Embed Size (px)
Citation preview
Journal of Nursing Scholarship Second Quarter 2002 173
Health Policy and Systems
Patient satisfaction with care and patients’ views ofdesired outcomes are increasingly important to payersand providers in evaluating quality of health care, to
market-driven purveyors of care in attracting and keepingcustomers, and to patients as they weigh alternatives in seekingelective care (Christensen & Inguanzo, 1989; Oswald, Turner,Snipes, & Butler, 1998; Rosenthal & Shannon, 1997). Althoughpatients were once thought ill-prepared to render appropriatejudgment regarding the technical components of quality of care(Cleary & McNeil, 1988), they are increasingly recognized askey informants about all aspects of quality including technicaland interpersonal (Rubin et al., 1993). Their viewpoints havebecome particularly important in the current economic climate,when providers of care compete more on quality than onuniformly discounted cost (Becker, 1998). The secondaryanalysis reported in this paper was done to compare patients’,nurses’, and physicians’ views’ of quality of care and patientsatisfaction.
Patients, Nurses, and Physicians HaveDiffering Views of Quality of Critical CareSarah E. Shannon, Pamela H. Mitchell, Kevin C. Cain
Purpose: To compare patient, nurse, and physician assessments of quality of care and patientsatisfaction in selected critical care units.
Design: As part of a study of patient outcomes from critical care, data were collected betweenDecember 1991 and March 1993 from 489 patients, 518 nurses, and 515 physicians in 25critical care units located in 14 hospitals in the U.S. Pacific Northwest.
Methods: Views of patient satisfaction and quality of care were measured using standardizedinstruments. All data were aggregated to the unit level (N=25) and were normalized to acommon scale for analysis.
Findings: Physicians rated quality of care higher than did either patients or nurses within thesame critical care unit, and nurses had the lowest perceptions of quality. Nurses and patientshad similar views of patient satisfaction, but physicians tended to overestimate patients’satisfaction. However, physicians’, nurses’, and patients’ scores varied considerably withinand between units. Physicians’ and nurses’ views of quality and patient satisfaction werestrongly related to processes such as MD-RN collaboration and outcomes such as nurses’job satisfaction.
Conclusions: Patients, nurses, and physicians viewed quality of care and patient satisfactiondifferently. Nurses’ and physicians’ perspectives were more related to their views of thework environment than to organizational factors, patient characteristics, or commonly usedoutcome measures.
JOURNAL OF NURSING SCHOLARSHIP, 2002; 34:2, 173-179. ©2002 SIGMA THETA TAU INTERNATIONAL.
[Key words: care delivery system, continuous quality improvement, outcome evaluation,patient outcomes, critical care, secondary analysis, correlational, systems]
* * *
Background
Obtaining patients’ viewpoints may be difficult, particularlyin settings such as critical care where the effects of illness ortreatment may interfere with patients’ cognition orconsciousness. In such situations, substituting provider ratingsfor patient ratings (Shortell et al., 1994) is tempting. Based
Sarah E. Shannon, RN, PhD, Psi-at-large, Associate Professor, Pamela H.Mitchell, RN, PhD, FAAN, Psi-at-large, Professor & Associate Dean, Kevin C.Cain, PhD, Associate Professor, all at University of Washington School ofNursing, Seattle. The authors acknowledge Dr. Sue Hegyvary, Dr. Karen Seachrist,and the graduate student research assistants from the CCNS Study. Fundingin part from NIH, NINR RO1 NR02343. Correspondence to Dr. Shannon,Box 357266, University of Washington, School of Nursing, Seattle, WA 98195-7266. E-mail: [email protected]
Accepted for publication October 24, 2000.

174 Second Quarter 2002 Journal of Nursing Scholarship
Views of Quality
on several research studies, Nelson and colleagues said that“Better quality in the eyes of patients will also be regardedas better quality in the eyes of other critical customer groups[physicians and nurses]” (Nelson et al., 1992).
A test of this assumption of interchangeability was foundin only three studies. One study reported patients’ and clinicalstaffs’ ratings of “ward atmosphere” in three VeteransAdministration neuropsychiatric hospitals (Rice, Berger, Klett,Sewall, & Lemkau, 1963). In that small study, the rank orderof satisfaction with ward atmosphere was identical betweenpatients and staff for four wards in each of two of thehospitals. However, ward atmosphere was a differentconstruct from the elements of quality typically included inmeasures of patient satisfaction. Carson and colleagues(1996) alluded to data regarding nurse, physician, and patientratings of aspects of quality care and satisfaction in acomparison of open versus closed medical staffing of anintensive care unit, but the results were not provided in thepublished paper. Kurata and colleagues reported physicians’and patients’ views of satisfaction with ambulatory care, andalso found patients more satisfied with most aspects of carethan were providers (Kurata, Nogawa, Phillips, Hoffman,& Werblun, 1992).
Multiple provider and patient assessments of quality andsatisfaction have rarely been gathered simultaneously in acutecare during the same time period (Mitchell, 1991). A multiple-site comparison of critical care unit outcomes andorganizational features showed data that allowed us toexamine patients’, physicians’, and nurses’ views of qualityof care and patient satisfaction measured concurrently to testthe assumption of interchangeability. Current questions aboutquality and satisfaction indicate the need to examine availabledatabases, such as this one, to identify relationships amongthese process and outcome variables.
Methods
Instruments and ProcedureThis report is based on a secondary analysis from a multisite
study of critical care unit outcomes and organizationalfeatures (Mitchell, Shannon, Cain, & Hegyvary, 1996). Dataabout patients’ severity of illness were collected over 1 yearin a convenience sample of 25 critical care units, with surveyand observational data collected over 1 to 2 months duringa unit’s study year. Because of the large number of units, theentire data-collection process occurred over 18 months, fromDecember 1991 through May 1993. Data regardingsatisfaction and quality of care were collected from 489patients (M=20 patients per unit; range=7-24), 518 nurses(M=21; range=6-41), and 515 physicians (M=21; range=4-40)in 25 critical care units and were aggregated to the unit levelfor correlational analysis. The critical care units were locatedin 14 hospitals in the greater Puget Sound region of the PacificNorthwest. Four hospitals were part of multiple hospitalsystems, and the critical care units ranged from specializedunits, such as cardiovascular or burn, to mixed medical-
surgical units. The majority were relatively small, mixedmedical-surgical units, averaging 12 beds per unit (range 4to 22 beds). Sixteen of the 25 critical care units were inteaching hospitals (nine members and seven nonmembers ofthe Council of Teaching Hospitals [COTH]). Five of thecritical care units were in one hospital; the others were theonly unit or one of two units in a given hospital. At the timeof the study, all units had all-registered-nurse (RN) staffingand none limited admitting privileges to physician intensivists.
Description and psychometric properties of instrumentshave been reported. All instruments retained acceptablepsychometric properties in the sample for this study, whenanalyzed at both the individual and unit-aggregate levels(Mitchell et al., 1996).
Patients’ perceptions of quality and satisfaction with careduring a critical care stay were measured by three subscalesfrom the Medicus “Viewpoint” instrument selected forrelevance to critical care patients’ experience (Hegyvary,Packard, & Jelinek, 1988). A 9-item subscale was focused onthe overall care environment such as “being cared for by friendlypeople” and “respect for my personal preferences in my careand treatment.” A 5-item subscale related to having assistancewith comfort and support such as “personal hygiene” and“coping with the emotional stress and strain.” Finally, a 7-item subscale was focused on being kept informed about thecourse of treatment, such as “who my main doctor would be”and “the medical purpose of the tests, treatments, surgery, orother procedures.”
The instrument was administered to patients within 48 hoursof transfer from intensive care to a general medical or surgicalunit. Patients were asked to rate the quality of care in the criticalcare unit for a given item on a 4-point scale (ranging from1=poor quality to 4=outstanding quality) and the importanceof that item to them on a similar scale (ranging from 1=notvery important to 4=extremely important). Satisfaction wascalculated as the patient’s perception of quality weighted bythe importance of the item, resulting in a 16-point scale rangingfrom -8 (low quality and very important) to +8 (high qualityand very important). All scores were then normalized to a 0-100 scale to allow for comparisons with other instruments.
Nurses’ and physicians’ views of unit quality and of patientsatisfaction with care were obtained from portions of the CharnsOrganizational Diagnosis Survey (CODS; Charns, Stoelwinder,Millen, & Schaefer, 1980). The CODS Physician Opinionnaireis a 24-item Likert-type scale to rate aspects of unit function.The physicians’ view of overall unit quality is measured byeight items such as “The medical needs of patients are met,”“There is a high quality of care,” and “The overall error ratefor patient care is low.” Physicians’ perception of patientsatisfaction is measured by two items: “Patients are satisfiedwith the care they receive,” and “Families of my patients arepleased with the nursing care they receive in this unit.” Thesurvey also indicates physicians’ views of RN and MD quality(three items each) and RN-MD collaboration (seven items).Four items were not included in this analysis.
The CODS Job Inventory, a 25-item survey withcomparable items to the Physician Opinionnaire, was given
Journal of Nursing Scholarship Second Quarter 2002 175
Views of Quality
to registered nurses. Nurse perception of unit quality wasmeasured by three items such as “Patients get better care onmy unit than on similar units in the city.” Nurse perceptionof patient satisfaction was measured by two items: “Patientson my unit are pleased with the care they receive” and“Families of my patients are pleased with the nursing carethey receive.” RN-MD collaboration is measured by fouritems and nurse job satisfaction by seven items. Nine itemswere not included in this analysis. Both physicians’ andnurses’ scores were normalized to a 0-100 scale.
Selected descriptive and outcome variables measured inthe original study were included in this analysis (Mitchell etal., 1996). Patients’ age, severity of illness, ICU length ofstay, and hospital length of stay were measured usingAPACHE III methodology (Knaus et al., 1991) from arandom sample of approximately 340 patients’ medicalrecords from each of the 25 critical care units (N=8,502).The outcome variable of observed quality of nursing carewas measured using the Medicus Quality First instrument(Hegyvary, Wood, & Jelinek, 1988) which allows rating sevencomponents of critical care nursing through researcherobservations of care delivery and documentation of care.
The study was approved for protection of human subjectsby institutional review boards of the university and the 14participating hospitals. Informed consent was obtained frompatients and staff who completed surveys. All physicians andnurses practicing in the 25 critical care units were invited byletter and during presentations at staff meetings to participatein the study. Similarly, patients who completed the satisfactionwith quality of care survey were a convenience sample ofcritical care patients who agreed to participate and wereavailable during data-collection periods.
Data Aggregation and AnalysisThe unit of analysis for this study was the critical care
unit, not individual clinicians or patients. Hence, data wereaggregated to the critical care unit level for all analyses andmet criteria for group referents, interitem, and intraclasscorrelations (Rousseau, 1985; Verran, Gerber, & Milton,1995; Verran, Mark, & Lamb, 1992). All data showedadequate instrument reliability at both individual and grouplevels. Intraclass correlations, eta-squared, and ANOVAindicated greater homogeneity within units than among units,indicating that unit level data were conceptually valid ratherthan merely showing the average of a group of unrelatedindividuals.
Results
Table 1 shows descriptive data about the key variables andstructural characteristics of the participating sites. The hospitalswere a mix of tertiary and community hospitals, with an averageof 316 beds. Critical care units were a mixture of special andmixed medical-surgical critical care units.
Overall, physicians’ opinions about unit quality andperceptions of patient satisfaction were higher than were
patients’ or nurses’ perspectives. Nurses and patients had similarviews of patient satisfaction, but nurses’ ratings of unit qualitywere generally lower than were patients’ ratings of the qualityof care they received. For both quality of care and patientsatisfaction, the variability of unit scores was relatively low(SD ranged from 4.76-5.87) except for nurses’ views of unitquality (SD=10.42), which varied considerably among units.The low variability on the other measures is similar to therelatively low variability on satisfaction measures reported inthe literature (Rosenthal & Shannon, 1997).
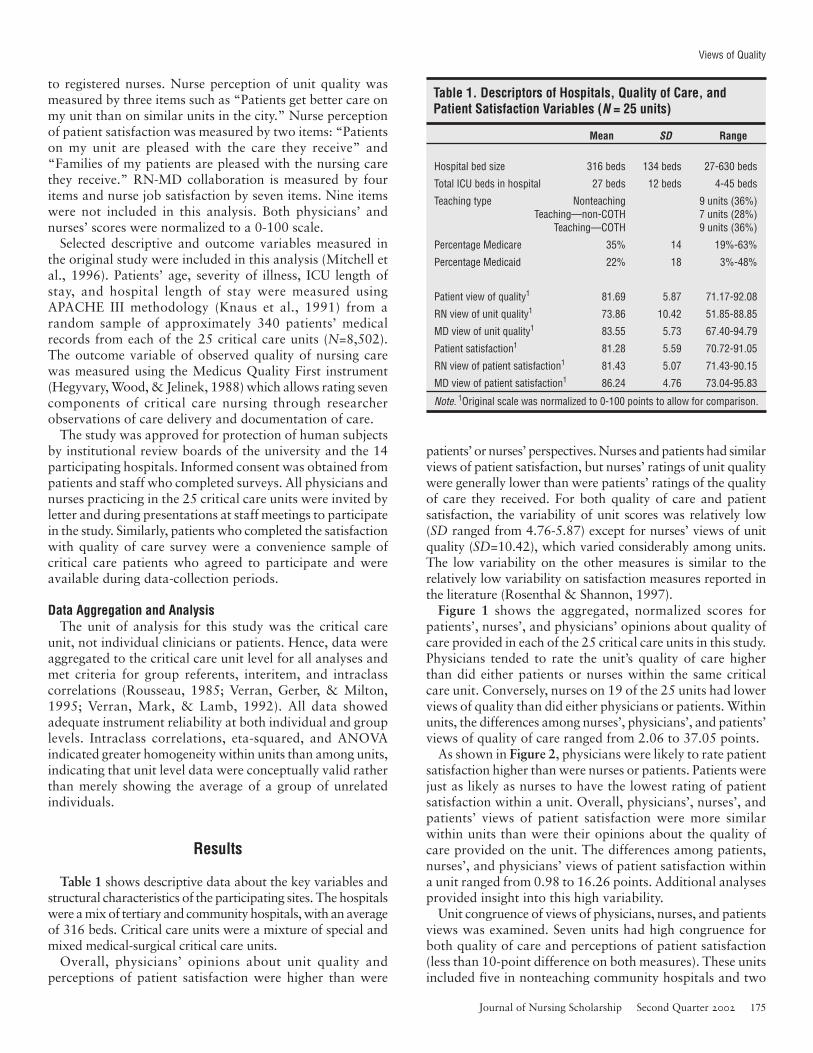
Figure 1 shows the aggregated, normalized scores forpatients’, nurses’, and physicians’ opinions about quality ofcare provided in each of the 25 critical care units in this study.Physicians tended to rate the unit’s quality of care higherthan did either patients or nurses within the same criticalcare unit. Conversely, nurses on 19 of the 25 units had lowerviews of quality than did either physicians or patients. Withinunits, the differences among nurses’, physicians’, and patients’views of quality of care ranged from 2.06 to 37.05 points.
As shown in Figure 2, physicians were likely to rate patientsatisfaction higher than were nurses or patients. Patients werejust as likely as nurses to have the lowest rating of patientsatisfaction within a unit. Overall, physicians’, nurses’, andpatients’ views of patient satisfaction were more similarwithin units than were their opinions about the quality ofcare provided on the unit. The differences among patients,nurses’, and physicians’ views of patient satisfaction withina unit ranged from 0.98 to 16.26 points. Additional analysesprovided insight into this high variability.
Unit congruence of views of physicians, nurses, and patientsviews was examined. Seven units had high congruence forboth quality of care and perceptions of patient satisfaction(less than 10-point difference on both measures). These unitsincluded five in nonteaching community hospitals and two
Table 1. Descriptors of Hospitals, Quality of Care, andPatient Satisfaction Variables (N = 25 units)
Mean SD Range
Hospital bed size 316 beds 134 beds 27-630 beds
Total ICU beds in hospital 27 beds 12 beds 4-45 beds
Teaching type Nonteaching 9 units (36%)Teaching—non-COTH 7 units (28%)
Teaching—COTH 9 units (36%)
Percentage Medicare 35% 14 19%-63%
Percentage Medicaid 22% 18 3%-48%
Patient view of quality1 81.69 5.87 71.17-92.08
RN view of unit quality1 73.86 10.42 51.85-88.85
MD view of unit quality1 83.55 5.73 67.40-94.79
Patient satisfaction1 81.28 5.59 70.72-91.05
RN view of patient satisfaction1 81.43 5.07 71.43-90.15
MD view of patient satisfaction1 86.24 4.76 73.04-95.83
Note. 1Original scale was normalized to 0-100 points to allow for comparison.
176 Second Quarter 2002 Journal of Nursing Scholarship
Views of Quality
units in COTH tertiary care facilities. Two of the criticalcare units were in the same hospital and the other five werethe only critical care units in the hospital. Three of the unitswere specialized units and the other four were mixed medical-surgical units.
Four units had low congruence among patients’, nurses’and physicians’ views for both quality of care and patientsatisfaction (greater than 20-point difference for qualityvariables and greater than 10-point difference for patientsatisfaction). All of these units were specialized critical careunits. Three were in non-COTH hospitals and one was in aCOTH hospital.
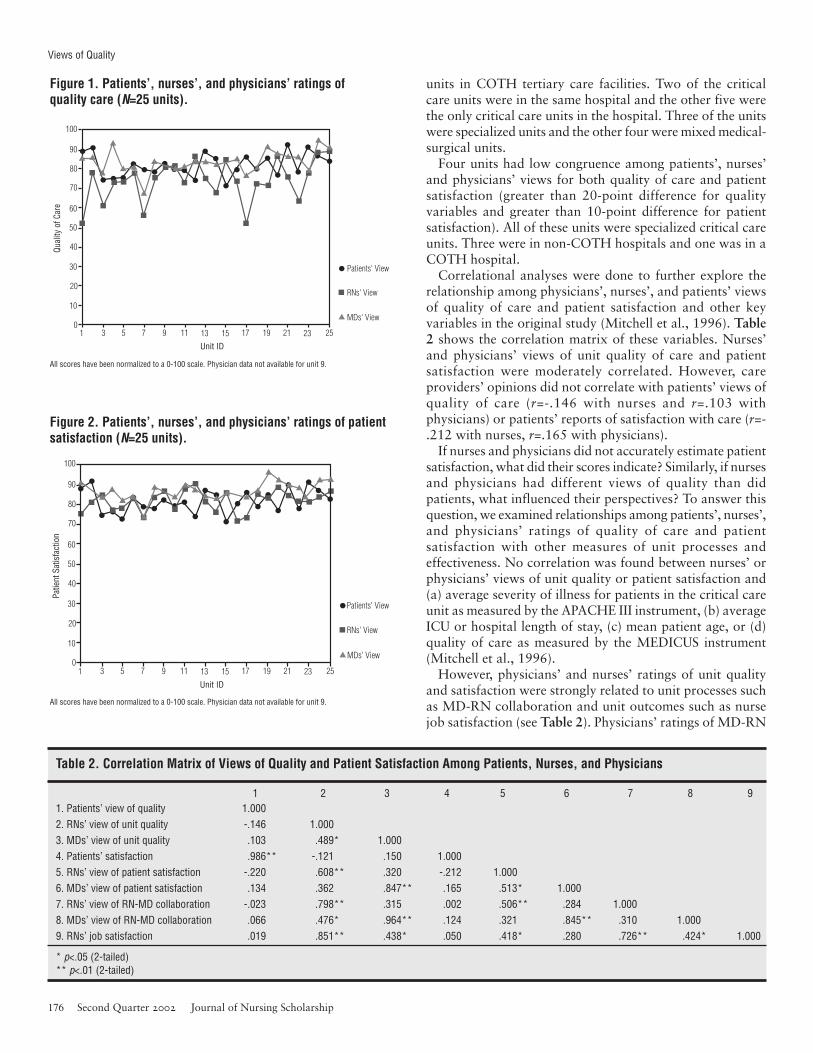
Correlational analyses were done to further explore therelationship among physicians’, nurses’, and patients’ viewsof quality of care and patient satisfaction and other keyvariables in the original study (Mitchell et al., 1996). Table2 shows the correlation matrix of these variables. Nurses’and physicians’ views of unit quality of care and patientsatisfaction were moderately correlated. However, careproviders’ opinions did not correlate with patients’ views ofquality of care (r=-.146 with nurses and r=.103 withphysicians) or patients’ reports of satisfaction with care (r=-.212 with nurses, r=.165 with physicians).
If nurses and physicians did not accurately estimate patientsatisfaction, what did their scores indicate? Similarly, if nursesand physicians had different views of quality than didpatients, what influenced their perspectives? To answer thisquestion, we examined relationships among patients’, nurses’,and physicians’ ratings of quality of care and patientsatisfaction with other measures of unit processes andeffectiveness. No correlation was found between nurses’ orphysicians’ views of unit quality or patient satisfaction and(a) average severity of illness for patients in the critical careunit as measured by the APACHE III instrument, (b) averageICU or hospital length of stay, (c) mean patient age, or (d)quality of care as measured by the MEDICUS instrument(Mitchell et al., 1996).
However, physicians’ and nurses’ ratings of unit qualityand satisfaction were strongly related to unit processes suchas MD-RN collaboration and unit outcomes such as nursejob satisfaction (see Table 2). Physicians’ ratings of MD-RN
1 2 3 4 5 6 7 8 91. Patients’ view of quality 1.0002. RNs’ view of unit quality -.146 1.0003. MDs’ view of unit quality .103 .489* 1.0004. Patients’ satisfaction .986** -.121 .150 1.0005. RNs’ view of patient satisfaction -.220 .608** .320 -.212 1.0006. MDs’ view of patient satisfaction .134 .362 .847** .165 .513* 1.0007. RNs’ view of RN-MD collaboration -.023 .798** .315 .002 .506** .284 1.0008. MDs’ view of RN-MD collaboration .066 .476* .964** .124 .321 .845** .310 1.0009. RNs’ job satisfaction .019 .851** .438* .050 .418* .280 .726** .424* 1.000
* p<.05 (2-tailed)** p<.01 (2-tailed)
Table 2. Correlation Matrix of Views of Quality and Patient Satisfaction Among Patients, Nurses, and Physicians
90
100
80
70
60
50
40
30
20
10
01 3 5 7 9 11 13 15 17 19 21 23 25
Patients' View
RNs' View
MDs' View
Unit ID
Patie
nt S
atis
fact
ion
Figure 2. Patients’, nurses’, and physicians’ ratings of patientsatisfaction (N=25 units).
All scores have been normalized to a 0-100 scale. Physician data not available for unit 9.
All scores have been normalized to a 0-100 scale. Physician data not available for unit 9.
90
100
80
70
60
50
40
30
20
10
01 3 5 7 9 11 13 15 17 19 21 23 25
Patients' View
RNs' View
MDs' View
Unit ID
Qual
ity o
f Car
e
Figure 1. Patients’, nurses’, and physicians’ ratings ofquality care (N=25 units).

Journal of Nursing Scholarship Second Quarter 2002 177
Views of Quality
collaboration on the critical care unit were positivelycorrelated to their ratings of unit quality (r=.964, p<.01) andpatient satisfaction (r=.845, p<.01). Nurse ratings of MD-RN collaboration were also strongly correlated to nurseratings of unit quality and patient satisfaction. In addition,nurses’ reports of job satisfaction were positively correlatedto nurse ratings of unit quality (r=.851, p<.01) and patientsatisfaction (r=.418; p<.05).
Discussion and Implications
In an intensive case study of two critical care units notedfor high quality organizational and clinical performance,patients’ and providers’ views of quality and patientsatisfaction had been remarkably similar (Mitchell, 1991).Nelson and colleagues (Nelson et al., 1992) noted thathospital employees’ and patients’ ratings of satisfactioncorrelated positively. However, that conclusion appeared tobe based on Rice’s study of Veteran’s Administrationneuropsychiatric hospitals, which did not include elementsof quality or satisfaction with care that are characteristic ofacute care general hospitals (Rice et al., 1963). In our studyof multiple critical care units of varying organizationalperformance, patients’ and care providers’ views of qualityand patient satisfaction were not equivalent, as indicated bythe low correlation between providers’ and patients’ viewsof care quality and satisfaction.
Merkel found that advanced resident physicians wereunsuccessful in predicting their patients’ satisfaction withmedical care, or in estimating the relative importance ofelements of patient satisfaction (Merkel, 1984). Lynn foundthat patients’ and nurses’ views of important qualityindicators differed from those used in traditional measures;nurses underestimated the degree to which patients’ valuequality nursing care (Lynn & McMillen, 1999). Hinshawand Oakes (1974) found that patients, nurses, and physicianshad differing views of the key predictors of quality nursingcare, except for the importance of technical competence(Hinshaw & Oakes, 1974). Furthermore, Sales and colleaguesfound that what was defined as important for qualitydepended on the discipline of the provider (Sales, Lurie,Moscovice, & Goes, 1995; Sales, Moscovice, & Lurie, 1996).
Other investigators have noted that nurses, physicians, andpatients rated such attributes as education, interpersonalrelationships, participation in decision-making, and needsfulfillment differently (Harvey, Kazis, & Lee, 1999; Pettit &White, 1991). Patients and providers may have differentpreferences and perceptions of desired health outcomes incritical illness (Gooding, Newcomb, & Mertens, 1999).
Patients’ current state of health has been found to be amajor factor in their ratings of quality and satisfaction (Kane,Maciejewski, & Finch, 1997), but it has not been wellcorrelated with provider perceptions of outcome, particularlyin the psychosocial dimensions of health (Becker, 1998).Severity of illness did not correlate with patients’ or providers’views of quality or satisfaction in our study. Others have
confirmed that severity of illness has not been consistentlyshown to influence patients’ views of satisfaction and quality(Covinsky et al., 1998; Woodbury, Tracy, & McKnight,1998).
The use of professionals’ perceptions of patient satisfactionand of perceived quality of care as proxies for patients’ viewsindicates that professionals proceed on invalid assumptions.When care providers estimate patients’ views of quality, theymay be projecting their own views of organizational harmonyor disharmony, as indicated by the findings of our study.Clinicians who report good working relationships betweenphysicians and nurses tended to overestimate patient viewsof quality and satisfaction with care. However on units whereMD-RN collaboration was rated lower, cliniciansunderestimated their patients’ perception of quality andsatisfaction.
Nurses’ satisfaction with their jobs appears to have a morecomplex relationship with these variables. Although jobsatisfaction was strongly related to nurses’ views of unitquality, it was more modestly correlated with estimates ofpatients’ satisfaction. This speculation is supported by a recentreport of staff perceptions of work environment and qualityof care following re-engineering in a large acute care hospital.Although objective evidence of quality of care did not change,staff perceived it to be lower, in parallel with their increasingdissatisfaction with their work environment (Woodward etal., 1999). More important, nurse satisfaction with workconditions has been compared with patient satisfaction withcare, and was found to be unrelated (Anderson, Maloney, &Beard, 1998; Kangas, Kee, & McKee-Waddle, 1999;Krugman & Preheim, 1999).
Two possible limitations to these data are their relativeage and the single geographical region from which the datawere obtained. Since these data were collected, the healthcare environment has shown an accelerated rate oforganizational change. A recent review of the efforts ofhospital restructuring on care and outcomes (Aiken, Clarke,& Sloane, 2000) showed that 57% of sampled hospitals hadbeen restructured resulting in decreased nurse perceptionsof resource adequacy, decreased support for professionalnursing practice provided by nurse managers, and decreasedstatus of nurses in the hospital organization. Barry-Walker(2000) examined the effects of a systems redesign on patient,financial, and nurse outcomes. Although nurse morale, jobsatisfaction, and perceptions of quality of patient caredeclined after the systems were redesigned, the quality oftwo objective aspects of patient care—the rate of patients’falls and rate of nurses’ medication errors—did not changesignificantly. A review of research evaluating the effects ofhospital ownership on performance and outcomes (Baker etal., 2000) showed that hospital ownership was related tonurses’ job satisfaction and turnover but was not consistentlycorrelated with patient satisfaction. Finally, a prospectivecohort study to measure the effect of total qualitymanagement (TQM), one of the organizational trendspopularized in the last decade, on patient outcomes (Shortellet al., 2000) showed no relationship between patient

178 Second Quarter 2002 Journal of Nursing Scholarship
satisfaction and TQM implementation or indicators of asupportive organizational culture.
Thus, the findings of recent research to evaluate change inthe health care environment are consistent with our results.Organizational changes consistently appear to affect staffattitudes but linkages to patient outcomes, in particularpatient satisfaction, are less conclusive.
The second limitation to these findings is that data werefrom one region of the United States. The study with similarfindings, indicating staff perceptions of decreased quality inparallel with decreased morale and satisfaction with the workenvironment, is from another geographical region(Woodward et al., 1999), showing that our findings may beapplicable in other areas.
Conclusions
These findings should challenge those who would claim torepresent perceived quality of care or patient satisfaction fromthe views of only health care professionals. These dataindicate that professionals and patients had differing viewsof care in the same critical care units. Patients were neitheras satisfied as professionals perceived them to be in unitswith better nurse-physician collaboration and commu-nication, nor were they as dissatisfied as nurses and physiciansperceived them to be in less well-functioning units. Neitherview can be taken as the “best” measure of quality or patientsatisfaction, because patients and professionals may have haddifferent standards and ways in which they viewed thesecharacteristics of care. As noted by Sales and colleagues,quality is in the eye of the beholder (Sales et al., 1995). Anyinvestigation of quality and patient satisfaction mustincorporate multiple views.
References
Aiken, L.H., Clarke, S.P., & Sloane, D.M. (2000). Hospital restructuring:Does it adversely affect care and outcomes. Journal of NursingAdministration, 30, 457-465.
Anderson, F.D., Maloney, J.P., & Beard, L.W. (1998). A descriptive,correlational study of patient satisfaction, provider satisfaction, andprovider workload at an Army medical center. Military Medicine, 163,90-4.
Baker, C.M., Messmer, P.L., Gyurko, C.C., Domagala, S.E., Conly, F.M.,Eads, T.S., et al. (2000). Hospital ownership, performance, and outcomes:Assessing the state-of-the-science. Journal of Nursing Administration,30, 227-240.
Barry-Walker, J. (2000). The impact of systems redesign on staff, patient,and financial outcomes. Journal of Nursing Administration, 30 (2), 77-89.
Becker, M. (1998). A US experience: Consumer responsive quality of lifemeasurement. Canadian Journal of Community Mental Health, 41-52,45-58.
Carson, S.S., Stocking, C., Podsadecki, T., Christenson, J., Pohlman, A.,MacRae, S., et al. (1996). Effects of organizational change in the medicalintensive care unit of a teaching hospital: A comparison of “open” and“closed” formats. JAMA, 276, 322-328.
Views of Quality
Charns, M.P., Stoelwinder, J.U., Millen, R.A., & Schaefer, M.J. (1980).Coordination and patient unit effectiveness. Paper presented at the annualmeeting of the Academy of Management. (Available from M.P. Charns,Management and Decision Research Center 152-M, Boston Veteran’sAdministration Medical Center, Boston, MA).
Christensen, M., & Inguanzo, J.M. (1989, August 20). Smart consumerspresent a marketing challenge. Hospitals, 42-47.
Cleary, P.D., & McNeil, B.J. (1988). Patient satisfaction as an indicator ofquality care. Inquiry, 25, 25-36.
Covinsky, K.E., Rosenthal, G.E., Chren, M.M., Justice, A.C., Fortinsky,R.H., Palmer, R.M., et al. (1998). The relation between health statuschanges and patient satisfaction in older hospitalized medical patients.Journal of General Internal Medicine, 13, 223-229.
Gooding, T.D., Newcomb, L., & Mertens, K. (1999). Patient-centeredmeasurement at an academic medical center. Joint Commission Journalon Quality Improvement, 25, 343-51.
Harvey, R.M., Kazis, L., & Lee, A.F. (1999). Decision-making preferenceand opportunity in VA ambulatory care patients: Association with patientsatisfaction. Research in Nursing and Health, 22, 39-48.
Hegyvary, S.T., Packard, N., & Jelinek, R.C. (1988). Viewpoint: A newhealthcare satisfaction survey. Unpublished report. Chicago: MedicusSystem Corporation.
Hegyvary, S.T., Wood, H., & Jelinek, R.C. (1988). Quality of nursing caremethodology: Revision of an instrument. Unpublished report. Chicago:Medicus System Corporation.
Hinshaw, A.S., & Oakes, D.L. (1974). Theoretical model-testing: Patients’,nurses’, and physicians’ expectations for quality nursing. CommunicatingNursing Research, 6, 163-189.
Kane, R.L., Maciejewski, M., & Finch, M. (1997). The relationship of patientsatisfaction with care and clinical outcomes. Medical Care, 35, 714-730.
Kangas, S., Kee, C.C., & McKee-Waddle, R. (1999). Organizational factors,nurses’ job satisfaction, and patient satisfaction with nursing care. Journalof Nursing Administration, 29, 32-42.
Knaus, W., Wagner, D., Draper, E., Zimmerman, J., Bergner, M., Bastos, P.,et al. (1991). The APACHE III prognostic system: Risk prediction ofhospital mortality for critically ill hospitalized adults. Chest, 100, 1619-1636.
Krugman, M., & Preheim, G. (1999). Longitudinal evaluation of professionalnursing practice redesign. Journal of Nursing Administration, 29, 10-20.
Kurata, J.H., Nogawa, A.N., Phillips, D.M., Hoffman, S., & Werblun, M.N.(1992). Patient and provider satisfaction with medical care. Journal ofFamily Practice, 35, 176-179.
Lynn, M.R., & McMillen, B.J. (1999). Do nurses know what patients thinkis important in nursing care? Journal of Nursing Care Quality, 13, 65-74.
Merkel, W.T. (1984). Physician perception of patient satisfaction: Do doctorsknow which patients are satisfied? Medical Care, 22, 453-459.
Mitchell, P.H. (1991). Clinical and organizational impact of multiple changesin critical care: A case study. Dissertation Abstracts International, 52/05,2847 (ATT 9131683).
Mitchell, P.H., Shannon, S.E., Cain, K.C., & Hegyvary, S.T. (1996). Criticalcare outcomes: Linking structures, processes, and organizational andclinical outcomes. American Journal of Critical Care, 5, 364-365.
Nelson, E.C., Rust, R.T., Zahorik, A., Rose, R.L., Batalden, P., & Siemanski,B.A. (1992). Do patient perceptions of quality relate to hospital financialperformance? Journal Health Care Marketing, 12, 6-13.
Oswald, S.L., Turner, D.E., Snipes, R.L., & Butler, D. (1998). Qualitydeterminants and hospital satisfaction: Perceptions of the facility andstaff might be key influencing factors. Marketing Health Services, 18,18-22.
Pettit, L.S., & White, C.L. (1991). Providers’ and consumers’ perceptionsof quality health care. Journal of Nursing Staff Development, 7, 5-10.
Rice, C.E., Berger, D.G., Klett, S.L., Sewall, L.G., & Lemkau, P.V. (1963).The ward evaluation scale. Journal of Clinical Psychology, 19, 251.
Rosenthal, G.E., & Shannon, S.E. (1997). The use of patient perceptions inthe evaluation of health-care delivery systems. Medical Care, 35 (suppl.11), NS58-NS-68.
Rousseau, D.M. (1985). Issues of level in organizational research: Multi-level and cross-level perspectives. Research in Organizational Behavior,7, 1-37.

Journal of Nursing Scholarship Second Quarter 2002 179
Rubin, H.R., Gandek, B., Rogers, W.H., Kosinski, M., McHorney, C.A., &Ware, J.E. Jr. (1993). Patients’ ratings of outpatient visits in differentpractice settings: Results from the Medical Outcomes Study. JAMA, 270,835-840.
Sales, A., Lurie, N., Moscovice, I., & Goes, J. (1995). Is quality in the eye ofthe beholder? Joint Commission Journal on Quality Improvement, 21,219-225.
Sales, A., Moscovice, I., & Lurie, N. (1996). Measuring seriousness ofhospital quality of care issues. Joint Commission Journal on QualityImprovement, 22, 811-816.
Shortell, S.M., Jones, R.H., Rademaker, A.W., Gillies, R. ., Dranove, D.S.,Hughes, E.F.X., et al. (2000). Assessing the impact of total qualitymanagement and organizational culture on multiple outcomes of carefor coronary artery bypass graft surgery patients. Medical Care, 38, 207-217.
Shortell, S.M., Zimmerman, J.E., Rousseau, D.M., Gillies, R.R., Wagner,D.P., Draper, E.A., et al. (1994). The performance of intensive care units:Does good management make a difference? Medical Care, 32, 508-25.
Verran, J.A., Gerber, R.M., & Milton, D.A. (1995). Data aggregation:Criteria for psychometric evaluation. Research in Nursing and Health,18, 77-80.
Verran, J.A., Mark, B., & Lamb, G. (1992). Psychometric examination ofinstruments using aggregated data. Research in Nursing and Health, 15,237-240.
Woodbury, D., Tracy, D., & McKnight, E. (1998). Does considering severityof illness improve interpretation of patient satisfaction data? Journal forHealthcare Quality, 20, 33-40.
Woodward, C.A., Shannon, H.S., Cunningham, C., McIntosh, J., Lendrum,B., Rosenbloom, D., et al. (1999). The impact of re-engineering and othercost reduction strategies on the staff of a large teaching hospital: Alongitudinal study. Medical Care, 37, 556-559.
Views of Quality