Embed Size (px)
Citation preview
Vol. 11: 139-146, September 2006
ORIGINALRESEARCH
PAPER
139
Key words: Attention-deficit/hyperactivity disorder, BMI,basal metabolic rate (BMR).Correspondence to:Prof. Dr. R.G. LaessleDepartment of PsychologyUniversity of Trier54286 TrierGermanyE-mail: [email protected]: November 28, 2005Accepted: February 21, 2006
Overweight and basal metabolic ratein boys with attention-deficit/hyperactivity disorder
R. Hubel*, J. Jass*, A. Marcus**, and R.G. Laessle**Department of Psychology, University of Trier, and **Child and Adolescent Psychiatry, Mutterhaus derBorromäerinnen, Trier, Germany
ABSTRACT. We investigated a possible association between attention-deficit/hyperactivitydisorder (ADHD) and overweight by measuring weight status and energy expenditure (basalmetabolic rate, BMR) in 39 ADHD-boys with hyperactivity (mixed hyperactive/impulsive andinattentive or predominantly hyperactive/impulsive) and 30 healthy boys. The age range forthe total group was 8-14 years. Weight and height were measured by a calibrated scales andstadiometer. Body mass index standard deviation scores (BMI-SDS) were calculated. BMRwas determined by indirect calorimetry. Significant differences were obtained between theADHD- and the control-group, but not between ADHD-subgroups. Both BMI-SDS and BMRwere higher in the group of ADHD-boys, whereby the differences were more marked whenthey were older. More overweight and obese subjects were found in the ADHD-sample.Impulsive behavior in ADHD-boys with hyperactivity may lead to an increased food intake,which is then likely to overcompensate the heightened energy expenditure.(Eating Weight Disord. 11: 139-146, 2006). ©2006, Editrice Kurtis
INTRODUCTION
Children with an attention-deficit/hyper-activity disorder (ADHD) are described asfidgety, having problems to sit still, to walkabout or to climb in situations were this isnot appropriate, having problems to playquietly, also they seem to be driven and/orto talk too much. Symptoms of frequentlyco-occuring impulsivity are answers toquestions before the question is finallyasked, problems to wait one´s turn and todisturb others frequently. In combinationwith these symptoms or exclusively, symp-toms of inattention (i.e. making oversights,maintain attention over longer periods oftime or not listening to others) may also beobservable (1). To fulfil the diagnosis of anADHD some of the symptoms have to beexistent before the age of seven, there haveto be disturbances in at least two areas(school, at home e.g.) and clinical significantdisturbances in at least one area and thereis no disorder which could explain thesymptoms better.
The prevalence of ADHD is 3-5% atschool age (1). Boys significantly moreoften suffer from an ADHD than girls. Theratio varies between 3:1 and 9:1 (2). In addi-tion boys more often show hyperactive
symptoms whereas girls with ADHD seemto be mainly inattentive.
Current etiologic and pathogenetic mod-els of ADHD combine neurological, geneticand psychosocial factors. In an integrativemodel of Döpfner (3) a genetic dispositionleads to biochemical dysfunctions in thedopamine-neurotransmitter-system andcerebral disorders. These disturbancescause problems in self-regulation andimpulse-inhibition (4) which finally generatesymptoms of inattention, impulsivity andhyperactivity. In addition adverse interac-tions with significant others can lead to co-morbid symptoms (e.g. aggressive behav-iors) and moderate the magnitude of symp-toms of ADHD. In psychiatric therapy stim-ulants are the most frequently administeredmedications.
While dopamine seems to play a promi-nent role in the development of ADHD, itshould be noted that also obesity seems tobe associated with an abnormal dopamine-metabolism. For example Wang et al. (5)examined ten morbidly obese patients (5men and 5 women, aged 26-54 years) with amean BMI of 51.2 kg/m2 and ten normalweight subjects (7 men and 3 women, aged25-45 years) with a mean BMI of 24.7 kg/m2.The association between availability of

dopamine-D2-receptors in the striatium (mea-sured per PET) and weight status was investi-gated. Obese subjects showed significantlylower values of dopamine-D2-receptor-avail-ability than the normal weights. Furthermore,availability of dopamine-D2-receptors was neg-atively correlated with BMI in the group ofobese subjects.
In addition the major dopamine gene that hasbeen associated with ADHD (i.e. DRD4) seemsto be associated with various aspects of feedingregulation and obesity in humans. For exampleLevitan et al. (6) found an association of the 7Rallele of DRD4 with a unique developmentaltrajectory characterized by attention deficitsand dysphoria in childhood and mild to moder-ate obesity in adulthood in 108 overeatingwomen with a seasonal affective disorder.
Epidemiological research suggests that obesityin childhood is associated with a reduced level ofphysical activity (7). Children with ADHD on theother hand are physically hyperactive per defini-tion and more active than healthy children. Onewould therefore expect hyperactive childrenrather to have a normal or low weight statusbecause of an increased energy expenditure (seebelow). Holtkamp et al. (8) investigated theprevalence of overweight and obesity in hyper-active children aged 5-15 years. The subjectswere inpatient and outpatient clients of a childand adolescent psychiatry. Ninety-seven boys(age: M=10 years) with a DSM-IV diagnosis ofADHD (mixed type hyperactive/impulsive andinattentive) who didn´t receive any orexigenicmedication and hadn´t any other psychiatricdiagnosis except conduct disorders were exam-ined. Fourteen boys received stimulant medica-tion. Body mass index standard deviation scores(BMI-SDS) were calculated und compared tothose of a German reference population. Themean BMI-SDS of the ADHD-children was sig-nificantly higher than in the reference popula-tion. Also there were more children with a BMIabove the 90th percentile (indicating overweight)and above the 97th percentile (indicating obesi-ty) than expected. These data support theassumption that ADHD-children with hyperac-tivity may be at risk for overweight in childhood.
Additionally, one should be aware of the factthat to date it is still unclear if merely hyperac-tivity/impulsivity or attentional problems orboth are related to an abnormal eating behaviorand/or obesity. For example Agranat-Meged etal. (9) investigated children, referred to a pedi-atric clinic because of severe obesity. The finalsample consisted of 26 children (50% male)aged 8-17 years (M=13.04 years) without anyclinical eating disorder or a binge eating disor-der. All children had a BMI higher than the 85th
percentile for age. Fifteen of the 26 (57.7%) chil-dren had a diagnosis of ADHD, which is higherthan in general population. The proportion ofboys to girls was 2:1, which is consistent withother results of prevalence-studies. Sixty percent of the children had a diagnosis of ADHDof the combined type, 40% a diagnosis ofADHD of the predominantly inattentive sub-type. Thus these results show a high comorbidi-ty of ADHD and obesity in children and adoles-cents, whereas the sample of this studyshouldn´t be taken as representative. Agranat-Meged et al. (9) speculate that obesity in chil-dren with ADHD can be ascribed to overeatingwhich is caused by a poor regulation, whichseems to be apparent even in ADHS of the pre-dominantly inattentive subtype.
Fleming et al. (10) investigated 75 women withsevere obesity, mean age 40.4 years and a meanBMI of 43.1 kg/m2, referred to na obesity-clinic.Patients filled out the Wender Utah Rating Scale(WURS), which retrospectively assesses symp-toms of ADHD in childhood. Additionally theConners´ Adult ADHD Rating Scale (CAARS)was applied, which asks for current symptomsof ADHD as well as the Brown ADD Scale forAdults (BASA), which mainly assesses symp-toms of inattention. Regarding the resultsachieved with the WURS 38.6% of patients wereabove the cut-off-value, therefore more patientsthan expected (4%) were affected with ADHD.Concerning the results achieved with theCAARS, patients had higher values than expect-ed in four out of six scales, which rather don´trefer to symptoms of inattention and impulsivity.Regarding the results of the BASA, patientsachieved high values in all scales. When allscales were combined, a prevalence-rate of26.6% for ADHD was estimated, which seemseminent higher than the expected rate of 3-5%.Fleming et al. (10) discuss instability of dieteticinterventions in obese patients with ADHD as apotential explanation for the high comorbidity ofobesity and ADHD (cf. (11)).
For the ratio of energy intake and energyexpenditure in the long run predicts the devel-opment of the weight status, it also seemsimportant to investigate energy requirementsin subjects with ADHD. Intuitively one wouldexpect hyperactive subjects to have anincreased energy expenditure in comparison tohealthy subjects acting as a preventive factor inthe development of overweight and/or obesity.Because the basal metabolic rate (BMR, equalsthe energy needed by a physically inactiveorganism) is the greatest part of the daily ener-gy expenditure, effects of physical activity onBMR are of great interest. In their reviewSpeakman and Selman (12) assume that the
R. Hubel, J. Jass, A. Marcus, et al.
140 Eating Weight Disord., Vol. 11: N. 3 - 2006
Overweight and BMR in boys with ADHD
excess post-exercise O2 consumption (EPOC)affects energy expenditure in two phases. Inthe first phase (within two hours after exercise)with significantly heightened energy consump-tion the products of the anaerobe metabolismof exercise are mobilised. The effects of thehypothesized second phase (until two daysafter activity) are relatively small and are pro-duced by the β-adrenergic system.
To our knowledge Butte et al. (13) were theonly ones who investigated energy expenditurein ADHD so far. They examined 31 children (26boys and 5 girls) aged 6-12 years all classified tohave an ADHD [according to the Diagnosticand Statistical Manual (DSM-IV) criteria] fortwo times. At the first measurement the chil-dren had not taken any stimulants for at least 24hours. At the second measurement two monthslater the children again took their prescribedmedication. Energy expenditure was calculatedby room respiration calorimetry. The total ener-gy expenditure and the resting metabolic ratewere significantly lower at the second measure-ment (7523 vs. 7276 kJ/day and 6.3 vs. 5.93kJ/min) while energy expenditure during sleepand BMR did not differ significantly (3.26 vs.3.35 kJ/min and 3.47 vs. 3.6 kJ/min). BecauseButte et al. also applied motion detectors theywere able to show that total and awake activitywere also lower at the second measurement (-16% and -22%) and therefore accounted for thelower rates of energy expenditure. They con-clude that stimulants decrease physical activityand hence lower energy expenditure in childrenwith ADHD. Unfortunately the authors do notdescribe data concerning the subtypes ofADHD of their subjects.
In our study we report data on BMI and BMRin boys with ADHD subtypes predominantlyhyperactive/impulsive (ICD-10 code: F90.1) or
mixed hyperactive/impulsive and inattentive(ICD-10 code: F90.0). The clinical group is com-pared to a control group consisting of healthyboys without any psychiatric diagnosis accord-ing to DSM-IV. We hypothesized both a higherBMI and BMR in ADHD-boys.
METHODS
SubjectsThe sample consists of 69 boys. All subjects
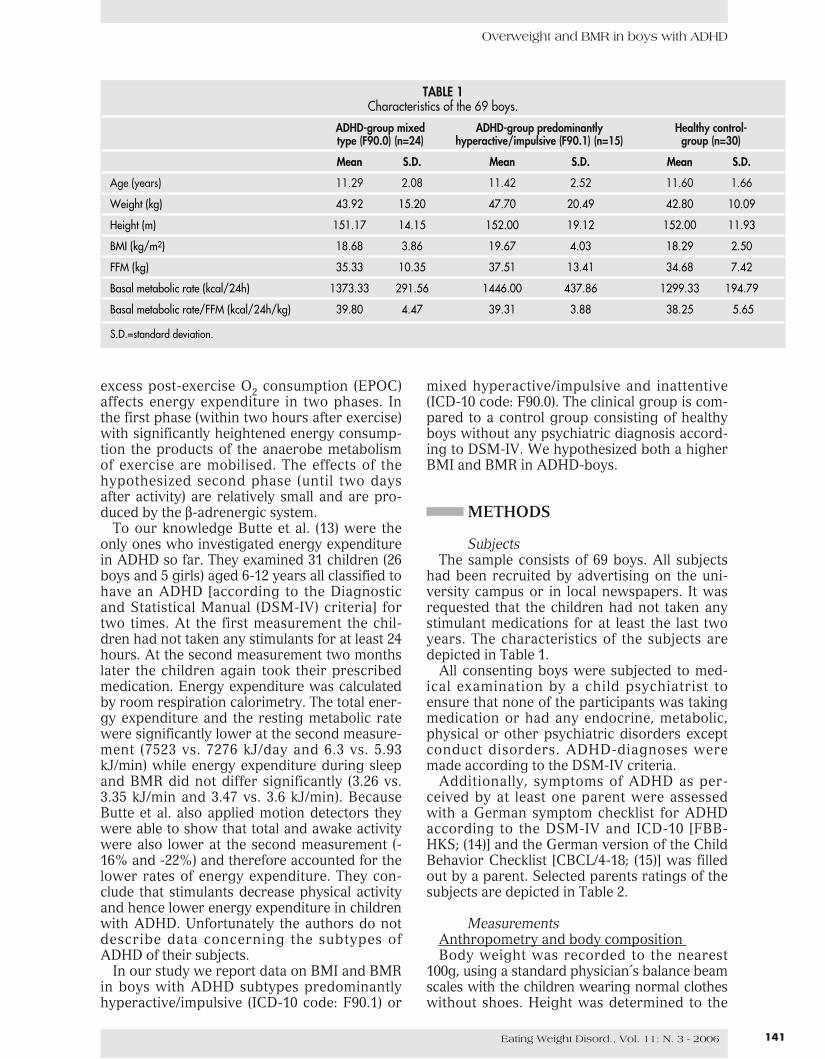
had been recruited by advertising on the uni-versity campus or in local newspapers. It wasrequested that the children had not taken anystimulant medications for at least the last twoyears. The characteristics of the subjects aredepicted in Table 1.
All consenting boys were subjected to med-ical examination by a child psychiatrist toensure that none of the participants was takingmedication or had any endocrine, metabolic,physical or other psychiatric disorders exceptconduct disorders. ADHD-diagnoses weremade according to the DSM-IV criteria.
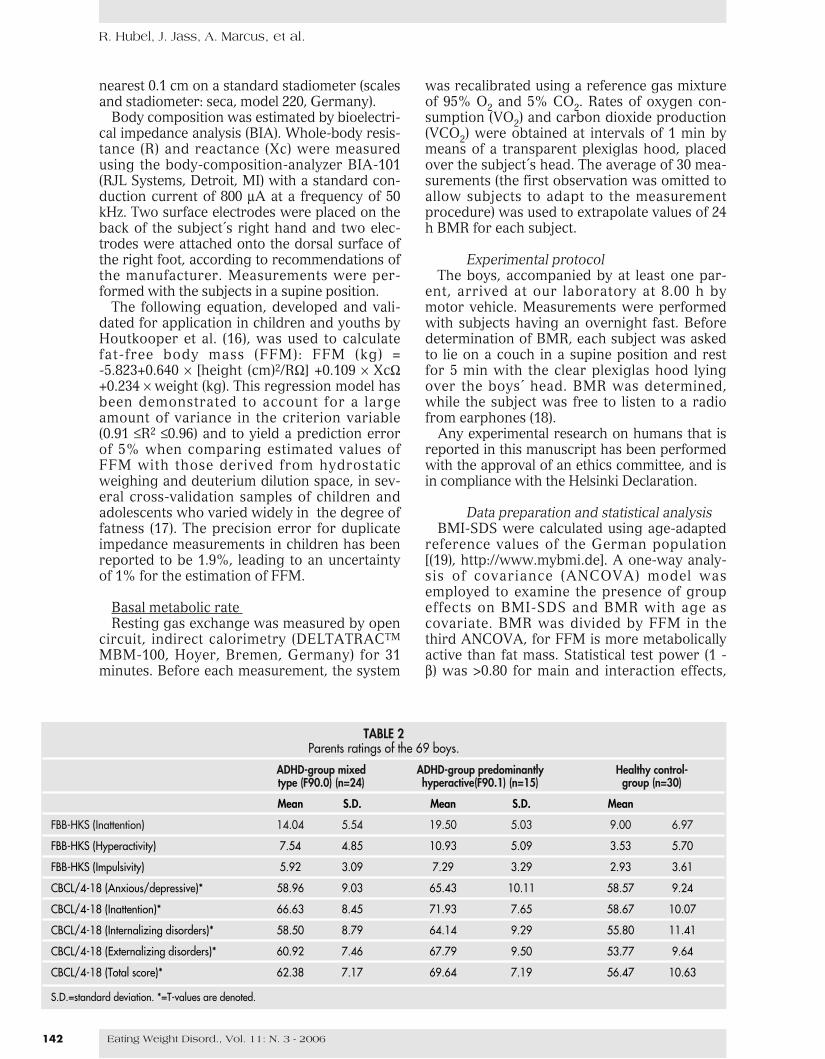
Additionally, symptoms of ADHD as per-ceived by at least one parent were assessedwith a German symptom checklist for ADHDaccording to the DSM-IV and ICD-10 [FBB-HKS; (14)] and the German version of the ChildBehavior Checklist [CBCL/4-18; (15)] was filledout by a parent. Selected parents ratings of thesubjects are depicted in Table 2.
MeasurementsAnthropometry and body composition Body weight was recorded to the nearest
100g, using a standard physician´s balance beamscales with the children wearing normal clotheswithout shoes. Height was determined to the
141Eating Weight Disord., Vol. 11: N. 3 - 2006
TABLE 1Characteristics of the 69 boys.
ADHD-group mixed ADHD-group predominantly Healthy control-type (F90.0) (n=24) hyperactive/impulsive (F90.1) (n=15) group (n=30)
Mean S.D. Mean S.D. Mean S.D.
Age (years) 11.29 2.08 11.42 2.52 11.60 1.66
Weight (kg) 43.92 15.20 47.70 20.49 42.80 10.09
Height (m) 151.17 14.15 152.00 19.12 152.00 11.93
BMI (kg/m2) 18.68 3.86 19.67 4.03 18.29 2.50
FFM (kg) 35.33 10.35 37.51 13.41 34.68 7.42
Basal metabolic rate (kcal/24h) 1373.33 291.56 1446.00 437.86 1299.33 194.79
Basal metabolic rate/FFM (kcal/24h/kg) 39.80 4.47 39.31 3.88 38.25 5.65
S.D.=standard deviation.
nearest 0.1 cm on a standard stadiometer (scalesand stadiometer: seca, model 220, Germany).
Body composition was estimated by bioelectri-cal impedance analysis (BIA). Whole-body resis-tance (R) and reactance (Xc) were measuredusing the body-composition-analyzer BIA-101(RJL Systems, Detroit, MI) with a standard con-duction current of 800 μA at a frequency of 50kHz. Two surface electrodes were placed on theback of the subject´s right hand and two elec-trodes were attached onto the dorsal surface ofthe right foot, according to recommendations ofthe manufacturer. Measurements were per-formed with the subjects in a supine position.
The following equation, developed and vali-dated for application in children and youths byHoutkooper et al. (16), was used to calculatefat-free body mass (FFM): FFM (kg) = -5.823+0.640 × [height (cm)2/RΩ] +0.109 × XcΩ+0.234 × weight (kg). This regression model hasbeen demonstrated to account for a largeamount of variance in the criterion variable(0.91 ≤R2 ≤0.96) and to yield a prediction errorof 5% when comparing estimated values ofFFM with those derived from hydrostaticweighing and deuterium dilution space, in sev-eral cross-validation samples of children andadolescents who varied widely in the degree offatness (17). The precision error for duplicateimpedance measurements in children has beenreported to be 1.9%, leading to an uncertaintyof 1% for the estimation of FFM.
Basal metabolic rate Resting gas exchange was measured by open
circuit, indirect calorimetry (DELTATRACTM
MBM-100, Hoyer, Bremen, Germany) for 31minutes. Before each measurement, the system
was recalibrated using a reference gas mixtureof 95% O2 and 5% CO2. Rates of oxygen con-sumption (VO2) and carbon dioxide production(VCO2) were obtained at intervals of 1 min bymeans of a transparent plexiglas hood, placedover the subject´s head. The average of 30 mea-surements (the first observation was omitted toallow subjects to adapt to the measurementprocedure) was used to extrapolate values of 24h BMR for each subject.
Experimental protocolThe boys, accompanied by at least one par-
ent, arrived at our laboratory at 8.00 h bymotor vehicle. Measurements were performedwith subjects having an overnight fast. Beforedetermination of BMR, each subject was askedto lie on a couch in a supine position and restfor 5 min with the clear plexiglas hood lyingover the boys´ head. BMR was determined,while the subject was free to listen to a radiofrom earphones (18).
Any experimental research on humans that isreported in this manuscript has been performedwith the approval of an ethics committee, and isin compliance with the Helsinki Declaration.
Data preparation and statistical analysisBMI-SDS were calculated using age-adapted
reference values of the German population[(19), http://www.mybmi.de]. A one-way analy-sis of covariance (ANCOVA) model wasemployed to examine the presence of groupeffects on BMI-SDS and BMR with age ascovariate. BMR was divided by FFM in thethird ANCOVA, for FFM is more metabolicallyactive than fat mass. Statistical test power (1 -β) was >0.80 for main and interaction effects,
R. Hubel, J. Jass, A. Marcus, et al.
142 Eating Weight Disord., Vol. 11: N. 3 - 2006
TABLE 2Parents ratings of the 69 boys.
ADHD-group mixed ADHD-group predominantly Healthy control-type (F90.0) (n=24) hyperactive(F90.1) (n=15) group (n=30)
Mean S.D. Mean S.D. Mean
FBB-HKS (Inattention) 14.04 5.54 19.50 5.03 9.00 6.97
FBB-HKS (Hyperactivity) 7.54 4.85 10.93 5.09 3.53 5.70
FBB-HKS (Impulsivity) 5.92 3.09 7.29 3.29 2.93 3.61
CBCL/4-18 (Anxious/depressive)* 58.96 9.03 65.43 10.11 58.57 9.24
CBCL/4-18 (Inattention)* 66.63 8.45 71.93 7.65 58.67 10.07
CBCL/4-18 (Internalizing disorders)* 58.50 8.79 64.14 9.29 55.80 11.41
CBCL/4-18 (Externalizing disorders)* 60.92 7.46 67.79 9.50 53.77 9.64
CBCL/4-18 (Total score)* 62.38 7.17 69.64 7.19 56.47 10.63
S.D.=standard deviation. *=T-values are denoted.
Overweight and BMR in boys with ADHD
given a total N of 69, α=0.05 and assuming amedium effect size (η2=0.06). We used agedependent international cut off points for BMIfor overweight and obesity defined to passthrough BMI of 25 and 30 kg/m2 at age 18 (20).Chi2-tests were used to examine if the propor-tions of normal weight to overweight or obesesubjects were different in the groups with andwithout ADHD. Statistical test power (1 - β )
was >0.98 for an interaction effect, given a totalN of 69, α =0.05 and assuming a large effectsize (w=0.50). A P-value <0.05 was considered asignificant effect. Statistical analyses were per-formed using SPSS Version 12.0.
RESULTS
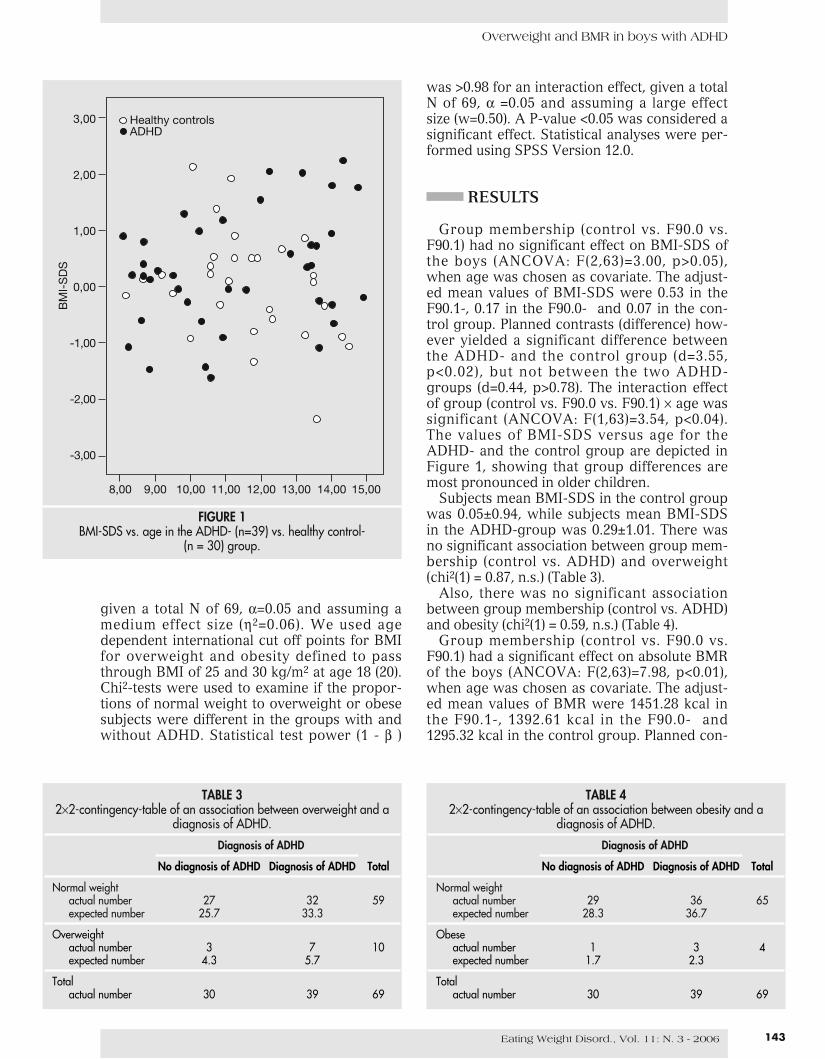
Group membership (control vs. F90.0 vs.F90.1) had no significant effect on BMI-SDS ofthe boys (ANCOVA: F(2,63)=3.00, p>0.05),when age was chosen as covariate. The adjust-ed mean values of BMI-SDS were 0.53 in theF90.1-, 0.17 in the F90.0- and 0.07 in the con-trol group. Planned contrasts (difference) how-ever yielded a significant difference betweenthe ADHD- and the control group (d=3.55,p<0.02), but not between the two ADHD-groups (d=0.44, p>0.78). The interaction effectof group (control vs. F90.0 vs. F90.1) × age wassignificant (ANCOVA: F(1,63)=3.54, p<0.04).The values of BMI-SDS versus age for theADHD- and the control group are depicted inFigure 1, showing that group differences aremost pronounced in older children.
Subjects mean BMI-SDS in the control groupwas 0.05±0.94, while subjects mean BMI-SDSin the ADHD-group was 0.29±1.01. There wasno significant association between group mem-bership (control vs. ADHD) and overweight(chi2(1) = 0.87, n.s.) (Table 3).
Also, there was no significant associationbetween group membership (control vs. ADHD)and obesity (chi2(1) = 0.59, n.s.) (Table 4).
Group membership (control vs. F90.0 vs.F90.1) had a significant effect on absolute BMRof the boys (ANCOVA: F(2,63)=7.98, p<0.01),when age was chosen as covariate. The adjust-ed mean values of BMR were 1451.28 kcal inthe F90.1-, 1392.61 kcal in the F90.0- and1295.32 kcal in the control group. Planned con-
143Eating Weight Disord., Vol. 11: N. 3 - 2006
TABLE 32×2-contingency-table of an association between overweight and a
diagnosis of ADHD.
Diagnosis of ADHD
No diagnosis of ADHD Diagnosis of ADHD Total
Normal weightactual number 27 32 59expected number 25.7 33.3
Overweightactual number 3 7 10expected number 4.3 5.7
Totalactual number 30 39 69
TABLE 42×2-contingency-table of an association between obesity and a
diagnosis of ADHD.
Diagnosis of ADHD
No diagnosis of ADHD Diagnosis of ADHD Total
Normal weightactual number 29 36 65expected number 28.3 36.7
Obeseactual number 1 3 4expected number 1.7 2.3
Totalactual number 30 39 69
3,00
2,00
1,00
0,00
-1,00
-2,00
-3,00
BM
I-S
DS
8,00 9,00 10,00 11,00 12,00 13,00 14,00 15,00
Healthy controlsADHD
FIGURE 1BMI-SDS vs. age in the ADHD- (n=39) vs. healthy control-
(n = 30) group.
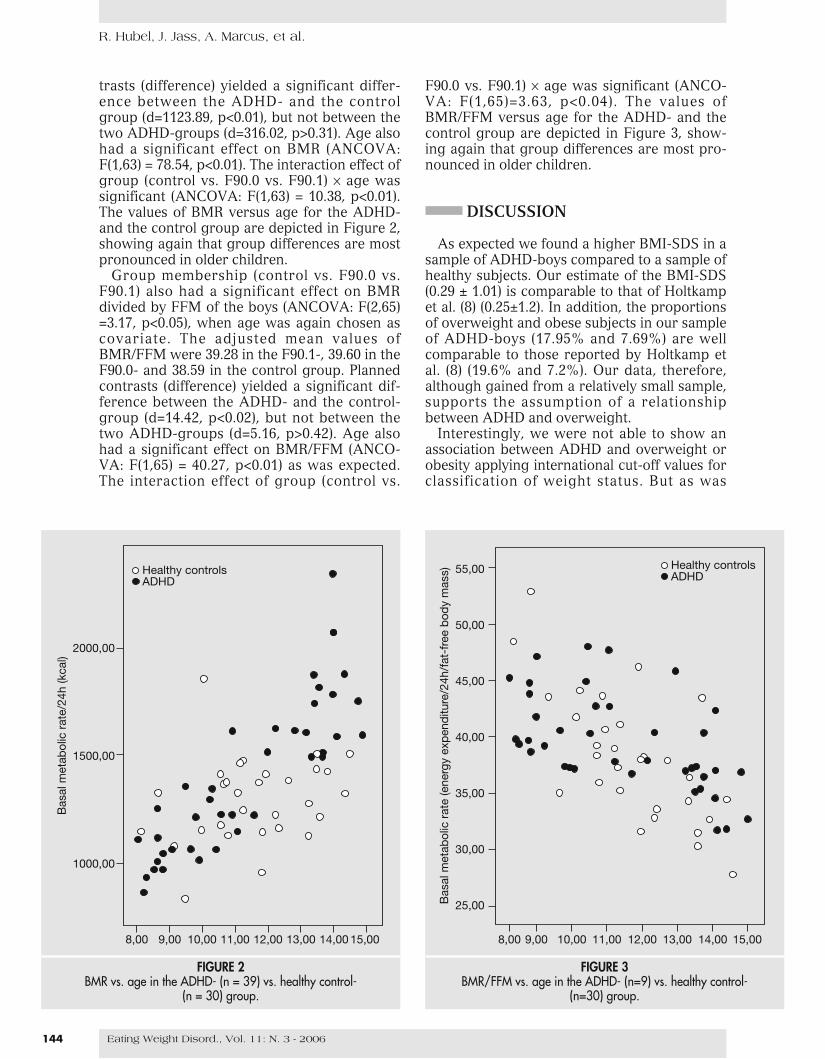
trasts (difference) yielded a significant differ-ence between the ADHD- and the controlgroup (d=1123.89, p<0.01), but not between thetwo ADHD-groups (d=316.02, p>0.31). Age alsohad a significant effect on BMR (ANCOVA:F(1,63) = 78.54, p<0.01). The interaction effect ofgroup (control vs. F90.0 vs. F90.1) × age wassignificant (ANCOVA: F(1,63) = 10.38, p<0.01).The values of BMR versus age for the ADHD-and the control group are depicted in Figure 2,showing again that group differences are mostpronounced in older children.
Group membership (control vs. F90.0 vs.F90.1) also had a significant effect on BMRdivided by FFM of the boys (ANCOVA: F(2,65)=3.17, p<0.05), when age was again chosen ascovariate. The adjusted mean values ofBMR/FFM were 39.28 in the F90.1-, 39.60 in theF90.0- and 38.59 in the control group. Plannedcontrasts (difference) yielded a significant dif-ference between the ADHD- and the control-group (d=14.42, p<0.02), but not between thetwo ADHD-groups (d=5.16, p>0.42). Age alsohad a significant effect on BMR/FFM (ANCO-VA: F(1,65) = 40.27, p<0.01) as was expected.The interaction effect of group (control vs.
F90.0 vs. F90.1) × age was significant (ANCO-VA: F(1,65)=3.63, p<0.04). The values ofBMR/FFM versus age for the ADHD- and thecontrol group are depicted in Figure 3, show-ing again that group differences are most pro-nounced in older children.
DISCUSSION
As expected we found a higher BMI-SDS in asample of ADHD-boys compared to a sample ofhealthy subjects. Our estimate of the BMI-SDS(0.29 ± 1.01) is comparable to that of Holtkampet al. (8) (0.25±1.2). In addition, the proportionsof overweight and obese subjects in our sampleof ADHD-boys (17.95% and 7.69%) are wellcomparable to those reported by Holtkamp etal. (8) (19.6% and 7.2%). Our data, therefore,although gained from a relatively small sample,supports the assumption of a relationshipbetween ADHD and overweight.
Interestingly, we were not able to show anassociation between ADHD and overweight orobesity applying international cut-off values forclassification of weight status. But as was
R. Hubel, J. Jass, A. Marcus, et al.
144 Eating Weight Disord., Vol. 11: N. 3 - 2006
2000,00
1500,00
1000,00
Bas
al m
etab
olic
rat
e/24
h (k
cal)
8,00 9,00 10,00 11,00 12,00 13,00 14,00 15,00
Healthy controlsADHD
FIGURE 2BMR vs. age in the ADHD- (n = 39) vs. healthy control-
(n = 30) group.
55,00
50,00
45,00
40,00
35,00
30,00
25,00Bas
al m
etab
olic
rat
e (e
nerg
y ex
pen
ditu
re/2
4h/f
at-f
ree
bod
y m
ass)
8,00 9,00 10,00 11,00 12,00 13,00 14,00 15,00
Healthy controlsADHD
FIGURE 3BMR/FFM vs. age in the ADHD- (n=9) vs. healthy control-
(n=30) group.

Overweight and BMR in boys with ADHD
shown, differences in weight status between thediagnostic groups are more pronounced in ado-lescence (Fig. 1). Because age effects weren´taccounted for in the chi2-analyses, they mayhave acted as error variance which covered anactually existing association between groupmembership and weight status in this analysis.
Furthermore, we did not find a possible asso-ciation between inattention (in the context ofADHD) rated by a psychiatrist and obesity asAgranat-Meged et al. (9) and Fleming et al. (10)suggested. But as should be kept in mind, on adescriptive level parents´ ratings of inattentionwere even higher in the children classified hav-ing ADHD predominantly hyperactive/impul-sive compared to the children classified havingADHD of mixed type (Table 2). Therefore inter-preting our results cautiously, it rather seemsthat hyperactivity/impulsivity, ADHD or maybea psychic dysfunction per se makes childrenmore prone to overweight and obesity becausethere was no difference in SDS-BMI betweenthe two ADHD-subgroups (F90.0 and F90.1).Anxiety/depression, internalizing and external-izing problems as well as general psychicimpairment (all rated by parents) were correlat-ed with subgroup membership (Table 2) andtherefore these variables also could explain forthe differences in BMI-SDS between the sub-groups. However, results of further analyses(i.e. ANCOVA with multiple covariates) suggestthat the results on BMI-SDS remain valid evenwhen the confounded variables mentionedabove are controlled for.
The mean BMR (in absolute values andadjusted for FFM) in our sample of ADHD-boyswas higher than in the control group and asone might have expected there wasn´t a differ-ence in BMR between the ADHD-subgroups.These data can´t be explained solely by a higherFFM in the ADHD-groups and therefore are inline with a post-exercise effect on BMR inADHD-children with hyperactivity, but are notconsistent with the results of Butte et al. (13)who didn´t find any differences in BMR.However, our control group design seems tobe more valid than the study of Butte et al. (13),because they only compared children withoutmedication (that means hyperactivity was pre-sent) and children under medication (thatmeans hyperactivity was not present).
The interpretation of our results should bemade considering other methodological con-straints. We did not measure objectively thephysical activity in the clinical and in the con-trol group. So we were not able to correlate theactual activity with BMR. Furthermore it isunclear whether the elevated BMR in hyperac-tive boys may result from an increased physical
activity in the morning before the calorimetricmeasurement. Careful observation during mea-surement, however, rules out the possibilitythat hyperactive boys had more movements onthe couch. Furthermore pulse rate indicatingan increased activity of the sympathetic ner-vous system which could have produced ahigher energy expenditure in the hyperactiveboys didn´t differ between the two groupsbefore calorimetry. At last it should be kept inmind that our sample is rather small and there-fore estimates of parameters may be biased.
At first glance, a high BMI and a high BMRin our sample seems to be incompatible. Theincreased BMR in hyperactive children is likelyto be explained by a post-exercise effect. Thehigher weight status of ADHD-children withhyperactivity could be the result of their impul-sive behavior making them more prone to eatmore food than healthy children which resultsin an increased energy intake and a positiveenergy balance which in the long run leads toweight gain (8, 11, 21). With increasing age thisbehavior might be further promoted because oflesser constraints and control by parents (22).
Future studies should focus on the eatingbehavior of ADHD-children and investigatewhether impulsivity can be detected in singlemeals or whether children with ADHD consumemore calories per day than healthy children.Furthermore, long-term studies are needed totest how the investigated behaviors changeover the span of life in subjects with ADHD.
ACKNOWLEDGEMENTS
This study was supported by a grant from theGerman Research Foundation (DeutscheForschungsgemeinschaft, DFG) (La 681/9-1).
REFERENCES
1. American Psychiatric Association. Diagnostic and sta-tistical manual of mental disorders, 4th ed. WashingtonD.C., American Psychiatric Association, 1994.
2. Anderson J.C., Williams S., McGee R., Silva P.A.:DSM-III disorders in preadolescent children.Prevalence in a large sample from the general popula-tion. Arch. Gen. Psychiatry, 44, 69-76, 1987.
3. Döpfner M.: Hyperkinetische Störungen. In:Petermann F. (Ed.), Lehrbuch der KlinischenKinderpsychologie und -psychotherapie. Göttingen,Hogrefe, 2000, pp. 151-187.
4. Barkley R.A.: Behavioral inhibition, sustained atten-tion, and executive functions: constructing a unifyingtheory of ADHD. Psychol. Bull., 121, 65-94, 1997.
5. Wang G.J., Volkow N.D., Logan J., Pappas N.R., WongC.T., Zhu W., Netusil N., Fowler J.S.: Brain dopamineand obesity. Lancet, 357, 354-357, 2001.
145Eating Weight Disord., Vol. 11: N. 3 - 2006

6. Levitan R.D., Masellis M., Lam R.W., Muglia P., BasileV.S., Jain U., Kaplan A.S., Tharmalingam S., KennedyS.H., Kennedy J.L.: Childhood inattention and dys-phoria and adult obesity associated with thedopamine D4 receptor gene in overeating womenwith seasonal affective disorder. Neuropsych-opharmacology, 29, 179-186, 2004.
7. Wareham N.J., van Sluijs E.M., Ekelund U.: Physicalactivity and obesity prevention: a review of the cur-rent evidence. Proc. Nutr. Soc., 64, 229-247, 2005.
8. Holtkamp K., Konrad K., Müller B., Heussen N.,Herpertz S., Herpertz-Dahlmann B., Hebebrand J.:Overweight and obesity in children with attention-deficit/hyperactivity disorder. Int. J. Obes. Relat.Metab. Disord., 28, 685-689, 2004.
9. Agranat-Meged A.N., Deitcher C., Goldzweig G.,Leibenson L., Stein M., Galili-Weisstub E.: Childhoodobesity and attention deficit/hyperactivity disorder: anewly described comorbidity in obese hospitalizedchildren. Int. J. Eat. Disord., 37, 357-359, 2005.
10. Fleming J., Levy L., Levitan R.D.: Symptoms of atten-tion deficit hyperactivity disorder in severely obeseadults. Eat. Weight Disord., 10, e10-e13, 2005.
11. Altfas J.R.: Prevalence of attention deficit/hyperactivi-ty disorder among adults in obesity treatment. BMCPsychiatry, 2, 9, 2002.
12. Speakman J.R., Selman C.: Physical activity and rest-ing metabolic rate. Proc. Nutr. Soc., 62, 621-634, 2003.
13. Butte N.F., Treuth M.S., Voigt R.G., Llorente A.M.,Heird W.C.: Stimulant medications decrease energyexpenditure and physical activity in children withattention-deficit/hyperactivity disorder. J. Pediatr.,135, 203-207, 1999.
14. Döpfner M., Lehmkuhl, G.: DISYPS-KJ. Diagnostik-System für psychische Störungen im Kindes- undJugendalter nach ICD-10 und DSM-IV. Bern, Huber,1998.
15. Arbeitsgruppe Deutsche Child Behavior Checklist:CBCL/4-18. Elternfragebogen über das Verhalten vonKindern und Jugendlichen. Köln, ArbeitsgruppeKinder-, Jugend- und Familiendiagnostik (KJFD),1998.
16. Houtkooper L.B., Lohman T.G., Going S.B., Hall M.C.:Validity of bioelectric impedance for body composi-tion assessment in children. J. Appl. Physiol., 66, 814-821, 1989.
17. Houtkooper L.B., Going S.B., Lohman T.G., RocheA.F., Van Loan M.: Bioelectrical impedance estima-tion of fat-free body mass in children and youth: across-validation study. J. Appl. Physiol., 72, 366-373,1992.
18. Feurer I.D., Mullen J.L.: Measurement of energyexpenditure. In: Rombeau J.L. (Ed.), Parenteral nutri-tion. Philadelphia, Saunders, 1986, pp. 224-236.
19. Kromeyer-Hauschild K., Wabitsch M., Geller F.,Ziegler A., Geiß H.C., Hesse V., Hippel V., Jaeger U.,Johnsen D., Kiess W., Korte W., Kunze D., Menner K.,Müller M., Niemann-Pilatus A., Remer T., Schaefer F.,Wittchen H.U., Zabransky S., Zellner K., HebebrandJ.: Perzentile für den Body Mass Index für dasKindes- und Jugendalter unter Heranziehung ver-schiedener deutscher Stichproben. Monatsschr.Kinderheilkd., 149, 807-818, 2001.
20. Cole T.J., Bellizzi, M.C., Flegal K.M., Dietz W.H.:Establishing a standard definition for child over-weight and obesity worldwide: international survey.BMJ, 320, 1240-1243, 2000.
21. Pine D.S., Cohen P., Brook J., Coplan J.D.: Psychiatricsymptoms in adolescence as predictors of obesity inearly adulthood: a longitudinal study. Am. J. PublicHealth, 87, 1303-1310, 1997.
22. Cusinato M.: Parenting over the family life cycle. In:L´Abate L. (Ed.), Handbook of family psychology andpsychopathology. New York, Wiley, 1994, pp. 83-115.
R. Hubel, J. Jass, A. Marcus, et al.
146 Eating Weight Disord., Vol. 11: N. 3 - 2006





























