Embed Size (px)
Citation preview

1
Conquering Osteoarthritis
By Tamara Mitchell
Osteoarthritis (OA) is not a repetitive strain injury, but it definitely compounds the problems of
RSI and shares the symptoms of inflammation and pain. OA can be caused by aging, heredity,
injury from trauma or overuse, or disease.1,2 It is the most common type of arthritis.1 OA is
degeneration of the cartilage which leads to inflammation, pain, and stiffness of the joints.3
Cartilage is spongy and filled with synovial fluid which lubricates the joints as they move. With
OA, the water content of cartilage increases, the protein of the cartilage degenerates, and the
cartilage starts to wear away and flake off.1 Inflammation of the cartilage can stimulate new bone
outgrowths or spurs called osteophytes.1
Illustration courtesy of MedicineNet.com
The symptoms of OA are swollen joints, joint stiffness, joint creaking, and loss of range of motion.1
There is no blood test for diagnosing OA.1 Diagnosis of osteoarthritis is made by determining if
symptoms are present: cracking and popping, inflammation of joints, reduced range of motion, pain
and tenderness when joints are moved or pressed on. X-rays of the affected joints will show
reduced space within joints, wear at ends of the bones and/or bone spurs.
OA most commonly affects the hands, feet, spine, and large weight-bearing joins such as the hips
and knees.1 OA doesn’t spread throughout the body, but only affects the joints that have
deteriorated.4 Where bone spurs have developed in the spine, nerves exiting the spine may be
irritated causing numbness, tingling, and severe pain in the back or limbs.4 Individuals vary widely
with regard to disability which is not necessarily related to the severity of the condition.4 In other
words, what looks severe in x-rays does not necessarily mean the person feels a lot of pain or vise
versa. Symptoms are often intermittent.4

2
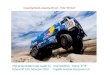
Healthy cartilage has four layers:5,6
Illustration courtesy of Reference 6
• Superficial layer – Flat and spindle-shaped cells parallel to the joint surface containing
mostly collagen fibers with high tensile mobility. In mild OA, some roughening and
thickening of this layer occurs.5
• Intermediate layer – Cells are rounded and larger than the superficial layer with more
proteoglycans and less collagen, with thicker more randomly spaced fibers.5 This layer
supports compression forces in the joint. As OA advances, this layer and the deep layer
become more disrupted, abnormal cells develop, and inflammatory cells appear.6
• Radial or Deep layer – Cells are rounded and are similar to the intermediate layer, but are
arranged in a columnar fashion perpendicular to the surface, also providing resistance to
compressive forces.6 Water content is less than the upper two layers and proteoglycans are
the most abundant.6
• Calcified layer – The calcified layer has few cells and the purpose of this layer is to anchor
the cartilage to the bone. In very advanced cases of OA, cartilage is lacking completely
and the bone is exposed.5
Cartilage of the joints has no blood vessels and no nerves, so nutrients are transported to the tissues
via the synovial fluid in the joint.5 Repair can be done in a limited fashion through regeneration of
the collagen matrix in healthy cartilage with minor injury.5 This is why it is important to prevent
injury and improve regeneration capacities of joint cartilage in the early stages.5
Primary OA is due to aging and hereditary factors, not injury or disease.1 One hereditary factor
includes a defect in the way the body produces collagen, the protein that makes up cartilage.2
Another inherited trait is the way bones are shaped and fit together so the cartilage wears away
faster in certain spots.2
Secondary OA is brought on by other factors including obesity, repeated trauma, surgery on the
joint, abnormal joints at birth, diabetes, or growth hormone disorders.1,2

3
Heberden’s nodes are hard bony enlargements in the fingers which may form with OA.
They are not necessarily painful, but do limit movement of the fingers.6
Photo courtesy of Wikipdedia.org
OA is not related to rheumatoid arthritis or other types of arthritis.1 There are over 100 types of
arthritis!9 Rheumatoid arthritis is a systemic autoimmune disease where the body’s immune system
attacks its own tissues leading to inflammation of the joints and around other organs.1,7 Blood tests
can show if rheumatoid arthritis is likely, however no tests are available for osteoarthritis.
Factors contributing to OA.
Clearly, if you’re overweight, have played contact sports, you are sedentary, your dietary habits are
poor, and you’re getting older, the likelihood of developing OA are relatively high. The most
common symptom of osteoarthritis is pain in the joints after repetitive use or after periods of
inactivity, such as sitting in a theatre or at a computer for a while. Joint pain is usually worse later
in the day.1 We can’t do anything about growing older or undo old sports injuries, but we can do
something about our weight and current habits.
Obesity and overweight. Obesity is the second most powerful risk factor for osteoarthritis of the
knees with aging being the first risk factor.1 Every extra pound you carry can have the impact of
four pounds of pressure on your knees and hips as you move.7 No research has actually shown that
losing weight will slow the progression of osteoarthritis, but it is clear that extra body weight adds
to the strain on the joints in the back and lower body.7 Research has shown a link between
overweight and OA in the hands.2 Fat tissues in the body actually produce chemicals (cytokines)
that increase inflammation and can damage the joints.2 So there appears to be two different ways
obesity contributes to OA:
1. through adding mechanical stress to the joints and triggering localized low-grade
inflammation in the joints (mechainflammation)
2. through metabolic stress, activation of inflammation through the metabolic system leading
to systemic low-grade inflammation, rather than localized inflammation
(metainflammation).8
Looking at the contributions of weight loss versus increase in inflammatory proteins as factors in
pain and function of obese subjects, research has found that weight loss actually had no effect on
pain and only a 4% improvement in functionality.9 A decrease in inflammatory proteins resulted
in a 15% decrease in pain and a 29% increase in functionality.9 This indicates that controlling
inflammation is an important factor in improving the status of obese patients (and probably all
patients), while weight loss has much less effect. As mentioned above, however, overweight
triggers low-grade inflammation in the joints, so even though there was little or no immediate direct
effect of obesity, the long-term effects are still counterproductive.

4
Metabolic syndrome. Metabolic syndrome is the presence of at least 3 of these 5 medical
conditions: obesity around the midriff, high blood pressure, high blood sugar, high serum
triglycerides, and low serum high-density lipoprotein.10 Besides being associated with the risk of
developing cardiovascular disease, type 1 diabetes, and some cancers, metabolic syndrome appears
to be associated with OA.8 Evidence from research is not clear.8 Some studies show a connection
and some don’t, especially after controlling for obesity. One study showed accelerated knee
cartilage matrix degradation in people with type 2 diabetes after correcting for ethnicity, age, sex,
baseline BMI (overweight), and severity of OA.8 It appears that there is some interaction going
on, but more research is needed to clarify exactly what factors are related to the development of
OA and how they are related.
High impact sports. Damage to the joints can begin at the age of 20 if someone participates in high
impact sports like football, soccer, tennis, basketball, and high-impact aerobics. Interestingly, long-
distance running has not been shown to increase the risk of osteoarthritis.1 The question remains
whether participation in sports contributes to OA or whether inactivity and associated loss of
muscle strength, resulting obesity, metainflammation, or telomere shortening are more important
contributors to OA than sports activities.8 From a historical standpoint, people tend to be far less
physically active today than they were in past generations, especially hunter/gatherer societies.8
Reduction in loading on the bones and joints may actually result in weaker, less stable joints that
are more susceptible to damage and deterioration, though certainly some types of injuries do lead
to high levels of OA.8 Hunting and foraging are quite different activities than sports. Regular daily
walking, hiking, or running are more similar than multi-directional loading and frequent impact
with objects, other players, or the ground in most sports.
Mismatch factors. The concept of mismatch factors or mismatch diseases is a theory that our
lifestyle today is dramatically different from what the lifestyle of humans has been for most of the
past 200,000 years as hunter-gatherers.8 In just 12,000 years most of the human population
transitioned to farming and agriculture, eating cereals, grains, and domesticated foods, and then to
our current post-industrial age which involves very low levels of physical activity and consumption
of highly processed or domesticated foods that are high in sugar and fat, low in fiber8 This is still
a largely untested theory, even though it conceptually makes sense. Our genes were adapted to
deal with certain demands and over a relatively short period of time, our lifestyle and diet has
changed dramatically and our evolution has been unable to keep up, so there is a mismatch between
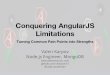
our genetic adaptation and our lifestyle today.8 Although OA has been documented among
Paleolithic hunter-gatherers and early farmers, it was far less prevalent after controlling for
variation in lifespan. Looking at skeletal remains from 2,576 adults over the age of 50 spanning
from prehistoric hunter-gatherers to 21st century city dwellers, it appears that OA is about twice as
common today as in early days.8 This study found that 25% of the people who died in the past few
decades were obese, while only 1% of the remains from earlier times were obese.8 In just half a
century, the risk of OA of the knee has dramatically increased alongside a steep rise in obesity
levels.8 Obesity, metabolic syndrome, dietary changes, and physical activity are the four most
obvious candidates of preventable mismatch diseases in the past 50 years.8

5
Illustration courtesy of Reference 8
Weather and Climate. A lot of people who have OA will tell you the weather has an impact on
their pain and stiffness. And there have been a lot of studies trying to understand if there is a
connection and what that connection might be. Unfortunately, it is difficult to run a long-term
study on this topic that is what researchers term double-blind (both the subject and the researcher
are unaware of the conditions being tested for each subject) or even single-blind (the subject is
unaware of the conditions), since people are pretty aware of the weather and are quite willing to
attribute OA difficulties to the conditions.11 Some studies simply asked subjects if they felt there
was a connection, which is a nearly worthless type of research. For studies which find no
connection between reported pain and current weather conditions (temperature, relative humidity,
barometric pressure, and precipitation13 there are other studies which do find a connection.12 One
well-conducted study found a connection between humidity and joint pain, as well as average daily
temperature and humidity where the effect of humidity was stronger in colder weather conditions.12
Changes in weather did not produce an increase in pain as has been a theory regarding the
connection of weather to OA.12 In the end, it appears that some, but not all of the better studies do
confirm that weather has a significant effect. Pain and stiffness appear to be worse during cold,
damp weather, especially for people with significant joint deterioration.11

6
Prevention Most sources say there is no way to prevent OA. But recent
research on various components in foods (bioactives) is
showing great promise in the prevention of cartilage
destruction by either directly inhibiting enzymes that break
down cartilage or through anti-inflammatory pathways that
result in release of enzymes that break down cartilage.14 A
lot more research is required to verify and enable a better
understanding of these mechanisms, but things may not be hopeless with regard to prevention! This
is covered in much more detail in the Treatment section of this article. But, since this is a preventive
measure, try to get the kids and young people in your life to love eating these foods. You might
save them a lot of agony later in life. We can all start consciously eating more of these foods right
now to halt the progress of cartilage breakdown.
About 1/3 of people in the U.S. from 45-64 years of age have doctor-diagnosed arthritis.15 About
½ of people in the U.S. 65 years of age or older have doctor-diagnosed arthritis. 15 There are
probably many more cases that are unreported and/or not doctor-diagnosed, so these numbers are
conservative. And the trend is upwards as population grows, more of the population is older people,
and obesity is on the rise.15
The best guidelines for avoiding OA are:
• Maintain a healthy weight.
• Get moderate daily exercise for strength, balance, coordination, posture, and
cardiovascular fitness.
• Eat foods based on the Mediterranean diet to head off inflammation and ensure a balance
of nutrients and a healthy balance of Omega fatty acids.
• Avoid high-impact sports.
• Use good posture when performing all daily activities to avoid unnecessary stress, strain,
and twisting of joints.
• Incorporate lots of fruits and vegetables into your diet, especially those listed in the
treatment section under “Diet”. Broccoli and veggies in the mustard family are all really
good for this, but so are many herbs, licorice root, apples, oranges, and other fruits, hot
peppers, and carrots.
Treatment Evidence of osteoarthritis in humans dates back to 4500 B.C. and has been referred to as the most
common ailment of prehistoric people.9 Evidence of OA has even been found in the remains of
dinosaurs.9 Since this ailment has been around for a very long time, remedies abound from copper
bracelets to prescription steroid shots, some highly speculative or somewhat superstitious, and
some posing serious side-effects and health risks of their own. There is currently no known cure
for osteoarthritis, however there are things that can make life much more comfortable and slow
down the progress of deterioration.1 Doctors ordinarily treat OA with anti-inflammatory medicines
and painkillers, but since these all have side effects, it is best to try a natural approach to see if you
can manage the pain and reduce deterioration.16
Cartilage regeneration is a hot area of research. In most cases, stimulation of cartilage regrowth by
various means results in growth of undifferentiated fibrous tissue that does not have good
biomechanical properties.17 There are bits and pieces of the process that are becoming understood,
but there is still a lot of work to be done to understand the factors that cause some people’s cartilage

7
to break down, factors that prohibit regeneration, and factors that may allow for regeneration and
differentiation of cartilage.17 There are several fronts being approached:18
1. Stopping cartilage breakdown.
2. Use of growth factors to aid regeneration of cartilage.
3. Reversing oxidative damage and synovial tissue inflammation.
4. Controlling gene expression as it affects the development of OA.
Basic treatment that aims at improving biomechanics and range of motion, injury prevention,
weight control, strengthening, and low-impact exercises should always be the first line of defense.
Treatment consists of attempting to aid the ailing joints through strengthening, support, reduction
of inflammation, and prevention of further damage to the cartilage, and secondarily to reduce pain.
Exercise. When your joints hurt, it is hard to feel motivated to exercise, but that is exactly what
will help relieve pain, limber up, lessen joint damage, and help to lose or maintain weight.16,67
Many people with OA have decreased muscle strength, physical energy, and endurance because
pain encourages a sedentary lifestyle which is a downward spiral.19 More inactivity leads to
increased pain and disability as well as greater stress, depression, reduced coping and immune
function, and overall reduced quality of life.19
A review of research examining the benefits of exercise on knee OA found that out of 44 trials,
exercise significantly reduced pain, improved functioning, and improved quality of life.20 The
form of exercise in the various studies was not consistent, so it is not possible to determine what
form or quantity is most effective, and it may be highly individual. It appears that land-based
exercise reduced pain 12 points on a scale from 0 to 100, while aquatic exercises reduced pain an
average of 5 points on a scale from 0 to 100.20,21 Quality of life was slightly higher over non-
exercisers with aquatic exercise, though both pain rating and quality of life appear to be short-term
benefits to this type of exercise. If you prefer aquatic exercise and find it more comfortable, by all
means do it because with any exercise program adherence is critical to gaining results, but round
out your exercise repertoire with several other activities as well.19 Few studies have evaluated the
effects of exercise on either altering the progression of OA or modifying it in humans, but it is clear
that it is effective in managing symptoms.22
A well-rounded exercise program should encompass some of all of the following activities
throughout the week. There are many exercise programs that integrate several, if not all in a
session.
• stretching and range of motion
• strength training
• aerobic or endurance exercise
• movement and body awareness like tai chi and yoga
• balance training
Being physically active encourages the production and flow of lubricating joint fluids, builds
muscle strength, helps weight control, improves flexibility and joint movement, and eases pain in
joints.19 Before starting an exercise program, it is a good idea to check with your health practitioner
to determine if there are any specific recommendations or concerns.19 Be aware that Western
medicine is often overly cautious about recommending exercise for people with vulnerable joints,
but research has shown that it is highly beneficial in a multitude of regards and is highly
recommended.19

8
• There are many low-impact aerobics classes at health clubs and online which minimize
jumping and pounding of the joints, yet still allow a great full-body workout.
• Bicycling or stationary cycling is great for strengthening the quadriceps above the knee
and can help reduce symptoms significantly in arthritis of the knee.
• Swimming and water aerobics are good non-impact activities which can improve strength,
though some impact is important to regenerate bone.
• Yoga can be very helpful in improving fitness, mood, stress levels, quality of life, vitality,
physical pain, and walking capacity. 19 Sessions involved in one particular study were one
hour twice/week with one at-home practice session.19 Even 9 months after the study on
yoga, most of the measures were still significantly improved. Hatha Yoga not only
increases flexibility, it emphasizes postural alignment, strength, endurance, balance, and
breathing in relationship to relaxation.19
Do some form of exercise every single day and make it a habit. Pay attention to your body’s pain
levels before you exercise. Alternate or rotate days of various types of activity to make sure you
are covering all bases: strength, endurance, cardiovascular fitness, range of motion, and balance.
More strenuous days of aerobic exercise or weight training may sometimes result in joint soreness
or muscle tightness that will benefit from a day of yoga, tai chi, or pilates. When you are feeling
great, take advantage of those days with more energetic workouts. Days when you’re hurting, don’t
force heavy exertion, but do participate in activity that will help lubricate joints and improve
flexibility. Inactivity is not good when you are stiff and sore. Half an hour of yoga focusing on
the areas of stiffness will really help you and make you feel more in control of your body.
Diet
What you eat has a big impact on inflammation and OA pain. Foods are the best way to ingest
bioactive nutrients because they supply a complete array of nutrition rather than isolating suspected
“active” components and taking those as dietary supplements. It is also much less expensive and
if people can learn to incorporate the most healthful foods into their diet, they will benefit from the
nutrients without having to remember to pop a handful of pills.
Research is now looking at three categories as targets in treating OA through diet.23 These targets
are inflammation, oxidative stress, and catabolic agents (or things that cause the cartilage to break
down).23 Designing a diet that addresses each of these targets is the most natural way to incorporate
these nutraceuticals.
The Mediterranean or anti-inflammatory diet is advised. We go into quite a bit of detail about the
Mediterranean diet in our article on Nutrients, Nutraceuticals, and Healing:
http://working-well.org/articles/pdf/NutritionNew.pdf
and in our article on Overweight and Obesity:
http://working-well.org/articles/pdf/Overweight.pdf
Hydration is important to maintain body functions, but how much you need is largely a factor of
how active you are, how dry or hot the weather is, how much water content is in the foods you have
consumed, and many other factors.24 You can pretty much disregard all hard and fast rules about
drinking 8 glasses of water a day. The best way to tell if you are consuming enough water is by
the color of your urine.24 Dark urine means you are not drinking enough water. Very pale urine
means you can back off. Urine should be pale straw colored. If that is what you see, you can relax
and stop worrying. Thirst is usually an accurate way to tell if you need to drink more fluids, too.
Older people should rely more on the color of their urine because they may not feel thirsty when

9
they are actually becoming somewhat dehydrated.25 If you want to read more about the topic of
hydration, please read our article on the subject:
http://working-well.org/articles/pdf/Hydration.pdf
Anti-catabolic foods. Certain foods have been found that reduce the breakdown of cartilage
(catabolism).
A compound in broccoli and other plants in the brassica family, sulforaphane, has been found to
block the enzymes that cause joint destruction in osteoarthritis. 14 Eating broccoli leads to a high
level of suforaphane in the blood, the plasma, and synovial fluid.26 Sulforaphane has been shown
to inhibit the production of pro-inflammatory compounds in the body as well as inhibiting
degradation of proteins and collagen in cartilage.27 All members of the mustard family have high
levels of sulforaphane and they are termed cruciferous vegetables.
Image courtesy of Reference 28
The table below shows the amount of glucoraphanin (the precursor of sulforaphane) in various
foods. A more exhaustive listing is available in Reference 31. Clearly broccoli is not the top
candidate, but it is one of many foods that contains this compound.29, 30 It should be noted that
glucoraphanin is water-soluble and easily destroyed by heat, so eating raw, or gently steaming or
microwaving will reduce losses.29 Average losses during cooking are approximately 36%.31
Food (raw) Serving in grams Total Glucosinolates (mg)
Broccoli sprouts 1+ cups (100 gms) 250
Wasabi powder 1 teaspoon (2.5 gms) 67
Garden cress 1/2 cup (25 gms) 98
Mustard Greens 1/2 cup, chopped (28 gms) 79
Brussels sprouts 1/2 cup (44 gms) 104
Horseradish 1 Tablespoon (15 gms) 24
Kale 1 cup, chopped (67 gms) 67

10
Watercress 1 cup, chopped (34 gms) 32
Turnip 1/2 cup, cubes (65 gms) 60
Cabbage, savoy 1/2 cup, chopped (45 gms) 35
Cabbage 1/2 cup, chopped (45 gms) 29
Broccoli 1/2 cup, chopped (44 gms) 27
Bok Choy (pak choi) 1/2 cup, chopped (35 gms) 19
Kohlrabi 1/2 cup, chopped (67 gms) 31
Cauliflower 1/2 cup, chopped 50 gms) 22
Further research by the same group, the University of East Anglia in Norwich, UK, went further
and profiled 96 diet-derived, primarily plant-based bioactive substances in the lab.14 Four bioactives
were determined to have the most activity with regard to regulating the genes relevant to cartilage
destruction and OA:
• apigenin – a flavonoid found in many fruits and vegetables including
apples, oranges, celery, onions, oregano, parsley, tarragon, basil,
cilantro, chamomile, bell peppers, garlic, guava, and bacopa
monnieri.14, 32
• isoliquiritigenin – a flavonoid found in licorice root
• luteolin – a flavonoid found in fresh thyme, parsley, fresh
peppermint, hot raw chili peppers, onions, carrots and olive oil14
• sulforaphane – see above for food sources.
All four bioactives were found to have a significant ability to inhibit cartilage degradation
correlated with dosage in laboratory tests.14 Testing determined that isoliquiritigenin and luteolin
had a dose-dependent inhibition of antioxidants which are a direct pathway to cartilage destruction.
The other two players, sulforaphane and apigenin, both inhibit various signaling pathways
indirectly operating to repress the enzymes that break down cartilage.14
The research went one step further to determine if there was a
synergistic effect of combining two, three, or all four of the
bioactives since foods are rarely eaten alone.14 These trials were
done with human cartilage The only combination that acted
synergistically was sulforaphane and isoliquiritegenin and it was a
robust effect. Combining sulforaphane and apigenin, as well as
combining apigenin and isoliquiritigenin showed results that were
about equal to each bioactive acting alone, or additive. Combining
sulforaphane and luteolin, as well as all the three and four bioactive
combinations actually resulted in less inhibition of the cartilage
degrading enzymes than each single one alone, so they seemed to reduce the effectiveness of each
other.14
Another study looked at the effects of diallyl disulfide found in garlic, onions, and other plants in
the allium family.33 This was a study of about 1000 female twins who were not overweight
comparing their dietary habits to find trends that might indicate whether alliums help prevent OA
in the hip.33 This type of study is very difficult to draw conclusions, since there are so many
variables that could be attributed to OA other than diet, however the conclusion of the study was
that a diet high in non-citrus fruits and alliums showed an inverse relationship to OA of the hip.33
In terms of preparing meals and diets to reduce cartilage degradation, the bottom line is to focus on
incorporating many of the flavonoids that have shown preliminary promise. Don’t be a fanatic

11
about excluding other produce! There are so many incredible nutrients in fruits and vegetables that
have nothing to do with OA, but provide a wide array of health benefits. Variety is the best idea
when dealing with any diet recommendation. Sulforaphane is the most-researched and so including
those foods on that list should top the list of anybody trying to prevent cartilage degradation. There
are many ways to prepare any of these vegetables to help mask the strong odor and flavor, if that
is objectionable and make sure not to overcook them! Mayonnaise dip or sesame oil and soy sauce
(or Bragg’s liquid aminos) are simple and delicious ways to serve broccoli, broccolini, or brussels
sprouts.
Licorice root is probably a bit trickier to find, but it is incorporated into many herb tea blends. The
remainder of the useful flavonoids can be used to season foods by the many herbs on the list, and
a generally healthy diet incorporating plenty of fresh fruits and vegetables.
Antioxidants and Anti-inflammatory foods.
Some research has been done to investigate whether dietary antioxidants have an effect on knee
OA.34 Oxidative damage could be part of the problem in degeneration of the cartilage of the knee,
and there is some evidence that consumption of antioxidant nutrients may influence the
development of OA.34 It is too soon to determine whether antioxidants have an effect on OA or
cartilage health, but at this time, the research has found little to no evidence of benefit.34
One study found that higher levels of Vitamin C were associated with higher incidence of knee
OA, though the effect was not linear.34 Vitamin C dietary consumption levels in the range of 81
to 136 mg/day were found to have the highest incidence of OA, while levels either lower or higher
that that range were associated with less OA.34 It is unknown what impact supplementing with
much higher dosages of Vitamin C has on OA.
Green tea is another powerful antioxidant. Human studies are lacking, but animal research has
shown a lowered incidence of OA and slower progression of the disease with consumption of green
tea primarily as a result of reduced inflammatory proteins.5
Pomegranate fruit or juice is also a powerful antioxidant and anti-inflammatory aid.23 Human
research is lacking, but animal studies have found that a two-week period of consumption of
pomegranate significantly reduced cartilage damage and proteoglycan (proteins composing
cartilage and connective tissue) loss, especially in groups receiving higher doses. 23
Ginger and turmeric have strong anti-inflammatory effects and possibly antioxidant properties.23
Curcumin (in turmeric) appears to also have an anti-catabolic effect.23 Curcumin has been found
to have a large and clinically important effect on reduction of pain in the short term.35 Ordinarily,
turmeric is not absorbed by the body well.37 Addition of black pepper while consuming turmeric
increases absorption by twenty-fold.37 Curcumin is discussed further in the section on supplements,
but incorporating these spices into the diet is encouraged. Indian food makes generous use of both!
Resveratrol has anti-inflammatory properties.23 It is found in grapes, berries, and peanuts.23
Rose hips, specifically Rosa canina, have been studied in a few trials, but quality of the research
and bias toward specific products has interfered with determining its efficacy. 23,38 There is
moderate evidence that Rosa canina products reduce pain and stiffness, but not functionality of
joints with OA.38
Correct dietary Omega fatty acid balance has an anti-inflammatory effect. Research has shown
that Omega-6 fatty acids not only increase inflammation, but they are associated with knee

12
osteoarthritis.39 Synovial fluid was sampled from 112 knees of people with and without OA and x-
rays were done on the knees over a period of 3.3 years to monitor progression of the knees. Both
the synovial fluid measures and the x-rays confirmed that higher levels of Omega-6 fatty acids were
significantly associated with knee OA.39
Overall, the effect of taking Omega-3 fatty acid supplements on OA pain appears to be small.5,40, 41
These generally consist of fish oil, krill oil, or green lipped mussel oil. Of the three, green lipped
mussel oil shows the most promise and in a review of research, it was the only supplement, as well
as undenatured type II collagen, that showed not only short-term reduction in pain, but medium
term reduction in pain.35,41 Not enough solid research has actually been done to conclude whether
fish oil supplements relieve pain and some research has significant flaws in implementation.41
Research on benefits to functionality is lacking which is often different from the results from pain
reduction. Since supplements do help improve the balance of Omega-3 to Omega-6 fatty acids and
a higher ratio of Omega-3 to Omega-6 is known to reduce inflammation, it is likely that
supplements cannot hurt and might help reduce inflammation and flexibility of joints with OA. We
suggest that people try some for a while and if it helps, use them. But, best yet, do your best to
improve your diet by reducing consumption of Omega-6 fatty acids and consuming more Omega-
3’s. Supplements are often used as a remedial effort rather than changing one’s dietary habits.
The association between circulating levels of various fatty acids and OA is not clear. One study
measured circulating levels of saturated fatty acids, monounsaturated fatty acids, polyunsaturated
fatty acids, omega-3 and omega-6 fatty acids in fasting men and women with knee and hand OA.42
Higher levels of all fatty acids were positively associated with hand OA in men only.42 It is
interesting that there was no association at all in women with knee or hand of OA.
Other research has been mixed with regard to the benefits of Omega-3, but one recent study looked
specifically at the ratio of Omega-6 fatty acids to Omega-3 fatty acids on: 43
• Functional limitations caused by pain
• Measures of pain derived from applying pressure to various points
• Psychosocial measures including depression, stress, positive/negative emotions, and
optimism.
Blood samples were taken and the ratio of Omega-6 to Omega-3 fatty acids were derived for each
of the 167 participants aged 45-85 years.43 People with lower ratios had significantly fewer
symptoms of knee pain, better functioning, and less psychosocial distress than the people with high
ratios of Omega-6 to Omega-3.43 The people with the high ratio averaged 9.92, almost twice the
recommended ratio of less than 5, while even the people with the low ratio averaged 5.08 which is
the top end of the recommended ratio. 21% of the people with lower ratios reported taking some
type of Omega-3 supplements while only 5% of the high ratio group reported taking supplements.43
Variables that were not a factor included age, sex, employment status, marital status, and exercise
frequency. Smoking and obesity were significantly associated with a high ratio score.43 Diet was
not directly investigated in this study, but it was surmised that there were likely significant
differences in dietary habits between the two groups based on the other evidence gathered.
Supplements and Neutraceuticals The USDA utilizes the term dietary supplement to describe pills, powders, and other non-food
compounds. Neutraceuticals are generally considered the bioactive chemical compound derived
from a food, but available in a non-food form.13 It’s always easier to pop a pill than to make lifestyle
modifications, but most supplements available have still not been found to be conclusively helpful
in dealing with OA. Many can help with the pain and inflammation, but few, if any have been

13
shown to reverse or diminish the deterioration of the joints. Supplements may help, but the biggest
things you can do to improve the situation are the suggestions preceding this section.
In reviewing the research, it seems as though almost everything under the sun has been tested for
its effect on OA in at least one study. We’ve limited our scope to some of the most common and/or
effective supplements. Some of the supplements most commonly recommended have not been
found to be the most effective, while some little-known supplements have shown fairly substantial
benefits.35 Supplements account for $25 billion of consumer spending. Of this, $872 million are
glucosamine and chondroitin.35 Unfortunately, a large number of studies are of very poor quality
or are likely biased due to conflict of interest, individuals, companies or pharmaceuticals
manufacturing products they wish to promote, etc.35 The following two charts summarize the
findings from numerous studies with various risk of bias. The first chart shows the effectiveness
of each supplement on pain in the short-term, medium-term, and long-term. The second chart
shows the effectiveness of each supplement on function in the short-, medium-, and long-term.35
Take these results with a grain of salt because of possible bias and limited number of studies, but
the results are fairly surprising. If a person is to maximize dollars spent on supplements, it makes
sense to focus on the ones that show the most promise for pain or function in the short or medium
term. Clearly, the ever-popular glucosamine and chondroitin do not make that list. Vitamin E
appears to actually be counterproductive. Nothing seemed to help in the long term, but at least
there is hope for more immediate relief.
Pick and choose what you take away from these charts, but it appears that the following list of
supplements would be the top pick for pain and/or function improvement:
• Undenatured type 2 collagen and/or collagen hydrolysate
• Curcumin and/or curcuma longa extract
• Passionfruit peel extract
• Pycnogenol
• Boswellia serrata extract
• L-carnitine
• Green lipped mussel extract (Omega-3)
• SAMe (s-adenosylmethionine)

14
Effectiveness of Supplements on Pain
Table from Reference 35

15
Effectiveness of Supplements on Function
Table from Reference 35
Pycnogenol. Pycnogenol is a type of pine bark extract. A review of research on dietary
supplements for treating OA found a significant moderate reduction of pain in the short pain, a
significant large improvement in physical function, non-significant improvement in stiffness all in
the short term.35 There was no significant improvement in medium or long term pain or
functionality.35

16
Type 2 collagen. It is important to pay attention to what type of collagen
is contained in supplements. Types 1 and 3 contribute to healthy skin,
muscles, bones, hair, and fingernails.45 Types 1 and 3 collagen are derived
primarily from beef cartilage. Type 2 collagen contributes to healthy joints
and cartilage.45 Type 2 collagen is derived primarily from poultry
cartilage.45
Hydrolyzed collagen means the bonds of the long chains of collagen
protein have been broken down into smaller sections with a water process,
which makes it easier for the intestines to absorb.44 This type of Type 2
Collagen has been shown to help relieve pain in the short term.35
Undenatured type 2 collagen, specifically a patented product called UC-II, has been studied and
found to improve pain, stiffness, and functionality in the knee for both people with and without
OA.46,47 40 mg of UC-II taken orally at bedtime works with the immune system to reduce
inflammatory cytokines, so inflammation is reduced.47 This type of type 2 collagen has been shown
to reduce pain in short and medium term, but not long term.35
Passionfruit peel. The peel of Passiflora edulis has been used as a traditional medicine in South
America. One double-blind study of 33 OA patients found that pain was significantly reduced after
60 days of use, while patients who received a placebo experienced an increase in pain.48 There is
not enough scientific research to conclude that this is an effective treatment, what is the active
component, or what dosage is effective, but it is worth further study.
L-carnitine. Carnitine is derived from an amino acid and is found in most cells
in the body.49 It is derived primarily from meat and dairy products and it is used
by the body to produce energy and transports toxic compounds out of the cells.49
Generally, humans do not require supplementation if the diet contains adequate
meat and milk products.49 Aging affects the concentration of carnitine in the
tissues.49 L-carnitine tartrate has specifically been studied in women with knee
OA.50,51 750 mg of l-carnitine tartrate was given in 250 mg doses three times
daily for 8 weeks.50,51 Pain, stiffness, and physical function were all significantly
reduced and were significantly improved over patients receiving a placebo. 50,51
L-carnitine is well-tolerated with no adverse effects on blood lipid levels.51
Another study with the same dosage and similar subjects found that l-carnitine tartrate significantly
reduced levels of IL-1β and matrix metaloproteinases (MMP-1), however CRP and MMP-13 blood
serum levels did not change significantly.52 IL-1β and CRP are inflammation markers. The
presence of the inflammatory cytokines IL-1β, CRP, and others can lead to the production of
enzymes that break down cartilage (MMP-1 and MMP-13).53 In two separate studies conducted by
different researchers, pain was significantly decreased in patients who received l-carnitine, but not
in subjects who received a placebo.52,53 In one study, blood serum levels of IL-1β was not
associated with joint stiffness or functionality and CRP had no effect on pain, stiffness, or
funtionality.53 In conclusion, it is too early to determine whether l-carnitine would be effective in
OA affecting other joints or in men. The mechanism by which is operates is also unknown, but
hopefully more research will be done to delve into this further. At this point, it appears quite
promising at least for women with knee OA.
Turmeric and Boswellia serrata. Turmeric is an Ayurvedic remedy for reducing inflammation and
is the root of the plant in the ginger family.37 Curcumin is the active ingredient in turmeric so most
supplements use the name curcumin because they are a more concentrated source. Look for
supplements that contain some black pepper (piperine) to greatly increase the amount of curcumin

17
your body absorbs and take them with a fatty meal since it is a fat soluble compound.37 Turmeric
has been well-researched. It is effective in reducing pain in OA and is an effective COX-2 inhibitor,
serving to reduce inflammation. 48 It is as effective as ibuprofen or diclofenac, but doesn’t present
the side effects and gastrointestinal problems experienced with the drugs.48
Boswellia serrata is also known as Frankincense. Both Curcumin and Boswellia extracts have been
found to significantly reduce symptoms of OA after 3 months of use.54 Interestingly, even a
placebo caused similar increase in functional measures and reduction in pain after four weeks of
treatment, but after continued use, both Curcumin and Boswellia alone or taken together provided
significant lasting benefits.54 The two substances together were more effective than either alone.54
This may be because Boswellia improved absorption of the Curcumin, though it could be other
interactive effects as well.
In conclusion, it is best to look for a supplement that contains a combination of curcumin,
Boswellia, and peperine or black pepper. Organic sourcing is preferred.
Glucosamine and Chondroitin. Some very well-controlled studies have been conducted, but the
findings are still inconclusive, with these supplements sometimes indicating significant
improvement in OA patients and other times, not.5,23,55 Glucosamine is thought to promote
formation and repair of cartilage, while Chondroitin is believed to increase water retention and
elasticity in cartilage and to inhibit enzymes that break down cartilage.23 The effect of these two
treatments is not synergistic, so even though supplements often include both glucosamine and
chondroitin, they do not work together in aiding cartilage.5 Some research indicates that these two
compounds taken along with Omega-3 fatty acids and/or hyaluronic acid improve joint health,
properties of synovial fluid, and helps regulate the chemistry of the joint.5 A review of research
on chondroitin as it affected joint space width (a decrease in joint space width indicates joint
degeneration) and pain after treatment for an average of 21 months were varied.55 Most studies
found that chondroitin sulfate reduced the loss of joint space width.55 Research was not consistent
on either joint space measures or pain reduction.55
The Osteoarthritis Research Society International has rated both glucosamine and chondroitin as
not appropriate in modifying OA and rated as uncertain for symptom relief.56,57
Glucosamine is derived from the shells of crustaceans like shrimp, lobster, crab, and crawfish.58
Cartilage and connective tissues of animals also contain glucosamine, but like crustacean shells,
they are not easily incorporated into the diet.58 So, for this reason, supplements are the easiest way
to ingest glucosamine if you want to see if it helps you.
Olive oil. There is very little research on the effects of olive oil in aiding OA. Research on rats
has shown that olive oil in the diet improved cartilage recovery following anterior cruciate ligament
surgery.5 In Iran, olive oil is topically applied to the affected joint. It is difficult to determine
whether the effect is due to the olive oil or the massage, though as discussed later, massage alone
has inconclusive effect on OA. One double-blind study found that this improved both pain levels
and physical functioning in knee OA.5 More research is required to verify the use of olive oil in
either diet or topically as a treatment for OA, but it is a main component of the highly recommended
Mediterranean diet and is known to reduce inflammation.
SAM-e (S-adenosylmethionine). SAM-e is synthesized by the body, but is sold as a supplement in
the U.S. because higher amounts than normally produced by the body can have several benefits.59
There are no dietary sources of SAM-e.59 A substantial body of research indicates that SAM-e can
relieve symptoms of OA, is about as effective as standard anti-inflammatory drugs at reducing

18
inflammation and pain, though it can take 2-4 weeks to be effective.59,60,61 SAM-e was not included
in the analysis by Ref. 35, so it does not appear in the preceding tables comparing various
supplements. SAM-e appears to be quite safe, only occasionally causing mild digestive distress,
though not causing damage to the stomach that most pain relievers do.59,61
SAM-e is expensive at the recommended dosage of 600 mg to 1,200 mg daily, so only 400 mg to
800 mg may be necessary for some people.61 Start with at least 400 mg (200 mg twice daily), and
adjust the dosage after two weeks. If it is effective at that dosage, try reducing it to 100 mg two
times daily (200 mg daily). Since it is so safe, people with severe OA symptoms may find it worth
the cost.26
Sam-e works closely with vitamins B-12, B-6, and folate, so it is best to supplement with B vitamins
while taking this supplement to maximize effectiveness.61
To avoid gastrointestinal distress, choose enteric-coated “butanedisulfonate” products and do not
buy bargain brands which may not contain the advertised dosage.62 There are several possible drug
interactions with other pain killers, antidepressants, and treatments for diabetes and Parkinson’s
disease, so if you are on other medications, consult with your doctor before trying it.59,62
Avocado Unsaponifiables (ASUs). Several controlled studies showed promise of ASUs in relieving
symptoms of OA, particularly knee OA. There was no significant difference between dosages of
300 mg or 600 mg daily.13 A more recent meta-analysis of research has resulted in an uncertain
recommendation from the Osteoarthritis Research Society International.57 There may be a small
benefit in relieving pain, especially in knee OA.57
Cetylated Fatty Acids. These naturally occurring fatty acids can be used as either a topical cream
or as a supplement. Solid controlled studies have shown that either of these appear to significantly
reduce swelling and pain while increasing mobility. Results are preliminary, but so far these look
promising.28 A typical oral dose of Cetylated Fatty Acids is 1,000 to 2,000 mg daily. Creams are
applied 2-4 times daily.28
MSM (methylsulfonylmethane). Research on MSM is lacking, though the claim is that MSM is
supposed to help relieve the pain associated with OA. Chemically, it is related to DMSO (dimethyl
sulfoxide), a chemical solvent, which is no longer approved as a supplement because of a large
range of adverse reactions.23 How MSM is used by the body is not well understood, though it
contributes to the sulfur in the body which can be used to synthesize certain amino acids (protein
building blocks), and it can act as an antioxidant.23 Evidence does not strongly support use of MSM
as a supplement.23
Yucca, Mangosteen, Copper bracelets, magnets, etc. – No scientific evidence shows that these
types of remedies are effective at all.40, 41

19
Therapies
The Osteoarthritis Research
Society International now
recommends balneotherapy for
patients with multiple-joint OA
and uncertain recommendation
for knee-only OA.56
Balneotherapy consists of baths
containing thermal mineral
waters such as Dead Sea salt,
mineral waters, sulfur baths, and
radon-carbon dioxide baths.57
Although this therapy is centuries
old and may seem completely
self-indulgent, there is enough
research to support its
effectiveness.63 Heat improves circulation, improves breathing and blood circulation, and lowers
stress.63 Although hydrogen sulfide (HsS) is life-threatening and corrosive, a very low content has
been shown to promote positive effects stimulating cellular defense systems and inducing healing.63
Even a warm Epsom salt bath in your own tub is likely to provide relief.
Use of TENS (transcutaneous electrical nerve stimulation) or ultrasound has an uncertain effect on
knee OA and is not recommended at all for multiple-joint OA.57,64 Electrotherapy/neuromuscular
electrical stimulation are both considered inappropriate until further research is done.57,64
Electromyograph biofeedback has not been shown to be beneficial in strengthening exercise pain,
function, or muscle strength.57
Research findings are mixed as to whether acupuncture helps, but in many cases, it does improve
function and reduces pain. A review of four studies of the effects of acupuncture on hip OA
compared to sham acupuncture controls found virtually no effect on either pain or functioning.65
Another review of ten studies of the effects of acupuncture on knee OA found significant pain
reduction and increased functioning in the short term (up to 13 weeks) and significantly improved
functioning in the long term (up to 26 weeks), but not improved pain.66 Currently, the
Osteoarthritis Research Society International reports that results are uncertain in its treatments of
OA and the American Academy of Orthopaedic Surgeons recommends against acupuncture in knee
OA because it finds that evidence against its effectiveness as compelling.57
Manual therapy has received an inconclusive rating from the American Academy of Orthopaedic
Surgeons because it finds that there is neither sufficient evidence that it benefits or harms patients
with knee OA.64 Manual therapy included joint mobilization, joint manipulation, chiropractic
therapy, patellar mobilization, myofascial release, or Swedish massage.64
NSAIDs, topicals, and pharmaceuticals
All NSAIDs, regardless of dose, have been found to be effective for the pain of OA.67 The
Osteoarthritis Research Society International recommends topical NSAIDs for knee-only
osteoarthritis which is safer and better tolerated than oral NSAIDs.56 The American Academy of
Orthopaedic Surgeons highly recommends the use of oral or topical NSAIDs or Tramadol for knee
OA.64 Most NSAIDs risk complications of serious gastrointestinal, cardiovascular, and kidney or
liver damage.57 Diclofenac is associated with the highest rate of liver abnormalities.57
Unfortunately, 150 mg of diclofenac was found in 74 trials to be the most effective for helping pain

20
and functionality.67 Celecoxib was associated with fewer gastrointestinal problems over ibuprofen
or naproxen.67 Celecoxib was also associated with kidney and high blood pressure problems
compared to ibuprofen.67 Pick your poison, but it is best to explore more natural ways to control
pain and functionality if possible. Save these options for flare-ups and short-term use.
Four research articles were reviewed that studied the effect of NSAIDs on the structure of joints
affected by OA.55 The NSAIDs celecoxib, diacerein, and diclofenac were included. There was no
significant difference in joint space width or in pain reduction with any of the three NSAIDs over
a placebo.55 What this means is that NSAIDs help with pain, but they are not a cure and they don’t
lessen the severity of the physical condition in any way.
Acetaminophen is generally recommended for OA for short-term pain relief, though the American
Academy of Orthopaedic Surgeons withholds a recommendation for its use due to research it found
inconclusive.64 Acetaminophen has negative effects on the gastrointestinal tract and can cause
multi-organ failure with long-term use, so is not recommended as a long-term solution to pain
management.57
Capsaicin creams have been found to be beneficial for knee OA and uncertain benefits for multi-
joint OA.57 Although it was found that there was 50% more pain reduction with users of capsaicin
creams than a placebo, there was also a significant increase in adverse effects such as skin
reactions.57 Overall, it is a fairly successful, inexpensive treatment available over-the-counter and
is probably worth trying. Capsaicin is the compound in hot peppers that makes them hot and it
operates by altering the pain messages sent to the brain.68 It creates a stinging or burning sensation
at first which may be unpleasant. Massage the cream or gel into the skin until it disappears, then
wash hands thoroughly to avoid getting it in the eyes, mouth, or on other sensitive tissues.68
Capsaicin cream should not be applied to damaged, irritated, or broken skin or wounds, should not
be used with a heating pad, should not be bandaged or wrapped, and should not be used after or
during swimming, bathing, sunbathing, hot tubbing, or after heat exposure to avoid skin
sensitivity.68 It is really simple to make your own capsaicin cream with organic ingredients! Mix
1 Tablespoon of organic cayenne pepper into 5 Tablespoons of organic raw coconut oil.69
Duloxetine. The pharmaceutical duloxetine has been found to be beneficial for most types of OA.
A review of research on patients with knee OA found significant reduction in pain (up to 50%) and
functionality over trials of 10-14 weeks.70,71 It has not been found to cause abnormalities in x-rays
or in knee joint mobility.71 It can cause nausea, dry mouth, drowsiness, fatigue, insomnia,
constipation, decreased appetite, and water retention in 7% or less of patients, which was a
significant effect over a placebo.57,70 More research is needed, especially to determine long-term
adverse effects of the drug, but if tolerated, this drug appears to reduce pain and increase
functionality effectively at least for short-term use.57, 70
Opioids. The positive effects of either transdermal or oral opioids for knee and hip OA are
uncertain and quite prone to experiencing adverse effects of the drug.57 The Osteoarthritis Research
Society International and the American Academy of Orthopaedic Surgeons have given them an
uncertain recommendation overall and conclusion that they have limited usefulness for long term
treatment.57,64
Corticosteroids. The American Academy of Orthopaedic Surgeons makes no recommendation
about the use of corticosteroids in knee OA due to inconclusive evidence in the research.64
CBD, marijuana, and synthetic cannabidiol. Almost no human research has been conducted on
cannabis products to determine their usefulness in the treatment of OA, but that is changing.72

21
There are plenty reports about the relief marijuana products give to OA sufferers and it has been
used since 2737 B.C. in Traditional Chinese Medicine.73,74 But it is important to identify in formal
research studies what strains and dosages are effective, when and if it is effective for all types of
OA, how it works in the body, as well as possible side effects.73 The body has an innate
endocannabinoid system (ECS) consisting of receptors, proteins, and signaling enzymes which has
been shown to relieve pain from inflammation and nerves.73,74 Use of cannabinoids appears work
directly within this unique system by acting on the nerves in the joints to reduce pain.72,73 Current
research in Canada sponsored by the Arthritis Society and funded at least partly by producers of
medical marijuana (Aphria, Inc. and Peace Naturals Project).72,75 As with most treatments that are
derived from plant sources, natural sources and use of a broad spectrum of components in the plant
are often more effective than synthetic or isolated compounds and may have fewer side effects.
This three-year study is under way as of this writing and findings will be reported in a year or two.
One study used a synthetic cannabidiol gel applied topically to people with knee OA.76 250 mg of
the gel resulted in a significant improvement in the average weekly worst pain score of at least 30%
and improvement in physical function of at least 20%.76 Men were found to respond more to the
treatment than women.76
Intrusive remedies
Honey Bee Venom. Bee venom has been used to treat arthritis for over 2,000 years and it contains
many anti-inflammatory properties.35 Many of the active components of bee venom are peptides,
one of which is melittin which stimulates the body to produce cortisone 100 times more potent than
hydrocortisone.35 Many other peptides in bee venom act in beneficial ways to reduce inflammation,
immunological effects and have multiple other beneficial effects. In addition to anecdotal evidence
and common knowledge among beekeepers that this treatment works, some controlled research
indicates that bee venom, either injected or used at acupuncture sites, can provide significant relief
to people suffering from OA, as long as they are not sensitive or allergic to bee venom.36,77 Several
deaths following successful honey bee venom acupuncture due to anaphylaxis in an allergic
response.78 It has been suggested that safety of bee venom may be increased with refinement and
removal of harmful substances to reduce its toxicity.78
Corticosteroid injection into joints for short-term pain management of all types of OA has been
recommended by the Osteoarthritis Research Society International.57 It is not recommended for
long-term treatment and pain management due to side effects of corticosteroids.
Research on injection of hyaluronic acid into joints with OA for an average of 16 months showed
inconsistent results in the effect on joint space width and pain.55 Unfortunately, all three studies
were flawed due to procedural or design flaws, or industry-supported bias.55 More research is
required to determine if this treatment is effective. Currently, the Osteoarthritis Research Society
International does not recommend this treatment for most OA, with uncertain status for knee-only
OA.57 The American Academy of Orthopaedic Surgeons strongly recommends against the use of
hyaluronic acid injections with evidence against its use consistent and compelling.64
Arthroscopic surgery in knee OA has been found to be of no benefit over regular non-invasive
treatments, so is now strongly advised against.64,67
Supports Use of knee braces, knee sleeves, foot orthoses, and walking canes are recommended for knee OA
by the Osteoarthritis Research Society International.57 Wearing shock absorbing insoles, shoes, or
orthopedic shoes can help in daily activities and during exercise. (See Resources). The American
Academy of Orthopaedic Surgeons found inconclusive evidence that neither a valgus directing

22
force brace (sleeve or rigid brace) nor wedge insoles are effective for knee OA, though they do give
a “moderate” rating to wedge insoles since they found some evidence that they helped.64
Article updated 10/7/2019
RESOURCES: (We do not receive any financial gain from promoting these companies.)
Mountain Rose Herbs – Certified Organic Herbs, Spices, Oils, Extracts, and Supplements
https://www.mountainroseherbs.com/
Frontier Natural Foods CoOp – Natural and Organic Foods and Spices (not all organic)
http://www.frontiercoop.com/
MEGAcomfort Insoles – Podiatrist designed memory foam and gel layered insoles. The Insole
Shop. http://www.insoleshop.com
REFERENCES:
1. Osteoarthritis. ©1996-2019, MedicineNet, Inc.
http://www.medicinenet.com/osteoarthritis/article.htm
2. Osteoarthritis Causes. Arthritis Foundation. https://www.arthritis.org/about-
arthritis/types/osteoarthritis/causes.php
3. What is Osteoarthritis? Arthritis Foundation. https://www.arthritis.org/about-
arthritis/types/osteoarthritis/what-is-osteoarthritis.php
4. Osteoarthritis Treatments. ©2019 Healthy Lifestyle Brands, LLC
https://www.drweil.com/health-wellness/body-mind-spirit/bone-joint/osteoarthritis/
5. Nutraceutical Supplements in the Management and Prevention of Osteoarthritis. By
Castrogiovanni, P., et al., International Journal of Molecular Science, Oct. 2016, Vol. 17(12),
Pg. 2042. https://www.mdpi.com/1422-0067/17/12/2042/htm
6. Mechanical Behavior of Articular Cartilage. By Landínez-Parra, N.S., Garzón-Alvarado,
D.A., and Venegas-Acosta, J.C. Nov. 22, 2011. DOI: 10.5772/48323.
https://www.intechopen.com/books/injury-and-skeletal-biomechanics/-mechanical-behavior-
of-articular-cartilage
7. Small Weight Loss Takes Big Pressure Off Knee. By Warner, J. June 29, 2005. ©2005 -
2019 WebMD LLC. https://www.webmd.com/osteoarthritis/news/20050629/small-weight-
loss-takes-pressure-off-knee
8. Modern-day environmental factors in the pathogenesis of osteoarthritis. By Berenbaum, F.,
Wallace, I.J., Lieberman, D.E., and Felson, D.T. Nature Reviews Rheumatology, Sept. 12,
2018, Vol 14, pgs. 674-681. https://www.nature.com/articles/s41584-018-0073-x
9. Inflammatory cytokines mediate the effects of diet and exercise on pain and function in knee
osteoarthritis independent of BMI. By Runhaar, J., et al. Osteoarthritis and Cartilage, Vol.
27(8), Aug. 2019, 1118-1123.
https://www.sciencedirect.com/science/article/pii/S1063458419309410
10. Metabolic syndrome. Edited July 11, 2019.
https://en.wikipedia.org/wiki/Metabolic_syndrome
11. Effect of Cold Weather on the Symptoms of Arthritic Disease: A Review of the Literature. By
Deall, C. and Majeed, H. Nov. 21, 2016, Journal of General Practice.
https://www.researchgate.net/publication/311393543_Effect_of_Cold_Weather_on_the_Sym
ptoms_of_Arthritic_Disease_A_Review_of_the_Literature
12. The Influence of Weather Conditions on Joint Pain in Older People with Osteoarthritis:
Results from the European Project on OSteoArthritis. By Timmermans, E.J., et al. The

23
Journal of Rheumatology, Vol. 42(10), Oct. 1, 2015.
https://www.ncbi.nlm.nih.gov/pubmed/26329341
13. The influence of weather on the risk of pain exacerbation in patients with knee osteoarthritis
– a case-crossover study. By Ferreira, M.L., et al. Osteoarthritis and Cartilage, Vol 24(12),
Dec. 2016, pgs. 2042-2047.
https://www.sciencedirect.com/science/article/pii/S1063458416302059
14. Identifying chondroprotective diet-derived bioactives and investigating their synergism. By
Davidson, R.K., et al. Scientific Reports, 2018, Vol. 8, 17173.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6249298/
15. Arthritis. Centers for Disease Control and Prevention. U.S. Department of Health & Human
Services. Reviewed July 18, 2018. https://www.cdc.gov/arthritis/data_statistics/arthritis-
related-stats.htm
16. Natural Relief From Arthritis Pain, by Ellis, M.E. Reviewed May 8, 2017. ©2005-2019
Healthline Media. https://www.healthline.com/health/osteoarthritis/arthritis-natural-relief
17. Cartilage regeneration and ageing: Targeting cellular plasticity in osteoarthritis. By Varela-
Eirin, M., et al., Ageing Research Reviews, Vol. 42, March 2018, pgs. 56-71.
https://www.sciencedirect.com/science/article/pii/S1568163717301502
18. New molecular targets for the treatment of osteoarthritis. By Alcaraz, M.J., et al.
Biochemical Pharmacology, Vol. 80(1), July, 2010, pgs. 13-21.
https://www.sciencedirect.com/science/article/abs/pii/S0006295210001590
19. Yoga in Sedentary Adults with Arthritis: Effects of a Randomized Controlled Pragmatic Trial.
By Moonaz, SH., Bingham, C.O., and Bartlett, S.J. Journal of Theumatology, July 2015,
Vol. 42(7), pgs. 1194-1202. https://www.ncbi.nlm.nih.gov/pubmed/25834206
20. Exercise for osteoarthritis of the knee. By Fransen, M, et al. Cochrane Systematic Review –
Intervention, Jan. 2015, Issue 1, Article No: CD004376.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004376.pub3/abstract
21. Aquatic exercise for the treatment of knee and hip osteoarthritis. By Bartels, E.M., et al.
Cochrane Database of Systematic Reviews 2016, Issue 3. Article No. CD005523.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD005523.pub3/abstract
22. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. By
Bennell, K.L. and Himnan, R.S. Journal of Science and Medicine in Sport, Vol. 14(1), Jan.
2011, pgs. 4-9. https://www.ncbi.nlm.nih.gov/pubmed/20851051/
23. Nutraceuticals: Potential for Chondroprotection and Molecular Targeting of Osteoarthritis.
By Leong, D.J., et al. International Journal of Molecular Sciences, 2013, Vol. 14(11), pgs.
13063-23085. https://www.mdpi.com/1422-0067/14/11/23063/htm
24. The Quest For Hydration. By Hatfield, H. ©2005-2015. WebMD, LLC.
http://www.webmd.com/food-recipes/quest-for-hydration
25. Human Water and Electrolyte Balance. By Kenefick, R.W., Cheuvront, S.N., Montain, S.J.,
Carter, R., and Sawka, M.N. Present Knowledge in Nutrition 10th Edition. International Life
Sciences Institute, ©2012 ILSI, Wiley and Sons, Inc. pgs. 493-505.
http://is.muni.cz/el/1411/jaro2013/BVAJ0222/um/39181669/39181807/Present_Knowledge_i
n_Nutri tion__10th_Ed_.pdf
26. Isothiocyanates are detected in human synovial fluid following broccoli consumption and can
affect the tissues of the knee joint. By Davidson, R., et al. Scientific Reports, Issue 7, Article
number 3398 (2017). https://www.ncbi.nlm.nih.gov/pubmed/28611391
27. Phase 2 enzyme inducer sulphoraphane blocks prostaglandin and nitric oxide synthesis in
human articular chondrocytes and inhibits cartilage matrix degradation. By Kim, H-A, et
al. Rheumatology, Vol. 51 (6), June 2012, pgs. 1006-1016.
https://academic.oup.com/rheumatology/article/51/6/1006/2463602

24
28. Kale, Broccoli, Brussels Sprouts, and Cabbage are All the Same Species. By Landis-Shack,
N. Sept. 16, 2013. ©Foodbeast, Inc. https://www.foodbeast.com/news/kale-broccoli-
brussels-sprouts-and-cabbage-are-all-from-the-same-family/
29. Foods That Are High in Sulforaphane. By Turcotte, M.
https://www.livestrong.com/article/307835-foods-that-are-high-in-sulforaphane/
30. Glucosinolate levels in Vegetables Introduction. July 26, 2014, World of Wasabi.
https://wasabi.org/glucosinolates-foods/
31. Development of a food composition database for the estimation of dietary intakes of
glucosinolates, the biologically active constituents of cruciferous vegetables. By
McNaughton, S.A. and Marks, G.C. British Journal of Nutrition, Vol. 90, 2003, pgs. 687-
697. https://www.cambridge.org/core/services/aop-cambridge-
core/content/view/4BD7F733AEE2CFC89DD28CD66AFAF22C/S0007114503001752a.pdf/
development_of_a_food_composition_database_for_the_estimation_of_dietary_intakes_of_g
lucosinolates_the_biologically_active_constituents_of_cruciferous_vegetables.pdf
32. The benefits and side effects of apigenin. By Magnifico, L. July 16, 2016. © Copyright
2013-2019 BodyNutrition.org. https://bodynutrition.org/apigenin/
33. Dietary garlic and hip osteoarthritis: evidence of a protective effect and putative mechanism
of action. By Williams, F.M.K, et al. BMC Musculoskeletal Disorders, 2010, Vol 11, 280.
©BioMed Central Ltd. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3018463/
34. Associations between dietary antioxidants intake and radiographic knee osteoarthritis. By
Hui, L., et al. Clinical Rheumatoloty, June 2016, Vol. 35(6), pgs. 158-1592.
https://link.springer.com/article/10.1007/s10067-016-3177-1
35. Dietary Supplements for Treating Osteoarthritis: A
36. systematic Review and Meta-Analysis. By Liu, X., et al. British Journal of Sports Medicine,
2018, Vol. 52(3), pgs. 167-175. https://bjsm.bmj.com/content/52/3/167.full
37. 10 Proven Health Benefits of Turmeric and Curcumin. By Gunnars, K. July 13, 2018.
©2005-2019 Healthline Media. https://www.healthline.com/nutrition/top-10-evidence-
based-health-benefits-of-turmeric
38. Rosa canina fruit (rosehip) for osteoarthritis: a cochrane review. By Hu, X.-Y., et
al. Osteoarthritis and Cartilage, Vol. 26, Supplement 1, April 2018, Pg.
S344. https://www.oarsijournal.com/article/S1063-4584(18)30785-4/fulltext
39. Omega-6 oxylipins generated by soluble epoxide hydrolase are associated with knee
osteoarthritis. By Valdes, A.M., et al. Journal of Lipid Research, Sept. 2018, Vol. 59, pgs.
1763-1770. https://www.ncbi.nlm.nih.gov/pubmed/29986999
40. Marine Oil Supplements for Arthritis Pain: A Systematic Review and Meta-Analysis of
Randomized Trials. My Senftleber, N.K., et al. Nutrients, Vol. 9(1), 2017, pg. 42.
https://www.mdpi.com/2072-6643/9/1/42
41. Which supplements can I recommend to my osteoarthritis patients? By Liu, X., Eyles, J.,
McLachaln, A.J., and Mobasheri, A. Rheumatology, Vol. 57 (suppl. 4), May 2018, pgs.
Vi75-iv87. https://academic.oup.com/rheumatology/article/57/suppl_4/iv75/4916021
42. The association of plasma fatty acids levels with hand and knee osteoarthritis. By Loef, M.,
et al. Annals of the Rheumatic Diseases, Vol. 78(Suppl 2), Poster Presentations, June 2019.
Pg. 509. https://www.researchgate.net/publication/333736803_THU0440_THE_ASSOCIATION_OF_PLASM
A_FATTY_ACIDS_LEVELS_WITH_HAND_AND_KNEE_OSTEOARTHRITIS 43. Omega-6:Omega-3 PUFA Ratio, Pain, Functioning, and Distress in Adults with Knee Pain.
By Sibille, K.T., et al. Clinical Journal of Pain, Feb. 2018, Vol. 34(1), pgs. 182-189.
https://www.ncbi.nlm.nih.gov/pubmed/28542024
44. Hydrolyzed Collagen vs. Denatured Collagen. Best5Supplements.com blog, Dec. 12, 2017.
https://best5supplements.com/blog/hydrolyzed-collagen-vs-denatured-collagen/

25
45. Collagen Types 1, 2, & 3 – Knowing the Important Differences. Nutrients for an Energetic
Lifestyle. https://www.energeticnutrition.com/blog/2016/04/collagen-types-1-2-3-knowing-
important-differences/
46. Undenatured type II collagen (UC-II®) for joint support: a randomized, double-blind,
placebo-controlled study in healthy volunteers. By Lugo, J.P., et al. Journal of the
International Society of Sports Nutrition, Vol 10, 2013.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4015808/
47. Efficacy and tolerability of an undenatured type II collagen supplement in modulating knee
osteoarthritis symptoms: a multicenter randomized, double-blind, placebo-controlled study.
By Lugo, J.P., Saiyed, Z.M., and Lane, N.E. Nutrition Journal, Vol. 15, 2016.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4731911/
48. Medical Plant Extracts for Treating Knee Osteoarthritis: a Snapshot of Recent Clinical
Trials and Their Biological Background. By Waltzer, S.M., Weinmann, D., and Toegel, S.,
Current Rheumatology Reports, Aug. 2015, 17:54,
https://link.springer.com/article/10.1007/s11926-015-0530-3
49. Carnitine. National Institutes of Health, Office of Dietary Supplements, U.S. Dept. Of
Health and Human Services. Oct. 10, 2017. https://ods.od.nih.gov/factsheets/Carnitine-
HealthProfessional/
50. Effect of l-carnitine supplementation on clinical symptoms in women with osteoarthritis of the
knee: A randomized, double-blind, placebo-controlled trial. By Kolahi, S., Mahdavi, A.M.,
Mahdavi, R., and Lak, S., European Journal of Integrative Medicine, Vol. 7(5), October 2015,
Pgs. 540-546. https://www.sciencedirect.com/science/article/abs/pii/S1876382015000670
51. L-Carnitine supplementation improved clinical status without changing oxidative stress and
lipid profile in women with knee osteoarthritis. By Mahdavi, A.M., Mahdavi, R., Kolahi, S,
Zemestani, M., and Vatankhah, A-M., Nutrition Research, Vol. 35(8), Aug. 2015, pgs. 707-
715. https://www.sciencedirect.com/science/article/pii/S0271531715001372Mahdavi2 -
Effects of L-Carnitine Supplementation on Serum Inflammatory Factors and Matrix
Metalloproteinase Enzymes in Females with Knee Osteoarthritis: A Randomized, Double-
Blind, Placebo-Controlled Pilot Study. By Mahdavi, A.M., Mahdavi, R., and Kolahi, S..
Journal of the American College of Nutrition, Vol. 35(7), March 2016.
https://www.tandfonline.com/doi/abs/10.1080/07315724.2015.1068139
52. Evaluation of Relationship between Serum Levels of Inflammatory Factors and Clinical
Symptoms in Females with Knee Osteoarthritis. By Jabbari, M.V. and Abolfathi, A. Medical
Laboratory Journal, Jan-Feb. 2018, Vol. 12(1), http://goums.ac.ir/mljgoums/article-1-1036-
en.pdf
53. Efficacy and safety of curcumin and its combination with boswellic acid in osteoarthritis: a
comparative, randomized, double-blind, placebo-controlled study. By Haroyan, A., et al.
BMC Complementary and Alternative Medicine, Vol. 18, Article number: 7 (2018).
https://bmccomplementalternmed.biomedcentral.com/articles/10.1186/s12906-017-2062-z
54. Chondroprotection and the Prevention of Osteoarthritis Progression of the Knee: A
Systematic Review of Treatment Agents. By Gallagher, B., et al. The American Journal of
Sports Medicine, 2014, Vol 43(3), pgs. 734-744.
https://journals.sagepub.com/doi/abs/10.1177/0363546514533777?journalCode=ajsbOARSIg
uide - OARSI Guidelines. ©2013 Osteoarthritis Research Society International.
https://www.oarsi.org/education/oarsi-guidelines
55. OARSI guidelines for the non-surgical management of knee Osteoarthritis. By McAlindon,
T.W., et al. Osteoarthritis and Cartilage, 2014, Vol 22. Pgs. 363-388.
https://www.oarsi.org/sites/default/files/docs/2014/non_surgical_treatment_of_knee_oa_marc
h_2014.pdf
56. What Foods Have Glucosamine? By Russo, J. Livestrong.com.
https://www.livestrong.com/article/203234-what-foods-have-glucosamine/

26
57. SAM-e (S-adenosylmethionine, SAMe), Reviewed by Ratini, M., March 26, 2019. ©2019
WebMD, LLC. https://www.webmd.com/diet/supplement-guide-sam-e#2
58. Safety and efficacy of S-adenosylmethionine (SAMe) for osteoarthritis, By Soeken, K.L., et
al. The Journal of Family Practic, May, 2002, Vol. 51(5).
https://pdfs.semanticscholar.org/5fdc/a3bd16a513e434b2301d1491b1bb1a19e39f.pdf
59. Sam-e. Arthritis Foundation, Atlanta, GA. https://www.arthritis.org/living-with-
arthritis/treatments/natural/supplements-herbs/guide/sam-e.php
60. Supplements For Bones And Joints. ©2019 Healthy Lifestyle Brands, LLC
https://www.drweil.com/health-wellness/body-mind-spirit/bone-joint/supplements-for-bones-
and-joints/Davinelli -Thermal Waters and the Hormetic Effects of Hydrogen Sulfide on
Inflammatory Arthritis and Wound Healing. By Davinelli, S., Bassetto, F., Vitale, M., and
Scapgnini, G. Chapter 10, The Science of Hormensis in Health and Longevity, 2019, pgs.
121-126. https://www.sciencedirect.com/science/article/pii/B9780128142530000103
61. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline, 2nd Edition. American
Academy of Orthopaedic Surgeons, May 18, 2013.
https://www.aaos.org/research/guidelines/TreatmentofOsteoarthritisoftheKneeGuideline.pdf
62. Acupuncture for hip osteoarthritis. By Manheimer, E., et al. Cochrane Database of
Systematic Reviews, May 5, 2018, Issue 5. Art. No. CD013010.
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013010/abstract
63. The Effects of Acupuncture on Chronic Knee Pain Due to Osteoarthritis: A Meta-Analysis.
By Xianfeng, L, et al. The Journal of Bone and Joint Surgery, Sept. 21, 2016, Vol. 98(18),
pgs. 1578-1586.
https://journals.lww.com/jbjsjournal/Abstract/2016/09210/The_Effects_of_Acupuncture_on_
Chronic_Knee_Pain.10.aspx
64. Osteoarthritis year in review 2017: clinical. By Nelson, A.E. Osteoarthritis and Cartilage,
Vol. 26 (3), March 2018, pgs. 319-325.
65. Benefits and uses of Capsaicin Cream. ©2017 HealthBenefitsTimes.com.
https://www.healthbenefitstimes.com/benefits-and-uses-of-capsaicin-cream/
66. Mittman - Homemade Capsaicin Cream for Pain Relief. By Lively, M. ©2019 Roberta
Mittman. https://www.robertamittman.com/recipes/homemade-capsaicin-cream-for-pain-
relief/
67. Efficacy and Safety of Duloxetine on Osteoarthritis Knee Pain: A Meta-Analysis of
Randomized Controlled Trials. By Wang, Z.Y., et al. Pain Medicine, Vol. 16(7), July 2015,
Pgs. 1373-1385. https://academic.oup.com/painmedicine/article/16/7/1373/1918203
68. A randomized, double-blind, placebo-controlled Phase III trial of duloxetine in Japanese
patients with knee pain due to osteoarthritis. By Uchio, Y., et al. Journal of Pain Research,
2018, Vol. 11, pgs. 809-821. https://www.dovepress.com/a-randomized-double-blind-
placebo-controlled-phase-iii-trial-of-duloxe-peer-reviewed-article-JPR
69. Dalhousie researcher investigates use of marijuana for arthritis pain. ©2019 CBC/Radio-
Canada. July 8, 2015. https://www.cbc.ca/news/canada/nova-scotia/dalhousie-researcher-
investigates-use-of-marijuana-for-arthritis-pain-1.3142592
70. Cannabis and joints: scientific evidence for the alleviation of osteoarthritis pain by
cannabinoids. By O’Brien, M., and McDougall, J.J. Current Opinion in Pharmacology, Vol.
40, June 2018, pgs. 104-109.
https://www.sciencedirect.com/science/article/pii/S1471489218300043
71. Is cannabis an effective treatment for joint pain? By Miller, R.J. and Miller, R.E. 2017,
Clinical Experiments in Rheumatology, Issue 35, pgs. 59-57.
https://www.clinexprheumatol.org/article.asp?a=12225
72. Can Cannabis Help Repair Arthritic Joints? By Rough, L. July 15, 2015. ©2019 Leafly.
https://www.leafly.com/news/science-tech/the-medical-minute-can-cannabis-help-repair-
arthritic-jointsHunterOldfield - Synthetic Transdermal Cannabidiol for the Treatment of

27
Knee Pain Due to Osteoarthritis. By Hunter, D., et al. Osteoarthritis and Cartilage, Vol. 26,
2018, pg. 526 https://www.oarsijournal.com/article/S1063-4584(18)30167-5/abstract
73. Efficacy and Safety of Honey Bee Venom (Apis mellifera) Dermal Injections to Treat
Osteoarthritis Knee Pain and Physical Disability: A Randomized Controlled Trial. By
Conrad, V.J., Hazan, L.l., Latorre, A.J., Jakubowska, A., and Kim, C.M.H. The Journal of
Complimentary and Alternative Medicine, Vol 25 (8), Aug. 2019.
https://www.ncbi.nlm.nih.gov/pubmed/31274334
74. To bee or not to bee: The potential efficacy and safety of bee venom acupuncture in humans.
By Cherniack, E.P. and Govorushko, S. Toxicon, Vol 154, Nov. 2018, pgs. 74-78.
https://www.sciencedirect.com/science/article/pii/S0041010118303933 ………………………………………………………………………
This article and all of our articles are intended for your information and education. We are not experts in
the diagnosis and treatment of specific medical or mental problems. When dealing with a severe problem,
please consult your healthcare or mental health professional and research the alternatives available for your
particular diagnosis prior to embarking on a treatment plan. You are ultimately responsible for your health
and treatment!
All Ergonomics Feature Articles are available online at:
http://working-well.org/articles/archive.html
………………………………………………………………………