Embed Size (px)
Citation preview
Definitions
• “Inflammatory bowel disease (IBD) is an idiopathic and chronic intestinal inflammation.” Harrison’s Textbook of Internal Medicine
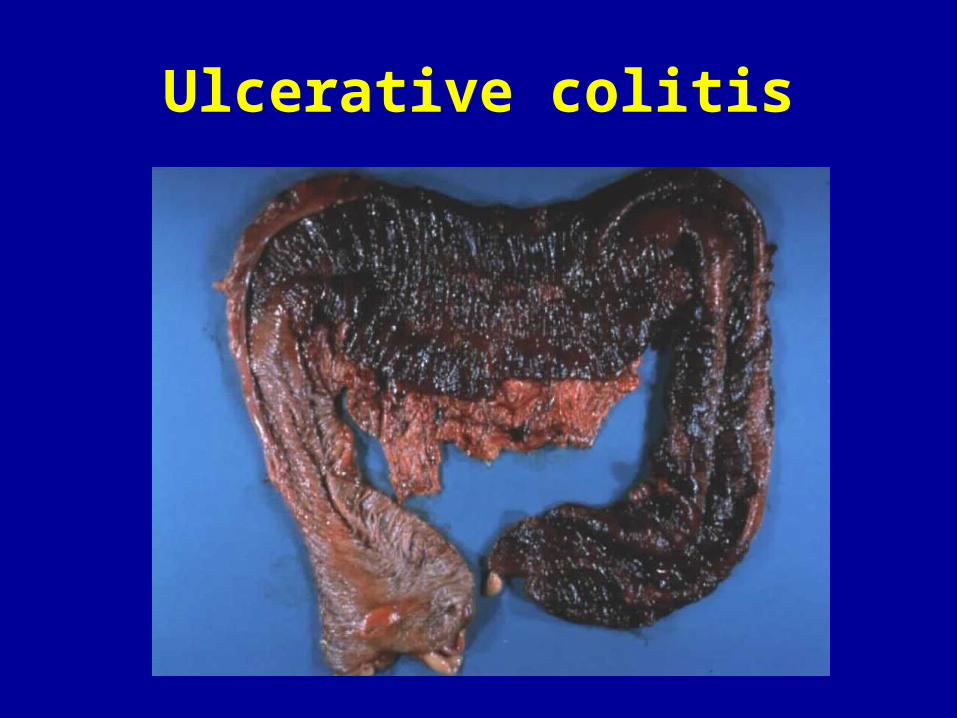
• Ulcerative Colitis (UC) is a mucosal disease that usually involves the rectum and extends proximally to involve part of or the entire colon.
• Crohn’s Disease (CD) is a disease that can effect any portion of the luminal GI tract and usually presents in two patters: obstructive/fibrostenotic and penetrating/fistulizing
IBD - Epidemiology
• Men = Women ; Jews > non-Jews
• Peak incidence is 15 - 25 years old
• Incidence is 5-15/100,000 but prevalence is much higher (133-181/100,000) and rising (Crohn’s/UC)
• 17% of UC and 23% of Crohn’s patients have a relative with IBD (usually same type of IBD)
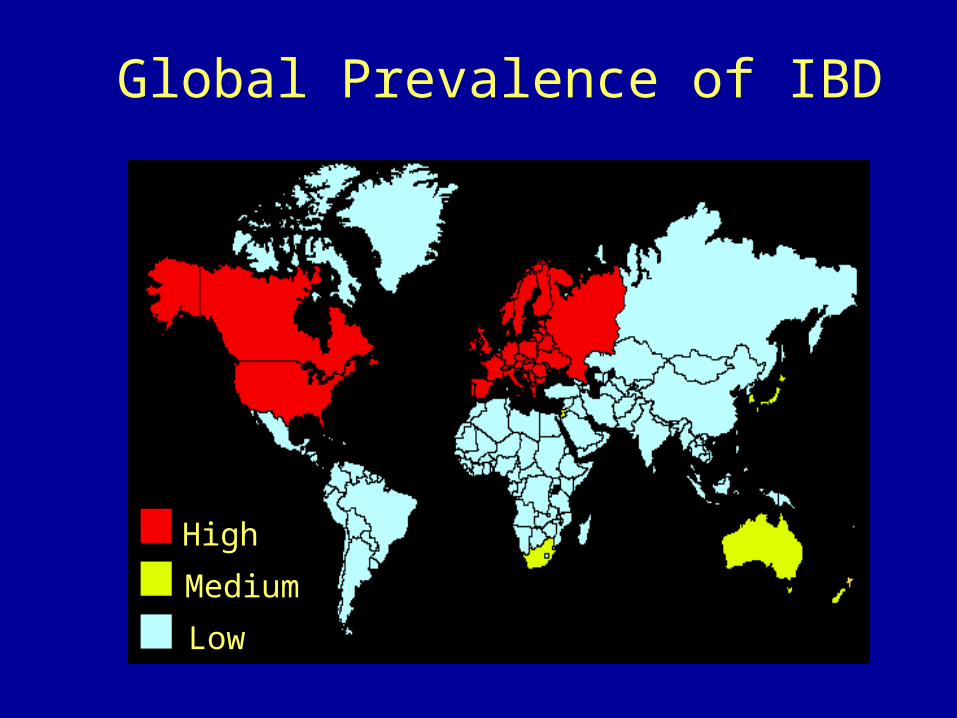
High
Medium
Low
Global Prevalence of IBD
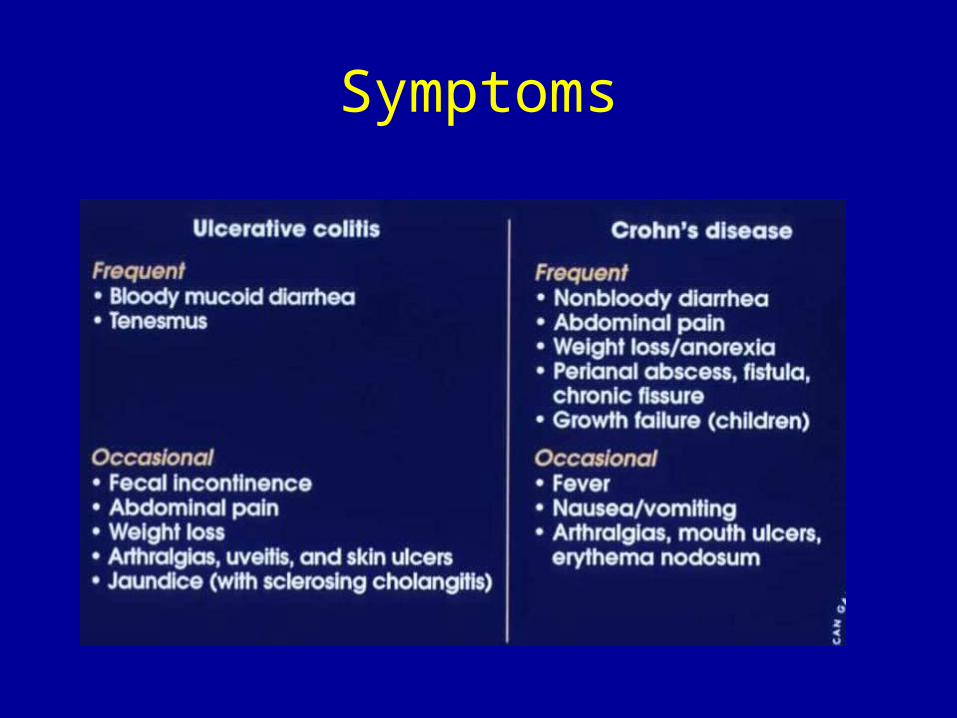
Symptoms
Infectious Mimics of IBD• Bacteria:
– Shigella – EHEC, EIEC – Campylobacter jejuni, – Salmonella– Yersinia enterocolitica– MTB – C. difficile, – Vibrio parahaemolyticus, – Chlamydia
• Parasites: Entamoeba histolytica, Trichinella • Viruses: Cytomegalovirus
• Proctitis: Neisseria gonorrhoeae, HSV, Chlamydia trachomatis, Treponema pallidum, Cytomegalovirus
Ulcerative Colitis
• Inflammatory disease of the colonic mucosa affecting the rectum with confluent proximal extention.
• Chronic, relapsing disease
• 30% will undergo colectomy over 30 years
• Colon cancer: 18% over 30 years (Mayo Clinic data)
• Primary Sclerosing Cholangitis 4%
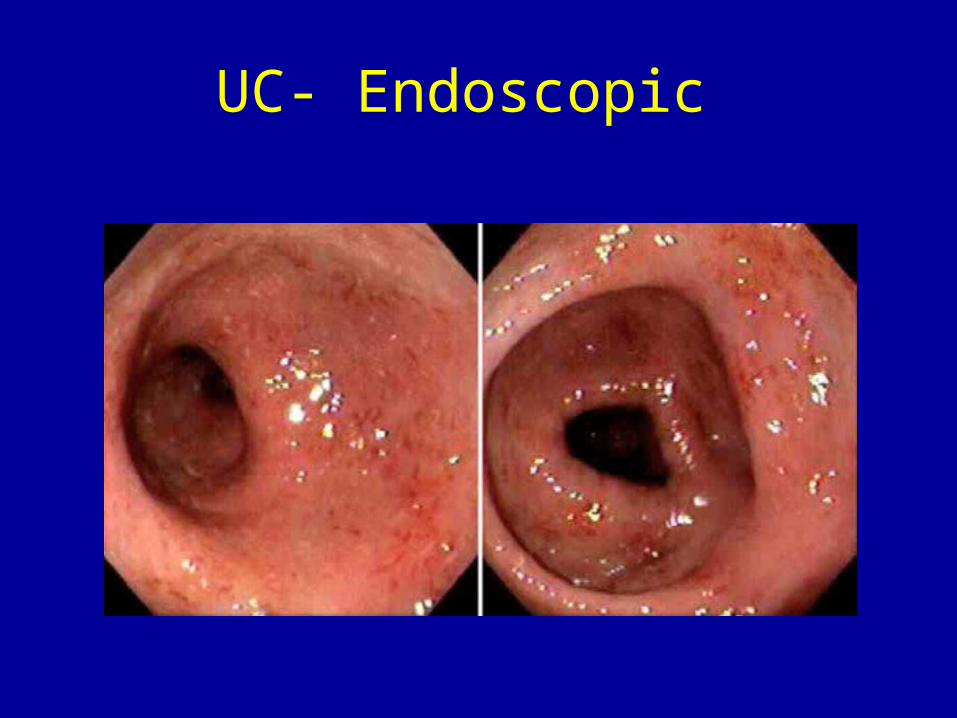
UC- Endoscopic
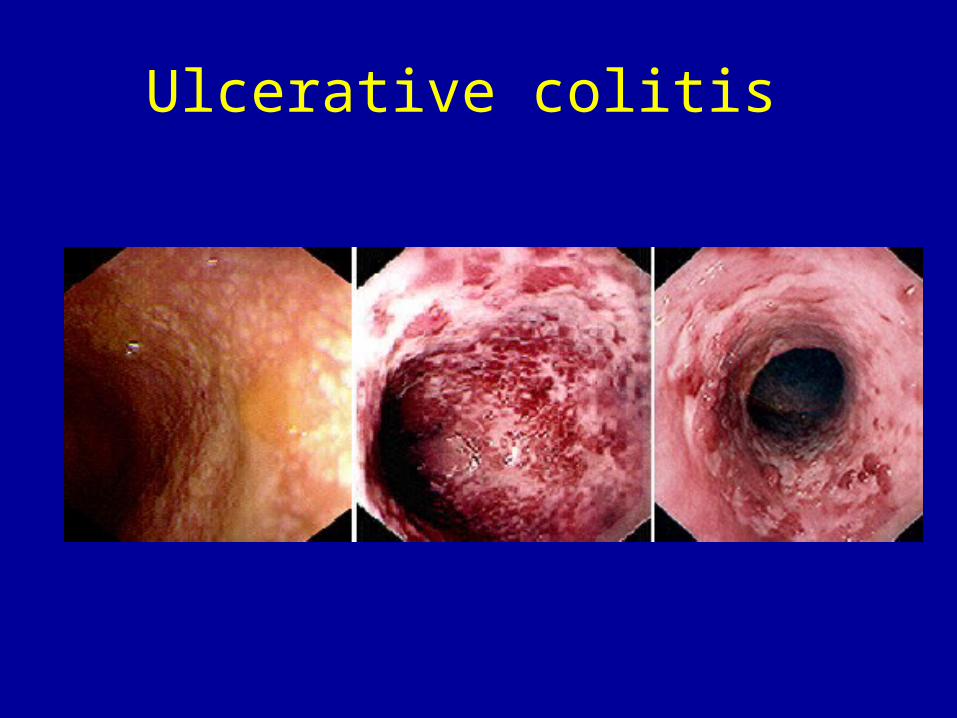
Ulcerative colitis
Ulcerative colitis
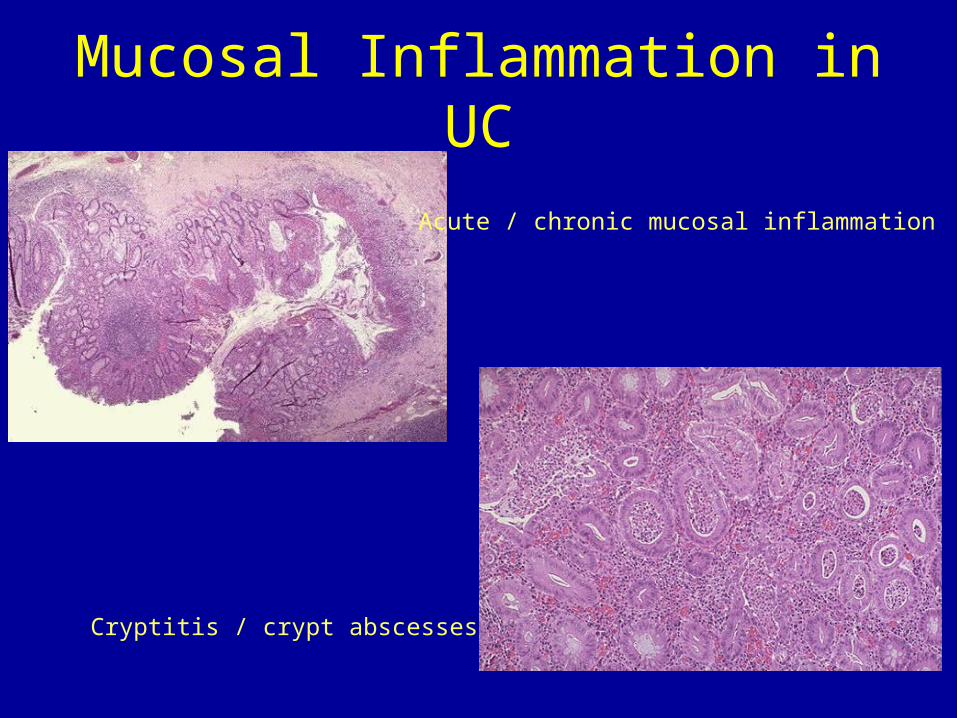
Mucosal Inflammation in UC
Acute / chronic mucosal inflammation
Cryptitis / crypt abscesses
Crohn’s Disease• A pan-enteric transmural inflammatory disease
– Mouth to sigmoid, usually spares rectum
• Usually (70%) involves the terminal ileum
• Skip lesions (patchy distribution)
• Perianal involvement
• Transmural complications – Fistulae, abscess, strictures
Crohn’s Disease
• Pain diarrhea, anemia, less often bleeding
• Subtypes: inflammatory/obstructive
penetrating/fistulous
• 80% require surgery by 15 years
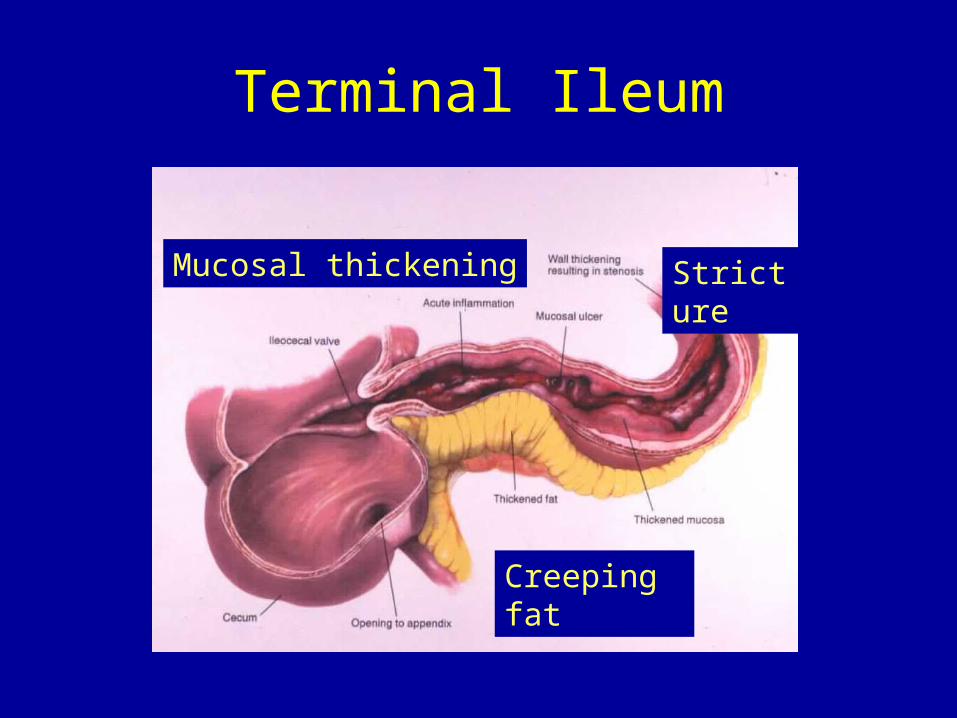
Terminal Ileum
Creeping fat
StrictureMucosal thickening
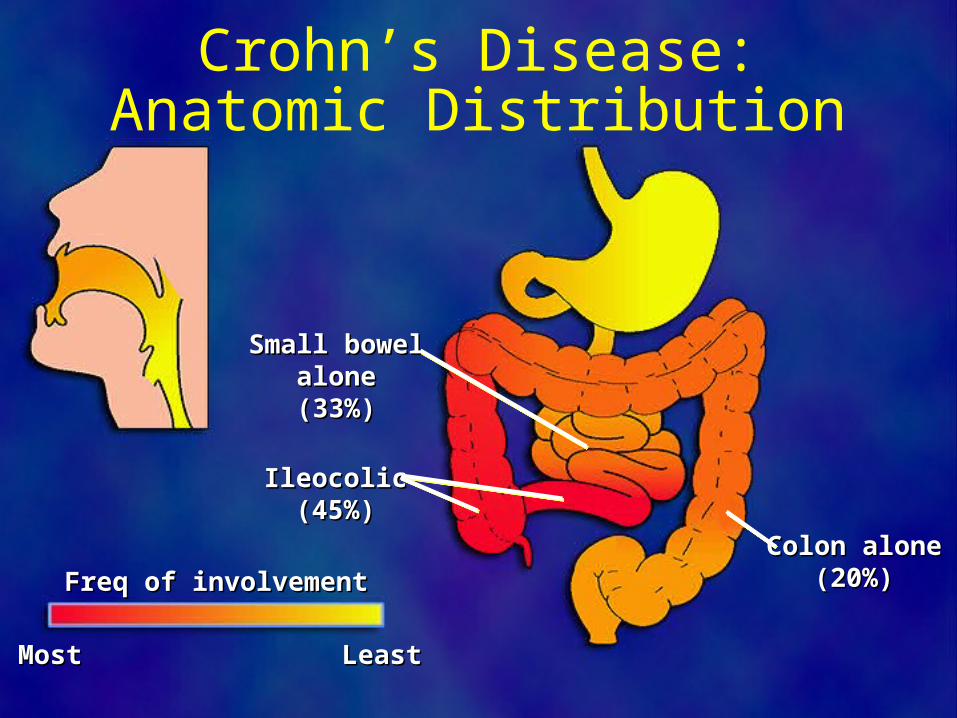
Crohn’s Disease:Anatomic Distribution
Small bowelSmall bowelalonealone(33%)(33%)
Colon aloneColon alone(20%)(20%)
IleocolicIleocolic(45%)(45%)
LeastLeastMostMost
Freq of involvementFreq of involvement

CD- endoscopic

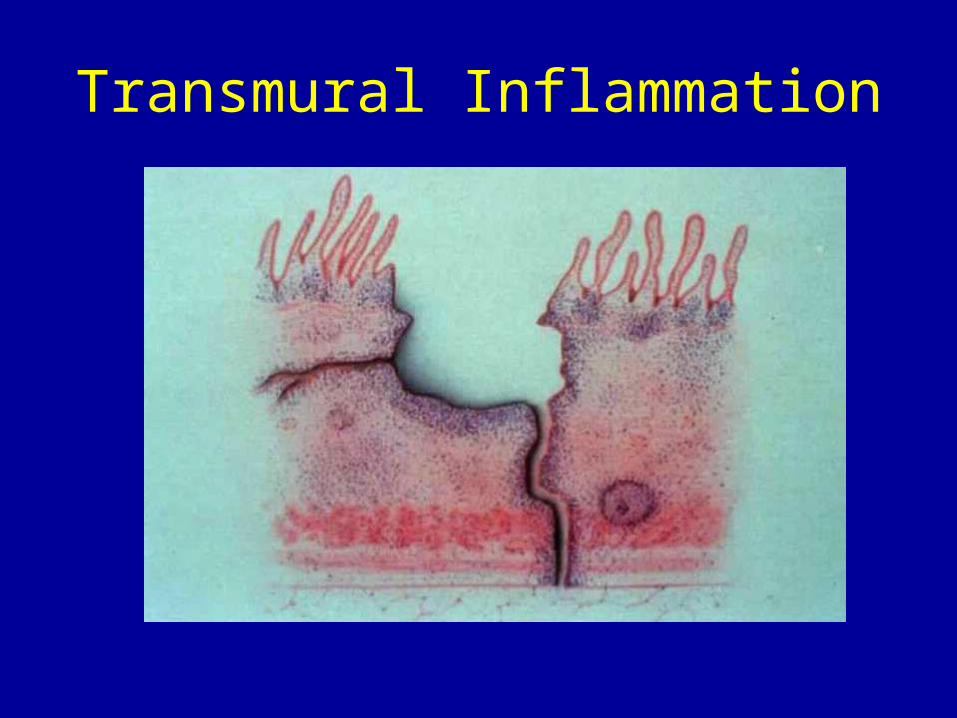
Transmural Inflammation
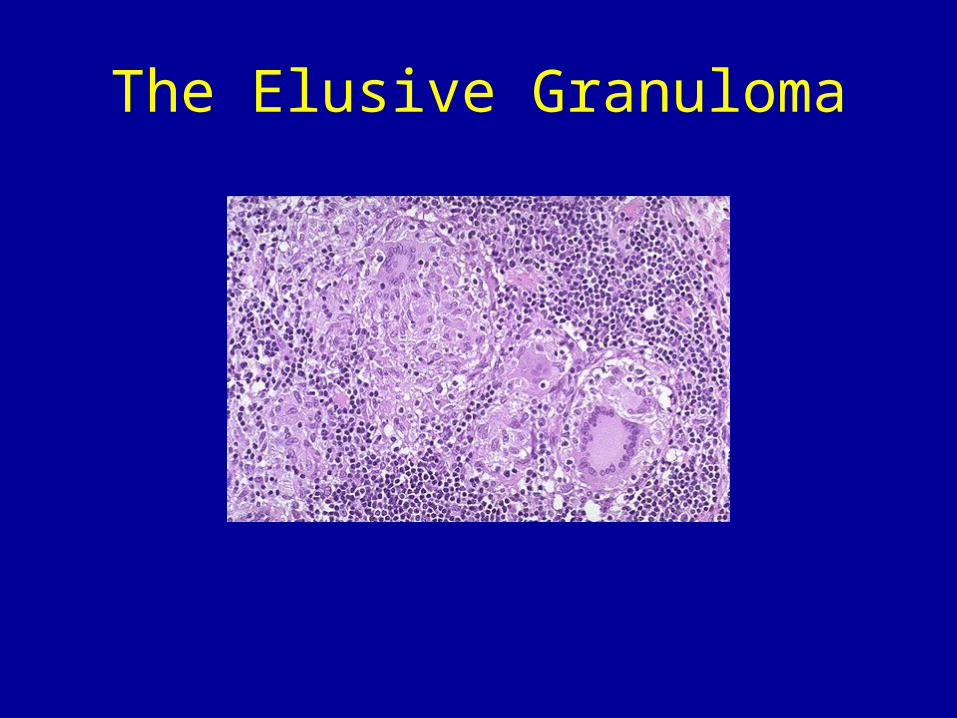
The Elusive Granuloma
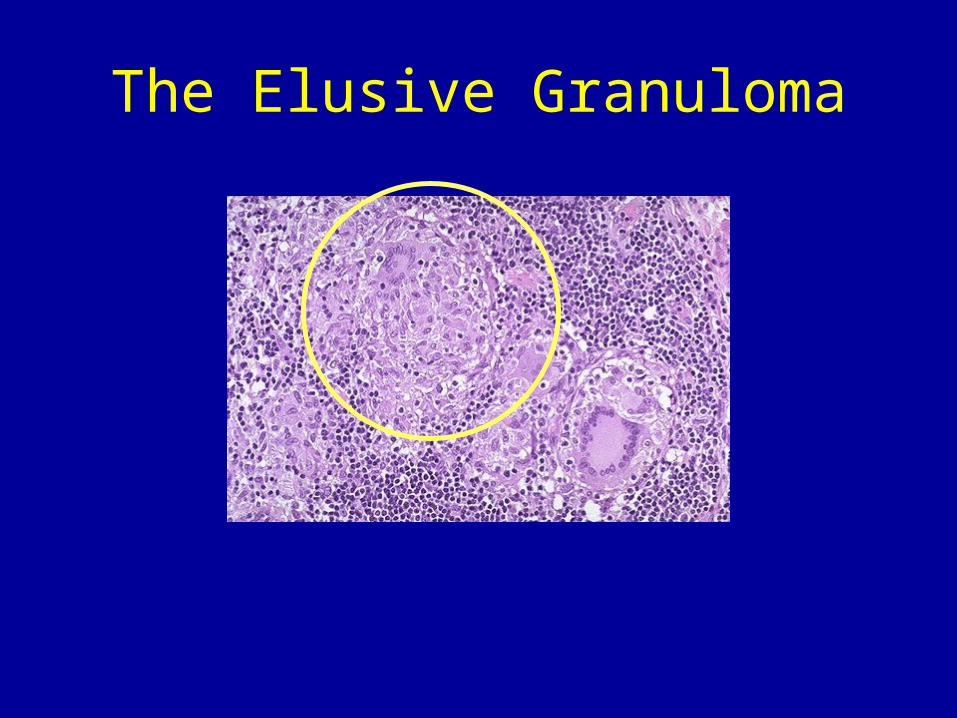
The Elusive Granuloma
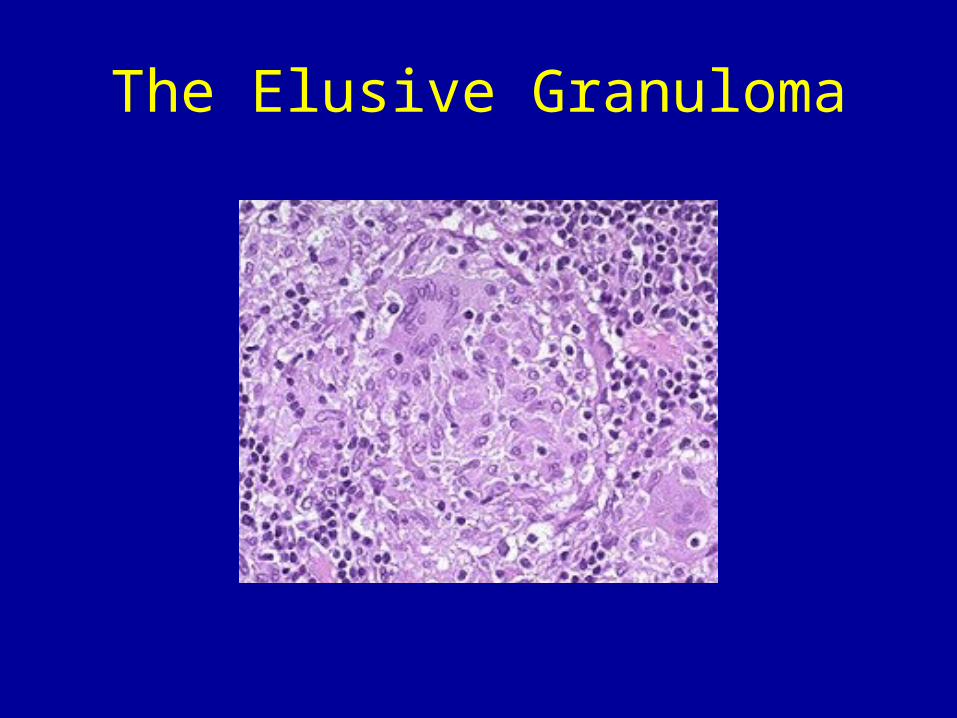
The Elusive Granuloma

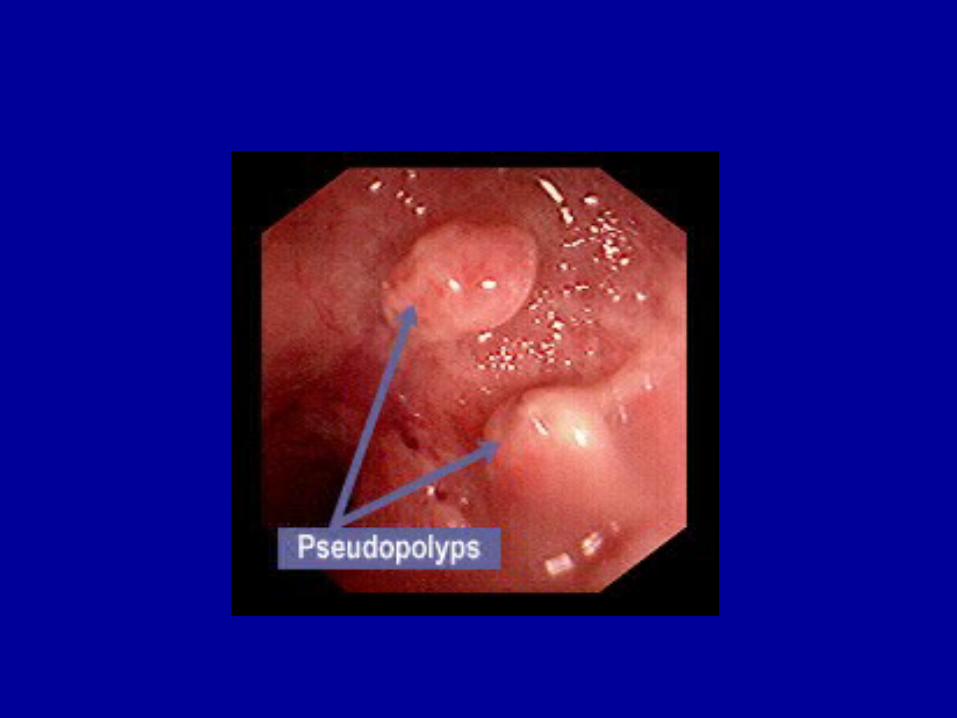
Inflammatory polyp
Crohn’s disease Linear Erosions
Ileitis
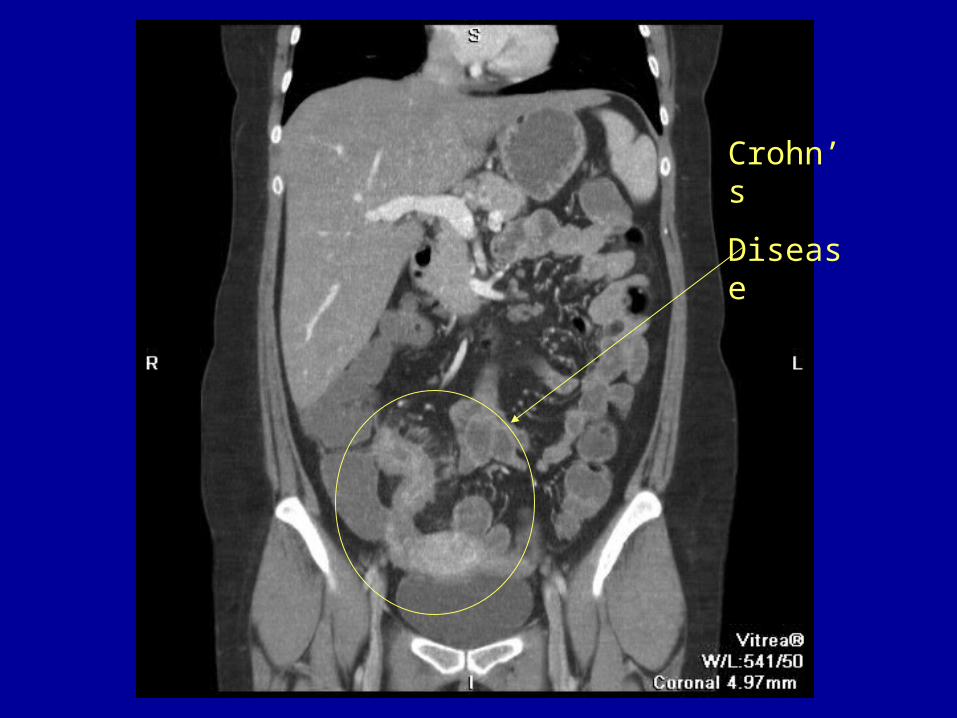
Crohn’s
Disease
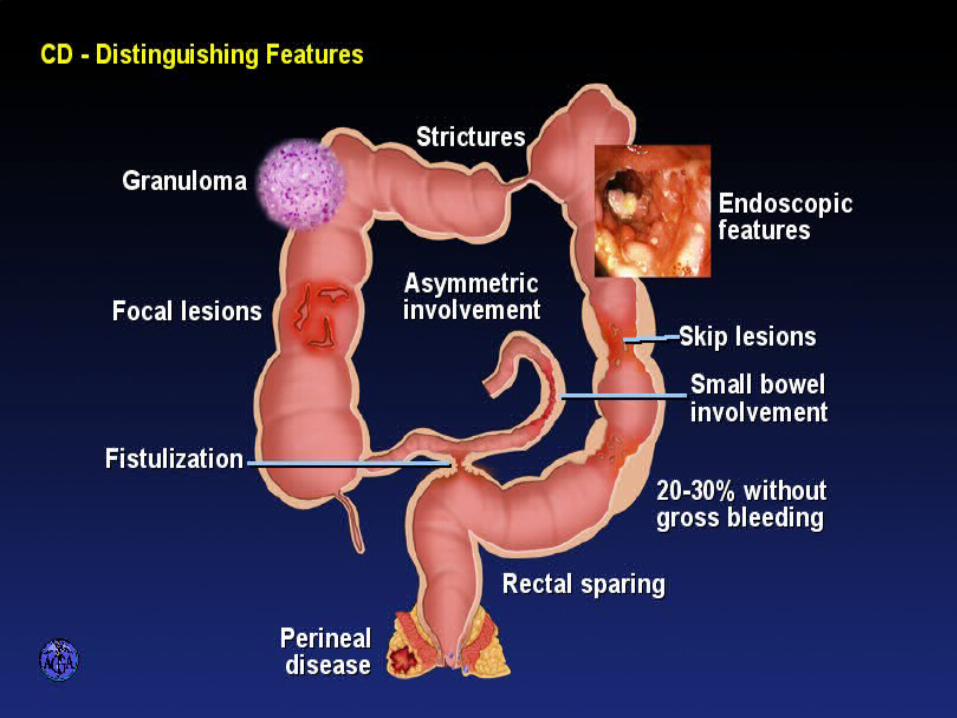
DISTINGUISHING FEATURES OF CROHN’S
DISEASE
Serologies
• May be helpful in “indeterminant colitis”
• Crohn’s– ASCA - anti-Saccharomyces cerevisiae
antibodies
• Ulcerative colitis– pANCA - perinuclear antineutrophil cytoplasmic
antibodies
IBD Extraintestinal Manifestations
• Musculoskeletal: Arthritis, ankylosing spondylitis, osteoporosis, sacroilitis
• Skin and mouth: erythema nodosum, pyoderma gangrenosum, aphthous ulcers, vitiligo, psoriasis, amyloidosis.
• Ocular: Uveitis, iritis, episcleritis.
• Hepatobiliary: Primary sclerosing cholangitis, cholangiocarcinoma, hepatitis, pericholangitis, gallstones (ileal Crohn's disease)
IBD Extraintestinal Manifestations
• Pancreatitis
• Thyroiditis
• Pulmonary: Bronchiolitis

Erythema Nodosum (EN)
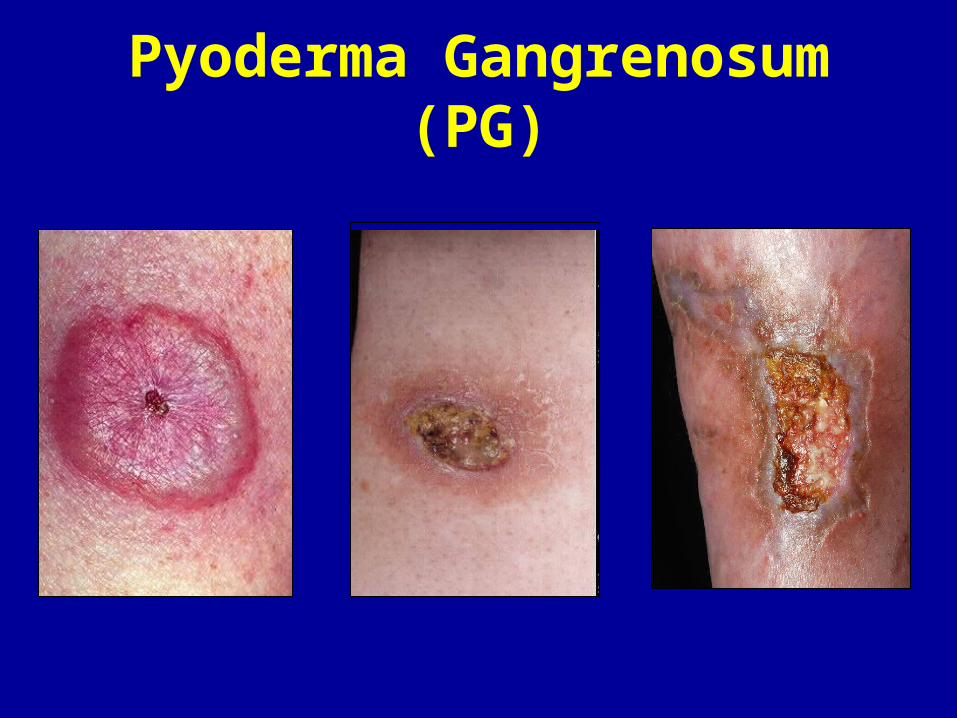
Pyoderma Gangrenosum (PG)
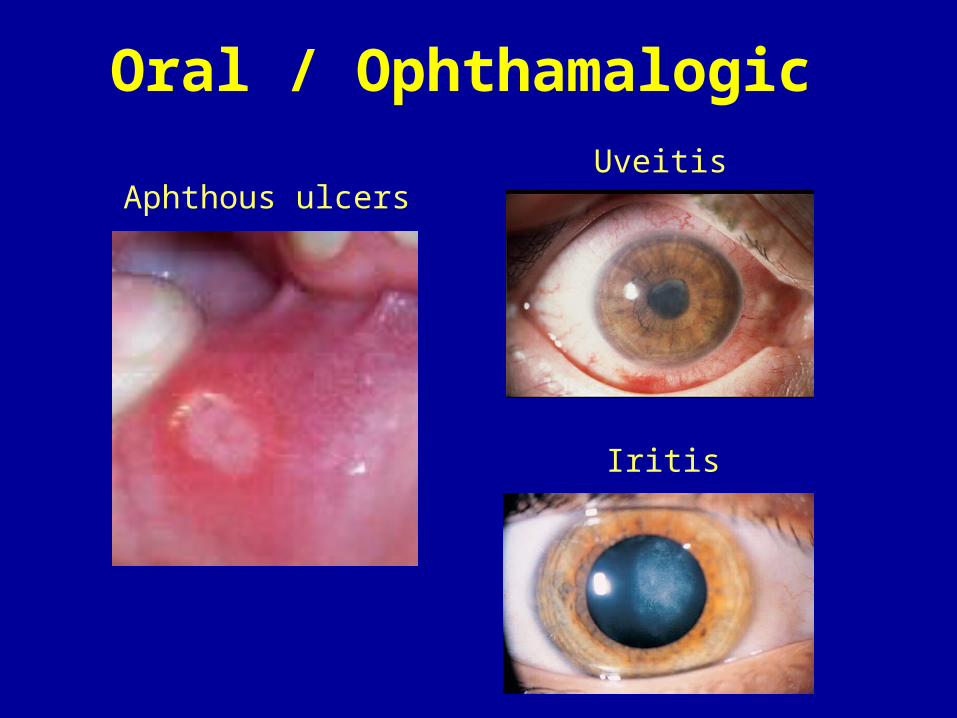
Oral / Ophthamalogic
Aphthous ulcersUveitis
Iritis
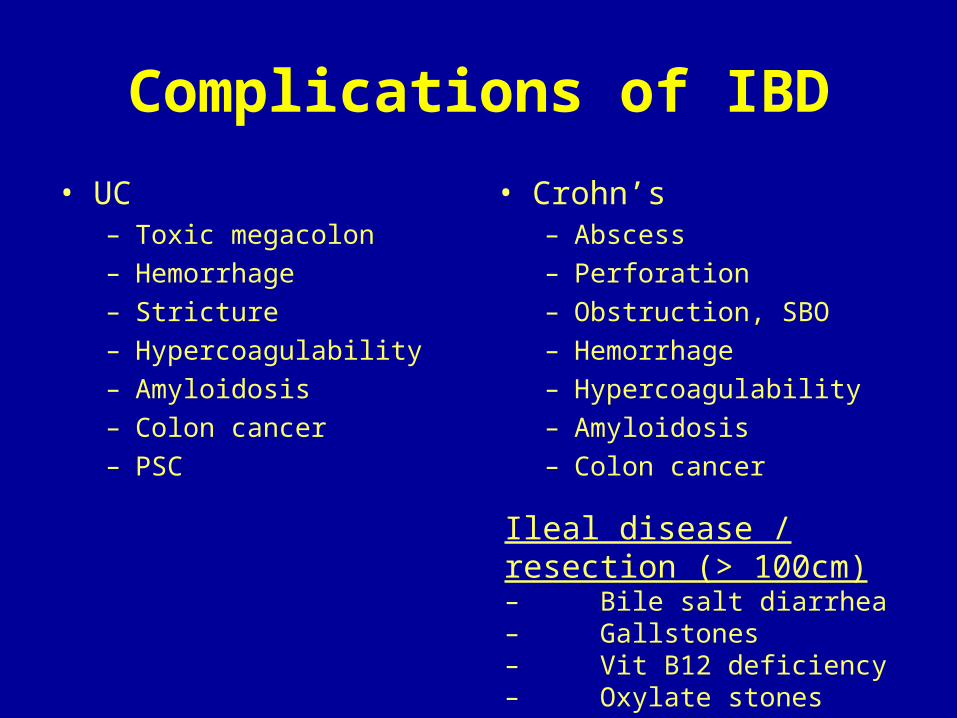
Complications of IBD
• UC– Toxic megacolon– Hemorrhage– Stricture– Hypercoagulability– Amyloidosis– Colon cancer– PSC
• Crohn’s– Abscess– Perforation– Obstruction, SBO– Hemorrhage– Hypercoagulability– Amyloidosis– Colon cancer
Ileal disease / resection (> 100cm)– Bile salt diarrhea– Gallstones– Vit B12 deficiency– Oxylate stones
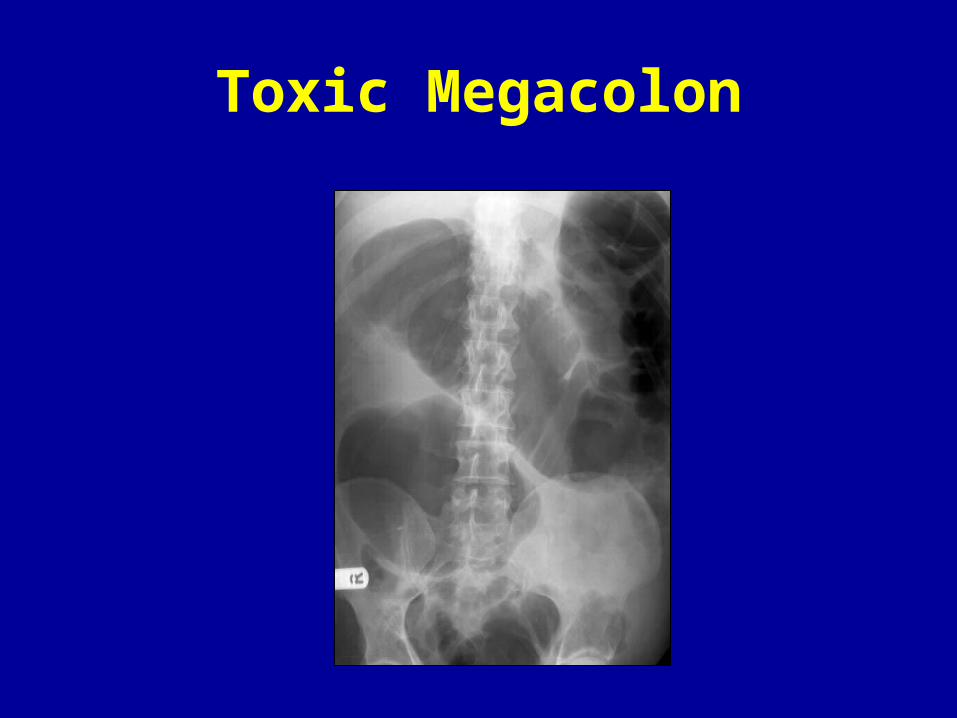
Toxic Megacolon
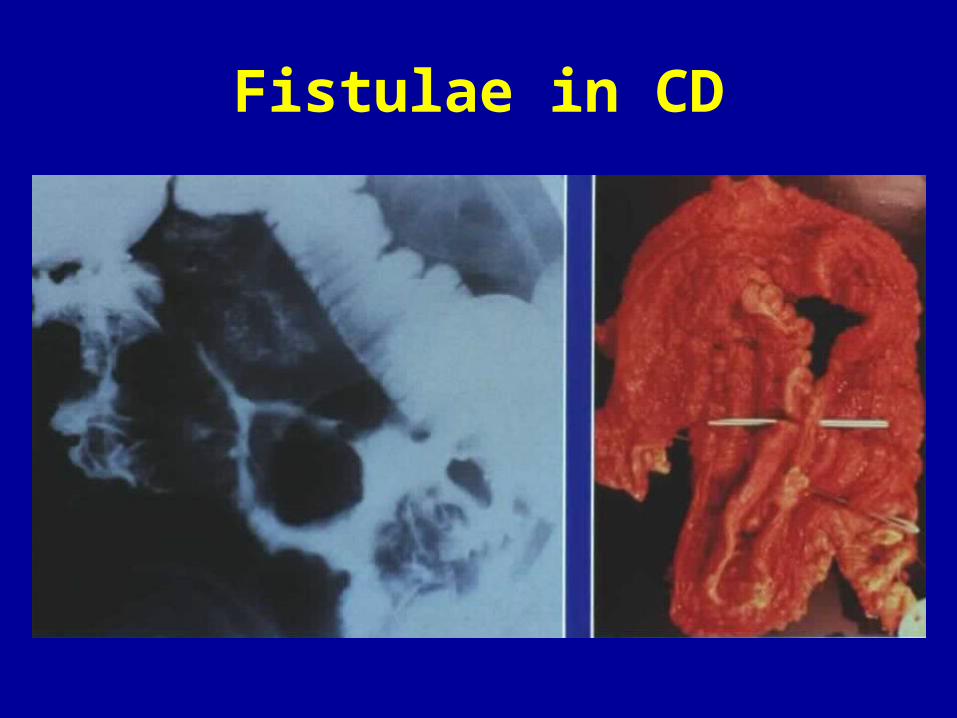
Fistulae in CD
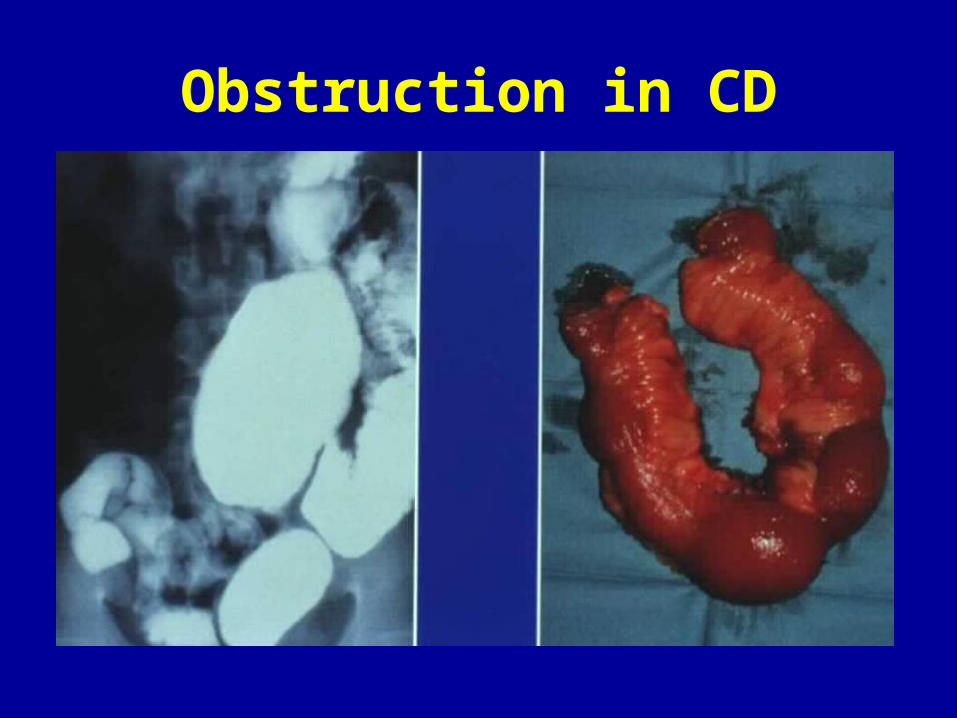
Obstruction in CD
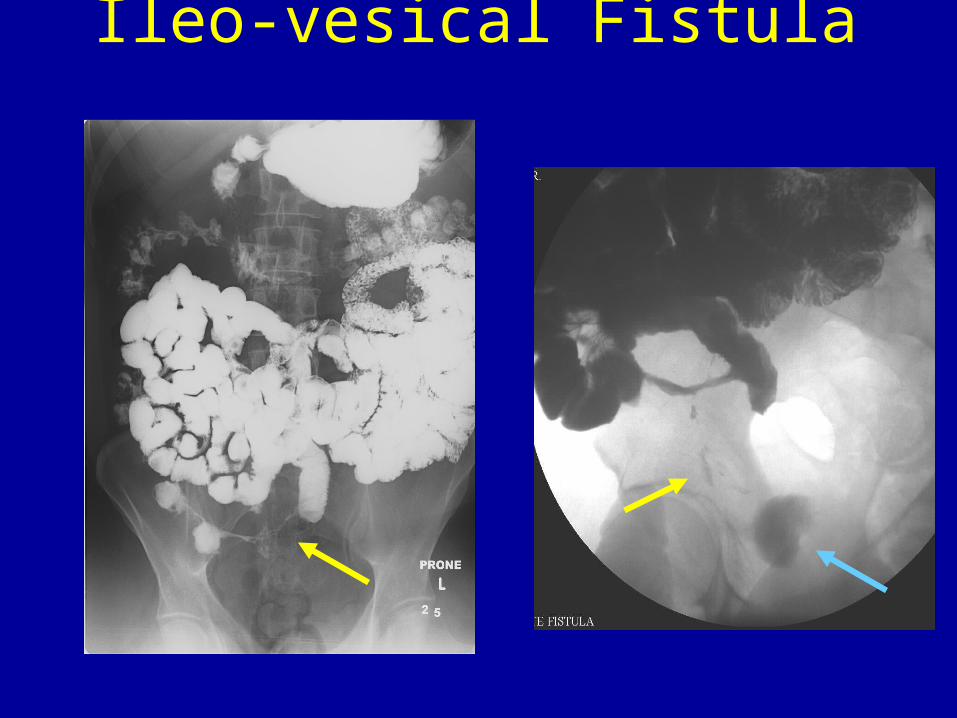
Ileo-vesical Fistula
Colorectal Cancer in IBD
• Increased risk (5%) 1-3% at 10 yrs and 18% at 30 years with pancolitis
• Flat or depressed adenomas—fields of dysplasia.
• Increased risk with:– Disease proximal to splenic flexure– > 8 years duration; young age at diagnosis– Primary sclerosing cholangitis – Family history of CRC– Pseudopolyps at colonoscopy
• 5-ASA treatment is protective
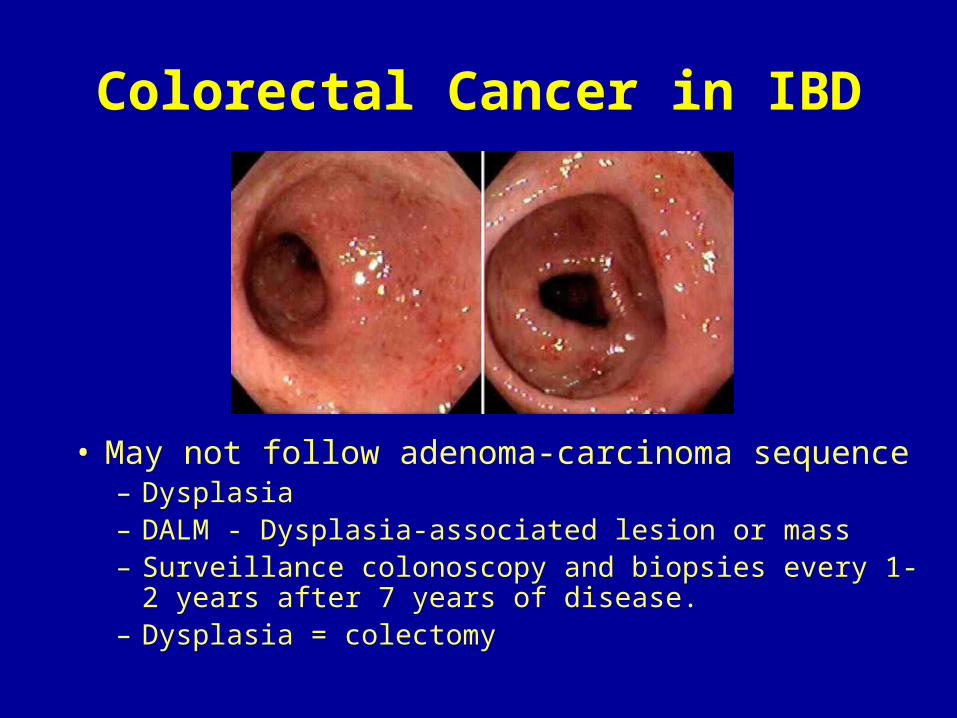
Colorectal Cancer in IBD
• May not follow adenoma-carcinoma sequence– Dysplasia– DALM - Dysplasia-associated lesion or mass– Surveillance colonoscopy and biopsies every 1-2
years after 7 years of disease.– Dysplasia = colectomy
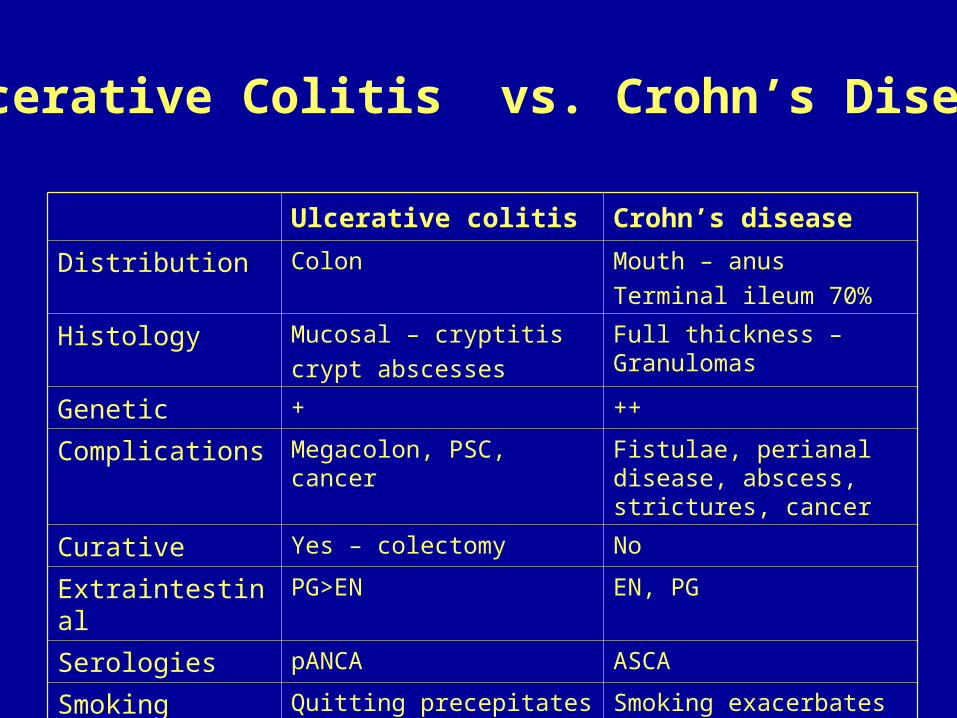
Ulcerative colitis Crohn’s disease
Distribution Colon Mouth – anus
Terminal ileum 70%
Histology Mucosal – cryptitis
crypt abscesses
Full thickness – Granulomas
Genetic + ++
Complications Megacolon, PSC, cancer Fistulae, perianal disease, abscess, strictures, cancer
Curative Yes – colectomy No
Extraintestinal PG>EN EN, PG
Serologies pANCA ASCA
Smoking Quitting precepitates Smoking exacerbates
Ulcerative Colitis vs. Crohn’s Disease
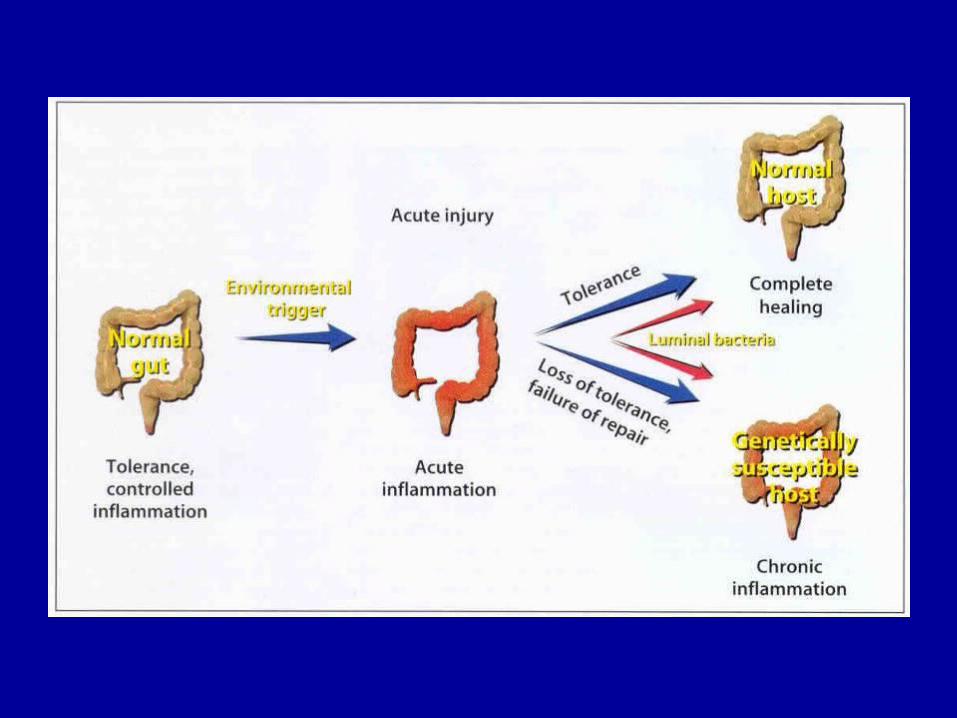
Pathogenesis in IBD• Abnormal function of the gut mucosal barrier results in
chronic intestinal inflammation
• Genetic susceptibility conferred by mutations at distinct chromosomal loci
• Dysregulation of mucosal proinflammatory immunity (Th1 responses) with resulting overactivity toward resident antigens
• Decreased regulatory T cell populations (suppressor T cells) lead to unfettered Th1 inflammatory responses to luminal antigens (loss of tolerance)
• Microbial antigens can lead to self-perpetuating inflammation in genetically susceptible hosts
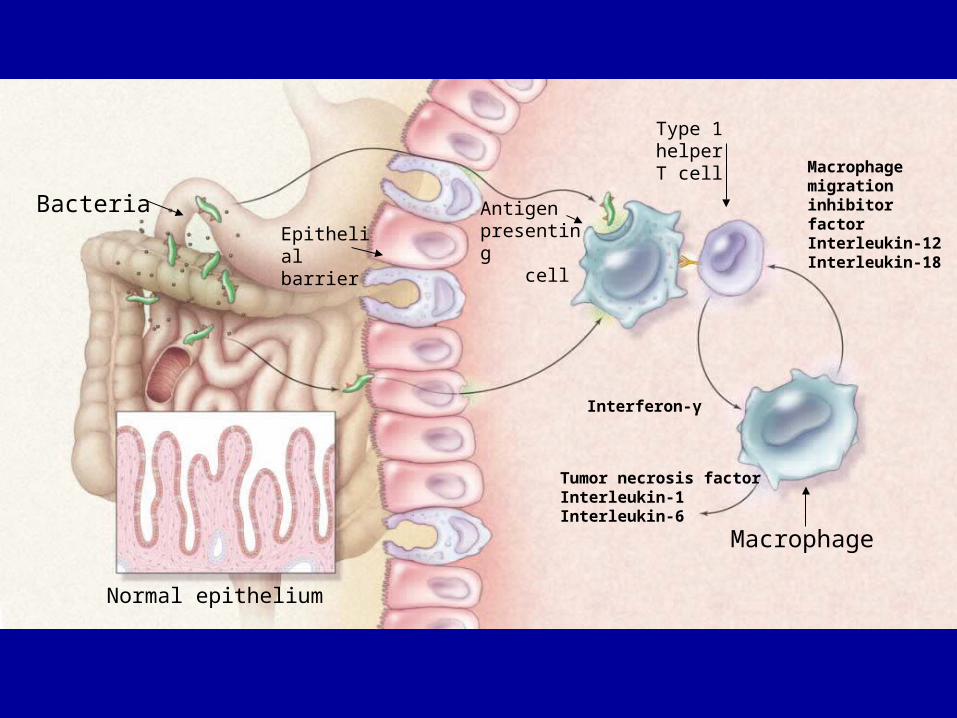
Bacteria Antigen presenting cell
Macrophage
Type 1 helperT cell
Macrophagemigration inhibitorfactorInterleukin-12Interleukin-18
Tumor necrosis factorInterleukin-1Interleukin-6
Normal epithelium
Epithelialbarrier
Interferon-γ
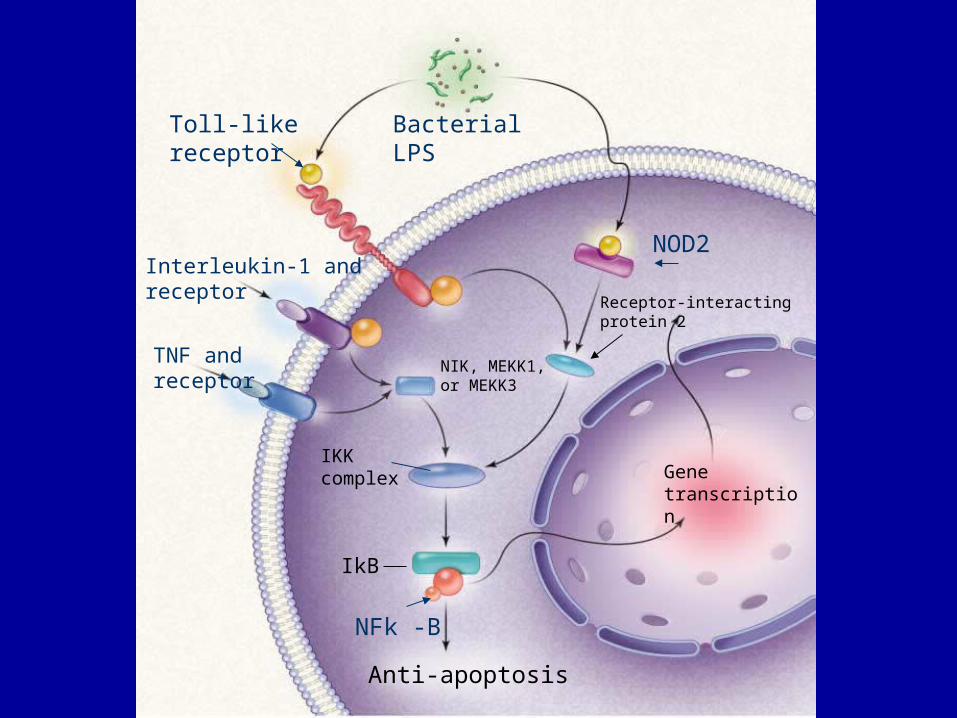
Toll-likereceptor
Bacterial LPS
NOD2
TNF and receptor
Interleukin-1 and receptor
NFk -B
Anti-apoptosis
NIK, MEKK1, or MEKK3
IKKcomplex
Receptor-interacting protein 2
Genetranscription
IkB
Environmental Influences
• Clean Kid hypothesis
• IBD more common in cold climates
• IBD more common in industrialized areas
• Crohn’s > UC are smokers; are s/p appendectomy
• Active disease increases risk to fetus and mother in pregnancy

Current Expectations for IBD Therapy
• Induce clinical remission
• Maintain clinical remission
• Improve patient quality of life
• Heal mucosa – endoscopic remission
• Decrease hospitalization/surgery and overall costs
• Minimize disease-related and therapy-related complications
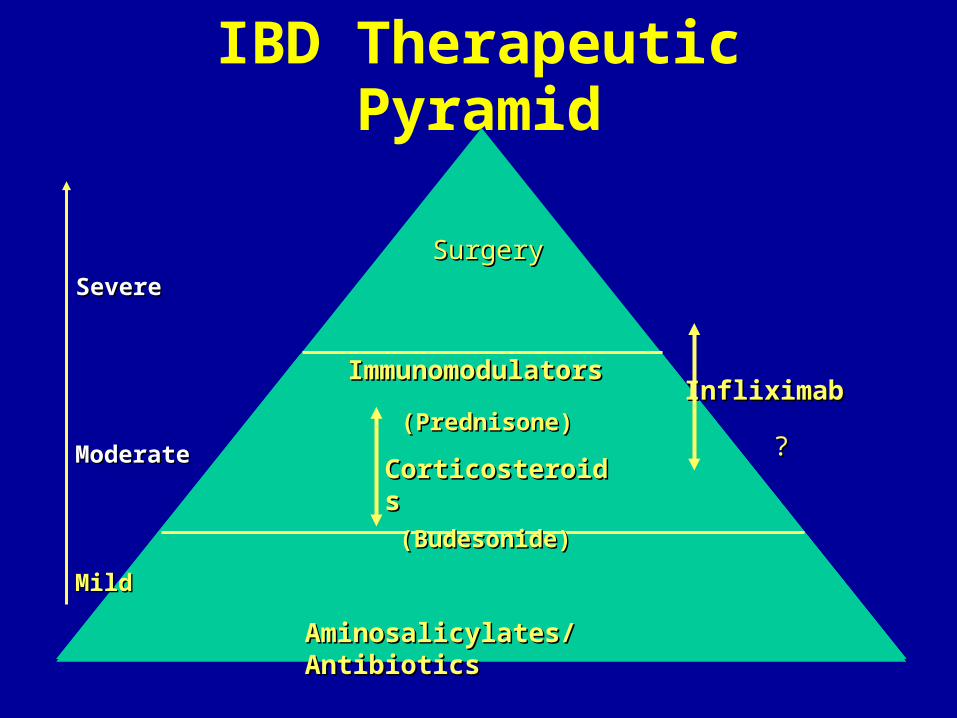
IBD Therapeutic Pyramid
SevereSevere
ModerateModerate
Aminosalicylates/AntibioticsAminosalicylates/Antibiotics
CorticosteroidsCorticosteroids
ImmunomodulatorsImmunomodulators
SurgerySurgery
InfliximabInfliximab
??(Prednisone)(Prednisone)
MildMild
(Budesonide)(Budesonide)
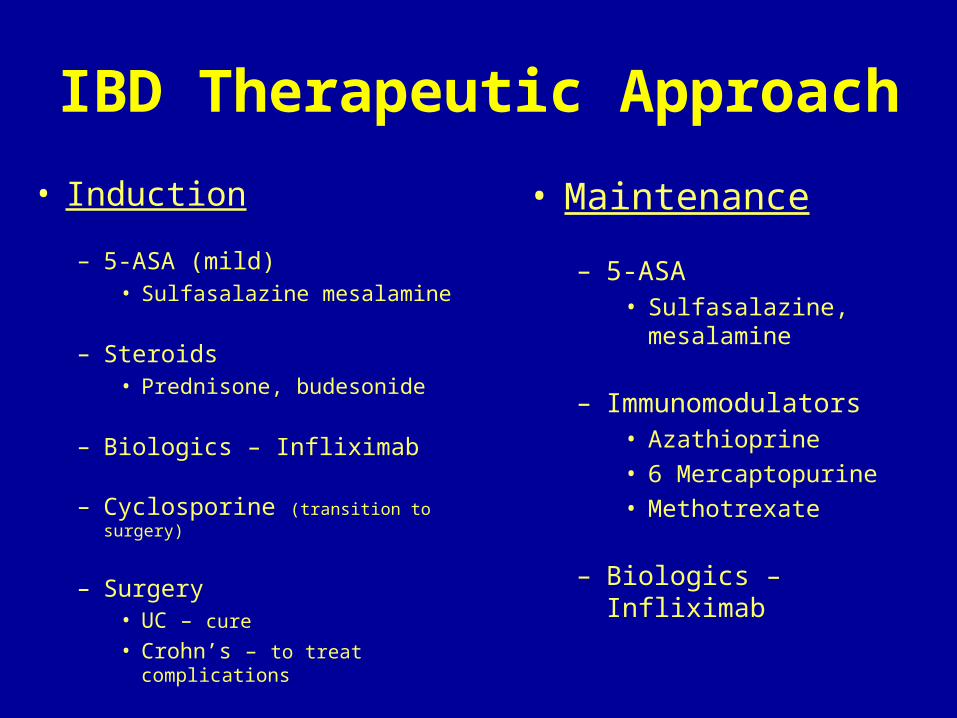
IBD Therapeutic Approach
• Induction
– 5-ASA (mild)• Sulfasalazine mesalamine
– Steroids• Prednisone, budesonide
– Biologics – Infliximab
– Cyclosporine (transition to surgery)
– Surgery• UC – cure
• Crohn’s – to treat complications
• Maintenance
– 5-ASA• Sulfasalazine,
mesalamine
– Immunomodulators• Azathioprine• 6 Mercaptopurine• Methotrexate
– Biologics – Infliximab
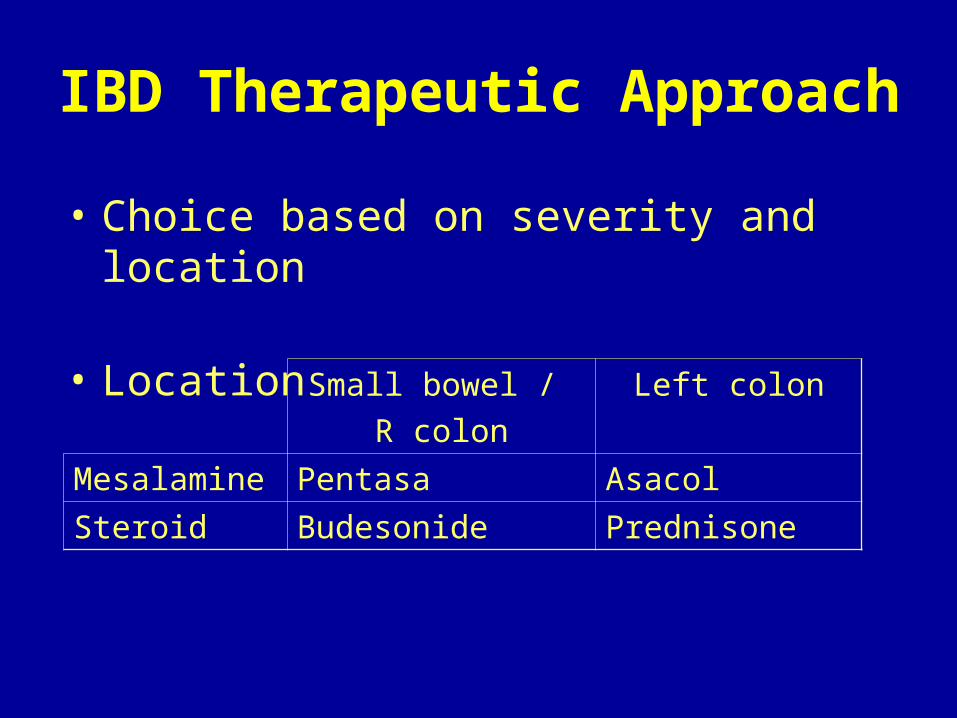
IBD Therapeutic Approach
• Choice based on severity and location
• Location Small bowel / R colon
Left colon
Mesalamine Pentasa Asacol
Steroid Budesonide Prednisone
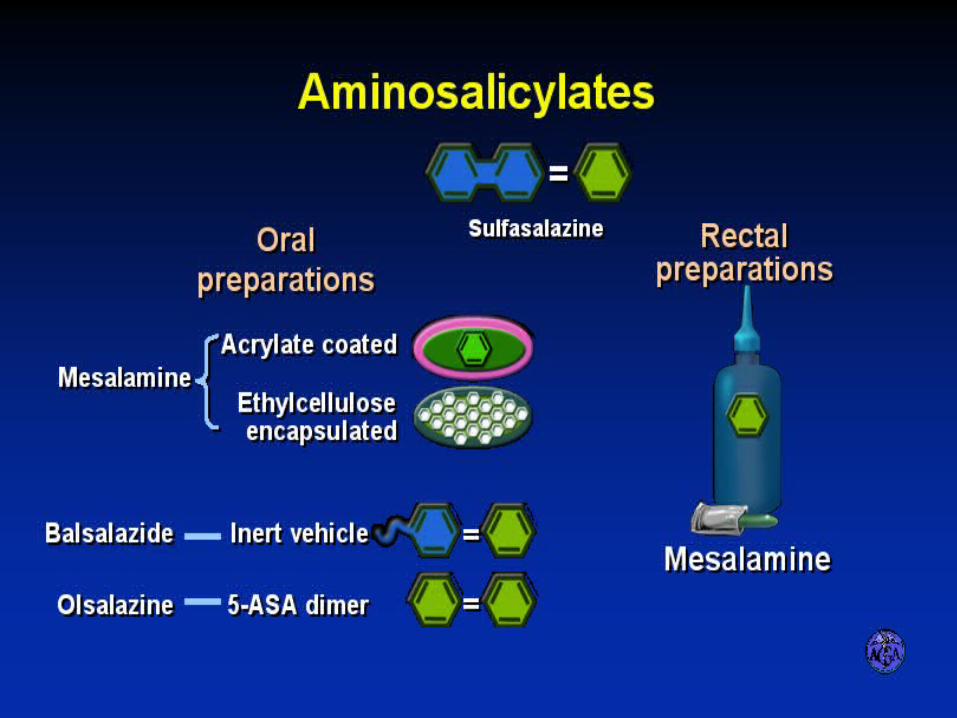
AMINOSALICYLATES
Steroid Toxicities
• Ocular – cataracts, glaucoma
• Skin – striae, atrophy, acne
• Endocrine – growth failure (pediatric), hypothalamic-pituitary-adrenal (HPA) axis suppression; glucose intolerance
• Cardiovascular – hypertension
• Other – Infection (abcess); myopathy
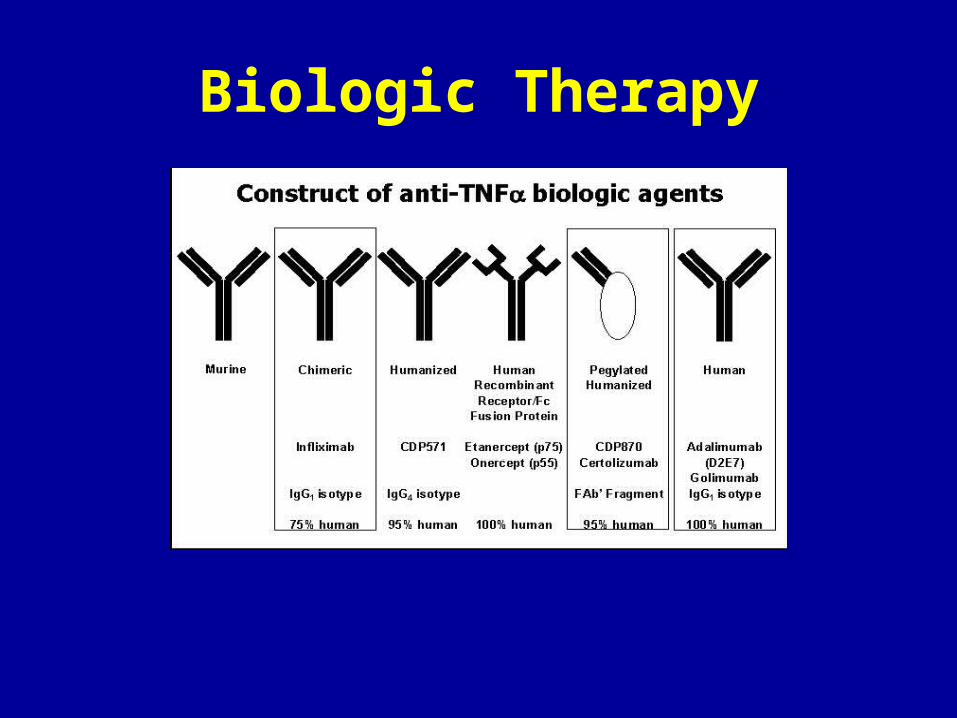
Biologic Therapy
TNF-α Inhibitors
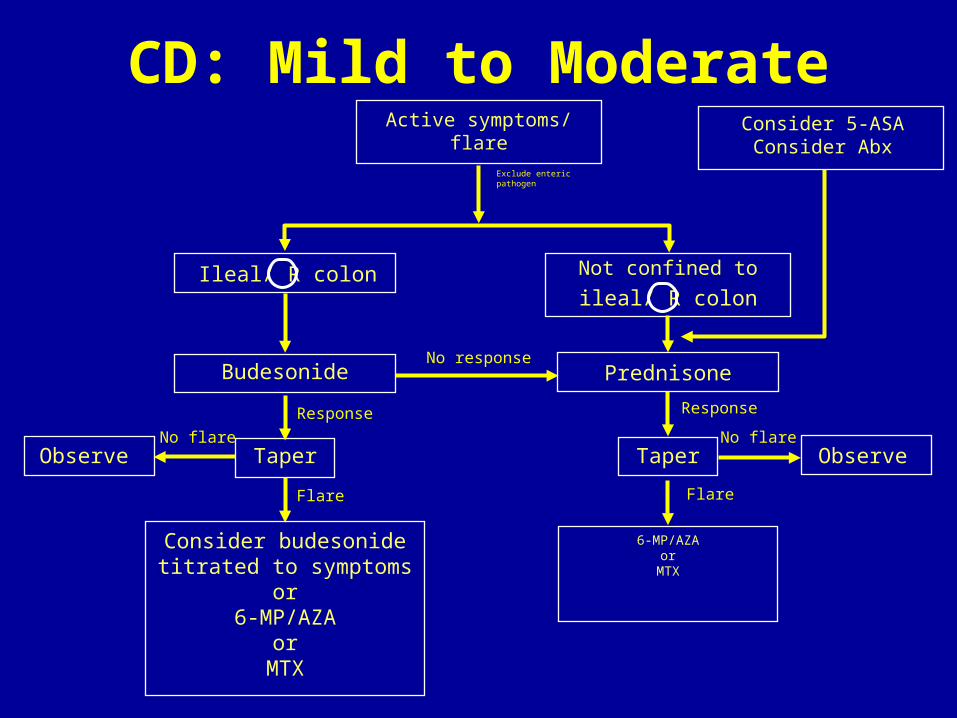
CD: Mild to ModerateActive symptoms/
flare
Budesonide
Observe Taper
Consider budesonidetitrated to symptoms
or6-MP/AZA
orMTX
Not confined to
Prednisone
Taper
6-MP/AZAor
MTX
Consider 5-ASAConsider Abx
ObserveNo flare No flare
Flare
Response
No response
Exclude entericpathogen
Flare
Response
Ileal/ R colonileal/ R colon
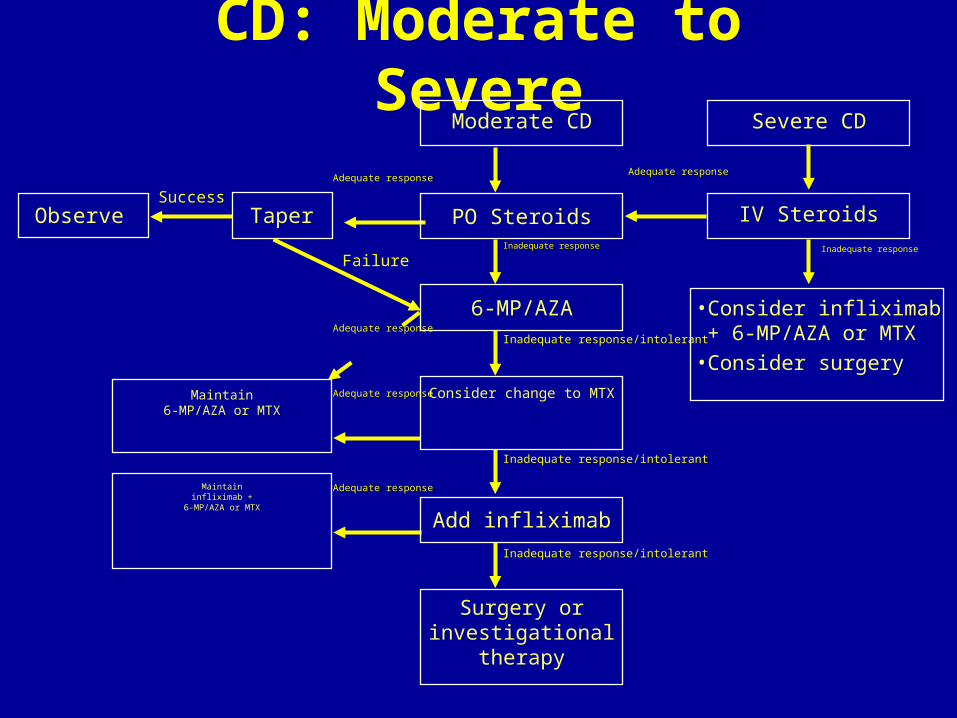
CD: Moderate to Severe
Moderate CD
Observe TaperSuccess
PO Steroids
6-MP/AZA
Consider change to MTX
Add infliximab
Surgery or investigational
therapy
Severe CD
IV Steroids
Adequate response
Inadequate response
•Consider infliximab+ 6-MP/AZA or MTX
•Consider surgery
Adequate response
Failure
Maintain6-MP/AZA or MTX
Maintaininfliximab +
6-MP/AZA or MTX
Adequate response
Adequate response
Adequate response
Inadequate response
Inadequate response/intolerant
Inadequate response/intolerant
Inadequate response/intolerant
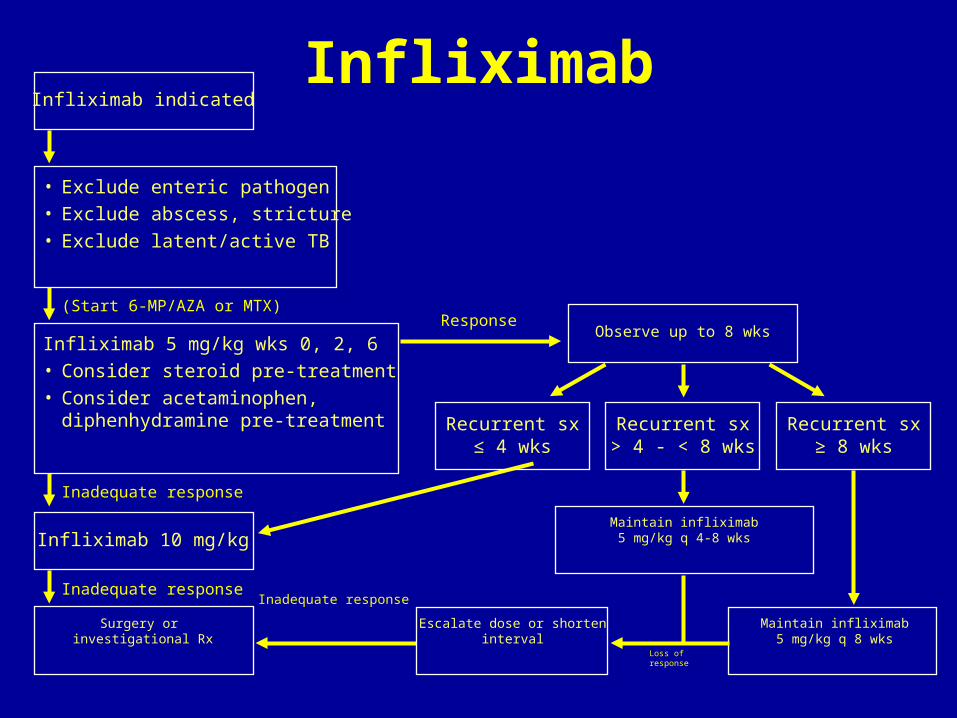
InfliximabInfliximab indicated
• Exclude enteric pathogen• Exclude abscess, stricture• Exclude latent/active TB
Infliximab 5 mg/kg wks 0, 2, 6• Consider steroid pre-treatment• Consider acetaminophen,
diphenhydramine pre-treatment
Infliximab 10 mg/kg
Surgery or investigational Rx
Observe up to 8 wks
Recurrent sx≤ 4 wks
Recurrent sx> 4 - < 8 wks
Recurrent sx≥ 8 wks
Response
Maintain infliximab5 mg/kg q 4-8 wks
Inadequate response
Escalate dose or shorten interval Maintain infliximab5 mg/kg q 8 wks
Loss of response
Inadequate response
Inadequate response
(Start 6-MP/AZA or MTX)
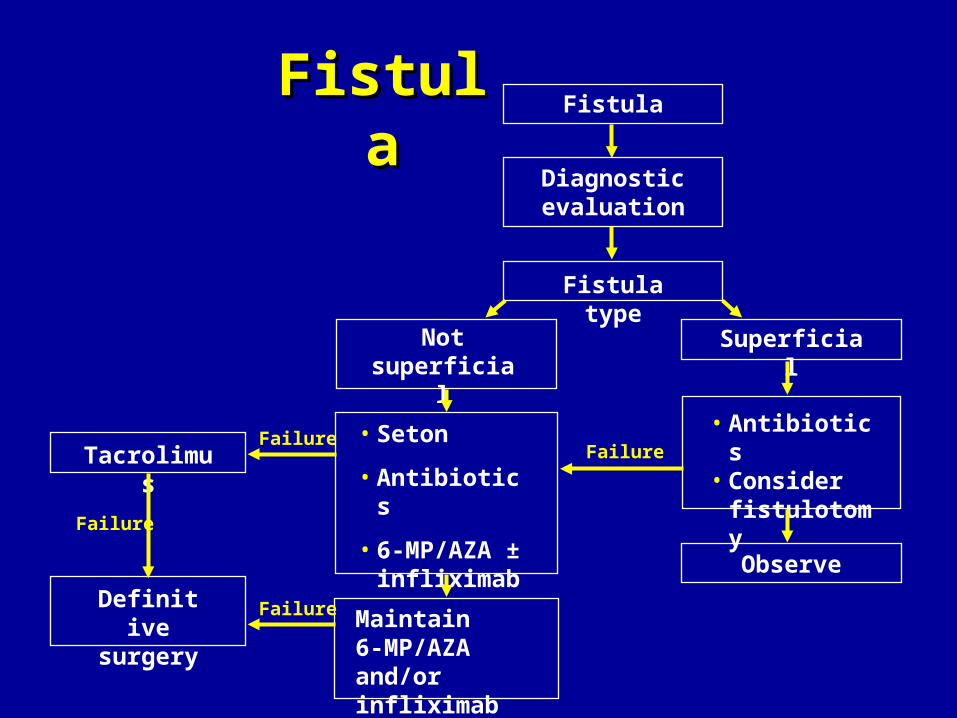
FistulaFistulaFistula
Diagnosticevaluation
Fistula type
Not superficial
Superficial
• Antibiotics• Consider
fistulotomy
Observe
FailureFailure
FailureDefinitivesurgery Maintain
6-MP/AZAand/or infliximab
Failure
Tacrolimus• Seton
• Antibiotics
• 6-MP/AZA ± infliximab
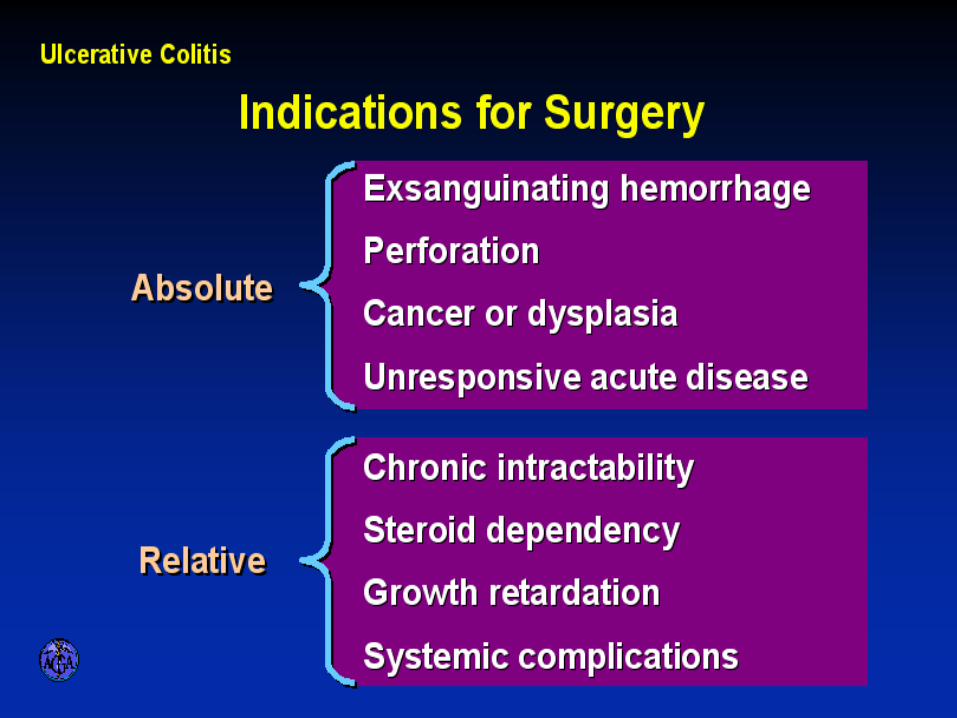
INDICATIONS FOR SURGERY IN ULCERATIVE
COLITIS
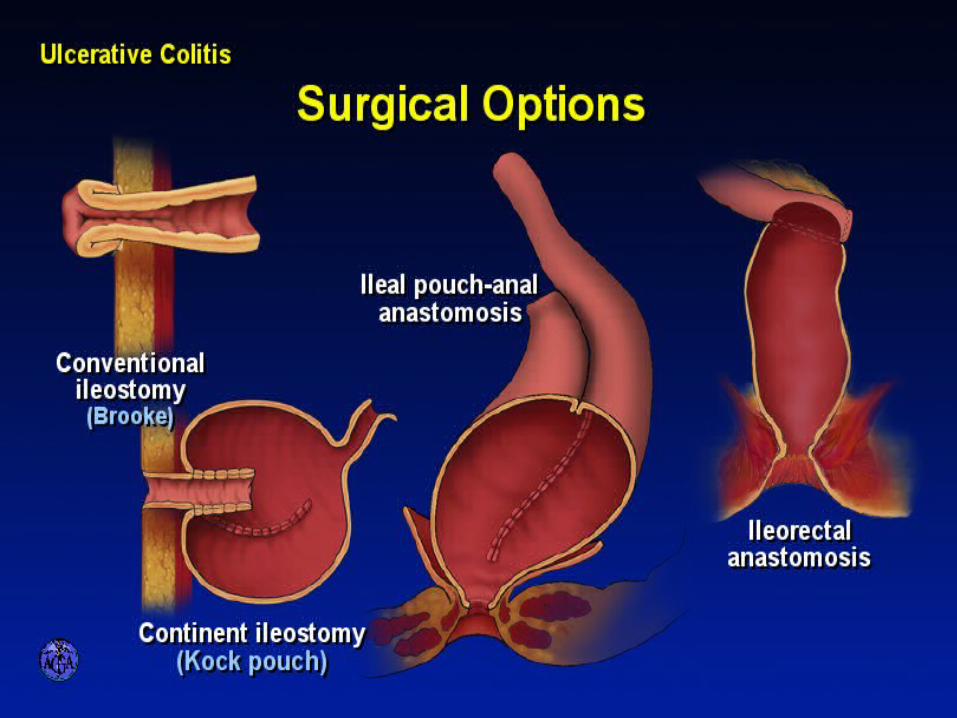
SURGICAL OPTIONS IN ULCERATIVE COLITIS
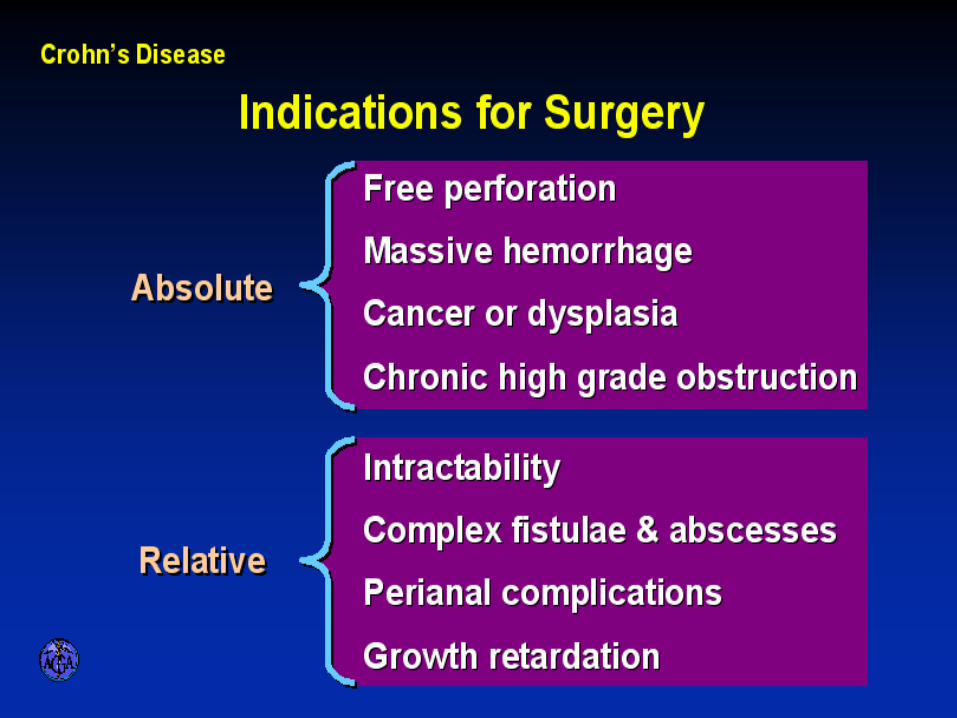
INDICATIONS FOR SURGERY IN CROHN’S
DISEASE