Embed Size (px)
Citation preview
Hernia (2008) 12:407–414
DOI 10.1007/s10029-008-0364-2ORIGINAL ARTICLE
Patient-reported outcomes in hernia repair
E. M. Bitzer · C. Lorenz · S. Nickel · H. Dörning · A. Trojan
Received: 21 August 2007 / Accepted: 29 February 2008 / Published online: 1 April 2008© Springer-Verlag 2008
AbstractBackground The project aimed at testing the feasibility ofa quality improvement system based on patient-reportedoutcomes in short-stay surgery for groin hernia repair.Methods In two centres for short-stay surgery all patientsreferred for hernia repair were surveyed between August1999 and January 2002. Patients reported on health-relatedquality of life (SF-36), symptoms (Hernia Symptom Check-list, HSCL) and other indicators pre-operatively (T0) and14 days (T1) and 6 months post-operatively (T2). Three ofthe eight SF-36 subscales (physical functioning, bodilypain, and role physical) and the HSCL at T2 were consi-dered as main outcome indicators. The main outcomes wereanalysed by generalized linear models with regard to pre-dictors.Results At T0 a total of 342 hernia patients wereincluded. The response rate at T2 was 54.1% (92.4% males,58.6 years of age). At T2 only 21.1% did not report com-plaints (i.e. haematoma, pain, numbness) post-operatively.The overall positive course is reXected by the HSCL: from
32.4% pre-operatively, it rises slightly to 38.5% at T1 anddecreases to 10.6% at T2 (T0–T2: P < 0.001). The SF-36subscales “physical functioning”, “bodily pain”, and “rolephysical” showed the same course over time (slightdecrease of health-related quality of life at T1 and largeincrease at T2). The main patient-reported outcomes weremainly inXuenced by the pre-operative level, age, and self-reported post-operative complaints.Conclusion The low response rate was mainly due tonon-delivery of questionnaires at T1 during the regularpost-operative visit by the operating physician. Thoughnon-response occurs under conditions of routine care,meaningful information was gained which should be usedfor quality improvement activities. Because the pre-opera-tive level is a major determinant of the post-operativehealth outcomes, the prospective pre–post measurementshould be standard, in case institutional comparisons areintended.
Keywords Hernia repair · Quality improvement · Health-related quality of life · Multivariable analysis · Patient-reported outcomes
AbbreviationsBP Bodily painGHP General health perceptionHSCL Hernia symptom checklistMH Mental healthPF Physical functioningRE Role emotionalRP Role physicalSF Social functioningSF-36 Short form-36VI Vitality
The study was funded within the Northern German Public Health Research Association by the Federal Ministry of Education, Science, Research and Technology (Grant ID: 01 EG 9814/9).
E. M. Bitzer (&) · C. Lorenz · H. DörningISEG, Institute for Social Medicine, Epidemiology and Health System Research, Lavesstr. 80, 30159 Hannover, Germanye-mail: [email protected]
S. Nickel · A. TrojanDepartment of Medical Sociology, University Medical Centre Hamburg-Eppendorf, Martinistr. 52, 20246 Hamburg, Germany
123

408 Hernia (2008) 12:407–414
Introduction
Hernia repair is a very common surgical procedure. In Ger-many it is the most frequent procedure in general surgerywith an estimated 200,000 operations per year performed inhospitals [1] and further operations performed in the out-patient setting, for which no data are currently available.
According to two recent systematic reviews [2, 3], noneof the available conventional and laparoscopic surgicaloptions is clearly superior in all aspects, at least in adulthernia repair. The documentation of high-quality care inhernia surgery has been subject to a long discussion [4–6],and the use of patient-reported outcomes in quality-improvement initiatives has been advocated for a long time,e.g. by Burney and colleagues [7]. The feasibility of in-hos-pital documentation of quality indicators and patient-reported outcomes was shown in the late 1990s [8, 9].Despite these early eVorts, asking patients systematicallyabout their perceived outcomes of care does not seem tohave been widely implemented. Patient-reported outcomesinclude health-related quality of life, symptom burden, andtreatment satisfaction [10]. They should be measured bystandardized, validated instruments [11, 12]. In view ofvery short surgical stays, the surgical unit that regularlywants to follow-up its patients after hernia repair to obtainpatient-reported outcomes faces considerable organiza-tional challenges trying to reach all patients before and afterthe operation [13]. The routine application of surveys onpatient-reported outcomes is further complicated, becausestatistical evaluation of patient-reported outcomes mightrequire expertise which is not always immediately availablein surgical practice. We conducted a study as part of anational public health research programme to assess thefeasibility, validity, and usefulness of a quality-monitoringsystem based on patient-reported outcomes in adult herniarepair within a short-stay surgery setting.
Methods
Study design
We conducted a longitudinal survey of patients in twoshort-stay surgical units between 08/1999 and 01/2002.Patients were supposed to be surveyed three times:T0 = 14 days pre-operatively, T1 = 14 days post-opera-tively and T2 = 6 months post-operatively. Questionnairesat T0 and T1 were handed out during the routine pre andpost-operative visits by the treating surgeon. The surgicalunits sent the questionnaires at T2 to those patients whoparticipated in the T1-survey. Patients were oVered a freereply envelope addressed to one of the research institutes(Department of Medical Sociology, Hamburg).
Sample size
Using a power calculation for dichotomous variables todetect diVerences of 25% points with a power of 90% at analpha-level of 0.05, the sample size required was n = 200.Calculating a response rate of 50% after three measure-ments, 400 patients had to be initially recruited.
Instruments to assess patient-reported outcomes
The questionnaires contained items on patient characteris-tics, expectations of the outcome of the surgery, subjectivereasons for undergoing hernia repair, subjective post-opera-tive complaints, and treatment satisfaction.
The hernia symptom checklist (HSCL) [14] was used toassess hernia-related symptoms pre and post-operatively.The HSCL has nine items concerning typical hernia-relatedsymptoms and impairments (i.e. diYculties while bendingforward, impairment in household activities or during stren-uous activities, groin pain, numbness). Symptoms/impair-ments are graded on a four point scale (none, little,moderate, strong). A total score for the HSCL is computedby summing the individual items and transforming thescore into values from 0 to 100, with higher values repre-senting greater impairment.
Health-related quality of life was measured with the Ger-man version of the SF-36 [15]. The SF-36 consists of 36items that are used to calculate eight subscales: physicalfunctioning (PF), role physical (RP), bodily pain (BP), gen-eral health perception (GHP), vitality (VI), social function-ing (SF), role emotional (RE), and mental health (MH). Thesubscales are transformed into values ranging from 0 (poorhealth) to 100 (best health) [16]. The SF-36 has been sug-gested as a core outcome instrument by others [7] and hasbeen applied frequently in hernia patients [2]. We com-pared the health-related quality of life of hernia patientswith that of the German reference population [16], usingnorm-based scoring. Norm-based scoring of the SF-36results in subscale scores, with a value of 50 in the studysample indicating a health-related quality of life equal tothat of the reference population.
Treatment satisfaction was assessed with one global item(“How satisWed are you with the outcome of your herniarepair?”) with four answer categories (very satisWed, rathersatisWed, rather dissatisWed, and very dissatisWed).
Main patient-reported outcomes were changes in theHSCL, the SF-36 subscales PF, BP, and RP, and treatmentsatisfaction at 6 months post-operatively.
Procedural aspects
The participating surgical units were asked to providepatient-related data on procedural aspects (e.g. type of
123

Hernia (2008) 12:407–414 409
hernia repair) from the electronic records of the mandatoryclinical audit. Beyond this no further activities were under-taken to gather such data.
Statistical analyses
Descriptive analyses were performed using frequency dis-tributions, cross tables, mean comparisons, and Spearmanor Pearson correlations. Statistical signiWcance was calcu-lated with the Chi-squared test, t-test for paired andunpaired samples, the Mann–Whitney-U test, and the Wil-coxon test. EVect sizes were calculated for the HSCL andthe three SF-36 subscales, dividing the pre–post-diVerence(pre-operative mean ¡ post-operative mean) by the stan-dard deviation of the pre-value [17]. EVect sizes of 0.8 orlarger were interpreted as large eVects [17].
We used generalized linear models (GLM) [18, 19] to Wtseparate regression models for the Wve main patient-reported outcomes 6 months post-operatively.
Additionally, we performed several analyses addressingnon-response bias (descriptive analysis, inverse probabilityweighted by propensity scores [20], and multiple imputa-tion [21, 22]).
All statistical analyses were performed with standardstatistical software packages (SPSS V14 and SAS V8).
Results
Feasibility
The recruitment of the planned number of patients tooklonger than anticipated. However, after more than two years,pre-operative data for 342 patients were available. Of thesepatients 70.2% (n = 240) answered the T1 questionnaire. Ofthe 240 persons with T1 data, n = 185 (77%) answered theT2 questionnaire also, resulting in an overall response rate of54.1%. Analysis of response rates by the surgical unitrevealed signiWcant diVerences: Surgical unit 1 obtained anoverall response rate of 65.1% whereas surgical unit 2 onlyachieved 40.5% (P < 0.001). Further analyses showed thatthe largest drop-outs occurred at T1, suggesting organiza-tional diYculties while distributing the questionnaires.
Overall, the intended schedule was achieved—the pre-operative survey was conducted on average 8 days beforethe surgery, T1 questionnaires were Wlled in 13 days post-operatively, and the T2 survey was answered 6.1 monthspost-operation (Table 1).
Only one of the surgical units was able to provide data onprocedural aspects (e.g. type of hernia repair); the other surgi-cal unit did not supply such data for technical reasons. There-fore, the percentage of patients with valid T0 questionnairesand information on procedural aspects was low (51.9%).
Sample characteristics
Patients answering the questionnaire at T2 had a mean ageof 58.6 years, and 92.4% were male. A Wfth of the patientswere operated at both sides at the same time, for every tenthpatient surgery was performed for recurrent groin hernia(Table 1).
As mentioned above, information on the type of surgerywas available for only 51.9% of the study population, allparticipants from the one surgical unit that provided data.Most of these patients had a conventional hernia repair(77.6%) and 16.4% a laparoscopic procedure.
Post-operative complaints
Many patients (79.8%) reported some sort of post-operativecomplaints (Table 2). Most cited were “haematoma” and“numbness”; almost every second patient reported suVeringfrom at least one of these two medical conditions after theoperation. Reporting a complaint did not depend on age,gender, and whether the surgery was for primary or recur-rent groin hernia (results not presented).
Time course of groin hernia-related symptoms
Table 3 provides an overview of the change in single symp-toms and in the HSCL-score over time. To simplify the inter-pretation, the four answer categories of the single items weresummarized into two categories, leaving “high = moderate or
Table 1 Patient characteristics (n = 185)
a Available for 98 patients from one of the surgical units only
Characteristic N (%)
Male 171 (92.4%)
Female 14 (7.6%)
Age (mean, median) 58.6 (60) years
Unilateral hernia repair 144 (78.2%)
Bilateral hernia repair 40 (21.7%)
Primary hernia repair 162 (89.0%)
Recurrent hernia repair 20 (10.9%)
Conventional surgerya 76 (77.6%)
with implant 40 (52.6%)
Laparoscopic surgerya 16 (16.4%)
with implant 16 (100%)
Length of stay (mean, median) 2 (2) days
Time to/from surgery
T0 (mean, median) ¡8.3 (4) days
T1 (mean, median) +13.3 (11) days
T2 (mean, median) +6.2 (6.1) months
123

410 Hernia (2008) 12:407–414
strong” and “low = no or little”. According to Table 3, nearlythree quarter of the patients were bothered by groin swelling,and more than half of the group felt pre-operatively highlyimpaired during strenuous activities or sport. About one thirdreported high levels of pain, burning, numbness, problemsduring work or household activities and while coughing orpressing before the operation.
As expected, the single items show that shortly after theoperation limitations in daily life are common. However,after 6 months the percentage of persons reporting highlevels of impairment has dropped dramatically. In general,more than 80% of the persons who report pre-operativehigh levels of impairment show large improvement6 months post-operatively.
As expected, the HSCL-score reXects the time course ofgroin hernia-related symptoms well: the pre-operative level
was 32.4%, showing signiWcant impairment in this popula-tion. Shortly after the surgery the HSCL-score increased to38.5%, indicating small but statistically signiWcant deterio-ration of symptoms (P < 0.01). After 6 months the HSCL-score decreased to a level of 10.6%. The diVerence betweenthe HSCL at T0 to the HSCL at T2 was statistically highlysigniWcant (P < 0.001) and the eVect size was high (1.16).
Time course of health-related quality of life
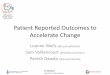
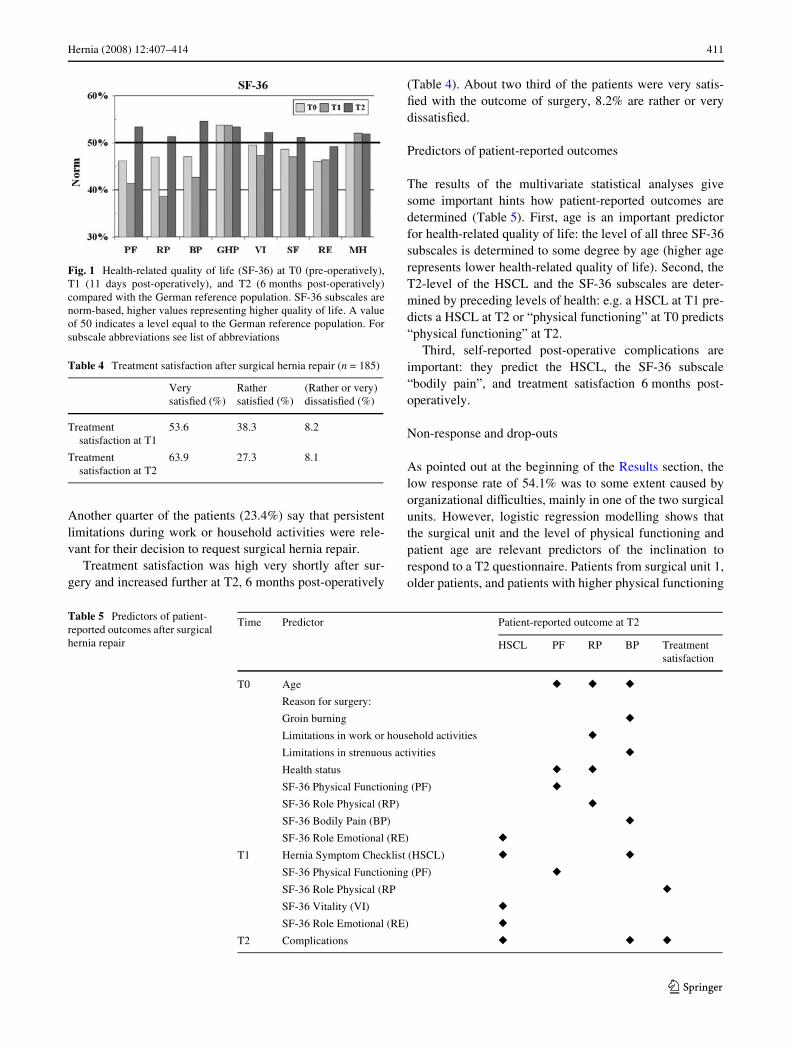
Figure 1 displays the SF-36 subscale scores at T0, T1, andT2, Table 4 summarizes the respective numbers and theresults of the statistical tests. From Fig. 1 one can see thatthe SF-36 subscales “physical functioning”, “bodily pain”,and “role physical” are the areas of health-related quality oflife most impaired before the surgery, compared with theGerman reference population. Shortly after surgery thelevel of the reference population has not reached the levelof the reference population in six of the eight SF-36 sub-scales, whereas 6 months post-operatively all eight sub-scales reach or surpass the level of the reference populationindicating high health-related quality of life.
Patient expectations and treatment satisfaction
Patients have high expectations of the outcome of surgicalhernia repair: 91.8% expect complete freedom from impair-ments or symptoms, 8.2% expect at least a signiWcantimprovement. Limitations in strenuous activities and sport,and groin burning are cited as “reason for undergoing sur-gery” by half of the study sample (50.5 and 45.1%).
Table 2 Post-operative complaints at T2 (n = 185, multiple answerswere possible)
a Males only (n = 170)
Complaint n (%)
Any Complaint 146 (79.9%)
Wound infection 1 (0.5%)
Seroma 17 (9.2%)
Numbness 67 (36.2%)
Haematoma 59 (31.9%)
Scrotal swellinga 38 (22.4%)
Problems passing urine 10 (5.4%)
Sexual dysfunctiona 18 (10.6%)
Other complaints 43 (23.2)
Table 3 Impairment by groin hernia before and at two points in time after surgical repair (n = 178)
Highly impaired: Answer categories “moderate” or “strong”
Example: 28.1% of the sample said that they felt moderately to strongly impaired by numbness in the groin, pre-operatively. Shortly after surgerythe percentage being highly impaired increases to 41.6%, but decreases to 13.5% 6 months post-operatively. 82% of the initially highly impairedpatients report little or no numbness 6 months after the operationa Percentage of patients who reported high impairment pre-operatively and low impairment post-operatively
Symptom/Impairment Highly impaired (%) Highly improved (%)a (T2)
T0 Pre-OP T1 Post-OP T2 Post-OP
Groin swelling 71.3 37.6 9.0 91.3
Limitation in strenuous or sporting activities 57.3 62.9 10.7 87.3
Groin burning 39.9 37.6 10.1 88.7
Pain 36.0 37.1 11.2 82.8
Limitation during work or household activities 33.7 47.2 5.1 88.3
Problems while coughing or pressing 33.1 42.1 2.8 100.0
Numbness 28.1 41.6 13.5 82.0
Problems while bending forward 15.7 32.6 3.4 96.4
Problems passing urine 7.9 5.1 5.1 64.3
HSCL (Mean) (Minimum–Maximum) 32.4 (0.0–88.9) 38.5 (0–92.6) 10.6 (0–63.0) EVect size: 1.16
123
Hernia (2008) 12:407–414 411
Another quarter of the patients (23.4%) say that persistentlimitations during work or household activities were rele-vant for their decision to request surgical hernia repair.
Treatment satisfaction was high very shortly after sur-gery and increased further at T2, 6 months post-operatively
(Table 4). About two third of the patients were very satis-Wed with the outcome of surgery, 8.2% are rather or verydissatisWed.
Predictors of patient-reported outcomes
The results of the multivariate statistical analyses givesome important hints how patient-reported outcomes aredetermined (Table 5). First, age is an important predictorfor health-related quality of life: the level of all three SF-36subscales is determined to some degree by age (higher agerepresents lower health-related quality of life). Second, theT2-level of the HSCL and the SF-36 subscales are deter-mined by preceding levels of health: e.g. a HSCL at T1 pre-dicts a HSCL at T2 or “physical functioning” at T0 predicts“physical functioning” at T2.
Third, self-reported post-operative complications areimportant: they predict the HSCL, the SF-36 subscale“bodily pain”, and treatment satisfaction 6 months post-operatively.
Non-response and drop-outs
As pointed out at the beginning of the Results section, thelow response rate of 54.1% was to some extent caused byorganizational diYculties, mainly in one of the two surgicalunits. However, logistic regression modelling shows thatthe surgical unit and the level of physical functioning andpatient age are relevant predictors of the inclination torespond to a T2 questionnaire. Patients from surgical unit 1,older patients, and patients with higher physical functioning
Fig. 1 Health-related quality of life (SF-36) at T0 (pre-operatively),T1 (11 days post-operatively), and T2 (6 months post-operatively)compared with the German reference population. SF-36 subscales arenorm-based, higher values representing higher quality of life. A valueof 50 indicates a level equal to the German reference population. Forsubscale abbreviations see list of abbreviations
Table 4 Treatment satisfaction after surgical hernia repair (n = 185)
Very satisWed (%)
Rather satisWed (%)
(Rather or very) dissatisWed (%)
Treatment satisfaction at T1
53.6 38.3 8.2
Treatment satisfaction at T2
63.9 27.3 8.1
Table 5 Predictors of patient-reported outcomes after surgical hernia repair
Time Predictor Patient-reported outcome at T2
HSCL PF RP BP Treatment satisfaction
T0 Age � � �
Reason for surgery:
Groin burning �
Limitations in work or household activities �
Limitations in strenuous activities �
Health status � �
SF-36 Physical Functioning (PF) �
SF-36 Role Physical (RP) �
SF-36 Bodily Pain (BP) �
SF-36 Role Emotional (RE) �
T1 Hernia Symptom Checklist (HSCL) � �
SF-36 Physical Functioning (PF) �
SF-36 Role Physical (RP �
SF-36 Vitality (VI) �
SF-36 Role Emotional (RE) �
T2 Complications � � �
123

412 Hernia (2008) 12:407–414
at T0 were more likely to respond at T2 than patients fromsurgical unit 2, younger patients, and patients with lowerlevels of physical functioning (results not depicted). Toaccount for drop-outs, we used the reciprocal of the indi-vidual probability to respond (derived from the logisticregression model) as a weight [20], and repeated alldescriptive and multivariate analyses. In a second approachwe used the rather complex technology of multiple imputa-tion to account for drop-outs (details not depicted).
Neither the weighted nor the multiple imputed scores ofthe patient-reported outcomes showed remarkable or statis-tically signiWcant diVerences compared with the observedscores in the responding population. For instance: theobserved HSCL-score was 10.5 points (95% CI 8.6–12.5),the weighted HCSL-score equalled 11.0 (95% CI 8.9–13.0), and the multiple imputed HSCL-score was 11.3 (9.1–13.5).
Discussion
Hernia symptom checklist and SF-36
Both instruments were able to provide detailed informationabout the post-operative course of impairments and health-related quality of life after hernia repair. The worsening ofthese outcomes shortly after surgery reXects the impairmentcaused by the surgical procedure itself whereas the largeimprovement 6 months post-operatively shows that most ofthe patients are well-oV after their groin hernia surgery.These data, gathered under routine surgical care for quality-management reasons, are comparable with results fromseveral randomised controlled trials for diVerent hernia-repair procedures that used either the SF-36 and/or otherhernia-speciWc questionnaires [23–27].
Treatment satisfaction
Levels of treatment satisfaction across diVerent studies arediYcult to compare, due to the diVerent measurementmethods used. We were able to compare our data with resultsfrom two other German surveys that used the same singleitem to assess treatment satisfaction with hernia repair andwere conducted in the years 1996/1997 [14] and 2005 [28].In both of these studies members of large German sicknessfunds were surveyed, so the results do not refer to a singleinstitution but rather represent a view on the overall level oftreatment satisfaction. The percentage of very satisWedpatients in these two studies was 62.9% [14] and 64.6%[28], in the study presented here it was 63.9%. This Wndingis reassuring, because not only has surgical management ofgroin hernia undergone signiWcant developments in the last10 years but also the Wnancial and resource constraints on
the hospital sector have led to a marked reduction in thelength of stay for hernia repair. In other words, the level oftreatment satisfaction reached by the two surgical units inthis study indicates that a short-stay surgery for groin her-nia repair leads to as much treatment satisfaction as otherorganizational forms.
Predictors of patient-reported outcomes
The predictors we identiWed can be classiWed as modiWableand non-modiWable—age, pre-operative symptom level,and pre-operative level of health-related quality of life arenot modiWable by a surgical unit but the frequency ofpatient-reported post-operative complaints might be. Theastonishingly high frequency of patient-reported post-oper-ative complaints and complications is diYcult to explain.On one side, the results from several randomised controlledtrials reveal quite divergent, and usually much lower, ratesof speciWc complications [23, 29]; on the other side, the twosurveys we conducted at our department [14, 28] had atleast to some degree similar results (i.e. 66.9% reporting atleast one complaint, 29.9% reporting numbness, about oneWfth of patients reporting haematoma or scrotal swelling[28]). Even if these complaints may not be serious in termsof re-hospitalisation or surgical revision, they predict thelevel of health-related quality of life and treatment satisfac-tion and, therefore, should be taken serious in terms ofquality management. For instance, clear and understand-able pre-operative counselling, addressing the impairmentsand symptoms that are “normal” after hernia repair mightenable patients to better anticipate the post-operativeburden.
If patient-reported outcomes are to be used as bench-marks, the pre-operative levels turn out to be of crucialimportance since they are major predictors of post-opera-tive outcomes. According to the results presented here,comparing diVerent surgical units by the patient-reportedoutcomes requires adjustment for pre-levels. Otherwise thevalidity of the comparisons might be questioned.
Feasibility, non-response, and drop-outs
In this study it proved diYcult to implement procedures todistribute survey materials within the surgical units. This isnot a particularly new problem, either in quality manage-ment or in clinical trials. However, these diYculties lead toa rather long recruiting period and a considerable numberof drop-outs.
Because of the long recruiting period the Wnal resultswere presented to the surgical units in March 2003, oneyear after the last patient had been enrolled, but almost4 years after the Wrst patient was recruited. One might arguethat the long time from the Wrst patient recruited until the
123

Hernia (2008) 12:407–414 413
availability of the results impedes timely integration of theWndings in quality-management activities. But in the caseof groin hernia repair, the overall quality is high, and severeadverse outcomes (e.g. mortality) that would call for imme-diate action are extremely rare in routine health care.Patient-reported outcomes in groin hernia repair might notbe suitable for monitoring rare adverse events, but can shedlight on other important aspects of quality of care from thepatient’s perspective.
The low response-rate at 6 months post-operativelyraises concern about how representative the sample is forall patients treated in the two participating surgical units.According to our diVerent approaches used to investigate apotential non-response bias, such bias is expected to besmall. However, high drop-outs lead to prolonged recruit-ing times and analysing non-responders further increasesthe statistical workload. And even with the best statisticaloptions, at least some doubts about the validity of theresults may remain.
As pointed out in the Introduction, one element thatmight hamper the routine use of patient-reported outcomesis the need for statistical expertise. This has been conWrmedin this study—although the instruments used to assesspatient-reported outcomes in this study were well docu-mented and detailed descriptions on how to score themwere available, this was only half the way. The calculationof scale-scores is only a small part of a comprehensive dataanalysis and further expertise is required, e.g. for multivari-able modelling or detailed non-response analyses.
So, from that point of view, the rapid implementation ofa comprehensive quality-monitoring system based onpatient-reported outcomes seems to be rather unlikely,unless there are incentives for surgical units for implement-ing or participating in such a system.
Acknowledgments We would like to thank both co-operating surgi-cal units, the interdisciplinary Centre for Short-stay Surgery at theKlinikum Nord-Heidberg, and the Short-stay Unit of the Klinik Eilbek,both located in Hamburg.
References
1. Bundesministerium für Gesundheit (1999) OperationshäuWgkeitenin Deutschland. Nomos, Baden-Baden
2. Gerhardus A, Jalivand N, Heintze C, Krauth C (2003) Ein Vergl-eich verschiedener chirurgischer Verfahren zur elektiven Leisten-hernienoperation bei Erwachsenen—Ein Health TechnologyAssessment. Schriftenreihe HTA des DIMDI (MedizinischeHochschule Hannover), Band 30. Asgard, Sankt Augustin
3. McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E,Vale L, Grant A (2005) Laparoscopic surgery for inguinal herniarepair: systematic review of eVectiveness and economic evalua-tion. Health Technol Assess 9:1–iv
4. Grundmann RT (1996) Qualitätssicherung in der Chirurgie-mehrals nur die Erfassung post-operativer Komplikationen. ZentralblChir 121:157–166
5. Troidl H (1997) Qualitätskontrolle in der Leistenhernienchirurgie.Chirurg 68:1225–1234
6. Hupe K, Wenning M (2000) Wert der heutigen Qualitätssicherungfur die Chirurgie. Zentralbl Chir 125(Suppl 2):146–148
7. Burney RE, Jones KR, Blewitt DK, Herm A, Peterson M (1997)Core outcomes measures for inguinal hernia repair. J Am CollSurg 185:509–515
8. Junginger T, Küchle R, Dutkowski P, Thumerer A (1998)Systematische klinikinterne Qualitätskontrolle in der Chirurgie1993 bis 1997. Z Ärztl Fortbild Qualitätssich 92:705–714
9. Jones KR, Burney RE, Peterson M, Christy B (1998) Measuringhealth-status improvement after surgery: experience with theSF-36. Semin Nurse Manag 6:139–143
10. Schwartz FW, Bitzer EM, Dörning H, Walter U (2002) Evaluationund Qualitätsmanagement. In: Hurrelmann K, Laser E (Hg) Hand-buch für Gesundheitswissenschaften. Juventa, Weinheim,
11. Kohlmann T, Steinke I, Berger K, Deck R, John J, Pohlabeln H,Rieger J, Nickel S, Uhlig S (2000) Empfehlungen zur Auswahlund Anwendung von Erhebungsinstrumenten und Auswertungs-verfahren in der Public Health-Forschung. Public Health Forum8:11–13
12. Garratt A, Schmidt L, Mackintosh A, Fitzpatrick R (2002) Qualityof life measurement: bibliographic study of patient assessed healthoutcome measures. Br Med J 324:1417
13. Lopez-Cano M, Vilallonga R, Sanchez JL, Hermosilla E,Armengol M (2007) Short postal questionnaire and selective clin-ical examination combined with repeat mailing and telephonereminders as a method of follow-up in hernia surgery. Hernia11:397–402
14. Bitzer EM, Dörning H, Schwartz FW (2000) Der Erfolg von Leis-tenbruchoperationen in der Routineversorgung aus der Sicht derPatienten. Chirurg 71:829–834
15. Bullinger M (1996) Erfassung der gesundheitsbezogenen Leb-ensqualität mit dem SF-36 Health Survey: Hinweise auf Bewer-tungsinstrumente zur Qualitätssicherung in der Rehabilitation—Blatt 7. Rehabilitation 35:XVII–XXXX
16. Bullinger M, Kirchberger I (1998) Der SF-36 Fragebogen zumGesundheitszustand. Handanweisung. Hogrefe, Göttingen
17. Norman GR, Wyrwich KW, Patrick DL (2007) The mathematicalrelationship among diVerent forms of responsiveness coeYcients.Qual Life Res 16:815–822
18. Nelder JA, Wedderburn RWM (1972) Generalized linear models.J R Stat Soc Ser A 135:370–384
19. McCullagh P, Nelder JA (1989) Generalized linear models, 2ndedn. Chapman and Hall, London
20. HöXer M, PWster H, Lieb R, Wittchen HU (2005) The use ofweights to account for non-response and drop-out. Soc PsychiatryPsychiatr Epidemiol 40:291–299
21. Rubin DB (1987) Multiple imputation for nonresponse in surveys.Wiley, Chichester
22. Schafer JL (1997) Analysis of incomplete multivariate data.monographs on statistics and applied probability, vol 72. Chapman& Hall, New York
23. Wellwood J, Sculpher MJ, Stoker D, Nicholls GJ, Geddes C,Whitehead A, Singh R, Spiegelhalter D (1998) Randomised con-trolled trial of laparoscopic versus open mesh repair for inguinalhernia: outcome and cost. Br Med J 317:103–110
24. Lawrence K, McWhinnie D, Jenkinson C, Coulter A (1997)Quality of life in patients undergoing inguinal hernia repair. AnnR Coll Surg Engl 79:40–45
25. Velanovich V (2000) Laparoscopic vs open surgery: a prelimi-nary comparison of quality-of-life outcomes. Surg Endosc14:16–21
26. Vrijland WW, van den Tol MP, Luijendijk RW, Hop WC, Bussch-bach JJ, de Lange DC, van Geldere D, Rottier AB, Vegt PA, IJzer-mans JN, Jeekel J (2002) Randomized clinical trial of non-mesh
123

414 Hernia (2008) 12:407–414
versus mesh repair of primary inguinal hernia. Br J Surg 89:293–297
27. Leibl B, Daubler P, Schwarz J, Ulrich M, Bittner R (1995) Stan-dardisierte laparoskopische Hernioplastik vs. Shouldice-Repara-tion. Ergebnisse einer randomisierten Vergleichsstudie. Chirurg66:895–898
28. Bitzer EM, Grobe TG, Dörning H, Schwartz FW (2006) GEK-Re-port akut-stationäre Versorgung 2006—Schwerpunkt: Leisten-bruchoperationen und Cholecystektomie. Asgard, St. Augustin
29. MRC Laparoscopic Groin Hernia Trial Group (1999) Laparo-scopic versus open repair of groin hernia: a randomised compari-son. Lancet 354:185–190
123