑n=1
xt−n+1,kg k = 1, . . . , K; t = 1, . . . , T ; g = 1, . . . , G
potentially assumes that gantry switching is not allowed (once a patient starts the
treatment in a certain gantry, he/she can not move to other gantries for the all treatment
fractions). If gantry switching is allowed, the following relationship has to hold:
G∑g=1
ytkg =G∑
g=1
nk∑n=1
xt−n+1,kg k = 1, . . . , K; t = 1, . . . , T.
4.2.3 The Optimization Model
The model without gantry switching and specialized gantries can now be formulated
as:
maximize1
T
T∑t=1
K∑
k=1
G∑g=1
fkytkg
subject to
78

y tkg
=
nk ∑ n
=1
xt−
n+
1,k
gk
=1,
...,
K;t=
1,..
.,T
;g
=1,
...,
G
K ∑ k=
1
c kx
tkg+
K ∑ k=
1
c kf k
y tkg≤
Cg−
α(
S ∑ s=1
I tsg−
1)t=
1,..
.,T
;g=
1,..
.,G
dk′
T ∑ t=1
K ∑ k=
1
G ∑ g=
1
xtk
g−
1 2≤
T ∑ t=1
G ∑ g=
1
xtk′ g≤
dk′
T ∑ t=1
K ∑ k=
1
G ∑ g=
1
xtk
g+
1 2k′ =
1,..
.,K
∑ k∈K
a
(ckx
tkg+
c kf k
y tkg)≤
C′ g−
α
S ∑ s=1
I′ ts
gt=
1,..
.,T
;g=
1,..
.,G
∑ k∈K
2
(ckx
tkg+
c ky t
kg)≤
Cg−
τt=
1,..
.,T
;g=
1,..
.,G
xtk
g=
0t∈
TN
A;k
=1,
...,
K;g
=1,
...,
G
∑ k∈K
s
y tkg≤
MI t
sgt=
1,..
.,T
;s
=1,
...,
S;g
=1,
...,
G
I tsg∈{0
,1}
t=
1,..
.,T
;s
=1,
...,
S;g
=1,
...,
G
∑
k∈K
s⋃
Ka
y tkg≤
MI′ ts
gt=
1,..
.,T
;s
=1,
...,
S;g
=1,
...,
G
I′ ts
g∈{0
,1}
t=
1,..
.,T
;s
=1,
...,
S;g
=1,
...,
G
xtk
g,y
tkg≥
0t=
1,..
.,T
;k
=1,
...,
K;g
=1,
...,
G
xtk
g,y
tkg∈
Nt=
1,..
.,T
;k
=1,
...,
K;g
=1,
...,
G
79

4.2.4 The Model with Penalty Function
The IP model in Section 4.2.3 requires a lot of computational effort to solve. We
notice that the patients mix constraints are very hard to satisfy because the feasible region
defined by these constraints is very limited and therefore finding a feasible solution is
very expensive. However, in practise, the actual patient mix is allowed to have a small
deviation with the planned one. We therefore split constraints into “hard” and “easy”:
eliminate “hard” constraints, but penalize the violation in the cost function. Then the
objective function and related constraints can be formulated as follows:
maximizeT∑
t=1
K∑
k=1
G∑g=1
fkytkg −K∑
k=1
wkUk
with additional constraints (A)
−Uk′ ≤T∑
t=1
G∑g=1
xtkg − dk′
T∑t=1
K∑
k=1
G∑g=1
xtkg ≤ Uk′ k′ = 1, . . . , K
Uk ≥ 0 k = 1, . . . , K.
Where wk is the penalty weight. The model explicitly maximizes the number the fractions
while ensures that the patient mix constraints can be satisfied in a certain level. When
solving this model, it is crucial to adjust the right penalty weights since assigning different
weights represents different levels of attention paid to satisfying the patient mix. Note that
both the number of fractions and the deviation of patient mix (|Uk|) decrease by increasing
the weights but larger penalty weights have longer running times, so the weights should be
chosen as small as possible while ensuring an acceptable level of patient mix. Moreover,
they should be adjusted in such a way that the exact patient mix is attainable for the
optimal solution of the LP relaxation model. Note here the LP relaxation model refers
to the model above by only setting xtkg’s and ytkg’s continuous (Itsg’s and I ′tsg’s are still
80

binary variables). We will denote the step size by s and the algorithm for adjusting the
weights would be as follows:
1. Set wk = 0 for k ∈ K.
2. Solve the LP relaxation of model (A).
3. If mink∈K
|Uk| > 0, go to Step 4 otherwise go to Step 5.
4. wk = wk + s for k ∈ K. Go to Step 2.
5. Solve MIP model (A).
4.2.5 Results
4.2.5.1 Input data
We tested the strategic model with penalty function in ILOG CPLEX 11.1 on a PC
with a 3.4 GHz Intel Pentium IV processor and 2 GB of RAM, running under Windows
XP. The input data was given by UFPTI. Table 4-1 shows the patient classification and
patient mix. In addition, the following concerns or constraints are applied to the model:
• The number of gantries is 3;
• The capacity of each gantry is 15 hours each day form Monday to Friday;
• New patients starting day is from Monday to Wednesday;
• New patients starting time is 7 hours per day;
• The minimal period between two fractions for twice-a-day fractions patients is 6hours;
• The availability of anesthesia team is 4 hours per day in Gantry 1;
• Desired patient mix is as stated;
• Gantry 3 is specified to patients in Category 1 (1-field prostate cancer);
• Snout changing time is 15 minutes;
• Gantry switches are not allowed during the treatment;
81

• The model is cyclic with a time horizon (T ) of 65 days.
4.2.5.2 Results for the basic scenario
Table 4-2 shows the results of the model: the average number of fractions per day is
100.34. We also solved LP relaxation model by setting xtkg’s and ytkg’s continuous which
could provide an upper bound of the objective value and the results are showed in Table
4-2 too: the average number of fractions per day is 103.28. Table 4-3 shows the gantry
utilizations.
4.2.5.3 Sensitivity analysis
One of goals is to identify the aspects of the current operations which have the largest
potential for increasing capacity by sensitivity analysis. For convenience, the definitions of
scenarios are listed in Table 4-4 and the results for Scenarios 1–20 are listed in Table 4-5.
Gantry switching – Scenario 1. In the basic scenario, the gantry switching is not
allowed: once a patient starts the treatment in a certain gantry, he/she will be treated
in this gantry till all fractions have been finished. We tested the effect that the gantry
switching is allowed (Scenario 1) and observed that the average number of fractions per
day has been slightly increased (see Table 4-5).
Gantry specification – Scenario 2. In the basic model, Gantry 3 can only
treat the patients in Category 1 and in this scenario, we identified if it is worthwhile to
commission gantry 3 for patients in other categories - no improvement has been found by
disallowing gantry specification.
Anesthesia patient – Scenario 3. In the basic scenario, the anesthesia patients
are arranged in Gantry 1 with 4 available hours per day. We tested the Scenario 3 in
which the anesthesia patients are arranged in 2 gantries with 2 available hours per day and
per gantry. We can see from the results that the affect is very slight so we could not get
improvement.
82

Snout changing time – Scenarios 4–6. In Scenarios 4–6, the snout changing time
has been set to 5, 7.5 and 10 minutes, respectively. However, no encouraging improvement
has been found.
The Treatment Time – Scenarios 7–10. In Scenarios 7-9, we tested the system
capacity by deducting the treatment time per fraction by 2, 3 and 5 minutes, respectively.
The number of fractions per day increased to 114.28 in Scenario 9. However, we noticed
that the utilization of Gantry 3 is only 74%. It is clear that in this scenario the patients in
Category 1 are insufficient, hence we tested the Scenario 10 which is the same as Scenario
9 except without gantry specification. Then the utilization has been increased to 96% and
the capacity has been increased to 124.03.
Patient mixes – Scenarios 11–16. We tested the different patient mixes. In order
to test the impact of the patient mix on the capacity of the center, Scenarios 11–14 have
been generated in Table 4-6 based on the percentages of patients in Categores 1 and 2
(C1 and C2), and at each scenario the patients’ percentage in C1 + C2 are forming 100%,
90%, 70% and 60% of the patients’ population, and the rest is proportionally assigned
to the other categories based on the basic scenario. Compared to the Scenario 14, we
decreased the percentages of anesthesia patients in Scenario 15 because there are only
four hours in one gantry available for anesthesia patients each day. We observed that
the average fractions per day decreased with the decreasing of percentages of Category
1 and 2 because the treatment time per fraction is the shortest for the patients in these
two categories. Note that the deviation of patient mix is very high (7%) due to the time
limitation of anesthesia patients for Scenario 14. Moreover, the gantry utilization in
gantry 3 for Category 5 is very low (72.9%) because the gantry 3 is only for the patients
in Category 1 but there are no sufficient such patients. Therefore, we tested the model
83

without gantry specification in Scenario 16 and the corresponding results are showed in
the Table 4-5: the Gantry 3 utilization has been increased to 95%.
Gantry available time – Scenarios 17–19. In table 4-3, one can notice that the
average gantry utilizations for Thursday and Friday are lower compared to the rest of the
week. It can be justified as follows: there exists an additional treatment time for the first
fraction and the first treatment can only be delivered between Monday and Wednesday.
Consequently, there is less load on gantries on Thursdays and Fridays. In order to get
more stable daily utilizations, we can let the model determine the daily available time for
each gantry. In scenario 17, we reduce the gantry availability on Thursday and Friday by
β time units and extend the availability on Monday to Friday by β units in return, and let
the model find the optimal β. Note that in this scenario, the total weekly gantry available
time has been increased by β time units. In scenario 18, we define the gantry available
time on Monday to Wednesday by β1 and on Thusday and Friday by β2 while keeping the
total gantry available time unchanged compared to the basic scenario. In scenario 19, we
denote the gantry available time from Mon to Fri by Γ1, . . . , and Γ5, respectively while
keeping the total weekly gantry available time unchanged. The results are shown in Table
4-7 and 4-8.
Revenue maximization – Scenario 20. In this scenario, we analyze the effect of
replacing the average daily fractions maximization with the revenue maximization as the
objective function. Table 4-9 shows the revenue per fraction delivered to each category. It
turned out that the optimal average revenue per day is $397,106.22 with the corresponding
average daily fractions of 100.15.
Pediatrics maximization – Scenarios 21–26. Alternatively, a model is considered
in which the number of fractions delivered to patients in a certain subset of the categories
is maximized while ensuring that the average number of treatment fractions per day
84

remains sufficiently high. Such a model can be used to, for example, increase the number
of pediatrics patients that is treated. Since pediatrics cases (Categories 6 and 8) are
extremely time consuming, the system capacity is highly affected by the number of
patients treated from these two categories; however, the UFPTI policy is to deliver
treatment to all patient types despite the fact that they may not be as profitable as other
cases. Nonetheless, to fulfil a certain set of financial goals, a minimum daily average
fractions should be delivered. Scenarios 21–26 are developed to investigate the effect of
treating more pediatrics patients.
In Scenario 21 the number of pediatrics patients is maximized and the following
operational improvements suggested by the UFPTI are included:
• treatment time /fraction reduction
– Category 1: 3 minutes, Category 2: 2 minutes, Category 6: 15 minutes
– Category 7: 15 minutes, Category 8: 30 minutes
• New prostate cases (Category 1 and 2) are set up on Saturday so there is noadditional treatment time for the first treatment fraction
• no gantry specification / no gantry switching
• Desired patient mix as in Scenario 14
The results are reported in Table 4-10.
Since pediatrics patients require anesthesia for treatment, there is a high correlation
between anesthesia team availability and the number of pediatrics patients treated. In
Scenario 22, we vary the availability of anesthesia team on different gantries: 4 hours on
one gantry (1 × 4); 5 hours on two gantries (2 × 5), etc. Moreover the input data is the
same as scenario 21 with no patient mix consideration and the following constraint has
been added to the model:
• Daily average fractions delivered ≥ 110
85

The results are shown in tables 4-11 and 4-12.
Since Scenario 22 only maximizes the number of pediatrics patients, there are
opportunities for improving the average daily fractions delivered. In Scenario 23, we
maximize the total number of fractions delivered while retaining the optimal number of
pediatrics patients. tables 4-13 and 4-14 show the corresponding results.
Category 8 has almost no patients in Scenarios 21–23 due to the fact that Category 8
has a longer treatment time compared to Category 6, so all pediatrics patients are selected
from Category 6 by the model. We therefore test these scenarios with an additional
constraint that the number of patients in Category 8 is at least as large as the number of
patients in Category 6, i.e.:
T∑t=1
G∑g=1
xt (k=8) g ≥T∑
t=1
G∑g=1
xt (k=6) g
These new scenarios are defined as Scenarios 24–25 and the corresponding results are
shown in tables 4-15 to 4-18.
In Scenarios 23–25 we have noticed that except for categories 1, 6, and 8, other
categories have no or only a few patients. So in Scenario 26, we add penalty if the number
of patients in each category is different with the desired patient mix. Then the objective
function and related constraints can be formulated as follows:
maximizeT∑
t=1
∑
k∈Ka
G∑g=1
xtkg −K∑
k′=1
wk′Uk′
with the following additional constraints:
86

1
T
T∑t=1
K∑
k=1
G∑g=1
fkytkg ≥ Nmin
−Uk′ ≤T∑
t=1
G∑g=1
xtk′g − dk′
T∑t=1
K∑
k=1
G∑g=1
xtkg ≤ Uk′ k′ = 1, . . . , K
T∑t=1
G∑g=1
xt(k=8)g ≥T∑
t=1
G∑g=1
xt(k=6)g t = 1, . . . , T ; g = 1, . . . , G.
We set the (average) minimal number of fractions per day is 110 and the results are
showed in Table 4-19 and 4-20.
4.2.6 Concluding Remarks
The results provide optimal number of treatment fractions under current operational
conditions and desired patient mix at UFPTI. Sensitively analysis quantifies the extent to
which shortening the treatment time per fraction can increase the capacity. Moreover, the
total number of treatment fractions can dramatically change as a function of the desired
case mix. However, no large benefits are found from (i) allowing/disallowing patient
gantry switching, or (ii) enhancing gantry flexibility or (iii) shortening the time required
for snout changes. Moreover, the models provide guidance on how to increase the number
of pediatrics patients treated while keeping the total number of treatment fractions at a
sufficiently high level.
87

Table 4-1. Patients Classification.
Cate. Anesth. Treat. # frac. #frac. Add. time Snout Case Comment(y/n) time/frac. /day for 1st size mix
(min) frac.(min) (%)1 n 18 40 1 15 18 65 1-Field Prostate2 n 30 40 1 15 18 15 2-Field Prostate3 n 35 62 2 20 18 7 H&N/BOS4 n 45 62 2 25 25 3 Thorax/Abdomen
chordomas5 n 35 30 1 20 10 3 Simple Brain6 y 55 30 1 20 18 2 Peds Brain
with Anesthesia7 n 60 30 1 45 25 1 CSI no Anesthesia8 y 90 30 1 45 25 1 CSI with Anesthesia9 n 50 42 1 30 18 2 Lung/Abdomen
with ABC/BodyFlX10 n 35 12 1 20 18 1 Concomitant
Boost Patients
Table 4-2. The results for the basic scenario model.
Scenario Average fraction Patient mix deviation CPU time/day (%) (seconds) (%)
Basic IP 100.34 3% 6819Basic LP 103.28 0 673
Table 4-3. Gantry utilization per day using IP model (%).
Gantry Mon. Tue. Wed. Thu. Fri. Average1 96.7 96.7 97.0 93.9 93.5 95.62 93.6 95.2 94.9 90.7 89.5 92.83 98.0 98.0 98.2 94.8 94.8 96.7
88

Table 4-4. The definitions of scenarios.
Scenario DescriptionBasic Current operational condition at UFPTI
1 Allowing gantry switching2 No gantry specification3 Changing anesthesia team availability to 2× 24 5-min snout changing time5 7.5-min snout changing time6 10-min snout changing time7 2-min reduction in treatment time per fraction8 3-min reduction in treatment time per fraction9 5-min reduction in treatment time per fraction10 Scenario 9 without gantry specialization
11-15 Different patient mixes16 Scenario 15 without gantry specialization
17-19 Gantry available time20 Revenue maximization
21-26 Pediatrics maximization
89

Table 4-5. Sensitivity analysis.
Scenario Average fraction Patient mix deviation Gantry 1 Gantry 2 Gantry 3/day (%) utilization utilization utilization
Basic 100.34 3 96 93 971 100.69 3 95 93 992 99.11 2 94 95 933 100.95 3 94 93 984 100.46 3 91 95 985 99.57 2 93 93 986 100.18 2 92 95 987 106.06 2 95 93 918 109.14 2 95 93 859 114.28 2 95 95 7410 124.03 1 94 94 9611 126.77 3 95 96 9812 108.49 3 93 95 9413 90.40 3 92 94 9414 82.03 7 92 87 8415 77.48 3 90 94 7316 82.92 3 92 92 9517 100.95 3 95 93 9618 102.31 4 95 94 9819 102.80 4 95 95 9820 101.15 3 93 94 95
90

Table 4-6. Patient mix scenarios (%).
Scenario C1 C2 C3 C4 C5 C6 C7 C8 C9 C10
11 81 19 0 0 0 0 0 0 0 012 73 17 3 1 1 1 1 1 1 113 57 13 11 5 5 3 1 1 3 114 49 11 14 6 6 4 2 2 4 215 49 11 14 7 7 2 2 1 5 216 49 11 14 7 7 2 2 1 5 2
Table 4-7. Scenarios 17–19: Gantry available time (minutes).
Scenario Mon. Tue. Wed. Thu. Fri.Basic 900 900 900 900 90017 916 916 916 884 88418 912 912 912 882 88219 982 886 894 872 866
Table 4-8. Scenario 17–19: Gantry utilization (%).
Scenario Mon. Tue. Wed. Thu. Fri. AverageBasic 96.1 96.6 96.7 93.4 92.6 95.117 95.4 95.4 94.2 94.7 94.4 94.818 94.6 96.1 97.4 94.8 94.3 95.419 93.3 96.4 96.7 97.3 97.3 96.2
91

Table 4-9. Scenario 20: Revenue per fraction.
C1 C2 C3 C4 C5 C6 C7 C8 C9 C10
Revenue ($) 3982 3982 3808 3808 4058 4058 4144 4144 3991 5261
Table 4-10. Results for Scenario 21.
Scenario # fx/day # ped Gantry 1 Gantry 2 Gantry 3utilization utilization utilization
Basic 100.34 (3,1) 96 93 9720 92.80 (6,3) 96 96 94
Table 4-11. Scenario 22: Patient mix for different anesthesia availabilities.
Anesth. 1 2 3 4 5 6 7 8 9 101× 4 54.5 23.7 1.0 0.5 1.5 4.5 0.0 0.5 1.0 12.62× 5 54.4 25.9 0.0 0.0 0.0 14.0 0.0 0.5 0.0 5.22× 8 56.8 0.0 0.0 0.0 0.0 20.3 0.4 0.0 0.0 22.53× 5 61.7 8.3 2.6 0.0 0.0 23.3 0.0 0.0 0.0 4.1
Table 4-12. Scenario 22: Other statistics for different anesthesia availabilities.
Anesth. G1 G2 G3 #ped1× 4 88.1 91.1 91.1 102× 5 90.8 91.0 89.1 282× 8 89.8 91.4 89.4 463× 5 93.5 88.0 92.7 45
Table 4-13. Scenario 23: Patient mix for different anesthesia availabilities.
Anesth. 1 2 3 4 5 6 7 8 9 101× 4 96.1 0.0 0.0 0.0 0.0 3.9 0.0 0.0 0.0 0.02× 5 82.0 0.8 0.8 0.0 0.4 11.2 0.0 0.0 0.0 4.82× 8 80.3 0.0 0.0 0.0 0.0 19.7 0.0 0.0 0.0 0.03× 5 76.6 0.0 0.9 0.0 0.0 19.1 0.0 0.0 0.0 3.4
Table 4-14. Scenario 23: Other statistics for different anesthesia availabilities.
Anesth. G1 G2 G3 #ped # fx/day1× 4 87.5 93.3 93.3 10 156.62× 5 96.4 96.7 99.5 28 144.92× 8 96.0 97.0 94.2 46 136.33× 5 97.3 96.7 97.1 45 134.9
92

Table 4-15. Scenario 24: Patient mix for different anesthesia availabilities.
Anesth. 1 2 3 4 5 6 7 8 9 101× 4 62.4 8.1 7.6 0.0 0.0 2.0 0.0 2.0 0.0 17.92× 5 68.1 2.9 1.5 1.0 0.0 5.4 0.0 5.4 0.0 15.72× 8 75.9 0.0 0.0 0.0 0.0 9.2 0.0 9.2 0.0 5.23× 5 76.6 0.0 0.0 0.0 0.0 8.1 0.0 8.1 0.0 7.2
Table 4-16. Scenario 24: Other statistics for different anesthesia availabilities.
Anesth. G1 G2 G3 #ped1× 4 84.8 89.4 88.6 82× 5 91.1 87.2 83.6 222× 8 90.9 85.8 83.6 363× 5 88.1 79.4 86.1 32
Table 4-17. Scenario 25: Patient mix for different anesthesia availabilities.
Anesth. 1 2 3 4 5 6 7 8 9 101× 4 97.0 0.0 0.0 0.0 0.0 1.5 0.0 1.5 0.0 0.02× 5 91.0 0.0 0.0 0.0 0.0 4.5 0.0 4.5 0.0 0.02× 8 79.5 0.0 0.0 0.0 3.7 8.4 0.0 8.4 0.0 0.03× 5 85.3 0.0 0.0 0.0 0.0 7.3 0.0 7.3 0.0 0.0
Table 4-18. Scenario 25: Other statistics for different anesthesia availabilities.
Anesth. G1 G2 G3 #ped # fx/day1× 4 96.4 93.8 99.5 8 167.42× 5 95.6 96.1 99.5 22 148.62× 8 93.3 95.2 98.5 36 124.93× 5 93.5 95.4 97.8 32 128.3
Table 4-19. Scenario 26: Patient mix for different anesthesia availabilities.
1 2 3 4 5 6 7 8 9 10Desired pat. mix n/a 15 7 3 3 n/a 1 n/a 2 1
1× 4 66.5 16.4 5.7 1.7 1.7 2.3 0.6 2.3 1.7 1.11× 5 65.3 15.9 5.1 2.8 1.2 2.8 1.2 2.8 1.7 1.22× 8 65.4 15.0 0.5 0.0 2.1 6.9 0.0 9.6 0.0 0.63× 5 66.8 15.2 0.5 0.0 2.1 7.4 0.0 7.4 0.0 0.5
93

Table 4-20. Scenario 26: Other statistics for different anesthesia availabilities.
Anesth. G1 G2 G3 #ped # fx/day1× 4 90.9 89.5 92.9 (4,4) 110.11× 5 95.5 92.1 93.0 (5,5) 110.12× 8 95.6 91.3 93.2 (13,18) 110.23× 5 95.4 92.1 92.4 (14,14) 110.1
4.3 A Heuristic Approach to On-line Patient (Re-)scheduling
4.3.1 Problem Definition
UFPTI is an outpatient facility in which patients receive treatment fractions five
days a week for a number of weeks depending on their disease and prescribed treatment;
this characterizes each patient as belonging to one of a number of categories. Once a
new patient is referred to the UFPTI, the center should schedule him/her for treatment.
The treatment should then start within a specific range of days since the treatment
planning preparation takes some time and, on the other hand, if the treatment starts
late the patient’s medical condition can deteriorate which is of course highly undesirable.
In addition to finding the best starting day, the patient should also be informed of the
treatment starting time on the first day of treatment. Although a projected schedule for
the entire treatment duration is set for the new patient, only the first fraction starting
day and time is revealed to the patient. On each treatment day, the patient will then
be informed of the starting time of treatment on the following day. This leads to more
flexibility in the scheduling process by allowing us to modify a projected schedule to
some extent to fit a new patient in (with the exception of the time and day of the first
treatment fraction of a patient). Operational restrictions, such as the availability of
a physician or anesthesiologist, may require a patient to be treated within a certain
so-called restricted time window on each day. In addition, each patient may specify a
desired time window during which he/she prefers to be treated. Finally, treatment of
patients in different categories require different so-called snouts to be installed on the
94

treatment gantry, potentially requiring setup time between treatment of patients in
different categories. A good schedule is basically one which respects the restricted time
windows and at the same time satisfies the desired time windows to the largest extent
possible. Moreover, in a good schedule the set-up time is kept as low as possible in order
to have a high gantry utilization, thereby allowing treatment of more patients. Based on
what mentioned above, we consider the following optimization problems:
(i) (Re-)Scheduling the set of current patientsHere we determine a high-quality treatment schedule given a set of patients andtheir corresponding first appointments.
(ii) Scheduling a new patientIn this problem we determine a high-quality schedule given both a set of patientsand a new patient whose first appointment day and time needs to be determined.
In the next section, the first optimization problem has been modeled using a
decomposition approach. In modeling the second problem, we have used the same
approach with some slight modifications.
4.3.2 Model Description
4.3.2.1 Sequence and timing decomposition
e decompose a treatment schedule into two components: sequence, and timing. In
fact, given a certain sequence we can determine the optimal timing associated with it.
Since in radiation therapy treatment fractions are delivered on a daily basis, we can
assume that, except for the first fraction (as well as the second one in case of patients
treated twice daily) which needs to be dealt with separately, the sequence for the rest
of treatment fractions are kept the same unless a patient’s treatment finishes or a
new patient is added into the sequence. This assumption results in a more stable and
consistent projected schedule. In other words, without such an assumption there might be
drastic daily changes in the (projected) schedule whenever a new patient is added, which is
95

not desirable due to the inconvenience this may cause for the patients. We introduce the
concept of union sequence as follows:
4.3.2.2 Union sequence
In order to maintain stability in the treatment schedule we use a common order
in which patients are treated for the entire planning horizon. However, care should be
taken since of course not all patients are treated on all days of the planning horizon and
there are some patients, so called BID patients, whom are treated twice daily. We let T
denote the planning horizon of the scheduling (which we choose large enough to include
the projected treatments of all patients under consideration). Given the set of all patients
present in the system from today to day T , we then define a so-called union sequence for a
gantry that contains all patients that are treated during the planning horizon. Moreover,
for all patients that start their treatment during the planning horizon we create two
patient copies: one representing the first day of treatment (which requires more time than
subsequent ones and also has different time window restrictions) and one representing
all remaining fractions. For BID patients, we then duplicate the patient (or two patient
copies) further to represent the two daily treatment fractions. In other words, each patient
is represented by a number of patient copies in the union sequence as follows:
• copy 1: represents the first fraction on the treatment starting day.
• copy 2: represents the second fraction on the treatment starting day (only in case ofa BID patient).
• copy 3: represents all first fractions on the rest of treatment days.
• copy 4: represents all second fractions on the rest of treatment days (only in case ofa BID patient).
In addition, in order to determine the relevant patient copies for a certain day, a binary
indicator array of length T is used to specify on which days during the planning horizon
96

the patient copy is treated. Using the union sequence and the corresponding indicator
arrays we can determine the list of patients treated on a certain day.
4.3.2.3 Restricted and desired time windows
Each patient copy has a restricted time window during which it should be scheduled
because of operational and technical restrictions; the loosest time windows represent the
operating hours of the clinic. Moreover, since there should be a minimum time between
receiving two fractions on the same day for a BID patient, pairs of copies 1 and 2 and
copies 3 and 4, respectively, have restricted time windows with a specific time difference.
Moreover, there may be a desired time window associated with each patient copy which
is given by the patient’s time preference. Finally, the first patient copy has a restricted
starting time which is equal to the first appointment time set for the corresponding
patient, from which we can only deviate marginally.
4.3.2.4 Evaluation criteria for the union sequence
Given a union sequence, indicator arrays, first copy restricted starting times, and
restricted and desired time windows, one can find the daily optimal timing and evaluate
the desirability of the obtained schedule using the following evaluation criteria:
• Infeasibility : measures the restricted time windows and restricted starting timesviolations.
• Weighted average of snout changes :measures the weighted daily average number ofsnout changes.
• Weighted average of patient dissatisfaction: measures the weighted daily desired timewindows violations.
While computing the weighted averages, the weights are chosen so that earlier days of the
planning horizon are more important than later days since the former are more likely to be
close to final. In the following we first formulate the daily timing optimization problem for
a given union sequence and propose an exact algorithm to solve it. Next, we quantify our
97

evaluation criteria, and finally we present the local search heuristic as the union sequence
optimizer.
4.3.3 Solution Approach
4.3.3.1 Timing optimizer for a single day
Given a fixed union sequence and the indicator arrays associated with the patient
copies, we can formulate the daily timing problem as a linear programming model to find
the optimal timing for each day such that the restricted time windows and restricted
starting times are respected and the weighted violation of desired time windows is
minimized. Let
• N = set of all patient copies in the union sequence
• T = scheduling horizon
• Nt = set of all patient copies in the union sequence present on day t = 1, . . . , T
• K = set of patient categories
• η = the waiting time threshold for new patients
• ck = treatment time per fraction for Category k ∈ K
• [LDn , UD
n ] = desired time window for patient copy n ∈ N
• [LRn , UR
n ] = restricted time window for patient copy n ∈ N
• τ(t, n) = fraction number of patient copy n ∈ N on day t = 1, . . . , T
• L = length of working day
• kn = category of patient copy n
• λ = snout changing time
• λn = snout size required for patient copy n ∈ N
• St = set of patient copies of type 1, i.e., starting their treatment on day t = 1, . . . , T
98

• sn = restricted starting time (i.e. first appointment time) for patient copy n ∈ St t =1, . . . , T
• α(τ) = weight of desired time window violation if the patient copy is receiving theτ th fraction today
Furthermore, let decision variable sn denote the starting time, and vn and un denote the
violation of the desired time window for patient copy n on day t. The LP formulation for
the timing optimization problem for day t is as follows:
minimize PDI(t) =∑n∈N
α(τ(t, n)) · (un + vn)
subject to (M1)
LRn ≤ sn ≤ UR
n n ∈ Nt
sn ≥ LDn − un n ∈ Nt
sn ≤ UDn + vn n ∈ Nt
sn ≤ sn ≤ sn + η n ∈ St
sn ≥ sn−1 + ckn−1 + λ1{λn−1 6=λn} n ∈ Nt
sn, un, vn ≥ 0 n ∈ Nt
where α(τ(t, n)) is the weight of the desired time window violation if patient copy n
is receiving the τ th fraction on day t. In M1 the objective function measures the total
weighted desired time window violation. The first set of constraints enforce the restricted
time windows. The second and third sets of constraints measure the violation of the
desired time window. The fourth set of constraints ensure that the violation of restricted
starting time is in [0, η] for patient copies of type 1. Finally, the last set of constraints
ensure that patient copy n’s treatment starts after patient copy n − 1’s treatment is over.
1{λn−1 6=λn} is an indicator variable which is set to one if patient copy n is using a different
99

snout size from patient copy n − 1 and zero otherwise. In the following we present an
exact algorithm, so called timing optimizer, to find the solution to M1 in case of feasibility
or return the total violation of restricted time windows and restricted starting times
otherwise.
Timing optimizer
1. Set sn =
{0, n = 1;sn−1 + ckn−1 + λ1{λn−1 6=λn}, otherwise.
2. Modify sn as follows:
• if n ∈ St and sn < sn then set sn = sn.
• if n ∈ Nt − St and sn < LRn then sn = LR
n .
3. Calculate infeasibility index as the summation of all restricted time windows andrestricted starting times violations.
4. If infeasibility index is positive goto Step 9 otherwise go to Step 5.
5. Let Q = Nt − St.
6. Let n be the first element in Q.
7. Shift patient copy n’s starting time forward as much as it touches min{LDn , UR
n − ckn}and provided that:
(i) the objective function value decreases.
(ii) none of subsequent patient copies violate their restricted time windows orrestricted starting times.
8. If we stop due to (ii) with n′ as the critical patient copy, set Q = Q∩{n′+1, . . . , |Nt|}and return to Step 6.
9. Return the infeasibility index.
If an optimal solution to M1 exists, then the timing optimizer provides the optimal timing
for the corresponding day, otherwise it returns the total infeasibility associated with
100

the day. In fact, implementing the timing optimizer will obviate the need to purchase a
commercial LP solver for the clinic.
4.3.3.2 Snout change index (SCI)
To ensure the efficient utilization of the facility, the number of snout changes should be
minimized, this index denoted by SCI(t), simply counts the number of snout changes
required on day t given a union sequence. The weighted average of snout changes with
discount factor W ≤ 1 is similarly calculated as:
SCI =
∑Tt=1 W tSCI(t)∑T
t=1 W t.
4.3.3.3 Patient dissatisfaction index (PDI)
The objective of the timing optimization problem is to minimize the total weighted desired
time windows violations for a single day. In fact, smaller violation of the desired time
windows implies higher levels of patient satisfaction. Currently at the UFPTI, patients
being treated for higher fractions are prioritized over patients with lower fractions, in other
words, patients who have started treatment earlier have more seniority in the system. In
order to capture this fact, we have set:
α(τ(t, n)) =2τ(t,n)
∑Nt
n=1 2τ(t,n)L
which guarantees that patients with higher fraction numbers have more priority in
satisfying their desired time windows. Finally, by running the timing optimizer for every
day in the planning horizon, the weighted average patient dissatisfaction index with
discount factor W ≤ 1 can be calculated as follows:
PDI =
∑Tt=1 W tPDI(t)∑T
t=1 W t.
101

4.3.3.4 Sequence optimizer
Given an initial sequence of patient copies, a local search heuristic called “sequence
optimizer” has been developed to find a high-quality union sequence with respect to the
evaluation criteria. The sequence optimizer uses a randomized neighborhood structure in
which the union sequence is iteratively perturbed to obtain improved ones. We consider
the following perturbations:
• Shifting a single or a subset of consecutive patient copies backward or forward in theunion sequence.
• Swapping two patient copies in the union sequence.
In selecting patient copies for shifting or swapping, the sequence optimizer is biased
towards closer patient copies in the union sequence rather than more distant ones, so that
perturbations are within a smaller range and consequently the new schedule obtained has
local changes compared to the previous schedule. In searching for a good union sequence,
sequence optimizer hierarchically restores feasibility, minimizes snout change index,
and finally minimizes patient dissatisfaction index. Given an initial sequence of copies,
sequence optimizer tries to obtain feasibility first and improve the evaluation criteria next
in four phases as follows:
Restoring feasibility using subset shift neighborhood. At this phase, we use
a local search based on a shift neighborhood structure in which a single or a consecutive
subset of copies are randomly chosen and shifted forward. Running the timing optimizer T
times will give us the optimal timing of the copies for every day or it will return the total
infeasibility in the sequence. So starting with an initial sequence, at each step of the local
search we randomly perturb the sequence and generate a neighbor sequence and by calling
the timing optimizer we find the infeasibility of the solution and also count the total
number of snout changes required. If the neighbor sequence has a less infeasibility index
102

we replace the current sequence with the neighbor; otherwise even if the infeasibility index
has the same value but the neighbor sequence has less total number of snout changes we
replace the current solution with the neighbor; otherwise we produce a new neighbor. If
after a certain number of consecutive trials no improvement obtained we go to the next
phase.
1. Generate three random numbers for the starting and ending copies in the sequenceand the length of the shift.
2. Perform the temporary subset shift.
3. Run the timing optimizer for t = 1, . . . , T and find the total infeasibility over theplanning horizon.
4. Calculate the total number of snout changes required.
5. If the neighbor sequence has less infeasibility make the shift permanent and go tostep 1.
6. If the neighbor sequence has the same infeasibility but less snout changes make theshift permanent and go to step 1.
7. Update the trial counter.
8. If termination condition is satisfied stop.
Restoring feasibility using copy 1 shift neighborhood. In the next phase, the
sequence optimizer tries to restore the feasibility of the sequence by only shifting the first
fraction copies, the advantage of first fraction copies is in the fact that they only appear
once in the planning horizon, so by shifting these copies we will try to schedule them
as closely as possible to their restricted starting times. A best improvement strategy is
applied to find the best shift per each first fraction copy.
1. Find an unvisited first fraction copy otherwise stop.
2. Run all possible shifts and choose the shift with the least infeasibility index for onlyday t.
103

3. If the neighbor sequence has less infeasibility index on day t make the shiftpermanent and go to step 1.
Improving SCI and PSI using subset shift neighborhood. In the next phase,
using the same neighborhood structure as phase 1, the sequence optimizer tries to
hierarchically minimize the weighted average snout changes (SCI) as well as maximize
the weighted average patient satisfaction (PSI) using the randomized first improvement
strategy and again by calling the timing optimizer back and forth. However, shifts
resulting in less infeasibility are always welcomed first!
1. Generate three random numbers for the starting and ending copies in the sequenceand the length of the shift.
2. Perform the temporary subset shift.
3. Run the timing optimizer for t = 1, . . . , T and find the total infeasibility over theplanning horizon.
4. Calculate SCI and PSI.
5. If the neighbor sequence has less total infeasibility make the shift permanent and goto step 1.
6. If the neighbor sequence has the same infeasibility but less SCI make the shiftpermanent and go to step 1.
7. If the neighbor sequence has the same infeasibility and SCI but bigger PSI make theshift permanent and go to step 1.
8. Update the trial counter.
9. If termination condition is satisfied stop.
Improving SCI and PSI using swapping neighborhood. Finally, since swapping
neighborhood structure is capable of capturing some improvements in the sequence
that cannot be achieved using shift neighborhood structures only (specially in case of
specialized gantries), the sequence optimizer will perform a local search to hierarchically
104

minimize SCI and maximize PSI. Again, shifts resulting in less infeasibility are always
welcomed first!
1. Generate two random numbers for two swapping copies in the sequence.
2. Perform the temporary swapping.
3. Run the timing optimizer for t = 1, . . . , T and find the total infeasibility over theplanning horizon.
4. Calculate SCI and PSI.
5. If the neighbor sequence has less total infeasibility make the shift permanent and goto step 1.
6. If the neighbor sequence has the same infeasibility but less SCI make the shiftpermanent and go to step 1.
7. If the neighbor sequence has the same infeasibility and SCI but bigger PSI make theshift permanent and go to step 1.
8. Update the trial counter.
9. If termination condition is satisfied stop.
4.3.3.5 Fitting a new patient
In case of introducing a new patient in the sequence, we initially add sufficient
number of copies (2 in case of a single fraction and 4 in case of a BID patient) to the
union sequence to represent the new patient, and basically add one more dimension to
the local search previously used to account for the new patient’s starting day. Now at
each iteration, we randomly generate ∆ ∈ {−1, 0, 1} and update the starting day and
subsequently the corresponding presence arrays of the copies relating to the new patient.
For example, the local search presented above for the first phase will be modified as
follows:
1. Add 2 copies (or 4 copies in case of a BID patient) to the union sequence.
2. Generate ∆ ∈ {−1, 0, 1}.
105

3. Update presence arrays for the newly added copies according to ∆.
4. Generate three random numbers for the starting and ending copies in the sequenceand the length of the shift.
5. Perform the temporary subset shift.
6. Run the timing optimizer for t = 1, . . . , T and find the total infeasibility over theplanning horizon.
7. Calculate the total number of snout changes required.
8. If the neighbor sequence has less infeasibility make the shift permanent and go tostep 2.
9. If the neighbor sequence has the same infeasibility but less snout changes make theshift permanent and go to step 2.
10. Undo the update made to presence arrays.
11. Update the trial counter.
12. If termination condition is satisfied stop.
4.3.3.6 Numerical example
Our local search has been implemented using C++ and now it is under clinical testing
at the UFPTI. The following table presents the results obtained from running the software
to schedule a new patient on each of the three gantries operating at the UFPTI using real
data for a planning horizon of 100 days.
Table 4-21. Results for scheduling a new patient on different gantries.
Gantry # of patients SCI PDI Running time(seconds)
G1 70 2.93 5% 42G2 63 1.95 7% 53G3 97 0.0 6% 55
In all of the three cases above, our local search was able to find high quality schedules
including the new patient in less than a minute, for instance, in case of scheduling the
106

new patient on gantry 1, with 70 patients at the time, it found the new schedule with the
snout change index (SCI) of 2.93 and the patient dissatisfaction index (PDI) as low as
5%, whereas previously there were around 9 snout changes per day on this gantry. Finally,
note that no snout changes were required on gantry 3 since all patients treated on this
gantry were belonging to the same category.
4.3.4 Concluding Remarks
In this section we have presented a new local search heuristic in order to schedule
patients for radiation therapy treatment considering their time preferences while
respecting operational and technical limitations. Our goal was to develop high-quality
schedules measured by three main indices: 1) infeasibility which measures the violation
of restricted time windows and starting times; 2) snout change index which measures the
efficiency of the schedule; and 3) patient dissatisfaction index which evaluates the weighted
violation of desired time windows. The local search proposed tries to hierarchically
improve these three indices via performing randomized biased search in a neighborhood
structure based on shifting or swapping patient copies in the union sequence. Patient
scheduling at the UFPTI was formerly done manually in a time-consuming process that
often resulted in poor schedules. With the developed algorithm it is now possible to
produce high-quality schedules in real-time.
107

REFERENCES
[1] R.K. Ahuja and H.W. Hamacher. A network flow algorithm to minimizebeam-on-time for unconstrained multileaf collimator problems in cancer radiationtherapy. Networks, 45(1):36–41, 2005.
[2] American Cancer Society. Cancer facts & figures. Report, 2006.http://www.cancer.org/.
[3] J.A. Antolak and I. Rosen. Planning target volumes for radiotherapy: how muchmargin is needed? 44:1165–1170, 1999.
[4] M.R. Arnfield, J.V. Siebers, J.O. Kim, Q. Wu, P.J. Keall, and R. Mohan. A methodfor determining multileaf collimator transmission and scatter for dynamic intensitymodulated radiotherapy. Medical Physics, 27:2231–2241, 2000.
[5] D. Baatar, H.W. Hamacher, M. Ehrgott, and G.J. Woeginger. Decomposition ofinteger matrices and multileaf collimator sequencing. Discrete Applied Mathematics,152(1):6–34, 2005.
[6] J.L. Bates and R.L. Constable. Proofs as programs. ACM Transactions on Program-ming Languages and Systems, 7(1):113–136, 1985.
[7] M.S. Bazaraa, H.D. Sherali, and C.M. Shetty. Nonlinear Programming: Theory andAlgorithms. John Wiley & Sons, 2 edition, 1993.
[8] G. Bednarz, D. Michalski, C. Houser, M.S. Huq, Y. Xiao, P.R. Anne, and J.M.Galvin. The use of mixed-integer programming for inverse treatment planning withpre-defined field segments. Physics in Medicine and Biology, 47:2235–2245, 2002.
[9] J. Bentley, editor. Programming Pearls. Addison-Wesley, Reading, MA, 1986.
[10] N. Boland, H.W. Hamacher, and F. Lenzen. Minimizing beam-on time in cancerradiationt treatment using multileaf collimators. Networks, 43(4):226–240, 2004.
[11] T.R. Bortfeld, D.L. Kahler, T.J. Waldron, and A.L. Boyer. X-ray field compensationwith multileaf collimators. International Journal of Radiation Oncology BiologyPhysics, 28:723–370, 1994.
[12] K.R. Britton, Y. Takai, M. Mitsuya, K. Nemoto, Y. Ogawa, and S. Yamada.Evaluation of inter- and intrafraction organ motion during intensity modulatedradiation therapy (imrt) for localized prostate cancer measured by a newly developedon-board image-guided system. Radiation Medicine, 23(1):14–24, 2005.
[13] T. Cayirli and E. Veral. Outpatient-scheduling in health care: a review of theliterature. Production and Operations Management, 12(4):519–549, 2003.
108

[14] T. Cayirli, E. Veral, and H. Rosen. Designing appointment scheduling systems forambulatory care services. Health Care Management Science, 9(1):47–58, 2006.
[15] T.C.Y. Chan, T. Bortfeld, and J.N. Tsitsiklis. A robust approach to imrtoptimization. Physics in Medicine and Biology, 51:2567–2583, 2006.
[16] S. Chen, A.P. Shah, J.B. Strauss, J.V. Turian, M.C. Kirk, J.C.H. Chu, andA. Dickler. Tomotherapy treatment of the prostate and pelvic lymph nodes witha sequential conedown. International Journal of Radiation Oncology Biology Physics,69(3):S692–S693, 2007.
[17] D. Conforti, F. Guerriero, and R. Guido. Optimization models for radiotherapypatient scheduling.
[18] T. Craig, J. Battista, and J.D. Van. Limitations of a convolution method formodeling geometric uncertainties in radiation therapy i: the effect of shift invariance.Medical Physics, 30:2012–2020, 2003.
[19] T. Craig, J. Battista, and J.D. Van. Limitations of a convolution method formodeling geometric uncertainties in radiation therapy ii: the effect of a finite numberof fractions. Medical Physics, 30:2001–2011, 2003.
[20] J. Dai and Y. Zhu. Minimizing the number of segments in a delivery sequence forintensity-modulated radiation therapy with a multileaf collimator. Medical Physics,28(10):2113–2120, 2001.
[21] M.A. Earl, M.K.N. Afghan, C.X. Yu, Z. Jiang, and D.M. Shepard. Jaws-only imrtusing direct aperture optimization. Medical Physics, 34:307–314, 2007.
[22] M. El-Bassiouni, J.B. Davis, I. El-Attar, G.M. Studer, U.M. Ltolf, and I.F. Ciernik.Target motion variability and on-line positioning accuracy during external-beamradiation therapy of prostate cancer with an endorectal balloon device. Strahlenthera-pie und Onkologie, 182(9):531–536, 2006.
[23] K. Engel. A new algorithm for optimal multileaf collimator field segmentation.Discrete Applied Mathematics, 152(1):35–51, 2005.
[24] H.W. Hamacher and K.-H. Kufer. Inverse radiation therapy planning – a multipleobjective optimization approach. Discrete Applied Mathematics, 118:145–161, 2002.
[25] M.v. Herk, P. Remeijer, C. Rasch, and J.V. Lebesque. The probability of correcttarget dosage: Dose-population histograms for deriving treatment margins inradiotherapy. International Journal of Radiation Oncology Biology Physics,47(4):1121–1135, 2000.
109

[26] International Commission on Radiation Units and Measurements. Prescribing,recording and reporting photon beam therapy (report 50). Technical report, 1993.
[27] International Commission on Radiation Units and Measurements. Prescribing,recording and reporting photon beam therapy (report 62). Technical report, 1999.
[28] T. Kalinowski. The algorithmic complexity of the minimization of the number ofsegments in multileaf collimator field segmentation. Technical report, FachbereichMathematik, Universitat Rostock, Rostock, Germany, August 2004.
[29] T. Kalinowski. A duality based algorithm for multileaf collimator field segmentationwith interleaf collision constraint. Discrete Applied Mathematics, 152(1):52–88, 2005.
[30] T. Kalinowski. Reducing the number of monitor units in multileaf collimator fieldsegmentation. Physics in Medicine and Biology, 50(6):1147–1161, 2005.
[31] S. Kamath, S. Sahni, J. Li, J. Palta, and S. Ranka. Leaf sequencing algorithms forsegmented multileaf collimation. Physics in Medicine and Biology, 48(3):307–324,2003.
[32] S. Kamath, S. Sahni, J. Palta, and S. Ranka. Algorithms for optimal sequencing ofdynamic multileaf collimators. Physics in Medicine and Biology, 49(1):33–54, 2004.
[33] S. Kamath, S. Sahni, J. Palta, S. Ranka, and J. Li. Optimal leaf sequencing withelimination of tongue-and-groove underdosage. Physics in Medicine and Biology,49(3):N7–N19, 2004.
[34] S. Kamath, S. Sahni, S. Ranka, J. Li, and J. Palta. A comparison of step-and-shootleaf sequencing algorithms that eliminate tongue-and-groove effects. Physics inMedicine and Biology, 49(14):3137–3143, 2004.
[35] S. Kamath, S. Sahni, S. Ranka, J. Li, and J. Palta. Optimal field splitting for largeintensity-modulated fields. Medical Physics, 31(12):3314–3323, 2004.
[36] K.M. Langen KM and D.T.L. Jones. Organ motion and its management. Interna-tional Journal of Radiation Oncology Biology Physics, 50:265–278, 2001.
[37] K.-H. Kufer, M. Monz, A. Scherrer, H.L. Trinkaus, T. Bortfeld, and C. Thieke.Intensity Modulated Radiotherapy - a large scale multi-criteria programming problem.OR Spektrum, 25:223–249, 2003.
[38] G.J. Kutcher and C. Burman. Calculation of complication probability factors fornon-uniform normal tissue irradiation: the effective volume method. InternationalJournal of Radiation Oncology Biology Physics, 16:1623–1630, 1989.
110

[39] M. Langer, V. Thai, and L. Papiez. Improved leaf sequencing reduces segments ormonitor units needed to deliver IMRT using multileaf collimators. Medical Physics,28(12):2450–2458, 2001.
[40] E.K. Lee, T. Fox, and I. Crocker. Optimization of radiosurgery treatment planningvia mixed integer programming. Medical Physics, 27(5):995–1004, 2000.
[41] E.K. Lee, T. Fox, and I. Crocker. Integer programming applied tointensity-modulated radiation treatment planning. Annals of Operations Research,119:165–181, 2003.
[42] F. Lenzen. An integer programming approach to the multileaf collimator problem.Master’s thesis, University of Kaiserslautern, Department of Mathematics,Kaiserslautern, Germany, June 2000.
[43] G.J. Lim and J. Choi. A two-stage integer programming approach for optimizingleaf sequence in IMRT. Technical report, Department of Industrial Engineering,University of Houston, Houston, Texas, 2006.
[44] W. Lu, G.H. Olivera, and T.R. Mackie. Motion-encoded dose calculation throughfluence/sinogram modification. Medical Physics, 32(1):118–127, 2005.
[45] X. Lu and L. Chin. Sampling techniques for the evaluation of treatment plans.Medical Physics, 20:151–161, 1993.
[46] A.E. Lujan, E.W. Larsen, J.M. Balter, and R.K. Ten Haken. A method forincorporating organ motion due to breathing into 3d dose calculations. MedicalPhysics, 26:715–720, 1999.
[47] S.D. McCarter and W.A. Beckham. Evaluation of the validity of a convolutionmethod for incorporating tumour movement and set-up variations into theradiotherapy treatment planning system. Physics in Medicine and Biology,45:923–931, 2000.
[48] V. Moiseenko, M. Liu, S. Kristensen, G. Gelowitz, and E. Berthelet. Effect of bladderfilling on doses to prostate and organs at risk: a treatment planning study. Journal ofApplied Clinical Medical Physics,, 8(1):55–68, 2007.
[49] A. Niemierko. Reporting and analyzing dose distributions: a concept of equivalentuniform dose. Medical Physics, 24:103–110, 1997.
[50] A. Niemierko. A generalized concept of equivalent uniform dose. Medical Physics,26:1100, 1999.
[51] B.C. Parker, A.S. Shiu, and M.H. Maor. Ptv margin determination in conformal srtof intracranial lesions. Journal of Applied Clinical Medical Physics,, 3:176–189, 2002.
111

[52] F. Preciado-Walters, R. Rardin, M. Langer, and V. Thai. A coupled columngeneration, mixed integer approach to optimal planning of intensity modulatedradiation therapy for cancer. Mathematical Programming, 101(2):319–338, 2004.
[53] R.A. Price. IMRT for prostate cancer. Technical report. Fox Chase Cancer Center.
[54] W. Que. Comparison of algorithms for multileaf collimator field segmentation.Medical Physics, 26(11):2390–2396, 1999.
[55] Radiation Therapy Oncology Group. H-0022: A phase I/II study of conformal andintensity modulated irradiation for oropharyngeal cancer.
http://www.rtog.org/members/protocols/h0022/h0022.pdf, 2000.
[56] Radiation Therapy Oncology Group. H-0225: A phase II study of intensity modulatedradiation therapy (IMRT) +/- chemotherapy for nasopharyngeal cancer.
http://www.rtog.org/members/protocols/0225/0225.pdf, 2002.
[57] Radiation Therapy Oncology Group. A phase III randomized study of high dose3D-CRT/IMRT versus standard dose 3D-CRT/IMRT in patients treated for localizedprostate cancer, 0126 edition, 10 2004.
[58] R.T. Rockafellar and S. Uryasev. Optimization of conditional value-at-risk. TheJournal of Risk, 2(3):21–41, 2000.
[59] G. Rodriguesa, S. Yartsevb, J. Chen, E. Wongb, D. D’Souzaa, M. Locka,G. Baumana, G. Grigorovd, and T. Kronb. A comparison of prostate imrt andhelical tomotherapy class solutions. Radiotherapy and Oncology, 80(3):374–377, 2006.
[60] H.E. Romeijn, R.K. Ahuja, J.F. Dempsey, and A. Kumar. A column generationapproach to radiation therapy treatment planning using aperture modulation. SIAMJournal on Optimization, 15(3):838–862, 2005.
[61] H.E. Romeijn, R.K. Ahuja, J.F. Dempsey, and A. Kumar. A new linear programmingapproach to radiation therapy treatment planning problems. Operations Research,54(2):201–216, 2006.
[62] H.E. Romeijn, J.F. Dempsey, and J.G. Li. A unifying framework for multi-criteriafluence map optimization models. Physics in Medicine and Biology, 49:1991–2013,2004.
[63] D.M. Shepard, M.A. Earl, X.A. Li, S. Naqvi, and C. Yu. Direct apertureoptimization: a turnkey solution for step-and-shoot IMRT. Medical Physics,29(6):1007–1018, 2002.
112

[64] D.M. Shepard, M.C. Ferris, G.H. Olivera, and T.R. Mackie. Optimizing the deliveryof radiation therapy to cancer patients. SIAM Review, 41(4):721–744, 1999.
[65] J.V. Siebers, M. Lauterbach, P.J. Keall, and R. Mohan. Incorporating multi-leafcollimator leaf sequencing into iterative IMRT optimization. Medical Physics,29(6):952–959, 2002.
[66] R.A.C. Siochi. Minimizing static intensity modulation delivery time using an intensitysolid paradigm. International Journal of Radiation Oncology Biology Physics,43(43):671–689, 1999.
[67] J.C. Stroom, H.C de Boer, H. Huizenga, and A.G. Visser. Inclusion of geometricaluncertainties in radiotherapy treatment planning by means of coverage probability.International Journal of Radiation Oncology Biology Physics, 43(4):905–919, 1999.
[68] Z.C. Taskın, J.C. Smith, H.E. Romeijn, and J.F. Dempsey. Optimal multileafcollimator leaf sequencing in IMRT treatment planning. Technical report, Departmentof Industrial and Systems Engineering, University of Florida, Gainesville, Florida,2007.
[69] L. Wang, R. Jacob, L. Chen, S. Feigenberg, A. Konski, C. Ma, and B. Movsas.Stereotactic imrt for prostate cancer: Setup accuracy of a new stereotactic bodylocalization system. Journal of Applied Clinical Medical Physics,, 5(2):18–18, 2004.
[70] P. Xia and L.J. Verhey. Multileaf collimator leaf sequencing algorithm for intensitymodulated beams with multiple static segments. Medical Physics, 25(8):1424–1434,1998.
[71] L.J. Verhey Y. Kim and P. Xia. A feasibility study of using conventional jaws todeliver IMRT plans in the treatment of prostate cancer. Physics in Medicine andBiology, 52:2147–2156, 2007.
113

BIOGRAPHICAL SKETCH
Chunhua Men was born in Xinjiang, China. She completed her bachelor’s and
master’s degree in power engineering at Hohai University in 1997 and 2000 respectively.
Then she worked at Nanjing Automation Research Institute and Shanghai Sunrise-power
Automation Co., till the end of 2003 then she moved to USA with her husband. In 2005,
Chunhua started her doctoral study at the University of Florida majoring in industrial
and systems engineering and received her Ph.D. in 2009. Then she joined the Department
of Radiation Oncology at University of California, San Diego Moores Cancer Center as a
postdoctoral fellow.
114