Embed Size (px)
Citation preview

Egyptian Journal of Neurosurgery Volume 31 / No. 3 / July – September 2016 181-188
Egyptian Journal of Neurosurgery
181
Original Article Lumbar Disc Herniation in Heavy Manual Workers: Conventional Discectomy
versus TLIF with Unilateral Fixation
Tariq Elemam Awad* and Mohamed Youssef Elqazaz Department of Neurosurgery, Faculty of Medicine, Suez Canal University, Ismailia, Egypt
ABSTRACT Received: 5 November 2016 Accepted: 24 December 2016 Key words:
Lumbar disc herniation, Heavy manual work, Discectomy, Unilateral pedicle screws, Transforaminal lumbar interbody fusion © 2016 Egyptian Journal of Neurosurgery. All rights reserved
Background: Conventional discectomy is a common surgical method for treating lumbar disc prolapse. The situation may differ in heavy manual workers who may have more pronounced degenerative spine disease, broad based disc herniations and are expected to be exposed postoperatively to the same preoperative manual stress. Objective: Our aim is to compare the clinical outcome in patients operated for conventional discetomy versus those operated for TLIF with unilateral spinal fixation. Patients and Methods: Sixty patients underwent surgeries for lumbar disc herniation. They were divided into two groups; the discectomy group and the fusion group. They were operated between 2008 and 2015. Par cipants were evaluated pre-operatively and post-opera vely at 3, 6, 9, and 12 month intervals. Pain was scored by a VAS for both lower limbs and back pain. The clinical outcomes were compared using the Prolo economic and functional rating scale and a new outcome score. Results: The two groups of patients were fairly homogeneous and comparable. The work load exposure to repetitive vibration was the most risk for disc prolapse and surgery (28.3 %). Fusion group showed be er clinical outcome parameters including better VAS for low back pain, better Prolo economic, functional rating scale and better new clinical outcome score. In comparison the discectomy group showed significantly higher recurrence rate and reoperation during the follow up period. Conclusion: Heavy manual workers treated with unilateral transforaminal interbody fusion reported less pain & lower disability scores all over the follow up period. This technique is preferable to conventional discectomy because it decreases back & leg pain while avoiding the possibility of recurrence by heavy duties and it maintains stability of the lumbar spine.
INTRODUCTION
Lumbar disc herniation is a common disease that
usually presents itself with low back and leg pain and sometimes with serious neurologic symptoms, as a result of nerve root or cauda equina compression. 1,2 Although lumbar discectomy has led to excellent outcomes in pain relief, return-to-work rates, and patient satisfaction in the general population, results in workers with heavy manual Loads may be significantly different because of the increased postoperative demands during heavy duties. 1-7
In 2003, Carragee et al have prospectively examined a group of 187 patients who underwent simple diskectomy and classified disc herniations on the basis of intraoperative findings into four categories: (1) Fragment-Fissure herniations (2) Fragment-Defect herniations (3) Fragment-Contained herniations and (4) No Fragment-Contained herniations. Carragee et al. found that herniations associated with a small annular defect (i.e., type 1- less than 6 mm) had a 1% recurrent
*Corresponding Author: Tariq Elemam Awad, M.D., Ph.D. Department of Neurological Surgery, School of Medicine, Suez Canal University Hospital 4.5 Kilo of the round road, Ismaillia, Egypt 15213. Email: [email protected]; Tel: +201281577570
herniation rate compared with those with a large defect (i.e., 6 mm or greater), which had 27% recurrent herniation rate and ultimately a 21% reoperation rate. Unfortunately Most of heavy manual workers have disc herniation with large defects. 8
Heavy manual workers are always having degenerative changes in their lumbar spine. There is disc space collapse, facet arthropathy, foraminal or central stenosis, and joint laxity. A study in 2012 examined active duty military men with lumbar disc herniation who were scheduled for surgery. The study showed that Modic changes were most common at the lower lumbar spine segments. In this study, the presence of a disk herniation and Modic changes at the same level was 37.7%. This warrants a different approach in the treatment of those patients. 7
Because lumbar surgery can be associated with a long recovery time and a protracted period of disability,5,6,9 this can lead to prolonged sick leave, decreased work performance, substantial loss of income, and/or an early retirement from the work in elite professional workers.
The situation may different in heavy manual workers who may have more pronounced degenerative spine disease, broad based disc herniations and are expected to be exposed postoperatively to the same preoperative manual stress. To overcome these factors,
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery
182
TLIF with unilateral fixation was supposed to be better than the traditional discectomy. 6
PATIENTS AND METHODS
This study was designed as a controlled, non - randomized, prospective, clinical study. Between February 2008 and July 2015, at Suez Canal area Hospitals (Ismailia, Egypt) a total of sixty consecutive patients were included. The patients were categorized into two groups: Group 1: Patients operated by conventional
discectomy (Thirty patients). Group 2: Patients operated by TLIF with unilateral
lumbar fixation (Thirty patients). Inclusion criteria required all patients to have (1)
predominantly radicular symptoms e.g. intolerable sciatica, or had severe neurological loss (motor loss or symptoms or signs of cauda equina syndrome) (2) a preoperative magnetic resonance imaging study confirming a disc herniation, (3) an age of 18 - 65 years, (4) heavy manual work load. All the patients were male working in a major construction company. They were walking or standing for at least 8 hours every day for many years ranging from 5 to 8 years.
Patients should have been unresponsive to conservative management for a minimum of 6 weeks
and should qualify for surgery for a single-level or contiguous two-level disc herniation between L2-S1.
Exclusion criteria ruled out patients (1) with previous back surgery, (2) with a foraminal or extraforaminal disc herniation, (3) with general diseases that preclude surgical management (severe osteoporosis, osteopenia, immune suppression, malignancy and active local and/or systemic infection), (4) with morbid obesity as measured by body mass index > 40, (5) those with spondylolisthesis or any form of degenerative segmental instability.
The preoperative assessment included patient history, physical examination and neurological examination. Imaging included antero-posterior, lateral and dynamic lateral X-rays and CT and MRI of the lumbo-sacral spine. Preoperative economic (activity) and functional (pain) statuses were assessed and the clinical outcome was evaluated using the Prolo economic and functional rating scale. 10 Additionally, the entire quantity of pain was evaluated using visual analog scale (VAS) for both leg and axial low back pain. 12
A new clinical outcome score for evaluation of clinical outcomes of spine surgery in manual workers was designed and used in this study. (Table 1) Its validity was measured in this study in comparison to the Prolo economic and functional rating scale.
Table 1: New clinical outcome score for evaluation of the outcomes of spine surgery in manual workers.
No Item score 1- Hours of daily work (Percentage of the actual to the proper working
hours) 2-
Days of work per month (Percentage of the attendant days to the proper)
3- 100 - the VAS for Low back pain (on 100 point score) 4- 100 – the VAS for lower limb pain (on 100 point score) 5- Self-estimation of job performance (percentage) 6- Supervisors' estimation of job performance (percentage) 7- Self-estimation of sexual activity (percentage) 8- Being free of Pain medication usage (100 = no pain medication, 80=
occasional NSAID 60 = regular NSAID 40 = narcotic pain medication 9- Self-satisfaction of the operative intervention (percentage) 10- Willingness to do the operative intervention again (percentage)
Each of these items got a score of 100 The final preoperative score record only the first 8 items and the sum is divided by 8 to got final 100 score The final postoperative score record the 10 items and the sum is divided by 10 to got also final 100 score
The hazardous manual work load, as defined by the Work Health and Safety regulations (WHS), is a task that requires a person to lift, lower, push, pull, carry or otherwise move, hold or restrain anything involving one or more of the following: 1. Repetitive or sustained force: Repetitive force like
Lifting, gripping and handling bricks or pressing components. Sustained force like pushing or pulling or carrying objects over long distances
2. high or sudden force: e.g. throwing or catching objects and digging
3. repetitive movement : e.g. painting 4. Sustained or awkward posture: e.g. plumbing or
bending posture. 5. Exposure to vibration: e.g. driving a vehicle over
rough land. 11 All patients were operated using midline posterior
skin incision and subperiosteal retraction of the paraspinal muscles to expose the affected segment.
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery 183
In patients randomized to receive conventional discectomy, a small laminotomy with rarely medial facetectomy were performed if the medial facet was clearly impinging on the nerve root. Exploration is then started to look for annular defect or any free fragments. If the annulus is intact, an oblique 45° incision was made with a number-15 blade and the slit was explored. The disc space was not curetted or debrided deep to the annulus except to remove loose fragments.
In patients randomized to receive TLIF with unilateral spinal fixation. Posterior decompression of the canal and vertebral foramen is done. Unilateral resection of the inferior articular facet of the superior vertebra and the upper part of the superior articular facet of the inferior vertebra is accomplished exposing unilaterally the intervertebral foramen. Then we expose the posterolateral portion of the ipsilateral disc space in the topography of the vertebral foramen. Coagulation (with bipolar) of the small epidural vessels, and visualization and protection of the dura medially was followed. Unilateral Pedicle screws are placed in the standard fashion followed by removal of the disc through the vertebral foramen, and also of the end plates. Harvested local bone is packed in the disk space transforaminally. Final rods of desired length were contoured to the appropriate lordotic curve and are applied over the pedicle screws in compression.
In both groups of patients, duration of surgery, blood loss, and the duration of inpatient treatment were recorded. Intraoperative and perioperative major and minor complications were assessed.
Patients were followed 3 weeks, 3, 6, 9 and 12 months after surgery. During follow up visit the following data were collected: location of pain; intensity of leg and back pain according to the VAS; neurological symptoms; medication, complications, recurrence of symptoms and subsequent spinal surgery.
Assessment of the patients’ clinical outcome were evaluated using the Prolo economic and functional rating scale (Table 1), in which there is a maximum score of 10 points. (Poor, 2–4; fair, 5–6; good, 7–8; and excellent, 9–10 points). Good and excellent results were considered a clinical success. 10 Finally patients were asked to rate their condition has improved, unchanged, or worse; they were also questioned as to whether they would undergo the same procedure again under the same circumstances. An occupational outcome score was designed from the sum of previous items and is used to summarize the data (Table 1).
Radiological interbody fusion in the fusion group was assessed at individual levels as observed on plain radiographs that were obtained postoperatively every three months. We used the criteria approved by the FDA for evaluation of lumbar intervertebral fusions. Fusion was defined as a continuous bone bridge between the vertebrae seen in lateral X- ray. 12- 14
RESULTS
A total of sixty patients (thirty in each group) were included in this study. The demographic data of the two study groups are presented in (Table 2), and showed that the two groups of patients were fairly homogeneous and comparable. The mean age in the Discectomy group was 32.3 years in comparison to 35.2 years in the fusion group. The average BMI was 27.9 in the discectomy group in comparison to 28.9 in the fusion group. The work load exposure to repetitive vibration was the most risk for disc prolapse and surgery (28.3 %) of the study group. A positive smoking history was recorded in sixteen patients of the study group (26.6%) and secondary gain issue was present in 20% of the study group. There is no statistical significant difference between the two groups for these parameters.
Table 2: Preoperative data of the study groups
Discectomy Fusion Total Patients / Sex: 30 male 30 male 60 male Age, yr 32.3 35.2 33.8 Age group
Age 20 - Age 30 - Age 40 - Age 50 -
8
11 7 4
6
12 9 3
14 23 16 7
Occupation repetitive or sustained force high or sudden force repetitive movement sustained or awkward posture Exposure to vibration.
6 5 6 7 8
4 5 5 7 9
10 10 11 14 17,
Body mass index * 27.9 28.9 28.4 Positive smoking history 7 (23.3 %) 9 (30 %) 16 (26.6 %) Secondary gain issue 5 (16.7 %) 7 (23.3 %) 12 (20 %)
* Obesity is defined as BMI that is higher than 30 of the body mass index.
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery
184
On average, patients had preoperative symptoms
duration for 1.5 years (range 0.2–2.9). Patients in the Discectomy group had mean preoperative symptoms duration for 1.3 ± 0.9 years in comparison to 1.6 ± 0.8 years in patients in the fusion group.
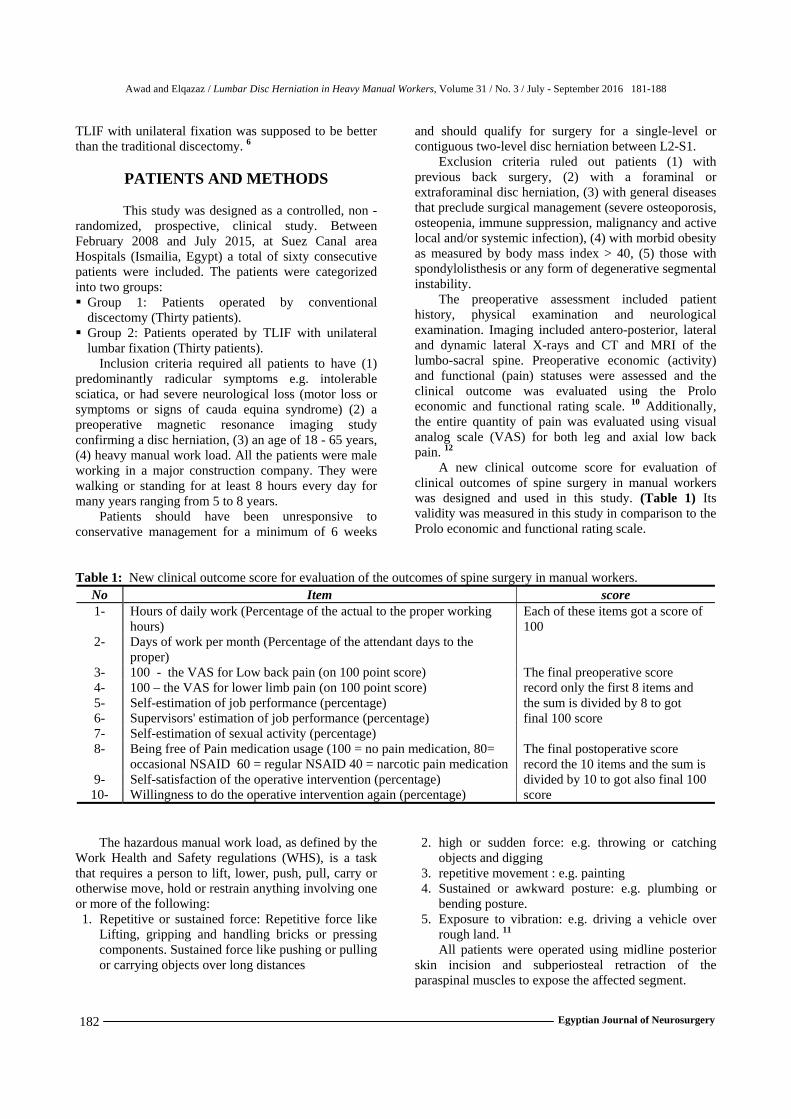
The primary indication for surgery in the whole series was Lumbar disc prolapse. 78.4% of the patients were treated with one-level surgery and 21.6% were treated with two-level surgery. Figure 1 shows distribution of the operative level by the level of the construct within the two study groups. About 46.6% of surgeries were done at L4-5 level.
Fig. 1: Distribution of level of surgery in the two
groups of patients
In regard to the perioperative findings in the 2 groups, the discectomy group showed less intraoperative blood loss, shorter operative time and hospital stay in comparison to the fusion group and this was statistically significant. (Table 3) Table 3: Peri operative data of the study groups
Discectomy group
Fusion Group
Blood Loss (ml) 250 ± 60 (170-460)
442 ± 80 (300-750)
Surgical Time (min) 75 ± 20 (50- 95)
130 ± 50 (100-180)
Days in hospital 1.7 ± 2.8 (1-11)
2.4 ± 1.5 (2 – 10)
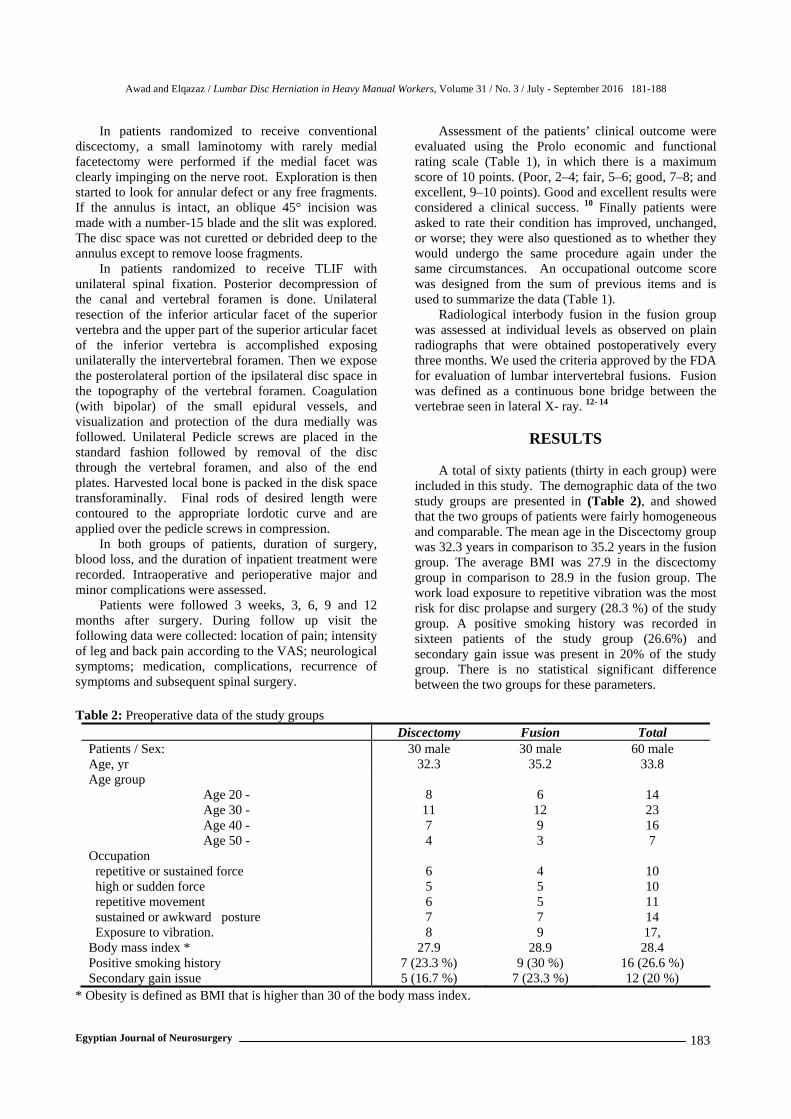
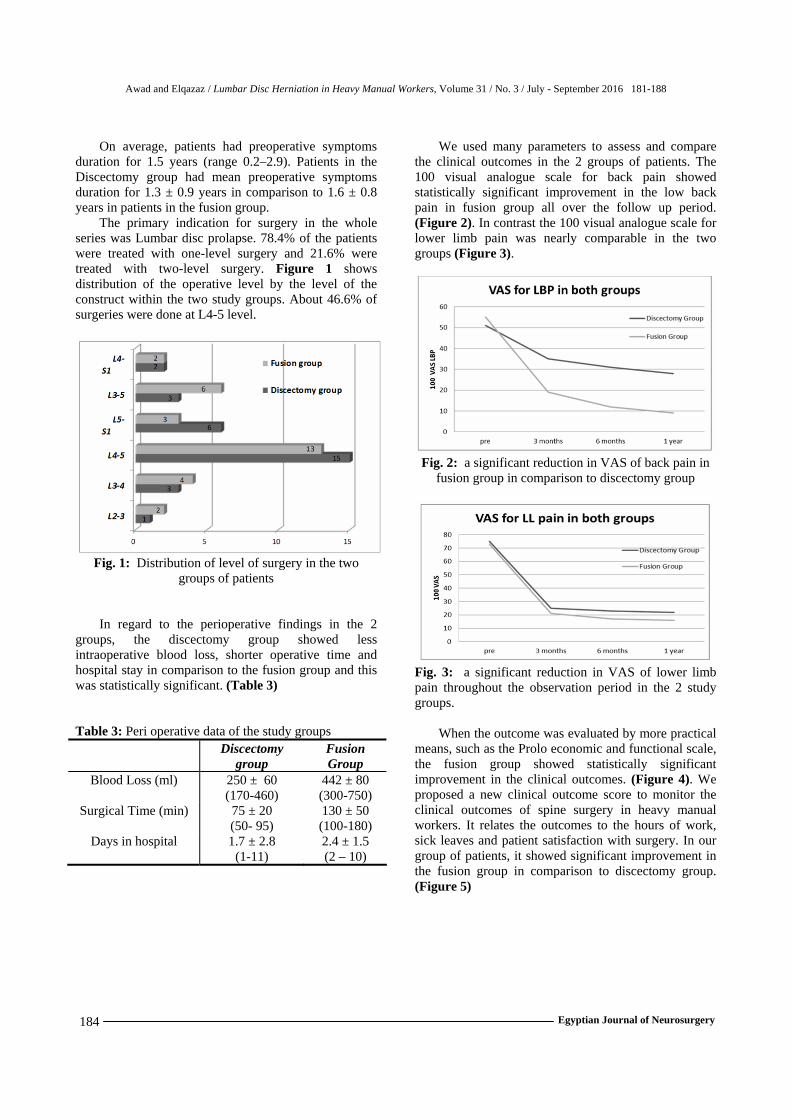
We used many parameters to assess and compare the clinical outcomes in the 2 groups of patients. The 100 visual analogue scale for back pain showed statistically significant improvement in the low back pain in fusion group all over the follow up period. (Figure 2). In contrast the 100 visual analogue scale for lower limb pain was nearly comparable in the two groups (Figure 3).
Fig. 2: a significant reduction in VAS of back pain in
fusion group in comparison to discectomy group
Fig. 3: a significant reduction in VAS of lower limb pain throughout the observation period in the 2 study groups.
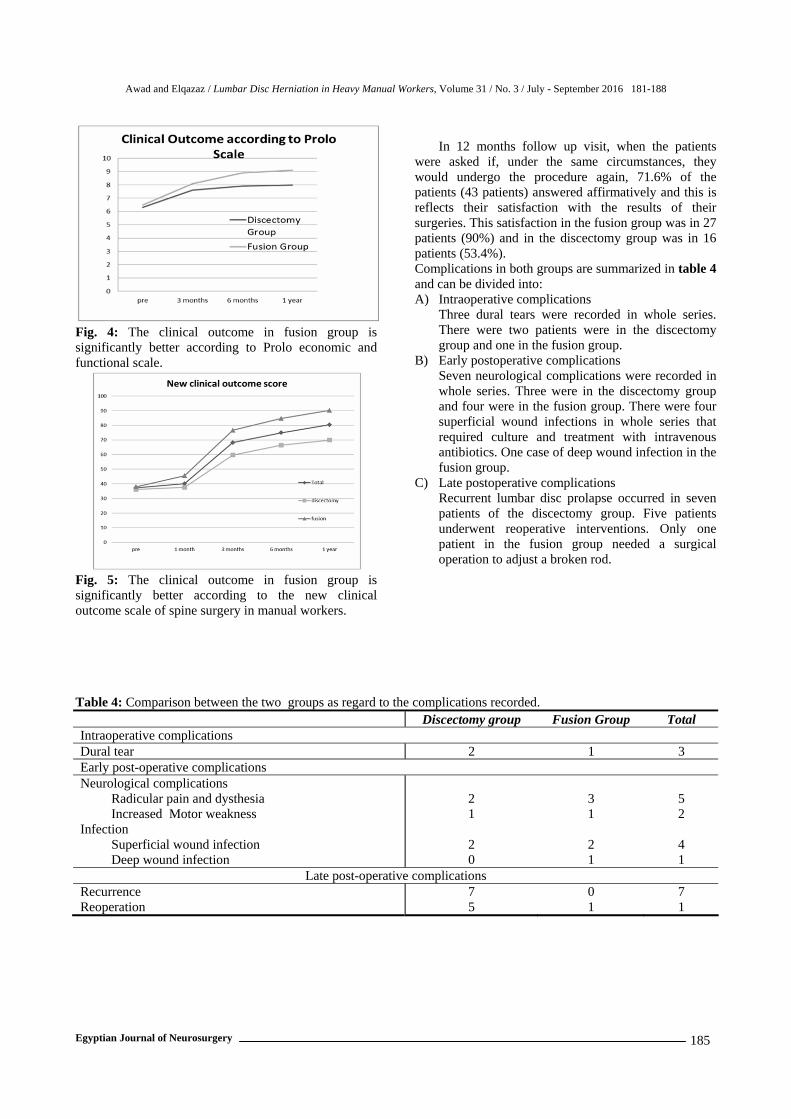
When the outcome was evaluated by more practical means, such as the Prolo economic and functional scale, the fusion group showed statistically significant improvement in the clinical outcomes. (Figure 4). We proposed a new clinical outcome score to monitor the clinical outcomes of spine surgery in heavy manual workers. It relates the outcomes to the hours of work, sick leaves and patient satisfaction with surgery. In our group of patients, it showed significant improvement in the fusion group in comparison to discectomy group. (Figure 5)
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery 185
Fig. 4: The clinical outcome in fusion group is significantly better according to Prolo economic and functional scale.
Fig. 5: The clinical outcome in fusion group is significantly better according to the new clinical outcome scale of spine surgery in manual workers.
In 12 months follow up visit, when the patients
were asked if, under the same circumstances, they would undergo the procedure again, 71.6% of the patients (43 patients) answered affirmatively and this is reflects their satisfaction with the results of their surgeries. This satisfaction in the fusion group was in 27 patients (90%) and in the discectomy group was in 16 patients (53.4%). Complications in both groups are summarized in table 4 and can be divided into: A) Intraoperative complications
Three dural tears were recorded in whole series. There were two patients were in the discectomy group and one in the fusion group.
B) Early postoperative complications Seven neurological complications were recorded in whole series. Three were in the discectomy group and four were in the fusion group. There were four superficial wound infections in whole series that required culture and treatment with intravenous antibiotics. One case of deep wound infection in the fusion group.
C) Late postoperative complications Recurrent lumbar disc prolapse occurred in seven patients of the discectomy group. Five patients underwent reoperative interventions. Only one patient in the fusion group needed a surgical operation to adjust a broken rod.
Table 4: Comparison between the two groups as regard to the complications recorded. Discectomy group Fusion Group Total
Intraoperative complications Dural tear 2 1 3 Early post-operative complications Neurological complications
Radicular pain and dysthesia Increased Motor weakness
Infection Superficial wound infection Deep wound infection
2 1
2 0
3 1
2 1
5 2
4 1
Late post-operative complications Recurrence Reoperation
7 5
0 1
7 1
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery
186
a b
c
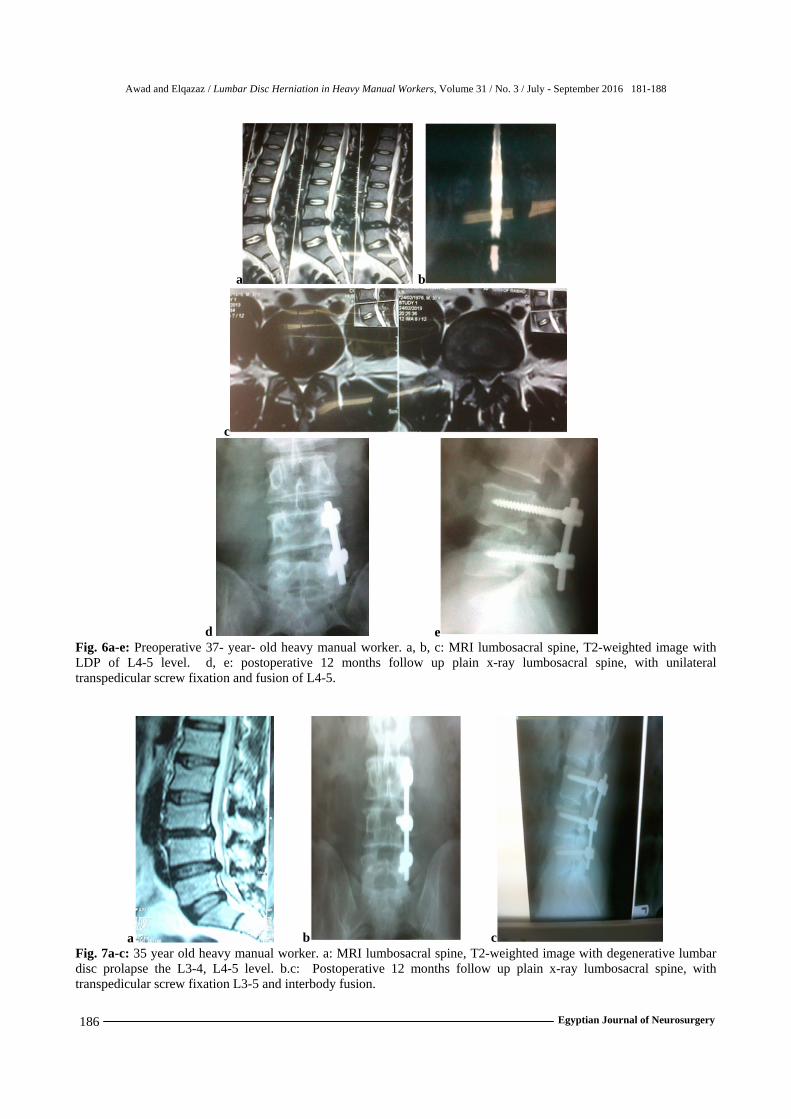
d e Fig. 6a-e: Preoperative 37- year- old heavy manual worker. a, b, c: MRI lumbosacral spine, T2-weighted image with LDP of L4-5 level. d, e: postoperative 12 months follow up plain x-ray lumbosacral spine, with unilateral transpedicular screw fixation and fusion of L4-5.
a b c Fig. 7a-c: 35 year old heavy manual worker. a: MRI lumbosacral spine, T2-weighted image with degenerative lumbar disc prolapse the L3-4, L4-5 level. b.c: Postoperative 12 months follow up plain x-ray lumbosacral spine, with transpedicular screw fixation L3-5 and interbody fusion.
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery 187
DISCUSSION
Lumbar disc prolapse in heavy manual workers is
an important and new issue to discuss. These patients are subjected to different preoperative and postoperative demands during heavy duties. The work load exposure to repetitive vibration was the most risk for disc prolapse and surgery (28.3%) according to our results. In addition the morphology of lumbar disc prolapse in heavy manual workers is different from the general population. Unfortunately Most of heavy manual workers have disc herniation with large defects which had 27% recurrent herniation rate and ultimately a 21% reoperation rate if treated by discectomy alone. 8 To overcome these factors, TLIF with unilateral fixation was supposed to be better than the traditional discectomy
In the guide lines for performance of fusion procedure for disc herniation and radiculopathy, both 2005 and 2014 statements recommend based on low-level evidence, the incorporation of a lumbar fusion may be considered an option when a herniation is associated with evidence of spinal instability, chronic low-back pain, and/or severe degenerative changes, or if the patient participates in heavy manual labor. Lumbar spinal fusion is a potential option in patients with herniated discs who have evidence of significant chronic axial back pain, work as manual laborers, have severe degenerative changes, or have instability associated with radiculopathy caused by herniated lumbar discs (Level IV evidence). 16
In a meta-analysis to more accurately estimate the effectiveness of unilateral versus bilateral pedicle screw fixation in lumbar spinal fusion. A total of nine studies involving 567 patients were included. Unilateral pedicle screw fixation was performed in 287 patients and bilateral pedicle screw fixation in 280 patients. The results indicated that In comparison with bilateral fixation, unilateral fixation can shorten the operation time, reduce the amount of bleeding, and reduce medical expenses. There were similar effects with regard to hospitalization days, fusion rate, complication rate, and excellent and good rates. This is true for one or two segmental lumbar spinal fusion. 17
In similar article to our study, 40 single-level lumbar disc herniation cases were treated with limited posterior lumbar microdiscectomy and posterior dynamic stabilization. It was observed that performing discectomy with posterior dynamic stabilization decreased the risk of recurrent disc herniations in Carragee type II, III, and IV groups, which had increased reherniation and persistent/continuous sciatica after limited lumbar microdiscectomy. 18-20
CONCLUSION
Heavy manual workers treated with unilateral transforaminal interbody fusion reported less pain & lower disability scores all over the follow up period. This technique is preferable to conventional discectomy because it decreases back & leg pain while avoiding the possibility of recurrence by heavy duties and it maintains stability of the lumbar spine. Long-term follow up studies are crucial to support the recommendation of this technique as the ideal method for treating heavy manual workers. Declaration
The author(s) declare no conflict of interest or any financial support and confirm the approval of the submitted article by the concerned ethical committee.
REFERENCES 1. Bernhardt M. Normal spinal anatomy: Normal
sagittal plane alignment. In: Bridwell KH, DeWald RL, eds: The Textbook of Spinal Surgery. Philadelphia: Lippincott–Raven; 185–191, 1997
2. Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM: Complications and predictive factors for the successful treatment of flat back deformity (fixed sagittal imbalance). Spine 24:1712–1720, 1999
3. Dubois B, de Germay B, Schaerer NS, Fennema P: Dynamic neutralization: A new concept for restabilization of the spine, in Szpalski M, Gunzburg R, Pope MH, (ed): Lumbar Segmental Instability. Philadelphia: Lippincott Williams & Wilkins, Ch 23, pp 233–240, 1999
4. Farcy FB, Schwab FJ: Management of flat back and related kyphotic decompensation syndromes. Spine 22:2452–2457, 1997.
5. Gelb DE, Lenke LG, Bridwell KH, Blanke K, McEnery KW: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 20:1351–1358, 1995
6. Grob D, Benini A, Junge A, Mannion AF: Clinical experience with the Dynesys semi rigid fixation system for the lumbar spine surgical and patient-oriented outcome in 50 Cases after an Average of 2 Years. Spine 30:324–331, 2005
7. Vredeveld T, Teitsma X, Mert A, and Van der Wurff P: Prevalence of Modic changes in active duty military men with lumbar disc who were scheduled for surgery. J Manipulative and Physiological Therapeutics 35, 2012
8. Carragee E, Han M, Suen P, Kim D: Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and annular competence. J Bone and Joint Surgery 85-A: 1, 2003
9. Jinkins JR: The related consequences of acquired collapse of the intervertebral discs at and
Awad and Elqazaz / Lumbar Disc Herniation in Heavy Manual Workers, Volume 31 / No. 3 / July - September 2016 181-188
Egyptian Journal of Neurosurgery
188
superjacent to the lumbosacral junction. Riv Neuroradiol 12:15–26, 1999
10. Prolo DJ, Oklund SA, Butcher M: Toward uniformity in evaluating results of lumbar spine operations. A paradigm applied to posterior lumbar interbody fusions. Spine 11: 601-606; 1986
11. Chapman CR, Casey KL, Dubner R: Pain measurement: an overview. Pain 22:1–31, 1985
12. Hazardous manual tasks (www.legislation.nsw.gov.au). Page 5. [Accessed October 11, 2015]
13. Brantigan JW: Carbon fiber I/F Cage system for interbody vertebral Fusion. In Haid RW, Mclaughlin MR, Fessler RG. Lumbar Interbody Fusion Techniques. Cages, Dowels, and Grafts. Quality Medical publishing, Inc. ST. Louis, Missori.Ch 19, pp 247-271, 2003
14. Tullberg T, Brandt B, Rydberg J, et al: Fusion rate after posterior lumbar interbody fusion with carbon fiber implant: l-year follow-up of 51 patients. Eur Spine J 5: 178-182, 1996
15. Umehara S, Zindrick MR, Patwardhan AG, Havey RM, Vrbos LA, Knight GW, et al.: The biomechanical effect of postoperative hypolordosis in instrumented lumbar fusion on instrumented and adjacent spinal segments. Spine 25:1617–1624, 2000
16. Wang JC, Dailey AT, Mummaneni PV, Ghogawala Z, Resnick DK, Watters WC 3rd, et al. Guideline for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 8: lumbar fusion for disc herniation and radiculopathy. J Neurosurg Spine 21:48-53, 2014
17. Hu XQ, Wu XL, Xu C, Zheng XH, Jin YL, Wu LJ, Wang XY, Xu HZ, Tian NF. A systematic review and meta-analysis of unilateral versus bilateral pedicle screw fixation in transforaminal lumbar interbody fusion. PLoS One, 29; 9: 2014
18. Kaner T, Sasani M, Oktenoglu T, Cosar M, Ozer A. Clinical outcomes after posterior dynamic transpedicular stabilization with limited lumbar discectomy: Carragee classification system for lumbar disc herniations. SAS Journal 4: 92–97, 2010
19. Hiett JM, Chan D, Clarke A., Challinor H, Hourigan P: Research. Returning to work and driving after spinal surgery: A web based survey investigating the opinions of UK spinal surgeons. International Journal of Therapy & Rehabilitation 22: 181-186 2015
20. Topuz K, Ergoglu A, Simsek H, Atabey C, Çetinkal A, Çolak A: Demographical Aspects of Central Large Lumbar Disc Herniation. Turkish Neurosurgery 26:111-118, 2015










![Disc Herniation Mobilization Comparisons · Lumbar disc herniation (LDH) is a common condition which frequently affects the spine in young and middle-aged patients [1-3]; it is one](https://img.pdfslide.net/doc/110x75/5c9206dd09d3f21a578ca604/disc-herniation-mobilization-comparisons-lumbar-disc-herniation-ldh-is-a-common.jpg)

![Percutaneous Endoscopic Lumbar Spine Surgery for …1.1. Lumbar Disc Herniation (LDH) Lumbar disc herniation [1][2] [3] (Figure 1(a)) is a medical condition affecting the spine in](https://img.pdfslide.net/doc/110x75/5f01e5a17e708231d4019244/percutaneous-endoscopic-lumbar-spine-surgery-for-11-lumbar-disc-herniation-ldh.jpg)