Embed Size (px)
Citation preview

AJR:182, April 2004
1051
Original Report
OBJECTIVE.
We sought to describe the radiographic and imaging features of cherubism.
CONCLUSION.
Cherubism is a rare osseous disorder of children and adolescents. Al-though the radiologic characteristics of cherubism are not pathognomonic, the diagnosis isstrongly suggested by bilateral relatively symmetric jaw involvement that is limited to the maxillaand mandible. Imaging typically shows expansile remodeling of the involved bones, thinning ofthe cortexes, and multilocular radiolucencies with a coarse trabecular pattern.
herubism is a benign disease ofchildhood characterized by osseousinvolvement limited specifically to
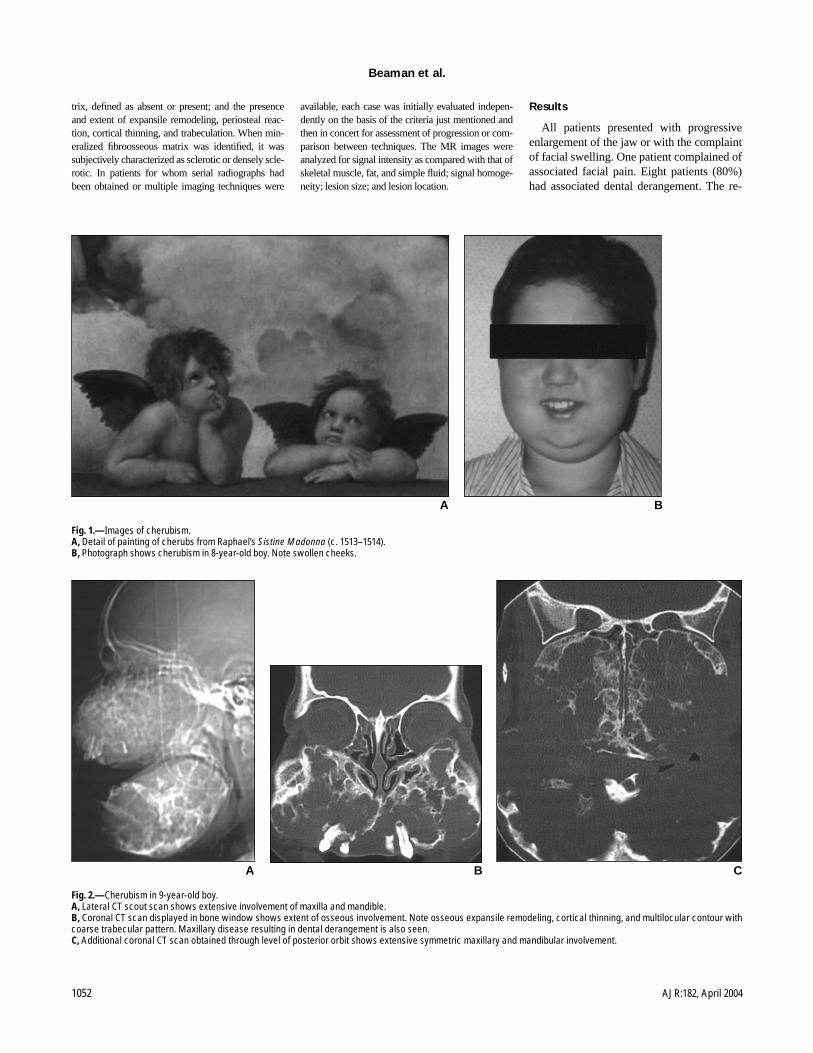
the mandible and maxilla. It was first describedin 1933 by Jones [1] as “familial multilocularcystic disease of the jaws,” but the term“cherubism” was later coined to describe therounded facial appearance resulting from jawhypertrophy that was reminiscent of cherubs de-picted throughout Renaissance art (Fig. 1A).The condition was initially characterized as fa-milial, but both hereditary and sporadic caseshave since been described.
Bilateral mandibular involvement is a distin-guishing feature; only one case report in the lit-erature describes unilateral involvement, in anadolescent [2]. Children typically present asearly as 2–3 years old with nontender enlarge-ment of the jaw. The lesions characteristicallycontinue a pattern of variable enlargement untilpuberty, and then they partially or fully regressand show sclerotic involution in adulthood.
Cherubism is similar to fibrous dysplasiaradiographically, especially when the latter isconfined to the jaw. The similarity in appear-ance has prompted the suggestion thatcherubism may be a familial form of fibrousdysplasia localized to the jaw [3–5]. Wepresent our experience with 10 cases ofcherubism and describe its radiographic andimaging features.
Materials and Methods
This study was conducted with the approval ofthe Mayo Clinic institutional review board, in ac-cordance with the requirements for a retrospectivereview; informed consent was not required.
Six patients were selected through an archivalsearch of institutional records via a review of com-puter-generated patient diagnoses. Four additionalpatients were identified from the archives of theArmed Forces Institute of Pathology. The diagno-sis of cherubism was based in all cases on a com-bination of histopathologic features, skeletaldistribution of lesions, and patient age.
The study group consisted of 10 patients, sixmales and four females, 5–19 years old (mean,13.5 years). One patient’s age was unknown. Im-aging types reviewed included radiography (
n
=5), unenhanced CT (
n
= 5), and unenhanced MRI(
n
= 1). MR images included spin-echo T1-weighted images and fast spin-echo T2-weightedimages with fat suppression. Two patients under-went serial radiography, and one patient under-went both CT and MRI. Three-dimensional CTreconstruction was available in one case. None ofthe patients who underwent CT or MRI examina-tions underwent radiography.
The clinical history and imaging characteristicswere reviewed for each patient. Clinical review incor-porated the documentation of sex and age at the timeof imaging; physical findings, specifically dental de-rangement; and family history. Radiographic and CTfeatures included assessment for bilaterality; location,in the mandible and maxilla; extent of involvement;margin, between involved and uninvolved bone; ma-
Francesca D. Beaman
1
Laura W. Bancroft
1
Jeffrey J. Peterson
1
Mark J. Kransdorf
1,2
Mark D. Murphey
2–4
David M. Menke
5
Received July 21, 2003; accepted after revision September 22, 2003.
Presented at the 2003 annual meeting of the American Roentgen Ray Society, San Diego, CA.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
1
Department of Radiology, Mayo Clinic, 4500 San Pablo Rd., Jacksonville, FL 32224-3899. Address correspondence to M. J. Kransdorf.
2
Department of Radiologic Pathology, Armed Forces Institute of Pathology, Walter Reed Army Medical Center, 6825 16th St. NW, Bldg. 54, Washington, DC 20306-6000.
3
Department of Radiology and Nuclear Medicine, Uniformed Services University of the Health Sciences, 4301 Jones Bridge Rd., Bethesda, MD 20814-4799.
4
Department of Radiology, University of Maryland School of Medicine, 22 S Greene St., Baltimore, MD 21201-1595.
5
Department of Pathology, Mayo Clinic, Jacksonville, FL 32224-3899.
AJR
2004;182:1051–1054
0361–803X/04/1824–1051
© American Roentgen Ray Society
C
Imaging Characteristics of Cherubism
1052
AJR:182, April 2004
Beaman et al.
trix, defined as absent or present; and the presenceand extent of expansile remodeling, periosteal reac-tion, cortical thinning, and trabeculation. When min-eralized fibroosseous matrix was identified, it wassubjectively characterized as sclerotic or densely scle-rotic. In patients for whom serial radiographs hadbeen obtained or multiple imaging techniques were
available, each case was initially evaluated indepen-dently on the basis of the criteria just mentioned andthen in concert for assessment of progression or com-parison between techniques. The MR images wereanalyzed for signal intensity as compared with that ofskeletal muscle, fat, and simple fluid; signal homoge-neity; lesion size; and lesion location.
Results
All patients presented with progressiveenlargement of the jaw or with the complaintof facial swelling. One patient complained ofassociated facial pain. Eight patients (80%)had associated dental derangement. The re-
Fig. 1.—Images of cherubism.A, Detail of painting of cherubs from Raphael’s Sistine Madonna (c. 1513–1514).B, Photograph shows cherubism in 8-year-old boy. Note swollen cheeks.
BA
BA
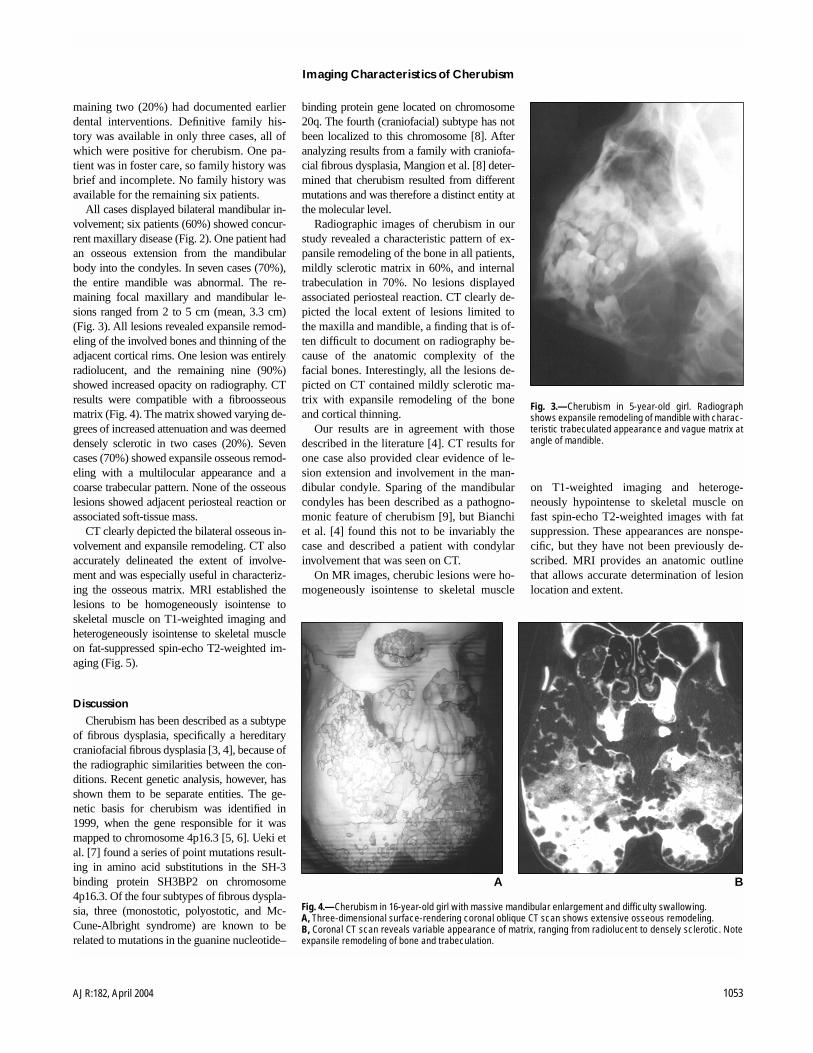
Fig. 2.—Cherubism in 9-year-old boy.A, Lateral CT scout scan shows extensive involvement of maxilla and mandible.B, Coronal CT scan displayed in bone window shows extent of osseous involvement. Note osseous expansile remodeling, cortical thinning, and multilocular contour withcoarse trabecular pattern. Maxillary disease resulting in dental derangement is also seen.C, Additional coronal CT scan obtained through level of posterior orbit shows extensive symmetric maxillary and mandibular involvement.
C
Imaging Characteristics of Cherubism
AJR:182, April 2004
1053
maining two (20%) had documented earlierdental interventions. Definitive family his-tory was available in only three cases, all ofwhich were positive for cherubism. One pa-tient was in foster care, so family history wasbrief and incomplete. No family history wasavailable for the remaining six patients.
All cases displayed bilateral mandibular in-volvement; six patients (60%) showed concur-rent maxillary disease (Fig. 2). One patient hadan osseous extension from the mandibularbody into the condyles. In seven cases (70%),the entire mandible was abnormal. The re-maining focal maxillary and mandibular le-sions ranged from 2 to 5 cm (mean, 3.3 cm)(Fig. 3). All lesions revealed expansile remod-eling of the involved bones and thinning of theadjacent cortical rims. One lesion was entirelyradiolucent, and the remaining nine (90%)showed increased opacity on radiography. CTresults were compatible with a fibroosseousmatrix (Fig. 4). The matrix showed varying de-grees of increased attenuation and was deemeddensely sclerotic in two cases (20%). Sevencases (70%) showed expansile osseous remod-eling with a multilocular appearance and acoarse trabecular pattern. None of the osseouslesions showed adjacent periosteal reaction orassociated soft-tissue mass.
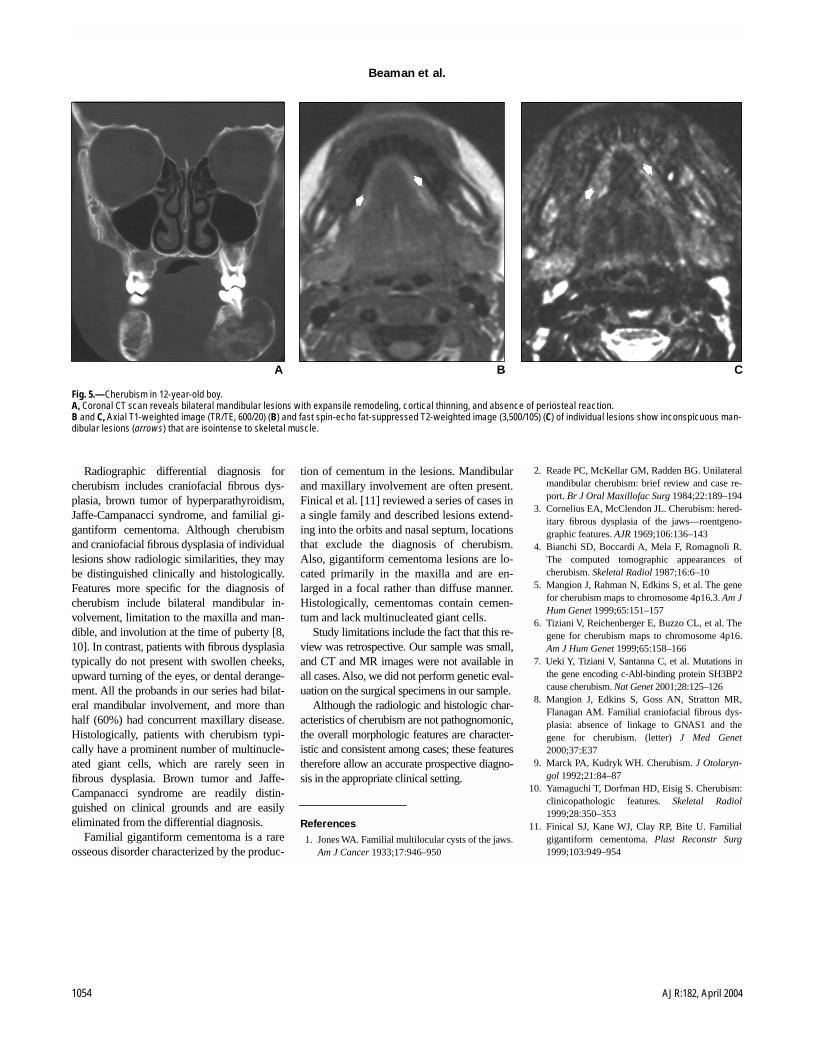
CT clearly depicted the bilateral osseous in-volvement and expansile remodeling. CT alsoaccurately delineated the extent of involve-ment and was especially useful in characteriz-ing the osseous matrix. MRI established thelesions to be homogeneously isointense toskeletal muscle on T1-weighted imaging andheterogeneously isointense to skeletal muscleon fat-suppressed spin-echo T2-weighted im-aging (Fig. 5).
Discussion
Cherubism has been described as a subtypeof fibrous dysplasia, specifically a hereditarycraniofacial fibrous dysplasia [3, 4], because ofthe radiographic similarities between the con-ditions. Recent genetic analysis, however, hasshown them to be separate entities. The ge-netic basis for cherubism was identified in1999, when the gene responsible for it wasmapped to chromosome 4p16.3 [5, 6]. Ueki etal. [7] found a series of point mutations result-ing in amino acid substitutions in the SH-3binding protein SH3BP2 on chromosome4p16.3. Of the four subtypes of fibrous dyspla-sia, three (monostotic, polyostotic, and Mc-Cune-Albright syndrome) are known to berelated to mutations in the guanine nucleotide–
binding protein gene located on chromosome20q. The fourth (craniofacial) subtype has notbeen localized to this chromosome [8]. Afteranalyzing results from a family with craniofa-cial fibrous dysplasia, Mangion et al. [8] deter-mined that cherubism resulted from differentmutations and was therefore a distinct entity atthe molecular level.
Radiographic images of cherubism in ourstudy revealed a characteristic pattern of ex-pansile remodeling of the bone in all patients,mildly sclerotic matrix in 60%, and internaltrabeculation in 70%. No lesions displayedassociated periosteal reaction. CT clearly de-picted the local extent of lesions limited tothe maxilla and mandible, a finding that is of-ten difficult to document on radiography be-cause of the anatomic complexity of thefacial bones. Interestingly, all the lesions de-picted on CT contained mildly sclerotic ma-trix with expansile remodeling of the boneand cortical thinning.
Our results are in agreement with thosedescribed in the literature [4]. CT results forone case also provided clear evidence of le-sion extension and involvement in the man-dibular condyle. Sparing of the mandibularcondyles has been described as a pathogno-monic feature of cherubism [9], but Bianchiet al. [4] found this not to be invariably thecase and described a patient with condylarinvolvement that was seen on CT.
On MR images, cherubic lesions were ho-mogeneously isointense to skeletal muscle
on T1-weighted imaging and heteroge-neously hypointense to skeletal muscle onfast spin-echo T2-weighted images with fatsuppression. These appearances are nonspe-cific, but they have not been previously de-scribed. MRI provides an anatomic outlinethat allows accurate determination of lesionlocation and extent.
Fig. 3.—Cherubism in 5-year-old girl. Radiographshows expansile remodeling of mandible with charac-teristic trabeculated appearance and vague matrix atangle of mandible.
Fig. 4.—Cherubism in 16-year-old girl with massive mandibular enlargement and difficulty swallowing. A, Three-dimensional surface-rendering coronal oblique CT scan shows extensive osseous remodeling.B, Coronal CT scan reveals variable appearance of matrix, ranging from radiolucent to densely sclerotic. Noteexpansile remodeling of bone and trabeculation.
BA
1054
AJR:182, April 2004
Beaman et al.
Radiographic differential diagnosis forcherubism includes craniofacial fibrous dys-plasia, brown tumor of hyperparathyroidism,Jaffe-Campanacci syndrome, and familial gi-gantiform cementoma. Although cherubismand craniofacial fibrous dysplasia of individuallesions show radiologic similarities, they maybe distinguished clinically and histologically.Features more specific for the diagnosis ofcherubism include bilateral mandibular in-volvement, limitation to the maxilla and man-dible, and involution at the time of puberty [8,10]. In contrast, patients with fibrous dysplasiatypically do not present with swollen cheeks,upward turning of the eyes, or dental derange-ment. All the probands in our series had bilat-eral mandibular involvement, and more thanhalf (60%) had concurrent maxillary disease.Histologically, patients with cherubism typi-cally have a prominent number of multinucle-ated giant cells, which are rarely seen infibrous dysplasia. Brown tumor and Jaffe-Campanacci syndrome are readily distin-guished on clinical grounds and are easilyeliminated from the differential diagnosis.
Familial gigantiform cementoma is a rareosseous disorder characterized by the produc-
tion of cementum in the lesions. Mandibularand maxillary involvement are often present.Finical et al. [11] reviewed a series of cases ina single family and described lesions extend-ing into the orbits and nasal septum, locationsthat exclude the diagnosis of cherubism.Also, gigantiform cementoma lesions are lo-cated primarily in the maxilla and are en-larged in a focal rather than diffuse manner.Histologically, cementomas contain cemen-tum and lack multinucleated giant cells.
Study limitations include the fact that this re-view was retrospective. Our sample was small,and CT and MR images were not available inall cases. Also, we did not perform genetic eval-uation on the surgical specimens in our sample.
Although the radiologic and histologic char-acteristics of cherubism are not pathognomonic,the overall morphologic features are character-istic and consistent among cases; these featurestherefore allow an accurate prospective diagno-sis in the appropriate clinical setting.
References
1. Jones WA. Familial multilocular cysts of the jaws.
Am J Cancer
1933;17:946–950
2. Reade PC, McKellar GM, Radden BG. Unilateralmandibular cherubism: brief review and case re-port.
Br J Oral Maxillofac Surg
1984;22:189–1943. Cornelius EA, McClendon JL. Cherubism: hered-
itary fibrous dysplasia of the jaws—roentgeno-graphic features.
AJR
1969;106:136–1434. Bianchi SD, Boccardi A, Mela F, Romagnoli R.
The computed tomographic appearances ofcherubism.
Skeletal Radiol
1987;16:6–105. Mangion J, Rahman N, Edkins S, et al. The gene
for cherubism maps to chromosome 4p16.3.
Am JHum Genet
1999;65:151–1576. Tiziani V, Reichenberger E, Buzzo CL, et al. The
gene for cherubism maps to chromosome 4p16.
Am J Hum Genet
1999;65:158–1667. Ueki Y, Tiziani V, Santanna C, et al. Mutations in
the gene encoding c-Abl-binding protein SH3BP2cause cherubism.
Nat Genet
2001;28:125–1268. Mangion J, Edkins S, Goss AN, Stratton MR,
Flanagan AM. Familial craniofacial fibrous dys-plasia: absence of linkage to GNAS1 and thegene for cherubism. (letter)
J Med Genet
2000;37:E379. Marck PA, Kudryk WH. Cherubism.
J Otolaryn-gol
1992;21:84–8710. Yamaguchi T, Dorfman HD, Eisig S. Cherubism:
clinicopathologic features.
Skeletal Radiol
1999;28:350–35311. Finical SJ, Kane WJ, Clay RP, Bite U. Familial
gigantiform cementoma.
Plast Reconstr Surg
1999;103:949–954
Fig. 5.—Cherubism in 12-year-old boy. A, Coronal CT scan reveals bilateral mandibular lesions with expansile remodeling, cortical thinning, and absence of periosteal reaction.B and C, Axial T1-weighted image (TR/TE, 600/20) (B) and fast spin-echo fat-suppressed T2-weighted image (3,500/105) (C) of individual lesions show inconspicuous man-dibular lesions (arrows) that are isointense to skeletal muscle.
BA C








![Investigation of the SH3BP2 Gene Mutation in Cherubism · genetic advances have been made in relation to cherubism with the identification of the gene SH3BP2 [2, 5]. SH3BP2 was initially](https://img.pdfslide.net/doc/110x75/5ed57c2b0bd3843450408d1d/investigation-of-the-sh3bp2-gene-mutation-in-genetic-advances-have-been-made-in.jpg)

![PUBLISHED VERSION Constrained density functional for ... · Althoughabinitiocalculationsoftenassumecollinearmag-netic configurations, spin-polarized density functional theory (DFT)[20]doesnotimposeanyconstraintsonthedirectionsof](https://img.pdfslide.net/doc/110x75/5b4935857f8b9a3a058d522d/published-version-constrained-density-functional-for-althoughabinitiocalculationsoftenassumecollinearmag-netic.jpg)


















![The Time&Averaged Paleomagnetic Field · netic studies [e.g., Hospets, 1954; Cox and Doell, 1960; Irving, 1964; Opdyke and Henry, 1969] and archeomag- netic investigation [Champion,](https://img.pdfslide.net/doc/110x75/610d3346ea5efe04b0355db7/the-timeaveraged-paleomagnetic-field-netic-studies-eg-hospets-1954-cox.jpg)