Embed Size (px)
Citation preview

Cancer Therapy: Clinical
Outcomes of Children and Adolescents withAdvanced Hereditary Medullary ThyroidCarcinoma Treated with VandetanibIra L. Kraft1, Srivandana Akshintala2, Yuelin Zhu3, Haiyan Lei1, Claudia Derse-Anthony4,EvaDombi1, SethM. Steinberg5,MayaLodish6, StevenG.Waguespack7,OxanaKapustina8,Elizabeth Fox9, Frank M. Balis9, Maria J. Merino10, Paul S. Meltzer3, John W. Glod1,Jack F. Shern1, and Brigitte C.Widemann1
Abstract
Purpose: Vandetanib is well-tolerated in patients withadvanced medullary thyroid carcinoma (MTC). Long-term out-comes and mechanisms of MTC progression have not beenreported previously.
Experimental Design: We monitored toxicities and diseasestatus in patients taking vandetanib for hereditary, advancedMTC. Tumor samples were analyzed for molecular mechanismsof disease progression.
Results: Seventeen patients [8 male, age 13 (9–17)� years]enrolled; 16 had a RET p.Met918Thr germline mutation. Theduration of vandetanib therapy was 6.1 (0.1–9.7þ)� years withtreatment ongoing in 9 patients. Best response was partialresponse in 10, stable disease in 6, and progressive disease inone patient. Duration of response was 7.4 (0.6–8.7þ)� and 4.9(0.6–7.8þ)� years in patients with PR and SD, respectively. Sixpatients died 2.0 (0.4–5.7)� years after progression. Median
progression-free survival (PFS) was 6.7 years [95% confidenceinterval (CI): 2.3 years–undefined] and 5-year overall survival(OS) was 88.2% (95% CI: 60.6%–96.9%). Of 16 patients with aRET p.Met918Thr mutation, progression-free survival was 6.7years (95% CI: 3.1–undefined) and 5-year overall survival was93.8% (95% CI: 63.2%–99.1%). No patients terminated treat-ment because of toxicity. DNA sequencing of tissue samples (n¼11) identified an increase in copy number alterations across thegenome as a potential mechanism of drug resistance [�median(range)].
Conclusions: This study demonstrates that vandetanib is safeand results in sustained responses in children and adolescentswithhereditaryMTC.Our preliminarymolecular data suggest thatan increase in copy number abnormalitiesmay be associatedwithtumor progression in hereditary MTC patients treated with van-detanib. Clin Cancer Res; 24(4); 753–65. �2017 AACR.
IntroductionMultiple Endocrine Neoplasia (MEN) Type II includes two
distinct genetic cancer predisposition syndromes, type IIA(MEN2A) and type IIB (MEN2B), caused by germline, activatingmutations in the REarranged during Transfection (RET) proto-oncogene. MEN2A is associated with mutations in extracellularcysteine residues, andMEN2B is associated with the p.Met918Thrpoint mutation in the kinase domain of the RET protein (1).Nearly all patients with MEN2B develop medullary thyroid car-cinoma (MTC) within the first few years of life andmost succumbto metastatic disease as adolescents or young adults (2).
On the basis of an improvement in progression-free survival inpivotal phase III studies RET-targeting tyrosine kinase inhibitors(TKI), vandetanib and cabozantinib, have been approved forthe treatment of patients with advanced MTC (3, 4). Vandetanibis a potent, orally bioavailable, small-molecule inhibitor of RET,VEGFR, andother related receptor tyrosine kinaseswith inhibitoryconcentrations in the low nanomolar range (5).
Initial studies of vandetanib in adults with metastatic breastcancer (6), relapsed/refractory solid tumors (7), multiple myelo-ma (8), non–small cell lung cancer (9), and advanced MTC (10)provided a robust toxicity profile, MTD of 100–300 mg/day, andpharmacokinetic characterization supportive of once-daily dos-ing. In our phase I/II trial of vandetanib for children with hered-itary MTC (NCT00514046), we showed that 100 mg/m2/day of
1Pediatric Oncology Branch, Center for Cancer Research, National CancerInstitute, Bethesda, Maryland. 2Department of Pediatrics, New York UniversityLangone Medical Center, New York, New York. 3Genetics Branch, Center forCancer Research, National Cancer Institute, Bethesda, Maryland. 4ClinicalResearch Directorate/Clinical Monitoring Research Program, Leidos BiomedicalResearch, Inc., NCI Campus at Frederick, Frederick, Maryland. 5Biostatistics andData Management Section, Center for Cancer Research, National Cancer Insti-tute, Bethesda, Maryland. 6Developmental Endocrine Oncology and Genetics,Eunice Kennedy Shriver National Institute of Child Health and Human Devel-opment (NICHD), Bethesda, Maryland. 7Department of Endocrine Neoplasia andHormonal Disorders, University of Texas MD Anderson Cancer Center, Houston,Texas. 8Clinical Research, Harris IT Services, Sterling, Virginia. 9Division ofOncology, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.10Translational Surgical Pathology Section, Center for Cancer Research, NationalCancer Institute, Bethesda, Maryland.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
J.W. Glod, J.F. Shern, and B.C. Widemann contributed equally to this article.
I.L. Kraft and S. Akshintala contributed equally to this article.
Corresponding Author: John W. Glod, NIH, Bethesda, MD 20892. Phone: 301-451-0391; Fax: 732-235-5331; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-17-2101
�2017 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 753
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

vandetanib administered on a continuous dosing scheduleinduced partial disease remission (11).
Most patients who respond to treatment with vandetanibeventually develop progressive disease (PD; ref. 12). Severalstudies have explored RET, RAS, and other genomic alterationsin MTC (13–15), yet few address mechanisms of disease progres-sion. Previously implicatedmechanisms of disease progression inMTC include RET mutations that impair TKI binding (16, 17),activity of miRNAs (18), mTOR pathway coactivation (19), andcompound RET mutations (20).
Here, we present an updated analysis of a preliminary phase I/IItrial with MEN2B and advanced MTC with a data cutoff of July2017 (11). We analyze the long-term outcomes of pediatricpatients and identify clinical and biologic markers of response,progression, and TKI resistance. We performed genomic andtranscriptomic analyses of tumor samples from patients whoexperienced PD while on TKI therapy. In addition, we performedan in-depth analysis on longitudinal tumor biopsies of a singlepatient who experienced progressive disease despite vandetaniband cabozantinib treatment.
MethodsPatients
Vandetanib was provided by AstraZeneca for the phase I/IIclinical trial. Sanofi/Genzyme continues to provide vandetanib tothe ongoing protocol.
The design, methods, and objectives of this single institutionphase I/II single-arm study (NCT00514046) were described pre-viously (11) and are briefly summarized. The trial enrolled July2007 to October 2012. Patients 5 to 18 years of age with mea-surable, locally advanced or metastatic, hereditary MTC wereeligible for participation in the trial. Other eligibility criteriaincluded recovery from toxic effects of prior therapy and adequateperformance score and organ function. All patients were enrolledin a National Cancer Institute, Pediatric Oncology Branch MTCnatural history study (NCT01660984) to allow for longitudinalfollow up. The data in the primary report was censored July 2011.
Both the phase I/II and the natural history protocols conformedto the Declaration of Helsinki, Good Clinical Practice guidelines,and were approved by the NCI Institutional Review Board. Allpatients or their legal guardians signed a document of informedconsent indicating their understanding of the investigationalnature and risks of this study. Assent was obtained per institu-tional guidelines.
Clinical trial proceduresPatients received oral vandetanib at two dose levels within the
100–150 mg/m2/day dose range once daily, continuously (in28-day cycles). A standard 3þ3 dose escalation design was fol-lowed in age groups 13–18 years and 5–12 years (21). Dose wascalculated on the basis of body-surface area using a dosingnomogram. The recommended phase II dose in the absence ofdose-limiting toxicitywas determined as 100mg/m2/day (11). Allpatients in a subsequent expansion cohort were treated at thisdose level.
Tumor response was quantified using RECIST v1.0 (22) as theprimary endpoint. Biomarker responses measuring serum levelsof calcitonin and carcinoembryonic antigen (CEA) were second-ary endpoints. Tumor response was assessed every 2months (twocycles) until cycle 8 and every 4 months thereafter. In July 2013,after the FDA approval of vandetanib for adults with advancedMTC and after report of our initial trial results (11), we amendedthe protocol to increase interval tumor responsemeasurements toevery 6 months and to allow patients who experienced diseaseprogression by RECIST after achieving a partial response (PR) tocontinue study treatment if there was ongoing clinical benefit (i.e.decrease in MTC-related diarrhea, constipation, and/or relief ofpain). In some patients, alternative treatments were discussed bythe investigators and offered if available.
The NCI CTEP Common Terminology Criteria for AdverseEvents Version 3.0 was used to quantify severity of adverseevents. Toxicity monitoring included physical exams, labora-tory tests, and serial imaging to quantify growth plate volume.Patients were assessed weekly during cycle 1, biweekly untilcycle 4, and then during each tumor response evaluation. The2013 protocol amendment also included less stringent tox-icity reporting criteria (to record only grade 3 or highertoxicities or those causing a medication hold) and allowedfor flexibility in dosing schedule to accommodate grade 1/2toxicities. Treatment limiting toxicity was defined as anyadverse event possibly, probably, or definitely attributed tovandetanib therapy and required the dose be held, decreased,or stopped.
Endpoints included assessment of antitumor activity as mea-sured by tumor response by RECIST, duration of response,progression-free survival (PFS), overall survival (OS), biomark-er response (percent change in calcitonin and CEA from base-line and doubling time), and determination of the safety andtolerability of vandetanib. Tumor biopsies were optional. Inaddition, analysis of tumor samples from patients enrolled onthe NCI Pediatric Oncology Branch MTC natural history study(NCT01660984) was performed.
DNA and RNA sequencingFormalin-fixed paraffin-embedded (FFPE) blocks or unstained
slides were collected at the time of diagnosis, prior to therapy,and/or at disease progression when available. Coded sampleswere compiled and annotated with histologic diagnosis and
Translational Relevance
Vandetanib is well tolerated in adults and children withadvanced MTC; however, long-term outcomes of patients onvandetanib have not been reported previously. This updatedreport of a phase I/II trial of vandetanib assessed the activity,safety, and outcome of children and adolescents withadvanced, hereditary MTC and MEN2B treated with vandeta-nib. Tumor samples taken at disease progression were ana-lyzed for genomic mechanisms of resistance. Patients exhib-ited durable partial responses and tolerated extended therapywith vandetanib. When disease progression occurred, tumorburden increased at an accelerated pace and subsequent ther-apies usually had limited activity. This study provides thelongest follow-up on patients taking continuous vandetanibto date. Patients experiencing progressive disease on vandeta-nib may not respond to another RET-targeting TKI. This studyprovides new insights into the tumorigenesis ofMTC in the eraof tyrosine kinase inhibitor therapy by illustrating genome-wide copy number changes at MTC progression.
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research754
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

clinical information. Quality control was performed on all sam-ples to ensure the match of tumor and normal pairs.
DNA and RNA samples from tumor and adjacent normal tissue(either unaffected thyroid or lymph node) were extracted fromFFPE blocks or unstained slides as described previously (23).Approximately 200 nanograms of DNA was used for librarypreparation with the Kapa Hyper Prep Kit. Custom gene captureandpaired end sequencingwas performed as described previously(23). Approximately 500 nanograms of DNA and 500 nanogramsof RNA from selected samples (patient #8) were subject to whole-exome sequencing and whole transcriptome sequencing. FFPEexome libraries were prepared by Genomics Lab using AgilentSureSelectXT Human All Exon V5 plus UTR target enrichment kit.Exome samples were pooled and run on a HiSeq3000 withIllumina TruSeq V4 chemistry. RNA-seq libraries were preparedwith the TruSeq Stranded Total RNA Sample Preparation kit andsequenced on one HiSeq2500 lane using Illumina TruSeq v4chemistry.
Data analysis was accomplished using the Pipeliner toolspackage available from The Center for Cancer Research Collab-orative Bioinformatics Resource (https://bioinformatics.cancer.gov/). After removal of duplicate reads, local realignment wasperformed with GATK version 3.5 and somatic point mutations,insertions, anddeletionswere called using theunionof the calls ofStrelka and Mutect version 2 bioinformatics platforms (24). Tofurther refine the accuracy of the calls, raw variants were furtherfiltered by requiring them to be nonsynonomous as well asrestricted only to areas of the genome designed to be capturedin the assay. For somatic calls, aminimum total coverage depth of5 reads and a variant allele frequency of greater than 5% wasrequired.DNA copy number (CN) discoverywas performed usingcnvKit and further visualized usingNEXUSCopyNumber Version9.0 fromBioDiscovery, Inc (25).Whole transcriptome sequencingfiles were assessed for quality and mapped using STAR (26).Resulting fastq files were analyzed by TopHat2 and Cufflinksusing Partek Flow version 6.0 and samples were comparedusing fragments per kilobase of transcript per Million (FPKM)values (27, 28). DNA and RNA correlations were performed usingLog2(Ratio) and Log2(FPKM) values, respectively.
All sequencing files reported were uploaded to dbGaP (https://www.ncbi.nlm.nih.gov/gap) to promote ongoing discovery.
Statistical analysisTime-to-event data were analyzed using the Kaplan–Meier
method to estimate median event times, and are reported withtwo-sided 95% confidence intervals (CI). Median duration offollow-upwas estimated using the reverse Kaplan–Meiermethod.Duration of PR and duration of SD were determined using theKaplan–Meier method. Duration of response for patients with aPR was measured from the date of PR until date of progression,censoring patients if they had not progressed as of July 1, 2017;duration of SD was measured from enrollment date until date ofprogression, censoring patients if they had not progressed by July1, 2017. A time-varying covariate analysis was performed using aCox proportional hazards model, along with a landmark analysisbeginning at the date the last PR was noted, to assess the asso-ciation between response and stable disease (SD) on overallsurvival. Rate of change (slope) and doubling time for calcitoninand CEA were calculated as reported previously (29, 30). Com-parisons of baseline clinical values were made among groups ofpatients based on response using the Kruskal–Wallis test and the
Jonckheere–Terpstra test for trend. Other reported values hereinare medians, P values were two-tailed, and reported withoutadjustment for multiple comparisons.
ResultsThe first patient was enrolled on July 13, 2007 and the last
patient was enrolled onOctober 17, 2012. For this report, the datacutoff was July 1, 2017. Seventeen patients (8 male, median age13 years, range 9–17) enrolled. Sixteen had a RET p.Met918Thrgermline mutation and one patient had a unique RET p.Ser836-Ser/p.Gly691Ser/p.Ser904Ser/p.Leu769Leu mutation (Supple-mentary Table S1). The median duration of treatment was6.1 years (range 0.1-9.7 years) and is ongoing in 9 patients, 7 ofwhom have not experienced disease progression.
All patients were evaluable for response. Ten (58.8%) achieveda PR and 6 (35.3%) had SD as best response (Fig. 1A). Sevenpatients maintained their best response (PR or SD) at the datacutoff (Fig. 1A). The median time to first documented PR was0.79 years (range, 0.45–2.41 years; Fig. 1B). Responses weresustained for a median of 7.4 years (range, 0.6–8.7þ) in patientsachieving best response of PR and 4.9 years (range, 0.6–7.8þ) inpatients achieving best response of SD.
Median progression-free survival (PFS) was 6.7 years (95% CI:2.3 years–undefined) and 5-year overall survival (OS) was 88.2%(95% CI 60.6-96.9%). A single patient with a unique RETp.Ser836Ser/p.Gly691Ser/p.Ser904Ser/p.Leu769Leu mutationhad rapid disease progression after one month of therapy. Ofthe 16 patients with the RET p.Met918Thr germline mutation,median follow-up was 8.0 years, the median PFS was 6.7 years(95% CI: 3.1–undefined), and median OS was not reached(Fig. 1C and D). The five-year OS probability was 93.8% (95%CI: 63.2%–99.1%) and the seven-year OS probability was 72.3%(95% CI: 41.5%–88.7%; Fig. 1D). The HR from a time-varyingcovariate analysis was 0.64 (95% CI: 0.10–3.93, P ¼ 0.63)comparing patients achieving PR versus SD as best response,indicating no association between response and duration ofsurvival. Landmark Kaplan–Meier analysis beginning 879 days(2.4 years) after enrollment, to reflect the time until the lastpatient was noted to respond, similarly did not show survivaladvantage in patients that achieved PR versus SD (P ¼0.64, Fig. 1E). The single patient harboring a non-MEN2B, RETmutation (#3) experienced tumor progression and succumbedto disease.
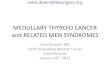
Tenpatients developeddisease progression on vandetanib. Fivepatients experienced PD with increase in nontarget lesions orpreviously unidentified lesions (#3, #4, #7, #8, #14), four patientsexperienced an increase in target lesions (#1, #6, #9, #12), andonepatient experienced increase in tumor markers concerning foroccult progression (#17). Sites of PD are demonstrated in Fig. 2and show a new inguinal lesion (pt #7; A–C), a prostate lesion (pt#8; ref. D-F), and increasing size of a lesionwithin the thyroid bed(pt #14; G-I). Seven patients stopped vandetanib after experienc-ing PD and patient #9 discontinued due to personal preference(Table 1). Patient #6 discontinued vandetanib for a surgicalprocedure and did not resume therapy by the data cutoffand patient #12 continues vandetanib despite experiencing PD(Table 1). Treatments after stopping vandetanib are also summa-rized in Table 1. One patient did not receive subsequent medicaltherapy directed at the MTC (#3), 5 patients did not achieveobjective responses on subsequent therapies (#1, #4, #7, #9, #14),
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 755
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

Figure 1.
Response and survival analysis of patients on vandetanib. A, Waterfall plot of best percent change in target lesions from baseline for 17 patients. Colorscorrespond to patient response at data cutoff and symbols indicate criteria for progression. B, Duration of initial response or stable disease and of ongoingvandetanib treatment in patients. Arrows indicate continued follow-up at data cutoff. C, Kaplan–Meier plot of progression-free survival of 16 patients harboringthe p.Met918Thr RET mutation. Eight patients were censored, 6 of whom remain in follow-up for progression-free survival. D, Kaplan–Meier plot of overallsurvival of 16 patients harboring the p.Met918Thr RET mutation. 11 patients were censored and remain in follow-up on a natural history protocol.E, Kaplan–Meier landmark analysis from median time to PR of 16 patients harboring the p.Met918Thr RET mutation.
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research756
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

two patients continued enrollment on the vandetanib protocoldue to clinical benefit (#6, #12), and two patients (#8, #17)responded to a second TKI (Table 1, Supplementary Fig. S1A–S1C). Four patients that experienced PD were alive after 0.4, 0.9,3.0 and 4.1 years (#6, #9, #12, #17), respectively. Six patients withPD experienced death from metastatic disease after a medianduration of 2.0 years (range 0.4-5.7 years). The Kaplan-Meierestimate of median OS from the date of progression for the 10patients who progressed was 3.0 years (95% CI: 0.4–5.7 years).
Patients with PR and SD at the data cutoff had similar baselinecalcitonin levels, CEA levels, tumor size per RECIST, percentchange in tumor size, and time to best response compared withpatients with PD (Supplementary Table S2). Patients exhibited atrend toward higher baseline calcitonin with increasing degree oftumor response (Supplementary Table S2). No other measuredbaseline characteristics were associated with sustained response.Sixteen patients exhibited overall decline or stabilization incalcitonin and CEA during vandetanib therapy (Fig. 3). Four of
Figure 2.
Radiographic responses and progression in children and adolescents with MEN2B and MTC. A–C, CT of the pelvis of patient #7, a male who achievedSD and subsequently experienced PD in a new lesion. D–F, CT of the prostate of patient #8, a male who achieved SD and subsequently experienced PDin a previously unrecognized lesion. G–I, T2-weighted MRI of the neck of patient #14, a female whom achieved PR and subsequently experienced PD in thethyroid bed.
Table 1. Patient course and management after disease progression
Patient Response Site(s) of progression Treatment(s) and duration (years) after vandetanibTime after stoppingvandetanib (years)
3 PD Nontarget- cervical spine lesionb None 0.4a
7 SD ! PD Non-target– groin Cabozantinib (0.44), sunitinib (0.8), sorafenib (1.35) 3.1a
8 Previously unidentified– prostateb Cabozantinib (0.79) 1.1a
9 Target–neck Neck dissection/debulking (5.14) 5.917 Elevation in CEA/calcitonin Cabozantinib (3.21) 4.11 PR ! PD Target – liver Cabozantinib (1.34), Sunitinib (2.33) 4.1a
4 Non-target– mediastinum Sorafenib (0.15), cabozantinib (0.22), cabozantinib (0.61), sunitinib (1.07) 3.1a
6 Target– neck, chest None 1.7312 Target– mediastinum None 0c
14 Non-target– neckb Sunitinib (0.13), Cabozantinib (0.15) 0.7a
aDeath from disease.bPresent on baseline imaging.cStill taking vandetanib at data cutoff.
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 757
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

8 patients maintained calcitonin levels below baseline through-out therapy despite eventual disease progression. Increase incalcitonin and CEA coincided with drug holds as demonstratedby patients #2, #6, and #13 (Fig. 3A–F; Supplementary Fig. S1A–S1C). There was no difference between patients that eventuallyprogressed on therapy in rate of change of tumor markers duringthe first four months of vandetanib treatment (SupplementaryFig. S2A and S2B). Nine of 10 patients that experienced progres-sive disease had increasing calcitonin or CEA levels correspondingto doubling times of less than five years prior to experiencing PD(Supplementary Fig. S2E). Interestingly, for somepatients, such aspatient #12, the doubling times of calcitonin and CEA decreasedone full year before the patientmet RECIST criteria for progressivedisease (Supplementary Fig. S3).
All patients experienced vandetanib related adverse events asdescribed previously (11). Most adverse events were grade 1 or 2and no patient was required to discontinue therapy due to drugtoxicity. No patient experienced QT-prolongation mandatinghold or discontinuation of therapy. Ten patients had adverseevents grade three or higher, required drug holds, or dose reduc-
tions during the follow-up period (Table 2). The most commonreason for a drug holdwas unrelated to vandetanib treatment, butwas instituted as a precaution for elective surgeries to allow forwound healing. Ten patients experienced grade 2 hypertensionthat required medical management (Supplementary Table S2).Vandetanib-related adverse events included bleeding propensity,weight loss, hypertension, hepatotoxicity (elevated liver functiontests), renal toxicity (elevated creatinine), pulmonary toxicity(abnormal pulmonary function tests), and gastrointestinal dis-turbances (diarrhea or constipation). Patient #12 and #16 expe-rienced disproportionate weight gain while on vandetanib; how-ever, this was not consistently observed (Supplementary Fig. S4).No meaningful change in growth plate volumes was observed inpatients treated with vandetanib (data not shown). Two patientscontinuing therapy had drug holds greater than one year due torecovery from scoliosis surgery (#6) and 9 months due to preg-nancy (#13). Both patients were holding vandetanib at the datacutoff. All patients adhered to greater than 95% of scheduleddoses during the follow-up period on the basis of patient diaryand pill counts. Individualized dose adjustments and schedules
Figure 3.
Biomarker response. The percentchange from baseline in calcitonin(A–C) and CEA (D–F) per RECIST atdata cutoff.
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research758
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

were common and the dose of vandetanib of patients continuingtherapy (n ¼ 9) at the data cutoff was 67–100 mg/m2 once daily.
Custom-capture genome sequencing of 241 cancer-implicat-ed genes was performed on 7 patients; 11 tumor biopsysamples, 10 with paired germline tissue. Seven samples weretaken before patients started vandetanib and four were takenfrom patient tumors at the time of disease progression (Table3). One patient (#8) had three longitudinal samples available.Except for the germline RET mutation, recurrent, nonsynon-ymous mutations were not found in this cohort (Table 3).Seven patients experienced few somatic mutations and no
difference in the number of mutations was noted comparingsamples before (n ¼ 6) and after (n ¼ 3) vandetanib therapy(Table 3; Fig. 4A). There was no difference in percent change ofgenome in germline tissue. However, a trend toward increasinggenome-wide, somatic CN changes was observed after vande-tanib therapy (Fig. 4B).
Patient #8 had three samples collected from different timepoints during MTC therapy that were used for in-depth analysisby whole-exome sequencing (WES) and whole transcriptomesequencing (RNA-Seq). Samples included a lymph node withoutevidence of MTC used as the germline sample, a primary MTC
Table 2. Toxicities
Patient CTC CriteriaGradeof AE
Time since startingvandetanib (years)
Duration ofhold (days)
Dose change(mg/m2)
2 Hemorrhage 2 4.75 83Weight loss 2 6.04 0 150 ! 100
5 ALT, SGPT 3 3.83 11Weight loss; proteinuria; hypertension 2 5.56 13 100 ! 67
6 Creatinine 2 6.32 699 150 ! 100Wound healinga N/A 7.22 630b
8 Wound healinga N/A 3.47 243.9 334.62 49
9 Patient preferencea N/A 1.93 2,144b discontinued10 Vomiting 3 3.9 7
Abdominal pain 2Constipation 3 5.27 51 150 ! 100
12 Diarrhea 2 3.92 0 150 ! 10013 Palpitations 2 1.81 28
Palpitations 2 3.49 112 150 ! 100DLCO; pulmonary other; pulmonary cysts by CT 2 4 112Pregnancya N/A 5.57 363b discontinued
14 Wound healinga N/A 1.99 12.05 2
Wound healinga N/A 8Oral hemorrhage 2 2.93 7
16 Supraventricular and nodal arrhythmia 2 0.11 7 150 ! 100Hypertension 2 0.15 7
17 Diarrhea 2 0.45 4 100 ! 67aUnrelated to therapy.bContinues to hold at data cutoff.
Table 3. Genomic alterations identified by panel sequencing of 7 patients with MEN2B-associated MTC
Case Pt Age (years) Tumor location Previous TKISomatic codingalterations CN Alterations (chromosome) Gene breaks
1a 4 9 Lymph node None 1p del BRCA1, TRAF7, PTEN2 8 12 Thyroid None3 8 12 Lymph node None4 17 9 Thyroid None MUTYH p.Ala59Val 1p del, 4 del, 9p del, 22 del5 22b 15 Thyroid None PRKAR1A sf 1p del, 8 amp, 16 amp CREBBP, RPTOR6 24b 12 Thyroid None 1p del, 1q amp7 24b 16 Prostate None SYNE1 sf 1p del, 4 del KMT2C8 7 19 Lymph node vandetanib EML4 p.Ile328Val,
RET p.Leu790Phe14 del, 22 del, 1q amp, 16 amp TRAF7
9c 7 22 Adrenal vandetanib, sunitinib,sorafinib
1q amp TSC2, AXIN1
10 8 16 Prostate vandetanib SMARCA4p.Leu783Arg
13 del, 1q amp, 7 amp, 10 amp, 14 amp,15 amp, 18 amp, 22 amp
KMT2C
11 14 16 Thyroid vandetanib 1p del, 3 del, 4 del, 9 del, 13 del, 14 del,17p del, 1q amp, 17q amp
TRAF7, RPTOR
NOTE: Genomic alterations were predicted with computational methods.Abbreviations: amp, amplification; del, deletion; sf, sequence feature not in coding region.aNormal sample unavailable.bPatient enrolled on the MTC natural history study (NCT01660984).cSample with low tumor %.
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 759
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

Figure 4.
Sequencing of DNA from biopsies of patients with MEN2B and MTC. A, Somatic genomic alterations found in a 241-gene panel in biopsy samples fromunique patients before vandetanib and after experiencing PD on therapy. B, Percent change in genome from CN alterations predicted by comparing DNAextracted from tumor lesions and germline tissue in unique patients before starting vandetanib and after experiencing progressive disease. Patient #8 and#24 had multiple tumor sample analyzed. C and D, CN gains and loss (C) and % genome and loss of heterozygosity (D) predicted in patient #8 before andafter vandetanib, and after cabozantinib by whole-exome sequencing. Representative H&E stains and genome-wide CN alterations from patient #8 areshown, and include lymph node (germline; E), primary MTC (F), prostate metastasis (G), and skin metastasis (H).
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research760
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

lesion taken before any TKI therapy, a prostate metastasis taken atdisease progression on vandetanib (Metastasis 1), and a skinlesion taken after disease progression on cabozantinib (Metastasis2). Molecular analysis on the longitudinal sample set demon-strated accumulation of whole-genome CN alterations and lossof heterozygosity throughout therapy at the DNA level (Fig. 4Cand D). Notably, the primary MTC sample (Fig. 4F) and theprostate metastasis (Fig. 4G) were separate samples taken fromdifferent regions of the same tumors used in the panel sequencing(case 2 and 10, respectively). Additional computationally pre-dicted deleterious, driving, and cancer-implicated mutationswere not found in the whole-exome data compared with thepanel sequencing. Representative IHC, CN alterations, and B-allele frequency plots are shown in Fig. 4E–H. The SMARCA4p.Leu783Arg somaticmutation found in case 10was also found intheWESdata frommetastasis one. Furthermore, copy neutral, lossof heterozygosity was observed on chr5, chr8, chr13, and chr19 inboth metastasis one and metastasis two (Fig. 4G and H). Metas-tasis two was noted to have an RB1 p.Val654fs somatic mutation.Together, these data verified the chromosomal gains and loss asdemonstrated by the targeted panel-sequencing results.
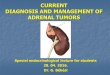
Analysis of the full transcriptome identified 54 genes meetingcomputational cutoffs (false discovery rate < 0.05, P < 0.01) as themost differentially expressed in biopsies from different pointsduring therapy (Fig. 5A). An increase in the RET proto-oncogenewas observed across time points. We examined the normalizedRNA expression of other genes known to be related to RET andobserved an increase in RNA expression of FLT4, coding for theVEGFR (VEGFR3) protein, and EGFR in the metastasis (Fig. 5B).We compared the RNA expression with CN changes to determinewhether the transcript changes were associated with genomicchanges. RET (r2 ¼ 0.985) and EGFR (r2 ¼ 0.948) expressioncorrelated with CN changes (Fig. 5C). FLT4 had an increase RNAexpression independent of DNA CN changes (Fig. 5C). Further-more, we noted an increase in transcription across cell-cycle geneswhen comparing the samples longitudinally from primary MTC,to metastasis one, to metastasis two (Supplementary Fig. S5).
DiscussionLong-term, continuous treatment with TKIs is beneficial in
patients with advancedMTC. In this updated analysis, vandetanibwas well tolerated and resulted in durable responses in pediatricpatients with hereditary, metastatic MTC, with 7 of 17 patientsmaintaining PR or SD for median follow up over 5 years. Ourstudy represents the largest prospectively followed cohort ofpatients with MEN2B and MTC and is consistent with other casereports and population-based studies characterizing the out-comes and lifespan of patients with MEN2B (31, 32).
While complete resection of the thyroid gland is the onlycurative therapy for patients with primary MTC, the presence oflocally advanced or metastatic disease at the time of diagnosislimits the possibility of surgical cure (33). In this study, treatmentwith vandetanib led to durable responses in patients with diseasenot amenable to surgical cure. The median time to achieve a PRwas 0.79 years with one patient taking as long as 2.41 years toachieve a response. Patients #14, #15, and #16 had SD at the timeof the initial report of this study but later achieved a PR at 1.72,1.21, and 2.41 years. This observation demonstrates the potentialbenefit of chronic TKI therapy for advanced MTC. Disease pro-gression generally occurred in new, previously unrecognized, or
nontarget lesions (patients #3, #4, #7, #8, #14) and one patient(#8) developed PD in the prostate. In this cohort, there was not acommon location of progressive metastasis highlighting theimportance of a careful imaging survey in patients withmetastaticdisease.
Six of 10 patients experiencing PD ultimately died from disease[median of 2.0 (range, 0.4–5.7) years] after stopping vandetanib.Of the 6 patients that died, only patient #4 experienced a briefresponse of 0.79 years to a second, RET-targeting TKI. Interest-ingly, patient #17 had a prolonged, objective response to asubsequent RET-targeting TKI. Patient #17 was taken off vande-tanib due to failure to meet secondary endpoints (increasingcalcitonin and CEA) and was enrolled on a subsequent clinicaltrial (Supplementary Fig. S1B). Discontinuation of vandetanibwas allowed and recommended for this patient after the 2013protocol amendment and based on health care provider experi-ence with previous patients.
In some cases, the ability of RECIST criteria to capture diseaseburdenmay be limited inmetastaticMTCdue to the large numberof lesions in a single patient, the presence of bonymetastasis, andoccult metastasis. This emphasizes the importance of biomarkercharacterization. Calcitonin and CEA doubling times are helpfulin determining the rate of growth of MTC (34). In addition, somestudies have carefully examined these biomarkers in patients onTKI therapy (35–37). Consistent with previous findings, weobserved that use of a single tumor biomarker may not accuratelydocument the presence of progressive disease; however, by using acombination of calcitonin and CEA slopes and doubling times,we noted a correlation with progressive disease via RECIST (Sup-plementary Fig. S2; ref. 36). We examined the slope of biomarkerchange between patients one year prior to experiencing PD versuspatients in the year prior to the data cutoff (SupplementaryFig. S3). This comparison is inherently flawed by the dissimila-rities in patients, time points, and logistical caveats, such as drugholds. Furthermore, calcitonin levels may vary greatly due to theassay used, the hook effect with markedly elevated levels, and fedversus fasting sampling. Prospective, properly controlled studiesare needed to truly validate use of biomarkers while on TKItherapy. Furthermore, findings in this population may havelimited applicability to adult patients with sporadicMTC.Despitethe caveats, our data agree with the American Thyroid Associationguidelines implying that patients with decreasing tumor markerdoubling time seem to have a worse prognosis (38). All together,we suggest that changes in tumor marker doubling time may bebest interpreted in context with additional clinical correlatesbefore therapy is altered.
Vandetanib was well tolerated and no patient discontinuedtherapy due to adverse events during the follow-up period.Fourteen patients experienced hypertension that was amenableto medical therapy and 3 patients required more than onemedication or dose adjustments to maintain normal blood pres-sures (Supplementary Table S3). No patients developed pheo-chromocytoma while on the study. Vandetanib was held inpatients recovering from injuries or surgeries per previous recom-mendations (33). Almost all common adverse events occurredearly in therapy; however, significant adverse events requiringdrug holds such as elevated creatinine (patient #6) were discov-ered after 6 years on vandetanib, illustrating the need for contin-uous monitoring. The decrease in adverse events later in therapymay be related to dose reductions that occurred due to eventsearlier during treatment. Eight patients required a dose reduction
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 761
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

Figure 5.
Gene expression changes across longitudinal biopsy specimens. A, Gene expression heat map of the 54 most differentially expressed transcripts.Expression levels are colored based on Z-scores across individual genes. Genes are grouped by unsupervised k-means clustering. B, Normalized expression ofRET-family genes by RNA-seq. C, Correlation of RET-family genes between RNA-seq and DNA CN across longitudinal biopsies. D, Model of diseaseprogression in patient #8 (male, best response SD) despite vandetanib and cabozantinib therapy.
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research762
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

during the follow-up period. Despite dose reductions or discon-tinuingmedication, many patientsmaintained responses for overone year. Patients who remain on vandetanib at the data cutoffcontinue a dose of 67–100 mg/m2/day, or incorporated analternate day dosing scheme to minimize toxicities.
Continued adherence is of great concern for many patients onoral TKI therapy. We did not observe significant noncompliancein patient reported medication logs and study mandated pillcounts. In addition, the original phase I/II study quantifiedplasma drug levels suggesting sufficient levels for effect modula-tion (11). This suggests that lack of compliance may not be amechanism of resistance in this clinical setting. We also notedinstances of patients maintaining SD despite significant drugholds. Patient #9 discontinued vandetanib after achieving SDand was followed for over 5 years outside of the NIH beforeexperiencing progressive disease (Supplementary Fig. S1B).Patient #12 experienced repeated decrease in CEA and calcitoninwithout increase in tumor size despite two significant drug holds(Supplementary Fig. S1B). These observations suggest that drugholidays may be useful in select patients without sacrificingefficacy.
Tumor samples were available for 5 patients before startingvandetanib (seven samples), 3 patients at progression on TKI (fivesamples), and one patient both pre-TKI and at progression (threesamples). A uniform molecular mechanism of treatment failurewas not observed in this small sample set. Pre-TKI samplesexhibited few tumor specific mutations or CN alterations and 4of 5 patients had loss of chromosome 1p. Copy number imbal-ances have been reported previously in both sporadic and hered-itary MTC (39, 40). Marsh and colleagues also found loss ofchromosome 1p in 21% of a cohort of MTC that included bothhereditary and sporadic disease suggesting that loss of 1p may beinvolved in early tumorigenesis (39). We identified a number ofgenomic changes in PD. Interestingly, progression for one patientwas associated with acquisition of a previously unidentifiedp.Leu790Phe somatic mutation within the kinase domain of theRET gene. However, a pretreatment sample was not available forthis patient limiting the interpretation of this finding. Previousreports of a RET p.Leu790Phe mutation are as germline findingsassociated with MEN2A/FMTC and have not previously beenreported in association with resistance to vandetanib (41, 42).Longitudinal data from patient #8 demonstrated acquisition of aSMARCA4mutation in thefirstmetastasis and anRB1mutation inthe second metastasis. Loss of heterozygosity and increase in CNvariations were noted in four of five samples at tumor progressionhighlighting aneuploidy as the dominant genetic marker of PD.Two patients had loss of chromosome 14 and three had gain ofchromosome 1q.
Activation of the PI3K/Akt/mTOR pathway has been reportedin MTC (43, 44). Four patient samples including two samplesobtained prior to TKI therapy and two samples following TKItherapy had breaks in genes coding for components of the PI3Ksignaling pathway including PTEN, RPTOR, and TSC2. It has beensuggested that the oncogenic activity of RET may be mediated, atleast partially, through the PI3K pathway (45, 46). Responses tothe TORC1 inhibitor, everolimus, have been reported in patientswith MTC (47). The presence of alterations in genes coding forPI3K pathway components is intriguing; however, the smallnumber of patients in this study and the lack of uniform samplecollection make assessment of the role of the PI3K pathway inoncogenesis and disease progression difficult.
Genome-wide CN alterations of rapidly progressive diseasewere recently documented in an autopsy case report of sporadicMTC (48). Such changes are recognized as a hallmark of manycancers, hereditary MTC is thought to be driven by a singleoncogene (1, 49). The observed genome-wide CN alterationsraise questions as to the underlying etiology, and whether CNalterations are induced by the TKI therapy or are selectedcellular clones that occur in the natural course of MTC pro-gression. As in other malignancies, the observed genomicaberrations are reflected at the transcriptional level (50).Regardless of underlying cause, the WES and RNA-seq data inthis longitudinal set may represent a transition away from thesingle oncogenic driver mutation (RET p.Met918Thr) to amalignancy with multiple oncogenic drivers as proposedin Fig. 5D. Currently, few options exist for patients that progresson RET-targeting medications. These data may provide evi-dence for use of nonspecific agents and highlight the need fordevelopment of therapies that target cells with genomic insta-bility in a PD setting (33).
Increased RNA expression of cell-cycle genes in the metastasiscompared to the primary tumor in patient #8 may be expected inrapidly dividing lesions (Supplementary Fig. S5). This findingwasconsistent with rapid clinical progression aswell as the loss ofRB1function in metastasis two. We also observed increased RET andFLT4 expression throughout the longitudinal course of MTCdisease suggesting potential gene upregulation in response totherapy.
Our data provide preliminary insights into mechanisms ofvandetanib resistance in hereditary MTC. These data must beinterpreted with caution and are best served as hypothesis gen-erating rather than conclusive. It is notable that an additional RETmutation was only identified in one case of progressive disease.Furthermore, a p.Leu790Phe mutation identified may not beexpected to lead to vandetanib resistance.Other possiblemechan-isms of drug resistance including changes in cellular and systemicmetabolism and aberrant activation of downstream targets of RETwere not assessed. Preclinical evaluations and future trials thatmore completely investigate these factors may lead to a betterunderstanding of vandetanib resistance and could inform treat-ment options for these patients. Limitations of these data arenotable for the small sample size and the heterogeneity in timingand anatomic location of the available clinical samples, thusrequiring independent confirmation of these observations. Aprospective trial with defined points for clinical sample collectionand the addition of pharmacokinetic analysiswouldhelp to betterdelineate mechanisms of resistance to vandetanib in this patientpopulation.
In conclusion, most children and adolescents with MEN2Bassociated MTC have sustained clinical responses on vandeta-nib. We observed genomic instability in MTC metastasis afterdisease progression on TKI therapy, postulating a departurefrom the single driver mutation. Genome-wide CN alterationswere correlated generally with RNA expression changes. Thesedata highlight the importance of longitudinal sampling oftumor tissue either via direct biopsy or potentially throughliquid biopsy as these technologies become available. Whiletrials evaluating more potent RET inhibitors are already under-way, future studies may also be warranted to assess the use ofcytotoxic or non-RET pathway targeting therapies in patientsthat experience progressive disease in the face of standardRET-targeted therapy.
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 763
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
DisclaimerThe content of this publication does not necessarily reflect the views or
policies of the Department of Health andHuman Services, nor doesmention oftrade names, commercial products, or organizations imply endorsement by theU.S. Government.
Authors' ContributionsConception and design: I.L. Kraft, S. Akshintala, E. Fox, J.W. Glod,B.C. WidemannDevelopment of methodology: S. Akshintala, E. Fox, J.W. Glod, J.F. Shern,B.C. WidemannAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): I.L. Kraft, S. Akshintala, C. Derse-Anthony, M. Lodish,S.G. Waguespack, E. Fox, F.M. Balis, M.J. Merino, P.S. Meltzer, J.W. Glod,J.F. Shern, B.C. WidemannAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): I.L. Kraft, S. Akshintala, Y.J. Zhu, H. Lei, E. Dombi,S.M. Steinberg, E. Fox, M.J. Merino, P.S. Meltzer, J.W. Glod, J.F. Shern,B.C. WidemannWriting, review, and/or revision of the manuscript: I.L. Kraft, S. Akshintala,C. Derse-Anthony, E. Dombi, S.M. Steinberg, M. Lodish, S. Waguespack, E. Fox,F.M. Balis, M.J. Merino, P.S. Meltzer, J.W. Glod, J.F. Shern, B.C. Widemann
Administrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C. Derse-Anthony, E. Dombi, O. Kapustina,M.J. MerinoStudy supervision: F.M. Balis, J.W. Glod, J.F. Shern
AcknowledgmentsWe thank the participating patients and their families. We recognize
Dr. Samuel Wells and Dr. David Venzon for their critical review of themanuscript and advice on data analysis. We are indebted to Dr. Keith J.Killian and David Petersen for their advice and expertise in nucleic acidextraction and sequencing of FFPE specimens. Finally, we recognize theNational Institutes of Health, Medical Research Scholars Program (https://clinicalcenter.nih.gov/training/mrsp/) for support in training the next gen-eration of clinician scientists. AstraZeneca provided vandetanib for the phaseI/II trial, Sanofi/Genzyme supports the ongoing trial. This research was, inpart, supported by the National Cancer Institute, Center for Cancer Research.CDA is a contractor for Leidos Biomedical Research, Inc., NCI Campus atFrederick (Frederick, MD 21702). This project has also been funded in wholeor in part with federal funds from the National Cancer Institute, NIH, undercontract no. HHSN261200800001E.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 21, 2017; revised October 4, 2017; accepted November 20,2017; published OnlineFirst November 29, 2017.
References1. Romei C, Ciampi R, Elisei R. A comprehensive overview of the role of the
RET proto-oncogene in thyroid carcinoma. Nat Rev Endocrinol 2016;12:192–202.
2. Dermody S,Walls A, Harley EH Jr. Pediatric thyroid cancer: an update fromthe SEER database 2007–2012. Int J Pediatr Otorhinolaryngol 2016;89:121–6.
3. Wells SA Jr, Robinson BG, Gagel RF, Dralle H, Fagin JA, Santoro M, et al.Vandetanib in patients with locally advanced or metastatic medullarythyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol2012;30:134–41.
4. Elisei R, SchlumbergerMJ,Muller SP, Schoffski P, BroseMS, ShahMH, et al.Cabozantinib in progressive medullary thyroid cancer. J Clin Oncol2013;31:3639–46.
5. Hennequin LF, Stokes ES, ThomasAP, JohnstoneC, Ple PA,OgilvieDJ, et al.Novel 4-anilinoquinazolines with C-7 basic side chains: design and struc-ture activity relationship of a series of potent, orally active, VEGF receptortyrosine kinase inhibitors. J Med Chem 2002;45:1300–12.
6. Miller KD, Trigo JM, Wheeler C, Barge A, Rowbottom J, Sledge G, et al. Amulticenter phase II trial of ZD6474, a vascular endothelial growth factorreceptor-2 and epidermal growth factor receptor tyrosine kinase inhibitor,in patients with previously treatedmetastatic breast cancer. ClinCancer Res2005;11:3369–76.
7. Holden SN, Eckhardt SG, Basser R, de Boer R, Rischin D, Green M, et al.Clinical evaluation of ZD6474, an orally active inhibitor of VEGF and EGFreceptor signaling, in patients with solid, malignant tumors. Ann Oncol2005;16:1391–7.
8. KovacsMJ, Reece DE,Marcellus D,Meyer RM,Mathews S, Dong RP, et al. Aphase II study of ZD6474 (Zactima, a selective inhibitor of VEGFR andEGFR tyrosine kinase in patients with relapsed multiple myeloma–NCICCTG IND.145. Invest New Drugs 2006;24:529–35.
9. Arnold AM, Seymour L, Smylie M, Ding K, Ung Y, Findlay B, et al. Phase IIstudy of vandetanib or placebo in small-cell lung cancer patients aftercomplete or partial response to induction chemotherapy with or withoutradiation therapy: national cancer institute of Canada clinical trials groupstudy BR.20. J Clin Oncol 2007;25:4278–84.
10. Wells SA Jr, Gosnell JE, Gagel RF, Moley J, Pfister D, Sosa JA, et al.Vandetanib for the treatment of patients with locally advanced or meta-static hereditary medullary thyroid cancer. J Clin Oncol 2010;28:767–72.
11. Fox E, Widemann BC, Chuk MK, Marcus L, Aikin A, Whitcomb PO, et al.Vandetanib in children and adolescents withmultiple endocrine neoplasia
type 2B associatedmedullary thyroid carcinoma. Clin Cancer Res 2013;19:4239–48.
12. Fallahi P, Ferrari SM, Baldini E, Biricotti M, Ulisse S, Materazzi G, et al.The safety and efficacy of vandetanib in the treatment of progressivemedullary thyroid cancer. Expert Rev Anticancer Ther 2016;16:1109–18.
13. Lian EY, Maritan SM, Cockburn JG, Kasaian K, Crupi MJ, Hurlbut D, et al.Differential roles of RET isoforms in medullary and papillary thyroidcarcinomas. Endocr Relat Cancer 2017;24:53–69.
14. Kato S, Subbiah V, Marchlik E, Elkin SK, Carter JL, Kurzrock R. RETaberrations in diverse cancers: next-generation sequencing of 4,871patients. Clin Cancer Res 2017;23:1988–97.
15. Mancikova V, Montero-Conde C, Perales-Paton J, Fernandez A, SantacanaM, Jodkowska K, et al. Multilayer OMIC data in medullary thyroidcarcinoma identifies the STAT3 pathway as a potential therapeutic targetin RETM918T tumors. Clin Cancer Res 2017;23:1334–45.
16. Carlomagno F, Guida T, Anaganti S, Provitera L, Kjaer S, McDonald NQ,et al. Identification of tyrosine 806 as a molecular determinant of RETkinase sensitivity to ZD6474. Endocr Relat Cancer 2009;16:233–41.
17. Carlomagno F, Guida T, Anaganti S, Vecchio G, Fusco A, Ryan AJ, et al.Disease associated mutations at valine 804 in the RET receptor tyrosinekinase confer resistance to selective kinase inhibitors. Oncogene 2004;23:6056–63.
18. Chu YH, Lloyd RV. Medullary thyroid carcinoma: recent advances includ-ing MicroRNA expression. Endocr Pathol 2016;27:312–24.
19. Heilmann AM, Subbiah V, Wang K, Sun JX, Elvin JA, Chmielecki J, et al.Comprehensive genomic profiling of clinically advanced medullary thy-roid carcinoma. Oncology 2016;90:339–46.
20. Romei C, Casella F, Tacito A, Bottici V, Valerio L, Viola D, et al. Newinsights in the molecular signature of advanced medullary thyroidcancer: evidence of a bad outcome of cases with double RET muta-tions., J Med Genet 2016 Jul 28. pii: jmedgenet-2016-103833. [Epubahead of print].
21. Storer BE. Design and analysis of phase I clinical trials. Biometrics1989;45:925–37.
22. Therasse P, Arbuck SG, Eisenhauer EA,Wanders J, Kaplan RS, Rubinstein L,et al. New guidelines to evaluate the response to treatment in solid tumors.European organization for research and treatment of cancer, nationalcancer institute of the United States, National Cancer Institute of Canada.J Natl Cancer Inst 2000;92:205–16.
Kraft et al.
Clin Cancer Res; 24(4) February 15, 2018 Clinical Cancer Research764
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

23. Killian JK, Miettinen M, Walker RL, Wang Y, Zhu YJ, Waterfall JJ, et al.Recurrent epimutation of SDHC in gastrointestinal stromal tumors. SciTransl Med 2014;6:268ra177.
24. Cibulskis K, LawrenceMS,Carter SL, SivachenkoA, JaffeD, SougnezC, et al.Sensitive detection of somatic point mutations in impure and heteroge-neous cancer samples. Nat Biotechnol 2013;31:213–9.
25. Talevich E, Shain AH, Botton T, Bastian BC. CNVkit: genome-wide copynumber detection and visualization from targeted DNA sequencing. PLoSComput Biol 2016;12:e1004873.
26. Dobin A, Davis CA, Schlesinger F, Drenkow J, Zaleski C, Jha S, et al. STAR:ultrafast universal RNA-seq aligner. Bioinformatics 2013;29:15–21.
27. Trapnell C, Pachter L, Salzberg SL. TopHat: discovering splice junctionswith RNA-Seq. Bioinformatics 2009;25:1105–11.
28. Trapnell C, Williams BA, Pertea G, Mortazavi A, Kwan G, van Baren MJ,et al. Transcript assembly and quantification by RNA-Seq reveals unan-notated transcripts and isoform switching during cell differentiation. NatBiotechnol 2010;28:511–5.
29. Barbet J, Campion L, Kraeber-Bodere F, Chatal JF, Group GTES. Prognosticimpact of serum calcitonin and carcinoembryonic antigen doubling-timesin patients with medullary thyroid carcinoma. J Clin Endocrinol Metab2005;90:6077–84.
30. Gawlik T, d'Amico A, Szpak-Ulczok S, Skoczylas A, Gubala E, Chorazy A,et al. The prognostic value of tumor markers doubling times in medullarythyroid carcinoma - preliminary report. Thyroid Res 2010;3:10.
31. Mathiesen JS, Kroustrup JP, Vestergaard P, Madsen M, Stochholm K,Poulsen PL, et al. Incidence and prevalence of multiple endocrine neo-plasia 2B in Denmark: a nationwide study. Endocr Relat Cancer 2017;24:L39–L42.
32. Narayanan VK, Ronghe M, MacGregor FB, Bradshaw N, Davidson R,Welbury R, et al. Use of vandetanib in metastatic medullary carcinomaof thyroid in a pediatric patient with multiple endocrine neoplasia 2B.J Pediatr Hematol Oncol 2016;38:155–7.
33. Ernani V, Kumar M, Chen AY, Owonikoko TK. Systemic treatment andmanagement approaches for medullary thyroid cancer. Cancer Treat Rev2016;50:89–98.
34. Meijer JA, le Cessie S, van den Hout WB, Kievit J, Schoones JW, Romijn JA,et al. Calcitonin and carcinoembryonic antigen doubling times as prog-nostic factors in medullary thyroid carcinoma: a structured meta-analysis.Clin Endocrinol 2010;72:534–42.
35. Hajje G, Borget I, Leboulleux S, Chougnet C, Al Ghuzlan A, Mirghani H,et al. Early changes in carcinoembryonic antigen but not in calcitonin levelsare correlated with the progression-free survival in medullary thyroidcarcinoma patients treated with cytotoxic chemotherapy. Eur J Endocrinol2013;168:113–8.
36. Werner RA, Schmid JS, Muegge DO, Luckerath K, Higuchi T, Hanscheid H,et al. Prognostic value of serum tumormarkers inmedullary thyroid cancerpatients undergoing vandetanib treatment. Medicine 2015;94:e2016.
37. KurzrockR, Atkins J,Wheler J, Fu S,NaingA, BusaidyN, et al. Tumormarkerand measurement fluctuations may not reflect treatment efficacy inpatients with medullary thyroid carcinoma on long-term RET inhibitortherapy. Ann Oncol 2013;24:2256–61.
38. Wells SA Jr, Asa SL, Dralle H, Elisei R, Evans DB, Gagel RF, et al. RevisedAmerican Thyroid Association guidelines for the management of medul-lary thyroid carcinoma. Thyroid 2015;25:567–610.
39. Marsh DJ, Theodosopoulos G, Martin-Schulte K, Richardson AL, Philips J,Roher HD, et al. Genome-wide copy number imbalances identified infamilial and sporadic medullary thyroid carcinoma. J Clin EndocrinolMetab 2003;88:1866–72.
40. Ye L, Santarpia L, Cote GJ, El-Naggar AK, Gagel RF. High resolution array-comparative genomic hybridization profiling reveals deoxyribonucleicacid copy number alterations associated with medullary thyroid carcino-ma. J Clin Endocrinol Metab 2008;93:4367–72.
41. Berndt I, Reuter M, Saller B, Frank-Raue K, Groth P, Grussendorf M, et al. Anew hot spot for mutations in the ret protooncogene causing familialmedullary thyroid carcinoma and multiple endocrine neoplasia type 2A.J Clin Endocrinol Metab 1998;83:770–4.
42. Elisei R, Romei C, Cosci B, Agate L, Bottici V, Molinaro E, et al. RET geneticscreening in patients with medullary thyroid cancer and their relatives:experience with 807 individuals at one center. J Clin Endocrinol Metab2007;92:4725–9.
43. Tamburrino A,Molinolo AA, Salerno P, Chernock RD, RaffeldM, Xi L, et al.Activation of the mTOR pathway in primary medullary thyroid carcinomaand lymph node metastases. Clin Cancer Res 2012;18:3532–40.
44. Kouvaraki MA, Liakou C, Paraschi A, Dimas K, Patsouris E, Tseleni-Balafouta S, et al. Activation of mTOR signaling in medullary and aggres-sive papillary thyroid carcinomas. Surgery 2011;150:1258–65.
45. Gild ML, Landa I, Ryder M, Ghossein RA, Knauf JA, Fagin JA. TargetingmTOR in RET mutant medullary and differentiated thyroid cancer cells.Endocr Relat Cancer 2013;20:659–67.
46. Manfredi GI, Dicitore A, Gaudenzi G, CaragliaM, Persani L, Vitale G. PI3K/Akt/mTOR signaling in medullary thyroid cancer: a promising moleculartarget for cancer therapy. Endocrine 2015;48:363–70.
47. Lim SM, Chang H, Yoon MJ, Hong YK, Kim H, Chung WY, et al. Amulticenter, phase II trial of everolimus in locally advanced or metastaticthyroid cancer of all histologic subtypes. Ann Oncol 2013;24:3089–94.
48. Das S, Kelly D, Moran B, Han K, Mulligan N, Barrett C, et al. Postmortemexamination of an aggressive case of medullary thyroid carcinoma char-acterized by catastrophic genomic abnormalities. JCO Precision Oncol2017 Jun 5. Doi: 10.1200/PO.16.00063. [Epub ahead of print].
49. Negrini S, Gorgoulis VG,Halazonetis TD.Genomic instability–an evolvinghallmark of cancer. Nat Rev Mol Cell Biol 2010;11:220–8.
50. Buccitelli C, Salgueiro L, Rowald K, Sotillo R, Mardin BR, Korbel JO. Pan-cancer analysis distinguishes transcriptional changes of aneuploidy fromproliferation. Genome Res 2017;27:501–11.
www.aacrjournals.org Clin Cancer Res; 24(4) February 15, 2018 765
Hereditary Medullary Thyroid Cancer Treated with Vandetanib
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101

2018;24:753-765. Published OnlineFirst November 29, 2017.Clin Cancer Res Ira L. Kraft, Srivandana Akshintala, Yuelin Zhu, et al. Medullary Thyroid Carcinoma Treated with VandetanibOutcomes of Children and Adolescents with Advanced Hereditary
Updated version
10.1158/1078-0432.CCR-17-2101doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2017/11/29/1078-0432.CCR-17-2101.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/24/4/753.full#ref-list-1
This article cites 48 articles, 15 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/24/4/753To request permission to re-use all or part of this article, use this link
on March 27, 2020. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst November 29, 2017; DOI: 10.1158/1078-0432.CCR-17-2101