Embed Size (px)
Citation preview
OHA contact info: [email protected] Topics may be subject to change due to availability
Oregon Health Authority
Quality and Health Outcomes Committee AGENDA
Wednesday, September 14, 2016
2:00 p.m. – 4:00 p.m.
MEETING INFORMATION Meeting Date: December 14, 2020 Time: 10:00a.m.- 12:00pm Location: Webinar Only Call in information: Toll free: 888-278-0293 Passcode: 310477 Webinar: https://attendee.gotowebinar.com/register/5243835245211654924 All meeting materials are posted on the QHOC Website
Clinical Director Workgroup 10:00 a.m. – 12:00 p.m.
TIME TOPIC OWNER MATERIALS (page#)
10:00 a.m. Welcome Holly Jo Hodges
10:05 a.m. Announcements Lisa Bui TC TA flyer (2-7)
10:15 a.m.
COVID-19
• Testing Capacity
• COVID vaccine update
Dana Hargunani Dawn Mautner
Presentation slides
10:45 a.m. HERC update Ariel Smits Meeting minutes (8-40) Presentation slides
11:00 a.m. Break
11:20 a.m. BH Topics - IIBHT - ABA - OSH
Lisa Bui Dave Inbody
OSH process map (41-44)
12:00 p.m. Adjourn
Everyone is welcome to the meetings. For questions about accessibility or to request an accommodation, please call 971-304-6236 or write [email protected]. Requests should be made at least 48 hours prior to the event. Documents can be provided upon request in an alternate format for individuals with disabilities or in a language other than English for people with limited English skills. To request a document in another format or language, please call 971-304-6236 or write [email protected].
OHA Transformation Center Technical Assistance (TA) for CCOs
TA index Metrics TA ............................................................................................................................................................................... 1
Adolescent immunizations ...................................................................................................................................................... 1
Diabetes: HbA1c poor control ................................................................................................................................................. 1
Kindergarten readiness ........................................................................................................................................................... 3
Screening, brief intervention and referral to treatment (SBIRT) ............................................................................................ 3
Tobacco cessation ................................................................................................................................................................... 3
Multiple metrics (non-Transformation Center TA) ................................................................................................................. 4
Non-metrics TA ....................................................................................................................................................................... 4
Community advisory councils ................................................................................................................................................. 4
Health-related services (HRS) ................................................................................................................................................. 5
REALD ...................................................................................................................................................................................... 5
Transformation and quality strategy ...................................................................................................................................... 6
Transformation Center technical assistance updates ........................................................................................................... 6
Metrics TA
Adolescent immunizations
You Are the Key to HPV Cancer Prevention (recorded webinar)
What: The Oregon Pacific Area Health Education Center invites you to its recorded “You are the Key to HPV Cancer
Prevention” webinar to learn about the adolescent HPV vaccination schedule and how to communicate with parents
about the HPV vaccine.
Audience: Physicians, pharmacists, nurse practitioners, physician assistants, nurses or any other staff who work with
children, adolescents and their parents in primary care settings.
Access the recording, along with other upcoming or recorded OPAHEC webinars: https://www.opahec.org/webinars-1
Diabetes: HbA1c poor control
Quality improvement training + TA for primary care: Diabetes control and dental care for patients with diabetes
What: Half-day virtual training plus an additional five hours per clinic team for individually tailored improvement
support targeting poor HbA1C and oral health evaluation. TA will be provided by the Oregon Rural Practice-based
Network and is sponsored by the OHA Transformation Center.
When: January 28 or March 11 (NEW); noon-4 p.m.
Audience: RNs, lead MAs, clinic managers, quality improvement staff and others interested in quality improvement for
type II diabetes patient management/ improving HBA1C poor control.
Register here: https://ohsu.ca1.qualtrics.com/jfe/form/SV_51QPh3AQbLSaxLv
Flier: https://www.oregon.gov/oha/HPA/dsi-tc/Documents/Diabetes-TA-Recruitment-Flier.pdf
December 2020 QHOC Meeting Packet Page 2 of 44
Questions? Contact Laura Ferrara at [email protected] or (971) 413-9585
Recorded diabetes care webinars with no-cost CME for clinicians
The Transformation Center invites clinicians who serve Oregonians to two no-cost CME-accredited recorded webinars
focused on lowering rates of HbA1c poor control The webinars feature Dr. Andrew Ahmann, director of the Harold
Schnitzer Diabetes Health Center and recipient of the 2018 Outstanding Physician Clinician in Diabetes Award from the
American Diabetes Association.
• Accreditation: This activity has been planned and implemented in accordance with the accreditation
requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the
joint providership of OHSU School of Medicine and Oregon Health Authority. The OHSU School of Medicine is
accredited by the ACCME to provide continuing medical education for physicians.
• Credit: OHSU School of Medicine designates this enduring material for a maximum of 1 AMA PRA Category 1
Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the
activity.
Working with pharmacists on a diabetes care team
• When: Available on demand through February 3, 2022.
• Watch webinar (once you register, recording will start automatically and cannot be paused):
https://attendee.gotowebinar.com/register/4590282230752581644
• Audience: Primary care physicians, specialty physicians, physician assistants, nurse practitioners, pharmacists
• After this one-hour presentation, participants will be able to:
1) Review CCO diabetes HbA1c poor control metric specifications
2) Explain what controlling diabetes means and why it is important
3) Name barriers to good glucose control
4) Identify ways for clinic and pharmaceutical staff to partner
5) Describe standards of care for adults with diabetes
6) Share strategies for breaking through drug regimen inertia
Patient education and engagement in diabetes care
• When: Available on demand through June 30, 2022
• Watch webinar (once you register, recording will start automatically and cannot be paused):
https://attendee.gotowebinar.com/register/3442121612601905932
• Audience: Primary care physicians, specialty physicians, physician assistants, nurse practitioners, pharmacists
• After this one-hour recorded presentation, participants will be able to:
1) Review CCO diabetes HbA1c poor control metric specifications
2) Explain what controlling diabetes means and why it is important
3) Name barriers to good glucose control
4) Identify the clinic’s role in lifestyle interventions
5) Understand how to promote diabetes education with your patients
6) Name current standards of care for your patients with diabetes
Questions? Please contact Sarah Wetherson ([email protected])
December 2020 QHOC Meeting Packet Page 3 of 44
Kindergarten readiness
Marketing toolkit for promoting kindergarten readiness incentive measures
Based on CCO feedback in prior needs assessments, Brink Communications developed marketing assets for CCOs to use
for promoting well-child (including childhood immunizations) and preventive dental visits. Our goal has been to create a
set of tools that all CCOs can easily use to reach out to members and encourage them to make these important
appointments for their children. The materials include a brochure, social media assets, advertising assets and more. All
materials are available in English and Spanish.
Marketing assets and an introductory webinar are available here: https://www.oregon.gov/oha/HPA/dsi-
tc/Pages/kindergarten-readiness.aspx
Screening, brief intervention and referral to treatment (SBIRT)
TA for clinics: addressing the increased prevalence of unhealthy alcohol (SBIRT) and opioid use
What: The OHA Transformation Center is partnering with the Oregon Rural Practice-based Research Network (ORPRN)
to support clinic technical assistance related to SBIRT for unhealthy alcohol and drug use. SBIRT is a “must-pass”
incentive measure for CCOs in 2021.
This collaborative project, ANTECEDENT, can provide primary care clinics with 12 months of tailored support to
implement changes to address unhealthy alcohol use at no-cost to the participating clinics. Additionally, ORPRN is
offering a complementary technical assistance opportunity regarding chronic pain management and opioid prescribing
(aka PINPOINT).
See flier: https://www.oregon.gov/oha/HPA/dsi-tc/Documents/ORPRN-SBIRT-Antecedent-Pinpoint.pdf.
Audience: Clinics across Oregon are invited to participate in these free technical assistance opportunities.
Questions? Contact Alissa Robbins ([email protected]) or contact the program directly at
Tobacco cessation
Free, quick online tobacco cessation counseling training to address higher COVID-19 risk for cigarette smokers
(with CME)
What: With cigarette smokers at higher risk for COVID-19, this short online course will improve your care team’s ability
to help patients quit tobacco. The course focuses on brief tobacco intervention and motivational interviewing
techniques.
Who: All members of the care team committed to supporting their patients to quit tobacco.
When: The course is self-paced and takes approximately 45 minutes. The course can be started, paused and resumed
later as needed.
CMEs: This training has been reviewed and is accepted for up to 1.0 prescribed credit from the American Academy of
Family Physicians (AAFP). For other licensing boards that may not pre-approve continuing education credits (for
example, the Board of Licensed Professional Counselors and Therapists), please submit the certificate of participation to
your accrediting body.
Access the training: https://tcrc.rapidlearner.com/3462253711
December 2020 QHOC Meeting Packet Page 4 of 44
Additional brief intervention training webinar: Available from the American Lung Association (ALA) with free continuing
education through the American Association of Nurse Practitioners, American Association of Respiratory Care, American
Association of Medical Assistants, and National Commission for Health Education Credentialing. The ALA’sr Ask, Advise,
Refer to Quit Don’t Switch training focuses on supporting quit efforts without switching to electronic nicotine device
systems. Access the recorded webinar here through December 31, 2020: https://quitdontswitchtraining.lung.org/
Questions? Contact Anona Gund ([email protected] or 503-750-3292)
Multiple metrics (non-Transformation Center TA)
TA for clinics: Chronic disease prevention and management webinar series + individual clinic TA
What: Primary care clinics are invited to participate in a no-cost Oregon Rural Practice-based Research Network (ORPRN)
project to support chronic disease prevention and management sponsored by the Oregon Health Authority. This series
will include six tailored webinars involving instruction from subject matter experts, facilitated discussion with other
participants, and quality improvement training related to hypertension, diabetes, arthritis, and tobacco cessation. All
practices are also eligible to participate in up to six hours of 1-on-1 technical assistance with a practice enhancement
research coordinator throughout the series.
When: Registration is open on a rolling basis. Webinars are held fall 2020–winter 2021.
Who: Up to 50 Oregon primary care practices
Register your practice here: https://ohsu.ca1.qualtrics.com/jfe/form/SV_e4pfQD6s6uQkVrD
Contact: [email protected]
Non-metrics TA
Community advisory councils
Updated CAC 101 presentation
The Transformation Center has recorded an updated version of the CAC 101 presentation that includes CAC
requirements established through CCO 2.0. This is an update to a presentation that was originally recorded in 2015. This
presentation is for new and existing CAC members, with the goal of providing an overview of CAC member roles and
responsibilities.
Link to presentation: https://www.oregon.gov/oha/HPA/dsi-tc/Documents/CAC%20101-final%20presentation.zip
Instructions: Download the zip file to access the PPT presentation. The PPT slides include narration. To enable narration,
click on Slide Show>Play Narrations. There are a few videos in the presentation that will also need to be started
manually.
Contact: Tom Cogswell ([email protected])
Learning collaborative: CAC members serving on CCO governing boards
The Transformation Center is convening a new learning collaborative for CAC members serving on CCO governing
boards. This peer-to-peer learning network is in support of the CCO 2.0 requirement that CCOs identify two CAC
members (at least one being a consumer) to serve on their CCO governing boards. The first meeting will take place on
December 7, 2–3:30 p.m. The group will meet five times between December 2020 and May 2021. Eligible CAC members
can contact Tom Cogswell to participate ([email protected]).
December 2020 QHOC Meeting Packet Page 5 of 44
Health-related services (HRS)
Health-related services technical assistance now available
As the Transformation Center’s contracted consultants, OHSU’s ORPRN team will soon begin providing health-related
services technical assistance to CCOs. In the coming weeks, ORPRN staff will be reaching out to CCOs to assess their HRS
TA needs. Technical assistance will be available through spring 2021.
Contact: Anona Gund ([email protected]) or Anne King ([email protected])
Health-related services webinar recording: Community benefit initiatives
What: The Transformation Center invites CCOs and their contracted providers and organizations to watch a recorded
webinar on health-related services (HRS) community benefit initiatives (CBIs). HRS CBIs are community-level
interventions supported by CCOs that are focused on improving population health and health care quality. A media
campaign to increase immunization rates is an example of a CCO CBI investment. Topics include:
• What CBIs are and how are they reported
• Common CBI investments by CCOs, and their potential impact
• Ways to align CBIs with other CCO and community priorities
• Snapshots of promising CCO CBI programs
Who: CCO staff, contracted providers, and organizations wishing to better understand how CBIs can be used to improve
population health
Watch recording: https://us02web.zoom.us/rec/share/rSG_oN6h_hOjXDZrnX8tcvD1wR5eyK-
7FWGCCiI2GslY6wPERC6hkeSiNherfXeX.JTBEjVIrxg8wu2rh?startTime=1605728126000
View slides: https://www.oregon.gov/oha/HPA/dsi-tc/Documents/HRS-CBI-101-Webinar-10-18-2020.pdf
REALD
REALD learning series for CCOs, clinics and hospitals
The OHA Transformation Center and Division of Equity & Inclusion hosted a learning series focused on the use of REALD
(race, ethnicity, language and disability) for CCOs, clinics and hospitals. REALD is an effort to increase and standardize
race, ethnicity, language and disability data collection across DHS and OHA. The series covers an introduction to REALD,
impact on health equity work, strategies for asking REALD questions, and using REALD data to advance health equity.
Recordings are available here: https://www.oregon.gov/oha/HPA/dsi-tc/Pages/Health-Equity.aspx
• An introduction to REALD
• Implementing new REALD data collection for providers
• Implementing REALD for providers: updates and FAQs
• Strategies for asking REALD questions
• Using REALD data to advance health equity
Audience: CCOs and clinics.
Contacts: Tom Cogswell ([email protected], 971-304-9642) or Marjorie McGee
December 2020 QHOC Meeting Packet Page 6 of 44
Transformation and quality strategy
2021 TQS guidance documents available
Updated 2021 TQS guidance documents were posted October 1, including an updated template, guidance document,
FAQs and scoring criteria (new this year): https://www.oregon.gov/oha/HPA/dsi-tc/Pages/Transformation-Quality-
Strategy-Tech-Assist.aspx
2021 TQS webinars and office hours
CCO staff are invited to participate in technical assistance for developing the 2021 Transformation and Quality Strategy
(TQS). Component-specific webinars will cover expectations, rationale and scoring criteria and include lots of time for
Q&A with OHA subject matter experts. For full webinar and office hours details, see this 2021 TQS webinar flier:
https://www.oregon.gov/oha/HPA/dsi-tc/Documents/2021-TQS-technical-assistance-schedule.pdf
Recordings are available here: https://www.oregon.gov/oha/HPA/dsi-tc/Pages/Transformation-Quality-Strategy-Tech-
Assist.aspx
• 2021 overview: updates and global feedback webinar
• Social determinants of health and equity webinar/office hours*
• Special health care needs webinar/office hours*
• Health equity and CLAS standards webinar/office hours*
Upcoming webinars:
• Severe and persistent mental illness webinar/office hours* o New date: Dec. 15, Noon-1 p.m.
• Access webinar/office hours* o New date: Feb. 1, 12:30-1:30 p.m.
• Additional general office hours are scheduled for January, February and March *All component-specific sessions and office hours will use the same GoToMeeting details (no registration needed):
• Join meeting: https://www.gotomeet.me/OHATransformationCenter/2021-tqs-ta
• Phone option: 1-646-749-3122
• Access code: 848-146-317
Transformation Center technical assistance updates For updates, sign up for the Transformation Center's events, resources and learning opportunities distribution list.
December 2020 QHOC Meeting Packet Page 7 of 44
MINUTES
HEALTH EVIDENCE REVIEW COMMISSION Virtual meeting
November 12, 2020 Members Present: Kevin Olson, MD, Chair; Holly Jo Hodges, MD, MBA, Vice-Chair; Leda Garside, RN, MBA; Gary Allen, DMD; Devan Kansagara, MD; Lynnea Lindsey, PhD; Leslie Sutton (arrived at 1:50 pm); Adriane Irwin, PharmD; Kathryn Schabel, MD; Max Kaiser, DO; Mike Collins; Deborah Espesete, LAc, MAcOM, MPH, DiplOM. Members Absent: Michael Adler, MD. Staff present: Ariel Smits, MD, MPH; Jason Gingerich; Liz Walker, PhD, MPH; Daphne Peck. Also Attending: Dawn Mautner, MD, MS & Dianne Quiring (Oregon Health Authority); Koa Kai; Renee Doan; Amara M, Ashely Svenson; Devki Nagar; Hannah Baer; Jeanne McLaws; Katy McDowell; Kellie Skenandore; Lisa Sumerlin; Rika (no last name); Wendy Sinclair; Karen Heller; Rodica; Steven Hix; Charice & Q; Mareinna (Shawn) Kangiser.
Call to Order Kevin Olson, Chair of the Health Evidence Review Commission (HERC), called the meeting to order; roll was called. A quorum of members was present at the meeting.
Minutes Approval MOTION: To approve the minutes of the 10/1/2020 meeting as presented. CARRIES 11-0. (Absent: Sutton)
Director’s Report COVID-19 updates Jason Gingerich reported that COVID-19 coding and telehealth related changes are ongoing. Coverage Guidance updates Gingerich said the December Evidence-based Guidelines Subcommittee (EbGS) meeting was cancelled. Staff are soliciting topics. One potential new topic, Expanded Carrier Screening, was identified today at the Value-based Benefits Subcommittee (VbBS) meeting. Membership updates Gingerich said, with Leda Garside’s departure, there is a potential replacement for the public health nurse role on the Commission. A new person will hopefully be appointed soon. He thanked Garside for
December 2020 QHOC Meeting Packet Page 8 of 44
all her work on the Commission for the past eight years. She expressed gratitude for the experience. Garside will remain on EbGS for the time being.
Value-based Benefits Subcommittee (VbBS) Report on Prioritized List Changes Meeting materials pages 56-120 Ariel Smits reported the VbBS met earlier in the day, 11/12/2020. She summarized the subcommittee’s recommendations. She asked Commissioners to contact her with any 2022 biennial review topics they may have. Biennial review topics generally involve either moving a line up or down the List or might impact costs. The two topics she has identified currently are 1) expansion of coverage for inguinal hernias and 2) creating a separate line for uterine polyps. Smits also reviewed the items that were reviewed by Leadership or advisory panels but not recommended for change:
• No change to Cologuard noncoverage • No change to sphenopalatine ganglion blocks for treatment of migraine • No recommendation for cone beam CT coverage expansion • No change to current coverage/guideline regarding whole exome sequencing • No change recommended to the lack of coverage for ICD10 F43.9 (Reaction to severe stress,
unspecified) as many more specific diagnoses exist • No change recommended for including HCPCS H0031 on the Diagnostic Procedures file
There was no discussion. Smits said between the VbBS and HERC meetings today, new COVID-19 codes were discovered. Recommendation to add the following codes to line 3 PREVENTION SERVICES WITH EVIDENCE OF EFFECTIVENESS:
• 91300 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted, for intramuscular use
• 91301 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage, for intramuscular use
• 0001A Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted; first dose
• 0002A Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted; second dose
• 0011A Immunization administration by intramuscular injection of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage; first dose
December 2020 QHOC Meeting Packet Page 9 of 44
• 0012A Immunization administration by intramuscular injection of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage; second dose
RECOMMENDED CODE MOVEMENT (changes to the 1/1/2021 Prioritized List unless otherwise noted) • Add new COVID testing codes to the Diagnostic Procedure File • Place the 2021 CDT codes on various lines and files • Finalize the placement of the 2021 CPT codes • Add an unspecified developmental code to three covered lines to allow therapy for young children
at risk of developmental delays • Make several straightforward coding changes RECOMMENDED GUIDELINE CHANGES (changes to the 1/1/2021 Prioritized List unless otherwise
noted) • Add a new guideline regarding nerve allografts to a funded line • Update the COVID testing guideline to allow antibody testing for patients undergoing evaluation for
multi-system inflammatory syndrome in adults (MIS-A) • Add a new guideline regarding dental implant removal • Delete the guideline regarding dental amalgam use • Edit the prenatal genetic testing guideline to allow non-invasive prenatal screening (NIPS) testing for
all pregnancies and correct CPT code errors • Edit the hereditary cancer genetic testing guideline to update the NCCN guideline references • Make minor changes to the neuropsychological testing guideline and the cognitive testing guideline • Revise the guideline for repetitive transcranial magnetic stimulation • Add a new guideline regarding coding related to developmental delays, including children at risk of
developmental delays • Substantially edit the guideline for opioids for conditions of the back and spine Expanded Carrier Screening is being considered as a possible coverage guidance topic through the EbGS. Olson asked the Commission if anyone had thoughts about the plan to explore this topic as a coverage guidance. There was no discussion. Smits said there were changes to Guideline Note 60 from the meeting materials, in particular language changed from “must” to “should” to account for patients who are unable to take part in the types of therapies described. Public testimony
Devki Nagar testified about Expanded Carrier Screening (ECS). Ms. Nagar is a Myriad Genetic’s genetic counselor and was otherwise silent on conflicts of interest. She applauded the Commission for continuing to review this topic. She feels that ECS provides equity across ethnicities. Ms. Nagar said there are a wide range of panels, including panels with 15 genes or more. Some labs are publishing data stating that their tests align with American College of Obstetricians and Gynecologists (ACOG) recommendations. ACOG supports this approach so that patients have a choice which would align with their values and preferences. Based on the information, patients are making appropriate changes for their current or future pregnancies.
December 2020 QHOC Meeting Packet Page 10 of 44
Guideline Note 60 Koa Kai from the Chronic Disease Coalition stated no conflicts of interest. Ms. Kai lauded the changes to Guideline Note 60 (GN 60). She said it is imperative to provide options for pain relief and patient safeguards from harm. She said one of the misperceptions HERC seems to have is that GN 60 is merely a guideline but in the past, this policy has been aggressively implemented without regard to patient safety. It is imperative to recognize the patient harms caused by the unintended consequences from the history of GN 60 and to recognize the organization’s responsibility to remedy the resulting harms from forced tapers and denials of pain medication. It is also important to recognize the damage this policy has done to the doctor-patient relationship. She urged HERC to make small changes and evaluate the outcomes and adjusting policies based on those assessments in a timely manner. There are other issues from the creation of GN 60 which must be acknowledged including one multi-committee member’s excessive participation in the policy’s conception authorship, voting, promotion and subsequent review participation. The additional destruction of the taskforces public records and the various taskforce member’s undisclosed conflicts of interest has allowed for a lack of public transparency and consideration of public input in the creation of public health policy. Wendy Sinclair, founder of the Oregon Pain Action Group, declared no conflicts of interest. Ms. Sinclair said she appreciated the proposed changes to Guideline Note 60. She has been involved with this issue for some time. She said people have reached out to her to share that they have been taken off their medication and are contemplating suicide as they try to cope with pain as they are unable to manage. Guideline Note 60 has caused a lot of harm to people. She said she was able to read letters given to doctors stating that opioids are not safe or effective for back pain, so you need to taper your patient. This has caused entire clinics to eliminate opioids for back pain for all Medicaid patients, sending patients into turmoil. She said she appreciates the language has changed but she is concerned that this new language will not get the same level of promotion as the taper-language notice did. She would like to see providers notified of these changes. Steven Hix testified; he declared no conflicts of interest. Mr. Hix said he is a pain patient and an advocate for pain patients. He thanked the Commission for hearing the concerns brought forward about GN 60. He asked if he would now get his medication paid for a whole month rather than seven days. He said he agreed with the first two speakers about the damage that has been done with the implementation of the original GN 60 and there is a lot of repair work that needs to be done.
Smits said there is nothing in the proposed revised guideline note that precludes writing a longer prescription for opioid medication. However, the Commission is not involved in the mechanics of how the CCOs administer medication plans. There may be prior authorization criteria in place that would limit prescriptions to 7 days. Mr. Hicks was advised to contact the OHA Ombuds office or his CCO care coordinator for assistance, as the Commission is not equipped to address individual cases.
Amara M, a mother, advocate for human rights and co-founder of the Oregon Pain Action Group testified. Ms. M. declared no conflicts of interest. She commended HERC for making significant positive changes to GN 60. She said she hopes the gravity of the effect the policy has had on patients is looked into further. She said she was a patient at a clinic when GN 60 was first enforced. All Medicaid patients with back conditions, regardless of severity, were handed a letter to inform them
December 2020 QHOC Meeting Packet Page 11 of 44
that patients would be force-tapered off their opioid medication in six weeks. Amara said her regular doctor at the clinic decided to retire rather than be instructed to go against her Hippocratic Oath. She said she had many meetings with the new clinic director and that led her to the underlying guideline note that caused the forced tapers. She then started attending meetings. She said she would like to see promotion and clarity of the new language given to the CCOs. EOCCO has force-taper language live on their website right now. She said an analysis of the Health Authority’s ombuds program said that the volume and acuity of client calls from pain conditions significantly increased in the last two years, more than doubled. The number one concern is continuity of care for pain management.
MOTION: To accept the VbBS recommendations on Prioritized List changes as stated. See the VbBS minutes of 11-12-2020 for a full description. Carries: 12-0. MOTION: To accept the new COVID-19 vaccine codes recommendations as stated. Carries: 12-0.
Public Comment
Mareinna (Shawn) Kangiser offered comments about facial feminization surgery (FFS). Ms. Kangiser said she wanted to talk about changing facial feminization surgery from a cosmetic procedure to a medical necessity. Ms. Kangiser said that gender reassignment surgery (GRS) changes a person’s relationship to their body and affects interactions with one’s partner but argued that one’s face is how a person is identified in society. She said that make up is cosmetic, meant to improve one’s appearance, but FFS is meant to feminize one’s appearance, not to make one more attractive. Part of the diagnostic criteria for gender dysphoria is the desire to live and be accepted as a member of the gender they identify as; the inability to achieve this can cause significant distress. That distress is why it's being treated, because of this need to be accepted as one's true gender. Part of treating gender dysphoria means helping one be accepted as their true gender. FFS is protective against violence and discrimination. Violence is often the result of being “visibly gender non-conforming,” which has been found to elicit anti-transgender bias. She said when a trans woman has an appearance that conforms to the typical conceptions of gender, it serves as protection from violence and discrimination, and by extension reduces their risk of depression and suicide. The high rates of suicide in transgender people is largely due to their treatment by society. She said this treatment is even cost effective. California did an economic-impact analysis and found that removing transgender exclusions had an immaterial effect on premium costs, which were far exceeded by the benefits. Those benefits include improved health outcomes among transgender people such as reduced suicide risk, lower rates of substance use and increased adherence to HIV treatment. She said a recent study estimated that without the transition surgeries (a one-time cost) healthcare for a transgender person is, on average, $10,712 a year. Therefore, FFS is a cost-effective intervention, and it needs to be covered by insurance policies. She said the fact that GRS is covered and FFS is not shows that gender dysphoria and its implications are not being well understood by insurance companies. Until one is accepted in society as their true gender, something necessary to function in our current American society, gender dysphoria will persist, and procedures such as FFS will still be medically necessary as a potential treatment of gender dysphoria.
December 2020 QHOC Meeting Packet Page 12 of 44
Smits said HERC will look at this issue when the World Professional Association for Transgender Health (WPATH) releases its updated guidelines. Ms. Kangiser asked to be contacted when the issue is up for review. Gingerich said we can make that happen. Ms. Kangiser said OHSU has a billing issue and she cannot be seen. She was advised to contact the OHA Ombuds office or her CCO care coordinator for assistance.
Adjournment Meeting adjourned at 3:00 pm. Next meeting will be from 1:30-4:30 pm on Thursday, 1/21/2021 virtually.
December 2020 QHOC Meeting Packet Page 13 of 44
Value-based Benefits Subcommittee Recommendations Summary For Presentation to:
Health Evidence Review Commission on November 12, 2020
For specific coding recommendations and guideline wording, please see the text of the 11/12/2020 VbBS minutes.
RECOMMENDED CODE MOVEMENT (changes to the 1/1/2021 Prioritized List unless otherwise noted) • Add new COVID testing codes to the Diagnostic Procedure File • Place the 2021 CDT codes on various lines and files • Finalize the placement of the 2021 CPT codes • Add an unspecified developmental code to three covered lines to allow therapy for young children
at risk of developmental delays • Make several straightforward coding changes ITEMS CONSIDERED BUT NO RECOMMENDATIONS FOR CHANGES MADE • Home intraocular pressure monitoring was not added to the glaucoma line RECOMMENDED GUIDELINE CHANGES (changes to the 1/1/2021 Prioritized List unless otherwise
noted) • Add a new guideline regarding nerve allografts to a funded line • Update the COVID testing guideline to allow antibody testing for patients undergoing evaluation for
multi-system inflammatory syndrome in adults (MIS-A) • Add a new guideline regarding dental implant removal • Delete the guideline regarding dental amalgam use • Edit the prenatal genetic testing guideline to allow non-invasive prenatal screening (NIPS) testing for
all pregnancies and correct CPT code errors • Edit the hereditary cancer genetic testing guideline to update the NCCN guideline references • Make minor changes to the neuropsychological testing guideline and the cognitive testing guideline • Revise the guideline for repetitive transcranial magnetic stimulation • Add a new guideline regarding coding related to developmental delays, including children at risk of
developmental delays • Substantially edit the guideline for opioids for conditions of the back and spine
December 2020 QHOC Meeting Packet Page 14 of 44
VALUE-BASED BENEFITS SUBCOMMITTEE Virtual Meeting
November 12, 2020 9:00 AM – 1:00 PM
Members Present: Kevin Olson, MD, Chair; Holly Jo Hodges, MD, MBA, Vice-chair; Gary Allen, DMD; Kathryn Schabel, MD; Brian Duty, MD; Adriane Irwin, PharmD; Regina Dehen, ND, Lac. Members Absent: Mike Collins. Staff Present: Ariel Smits, MD, MPH; Jason Gingerich; Liz Walker, PhD, MPH; Daphne Peck. Also Attending: Dawn Mautner MD MPH, Diane Quiring and Kellie Skenandore (OHA); Amara M; An Do; DeAnn (no last name); Devki Saraiya and Ashley Svenson (Myriad Genetics); Eric Owens; Karen Heller; Kim Martin; Koa Kai; Manu Chaudhry; Rashelle Kukuk; Robin (no last name); Stacey (no last name); Taryn Couture; Tracy Futch; Vanessa Nitibhon (Integrated Genetics); Hannah Proffitt-Allee; Jenn O’Neill; Rika (no last name); Anne Fuqua; Hannah Baer (Coalition for Access to Prenatal Screening); Nidhi Maheshwari; Dana Peterson; Robert Slotnick MD; Jeanne McLaws; Katy McDowell; Peggy Tighe; Tedra Stuart; Kareem Shafi; Wendy Sinclair; Mareinna/Shawn Kangiser. Roll Call/Minutes Approval/Staff Report
The meeting was called to order at 9:00 am and roll was called. A quorum of members was present at the meeting. Minutes from the 10/1/2020 VbBS meeting were reviewed and approved. Smits noted the errata document; there was no discussion. She also reviewed the items not recommended for change in consultation with leadership or advisory panels. There was also no discussion on these items. Smits then brought up the upcoming 2022 biennial review. The two topics to date that staff are working on are 1) expansion of coverage for inguinal hernias, and 2) creating a separate line for uterine polyps. She invited members to send staff suggestions for other topics.
December 2020 QHOC Meeting Packet Page 15 of 44
Topic: Straightforward/Consent Agenda Discussion: There was no discussion about the consent agenda items. Recommended Actions: 1) Add 11981-11983 (Insertion/removal/removal with reinsertion, non-biodegradable drug
delivery implant) to line 312 GENDER DYSPHORIA/TRANSEXUALISM 2) Add 26480 and 26483 (Transfer or transplant of tendon, carpometacarpal area or dorsum of
hand; without/with free graft, each tendon) to line 356 RHEUMATOID ARTHRITIS, OSTEOARTHRITIS, OSTEOCHONDRITIS DISSECANS, AND ASEPTIC NECROSIS OF BONE
3) Add CPT 64912-64913 (Nerve repair; with nerve allograft) to line 536 PERIPHERAL NERVE DISORDERS
4) Modify GN173 INTERVENTIONS THAT ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS FOR CERTAIN CONDITIONS as shown in Appendix A
5) Add a new guideline regarding nerve allographs as shown in Appendix B
MOTION: To approve the recommendations stated in the consent agenda. CARRIES 7-0.
Topic: COVID-19 Updates Discussion: There was no discussion about the new COVID-19 CPT codes or the testing guideline modification. Note: Additional new CPT codes were identified after the VbBS meeting and placements were approved at the afternoon HERC meeting. Recommended Actions: 1) Modify Diagnostic Guideline D27 SARS-COV-2 (COVID-19) TESTING as shown in Appendix A 2) Advise HSD to place CPT 87636 (Infectious agent detection by nucleic acid (DNA or RNA); severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) and influenza virus types A and B, multiplex amplified probe technique), 87637 (Infectious agent detection by nucleic acid (DNA or RNA); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), influenza virus types A and B, and respiratory syncytial virus, multiplex amplified probe technique) and 87811 (Infectious agent antigen detection by immunoassay with direct optical (ie, visual) observation; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19])) to the DIAGNOSTIC PROCEDURES file
Note: In the afternoon, the Health Evidence Review Commission (HERC) added the following codes to line 3 PREVENTION SERVICES WITH EVIDENCE OF EFFECTIVENESS: 1) 91300 (Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease
[COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted, for intramuscular use)
2) 91301 (Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage, for intramuscular use)
December 2020 QHOC Meeting Packet Page 16 of 44
3) 0001A (Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted; first dose)
4) 0002A (Immunization administration by intramuscular injection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 30 mcg/0.3mL dosage, diluent reconstituted; second dose)
5) 0011A (Immunization administration by intramuscular injection of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage; first dose)
6) 0012A (Immunization administration by intramuscular injection of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]) vaccine, mRNA-LNP, spike protein, preservative free, 100 mcg/0.5mL dosage; second dose)
MOTION: To recommend the code and guideline note changes as presented. CARRIES 7-0.
Topic: Oral Health Advisory Panel Report Discussion: A. 2021 CDT code placement: There was no discussion on code placement B. Straightforward CDT code changes: There was no discussion on this topic C. Dental implant removal guideline: Allen noted that this guideline will be helpful for the Dental
Care Organizations (DCOs.) D. Mercury containing amalgam: There was no discussion on this topic Recommended Actions: 1) 2021 CDT code placement as shown in Appendix D 2) GN139 FRENOTOMY FOR TONGUE TIE IN NEWBORNS was modified as shown in Appendix A 3) Add D0320 (Temporomandibular joint arthrogram, including injection) to line 643 TMJ
DISORDERS a. Advise HSD to remove D0320 from the DIAGNOSTIC PROCEDURES file
4) Add D0321 (Other temporomandibular joint radiographic images, by report) to line 643 TMJ DISORDERS
a. Advise HSD to remove D0321 from the DIAGNOSTIC PROCEDURES file 5) A new guideline regarding implant removal was adopted as shown in appendix B 6) GN123 DENTAL FILLINGS FOR POSTERIOR TEETH was deleted as shown in Appendix A
MOTION: To recommend the code and guideline note changes as presented. CARRIES 7-0.
Topic: Genetic Advisory Panel Report Discussion: A. Genetic 2021 CPT code placement: There was no discussion
B. Prenatal genetic testing guideline
a. Update to aneuploidy testing CPT codes: There was no discussion.
December 2020 QHOC Meeting Packet Page 17 of 44
b. Non-invasive prenatal screening for aneuploidies (NIPS): Smits introduced the topic. Schabel stressed the importance of reduced amniocentesis rates with this technology. She asked about comparative costs of different screening strategies and staff provided estimates.
Testimony: 1. Hannah Baer: Coalition for Access to Prenatal Screening (CAPS) representative. CAPS is a group
sponsored by seven genetic testing companies. Ms. Baer testified that NIPS is a sensitive and specific screening tool that should be offered to all pregnant women. In 2020, Washington and Idaho Medicaid programs added NIPS for average-risk pregnancies. Other states’ Medicaid program, such as Alaska and Delaware, changed their policy to cover NIPS for all pregnant women (CPTs 81420 and 81507). Additionally, Connecticut and Wisconsin made changes in their Medicaid policy based on Practice Bulletin 226 by the American College of Obstetricians and Gynecologists (ACOG, August 2020). Many private insurers cover NIPS testing for average-risk pregnancies. Six other state Medicaid programs (Iowa, Massachusetts, Louisiana, Maryland, Nevada and Texas) are considering coverage for NIPS. Ms. Baer said these tests should be covered for all women regardless of age or risk.
2. Vanessa Nitibhon: Ms. Nitibhon is a certified genetic counselor employed by and speaking on behalf of Integrated Genetics. She was formerly a genetic counselor at OHSU. She testified that NIPS coverage ensured the most equitable care for all pregnant women. ACOG and SMFM support NIPS testing for all women per ACOG’s Practice Bulletin 226. NIPS screening has the lowest chance for error and has the best detection rate for the common aneuploidies. Fewer false positive results means fewer invasive procedures. Ms. Nitibhon cited a paper by Norton (2015) which stated that the false positive rate is 100 times lower than standard serum screening. A reduction in false positive rates also reduces anxiety as well as complications from invasive testing. Ms. Nitibhon shared scenarios she encountered when counseling average-risk women in her practice, stating that those commercially-insured patients who had access to NIPS had more timely results than her Medicaid patients, leading to a division of care based on insurance coverage. Covering NIPS can also allow patients and families prepare for the arrival of a special needs baby. This test is more equitable, and, in rural areas, easier to access than fetal nuchal lucency ultrasound.
3. Ashley Svenson: Ms. Svenson is a policy specialist employed by Myriad Genetics. She was formerly a genetic counselor practicing at a large academic perinatology clinic. Ms. Svenson cited cost-effectiveness modeling studies that demonstrated NIPS as net cost effective when additional costs are taken into account such as increased number of ultrasounds, consults, amniocenteses, etc. Svenson stated that NIPS is also easier for women with low medical literacy or resource constraints, underscoring the anxiety and emotional burden of a positive screening test. Svenson read a patient quote from “Stand Up for Accurate Prenatal Answers,” a patient group. The patient quote recounted a women’s second trimester of pregnancy while waiting for a diagnostic test result from a positive 20-week ultrasound. Ms. Svenson cited her own clinical experience stating that false positive results after traditional serum screening were common. Svenson concluded by citing an article from the “Healthy African American Families” patient group, who stated that disparities in coverage lead to racial disparities in aneuploidy screening, with women of color disproportionately not being screened. Svenson stated that non-white women are significantly less likely to pursue NIPS when coverage is unclear.
4. Kim Martin: Dr. Martin is an obstetrician-gynecologist and board-certified clinical geneticist. She is also a consultant to a genetics testing company but states she is not being reimbursed for her testimony today. Dr. Martin stated that the introduction of cell-free DNA in 2012 should have
December 2020 QHOC Meeting Packet Page 18 of 44
revolutionized aneuploidy screening for all women regardless of age or risk given the dramatically improved performance of the screen as well as the ability to perform it early in pregnancy. This test can be performed in the office during a routine OB visit. This is in contrast to the second most sensitive test, which is the nuchal translucency ultrasound, which requires a certified nuchal translucency provider. Oregon has 22 of these certified providers in Oregon, but the vast majority are not in rural areas. Martin states this disadvantages woman living in rural areas. Martin also states that over 80% of Asian and Caucasian women enter prenatal care in first trimester of pregnancy compared to <70% of women of color, leaving women of color with less access to tests like fetal nuchal lucency screening that need to be performed early in pregnancy. Another test, the quad screen, has poor accuracy if the dating is poor for the pregnancy. Martin stated that about 10% of women get poorly dated. NIPS is better for uncertain dates, as its results are independent of gestational age.
5. Nathan Slotnick: He is a medical geneticist and high-risk obstetrician, practicing in Nevada. Dr. Slotnick spoke about his clinical experience. He cited Norton’s 2015 study that NIPS has a higher positive predictive value and a high negative predictive value. If the test is negative, the chance that the result is wrong is near zero, which makes this a powerful screening tool. Slotnick says that the question of screening then becomes a question of justice and equity. He noted the equity issue with limited access in rural areas.
There was little additional discussion. The VBBS members present voted unanimously to expand NIPS coverage to all pregnant women.
c. Expanded carrier testing: Smits introduced the topic. Duty expressed concern about the
high rate of positive results, and the consequences of trying to interpret these. Irwin noted that the proposed guideline might be hard to operationalize for the CCOs. She felt that the VBBS needed to know cost comparisons. Hodges agreed that it might be hard for CCOs to operationalize. She requested adding the CPT code (81443) to the guideline for clarity. Hodges was also concerned with the proposed guideline wording. How were reviewers supposed to verify genetic counseling is ordered or obtained? Should the CPT 81443 only be submitted with genetic counseling codes?
Testimony:
1. Devki Nagar: Nagar is a genetic counselor, employed by and representing Myriad Genetic Laboratories. She supports the staff and GAP recommendation to add coverage. She feels that expanded carrier screening (ECS) provides equity across ethnicities. A Blue Cross Blue Shield TEC review recently found that ECS improved net health outcomes. The test might also reduce barriers to care. She agrees with adding the CPT code 81443 to the guideline to allow for consistency of adoption. She said that only clinically meaningful variants and those that are pathogenic are reported by labs (variants of uncertain significance are not reported), given that these test results can potentially be used to make pregnancy-related decisions. Ms. Nagar stated that different companies offer different panels which vary in the number of included genes. She feels that pretest education is important, but limiting access to testing to patients seeing genetic counselors is problematic given the time sensitivity of carrier screening during pregnancy and limited availability of genetic counselors. Currently, the other screenings allowed in the prenatal genetic testing guideline do not require genetic counseling (CF, SMA, etc.) Thus, this could reintroduce inequity in care by requiring genetic counseling for this one particular type of test. ACOG endorses ECS in Committee Opinion 690 as an appropriate option given the diversity of
December 2020 QHOC Meeting Packet Page 19 of 44
Americans. She requested that the proposed guideline be changed to allow prenatal care providers to be able to order test or include components of informed consent in the guideline.
2. Kim Martin: Dr. Martin is an OB-Gyn who consults for a genetic testing company. Martin said
that professional societies have recommendations regarding ECS coverage. She noted that the increasing diversity of the US population makes ethnicity-based testing more problematic given two societal changes: 1) individuals partnering with those of different ethnicities, and 2) individuals cannot or do not accurately report their ancestry, as defined by the ethnicity of the individual’s four biological grandparents. Pan-ethnic expanded carrier screening results in identifying more at-risk couples, who are commonly missed. Martin concludes that professional societies have not acknowledged X-linked disorders (such as Fragile X), which should be included in pan-ethnic panels, as carriers of these disorders are at increased risk of premature ovarian failure, cardiomyopathies, and arrythmias, among other conditions.
Olson questioned requiring pretest genetic counseling before this test. Genetic counseling is a rare resource; specialty societies expect counseling to take place in the maternity care provider office. Duty was concerned that there were a lot of genes tested, which may result in unintended results, unlike simpler testing like CF screening. Dehen also had concerns about the types of genes included and about the possible lack of coverage for partner testing. Irwin noted that the VBBS had a similar conversation in 2018, with similar concerns brought up. Olson felt that practicing OBs and family doctors should be brought into the conversation to find out what they feel about ECS testing. Schabel echoed this thought, asking if this is actually a test that providers what to offer or that patients are requesting. Duty felt that there should be a content specialist to assist the VBBS in determining coverage for ECS. Schabel and Dehen both expressed concern about the tension between the harm to the couple with lack of knowledge of a gene defect vs the harm of knowledge of a defect of unknown significance. The VBBS decision was to table this topic. HERC staff were directed to get additional input from maternity care providers and content experts. HERC staff will look into putting this topic through the coverage guidance process with EGBS.
C. Hereditary cancer genetic testing guideline updates: There was no discussion Recommended Actions: 1) Add CPT 81351-81353 (TP53 (tumor protein 53) (eg, Li-Fraumeni syndrome) gene analysis) to
the Diagnostic Procedures File 2) Add CPT 81419 (Epilepsy genomic sequence analysis panel, must include analyses for ALDH7A1,
CACNA1A, CDKL5, CHD2, GABRG2, GRIN2A, KCNQ2, MECP2, PCDH19, POLG, PRRT2, SCN1A, SCN1B, SCN2A, SCN8A, SLC2A1, SLC9A6, STXBP1, SYNGAP1, TCF4, TPP1, TSC1, TSC2, and ZEB2) to line 30 EPILEPSY AND FEBRILE CONVULSIONS
3) The prenatal genetic testing guideline was modified as shown in Appendix A 4) Expanded carrier screening was recommended for referral to EGBS as a possible coverage
guidance 5) Diagnostic Guideline D25 HEREDITARY CANCER GENETIC TESTING was modified as shown in
Appendix A
December 2020 QHOC Meeting Packet Page 20 of 44
MOTION: To recommend the code and guideline note changes as modified. CARRIES 7-0.
Topic: Behavioral Health Advisory Panel report Discussion: A. Straightforward code change recommendations: There was no discussion B. Neurobehavioral status exam and neuropsychological testing guideline: There was no discussion C. Cognitive rehabilitation guideline: There was no discussion D. Repetitive transcranial magnetic stimulation: Hodges requested clarification about how often Repetitive Transcranial Magnetic Stimulation (rTMS) should be administered. Staff suggested adding language limiting rTMS therapy to one session per day, which is consistent with the studies supporting effectiveness. Hodges said she had seen requests for multiple sessions per day with different magnet settings; one session would target depression and the other would target obsessive compulsive disorder. Smits said that rTMS is covered only for depression. Recommended Actions: 1) Add H2014 (Skills training and development) to line 4 SUBSTANCE USE DISORDER 2) Remove 96156-96159 (Health and behavior assessment codes) from line 4 SUBSTANCE USE
DISORDER 3) Modify Diagnostic Guideline D26 NEUROBEHAVIORAL STATUS EXAMS AND
NEUROPSYCHOLOGICAL TESTING as shown in Appendix A 4) Remove CPT 97129 and 97130 (Therapeutic interventions that focus on cognitive function) from
lines 201 CHRONIC ORGANIC MENTAL DISORDERS INCLUDING DEMENTIAS, 345 NEUROLOGICAL DYSFUNCTION IN COMMUNICATION CAUSED BY CHRONIC CONDITIONS, and 377 DYSFUNCTION RESULTING IN LOSS OF ABILITY TO MAXIMIZE LEVEL OF INDEPENDENCE IN SELF-DIRECTED CARE CAUSED BY CHRONIC CONDITIONS THAT CAUSE NEUROLOGICAL DYSFUNCTION
5) Add CPT 97129 and 97130 (Therapeutic interventions that focus on cognitive function) to line 294 CANCER OF BRAIN AND NERVOUS SYSTEM
6) Modify GN90 COGNITIVE REHABILITATION as shown in Appendix A 7) Modify GN102 REPETITIVE TRANSCRANIAL MAGNETIC STIMULATION as shown in Appendix A MOTION: To recommend the code and guideline note changes as presented. CARRIES 7-0.
Topic: 2021 CPT code placement Discussion: There was no discussion about placement of the new CPT code 76145 3D rendering with interpretation and reporting of computed tomography, magnetic resonance imaging, ultrasound, or other tomographic modality with image postprocessing under concurrent supervision; not requiring image postprocessing on an independent workstation. Smits reported that the 2021 HCPCS codes have not yet been released. These codes will be reviewed at the January 2021 VBBS meeting. In the meantime, staff will publish recommendations and the Health Systems may make changes to its systems in order to ensure appropriate claims processing.
December 2020 QHOC Meeting Packet Page 21 of 44
Recommended Actions: 1) Advise HSD to place CPT 76145 (Medical physics dose evaluation for radiation exposure that
exceeds institutional review threshold, including report) on the EXCLUDED FILE 2) See all 2021 CPT code placements in Appendix C MOTION: To recommend the code placement as presented. CARRIES 7-0.
Topic: Home intraocular pressure monitoring Discussion: Smits reviewed the summary document. There was no discussion. Recommended Actions: 1) Do not add CPT 99453 [Remote monitoring of physiologic parameter(s) (eg, weight, blood
pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment] to Line 139 GLAUCOMA, OTHER THAN PRIMARY ANGLE-CLOSURE
Topic: Developmental motor delay update
Discussion: Smits reviewed the summary document. There was no discussion. Recommended Actions: 1) Add ICD-10-CM code R62.50 Unspecified lack of expected normal physiological development in
childhood to the three dysfunction lines to enable pairing with physical, occupational, and speech therapy. • 292 NEUROLOGICAL DYSFUNCTION IN POSTURE AND MOVEMENT CAUSED BY CHRONIC
CONDITIONS • 345 NEUROLOGICAL DYSFUNCTION IN COMMUNICATION CAUSED BY CHRONIC CONDITIONS • 377 DYSFUNCTION RESULTING IN LOSS OF ABILITY TO MAXIMIZE LEVEL OF INDEPENDENCE
IN SELF-DIRECTED CARE CAUSED BY CHRONIC CONDITIONS THAT CAUSE NEUROLOGICAL DYSFUNCTION
2) Delete the coding specification from line 292, 345 and 377 o ICD-10-CM R62.0 is included on Lines 292, 345 and 377 for children 8 and under.
3) Delete the following coding specification from lines 292, 345, 377 and 661. o ICD-10-CM F88 is included on these lines for developmental delay. When it is used to
indicate sensory integration disorder or sensory processing disorder, it is included on Line 661.
4) Adopt a new guideline for lines 292, 345, 377 and 661 as shown in Appendix B Note: The meeting materials incorrectly omitted the deletion of the coding specification from line 661 and the attachment of the new guideline note to line 661. MOTION: To recommend the code and guideline note changes as presented. CARRIES 7-0.
Topic: Opioid guideline for conditions of the back and spine
December 2020 QHOC Meeting Packet Page 22 of 44
Discussion: Smits introduced the topic. Olson asked who created the Oregon opioid guidelines referenced in the revised guideline. Smits explained that they were created by a multi-stakeholder group convened by the state.
Testimony: 1. Koa Kai: Ms. Kai is a patient advocate with the Chronic Disease Coalition and declared no conflicts of
interest. She testified that the proposed guideline changes will decrease patient harms. She noted that while integrated care is the gold standard, disabilities can affect a patient’s ability to participate in complementary therapies. The option of alternative and complementary therapies can be beneficial, but making it a requirement may be harmful for the over 170 diagnoses this guideline affects. She recommended changing the section where the guideline had a “must” for having patients participate in alternative care be changed to “providers can consider when clinically appropriate”. She also said that the requirement to take into account “biological, behavioral, psychosocial factors” is confusing. She stated that the requirement for assessment of risk can be discriminatory. Patients with a history of opioid misuse can safely use opioids with close clinical monitoring.
2. Amara M: Ms. M is an advocate and cofounder of the Oregon Pain Action Group and declared no
conflicts of interest. She said that many of the proposed guideline changes are positive. She requested research into impact of the policy. She noted that mandates are not good care and undermine patient-doctor relationships. She also asked for more patient input in HERC decisions on future policy decisions. She also requested that the guideline not require additional therapies as a mandatory requirement and instead be reworded as “when medically advisable.”
3. Wendy Sinclair: Ms. Sinclair is an advocate from the Oregon Pain Action Group. She thanked the
committee for listening to stakeholders and advocates. Doctors should be able to practice individualized care. Chronic pain is a broad category, and it is wrong to assume everyone will respond to the same treatments. When GN60 was enacted, providers received a letter requesting they taper patients. She expressed concern with the current changes not being promoted as strongly to providers. She also requested that the VBBS consider adding “when medically advisable” to phrases about alternative treatments.
The subcommittee made several changes to the proposed guideline edits, including changing “must” be prescribed when referring to alternative treatments to “should” be prescribed “unless contraindicated.” Recommended Actions: 1) GN60 OPIOIDS FOR CONDITIONS OF THE BACK AND SPINE was modified as shown in Appendix A MOTION: To recommend the guideline note changes as modified. CARRIES 7-0.
Public Comment: Mareinna Kansiger testified; she is a transgender person and declared no affiliations or conflicts of interest. She testified on facial feminization surgery (FFS) procedures. Facial feminization is not covered by the Oregon Health Plan as cosmetic, where there is comorbidity. Because of this policy,
December 2020 QHOC Meeting Packet Page 23 of 44
OHSU (the only provider of FFS procedures in the area) won’t schedule a consultation with her, and there is no way to start an appeal process as no treatment has been denied, creating a Catch-22. Part of the diagnostic criterial for gender dysphoria is the desire to live and be accepted as the gender one identifies with. Treating gender dysphoria means helping one be accepted as their true gender. Kansiger said that gender reassignment surgery (GRS) is only a partial treatment for gender dysphoria. The primary way people gender you is the face. The face is one’s identity. Thus, FFS is as important or more important than GRS for treatment of gender dysphoria. Prioritizing which body part gets treatment is in direct opposition to scientific understanding of gender dysphoria and professional guidelines; FFS is not cosmetic, as it is designed to make a patient’s appearance feminine, not to make it more attractive. It is recommended for coverage by the World Professional Association for Transgender Health (WPATH). She said that facial gender confirming surgery is a newer term for this surgery because the purpose is to treat gender dysphoria. FFS helps protect people against violence and helps the mental health of patient. FFS is also cost effective—its benefits include lower rates of suicide and depression along with higher rates of HIV treatment. Until insurance companies better understand gender dysphoria and cover FFS, gender dysphoria will persist. Olson said we would look at this offline before the next meeting.
Issues for next meeting: • 2021 HCPCS codes
Next meeting:
January 21, 2021, virtual meeting
Adjournment:
The meeting adjourned at 12:35 PM.
December 2020 QHOC Meeting Packet Page 24 of 44
Revised Guideline Notes DIAGNOSTIC GUIDELINE D17, PRENATAL GENETIC TESTING
The following types of prenatal genetic testing and genetic counseling are covered for pregnant women:
A) Genetic counseling (CPT 96040, HPCPS S0265) for high-risk women who have family history of inheritable disorder or carrier state, ultrasound abnormality, previous pregnancy with aneuploidy, or elevated risk of neural tube defect.
B) Genetic counseling (CPT 96040, HPCPS S0265) prior to consideration of chorionic villus sampling (CVS), amniocentesis, microarray testing, Fragile X, and spinal muscular atrophy screening
C) Validated questionnaire to assess genetic risk in all pregnant women D) Screening high-risk ethnic groups for hemoglobinopathies (CPT 83020, 83021) E) Screening for aneuploidy with any of five six screening strategies [first trimester (nuchal
translucency, beta-HCG and PAPP-A), integrated, serum integrated, stepwise sequential, and contingency, and cell free fetal DNA testing] (CPT 76813, 76814, 81508, -81510, 81511, 81420, 81507, 81512, 82105, 82677,84163)
F) Cell free fetal DNA testing (CPT 81420, 81507) for evaluation of aneuploidy in women who have an elevated risk of a fetus with aneuploidy (maternal age >34, family history or elevated risk based on screening).
G) Ultrasound for structural anomalies between 18 and 20 weeks gestation (CPT 76811, 76812) H) CVS or amniocentesis (CPT 59000, 59015, 76945,76946, 82106, 88235, 88261-88264, 88267,
88269, 88280, 88283, 88285, 88289,88291) for a positive aneuploidy screen, maternal age >34, fetal structural anomalies, family history of inheritable chromosomal disorder or elevated risk of neural tube defect.
I) Array CGH (CPT 81228, 81229) when major fetal congenital anomalies are apparent on imaging, or with normal imaging when array CGH would replace karyotyping performed with CVS or amniocentesis in (H) above.
J) FISH testing (CPT 88271, 88272, 88274, 88275, 81171, 81172) only if karyotyping is not possible due a need for rapid turnaround for reasons of reproductive decision-making (i.e. at 22w4d gestation or beyond)
K) Screening for Tay-Sachs carrier status (CPT 81255) in high-risk populations. First step is hex A, and then additional DNA analysis in individuals with ambiguous Hex A test results, suspected variant form of TSD or suspected pseudodeficiency of Hex A
L) Screening for cystic fibrosis carrier status once in a lifetime (CPT 81220-81224) M) Screening for fragile X status (CPT 81243, 81244, 81171. 81172) in patients with a personal or
family history of a. fragile X tremor/ataxia syndrome b. premature ovarian failure c. unexplained early onset intellectual disability d. fragile X intellectual disability e. unexplained autism through the pregnant woman’s maternal line
N) Screening for spinal muscular atrophy (CPT 81329) once in a lifetime O) Screening those with Ashkenazi Jewish heritage for Canavan disease (CPT 81200), familial
dysautonomia (CPT 81260), and Tay-Sachs carrier status (CPT 81255). Ashkenazi Jewish carrier panel testing (CPT 81412) is covered if the panel would replace and would be of similar or lower cost than individual gene testing including CF carrier testing.
P) Expanded carrier screening only for those genetic conditions identified above
December 2020 QHOC Meeting Packet Page 25 of 44
The following genetic screening tests are not covered: A) Serum triple screen B) Expanded carrier screening which includes results for conditions not explicitly recommended for
coverage The development of this guideline note was informed by a HERC coverage guidance. See https://www.oregon.gov/oha/HPA/DSI-HERC/Pages/Evidence-based-Reports.aspx. DIAGNOSTIC GUIDELINE D25, HEREDITARY CANCER GENETIC TESTING
Related to genetic testing for patients with breast/ovarian and colon/endometrial cancer or other related cancers suspected to be hereditary, or patients at increased risk to due to family history, services are provided according to the Comprehensive Cancer Network Guidelines.
A) Lynch syndrome (hereditary colorectal, endometrial and other cancers associated with Lynch syndrome) services (CPT 81288, 81292-81300, 81317-81319, 81435, 81436) and familial adenomatous polyposis (FAP) services (CPT 81201-81203) should be provided as defined by the NCCN Clinical Practice Guidelines in Oncology. Genetic/Familial High-Risk Assessment: Colorectal V1.2018 (7/12/18). V1.2020 (7/21/20) www.nccn.org.
B) Breast and ovarian cancer syndrome genetic testing services (CPT 81162-81167, 81212, 81215-81217) for patients without a personal history of breast, ovarian and other associated cancers should be provided to high-risk patients as defined by the US Preventive Services Task Force or according to the NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian and Pancreatic and ovarian. V2.2019 (7/30/18). V1.2021 (9/8/20) www.nccn.org.
C) Breast and ovarian cancer syndrome genetic testing services (CPT 81162-81167, 81212, 81215-81217)) for women with a personal history of breast, ovarian, or other associated cancers and for men with breast or other associated cancers should be provided according to the NCCN Clinical Practice Guidelines in Oncology. Genetic/Familial High-Risk Assessment: Breast, Ovarian and Pancreatic and ovarian. V2.2019 (7/30/18). V1.2021 (9/8/20) www.nccn.org.
D) PTEN (Cowden syndrome) services (CPT 81321-81323) should be provided as defined by the NCCN Clinical Practice Guidelines in Oncology. Genetic/Familial High-Risk Assessment: Breast and Ovarian. V2.2019 (7/30/18) or Genetic/Familial High-Risk Assessment: Colorectal V1.2018 (7/12/18). V1.2020 (7/21/20) www.nccn.org.
Genetic counseling should precede genetic testing for hereditary cancer whenever possible.
A) Pre and post-test genetic counseling should be covered when provided by a suitable trained health professional with expertise and experience in cancer genetics. Genetic counseling is recommended for cancer survivors when test results would affect cancer screening. 1) “Suitably trained” is defined as board certified or active candidate status from the American
Board of Medical Genetics, American Board of Genetic Counseling, or Genetic Nursing Credentialing Commission.
B) If timely pre-test genetic counseling is not possible for time-sensitive cases, appropriate genetic testing accompanied by pre- and post- test informed consent and post-test disclosure performed by a board-certified physician with experience in cancer genetics should be covered. 1) Post-test genetic counseling should be performed as soon as is practical.
If the mutation in the family is known, only the test for that mutation is covered. For example, if a mutation for BRCA 1 has been identified in a family, a single site mutation analysis for that mutation is covered (CPT 81215), while a full sequence BRCA 1 and 2 (CPT 81163) analyses is not. There is one
December 2020 QHOC Meeting Packet Page 26 of 44
exception, for individuals of Ashkenazi Jewish ancestry with a known mutation in the family, the panel for Ashkenazi Jewish BRCA mutations is covered (CPT 81212). DIAGNOSTIC GUIDELINE D26, NEUROBEHAVIORAL STATUS EXAMS AND NEUROPSYCHOLOGICAL TESTING
Neurobehavioral status exams (CPT 96116 and 96121) and neuropsychological testing services (CPT 96132 and 96133) are only covered when all of the following are met:
A) Symptoms are not explained by an existing diagnosis; AND B) When the results of such testing will be used to develop a care plan.
OR when neuropsychological testing is done as part of the pre-operative evaluation prior to epilepsy surgery or post-operative follow up after epilepsy surgery. DIAGNOSTIC GUIDELINE D27, SARS-COV-2 (COVID-19) TESTING
Testing for SARS-CoV-2 (COVID-19) virus RNA or viral antigen is a covered diagnostic service. Antibody testing for SARS-CoV-2 (COVID-19; CPT 86413, 86328 or 86769) is covered as diagnostic only when such testing meets the following criteria:
A) Testing is done using tests that have FDA Emergency Use Authorization (EUA) or FDA approval; AND
B) Testing is used as part of the diagnostic work up of multisystem inflammatory syndrome in children (MIS-C) or multisystem inflammatory syndrome in adults (MIS-A) for hospitalized persons under the age of 21.
GUIDELINE NOTE 60, OPIOIDS FOR CONDITIONS OF THE BACK AND SPINE
Lines 346,361,402,529
Opioid medications are only included on these lines under the following criteria. Time periods described below are relative to the patient’s initial injury or condition for which opioids were originally prescribed, regardless of whether the individual or any plan paid for the medication. Providers are encouraged to consider the recommendations of the Oregon Opioid Prescribing Guidelines Task Force when prescribing opioid medications: Oregon Acute Opioid Prescribing Guideline (October 2018) and the Oregon Chronic Opioid Prescribing Guidelines (2017-2018). For acute injury, acute flare of chronic pain, or after surgery: For acute conditions and flares During the first 6 weeks after an acute injury, acute flare of chronic pain, or surgery opioid treatment is included on these lines ONLY:
1) When each prescription is limited to 7 days of treatment, AND 2) For short acting opioids only, AND 3) When one or more alternative first line pharmacologic therapies such as NSAIDs, acetaminophen,
and muscle relaxers have been tried and found not effective or are contraindicated, AND
December 2020 QHOC Meeting Packet Page 27 of 44
4) When prescribed with a plan to keep active (home or prescribed exercise regime) and with consideration of additional therapies such as spinal manipulation, physical therapy, yoga, or acupuncture, AND
5) There is documented verification that evaluation of the patient’s risk factors is not high risk for opioid misuse or abuse (e.g. history of opioid misuse, verification of prescription history in the PDMP, etc.).
During subacute period Treatment with opioids after 6 weeks of continuous therapy and up to 90 days after the initial injury/flare/surgery is included on these lines ONLY:
1) With documented evidence of improvement of function of at least thirty percent as compared to baseline based on a validated tools (e.g. Oswestry, Neck Disability Index, SF-MPQ, and MSPQ).
2) When prescribed with a plan to keep active (home or prescribed exercise regime) and with consideration of additional therapies such as spinal manipulation, physical therapy, yoga, or acupuncture, AND
3) With verification that the patient is not high risk for opioid misuse or abuse. Such verification may involve
a) Documented verification from the state's prescription monitoring program database that the controlled substance history is consistent with the prescribing record
b) Use of a validated screening instrument to verify the absence of a current substance use disorder (excluding nicotine) or a history of prior opioid misuse or abuse
c) Administration of a baseline urine drug test to verify the absence of illicit drugs and non-prescribed opioids.
4) Each prescription must be limited to 7 days of treatment and for short-acting opioids only
Long-term opioid therapy Long-term opioid treatment (>90 days) after the initial injury/flare/surgery is not included on these lines except for the taper process as described below. Transitional coverage for patients on long-term opioid therapy: For patients receiving long-term opioid therapy (>90 days) for conditions of the back and spine, continued coverage of opioid medications requires a comprehensive individual treatment plan for chronic pain, taking into account the biological, behavioral, psychological and social factors which may influence each individual’s experience of chronic pain as well as any current and past treatments. Treatment plans should be prescribed (unless contraindicated) with a plan to keep active (home or prescribed exercise regime) and should include additional therapies such as spinal manipulation, physical therapy, yoga or acupuncture unless contraindicated if available in a patient’s community and reasonably accessible to the patient. The treatment plan should conform with the Oregon Chronic Opioid Prescribing Guidelines (2017-2018). A taper plan may be included if and when clinically appropriate. Opioid tapers Opioid taper plans are not required in order for continued inclusion of long-term opioid therapy on these lines. Providers initiating taper plans are encouraged to follow Oregon Opioid Tapering Guidelines
December 2020 QHOC Meeting Packet Page 28 of 44
(January 2020). For patients receiving long-term opioid therapy (>90 days) for conditions of the back and spine, continued coverage of opioid medications requires an individual treatment plan which includes a taper plan when clinically indicated. Opioid tapering should be done on an individualized basis with a shared goal set by the patient and provider based on the patient’s overall status. Taper plans should include nonpharmacological treatment strategies for managing the patient’s pain. During the taper, behavioral health conditions need to be regularly assessed and appropriately managed. In some situations (e.g., in the setting of active substance use disorder, history of opioid overdose, aberrant behavior), more rapid tapering or transition to medication assisted treatment may be appropriate and should be directed by the prescribing provider. If a patient has developed an opioid use disorder, treatment is included on Line 4 SUBSTANCE USE DISORDER. GUIDELINE NOTE 90, COGNITIVE REHABILITATION
Lines 91,178,196,201,285,294,317,345,377 Once physical stabilization from acute brain injury has occurred, as determined by an attending physician, cognitive rehabilitation (CPT 97129 and 97130) is included on this line for a three month period. This three month period does not have to be initiated immediately following stabilization from the injury. For up to 3 years following the acute event, an additional 6 visits of cognitive rehabilitation are included on this line each time the patient has a major change in status resulting in a significantly improved prognosis. Cognitive rehabilitation is not included on this line for those in a vegetative state or for those who are unable or unwilling to participate in therapy GUIDELINE NOTE 102, REPETITIVE TRANSCRANIAL MAGNETIC STIMULATION
Line 7
Repetitive transcranial magnetic stimulation (CPT 90867-90869 90868) is covered included on this line only after failure of at least two antidepressants. when ALL of the following criteria are met
1) The patient has a confirmed diagnosis of severe major depressive disorder based on standardized rating scales, AND
2) The patient has treatment resistant depression as evidenced by BOTH of the following a. ongoing symptoms despite treatment with at least 2 psychopharmacologic regimens
each used for 8 weeks unless not tolerated or contraindicated, AND b. failure of a trial of psychotherapy conducted for a minimum duration of 6 weeks at least
1 time a week with no improvement in depressive symptoms as documented by standardized rating scales; AND
3) The patient does not have psychosis, acute suicidal risk, catatonia, significantly impaired essential function, or other condition for which electroconvulsive therapy (ECT) would be clinically superior to TMS; AND
4) The patient has no contraindications to rTMS such as implanted devices in or around the head, increased risk of seizure, etc.; AND
5) The therapy is administered by an FDA approved device in accordance to labeled indications; AND
6) The patient is 18 years of age or older.
December 2020 QHOC Meeting Packet Page 29 of 44
Repetitive transcranial magnetic stimulation is covered for a maximum of 30 sessions (once a day up to 5 times a week for 6 weeks) for initial treatment. Repeat treatment may be covered if the patient responded to the initial treatment (defined as at least of 50 percent reduction in depression score on standardized rating scale) and at least 3 months have elapsed since the initial treatment. The development of this guideline note was informed by a HERC coverage guidance. See https://www.oregon.gov/oha/HPA/DSI-HERC/Pages/Evidence-based-Reports.aspx. GUIDELINE NOTE 123, DENTAL FILLINGS FOR POSTERIOR TEETH
Line 343 For dental fillings in posterior teeth, amalgam is preferred for extensive restorations. If amalgam is unavailable or contraindicated, composite is acceptable. GUIDELINE NOTE 139, FRENOTOMY FOR TONGUE TIE IN NEWBORNS
Lines 18,596
Ankyloglossia (ICD-10-CM Q38.1 is included on Line 18 for pairing with frenotomy (CPT 41010, CDT D7962 D7960) only when it interferes with breastfeeding. Otherwise, Q38.1 and CPT 41010 are included on Line 596 GUIDELINE NOTE 173, TREATMENTS THAT HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS FOR CERTAIN CONDITIONS; UNPROVEN TREATMENTS The following treatments are prioritized on Line 662, CONDITIONS FOR WHICH CERTAIN TREATMENTS HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS; UNPROVEN TREATMENTS for the conditions listed here: CPT/HCPCS code
INTERVENTION Rationale Date of last Review
64912-64913 Nerve repair; with nerve allograft Unproven treatment November, 2017
December 2020 QHOC Meeting Packet Page 30 of 44
New Guideline Notes GUIDELINE NOTE XXX NERVE ALLOGRAFTS
Line 536
Nerve allografts (CPT 64912-64913) are only on this line for repair of digital nerve injury (ICD-10-CM S64.4 code category). GUIDELINE NOTE XXX DENTAL IMPLANT REMOVAL
Lines 344, 619
Removal of dental implants (D6100) is included on line 344 only when there is advanced peri-implantitis with bone loss and mobility, abscess or implant fracture. Otherwise, this procedure is included on line 619. GUIDELINE NOTE XXX DEVELOPMENTAL DELAY CODING
Lines 292,345,377,661
ICD-10-CM R62.0 and R62.50 are included on these lines for children 5 and under used to identify dysfunction substantially below chronological age, when significantly and persistently interfering with activities of daily living appropriate for chronological age, and there is an opportunity for skill learning. ICD-10-CM F88 is included on these lines for developmental delay. When it is used to indicate sensory integration disorder or sensory processing disorder, it is included on Line 661.
December 2020 QHOC Meeting Packet Page 31 of 44
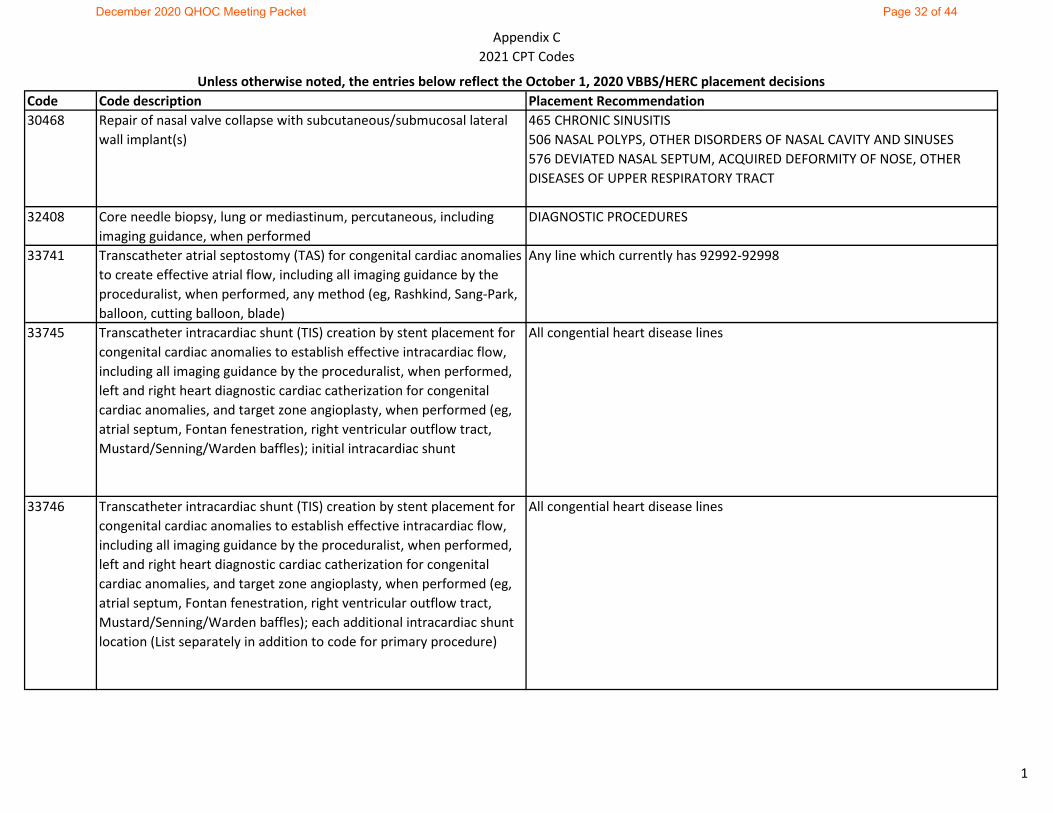
Appendix C2021 CPT Codes
Code Code description Placement Recommendation30468 Repair of nasal valve collapse with subcutaneous/submucosal lateral
wall implant(s)465 CHRONIC SINUSITIS 506 NASAL POLYPS, OTHER DISORDERS OF NASAL CAVITY AND SINUSES 576 DEVIATED NASAL SEPTUM, ACQUIRED DEFORMITY OF NOSE, OTHER DISEASES OF UPPER RESPIRATORY TRACT
32408 Core needle biopsy, lung or mediastinum, percutaneous, including imaging guidance, when performed
DIAGNOSTIC PROCEDURES
33741 Transcatheter atrial septostomy (TAS) for congenital cardiac anomalies to create effective atrial flow, including all imaging guidance by the proceduralist, when performed, any method (eg, Rashkind, Sang-Park, balloon, cutting balloon, blade)
Any line which currently has 92992-92998
33745 Transcatheter intracardiac shunt (TIS) creation by stent placement for congenital cardiac anomalies to establish effective intracardiac flow, including all imaging guidance by the proceduralist, when performed, left and right heart diagnostic cardiac catherization for congenital cardiac anomalies, and target zone angioplasty, when performed (eg, atrial septum, Fontan fenestration, right ventricular outflow tract, Mustard/Senning/Warden baffles); initial intracardiac shunt
All congential heart disease lines
33746 Transcatheter intracardiac shunt (TIS) creation by stent placement for congenital cardiac anomalies to establish effective intracardiac flow, including all imaging guidance by the proceduralist, when performed, left and right heart diagnostic cardiac catherization for congenital cardiac anomalies, and target zone angioplasty, when performed (eg, atrial septum, Fontan fenestration, right ventricular outflow tract, Mustard/Senning/Warden baffles); each additional intracardiac shunt location (List separately in addition to code for primary procedure)
All congential heart disease lines
Unless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
1
December 2020 QHOC Meeting Packet Page 32 of 44
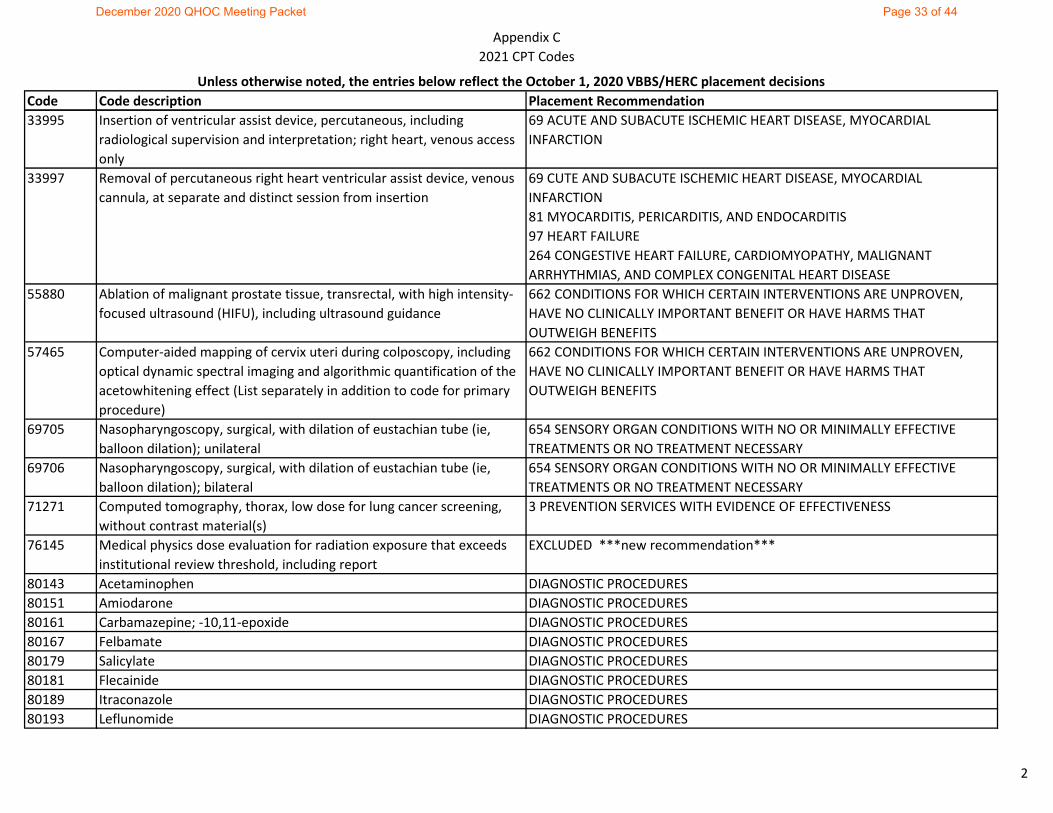
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
33995 Insertion of ventricular assist device, percutaneous, including radiological supervision and interpretation; right heart, venous access only
69 ACUTE AND SUBACUTE ISCHEMIC HEART DISEASE, MYOCARDIAL INFARCTION
33997 Removal of percutaneous right heart ventricular assist device, venous cannula, at separate and distinct session from insertion
69 CUTE AND SUBACUTE ISCHEMIC HEART DISEASE, MYOCARDIAL INFARCTION 81 MYOCARDITIS, PERICARDITIS, AND ENDOCARDITIS97 HEART FAILURE 264 CONGESTIVE HEART FAILURE, CARDIOMYOPATHY, MALIGNANT ARRHYTHMIAS, AND COMPLEX CONGENITAL HEART DISEASE
55880 Ablation of malignant prostate tissue, transrectal, with high intensity-focused ultrasound (HIFU), including ultrasound guidance
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
57465 Computer-aided mapping of cervix uteri during colposcopy, including optical dynamic spectral imaging and algorithmic quantification of the acetowhitening effect (List separately in addition to code for primary procedure)
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
69705 Nasopharyngoscopy, surgical, with dilation of eustachian tube (ie, balloon dilation); unilateral
654 SENSORY ORGAN CONDITIONS WITH NO OR MINIMALLY EFFECTIVE TREATMENTS OR NO TREATMENT NECESSARY
69706 Nasopharyngoscopy, surgical, with dilation of eustachian tube (ie, balloon dilation); bilateral
654 SENSORY ORGAN CONDITIONS WITH NO OR MINIMALLY EFFECTIVE TREATMENTS OR NO TREATMENT NECESSARY
71271 Computed tomography, thorax, low dose for lung cancer screening, without contrast material(s)
3 PREVENTION SERVICES WITH EVIDENCE OF EFFECTIVENESS
76145 Medical physics dose evaluation for radiation exposure that exceeds institutional review threshold, including report
EXCLUDED ***new recommendation***
80143 Acetaminophen DIAGNOSTIC PROCEDURES80151 Amiodarone DIAGNOSTIC PROCEDURES80161 Carbamazepine; -10,11-epoxide DIAGNOSTIC PROCEDURES80167 Felbamate DIAGNOSTIC PROCEDURES80179 Salicylate DIAGNOSTIC PROCEDURES80181 Flecainide DIAGNOSTIC PROCEDURES80189 Itraconazole DIAGNOSTIC PROCEDURES80193 Leflunomide DIAGNOSTIC PROCEDURES
2
December 2020 QHOC Meeting Packet Page 33 of 44
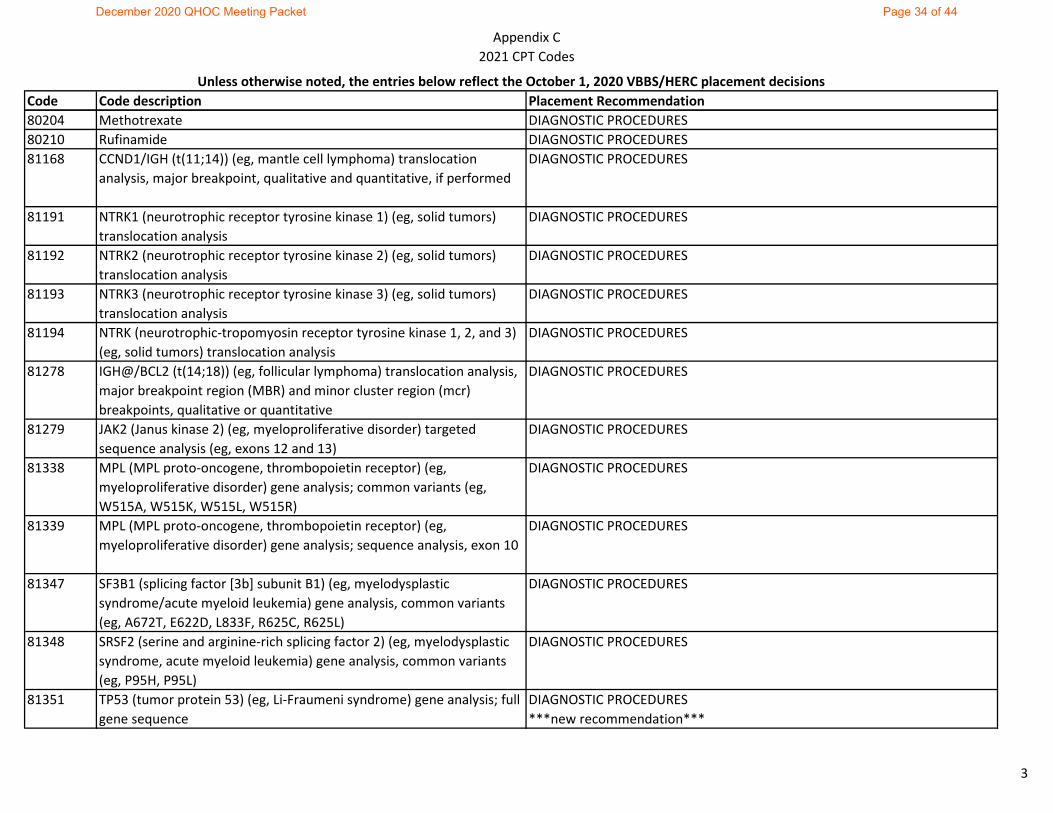
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
80204 Methotrexate DIAGNOSTIC PROCEDURES80210 Rufinamide DIAGNOSTIC PROCEDURES81168 CCND1/IGH (t(11;14)) (eg, mantle cell lymphoma) translocation
analysis, major breakpoint, qualitative and quantitative, if performedDIAGNOSTIC PROCEDURES
81191 NTRK1 (neurotrophic receptor tyrosine kinase 1) (eg, solid tumors) translocation analysis
DIAGNOSTIC PROCEDURES
81192 NTRK2 (neurotrophic receptor tyrosine kinase 2) (eg, solid tumors) translocation analysis
DIAGNOSTIC PROCEDURES
81193 NTRK3 (neurotrophic receptor tyrosine kinase 3) (eg, solid tumors) translocation analysis
DIAGNOSTIC PROCEDURES
81194 NTRK (neurotrophic-tropomyosin receptor tyrosine kinase 1, 2, and 3) (eg, solid tumors) translocation analysis
DIAGNOSTIC PROCEDURES
81278 IGH@/BCL2 (t(14;18)) (eg, follicular lymphoma) translocation analysis, major breakpoint region (MBR) and minor cluster region (mcr) breakpoints, qualitative or quantitative
DIAGNOSTIC PROCEDURES
81279 JAK2 (Janus kinase 2) (eg, myeloproliferative disorder) targeted sequence analysis (eg, exons 12 and 13)
DIAGNOSTIC PROCEDURES
81338 MPL (MPL proto-oncogene, thrombopoietin receptor) (eg, myeloproliferative disorder) gene analysis; common variants (eg, W515A, W515K, W515L, W515R)
DIAGNOSTIC PROCEDURES
81339 MPL (MPL proto-oncogene, thrombopoietin receptor) (eg, myeloproliferative disorder) gene analysis; sequence analysis, exon 10
DIAGNOSTIC PROCEDURES
81347 SF3B1 (splicing factor [3b] subunit B1) (eg, myelodysplastic syndrome/acute myeloid leukemia) gene analysis, common variants (eg, A672T, E622D, L833F, R625C, R625L)
DIAGNOSTIC PROCEDURES
81348 SRSF2 (serine and arginine-rich splicing factor 2) (eg, myelodysplastic syndrome, acute myeloid leukemia) gene analysis, common variants (eg, P95H, P95L)
DIAGNOSTIC PROCEDURES
81351 TP53 (tumor protein 53) (eg, Li-Fraumeni syndrome) gene analysis; full gene sequence
DIAGNOSTIC PROCEDURES***new recommendation***
3
December 2020 QHOC Meeting Packet Page 34 of 44
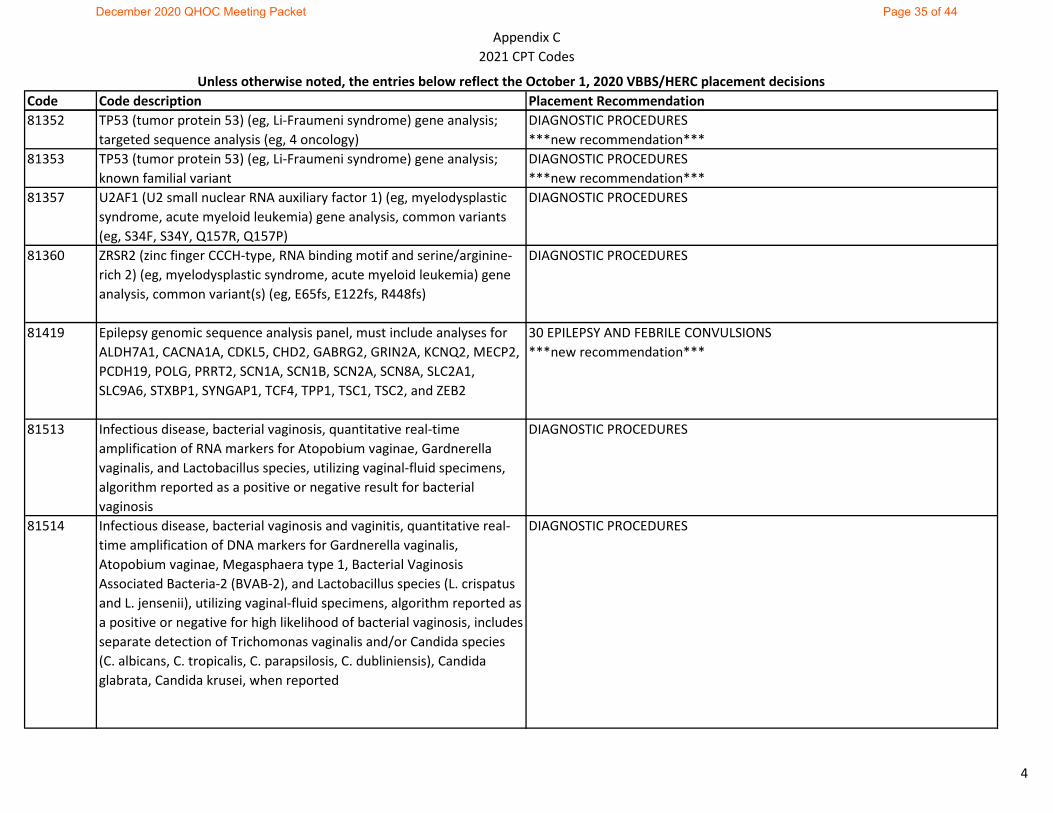
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
81352 TP53 (tumor protein 53) (eg, Li-Fraumeni syndrome) gene analysis; targeted sequence analysis (eg, 4 oncology)
DIAGNOSTIC PROCEDURES***new recommendation***
81353 TP53 (tumor protein 53) (eg, Li-Fraumeni syndrome) gene analysis; known familial variant
DIAGNOSTIC PROCEDURES***new recommendation***
81357 U2AF1 (U2 small nuclear RNA auxiliary factor 1) (eg, myelodysplastic syndrome, acute myeloid leukemia) gene analysis, common variants (eg, S34F, S34Y, Q157R, Q157P)
DIAGNOSTIC PROCEDURES
81360 ZRSR2 (zinc finger CCCH-type, RNA binding motif and serine/arginine-rich 2) (eg, myelodysplastic syndrome, acute myeloid leukemia) gene analysis, common variant(s) (eg, E65fs, E122fs, R448fs)
DIAGNOSTIC PROCEDURES
81419 Epilepsy genomic sequence analysis panel, must include analyses for ALDH7A1, CACNA1A, CDKL5, CHD2, GABRG2, GRIN2A, KCNQ2, MECP2, PCDH19, POLG, PRRT2, SCN1A, SCN1B, SCN2A, SCN8A, SLC2A1, SLC9A6, STXBP1, SYNGAP1, TCF4, TPP1, TSC1, TSC2, and ZEB2
30 EPILEPSY AND FEBRILE CONVULSIONS***new recommendation***
81513 Infectious disease, bacterial vaginosis, quantitative real-time amplification of RNA markers for Atopobium vaginae, Gardnerella vaginalis, and Lactobacillus species, utilizing vaginal-fluid specimens, algorithm reported as a positive or negative result for bacterial vaginosis
DIAGNOSTIC PROCEDURES
81514 Infectious disease, bacterial vaginosis and vaginitis, quantitative real-time amplification of DNA markers for Gardnerella vaginalis, Atopobium vaginae, Megasphaera type 1, Bacterial Vaginosis Associated Bacteria-2 (BVAB-2), and Lactobacillus species (L. crispatus and L. jensenii), utilizing vaginal-fluid specimens, algorithm reported as a positive or negative for high likelihood of bacterial vaginosis, includes separate detection of Trichomonas vaginalis and/or Candida species (C. albicans, C. tropicalis, C. parapsilosis, C. dubliniensis), Candida glabrata, Candida krusei, when reported
DIAGNOSTIC PROCEDURES
4
December 2020 QHOC Meeting Packet Page 35 of 44
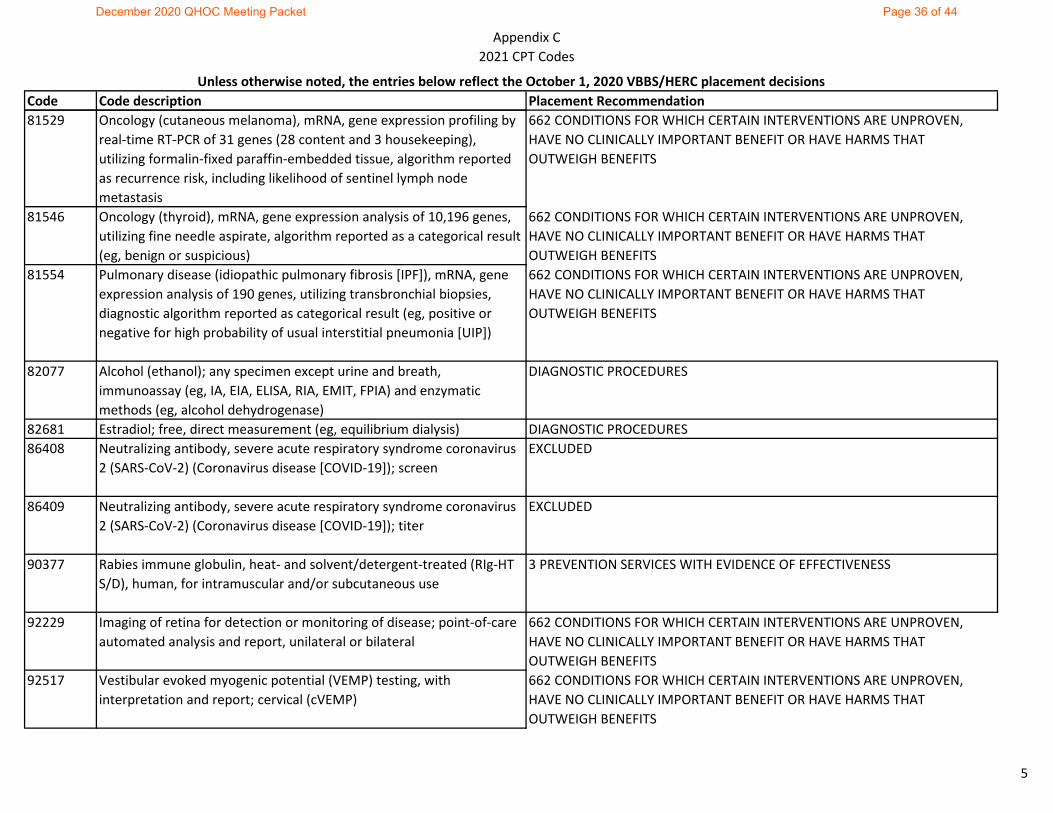
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
81529 Oncology (cutaneous melanoma), mRNA, gene expression profiling by real-time RT-PCR of 31 genes (28 content and 3 housekeeping), utilizing formalin-fixed paraffin-embedded tissue, algorithm reported as recurrence risk, including likelihood of sentinel lymph node metastasis
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
81546 Oncology (thyroid), mRNA, gene expression analysis of 10,196 genes, utilizing fine needle aspirate, algorithm reported as a categorical result (eg, benign or suspicious)
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
81554 Pulmonary disease (idiopathic pulmonary fibrosis [IPF]), mRNA, gene expression analysis of 190 genes, utilizing transbronchial biopsies, diagnostic algorithm reported as categorical result (eg, positive or negative for high probability of usual interstitial pneumonia [UIP])
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
82077 Alcohol (ethanol); any specimen except urine and breath, immunoassay (eg, IA, EIA, ELISA, RIA, EMIT, FPIA) and enzymatic methods (eg, alcohol dehydrogenase)
DIAGNOSTIC PROCEDURES
82681 Estradiol; free, direct measurement (eg, equilibrium dialysis) DIAGNOSTIC PROCEDURES86408 Neutralizing antibody, severe acute respiratory syndrome coronavirus
2 (SARS-CoV-2) (Coronavirus disease [COVID-19]); screenEXCLUDED
86409 Neutralizing antibody, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]); titer
EXCLUDED
90377 Rabies immune globulin, heat- and solvent/detergent-treated (RIg-HT S/D), human, for intramuscular and/or subcutaneous use
3 PREVENTION SERVICES WITH EVIDENCE OF EFFECTIVENESS
92229 Imaging of retina for detection or monitoring of disease; point-of-care automated analysis and report, unilateral or bilateral
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
92517 Vestibular evoked myogenic potential (VEMP) testing, with interpretation and report; cervical (cVEMP)
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
5
December 2020 QHOC Meeting Packet Page 36 of 44
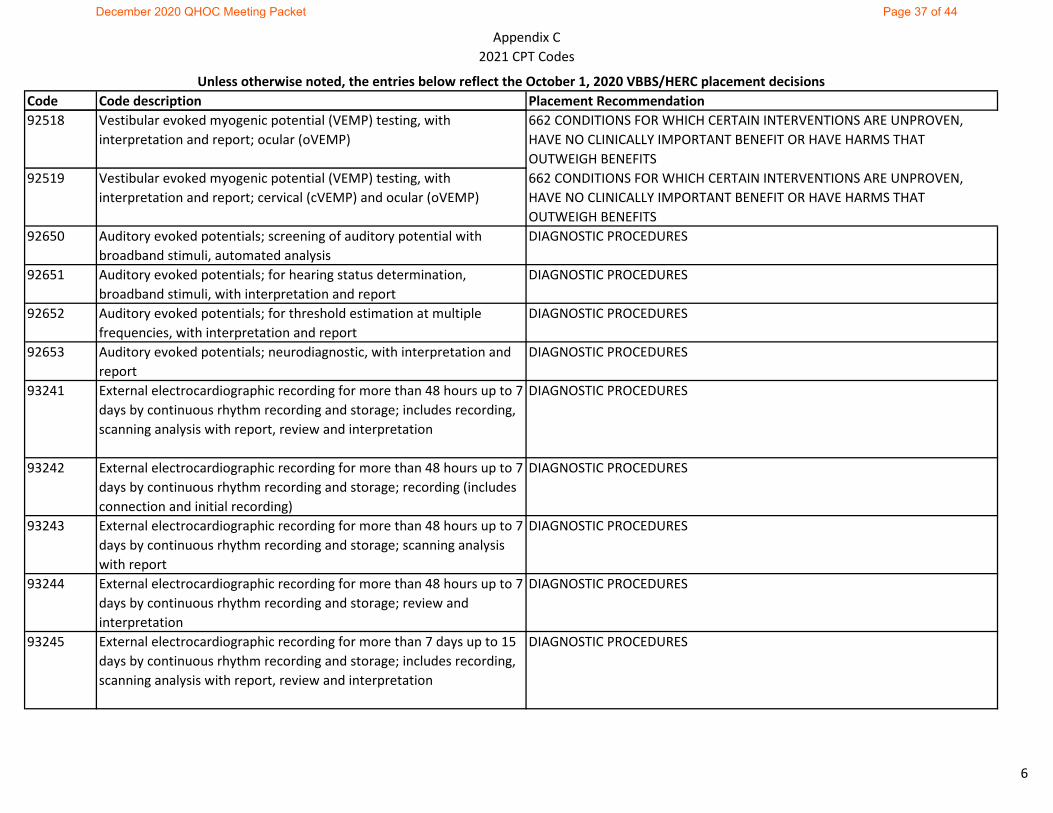
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
92518 Vestibular evoked myogenic potential (VEMP) testing, with interpretation and report; ocular (oVEMP)
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
92519 Vestibular evoked myogenic potential (VEMP) testing, with interpretation and report; cervical (cVEMP) and ocular (oVEMP)
662 CONDITIONS FOR WHICH CERTAIN INTERVENTIONS ARE UNPROVEN, HAVE NO CLINICALLY IMPORTANT BENEFIT OR HAVE HARMS THAT OUTWEIGH BENEFITS
92650 Auditory evoked potentials; screening of auditory potential with broadband stimuli, automated analysis
DIAGNOSTIC PROCEDURES
92651 Auditory evoked potentials; for hearing status determination, broadband stimuli, with interpretation and report
DIAGNOSTIC PROCEDURES
92652 Auditory evoked potentials; for threshold estimation at multiple frequencies, with interpretation and report
DIAGNOSTIC PROCEDURES
92653 Auditory evoked potentials; neurodiagnostic, with interpretation and report
DIAGNOSTIC PROCEDURES
93241 External electrocardiographic recording for more than 48 hours up to 7 days by continuous rhythm recording and storage; includes recording, scanning analysis with report, review and interpretation
DIAGNOSTIC PROCEDURES
93242 External electrocardiographic recording for more than 48 hours up to 7 days by continuous rhythm recording and storage; recording (includes connection and initial recording)
DIAGNOSTIC PROCEDURES
93243 External electrocardiographic recording for more than 48 hours up to 7 days by continuous rhythm recording and storage; scanning analysis with report
DIAGNOSTIC PROCEDURES
93244 External electrocardiographic recording for more than 48 hours up to 7 days by continuous rhythm recording and storage; review and interpretation
DIAGNOSTIC PROCEDURES
93245 External electrocardiographic recording for more than 7 days up to 15 days by continuous rhythm recording and storage; includes recording, scanning analysis with report, review and interpretation
DIAGNOSTIC PROCEDURES
6
December 2020 QHOC Meeting Packet Page 37 of 44
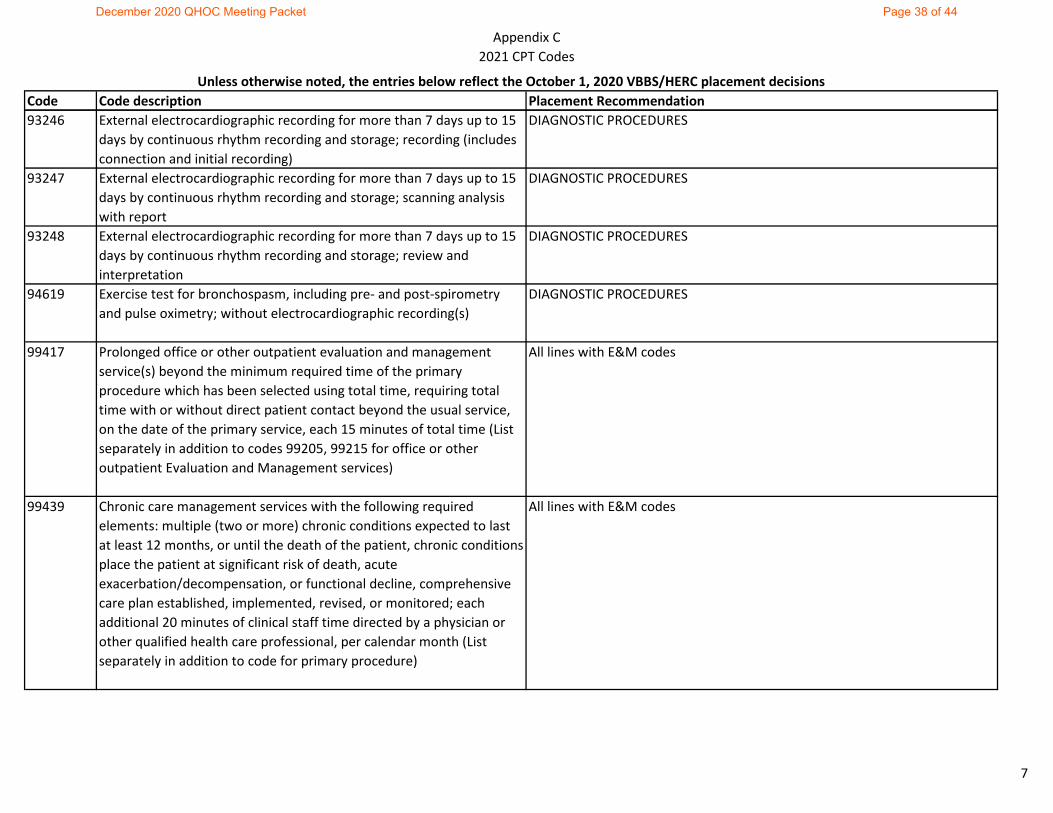
Appendix C2021 CPT Codes
Code Code description Placement RecommendationUnless otherwise noted, the entries below reflect the October 1, 2020 VBBS/HERC placement decisions
93246 External electrocardiographic recording for more than 7 days up to 15 days by continuous rhythm recording and storage; recording (includes connection and initial recording)
DIAGNOSTIC PROCEDURES
93247 External electrocardiographic recording for more than 7 days up to 15 days by continuous rhythm recording and storage; scanning analysis with report
DIAGNOSTIC PROCEDURES
93248 External electrocardiographic recording for more than 7 days up to 15 days by continuous rhythm recording and storage; review and interpretation
DIAGNOSTIC PROCEDURES
94619 Exercise test for bronchospasm, including pre- and post-spirometry and pulse oximetry; without electrocardiographic recording(s)
DIAGNOSTIC PROCEDURES
99417 Prolonged office or other outpatient evaluation and management service(s) beyond the minimum required time of the primary procedure which has been selected using total time, requiring total time with or without direct patient contact beyond the usual service, on the date of the primary service, each 15 minutes of total time (List separately in addition to codes 99205, 99215 for office or other outpatient Evaluation and Management services)
All lines with E&M codes
99439 Chronic care management services with the following required elements: multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline, comprehensive care plan established, implemented, revised, or monitored; each additional 20 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month (List separately in addition to code for primary procedure)
All lines with E&M codes
7
December 2020 QHOC Meeting Packet Page 38 of 44
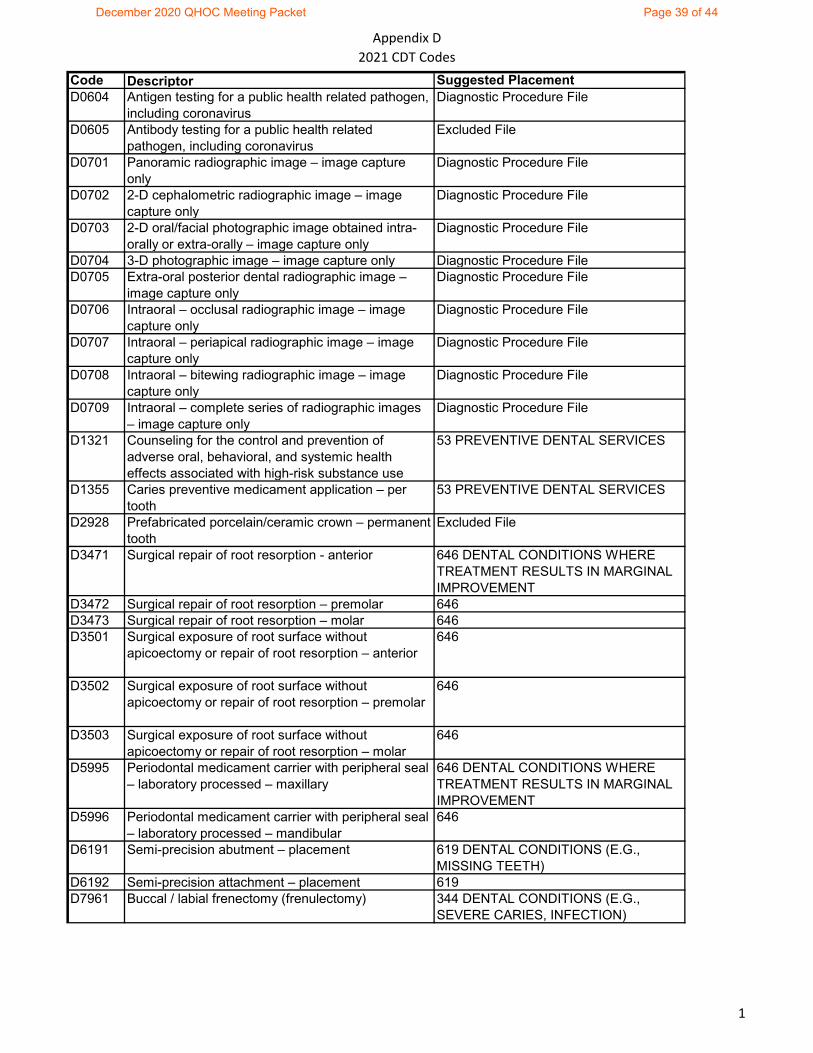
Appendix D2021 CDT Codes
Code Descriptor Suggested PlacementD0604 Antigen testing for a public health related pathogen,
including coronavirusDiagnostic Procedure File
D0605 Antibody testing for a public health related pathogen, including coronavirus
Excluded File
D0701 Panoramic radiographic image – image capture only
Diagnostic Procedure File
D0702 2-D cephalometric radiographic image – image capture only
Diagnostic Procedure File
D0703 2-D oral/facial photographic image obtained intra-orally or extra-orally – image capture only
Diagnostic Procedure File
D0704 3-D photographic image – image capture only Diagnostic Procedure FileD0705 Extra-oral posterior dental radiographic image –
image capture onlyDiagnostic Procedure File
D0706 Intraoral – occlusal radiographic image – image capture only
Diagnostic Procedure File
D0707 Intraoral – periapical radiographic image – image capture only
Diagnostic Procedure File
D0708 Intraoral – bitewing radiographic image – image capture only
Diagnostic Procedure File
D0709 Intraoral – complete series of radiographic images – image capture only
Diagnostic Procedure File
D1321 Counseling for the control and prevention of adverse oral, behavioral, and systemic health effects associated with high-risk substance use
53 PREVENTIVE DENTAL SERVICES
D1355 Caries preventive medicament application – per tooth
53 PREVENTIVE DENTAL SERVICES
D2928 Prefabricated porcelain/ceramic crown – permanent tooth
Excluded File
D3471 Surgical repair of root resorption - anterior 646 DENTAL CONDITIONS WHERE TREATMENT RESULTS IN MARGINAL IMPROVEMENT
D3472 Surgical repair of root resorption – premolar 646D3473 Surgical repair of root resorption – molar 646D3501 Surgical exposure of root surface without
apicoectomy or repair of root resorption – anterior646
D3502 Surgical exposure of root surface without apicoectomy or repair of root resorption – premolar
646
D3503 Surgical exposure of root surface without apicoectomy or repair of root resorption – molar
646
D5995 Periodontal medicament carrier with peripheral seal – laboratory processed – maxillary
646 DENTAL CONDITIONS WHERE TREATMENT RESULTS IN MARGINAL IMPROVEMENT
D5996 Periodontal medicament carrier with peripheral seal – laboratory processed – mandibular
646
D6191 Semi-precision abutment – placement 619 DENTAL CONDITIONS (E.G., MISSING TEETH)
D6192 Semi-precision attachment – placement 619D7961 Buccal / labial frenectomy (frenulectomy) 344 DENTAL CONDITIONS (E.G.,
SEVERE CARIES, INFECTION)
1
December 2020 QHOC Meeting Packet Page 39 of 44
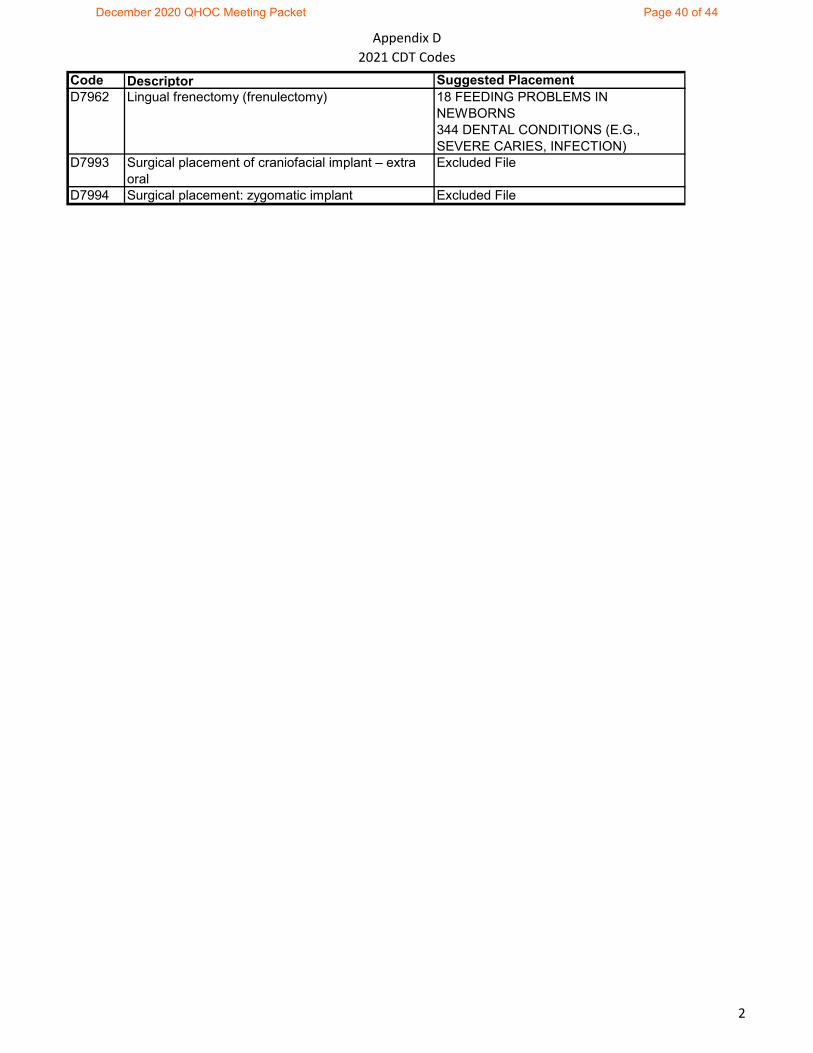
Appendix D2021 CDT Codes
Code Descriptor Suggested PlacementD7962 Lingual frenectomy (frenulectomy) 18 FEEDING PROBLEMS IN
NEWBORNS344 DENTAL CONDITIONS (E.G., SEVERE CARIES, INFECTION)
D7993 Surgical placement of craniofacial implant – extra oral
Excluded File
D7994 Surgical placement: zygomatic implant Excluded File
2
December 2020 QHOC Meeting Packet Page 40 of 44
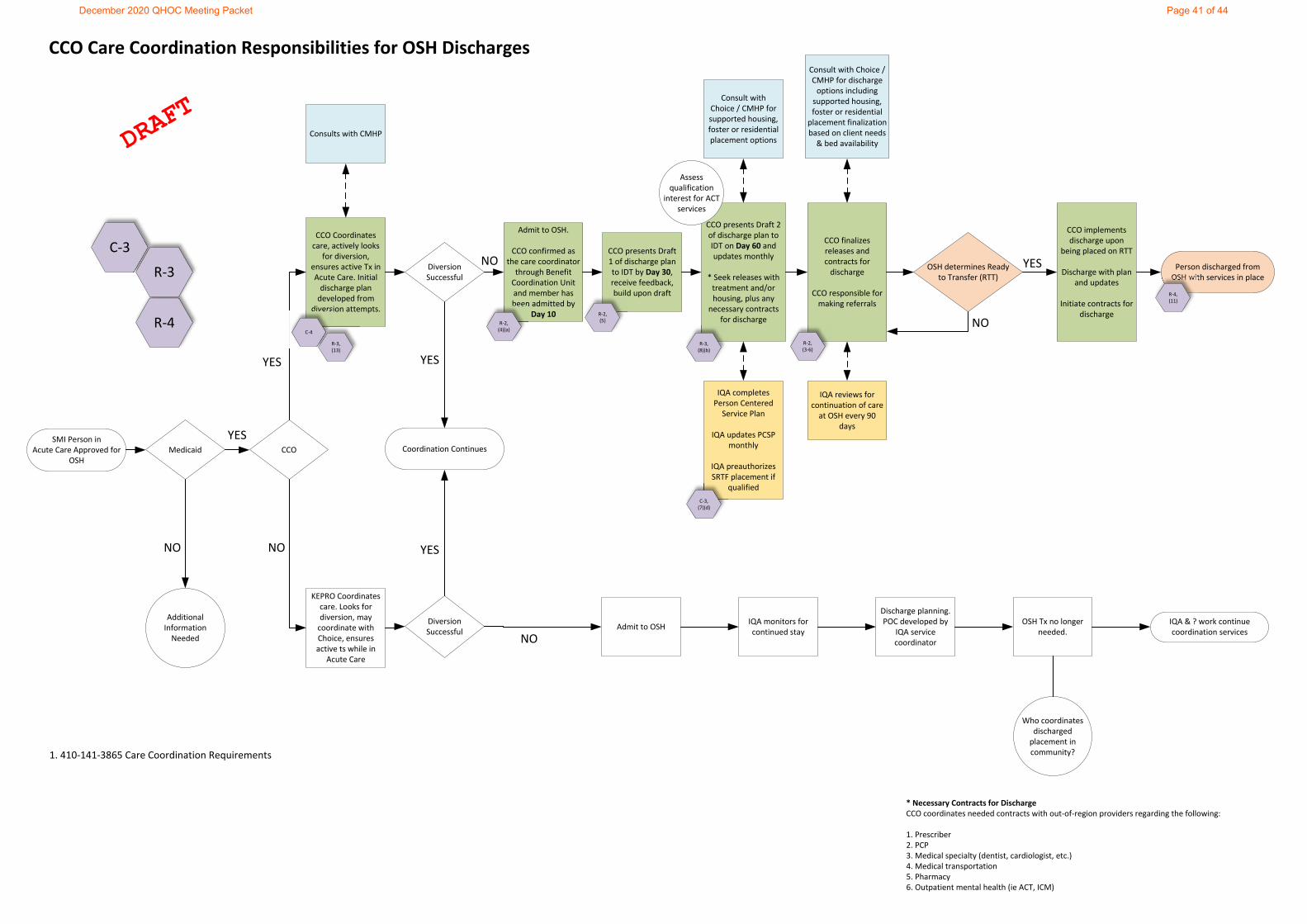
R‐4
SMI Person in Acute Care Approved for
OSHMedicaid CCO
KEPRO Coordinates care. Looks for diversion, may coordinate with Choice, ensures active ts while in
Acute Care
CCO Coordinates care, actively looks
for diversion, ensures active Tx in Acute Care. Initial discharge plan developed from
diversion attempts.
YES
YES
NO
Coordination Continues
Diversion Successful
Diversion Successful
Admit to OSH.
CCO confirmed as the care coordinator through Benefit Coordination Unit and member has been admitted by
Day 10
Admit to OSHNO
NO
CCO presents Draft 2 of discharge plan to IDT on Day 60 and updates monthly
* Seek releases with treatment and/or housing, plus any necessary contracts
for discharge
CCO finalizes releases and contracts for discharge
CCO responsible for making referrals
CCO implements discharge upon
being placed on RTT
Discharge with plan and updates
Initiate contracts for discharge
IQA monitors for continued stay
Discharge planning. POC developed by
IQA service coordinator
OSH Tx no longer needed.
Person discharged from OSH with services in place
IQA & ? work continue coordination services
Who coordinates discharged placement in community?
Additional Information Needed
NO
* Necessary Contracts for DischargeCCO coordinates needed contracts with out‐of‐region providers regarding the following:
1. Prescriber2. PCP3. Medical specialty (dentist, cardiologist, etc.)4. Medical transportation 5. Pharmacy6. Outpatient mental health (ie ACT, ICM)
Consults with CMHP
CCO presents Draft 1 of discharge plan to IDT by Day 30, receive feedback, build upon draft
YES
YES
IQA completes Person Centered Service Plan
IQA updates PCSP monthly
IQA preauthorizes SRTF placement if
qualified
IQA reviews for continuation of care at OSH every 90
days
Consult with Choice / CMHP for supported housing, foster or residential placement options
Consult with Choice / CMHP for discharge options including supported housing, foster or residential placement finalizationbased on client needs & bed availability
Assess qualification
interest for ACT services
OSH determines Ready to Transfer (RTT)
NO
YES
R‐2, (4)(a)C‐4
1. 410‐141‐3865 Care Coordination Requirements
C‐3
R‐3R‐4, (11)
R‐2, (3‐6)
C‐3, (7)(d)
R‐2, (5)
R‐3, (8)(b)
R‐3, (13)
CCO Care Coordination Responsibilities for OSH Discharges
December 2020 QHOC Meeting Packet Page 41 of 44
CCO Contractual and Rule Obligations Relating to OSH October 14, 2020
Relevant Contract Citations (from draft 2021 contract dated 8/21/2020) C-1 Exhibit B, Part 4 - Providers and Delivery System Section 7 - Care Coordination
Contractor shall provide all of the elements of Care Coordination as set for the below in this Sec. 7, Ex. B, Part 4.
f. Contractor shall coordinate with the Oregon State Hospital, other State institutions, and other Behavioral Health Hospital settings, to facilitate Member transition into the most appropriate, independent, and integrated Community-based settings.
C-2 Exhibit M - Behavioral Health Section 9 - Peer Delivered Services
c. Contractor may utilize PDS in providing other Behavioral Health services such as ACT, crisis services, Warm Handoffs from Hospitals, and services at Oregon State Hospital.
C-3 Exhibit M – Behavioral Health Section 13 - Oregon State Hospital
a. Contractor shall be financially responsible for Members on the waitlist for OSH.
b. Contractor shall share financial risk for Members in OSH beginning in Contract Year three (2022).
c. Contractor shall, in accordance with OAR 309-091-0000 through 309-091-005030:
(1) Coordinate with applicable Subcontractors as needed regarding discharges for all adult Members with SPMI; (2) Coordinate care for Members during discharge planning for the return to Home Contractor or to the Receiving Contractor if Member will be discharged into a different Service Area when Member has been deemed ready to transition; (3) Arrange for both physical and Behavioral Health care Services Care Coordination; (4) Provide Case Management Services, Care Coordination and discharge planning for timely follow up to ensure Continuity of Care; (5) Coordinate with OHA regarding Members who are presumptively or will be retroactively enrolled in Oregon Health Plan upon discharge; (6) Arrange for all services to be provided post-discharge in a timely manner; and (7) Provide access to Evidence-Based intensive services for adult Members with SPMI discharged from OSH who refuse ACT services.
d. Discharges from OSH shall not be to a secure residential treatment facility unless Medically Appropriate. No Member shall be discharged to a secure residential treatment facility without the expressed prior written approval of the Director of OHA or the Director’s designee.
e. Contractor shall ensure a Member discharged from OSH who is determined not to meet the level of care for ACT shall be discharged with services appropriate to meet Member’s needs.
December 2020 QHOC Meeting Packet Page 42 of 44
C-4 Exhibit M – Behavioral Health Section 16 - Long Term Psychiatric Care
b. For a Member age 18 or older:
(1) If Contractor identifies a Member, age 18 to age 64, with no significant nursing care needs due to a general medical condition, Acute medical condition or physical disorder of an enduring nature, is appropriate for LTPC, Contractor shall request a LTPC determination from the applicable Health Services Division, Adult Mental Health Services Unit, as described in the procedure for LTPC Determinations for Members 18 to 64, available on the CCO Contract Forms Website.
(a) HSD Adult Mental Health Services Unit will respond to Contractor no more than three (3) Business Days following the date HSD receives a completed Request for LTPC Determination for Member 18-64.
Relevant Division 410 Chapter 141 CCO Administrative Rule Citations R-1 410-141-3500 Definitions
(37) “Home CCO” means the CCO enrollment situation that existed for a member prior to placement, including services received through OHP fee-for-service, based on permanent residency.
(70) “Temporary Placement” means, for purposes of this rule, hospital, institutional, and residential placement only, including those placements occurring inside or outside of the service area with the expectation to return to the Home CCO service area.
R-2 410-141-3815 CCO Enrollment for Temporary Out-of-Area Behavioral Health Treatment Services
(3) Home CCO assignment is based on the member’s residence. Home CCO enrollment for temporary out-of-area placement shall:
(a) Meet Oregon residency requirements defined in OAR 410-200-0200; (b) Comply with the CCO enrollment rules specified in OAR 410-141-3805; (c) Be based on most recent permanent residency and related CCO enrollment history prior to temporary placement. If the client has no enrollment history, new enrollment shall reflect most recent permanent residence prior to hospital, institutional, and residential placement; and (d) Be consistent with OAR 410-141-3810 when the client exercises recipient choice, where the client is able to actively participate in their own recovery and direct their own care. If the client is unable to designate county of residence, as indicated in OAR 410-200-0200, the Authority shall designate the Home CCO as the geographic location of the client at the most recent residency and CCO enrollment prior to hospitalization.
(4) Home CCO enrollment policy for State Hospital discharges shall be implemented as follows:
(a) Upon State Hospital discharge, the State Hospital Benefit Coordination Unit shall consult and coordinate with the Home CCO for client placement; (b) Beginning in Contract year 2022 (or later if specified by the Authority), if the client is enrolled in a CCO at the time of the acute care admission to the State Hospital when a bed becomes available, the CCO shall be responsible for the covered services during that placement even if the location of the facility is outside of the CCO’s service area. The CCO’s responsibility shall be in accordance with a risk sharing agreement to be entered into between the CCO and the State Hospital, in a form
December 2020 QHOC Meeting Packet Page 43 of 44
required by the Authority. The individual is presumed to continue to be enrolled in the CCO with which the individual was most recently enrolled.
(5) For new and existing temporary residential placements, CCOs shall coordinate all behavioral health care and needs including, but not limited to, medication assisted treatment, routine non-emergent physical health care, oral, and transportation when within the scope of the CCO’s contract, including when member’s temporary placements are outside the CCO service area. CCO’s shall coordinate care for members receiving behavioral health treatment while in temporary placement and discharge planning for the return to the Home CCO. Additionally, CCO’s shall coordinate all care for accompanying dependent members.
(6) Enrollment shall follow the Home CCO enrollment policy outlined in this rule, except when:
(a) The Home CCO enrollment hinders access to care or puts the client at potential harm, or the Home CCO is unable to provide needed unique services, a change in enrollment may be requested for the member to a CCO serving the service area of the temporary out-of-area placement; or (b) Home CCO enrollment may create a continuity of care concern, as specified in OAR 410-141-3810. If a continuity interruption to a client’s care is indicated, the Authority shall align enrollment with the care and claims history.
R-3 410-141-3860 Integration and Coordination of Care
(8) CCOs shall meet all of the following requirements relating to transitions of care:
(b) Ensure members are transitioned out of hospital settings into the most appropriate independent and integrated community settings and provided the supportive services needed to ensure successful transition. This includes transitional services and supports for children, adolescents, and adults with serious behavioral health conditions facing admission to or discharge from acute psychiatric care, residential treatment settings, skilled nursing or other long term care settings, and the State Hospital;
(13) CCOs shall ensure that members receiving services from extended or long-term psychiatric care programs, such as secure residential facilities, shall receive follow-up services as medically appropriate to facilitate discharge as soon as reasonably possible. CCOs shall coordinate the care of members who enter the Oregon State Hospital and develop agreements with community mental health programs regarding the management of adults who were members upon entering the Oregon State Hospital and when they are transitioning out of the Oregon State Hospital.
R-4 410-141-3865 Care Coordination Requirements
(11) CCOs must facilitate transition planning for members. In addition to the requirements of 410-141-3860, care coordinators shall facilitate transitions and ensure applicable services and appropriate settings continue after discharge by taking the steps set forth below.
(b) For discharges from the State Hospital and residential care, the care coordinator shall do all of the following:
(A) Have contact with the member no less than two times per month prior to discharge and two times within the week of discharge;
(B) Assist in the facilitation of a warm handoff to relevant care providers during transition of care and discharge planning; and
(C) Engage with the member, face to face, within two days post discharge.
December 2020 QHOC Meeting Packet Page 44 of 44