Embed Size (px)
Citation preview
PARAPNEUMONIC EMPYEMA
• Uncomplicated effusion.
• Thoracic empyema.
Uncomplicated Effusion
• Nonpurulent. • Negative Gram’s stain result, negative
culture. • Free flowing, pH 7.3, normal glucose level,
LDH less than 1000 IU/L. • Most resolve with appropriate antibiotics
treatment and resolution of the pulmonary infection.
Thoracic Empyema
• Bacteria invade the normally sterile pleural space.
• Three stage
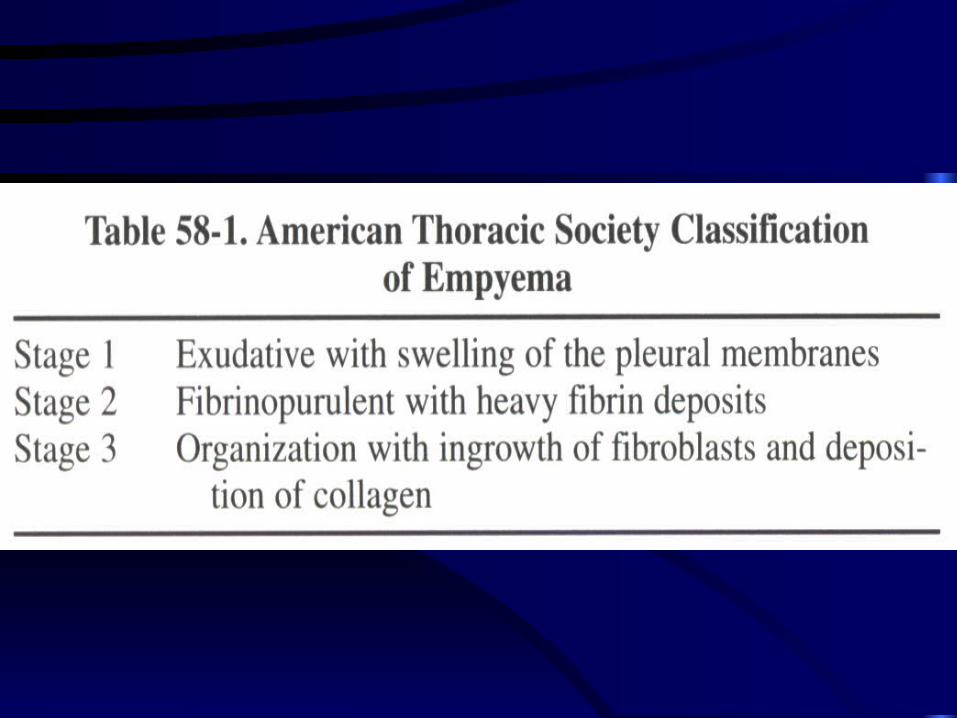
• Table 58-1
Thoracic Empyema-- Stage 1
• Exudative effusion.
• Increase permeability of the inflammatory and swollen pleural surface.
• Correspond to the uncomplicated parapneumonic effusion.
• Sterile, fibrin and PMN may present.
Thoracic Empyema-- Stage 2• Fibropurulent, true empyema, complicated pleural
effusion.• Initial-- fluid is clear : WBC greater than 500
cell/μL, gravity greater than 1.08, protein level greater than 2.5 g/dL, ph less 7.2, LDH reach 1000 IU/L, fibrin deposit.
• Angioblastic and fibroblastic proliferation, heavy fibrin deposition on both pleura, particularly the parietal pleura.
• Later– fluid purulent, WBC 15000, ph less 7.0, glucose less than 50 mg/dL, LDH greater 1000 IU/L.
Thoracic Empyema-- Stage 3
• 1 week after infection-- collagen organization, entrapment the underlying lung.
• 3-4 week-- mature, turned peel. • Chronic-- dense fibrosis contraction and trapping
the lung, atelectasis and prolonged pulmonary infection, reduction the size of hemithorax.
• Fibrothorax-- invasion the chest wall and narrow the intercostals space-- As the end stage of the process.
Complication of Empyema
• Early or late.
• Necrosis of visceral pleura.
• Bronchopleural fistula.
• Necrosis parietal pleura and chest wall.
• Osteomyelitis of rib or spine.
• Esophageal fistula.
• Metastatic spread ( brain abscess ) .
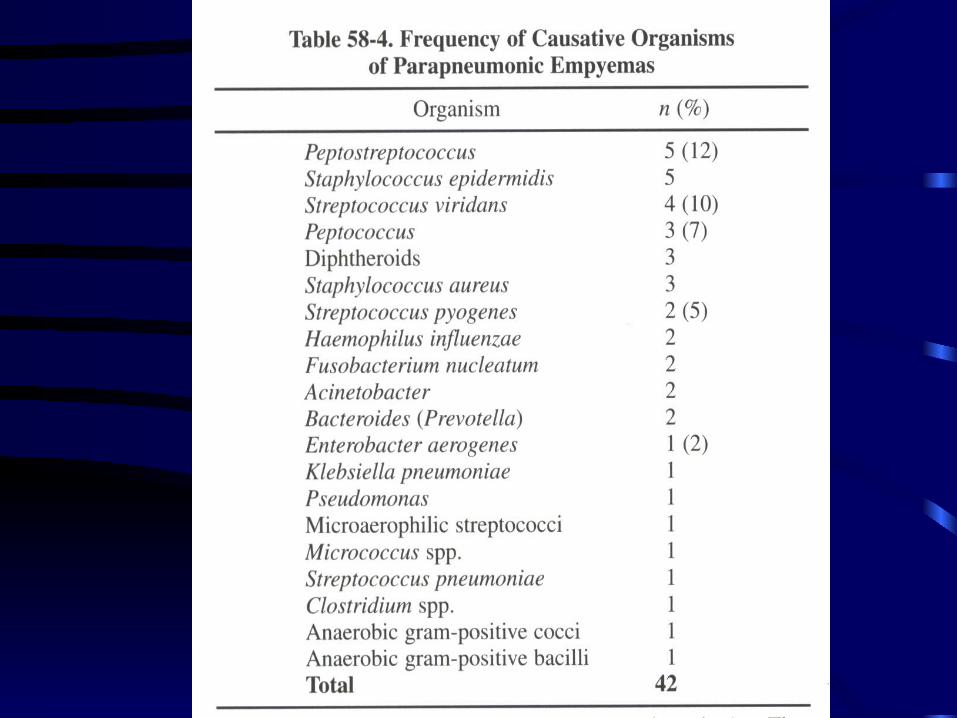
BACTERIOLOGY
• Before antibiotics ( 1941 ) , 10% pf pneumonia develop the empyema, the streptoccus and pneumococcus were most frequently.
• After antibiotics, the empyema decrease as mortality. Staphylococcus became the most prevalent.
• Recently, the penicillin-resistant staphylococcus, gram’s –negative, anaerobic been predominant microbes.
BACTERIOLOGY
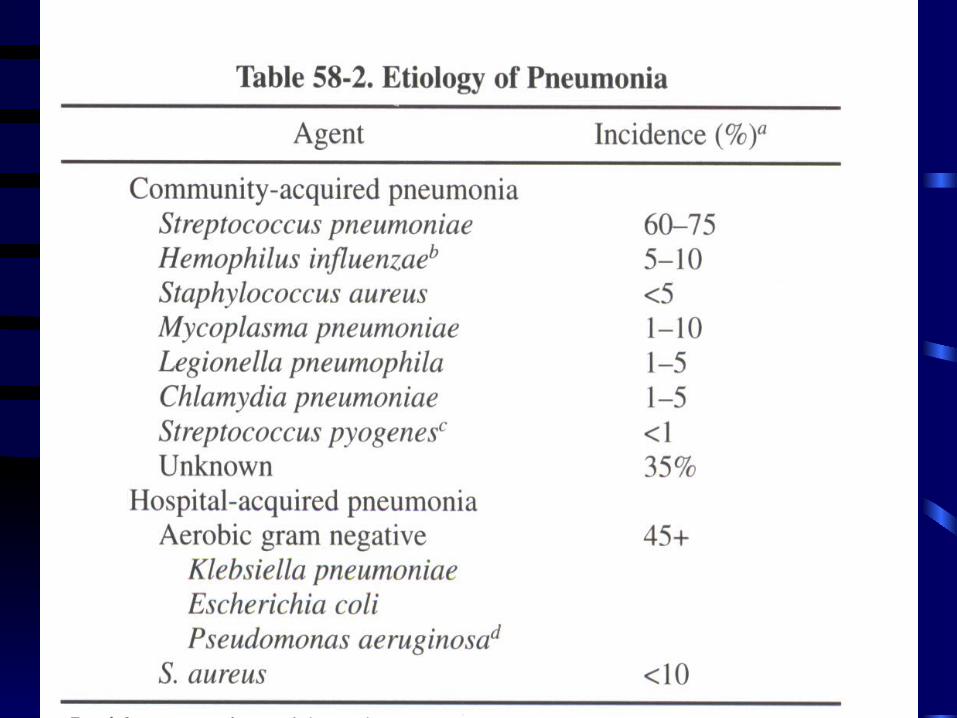
• Predominant aerobic-- Streptococcus pneumonia, Staphylococcus aureus, E. coli, Klebsiella pneumoniae, Hoemophilus influenzae.
• Predominat anaerobic-- Anaerobic cocci, pigmented prevotella, porphyromonas, bacteroid fragilis, fusobacterium spp.
BACTERIOLOGY
• Older children-- Most commonly caused by pneumococcus.
• Child-- 40% empyema caused by S. pneumoniae, 15% were penicillin-resistant, 44% negative culture ( pretreatment with antibiotics in community setting ) .
BACTERIOLOGY
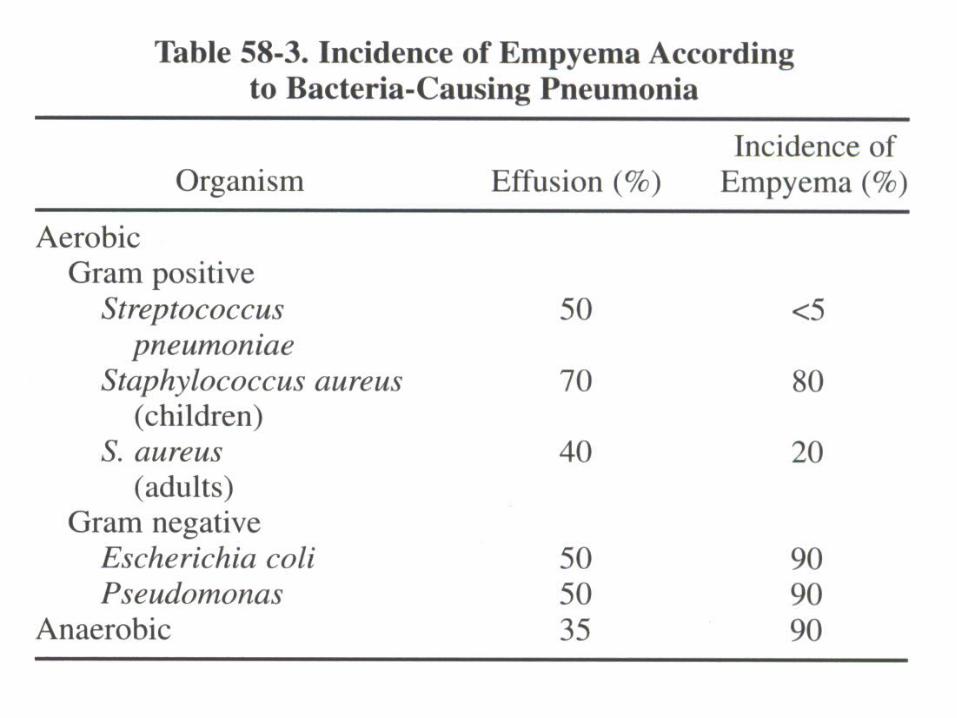
• S. pneumoniae responsible for 60%-75% community acquired pneumonia, only 2% develop empyema.
• S. aures account 1-2% community-acquired pneumonia, 10% adult and 50% children develop empyema.
• In hospital, the staphylococcus and gram’negative are most common.
CLINICAL FEATURE
• Shortness of breath, cough , chest pain-- common to pneumonia.
• Febrile respiratory illness, accentuation, prolongation the symptoms in pneumonia-- alert the possibility of empyema.
• Aerobic empyema-- acute febrile illness. • Anaerobic empyema-- more indolent,
usually 10 days.
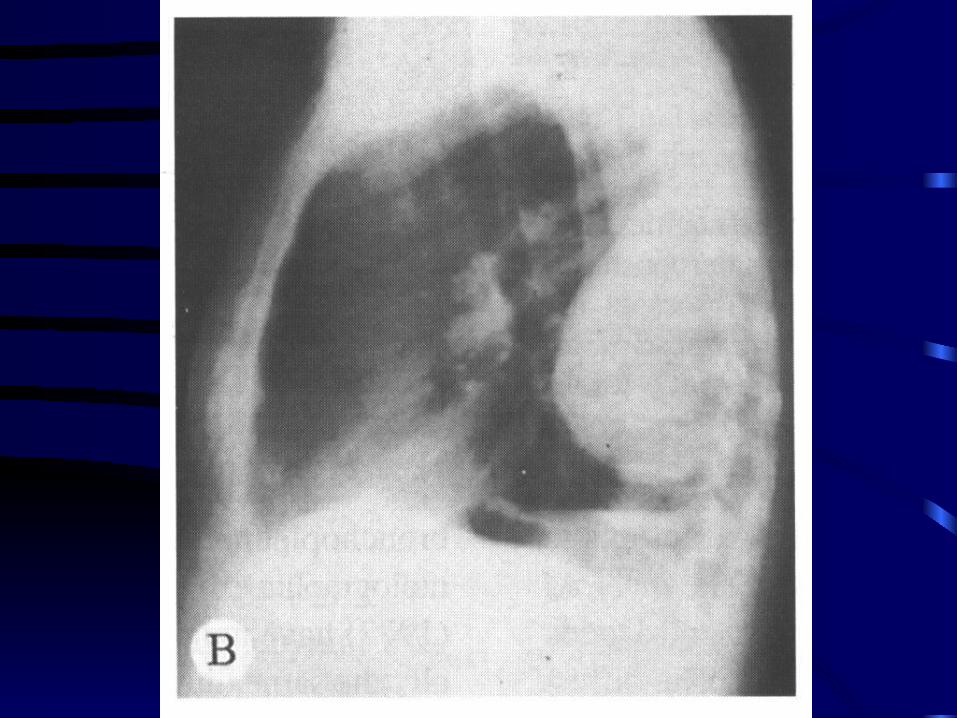
DIAGNOSIS
• Chest x-ray—The posterior lateral diaphragmatic angle-- The most dependent position-- Most empyema are found. (Inverted D or pregnant lady sign).
• Sonography– guide thoracocentesis. • Fluid analysis. • Aerobic pus-- little odor. • Anaerobic-- foul smelling.
Differential diagnosis
• Lung abscess.
• Bronchopleural fistula.
• Lung abscess-- air-fluid level in both PA and lateral view.
• Empyema-- air-fluid level rare in same in these view.
MAMAGEMENT
• Effective management require:
1) Control infection and sepsis by antibiotics.
2) Evacuation of pus from pleural space.
3) Obliteration the empyema cavity.
﹡Delay in drainage increase mortality from 3.4% to 16%.
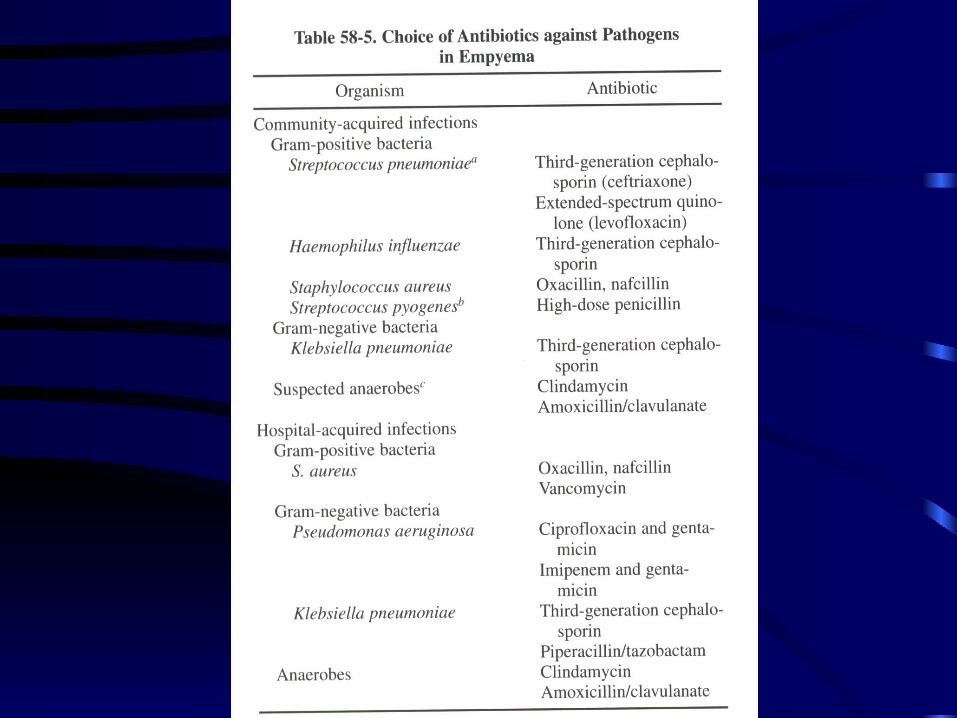
Antibiotics Therapy
• Blood, empyema culture, gram stain.
• Community-acquired--- Third-generation cephalosporin or clindamycin.
• Gram negative or anaerobes-- third generation cephalosporin and clindamycin.
• Hospital-acquired-- should guide by culture.
Thoracocentesis
• 18-gauge needle.
• Fluid analysis.
• Chest x ray repeated in 24 hours.
• Repeated thoracocentesis if volume increased.
Chest tube drainage
• First step in treatment of acute empyema. • Highly effective in treating-- Uncomplicated
parapneumonic effusion and classic empyema without loculation.
• 36 Fr, suction –20 cmH2O.
• Clinical improve in 48-72 hour.• Remove-- drainage less than 50 ml within 24 hour,
lung re-expansion. Usually within 5-10 day. • Antibiotics should continue 6 week.
Intrapleural fibrinolytic agents
• Empyema cavity– Composed of fibrin. • Fibrolysis agent—Streptokinase and
Streptodornase— Significant systemic reaction, unsatisfactory.
• Purified streptokinase, urokinase– Not allergic– • Success rate– 80% for streptokinase ( 250000
U/100ml normal saline ) , 90% for urokinase ( 100000U/100ml normal saline ) .
Open drainage
• Cutting off the chest tube a few centimeter from the skin.
• Anchoring it with safety pin and tape.
• Tube may withdrawn a few centimeter each week as the granulation tissue fill the tract.
Video-assisted thoracoscopy ( VATS )
• Primary modality for treating complicated empyema after initial therapy.
• Adhesiolysis and débridement with better exposure and mini-thoracotomy, decortation for lung expansion.
• Higher successful rate ( 90% ) , shorter hospital stay, less cost.
• Three-port triangle approach. • Morbidity low, chest tube can be removed 3-4 day.
Chronic Empyema.
• Chronicity– continued infection associated with both fibrosis and bronchopleural fistula.
• Uncommon.
• Thoracotomy and decortication
• Empyemectomy.
• Thoracoplasty.
EMPYEMA IN CHILDREN
• Associated with pneumonia.
• Incidence– Decrease greatly in successful treatment of pneumonia with antibiotics.
• Past– H. influenzae, β-hemolytic streptococci, S. pneumoniae, anaerobes.
• Recently– S. pneumoniae, often penicillin resistant is most.
EMPYEMA IN CHILDREN
• S/S– Fever, cough, dyspnea, tactile and vocal fremitus tachypnea, tachycardia.
• Goal of therapy– Antibiotics, chest tube drainage, aggressive care.
• Early thoracotomy– Led early recovery and excellent long-term results.
• VATS. • Open drainage– Not indicated-- because of late
skeletal deformities. • Enzyme– Not used.