Embed Size (px)
Citation preview
Treat Respir Med 2005; 4 (6): 409-422REVIEW ARTICLE 1176-3450/05/0006-0409/$34.95/0
© 2005 Adis Data Information BV. All rights reserved.
Oral Appliance Therapy for ObstructiveSleep ApneaAndrew Ng,1 Helen Gotsopoulos,1 Ali M. Darendeliler2 and Peter A. Cistulli3
1 Department of Respiratory & Sleep Medicine, St George Hospital; Department of Medicine, University of New SouthWales, Sydney, Australia
2 United Dental Hospital, Faculty of Dentistry, University of Sydney, Sydney, Australia3 University of Sydney & Royal North Shore Hospital, Sydney, Australia
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4091. Pathophysiological Basis for Oral Appliance Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 410
1.1 Pathophysiology of Obstructive Sleep Apnea (OSA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4101.2 Therapeutic Rationale in OSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4111.3 Oral Appliance Therapy for OSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411
1.3.1 Types of Oral Appliances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4111.3.2 Mechanism of Action of Oral Appliances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 411
2. Efficacy of Oral Appliances in OSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4122.1 Effect on Polysomnographic Variables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4122.2 Comparison with Nasal Continuous Positive Airway Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4122.3 Comparison with Surgical Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4142.4 Impact of Oral Appliance Therapy on Symptoms in OSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 414
2.4.1 Daytime Sleepiness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4142.4.2 Snoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4142.4.3 Impact on Neuropsychological Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4172.4.4 Other Symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 417
2.5 Cardiovascular Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4172.6 Efficacy in Upper Airway Resistance Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 417
3. Prediction of Treatment Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4174. Oral Appliance Design and Titration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 418
4.1 Influence of Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4184.2 Oral Appliance Titration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 418
5. Adverse Effects and Complications of Oral Appliances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4195.1 Short-Term Adverse Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4195.2 Long-Term Adverse Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 419
6. Clinical Practice Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4197. Unresolved Issues and Future Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4208. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 420
Obstructive sleep apnea (OSA) is a common disorder characterized by repetitive, complete or partial closureAbstractof the upper airway during sleep, resulting in sleep fragmentation and oxygen desaturation. The disorder causessignificant morbidity, particularly in terms of impairment of daytime functioning and the impact this has onquality of life. There is also evidence that links OSA to long-term cardiovascular morbidity, includinghypertension, myocardial infarction, and stroke, and increased risk of motor vehicle accidents. There is clearevidence that effective treatment of OSA provides major benefit to patients.

410 Ng et al.
Nasal continuous positive airway pressure (CPAP) is the current treatment of choice, but its cumbersomenature makes tolerance and compliance less than optimal. This gives rise to the need for other alternatives thatare equally effective, but more tolerable. There is growing interest in the use of oral appliances to treat snoringand OSA. The rationale is that advancement of the mandible and tongue impacts positively on upper airwaycaliber and function. There are many such types of appliances, and they have potential advantages over CPAP inthat they are unobtrusive, make no noise, do not need a power source, and are potentially less costly.
There is a growing evidence base to support the use of oral appliances in the management of OSA. Recentevidence from randomized controlled trials indicates that oral appliance therapy is effective in controlling OSAin up to 50% of patients, including some patients with more severe forms of OSA. This is associated with asignificant improvement in symptoms, including snoring and daytime sleepiness. This evidence is strong forshort term, and emerging for long-term treatment of OSA with oral appliances. Whilst direct comparisons withCPAP indicate the superiority of CPAP overall, similar outcomes between the two treatments appear to beachieved in a substantial subgroup of patients. Patient acceptance has, in general, been in favor of oralappliances.
Notwithstanding the expanding role of oral appliance therapy, there are a number of limitations that are yet tobe overcome. Key issues include the inability to reliably predict treatment outcome, the apparent need for anacclimatization period to attain maximal efficacy of treatment, uncertainty about selection of the appropriate‘dosage’ of mandibular advancement required to control OSA in the individual patient, uncertainty about theinfluence of appliance design on treatment outcome and adverse effects, adherence to treatment, and potentiallong-term complications of therapy. These issues require resolution before oral appliance therapy can surpassCPAP as first-line treatment for OSA.
Obstructive sleep apnea (OSA) is a disorder characterized by treatment.[11-13] Hence there is an ongoing clinical need for alterna-tive therapies that overcome these disadvantages.repetitive, complete or partial closure of the upper airway during
With growing awareness of the craniofacial aspects of thesleep, resulting in sleep fragmentation and oxygen desaturation.[1]
pathophysiology of OSA,[14] there has been an increasing focus onOSA, defined as more than five apneas and/or hypopneas per hourdental therapies for OSA. The concept of using a dental applianceof sleep, is most prevalent in the middle-aged population, affectingto relieve upper airway obstruction was first reported by Robin.[15]5–24% of men[2,3] and 9% of women.[3] When this definition isThe use of oral appliances for OSA was first reported almost 20combined with sleepiness as an additional disease defining criteri-years ago,[16,17] but it is only in the last 10 years that their clinicalon, OSA syndrome has been estimated to be present in 1.4–6.5%role has emerged.[18] Oral appliances have potential advantagesof men and 1.1–2.5% of women.[3-5] The key symptoms areover nasal CPAP, particularly their relatively unobtrusive nature.snoring, witnessed apneas, excessive daytime sleepiness and defi-There is now mounting evidence that oral appliances have ancits in neuropsychological function,[6] adversely impacting onimportant role as a treatment modality for OSA, and this articlequality of life.[7] There is also evidence that links OSA to longtermwill review the evidence base to date.cardiovascular morbidity, including hypertension, myocardial in-
farction, and stroke,[8] and increased risk of motor vehicle acci-1. Pathophysiological Basis for Oral
dents.[9] Hence, it is now recognized that OSA is a serious publicAppliance Therapy
health problem.
Continuous positive airway pressure (CPAP), applied to the1.1 Pathophysiology of Obstructive Sleep Apnea (OSA)
upper airway via a nose mask during sleep, remains the acceptedtreatment of choice for more than 20 years since its use was first The patency of the upper airway is dependent on the balancereported.[10] There is high-level evidence of the effectiveness of between two opposing forces, namely the subatmospheric in-CPAP in the control of respiratory abnormalities during sleep, and traluminal pressure during inspiration tending to collapse thesymptoms during long-term use. Whilst it is an extremely effective airway, and the upper airway dilator muscles that act to preventtreatment because it diffusely splints the upper airway, its cumber- collapse.[1] OSA is thought to result from a combination of abnor-some nature makes tolerance and compliance less than optimal, mal anatomy, leading to reduced upper airway caliber, and sleep-with a significant proportion of patients declining or discontinuing induced loss of muscle tone. Patients with OSA have generally
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)

Oral Appliances for OSA 411
1.3.2 Mechanism of Action of Oral Appliancesbeen found to have smaller upper airways, especially in theThe majority of oral appliances are thought to act by eithervelopharyngeal and oropharyngeal regions;[19,20] this may be due
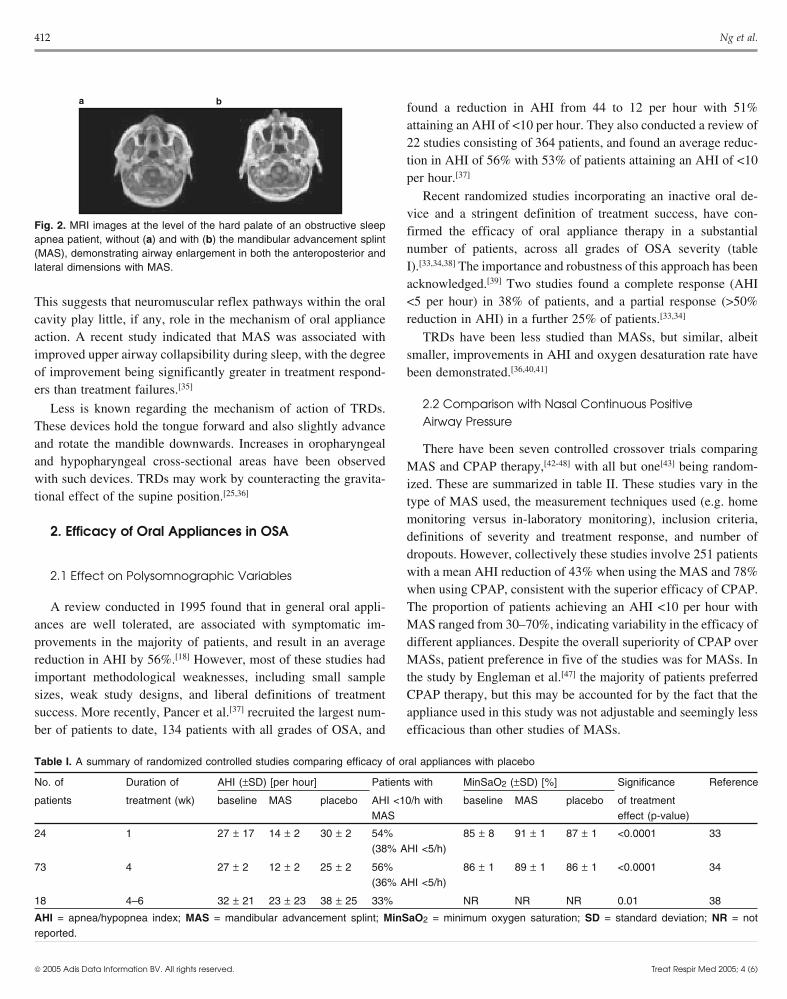
advancing the mandible and/or tongue with variable downwardto soft tissue or craniofacial skeletal abnormalities, and commonlyrotation of the mandible (see figure 1). This is thought to lead to ana combination of these factors. Patients with OSA rely on in-improvement in upper airway dimensions and possibly to positivecreased dilator muscle activity to maintain upper airway patency.effects on neuromuscular activity and/or airway compliance.Whilst this reflex activation of dilator muscles is effective duringHowever, there is little direct evidence available on the effect ofwakefulness, it is markedly attenuated during sleep leading tooral appliances on upper airway structure. It has been proposedinstability of the airway.[21]
that, because these devices move the mandible forward, theyinduce enlargement of the oropharyngeal airway in the anteropos-
1.2 Therapeutic Rationale in OSAterior (AP) dimension. However, a preliminary MRI study ob-served increases in the lateral dimension.[26] A number of studies
Treatment of OSA is aimed at preventing upper airway collapseusing a variety of methodologies, including nasopharyngosco-
through a variety of means that attempt to overcome thepy,[27] MRI,[28,29] and fluoroscopy[30] in healthy patients or OSA
pathophysiological factors described above. The most effectivepatients indicate increases in cross-sectional area of the velo-
approaches are either to pneumatically splint the entire airway, aspharynx, in the lateral and AP dimensions, and high up in the
achieved with CPAP, or to bypass the upper airway altogether byoropharynx (see figure 2). Hence, it appears that the tongue, soft
tracheostomy. Surgical treatments involve localized ameliorationpalate, lateral pharyngeal walls, and mandible interact to control
of upper airway caliber through the excision of redundant softairway size, and that mandibular advancement induces complex
tissue or upper airway lesions, or alteration of the skeletal struc-and variable changes in these structures.
tures. A diverse range of surgical procedures for OSA has beenThe mechanism by which mandibular advancement appears to
described, but with the exception of tracheostomy and majorincrease the lateral dimensions of the velopharynx is uncertain.
maxillofacial procedures, their role as sole treatments for OSA isIsono et al.[31] have suggested that because the lateral walls of the
limited.[22] Improving upper airway muscle tone during sleepsoft palate are connected to the base of the tongue through the
through the use of electrical stimulation[23] or pharmacologicalpalatoglossal arch, advancing the mandible, and hence the tongue,
compounds[24] have also been reported, but limited benefit hascould stiffen the velopharynx in the lateral dimension. Increased
precluded their clinical use to date.neuromuscular activity is another potential mechanism of action of
The potential for oral appliances to positively impact on airwayoral appliances. Yoshida[32] studied genioglossus, masseter and
anatomy by altering the position of soft tissue and skeletal struc-lateral pterygoid function in 15 patients with OSA, and found an
tures, and possibly neuromuscular function, makes them an attrac-increase in genioglossus and lateral pterygoid activity following
tive proposition. Potential advantages over other forms of therapyappliance insertion. Potentially, this could be mediated via oral
are their ease of use, reversibility, portability, lack of noise, nosensory receptors involved in upper airway neuromuscular con-
power source required, and potentially lower cost.trol. However, two recent studies using an inactive oral plate as acontrol treatment did not observe any significant improvement in
1.3 Oral Appliance Therapy for OSA apnea/hyponea index (AHI) or minimum oxygen saturation.[33,34]
1.3.1 Types of Oral Appliances
Many different oral appliances have been reported in the litera-ture and are available commercially, but it is beyond the scope ofthis review to describe and compare all of these. Despite theirdifferences, oral appliances share many common attributes. Theycan be broadly classified as mandibular advancement splints(MASs) or tongue retaining devices (TRDs). Most oral appliancesare of the MAS type, and attach to one or both dental arches andinduce protrusion of the mandible.[25] In contrast, the TRD drawsand holds the tongue in an anterior position during sleep by meansof negative pressure in a soft plastic bulb. It has the advantage ofbeing able to be used in edentulous patients.
a b
Fig. 1. Lateral cephalometric x-rays without (a) and with (b) mandibularadvancement splint in situ demonstrating bite opening, downward rotationof the mandible, and anteroposterior enlargement of the retropalatal andretroglossal airway.
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)
412 Ng et al.
found a reduction in AHI from 44 to 12 per hour with 51%attaining an AHI of <10 per hour. They also conducted a review of22 studies consisting of 364 patients, and found an average reduc-tion in AHI of 56% with 53% of patients attaining an AHI of <10per hour.[37]
Recent randomized studies incorporating an inactive oral de-vice and a stringent definition of treatment success, have con-firmed the efficacy of oral appliance therapy in a substantialnumber of patients, across all grades of OSA severity (tableI).[33,34,38] The importance and robustness of this approach has been
a b
Fig. 2. MRI images at the level of the hard palate of an obstructive sleepapnea patient, without (a) and with (b) the mandibular advancement splint(MAS), demonstrating airway enlargement in both the anteroposterior andlateral dimensions with MAS.
acknowledged.[39] Two studies found a complete response (AHI<5 per hour) in 38% of patients, and a partial response (>50%This suggests that neuromuscular reflex pathways within the oralreduction in AHI) in a further 25% of patients.[33,34]cavity play little, if any, role in the mechanism of oral appliance
action. A recent study indicated that MAS was associated with TRDs have been less studied than MASs, but similar, albeitimproved upper airway collapsibility during sleep, with the degree smaller, improvements in AHI and oxygen desaturation rate haveof improvement being significantly greater in treatment respond- been demonstrated.[36,40,41]
ers than treatment failures.[35]
2.2 Comparison with Nasal Continuous PositiveLess is known regarding the mechanism of action of TRDs.Airway PressureThese devices hold the tongue forward and also slightly advance
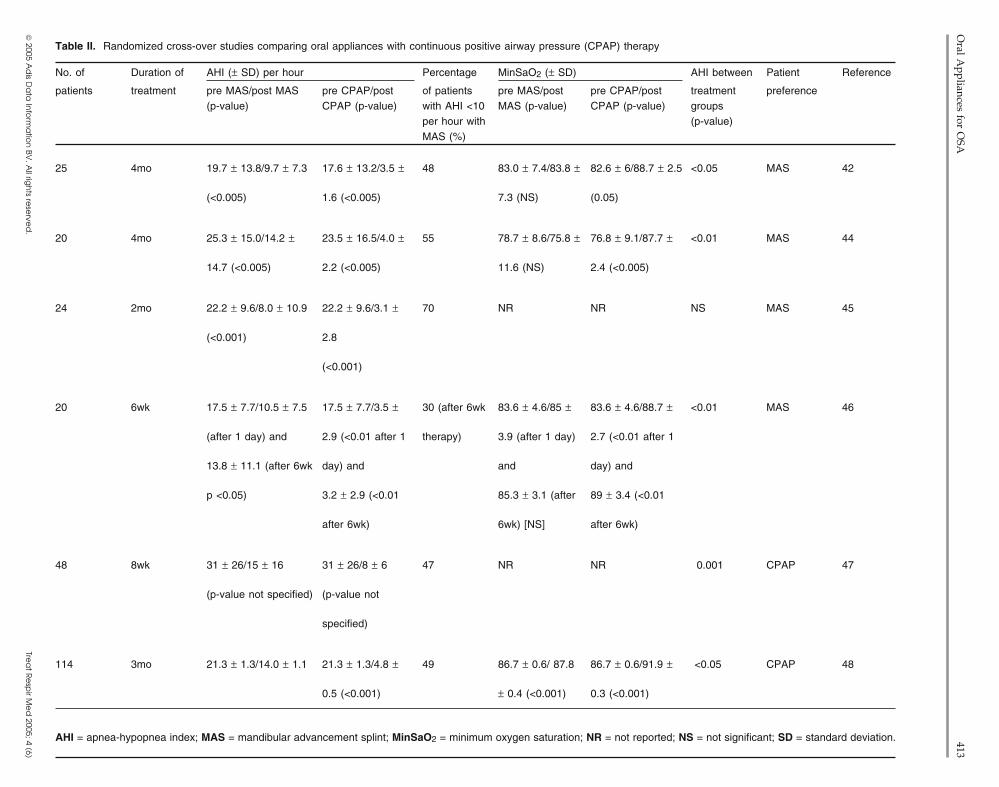
and rotate the mandible downwards. Increases in oropharyngeal There have been seven controlled crossover trials comparingand hypopharyngeal cross-sectional areas have been observed MAS and CPAP therapy,[42-48] with all but one[43] being random-with such devices. TRDs may work by counteracting the gravita- ized. These are summarized in table II. These studies vary in thetional effect of the supine position.[25,36]
type of MAS used, the measurement techniques used (e.g. homemonitoring versus in-laboratory monitoring), inclusion criteria,
2. Efficacy of Oral Appliances in OSA definitions of severity and treatment response, and number ofdropouts. However, collectively these studies involve 251 patientswith a mean AHI reduction of 43% when using the MAS and 78%2.1 Effect on Polysomnographic Variableswhen using CPAP, consistent with the superior efficacy of CPAP.
A review conducted in 1995 found that in general oral appli- The proportion of patients achieving an AHI <10 per hour withances are well tolerated, are associated with symptomatic im- MAS ranged from 30–70%, indicating variability in the efficacy ofprovements in the majority of patients, and result in an average different appliances. Despite the overall superiority of CPAP overreduction in AHI by 56%.[18] However, most of these studies had MASs, patient preference in five of the studies was for MASs. Inimportant methodological weaknesses, including small sample the study by Engleman et al.[47] the majority of patients preferredsizes, weak study designs, and liberal definitions of treatment CPAP therapy, but this may be accounted for by the fact that thesuccess. More recently, Pancer et al.[37] recruited the largest num- appliance used in this study was not adjustable and seemingly lessber of patients to date, 134 patients with all grades of OSA, and efficacious than other studies of MASs.
Table I. A summary of randomized controlled studies comparing efficacy of oral appliances with placebo
No. of Duration of AHI (±SD) [per hour] Patients with MinSaO2 (±SD) [%] Significance Reference
patients treatment (wk) baseline MAS placebo AHI <10/h with baseline MAS placebo of treatmentMAS effect (p-value)
24 1 27 ± 17 14 ± 2 30 ± 2 54% 85 ± 8 91 ± 1 87 ± 1 <0.0001 33(38% AHI <5/h)
73 4 27 ± 2 12 ± 2 25 ± 2 56% 86 ± 1 89 ± 1 86 ± 1 <0.0001 34(36% AHI <5/h)
18 4–6 32 ± 21 23 ± 23 38 ± 25 33% NR NR NR 0.01 38
AHI = apnea/hypopnea index; MAS = mandibular advancement splint; MinSaO2 = minimum oxygen saturation; SD = standard deviation; NR = notreported.
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)
Oral A
ppliances for OSA
413
© 2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Tre
at R
esp
ir Me
d 2005; 4 (6)
Table II. Randomized cross-over studies comparing oral appliances with continuous positive airway pressure (CPAP) therapy
No. of Duration of AHI (± SD) per hour Percentage MinSaO2 (± SD) AHI between Patient Reference
patients treatment pre MAS/post MAS pre CPAP/post of patients pre MAS/post pre CPAP/post treatment preference(p-value) CPAP (p-value) with AHI <10 MAS (p-value) CPAP (p-value) groups
per hour with (p-value)MAS (%)
25 4mo 19.7 ± 13.8/9.7 ± 7.3 17.6 ± 13.2/3.5 ± 48 83.0 ± 7.4/83.8 ± 82.6 ± 6/88.7 ± 2.5 <0.05 MAS 42
(<0.005) 1.6 (<0.005) 7.3 (NS) (0.05)
20 4mo 25.3 ± 15.0/14.2 ± 23.5 ± 16.5/4.0 ± 55 78.7 ± 8.6/75.8 ± 76.8 ± 9.1/87.7 ± <0.01 MAS 44
14.7 (<0.005) 2.2 (<0.005) 11.6 (NS) 2.4 (<0.005)
24 2mo 22.2 ± 9.6/8.0 ± 10.9 22.2 ± 9.6/3.1 ± 70 NR NR NS MAS 45
(<0.001) 2.8
(<0.001)
20 6wk 17.5 ± 7.7/10.5 ± 7.5 17.5 ± 7.7/3.5 ± 30 (after 6wk 83.6 ± 4.6/85 ± 83.6 ± 4.6/88.7 ± <0.01 MAS 46
(after 1 day) and 2.9 (<0.01 after 1 therapy) 3.9 (after 1 day) 2.7 (<0.01 after 1
13.8 ± 11.1 (after 6wk day) and and day) and
p <0.05) 3.2 ± 2.9 (<0.01 85.3 ± 3.1 (after 89 ± 3.4 (<0.01
after 6wk) 6wk) [NS] after 6wk)
48 8wk 31 ± 26/15 ± 16 31 ± 26/8 ± 6 47 NR NR 0.001 CPAP 47
(p-value not specified) (p-value not
specified)
114 3mo 21.3 ± 1.3/14.0 ± 1.1 21.3 ± 1.3/4.8 ± 49 86.7 ± 0.6/ 87.8 86.7 ± 0.6/91.9 ± <0.05 CPAP 48
0.5 (<0.001) ± 0.4 (<0.001) 0.3 (<0.001)
AHI = apnea-hypopnea index; MAS = mandibular advancement splint; MinSaO2 = minimum oxygen saturation; NR = not reported; NS = not significant; SD = standard deviation.

414 Ng et al.
2.3 Comparison with Surgical Treatment cy of MASs in controlling EDS, although limited, point towards asustained long-term benefit.[60]
To date only one study has compared MASs with surgical The effect of MASs on objective EDS is uncertain, as fewtreatment. Ninety-five patients with mild to moderate OSA were studies have investigated this outcome. In a case series by Meier-randomized to either uvulopalatopharyngoplasty (UPPP) or a one- Ewert and Brosig,[61] vigilance test improvements were related topiece acrylic MAS that protruded the mandible to 50% of the an improvement in AHI. Menn et al.[62] reported a significantmaximum,[49] and followed for 4 years. This study demonstrated a increase in maintenance of wakefulness test (MWT) mean sleepsignificantly higher success rate with MASs compared with UPPP, latency, in a volunteer subsample after MAS therapy (25 ± 9 minand with fewer adverse effects.[49] Interestingly, significantly vs 32 ± 10 min). Ten of the 13 patients achieved a mean sleepgreater contentment was demonstrated after UPPP than with the latency of >32 minutes, which is considered normal. Interestingly,dental appliance.[49] One study has suggested that oral appliance whilst a highly positive correlation between the decrease in AHItherapy may be an effective modality to control OSA after an and increase in MWT mean sleep latency was found, of the threeunsuccessful UPPP.[50]
patients with abnormal post-treatment mean sleep latencies, twowere responders.[62] The first randomized, controlled study to
2.4 Impact of Oral Appliance Therapy on Symptoms show an objective improvement in daytime sleepiness with MASin OSA therapy for OSA was reported by Gotsopoulos et al.[34] The mean
sleep latency on the multiple sleep latency test (MSLT) wasPatients with OSA experience diurnal symptoms. The three
significantly improved with MAS compared with the controlmost common symptoms of OSA are excessive daytime sleepiness
device (inactive oral plate) after 4 weeks of therapy, but the effect(EDS), snoring, and witnessed apneas.[6] The treatment objective
was relatively small (10.3 ± 0.5 min vs 9.1 ± 0.5 min). Noin patients with OSA is to relieve symptoms and to normalize the
significant predictors of objective daytime sleepiness treatmentAHI and oxygen saturation.[51]
outcome were detected in this study.[34]
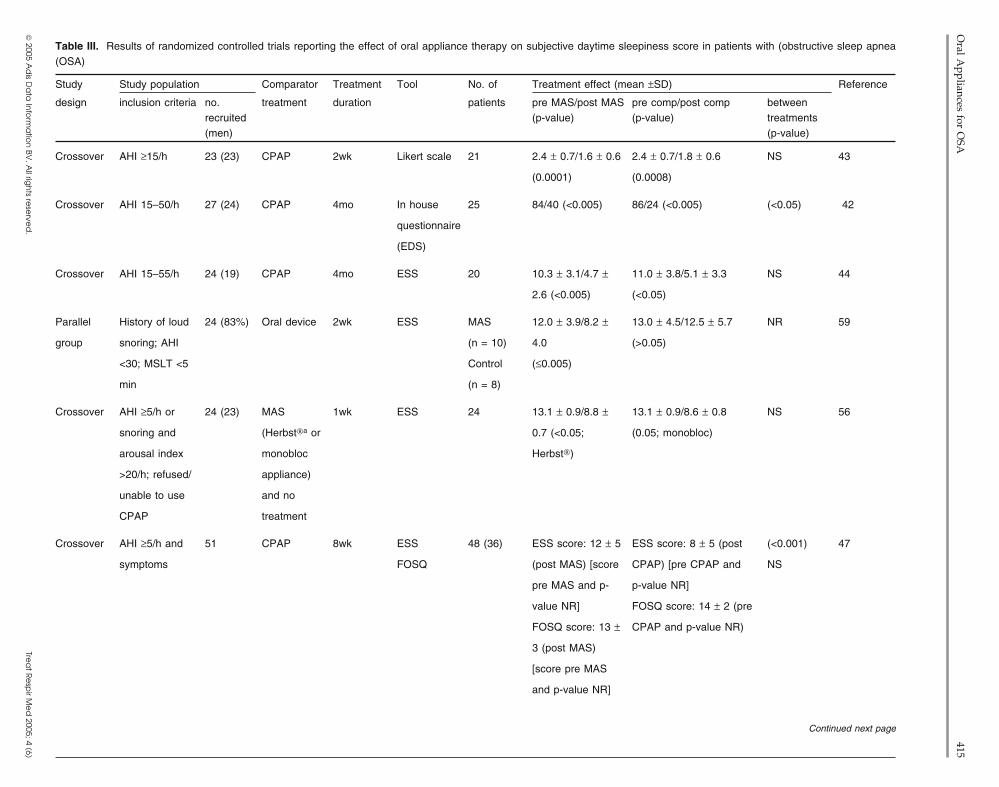
Findings from comparisons of MAS with CPAP in the resolu-2.4.1 Daytime Sleepinesstion of subjective EDS have been inconsistent (see table III), withThe EDS associated with OSA has serious public health impli-some studies demonstrating similar effects between treat-cations.[52] Epidemiological evidence suggests that OSA is linkedments,[43-46] but others showing the oral appliance to be lessto road traffic accidents, and this is thought to be primarily relatedeffective than CPAP.[42,47] Such disparities are most likely theto the symptom of EDS.[9,53,54] EDS can also contribute to emo-result of differences in patient populations, device design (e.g.tional, marital, social and occupational impairment.[55]
adjustable vs fixed MAS), degree of mandibular protrusion withEvidence suggests a beneficial effect of oral appliance therapythe MAS, treatment periods, and means of assessment.[42-47] Thefor OSA on daytime sleepiness. In their review, Schmidt-Nowaraefficacy of the MAS in resolving objective sleepiness in compari-et al.[18] reported improvement in subjective daytime sleepiness inson with CPAP remains uncertain as only one study has investigat-most (85%), but not all, patients. MAS therapy has been shown toed this. Engleman et al.[47] reported no significant difference insignificantly improve subjective daytime sleepiness associatedmean sleep onset latency on MWT between CPAP and MAS in tenwith OSA in comparison to no treatment.[56-58] However, findingssubjectively sleepy patients after 4–8 weeks of treatment.from comparisons to control oral devices were inconsistent; two
trials demonstrated significantly less daytime sleepiness with2.4.2 SnoringMAS,[34,59] whilst one did not.[38] This disparity does not seem toSnoring has been estimated by community-based surveys tobe related to treatment outcome.[34,38,59] An explanation may be the
affect 40–60% of adults.[63,64] Ohayon et al.[64] reported a 2.5%difference among studies in MAS compliance. For instance, whilstprevalence of combined snoring and witnessed apneas in adults.based on self-reported data, Gotsopoulos et al.[34] reported patientsOral appliances may be particularly useful in relieving this symp-wearing the MAS on average 97% ± 1 of nights during the 4-weektom, whether or not OSA is coexistent.treatment interval compared with Johnston et al.[38] who reported
68% of patients wearing their appliance 6–7 nights per week According to Schmidt-Nowara et al.,[18] various oral devices forduring an equivalent therapeutic period. Studies comparing differ- OSA showed subjective improvement in snoring in a high propor-ent types of MAS have shown no significant differences in im- tion of patients. This evidence is supported by more recentlyprovement of daytime sleepiness between appliances.[56,58] Ran- conducted randomized controlled trials of MAS indomized controlled trials on the effect of MASs on subjective EDS OSA.[34,38,56,58,65] Both snoring frequency and intensity are signifi-are summarized in table III. The data existing on long-term effica- cantly reduced compared to no treatment[56,66,67] and a control oral
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)
Oral A
ppliances for OSA
415
© 2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Tre
at R
esp
ir Me
d 2005; 4 (6)
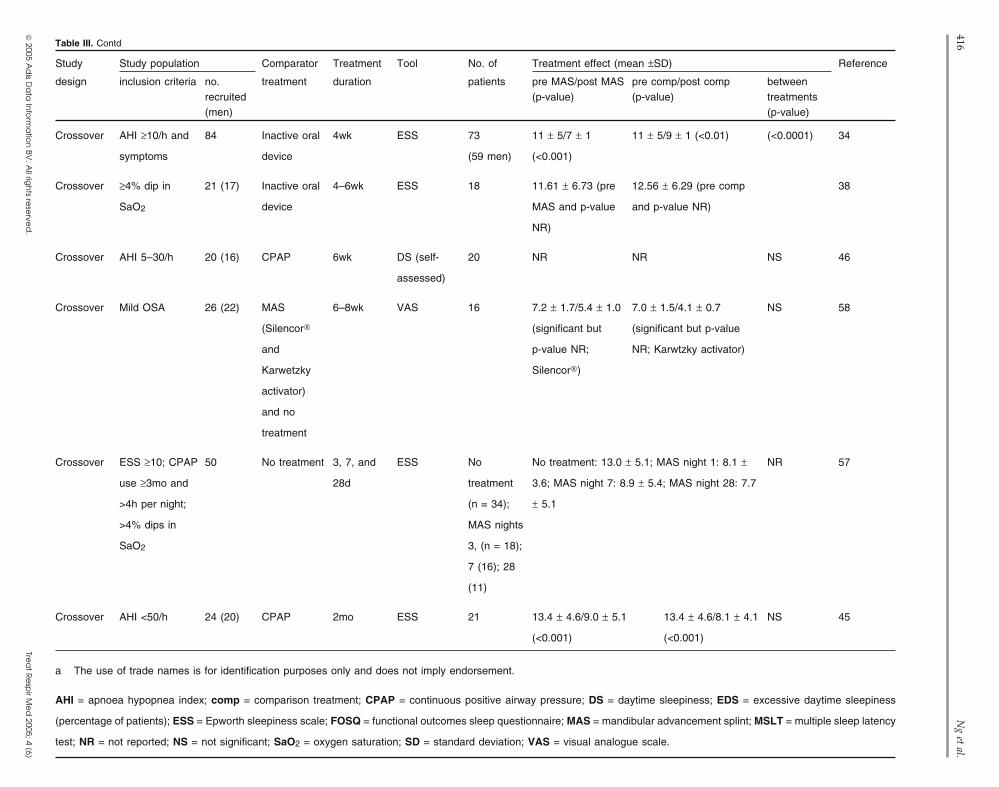
Table III. Results of randomized controlled trials reporting the effect of oral appliance therapy on subjective daytime sleepiness score in patients with (obstructive sleep apnea(OSA)
Study Study population Comparator Treatment Tool No. of Treatment effect (mean ±SD) Reference
design inclusion criteria no. treatment duration patients pre MAS/post MAS pre comp/post comp betweenrecruited (p-value) (p-value) treatments(men) (p-value)
Crossover AHI ≥15/h 23 (23) CPAP 2wk Likert scale 21 2.4 ± 0.7/1.6 ± 0.6 2.4 ± 0.7/1.8 ± 0.6 NS 43
(0.0001) (0.0008)
Crossover AHI 15–50/h 27 (24) CPAP 4mo In house 25 84/40 (<0.005) 86/24 (<0.005) (<0.05) 42
questionnaire
(EDS)
Crossover AHI 15–55/h 24 (19) CPAP 4mo ESS 20 10.3 ± 3.1/4.7 ± 11.0 ± 3.8/5.1 ± 3.3 NS 44
2.6 (<0.005) (<0.05)
Parallel History of loud 24 (83%) Oral device 2wk ESS MAS 12.0 ± 3.9/8.2 ± 13.0 ± 4.5/12.5 ± 5.7 NR 59
group snoring; AHI (n = 10) 4.0 (>0.05)
<30; MSLT <5 Control (≤0.005)
min (n = 8)
Crossover AHI ≥5/h or 24 (23) MAS 1wk ESS 24 13.1 ± 0.9/8.8 ± 13.1 ± 0.9/8.6 ± 0.8 NS 56
snoring and (Herbst®a or 0.7 (<0.05; (0.05; monobloc)
arousal index monobloc Herbst®)
>20/h; refused/ appliance)
unable to use and no
CPAP treatment
Crossover AHI ≥5/h and 51 CPAP 8wk ESS 48 (36) ESS score: 12 ± 5 ESS score: 8 ± 5 (post (<0.001) 47
symptoms FOSQ (post MAS) [score CPAP) [pre CPAP and NS
pre MAS and p- p-value NR]
value NR] FOSQ score: 14 ± 2 (pre
FOSQ score: 13 ± CPAP and p-value NR)
3 (post MAS)
[score pre MAS
and p-value NR]
Continued next page
416N
g et al.
© 2005 A
dis D
ata
Info
rma
tion
BV. A
ll righ
ts rese
rved
.Tre
at R
esp
ir Me
d 2005; 4 (6)
Table III. Contd
Study Study population Comparator Treatment Tool No. of Treatment effect (mean ±SD) Reference
design inclusion criteria no. treatment duration patients pre MAS/post MAS pre comp/post comp betweenrecruited (p-value) (p-value) treatments(men) (p-value)
Crossover AHI ≥10/h and 84 Inactive oral 4wk ESS 73 11 ± 5/7 ± 1 11 ± 5/9 ± 1 (<0.01) (<0.0001) 34
symptoms device (59 men) (<0.001)
Crossover ≥4% dip in 21 (17) Inactive oral 4–6wk ESS 18 11.61 ± 6.73 (pre 12.56 ± 6.29 (pre comp 38
SaO2 device MAS and p-value and p-value NR)
NR)
Crossover AHI 5–30/h 20 (16) CPAP 6wk DS (self- 20 NR NR NS 46
assessed)
Crossover Mild OSA 26 (22) MAS 6–8wk VAS 16 7.2 ± 1.7/5.4 ± 1.0 7.0 ± 1.5/4.1 ± 0.7 NS 58
(Silencor® (significant but (significant but p-value
and p-value NR; NR; Karwtzky activator)
Karwetzky Silencor®)
activator)
and no
treatment
Crossover ESS ≥10; CPAP 50 No treatment 3, 7, and ESS No No treatment: 13.0 ± 5.1; MAS night 1: 8.1 ± NR 57
use ≥3mo and 28d treatment 3.6; MAS night 7: 8.9 ± 5.4; MAS night 28: 7.7
>4h per night; (n = 34); ± 5.1
>4% dips in MAS nights
SaO2 3, (n = 18);
7 (16); 28
(11)
Crossover AHI <50/h 24 (20) CPAP 2mo ESS 21 13.4 ± 4.6/9.0 ± 5.1 13.4 ± 4.6/8.1 ± 4.1 NS 45
(<0.001) (<0.001)
a The use of trade names is for identification purposes only and does not imply endorsement.
AHI = apnoea hypopnea index; comp = comparison treatment; CPAP = continuous positive airway pressure; DS = daytime sleepiness; EDS = excessive daytime sleepiness
(percentage of patients); ESS = Epworth sleepiness scale; FOSQ = functional outcomes sleep questionnaire; MAS = mandibular advancement splint; MSLT = multiple sleep latency
test; NR = not reported; NS = not significant; SaO2 = oxygen saturation; SD = standard deviation; VAS = visual analogue scale.

Oral Appliances for OSA 417
appliance.[33,34] The long-term efficacy of MASs on subjective However, these findings have recently been challenged by Engle-snoring has been shown to be satisfactorily maintained in most man et al.[47] who showed symptoms to be significantly betterpatients.[49,60] Similar long-term snoring outcomes have been re- controlled with CPAP compared with MAS.[47] This finding mayported with MASs in comparison to UPPP.[49] be due in part to the choice of a study population specifically with
symptomatic OSA. In comparison to UPPP, no difference hasOne study alone has compared the effect of different types ofbeen found in vitality, and sleep. Significantly greater contentmentoral appliances on snoring. Marklund and Franklin[68] comparedhas been demonstrated with UPPP therapy compared with dentalthe effects of a MAS (activator), a soft palate lifter and a mouthappliance.[49]shield in 15 (12 men) habitual snorers. The MAS was the most
successful device in controlling subjective snoring during both the2.5 Cardiovascular Effectsshort- and long-term.[68]
To date there has been little research on the impact of oral2.4.3 Impact on Neuropsychological Functionappliance therapy on cardiovascular outcomes. Data from twoStudies evaluating neuropsychological functioning in patientsrecent randomized controlled studies evaluating the effect ofwith OSA have reported performance decrements across the do-MASs on blood pressure suggest a small but significant reductionmains of attention, working memory, memory, visuoconstruction-in blood pressure with MAS treatment compared with controlal, motor, and executive functioning. While varying associationstreatment (inactive oral plate).[48,74] Further work in this area isbetween such domains and OSA severity are evident, a recentrequired to evaluate whether the apparent beneficial effect ofreview of randomized placebo-controlled studies found only smallCPAP on blood pressure[75,76] also occurs with MAS treatment.effect size improvements in neuropsychological functioning with
CPAP treatment.[69] Other studies have shown a lack of improve-2.6 Efficacy in Upper Airway Resistance Syndromement, or improvements only to the extent of placebo or sub-
therapeutic treatment.[70-72] Thus, the therapeutic benefit of CPAP Upper airway resistance syndrome (UARS) is a subtle varianttherapy on aspects of daytime functioning remains uncertain, and of OSA.[77,78] Yoshida[79] performed a prospective trial on 32is likely to be influenced by factors such as apnea severity, pre- patients with UARS. Statistically and clinically significant im-morbid level of functioning, daytime sleepiness, co-morbid medi- provements in multiple variables were seen; Epworth sleepinesscal illness and, potentially, irreversible brain damage that cannot score improved from 13.2 to 5.8, mean sleep latency improvedbe alleviated despite adequate treatment. from 6.3 to 12.9 minutes, arousal index improved from 35.5 to 5.8
The impact of oral appliance therapy on neuropsychological per hour, oxygen saturation improved from 85.4% to 89.4% andfunctioning is yet to receive significant attention. Engleman et sleep efficiency improved from 85.4% to 90.3%. These dataal.[47] compared CPAP with an oral appliance and found no signifi- suggest that MAS may be helpful in the treatment of UARS.cant differences in cognitive performance between treatments.[47]
In a controlled study, Naismith et al.[73] found that MASs (com- 3. Prediction of Treatment Outcomepared with inactive oral plate) resulted in small to moderate
Given that treatment success with oral appliances is not achiev-enhancement in psychomotor speed in patients with OSA, but noable in all patients, it would be advantageous to be able to predictsignificant change in other neurocognitive measures.[73]
which patients will derive benefit so as to avoid inappropriate2.4.4 Other Symptoms delays in therapy and wastage of resources. A few studies haveOther common symptoms of OSA are nocturnal choking epi- attempted to predict the outcome of treatment with oral appliances.
sodes and arousals, sleep disruption, headaches, concentration and One study, using lateral cephalometry in 19 OSA patients, foundmemory deficits, personality changes and depression.[6] that a shorter soft palate and a decreased distance between the
Patients have reported significant improvements in their quality hyoid bone and the mandibular plane were associated with aof sleep with MAS compared with no treatment[58,65] or compared successful treatment outcome with a mandibular repositioningwith a control oral appliance.[34] However, Gotsopoulos et al.[34] appliance.[80] Another cephalometric study found that a combina-found no statistically significant difference in the number of tion of relative mandibular deficiency, shorter soft palate andpatients who reported sleep fragmentation (mainly attributed to narrow oropharynx gave the maximal efficacy with the Esmarchnocturia), choking episodes or witnessed apneas between treat- device.[81] Using multiple regression analysis, Mehta et al.[33]
ments. identified four independent predictors of outcome, viz. neck cir-In comparison to CPAP, studies have shown similar improve- cumference, baseline AHI, and two lateral cephalometric measure-
ments in OSA symptoms with both treatment types.[42,43,45,46] ments, viz. retropalatal airway space, and the angle between
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)

418 Ng et al.
anterior cranial base and mandibular plane.[33] Liu et al.[82] evalu- sion.[89] Good retention to both the upper and lower teeth isated a range of cephalometric and physiological parameters to important to ensure that the lower jaw does not drop out of theassess their ability to predict efficacy of an adjustable oral appli- appliance during sleep. Without good maxillary retention theance. Using stepwise regression analysis they observed a better entire appliance can dislodge. MASs that permit lateral jaw move-treatment response in patients who were younger and had a lower ment[25] or opening and closing whilst maintaining advance-body mass index, longer maxilla, smaller oropharynx, smaller ment[33,34] may offer advantages in terms of reduction of the risk ofoverjet, less erupted maxillary molars, and a larger ratio of vertical complications and better patient acceptance. However, it is evidentairway length to cross-sectional area of the soft palate. Collective- from the literature that most splints do not meet these designly, these studies suggest that treatment outcome is related criteria.[42,66,81,90] To date, it is also unclear whether custom-fittedpredominantly to anatomical characteristics. or serially-adjusted appliances are more effective than pre-fitted
appliances in the treatment of snoring and OSA. Most commonSanner et al.[83] studied 13 awake patients in the supine posi-splints are either one-piece or two-pieces, and connected with antion. MRI of the pharynx was performed at rest and during theintermaxillary coupling mechanism. One-piece splints are moreMueller maneuver, with and without MASs. Seven patients wererigid and bulky, however, they are sometimes indicated because ofknown MAS-treatment successes (defined as an AHI <10 perdental conditions and the occlusal relationship. There are severalhour) while the other six were treatment failures. All 13 patientsmodes of coupling between the upper and the lower parts of thehad pharyngeal occlusion when performing the Mueller maneuversplint such as elastic or plastic connectors, metal pin and tubewithout the MAS. Five of the seven treatment successes displayedconnectors, or hook connectors. Magnetic advancement splintsno significant occlusion when performing the maneuver with thehave also been evaluated.[91]MAS. In contrast, all six treatment-failure patients exhibited oc-
clusion despite wearing the MAS.[83] There are conflicting data on the effect of the degree of biteopening (vertical dimension of opening) induced by oral appli-Henke et al.[84] measured pharyngeal pressure in 12 patientsances on treatment outcome. The minimum and desirable inter-during sleep. Three patients demonstrated oropharyngeal collapseocclusal openings need to be considered separately on a case-by-and all three had >80% improvement in AHI which had decreasedcase basis. Depending on the amount of overbite, initial openingto <6 per hour. Nine patients demonstrated velopharyngeal col-may be required before advancement of the mandible is possible.lapse and two of these patients had a >80% reduction in AHI withInstead, if overbite is absent there may be no necessity to increasea further five patients having >50% reduction. They found thatthe vertical dimension. Some studies have shown that splints thatwhilst oropharyngeal collapse had a very favorable response toincrease the vertical dimension (10–15mm) are effective.[66] Simi-MASs, velopharyngeal closure did not preclude a favorable re-larly, Lamont et al.[92] reported greater success with a splintsponse. Preliminary data from another study suggests that primaryproducing 6–9mm of bite opening, compared with a splint produc-oropharyngeal collapse, rather than velopharyngeal collapse, maying 3–4mm of bite opening.[92] In contrast, a fluoroscopic studypredict good treatment response.[85]
showed that jaw opening is associated with synchronous posteriormovement of both tongue and soft palate, with consequent narrow-4. Oral Appliance Design and Titrationing of the oropharyngeal airway,[30] suggesting that bite openingshould be kept to a minimum to optimize outcome. All oral
4.1 Influence of Designappliances produce some downward rotation of the mandible andthis effect varies from person to person. A recent randomized,Various designs of MASs have been described for the treatmentcontrolled study found that the amount of vertical opening did notof snoring or OSA. Most of these appliances use traditional dentalimpact significantly on treatment outcome, but that minimal bitetechniques to attach the device to one or both dental arches andopening was better tolerated by patients.[93] Hence, it would appearvary in design from relatively simple acrylic moldings[86] to appli-that minimization of bite opening is desirable, at least from aances incorporating metallic rod and tube fittings and interarchtolerance point of view.elastics.[43,87] Construction requires dental impressions, a protru-
sive bite registration and fabrication by a dental laboratory. Pre-fabricated forms are also available and according to a recent 4.2 Oral Appliance Titrationsurvey of oral appliance use in the US,[88] these designs represent14% of oral appliances used by dentists to treat patients with OSA. Determination of the amount of mandibular advancement re-
The important aspects of the MAS design are said to include the quired to prevent OSA in a given patient is currently problematic.need for good retention, sufficient protrusion and vertical dimen- There does not appear to be a correlation between the amount of
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)

Oral Appliances for OSA 419
advancement and therapeutic effect.[33,84] Some authors have pro- ies.[18] Hence, whilst adverse effects are common, for most pa-posed 75% of maximal protrusion as a standard.[66,87] However, the tients these are minor and transient, subsiding with continued usedegree of protrusion required seems to vary from person to person, of the oral appliance.just like CPAP pressure varies between CPAP users, and is ulti-
5.2 Long-Term Adverse Effectsmately determined by the specific pathophysiological factors in-volved in the individual case. Some patients show no alteration in
With the growing use of oral appliances in the management ofairway dimensions even with maximal protrusion.[30] Hence, thereOSA attention has understandably turned to long-term adverseis no scientific basis in proposing a fixed percentage of maximaleffects. A number of studies have reported on clinical experienceprotrusion as the ideal advancement. Furthermore, patient toler-extending up to 5 years. Occlusal changes are predominantlyance will also determine the feasibility of advancement. Sincecharacterized by a reduction in overjet and overbite.[7,9,95-97] Pantintolerance increases with time, splints capable of incremental ad-et al.[95] showed that 14% of patients using MASs over a 5-yearvancement seem to have a clear practical advantage in this re-period had occlusal changes characterized by a 1–3mm decrease ingard.[33,44] In the study by Gotsopoulos et al.[34] the endpoint ofoverjet.[95] They found that the proportion of patients with occlusaltitration was the maximum comfortable limit of advancementchanges increased with the length of MAS use up to 2 years, afterrather than symptomatic response, and they found that a meanwhich the proportion remained relatively stable. Bondemark etadvancement of 7mm (3–13mm), representing 50–95% of maxi-al.[98] found a small forward (0.4mm) and downward (0.3mm)mal jaw protrusion, was the most comfortable position, and thischange in mandibular position after 2 years of MAS use. Occlusalwas generally achieved by incremental advancement over anchanges have been found to be less with a soft elastomeric device8-week (mean) period of acclimatization.[34] Reliance on sympto-as opposed to a hard acrylic device.[97] Robertson[99] conducted amatic response alone is problematic in light of the apparent place-longitudinal observational study over 5 years in 100 consecutivebo effect associated with oral appliance therapy.[33]
snoring and/or OSA patients using a MAS, and found evidence ofThe need for acclimatization over a period of weeks is a majoran increase in face height and reductions in overbite and overjet atdisadvantage compared with CPAP treatment, which can be insti-6 months, and over-eruption of the lower incisors at 24 months.tuted quickly. To overcome this, a recent study evaluated the
It is important to note that, in general, these changes are minorfeasibility of a single night titration procedure using a hydraulical-or even subclinical, and rarely warrant cessation of treatment.ly-controlled appliance in seven patients with severe OSA.[94]
Should significant occlusal changes occur, then the decisionThey achieved a mean advancement of 12.6mm without inducingwhether to discontinue therapy needs to balance the magnitude ofarousal, resulting in a significant reduction in mean AHI from 66.9the occlusal changes, the severity of OSA, and the desirability ofto 26.1 per hour during the titration night. A subsequent sleeptreatment alternatives (e.g. CPAP). At present, there is no evi-study to evaluate the efficacy of the oral appliance, set at the leveldence to suggest that there are consistent undesirable long-termof advancement determined on the titration night, indicated a meaneffects of MASs on the temporomandibular joints, but carefulAHI of 19.6 per hour, with three patients achieving an AHI <10monitoring for this potential complication is recommended.per hour.[94] This has the potential to overcome the current draw-
back of an acclimatization period.6. Clinical Practice Issues
5. Adverse Effects and Complications of It is generally considered that the effective delivery of oralOral Appliances appliance therapy for patients with snoring and OSA requires a
multidisciplinary approach, with involvement of a physician, sleeplaboratory personnel and the dentist. Local regulatory issues may5.1 Short-Term Adverse Effectsdictate the absolute requirement for certain health professionals in
The majority of patients experience adverse effects during the the delivery of care. The Academy of Dental Sleep Medicineinitiation phase of treatment. These include dental discomfort advocates an initial medical assessment from a physician with(33%) particularly of the upper and lower incisors, temporo- relevant sleep expertise, and overnight polysomnography ifmandibular joint pain (12.5–33%), dry mouth (28–46%), saliva- deemed to be clinically indicated.[25] This is followed by referral totion (38–50%), gum irritation (20%), and bruxism (12.5%).[33,95] an appropriately skilled dentist, whose role it is to assess theThese are generally described as mild to moderate, lasting less patient’s suitability for oral appliance therapy, determination ofthan a few weeks, and do not preclude continued use of the MAS the appropriate appliance design, and subsequent delivery of treat-in most patients. These are consistent observations across stud- ment. Once titration of the oral appliance is complete, the patient
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)

420 Ng et al.
should return to the physician for medical follow-up, and repeat patients in whom this therapy is likely to be successful. It is hopedovernight polysomnography as needed. The importance of objec- that a simple screening technique, possibly involving clinical and/tive verification of treatment outcome by polysomnography is or radiological measurements, will be developed. Whilst there issupported by evidence of a placebo effect.[33] Both medical and now good evidence for the efficacy of oral appliances over thedental follow-up are required for patients who embark on long- short-term, long-term studies using objective measures of efficacyterm treatment with an oral appliance to monitor the effectiveness are lacking. Another drawback is the duration of time required toof therapy in controlling OSA and for the appearance of dental attain maximal efficacy of treatment, as a result of the titrationadverse effects. procedure usually employed. This limits the use of such therapy in
circumstances where rapid establishment of treatment is desirableClinical practice parameters developed by the American Sleep(e.g. severe OSA or a sleepy driver). The ‘dosage’ of mandibularDisorders Association (now the American Academy of Sleepadvancement required to control OSA in an individual patient is atMedicine) in 1995 recommended that oral appliances be consid-this stage a matter of trial and error, and further research isered only for snoring and mild OSA, or for patients with morerequired to develop a more scientific approach. The influence ofsevere OSA who refuse, or are unable to tolerate, CPAP.[51]
appliance design on treatment outcome and adverse effects isHowever, the evidence base has progressed considerably since theuncertain, and studies comparing different appliances are war-time of that review and now lends support for the consideration ofranted to resolve this issue. Long-term follow-up of patients isthe use of oral appliances as first-line therapy in patients withrequired to determine treatment compliance and whether improve-moderate OSA, with a strong proviso that efficacy be monitoredment in symptoms is sustained. Prospective studies are needed toobjectively.assess the impact of oral appliance therapy on morbidity andWhilst oral appliances may be effective in OSA, they do notmortality associated with sleepiness and cardiovascular outcomeshave any role in treating central forms of sleep apnea, includingin OSA.hypoventilation syndromes. There are reports of OSA being wors-
ened by oral appliance therapy,[25,84] and hence clinical vigilance8. Conclusionand objective monitoring of outcome is critical in all OSA pa-
tients. Extreme caution is warranted in treating OSA patients with Effective treatment of OSA is critical in the light of its highmedicolegal concerns, e.g. a commercial driver with excessive prevalence and diverse adverse effects on patients and the commu-daytime sleepiness. These types of cases are best managed with nity at large. CPAP is unquestionably an effective treatment but itsCPAP until evidence supporting the use of oral appliances in this obtrusive nature undermines its benefit. There is a need for genu-situation is forthcoming. ine alternative treatments that are better accepted by patients. Oral-
From a dental perspective, the presence of temporomandibular appliance therapy is an effective alternative for a substantialdysfunction may be a contraindication to the use of oral appli- number of patients with OSA. Notwithstanding the unresolvedances, although this should be assessed on a case-by-case basis by issues that preclude its use as first-line therapy in all patients witha dentist. Insufficient teeth to support the device or the presence of OSA, the evidence base for its consideration in some patients isperiodontal disease inducing tooth mobility may preclude treat- now strong. The challenge for researchers in the field is to contin-ment. Similarly, a limited capacity for mandibular protrusion ue to build the evidence, and to more clearly define the role of oral(<6mm) has been suggested to be a contraindication, although appliance therapy in the management of OSA.studies have reported success with lesser degrees of mandibularadvancement.[34] Petit et al.[100] reported results of a study in 100 Acknowledgementsconsecutive OSA patients in which 34% of the patients were
The authors have received grant support from NHMRC of Australia. Drassessed to have dental contraindications to oral appliance therapy. Cistulli is on the Medical Advisory Board of SomnoMed, a company that isThese investigators suggested that this limited the scope of oral commercializing an oral appliance for snoring and OSA, has received consult-appliance therapy. ing fees and holds shares in SomnoMed; and has been a principal investigator
in sleep apnea clinical trials supported by ResMed and Cephalon.
7. Unresolved Issues and Future ResearchReferences
1. Cistulli PA, Sullivan CE. Pathophysiology of sleep apnea. In: Saunders NA,Whilst a role for oral appliances in the management of OSA is Sullivan CE, editors. Sleep and breathing. 2nd ed. New York: Marcel Dekker
Inc., 1994: 405-48now unquestionable, a number of unresolved issues make their2. Cirignotta F, D’Alessandro R, Partinen M, et al. Prevalence of every night snoringroutine use uncertain. A key issue is the inability to predict and obstructive sleep apnoeas among 30–69-year-old men in Bologna, Italy.
treatment outcome, in order to be able to target the subgroup of Acta Neurol Scand 1989; 79: 366-72
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)
Oral Appliances for OSA 421
3. Young T, Palta M, Dempsey J, et al. The occurrence of sleep disordered breathing 29. Gao XM, Zeng XL, Fu MK. Magnetic resonance imaging of the upper airway inamong middle-aged adults. N Engl J Med 1993; 328: 1230-5 obstructive sleep apnea before and after oral appliance therapy. Chin J Dent Res
1999; 2: 27-354. Gislason T, Almqvist M, Eriksson G, et al. Prevalence of sleep apnea syndrome30. L’Estrange PR, Battagel JM, Harkness B. A method of studying adaptive changesamong Swedish men: an epidemiological study. J Clin Epidemiol 1988; 41:
of the oropharynx to variation in mandibular position in patients with obstruc-571-6tive sleep apnoea. J Oral Rehab 1996; 23: 699-7115. Gislason T, Benediktsdottir B, Bjornsson JK, et al. Snoring, hypertension, and the
31. Isono S, Tanaka A, Tagaito Y, et al. Pharyngeal patency in response to advance-sleep apnea syndrome. An epidemiologic survey of middle-aged women. Chestment of the mandible in obese anesthetized persons. Anesthesiology 1997; 87:1993; 103: 1147-511055-626. McNamara S, Cistulli PA, Sullivan CE, et al. Clinical aspects of sleep apnea. In:
32. Yoshida K. Effect of a prosthetic appliance for treatment of sleep apnea syndromeSaunders NA, Sullivan CE, editors. Sleep and breathing. 2nd ed. New York:on masticatory and tongue muscle activity. J Prosthet Dent 1998; 79: 537-44Marcel Dekker Inc., 1994: 493-528
33. Mehta A, Qian J, Petocz P, et al. A randomized, controlled study of a mandibular7. D’Ambrosio C, Bowman T, Mohsenin V. Quality of life in patients with obstruc-advancement splint for obstructive sleep apnea. Am J Respir Crit Care Medtive sleep apnea: effect of nasal continuous positive airway pressure: a prospec-2001; 163: 1457-61tive study. Chest 1999; 115: 123-9
34. Gotsopoulos H, Chen C, Qian J, et al. Oral appliance therapy improves symptoms8. Weiss JW, Launois SH, Anand A, et al. Cardiovascular morbidity in obstructivein obstructive sleep apnea: a randomized, controlled trial. Am J Respir Crit Caresleep apnea. Prog Cardiovasc Dis 1999; 41: 367-76Med 2002; 166: 743-8
9. Teran-Santos J, Jimenez-Gomez A, Cordero-Gueva J. The association between35. Ng AT, Gotsopoulos H, Qian J, et al. Effect of of appliance therapy on upper
sleep apnea and the risk of traffic accidents. N Engl J Med 1999; 340: 847-51airway collapsibility in obstructive sleep apnea. Am J Respir Crit Care Med
10. Sullivan CE, Issa FG, Berthon-Jones M, et al. Reversal of obstructive sleep apnea 2003; 168: 238-41by continuous positive pressure applied through the nares. Lancet 1981; I:
36. Ono T, Lowe AA, Ferguson KA, et al. A tongue retaining device and sleep-state862-5
genioglossus muscle activity in patients with obstructive sleep apnea. Angle11. McArdle N, Devereux G, Heidarnejad H, et al. Long-term use of CPAP therapy for Orthod 1996; 66: 273-80
sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 1999; 159: 37. Pancer J, Al-Faifi S, Al-Faifi M, et al. Evaluation of variable mandibular advance-1108-14 ment appliance for treatment of snoring and sleep apnea. Chest 1999; 116:
12. Weaver TE, Kribbs NB, Pack AI, et al. Night-to-night variability in CPAP use over 1511-8the first three months of treatment. Sleep 1997; 20: 278-83 38. Johnston CD, Gleadhill IC, Cinnamond MJ, et al. Mandibular advancement appli-
13. Kribbs NB, Pack AI, Kline LR, et al. Objective measurement of patterns of nasal ances and obstructive sleep apnoea: a randomized clinical trial. Eur J OrthodCPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 1993; 2002; 24: 251-62147: 887-95 39. Ferguson K. Oral appliance therapy for obstructive sleep apnea: finally evidence
14. Cistulli PA. Craniofacial abnormalities in obstructive sleep apnoea: implications you can sink your teeth into. Am J Respir Crit Care Med 2001; 163: 1294-5for treatment. Respirology 1996; 3: 167-74 40. Cartwright R, Stefosko D, Caldarelli D, et al. Toward a treatment logic for sleep
15. Robin P. Glossoptosis due to atresia and hypotrophy of the mandible. Am J Dis apnea: the tongue retaining device. Behav Res Ther 1988; 26: 121-6Child 1934; 48: 541-7 41. Higurashi N, Kikuchi M, Miyazaki S, et al. Effectiveness of a tongue-retaining
device. Psychiatry Clin Neurosci 2002; 56: 331-216. Meier-Ewert K, Schafer H, Kloss W. Proceedings of the Seventh EuropeanCongress on Sleep Research; 1984; Munich 42. Ferguson KA, Ono T, Lowe AA, et al. A randomized crossover study of an oral
appliance vs nasal continuous positive airway pressure in the treatment of mild-17. Soll BA, George PT. Treatment of obstructive sleep apnea with a nocturnal airway-moderate obstructive sleep apnea. Chest 1996; 109: 1269-75patency appliance [letter]. N Engl J Med 1985; 313: 386-7
43. Clark GT, Blumenfeld I, Yoffe N, et al. A crossover study comparing the efficacy18. Schmidt-Nowara W, Lowe A, Wiegand L, et al. Oral appliances for the treatmentof CPAP with anterior mandibular positioning devices on patients with obstruc-of snoring and obstructive sleep apnea: a review. Sleep 1995; 18: 501-10tive sleep apnoea. Chest 1996; 109: 1477-8319. Haponik EF, Smith P, Bohlman M, et al. Computerized tomography in obstructive
44. Ferguson KA, Ono T, Lowe AA, et al. A short term controlled trial of an adjustablesleep apnea: correlation of airway size with physiology during sleep andoral appliance for the treatment of mild to moderate obstructive sleep apnoea.wakefulness. Am Rev Respir Dis 1983; 127: 221-6Thorax 1997; 52: 362-820. Suratt PM, Dee R, Atkinson RL, et al. Fluoroscopic and computed tomographic
45. Tan YK, L’Estrange PR, Luo YM, et al. Mandibular advancement splints andfeatures of the pharyngeal airway in obstructive sleep apnea. Am Rev Respircontinuous positive airway pressure in patients with obstructive sleep apnoea: aDis 1983; 127: 487-92randomized cross-over trial. Eur J Orthod 2002; 24: 239-49
21. White DP. Pathophysiology of obstructive sleep apnoea. Thorax 1996; 50: 797-80446. Randerath WJ, Heise M, Hinz R, et al. An individually adjustable oral appliance vs
22. Riley RW, Powell NB, Li KK, et al. Surgical therapy for obstructive sleep apnea-continuous positive airway pressure in mild to moderate obstructive sleep apnea
hypopnea syndrome. In: Kryger MH, Roth T, Dement WC, editors. Principlessyndrome. Chest 2002; 122: 569-75
and practice of sleep medicine. 3rd ed. Philadelphia (PA): WB Saunders Co.,47. Engleman HM, McDonald JP, Graham D, et al. Randomized crossover trial of two
2000: 913-28treatments for sleep apnea/hypopnea syndrome: continuous positive airway
23. Smith PL, Eisele DW, Podszus T, et al. Electrical stimulation of upper airway pressure and mandibular repositioning splint. Am J Respir Crit Care Med 2002;musculature. Sleep 1996; 19: S284-7 166: 855-9
24. Hudgel DW. Thanakitcharu S. Pharmacologic treatment of sleep-disordered 48. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure andbreathing. Am J Respir Crit Care Med 1998; 158: 691-9 oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit
25. Lowe AA. Oral appliances for sleep breathing disorders. In: Kryger MH, Roth T, Care Med 2004; 170: 656-64Dement WC, editors. Principles and practice of sleep medicine. 3rd ed. Phila- 49. Walker-Engstrom ML, Tegelberg A, Wilhelmsson B, et al. 4-Year follow-up ofdelphia (PA): WB Saunders Co., 2000: 929-39 treatment with dental appliance or uvulopalatoplasty in patients with obstruc-
26. Schwab RJ. Upper airway soft tissue structural changes with a dental appliance in tive sleep apnea: a randomized study. Chest 2002; 121: 739-46apneics. Am J Respir Crit Care Med 1996; 153: 719 50. Millman RP, Rosenberg CL, Carlisle CC, et al. The efficacy of oral appliances in
27. Ryan CF, Love LL, Peat D, et al. Mandibular advancement oral appliance therapy the treatment of persistent sleep apnea after vulopalatopharyngoplasty. Chestfor obstructive sleep apnoea: effect on awake calibre of the velopharynx. 1998; 113: 992-6Thorax 1999; 54: 972-7 51. American Sleep Disorders Association. Practice parameters for the treatment of
snoring and obstructive sleep apnea with oral appliances. Sleep 1995; 18: 511-328. Ishida M, Inoue Y, Suto Y. Mechanisms of action and therapeutic indication ofprosthetic mandibular advancement in obstructive sleep apnea syndrome. Psy- 52. Mitler MM, Carskadon MA, Czeisler CA, et al. Catastrophes, sleep, and publicchiatry Clin Neurosci 1998; 52: 227-9 policy: consensus report. Sleep 1988; 11: 100-9
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)
422 Ng et al.
53. Findley LJ, Fabrizio M, Thommi G, et al. Severity of sleep apnea and automobile 77. Guilleminault C, Chowdhuri S. Upper airway resistance syndrome is a distinctcrashes. N Engl J Med 1989; 320: 868-9 syndrome. Am J Respir Crit Care Med 2000; 161: 1412-3
54. Findley L, Unverzagt M, Guchu R, et al. Vigilance and automobile accidents in 78. Douglas NJ. Upper airway resistance syndrome is not a distinct syndrome. Am Jpatients with sleep apnea or narcolepsy. Chest 1995; 108: 619-24 Respir Crit Care Med 2000; 161: 1413-6
55. Guilleminault C, Carskadon M. Relationship between sleep disorders and daytime 79. Yoshida K. Oral device therapy for the upper airway resistance syndrome patient. Jcomplaints. In: Koella P, Levin P, editors. Proceedings of the Third European Prosthet Dent 2002; 87: 427-30Congress on Sleep Research; 1976 Sep 6–10; Montpellier. Basel: Karger, 1976 80. Eveloff SC, Rosenberg CL, Carlisle CC, et al. Efficacy of a herbst mandibular
56. Bloch KE, Iseli A, Zhang JN, et al. A randomized, controlled crossover trial of two advancement device in obstructive sleep apnea. Am J Respir Crit Care Medoral appliances for sleep apnea treatment. Am J Respir Crit Care Med 2000; 1994; 149: 905-9162: 246-51
81. Mayer G, Meier-Ewert K. Cephalometric predictors for orthopaedic mandibular57. Smith DM, Stradling JR. Can mandibular advancement devices be a satisfactory advancement in obstructive sleep apnoea. Eur J Orthod 1995; 17: 35-43
substitute for short term use in patients on nasal continuous positive airway82. Liu Y, Lowe AA, Fleetham JA, et al. Cephalometric and physiological predictors
pressure? Thorax 2002; 57: 305-8of the efficacy of an adjustable oral appliance for treating obstructive sleep
58. Rose E, Staats R, Virchow C, et al. A comparative study of two mandibular apnea. Am J Orthod Dentofacial Orthop 2001; 120: 639-47advancement appliances for the treatment of obstructive sleep apnoea. Eur J
83. Sanner BM, Heise M, Knoben B, et al. MRI of the pharynx and treatment efficacyOrthod 2002; 24: 191-8of a mandibular advancement device in obstructive sleep apnoea syndrome. Eur
59. Hans MG, Nelson S, Luks VG, et al. Comparison of two dental devices for Respir J 2002; 20: 143-50treatment of obstructive sleep apnea syndrome (OSAS). Am J Orthod
84. Henke KG, Frantz DE, Kuna ST. An oral elastic mandibular advancement deviceDentofacial Orthop 1997; 111: 562-70for obstructive sleep apnea. Am J Respir Crit Care Med 2000; 161: 420-5
60. Marklund M, Sahlin C, Stenlund H, et al. Mandibular advancement device in85. Ng AT, Gotsopoulos H, Qian J, et al. Influence of site of upper airway obstructionpatients with obstructive sleep apnea: long-term effects on apnea and sleep.
during sleep on response to oral appliance therapy in obstructive sleep apneaChest 2001; 120: 162-9[abstract]. Am J Respir Crit Care Med 2003; 167: A324
61. Meier-Ewert K, Brosig B. Treatment of sleep apnea by prosthetic mandibular86. Nakazawa Y, Sakamoto T, Yasutake R, et al. Treatment of sleep apnea withadvancement. In: Peter H, Podszus T, von Wichert P, editors. Sleep related
prosthetic mandibular advancement (PMA). Sleep 1992; 15: 499-504disorders and internal diseases. Berlin: Springer-Verlag, 1987: 341-4587. Clark GT, Arand D, Chung E, et al. Effect of anterior mandibular positioning on62. Menn SJ, Loube DI, Morgan TD, et al. The mandibular repositioning device: role
obstructive sleep apnoea. Am Rev Respir Dis 1993; 147: 624-9in the treatment of obstructive sleep apnea. Sleep 1996; 19: 794-80088. Loube DI, Strauss AM. Survey of oral appliance practice among dentists treating63. Norton PG, Dunn EV. Snoring as a risk factor for disease: an epidemiological
obstructive sleep apnoea patients. Chest 1997; 111: 382-6survey. BMJ 1985; 291: 630-2
89. Battagel JM. Obstructive sleep apnoea: fact not fiction. Br J Orthod 1996; 23:64. Ohayon MM, Guilleminault C, Priest RG, et al. Snoring and breathing pauses315-24during sleep: telephone interview survey of a United Kingdom population
sample. BMJ 1997; 314: 860-3 90. Schmidt-Nowara WW, Meade TE, Hays MB. Treatment of snoring and obstructive65. Cameron DA, Lyons MF, Fox DL, et al. Pilot study of a semi-flexible intra-oral sleep apnea with a dental orthosis. Chest 1991; 99: 1378-85
appliance for the control of snoring. Br Dent J 1998; 185: 304-7 91. Gavish A, Vardimon AD, Rachima H, et al. Cephalometric and polysomnographic66. O’Sullivan RA, Hillman DR, Mateljan R, et al. Mandibular advancement splint: an analyses of functional magnetic system therapy in patients with obstructive
appliance to treat snoring and obstructive sleep apnea. Am J Respir Crit Care sleep apnea. Am J Orthod Dentofacial Orthop 2001; 120: 169-77Med 1995; 151: 194-8 92. Lamont J. Effect of two types of mandibular advancement splints on snoring and
67. Stradling JR, Negus TW, Smith D, et al. Mandibular advancement devices for the obstructive sleep apnoea. Eur J Orthod 1998; 20: 293-7control of snoring. Eur Respir J 1998; 11: 447-50 93. Pitsis A, Darendeliler MA, Gotsopoulos H, et al. Effect of vertical dimension on
68. Marklund M, Franklin KA. Dental appliances in the treatment of snoring: a efficacy of mandibular advancement splint therapy in obstructive sleep apnea.comparison between an activator, a soft-palate lifter, and a mouth-shield. Swed Am J Respir Crit Care Med 2002; 166: 860-4Dent J 1996; 20: 183-8
94. Petele B, Vincent G, Gagnadoux F, et al. Am J Respir Crit Care Med 2002; 165:69. Engleman HM, Kingshott RN, Martin SE, et al. Cognitive function in the sleep 1150-1153
apnea/hypopnea syndrome (SAHS). Sleep 2000; 23: S102-795. Pantin CC, Hillman DR, Tennant M. Dental side effects of an oral device to treat
70. Henke KG, Grady JJ, Kuna ST. Effect of nasal continuous positive airway pressure snoring and obstructive sleep apnoea. Sleep 1999; 22: 237-40on neuropsychological function in sleep apnea-hypopnea syndrome: a random-
96. Fritsch KM, Iseli A, Russi W, et al. Side effects of mandibular advancementized, placebo-controlled trial. Am J Respir Crit Care Med 1999; 163: 911-7devices for sleep apnoea treatment. Am J Respir Crit Care Med 2001; 164:
71. Yu B, Ancolio-Israel S, Dimsdale JE. Effect of CPAP treatment on mood states in813-8
patients with sleep apnea. J Psychiatr Res 1999; 33: 427-3297. Marklund M, Franklin KA, Persson M. Orthodontic side-effects of mandibular
72. Engleman HM, Martin SE, Deary IJ, et al. Effect of CPAP therapy on daytimeadvancement devices during treatment of snoring and sleep apnoea. Eur J
function in patients with mild sleep apnoea/hypopnea syndrome. Thorax 1997;Orthod 2001; 23: 135-44
52: 114-998. Bondemark L. Does 2 years nocturnal treatment with mandibular advancement73. Naismith S, Winter V, Hickie I, et al. Effect of oral appliance therapy on
splint in adult patients with snoring and OSAS cause a change in the posture ofneurobehavioural functioning in obstructive sleep apnea: a randomised con-the mandible? Am J Orthod Dentofacial Orthop 1999; 116: 621-8trolled trial. J Clin Sleep Med 2005; 1 (4): 278-84
99. Robertson C. Dental and skeletal changes associated with long-term mandibular74. Gotsopoulos H, Keyy JJ, Cistulli P. Appliance therapy reduces blood pressure inadvancement. Sleep 2001; 24: 531-7obstructive sleep apnea: a randomized, controlled trial. Sleep 2005; 1 (4):
100. Petit F, Pepin J, Bettega G, et al. Mandibular advancement devices: rate of934-41contraindications in 100 consecutive obstructive sleep apnea patients. Am J75. Faccenda JF, Mackay TW, Boon NA, et al. Randomized placebo-controlled trial ofRespir Crit Care Med 2002; 166: 274-8continuous positive airway pressure on blood pressure in the sleep apnea-
hypopnea syndrome. Am J Respir Crit Care Med 2001; 163: 344-8
76. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, et al. Ambulatory bloodCorrespondence and offprints: Peter A. Cistulli, University of Sydney &pressure after therapeutic and subtherapeutic nasal continuous positive airwayRoyal North Shore Hospital, St Leonard’s, Sydney, 2065, NSW, Australia.pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002;
359: 204-10 E-mail: [email protected]
© 2005 Adis Data Information BV. All rights reserved. Treat Respir Med 2005; 4 (6)





























