Embed Size (px)
Citation preview
Pantoprazole versus one-week Helicobacter pylori eradicationtherapy for the prevention of acute NSAID-related gastroduodenaldamage in elderly subjects
A. PILOTTO*, F. DI MARIO , M. FRANCESCHI*, G. LEANDROà , G. BATTAGLIA§,
B. GERMANAÁ ± , R. MARIN** & G. VALERIO*
*Digestive Pathophysiology Center, Department of Geriatrics, Vicenza, Italy; Department of Gastroenterology, Padova, Italy;
àDepartment of Gastroenterology, Castellana Grotte (BA), Italy; §Department of Gastroenterology, Venezia, Italy;
±Department of Gastroenterology, Belluno, Italy; and **Department of Gastroenterology, Dolo (VE), Italy
Accepted for publication 5 April 2000
INTRODUCTION
Helicobacter pylori (H. pylori) infection and nonsteroidal
anti-in¯ammatory drug (NSAID) use account for over
75% of gastric and duodenal ulcers in elderly sub-
jects.1, 2 H. pylori is present in approximately 50% of
patients with NSAID-associated gastroduodenal injury,3
yet it is still not clear if a signi®cant relationship exists
between these two factors in inducing gastroduodenal
damage.4, 5
Previous studies have shown that prophylactic therapy
with misoprostol,6 famotidine7 or omeprazole8, 9 is
effective in the prevention of NSAID-induced ulcers,
while reports are con¯icting about whether eradication
therapy for H. pylori may prevent NSAID-induced peptic
ulcers.10, 11
The aim of the present study was to compare the effect
of eradication of H. pylori infection using a one-week
triple therapy to that of a maintenance therapy with the
SUMMARY
Aim: To compare the ef®cacy of pantoprazole vs. a one-
week Helicobacter pylori eradication therapy for the
prevention of NSAID-related gastroduodenal damage.
Methods: Patients over 60 years old with symptoms
and/or a history of ulcer who needed NSAID treatment
were evaluated by endoscopy. H. pylori positive subjects
who had no severe gastroduodenal lesions were ran-
domized to take, concomitantly with NSAID therapy,
either: (i) pantoprazole 40 mg daily plus amoxycillin
1 g b.d. and clarithromycin 250 mg b.d. for 1 week (35
subjects, Group PAC) or (ii) pantoprazole 40 mg daily
for 1 month (34 subjects, Group P). Endoscopy was
repeated after 1 month.
Results: A signi®cantly higher incidence of severe
gastroduodenal damage was found in Group PAC than
in Group P (29% vs. 9%, P < 0.05). The percentages of
patients worsened, unchanged and improved after
1 month were, respectively: Group PAC: 46%, 46%,
and 9% and Group P: 7%, 65%, and 29% (P < 0.0008).
The percentage of H. pylori-negative subjects was 89%
in Group PAC and 52% in Group P (P � 0.0009). The
incidence of gastroduodenal damage was higher in
Group PAC treatment failures than in cured patients
(50% vs. 25.8%, P � ns).
Conclusion: One month of pantoprazole was more
effective than a proton pump inhibitor-based triple
therapy in the prevention of gastroduodenal damage in
elderly H. pylori-positive NSAID users.
Correspondence to: Dr A. Pilotto, Centro di Fisiopatologia Digestiva dell¢Anziano, UnitaÁ Operativa di Geriatria, Ospedale S. Bortolo ± Via Rodol®,
37, 36100 Vicenza, Italy.E-mail: [email protected]
Aliment Pharmacol Ther 2000; 14: 1077±1082.
Ó 2000 Blackwell Science Ltd 1077

proton pump inhibitor, pantoprazole, for the prevention
of acute NSAID-related gastroduodenal damage in
H. pylori positive elderly NSAID users.
MATERIALS AND METHODS
Patients
Patients were recruited from March to October 1998.
Eligible patients were (a) older than 60 years of age; (b)
with musculoskeletal pain requiring NSAID treatment
for at least one month and (c) with dyspeptic symptoms
or a personal history of gastritis or peptic ulcer. Patients
received a clear explanation of the purpose of the study
and agreed to participate with informed consent.
Endoscopy
At endoscopy, ulcers, erosions and intramucosal hae-
morrhages were recorded separately for the oesophagus,
stomach and duodenum. An ulcer was de®ned as a
circumscribed mucosal break of 3 mm or more in
diameter with a well-de®ned ulcer crater, whereas
smaller or super®cial lesions were classi®ed as erosions.
Intramucosal haemorrhages were de®ned as haemor-
rhagic lesions without overlying mucosal breaks.6, 7 The
severity of NSAID-related gastroduodenal injury was
classi®ed according to a modi®ed Lanza score12 from 0 to
4: 0 � no lesions; 1 � 1±3 erosions or petechie or
intramucosal haemorragic lesions; 2 � < 10 erosions
or petechie or intramucosal haemorragic lesions; 3 � >
10 erosions or petechie or intramucosal haemorragic
lesions; 4 � a well de®ned ulcer. We de®ned `severe'
gastroduodenal injury as the presence of an endoscopic
diagnosis of grade 3 or 4 using the Lanza scoring system.
H. pylori infection
During endoscopy, six gastric biopsies were taken from
both the antrum (three biopsies), and from the body
(three biopsies). Two antral and two body biopsies were
used for histological analysis, while one from each site
was used for the rapid urease test (CLO test, Delta West
Pty Ltd, Western Australia, Australia).
For histological examinations, biopsy specimens were
immediately ®xed in buffered neutral formalin and
embedded in paraf®n. Sections were stained with
haematoxylin±eosin and modi®ed Giemsa stains for
the detection of H. pylori.
At baseline, patients were considered to be H. pylori
positive if both their histology and rapid urease tests
were positive for H. pylori infection. After therapy, a
patient was considered as being H. pylori negative if
both histology and rapid urease tests were negative;
patients were considered H. pylori positive if either their
histology or rapid urease tests, or both, were positive for
H. pylori infection.
Therapy
Patients who were con®rmed to have: (a) the presence
of gastric H. pylori infection, and (b) no severe
gastroduodenal lesions (Lanza score £ 2), after endo-
scopy were included in the study.
After inclusion, elderly H. pylori-positive patients were
consecutively randomized to one of the following
treatments:
1 eradication therapy with pantoprazole 40 mg once
daily plus amoxycillin 1 g b.d. and clarithromycin
250 mg bi.d. for 1 week (Group PAC) or
2 pantoprazole 40 mg once a day (in the morning) for
1 month (Group P).
After 1 month, all patients had a repeated endoscopy,
with gastric biopsies for histology and the rapid urease
test. During the 1-month period of the study, patients of
both Groups PAC and P were treated daily with
diclofenac 50 mg (20 subjects of Group PAC and 18
subjects of Group P) or 100 mg (15 subjects of Group
PAC and 13 of Group P).
Statistics
Results were evaluated using both `per protocol' (PP)
and `intention-to-treat' (ITT) analyses. The ITT popula-
tion was de®ned as all patients initially enrolled who
had taken at least one dose of study medication. A
statistical analysis was performed using the v2 test with
standard deviations: these were de®ned as (O ± E)/ÖE
(where O is the observed frequency and E the expected
frequency). All P-values were two-tailed, with statistical
signi®cance set at P < 0.05.
RESULTS
Of 127 eligible subjects observed over 8 months, 108
consecutive patients agreed to take part and underwent
endoscopy for enrolment in the study. Of these patients,
1078 A. PILOTTO et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 1077±1082
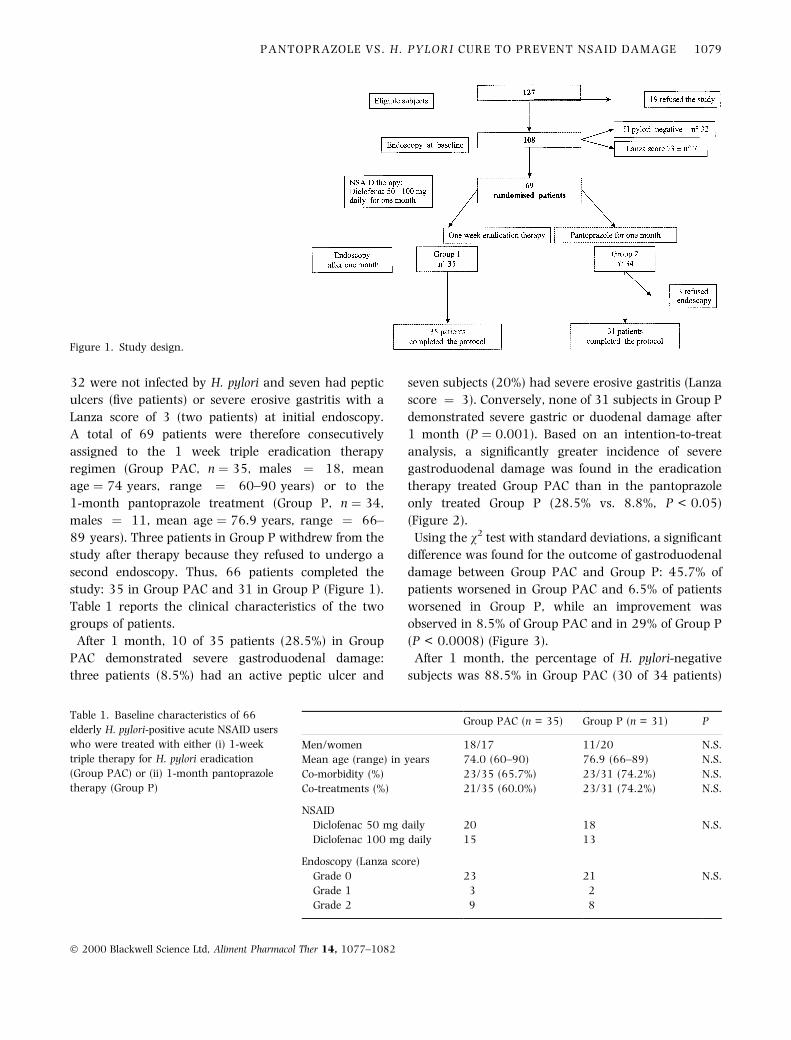
32 were not infected by H. pylori and seven had peptic
ulcers (®ve patients) or severe erosive gastritis with a
Lanza score of 3 (two patients) at initial endoscopy.
A total of 69 patients were therefore consecutively
assigned to the 1 week triple eradication therapy
regimen (Group PAC, n � 35, males � 18, mean
age � 74 years, range � 60±90 years) or to the
1-month pantoprazole treatment (Group P, n � 34,
males � 11, mean age � 76.9 years, range � 66±
89 years). Three patients in Group P withdrew from the
study after therapy because they refused to undergo a
second endoscopy. Thus, 66 patients completed the
study: 35 in Group PAC and 31 in Group P (Figure 1).
Table 1 reports the clinical characteristics of the two
groups of patients.
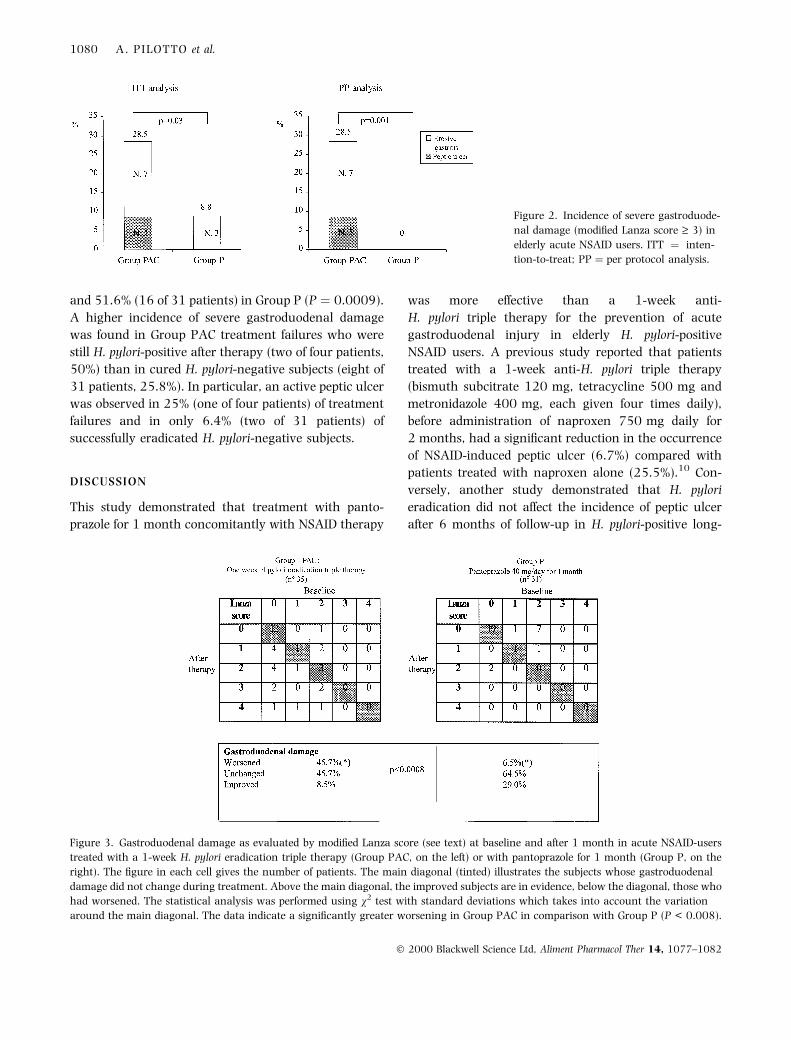
After 1 month, 10 of 35 patients (28.5%) in Group
PAC demonstrated severe gastroduodenal damage:
three patients (8.5%) had an active peptic ulcer and
seven subjects (20%) had severe erosive gastritis (Lanza
score � 3). Conversely, none of 31 subjects in Group P
demonstrated severe gastric or duodenal damage after
1 month (P � 0.001). Based on an intention-to-treat
analysis, a signi®cantly greater incidence of severe
gastroduodenal damage was found in the eradication
therapy treated Group PAC than in the pantoprazole
only treated Group P (28.5% vs. 8.8%, P < 0.05)
(Figure 2).
Using the v2 test with standard deviations, a signi®cant
difference was found for the outcome of gastroduodenal
damage between Group PAC and Group P: 45.7% of
patients worsened in Group PAC and 6.5% of patients
worsened in Group P, while an improvement was
observed in 8.5% of Group PAC and in 29% of Group P
(P < 0.0008) (Figure 3).
After 1 month, the percentage of H. pylori-negative
subjects was 88.5% in Group PAC (30 of 34 patients)
Figure 1. Study design.
Table 1. Baseline characteristics of 66
elderly H. pylori-positive acute NSAID users
who were treated with either (i) 1-week
triple therapy for H. pylori eradication
(Group PAC) or (ii) 1-month pantoprazole
therapy (Group P)
Group PAC (n = 35) Group P (n = 31) P
Men/women 18/17 11/20 N.S.
Mean age (range) in years 74.0 (60±90) 76.9 (66±89) N.S.
Co-morbidity (%)2 23/35 (65.7%) 23/31 (74.2%) N.S.
Co-treatments (%) 21/35 (60.0%) 23/31 (74.2%) N.S.
NSAID
Diclofenac 50 mg daily 20 18 N.S.
Diclofenac 100 mg daily 15 13
Endoscopy (Lanza score)
Grade 0 23 21 N.S.
Grade 1 3 2
Grade 2 9 8
PANTOPRAZOLE VS. H. PYLORI CURE TO PREVENT NSAID DAMAGE 1079
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 1077±1082
and 51.6% (16 of 31 patients) in Group P (P � 0.0009).
A higher incidence of severe gastroduodenal damage
was found in Group PAC treatment failures who were
still H. pylori-positive after therapy (two of four patients,
50%) than in cured H. pylori-negative subjects (eight of
31 patients, 25.8%). In particular, an active peptic ulcer
was observed in 25% (one of four patients) of treatment
failures and in only 6.4% (two of 31 patients) of
successfully eradicated H. pylori-negative subjects.
DISCUSSION
This study demonstrated that treatment with panto-
prazole for 1 month concomitantly with NSAID therapy
was more effective than a 1-week anti-
H. pylori triple therapy for the prevention of acute
gastroduodenal injury in elderly H. pylori-positive
NSAID users. A previous study reported that patients
treated with a 1-week anti-H. pylori triple therapy
(bismuth subcitrate 120 mg, tetracycline 500 mg and
metronidazole 400 mg, each given four times daily),
before administration of naproxen 750 mg daily for
2 months, had a signi®cant reduction in the occurrence
of NSAID-induced peptic ulcer (6.7%) compared with
patients treated with naproxen alone (25.5%).10 Con-
versely, another study demonstrated that H. pylori
eradication did not affect the incidence of peptic ulcer
after 6 months of follow-up in H. pylori-positive long-
Figure 2. Incidence of severe gastroduode-
nal damage (modi®ed Lanza score ³ 3) in
elderly acute NSAID users. ITT � inten-
tion-to-treat; PP � per protocol analysis.
Figure 3. Gastroduodenal damage as evaluated by modi®ed Lanza score (see text) at baseline and after 1 month in acute NSAID-users
treated with a 1-week H. pylori eradication triple therapy (Group PAC, on the left) or with pantoprazole for 1 month (Group P, on the
right). The ®gure in each cell gives the number of patients. The main diagonal (tinted) illustrates the subjects whose gastroduodenal
damage did not change during treatment. Above the main diagonal, the improved subjects are in evidence, below the diagonal, those who
had worsened. The statistical analysis was performed using v2 test with standard deviations which takes into account the variation
around the main diagonal. The data indicate a signi®cantly greater worsening in Group PAC in comparison with Group P (P < 0.008).
1080 A. PILOTTO et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 1077±1082

term NSAID users who continued NSAID treatment
without anti-ulcer treatment.11 Similarly, a study of
chronic NSAID users with healed ulcers followed for
6 months after stopping anti-ulcer therapy while con-
tinuing NSAIDs, failed to demonstrate any difference in
cumulative recurrence rates of peptic ulcer among
patients who were H. pylori-negative (27%), H. pylori-
negative after eradication therapy (31%) or H. pylori-
positive (46%).13 However, none of these studies had
evaluated the preventative effect of H. pylori eradication
compared to a maintenance therapy with effective anti-
ulcer drugs such as misoprostol or proton pump
inhibitors.
The only previous study that compared H. pylori
eradication with proton pump inhibitor therapy was
performed by Chan et al. in high risk NSAID users who
had developed NSAID-associated ulcer bleeding14 and
who had resumed NSAID use (naproxen 500 mg b.d.
for 6 months) after ulcer healing. A signi®cantly higher
incidence of recurrent ulcer bleeding was observed in
patients treated with a 1-week H. pylori eradication
therapy (20%) compared to patients who received
omeprazole as prophylactic treatment concomitantly
with naproxen (2%, P < 0.01).
The present ®ndings are in agreement with the
results of this last study. For the ®rst time, a
signi®cant effect of 1 month of 40 mg daily pan-
toprazole in the prevention of NSAID-related gas-
troduodenal damage was documented in high risk
(subjects with dyspeptic symptoms and/or a personal
history of gastritis or ulcer) elderly patients, who are
usually prescribed a gastroprotective therapy concom-
itant with NSAID treatment for musculoskeletal pain.
Furthermore, this study demonstrated that prevention
with proton pump inhibitors was effective during an
acute NSAID treatment of only 1 month. This ®nding
may be clinically relevant, since it is known that over
50% of NSAID-related gastroduodenal lesions, includ-
ing bleeding complications, occurred after occasional
(within 1 week) or acute (within 1 month) NSAID
treatment in elderly patients.3, 15, 16 Recently, several
studies have reported that proton pump inhibitors
such as omeprazole were very effective in the
prevention of NSAID-related gastric and duodenal
injuries.8, 9, 17±19 Such an activity has also been
previously been reported for pantoprazole,20, 21 but
not in the elderly.
None of the 34 patients treated with pantoprazole
(Group P) reported relevant side-effects, demonstrating
that the drug was safe and well tolerated in elderly
subjects who are affected with a high percentage (over
74%) of concomitant diseases and treatments. This high
level of tolerance may be due to the lack of pharmaco-
kinetic interaction between pantoprazole and other
drugs, including diclofenac, as has been reported in
previous studies.22, 23
The cure rate of H. pylori infection with pantopra-
zole 40 mg daily plus amoxycillin 1 g b.d. and
clarithromycin 250 mg b.d. was 88.5%, a very
similar result to those reported for non-NSAID-using
elderly subjects,24, 25 suggesting that concomitant
treatment with diclofenac did not in¯uence cure
rates for H. pylori infection. Successfully cured
H. pylori negative patients were shown to have a
lower incidence of severe gastroduodenal damage
than treatment failures still H. pylori-positive after
therapy. This difference was not statistically signi®-
cant, probably due to the small number of subjects
who remained H. pylori positive after therapy (only
four patients).
In Group P, 51.6% of patients treated with pantopra-
zole without antibiotics were H. pylori-negative after
1 month. To date, a direct effect of pantoprazole on
H. pylori infection has not been reported. However, a
temporary suppression of H. pylori activity during
proton pump inhibitor treatment,26 as well as a
proximal migration of H. pylori towards the gastric
fundus,27 may explain this ®nding. Indeed, no differ-
ences in terms of the prevention of NSAID-related
damage were found between H. pylori-negative and
H. pylori-positive subjects treated with pantoprazole.
This suggests that the control of gastric acid secretion
alone, may prevent acute NSAID-related damage in
elderly subjects, and that such an effect is independent
from H. pylori infection.
In conclusion, 1 month of concomitant pantoprazole
therapy was more effective than a proton pump
inhibitor-based triple therapy in the prevention of
severe acute NSAID-related gastroduodenal damage in
elderly H. pylori-positive NSAID users. The data suggest
that it appears less critical to test and treat H. pylori
infection in elderly patients who require acute NSAID
treatment than to prevent gastroduodenal injuries using
effective antisecretory drugs.28
ACKNOWLEDGEMENTS
This work was supported by the host institutions.1
PANTOPRAZOLE VS. H. PYLORI CURE TO PREVENT NSAID DAMAGE 1081
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 1077±1082

REFERENCES
1 Pilotto A. Helicobacter pylori infection in the elderly. Clin
Geriatrics 1996; 4: 53±70.
2 Kemppainen H, Raiha I, Kujari H, Sourander L. Characteris-
tics of Helicobacter pylori-negative and -positive peptic ulcer
disease. Age Ageing 1998; 27: 427±31.
3 Pilotto A, Franceschi M, Leandro G, Di Mario F, Valerio G. The
effect of Helicobacter pylori infection on NSAID-related gas-
troduodenal damage in the elderly. Eur J Gastroenterol Hep-
atol 1997; 9: 951±6.
4 Hawkey CJ. Personal review: Helicobacter pylori, NSAIDs and
cognitive dissonance. Aliment Pharmacol Ther 1999; 13:
695±702.
5 Bretagne JF, Quina MG. Helicobacter pylori and non-steroidal
anti-in¯ammatory drugs. Curr Opin Gastroenterol 1999;
15(Suppl. 1): S61±5.
6 Graham DY, White RH, Moreland LW, et al. Duodenal and
gastric ulcer prevention with misoprostol in arthritic patients
taking NSAIDs. Ann Intern Med 1993; 119: 257±62.
7 Taha AS, Hudson N, Hawkey CJ, et al. Famotidine for the
prevention of gastric and duodenal ulcers caused by non-
steroidal antiin¯ammatory drugs. N Engl J Med 1996; 334:
1435±9.
8 Yeomans ND, Tulassay Z, Juhasz L, et al. For the ASTRONAUT
Study Group. A comparison of omeprazole with ranitidine for
ulcers associated with nonsteroidal antiin¯ammatory drugs.
N Engl J Med 1998; 338: 719±26.
9 Hawkey CJ, Karrasch JA, Szczepanski L, et al. For the OMNI-
UM Study Group. Omeprazole compared with misoprostol for
ulcers associated with nonsteroidal antiin¯ammatory drugs.
N Engl J Med 1998; 338: 727±34.
10 Chan FKL, Sung JJY, Chung SCS, et al. Randomised trial of
eradication of Helicobacter pylori before non-steroidal anti-
in¯ammatory drug therapy to prevent peptic ulcers. Lancet
1997; 350: 975±9.
11 Hawkey CJ, Tulassay Z, Szczepanski L, et al. Randomised
controlled trial of Helicobacter pylori eradication in patients on
non-steroidal anti-in¯ammatory drugs: HELP NSAIDs study.
Lancet 1998; 352: 1016±21.
12 Aadland E, Fausa O, Vatn M. Protection by misoprostol
against naproxen-induced gastric mucosal damage. Am J Med
1987; 83(Suppl. 1): 37±40.
13 Bianchi Porro G, Parente F, Imbesi V, Montrone F, Caruso I.
Role of Helicobacter pylori infection in ulcer healing and
recurrence of gastric and duodenal ulcers in longterm NSAID
users. Response to omeprazole dual therapy. Gut 1997; 39:
22±6.
14 Chan FKL, Sung JY, Suen R, et al. Eradication of H. pylori versus
maintenance acid suppression to prevent recurrent ulcer
haemorrhage in high risk NSAID users. A prospective rando-
mised study. Gastroenterology 1998; 114: A87(Abstract).
15 Kemppainen H, Raiha I, Sourander L. Clinical presentation of
bleeding peptic ulcer in the elderly. Aging Clin Exp Res 1996;
42: 184±8.
16 Pilotto A, Leandro G, Di Mario F, Franceschi M, Bozzola L,
Valerio G. Role of Helicobacter pylori infection on upper gas-
trointestinal bleeding in the elderly. A case-control study. Dig
Dis Sci 1997; 42: 586±91.
17 Ekstrom P, Carling S, Wetterhus S, et al. Prevention of peptic
ulcer and dyspeptic symptoms with omeprazole in patients
receiving continuous non steroidal anti-in¯ammatory drugs.
Scand J Gastroenterol 1996; 31: 753±8.
18 Bianchi Porro G, Lazzaroni M, Petrillo M, Manzionna G,
Montrone F, Caruso I. Prevention of gastrodudoenal damage
with omeprazole in patients receiving continuous NSAIDs
treatment. A double blind placebo controlled study. Ital J
Gastroenterol Hepatol 1998; 30: 43±7.
19 Cullen D, Bardhan KD, Eisner M, et al. Primary gastroduode-
nal prophylaxis with omeprazole for non-steroidal anti-
in¯ammatory drug users. Aliment Pharmacol Ther 1998;
12: 135±40.
20 Bianchi Porro G, Imbesi V, Lazzaroni M, Montrone F, San-
tagada T. Pantoprazole versus placebo in prevention of
NSAID-induced ulcers. Gastroenterology 1998; 114(Suppl.):
G-806.
21 Simon B, Muller P. Pantoprazole protects against aspirin-
induced damage in the upper gastro-intestinal tract. Gut 41
(Suppl, 1997; 3): A198(Abstract).
22 Zech K, Steinijans VW, Huber R, Kolassa N, Radtke HW.
Pharmacokinetics and drug interactions: relevant factors for
the choice of a drug. Int J Clin Pharmacol Ther 1996;
34(Suppl. 1): S3±S6.
23 Bliesath H, Huber R, Steinijans VW, Koch HJ, Wurst W,
Mascher H. Lack of pharmacokinetic interaction between
pantoprazole and diclofenac. Int J Clin Pharmacol Ther 1996;
34: 152±6.
24 Pilotto A, Franceschi M, Leandro G, et al. Ef®cacy of 7 day
lansoprazole-based triple therapy for Helicobacter pylori infec-
tion in elderly patients. J Gastroenterol Hepatol 1999; 14:
468±75.
25 Pilotto A, Leandro G, Franceschi M, et al. The effect of anti-
biotic resistance on the outcome of three 1-week triple ther-
apies against Helicobacter pylori. Aliment Pharmacol Ther
1999; 13: 667±73.
26 Williams MP, Sercombe JC, Lawson AJ, Slater E, Owen RJ,
Pounder RE. The effect of omeprazole dosing on the isolation
of Helicobacter pylori from gastric aspirates. Aliment Pharma-
col Ther 1999; 13: 1161±9.
27 Vigneri S, Termini R, Di Mario F, Scialabba A, Pisciotta G.
Omeprazole therapy modi®es the gastric localization of Heli-
cobacter pylori. Am J Gastroenterol 1991; 86: 1276.
28 Marshall B. NSAIDs and Helicobacter pylori: therapeutic
options. Lancet 1998; 352: 1001±3.
1082 A. PILOTTO et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 1077±1082


![Prevention of NSAID-induced gastroduodenal ulcerspaindr.com/wp-content/uploads/2012/10/2011_Prevention-of... · 2008. 7. 16. · [Intervention Review] Prevention of NSAID-induced](https://img.pdfslide.net/doc/110x75/5fe26ff11d818a6d47357d27/prevention-of-nsaid-induced-gastroduodenal-2008-7-16-intervention-review.jpg)