Embed Size (px)
Citation preview
Overview of Colorectal Cancer and CRC Screening Program
CDC CRC Control ProgramDHMH—Baltimore City
March 29, 2010
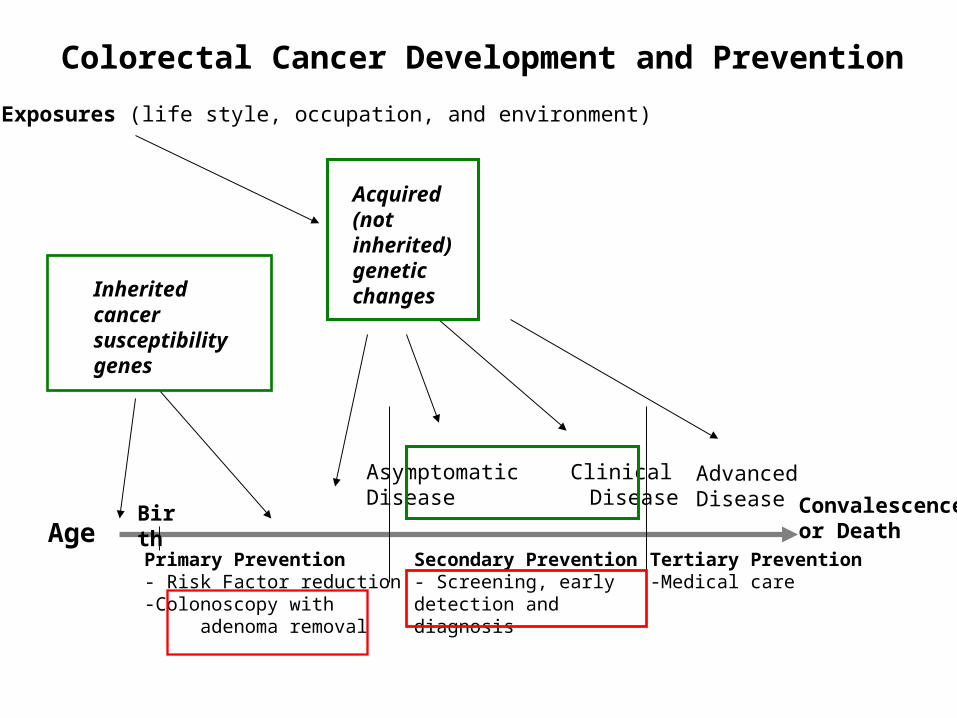
Birth
Inheritedcancer susceptibilitygenes
Age
Asymptomatic ClinicalDisease Disease
AdvancedDisease
Exposures (life style, occupation, and environment)
Acquired (not inherited) genetic changes
Primary Prevention- Risk Factor reduction-Colonoscopy with adenoma removal
Secondary Prevention- Screening, early detection and diagnosis
Convalescenceor Death
Tertiary Prevention-Medical care
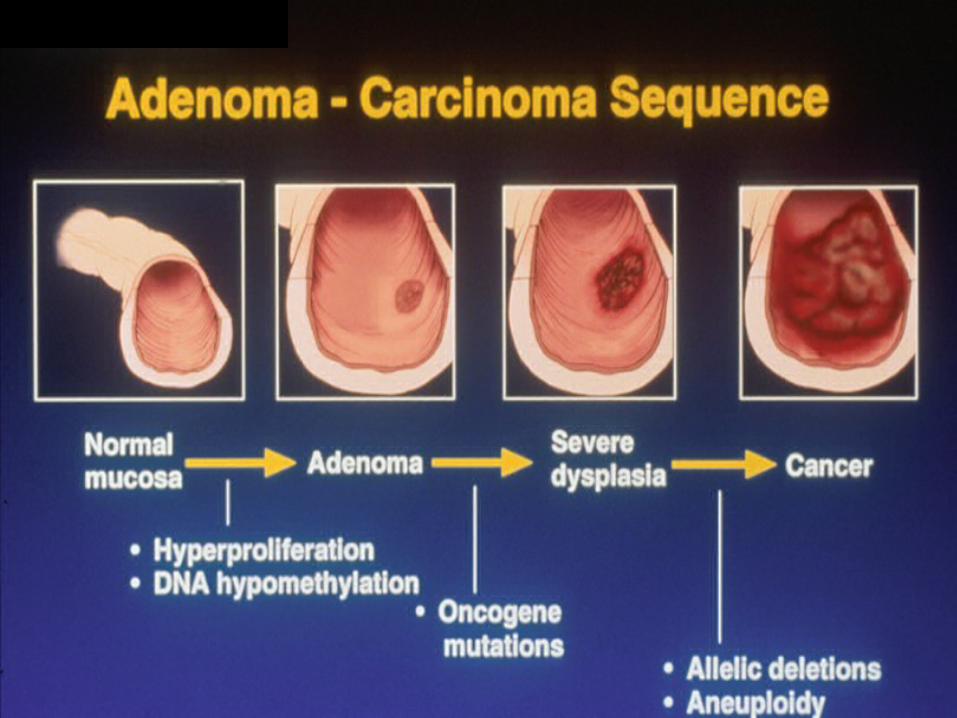
Colorectal Cancer Development and Prevention
CRC Incidence and Mortality
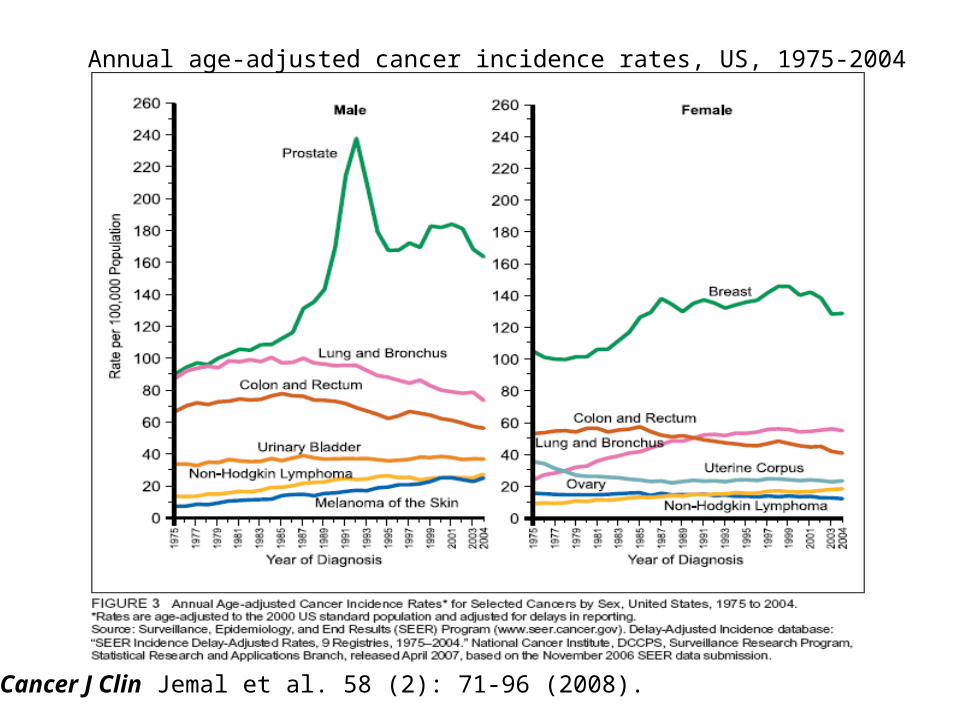
Annual age-adjusted cancer incidence rates, US, 1975-2004
CA Cancer J Clin Jemal et al. 58 (2): 71-96 (2008).
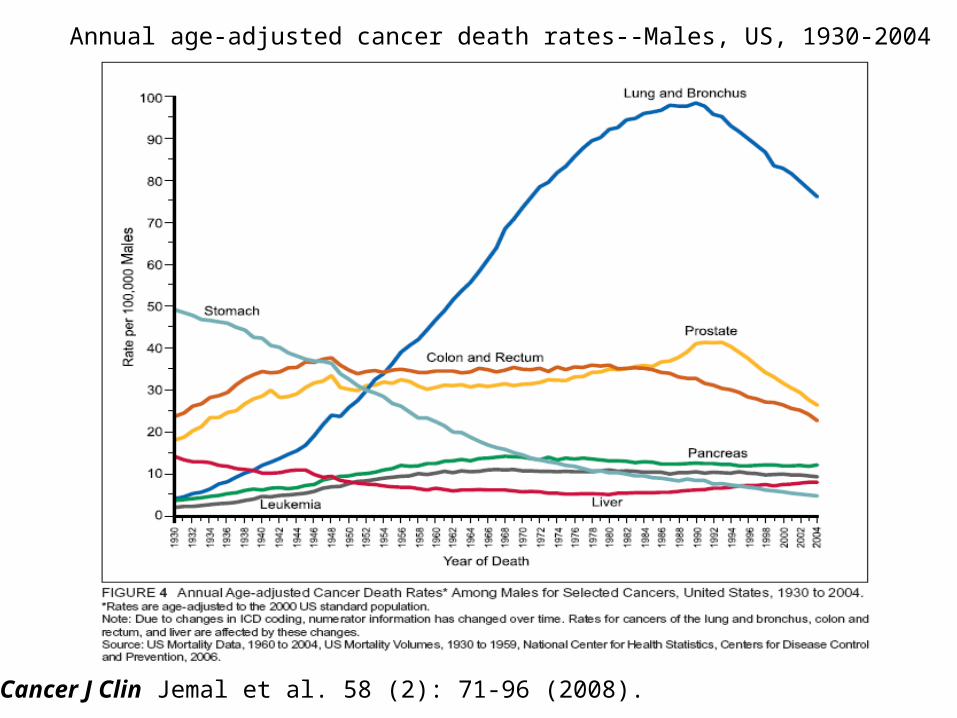
Annual age-adjusted cancer death rates--Males, US, 1930-2004
CA Cancer J Clin Jemal et al. 58 (2): 71-96 (2008).
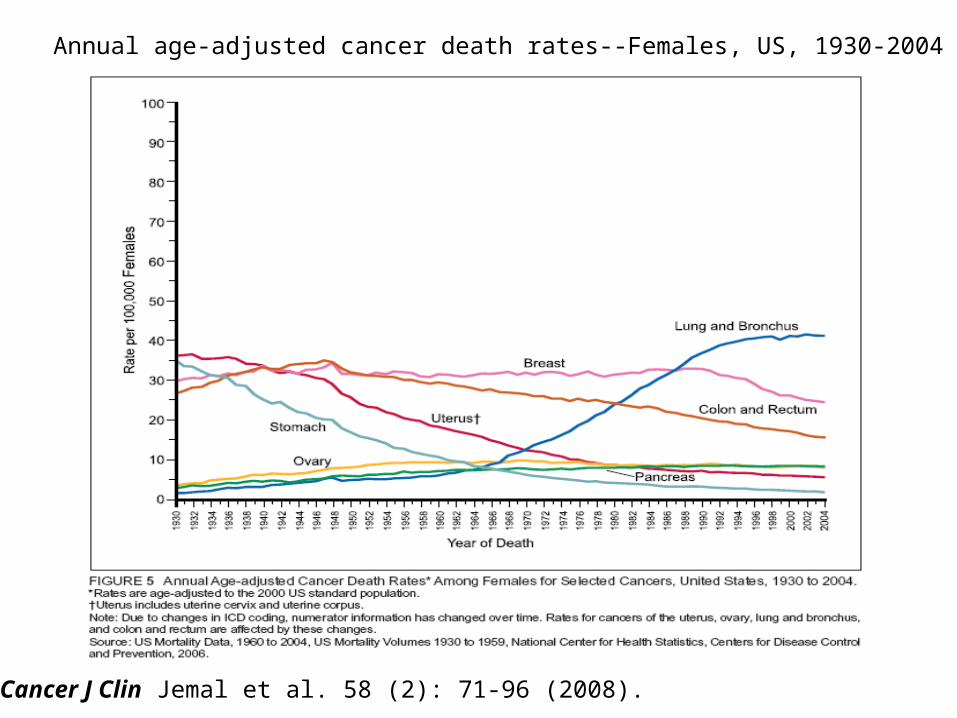
Annual age-adjusted cancer death rates--Females, US, 1930-2004
CA Cancer J Clin Jemal et al. 58 (2): 71-96 (2008).
CRC Screening
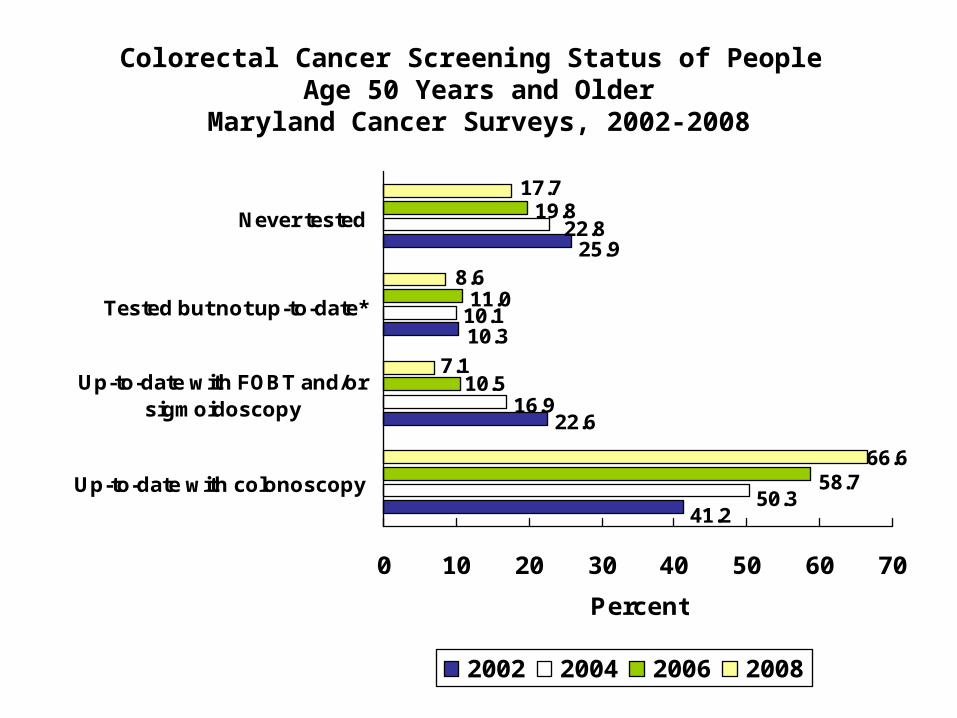
Colorectal Cancer Screening Status of People Age 50 Years and Older
Maryland Cancer Surveys, 2002-2008
22.616.9
10.111.0
19.8
25.9
10.3
41.2
22.8
50.3
10.5
58.7
8.6
7.1
17.7
66.6
0 10 20 30 40 50 60 70
Up-to-date with colonoscopy
Up-to-date with FOBT and/orsigmoidoscopy
Tested but not up-to-date*
Never tested
Percent
2002 2004 2006 2008
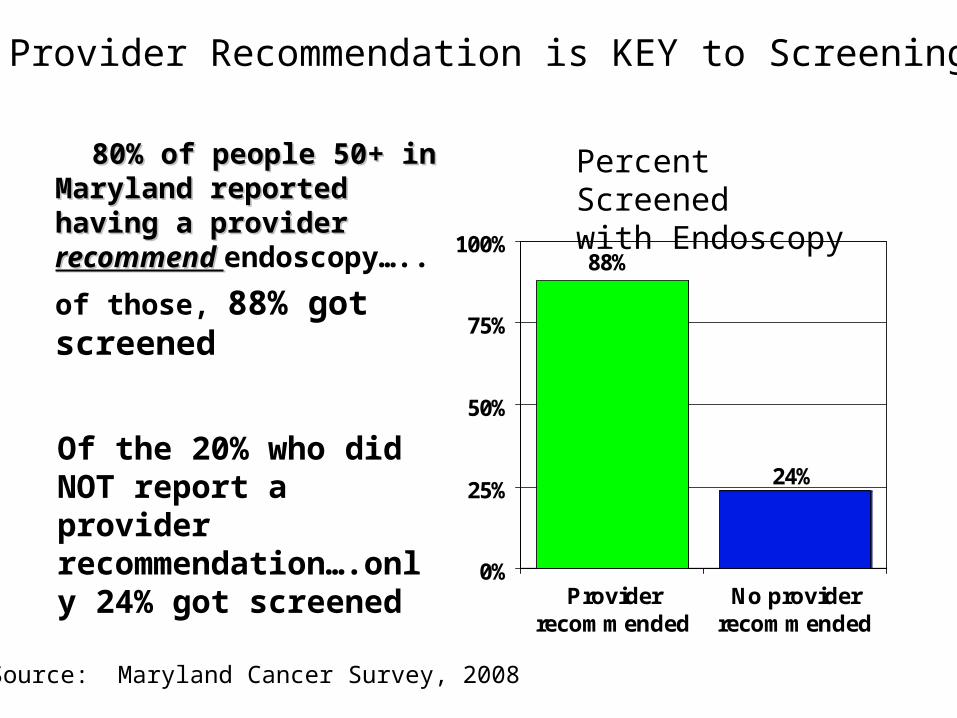
80% of people 50+ in 80% of people 50+ in Maryland reported having a Maryland reported having a provider provider recommend recommend endoscopy…..
of those, 88% got screened
88%
24%
0%
25%
50%
75%
100%
Providerrecommended
No providerrecommended
Percent Screened with Endoscopy
Source: Maryland Cancer Survey, 2008
Provider Recommendation is KEY to Screening
Of the 20% who did NOT report a provider recommendation….only 24% got screened
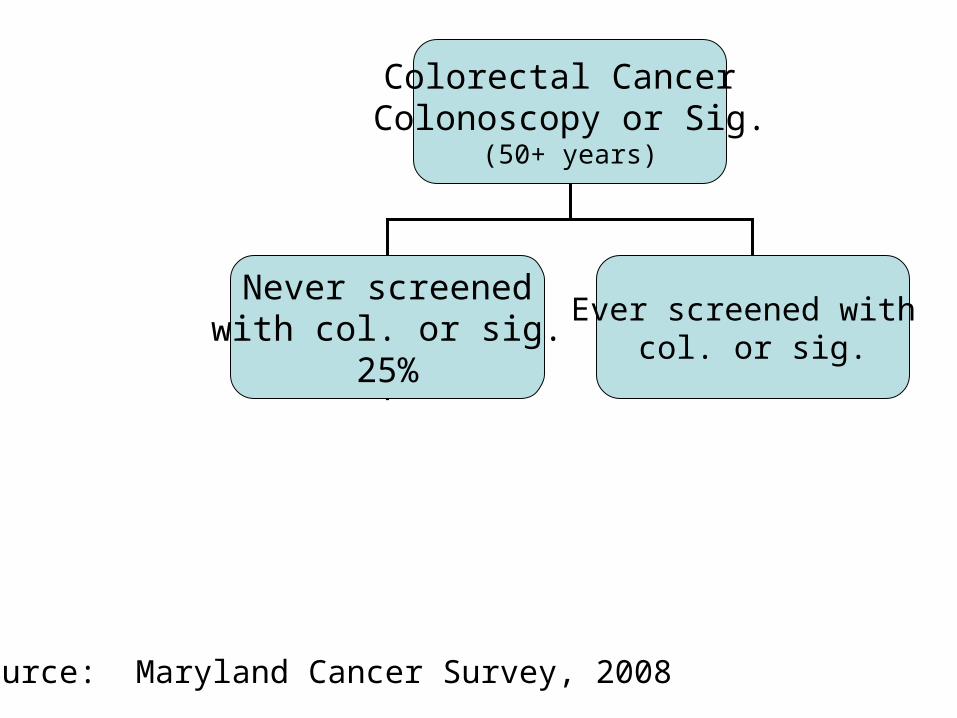
Colorectal Cancer Colonoscopy or Sig.
(50+ years)
Never screenedwith col. or sig.
25%
Ever screened with col. or sig.
Source: Maryland Cancer Survey, 2008
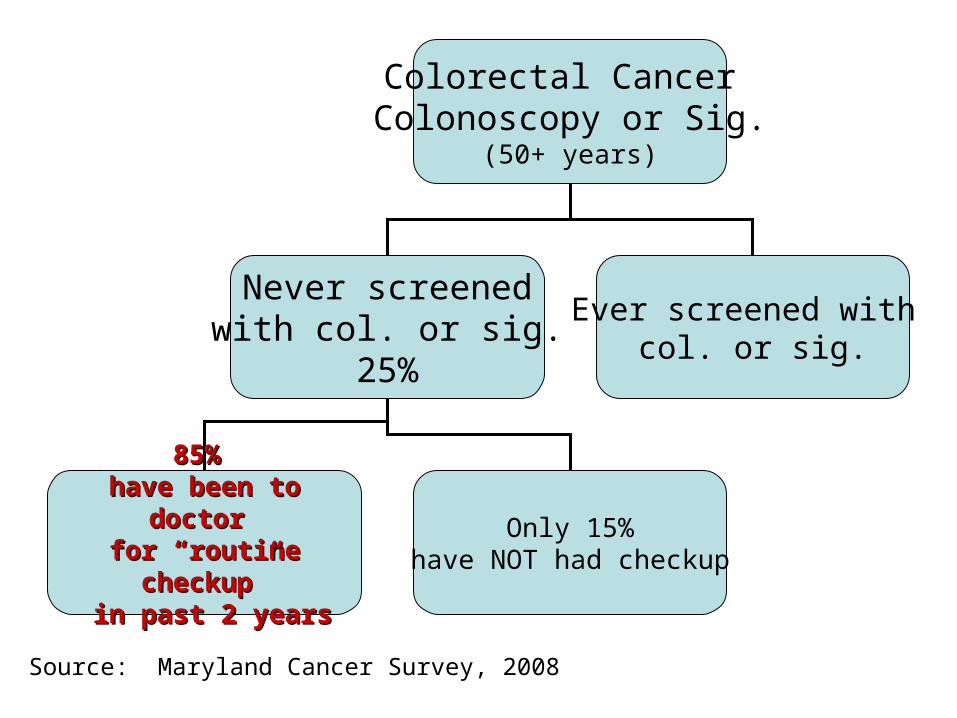
Colorectal Cancer Colonoscopy or Sig.
(50+ years)
Never screenedwith col. or sig.
25%
Ever screened with col. or sig.
85% 85% have been to doctor have been to doctor
for “routine checkup”for “routine checkup” in past 2 yearsin past 2 years
Only 15%have NOT had checkup
Source: Maryland Cancer Survey, 2008
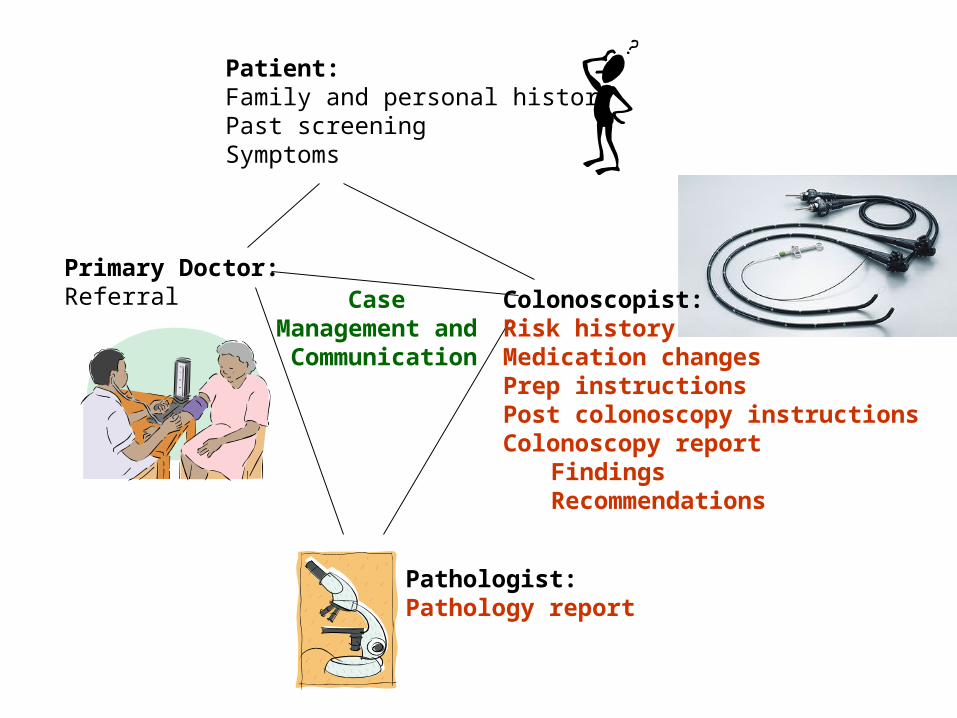
Patient:Family and personal historyPast screeningSymptoms
Primary Doctor:Referral
Pathologist:Pathology report
Case Management and Communication
Colonoscopist:Risk historyMedication changesPrep instructionsPost colonoscopy instructionsColonoscopy report
FindingsRecommendations

Who needs CRC screening?Who needs CRC screening?
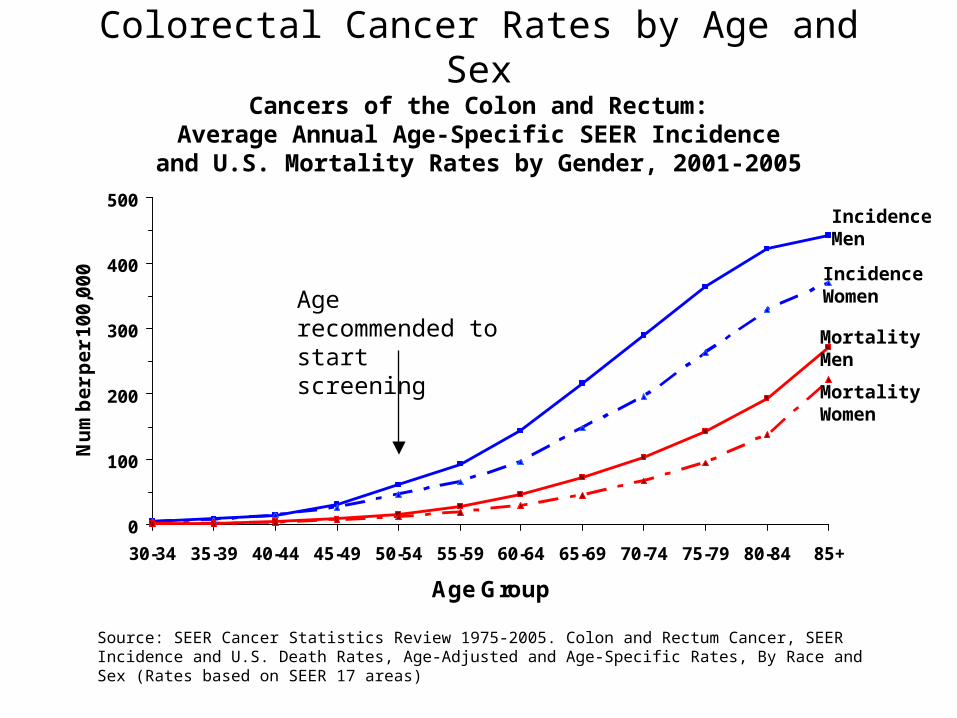
Colorectal Cancer Rates by Age and SexCancers of the Colon and Rectum:
Average Annual Age-Specific SEER Incidenceand U.S. Mortality Rates by Gender, 2001-2005
Source: SEER Cancer Statistics Review 1975-2005. Colon and Rectum Cancer, SEER Incidence and U.S. Death Rates, Age-Adjusted and Age-Specific Rates, By Race and Sex (Rates based on SEER 17 areas)
0
100
200
300
400
500
30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Age Group
Nu
mb
er
pe
r 1
00
,00
0
Incidence Men
Incidence Women
MortalityMen
MortalityWomen
Age recommended to start screening
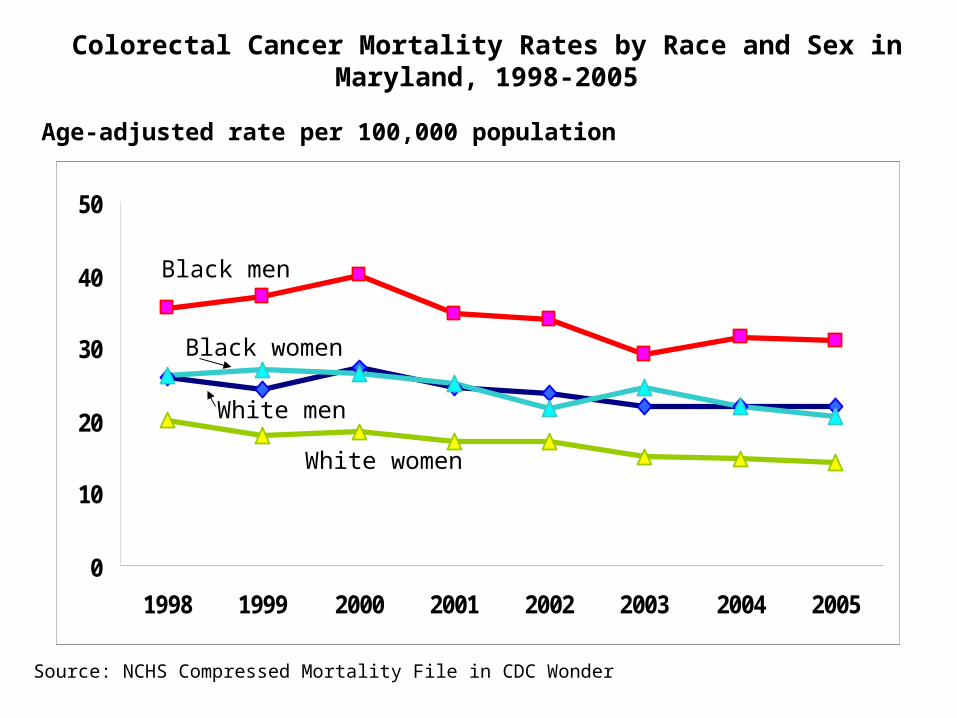
Colorectal Cancer Mortality Rates by Race and Sex in Maryland, 1998-2005
Age-adjusted rate per 100,000 population
Source: NCHS Compressed Mortality File in CDC Wonder
0
10
20
30
40
50
1998 1999 2000 2001 2002 2003 2004 2005
White men
Black women
White women
Black men
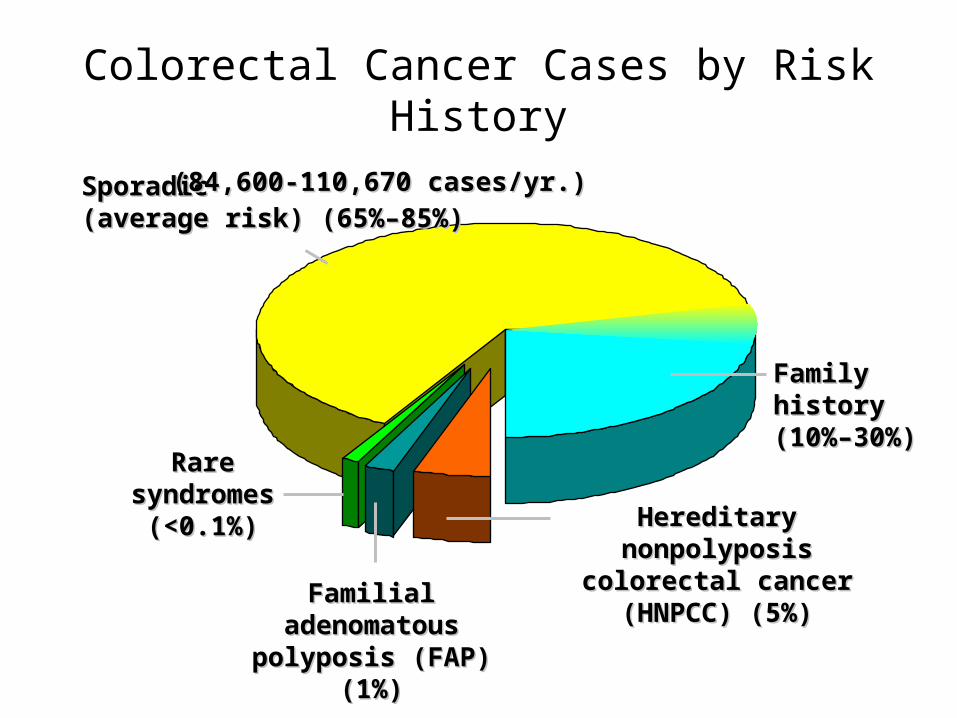
Colorectal Cancer Cases by Risk History
Sporadic Sporadic (average risk) (65%–85%)(average risk) (65%–85%)
FamilyFamilyhistoryhistory(10%–30%)(10%–30%)
Hereditary nonpolyposis Hereditary nonpolyposis colorectal cancer colorectal cancer
(HNPCC) (5%)(HNPCC) (5%)Familial adenomatous Familial adenomatous polyposis (FAP) (1%)polyposis (FAP) (1%)
Rare Rare syndromes syndromes
(<0.1%)(<0.1%)
(84,600-110,670 cases/yr.)(84,600-110,670 cases/yr.)
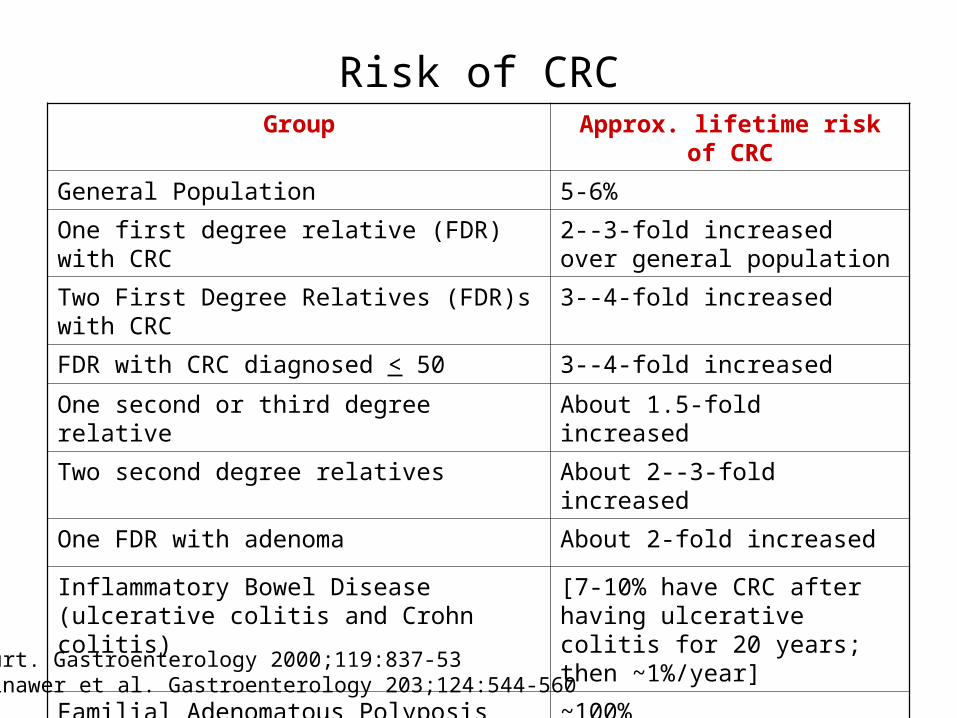
Risk of CRCGroup Approx. lifetime risk of CRC
General Population 5-6%
One first degree relative (FDR) with CRC 2--3-fold increased over general population
Two First Degree Relatives (FDR)s with CRC 3--4-fold increased
FDR with CRC diagnosed < 50 3--4-fold increased
One second or third degree relative About 1.5-fold increased
Two second degree relatives About 2--3-fold increased
One FDR with adenoma About 2-fold increased
Inflammatory Bowel Disease (ulcerative colitis and Crohn colitis)
[7-10% have CRC after having ulcerative colitis for 20 years; then ~1%/year]
Familial Adenomatous Polyposis
Hereditary Non-polyposis Colorectal Cancer
~100%
~80+%
Burt. Gastroenterology 2000;119:837-53 Winawer et al. Gastroenterology 203;124:544-560
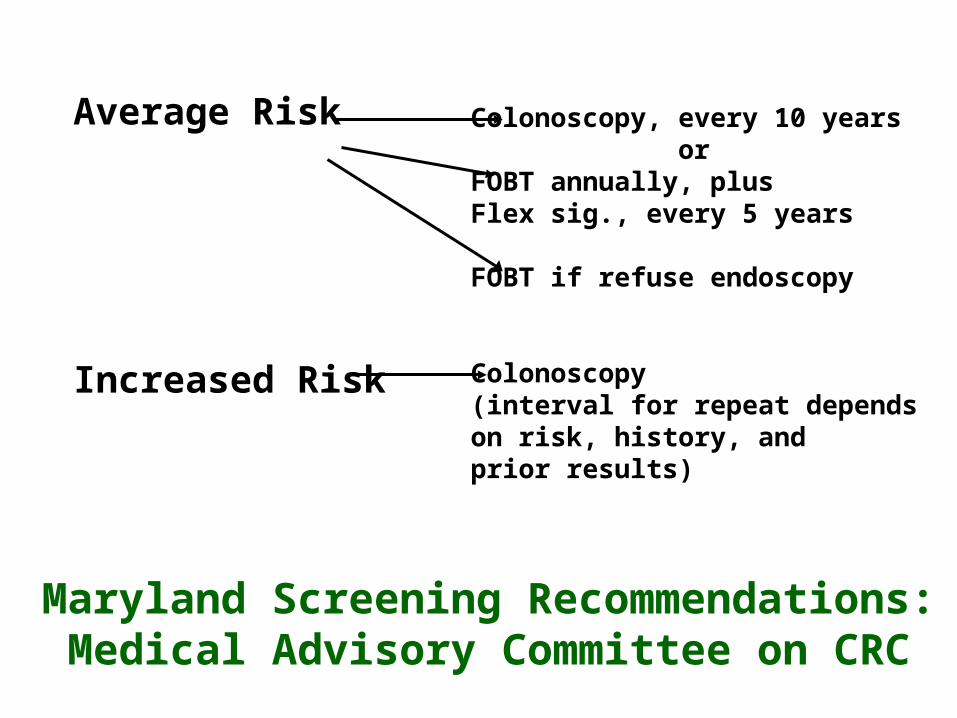
Average Risk
Increased Risk
Colonoscopy, every 10 years orFOBT annually, plus Flex sig., every 5 years
FOBT if refuse endoscopy
Colonoscopy(interval for repeat depends on risk, history, and prior results)
Maryland Screening Recommendations:Medical Advisory Committee on CRC
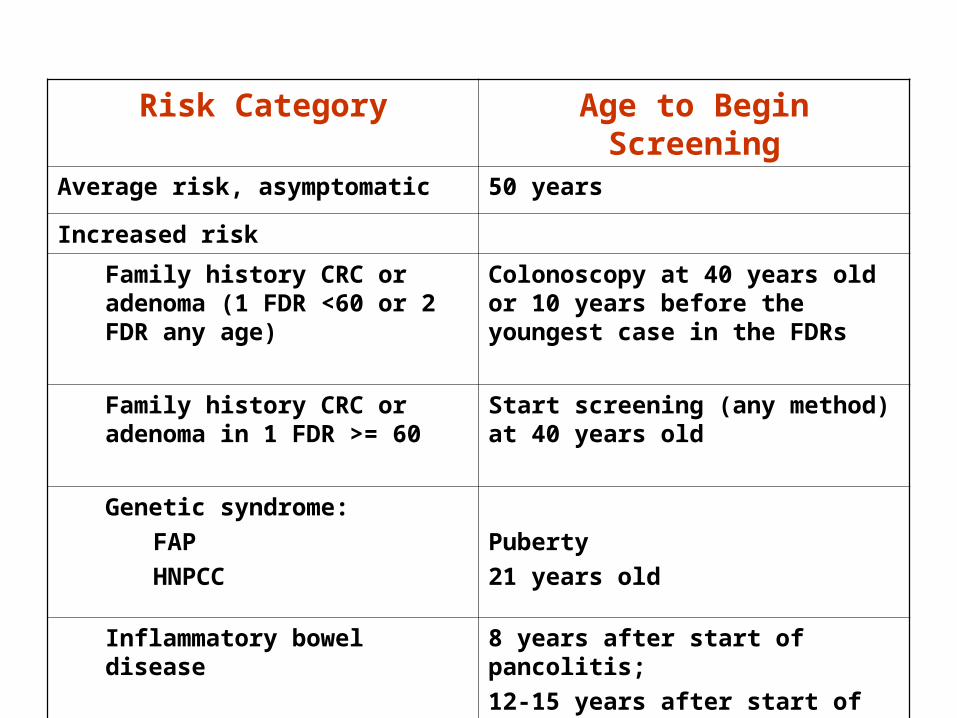
Risk Category Age to Begin ScreeningAverage risk, asymptomatic 50 years
Increased risk
Family history CRC or adenoma (1 FDR <60 or 2 FDR any age)
Colonoscopy at 40 years old or 10 years before the youngest case in the FDRs
Family history CRC or adenoma in 1 FDR >= 60
Start screening (any method) at 40 years old
Genetic syndrome:
FAP
HNPCC
Puberty
21 years old
Inflammatory bowel disease 8 years after start of pancolitis;
12-15 years after start of left sided colitis
See Program Manual 1A, Attachment 1
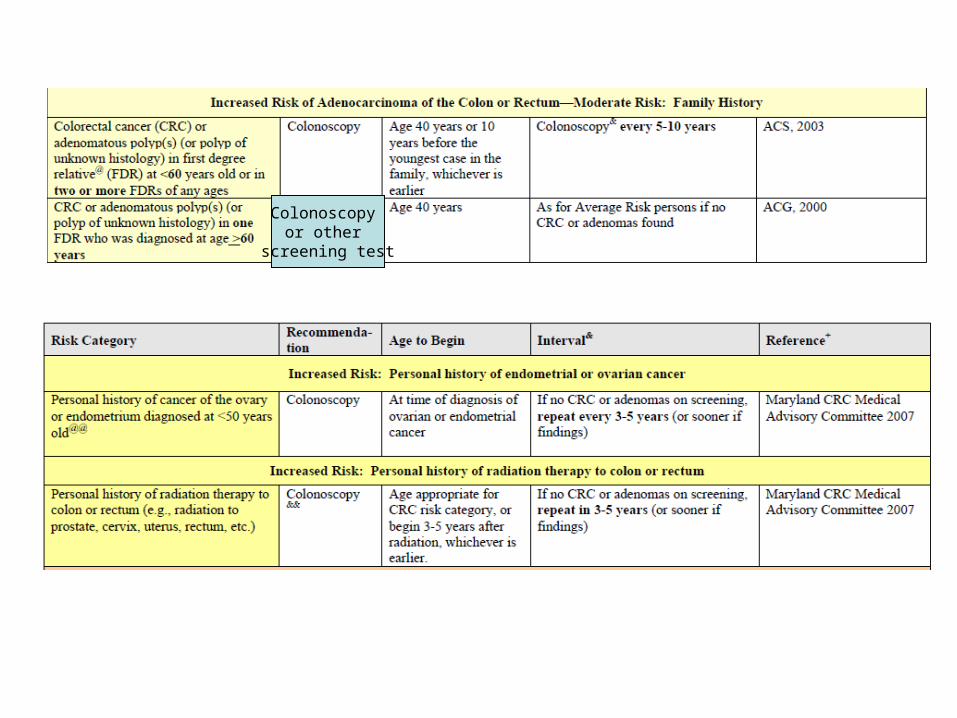
Colonoscopy or other
screening test
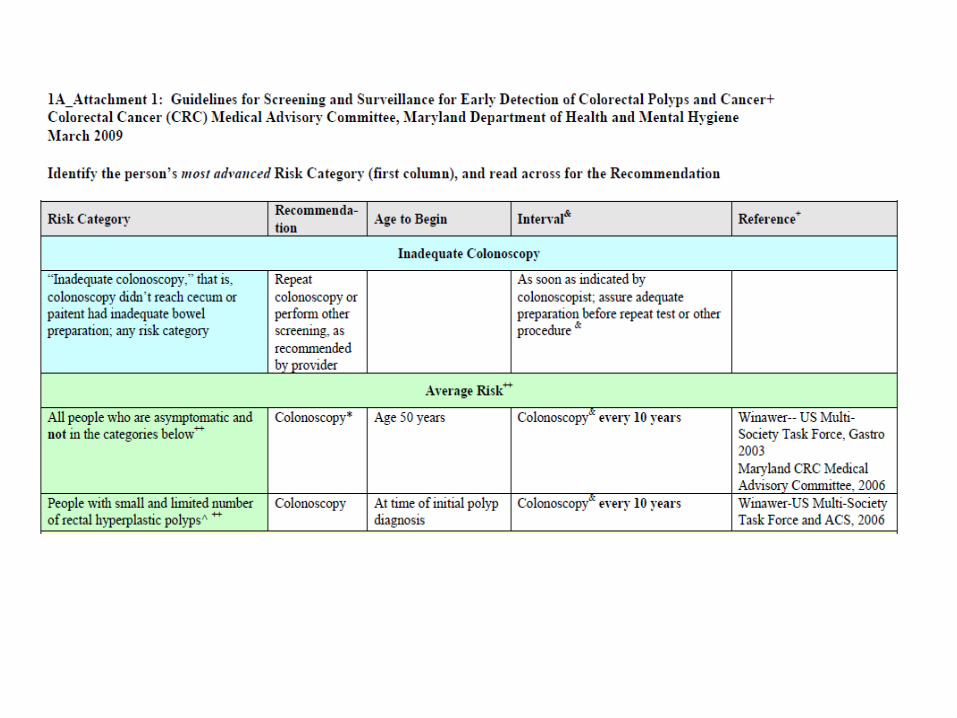
New Guidelines
Screening and Surveillance for the Early Detection of Colorectal Cancer and
Adenomatous Polyps, 2008:
A Joint Guideline from the American Cancer Society,
the US Multi-Society Task Force on CRC, and the American College of Radiology
CA Cancer J Clin 58: 130-160 (May 2008)
Tests that Find Both Polyps and Cancer
Flexible sigmoidoscopy every 5 years
Colonoscopy every 10 years
Double contrast barium enema every 5 years
CT colonography (virtual colonoscopy) every 5 years
New Guidelines American Cancer Society, May 2008
Tests that Primarily Find Cancer
Guaiac-based fecal occult blood testing (gFOBT) every year
Fecal immunochemical test (FIT) every year
Stool DNA test (unclear how often this is needed)
New Guidelines American Cancer Society, May 2008
New CRC Screening Guidelines American Cancer Society, May 2008
• Beginning at age 50, men and women at average risk for CRC should use one of the screening tests
• The tests that are designed to find both early cancer and polyps are preferred if these tests are available to you and you are willing to have one of these more invasive tests.
• Talk to your doctor about which test is best for you.
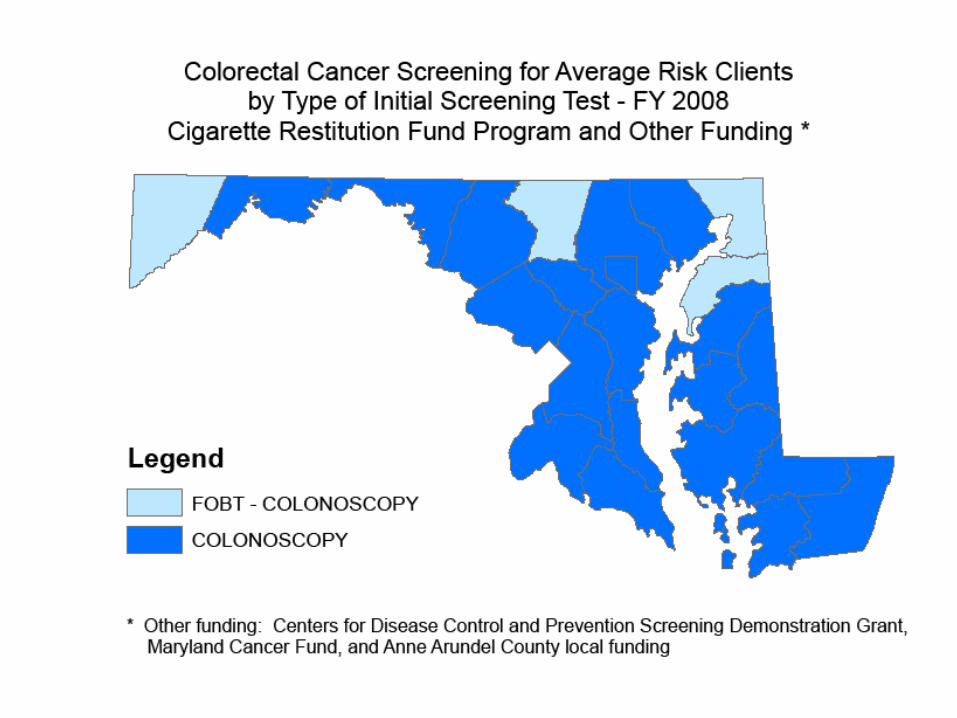
CRC Screening Program in Maryland
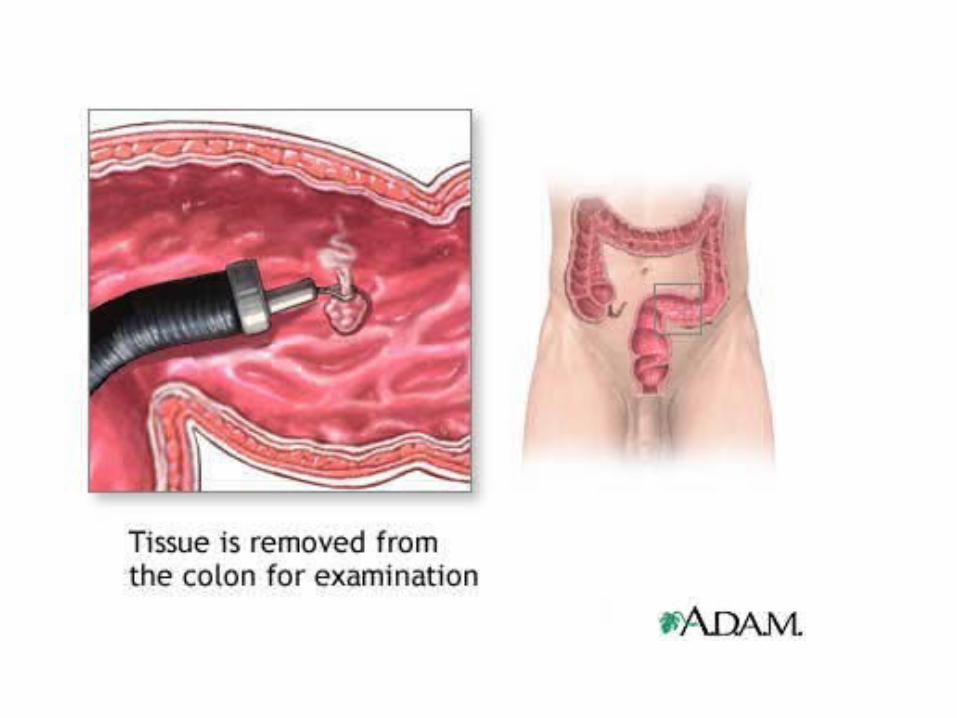
Colonoscopy Equipment

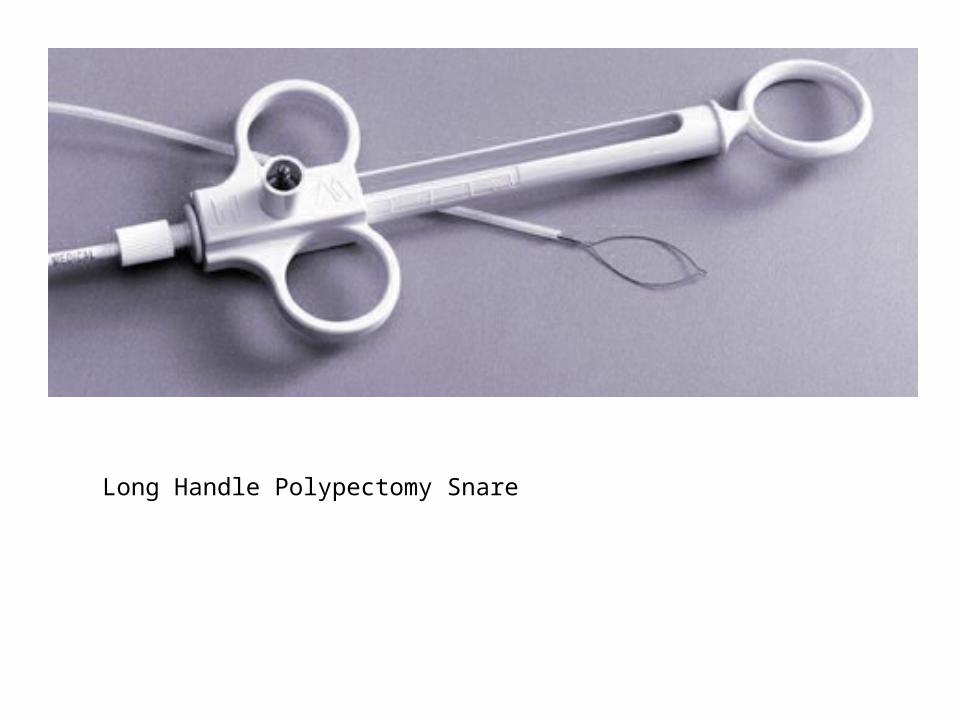
Long Handle Polypectomy Snare
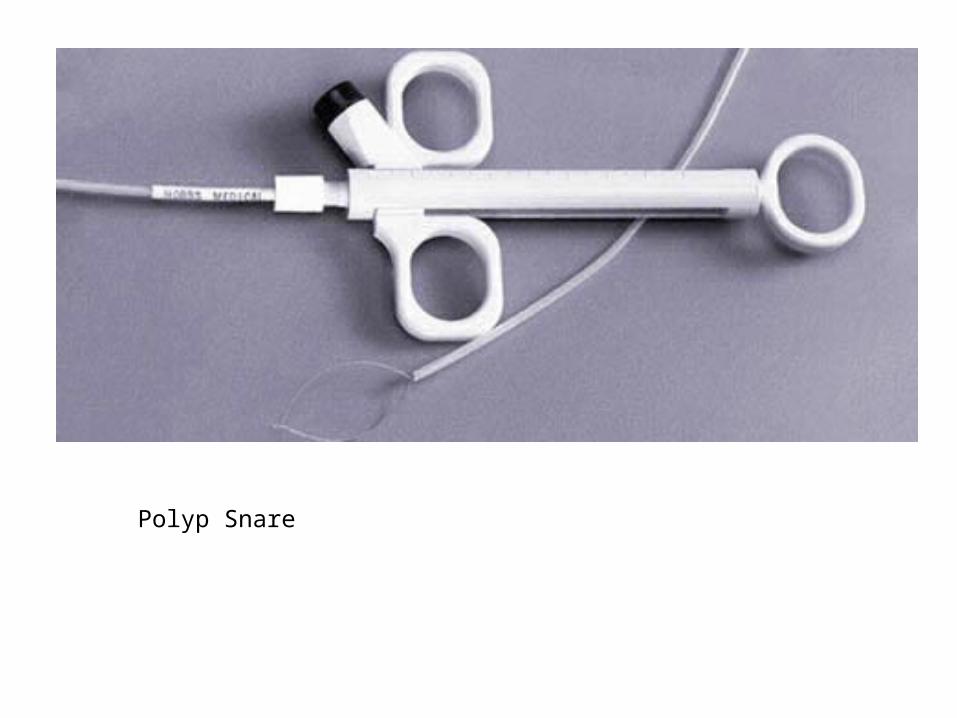
Polyp Snare
Reusable Biopsy Forceps
Hot Biopsy Forceps
Disposable Retriever
Prong Retriever
Brush Biopsy
Injection
Colonoscopy Findings: Pathology
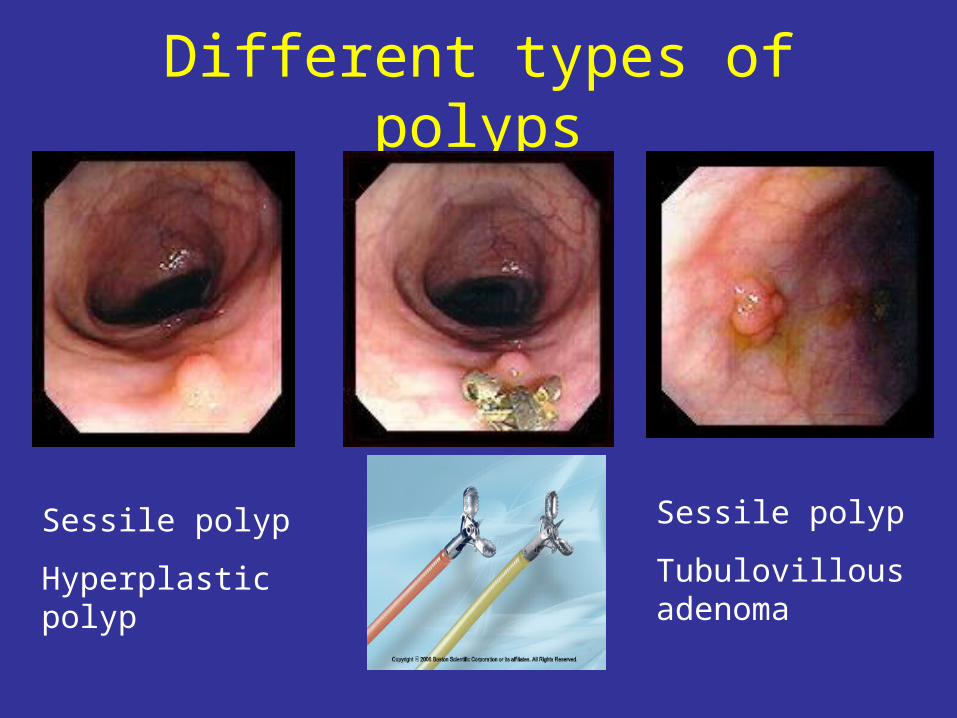
Different types of polyps
Sessile polyp
Hyperplastic polyp
Sessile polyp
Tubulovillous adenoma
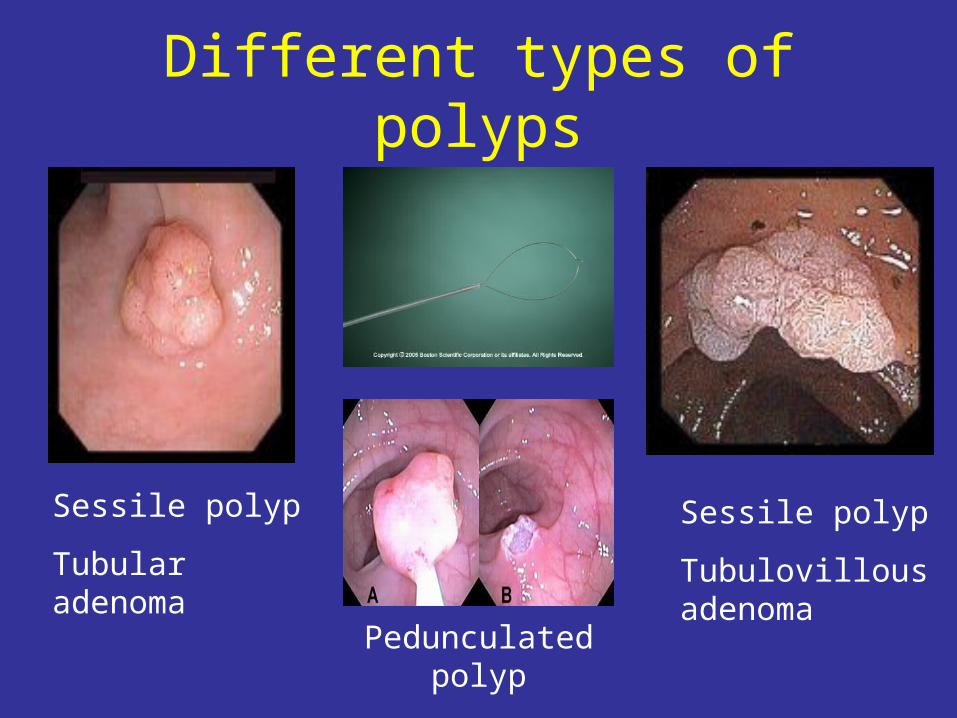
Different types of polyps
Sessile polyp
Tubular adenoma
Sessile polyp
Tubulovillous adenoma
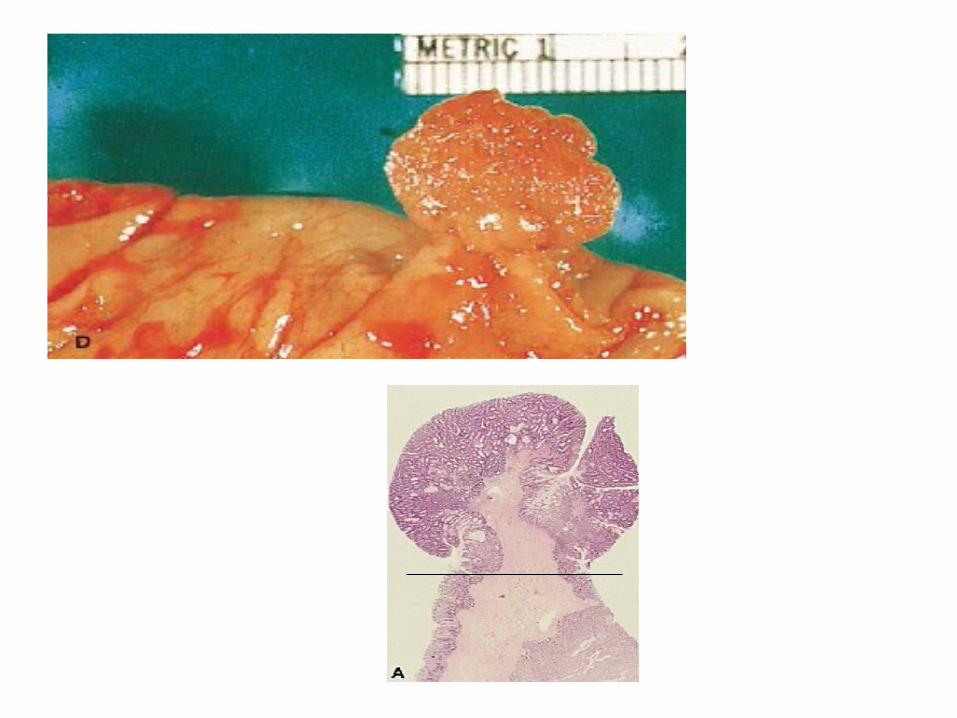
Pedunculated polyp
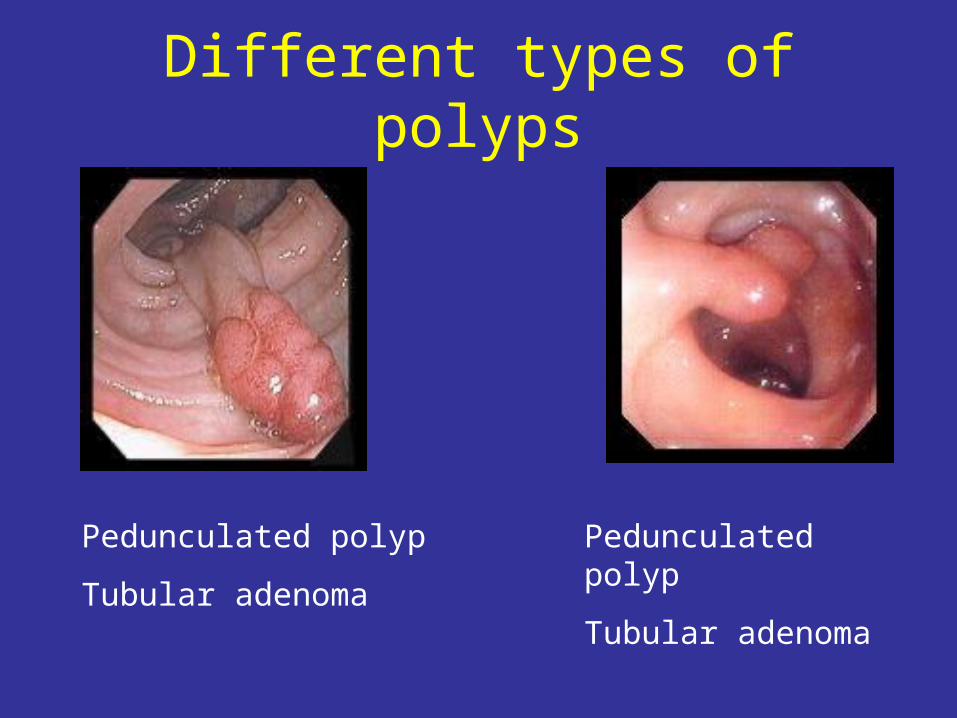
Different types of polyps
Pedunculated polyp
Tubular adenoma
Pedunculated polyp
Tubular adenoma
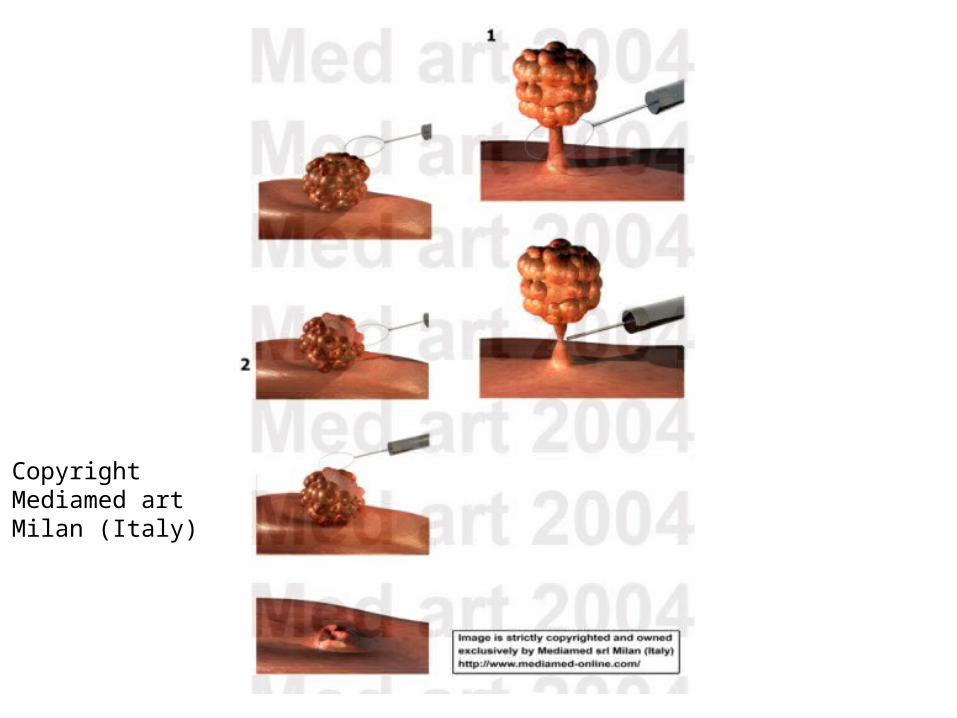
CopyrightMediamed artMilan (Italy)
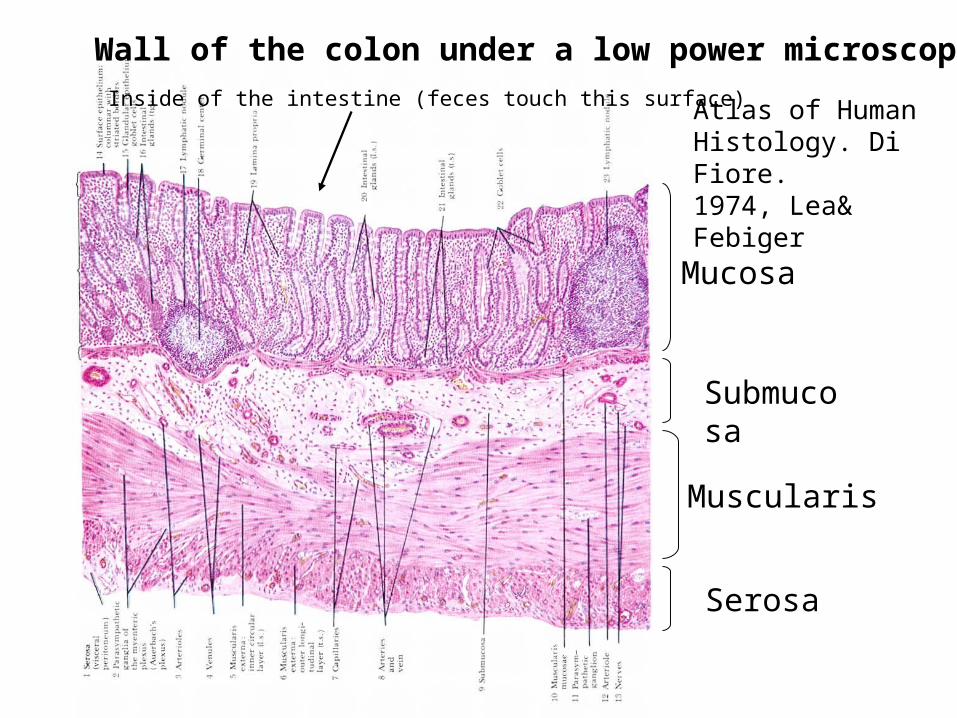
Wall of the colon under a low power microscope
Mucosa
Submucosa
Muscularis
Serosa
Atlas of Human Histology. Di Fiore. 1974, Lea& Febiger
Inside of the intestine (feces touch this surface)
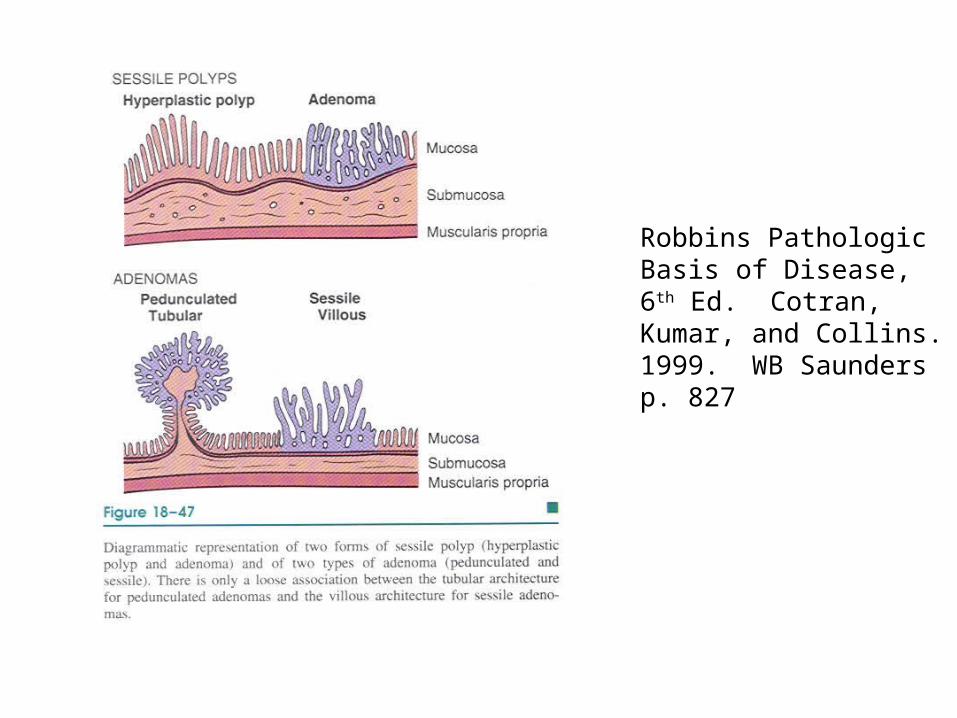
Robbins Pathologic Basis of Disease, 6th Ed. Cotran, Kumar, and Collins. 1999. WB Saundersp. 827
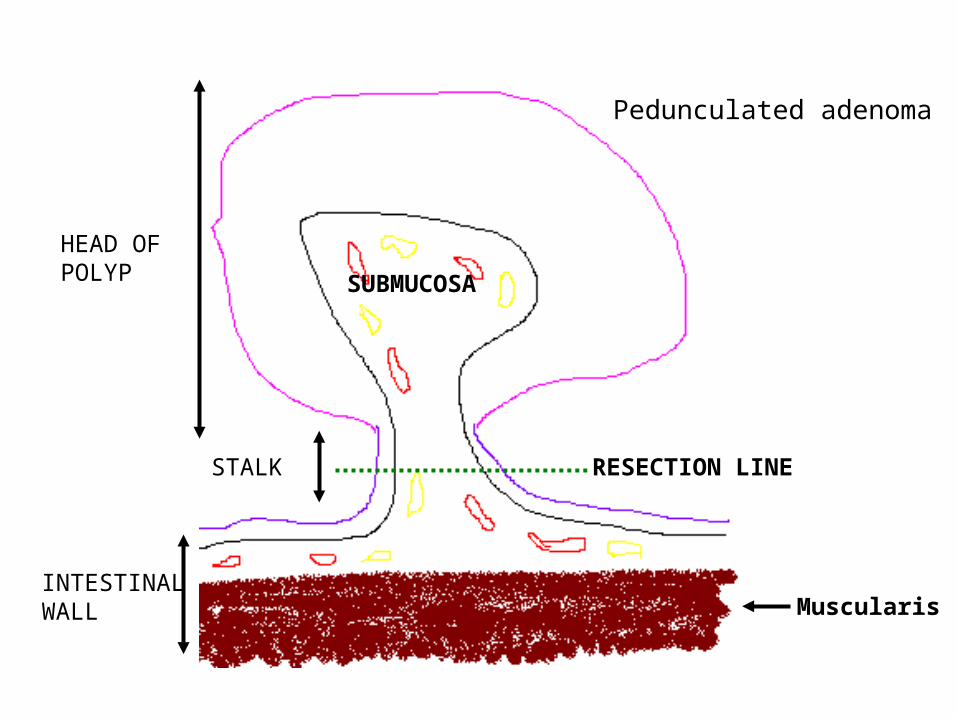
RESECTION LINE
SUBMUCOSA
HEAD OFPOLYP
STALK
INTESTINALWALL Muscularis
Pedunculated adenoma
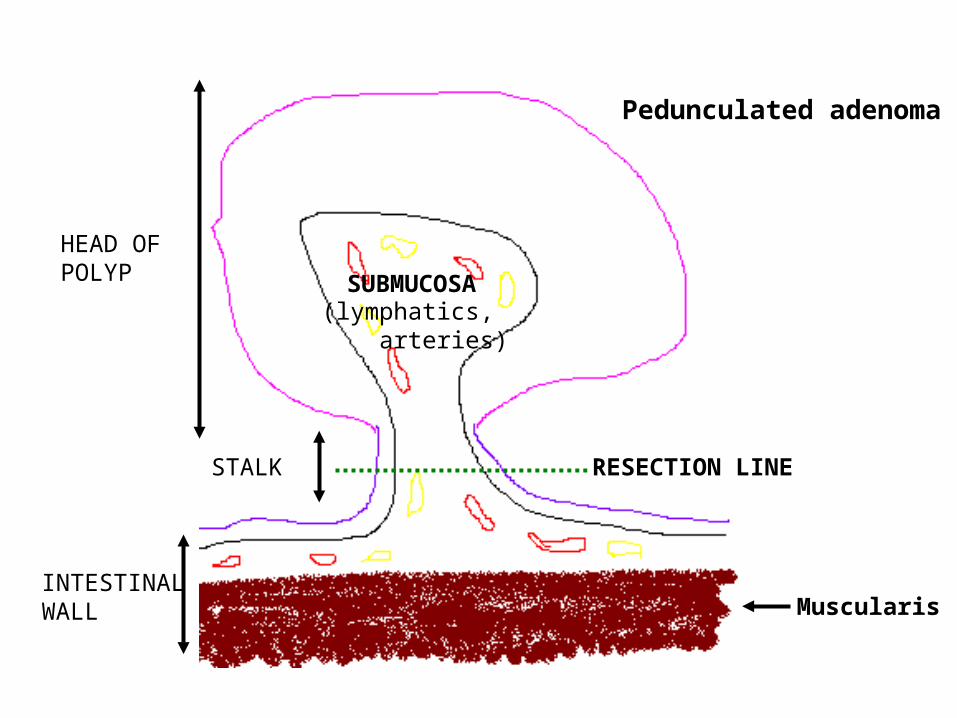
RESECTION LINE
SUBMUCOSA
HEAD OFPOLYP
STALK
INTESTINALWALL
(lymphatics, arteries)
Pedunculated adenoma
Muscularis
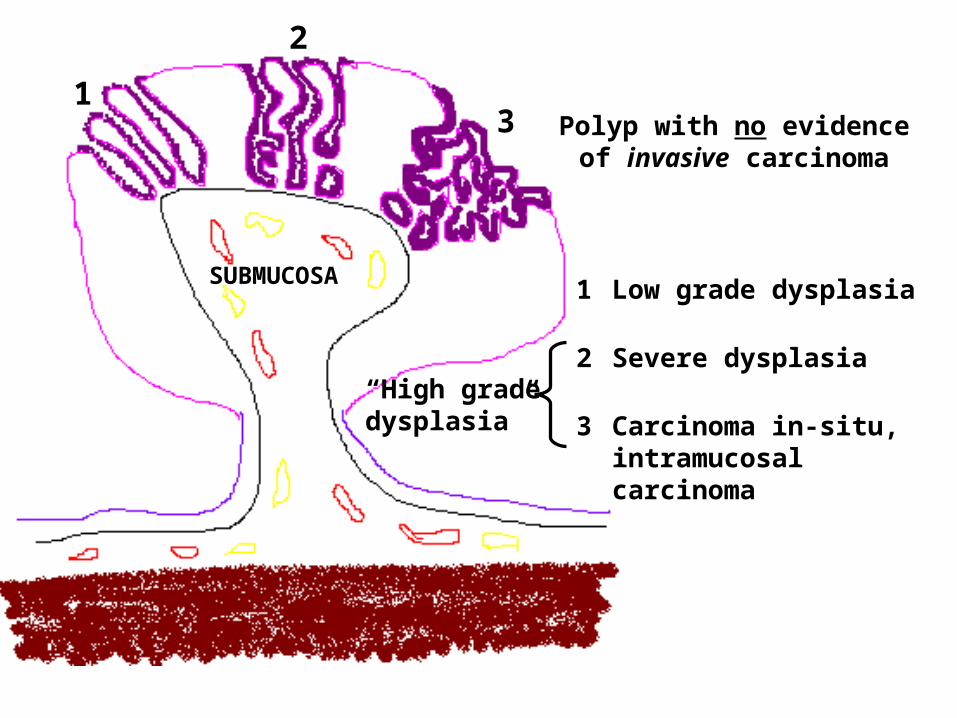
1
2
3
SUBMUCOSA1 Low grade dysplasia
2 Severe dysplasia
3 Carcinoma in-situ, intramucosal carcinoma
Polyp with no evidence of invasive carcinoma
“High gradedysplasia”
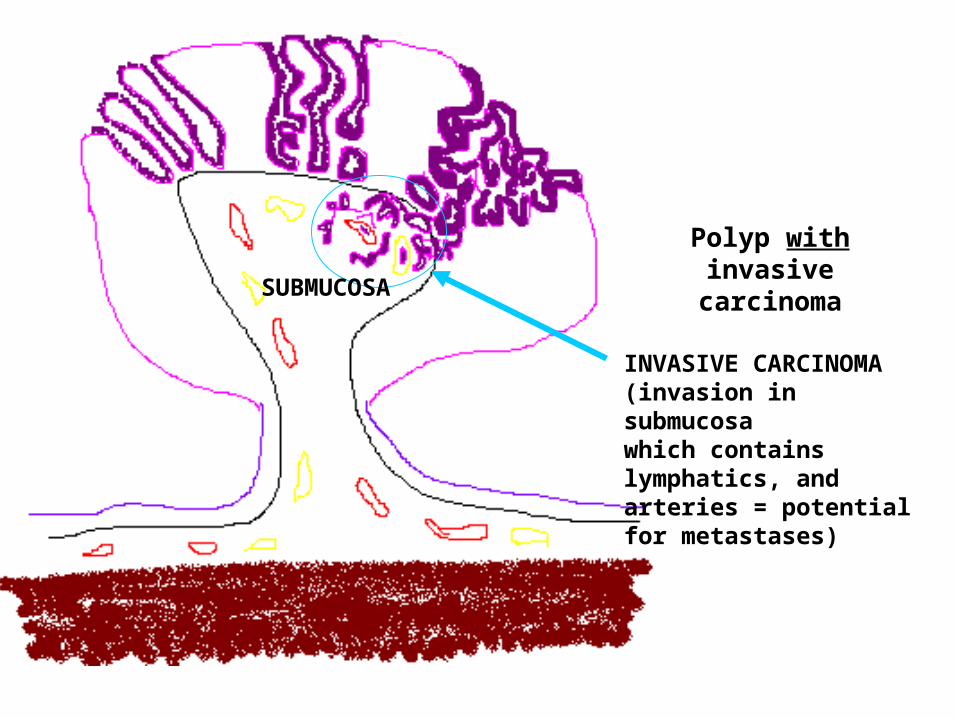
SUBMUCOSA
INVASIVE CARCINOMA(invasion in submucosa which contains lymphatics, and arteries = potential for metastases)
Polyp with invasive carcinoma
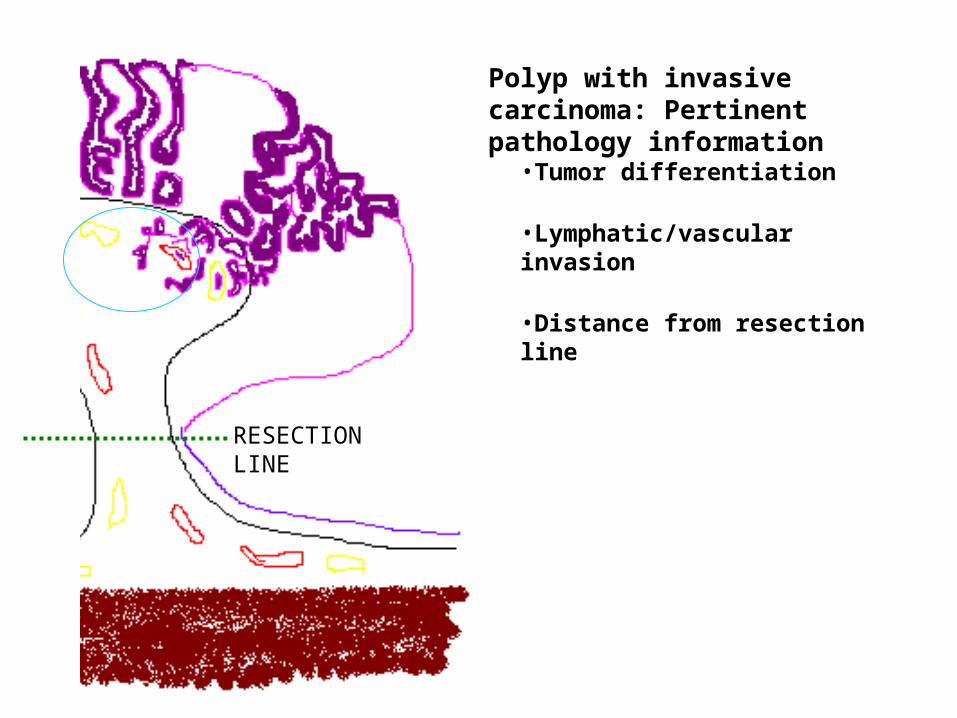
Polyp with invasive carcinoma: Pertinent pathology information
•Tumor differentiation
•Lymphatic/vascular invasion
•Distance from resection line
RESECTION LINE
Sessile Polyps
• Usually submitted in several pieces• Difficult to determine the orientation of the specimen
(“is the margin free of tumor?”)• Other issues—type of polyp?
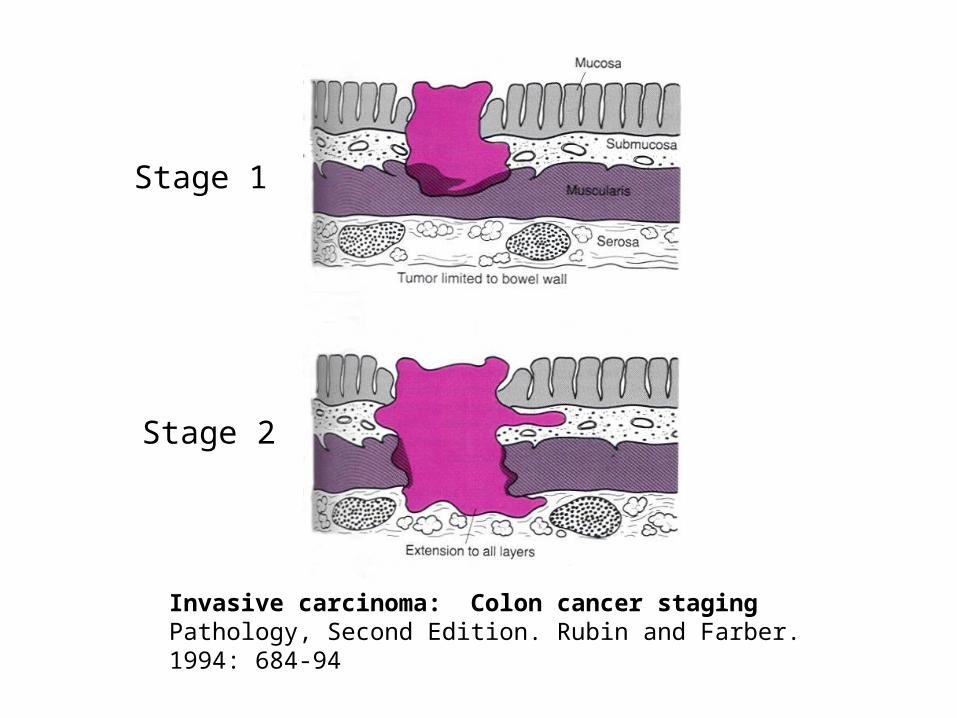
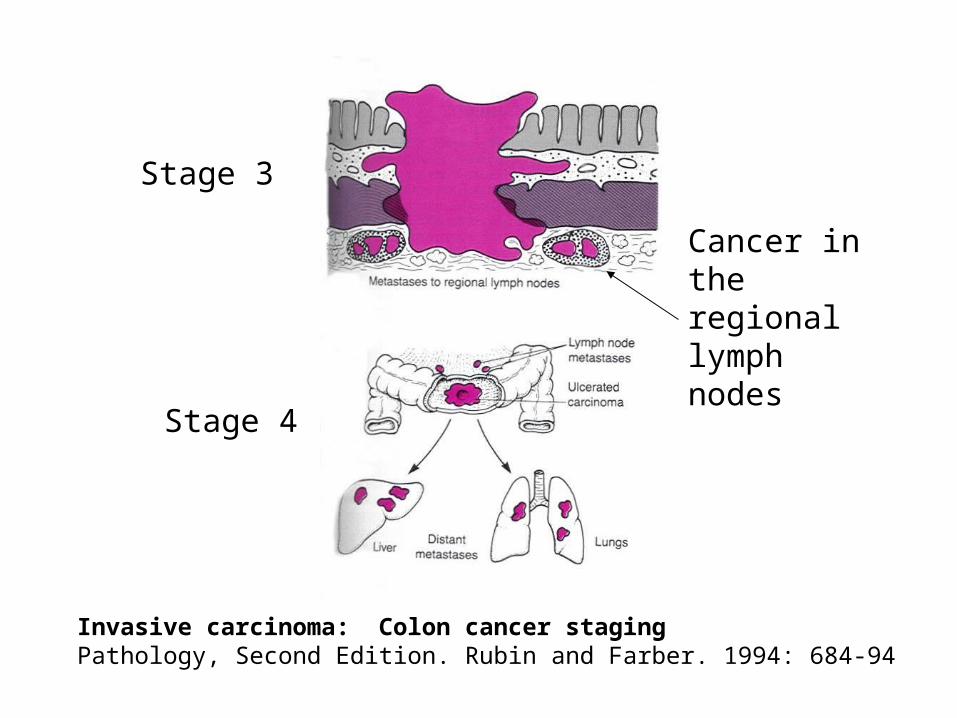
Invasive carcinoma: Colon cancer stagingPathology, Second Edition. Rubin and Farber. 1994: 684-94
Stage 1
Stage 2
Invasive carcinoma: Colon cancer stagingPathology, Second Edition. Rubin and Farber. 1994: 684-94
Stage 3
Stage 4
Cancer in the regional lymph nodes
Colonoscopy Findings:Adequacy of the Exam
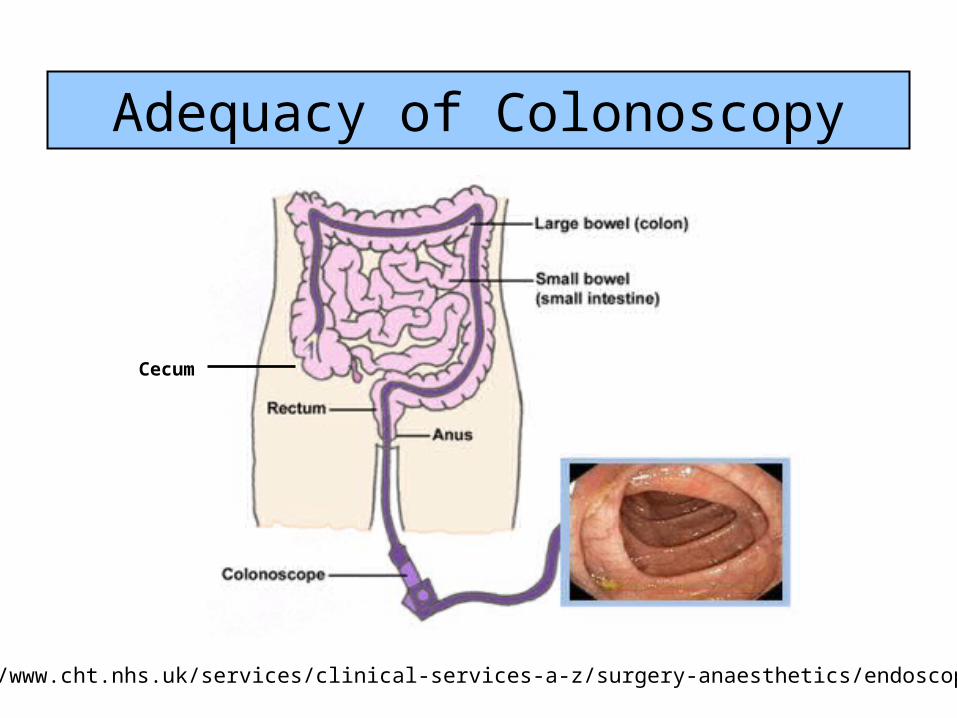
Adequacy of Colonoscopy
http://www.cht.nhs.uk/services/clinical-services-a-z/surgery-anaesthetics/endoscopy/
Cecum
Adequate Colonoscopy?
• Reached the cecum?– Reached and explored?– Reached and intubated the terminal ileum?– Peeked into the cecum but couldn’t get in
• Adequate bowel prep?– “Adequate to visualize any lesion >5mm”– “Adequate enough”– “Adequate”– “Fair”– “Excellent”
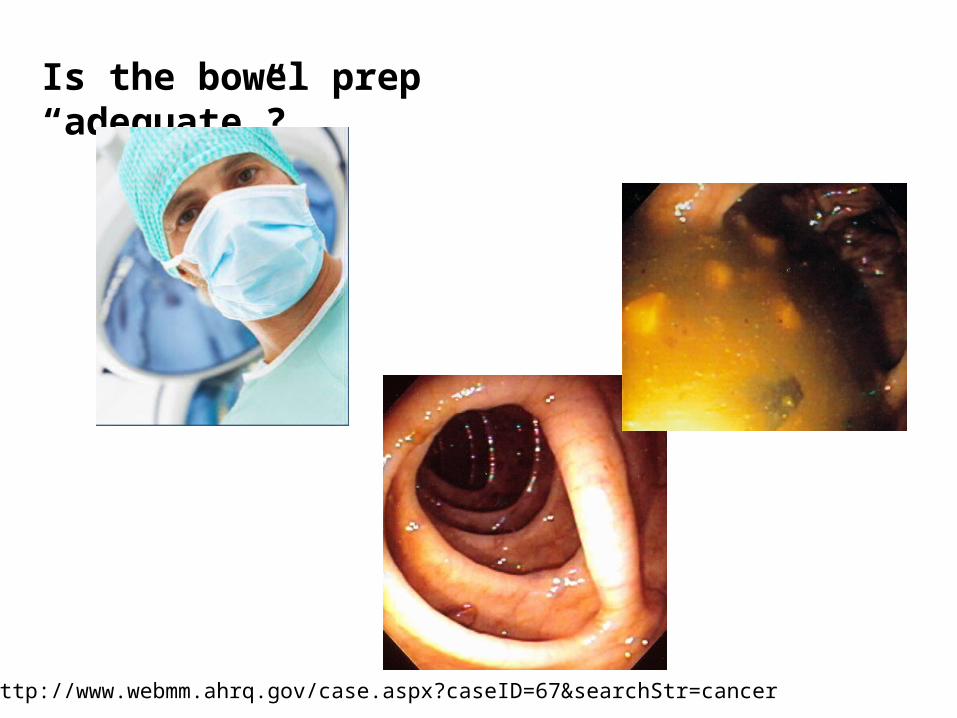
Is the bowel prep “adequate”?
http://www.webmm.ahrq.gov/case.aspx?caseID=67&searchStr=cancer
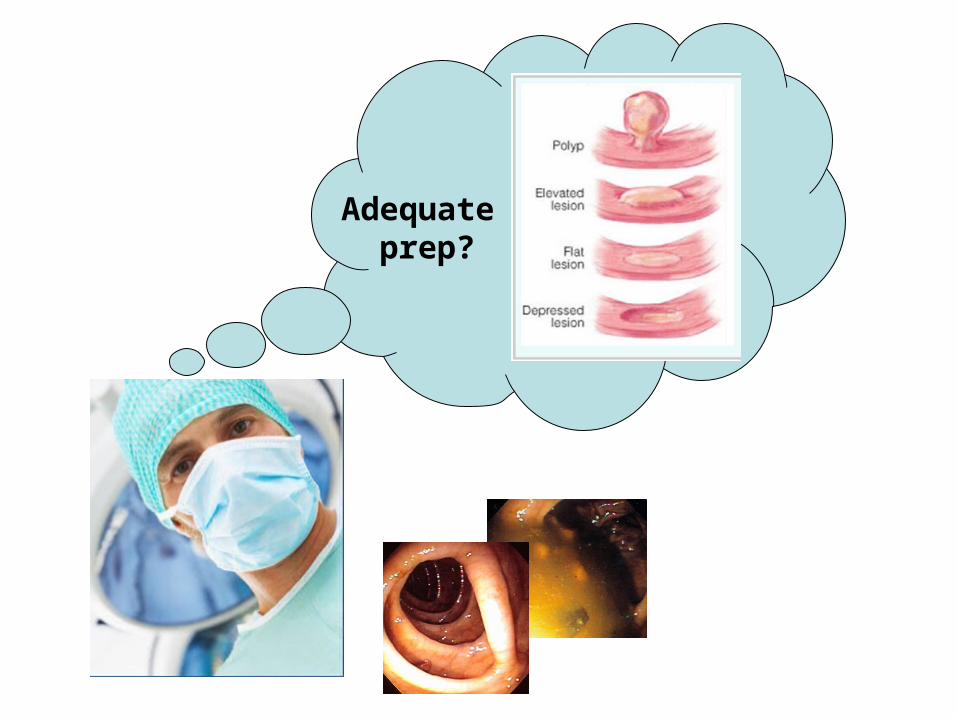
Adequate prep?
How can I dictate a picture of what I’m seeing here?
What to think about if prep was inadequate:
• Can you figure out why this patient might have had inadequate prep?
• Is there anything that could have been done differently?– By the provider– By your program– By the patient
• Are there lessons learned for future clients and for this client’s next colonoscopy?– Different instructions, different prep– Discussion with the provider(s)– Other
Case Management
Roles before Colonoscopy
• Administrative Case Manager (nurse or other case manager in program)– Obtain information for enrollment– Schedule appointment and colonoscopy– Instruct about bowel prep and procedures– Solve any barriers (transportation, accompaniment home)
• Medical Case Manager – Do an exam and clear the patient for colonoscopy– Give instructions about medication changes if needed– Instruct on bowel prep and procedures– Schedule specifics about the colonoscopy
Roles after Colonoscopy
• Medical Case Manager (doctor who did the endoscopy)– Give you a report of the colonoscopy– Give you the recall interval– Give the client the results
• Administrative Case Manager – Obtain colonoscopy and pathology reports– Review recall recommendation—is it correct per program
standards?– Enter data in computer– Notify client of their results (verbal; written)– Ask about complications– Inform the primary care provider
Recommended screening afterafter initial screening--
rescreening or surveillance colonoscopy
“Recall Interval”
Keys to the right recall
1. Colonoscopy Report
2. Pathology Report
3. Recommendation based on guidelines
4. Communication
After first colonoscopy, then whatthen what?
• Recall interval between colonoscopies will depend on:
– findings,
– risk history, and
– symptoms
Interval between colonoscopies
IF IF Findings on colonoscopy were negative:– No CRC;
– No adenomas; and
– No or only a few hyperplastic polyps,
Average risk, and
No CRC symptoms
• Recall interval will usually be 10 years • See guidelines for recommended interval
See Program Manual 1A, Attachment 1
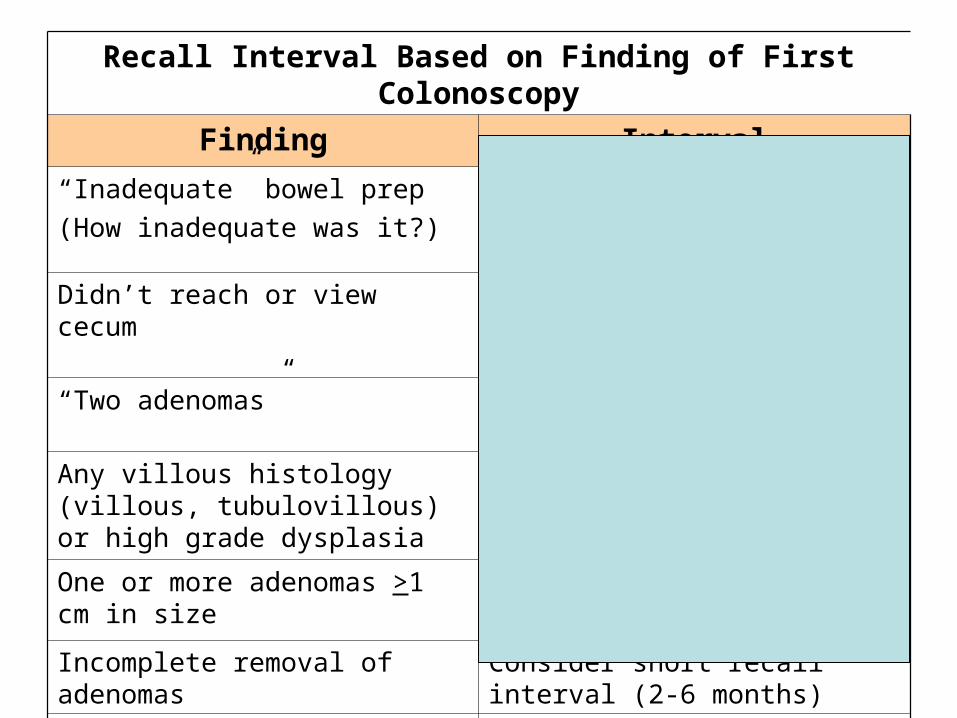
Recall Interval Based on Finding of First Colonoscopy
Finding Interval
“Inadequate” bowel prep
(How inadequate was it?)
Repeat right away or do other screening (e.g., DCBE)
Didn’t reach or view cecum Repeat right away or do other screening to check cecum
“Two adenomas” Need to know histology and size
Any villous histology (villous, tubulovillous) or high grade dysplasia
If completely removed, repeat in 3 years
One or more adenomas >1 cm in size
Repeat in 3 years
Incomplete removal of adenomas Consider short recall interval (2-6 months)
1-2 tubular adenomas, <1 cm size Repeat in 5-10 years
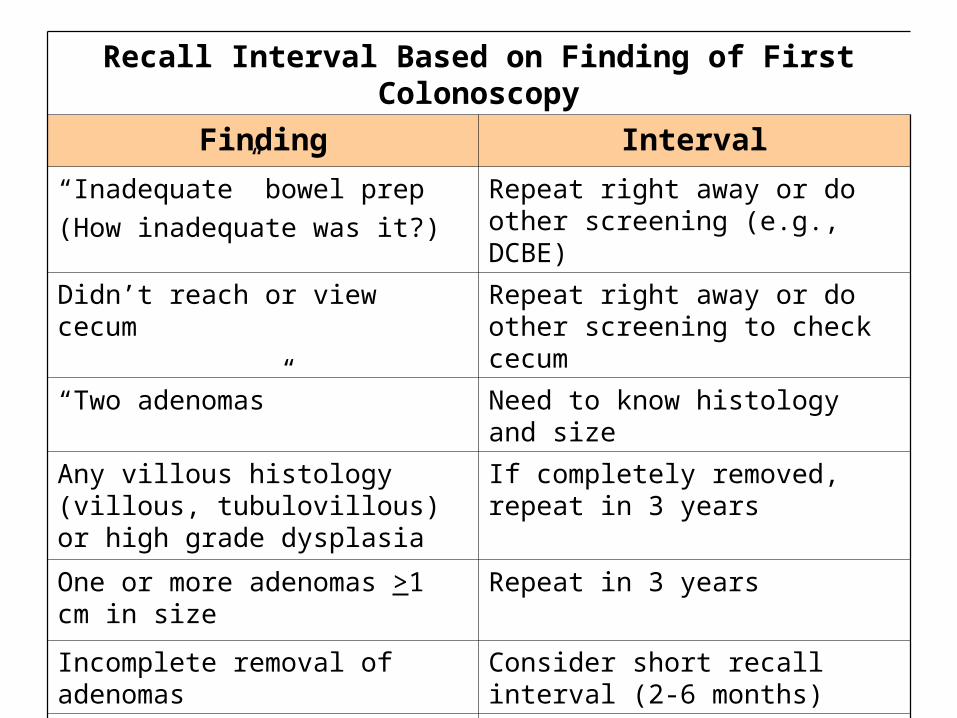
Recall Interval Based on Finding of First Colonoscopy
Finding Interval
“Inadequate” bowel prep
(How inadequate was it?)
Repeat right away or do other screening (e.g., DCBE)
Didn’t reach or view cecum Repeat right away or do other screening to check cecum
“Two adenomas” Need to know histology and size
Any villous histology (villous, tubulovillous) or high grade dysplasia
If completely removed, repeat in 3 years
One or more adenomas >1 cm in size
Repeat in 3 years
Incomplete removal of adenomas Consider short recall interval (2-6 months)
1-2 tubular adenomas, <1 cm size Repeat in 5-10 years
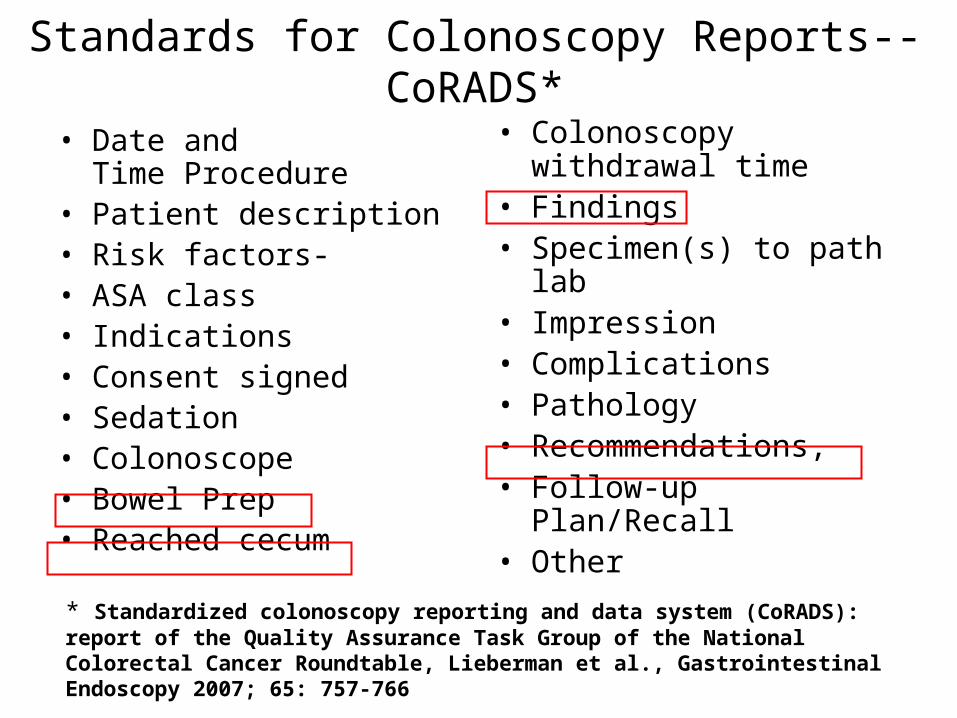
Standards for Colonoscopy Reports--CoRADS*
• Date and Time Procedure
• Patient description • Risk factors-• ASA class • Indications• Consent signed • Sedation • Colonoscope • Bowel Prep • Reached cecum
• Colonoscopy withdrawal time
• Findings• Specimen(s) to path lab • Impression • Complications • Pathology • Recommendations, • Follow-up Plan/Recall • Other
* Standardized colonoscopy reporting and data system (CoRADS): report of the Quality Assurance Task Group of the National Colorectal Cancer Roundtable, Lieberman et al., Gastrointestinal Endoscopy 2007; 65: 757-766
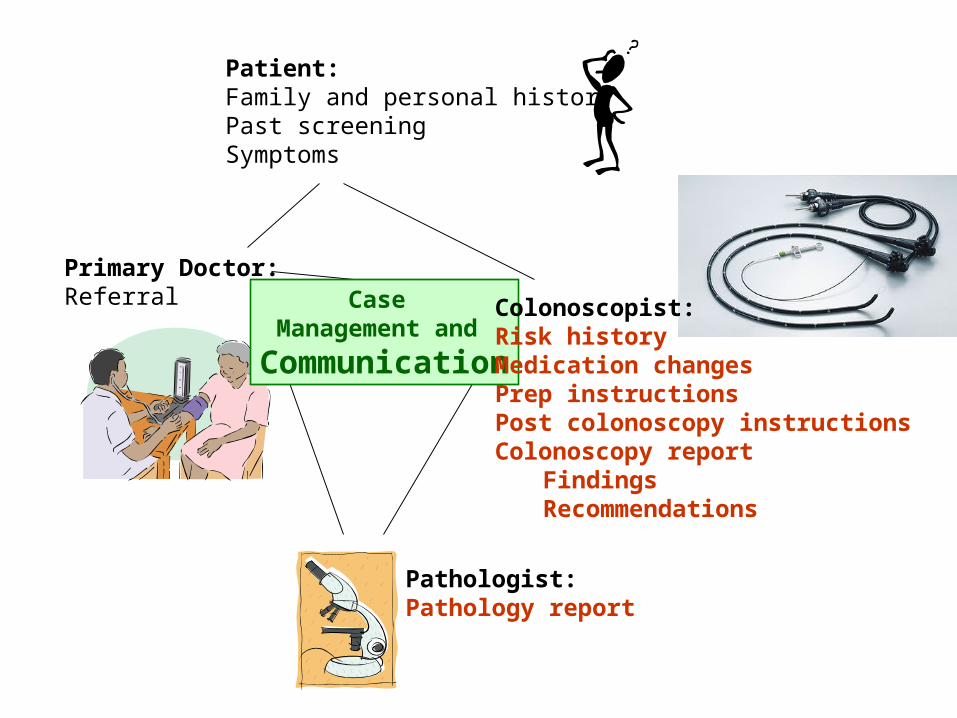
Patient:Family and personal historyPast screeningSymptoms
Primary Doctor:Referral
Pathologist:Pathology report
Case Management and
Communication
Colonoscopist:Risk historyMedication changesPrep instructionsPost colonoscopy instructionsColonoscopy report
FindingsRecommendations
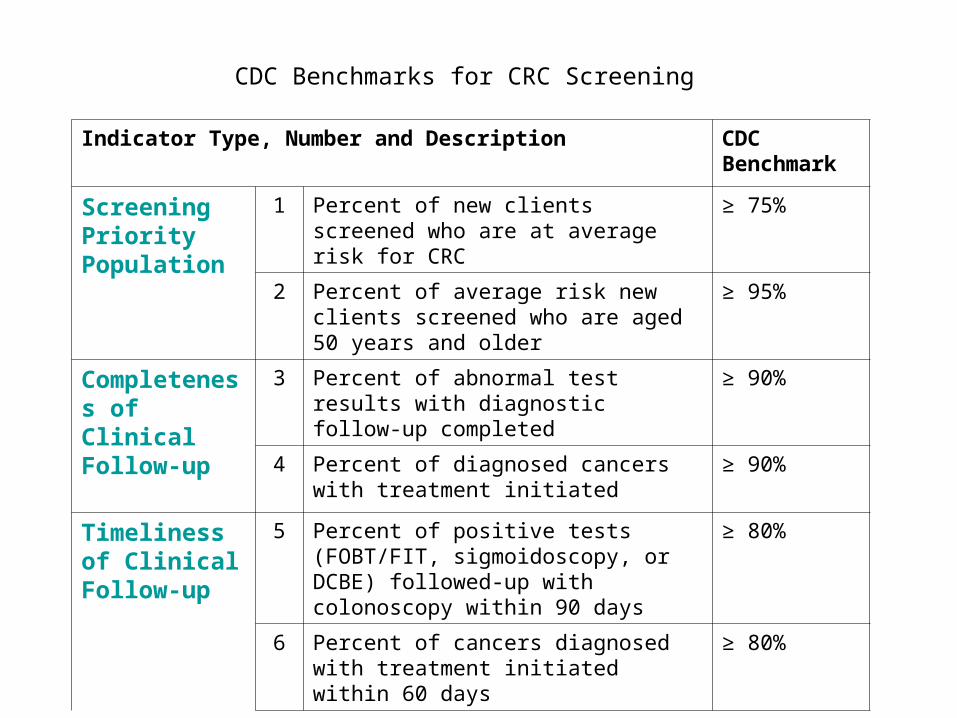
Indicator Type, Number and Description CDC Benchmark
Screening Priority Population
1 Percent of new clients screened who are at average risk for CRC
≥ 75%
2 Percent of average risk new clients screened who are aged 50 years and older
≥ 95%
Completeness of Clinical Follow-up
3 Percent of abnormal test results with diagnostic follow-up completed
≥ 90%
4 Percent of diagnosed cancers with treatment initiated
≥ 90%
Timeliness of Clinical Follow-up
5 Percent of positive tests (FOBT/FIT, sigmoidoscopy, or DCBE) followed-up with colonoscopy within 90 days
≥ 80%
6 Percent of cancers diagnosed with treatment initiated within 60 days
≥ 80%
CDC Benchmarks for CRC Screening





























