Embed Size (px)
Citation preview
APORUpdates
1Departments of Medicine, Pharmacology, and International Health, Johns Hopkins University, Baltimore, Maryland, USA. Correspondence: fl [email protected] DOI: 10.1111/j.1752-8062.2009.00127.x
Our Students, Our SelvesMultidisciplinary training is changing who we are Charles Flexner, MD1
W hen I was looking for my fi rst full-time job aft er fellowship, there were two questions I was always asked: “Where did you train?” and “Who trained
you?” Just two decades ago, preparing for a career in biomedical
science was the equivalent of an apprenticeship, with one student learning at the heels of a single master. Th is is a model that served us well for many years. But for the contemporary trainee in clinical and translational science, it is increasingly diffi cult to fi nd a single “chief ” with suffi cient expertise in all the skills needed to pursue
research in this increasingly complex world. Today’s training model is both complicated and organic. We
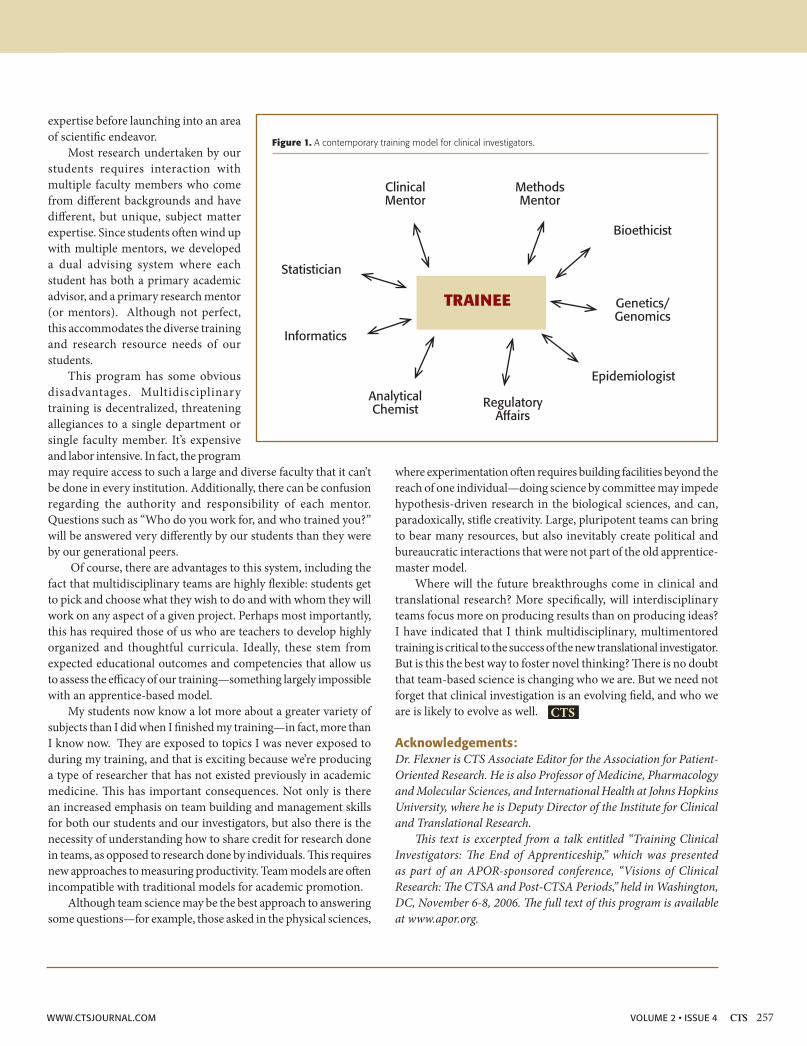
expect our students to master an almost overwhelming array of subject matter. Th is includes biostatistics and biomathematics, epidemiology, genetics, proteomics, bioethics, informatics, data management, regulatory aff airs, and health economics, even international aff airs and geomedicine. Th is requires a very diff erent kind of learning environment (Figure 1).
At Johns Hopkins University, we had to create a completely new training program to serve the needs of our trainees. I know we are not unique in this regard. Today this program, the Graduate Training Program in Clinical Investigation (GTPCI), begun in 1993, off ers three diff erent degrees: one Ph.D. degree and two masters degrees. Th e program’s main objective is to provide graduate training for clinical and translational researchers that is as rigorous as that provided to graduate students in the basic sciences. Th is requires
exposing students to many of the topics just mentioned, as well as laboratory analytical methodology, drug and device development, biomedical writing, and outcomes and eff ectiveness research. Core courses are taken over a 10-month period, in most cases as a full-time student. Th is coursework underlies competencies in 18 knowledge areas that we have developed over the last 10 years that include problem identifi cation, study design, quantitative data analysis, human subjects management, informed consent, and regulatory aff airs.
In addition to this very broad array of subject matter, we have
a very broad array of trainees. Our program started out with its greatest number of students coming from internal medicine but we have evolved to the point where internists are now in the minority. We have pediatricians, psychiatrists, neurologists, surgeons, dermatologists, dentists, and physical medicine and rehabilitation practitioners. All have diff erent needs, wants, and backgrounds. Th ey bring diff erent experiences and skills to the program. Th is, in turn, makes the program more diverse and exciting in the topics we discuss, and in the kinds of research our trainees undertake.
We emphasize hypothesis testing, including, when appropriate, designing studies around acceptance or rejection of a null hypothesis. We emphasize the importance of appropriate experimental controls, recognizing dependent and independent variables in experimental design. Perhaps most importantly, our program emphasizes the acquisition of critical subject matter
My students now know a lot more about a greater variety
of subjects than I did when I fi nished my
training—in fact, more than I know now.
Alex
ande
r Rat
hs /
Dre
amst
ime.
com
256 VOLUME 2 • ISSUE 4 WWW.CTSJOURNAL.COM
expertise before launching into an area of scientifi c endeavor.
Most research undertaken by our students requires interaction with multiple faculty members who come from diff erent backgrounds and have diff erent, but unique, subject matter expertise. Since students oft en wind up with multiple mentors, we developed a dual advising system where each student has both a primary academic advisor, and a primary research mentor (or mentors). Although not perfect, this accommodates the diverse training and research resource needs of our students.
This program has some obvious disadvantages. Multidisciplinary training is decentralized, threatening allegiances to a single department or single faculty member. It’s expensive and labor intensive. In fact, the program may require access to such a large and diverse faculty that it can’t be done in every institution. Additionally, there can be confusion regarding the authority and responsibility of each mentor. Questions such as “Who do you work for, and who trained you?” will be answered very diff erently by our students than they were by our generational peers.
Of course, there are advantages to this system, including the fact that multidisciplinary teams are highly fl exible: students get to pick and choose what they wish to do and with whom they will work on any aspect of a given project. Perhaps most importantly, this has required those of us who are teachers to develop highly organized and thoughtful curricula. Ideally, these stem from expected educational outcomes and competencies that allow us to assess the effi cacy of our training—something largely impossible with an apprentice-based model.
My students now know a lot more about a greater variety of subjects than I did when I fi nished my training—in fact, more than I know now. Th ey are exposed to topics I was never exposed to during my training, and that is exciting because we’re producing a type of researcher that has not existed previously in academic medicine. Th is has important consequences. Not only is there an increased emphasis on team building and management skills for both our students and our investigators, but also there is the necessity of understanding how to share credit for research done in teams, as opposed to research done by individuals. Th is requires new approaches to measuring productivity. Team models are oft en incompatible with traditional models for academic promotion.
Although team science may be the best approach to answering some questions—for example, those asked in the physical sciences,
where experimentation oft en requires building facilities beyond the reach of one individual—doing science by committee may impede hypothesis-driven research in the biological sciences, and can, paradoxically, stifl e creativity. Large, pluripotent teams can bring to bear many resources, but also inevitably create political and bureaucratic interactions that were not part of the old apprentice-master model.
Where will the future breakthroughs come in clinical and translational research? More specifi cally, will interdisciplinary teams focus more on producing results than on producing ideas? I have indicated that I think multidisciplinary, multimentored training is critical to the success of the new translational investigator. But is this the best way to foster novel thinking? Th ere is no doubt that team-based science is changing who we are. But we need not forget that clinical investigation is an evolving fi eld, and who we are is likely to evolve as well.
Acknowledgements:Dr. Flexner is CTS Associate Editor for the Association for Patient-Oriented Research. He is also Professor of Medicine, Pharmacology and Molecular Sciences, and International Health at Johns Hopkins University, where he is Deputy Director of the Institute for Clinical and Translational Research.
Th is text is excerpted from a talk entitled “Training Clinical Investigators: Th e End of Apprenticeship,” which was presented as part of an APOR-sponsored conference, “Visions of Clinical Research: Th e CTSA and Post-CTSA Periods,” held in Washington, DC, November 6-8, 2006. Th e full text of this program is available at www.apor.org.
Figure 1. A contemporary training model for clinical investigators.
Clinical Mentor
MethodsMentor
RegulatoryAffairs
AnalyticalChemist
Informatics
Statistician
Bioethicist
Genetics/Genomics
Epidemiologist
TRAINEE
CTS
WWW.CTSJOURNAL.COM 257VOLUME 2 • ISSUE 4