Embed Size (px)
Citation preview
known to occur in several epithelial fragility syn-dromes.6 K-based diagnostic tools have been ofincreased interest, and may provide a better un-derstanding of some dermatologic syndromes.
Gisele Viana de Oliveira, MD, MsC a,d
Hal K. Hawkins, MD, PhDb
Antonio Carlos Martins Guedes, MD, PhDc
Luis Felipe Pinto, MDd
Gloria Oliveras, MsCe
Gregory T. Kitten, PhDd
Ramon Sanchez, MD, PhDa
Departments of Dermatologya and Pathologyb
University of Texas Medical BranchGalveston, Texas
Departments of Dermatologycand Morphologyd
Federal University of Minas GeraisBelo Horizonte, Brazil
Shriners Hospital for Childrene
Galveston, Texas
Correspondence to: Ramon Sanchez, MD, PhDDepartment of Dermatology
University of Texas Medical Branch301 University Blvd
Galveston, TX 77555
E-mail: [email protected]
This study was developed in the University of TexasMedical BranchGalveston, Texas
REFERENCES
1. Muller FB, Hausser I, Berg D, Casper C, Maiwald R, Jung A, et al.
Genetic analysis of a severe case of Netherton syndrome and
application for prenatal testing. Br J Dermatol 2002;146:495-9.
2. Comel M. Ichthyosis linearis circumflexa. Dermatologica 1949;
19:133-6.
3. Fartasch M, Williams ML, Elias PM. Altered lamellar body
secretion and stratum corneum membrane structure in Nether-
ton syndrome differentiation from other infantile erythroder-
mas and pathogenic complications. Arch Dermatol 1999;135:
823-32.
4. Freedberg IM, Tomic-Canic M, Komine M, Blumenberg M.
Keratins and the keratinocyte activation cycle. J Invest Dermatol
2001;16:633-40.
5. Algermissen B, Sitzmann J, LeMotte P, Czarnetzki B. Differential
expression of CRABP II, psoriasin and cytokeratin 1 mRNA in
human skin diseases. Arch Dermatol Res 1996;288:426-30.
6. Corden LD, McLean WH. Human keratin diseases: hereditary
fragility of specific epithelial tissues. Exp Dermatol 1996;5:
297-307.
doi:10.1016/j.jaad.2004.11.033
Fig 1. The 903 cocktail of keratins (K1, K5, K10, and K14;dilution 1:100; Enzo, New York, NY) showed positivestaining on the full-thickness skin of patients with Nether-ton’s syndrome, including the corneal layer (A). The 903cocktail displayed negative staining in most of the corneallayer in the skin of patients with psoriasis (B). (Originalmagnification: 3200.)
Fig 2. Immunohistochemical findings for Netherton’ssyndrome and comparison with psoriasis. Stainings forNetherton’s syndrome are displayed in the left column andpsoriasis in the right column. A, K 5/6 (dilution 1:100;Dako, Carpinteria, Calif) was positive in all layers ofNetherton skin. B, K 5/6 was positive in all layers ofpsoriasis. C, K16 staining (dilution 1:40; Novocastra,Newcastle, UK) was positive in upper layers of Netherton.D, K16 showed a similar staining in psoriasis. (Originalmagnifications: 3200.)
J AM ACAD DERMATOL
APRIL 2005
726 Letters
Painful subungal dyskeratotic tumors inincontinentia pigmenti
To the Editor: Familial incontinentia pigmenti (IP) isan X-linked dominant disorder characterized byabnormal skin pigmentation, retinal detachment,dental anomalies, alopecia, nail dystrophy, andcentral nervous system defects.1 The disorder islethal prenatally in males and variably expressed inaffected females. Cells expressing the mutated Xchromosome are eliminated selectively at birth.Hence, females with IP exhibit extremely skewedX-inactivation.1 Most cases of IP are caused bymutations in the nuclear factor kappa B (NF-kB)essential modulator (NEMO) gene, which encodes
J AM ACAD DERMATOL
VOLUME 52, NUMBER 4
Letters 727
a regulatory component of the IkB kinase complexrequired to activate NF-kB.1 NF-kB protects againstTNF-aeinduced apoptosis and is defective in IPcells. Thus, IP can be viewed as a pro-apoptotic state,giving rise to male lethality and cell destruction infemales. This may account for the marked dysker-atosis seen in cutaneous lesions of the verrucousstage of IP, as well as subungal tumors of IP (STIPs).Painful subungal dyskeratotic tumors have beenreported in patients with IP, and they have beenrecognized as a late manifestation of the disorder.2,3,4
CASE REPORTA 65-year-old woman with a history of IP de-
veloped painful subungal nodules on the rightthumb and ring finger over the course of 2 months.She was diagnosed with IP during infancy when shedeveloped a linear vesiculobullous eruption on herlegs. Crusts and eventually hyperpigmented lesionsresolved leaving subtle linear hypopigmentedpatches in the same distribution (Fig 1). She com-plained of multiple subungal lesions for 40 years.These lesions grew quickly and were associated withincreasing pain relieved only by surgical destruction.Although the nodules were initially thought torepresent warts, a biopsy of one lesion was inter-preted as squamous cell carcinoma (SCC) with sub-sequent partial amputation of the right index finger.Spontaneous regression of the lesions did not occur,but no new lesions occurred during her followingpregnancies and existing lesions remained stable.
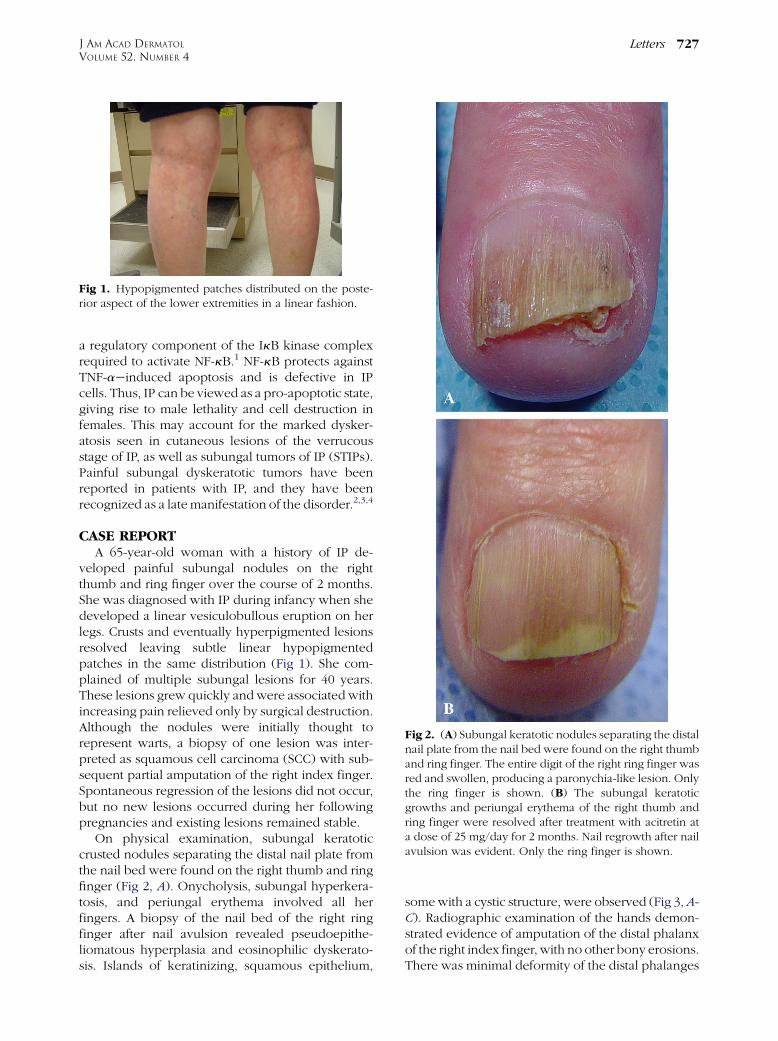
On physical examination, subungal keratoticcrusted nodules separating the distal nail plate fromthe nail bed were found on the right thumb and ringfinger (Fig 2, A). Onycholysis, subungal hyperkera-tosis, and periungal erythema involved all herfingers. A biopsy of the nail bed of the right ringfinger after nail avulsion revealed pseudoepithe-liomatous hyperplasia and eosinophilic dyskerato-sis. Islands of keratinizing, squamous epithelium,
Fig 1. Hypopigmented patches distributed on the poste-rior aspect of the lower extremities in a linear fashion.
somewith a cystic structure, were observed (Fig 3,A-C). Radiographic examination of the hands demon-strated evidence of amputation of the distal phalanxof the right index finger, with no other bony erosions.There was minimal deformity of the distal phalanges
Fig 2. (A) Subungal keratotic nodules separating the distalnail plate from the nail bed were found on the right thumband ring finger. The entire digit of the right ring finger wasred and swollen, producing a paronychia-like lesion. Onlythe ring finger is shown. (B) The subungal keratoticgrowths and periungal erythema of the right thumb andring finger were resolved after treatment with acitretin ata dose of 25 mg/day for 2 months. Nail regrowth after nailavulsion was evident. Only the ring finger is shown.

J AM ACAD DERMATOL
APRIL 2005
728 Letters
of the right thumb and ring finger. The patient wastreated with acitretin at a daily dose of 25 mg for 2months, and her symptoms resolved (Fig 2, B).
DISCUSSIONPainful subungal dyskeratotic tumors are one of
the late manifestations of IP,2-4 appearing afterpuberty (between the ages of 15 and 31). STIPs aremore frequent on the fingers than on the toes. Theytend to destroy the distal phalanx by pressurenecrosis of the underlying bone, and they displacethe nail from the nail bed, causing nail dystrophy.Partial onycholysis often precedes the appearance of
Fig 3. Histologic examination with hematoxylin and eosinstaining of the nail bed of the right ring finger revealedpseudoepitheliomatous hyperplasia and marked dysker-atosis at magnifications of 320 (A), 340 (B), and 380(C). Islands of keratinizing, squamous epithelium, somewith a cystic structure, were observed. The dyskeratoticcells have a distinctive eosinophilic cytoplasm.
keratotic crusted papules and nodules at the distalnail bed. Pain is initially intermittent, but increasesin intensity and duration as the tumor enlarges. Inthe proximal subungal tissue, the tumors may pro-duce a paronychia-like lesion. Drainage of firmkeratinaceous plugs or purulent debris secondaryto bacterial infection may be present.
Clinically, STIPs resemble verruca vulgaris, epi-dermoid cysts, subungal keratoacanthomas (KAs),SCCs, subungal fibromas,5 and chronic paronychia.6
Microscopic features include pseudoepithelioma-tous hyperplasia, eosinophilic dyskeratosis, andcystic squamoid islands. Histologically, they havebeen misdiagnosed as subungal KAs and SCCs.4
However, crater-like lesions seen in KA, or atypicalkeratinocytes in SCC, are not identified. The radio-graphic appearance of STIPs is similar to that ofsubungal KAs, and consists of lytic bone destructionin the distal phalanx with well-circumscribed, cres-cent-shaped radiologic defects, without accompany-ing sclerosis or periosteal reaction.4
STIPs are erroneously considered by some authorsto be subungal KAs, characterized by rapid growthand spontaneous resolution.4 Although spontaneousregression of STIPs is possible, the most commonform of evolution is the painful progression oftumors.7 The remission of tumors during pregnancyfollowed by eruption of new lesions after pregnancysuggests a hormonal influence.7 The distinguishingfeatures of STIPs from subungal KAs are theiroccurrence in young women with multiple lesionsover a course of several years and accompanyingsigns of IP. Subungal KAs are more frequent in malepatients aged over 40 (80% of reported cases) andthey present more often as single lesions.8 The rapidgrowth of these tumors within a period of weeksdifferentiates them from SCCs. Unlike SCCs, the bonyerosions are likely the result of a pressure phenom-enon, rather than true invasion of underlying tissueand bone.
The initial treatment of STIP is surgical excisionwith bone curettage. Although no recurrence hasbeen reported in STIP after surgical therapy, multiplenew lesions appear in other locations, requiringrepeated surgeries. Mohs micrographic surgery todetermine the adequacy of surgical margins mayreduce the risk of persistent or recurrent tumors andallow preservation of the involved fingertip. Somesuccess has been achieved with intralesional 5-fluorouracil injection.9 Malvehy et al7 reported thattreatment of STIP with etretinate caused rapid re-solution of the tumor without recurrence during thefollowing 37 months.
All-trans-retinoic acid (ATRA) has been shown toinduce the activation of NF-kB and apoptosis in

Necrobiotic xanthogranuloma: Isolatedskeletal muscle involvement and unusualchanges
To the Editor: Necrobiotic xanthogranuloma (NXG)is a rare granulomatous disease often accompaniedwith paraproteinemia. It presents as a red-orangeindurated papule or plaque and has a predilectionfor the periorbital area.1 We present an unusual caseof NXG with isolated skeletal muscle involvement,and show some interesting changes in a patient’scutaneous NXG lesion over a 7-year course.
A 69-year-old Japanese woman presented with anorange erythematous plaque with central atrophy onthe lower leg (Fig 1, a) and violaceous red noduleson her trunk (Fig 1, e) that had appeared gradually in1997. She has suffered from IgG kappa type mono-clonal gammopathy with leukopenia since 1985. Thebiopsy specimen showed a granulomatous lesionconsisting of lymphocytes, histiocytes, and manyirregular-shaped giant cells (Fig 1, i and h) withnecrobiosis in the dermis. The plaque on the lowerleg gradually enlarged (Fig 1, b) and then regressed(Fig 1, c). The orange erythematous plaque almostresolved and changed to a subcutaneous tumor in2004 (Fig 1, d). Subsequently, she developed multi-ple subcutaneous nodules without overlying skin
J AM ACAD DERMATOL
VOLUME 52, NUMBER 4
Letters 729
various cancer cell lines.10-12 ATRA stimulates malig-nant neuroblastoma cell behavior by inducing NF-kBtranscription factor (TF) activity10 and acts synergis-tically with TNF in inducing NF-kB target genes inacute leukemia cells.12 NF-kB TFs are comprised ofheterodimers between members of the rel familyincluding RelA, RelB, p50, and p65 protein.10 NF-kBactivity is determined by de novo componentsynthesis, nuclear p50 translocation (which is in turnregulated by IkB as it retains p50/p65 heterodimerswithin the cytoplasm), and redox conditions in thenucleus.10 As ATRA regulates the synthesis of NF-kBTF components, including p50 and p65,10 it is likelythat acitretin, a synthetic analog of retinoic-acid-receptor (RAR)eselective retinoids, prevents theformation of STIPs by inducing the activation ofNF-kB via an IkB- and NEMO-independent mecha-nism.
We report a patient with STIP who responded toacitretin, with resolution of the tumor and associatedsymptoms within 2 months. Even though spontane-ous resolution may have been possible, this wasconsidered unlikely, because her subungal tumorshad progressed over the course of several months,and none of her tumors had resolved withouttreatment over the last 40 years. Although the useof systemic retinoids has not been compared withsurgery in the management of this rare disorder, wepropose that RAR-selective retinoids could be usefulin the management of STIP.
Alison Young, MD, PhDPamela Manolson, MD
Benard Cohen, MDMitchell Klapper, MD
Terry Barrett, MDDepartment of Dermatology
The Johns Hopkins Medical InstitutionsBaltimore, Maryland
Correspondence to: Terry Barrett, MDDepartment of Dermatology
The Johns Hopkins Medical Institutions601 N. Caroline Street, 6th Floor
Baltimore, MD 21287
REFERENCES
1. International IP Consortium. Genomic rearrangement in NEMO
impairs NF-kB activation and is a cause of incontinentia
pigmenti. Nature 2000;405:466-72.
2. Hartman DL. Incontinentia pigmenti associated with subungal
tumors. Arch Dermatol 1966;94:632-5.
3. Mascaro JM, Palou J, Vives P. Painful subungal keratotic
tumors in incontinentia pigmenti. J Am Acad Dermatol 1985;
13:913-8.
4. Baran R, Goettmann S. Distal digital keratoacanthoma: a report
of 12 cases and a review of the literature. Br J Dermatol 1998;
139:512-5.
5. Simmons DA, Kegel MF, Scher RK, Hines YC. Subungal tumors
in incontinentia pigmenti. Arch Dermatol 1986;122:1431-4.
6. Adeniran A, Townsend PL, Peachey RD. Incontinentia pig-
menti (Bloch-Sulzberger syndrome) manifesting as painful
periungal and subungal tumors. J Hand Surg (Br) 1993;18:
667-9.
7. Malvehy J, Palou J, Mascaro JM. Painful subungal tumor in
incontinentia pigmenti. Response to treatment with etreti-
nate. Br J Dermatol 1998;138:554-5.
8. Patel MR, Desai S. Subungal keratoacanthoma in the hand.
J Hand Surg (Am) 1989;14:139-42.
9. Rogers M. Nail manifestations of some important genetic
disorders in children. Dermatol Ther 2002;15:111-20.
10. Farina AR, Masciulli M-P, Tacconelli A, Cappablanca L, De
Santis G, Gulino A, et al. All-trans-retinoic acid induces nuclear
factor kappaB activation and matrix metalloproteinase-9
expression and enhances basement membrane invasivity of
differentiation-resistant human SK-N-BE 9N neuroblastoma
cells. Cell Growth & Differentiation 2002;13:343-54.
11. Manna SK, Aggarwal BB. All-trans-retinoic acid upregulates
TNF receptors and potentiates TNF-induced activation of
nuclear factors-kappaB, activated protein-1 and apoptosis in
human lung cancer cells. Oncogene 2000;19:2110-9.
12. Witcher M, Ross DT, Rousseau C, Deluca L, Miller WH Jr.
Synergy between all-trans-retinoic acid and tumor necrosis
factor pathways in acute leukemia cells. Blood 2003;102:
237-45.
doi:10.1016/j.jaad.2004.11.056














![First IKBKG Gene Mutation Study in Serbian Incontinentia ... · Incontinentia pigmenti (IP; Bloch-Sulzberg-er syndrome; MIM 308300) is a rare X-linked dominant genodermatosis [5]](https://img.pdfslide.net/doc/110x75/5f3bedf5651a4c1377610355/first-ikbkg-gene-mutation-study-in-serbian-incontinentia-incontinentia-pigmenti.jpg)














