Embed Size (px)
Citation preview

scribed the case of a traumatic rupture of the ascendingaorta and aortic valve in a 56 year-old man followingblunt chest trauma sustained in a motor vehicle accident[3]. The classic radiologic sign of traumatic rupture of theaorta, a widened superior mediastinum, was completelyabsent despite the severe vascular injury which he hadsustained. More recently, Dunn and Williams describeda patient with an ascending aortic rupture sustained fromimpact with an air-bag during a motor vehicle accident[4]. Again, the chest radiograph demonstrated a normalmediastinum. In a recent review, Symbas and coworkersreported on three cases of traumatic rupture of theascending aorta and reported the literature on 17 others.In their review, most of the patients presented withmultiple trauma or signs of cardiac tamponade. Six of 14patients had a normal chest roentgenogram despite theunderlying injury [5]. In our patient, every chest radio-graph that was taken demonstrated a normal vascularpedicle with no change in the superior mediastinalshadow. Thus, classic imaging techniques may not besensitive enough to detect this type of injury, and mighthave contributed to the delay in his diagnosis. As theworkup progressed, the presence of a right pleural effu-sion on both chest roentgenogram and CT scan led toconfusion in the diagnosis. When the effusion was aspi-rated and found to be chylous in nature, the possibility ofa lymphatic duct injury was entertained. The transesoph-ageal echocardiogram was the first diagnostic test toclearly demonstrate the injury to the ascending aorta.Because the mechanism of injury this child sustainedusually causes injury at the aortic isthmus, an area notwell visualized by transesophageal echocardiography,the patient underwent cardiac catheterization. The aor-togram excluded a distal aortic transection.
This case represents an unusual decelerating injury tothe ascending aorta after heart transplant. It illustratesthat the clinical presentation may be itself atypical andpersistence in accurately determining the cause of anyunusual clinical findings is imperative and may be life-saving.
References
1. Cowley RA, Turney SZ, Hankins JR, Rodriguez A, Attar S,Shankar BS. Rupture of the thoracic aorta caused by bluntchest trauma: a fifteen year experience. J Thorac CardiovascSurg 1990;100:652–61.
2. Dowling RD, Baladi N, Zenati M, et al. Disruption of the aorticanastomosis after heart-lung transplantation. Ann ThoracSurg 1990;49:118–22.
3. Charles KP, Davidson KG, Miller H, Caves RK. Traumaticrupture of the ascending aorta and aortic valve followingblunt chest trauma. J Thorac Cardiovasc Surg 1977;73:208–211.
4. Dunn JA, Williams MG. Occult ascending aortic rupture inthe presence of an air bag. Ann Thorac Surg 1996;62:577–8.
5. Symbas PJ, Horsley WS, Symbas PN. Rupture of the ascend-ing aorta caused by blunt trauma. Ann Thorac Surg 1998;66:113–7.
6. Treasure T. Imaging the thoracic aorta in the injured patient.Heart 1997;78:207–8.
Partial Mitral Valve Replacementfor Acute EndocarditisJ. Mark Jones, AFRCS(Ed), and Mazin A. I. Sarsam,FRCS(CTh)
Department of Cardiac Surgery, Royal Victoria Hospital,Belfast, Northern Ireland
We present a case of acute endocarditis involving theposteromedial commissure and both leaflets of the mitralvalve, including a vegetation on and perforation of theanterior leaflet, in a young man with active Crohn’sdisease. Repair was performed using glutaraldehyde-treated bovine pericardium. Competence of the valve wasachieved with no recurrence of endocarditis. This casedemonstrates that extensive destruction of both leafletsof the mitral valve does not prohibit repair.
(Ann Thorac Surg 2001;72:255–7)© 2001 by The Society of Thoracic Surgeons
Mitral valve repair has gained increasing acceptanceas the procedure of choice for mitral regurgitation
[1]. It is also established as a treatment of acute infectiveendocarditis in the presence of abscess formation, septicemboli, conduction disturbance, or hemodynamic com-promise despite antibiotic therapy [2, 3]. However, repairhas not been described in the presence of extensiveinfection involving both leaflets of the mitral valve. Wepresent a case of successful repair of the mitral valve inthis situation.
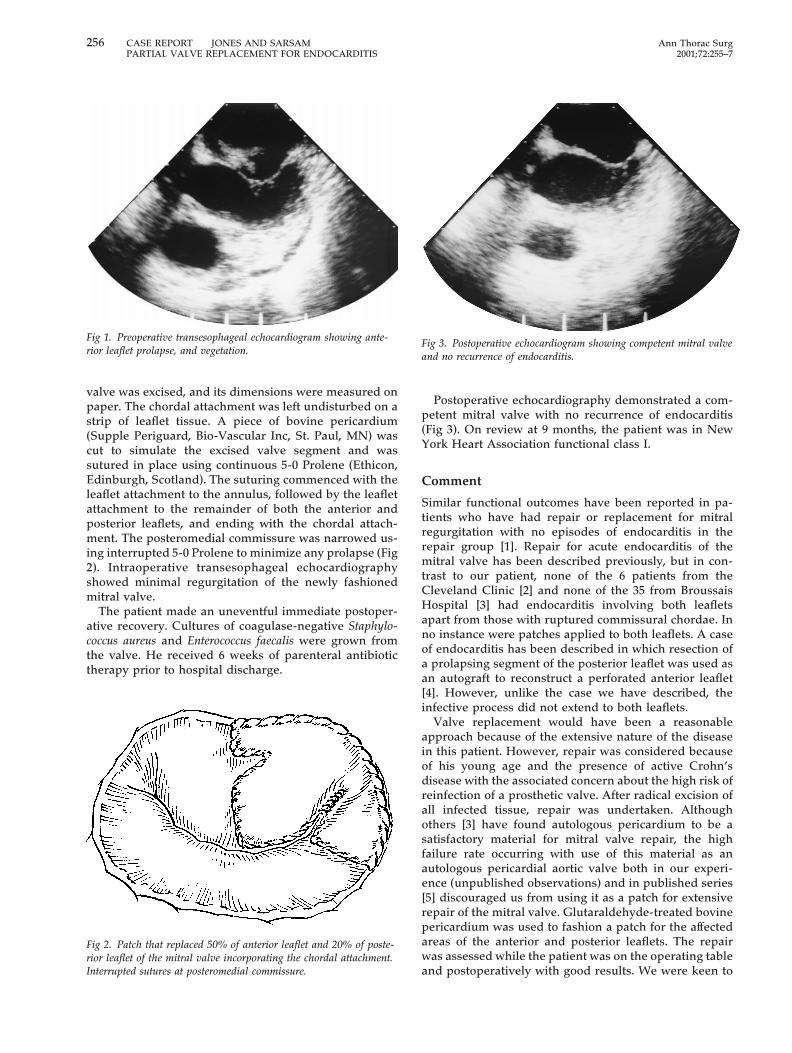
A 28-year-old man with active Crohn’s disease was seenwith a 2-week history of pyrexia, hemoptysis, pleuriticchest pain, and dyspnea. He had a systolic murmur andleukocytosis of 23 3 109/L. Colectomy and ileostomy hadbeen performed 7 years previously with subsequentreversal by ileorectal anastomosis 4 years later. He cur-rently had multiple perianal fistulas. Six months earlier,he had had a dental abscess drained. Blood cultures didnot identify any organisms. Transesophageal echocardi-ography demonstrated good left ventricular function,mitral regurgitation, anterior leaflet prolapse, and a veg-etation (Fig 1).
Urgent surgical intervention was advocated. Standardcardiopulmonary bypass was established, and a Cos-grove mitral valve retractor (Kapp Surgical InstrumentInc, Cleveland, OH) was used to aid access to the mitralvalve through the small left atrium. Endocarditis affected50% of the anterior leaflet with a vegetation and aperforation and 20% of the posterior leaflet including theposteromedial commissure. The damaged area of the
Accepted for publication June 3, 2000.
Address reprint requests to Dr Jones, Department of Cardiac Surgery,Royal Victoria Hospital, Grosvenor Rd, Belfast BT12 6BA, NorthernIreland; e-mail: [email protected].
255Ann Thorac Surg CASE REPORT JONES AND SARSAM2001;72:255–7 PARTIAL VALVE REPLACEMENT FOR ENDOCARDITIS
© 2001 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)02582-0
valve was excised, and its dimensions were measured onpaper. The chordal attachment was left undisturbed on astrip of leaflet tissue. A piece of bovine pericardium(Supple Periguard, Bio-Vascular Inc, St. Paul, MN) wascut to simulate the excised valve segment and wassutured in place using continuous 5-0 Prolene (Ethicon,Edinburgh, Scotland). The suturing commenced with theleaflet attachment to the annulus, followed by the leafletattachment to the remainder of both the anterior andposterior leaflets, and ending with the chordal attach-ment. The posteromedial commissure was narrowed us-ing interrupted 5-0 Prolene to minimize any prolapse (Fig2). Intraoperative transesophageal echocardiographyshowed minimal regurgitation of the newly fashionedmitral valve.
The patient made an uneventful immediate postoper-ative recovery. Cultures of coagulase-negative Staphylo-coccus aureus and Enterococcus faecalis were grown fromthe valve. He received 6 weeks of parenteral antibiotictherapy prior to hospital discharge.
Postoperative echocardiography demonstrated a com-petent mitral valve with no recurrence of endocarditis(Fig 3). On review at 9 months, the patient was in NewYork Heart Association functional class I.
Comment
Similar functional outcomes have been reported in pa-tients who have had repair or replacement for mitralregurgitation with no episodes of endocarditis in therepair group [1]. Repair for acute endocarditis of themitral valve has been described previously, but in con-trast to our patient, none of the 6 patients from theCleveland Clinic [2] and none of the 35 from BroussaisHospital [3] had endocarditis involving both leafletsapart from those with ruptured commissural chordae. Inno instance were patches applied to both leaflets. A caseof endocarditis has been described in which resection ofa prolapsing segment of the posterior leaflet was used asan autograft to reconstruct a perforated anterior leaflet[4]. However, unlike the case we have described, theinfective process did not extend to both leaflets.
Valve replacement would have been a reasonableapproach because of the extensive nature of the diseasein this patient. However, repair was considered becauseof his young age and the presence of active Crohn’sdisease with the associated concern about the high risk ofreinfection of a prosthetic valve. After radical excision ofall infected tissue, repair was undertaken. Althoughothers [3] have found autologous pericardium to be asatisfactory material for mitral valve repair, the highfailure rate occurring with use of this material as anautologous pericardial aortic valve both in our experi-ence (unpublished observations) and in published series[5] discouraged us from using it as a patch for extensiverepair of the mitral valve. Glutaraldehyde-treated bovinepericardium was used to fashion a patch for the affectedareas of the anterior and posterior leaflets. The repairwas assessed while the patient was on the operating tableand postoperatively with good results. We were keen to
Fig 1. Preoperative transesophageal echocardiogram showing ante-rior leaflet prolapse, and vegetation.
Fig 2. Patch that replaced 50% of anterior leaflet and 20% of poste-rior leaflet of the mitral valve incorporating the chordal attachment.Interrupted sutures at posteromedial commissure.
Fig 3. Postoperative echocardiogram showing competent mitral valveand no recurrence of endocarditis.
256 CASE REPORT JONES AND SARSAM Ann Thorac SurgPARTIAL VALVE REPLACEMENT FOR ENDOCARDITIS 2001;72:255–7
minimize insertion of foreign material, and as the repairwas satisfactory, there was no indication to perform anadditional annuloplasty either with a prosthetic ring orwith pericardium [6].
The principle for surgical treatment of endocarditis isexcision of all necrotic and infected tissue. Assessmentshould then be made regarding repair. We have shownthat despite active destruction of major segments of bothleaflets, repair can be achieved with excellent short-termresults in terms of functional status and freedom fromendocarditis in a patient at risk for recurrent endocarditis.
References
1. Sand ME, Naftel DC, Blackstone EH, Kirklin JW, Karp RB. Acomparison of repair and replacement for mitral valve incom-petence. J Thorac Cardiovasc Surg 1987;94:208–19.
2. Hendren WG, Morris AS, Rosenkranz ER, et al. Mitral valverepair for bacterial endocarditis. J Thorac Cardiovasc Surg1992;103:124–9.
3. Dreyfus G, Serraf A, Jebara VA, et al. Valve repair in acuteendocarditis. Ann Thorac Surg 1990;49:706–13.
4. Penta de Peppo A, Zeitani J, De Paulis R, Chiariello L.Autograft from quadrangular resection for floppy valve repairin endocarditis. Ann Thorac Surg 1998;66:270–1.
5. Gross C, Simon P, Grabenwoger M, et al. Midterm resultsafter aortic valve replacement with the autologous tissuecardiac valve. Eur J Cardio-thorac Surg 1999;16:533–9.
6. Scrofani R, Moriggia S, Salati M, Fundaro P, Danna P, SantoliC. Mitral valve remodeling: long-term results with posteriorpericardial annuloplasty. Ann Thorac Surg 1996;61:895–9.
Traumatic Papillary MuscleRuptureTimothy A. Simmers, MD, PhD, Huub W. J. Meijburg,MD, PhD, and Aart Brutel de la Riviere, MD, PhD
Departments of Cardiology and Cardiothoracic Surgery,Heart-Lung Institute, University Medical Center, Utrecht, TheNetherlands
Papillary muscle rupture caused by blunt chest trauma isa relatively rare cause of mitral incompetence. To dateonly 25 cases of surgically corrected posttraumatic mitralregurgitation have been reported, of which only eightresulted from rupture of the anterolateral papillary muscle.
(Ann Thorac Surg 2001;71:257–9)© 2001 by The Society of Thoracic Surgeons
Blunt chest trauma is a rare cause of acute mitralregurgitation. Sudden deceleration or compression
of the heart with subsequent damage to the closed
atrioventricular valve or subvalvular apparatus is re-sponsible; patients are thus generally motor vehicle ac-cident victims. Presentation, diagnosis, and treatment ofthis potentially fatal complication are illustrated by thefollowing case.
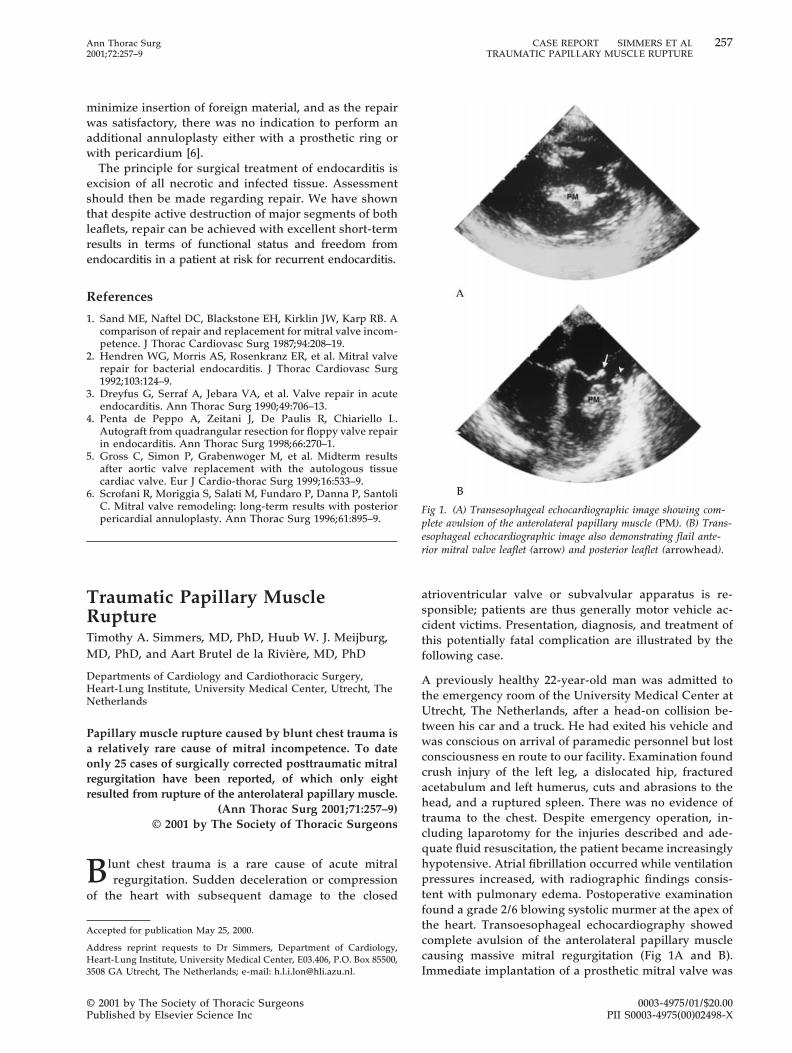
A previously healthy 22-year-old man was admitted tothe emergency room of the University Medical Center atUtrecht, The Netherlands, after a head-on collision be-tween his car and a truck. He had exited his vehicle andwas conscious on arrival of paramedic personnel but lostconsciousness en route to our facility. Examination foundcrush injury of the left leg, a dislocated hip, fracturedacetabulum and left humerus, cuts and abrasions to thehead, and a ruptured spleen. There was no evidence oftrauma to the chest. Despite emergency operation, in-cluding laparotomy for the injuries described and ade-quate fluid resuscitation, the patient became increasinglyhypotensive. Atrial fibrillation occurred while ventilationpressures increased, with radiographic findings consis-tent with pulmonary edema. Postoperative examinationfound a grade 2/6 blowing systolic murmer at the apex ofthe heart. Transoesophageal echocardiography showedcomplete avulsion of the anterolateral papillary musclecausing massive mitral regurgitation (Fig 1A and B).Immediate implantation of a prosthetic mitral valve was
Accepted for publication May 25, 2000.
Address reprint requests to Dr Simmers, Department of Cardiology,Heart-Lung Institute, University Medical Center, E03.406, P.O. Box 85500,3508 GA Utrecht, The Netherlands; e-mail: [email protected].
Fig 1. (A) Transesophageal echocardiographic image showing com-plete avulsion of the anterolateral papillary muscle (PM). (B) Trans-esophageal echocardiographic image also demonstrating flail ante-rior mitral valve leaflet (arrow) and posterior leaflet (arrowhead).
257Ann Thorac Surg CASE REPORT SIMMERS ET AL2001;72:257–9 TRAUMATIC PAPILLARY MUSCLE RUPTURE
© 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(00)02498-X





























