Embed Size (px)
Citation preview

THE INFLUENCE OF HYPERSENSITIVITY ON THEPATHOGENESIS OF OCULAR TOXOPLASMOSIS*
BY G. Richard O'Connor, MDt
ALTHOUGH THE PROTOZOAN PARASITE Toxoplasma gondii, or otherorganisms morphologically identical to it, for nearly half a century hasbeen known to cause a particularly destructive inflammatory diseaseof the eye, no unifying concept of the pathogenesis of this disease hasappeared in the literature. It seems both timely and appropriate tore-examine the theories of earlier workers in this field and to sum-marize the large volume of laboratory and clinical data that hasrecently become available on the role of hypersensitivity in oculartoxoplasmosis.When this is done, the following cardinal facts come to light:(1) Antimicrobial agents such as pyrimethamine, the sulfonamides,
and spiramycin - substances known to possess definite toxoplasma-static activity in acutely infected animals or in tissue cultures - pro-duce disappointing or highly unpredictable results in the treatmentof human ocular disease.
(2) Corticosteroids, ordinarily useful in quelling inflammation, pro-duce little effect on most toxoplasmic ocular lesions, and under certaincircumstances may, indeed, be responsible for the organism's acceler-ated proliferation.
(3) A considerable body of data suggests that immunologicallycommitted lymphocytes, rather than serum antibodies, are of primeimportance in the host's defense against the ravages of the parasite.The ever-increasing use of immunosuppressive agents (e.g., cytotoxicdrugs, total body irradiation, and antilymphocyte serum) in thetreatment of both inflammatory and neoplastic diseases increases the
*This work was supported in part by Program Grant EY 00310 from theNational Institutes of Health, Department of Health, Education and Welfare,Bethesda, Maryland.fFrom the Francis I. Proctor Foundation for Research in Ophthalmology and
the Department of Ophthalmology, University of California Medical Center,San Francisco, California.

G. Richard O'Connor
likelihood of undesirable complications from the suppression of lym-phoid cells. Once released from the influence of these cells, Toxo-plasma organisms might then be free to proliferate without inhibitionand to produce necrotizing lesions within the eye or elsewhere in thebody.
(4) The role of the Toxoplasma cyst has recently been seriouslyquestioned. Do cysts of the organism break down spontaneously inhuman retinas; and if so, what are the consequences?
(5) There is renewed interest in "toxotoxin," a substance (or groupof substances) supposedly liberated by the parasite into its immediateenvironment and said to be toxic to normal cells. Toxic destruction ofretinal cells, independent of actual penetration by the parasite, couldresult in alterations of tissue that would, perhaps, be unaffected bycorticosteroids or antimicrobial agents.The purpose of this paper is to explore the pathogenetic mechanisms
underlying the development of ocular lesions due to Toxoplasma infec-tion. Recurrent lesions will receive special attention, and the role ofhypersensitivity in producing them will be examined. A concertedeffort will be made to explain conflicting data presented by variousauthors in the past, and the relevance of these data to various formsof therapy will be discussed in the light of experiments recently per-formed by the author and his associates.
REVIEW AND DISCUSSION OF THE LITERATURE
RECOGNITION OF OCULAR TOXOPLASMA INFECIION
As long ago as 1908, Nicolle and Manceauxl described Toxoplasmaas an intracellular parasite of the gondi (a North African rodent),and recognized its two morphologically distinct forms. The crescent-shaped, proliferative form was rightly assumed to be the invader oftissue cells; and the encysted form, containing hundreds of organismsin a dormant or metabolically depressed state, was recognized as theend-stage of a multiplicative process within the tissues of the infectedhost. This encysted form was rightly assumed to play a major role inthe transmission of the disease. Its role in the production of inflamma-tory disease was not assessed, however.The Czechoslovakian ophthalmologist, Janku (1923) ,2 drew the
attention of the ophthalmic profession to organisms in the retinas ofinfants with macular "congenital colobomata" that were identical tothe organisms found by Nicolle and Manceaux in the gondi. Althoughno effort was made to subculture the organisms in susceptible test
502

Ocular Toxoplasmosisainimals or tissue cultures, they were seen in sections of what wouldnow be considered the typical lesions of congenital toxoplasmosis.After Janku's report, the production of ocular lesions by Toxoplasmawas largely ignored until 1939, when Wolf, Cowen and Paige3 de-scribed chorioretinitis in an infant who died of neonatal encephalitisattributable to Toxoplasma. The details of the ocular lesions werestudied carefully by Koch,4 who noted that proliferation of the parasitetook place only in the retina despite the obvious inflammatory involve-ment of contiguous tissues.
In the ten-year interval that followed, little thought was given tothe possibility that Toxoplasma could be the cause of retinochoroiditisin the adult. Had it not been for the now classical works of Wilder5and of Jacobs, Bickerton, and Fair,6 focal exudative retinochoroiditisof the type currently considered to be typical of ocular toxoplasmosismight have continued to be associated with the "popular" diseasecategories of the day: namely, tuberculosis and lues. Indeed, thevery tissue sections formerly used by the us Armed Forces Instituteof Pathology to illustrate the histopathology of tuberculous chorio-retinitis were later found to contain Toxoplasma organisms.Wilder5 described organisms morphologically identical to Toxo-
plasma gondii in tissue sections from 53 adult eyes. It was especiallyinteresting that the patients' Toxoplasma dye-tests were generallylow in titer, but that all were positive. In addition to the cystic formof the organism, Wilder also found evidence of the proliferative formin sections of eyes removed from patients with chronic progressiveinflammatory disease.
Jacobs, Bickerton, and Fair6 adduced truly convincing evidence ofthe role of Toxoplasma gondii in adult retinochoroiditis. They ob-tained an eye that had been removed from a patient with massive, long-standing retinochoroiditis, severe secondary glaucoma, and intractablepain. The eye was hemisected, and half of the globe was submitted toroutine fixation and histopathologic examination. The soft tissues ofthe other half were minced and injected into embryonated chickeneggs, tissue cultures, and susceptible mice. Viable organisms, typicalof Toxoplasma, grew in each of these media; and one of the chickembryos developed an ocular lesion. Although the latter circum-stance may have been fortuitous, Jacobs, Bickerton, and Fair havecome closer than any other investigators to fulfilling Koch's postulatesfor ocular toxoplasmosis. It is noteworthy that their patient alsoshowed proliferative forms of the organism in tissue sections of theretina.
503

G. Richard O'Connor
By injecting minced ocular tissues into susceptible test animals, itis possible to recover Toxoplasmna organismis from eyes affected bytwo categories of disease: (1) chronic progressive inflammatorydisease, and (2) inactive disease characterized by atrophic, pigmentedscars. A scanning of the literature5"7"31"33 shows that the proliferativeform of the organism is found more commonly in tissue sections ofeyes with chronic progressive disease, and that the cystic form isfound more commonly in eyes with inactive disease. Neither categorycan be associated with a particular level of serum dye-test reactivity,although Desmonts7 maintains that the serum dye-test tends to behigher in patients with chronic progressive disease.
Dye-test antibodies represent one of a number of types of circulat-ing antibodies to Toxoplasma. It is not the purpose of this paper,however, to discuss the nature of the Toxoplasma dye-test reaction(Sabin-Feldman test)8 or the immune responses of the body as awhole to Toxoplasma infection. Dye-test antibodies represent a formof immediate hypersensitivity; and as such, they will concern us inboth this section and the section devoted to our own experimentalstudies.
HYPERSENSITIVITY TO TOXOPLASMA
The work of many investigators7"16"9' 20 provides evidence that Toxo-plasma infection gives rise to both immediate and delayed hypersensi-tivity reactions. Hypersensitivity is defined here as an increased reac-tivity to an antigen as a consequence of previous exposure to it. Inimmediate hypersensitivity reactions, pathologic lesions are initiatedthrough the activity of circulating antibody. Contact of the latter withantigen may trigger a number of immediate reactions ranging fromacute systemic anaphylaxis to the Arthus phenomenon.9 This type ofreactivity is transmissible to otherwise normal animals by passiveimmunization, e.g., the intravenous injection of serum from a previ-ously infected animal into a normal animal.Delayed hypersensitivity, on the other hand, is a cell-mediated form
of immunity which is usually caused by prolonged exposure of thehost to an infectious agent or to a hapten-protein complex of largemolecular size. This hypersensitivity is not transmissible by transfusionof serum into a normal animal. Intradermal injection of the offendingantigen into a sensitive subject results in the production of a typical,erythematous, indurated lesion of the skin after 48 to 72 hours. Thistype of reaction, in which cells of the mononuclear series participatepredominantly, is represented by the tuberculin skin test. It is also
504

Ocular Toxoplasmosis
the typical response of the uvea to many types of chronic infection,including toxoplasmosis.
Toxoplasmic retinochoroiditis and hypersensitivity.Frenkel10 is largely responsible for the promulgation of a theorythat links recurrent toxoplasmic retinochoroiditis with hypersensitivityphenomena in the retina and uvea. Frenkel, like most other authors,has assumed that the initial ocular lesions result from the invasion ofretinal cells by rapidly multiplying organisms. After a period ofmultiplication of variable duration, the parasites enter a cystic phase,and the lesion becomes quiescent. Recurrence of the inflammation hasbeen thought by some observers to occur after spontaneous ruptureof the cysts, but the cause of the rupture never has been determined.Frenkel postulates that when the cyst ruptures, its contents arespilled into the surrounding retinal tissues. Organisms liberated bythis process fail to invade previously uninvolved retinal cells, however,because of protective immune reactions established at the time of theinitial infection. Frenkel states that the exuberant, relatively short-lived inflammatory reaction, so characteristic of the recurrent lesion,is the result of a hypersensitivity reaction in the area of cyst rupture,antigen having been liberated from the cyst into highly sensitizedtissues.
This attractive hypothesis, based largely on Frenkel's" observationsof the cysts of Besnoitia jellisoni in hamster eyes, has provided therationale for most of our current systemic therapy of ocular toxoplas-mosis. It has provided the basis for Desmonts'7 interpretations of anti-body tests, which he performs simultaneously on aqueous humor andserum samples; by comparing the results on the two samples, he claimsto be able to discern the stage and prognosis of a given patient'sdisease. It is implicit in Spalter's'2 rationale for the prophylactictreatment of patients with recurrent retinal inflammatory disease bylaser coagulation, and in Beverley's"3 advocacy of systemic corticos-teroid therapy in recurrent inflammations due to toxoplasmosis.
Frenkel's argument is weakened somewhat by a number of clinicalobservations. It has often been noted that recurrent lesions are neitherself-limited nor short-lived. They often progress to large, fulminatinglesions that resist massive doses of systemic corticosteroids and resultin disastrous complications, such as retinal detachment and severesecondary glaucoma.The recurrent lesion often produces extensive retinal necrosis, yet
histological sections show an almost exclusively mononuclear cell
505

G. Richard O'Connor
infiltrate. As a general rule, hypersensitivity reactions are not followedby necrosis unless polymorphonuclear leukocytes constitute a signifi-cant proportion of the lesion's cell population. The Arthus reaction,for example, represents a typical, acute, necrotizing hypersensitivityreaction in which polymorphonuclear leukocytes always participate.They are also the cells seen in great numbers in the recurrent Besnoitialesions described by Frenkel.1" His illustrations show them invading aruptured cyst where they presumably participate in the elimination ofdead organisms and possibly of antigen-antibody precipitates. Butsince polymorphonuclear leukocytes are not characteristic of therecurrent lesions seen in human or animal eyes infected with Toxo-plasma, one is led to speculate that even in the recurrent lesions,necrosis may be attributable to proliferative activity of the parasiteitself.
Frenkel" does not exclude this possibility, for he shows in one ofhis illustrations the invasion of a few retinal cells by organisms newlyliberated from a ruptured cyst. His contention, however, is that thereaction is for the most part an acute hypersensitivity phenomenonbrought about by the release of antigen in the tissues of a hypersensi-tive individual.
It should also be stated, in some defense of Frenkel, that underspecial circumstances delayed hypersensitivity reactions may result inthe destruction of cells. Rosenau and his group14 have presented evi-dence that sensitized lymphocytes may destroy target cells in tissueculture; and Cohn and Wiener15 have shown that macrophages con-tain lysosomes capable of liberating hydrolases in tissue. It seems pos-sible, therefore, though not probable, that delayed hypersensitivityreactions could result in the destruction of tissue through the agencyof lymphoid cells alone.Van Metre and his group"6 have shown that focal exudative retino-
choroiditis of the type considered typical of toxoplasmosis can becorrelated with a positive toxoplasmin skin-test in about 95 per centof cases. This is an indication that delayed hypersensitivity to theantigens of Toxoplasma is widespread among patients with oculartoxoplasmosis, but nothing can be said of the role that this plays inthe eye disease itself.The same is true of the Toxoplasma dye-test,'7 the hemagglutination
test,18 the available tests for precipitating antibody to Toxoplasma,19'20and the complement-fixation test.2' The first two of these are almostroutinely positive in patients with the clinical picture of ocular toxo-plasmosis. In Van Metre's series,16 the Toxoplasma dye-test of Sabin
506

Ocular Toxoplasmosisand Feldmian was positive at a titer of 1:8 in 95 per cent of thepatients with presumptive ocular toxoplasmosis. The blood samplesof such patients usually have comparable titers (within one four-folddilutioni) of hemagglutinating antibodies, although Lunde andJacobs'2) maintain that one antigen is responsible for dye-test anti-bodies and another for hemagglutinating antibodies.By contrast, the complement fixation reaction and the precipitin
reaction are often negative in ocular toxoplasmosis. O'Connor19 hasfound the precipitin reaction positive in only 10 per cent of hispatients with typical ocular toxoplasmosis, and of these the majorityshowed very weak reactions in a test that was running according tohis modification of the Ouchterlony technique.'3 In this connection,it should be noted that the majority of serological tests for toxoplas-mosis indicate low titers in patients who are asymptomatic except forocular manifestations. This was particularly true of Wilder's24 seriesof 53 documented cases in which the dye-test was usually positive ata dilution of 1:32 or lower, and in some cases at only 1:2. Since thetime of Wilder's publication, Zscheile25 has demonstrated numerousorganisms in the retina of a patient whose serum dye-test was posi-tive only in the undiluted serum; and Franceschetti2", has isolated theparasite from the subretinal fluid of a patient whose serum dye-testwas absolutely negative. Desmonts7 has stated that the majority ofadults with ocular toxoplasmosis are suffering from a chronic form ofthe infection, whether this is acquired disease or congenital diseasein late relapse. Whatever the case, it would appear that the ocularlesion plays only a minor role as a source of antigenic stimulation forthe body as a whole.
Generally speaking, the titer of serum antibody cannot be corre-lated wvith the degree of activity or the size of the ocular lesion insuspected toxoplasmlosis. Since this disease is basically a systemicdisease affecting many different tissues, precipitous rises of antibodytiter are much more likely to be associated with acute lymph nodeinvolvement27 than with changes in the activity of an ocular lesion.As will be discussed later, immediate hypersensitivity of the typerelated to circulating antibody has a limited but definite role to playin the ocular disease.Although ocular lesions can generally be shown to be independent
of the level of Iunmoral antibody in the serum, the same is probablynot true of aqueous humor obtained by paracentesis of the anteriorchamber. O'Connor"1 was able to show precipitating antibodies toToxoplasta in the aqueous humor of patients whose sera were nega-
507

G. Richard O'Connor
tive for precipitins. Desmonts,7 in turn, showed that dye-test anti-bodies were actually formed in the eye, presumably by lymphoid cellsof the anterior uvea. His proof rested on the fact that more antibodyper unit of gamma globulin could be found in the eye than one wouldanticipate on the basis of altered vascular permeability. Particularly inthe subsiding phase of an attack of recurrent uveitis, Desmonts founda much higher ratio of antibody per unit of gamma globulin in theaqueous humor than in the serum. That it is largely plasma cells inthe ciliary body and iris that are responsible for antibody productionseems clear from the work of Witmer28 and Silverstein.29 Silverstein,moreover, has postulated that the act of antibody formation itself,together with the proliferative cellular events that accompany it, maybe the essential feature of recurrent anterior uveitis.
Toxoplasmic iridocyclitis and hypersensitivity.Although the proliferation of Toxoplasma organisms has never beenestablished in the anterior uveas of human subjects, iridocyclitis is afrequent accompaniment of the retinochoroiditic lesions consideredtypical of the disease. Usually mild and self-limited, it occasionallypursues a stormy course that results in an outpouring of many mono-nuclear cells and fibrinous exudate into the anterior chamber, synechiaformation, and acute secondary glaucoma. Since organisms cannot befound in the anterior uveas of these patients, it seems reasonable topostulate that some form of immune mechanism is responsible for theanterior signs of the disease. This classical view, which has been heldby Woods30 and others,31 will be referred to later in connection withthe author's experimental work.
Toxoplasmic perivascular inflammation and hypersensitivity.In addition to focal necrotizing retinochoroiditis and a granulomatousform of iridocycitis, perivascular inflammation of the retinal vesselshas been noted by many authors, including Wilder,32 Zimmerman,33and Hogan.34 Cuffs of mononuclear cells surround the retinal vesselsat irregular intervals, giving an ophthalmoscopic picture suggestingwidely spaced beads knotted along the course of a slender thread.Although Woods35 described this condition as a periphlebitis, manyobservers34'36 have found the retinal arterioles more often involvedthan the venules. The affected arterioles are usually in the vicinity ofa fresh or recurrent retinochoroiditic lesion and are never seen in theabsence of focal activity somewhere in the retina. Organisms have not
508

Ocular Toxoplasmosis
been identified in these cuffs of exudate. The reaction has been re-garded as immunologic, but the basis for it has not been delineated.Of parallel interest is the perivascular inflammation around the
choroid plexus of the third ventricle that Frenkel" observed in thebrains of congenital toxoplasmosis victims. Since free antigen is knownto be present in the ventricular fluid, and since high levels of antibodycould be detected in the circulating plasma. Frenkel assumed that thisform of inflammation was immunogenic in nature, related perhaps tothe precipitation of antigen-antibody complexes in the walls of thechoroid plexus vessels. It is, of course, tempting to extend these obser-vations to retinal vessels, assuming that a freely diffusable antigencan make its way to the surface of the affected vessels from a nearbylesion.
Toxoplasmic papillitis and hypersensitivity.Optic neuritis, or more specifically papillitis, has been described asa complication of ocular toxoplasmosis.37 Although the inexperiencedobserver sometimes mistakes juxtapapillary retinochoroiditis for atrue papillitis, it appears that there are certain bona fide cases ofclassical optic neuritis due to toxoplasmosis. Both Berengo and Frez-zotti38 of Sienna, and Manschot and Daamen39 of Holland have de-scribed direct involvement of the optic nerve by the parasite. Havingdemonstrated the parasites in the spinal fluid of patients thus affected,Berengo and Frezzoti felt that neuro-ophthalmic toxoplasmosis wasa special entity. They also suggested that the optic nerve was theroute of entry for such infections into the eye.An alternative theory is that the capillary network of the optic
nerve head, including its feeder vessels from the posterior ciliaryarteries, is the special target of antigen-antibody reactions of thetype described above. Such reactions appear to result in considerableswelling of the optic nerve head and occasionally in small hemorrhages.
"TOXOTOXIN" AND TOXOPLASMA LYSATES
No discussion of the pathogenesis of ocular toxoplasmosis would becomplete without some mention of the toxic theory of cell damage.Weinman and Klatchko40 described a heat-stable toxin derived fromthe peritoneal exudates of mice infected with Toxoplasma. This sub-stance, later referred to as "toxotoxin," produced immediate lethalconvulsions in mice when injected into their tail veins. It was precipi-tated in 50 per cent saturated ammonium sulfate solution and was
509

G. Richar(l O'Connor
sensitive to the digestive action of trypsin. Heating it to 560 c for30( minutes had a potentiating effect. Subsequent studies, includingthose of Varela4l and of Nozik and O'Connor42 showed that the lethaleffect of this substance could not be attributed clirectly to a specifictoxin secreted by Toxoplasmna itself, since viscous peritoneal fluidstimulated by other means produced the same effect. Furthermore,supernatant fluids from tissue cultures of Toxoplasma, known to con-tain the soluble antigens of Toxoplasnma, failed to produce lethalconvulsions in mice.
In the meantime, Zardi et al.43 revived interest in a substance whichthey also called "toxotoxin." Prepared from the supernatant fluid ofinfected mouse peritoneal exudate, this material was first absorbedby mixing it with antimouse guinea pig spleen cells. It was thoughtto be free of all contaminating mouse proteins. The physical andchemical properties of this substance were described by Zardi et al.,43and still later, Hogan and Zardi44 injected it into the eyes of rabbitsand other experimental animals. Histological studies on these eyesshowed a marked inflammatory response and severely destructivechanges in the tissues. The likelihood that these changes were not theresult of an exotoxin of Toxoplasmna, however, will be discussed in alater section.
Hansson45 has produced convincing evidence that lysosomes arepresent in the cytoplasm of Toxoplasnma organisms. This information,coupled with Lund's46 earlier data on the acid phosphatases of Toxo-plasina, may furnish a key to the method by which Toxoplasma pene-trates the host cells. There is no indication, however, that the phos-phatases are secreted into the external environment of the parasitein the way, for example, that the lytic toxins of Clostridium speciesare secreted. Furthermore, the substances described by Hansson andLund may bear no relationship to the toxic substances describedearlier by Lunde and Jacobs.47 These latter investigators showed thatlysates of carefully purified suspensions of Toxoplasmiia organismsproduced death in rabbits when injected intravenously. The animalsappeared to be perfectly well during the first few hours after injec-tion, but became comatose at about 18 hours and died shortly there-after. Although the pathogenesis of this phenomenon was not ex-plained, the effect of injected lysates was certainly different from theeffect of Weiman's "toxotoxin." Significant, perhaps, is the fact thatanimals previously immunized by low-grade Toxoplasnma infectionswere resistant to the lethal effects of intravenously injected lysate.This may indicate that certain toxic substances are neutralized by
510

Ocular Toxoplasmosiscirculating antibody. In Ino casc were ocular lesionis produced by tllesystemic adimiinistration of lysates.
HUNIORlAL AND CELLULAR IMMUNITY: TIIE RIOLE OF l)ELAYED)
HYPERSENSITIVITY
Studies on the protective nature of humoral and cellular immunityhave a bearing on the problem of ocular hypersensitivity to Toxo-plasma. From the studies of Foster and MIcCulloch48 it seemCls clearthat circulating antibody itself cannot protect an animiial fromn infec-tion nor hinder the multiplication of the organism within tissues. Anever enlarging body of evidence indicates that celluilacr immumnity (dce-layed hypersensitivity) is responsible for keeping the infection at bayin chronically infected human subjects or animals. According to thisconcept, the sensitized lymphocyte in some way inhibits the multipli-cation or penetrating ability of the organism. It is known from thework of Rosenau and Moon14 that the sensitized lymphocyte can pene-trate target cells and destroy them. Although it seems unlikely thatsensitized lymphocytes could penetrate the cysts of Toxoplasma, it isentirely possible that they could pcnetrate the proliferating form ofthe organism or the infected host cell.There is now abundant evidence that chronically infected, asymto-
matic individuals may suffer exacerbationis of toxoplasmic diseasewith widespread destruction of their tissues when either disease orcertain therapeutic macasures alter the normlal response pattern oftheir lymphoid cells. Vietzke49 has demonstrated this again and againin adults with neoplasms of lymphoid origin, rainging from chroniclymphatic leukemia to Hodgkin's disease. Theologides51 has demon-strated it in multiple mycloma. Reynolds51 has described widespreadtoxoplasmosis in a renal transplant patienit who had reccived bothimmunosuppressive agents and corticosteroids in order to retardrejection of the graft; and similar phenomena have been describedby Deodhar.52 Frenkel.53 has shown that x-irradiation of hamsterschronically infected with Toxoplasma will result in a severe exacerba-tion of their systemic disease.
Simultaneous infection of the host by two differenit intracellularparasites may also permit widespread multiplication of Toxoplasma.This has been described in toxoplasmosis associated with cytomegalicinclusion disease,54 herpes simplex infection,55 and distemper.5; Prob-ably any disease state that diminishes the availability of immuno-competent lymphocytes at the site of multiplication of Toxoplasmaparasites may contribute to progressive toxoplasmic disease at that site.
511

G. Riclhard O'Connior
What the nature of the competition for these lmphocytes may beremains unkniown, anid the same is cz'rtainly true of the mneans bywhich immunocompetent lymphocytes may restrict the multiplicationof Toxoplasmna parasites.There are many investigators, including Remington,57 who doubt
that Toxoplasmna cysts ever rupture in tissue under normal circum-stances. Their spontaneous rupture in the human retina has certainlynever been documented. The proliferative form of the organism, onthe other hand, has been seen by Wilder5 and others3' in the chronicprogressive form of the retinal disease. It may very well be that Toxo-plasma, like herpes simplex virus, is present in many tissues in aslowly multiplying or latent form. It may also be that when changesoccur in the humoral or cellular factors that normally control theinfection, exacerbations of the disease may supervene.
EXPERIMIENTAL STUDIES
With this background of pertinent contributions from the literaturein mind, Dr Robert A. Nozik and I undertook a series of experimentson induced ocular toxoplasmosis in the rabbit. These experiments,which will be summarized below, were designed for the followingpurposes: (1) to define the normal course of experimental toxoplas-mic retinochoroiditis in the rabbit; (2) to study specifically controlledfactors that might be related to the recurrence of toxoplasmic retino-choroiditis; (3) to elucidate the role of hypersensitivity to the antigensof Toxoplasmia in ocular inflammatory disease; and (4) to providea standard model of toxoplasmic retinochoroiditis for the evaluationof various forms of therapy.
EXPERINIENT I: The Normal Course of Experimental Toxoplasmic Retino-choroiditis in the Rabbit.Alaterials atnd AMethodsCalifornia pigmented rabbits of both sexes, weighing 2-5 lbs at the timeof injection, were used for this experiment. Serum dye-tests were negativeon all animals. Chlorpromaziine, 2 mg, lb, was adminiistered intramuscularly15 to 30 minutes preoperatively. After inducing brief general anesthesiaby the intravenious administration of thiopental sodium (6 mg//lb), wemade a retrobulbar injection of 2 ml of 1 per cenit lidocainie in each eye.The right eye was then proptosed with a curved blunt metal probe, and
a 25-gauge needle attached to a Hamilton microliter syringe was passedaround the back of the globe. The sclera was engaged by the tip of theneedle at a point near the posterior pole. The tip was then advanced by
512

Ocular Toxoplasmosisgentle pressuire on the syrinige, the barrel of which was rotated in smallturns betweeni the operator's fingers. Finially, the bevel of the needle wasobserved by direct ophthalmoscopic examiination in the suprachoroidalspace (Figure 1). An assistant was then instructed to advance the plungerof the syringe so as to inject one microliter of a stuspension of approximately2000 Beverley str-ain Toxe plasma orgainisms (Figure 2), purified accord-ing to a method previously described by Nozik and O'Connor.58
FIGURE 1
Schematic diagram of injection site in the suprachoroidal space of the rabbit eye.
The left eye was similarly proptosed and injected with one microliterof a suspension of complete Freund's adjuvants - a procedure known toresult in a small, self-limited granuloma that eventuates in a discrete pig-mented scar. This lesion served as a control for the lesion produced in theright eye.
ResultsCLINICAL COURSE OF EXPERIMENTAL DISEASE. The rabbits recoveredfrom anesthesia in about 20 minutes and appeared completely normalfor the next three days. On or about the fourth day, retinal edemadeveloped in the right eye in a discrete area corresponding to the site
513

:..e._s ilL _rb..s-s s
*: ..
::.: .. .. :.
..: ...sE:f. ...e...>!::if ..;u;*:w:::;
*: . :X5g::
ffie
iE'U.. ..;>eAStS.Mk* .. : :.: :.: ::: : .:......... .. : .: . :. ...... ... ::.: t:
....
*.:::: :. :: ::*:: .: . :: :: ::... . :.:. .... . :.. w:
S::... ...... .. ... w= .......... .0:w s
...'K._ ;' ? . . 1r ...... ....SS '^F - ; s
.......... v s.
C
x-
.0
0
*4-1
0
0
Cd
0
40
CI
... .. .......... ............................. ..................... ................ .... ...... .... ........ .. ....... .. ... ........... ...... .... ..... ......... ....

Ocular Toxoplasnmosis
FIGURE 3
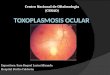
Rabbit fundus 6 days post-injection. N Mlyelinated fibers of optic nervehead. L Lesion with indistinct edges.
of injection. By the sixth or seventh day, this area showed a whiteinfiltrate with indistinct borders, clearly discernible against the back-ground of the pigmented fundus (Figure 3). At ten days, considerablecellular infiltration of the vitreous could be detected, and occasionallya serous detachment of the retina occurred. At no time, however, wasthe retinal lesion excluded from ophthalmoscopic view.The lesions usually reached a point of maximumii inflammatory
activity two to three weeks after injection (Figure 4). By thenthe vitreous was moderately hazy, and the anterior chamber showed1+ to 3+ cells and flare. The lesions began to subside spontaneouslythree to five weeks after injection, and by the end of two months hadconverted to atrophic, pigmented scars similar to those seen in humanlesions.
515

G. Richard O'Connor
FIGURE 4
Rabbit fundus 2 weeks post-inoculation. N Optic nerve head. L Toxo-plasmic lesion at height of inflammation.
Small, atrophic, pigmented scars developed in the control left eyesof all animals approximately two or three weeks after injection. In nocase wvas the vitreous clouded in these eyes (Figure 5).SEROLOGY OF EXPERINIENTAL DISEASE. The Toxoplasma dye-test waspositive in all animals injected, occasionally as early as the firt weekafter injection. The antibody titer often reached a level of 1:1024or higher, but the ocular lesions in animals with high titers were nomore severe than in animals with relatively low titers, e.g., 1:16.Precipitating antibodies to Toxoplasma could be detected in theserum of about 90 per cent of the animals by O'Connor's59 modifica-tion of the Ouchterlony technique.23 Here again there was no apparentcorrelation between the severity of the lesion and the antibody level.Precipitating antibodies appeared in the circulation four to eightweeks after injection, the time of appearance and level of antibodyvarying from animal to animal.
516

Ocular Toxoplasmosis
FIGURE 5
Left fundus 2 weeks post-inoculation. N Optic nerve head. FA Smalllesion produced by Freund's adjuvants.
HISTOLOGY OF EXPERIMENTAL DISEASE. The acute lesions showed grossthickening and infiltration of the retina by mononuclear cells, whichinvolved both the underlying choroid and sclera and the overlyingvitreous (Figure 6). The normal retinal architecture was completelydisrupted in the area of the lesion. Organisms were seen more oftenin the anterior layers of the retina than anywhere else (Figure 7). Theacute lesion was marked by dilatation of the capillaries in areas sub-jacent to the necrotic retina. The endothelial cells of these vessels wereswollen, and there was marked perivascular infiltration by round cells.Polymorphonuclear leukocytes were occasionally seen in the earlylesions and probably represented a response to the severe necrosis.The late lesions showed a thin, atrophic retina, occasionally reduced
to a thickness of only one or two cells. At the edges of the lesions,pigment accumulations could be seen in the deep layers of the retina
517

C.
:-
* - 4
.. - ~ ~~~C.. .i1
. s Q~~~c....)-
... *d
0-4* 0zco c
' :: 4-i..asmS~~~~~C.
o~~~~~~~~~L
% cB)s~~~r& ~~~~~~~~~.)
-4s': s .. cb.
I .:or
J. 1:. 1.

.cis
b.
... r ......
t.
.......usz

0
x
-
0
ctsc)CA
roo
* -
)0
0

Ocular Toxoplasmosis
(Figure 8), engulfed for the most part by macrophages. The retinalarchitecture in areas adjacent to the atrophic lesions was usually per-fectly normal. In this sense the lesions were strictly analogous to thehuman lesions described by Zimmerman.33The anterior eye was only mildly involved in the majority of cases.
Small collections of lymphocytes and plasma cells were seen in thestroma of the ciliary body and iris in the first few weeks of infection.In our animals, however, there was none of the severe granulomatousdestruction of the anterior uvea with synechia formation, neo-vascularization, and secondary glaucoma, that Jacobs60 produced byinjecting organisms directly into the anterior chamber.
FAILURE OF SPONTANEOUS RECURRENCE. Approximately 250 animals havenow been subjected to experimental ocular infections in the courseof a project that has lasted nearly three years. The periods of obser-vation have ranged from four months to a year and a half. As yetwe have not been able to document a single instance of spontaneousrecurrence of the ocular inflammation by serial ophthalmoscopicexamination. The vitreous of these animals has remained clear, andthe margins of the atrophic, pigmented lesions have remained sharplydemarcated from the normal surrounding retina.
Cysts could be seen in areas of uninflamed retina for as long asone year after the original inoculation of the eye. The viability of theparasite was proved by inoculating minced uveal tissues from theinfected rabbit eye into the peritoneal cavities of Swiss Webstermice that were dye-test negative. Seroconversion of these mice andthe subsequent recovery of viable Toxoplasma parasites from theirbrain tissues indicated the persistence of infective cysts in the eyesof our experimental rabbits.Although the experimental lesions became clinically quiet after
four to six weeks, and although the vitreous body was then crystalclear, histologic examination showed that nests of mononuclear cellspersisted for many months in the choroid subjacent to the retinalscars. For this reason the apparent resolution of the inflammatorylesion, as viewed through the ophthalmoscope, could not be reliedupon as an absolute criterion of inactivity.
CONCLUSIONS
Experimental toxoplasmic retinochoroiditis, analogous in many re-spects to the lesions seen in human subjects, can be produced in thepigmented rabbit. Although serologic data can be used to confirm
521

G. Richard O'Connor
infectionl in every case, no correlation canl be miiade between theactivity of the ocular lesioni and the level of the dye-test titer. Thesame is true of precipitating antibodies analyzed by double diffusionin agar. It seems likely that a generalized infection is set up at thetime of ocular inoculation, possibly as the result of escape of viableorganisms along the needle track. This was confirmed in one instanceby the isolation of viable organisms from the heparinized venousblood of a rabbit within one week after infection. If this is the case,the serum antibody level is much more likely to reflect the activityof the body's widespread reticuloendothelial organs than the activityof the ocular lesion. It seems almost a foregone conclusion that thesame thing holds true for human disease, i.e., that toxoplasmosis isprimarily a systemic infection and only incidentally an eye infection.The fact that it produces symptonms in the eye and not elsewhere isirrelevant.These experimentally induced ocular infections in the rabbit differ
from naturally acquired human retinochoroiditis in certain importantrespects. Although discrete single foci of necrotizing retinochoroiditiscan be produced in the posterior pole of the rabbit eye with Beverleystrain T. gondii, the experimental disease has a shorter clinicalcourse than most human infections. It is likely that severely destruc-tive progressive lesions, resembling the majority of human lesions,could be produced with the more virulent RH strain of Toxoplasma.However, this strain usually causes death from encephalitis, and wehave been reluctant to cloud our results by the use of life-savingantimicrobial drugs.Although viable organisms persist for a long time in the experi-
mentally infected rabbit eye, the lesion itself does not recur spon-taneously; at least, we have not observed any ophthalmoscopicallyapparent recurrences in a period of over two years. This may not bea serious objection to the model, however, since recurrences inhuman disease are as yet unexplained and in no way predictable.The anatomy of the rabbit eye differs in certain essential respects
from the anatomy of the human eye. The configuration of the rabbit'soptic nerve head is grossly different; it has no macula, and the surfacevasculature of the retina is limited to the region of the papilla. Allof these shortcomings were appreciated at the outset of our experi-ments, and the desirability of developing an anthropoid animal modelwas recognized. In the interest of producing large numbers of repro-ducible lesions, however, the inexpensive rodent imiodel was developed.
522

Ocular ToxoplasmosisEXPERLIMENT 11: The Effect of Autigeniic Stimulation.
Afaterials atid AlcthiodsRII strain Toxoplasma orgainisms from the pooled peritoneal exudates ofinifected mice were purified according to a method previously describedby Nozik aind O'Connor.)8 A portion of the suspension was set aside toser-ve as anI inoculum of living parasites. Another portion was suspendedin Hanks' balainced salt solution aind placed in a water bath at 56°c for90 miniutes. A third portioin was treated so as to obtain a mixture of thesoluble, cell-firee antigens derived from the purified organisms. To thisend, the fluid medium (Hanks' balainced salt solution) was removed aftercentrifugatioin of the suspension for five minutes at 700 g, and was re-placed by an equal volume of distilled water. This produced an almostimmediate lysis of the organisms due to the hypotonicity of the medium.After maintaiining the tube at 4°c for another hour, with occasional shak-inlg, we added an equal voltume of 0.17 per cent sodium chloride to thesuspension. After further vigorous shaking, the suspension was againcentrifuged at 11,500 g for 20 minutes, and the clear, supernatant fluidwas decanted inito sterile vials.
This supernaite, referred to as "lysate," conitainied several ToxoplasmaaIItigens, as inidicated by diffusion-in-agar tests against rabbit and humansera known to contain aintibodies to Toxoplasma. This material consistentlyshowed no reaction wheni tested agaiinst goat antimouse serum. Althoughthis provided acceptable evidence that the antigen soltution was free ofmouse serum proteins, anl additionial cointrol aIntigen was made from theperitoneal exudates of mice, stimuilated only by the serial injection ofcomplete Fretunid's adjuvaints into their peritoneal cavities. Following thedevelopment of ascites in these mice, the exudate was harvested, pooled,anid centrifuged according to the method of Munoz.61 This material hadno relation to Toxoplasma or any of its antigens. It was used only as acontrol to exclude the possibility that mouse proteins might play somerole in the attempted experimental reactivation of toxoplasmic retino-choroiditis.
For reactivation attempts we selected 45 pigmented rabbits with healedretinochoroiditic lesions of the type described in Experimenlt i.* Reckonedfrom the date of the initial inoculation into the suprachoroidal space, theaverage age of these lesions was four months. Thirteen rabbits receivedintravenous injections of Toxoplasma lysate with a protein content of 0.18gm per cent as determinied by the Biuret method. Five of the 13 weregiven 50 mg/kg; five were given 100 mgr kg; one was given 150 mg/kg;' Reports containing additional details of these and other related experimentshave been submitted to the ANIA Archives of Ophthalmology as part of a seriesof articles on experimenteal ocular toxoplasmosis in the rabbit. These reportshalve not yet been published.
523

and two were giveni 200 mg/kg. One of the latter died 18 hours afterinjection, but its eyes were saved for sectioniing.
Eleven rabbits received intravenous injections of a suspension of heat-killed organisms (approximately 7.1 x 107 organisms as determined bycounts of aliquots in a bright-line counting chamber). Five other rabbitsreceived intravenous injections of living organisms (approximately 8.4 X106 organisms in 0.3 ml Hanks' solution).Twelve rabbits received a second suprachoroidal space injection at a
site contiguous to an old, healed lesion. Three of the 12 received onemicroliter of lysate (protein content: 0.96 gm per cent); three receivedone microliter of a suspension of heat-killed organisms (approximately5.5 x 105); two received suprachoroidal injections of normal mouse peri-toneal cells (Munoz'61 technique); and four received a second supra-choroidal injection of living, virulent Toxoplasma organisms (approxi-mately 1.1 x 105 organisms) into both the right and left eyes.
Additional experiments were performed on the four remaining animalsthat had been specially selected for their high levels of circulating precipi-tins. Two of these had lesions that were more than a year old. Two hadlesions that were only four months old. The sera of all rabbits showedmultiple bands of precipitating antibody on diffusion-in-agar tests againsta standard antigen. Injection of 0.05 ml lysate into the mid-vitreous ofboth eyes was performed in order to see whether an ocular Arthus-typereaction could be elicited. Three of the rabbits were killed six hours afterinoculation. The fourth was sacrificed three days post-injection, followingthe development of an obvious iridocyclitis.
ResultsNone of the animals receiving intravenous injections of cell-freelysate, killed organisms, or living organisms suffered any form ofreactivation of their eye disease. Ophthalmoscopically, the lesionsappeared unaltered. The vitreous bodies and anterior segments re-mained clear. Histologic examination failed to reveal any changein the inflammatory status of their lesions (Figure 8).The animal that died 18 hours after the intravenous injection of
200 mg/kg of the lysate showed hemorrhagic lesions in the kidneysand lungs, but sections of his ocular lesion revealed only an atrophicscar without any form of inflammatory response.None of the animals receiving a second suprachoroidal injection
of lysate, killed organisms, or mouse peritoneal cells showed anyform of exacerbation.The group of animals that received a second suprachoroidal injec-
tion of living organisms into both eyes did show some response,however. Minimal retinal edema appeared at the injection site on
G. Richard O'Connor524

Ocuilar Toxoplasmiosisthe day after injection and resolved about four days later. The eyesthen remained inactive for about 14 days. At the end of this time,mottled pigmentation, more prominent in the left eye than in theright, appcared at the injection site. Histologic sections of these eyesshowed definite evidence of mild inflammatory disease. In the exu-date overlying the optic n-2rve of one specimen, evidence of multi-plying Toxoplasma parasites could be seen.When cell-free antigen was injected into the vitreous of an animal,
the immediate reaction in the anterior segment that might have beenpredicted from Silverstein's;11 studies on the Arthus phenomenon inthe eye did not materialize. After remaining quiet for three days,one such eye then developed an exuberant reaction in the anteriorsegment. The globe bccame moderately hyperemic, and a vigorouscellular response was evident in both the anterior chamber and theanterior vitreous. Histologic studies revealed marked round-cellinfiltration of the iris and ciliary body and many plasma cells (Figure9). The vessels of the ciliary body were markedly engorged. Therewas also a good deal of involvement of the choroidal vessels whichwere distended and surrounded by cuffs of inflammatory cells. Thecells encountered in all of these lesions were exclusively mononuclear.Thus, from both the time of onset of the inflammatory lesion and thecell type observed, one might think of this as a typical delayedhypersensitivity reaction rather than an Arthus phenomenon. Noreaction whatever was seen in an area containing cysts of Toxo-plasma (Figure 10), and no reaction occurred in the left eye of theanimal.Three other rabbits with a similarly high level of circulating pre-
cipitating antibody were sacrificed six hours after intravitreal injec-tion of lysate. Neither gross nor histologic examination revealed anysign of anterior segmlent inflammation. On the other hand, the opticnerve head (Figure 11) and areas of the juxtapapillary choroid (Fig-ure 12) appeared grossly infiltrated. Over the optic nerve head therewas evidence not only of mononuclear cell infiltration but of poly-morphonuclear cells as well. Additional studies are currently underway which, we hope, will confirm these observations. No inflamma-tion was detectable in any of the left eyes.
CONCLUSIONS
Recurrence of inflammation at or near the site of healed retino-choroiditic lesions could not be induced by the intravenous injection
525

Tya
I.!_
0 _ * 7la
04"'f. & 4*
b _. ,*
}4.
FeC
0
ip: -
lirI0.
. -': W.,
It '"':
A
#A& -S. ft:
W
3c0
I g~
t-q c)
CO)
0
h
0
iit 0
Cs.
Y~~~o*- * #-
0. a P
'* lptCa A
O.r 4.' 46.
wI.'
- me
*.,ftIt
w . .40

0-Co
Eu-s- U
wa.S
eC)>_ C
_
0
..X. o U
_ S=*-a_flE
-.A
S
(I::4,
:-..
F
4r*I -A
rM
..
_ .: ::
wFFD''!X *.i ' , .t .....
...,
.i:..,6:
orw:,17717I" - .:
:.40: VIII.X.:. -.: -...
t.

j:1... U.x :z.
AA,. 0
..-W*:.;,1 t:!.
AP*.:;, .,i*,0. Ca * s.'
CO
0
.. ...:
44W
04
C'S
::s. 4> e~~~~C'....... . ] . ,Q >.::
..
__
..: w.
.3..s
iix
k.. 40
.6:,

covce
or0-00
I o
*q >
co4- c.)4-4
'4 4
0
el . z
x
4i
Cd
C.)
c)
a)

G. Richard O'Connor
of livinig Toxoplasmtia organiismiis, killed Toxoplasma organisms, oraqueous extracts of Toxoplasma known to be antigenically active.From these data it would seem that the ocular lesions are not "lightedup" by intravenous challenge with an antigen known to have beeninvolved in the original inflammation. This is in marked contrast toSilverstein's 67 observations on other antigenic systems.
Suprachoroidal injections of either killed organisms or antigenicextracts of Toxoplasma failed to induce the recurrence of inflammatoryactivity at sites contiguous to previously established, healed lesions.From these data it would seem that the retina and choroid are notanaphylactically sensitized by the original lesion. If, as Frenkel states,recurrences are due to the leakage of Toxoplasma antigens from rup-tured cysts in the vicinity of healed lesions, these antigens must dif-fer in some way from those which we supplied to the retina. Nothingwe observed corroborates his theory, though it must be conceded thatour models are somewhat different.On the other hand, evidence of other types of immune phenomena
can be adduced from our experiments. Second suprachoroidal injec-tions of living Toxoplasma organisms into previously infected animalsproduced an attenuated response. A definite inflammatory reactionwas produced by organisms engaged in active multiplication, but itdid not progress with the same violence or to the same extent as theoriginal infection. Since this was true of the control (left) eye as wellas of the previously infected right eye, one might well assume thatimmune factors of systemic origin were at work here.
Injection of cell-free antigens into the vitreous body of animalswith high levels of circulating precipitins produced unexpectedresults. The lack of acute inflammatory response in the anterior seg-ment indicates that the classical Arthus phenomenon described bySilverstein62 in connection with the sensitization of guinea pigs toheterologous serum proteins did not obtain here. On the contrary,the reaction in the anterior segment seemed typical of the so-calleddelayed hypersensitivity reaction, and fitted in well with the classicconcept35 of the ocular response to chronic granulomatous infections.The early response of the optic nerve head and contiguous choroid
to intravitreal injections of lysate came closer than any other reactionto the classical Arthus phenomenon. Polymorphonuclear leukocyteswere observed at six hours in the cellular infiltrate of this lesion.Such injections must be repeated in animals in whom the level ofprecipitins has declined before any definitive statement can be made.This is obviously an area where further investigation is needed.
530

Ocular Toxoplasmosis
EXPERIMENT IIIA: The Effect of Antilymphocyte Serum and Normal HorseSerum.Starzl63 has reported the overgrowth of such organisms as herpes simplexvirus, Pneumocystis, and Toxoplasma in patients receiving antilymphocyteglobulin for the retardation of renal graft rejection. The bulk of preliminaryevidence indicates that under these circumstances the lymphocyte can nolonger function protectively. In order to evaluate the role of lymphocytesin recurrent toxoplasmic retinochoroiditis, Dr Nozik and I performed thefollowing experiment.
Materials and MethodsFour rabbits with healed retinochoroiditic lesions of the type producedin Experiment i were given a series of three intravenous injections ofhorse anti-rabbit-lymphocyte serum. This serum, supplied by Dr GilbertSmolin of the Francis I. Proctor Foundation in San Francisco, was origi-nally designed for experiments concerned with the suppression of cornealxenograft reactions in the rabbit. It was prepared by serial intravenousinjections of rabbit lymphocytes (derived from thymus) into a horse. Itscytotoxicity titer was reported to be 1:256.
Rabbits selected for this experiment received three intravenous injectionsof 2.75 ml of this serum on a schedule of one injection every three days.A control group of four rabbits with similar lesions received normal horseserum (NHS) in the same amount and at the same intervals. The animalswere observed ophthalmoscopically for the following signs of recurrence:retinal edema; gray-white infiltrations in or near old, healed lesions; fuzzymargins at the site of healed lesions; and vitreous cellularity.
ResultsAbout seven days after the last of the three injections, two of thefour rabbits injected with anti-lymphocyte serum developed recurrentinflammation in or near the old lesions. These changes were charac-terized by (1) gray-white infiltrates at one or more margins of theold lesion; (2) a fuzzy appearance at the site of what was formerly asharply demarcated scar; (3) vitreous opacities ranging from smallcellular opacities to large clumps and strands; and (4) a variableamount of cells and flare in the anterior chamber.
Identical changes were observed in all four of the control animals,i.e., those that received normal horse serum. In histologic sections,both groups showed almost identical changes. The choroid andretina were infiltrated with large numbers of mononuclear cells,many of which were plasmacytes. There was disruption of the nor-mal retinal architecture in or near the site of the original atrophiclesion (Figure 13), and in several areas multiplication of the parasite
531

%4 --
oC.)
- ot
0%4-
0
ce4
co *.o) v
-4,
Q Q
000u
c0
0cA
C')
C'S
cis
.0
... E
V. .....

Oc lfar Toxoplasmiosiscould be discerned. In the areas of severe infiltration the retina ap-peared necrotic, aind inflammatory cells were thrown off into thevitreous fromii the retinal surface. The iris and ciliary body showedvarying degrees of infiltrationi by mononuclear cells. Throughout theuvea there was cngorgement of the blood vessels, swelling of theendothelial cells, and perivascular infiltration.
CONCLUSIONS
What at first seemed to be a specific effect of antilymphocyte serumwas in fact duplicated by normnal horse serum. Some seven daysafter the last injection of either serum, inflammatory activity recur-red at the site of old, healed lesions. The mononuclear infiltration ofareas adjacent to old scars was accompanied by additional necrosisand by what was tentatively identified as the proliferation of Toxo-plasma parasites.To account for these phenomena, we considered the possibility
that they were due to altered vascular permeability to heterologousserum proteins at the site of the lesion. To test this possibility, thefollowing investigation was carried out jointly with Dr SamuelAronson of the San Francisco General Hospital and with Dr RobertA. Nozik of the Francis I. Proctor Foundation.
EXPERINIENT IIIB: Determiniations of the Extravascullar Albuimiin Space inRabbits with Healed Toxoplasmic Retinochoroiditis.
Materials and MethodsSeven rabbits with healed retiniochoroiditic lesions, produced as in Experi-ment i, were subjected to study. As reckoined from the date of initialinoculation, the lesions were four to six months old. Each rabbit receivedan intravenous injection of a measured amount of 59Fe-labelled rabbiterythrocytes, together w-ith a measured amount of 1251-labelled humanserum albumin. After anI initial determinationi of hematocrit and bloodvolume, equilibration of the intravascular and extravascular componentswas allowed to take place over a six-hour period. According to a methoddescribed by Fish et al.64 the extravascular albumin space of each eyewas then determined. The result, based on differential radioactivity countsof each enucleated eye, represented the degree to which proteins, suchas human serum albumin, canl leak out of vessels into the extravascularspace of the eye.
Similar measurements were made on seven additional rabbits withhealed retinochoroiditic lesions seven days after the last of a series ofthree intravenious injectionis of normal horse serum. The right eyes of twoof these rabbits had definite ophthalmoscopic signs of recurrence.
533

C) 00
CO C~ -
r-I-4
r-0l
CD oo bC~00 ),t O =
Cl C:
CO N. 00 .)
Oq cl
X i M2-*)-* -O
C.() 41
U) 4-.?on ¢s.
C)1 -4 f
t- 00 -
C' -r4
-
N.0 N.
Cl 0
bCO
4-''-- b1dwW)
V)
6z.0CD
00
0._
0n0o0u
._
3-
._
0o
¢0
._
._
0
0
E00
000
0
U)
00
0
0
-oN..0C)C)
0
0
C)
.0C)cCC).0.0
.0CCI-
-eC)0C)E
0.
0
0
H
CD
w
H
z
a
U)
04
m
Hz
(n
H
0
z
CC
¢
H
¢CC
Y)
m
¢-t
Cl
0Cl
6zo
._CD

Ocul ar Toxoplasnosios5i5RestultsThe determinationis on the first series of animals are listed in Table 1A.These show a larger extravascular albumin space in the right eye ofevery animnal tested (with the exception of Rabbit 116). The meanof the ratios of the extravascular albumin spaces (right eye/left eye)is 1.24 (standard deviation = 0.203).The determinationis on the group of rabbits subjected to three injec-
tions of normal horse serum show even larger differences (Table 1B).The mean of the ratios in this instance (right eye/left eye) is 1.70(standard deviation = 0.535).
CONCLUSIONS
These results suggest that the blood vessels of the right eyes of allanimals tested were more permeable to serum proteins than those ofthe left eyes. This was possibly the result of damage sustained by theblood vessels of the right eyes during the initial stage of the necro-tizing inflammation.
If this was the case, then it may be that antigens, antibodies, oreven antigen-antibody complexes could gain access to the site ofinflammation through local alterations in vascular permeability. Theconsequences of this are discussed by Gamble65 in his study ofaltered vascular permeability induced experimentally in the rabbiteye by small doses of bacterial endotoxin.
It is conceivable that the union of horse serum proteins with rabbitantibodies to these proteins might result in severe inflammatory re-actions of the type described as "serum sickness." This, in turn,might trigger recurrence of dormant toxoplasmic lesions if locallymphocytes, normally occupied with the defense of the host againstToxoplasmna, were diverted to reactions in which heterologous serumproteins participated.
DISCUSSION
Although the eye appears to be able to participate in a number ofimmunologic reactions related to various types of hypersensitivityto Toxoplasma, the investigative work performed in our laboratorygives no support to the concept that toxoplasmic retinochoroiditis isitself a manifestation of hypersensitivity. More likely, it is directlyattributable to multiplication of the parasite in the tissues.
If one supposes that Toxoplasnia cysts periodically break down inthe tissues of chronically infected individuals, it may be that there
535

G. Richard O'Connor
is at least some invasion of previously uninvolved cells by the lib-erated parasites. Frenkel'1 himself has published pictures showingthat this occurs in the hamster eye. The extent of the multiplicationof the parasite in retinal cells and the subsequent activities of thefree-swimming organisms that have been released from bursting hostcells may be limited to some degree by immune reactions on the partof the host.From a survey of the literature, it seems most likely that the host's
major defense against the parasite is a cellular response in whichimmunocompetent lymphocytes participate. Humoral factors cannotbe excluded, however, since we have shown in our studies that thevascular permeability of eyes previously infected by Toxoplasma isaltered. If neutralizing antibody of high titer were present in thecirculation, it could conceivably gain access to the ocular lesion andprevent the multiplication of the parasite.On the other hand, the experiments of Huldt66 and of Foster and
McCulloch48 suggest that dye-test antibody alone is not effective inprotecting the host against the ravages of the organism. Passivelytransferred antibodies will not protect a prospective host to anysignificant degree. According to Foster and McCulloch, the onlysignificant protection is either a previous infection or an experiment-ally produced contact of the host's reticuloendothelial system withkilled Toxoplasma parasites, combined with Freund's adjuvants. Thisimplies some type of immunity based on a specific cellular response.It remains to be seen whether this is (1) some special type of spe-cifically facilitated phagocytosis, (2) protection by interferon, aselaborated by the host cells, (3) cytophilic antibody, (4) antibodyproduced by plasma cells in situt, or (5) the destructive effect ofspecific immunocompetent lymphocytes on target cells, as describedby Rosenau.14The fact that plasma cells are so abundant in both the subacute
phase of newly produced experimental lesions and the recurrentphase of clinical lesions suggests that this particular cellular elementis of prime importance in the host's defense against widespreadmultiplication by the parasite. Do these plasma cells develop fromlymphocytic precursors, left behind in the ocular tissues followingthe acute phase of infection; or are they freshly recruited from centralreticuloendothelial organs such as the spleen or bone marrow? Thework of Silverstein 67 and others suggests that a combination of thesetwo mechanisms occurs in experimental systems in which the rabbiteye is sensitized to heterologous serum proteins. We might tenta-
536

Ocular Toxoplasmosis
tively extrapolate his findings to the eye infected with Toxoplasma.The release of living organisms into the retina may trigger the con-version of the few immunocompetent lymphocytes remaining in theeye into plasma cells. In addition, uncommitted lymphocytes passingthrough the area may be arrested by the factors described by Davidand Lawrence,"8 and these lymphocytes may similarly be recruitedfor specific anti-Toxoplasmia activity, provided the host is normal.
It is known that there is considerable variation from host to hostin the ability to mobilize cellular defense mechanisms. This is quiteindependent of the host's ability to make humoral antibody (of thetype that might be detected by dye-test analysis of his venous blood).Graphic evidence of this variation in one's ability to mobilize hislymphoid defense system is seen in patients with malignancies of thelymphoid system. Vietzke49 has summarized a number of such dis-eases, including chronic lymphatic leukemia, multiple myeloma, andHodgkin's disease. Patients affected with these diseases may die ofwidespread systemic toxoplasmosis, yet they usually have high Toxo-plasma dye-test titers.The host's defenses can be compromised by a number of other
circumstances besides neoplasms of the lymphoid cells. Frenkel53 hasshown, for example, that chronically infected hamsters may succumbto acute exacerbations of toxoplasmic disease when treated withx-irradiation or large doses of systemic corticosteroids. And Kauf-man"9 has shown that rabbits with experimentally induced eye infec-tions may succumb to systemic disease (probably encephalitis)when treated with massive doses of corticosteroids alone. As mentionedabove, widespread systemic involvement with Toxoplasma has beenattributed to the use of antilymphocyte serum in renal transplantpatients. In all of these studies, the lymphocyte, when altered bydisease, irradiation, or medication, no longer played its protective roleagainst Toxoplasma.The reader may ask, how does all this affect the "normal" eye
patient who is apparently free from these other forms of bizarredisease? Why does recurrent toxoplasmosis appear to be a self-limited disease of short duration in some patients, and a progressive,disastrous disease in others? If we are to assume that lymphoid de-fenses are responsible for keeping the infection at bay, why isn'tthis protection more uniform among the so-called "normal" patients?Although the answers to these questions are not known, it is per-
haps reasonable to speculate that differences in the virulence ofvarious Toxoplasma strains may account for the inability of some
537

G. Richard O'Connor
"normal" lymphoid systems to cope with the infection. Kaufman70and Hogan71 have both shown that strains of Toxoplasma with astrong proclivity for early cyst formation are relatively avirulent,whereas virulent strains show little tendency to cyst formation. TheME 49 strain is a good example of the former and the Pm strain of thelatter. The balance between the proliferative activity of the organismon the one hand, and the defensive activity of the host's lymphoidcells on the other, may be a delicate one. A high degree of lympho-cyte mobilization would probably be necessary to keep the multipli-cative activity of the RH strain at bay. Even if this were possible,minor variations in other physiologic factors, such as the level ofcirculating corticosteroids, might influence this delicate balance ad-versely, allowing for periodic multiplication of the organism in ornear the site of an old lesion. On the other hand, very little lymphoidactivity might be necessary to keep the ME 49 strain at bay.A few authors, such as Remington72 and Beverley,73 have raised
doubts as to whether Toxoplasma cysts ever break down spontane-ously in tissues. Cysts are not universally present in the sections ofeyes taken from patients with presumptive ocular toxoplasmosis; itis possible that these patients are infected with strains that showlittle tendency to cyst formation. How do such patients become af-fected by recurrent ocular toxoplasmosis? In what form does theparasite reside in the tissues if not in the cystic form? Here againlittle concrete information is available, but one is led to speculatethat the organism may be living in such tissues in a form that repro-duces very slowly. The metabolic and reproductive requirements ofthe parasite may be so low as to cause very little tissue destructionunder these circumstances, and the patient may accordingly haveno symptoms during these periods of relative inactivity. Activeinflammation with necrosis may occur only when the balance offactors ordinarily responsible for keeping the parasite under controlis altered.
If corticosteroids ordinarily favor the multiplication of the para-site by diminishing the effectiveness of the lymphoid defense system,why do they sometimes benefit the ocular lesion? Although Kauf-man70 was able to show that the extent of experimental ocular lesionsin the rabbit could be limited by the use of systemic corticosteroids,it is a common clinical experience to see the ocular lesions of mantake a relentless downhill course under the influence of corticosteroids.Assuming that the diagnosis is correct, how can these seeminglyparadoxical observations be reconciled?
5<38

Ocular ToxoplasmosisIt must be realized at the outset that the corticosteroids have mul-
tiple effects on man. Although they are mildly lymphocytolytic inman, they are much more so in the rabbit;74 and this may accountfor the systemic deaths that Kaufrnan observed among his rabbits.In addition, of course, corticosteroids are primarily and profoundlyanti-inflammatory. They stabilize the lysosome, preventing the re-lease of hydrolytic enzymes that might be involved in tissue destruc-tion; and since Toxoplasma organisms are known to contain lysosomes,corticosteroids may be effective in mitigating their effect. If antigen-antibody complexes bind complement in the tissue, pharmacologicagents (histamine, serotonin, etc.) capable of bringing about capil-lary dilatation and edema are also released. These reactions aremodified by corticosteroids in much the same way that other antigen-antibody reactions such as serum sickness are modified. The neteffect, then, may be one of limiting the extent and severity of theocular inflammation even though multiplication of the organism isgenerally favored.Mention has been made of the "toxic theory" of cell damage by
Toxoplasma. Hogan, Moschini, and Zardi44 claim to have isolateda substance from the peritoneal exudates of infected mice whichthey, like Weinman and Klatchko,40 called "toxotoxin". When injectedintracamerally or intravitreally in the eyes of rabbits, this substanceproduced severe immediate inflammatory changes in the eyes. Asearly as three hours after injection, hemorrhagic and thromboticchanges occurred in the anterior uveal vessels. Severe endothelialdamage was occasionally noted in the later, and polymorphonuclearleukocyte infiltration was a prominent feature. Injections into theposterior vitreous resulted in edema and degeneration of the sup-porting cells of the retina, swelling and basophilia of the cells in theexternal nuclear layer, loss of the outer processes of the receptorcells, and eventual migration of the retinal pigment epithelium.The authors claimed that their material was free of residual mouse
protein. It was thus different from the "toxotoxin" originally describedby Weinman and Klatchko,40 and different from the lysate of purifiedToxoplasma organisms with which both Lunde and Jacobs47 andNozik and O'Connor42 have worked. Whatever its nature, it wouldappear that this substance is not a true exotoxin of the type secretedby Clostridium sp. If one examines tissue cultures infected withToxoplasma (Figure 14), one sees perfectly normal cells in the im-mediate vicinity of the parasitized host cells. When the host cellruptures, it is completely destroyed, and an empty space correspond-
539

_
4b .......: Au. I% 1_
j; ...
....
:: * * to..
.._i . i
e _
0
14'-.4
-.
00
03
0
oH
~cq
00a
$--
r'
.:
:., AM N:
0:M. ''
::
-t
0 "M
-:: .:
.jw ::,
. &.4
..:.
'14.:..

Ocular Toxoplasmosising to one of Lycke's75 "plaques" is left behind; but nothing happensto the adjacent cells until they themselves become parasitized. Itseems unlikely, therefore, that there is any lytic toxin excreted bythe parasite into the medium. Perhaps the term "eso-metabolite"coined by Zardi et al.43 is more appropriate.
Although it is freely granted that hemorrhage sometimes compli-cates the early picture of retinochoroiditic inflammation in the humansubject, invasion of the vessel walls cannot be excluded as the causeof the hemorrhage. Some polymorphonuclear leukocyte accumulationsare also seen in the acute necrotic lesions. Since they may be expectedin the wake of any extensive tissue necrosis, it is not necessary toinvoke a theory of toxic damage to explain their presence.
Lastly, it must be stated that none of the "toxic" phenomenadescribed by Hogan et al.44 occurred in rabbit eyes which were injectedwith Toxoplasma lysates, prepared according to the method describedin Experiment II. Whether such phenomena would have occurred ifthe lysates had been recombined with cellular or humoral productsfrom mouse peritoneal exudates is a matter of conjecture.Although the limitations of working with a rabbit model should be
borne in mind, it must be considered significant that in all the fore-going experiments there is no evidence that hypersensitivity itself couldaccount for the necrotizing retinochoroiditis of toxoplasmosis. Fromthese experiments, it can only be concluded that necrotizing retino-choroiditis of both the acute and recurrent varieties is the direct resultof multiplicative activities of the parasite. Although evidence ofhypersensitivity to Toxoplasma was certainly adduced in these eyes,it could be demonstrated only in the anterior uvea, the peripapillarychoroid, and the optic nerve head. Injections of antigens into thesuprachoroidal space in the form of either killed organisms or solubleextracts of the parasites produced no chorioretinitic reaction. Sincethese animals manifested signs of previously established immediateand delayed hypersensitivity to Toxoplasma (precipitin activity inthe serum and skin test reactivity to toxoplasmin), they would havebeen expected to manifest some signs of reaction at the posterior pole,if Frenkel's hypothesis were correct. However, no such reactions wereobserved.The introduction of soluble antigens into the vitreous, on the other
hand, produced an almost immediate reaction in and around theoptic nerve head. This was principally a mononuclear cell reaction,but a few polymorphonuclear cells could be seen in the overlyingexudate. The duration of the reaction (six hours) and the cell types
541

G. Richard O'Connor
observed suggest that this was a manifestation of immediate hyper-sensitivity. Since these animals had high levels of circulating precipi-tins at the time of antigen injection, the reaction might well be inter-preted as a type of Arthus phenomenon.The reaction produced in the anterior uvea was typical of delayed
hypersensitivity. No reaction whatever was evident at six hours, norindeed at 24 or 36 hours after injection. However, between two andthree days after injection, an exuberant reaction occurred in theciliary body, iris, and part of the choroid. The inflammatory exudatewas exclusively mononuclear, and many plasma cells were in evi-dence. Capillary dilatation and edema of the iris stroma were alsoobserved, together with nodular accumulations of lymphocytes. It isnot difficult to imagine that this is the counterpart of the granulo-matous iridocyclitis seen in cases of human toxoplasmic uveitis. Toxo-plasma organisms have never been seen in the anterior uvea of man;yet the iridocyclitis is often stormy in character, producing extensiveposterior synechiae and granulomatous nodules. It is of interest thatthis type of iridocyclitis can be produced by injection of soluble anti-gens into the vitreous and is independent of the multiplicative activityof the parasite.Although it was not the primary purpose of this paper to discuss
the treatment of toxoplasmic uveitis, it is perhaps appropriate todiscuss the justification for some of the various forms of therapy thathave been given in the past. If one assumes that the major cause ofthe necrotizing retinochoroiditis is the proliferation of parasites withinretinal tissue, then it seems appropriate to administer antimicrobialagents such as pyrimethamine, the sulfonamides, aureomycin, orspiramycin. These agents are said to be toxoplasmastatic;76 that is,none of them singly or in combination, is toxoplasmacidal. AlthoughKaufman77 has shown that by giving appropriate loading-doses, it ispossible to achieve levels of pyrimethamine in the retina that are lethalto the parasite, death of the parasite may be due to the combined effectof the drug and the lymphoid defense system of the host. It seemslikely that the progressive downhill course that many ocular lesionshave taken in spite of antimicrobial therapy may be due to deficien-cies in the lymphoid response of the individual or to the geometry ofthe lesion itself. It may not be reasonable to expect antimicrobialagents such as pyrimethamine to penetrate a large, thickened granu-loma such as one often sees in the progressive form of the disease.
Systemic corticosteroid administration can be justified on the basisof its primary anti-inflammatory activity, its ability to stabilize lyso-
542

Ocular ToxoplasmosisSomiecs, and its proven ability to limit the size of experimental lesionsin the ocular fundus of the rabbit.' Since corticosteroids may decreasethe effectiveness of the lymphoid responise, however, it would seemsafer to administer simultaneously at least one antimicrobial agentknown to be effective against the proliferative form of Toxoplasma.For the control of perivasculitis, papillitis, and iridocyclitis, which arealmost surely manifestations of hypersensitivity to the antigens ofToxoplasma, the administration of corticosteroids would seem to befully justified.
Treatmenit of Toxoplasma lesions of the retina with light coagula-tion (xenon arc) or laser irradiation is probably also justified since itkills organisms in the areas treated and provokes a certain amount ofgliotic reaction, which may wall off the inflammatory process. Unfor-tunately, treatment of sufficient intensity to create gliotic reactions mayalso give rise to serious complications, such as retinal detachments orretinal hemorrhages. The same is true of cryotherapy as applied byDobbie.78 Treatment of lesser intensity may produce only localizeddisturbances of the pigment epithelium or atrophy, in which case theorganisms may still be free to proliferate once again. Both lightcoagulation therapy and cryotherapy have been criticized becausethey might relcase antigens into anaphylactically sensitized tissues. Inview of the results of experiments described in this paper, this criti-cism seems wholly unjustified.
SUMMARY
On the basis of experiments performed on the eyes of pigmentedrabbits, and a survey of pertinent studies reported in the literatureon the pathogenesis of ocular toxoplasmosis, the following statementswould seem to be justified:
(1) Both the acute and recurrent types of necrotizing retinocho-roiditis are due to multiplication of Toxoplasma parasites in theretina.
(2) Release of Toxoplasmna antigens into the retina and choroidof individuals with previously established retinochoroiditic scars doesnot result in recurrence of the inflammatory disease.
(3) Iridocyclitis, optic neuritis, and perivasculitis of both retinaland uveal vessels are manifestations of hypersensitivity to Toxo-plasmia.
(4) Experimental toxoplasmic lesions alter the vascular perme-ability of affected eyes, and this permits the leakage of serum pro-
543

G. Richard O'Connor
teins into the extravascular spaces of such eyes for months afterthe original infection.
(5) Factors that interfere with the normal functioning of lympho-cytes and of the lymphoid cells they generate (e.g., plasma cells)favor the multiplication of Toxoplasma parasites in tissue. Thesefactors seem to be considerably more important than circulatinghumoral antibody.
REFERENCES
1. Nicolle, C., and L. Manceaux, Sur une infection 'a corps de Leishman (ouorganismes voisins du gondi), Corpt. Rend. Acad. Sci. Paris, 147:763, 1908.
2. Janku, J., Pathogenesa a Pathologicka Anatomie T. Zv. Vrozeneho Kolobomu2lute Skurny Oku Norm'al ne Velikem a Mikrophtalmickem s N'alezem Para-situ v Sitnici, Cvas. Lek. Ces., 62:1021, 1923.(See later German translation, 2A.)
2A. Jank'u, J., Die Pathgenese und Pathologische Anatomic des sogennantenangeborenen Koloboms des gelben Fleckes im normal grossen sowie immikrophthalmischen Auge mit Parasitenbefund in der Netzhaut., 2sl.Parasit., 6:9, 1959.
3. Wolf, A., D. Cowen, and B. H. Paige, Human toxoplasmosis: occurrence ininfants as an encephalomyelitis: verification by transmission to animals,Science 89:226, 1939.
4. Koch, F. L. P., D. Wolf, D. Cowen, and B. H. Paige, Toxoplasmic enceph-alomyelitis. vii Significance of ocular lesions in the diagnosis of infantileor congenital toxoplasmosis, A.M.A. Arch. Ophth., 29:1, 1943.
5. Wilder, H. C., Toxoplasma chorioretinitis in adults, A.M.A. Arch. Ophth.,48:127, 1952.
6. Jacobs, L., J. R. Fair, and J. H. Bickerton, Adult ocular toxoplasmosis(Report of a parasitologically proved case), A.M.A. Arch. Ophth., 52:63,1954.
7. Desmonts, G., Definitive serological diagnosis of ocular toxoplasmosis, A.M.A.Arch. Ophth., 76:839, 1966.
8. Sabin, A., and H. A. Feldman, Dyes as microchemical indicators of a newimmunity phenomenon affecting a protozoan parasite (Toxoplasma),Science, 108:660, 1948.
9. Arthus, M., Injections repetees de serum de cheval chez le lapin., Compt.Rend. Soc. Biol. (Paris), 55:817, 1903.
10. Frenkel, J. K., Pathogenesis of toxoplasmosis and of infections with organismsresembling Toxoplasma, Ann. N.Y. Acad. Sci., 64:215, 1956.
11. Frenkel, J. K., Pathogenesis of toxoplasmosis with a consideration of cystrupture in Besnoitia infection, Survey Ophth., 6:799, 1961.
12. Spalter, H. F., C. J. Campbell, K. S. Noyori, M. C. Rittler, and C. J. Koes-ter, Prophylactic photocoagulation of recurrent toxoplasmic retinochoroiditis:a preliminary report, A.M.A. Arch. Ophth., 75:21, 1966.
13. Beverley, J. K. A., A rational approach to the treatment of toxoplasmicuveitis, Trans. Ophth, Soc. U.K., 78:109, 1958.
14. Rosenau, W., and H. D. Moon, Lysis of homologous cells by sensitizedlymphocytes in tissue culture, Jour. Nat. Cancer Inst., 27:471, 1961.
15 Cohn, Z. A., and E. Wiener, The particulate hydrolases of macrophages.i. Comparative isolation and properties, J. Exp. Med., 118:951, 1963.
544

Ocular Toxoplasmosis
16. Van Metre, T. E., D. L. Knox, and A. E. Maumenee, The relation betweentoxoplasmosis and focal exudative retinochoroiditis, Am. J. Ophth., 58:6,1964.
17. Kaufman, H. E., Uveitis accompanied by a positive Toxoplasma dye-test,A.M.A. Arch. Ophth., 63:767, 1960.
18. Jacobs, L., and M. N. Lunde, A hemagglutination test for toxoplasmosis,J. Parasit., 43:308, 1957.
19. O'Connor, G. R., Precipitating antibody to Toxoplasma. A follow-up studyon findings in the blood and aqueous humor, Am. J. Ophth., 44: Part iI,75, 1957.
20. Stranneg'ard, O., Studies of Toxoplasma precipitinogens and their correspond-ing antibodies by means of diffusion-in-gel methods, Brit. J. Exp. Path.,43:600, 1962.
21. Huldt, G., The dye-test and complement-fixation test in toxoplasmosis; acomparative investigation, Acta. Path. Microbiol. Scand., 43:141, 1958.
22. Lunde, M. N., and L. Jacobs, Differences in Toxoplasma dye-test andhemagglutination antibodies shown by antigen fractionation, Am. J. Trop.Med. Hyg., 16:26, 1967.
23. Ouchterlony, 0., Antigen-antibody reactions in gels, Acta. Path. Microbiol.Scand., 26:507, 1949.
24. Jacobs, L., M. K. Cook, and H. C. Wilder, Serologic data on adults withhistologically diagnosed toxoplasmic chorioretinitis, Trans. Amer. Acad.Ophth. Oto., 58:193, 1954.
25. Zscheile, F. P., Recurrent toxoplasmic retinitis with weakly positive methy-lene blue dye-test, A.M.A. Arch. Ophth., 71:645, 1964.
26. Franceschetti, A., and E. Engelbrecht, Mise en evidence de toxoplasmasdans un cas de chorioretinite seronegative, Ophthamologica (Basel),147:273, 1964.
27. Remington, J. S., L. Jacobs, and H. E. Kaufman, Toxoplasmosis in the adult,New Eng. J. Med., 262:180, 1960.
28. Witmer, R. H., Experimental leptospiral uveitis in rabbits, A.M.A. Arch.Ophth., 53:547, 1955.
29. Silverstein, A. M., Ectopic antibody formation in the eye: pathologicalimplications. In Immunopathology of Uveitis. Ed. by A. E. Maumenee andA. M. Silverstein, Baltimore, Williams and Wilkins, 1964.
30. Woods, A. C., Discussion of a paper by M. J. Hogan, et al, Trans. Amer.Ophth. Soc., 55:275, 1957.
31. Beverley, J. K. A., Ocular toxoplasmosis, in Human Toxoplasmosis. Ed. byJ. C. Siim, Copenhagen, Munksgaard, 1960.
32. Wilder, H. C., Toxoplasma chorioretinitis in adults, A.M.A. Arch. Ophth.,47:425, 1952.
33. Zimmerman, L. E., Ocular pathology of toxoplasmosis, Survey Ophth.,6:832, 1961.
34. Hogan, M. J., Ocular Toxoplasmosis, New York, Columbia University Press,1951, p. 35.
35. Woods, A. C., Endogenous Inflammations of The Uveal Tract, Baltimore,Williams and Wilkins, 1961, p. 91.
36. Kimura, S. J., P. Thygeson, and M. J. Hogan, Signs and symptoms of uveitis.ii. Classification of the posterior manifestations of uveitis, Am. J. Ophth., 47:Part II, 171, 1959.
37. Rieger, H., Uber weitere auf Toxoplasmosis adultorum acquisita verdach-tige Falle von Retinitis exsudativa externa centralis, Klin. Monatsbl. Augenh.,120:33, 1952.
545

546 G. Richard O'Connor
38. Berengo, A., and R. Frezzotti, Active neuro-ophthalmic toxoplasmosis. Aclinical study on nineteen patients, Advances Ophth., 12:265, 1962.
39. Manschot, W A., and C. B. F. Daamen, Connatal ocular toxoplasmosis,A.M.A. Arch. Ophth., 74:48, 1965.
40. Weinman, D., and H. J. Klatchko, Description of toxin in toxoplasmosis,Yale J. Biol. Med., 22:323, 1950.
41. Varela, G., E. Roch, and A. Vaizquez, Virulencia, cultivo polis'acuridas, tox-inas y la prueba del colorante, estudiados con una cepa de Toxoplasmagondii, Rev. Inst. Salub. y Enferm. Trop., 15:73, 1955.
42. Nozik, R. A., and G. R. O'Connor, The so-called toxin Off Toxoplasma, Am.J. Trop. Med. Hyg., 18:511, 1969.
43. Zardi, O., G. Giorgi, A. Pana, and V. Monaco, Caratteristiche fisico-chimichbe biologiche della toxotossina, Recent Progr. Med. (Rome), 46:266, 1967.
44. Hogan, M. J., G. B. Moschini, and 0. Zardi, Effects of Toxop!asma gondiitoxin on the rabbit eye, Manuscript, in preparation.
45. Hansson, H. A., and P. Sourander, Ultrastructural demonstration of lyso-somes in Toxoplasma gondii, Acta Path. Microbiol. Scand., 74:431, 1968.
46. Lund E., H. Hansson, E. Lycke, and P. Sourander, Enzymatic activities ofToxoplasma gondii, Acta Path. Microbiol. Scand., 68:59, 1966.
47. Lunde, M., and L. Jacobs, Froperties of Toxoplasma lysates toxic to rabbitson intravenous injection, J. Parasit., 50:49, 1964.
48. Foster, B. G., and W. F. McCulloch, Studies of active and passive immunityin animals inoculated with Toxoplasma gondii, Canad. J. Microbiol., 14:103,1967.
49. Vietzke, W. M., A. H. Gelderman, P. M. Grimley, and M. D. Valsamis,Severe course of toxoplasmosis in cancer patients, Cancer, 21:816, 1968.
50. Theologides, A., K. Osterberg, and B. J. Kennedy, Cerebral toxoplasmosisin multiple myeloma, Ann. Intern. Med., 64:1071, 1966.
51. Reynolds, E. S., K. W. Walls, and R. I. Pfeiffer, Generalized toxoplasmosisfollowing renal transplantation, Arch. Intern. Med., 118:401, 1966.
52. Deodhar, S., K. Tung, A. L. Robertson, and S. Nakamoto, Pathology ofrenal transplantation in man, Exhibit presented at the national conventionof Am. Med. Assoc., San Francisco, Calif., June, 1968.
53. Frenkel, J. K., Effects of cortisone, total body irradiation, and nitrogenmustard on chronic latent toxoplasmosis, Am. J. Path., 33:618, 1957.
54. Hemsath, F. A., and H. Pinkerton, Disseminated cytomegalic inclusion dis-ease and disseminated toxoplasmosis in an adult with myeloid metaplasia,Am. J. Clin. Path., 26:36, 1956.
55. Cheever, A. W., M. P. Valsamis, and A. S. Rabson, Necrotizing toxoplasmicendophthalmitis and herpetic pneumonia complicating treated Hodgkin'sdisease, New Eng. J. Med., 272:26, 1965.
56. M0ller, T., and S. W. Nielsen, Toxoplasmosis in distemper susceptible car-nivora, Path. Vet., 1: 189, 1964.
57. Remington, J. S., Discussion of a paper by L. E. Zimmerman: Ocularpathology of toxoplasmosis, Survey Ophth., 6:844, 1961.
58. Nozik, R. A., and G. R. O'Connor, Experimental toxoplasmic retinocho-roiditis, A.M.A. Arch. Ophth., 79:485, 1968.
59. O'Connor, G. R., Anti-toxoplasma precipitins in aqueous humor: New ap-plication of the agar-diffusion technique, A.M.A. Arch. Ophth., 57:52, 1957.
60. Jacobs, L., The production and treatment of acute toxoplasmic uveitis inthe anterior segment of the rabbit eye, Amer. J. Trop. Med. Hyg., 5:375,1956.
61. Munoz, J. Production in mice of large volumes of ascites fluid containingantibodies, Proc. Soc. Exp. Biol. Med., 95:757, 1957.

Ocular Toxoplasmosis
62. Silverstein, A. M., and L. E. Zimmerman, Immunogenic endophthalmitisproduced in the guinea pig by different pathogenetic mechanisms, Am. J.Ophth., 48:435, 1959.
63. Starzl, T. E., Experience in Renal Transplantation, Philadelphia, Saunders,1964.
64. Fish, M. B., S. B. Aronson, M. Polycove, and M. A. Coon, Ocular bloodvolume, A.M.A. Arch. Ophth., 82:377, 1969.
65. Gamble, C. N., The ocular Auer reaction and its possible relationship torecurrent uveitis, in Clinical Methods in Uveitis. Ed. by S. B. Aronson, et al.,St. Louis, Mosby, 1968, p. 147.
66. Huldt, G., Experimental toxoplasmosis. Effect of corticosteroids on rabbitswith varying degrees of immunity, Acta Path. Microbiol. Scand., 68:605,1966.
67. Silverstein, A. M., Uveal hypersensitivity reactions to protein antigens. InImmutnopathology of Uveitis. Ed. by A. E. Maumenee and A. M. Silverstein,Baltimore, Williams and Wilkins, 1964, p. 209.
68. David, J. R., S. Al-Askari, H. S. Lawrence, and L. Thomas, Delayed hyper-sensitivity in vitro. i. The specificity of inhibition of cell migration by anti-gens, J. Immunol., 93:264, 1964.
69. Kaufman, H. E., The effect of corticosteroid on experimental ocular toxo-plasmosis, Amer. J. Ophth., 50: Part ii, 919, 1960.
70. Kaufman, H. E., M. L. Melton, J. S. Remington, and L. Jacobs, Strain dif-ferences of Toxoplasma gondii, J. Parasitol., 45:189, 1959.
71. Hogan, M. J., C. Yoneda, and P. Zweigart, Growth of toxoplasma strains intissue culture, Am. J. Ophth., 51:920, 1961.
72. Remington, J. S., Personal communication.73. Beverley, J. K. A., Experimental ocular toxoplasmosis, Survey Ophth.,
6:897, 1961.74. Schwartz, R. S., Therapeutic strategy in clinical immunology, New Eng. J.
Med., 280:367, 1969.75. Lycke, E., and E. Lund, A tissue culture method for titration of infectivity
and determination of growth rate of Toxoplasma gondii, Acta Path. Microbiol.Scand., 60:209, 1964.
76. Leopold, I. H., Therapy of ocular toxoplasmosis, Survey Ophth., 6:955,1961.
77. Kaufman, H. E., The penetration of Daraprim (pyrimethamine) into themonkey eye, Am. J. Ophth., 52:402, 1961.
78. Dobbie, J. G., Cryotherapy in the management of toxoplasma retinocho-roiditis, Trans. Amer. Acad. Ophth. Oto., 72:364, 1968.
547