Embed Size (px)
Citation preview

Overview of Oral ApplianceTherapy for the Managementof Obstructive Sleep Apnea
Leopoldo P. Correa, BDS, MSKEYWORDS
� Obstructive sleep apnea � Oral appliance therapy � Continuous positive airway pressure� Multidisciplinary approach
KEY POINTS
� Oral appliances are increasingly used in dental practices, and are indicated for the management ofmild to moderate obstructive sleep apnea (OSA) and sometimes for patients with severe OSA whocannot tolerate continuous positive airway pressure therapy.
� Short-term and long-term follow-up is necessary to assess the efficacy of the device from subjec-tive and objective measurements.
� A multidisciplinary approach involving a sleep physician, a dentist, an ear/nose/throat specialist,and a primary care physician is imperative for a better treatment outcome.
� Short-term and long-term side effects may occur with appliance therapy; it is recommended thatdentists offering oral appliance therapy be educated and gain knowledge about the diagnosis, pre-vention, and management of common side effects, including temporomandibular disorders thatoccur with the use of such devices.
INTRODUCTION
Obstructive sleep apnea (OSA) is a common disor-der in the general population, with an estimatedprevalence of 4% in men and 2% in womenaged between 30 and 60 years.1 OSA is a condi-tion characterized by frequent episodes of upperairway obstruction that occurs during sleep,resulting in reduction of blood oxygen saturationand arousals from sleep.2 It is a common diseasethat is largely underdiagnosed and untreated,resulting in significant implications for cardiovas-cular disease,3 mortality,4 and economic impact.5
Affected patients have neurocognitive and neuro-behavioral impairment.6 Population-based epide-miologic studies have estimated the prevalence
Statement of Interest: The author declares no conflict ofDepartment of Oral and Maxillofacial Pathology, Oral Mof Dental Medicine, 1 Kneeland Street # 601, Boston, ME-mail address: [email protected]
Sleep Med Clin 8 (2013) 505–516http://dx.doi.org/10.1016/j.jsmc.2013.07.0071556-407X/13/$ – see front matter � 2013 Elsevier Inc. Al
and severity spectrum of undiagnosed OSA, andhave found that even mild severity is associatedwith significant morbidity.1
Common symptoms reported by patientsinclude excessive daytime sleepiness, snoring,and gastroesophageal reflux.7 Snoring is com-monly reported in these patients; the complaintof snoring precedes the complaint of daytimesleepiness, and the intensity of both increaseswith weight gain and alcohol intake.8 Retro-positioning of the tongue is one of the most com-mon features of patients with OSA. The dimensionof pharyngeal lumen and the elongation of theuvula and soft palatal draping also seem to playimportant roles in the partial or complete obstruc-tion of the upper airway.9 Other anatomic features
interest.edicine and Craniofacial Pain, Tufts University SchoolA 02111, USA
l rights reserved. sleep.theclinics.com
Correa506
common to those with OSA include mandibularretrognathism, inferiorly positioned hyoid bone,tonsillar hypertrophy, deviated septum, nasalpolyp, and enlarged nasal turbinates.10–14
Because of their practice of constant examina-tion of the maxilla, mandible, and oropharyngealareas, dental professionals have been recognizedas being part of the multidisciplinary therapeuticteam for the management of OSA by helpingto identify possible risk factors for the develop-ment of a narrow upper airway.15 The updatedpractice parameters from the American Academyof Sleep Medicine recommend the use of oralappliances for patients with mild to moderateOSA and for those with severe OSA who cannottolerate continuous positive airway pressure(CPAP) therapy.16 Current guidelines also recom-mend face-to-face evaluation with a sleep physi-cian as part of a diagnostic process that musttake place before initiation of oral appliancetherapy.
CLASSIFICATION AND MECHANISM OFACTION
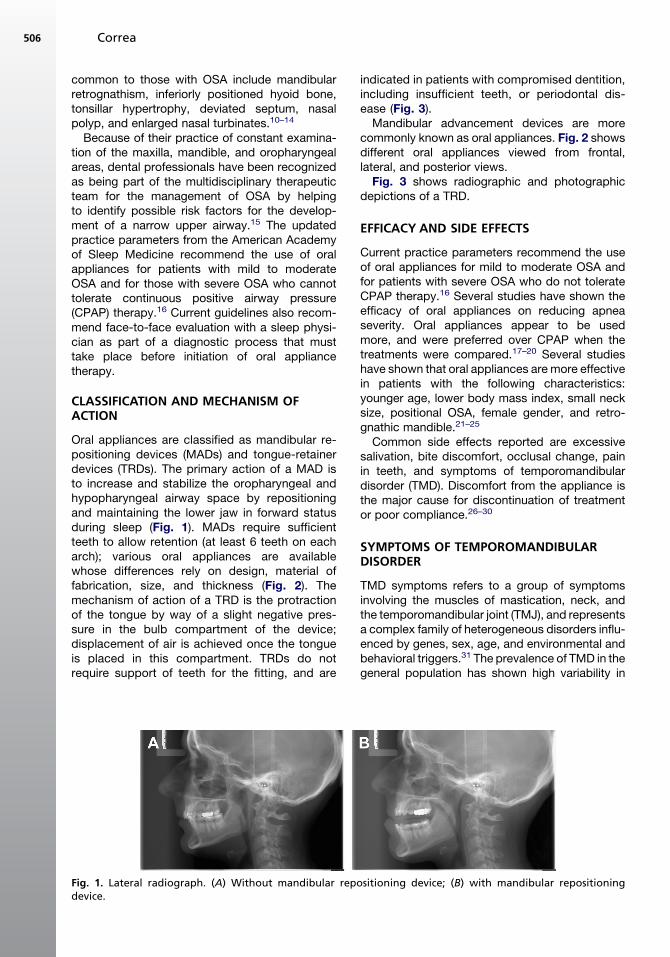
Oral appliances are classified as mandibular re-positioning devices (MADs) and tongue-retainerdevices (TRDs). The primary action of a MAD isto increase and stabilize the oropharyngeal andhypopharyngeal airway space by repositioningand maintaining the lower jaw in forward statusduring sleep (Fig. 1). MADs require sufficientteeth to allow retention (at least 6 teeth on eacharch); various oral appliances are availablewhose differences rely on design, material offabrication, size, and thickness (Fig. 2). Themechanism of action of a TRD is the protractionof the tongue by way of a slight negative pres-sure in the bulb compartment of the device;displacement of air is achieved once the tongueis placed in this compartment. TRDs do notrequire support of teeth for the fitting, and are
Fig. 1. Lateral radiograph. (A) Without mandibular repodevice.
indicated in patients with compromised dentition,including insufficient teeth, or periodontal dis-ease (Fig. 3).Mandibular advancement devices are more
commonly known as oral appliances. Fig. 2 showsdifferent oral appliances viewed from frontal,lateral, and posterior views.Fig. 3 shows radiographic and photographic
depictions of a TRD.
EFFICACY AND SIDE EFFECTS
Current practice parameters recommend the useof oral appliances for mild to moderate OSA andfor patients with severe OSA who do not tolerateCPAP therapy.16 Several studies have shown theefficacy of oral appliances on reducing apneaseverity. Oral appliances appear to be usedmore, and were preferred over CPAP when thetreatments were compared.17–20 Several studieshave shown that oral appliances are more effectivein patients with the following characteristics:younger age, lower body mass index, small necksize, positional OSA, female gender, and retro-gnathic mandible.21–25
Common side effects reported are excessivesalivation, bite discomfort, occlusal change, painin teeth, and symptoms of temporomandibulardisorder (TMD). Discomfort from the appliance isthe major cause for discontinuation of treatmentor poor compliance.26–30
SYMPTOMS OF TEMPOROMANDIBULARDISORDER
TMD symptoms refers to a group of symptomsinvolving the muscles of mastication, neck, andthe temporomandibular joint (TMJ), and representsa complex family of heterogeneous disorders influ-enced by genes, sex, age, and environmental andbehavioral triggers.31 The prevalence of TMD in thegeneral population has shown high variability in
sitioning device; (B) with mandibular repositioning
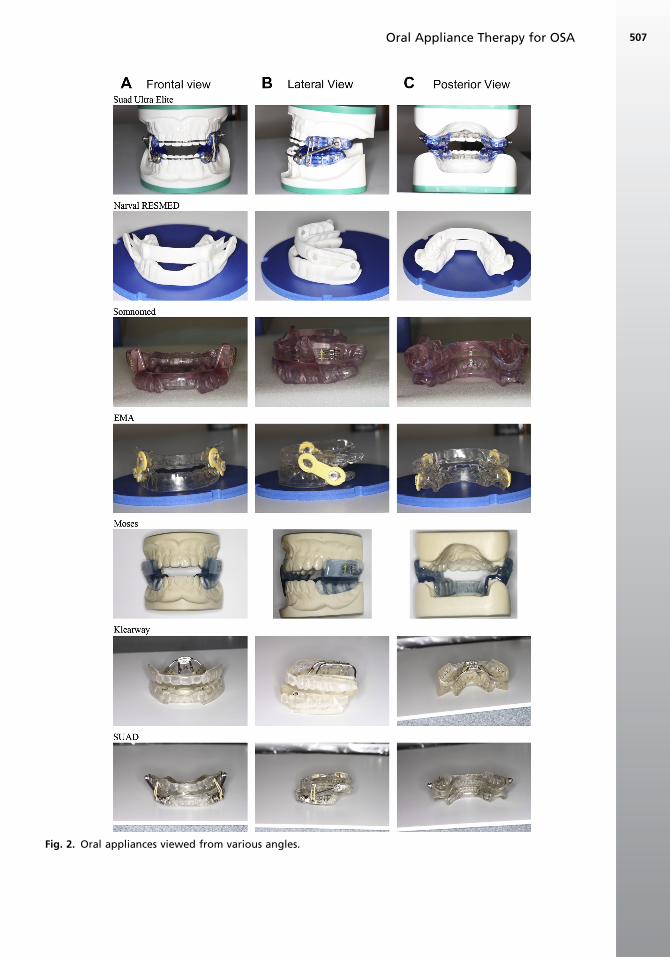
Fig. 2. Oral appliances viewed from various angles.
Oral Appliance Therapy for OSA 507
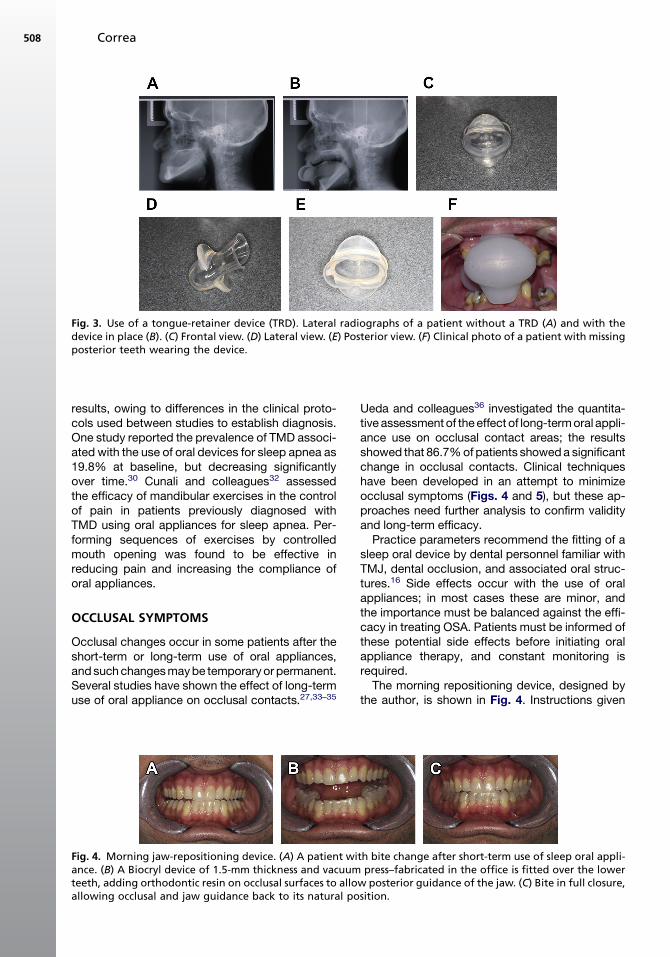
Fig. 3. Use of a tongue-retainer device (TRD). Lateral radiographs of a patient without a TRD (A) and with thedevice in place (B). (C) Frontal view. (D) Lateral view. (E) Posterior view. (F) Clinical photo of a patient with missingposterior teeth wearing the device.
Correa508
results, owing to differences in the clinical proto-cols used between studies to establish diagnosis.One study reported the prevalence of TMD associ-ated with the use of oral devices for sleep apnea as19.8% at baseline, but decreasing significantlyover time.30 Cunali and colleagues32 assessedthe efficacy of mandibular exercises in the controlof pain in patients previously diagnosed withTMD using oral appliances for sleep apnea. Per-forming sequences of exercises by controlledmouth opening was found to be effective inreducing pain and increasing the compliance oforal appliances.
OCCLUSAL SYMPTOMS
Occlusal changes occur in some patients after theshort-term or long-term use of oral appliances,andsuchchangesmaybe temporaryor permanent.Several studies have shown the effect of long-termuse of oral appliance on occlusal contacts.27,33–35
Fig. 4. Morning jaw-repositioning device. (A) A patient wiance. (B) A Biocryl device of 1.5-mm thickness and vacuumteeth, adding orthodontic resin on occlusal surfaces to alloallowing occlusal and jaw guidance back to its natural po
Ueda and colleagues36 investigated the quantita-tive assessmentof theeffect of long-termoral appli-ance use on occlusal contact areas; the resultsshowed that 86.7%of patients showeda significantchange in occlusal contacts. Clinical techniqueshave been developed in an attempt to minimizeocclusal symptoms (Figs. 4 and 5), but these ap-proaches need further analysis to confirm validityand long-term efficacy.Practice parameters recommend the fitting of a
sleep oral device by dental personnel familiar withTMJ, dental occlusion, and associated oral struc-tures.16 Side effects occur with the use of oralappliances; in most cases these are minor, andthe importance must be balanced against the effi-cacy in treating OSA. Patients must be informed ofthese potential side effects before initiating oralappliance therapy, and constant monitoring isrequired.The morning repositioning device, designed by
the author, is shown in Fig. 4. Instructions given
th bite change after short-term use of sleep oral appli-press–fabricated in the office is fitted over the lower
w posterior guidance of the jaw. (C) Bite in full closure,sition.
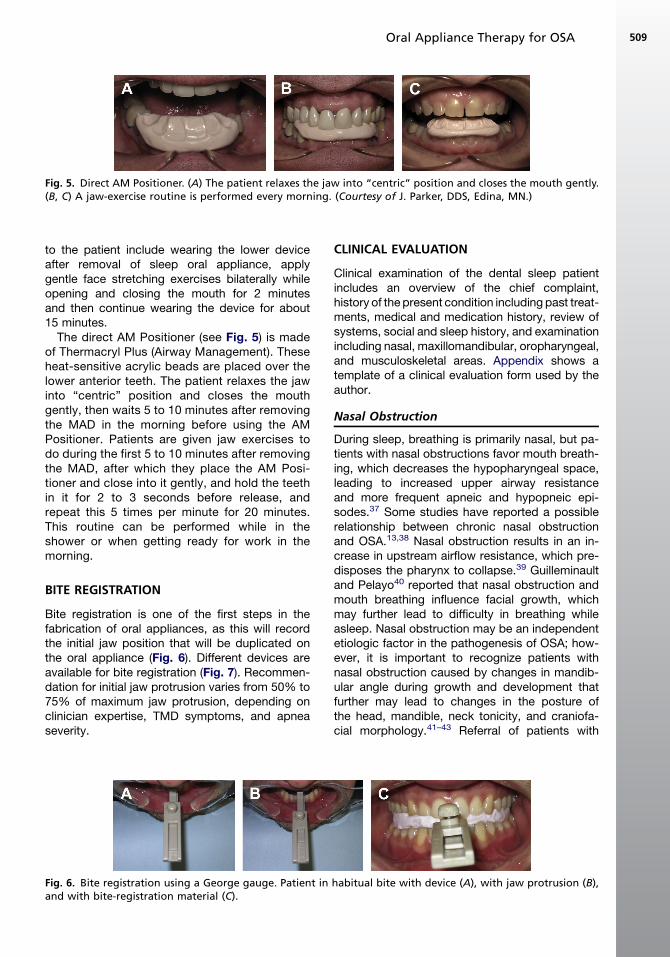
Fig. 5. Direct AM Positioner. (A) The patient relaxes the jaw into “centric” position and closes the mouth gently.(B, C) A jaw-exercise routine is performed every morning. (Courtesy of J. Parker, DDS, Edina, MN.)
Oral Appliance Therapy for OSA 509
to the patient include wearing the lower deviceafter removal of sleep oral appliance, applygentle face stretching exercises bilaterally whileopening and closing the mouth for 2 minutesand then continue wearing the device for about15 minutes.
The direct AM Positioner (see Fig. 5) is madeof Thermacryl Plus (Airway Management). Theseheat-sensitive acrylic beads are placed over thelower anterior teeth. The patient relaxes the jawinto “centric” position and closes the mouthgently, then waits 5 to 10 minutes after removingthe MAD in the morning before using the AMPositioner. Patients are given jaw exercises todo during the first 5 to 10 minutes after removingthe MAD, after which they place the AM Posi-tioner and close into it gently, and hold the teethin it for 2 to 3 seconds before release, andrepeat this 5 times per minute for 20 minutes.This routine can be performed while in theshower or when getting ready for work in themorning.
BITE REGISTRATION
Bite registration is one of the first steps in thefabrication of oral appliances, as this will recordthe initial jaw position that will be duplicated onthe oral appliance (Fig. 6). Different devices areavailable for bite registration (Fig. 7). Recommen-dation for initial jaw protrusion varies from 50% to75% of maximum jaw protrusion, depending onclinician expertise, TMD symptoms, and apneaseverity.
Fig. 6. Bite registration using a George gauge. Patient inand with bite-registration material (C).
CLINICAL EVALUATION
Clinical examination of the dental sleep patientincludes an overview of the chief complaint,history of thepresent condition including past treat-ments, medical and medication history, review ofsystems, social and sleep history, and examinationincluding nasal, maxillomandibular, oropharyngeal,and musculoskeletal areas. Appendix shows atemplate of a clinical evaluation form used by theauthor.
Nasal Obstruction
During sleep, breathing is primarily nasal, but pa-tients with nasal obstructions favor mouth breath-ing, which decreases the hypopharyngeal space,leading to increased upper airway resistanceand more frequent apneic and hypopneic epi-sodes.37 Some studies have reported a possiblerelationship between chronic nasal obstructionand OSA.13,38 Nasal obstruction results in an in-crease in upstream airflow resistance, which pre-disposes the pharynx to collapse.39 Guilleminaultand Pelayo40 reported that nasal obstruction andmouth breathing influence facial growth, whichmay further lead to difficulty in breathing whileasleep. Nasal obstruction may be an independentetiologic factor in the pathogenesis of OSA; how-ever, it is important to recognize patients withnasal obstruction caused by changes in mandib-ular angle during growth and development thatfurther may lead to changes in the posture ofthe head, mandible, neck tonicity, and craniofa-cial morphology.41–43 Referral of patients with
habitual bite with device (A), with jaw protrusion (B),
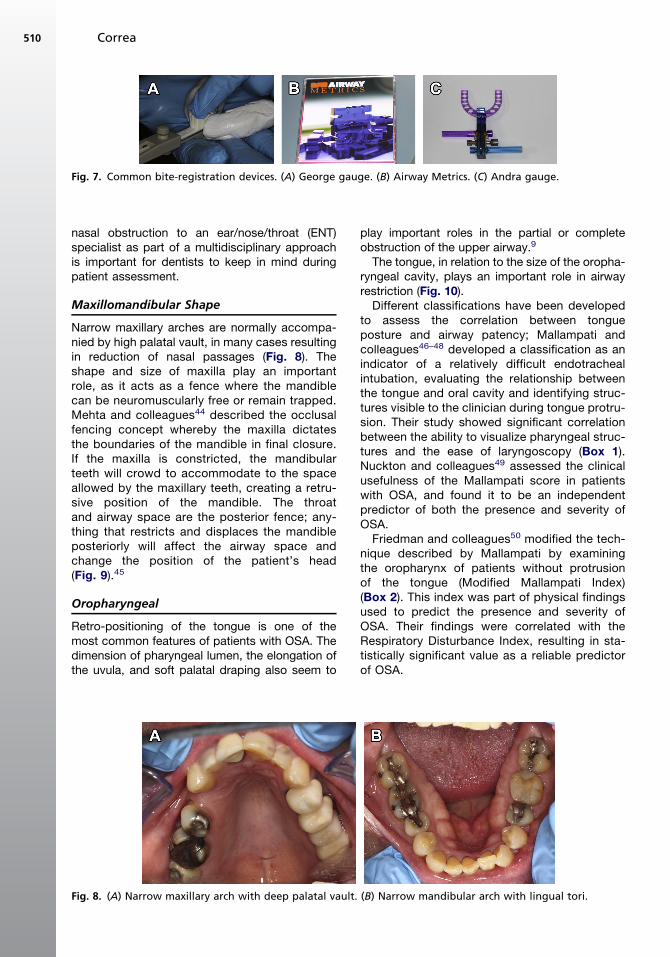
Fig. 7. Common bite-registration devices. (A) George gauge. (B) Airway Metrics. (C) Andra gauge.
Correa510
nasal obstruction to an ear/nose/throat (ENT)specialist as part of a multidisciplinary approachis important for dentists to keep in mind duringpatient assessment.
Maxillomandibular Shape
Narrow maxillary arches are normally accompa-nied by high palatal vault, in many cases resultingin reduction of nasal passages (Fig. 8). Theshape and size of maxilla play an importantrole, as it acts as a fence where the mandiblecan be neuromuscularly free or remain trapped.Mehta and colleagues44 described the occlusalfencing concept whereby the maxilla dictatesthe boundaries of the mandible in final closure.If the maxilla is constricted, the mandibularteeth will crowd to accommodate to the spaceallowed by the maxillary teeth, creating a retru-sive position of the mandible. The throatand airway space are the posterior fence; any-thing that restricts and displaces the mandibleposteriorly will affect the airway space andchange the position of the patient’s head(Fig. 9).45
Oropharyngeal
Retro-positioning of the tongue is one of themost common features of patients with OSA. Thedimension of pharyngeal lumen, the elongation ofthe uvula, and soft palatal draping also seem to
Fig. 8. (A) Narrow maxillary arch with deep palatal vault.
play important roles in the partial or completeobstruction of the upper airway.9
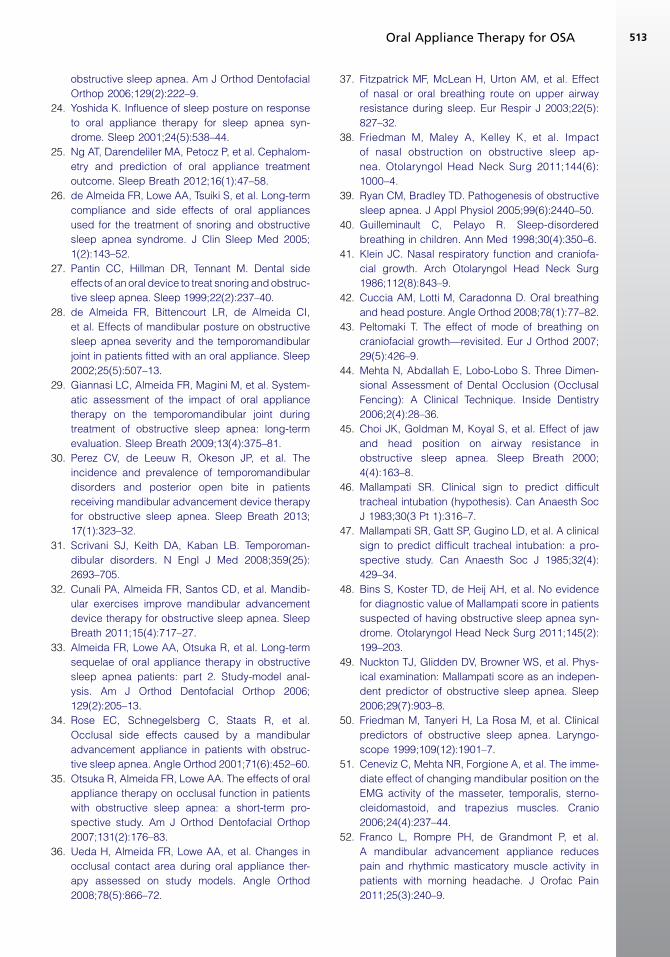
The tongue, in relation to the size of the oropha-ryngeal cavity, plays an important role in airwayrestriction (Fig. 10).Different classifications have been developed
to assess the correlation between tongueposture and airway patency; Mallampati andcolleagues46–48 developed a classification as anindicator of a relatively difficult endotrachealintubation, evaluating the relationship betweenthe tongue and oral cavity and identifying struc-tures visible to the clinician during tongue protru-sion. Their study showed significant correlationbetween the ability to visualize pharyngeal struc-tures and the ease of laryngoscopy (Box 1).Nuckton and colleagues49 assessed the clinicalusefulness of the Mallampati score in patientswith OSA, and found it to be an independentpredictor of both the presence and severity ofOSA.Friedman and colleagues50 modified the tech-
nique described by Mallampati by examiningthe oropharynx of patients without protrusionof the tongue (Modified Mallampati Index)(Box 2). This index was part of physical findingsused to predict the presence and severity ofOSA. Their findings were correlated with theRespiratory Disturbance Index, resulting in sta-tistically significant value as a reliable predictorof OSA.
(B) Narrow mandibular arch with lingual tori.
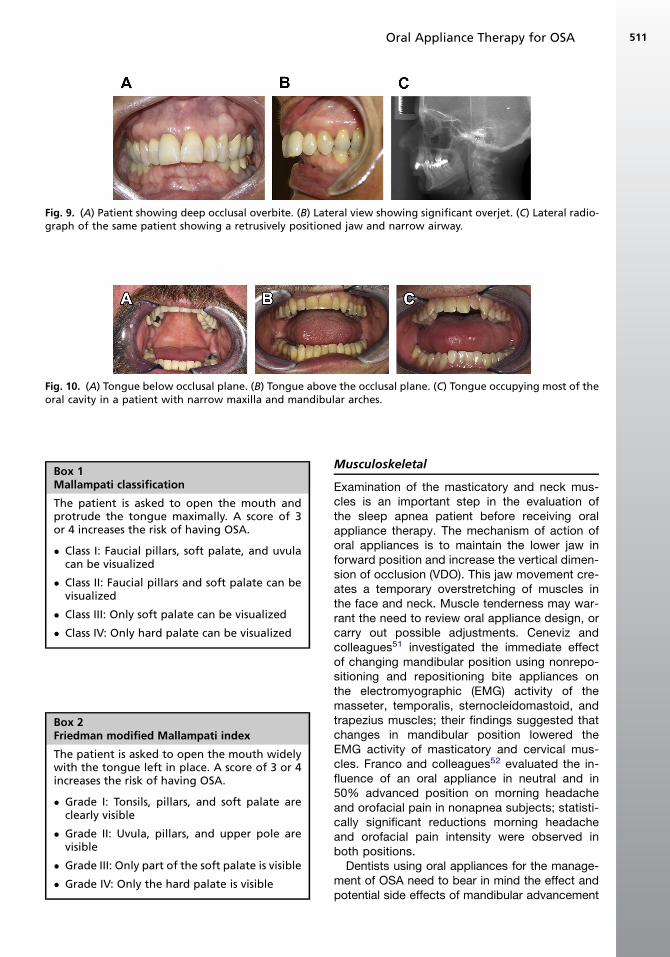
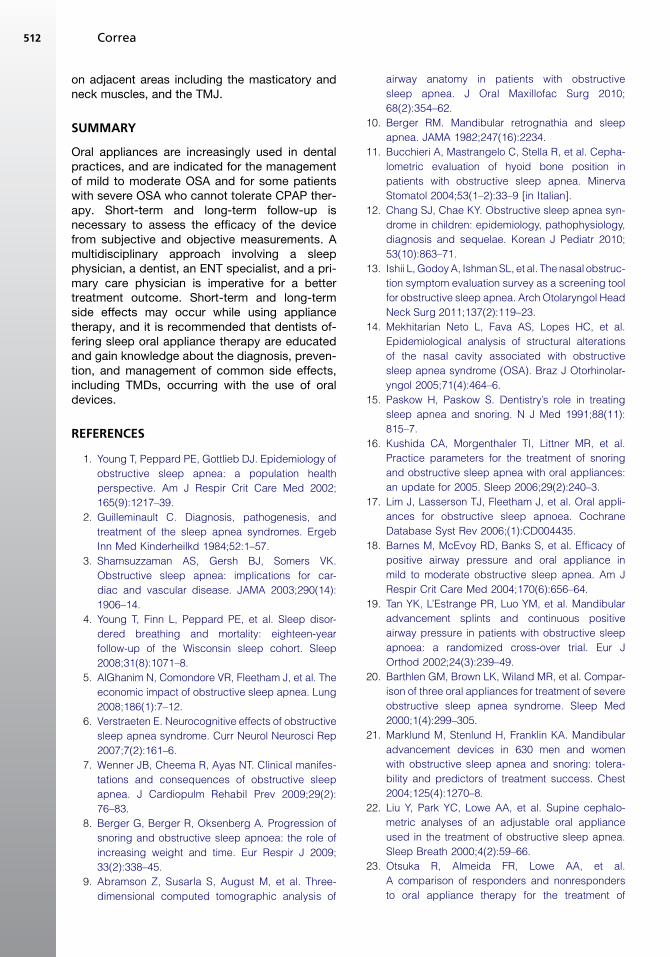
Fig. 9. (A) Patient showing deep occlusal overbite. (B) Lateral view showing significant overjet. (C) Lateral radio-graph of the same patient showing a retrusively positioned jaw and narrow airway.
Fig. 10. (A) Tongue below occlusal plane. (B) Tongue above the occlusal plane. (C) Tongue occupying most of theoral cavity in a patient with narrow maxilla and mandibular arches.
Box 1Mallampati classification
The patient is asked to open the mouth andprotrude the tongue maximally. A score of 3or 4 increases the risk of having OSA.
� Class I: Faucial pillars, soft palate, and uvulacan be visualized
� Class II: Faucial pillars and soft palate can bevisualized
� Class III: Only soft palate can be visualized
� Class IV: Only hard palate can be visualized
Box 2Friedman modified Mallampati index
The patient is asked to open the mouth widelywith the tongue left in place. A score of 3 or 4increases the risk of having OSA.
� Grade I: Tonsils, pillars, and soft palate areclearly visible
� Grade II: Uvula, pillars, and upper pole arevisible
� Grade III: Only part of the soft palate is visible
� Grade IV: Only the hard palate is visible
Oral Appliance Therapy for OSA 511
Musculoskeletal
Examination of the masticatory and neck mus-cles is an important step in the evaluation ofthe sleep apnea patient before receiving oralappliance therapy. The mechanism of action oforal appliances is to maintain the lower jaw inforward position and increase the vertical dimen-sion of occlusion (VDO). This jaw movement cre-ates a temporary overstretching of muscles inthe face and neck. Muscle tenderness may war-rant the need to review oral appliance design, orcarry out possible adjustments. Ceneviz andcolleagues51 investigated the immediate effectof changing mandibular position using nonrepo-sitioning and repositioning bite appliances onthe electromyographic (EMG) activity of themasseter, temporalis, sternocleidomastoid, andtrapezius muscles; their findings suggested thatchanges in mandibular position lowered theEMG activity of masticatory and cervical mus-cles. Franco and colleagues52 evaluated the in-fluence of an oral appliance in neutral and in50% advanced position on morning headacheand orofacial pain in nonapnea subjects; statisti-cally significant reductions morning headacheand orofacial pain intensity were observed inboth positions.
Dentists using oral appliances for the manage-ment of OSA need to bear in mind the effect andpotential side effects of mandibular advancement
Correa512
on adjacent areas including the masticatory andneck muscles, and the TMJ.
SUMMARY
Oral appliances are increasingly used in dentalpractices, and are indicated for the managementof mild to moderate OSA and for some patientswith severe OSA who cannot tolerate CPAP ther-apy. Short-term and long-term follow-up isnecessary to assess the efficacy of the devicefrom subjective and objective measurements. Amultidisciplinary approach involving a sleepphysician, a dentist, an ENT specialist, and a pri-mary care physician is imperative for a bettertreatment outcome. Short-term and long-termside effects may occur while using appliancetherapy, and it is recommended that dentists of-fering sleep oral appliance therapy are educatedand gain knowledge about the diagnosis, preven-tion, and management of common side effects,including TMDs, occurring with the use of oraldevices.
REFERENCES
1. Young T, Peppard PE, Gottlieb DJ. Epidemiology of
obstructive sleep apnea: a population health
perspective. Am J Respir Crit Care Med 2002;
165(9):1217–39.
2. Guilleminault C. Diagnosis, pathogenesis, and
treatment of the sleep apnea syndromes. Ergeb
Inn Med Kinderheilkd 1984;52:1–57.
3. Shamsuzzaman AS, Gersh BJ, Somers VK.
Obstructive sleep apnea: implications for car-
diac and vascular disease. JAMA 2003;290(14):
1906–14.
4. Young T, Finn L, Peppard PE, et al. Sleep disor-
dered breathing and mortality: eighteen-year
follow-up of the Wisconsin sleep cohort. Sleep
2008;31(8):1071–8.
5. AlGhanim N, Comondore VR, Fleetham J, et al. The
economic impact of obstructive sleep apnea. Lung
2008;186(1):7–12.
6. Verstraeten E. Neurocognitive effects of obstructive
sleep apnea syndrome. Curr Neurol Neurosci Rep
2007;7(2):161–6.
7. Wenner JB, Cheema R, Ayas NT. Clinical manifes-
tations and consequences of obstructive sleep
apnea. J Cardiopulm Rehabil Prev 2009;29(2):
76–83.
8. Berger G, Berger R, Oksenberg A. Progression of
snoring and obstructive sleep apnoea: the role of
increasing weight and time. Eur Respir J 2009;
33(2):338–45.
9. Abramson Z, Susarla S, August M, et al. Three-
dimensional computed tomographic analysis of
airway anatomy in patients with obstructive
sleep apnea. J Oral Maxillofac Surg 2010;
68(2):354–62.
10. Berger RM. Mandibular retrognathia and sleep
apnea. JAMA 1982;247(16):2234.
11. Bucchieri A, Mastrangelo C, Stella R, et al. Cepha-
lometric evaluation of hyoid bone position in
patients with obstructive sleep apnea. Minerva
Stomatol 2004;53(1–2):33–9 [in Italian].
12. Chang SJ, Chae KY. Obstructive sleep apnea syn-
drome in children: epidemiology, pathophysiology,
diagnosis and sequelae. Korean J Pediatr 2010;
53(10):863–71.
13. Ishii L, GodoyA, IshmanSL, et al. The nasal obstruc-
tion symptom evaluation survey as a screening tool
for obstructive sleep apnea. Arch Otolaryngol Head
Neck Surg 2011;137(2):119–23.
14. Mekhitarian Neto L, Fava AS, Lopes HC, et al.
Epidemiological analysis of structural alterations
of the nasal cavity associated with obstructive
sleep apnea syndrome (OSA). Braz J Otorhinolar-
yngol 2005;71(4):464–6.
15. Paskow H, Paskow S. Dentistry’s role in treating
sleep apnea and snoring. N J Med 1991;88(11):
815–7.
16. Kushida CA, Morgenthaler TI, Littner MR, et al.
Practice parameters for the treatment of snoring
and obstructive sleep apnea with oral appliances:
an update for 2005. Sleep 2006;29(2):240–3.
17. Lim J, Lasserson TJ, Fleetham J, et al. Oral appli-
ances for obstructive sleep apnoea. Cochrane
Database Syst Rev 2006;(1):CD004435.
18. Barnes M, McEvoy RD, Banks S, et al. Efficacy of
positive airway pressure and oral appliance in
mild to moderate obstructive sleep apnea. Am J
Respir Crit Care Med 2004;170(6):656–64.
19. Tan YK, L’Estrange PR, Luo YM, et al. Mandibular
advancement splints and continuous positive
airway pressure in patients with obstructive sleep
apnoea: a randomized cross-over trial. Eur J
Orthod 2002;24(3):239–49.
20. Barthlen GM, Brown LK, Wiland MR, et al. Compar-
ison of three oral appliances for treatment of severe
obstructive sleep apnea syndrome. Sleep Med
2000;1(4):299–305.
21. Marklund M, Stenlund H, Franklin KA. Mandibular
advancement devices in 630 men and women
with obstructive sleep apnea and snoring: tolera-
bility and predictors of treatment success. Chest
2004;125(4):1270–8.
22. Liu Y, Park YC, Lowe AA, et al. Supine cephalo-
metric analyses of an adjustable oral appliance
used in the treatment of obstructive sleep apnea.
Sleep Breath 2000;4(2):59–66.
23. Otsuka R, Almeida FR, Lowe AA, et al.
A comparison of responders and nonresponders
to oral appliance therapy for the treatment of
Oral Appliance Therapy for OSA 513
obstructive sleep apnea. Am J Orthod Dentofacial
Orthop 2006;129(2):222–9.
24. Yoshida K. Influence of sleep posture on response
to oral appliance therapy for sleep apnea syn-
drome. Sleep 2001;24(5):538–44.
25. Ng AT, Darendeliler MA, Petocz P, et al. Cephalom-
etry and prediction of oral appliance treatment
outcome. Sleep Breath 2012;16(1):47–58.
26. de Almeida FR, Lowe AA, Tsuiki S, et al. Long-term
compliance and side effects of oral appliances
used for the treatment of snoring and obstructive
sleep apnea syndrome. J Clin Sleep Med 2005;
1(2):143–52.
27. Pantin CC, Hillman DR, Tennant M. Dental side
effects of an oral device to treat snoring andobstruc-
tive sleep apnea. Sleep 1999;22(2):237–40.
28. de Almeida FR, Bittencourt LR, de Almeida CI,
et al. Effects of mandibular posture on obstructive
sleep apnea severity and the temporomandibular
joint in patients fitted with an oral appliance. Sleep
2002;25(5):507–13.
29. Giannasi LC, Almeida FR, Magini M, et al. System-
atic assessment of the impact of oral appliance
therapy on the temporomandibular joint during
treatment of obstructive sleep apnea: long-term
evaluation. Sleep Breath 2009;13(4):375–81.
30. Perez CV, de Leeuw R, Okeson JP, et al. The
incidence and prevalence of temporomandibular
disorders and posterior open bite in patients
receiving mandibular advancement device therapy
for obstructive sleep apnea. Sleep Breath 2013;
17(1):323–32.
31. Scrivani SJ, Keith DA, Kaban LB. Temporoman-
dibular disorders. N Engl J Med 2008;359(25):
2693–705.
32. Cunali PA, Almeida FR, Santos CD, et al. Mandib-
ular exercises improve mandibular advancement
device therapy for obstructive sleep apnea. Sleep
Breath 2011;15(4):717–27.
33. Almeida FR, Lowe AA, Otsuka R, et al. Long-term
sequelae of oral appliance therapy in obstructive
sleep apnea patients: part 2. Study-model anal-
ysis. Am J Orthod Dentofacial Orthop 2006;
129(2):205–13.
34. Rose EC, Schnegelsberg C, Staats R, et al.
Occlusal side effects caused by a mandibular
advancement appliance in patients with obstruc-
tive sleep apnea. Angle Orthod 2001;71(6):452–60.
35. Otsuka R, Almeida FR, Lowe AA. The effects of oral
appliance therapy on occlusal function in patients
with obstructive sleep apnea: a short-term pro-
spective study. Am J Orthod Dentofacial Orthop
2007;131(2):176–83.
36. Ueda H, Almeida FR, Lowe AA, et al. Changes in
occlusal contact area during oral appliance ther-
apy assessed on study models. Angle Orthod
2008;78(5):866–72.
37. Fitzpatrick MF, McLean H, Urton AM, et al. Effect
of nasal or oral breathing route on upper airway
resistance during sleep. Eur Respir J 2003;22(5):
827–32.
38. Friedman M, Maley A, Kelley K, et al. Impact
of nasal obstruction on obstructive sleep ap-
nea. Otolaryngol Head Neck Surg 2011;144(6):
1000–4.
39. Ryan CM, Bradley TD. Pathogenesis of obstructive
sleep apnea. J Appl Physiol 2005;99(6):2440–50.
40. Guilleminault C, Pelayo R. Sleep-disordered
breathing in children. Ann Med 1998;30(4):350–6.
41. Klein JC. Nasal respiratory function and craniofa-
cial growth. Arch Otolaryngol Head Neck Surg
1986;112(8):843–9.
42. Cuccia AM, Lotti M, Caradonna D. Oral breathing
and head posture. Angle Orthod 2008;78(1):77–82.
43. Peltomaki T. The effect of mode of breathing on
craniofacial growth—revisited. Eur J Orthod 2007;
29(5):426–9.
44. Mehta N, Abdallah E, Lobo-Lobo S. Three Dimen-
sional Assessment of Dental Occlusion (Occlusal
Fencing): A Clinical Technique. Inside Dentistry
2006;2(4):28–36.
45. Choi JK, Goldman M, Koyal S, et al. Effect of jaw
and head position on airway resistance in
obstructive sleep apnea. Sleep Breath 2000;
4(4):163–8.
46. Mallampati SR. Clinical sign to predict difficult
tracheal intubation (hypothesis). Can Anaesth Soc
J 1983;30(3 Pt 1):316–7.
47. Mallampati SR, Gatt SP, Gugino LD, et al. A clinical
sign to predict difficult tracheal intubation: a pro-
spective study. Can Anaesth Soc J 1985;32(4):
429–34.
48. Bins S, Koster TD, de Heij AH, et al. No evidence
for diagnostic value of Mallampati score in patients
suspected of having obstructive sleep apnea syn-
drome. Otolaryngol Head Neck Surg 2011;145(2):
199–203.
49. Nuckton TJ, Glidden DV, Browner WS, et al. Phys-
ical examination: Mallampati score as an indepen-
dent predictor of obstructive sleep apnea. Sleep
2006;29(7):903–8.
50. Friedman M, Tanyeri H, La Rosa M, et al. Clinical
predictors of obstructive sleep apnea. Laryngo-
scope 1999;109(12):1901–7.
51. Ceneviz C, Mehta NR, Forgione A, et al. The imme-
diate effect of changing mandibular position on the
EMG activity of the masseter, temporalis, sterno-
cleidomastoid, and trapezius muscles. Cranio
2006;24(4):237–44.
52. Franco L, Rompre PH, de Grandmont P, et al.
A mandibular advancement appliance reduces
pain and rhythmic masticatory muscle activity in
patients with morning headache. J Orofac Pain
2011;25(3):240–9.
Correa514
APPENDIX: CLINICAL EVALUATION FORM
Date of Service:
Patient: Date of Birth: Primary Care Physician: Sleep Physician:
REASON FOR VISIT:
CHIEF COMPLAINT (concise statement in the patient’s
HISTORY OF PRESENT ILLNESS / PROBLEM (chronpatient’s present illness/ medical condition from the first encounter to the present-Quality-Duration-severity-timinsymptoms):
REVIEW OF SYSTEMS (An inventory of body systemsorder to identify signs and/or symptoms that the patient m
• Constitutional (Unexplained weight loss, nightitch/rash, recent trauma, lumps/bumps/masses,
• Eyes (Visual changes, headache, eye pain, dou
• Ear, Nose, Mouth, Throat: (Runny nose, frequringing in ears, gingival bleeding, toothache, so
• Cardiovascular (Chest pain, shortness of breathloss of consciousness):
• Respiratory (Shortness of breath, cough, exercinose, mouth breather):
• Gastrointestinal (Abdominal pain, changes in avomiting, diarrhea, constipation):
• Musculoskeletal (TMJ, neck, pain, misalignmeimproves/worsens with activity), joint swelling
• Urinary (Incontinence, frequency, urgency, noc
• Skin (Pruritus, rashes, stria, lesions, wounds, indryness and/or discoloration):
• Neurological (Fainting, numbness, tingling, treand taste, seizures, headache, poor balance, spe
• Psychiatric (Memory loss, depression, anxiety,performance):
• Endocrine (Thyroid disfunction, diabetes):
• Hematologic (Anemia, bleeding disorders, exc
• Allergic / Immunologic (Difficulty breathing oanything, swelling or pain swollen, allergic resreaction to bee sting, unusual sneezing, runny nenvironmental allergy):
own words):
ological description of the development of the sign and/or symptom or from the previous g-modifying factors, associated signs and
obtained by asking a series of questions in ay be experiencing or has experienced):
sweats, fatigue, sleeping pattern, appetite, fever, unexplained falls):
ble vision, blind spots, floaters):
ent nose bleeds, sinus pain, stuffy ears, ear pain, re throat, pain with swallowing):
, exercise intolerance, palpitations, faintness,
se intolerance, difficulty breathing through the
ppetite, heartburn, indigestion, nausea,
nt, stiffness morning vs day long; , decreased range of motion, crepitus, arthritis):
turia, pain):
cisions, nodules, tumors, eczema, excessive
mors, weakness, changes in sight, smell, hearing ech problems):
stress, mood changes, school or work
essive bleeding, blood transfusion):
r feeling of choking as a result of exposure to ponse (rash/itch) to materials, foods, animals; ose or itchy/teary eyes; food, medication or
PAST FAMILY AND SOCIAL HISTORY: MEDICAL HISTORY (Total sum of health status prior to the presenting problem):
• General state of health (excellent, good, fair, poor):
• Medical conditions:
• Prescription medications:
• Over the counter medications:
• Supplements and herbs:
• Allergies (to medications, latex, environment, food, animals):
• Injuries (note the type and date of injury):
• Surgical procedures:
• Hospitalizations (including all surgical, medical, and psychiatric hospitalizations):
FAMILY HISTORY (Review of medical events in the patient’s family):
• Father:
• Mother:
• Sister(s):
• Brother(s):
SOCIAL HISTORY (An age appropriate review of past and current activities):
• Marital status (Single, married, divorced, widow)
• Children (number, gender, and ages):
• Occupation (some occupations linked to health problems):
• Work schedule (day / night shift):
• Caffeine intake (type, amount, and duration):
• Alcohol intake (type, amount, and duration):
• History of substance abuse (type, amount, duration, and rehabilitation):
• Smoking history (type, amount, and duration):
• Diet history (balance of food, time of meals, snacks, soda intake, water intake):
• Physical exercise (type, amount, and duration):
• Psychiatric History: (Affective symptoms-Depression-anxiety-stress-suicidal ideation-domestic violence-litigation “disability”-functional impairmentents)
SLEEP HISTORY:
• Bed time schedule (weekdays and weekends):
• Time to fall asleep (activities before falling asleep-reading, watching TV, social media):
• Difficulty falling asleep:
• Difficulty maintaining asleep:
• Hours of sleep (weekdays and weekends):
• Wake up schedule (weekdays and weekends):
• Night time symptoms: (Snoring, witnessed apnea episodes, excessive movement, violent sleep behavior, sleep walking, sleep talking, frequent awakenings, clenching and grinding, headaches, TMJ pain)
• Daytime symptoms: (Excessive daytime sleepiness, fatigue, need to take naps, morning headaches
• Impairments: Drowsy driving, difficulty concentrating, memory problems)
PSG SLEEP STUDY DATASleep efficiency: Apnea Hypopnea Index (AHI): Respiratory Disturbance Index (RDI): # Apneas: # Hypopneas: # RERAS # Central Apneas: Minimum 02: Nadir O2:
Oral Appliance Therapy for OSA 515
EXAMINATION:
GENERAL APPEARENCE (Development – Nutrition - Deformities - Attention to grooming):
VITAL SIGNS (Blood pressure - Pulse rate- Respiratory rate- Height – Weight – Pain Level):
OROPHARYNGEAL: Lips (Presence of sores, dryness, bleeding) :
Teeth (Missing teeth, dental work, wear facets, decay, fractures, occlusion classification, dental midline deviation):
Gums (Periodontal disease, gum recession, inflammation, frenum midline deviation):
Maxillary Arch (Arch size and shape (small-medium-large-narrow-V shape-constricted), palatal vault (deep, normal), presence of palatal tori, maxillary canting, occlusal plane/curve):
Mandibular Arch (Arch size and shape (small-medium-large-retrognatic-constricted), presence of lingual tori, occlusal plane/curve):
Maxillo-Mandibular Relationship (Point of first contact on closure, jaw shifting after point of first contact, occlusal fence I (antero-posterior restriction-incisors inclination), occlusal fence II (lateral restriction- canines inclination), occlusal fence III (Reduction of VDO- molars inclination):
Soft palate (Short-elongated) - Tongue (Size, posture related to occlusal plane (above-below), scalloped) –
Uvula (small-medium-large-absent) - Tonsils (small-medium-large-absent)- Mallampati classification (I - II – III - IV)
MUSCULOSKELETAL: Head posture (Normal - mild - moderate - severe):
Shoulders posture (Normal – rounded):
Masticatory muscles Palpation: Tenderness / pain (mild-moderate-severe-right-left) on masseter (deep and superficial), temporal tendon, lateral and medial pterygoids, digastric, hyoid muscles (supra-infra), temporalis (anterior-medial-posterior fibers)
Neck and shoulder muscle palpation: Tenderness / pain (mild-moderate-severe-unilateral-bilateral) on sternocleidomastoid, mastoids, scalenus, trapezius, deltoids, posterior neck muscles.
Temporomandibular Joint (TMJ): Palpation (pain-tenderness), auscultation (clicking, crepitus, unilateral-bilateral-early opening-late opening), subluxation, open lock, range of motion (opening-lateral-protrusion), deviation on opening (left-right-straight).
RADIOGRAPHIC IMAGING FINDINGS: Panoramic: / Cephalogram / CT scan
ASSESSMENT: (Diagnosis with medical codes + Summary of today’s procedures)
TREATMENT PLAN (Treatment recommendations - Referrals – Prescriptions - Future plan – Next visit):
DENTIST NAME (Provider):
Signature: ______________________________ DATE: ___________
Correa516





























