Embed Size (px)
Citation preview

Research
Outcomes in acute ischemic strokes presenting withdisabling neurologic deficits without intracranialvascular occlusion
Nandavar Shobha1, Rohit Bhatia1, Matthew Boyko1, Sarah Tymchuk1,
Gopukumar Kumarpillai1, Eric Smith1,2, and Andrew M. Demchuk1,2�
Background Patients with moderate to severe acute ischemic
stroke without intracranial vessel occlusion are an intriguing
subset of stroke patients. They pose diagnostic and therapeu-
tic challenges to the physician. We sought to study these
patients with an emphasis on their radiological and clinical
outcomes.
Methods This is a retrospective cohort study of ischemic
stroke patients (NIHSSZ6), with no intracranial vessel occlu-
sion on computed tomography angiography within six-hours
of symptom onset. Follow-up imaging – either computed
tomography brain or magnetic resonance imaging – was
performed within one- to seven-days. The primary outcome
was modified Rankin Scale scorer2 at three-months.
Results In a database of 1308 patients, we identified 99
(7.6%) patients with NIHSSZ6 and no intracranial vessel
occlusion on computed tomography angiography. The mean
age was 67.8715.4 years and 60 (60.6%) were men. The
median baseline NIHSS was nine (6–28). The initial computed
tomography head was normal in 79 (79.8%) patients. Dra-
matic early clinical improvement at 24 h (NIHSS score r2
at 24 h or change between baseline and 24 h NIHSS score
Z15 points) was seen in 38 (38.4%) patients. Follow-up scans
showed infarcts in 66 (66.7%) patients. Fifty (50.5%) patients
received tissue plasminogen activator; one (2%) tissue
plasminogen activator-treated patient developed sympto-
matic intracranial hemorrhage. At three-months; 59 (59.6%)
patients were independent (modified Rankin Scaler2),
34 (34.3%) patients were dependent (modified Rankin
Scale 3-5), and six (6.1%) were dead. The factors associated
with the unlikelihood of good outcome were higher initial
NIHSS (odds ratio 0.86 per additional point, 95% confidence
interval 0.77–0.95, P 5 0.003), and older age (odds ratio 0.95
per additional year, 95% confidence interval 0.92–0.98,
P 5 0.004).
Conclusion Stroke without intracranial occlusions are not a
benign entity. Factors that are independently associated with
decreased likelihood of a good outcome are higher baseline
NIHSS, and older age. Treatment with tissue plasminogen
activator is not a predictor of outcome.
Key words: arterial occlusive disease, computed tomography,
stroke, thrombolytic therapy, treatment outcome
Introduction
Intracranial large vessel occlusions independently predict a
poor outcome (1). The presence of occlusion on computed
tomography angiography (CTA) at presentation correlates
strongly and independently with clinical outcome (2). There
are some ischemic stroke patients who present with moderate
to severe deficits, but do not have intracranial occlusion.
Cerebral angiography performed within six-hours of symptom
onset does not show an arterial occlusion in 20–30% of
ischemic stroke patients (3). There are limited studies of stroke
patients with no visible occlusion on angiography (4–8).
Angiography is an invasive procedure and performing it in
an emergent situation in all patients of stroke is not feasible.
The CTA in the emergency department is a readily accessible,
noninvasive imaging modality for triaging acute stroke pa-
tients. It demonstrates areas of arterial stenosis or occlusion
with nearly the same accuracy as digital subtraction angiogra-
phy (9–11). Studies describing the outcomes of disabling
stroke patients without intracranial vessel occlusion on CTA
are few (12, 13). We sought to study the clinical and radi-
ological outcomes of stroke patients with an NIHSSZ6 and
without intracranial vessel occlusion or stenosis on CTA.DOI: 10.1111/j.1747-4949.2011.00607.x
Conflict of interest: None declared.
Correspondence: Andrew M. Demchuk�, Department of Clinical
Neurosciences, Calgary Stroke Program, Foothills Medical Centre,
Room 1162, University of Calgary, Calgary, Alberta T2N2T9, Canada.
E-mail [email protected] of Clinical Neurosciences, Calgary Stroke Program, Foothills
Medical Centre, University of Calgary, Calgary, Alberta, Canada2Department of Radiology , Calgary Stroke Program, Foothills Medical
Centre, University of Calgary, Calgary, Alberta, Canada
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397392

Materials and methods
This is a retrospective cohort study of stroke patients who
presented acutely to the stroke service at the Foothills Medical
Center, Calgary .The eligible population consisted of patients
who underwent noncontrast CT (NCCT) and CTA for sus-
pected acute ischemic stroke or transient ischemic attack
(TIA) from April 2002 to November 2007. Patients with
premorbid modified Rankin scale score (mRS) of Z2 were
not included in the CTA database. Demographic data, stroke
risk factors, clinical characteristics, baseline and 24 h NIHSS,
and the final diagnosis documented by a stroke neurologist
were extracted from the medical record. The study was
approved by the Institutional Review Board under a waiver
of consent.
The following patients from the database were included in
this study:
� patients with a final diagnosis of stroke
� those with a baseline NIHSS of six or more
� patients that underwent the initial CT brain and CT angio-
gram of head and neck within six-hours of symptom onset
� those with no visible intracranial vessel occlusion on CTA, and
� with a follow-up imaging (CT or magnetic resonance
imaging (MRI)) within one- to seven-days of stroke.
Patients were treated at the discretion of the attending stroke
neurologist. The primary outcome measure was mRS score at
three-months, categorized into independence (mRS 0–2), or
dependence or death (mRS 3–6). The functional status at
three-month follow-up (mRS grading) was obtained from the
stroke clinic. Missing functional outcome data were imputed
from the discharge mRS using the last score carried forward
principle. Dramatic early clinical improvement (14) defined as
a 24 h NIHSSZ2 or an improvement in the 24 h NIHSSZ15
was also recorded.
Image acquisition
Standard nonhelical NCCT was performed on a multislice CT
scanner (GE Medical Systems, Quebec, Canada or Siemens,
Ontario, Canada) using 120 kV, 170 mAs with 5 mm slice
thickness. Continuous axial slices parallel to the orbitomeatal
line were obtained from skull base to vertex. The NCCT was
followed by CTA with a helical scan technique. Acquisitions
were obtained after single bolus IV contrast injection of
90–120 ml nonionic contrast media into an antecubital vein
at 3–5 ml/s. Imaging was autotriggered by the appearance of
contrast media in the ascending aorta. Coverage was from arch
to vertex with 0�6–1�0 mm slice thickness. Source images were
reconstructed at 1�25, 2�5, or 4�0 mm thickness in axial planes
at half-thickness intervals.
The CT angiograms were read by the neuroradiologist and
the attending staff neurologist at the time of treating the
patient. All the images were separately reviewed by two stroke
fellows who were blinded to clinical details and final diagnosis.
The initial NCCT and CTA source images were read for any
infarct or early ischemic change. A thorough search was made
for any intracranial vascular stenosis or occlusion on the CT
angiogram. Follow-up imaging – either CT brain or MRI – was
performed in one- to seven-days after the initial event.
Symptomatic intracranial hemorrhage (sICH) was defined as
an increase in NIHSSZ4 associated with hemorrhage on
follow-up imaging not seen on a previous imaging study (15).
Statistical analysis
Descriptive statistical methods were used to summarize demo-
graphics. Comparisons between thrombolysed and the non-
thrombolysed groups, and patients with good and poor
outcomes were made using the Fisher’s exact test, t-test, or
Wilcoxon rank-sum test as appropriate. Binary logistic regres-
sion analysis was used to find out the independent predictors
of 90-day independence and early clinical improvement.
Candidate variables were; age, NIHSS, tissue plasminogen
activator (tPA) and any others associated with the outcome
in univariate analysis (Po0�15). Nonsignificant variables
(P40�05) were removed from the model by stepwise backward
elimination. The use of tPAwas forced into the model to obtain
an adjusted estimate of the effect of tPA on outcomes in this
population. The Statistical Package for the Social Sciences
(SPSS, version 15) was used to analyze the data. Statistical
significance was set at P40�05.
Results
In a database of 1308 patients who had CT/CT angiograms for
suspected acute stroke, we identified 518 patients (39�6%) who
had an NIHSSZ6 at presentation. Of these patients, 171
(13�1%) patients had no intracranial occlusion. However, a
final diagnosis other than stroke was made in 15/171 (8�8%)
patients (seizures, six; peripheral vestibulopathy, two; non
organic, two; cerebral venous sinus thrombosis, one; migraine,
one; demyelination, one; narcotic overdose, one; syncope,
one). Of the 156 patients with a final diagnosis of acute stroke
and no intracranial occlusion, 99 patients (7�6%) underwent
baseline imaging CT and CTA within six-hours of symptom
onset.
The data of these 99 patients is the subject of this study. The
mean age was 67�8715�4 years; 60 (60�6%) were men. The
median baseline NIHSS on admission was nine (mean
10�374�9) and ranged from six to 28. The following risk
factors were noted: coronary artery disease, 25 (25�3%);
hypertension, 62 (62�6%); diabetes mellitus, 17 (17�2%); atrial
fibrillation, 15 (15�2%); smoking, 37 (37�4%); and past history
of strokes/TIAs, 20 (20�2%). The following were the presenting
features: right-sided motor/sensorimotor symptoms, 49
(49�5%); left-sided motor/sensorimotor symptoms, 41
(41�4%); aphasia, four (4�0%); and nonfocal symptoms, five
(5�1%). All patients underwent CT brain and CTA of the head
and neck. The initial CT scan was abnormal in 20 (20�2%)
patients.
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397 393
N. Shobha et al. Research

Abnormalities consisted of early ischemic changes such as
loss of gray white differentiation or loss of the insular ribbon.
Blinded examination of the CTA source images yielded subtle
changes in two (2%) additional patients. The mean onset to
CTA time was 2�6771�46 h; ranging from 31 min to six-hours.
The CTA of the neck showed significant stenosis (470%) in 12
(12�3%) patients. Three patients had ICA occlusion.
Fifty (50�5%) patients underwent thrombolysis. Intrave-
nous tPA was administered in 49 (49.5%) patients; one patient
received intra-arterial thrombolysis. Seven (7�1%) patients
underwent conventional angiogram. One angiogram showed
evidence of intracranial thrombosis. This patient was sus-
pected to have basilar ischemia based on clinical features, was
found to have a mid-basilar thrombus, and received intra-
arterial thrombolysis. The median baseline NIHSS of the
thrombolysed cohort was 10 (7–14) and the median baseline
NIHSS of the nonthrombolysed cohort was seven (6–11)
(P 5 0�002). The mean onset to CTA time of the thrombolysed
group was 2�071�1 h, and the mean onset to CTA time of the
nonthrombolysed group was 3�371�5 h (P 5 0�0001). One
patient (2%) who received tPA developed sICH – PH1. In the
tPA-treated cohort, two patients (4%) developed hemorrhagic
transformation 1 (HT 1) and one patient (2%) developed
hemorrhagic transformation 2 (HT 2). Dramatic early clinical
improvement was seen in 38 (38�4%) patients. It was seen in
17/50 (34%) tPA-treated patients compared with 21/49
(42�9%) patients who did not receive tPA (P 5 0�41). There
were no factors that predicted dramatic early clinical recovery.
All patients had follow-up imaging within seven-days.
Forty-four (44�4%) patients had a CT, 25 (25�2%) patients
had MRI scan, and 30 (30�3%) patients had both CT and MRI
scans. The imaging findings were as follows:
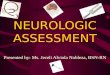
� 32 (32�3%) cortical/sub-cortical infarcts in a single territory
� 22 (22�2%) lacunar infarcts
� 33 (33�3%) normal scans, and
� 12 (12�1%) cortical/sub-cortical infarcts in multiple terri-
tories (Fig. 1).
Out of 30 patients who had both CT and MRIs, three
patients had normal CTs but their MRIs demonstrated lacunar
infarcts in two patients and a single territory cortical infarct in
one patient. Out of 33 patients who had normal scans at follow
up, 15 had MRI. Of 55 patients who underwent MR brain – 19
(34�6%) had single territory cortical infarcts, six (10�9%) had
multiple territory cortical infarcts, 15 (27�3%) had lacunar
infarcts, and 15 (27�3%) had normal scans. Five of the 32
patients who had single territory infarcts and three of the 12
patients who had multiple territory infarcts had significant
carotid disease.
Follow-up outcomes were available in 83 patients (83�8%).
Data were imputed from the discharge mRS using the last score
carried forward principle for the remaining 16 patients
(16�2%). At three-months, 59 (59�6%) patients were indepen-
dent (mRSr2), 34 (34�3%) patients were dependent (mRS 3–
5) and six (6�1%) died. The distribution of mRS scores did not
differ between tPA-treated and conservatively managed pa-
tients (P 5 0�88). The clinical and radiological outcomes of the
tPA-treated and the conservatively treated groups are shown in
Table 1.
Out of the 33 patients who had normal imaging (CTor MRI)
at follow up; 10 patients had an mRS of 0, 14 had an mRS of 1–2,
seven had an mRS of 3–4, two patients were dead at three-
months. Out of the 10 patients who had an mRS of 0 at follow
up, four patients had MRI as well, which is normal. Out of these
four patients, two had received tPA. The other two patients
being stroke mimics cannot be ruled out. Of patients who had
severe carotid disease, four patients had an mRSr2, six patients
had an mRS of 3–4, and two patients were dead at three-months.
Of the three patients with ICA occlusion; one had an mRS of 1,
one had an mRS of 2 and the other, 3. Out of five patients who
died in the tPA group, four died in-hospital. The cause of death
was pulmonary, cardiac, recurrent in-hospital stroke, and
extensive basilar thromboembolism. Symptomatic hemorrhage
(15) was witnessed in one tPA-treated patient, who survived.
Patient characteristics associated with good outcome de-
fined as mRSr2, on univariate analysis are shown in Table 2a.
On univariate analysis, the baseline factors related to outcome
were age (P 5 0�005), baseline NIHSS (P 5 0�006), hyperten-
sion (P 5 0�02), coronary artery disease (P 5 0�03), and sig-
nificant carotid disease of the neck (P 5 0�06). On binary
logistic regression analysis, the factors associated with less
likelihood of good outcome were higher initial NIHSS (odds
ratio (OR) 0�86 per additional point, 95% confidence interval
(CI) 0�77–0�95, P 5 0�003), and older age (OR 0�95 per
additional year, 95% CI 0�92–0�98, P 5 0�004) (Table 2b).
Fig. 1 (a) Cortical and sub-cortical single territory stroke. (b) Multiple territory stroke. (c) Lacunar infarct in globus pallidus on magnetic resonance.
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397394
Research N. Shobha et al.

Treatment with tPA was not a predictor of prognosis (OR 1�40,
95% CI 0�55–3�56, P 5 0�480).
Discussion
In our study of ischemic stroke patients without intracranial
occlusions on CTA, a good outcome at three-months was seen
in 59�6% patients. No changes on baseline NCCTwere noted in
79�8%. Fifty (50�5%) patients received thrombolysis. Dramatic
early clinical improvement was noted in 38% patients. The
majority of the patients (66�7%) had an abnormal follow-up
scan at one- to seven-days of stroke – the most common
abnormality being a single territory cortical infarct (32�3%).
Thrombolysis did not predict early clinical improvement or
three-month outcome in our cohort. Only one tPA-treated
patient had sICH. The factors linked with a good outcome
were lower NIHSS, and a younger age.
There are several potential mechanisms that could lead to
severe stroke in the absence of demonstrable intracranial
occlusion:
� embolism from proximal sources like the heart, aorta or
large vessels of the neck with spontaneous recanalization but
persisting penumbral tissue
� embolism with recanalization but with irreversible ischemic
damage
� distal vessel occlusion not visible on CTA
� small vessel occlusion leading to lacunar infarction
Table 1 Outcomes of thrombolysed and nonthrombolysed cohort
Dramatic early
clinical
improvement
Good
outcome�Poor
outcomew sICHzSingle territory
cortical infarctyMultiple territory
cortical infarctyLacunar
infarctyNormal
scany
Thrombolysed group (n 5 50) 17 (38�0%) 30 (60�0%) 20 (40�0%) 1 (2%) 16 (32�0%) 5 (10�0%) 12 (24�0%) 16 (32�0%)
Nonthrombolysed group (n 5 49) 21 (42�9%) 29 (59�2%) 20 (40�8%) 0 (0%) 16 (32�6%) 7 (14�3%) 10 (20�4%) 17 (34�7%)
�mRSr2 at three-month follow up .wmRS42 at three-month follow up. zSymptomatic intracerebral hemorrhage. yFollow-up imaging finding (CT/MRI)
within one- to seven-days of the event.
Table 2a Clinical, demographic and radiologic features associated with good outcome on univariate analysis at three-months
mRS42 (n 5 59) (%) mRS42 (n 5 40) (%) P-value
Female gender 19 (32�2%) 15 (37�5%) 0�67
Hypertension 31 (52�5%) 31 (77�5%) 0�02
AF 9 (15�3%) 6 (15�0%) 1�00
Valvular heart disease 2 (3�4%) 2 (5�0%) 1�00
CAD 10 (16�9%) 15 (37�5%) 0�03
Antiplatelet therapy 2 (3�4%) 1 (2�5%) 1�00
Significant carotid disease 4 (6�8%) 8 (20�0%) 0�06
Current smoker 15 (25�4%) 10 (25�0%) 1�00
Exsmoker 5 (8�5%) 7 (17�5%) 0�22
Dyslipidemia 12 (20�3%) 7 (17�5%) 0�80
Previous stroke/TIA 10 (16�9%) 10 (25�0%) 0�44
Diabetes mellitus 11 (18�6%) 6 (15�0%) 0�79
Anterior circulation 41 (69�5%) 30 (75�0%) 0�65
Cardioembolic 15 (25�4%) 9 (22�5%) 0�81
Small vessel disease 15 (25�4%) 9 (22�5%) 0�81
Stroke of undetermined etiology 18 (30�5%) 14 (35�0%) 0�67
Treatment with tPA 30 (50�8%) 20 (50�0%) 1�00
Age (mean7SD) years 64�1716�2 73�2712�6 0�003
Baseline NIHSS (median) 7 (6–10) 12 (8–15) 0�001
Normal initial scan 46 (78�0%) 31 (77�5%) 1�00
Single territory cortical infarct 19 (32�2%) 13 (32�5%) 1�00
Multiple territory cortical infarct 6 (10�2%) 6 (15�0%) 0�54
Lacunar infarct 10 (16�9%) 12 (30�0%) 0�14
Normal follow-up scan 24 (40�7%) 9 (22�5%) 0�08
AF, atrial fibrillation; TIA, transient ischemic attack; tPA, tissue plasminogen activator; CAD, coronary artery disease.
Table 2b Baseline factors associated with good outcome at three-
months on logistic regression
Risk factor Odds ratio (95% CI) P-value
Age� 0�95 (0�92–0�98) 0�004
Baseline NIHSSw 0�86 (0�77–0�95) 0�003
�Per additional year of age. wPer additional point.
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397 395
N. Shobha et al. Research

� hemodynamic consequence of significant neck vessel dis-
ease, and
� cerebral ischemia secondary to metabolic poisons, hypoxia,
or systemic hypotension from various causes.
There are two earlier smaller studies of CTA negative
ischemic stroke patients (12, 13). There are a few differences
between our study and the previous studies. Both these studies
included patients treated with tPA and there were no patients
treated conservatively. The patients included in the previous
studies presented within three-hours of symptom onset. An
mRS 0–1 was achieved in 46% of patients in a study by Mikulik
et al. (12) similar to our study where an mRSr1 was achieved
in 44% at three-months. Older age and baseline NIHSS412
were predictors of poor outcome in their study. We noted
similar findings in our study, where younger age and lower
baseline NIHSS were the only predictors of good outcome at
three-months. Only one tPA-treated patient (2%) had sICH in
our cohort. The low rate of ICH in our study is consistent with
a study by Sims et al. (13) that found patients with patent
vasculature treated with tPA had a lower incidence of tPA-
related ICH. The lower rate of sICH in our study compared
with 8% sICH in the study by Mikulik et al. could be explained
by the lower baseline median
NIHSS and younger age of the thrombolysed cohortin our study
The radiological and clinical outcomes at three-months and
the dramatic early clinical improvement were not significantly
different between the conservatively treated and thrombolysed
patients in our cohort. Although 33 (33%) patients did not
have infarcts on the follow-up imaging studies, 23 of them still
had clinical deficits at three-months, suggesting they had
strokes that went undetected on imaging, either because of
the modality or timing of the imaging. Out of the remaining 10
patients, six patients had undergone only CT brain. Had they
undergone MRI we might have detected infarcts. One-week
head CTmay miss small infarcts because of lack of sensitivity or
other infarcts due to a fogging effect (16). Out of the remaining
four patients who had normal CT and also normal MRI, two
had received tPA, which indicates that the physician was quite
sure of the stroke diagnosis and it is possible that infarction was
prevented by successful early reperfusion by tPA.
The most common radiological finding at one- to seven-
days in our cohort was a single territory cortical infarct
(32�3%). In contrast, the most common finding at follow-up
in the study by Arnold et al. (6), a study based on conventional
angiography, was lacunar infarct. This difference can be
explained by different study inclusion criteria – nearly 30%
of the patients reported by Arnold and colleagues had a
baseline NIHSSr5, whereas our study only included patients
with NIHSSZ6 who are probably more likely to have larger
nonlacunar infarcts.
The rates of favorable outcomes in patients who had
undergone conventional angiography and were angio-negative
ranged from 33% to 75% in various studies (4–8). One of the
two (6) studies which documented a favorable outcome in
470% had patients with younger age (58715 years) and a
lower median baseline NIHSS of seven (range 4–25), com-
pared with 67�8715�4 years and a higher median baseline
NIHSS of nine (range 6–28) in the current study. Another
study (10) documented 71% favorable outcome. There were
two main differences between this and our study, the setting of
the former was that of a trial with symptom onset r4 h, while
ours was a retrospective study in a routine clinical setting with
symptom onset r6 h. Unfavorable outcome in the form of
disability was seen in 41% patients in a series of pooled analysis
of stroke patients without angiographically demonstrable
vascular occlusion (4). The dependency rate was similar (40
%) in our study. In our study, 38% of the patients had a
dramatic early clinical improvement at 24 h suggestive of early
recanalization. This effect could be due to spontaneous
recanalization of the occluded vessel in the setting of a good
collateral circulation. In the first six- to eight-hours from
stroke onset, spontaneous recanalization occurs in approxi-
mately 17% of patients (3).
Treatment with tPA was not a predictor of good outcome.
This could partly be secondary to the lower median baseline
NIHSS of the nontreated patients, even though we controlled
for stroke severity in the multivariable model. On the other
hand, tPA may be less effective in patients without demon-
strable occlusion because of a high frequency of spontaneous
recanalization and good endogenous thrombolytic mechan-
isms. Outcomes in stroke patients without demonstrable
occlusion are not uniformly good. However, as shown in this
study and others (7), there remains the possibility that distal
vessel occlusion could be missed on CTA. The rate of sICH in
our study was low (2%) compared with the 7�3% sICH in the
SITS-MOST (17). Therefore use of tPA in this group of
patients appears justified.
Limitations
This is a retrospective study and the data were collected by
chart review. Stroke patients without CTA have not been
included introducing a bias, although 90% of the patients
undergo CTA at our center. Only 7% patients underwent a
conventional angiogram, and one of them was positive despite
CTA appearing normal. This raises the possibility that CTA
might have missed some occlusions, and that conventional
angiography might still be considered when there is a high
index of suspicion for proximal vessel occlusion. Our data,
based mostly on CTA, are very relevant to clinical practice
because CTA is one of the most commonly used modalities for
emergent vascular imaging in stroke. However, the incidence
of brain infarction on imaging may have been underestimated
in our study because only 55/99 patients had MRI. However,
MRI demonstrated an infarct where CT was normal in only 3/
30 patients who underwent both MRI and CT, suggesting that
this underestimation may be minimal. No comprehensive
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397396
Research N. Shobha et al.

details about higher mental functions were available presum-
ably because of the acute care settings. About 2% of our
patients being stroke mimics cannot be ruled out. Follow-up
was not available in 16�2% patients; in these cases 90-day
follow-up was imputed based on mRS recorded at discharge
(that is, last observation carried forward), which is highly
correlated with 90-day mRS (18).
Conclusion
Stroke without intracranial occlusions is not a benign entity.
An unfavorable outcome at three-months was noted in 40�4%
patients. However 38% had an early clinical improvement.
Most patients (66%) had infarcts on their follow-up scans.
Factors that were independently associated with decreased
likelihood of a good outcome were higher baseline NIHSS, and
older age. Although tPA was not a predictor of good outcome,
tPA-related symptomatic hemorrhage was low.
References
1 Smith WS, Tsao JW, Billings ME et al. Prognostic significance of
angiographically confirmed large vessel intracranial occlusion in
patients presenting with acute brain ischemia. Neurocrit Care 2006;
4:14–7.
2 Verro P, Tanenbaum LN, Borden NM, Sen S, Eshkar N. CTangiography
in acute ischemic stroke: preliminary results. Stroke 2002; 33:276–8.
3 Kassem-Moussa H, Graffagnino C. Nonocclusion and spontaneous
recanalization rates in acute ischemic stroke: a review of cerebral
angiography studies. Arch Neurol 2002; 59:1870–73.
4 Shah QA, Zeeshan Memon M, Vazquez G et al. Clinical and radi-
ological outcomes of acute ischemic stroke patients without angio-
graphic occlusion on digital subtraction angiogram. A pooled analysis
of case series. Neuroradiology 2008; 50:963–8.
5 Qureshi AI, Kirmani JF, Siddiqui AM, Hanel RA, Kim SH, Hopkins LN.
Outcomes in acute ischemic stroke patients without angiographically
documented arterial occlusion. J Neuroimaging 2005; 15:37–42.
6 Arnold M, Nedeltchev K, Brekenfeld C et al. Outcome of acute stroke
patients without visible occlusion on early arteriography. Stroke 2004;
35:1135–8.
7 Derex L, Tomsick TA, Brott TG et al. Outcome of stroke patients
without angiographically revealed arterial occlusion within four hours
of symptom onset. Am J Neuroradiol 2001; 22:685–90.
8 Slivka AP, Christoforidis GA, Bourekas EC, Calendine PE, Notestine
MA. Clinical and imaging outcomes after stroke with normal angio-
grams. Am J Neuroradiol 2005; 26:242–5.
9 Zubkov AY, Uschmann H, Rabinstein AA. Rate of arterial occlusion in
patients with acute ischemic stroke. Neurol Res 2008; 30:835–8.
10 Klingebiel R, Kentenich M, Bauknecht HC et al. Comparative evalua-
tion of 64-slice CTangiography and digital subtraction angiography in
assessing the cervicocranial vasculature. Vasc Health Risk Manag 2008;
4:901–7.
11 Shrier DA, Tanaka H, Numaguchi Y, Konno S, Patel U, Shibata D. CT
angiography in the evaluation of acute stroke. Am J Neuroradiol 1997;
18:1011–20.
12 Mikulik R, Goldemund D, Reif M, Aulicky P, Krupa P. Outcome of
patients with negative CT angiography results for arterial occlusion
treated with intravenous thrombolysis. Stroke 2009; 40:868–72.
13 Sims JR, Rordorf G, Smith EE et al. Arterial occlusion revealed by CT
angiography predicts NIH stroke score and acute outcomes after IV
tPA treatment. Am J Neuroradiol 2005; 26:246–51.
14 Broderick JP, Lu M, Kothari R et al. Finding the most powerful
measures of the effectiveness of tissue plasminogen activator in the
NINDS tPA stroke trial. Stroke 2000; 31:2335–41.
15 Fiorelli M, Bastianello S, von Kummer R et al. Hemorrhagic transfor-
mation within 36 hours of a cerebral infarct: relationships with early
clinical deterioration and 3-month outcome in the European Co-
operative Acute Stroke Study I (ECASS I) cohort. Stroke 1999; 30:
2280–4.
16 Saver JL, Johnston KC, Homer D et al. Infarct volume as a surrogate or
auxiliary outcome measure in ischemic stroke clinical trials. The
RANTTAS Investigators. Stroke 1999; 30:293–8.
17 Kulkens S, Hacke W. Thrombolysis with alteplase for acute ischemic
stroke: review of SITS-MOST and other Phase IV studies. Expert Rev
Neurother 2007; 7:783–8.
18 Ovbiagele B, Saver JL. Day-90 acute ischemic stroke outcomes can be
derived from early functional activity level. Cerebrovasc Dis 2010;
29:50–6.
& 2011 The Authors.International Journal of Stroke & 2011 World Stroke Organization Vol 6, October 2011, 392–397 397
N. Shobha et al. Research