Embed Size (px)
Citation preview

This article was downloaded by: [Tufts University]On: 07 October 2014, At: 03:22Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
European Journal of Special NeedsEducationPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rejs20
Parents’ view of respite careservices for families with childrenwith disabilities in SwedenJane Brodin a & Sanja Paulin aa Stockholm Institute of Education , SwedenPublished online: 09 Jul 2006.
To cite this article: Jane Brodin & Sanja Paulin (1997) Parents’ view of respite care servicesfor families with children with disabilities in Sweden, European Journal of Special NeedsEducation, 12:3, 197-208, DOI: 10.1080/0885625970120303
To link to this article: http://dx.doi.org/10.1080/0885625970120303
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information(the “Content”) contained in the publications on our platform. However, Taylor& Francis, our agents, and our licensors make no representations or warrantieswhatsoever as to the accuracy, completeness, or suitability for any purposeof the Content. Any opinions and views expressed in this publication are theopinions and views of the authors, and are not the views of or endorsed by Taylor& Francis. The accuracy of the Content should not be relied upon and should beindependently verified with primary sources of information. Taylor and Francisshall not be liable for any losses, actions, claims, proceedings, demands, costs,expenses, damages, and other liabilities whatsoever or howsoever caused arisingdirectly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expresslyforbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
European Journal of Special Needs Education, Vol. 12, No. 3 (1997), pp. 197-208© 1997 Routledge 0885-6257
Parents' view of respite care services forfamilies with children with disabilities in
Sweden
JANE BRODIN AND SANJA PAULIN
Stockholm Institute of Education, Sweden
Address for correspondence:Jane Brodin, Department of Special Education, Stockholm
Institute of Education, PO Box 47 308, S-100 74 Stockholm, Sweden. Tel: +46 8 737 96 26;Fax: +46 8 737 96 30; e-mail: [email protected].
ABSTRACT
In Sweden respite care is a legal right for families of children with disabilities.The Act Concerning Support and Service for Persons with Certain FunctionalImpairments (LSS) was passed in 1994. A previous study on respite care illuminatedthe municipalities' view of the service. This article focuses on the parents' view. Thestudy is based on questionnaire responses from 141 families and interviews with25 families. The results show that there is a widespread perception by familiesthat there is not enough support and that the need for respite care is not met. Thereis also a lack of information about the service. More flexible, family-orientedapproaches are needed.
KEYWORDS
Respite care service, short-term service, family support, social service, children withdisabilities
INTRODUCTION
Families of children with special needs require different kinds of social support inorder to live on an equal footing with other families and to be able to participate insociety. A well-functioning respite care service is often a prerequisite for the familyto have enough strength for demanding nursing work and for good parenting(Brodin, 1991). In Sweden respite care is a legal right for families of children with
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014

198 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
disabilities (LSS, 1994). From a study of children with severe intellectual impair-ments and multiple disabilities and their families, it appeared that there was agreat need for respite care as there is a risk that these families will otherwisebecome isolated from friends. The parents stated that it was not only that otherpeople - i.e. friends, neighbours and acquaintances - avoided them, but that theyoften found they consciously avoided being with other families with children(Brodin, 1991).
Children with disabilities are in contact with different experts from early on. Inspite of this, the parents are central to the child's development (Roden, 1989;Wachtel, 1995). Staff often experience a challenge in their efforts to give parents anindependent life and to support their family relations. As one parent said: 'Pleasetake good care of us parents. Remember that we shall last for the whole life'(Saetersdal, 1989, p. 33).
Many parents describe that for many years they have taken two steps forwardand one step back. Also when they later on have reached psychical balance theyhave a temporary relapse when something happens that reminds them of what lifecould have been if the child had not been disabled (Bakk and Grunewald, 1993,p. 145).
The family's perspective on support has different dimensions, for example, theroles of different family members and those of peripheral participants, the respon-sibility and influence of the parents and the well-being of the whole family as a unit.This means that a holistic view has to be taken in families with a child withdisability, and that a more family-oriented view would be best for the family.However, the most important requirement for all children with severe disabilities isa stable family and feeling of belonging.
Parents of children with severe disabilities need respite care support fromsociety and need to be offered alternative solutions and possibilities to influencehow and when the service should be given in order to meet the needs of the family.Grunewald and Leczinsky (1994) stress that family members, relatives, friends andneighbours take the responsibility for a great part of the service, and sometimes itis reasonable to argue that the efforts from society complement the work of therelatives and not the opposite.
Several studies emphasize families' need for respite care (e.g. Brodin, 1996;Lindblom and Moller, 1993; Robinson, 1994; Salisbury, 1990). A study conductedin 245 municipalities, in Sweden, illustrated how the municipalities met the needsof families with children with disabilities with regard to respite care. The resultsshowed that the service was offered to all families in need of support, and in 67 percent of the municipalities the service was given free of charge. In some cases, itseemed to be more difficult to receive help if you had a child with severe disabilitiesor with medical handicaps. Whether or not a family was satisfied with the serviceseemed to be connected to the possibility of influencing decisions taken concerningtheir own lives - e.g. to choose day and time for using the service, and to choosethe staff who look after their child (Brodin, 1996). A complementary study wasmade on the parental perspective to examine how respite care meets the needs ofparents with children with disabilities (Paulin, 1996), and a study was also madeon staff aspects of respite care (Claesson, 1996).
AIMS AND METHOD
The aim of this paper is to increase the knowledge of respite care from a parentalperspective - i.e. parents' need for respite care, how respite care functions, if there
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
Respite care in Sweden: parents' views 199
is a goal description and if the municipality has evaluated the service. The study isbased on a questionnaire (Brodin, 1995), with 32 questions sent out through threeof the main handicap associations to families with children, adolescents and adultswith severe disabilities (see Appendix). The questions cover qualitative and quanti-tative aspects of the service - e.g. how many hours the service may be used, howmuch does the service cost, when can you obtain the service, are you satisfied withthe service and can you choose staff?
The questionnaires were sent out by post to all families who were membersof any of these handicap associations in Skaraborg County Council in Sweden;358 questionnaires were posted with return envelopes to the families and there were141 responses. It appeared from a telephone conversation with a representativeof one of the handicap associations that many of the parents were members of twoor all three handicap associations and thus received two or three questionnaires,but answered only one. The aim of this procedure was, however, to preserve secrecyand integrity for the families and, consequently, the number of responses was lessthan expected compared with the questionnaires distributed. Data from the ques-tionnaires were compiled and illustrated in tables. The items in the tables here havebeen numbered in parentheses, in order to make it possible to check questions inthe Appendix; some of the questions are not illustrated in the tables, but reportedin the text.
All parents were asked if they were interested in participating in an interviewand 58 (41 per cent) agreed to be interviewed. Twenty-five families with childrenof varying ages and disabilities were selected to participate in the interviews. Thesefamilies had between them 29 children. Three families had 2 children with dis-abilities, and one family had 2 foster children with disabilities. The selection of thefamilies was made with the aim of obtaining a broad geographical cover fromthe council, which consisted of 17 municipalities. All interviews except one weretape recorded. One parent did not want to participate if the interview was recorded,due to earlier negative experiences, and in this case notes were taken instead.The interviews were transcribed immediately in order to facilitate the processing.The comments from the parents have been translated into English, and the quo-tations throughout the text are reproduced as close to the original utterances aspossible.
RESULTS
Results from the Questionnaire
Data from the questionnaire was, as mentioned earlier, compiled and illustratedin tables, followed by comments from the parents. Out of the 358 distributedquestionnaires, the number of replies was 141. Some of the questions are closelyrelated to the disability law (LSS), which was passed on 1 January 1994. The resultsfrom the questionnaire shown in the tables cover only the answers 'yes'> ' n o 'and 'do not know'. The remaining numbers - i.e. those who did not reply to thequestion - are excluded from the tables and, consequently, the tables do not sumto a total of 141 replies to all questions. In some cases, the families have given twoanswers to the same question.
The results from the questionnaire revealed that there is a confusion regardingthe concept of respite care among parents. Some families confused respite careservice with short-term homes and support families. However, respite care is aseparate service in the Disability Act, which makes it possible to receive support
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
1035514913231498
49961642431710
261117018421009351108
200 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
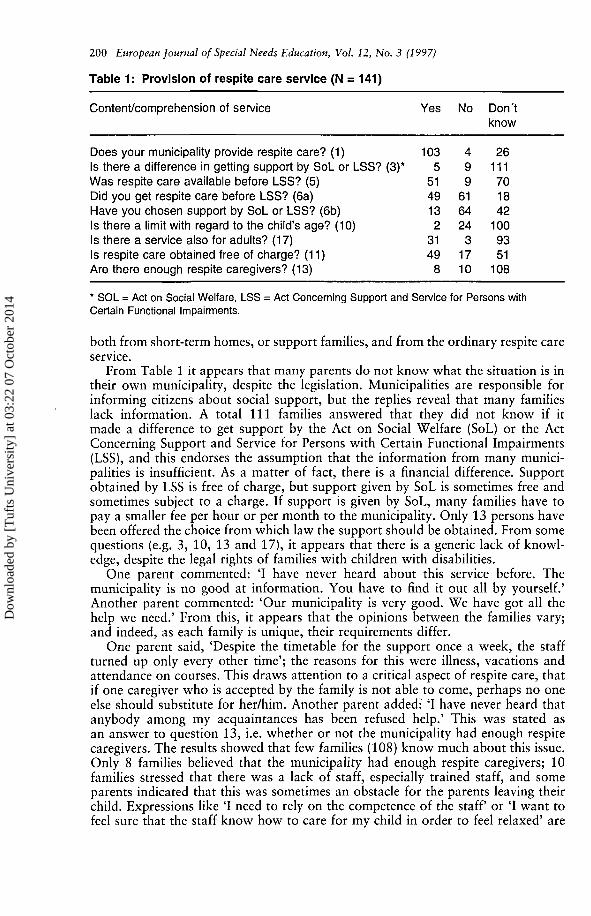
Table 1: Provision of respite care service (N = 141)
Content/comprehension of service Yes No Don'tknow
Does your municipality provide respite care? (1)Is there a difference in getting support by SoL or LSS? (3)*Was respite care available before LSS? (5)Did you get respite care before LSS? (6a)Have you chosen support by SoL or LSS? (6b)Is there a limit with regard to the child's age? (10)Is there a service also for adults? (17)Is respite care obtained free of charge? (11)Are there enough respite caregivers? (13)
* SOL = Act on Social Welfare, LSS = Act Concerning Support and Service for Persons withCertain Functional Impairments.
both from short-term homes, or support families, and from the ordinary respite careservice.
From Table 1 it appears that many parents do not know what the situation is intheir own municipality, despite the legislation. Municipalities are responsible forinforming citizens about social support, but the replies reveal that many familieslack information. A total 111 families answered that they did not know if itmade a difference to get support by the Act on Social Welfare (SoL) or the ActConcerning Support and Service for Persons with Certain Functional Impairments(LSS), and this endorses the assumption that the information from many munici-palities is insufficient. As a matter of fact, there is a financial difference. Supportobtained by LSS is free of charge, but support given by SoL is sometimes free andsometimes subject to a charge. If support is given by SoL, many families have topay a smaller fee per hour or per month to the municipality. Only 13 persons havebeen offered the choice from which law the support should be obtained. From somequestions (e.g. 3, 10, 13 and 17), it appears that there is a generic lack of knowl-edge, despite the legal rights of families with children with disabilities.
One parent commented: 'I have never heard about this service before. Themunicipality is no good at information. You have to find it out all by yourself.'Another parent commented: 'Our municipality is very good. We have got all thehelp we need.' From this, it appears that the opinions between the families vary;and indeed, as each family is unique, their requirements differ.
One parent said, 'Despite the timetable for the support once a week, the staffturned up only every other time'; the reasons for this were illness, vacations andattendance on courses. This draws attention to a critical aspect of respite care, thatif one caregiver who is accepted by the family is not able to come, perhaps no oneelse should substitute for her/him. Another parent added: 'I have never heard thatanybody among my acquaintances has been refused help.' This was stated asan answer to question 13, i.e. whether or not the municipality had enough respitecaregivers. The results showed that few families (108) know much about this issue.Only 8 families believed that the municipality had enough respite caregivers; 10families stressed that there was a lack of staff, especially trained staff, and someparents indicated that this was sometimes an obstacle for the parents leaving theirchild. Expressions like 'I need to rely on the competence of the staff or 'I want tofeel sure that the staff know how to care for my child in order to feel relaxed' are
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
Respite care in Sweden: parents' views 201
typical examples of comments from parents. One mother stressed, 'I think it takesa very long time to find a suitable respite family. There are few of them, and there-fore you have to start looking for one in due course.'
One question (no. 9) was about the accessibility of the service, that is who couldbenefit from the service. Results revealed that respite care service was availablevariously for all families with children and adolescents with severe disabilities (51);only families with children with mental retardation (11); only families with childrenwith severe motor disabilities (10); primarily families with children with multipledisabilities (14); families with children with social difficulties (9); or families withchildren who receive support by LSS (39). Thirty-one families did not reply to thisquestion, thus some families had given more than one answer. Respite care isadministered by the child care service (14), by the home-help service (41) or bya special body in the municipality (27); 63 persons replied that they did not knowwhich body administered it. Some parents argued that they were not satisfiedwith the 'home-help solution', as many of the staff had insufficient knowledge andexperience of children and normally worked with elderly people.
The service is based on the individual needs of the family, which means that thenumber of hours' support varies; however, most families received support forbetween 20 and 30 hours per month. Some families had no time limit and couldthus use the service for as many hours as they needed. They pointed out that therewas no risk of over-consumption of the service, even if it was free of charge: 'Whowants to have strangers at home if there is no real need for it?' asked a parent.
One mother commented that her family had been allowed respite care, but themunicipality had not yet been able to find a caregiver competent in sign languagein order to communicate with her child. It is reasonable to believe, then, that themore specific the requirements on the staff, the more difficult it is to find a respitecaregiver.
One question (no. 14) was related to the disability of the child and whether/how this influenced the opportunities to receive support. The results show that27 families believed that the disability of the child made no difference, 10 familiesargued that it was more difficult where a child had profound mental retardationor severe multiple disabilities and 12 families stated that it is more difficult wherea child had medical disabilities or invisible disabilities. The reply frequency to thisquestion was low; one reason for this could be that only families who had experi-enced difficulties in obtaining support actually answered the question.
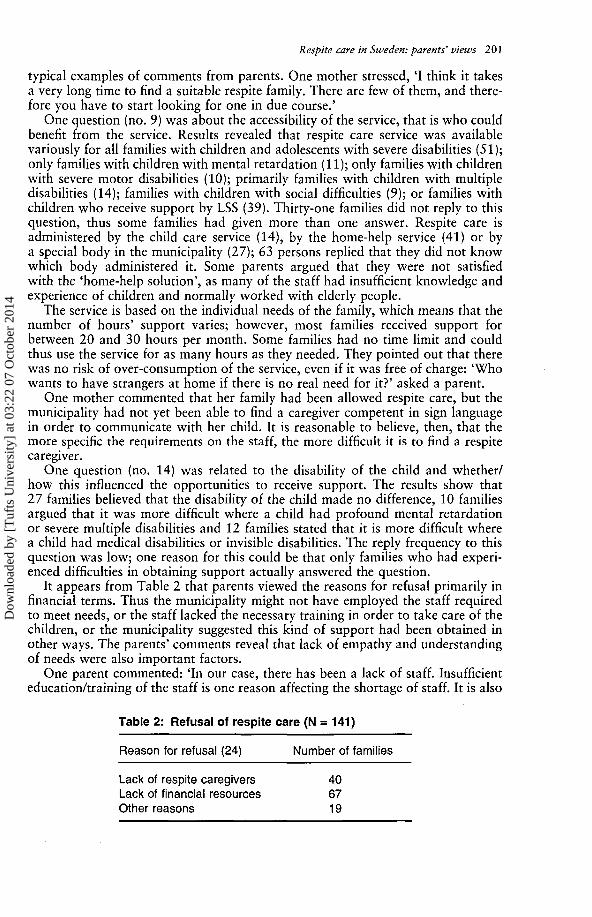
It appears from Table 2 that parents viewed the reasons for refusal primarily infinancial terms. Thus the municipality might not have employed the staff requiredto meet needs, or the staff lacked the necessary training in order to take care of thechildren, or the municipality suggested this kind of support had been obtained inother ways. The parents' comments reveal that lack of empathy and understandingof needs were also important factors.
One parent commented: 'In our case, there has been a lack of staff. Insufficienteducation/training of the staff is one reason affecting the shortage of staff. It is also
Table 2: Refusal of respite care (N = 141)
Reason for refusal (24) Number of families
Lack of respite caregivers 40Lack of financial resources 67Other reasons 19
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
5810
1935
00
20107
6287
85110111
202 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
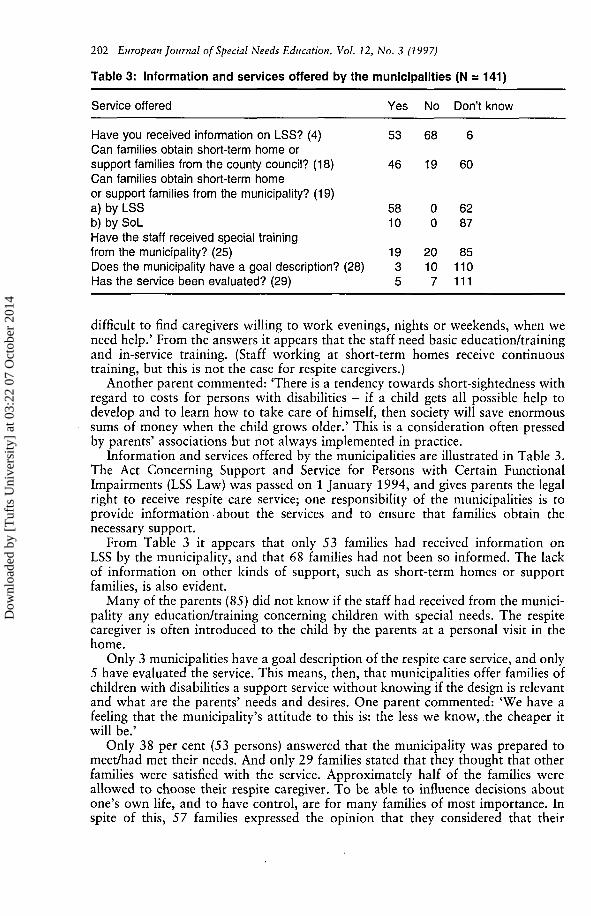
Table 3: Information and services offered by the municipalities (N = 141)
Service offered Yes No Don't know
Have you received information on LSS? (4) 53 68 6Can families obtain short-term home orsupport families from the county council? (18) 46 19 60Can families obtain short-term homeor support families from the municipality? (19)a) by LSSb) by SoLHave the staff received special trainingfrom the municipality? (25)Does the municipality have a goal description? (28)Has the service been evaluated? (29)
difficult to find caregivers willing to work evenings, nights or weekends, when weneed help.' From the answers it appears that the staff need basic education/trainingand in-service training. (Staff working at short-term homes receive continuoustraining, but this is not the case for respite caregivers.)
Another parent commented: 'There is a tendency towards short-sightedness withregard to costs for persons with disabilities - if a child gets all possible help todevelop and to learn how to take care of himself, then society will save enormoussums of money when the child grows older.' This is a consideration often pressedby parents' associations but not always implemented in practice.
Information and services offered by the municipalities are illustrated in Table 3.The Act Concerning Support and Service for Persons with Certain FunctionalImpairments (LSS Law) was passed on 1 January 1994, and gives parents the legalright to receive respite care service; one responsibility of the municipalities is toprovide information about the services and to ensure that families obtain thenecessary support.
From Table 3 it appears that only 53 families had received information onLSS by the municipality, and that 68 families had not been so informed. The lackof information on other kinds of support, such as short-term homes or supportfamilies, is also evident.
Many of the parents (85) did not know if the staff had received from the munici-pality any education/training concerning children with special needs. The respitecaregiver is often introduced to the child by the parents at a personal visit in thehome.
Only 3 municipalities have a goal description of the respite care service, and only5 have evaluated the service. This means, then, that municipalities offer families ofchildren with disabilities a support service without knowing if the design is relevantand what are the parents' needs and desires. One parent commented: 'We have afeeling that the municipality's attitude to this is: the less we know, the cheaper itwill be.'
Only 38 per cent (53 persons) answered that the municipality was prepared tomeet/had met their needs. And only 29 families stated that they thought that otherfamilies were satisfied with the service. Approximately half of the families wereallowed to choose their respite caregiver. To be able to influence decisions aboutone's own life, and to have control, are for many families of most importance. Inspite of this, 57 families expressed the opinion that they considered that their
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
3853
7
2975
424
132
75
8549
2
9040
Respite care in Sweden: parents' views 203
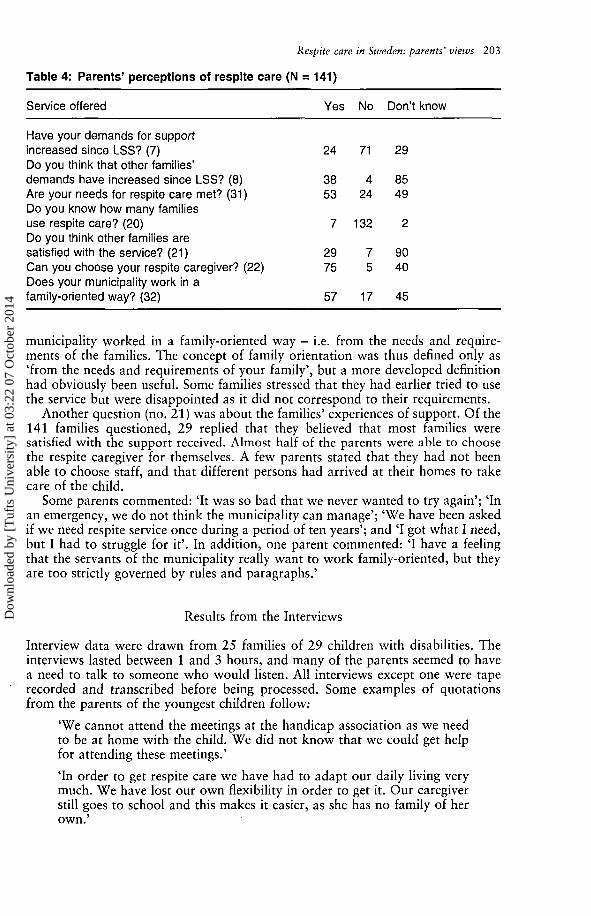
Table 4: Parents' perceptions of respite care (N = 141)
Service offered Yes No Don't know
Have your demands for supportincreased since LSS? (7) 24 71 29Do you think that other families'demands have increased since LSS? (8)Are your needs for respite care met? (31)Do you know how many familiesuse respite care? (20)Do you think other families aresatisfied with the service? (21)Can you choose your respite caregiver? (22)Does your municipality work in afamily-oriented way? (32) 57 17 45
municipality worked in a family-oriented way - i.e. from the needs and require-ments of the families. The concept of family orientation was thus defined only as'from the needs and requirements of your family', but a more developed definitionhad obviously been useful. Some families stressed that they had earlier tried to usethe service but were disappointed as it did not correspond to their requirements.
Another question (no. 21) was about the families' experiences of support. Of the141 families questioned, 29 replied that they believed that most families weresatisfied with the support received. Almost half of the parents were able to choosethe respite caregiver for themselves. A few parents stated that they had not beenable to choose staff, and that different persons had arrived at their homes to takecare of the child.
Some parents commented: 'It was so bad that we never wanted to try again'; 'Inan emergency, we do not think the municipality can manage'; 'We have been askedif we need respite service once during a period of ten years'; and 'I got what I need,but I had to struggle for it'. In addition, one parent commented: 'I have a feelingthat the servants of the municipality really want to work family-oriented, but theyare too strictly governed by rules and paragraphs.'
Results from the Interviews
Interview data were drawn from 25 families of 29 children with disabilities. Theinterviews lasted between 1 and 3 hours, and many of the parents seemed to havea need to talk to someone who would listen. All interviews except one were taperecorded and transcribed before being processed. Some examples of quotationsfrom the parents of the youngest children follow:
'We cannot attend the meetings at the handicap association as we needto be at home with the child. We did not know that we could get helpfor attending these meetings.'
'In order to get respite care we have had to adapt our daily living verymuch. We have lost our own flexibility in order to get it. Our caregiverstill goes to school and this makes it easier, as she has no family of herown.'
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
204 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
'We have chosen respite care at home as we believe it is good for thechild to be at home as much as possible, but it is not easy to let some-one into your home. If you feel that you must show a very tidy houseeach time, it is not possible to have respite care at home. Sometimes wewould prefer not to have respite care at home.'
From the interviews with the parents of older children are the following:
'We have got five hours a week but we were never asked about our needsof support. We need more support.'
'Sometimes we would prefer to have respite care at home overnight.'
'The most important is that the right person looks after your child. Thepersonal chemistry must correspond.'
On the problem of obtaining a caregiver in emergency situations, one parentcommented:
'I wish we could have more free time. The acute situations which youcannot control, do not work as you have to plan your respite care inadvance.'
A lack of respite care is obvious during the summer vacation, when schools areclosed for 10 weeks:
'The 10 weeks he is away from school are like a nightmare. He misseshis peers and it is very difficult.'
Out of the 29 children involved in this study, 23 have a severe intellectualimpairment, often with additional disabilities. The families chose respite care athome because they wanted their child to be in a home environment; but theyrealized too that it was sometimes difficult having a stranger in their home.
Many of the parents interviewed said that they enjoyed a very close relationshipwith their child. Expressions like: 'When they look after my child, it feels as thoughthey were looking after me', clearly support this relation.
The need for support care exists not only in the daytime, but also in the evenings,at night and during weekends; but on these occasions, parents have sometimes metresistance in obtaining support. A system where the family must make a telephonecall each time they need help probably militates against using the service.
The interviews also highlighted the importance of empathy and awareness of theneeds of each family. Many parents searched for personal, flexible solutions, as eachfamily and child is unique. One of the parents said that their knowledge as parentsof a child with disability was not accepted or endorsed by the professionals.
DISCUSSION
The overall aim of this article has been to indicate and describe how respitecare services at home work for families of children with severe disabilities. Keyquestions have been the need for respite care; how respite care works; and the goaldescription and evaluations of those responsible for providing the service. The needfor respite care has been demonstrated in several studies (e.g. Brodin, 1995; Paulin,1996; Robinson, 1994; Wachtel, 1995).
One shortcoming concerns information about the service. Parents do not knowwhat kind of support is obtainable. When they do find out, many of them have a
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014

Respite care in Sweden: parents' views 205
struggle to obtain it. Using relatives, friends and neighbours as caregivers seemsto be common, but there is always a risk that the social responsibility may betransferred to the family (Grunewald and Leczinsky, 1994). The family has, ofcourse, the main responsibility for the well-being of their child, but social legisla-tion (LSS, 1994) has placed some responsibilities upon the municipalities. The aimmust be to find a balance between family responsibility and societal responsibility,in order to approach normalization - namely, to live in conditions equal to thoseof other families with children. Mutual goals should be set in collaborationwith family, staff and the municipality, and the starting-point for this must be theindividual needs of the family. A holistic view of the family is necessary as the firststep in developing an individual plan for each child (Claesson and Paulin, 1995).
One difficulty seems to be that of obtaining help in emergency cases, that is onoccasions not planned weeks in advance. This is probably a result of poor planningon the part of the municipalities. Few municipalities have goal descriptions for theirservice, and few have evaluated the service: they have not asked the parents whattheir needs are, nor have they asked the families' opinions on the municipalities'fulfilment of these needs.
Seventy-nine per cent of the families replied that they believed the main reasonfor refusal of support service is a lack of financial resources, but this is contra-dictory as families of children with severe disabilities are entitled to respite careservice by Swedish legislation (LSS, 1994). How can they then get support if themunicipality does not follow the law? Unfortunately, it seems impossible today todo anything about it; except to take the case to court and then wait a long time fora hearing and judgment. Even if the individual is found to be right, it does notalways bring the support requested. Legislation does not necessarily ensure justice,especially if it is without influence in daily life.
One limitation of this study is that the interviews were restricted to only onearea of the country and the situation might be slightly different in other places.However, previous studies of municipalities' views on respite care revealed nodifferences in other parts of the country (Brodin, 1995, 1996). Another limitationis that only 25 families were interviewed, but number of interviews is not the onlyway to decide how generic are the answers. Two sources were used for the datacollection, questionnaires and interviews; furthermore, the results from the parentalperspective can be compared with the municipal perspective.
In order to increase the quality of respite care services, the municipalities needto make an inventory of the needs of the families. What kind of support do theyneed?; when do they need support?; do parents have any suggestions on how todevelop the services?; and what education do parents require from caregivers?, aresome of the questions that must be put. Collaboration between all parties involvedin the support service (parents, caregivers and municipalities) is needed but the mostimportant task for providing a well-functioning respite care must be to listen to theparents. They are the ones who are going to use the service!
NOTE
The present article complements the earlier article: J. Brodin, 'Municipalities' viewof respite care service for families in Sweden: a comparison between two studies,European Journal of Special Needs Education, 11, 3, 330-336 (1996).
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
206 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
ACKNOWLEDGEMENT
The above studies have been supported by the Swedish National Inheritance Fund,and are part of the Family Support project (FAS), conducted in cooperation withWRP International (Women Researchers in Play and Disability).
REFERENCES
BAKK, A. and GRUNEWALD, K. (1993). Omsorgsboken [Book on care of persons withmental retardation]. Uppsala: Liber Utbildning.
BRODIN, J. (1991). Att tolka barns signaler. Gravt utvecklingsstorda flerhandikappadebarns lek och kommunikation [To Interpret Children's Signals. Play and Communicationin Children with Profound Mental Retardation and Multiple Disabilities], StockholmUniversity, Department of Education.
BRODIN, J. (1995). Avlosarservice som stöd till familjer med barn med funktionsnedsätt-ningar [Respite Care as Support for Families with Children with Disabilities], Report No.11, Stockholm Institute of Education, Department of Special Education.
BRODIN, J. (1996). 'Municipalities' view of respite care service for families in Sweden: acomparison between two studies', European Journal of Special Needs Education, 11, 3,330-336.
CLAESSON, I. (1996). Avlosarservice sedd ur avlösarens perspektiv. [Respite Care from aStaff Perspective], Report No. 17, Stockholm Institute of Education, Department ofSpecial Education.
CLAESSON, I. and PAULIN, S. (1995). Skolans/sarskolans and förskolans ansvar for barnmed funktionshinder [Responsibility of School and Preschool for Children withDisabilities]. Jonkoping: Jonkoping University College.
GRUNEWALD, K. and LECZINSKY, C. (1994). Handikapplagen [The Act on Disability].Stockholm: Gotab.
LINDBLOM, M. and MOLLER, A. (1993). 'Få handikappfamiljer får avlastningshjalp'['Few families get respite care'], Läkartidningen, 90, 12, 1182-1186.
LSS (1994). The Act Concerning Support and Service for Persons with Certain FunctionalImpairments. Stockholm: Government Printers.
PAULIN, S. (1996). Föräldrars syn på avlösning [Respite Care from a Parental Perspective],Report No. 18, Stockholm Institute of Education, Department of Special Education.
ROBINSON, C. (1994). 'Making the break from "respite care": a keynote review', BritishJournal of Learning Disabilities, 22, 42-45.
RÖDÉN, G. (1989). 'Förälldrautbildning vid omsorsverksamheten i Stockholms län' ['Parenteducation in the county of Stockholm']. In: ROREN, O. and WINLUND, G. (Eds) Motetmellan föräldrar och personal [The Meeting between Parents and Staff]. Stockholm: ALAFoundation, pp. 59-60.
SAETERSDAL, B. (1989). 'Öst är öst och väst är väst och aldrig mötas de två' ['East is eastand west is west and they never meet']. In: ROREN, O. and WINLUND, G. (Eds) Motetmellan foraldrar och personal. Stockholm: ALA Foundation, pp. 28-33.
SALISBURY, C. (1990). 'Characteristics of users and nonusers of respite care', MentalRetardation, 28, 5, 291-297.
WACHTEL, G. (1995). Respite care service for families with disabled members in Germany- a survey and some problems. Paper presented at Respite on Rendezvous Conference,Thunder Bay, Canada, 6-8 March 1995.
APPENDIX: QUESTIONS ON RESPITE CARE
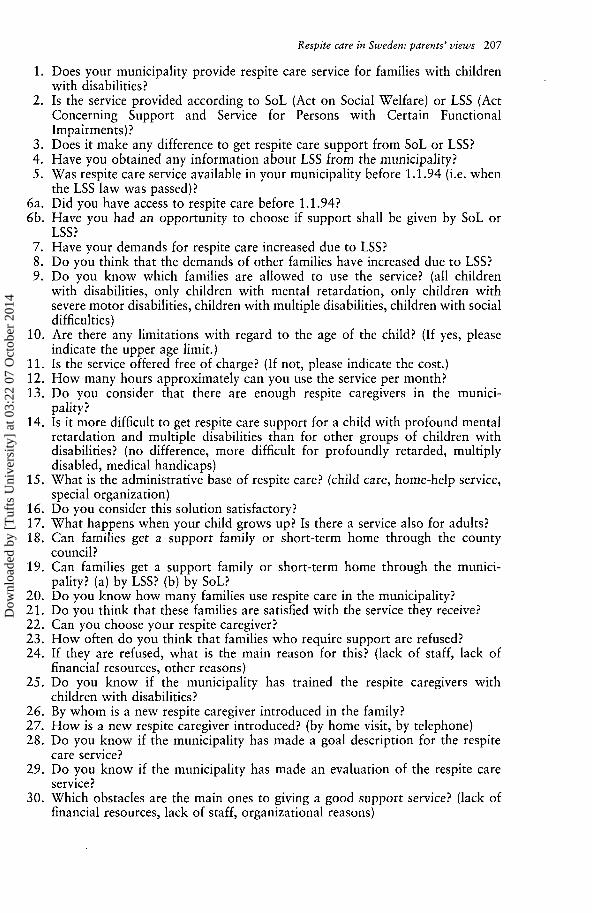
Most of the questions had triple-choice reply alternatives: 'yes', 'no', 'do notknow'. Below each question there was extra space for comments. The questionsare shortened and numbered in brackets in the tables.
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
Respite care in Sweden: parents' views 207
1. Does your municipality provide respite care service for families with childrenwith disabilities?
2. Is the service provided according to SoL (Act on Social Welfare) or LSS (ActConcerning Support and Service for Persons with Certain FunctionalImpairments)?
3. Does it make any difference to get respite care support from SoL or LSS?4. Have you obtained any information about LSS from the municipality?5. Was respite care service available in your municipality before 1.1.94 (i.e. when
the LSS law was passed)?6a. Did you have access to respite care before 1.1.94?6b. Have you had an opportunity to choose if support shall be given by SoL or
LSS?7. Have your demands for respite care increased due to LSS?8. Do you think that the demands of other families have increased due to LSS?9. Do you know which families are allowed to use the service? (all children
with disabilities, only children with mental retardation, only children withsevere motor disabilities, children with multiple disabilities, children with socialdifficulties)
10. Are there any limitations with regard to the age of the child? (If yes, pleaseindicate the upper age limit.)
11. Is the service offered free of charge? (If not, please indicate the cost.)12. How many hours approximately can you use the service per month?13. Do you consider that there are enough respite caregivers in the munici-
pality?14. Is it more difficult to get respite care support for a child with profound mental
retardation and multiple disabilities than for other groups of children withdisabilities? (no difference, more difficult for profoundly retarded, multiplydisabled, medical handicaps)
15. What is the administrative base of respite care? (child care, home-help service,special organization)
16. Do you consider this solution satisfactory?17. What happens when your child grows up? Is there a service also for adults?18. Can families get a support family or short-term home through the county
council?19. Can families get a support family or short-term home through the munici-
pality? (a) by LSS? (b) by SoL?20. Do you know how many families use respite care in the municipality?21. Do you think that these families are satisfied with the service they receive?22. Can you choose your respite caregiver?23. How often do you think that families who require support are refused?24. If they are refused, what is the main reason for this? (lack of staff, lack of
financial resources, other reasons)25. Do you know if the municipality has trained the respite caregivers with
children with disabilities?26. By whom is a new respite caregiver introduced in the family?27. How is a new respite caregiver introduced? (by home visit, by telephone)28. Do you know if the municipality has made a goal description for the respite
care service?29. Do you know if the municipality has made an evaluation of the respite care
service?30. Which obstacles are the main ones to giving a good support service? (lack of
financial resources, lack of staff, organizational reasons)
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014
208 European Journal of Special Needs Education, Vol. 12, No. 3 (1997)
31. Do you consider that your municipality will meet your needs/demands forrespite care service in the future?
32. Do you consider your municipality works in a family-oriented way, i.e. fromthe needs and requirements of your family?
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
03:
22 0
7 O
ctob
er 2
014