Embed Size (px)
Citation preview
Panacea’s Glass: Mobile Cloud Framework forCommunication in Mass Casualty Disaster Triage
John Gillis, Prasad Calyam, Ashley Bartels, Mihai Popescu, Stephen Barnes,Jennifer Doty, Dena Higbee, Salman Ahmad
University of Missouri-Columbia, USA{gillisj, calyamp}@missouri.edu; {bartelsan, popescum, barnesste, dotyj, higbeed, ahmadsa}@health.missouri.edu
Abstract—When working with critical-care patients, doctorsand nurses need a hands-free way to stay updated on the currentstatus of incoming patients and their needed-care levels. Thisneed to stay updated on new patients is even more critical in anatural disaster scenario where a large volume of patients withvarying states of injuries need to be treated by a limited medicalstaff. Using Google Glass, we can open up new possibilitiesfor mobile healthcare communication allowing for cloud-basedcoordination with other medical personnel even in a disasterscenario. In this paper, we present our ‘Panacea Glass’, a mobilecloud framework that allows triage personnel who require hands-free communication capabilities along with situational-awarenessof patient care coverage. We implement this framework within aWebRTC-based ‘Responder Theater Application’ with featuressuch as video chat application on Google Glass devices, and useof virtual beacon tracking devices. Lastly, we show experimentsconducted in determining optimal settings of the application, aswell as its utility within an actual ‘Lake Simulation’.
Index Terms—hands-free video chat, mobile cloud for healthcare, mobile network-as-a-service, smart triage
I. INTRODUCTION
Disaster occurrence is a series of unexpected events in asystem. These events could result from natural or human-made calamities that cause destruction to the environmentand surrounding life forms. Various types of disasters includenatural type such as floods, volcanos, Tsunamis, and man-made disasters such as the 9/11 terrorist attacks in New York,USA. Disasters could very likely lead to destruction of anumber of critical resources such as network connectivity,and infrastructures such as residential buildings, which conse-quently leaves disaster relief operations with limited amountof resources. One of the major goals during a disaster recov-ery response should be to provide proper medical treatment(in addition to other responses relating to food, temporaryshelter) to those affected by this disaster. According to 2014IBISWorld Report [1], medical responders are a major portionof the ‘disaster and emergency relief services’ market thatcovers over 3700 businesses (includes Mass Casualty Trainingorganizations and hospitals).
In the adversity of disaster related events, it becomes im-portant to properly handle the limited amount of networking/-physical/human resources available in order to provide as-best-possible treatment of critically injured patients affected by thedisaster. When working with critical-care patients, doctors andnurses in the disaster relief operations team need both audioand video communication to collaborate with other doctors
and update each other on the status of incoming critical-carepatients. The speed with which the doctor treats the patientand the number of suggestions he/she takes from counterpartdoctors also greatly affects the chances of a patient’s life incritical-care conditions. Today, traditional video based applica-tions requires the doctor/nurse to hold the video camera device,which restricts the doctor/nurse to use only one hand whiletreating the patient. The need of a hands-free communicationsystem in a disaster scenario to treat the incoming patients isthus clearly evident and can free the doctor/nurse from theburden of worrying about manual handling of video devicesduring treatment of critical patients or collaboration with othercolleagues at the disaster scene.
Especially in a disaster scenario with a mass-casualty inci-dent, the ability of medical professionals to properly managepatients and communicate is highly degraded. Doctors andnurses are deeply engaged with individual patients makingboth themselves and incident commanders unaware of theirstatus and how it impacts the entire disaster relief facility’sstatus. Further, emergency response in disaster scenarios re-quires all first responder groups such as Fire, Police, EMS andhealth services to co-ordinate closely rather than act as isolatedunits [2]. A lack of pertinent communication and situationalawareness can cause many problems in a particularly fastpaced mass-casualty event such as the mis-triage of patients orduplication of efforts which waste precious time and resources.They also limit the ability of a medical director or incidentcommander to sense the scene status events and strategicallydelegate triage responsibility to the first responders, directingthem remotely using audiovisual communication. In addi-tion to the hands-free communication system, integration ofsensing technologies that automatically update the situationalawareness of the various clinical processes amongst the fieldteam such as [3] is highly desirable and can further improvethe care co-ordination on the disaster scene.
The challenges of a mass-casualty incident are amplifiedwhen typical support structure for managing medical care maybe partially or completely unavailable. Current communicationsystems that are typically used by medical professionals re-quire an already established infrastructure in a typical hospitalenvironment. This is a valid solution for carefully planningahead and designing a highly customized setup; however,when a disaster occurs causing the hospital’s customizedinfrastructure to be compromised or a medical theater has to
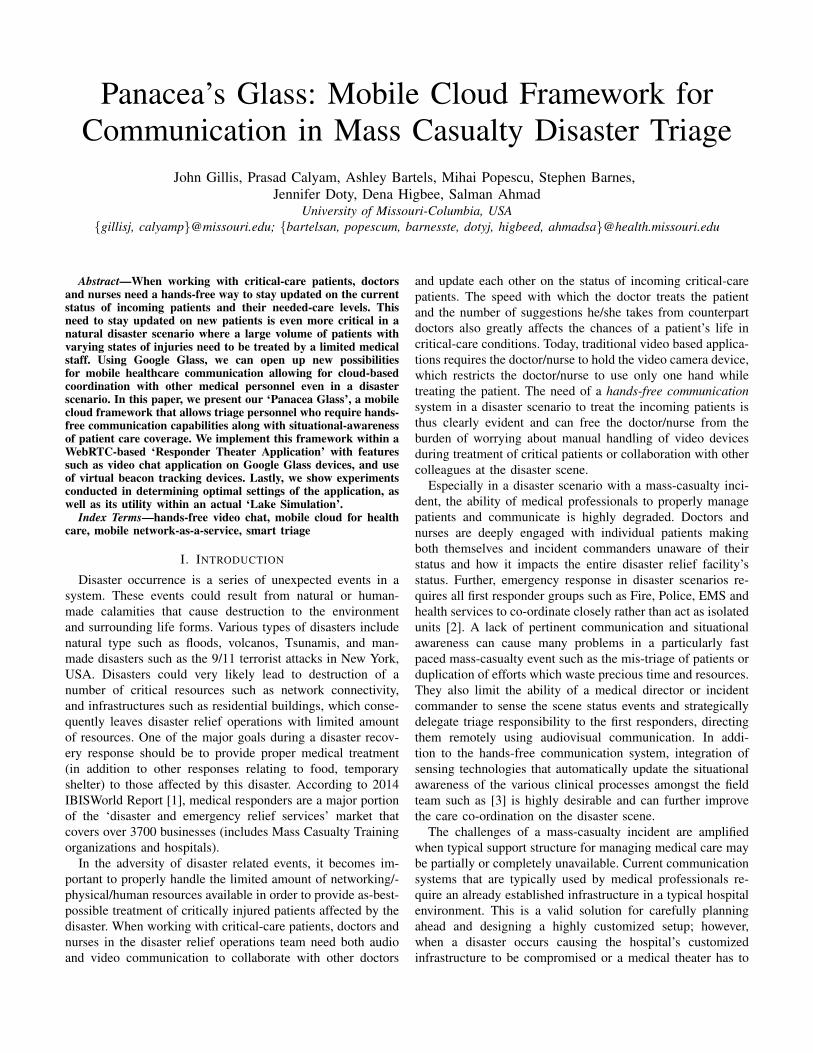
be setup closer to the injured patients in the field, currentcommunication systems can not be used. Having a easilydeployable hands-free communication solution that is self-contained and infrastructure-independent is crucial to beingable to serve the relief needs in any disaster scenario [4].Particularly, solutions such as a wireless mesh network aresuitable to address such concerns and can make the systemdeployable regardless of the location. Moreover, the networkshould be reliable, portable, quickly deployable, and low-cost in order address any disaster situation’s needs. However,the system should be able to leverage any existing parallelinfrastructure available such as an ambulance or pre-existinghospital network as shown in Figure 1. In such a context, theintegration of setting up a private cloud to interface with themobile hands-free communication system can allow for largercomputation and data handling to further help with the disasterrelief services.
Fig. 1: Quick-deploy mesh network can be combined with paral-lel infrastructures, such as an ambulance and pre-existing hospitalnetwork, to extend the hands-free communication system’s reach
To address the above needs of infrastructure and co-ordination challenges, in this paper, we propose the ‘Panacea’sGlass’1 mobile cloud framework for hands-free communica-tion in mass casualty disaster triage scenarios. Panacea Glasscomprises of a secure, reliable, adhoc network consisting ofmeshed access points placed to extend its range in a mass casu-alty disaster environment. A low-power computer, RaspberryPi appliance is used to control the network at each access pointand ensure communication between all points, even if oneof the points experiences failures. The recently commerciallyavailable, hands-free communication device, Google Glass isused in the transmission of an audio and video stream usingWebRTC-based ‘Responder Theater Application’ with featuressuch as video chat over the network and support for virtualbeacon tracking devices, without any necessity to connect tothe Internet.
We study various aspects of our Panacea solution andpresent results. In one aspect, we present results from ourstudy on how having a quick setup infrastructure-independent
1Panacea in English means a solution or remedy for all difficulties ordiseases, but comes from the Greek goddess of universal remedy namedPanacea. This project could be equated to a piece of glass that Panacea couldhave looked through to treat many patients.
hands-free communication system for medical professionalscan improve the efficiency and effectiveness of medical carein a variety of environments. We also describe the differentconfiguration options we explored on how the users could beplaced around a mass casualty disaster scenario. In another as-pect, we present our experiments with integration of softwaretechnologies such as WebRTC and Google Glass, and showhow we adapt our design to deal with range and heat issuesin order to calibrate our solution. Lastly, we present ease-of-use and communication system performance results from ourtesting of our Panacea Glass solution as part of a mass casualtylake simulation.
The remainder of this paper is organized as follows: Sec-tion II presents related work. Section III discusses the health-care needs and requirements for the mass casualty triage ina disaster scenario. Section IV describes our Panacea Glasssolution components within a mobile cloud framework forcommunication in mass casualty disaster triage. Section Vdescribes our experiments and results in the lab and in thelake simulation outdoors. Section VI concludes the paper.
II. RELATED WORK
Earlier works such as [5] estimate the effects of a disaster,the work in this paper builds on their motivations and focuseson using the existing network conditions along with the videodata from Google Glass device to provide better medicaltreatment to affected patients. The work in [6] addresses theissue of recovering data during a disaster scenario. The authorsin [7] describe a solution for achieving high availability,high survivability during a disaster scenario. The paper [8]describes features of emergence response systems during adisaster scenario. The systems in these works could use ourPanacea Glass technology coupled with wireless networkingand mobile cloud technology to provide better medical treat-ment to patients through smart communications. Our workis closely similar to the AID-N effort [2] done over 7 yearsback, where technologies such as electronic triage tags, web-portals, legacy wearable vital sign sensors, legacy hand-heldinterface devices and regular teleconferencing were used toenable collaboration between emergency response personnel.
Google Glass [9] is a latest innovation in wearable devices,which can be used in the disaster scenario be the medical teamalong with the existing network after disaster. Google Glassincludes a small camera in front of it which can be used tosend and receive scene related information by the collaboratingdoctor and the doctor treating the patient on the field usingvideo collaboration applications. Previously, people have usedGoogle Glass for medical image retrieval system as in [10]and for drone structural inspection as in [11]. This paper isnovel due to its proposed use of Google Glass through avideo collaboration application along with virtual beacons forcritical patient treatment during disaster scenarios. However,we remark that our Panacea solution is independent of thewearable technology (i.e., Recon Jet or other equivalent HUDcan be used), and builds on several proven studies that showhow Surgeons benefit from the care efficiency gained throughwearable technologies [12] [13].
III. HEALTHCARE CO-ORDINATION USE CASE
In this section, we first describe roles and workflows of thePanacea Glass system’s users. Following this, we describe thehealthcare demands and requirements for the design of oursystem to function in a mass casualty incident scenario.
A. Roles and WorkflowThis overall roles and communications in terms of data
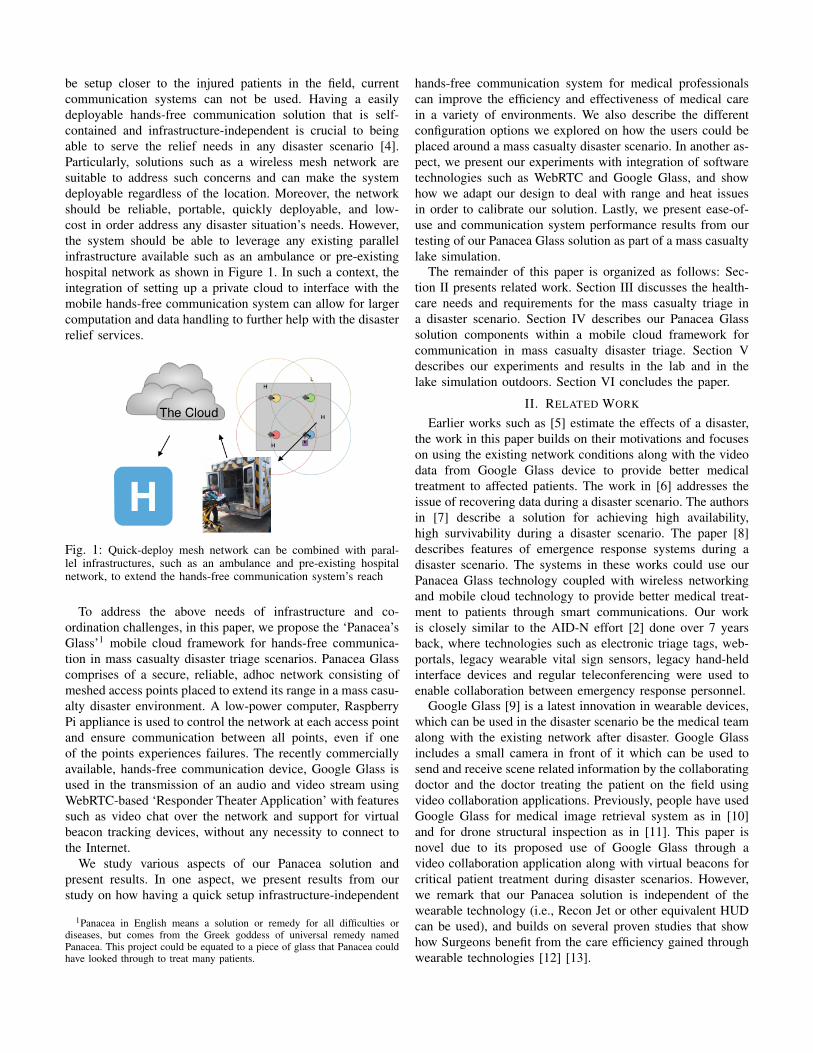
flow and control flow between the various roles in a masscasualty incident can be summarized as shown in Figure 2. Wecan see that there is a central Incident Command Center thatis responsible for co-ordination of multiple scenes through amesh network. The Incident Command Center is comprised ofa Incident Commander who has access to the Scene Databasethat has various information regarding geographic data, ex-perts, patients data and available medical experts as wellas other resources (e.g., Blood bank availability). Providingefficient healthcare to critical patients in the scenes requiresplanned co-ordination between all steps of the assessment andtreatment processes. In general, the co-ordination boils downto interactions between two main role groups: “stationaryexpert administrators” and “free-moving acting units”. Thestationary expert administrators would be focused on theoverall status of the healthcare effort as well as empoweringthe individual free-moving actors. The free-moving actorswould be the doctors, nurses, and other medical professionalswho would be at the front-line in healthcare. They would usehands-free devices in order to communicate their status and getthe necessary information to exemplarily perform their disasterrelief designated medical tasks.
B. Requirements during a disasterThe ability to efficiently operate the above workflow and
allow co-ordination with the various roles during a man-madeor natural disaster places significant design challenges on thePanacea Glass system. Firstly, a reliable, system-wide com-munication is essential to successful field triage and pertinentmobilization of care management actions at the various scenes,without being reliant of no or minimal infrastructure resourcesas described in the context of Figure 1. This independencenecessitates that the system provide all of it’s own power,network, and any other distributed system functions at leaston a temporary basis. In the worst case scenario, there may beno already installed network or available Internet connectionresulting in a severe limitation of having to operate completelyoffline. Further, our Panacea Glass solution needs to imple-ment best practices for mass-causality and disaster scenarios.Particularly, we implement a solution that involves having alead stationary administrator with many moving agents that areco-ordinating with the administrator as per the ‘Code Silver’protocol followed at our University of Missouri Hospital.The Code Silver organization style is in alignment with theHospital Incident Command System [3] as shown in Figure 3.
IV. PANACEA GLASS SOLUTION
The Panacea Glass solution that best meets the health careneeds and technical design requirements is shown in Figure 4,
Fig. 2: Diagram of the control and data flow in a mass casualtyincident site
and can be broken down into four main components whichare outlined below.
1) Mesh Network and Fault-Tolerant Server: A mesh net-work is ideal for quick versatile deployment which is importantfor quick setup in a disaster. The mesh network allows for“plug-and-play” deployment in unknown environments. Asshown in Figure 2, clients of the network, namely the usersof the hands-free communication application and the admindashboard, can freely roam within the network’s coveragerange. The network is also capable of handling a node failureby re-routing traffic through still online nodes.
Another option for a network setup is to have a longerrange deployment rather than a full mesh. The long-rangedeployment can be seen in Figure 5. This type of networkwould use a primary sector antenna to extend the range of anindividual access point to a greater distance with the possibilityof having additional access points to extend the network evenfurther. By doing this, the network becomes less fault-tolerantbecause if the primary access point fails, there would be alarge area in which the network would no longer cover andthe network may become segmented and separated. For thesereasons, we propose that the full mesh network shown inFigure 6 is more optimal in most cases than the long-rangenetwork shown in Figure 5.
A sever is needed to provide a consistent point of contact forall of the clients and facilitate the connection of users. It also

Fig. 3: Diagram of the Incident Command structure
Fig. 4: Overview of the Panacea Glass Solution
provides hosting for the Admin Dashboard. This server mustbe able to recover from a full or partial failure of the networkin addition to an unexpected temporary power outage. Wedesign such that the server be able to automatically reconnectwith clients through the reception of heartbeat requests.
2) Hands-free Communication Application: The free-moving actors need an application that allows them to com-municate without obstructing their primary directive in serving
Fig. 5: Communication through a long-range network deployment
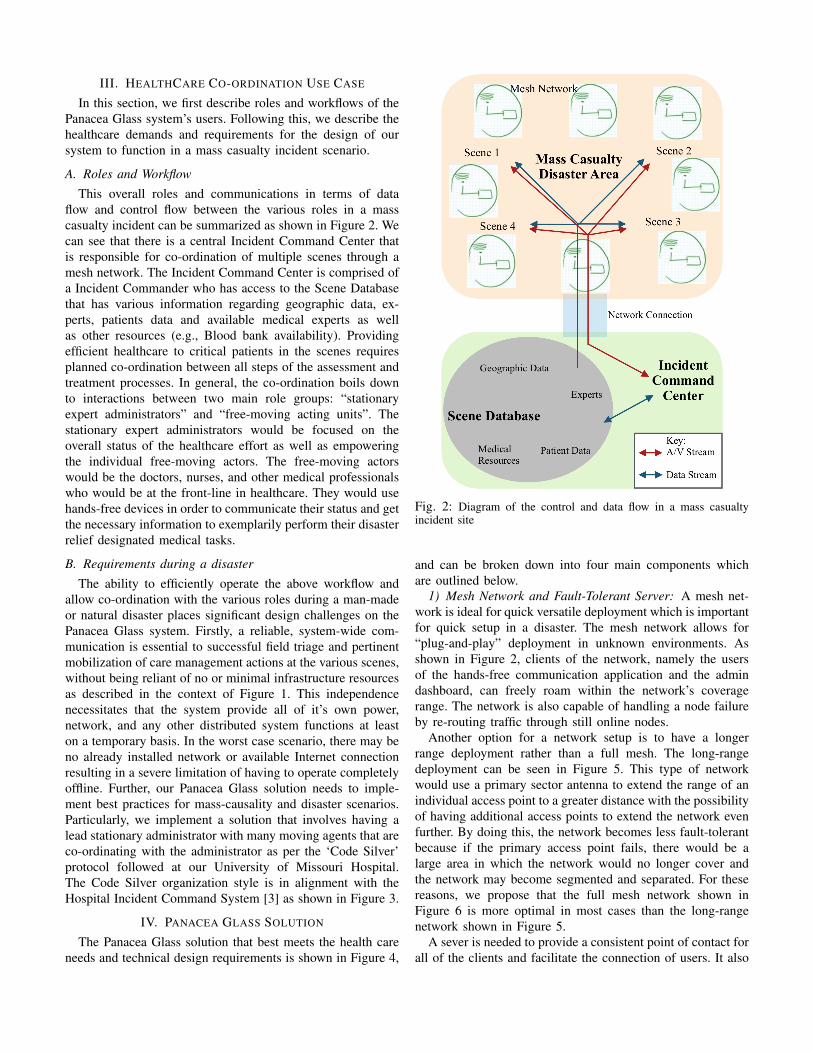
patients. This requires then that the application can be oper-ated primarily hands-free. We suppose that the focus of thefree-moving actor should remain on the patients while stillproviding as much information back as possible. The hands-free need was demonstrated in the lake disaster simulationuse case as shown in Figure 7. This leads to the ultimateconclusion that the hands-free application should stream thefree-moving actor’s audio and video feed back to the AdminDashboard automatically with the ability to receive audio callsfrom experts/administrators.
In order to make the application more fault-tolerant, thehands-free communication application should be able to el-egantly and automatically handle if the server is not reach-able, due to partial network failure or server failure. Wepropose using a peer-to-peer protocol for video and audiocommunication to allow the already initiated communicationto continue in the event of the server becoming unreachable.
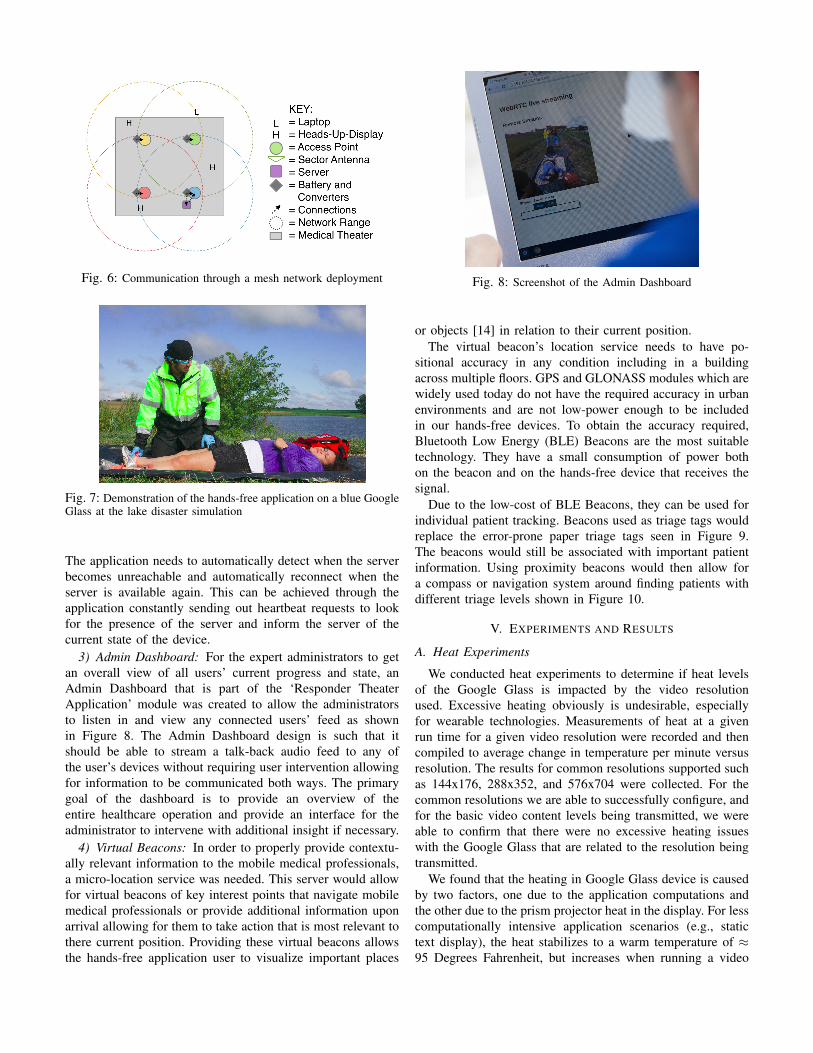
Fig. 6: Communication through a mesh network deployment
Fig. 7: Demonstration of the hands-free application on a blue GoogleGlass at the lake disaster simulation
The application needs to automatically detect when the serverbecomes unreachable and automatically reconnect when theserver is available again. This can be achieved through theapplication constantly sending out heartbeat requests to lookfor the presence of the server and inform the server of thecurrent state of the device.
3) Admin Dashboard: For the expert administrators to getan overall view of all users’ current progress and state, anAdmin Dashboard that is part of the ‘Responder TheaterApplication’ module was created to allow the administratorsto listen in and view any connected users’ feed as shownin Figure 8. The Admin Dashboard design is such that itshould be able to stream a talk-back audio feed to any ofthe user’s devices without requiring user intervention allowingfor information to be communicated both ways. The primarygoal of the dashboard is to provide an overview of theentire healthcare operation and provide an interface for theadministrator to intervene with additional insight if necessary.
4) Virtual Beacons: In order to properly provide contextu-ally relevant information to the mobile medical professionals,a micro-location service was needed. This server would allowfor virtual beacons of key interest points that navigate mobilemedical professionals or provide additional information uponarrival allowing for them to take action that is most relevant tothere current position. Providing these virtual beacons allowsthe hands-free application user to visualize important places
Fig. 8: Screenshot of the Admin Dashboard
or objects [14] in relation to their current position.The virtual beacon’s location service needs to have po-
sitional accuracy in any condition including in a buildingacross multiple floors. GPS and GLONASS modules which arewidely used today do not have the required accuracy in urbanenvironments and are not low-power enough to be includedin our hands-free devices. To obtain the accuracy required,Bluetooth Low Energy (BLE) Beacons are the most suitabletechnology. They have a small consumption of power bothon the beacon and on the hands-free device that receives thesignal.
Due to the low-cost of BLE Beacons, they can be used forindividual patient tracking. Beacons used as triage tags wouldreplace the error-prone paper triage tags seen in Figure 9.The beacons would still be associated with important patientinformation. Using proximity beacons would then allow fora compass or navigation system around finding patients withdifferent triage levels shown in Figure 10.
V. EXPERIMENTS AND RESULTS
A. Heat Experiments
We conducted heat experiments to determine if heat levelsof the Google Glass is impacted by the video resolutionused. Excessive heating obviously is undesirable, especiallyfor wearable technologies. Measurements of heat at a givenrun time for a given video resolution were recorded and thencompiled to average change in temperature per minute versusresolution. The results for common resolutions supported suchas 144x176, 288x352, and 576x704 were collected. For thecommon resolutions we are able to successfully configure, andfor the basic video content levels being transmitted, we wereable to confirm that there were no excessive heating issueswith the Google Glass that are related to the resolution beingtransmitted.
We found that the heating in Google Glass device is causedby two factors, one due to the application computations andthe other due to the prism projector heat in the display. For lesscomputationally intensive application scenarios (e.g., statictext display), the heat stabilizes to a warm temperature of ≈95 Degrees Fahrenheit, but increases when running a video
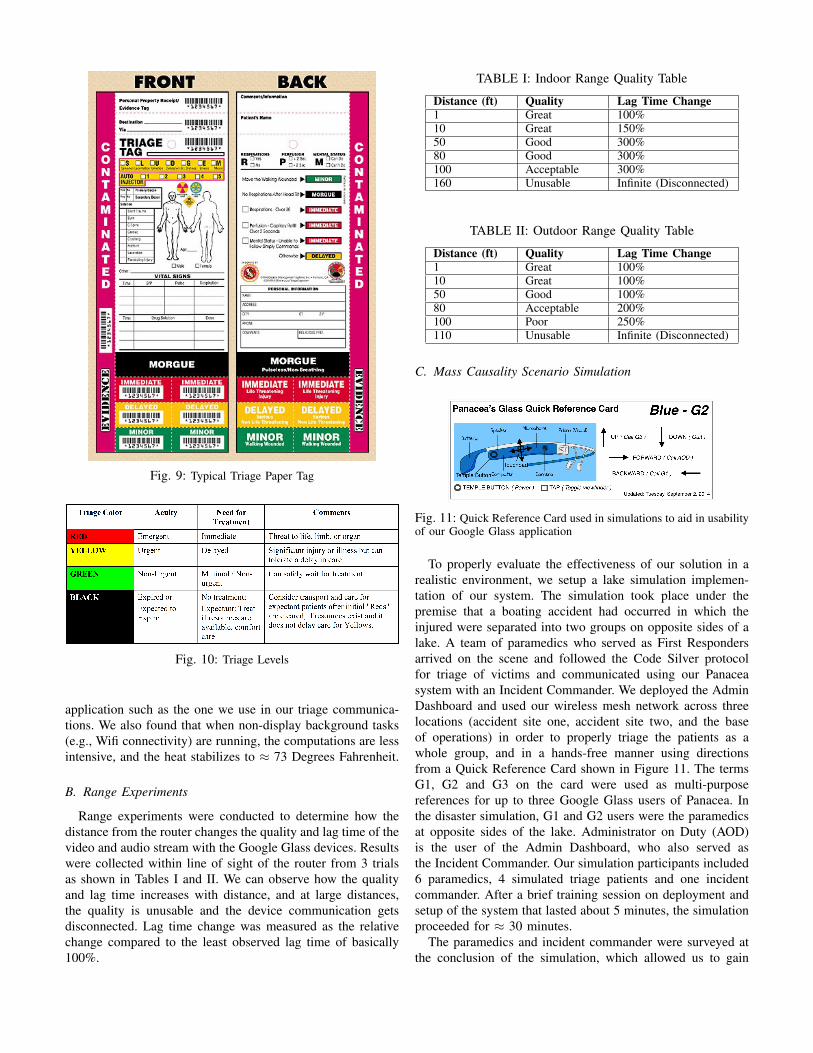
Fig. 9: Typical Triage Paper Tag
Fig. 10: Triage Levels
application such as the one we use in our triage communica-tions. We also found that when non-display background tasks(e.g., Wifi connectivity) are running, the computations are lessintensive, and the heat stabilizes to ≈ 73 Degrees Fahrenheit.
B. Range Experiments
Range experiments were conducted to determine how thedistance from the router changes the quality and lag time of thevideo and audio stream with the Google Glass devices. Resultswere collected within line of sight of the router from 3 trialsas shown in Tables I and II. We can observe how the qualityand lag time increases with distance, and at large distances,the quality is unusable and the device communication getsdisconnected. Lag time change was measured as the relativechange compared to the least observed lag time of basically100%.
TABLE I: Indoor Range Quality Table
Distance (ft) Quality Lag Time Change1 Great 100%10 Great 150%50 Good 300%80 Good 300%100 Acceptable 300%160 Unusable Infinite (Disconnected)
TABLE II: Outdoor Range Quality Table
Distance (ft) Quality Lag Time Change1 Great 100%10 Great 100%50 Good 100%80 Acceptable 200%100 Poor 250%110 Unusable Infinite (Disconnected)
C. Mass Causality Scenario Simulation
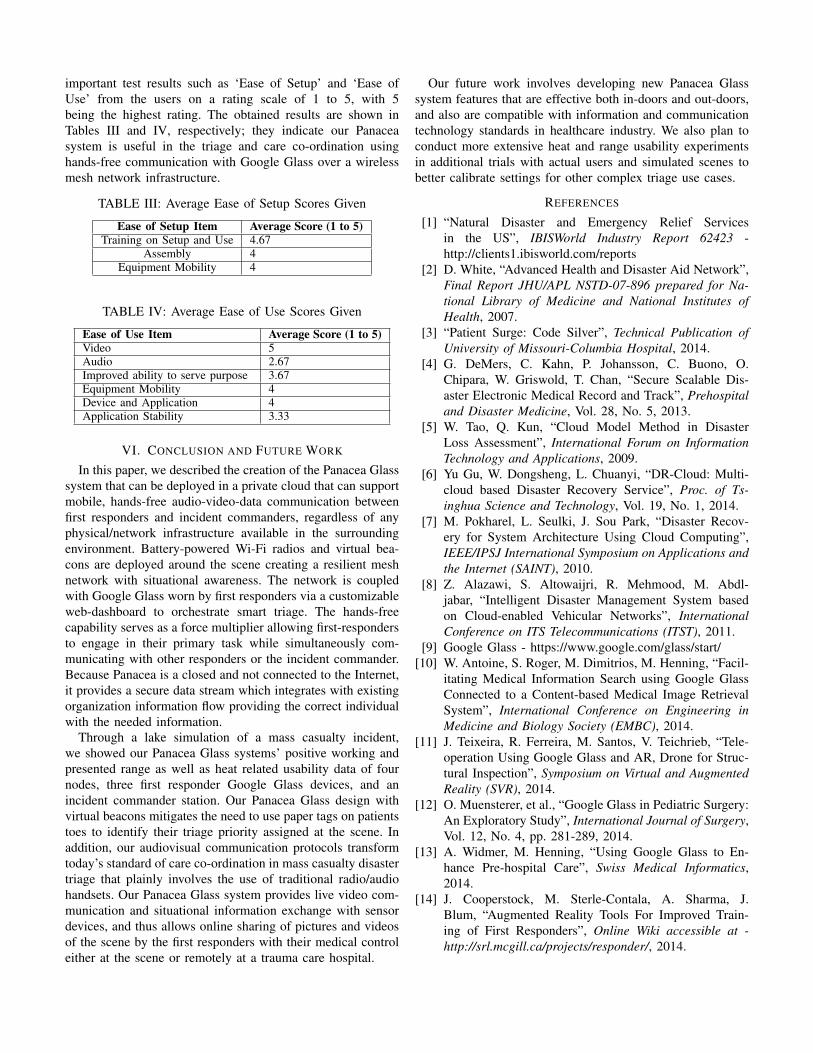
Fig. 11: Quick Reference Card used in simulations to aid in usabilityof our Google Glass application
To properly evaluate the effectiveness of our solution in arealistic environment, we setup a lake simulation implemen-tation of our system. The simulation took place under thepremise that a boating accident had occurred in which theinjured were separated into two groups on opposite sides of alake. A team of paramedics who served as First Respondersarrived on the scene and followed the Code Silver protocolfor triage of victims and communicated using our Panaceasystem with an Incident Commander. We deployed the AdminDashboard and used our wireless mesh network across threelocations (accident site one, accident site two, and the baseof operations) in order to properly triage the patients as awhole group, and in a hands-free manner using directionsfrom a Quick Reference Card shown in Figure 11. The termsG1, G2 and G3 on the card were used as multi-purposereferences for up to three Google Glass users of Panacea. Inthe disaster simulation, G1 and G2 users were the paramedicsat opposite sides of the lake. Administrator on Duty (AOD)is the user of the Admin Dashboard, who also served asthe Incident Commander. Our simulation participants included6 paramedics, 4 simulated triage patients and one incidentcommander. After a brief training session on deployment andsetup of the system that lasted about 5 minutes, the simulationproceeded for ≈ 30 minutes.
The paramedics and incident commander were surveyed atthe conclusion of the simulation, which allowed us to gain
important test results such as ‘Ease of Setup’ and ‘Ease ofUse’ from the users on a rating scale of 1 to 5, with 5being the highest rating. The obtained results are shown inTables III and IV, respectively; they indicate our Panaceasystem is useful in the triage and care co-ordination usinghands-free communication with Google Glass over a wirelessmesh network infrastructure.
TABLE III: Average Ease of Setup Scores Given
Ease of Setup Item Average Score (1 to 5)Training on Setup and Use 4.67
Assembly 4Equipment Mobility 4
TABLE IV: Average Ease of Use Scores Given
Ease of Use Item Average Score (1 to 5)Video 5Audio 2.67Improved ability to serve purpose 3.67Equipment Mobility 4Device and Application 4Application Stability 3.33
VI. CONCLUSION AND FUTURE WORK
In this paper, we described the creation of the Panacea Glasssystem that can be deployed in a private cloud that can supportmobile, hands-free audio-video-data communication betweenfirst responders and incident commanders, regardless of anyphysical/network infrastructure available in the surroundingenvironment. Battery-powered Wi-Fi radios and virtual bea-cons are deployed around the scene creating a resilient meshnetwork with situational awareness. The network is coupledwith Google Glass worn by first responders via a customizableweb-dashboard to orchestrate smart triage. The hands-freecapability serves as a force multiplier allowing first-respondersto engage in their primary task while simultaneously com-municating with other responders or the incident commander.Because Panacea is a closed and not connected to the Internet,it provides a secure data stream which integrates with existingorganization information flow providing the correct individualwith the needed information.
Through a lake simulation of a mass casualty incident,we showed our Panacea Glass systems’ positive working andpresented range as well as heat related usability data of fournodes, three first responder Google Glass devices, and anincident commander station. Our Panacea Glass design withvirtual beacons mitigates the need to use paper tags on patientstoes to identify their triage priority assigned at the scene. Inaddition, our audiovisual communication protocols transformtoday’s standard of care co-ordination in mass casualty disastertriage that plainly involves the use of traditional radio/audiohandsets. Our Panacea Glass system provides live video com-munication and situational information exchange with sensordevices, and thus allows online sharing of pictures and videosof the scene by the first responders with their medical controleither at the scene or remotely at a trauma care hospital.
Our future work involves developing new Panacea Glasssystem features that are effective both in-doors and out-doors,and also are compatible with information and communicationtechnology standards in healthcare industry. We also plan toconduct more extensive heat and range usability experimentsin additional trials with actual users and simulated scenes tobetter calibrate settings for other complex triage use cases.
REFERENCES
[1] “Natural Disaster and Emergency Relief Servicesin the US”, IBISWorld Industry Report 62423 -http://clients1.ibisworld.com/reports
[2] D. White, “Advanced Health and Disaster Aid Network”,Final Report JHU/APL NSTD-07-896 prepared for Na-tional Library of Medicine and National Institutes ofHealth, 2007.
[3] “Patient Surge: Code Silver”, Technical Publication ofUniversity of Missouri-Columbia Hospital, 2014.
[4] G. DeMers, C. Kahn, P. Johansson, C. Buono, O.Chipara, W. Griswold, T. Chan, “Secure Scalable Dis-aster Electronic Medical Record and Track”, Prehospitaland Disaster Medicine, Vol. 28, No. 5, 2013.
[5] W. Tao, Q. Kun, “Cloud Model Method in DisasterLoss Assessment”, International Forum on InformationTechnology and Applications, 2009.
[6] Yu Gu, W. Dongsheng, L. Chuanyi, “DR-Cloud: Multi-cloud based Disaster Recovery Service”, Proc. of Ts-inghua Science and Technology, Vol. 19, No. 1, 2014.
[7] M. Pokharel, L. Seulki, J. Sou Park, “Disaster Recov-ery for System Architecture Using Cloud Computing”,IEEE/IPSJ International Symposium on Applications andthe Internet (SAINT), 2010.
[8] Z. Alazawi, S. Altowaijri, R. Mehmood, M. Abdl-jabar, “Intelligent Disaster Management System basedon Cloud-enabled Vehicular Networks”, InternationalConference on ITS Telecommunications (ITST), 2011.
[9] Google Glass - https://www.google.com/glass/start/[10] W. Antoine, S. Roger, M. Dimitrios, M. Henning, “Facil-
itating Medical Information Search using Google GlassConnected to a Content-based Medical Image RetrievalSystem”, International Conference on Engineering inMedicine and Biology Society (EMBC), 2014.
[11] J. Teixeira, R. Ferreira, M. Santos, V. Teichrieb, “Tele-operation Using Google Glass and AR, Drone for Struc-tural Inspection”, Symposium on Virtual and AugmentedReality (SVR), 2014.
[12] O. Muensterer, et al., “Google Glass in Pediatric Surgery:An Exploratory Study”, International Journal of Surgery,Vol. 12, No. 4, pp. 281-289, 2014.
[13] A. Widmer, M. Henning, “Using Google Glass to En-hance Pre-hospital Care”, Swiss Medical Informatics,2014.
[14] J. Cooperstock, M. Sterle-Contala, A. Sharma, J.Blum, “Augmented Reality Tools For Improved Train-ing of First Responders”, Online Wiki accessible at -http://srl.mcgill.ca/projects/responder/, 2014.





























