Embed Size (px)
Citation preview
LeoLiving with hATTR Amyloidosis
Patisiran, an Investigational RNAi Therapeutic
for the Treatment of Hereditary Transthyretin-
Mediated (hATTR) Amyloidosis
Thursday, August 3, 2017
2
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
3
Reminders
Event will run for approximately 75 minutes
Q&A Session at end of presentation
• Submit questions at top of webcast screen
• Questions may be submitted at any time
Replay, slides and transcript available at www.alnylam.com
4
Alnylam Forward Looking Statements
This presentation contains forward-looking statements, within the meaning of Section 27A of the Securities
Act of 1933 and Section 21E of the Securities Exchange Act of 1934. There are a number of important
factors that could cause actual results to differ materially from the results anticipated by these forward looking statements. These important factors include our ability to discover and develop novel drug
candidates and delivery approaches and successfully demonstrate the efficacy and safety of our product
candidates; pre-clinical and clinical results for our product candidates; actions or advice of regulatory
agencies; delays, interruptions or failures in the manufacture and supply of our product candidates; our
ability to obtain, maintain and protect intellectual property, enforce our intellectual property rights and defend
our patent portfolio; our ability to obtain and maintain regulatory approval, pricing and reimbursement for
products; our progress in establishing a commercial and ex-United States infrastructure; competition from
others using similar technology and developing products for similar uses; our ability to manage our growth
and operating expenses, obtain additional funding to support our business activities and establish and
maintain business alliances; the outcome of litigation; and the risk of government investigations; as well as
those risks more fully discussed in our most recent quarterly report on Form 10-Q under the caption “Risk
Factors.” If one or more of these factors materialize, or if any underlying assumptions prove incorrect, our
actual results, performance or achievements may vary materially from any future results, performance or
achievements expressed or implied by these forward-looking statements. All forward-looking statements
speak only as of the date of this presentation and, except as required by law, we undertake no obligation to
update such statements
5
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
6
RNAi Therapeutics
New Class of Innovative Medicines
Harness natural pathway
Catalytic mechanism
Silence any gene in genome
Upstream of today’s medicines
Clinically proven approach
7
HUMAN POC* EARLY STAGE(IND or CTA Filed-Phase 2)
LATE STAGE (Phase 2-Phase 3)
REGISTRATION/
COMMERCIAL
COMMERCIAL
RIGHTS
PatisiranHereditary ATTR
Amyloidosis ● US, Canada,
Western Europe
FitusiranHemophilia and Rare
Bleeding Disorders ●50%
US, Canada,
Western Europe
Inclisiran Hypercholesterolemia ● Milestones &
Royalties
GivosiranAcute Hepatic
Porphyrias ● Global
ALN-CC5Complement-
Mediated Diseases ● Global
ALN-GO1Primary
Hyperoxaluria Type 1 ●Subject to
partner option
rights
ALN-TTRsc02Hereditary ATTR
Amyloidosis ●Subject to
partner option
rights
ALN-HBVHepatitis B Virus
Infection ● Global
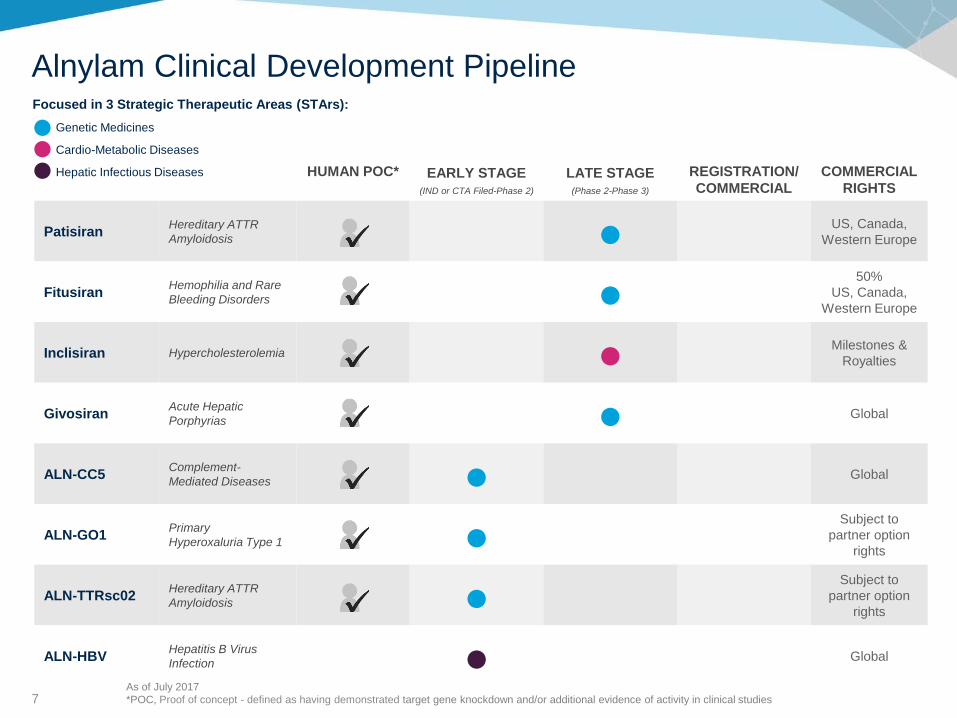
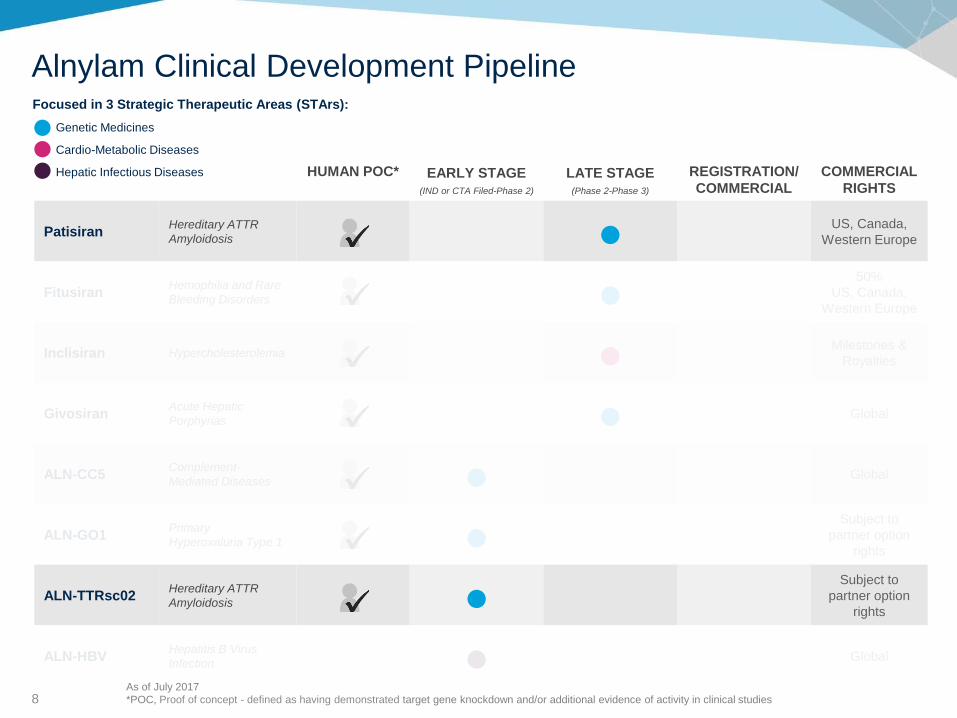
Focused in 3 Strategic Therapeutic Areas (STArs):
Genetic Medicines
Cardio-Metabolic Diseases
Hepatic Infectious Diseases
Alnylam Clinical Development Pipeline
As of July 2017
*POC, Proof of concept - defined as having demonstrated target gene knockdown and/or additional evidence of activity in clinical studies
8
HUMAN POC* EARLY STAGE(IND or CTA Filed-Phase 2)
LATE STAGE (Phase 2-Phase 3)
REGISTRATION/
COMMERCIAL
COMMERCIAL
RIGHTS
PatisiranHereditary ATTR
Amyloidosis ● US, Canada,
Western Europe
FitusiranHemophilia and Rare
Bleeding Disorders ●50%
US, Canada,
Western Europe
Inclisiran Hypercholesterolemia ● Milestones &
Royalties
GivosiranAcute Hepatic
Porphyrias ● Global
ALN-CC5Complement-
Mediated Diseases ● Global
ALN-GO1Primary
Hyperoxaluria Type 1 ●Subject to
partner option
rights
ALN-TTRsc02Hereditary ATTR
Amyloidosis ●Subject to
partner option
rights
ALN-HBVHepatitis B Virus
Infection ● Global
Focused in 3 Strategic Therapeutic Areas (STArs):
Genetic Medicines
Cardio-Metabolic Diseases
Hepatic Infectious Diseases
Alnylam Clinical Development Pipeline
As of July 2017
*POC, Proof of concept - defined as having demonstrated target gene knockdown and/or additional evidence of activity in clinical studies
9
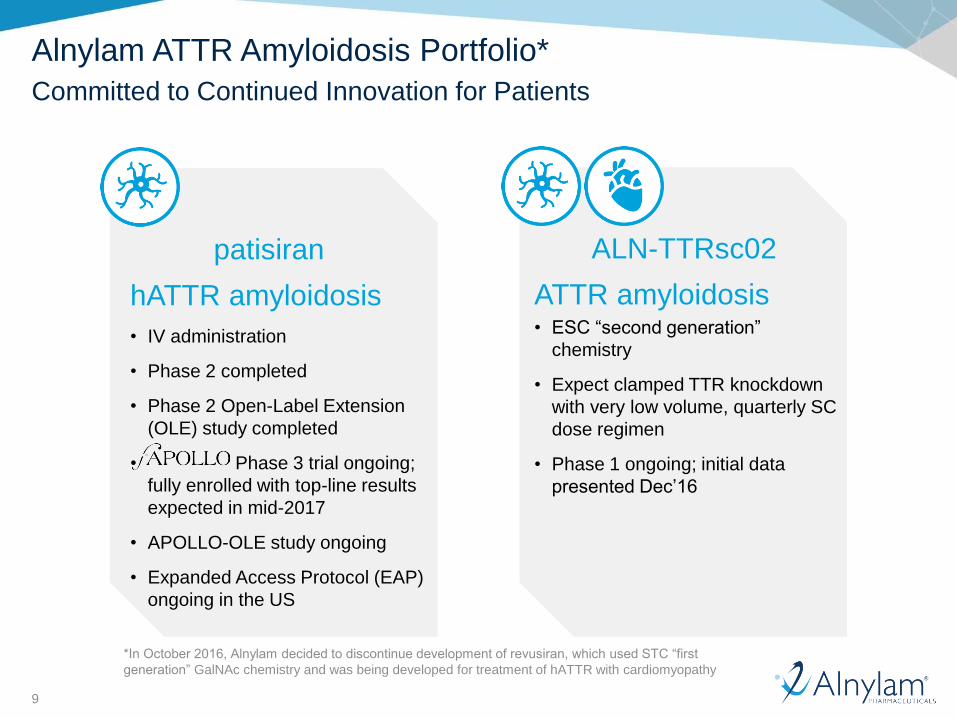
Alnylam ATTR Amyloidosis Portfolio*
Committed to Continued Innovation for Patients
hATTR amyloidosis
• IV administration
• Phase 2 completed
• Phase 2 Open-Label Extension
(OLE) study completed
• Phase 3 trial ongoing;
fully enrolled with top-line results
expected in mid-2017
• APOLLO-OLE study ongoing
• Expanded Access Protocol (EAP)
ongoing in the US
patisiran ALN-TTRsc02
ATTR amyloidosis• ESC “second generation”
chemistry
• Expect clamped TTR knockdown
with very low volume, quarterly SC
dose regimen
• Phase 1 ongoing; initial data
presented Dec’16
*In October 2016, Alnylam decided to discontinue development of revusiran, which used STC “first
generation” GalNAc chemistry and was being developed for treatment of hATTR with cardiomyopathy
10
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
11
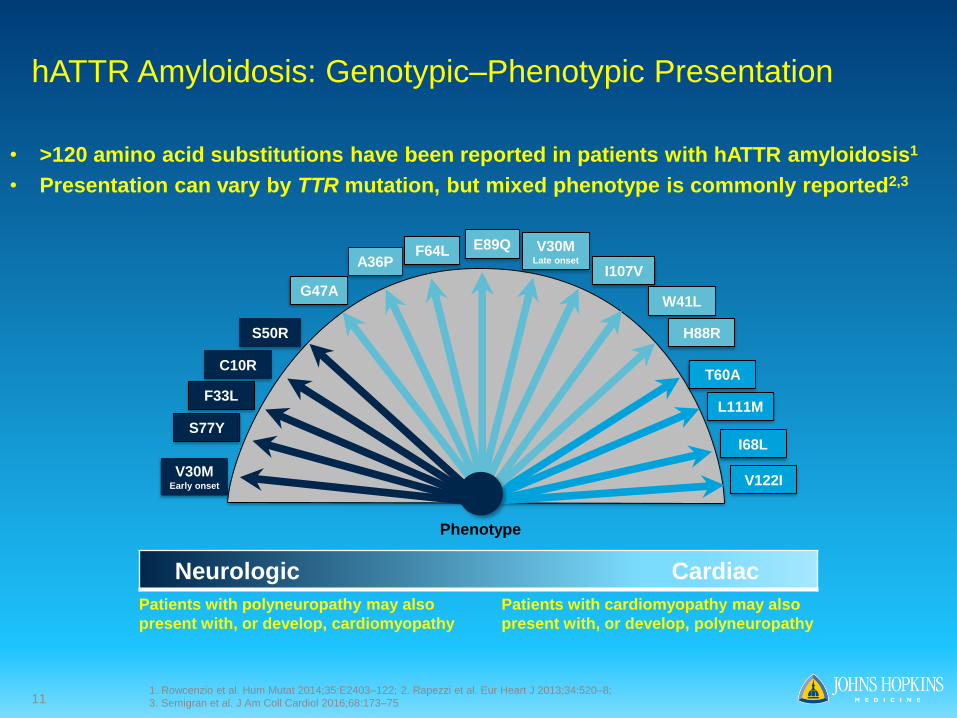
hATTR Amyloidosis: Genotypic–Phenotypic Presentation
• >120 amino acid substitutions have been reported in patients with hATTR amyloidosis1
• Presentation can vary by TTR mutation, but mixed phenotype is commonly reported2,3
Phenotype
V30MEarly onset
S77Y
C10R
S50R
G47A
E89Q V30MLate onset
I68L
L111M
T60A
H88R
I107V
V122I
F33L
F64L
W41L
A36P
Neurologic Cardiac
Patients with polyneuropathy may also
present with, or develop, cardiomyopathy
Patients with cardiomyopathy may also
present with, or develop, polyneuropathy
1. Rowcenzio et al. Hum Mutat 2014;35:E2403–122; 2. Rapezzi et al. Eur Heart J 2013;34:520–8;
3. Semigran et al. J Am Coll Cardiol 2016;68:173–75
12
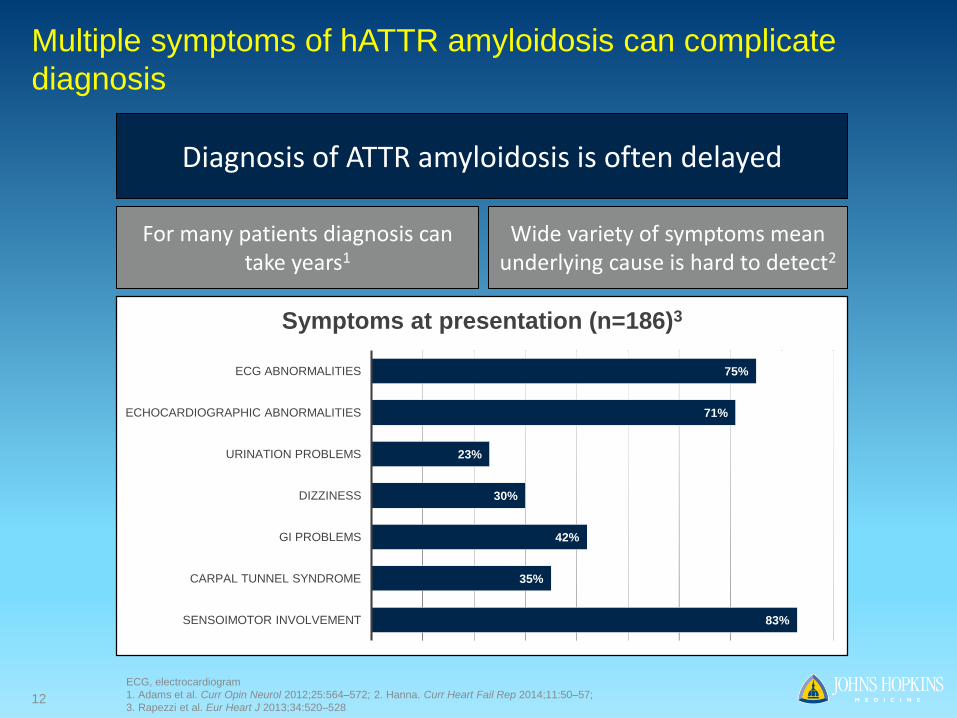
Multiple symptoms of hATTR amyloidosis can complicate
diagnosis
Diagnosis of ATTR amyloidosis is often delayed
Wide variety of symptoms mean underlying cause is hard to detect2
For many patients diagnosis can take years1
83%
35%
42%
30%
23%
71%
75%
SENSOIMOTOR INVOLVEMENT
CARPAL TUNNEL SYNDROME
GI PROBLEMS
DIZZINESS
URINATION PROBLEMS
ECHOCARDIOGRAPHIC ABNORMALITIES
ECG ABNORMALITIES
Symptoms at presentation (n=186)3
ECG, electrocardiogram
1. Adams et al. Curr Opin Neurol 2012;25:564–572; 2. Hanna. Curr Heart Fail Rep 2014;11:50–57;
3. Rapezzi et al. Eur Heart J 2013;34:520–528
13
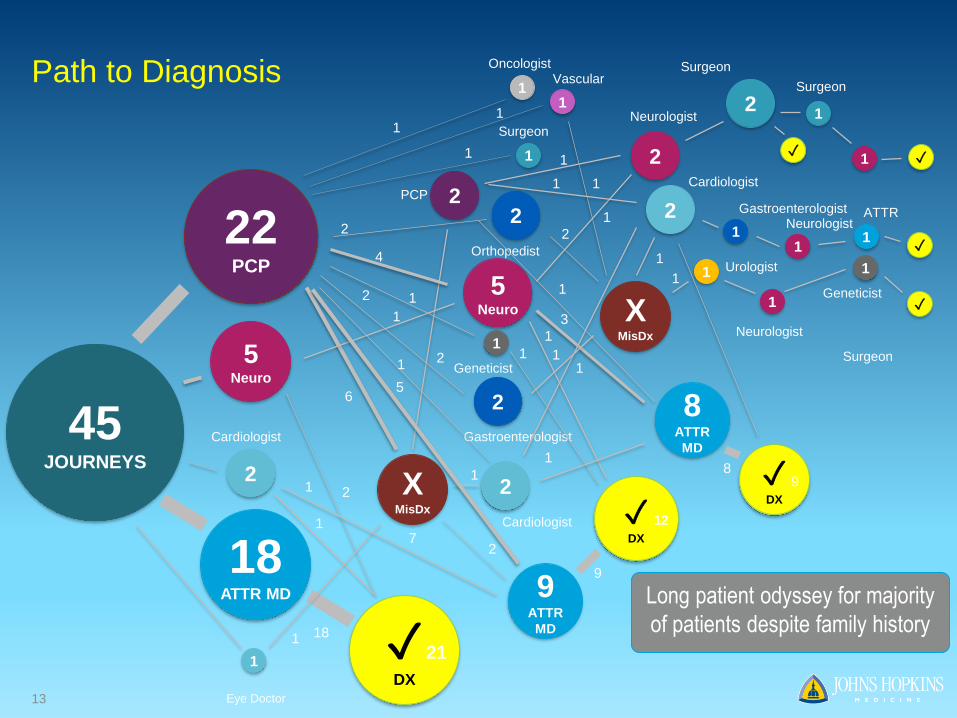
Path to Diagnosis
22PCP
5Neuro
2
Cardiologist
18ATTR MD
1
Eye Doctor
✓DX
18
2
1
XMisDx
1
6
7
21
2
2
PCP
5Neuro
✓DX
1
4
1
2
Gastroenterologist
2
2
Cardiologist
1
1
2
Orthopedist
2
XMisDx
2
9ATTR
MD
2
5
1
9
12
1
1
Geneticist1
1
1
Vascular
1
1
1
Oncologist
1
Surgeon
1
1 2
Neurologist
1
1
2
Cardiologist1
8ATTR
MD
✓DX
8
3
1
1
1
111
Urologist
1
Neurologist
1
Geneticist
2
Surgeon
✓
1
Surgeon
Surgeon
1 ✓
✓
9
1
Gastroenterologist
1
Neurologist1
ATTR
✓
45JOURNEYS
Long patient odyssey for majority
of patients despite family history
14
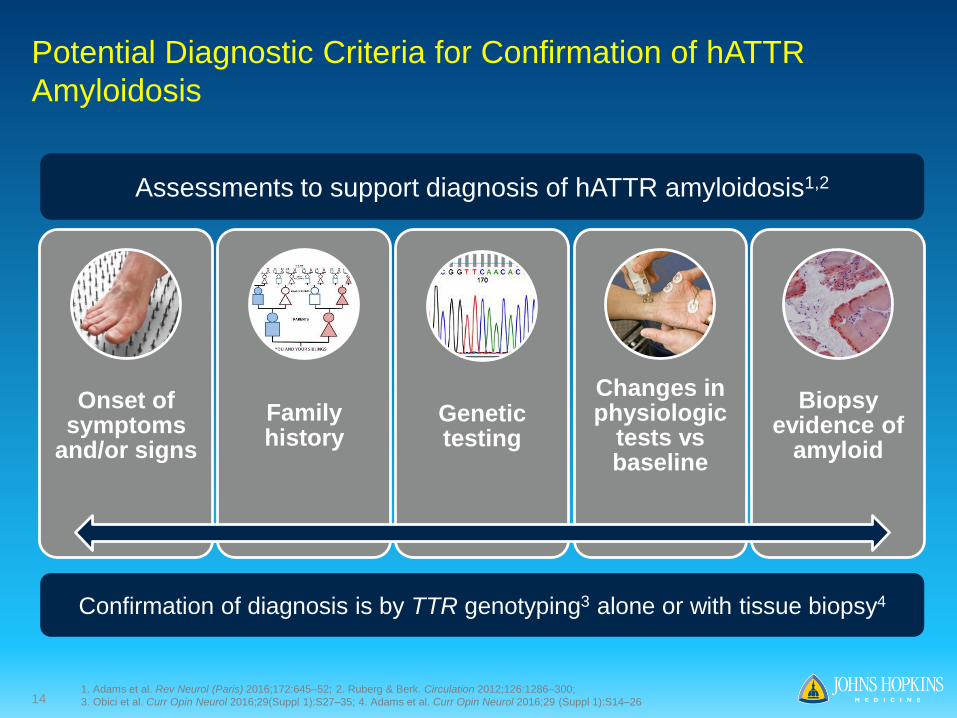
Potential Diagnostic Criteria for Confirmation of hATTR
Amyloidosis
Onset of symptoms
and/or signs
Family history
Genetic testing
Changes in physiologic
tests vs baseline
Biopsy evidence of
amyloid
Assessments to support diagnosis of hATTR amyloidosis1,2
Confirmation of diagnosis is by TTR genotyping3 alone or with tissue biopsy4
1. Adams et al. Rev Neurol (Paris) 2016;172:645–52; 2. Ruberg & Berk. Circulation 2012;126:1286–300;
3. Obici et al. Curr Opin Neurol 2016;29(Suppl 1):S27–35; 4. Adams et al. Curr Opin Neurol 2016;29 (Suppl 1):S14–26
15
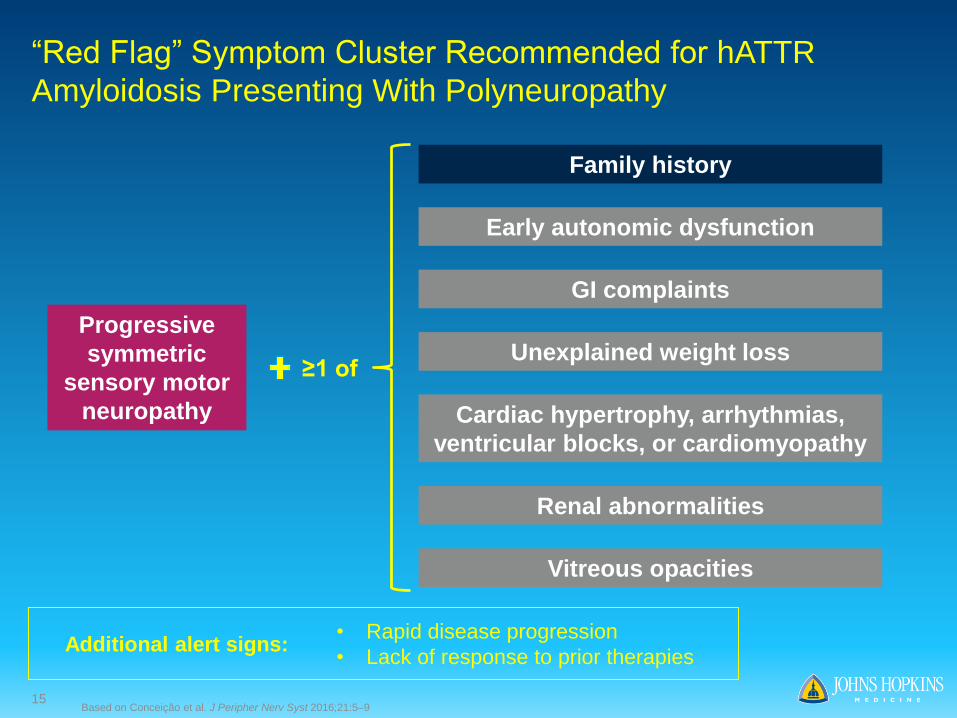
“Red Flag” Symptom Cluster Recommended for hATTR
Amyloidosis Presenting With Polyneuropathy
Progressive
symmetric
sensory motor
neuropathy
Family history
Early autonomic dysfunction
GI complaints
Unexplained weight loss
Cardiac hypertrophy, arrhythmias,
ventricular blocks, or cardiomyopathy
Renal abnormalities
Vitreous opacities
≥1 of
Additional alert signs:• Rapid disease progression
• Lack of response to prior therapies
Based on Conceição et al. J Peripher Nerv Syst 2016;21:5–9
16
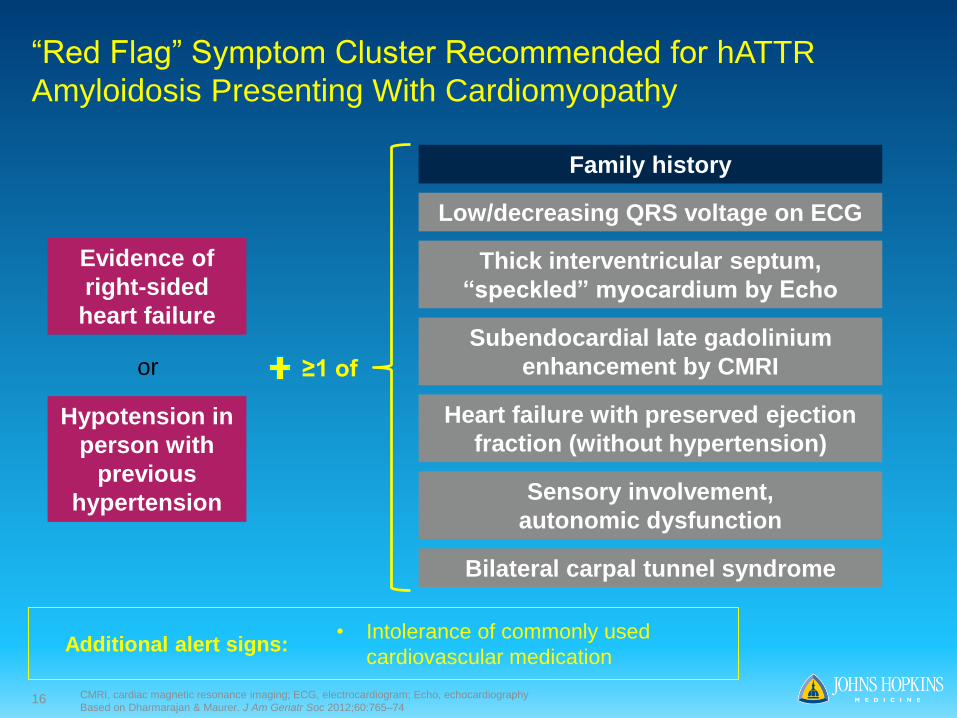
“Red Flag” Symptom Cluster Recommended for hATTR
Amyloidosis Presenting With Cardiomyopathy
Evidence of
right-sided
heart failure
Thick interventricular septum,
“speckled” myocardium by Echo
Low/decreasing QRS voltage on ECG
Subendocardial late gadolinium
enhancement by CMRI
Heart failure with preserved ejection
fraction (without hypertension)Hypotension in
person with
previous
hypertension
or
Sensory involvement,
autonomic dysfunction
CMRI, cardiac magnetic resonance imaging; ECG, electrocardiogram; Echo, echocardiography
Based on Dharmarajan & Maurer. J Am Geriatr Soc 2012;60:765–74
≥1 of
Family history
Additional alert signs:• Intolerance of commonly used
cardiovascular medication
Bilateral carpal tunnel syndrome
17
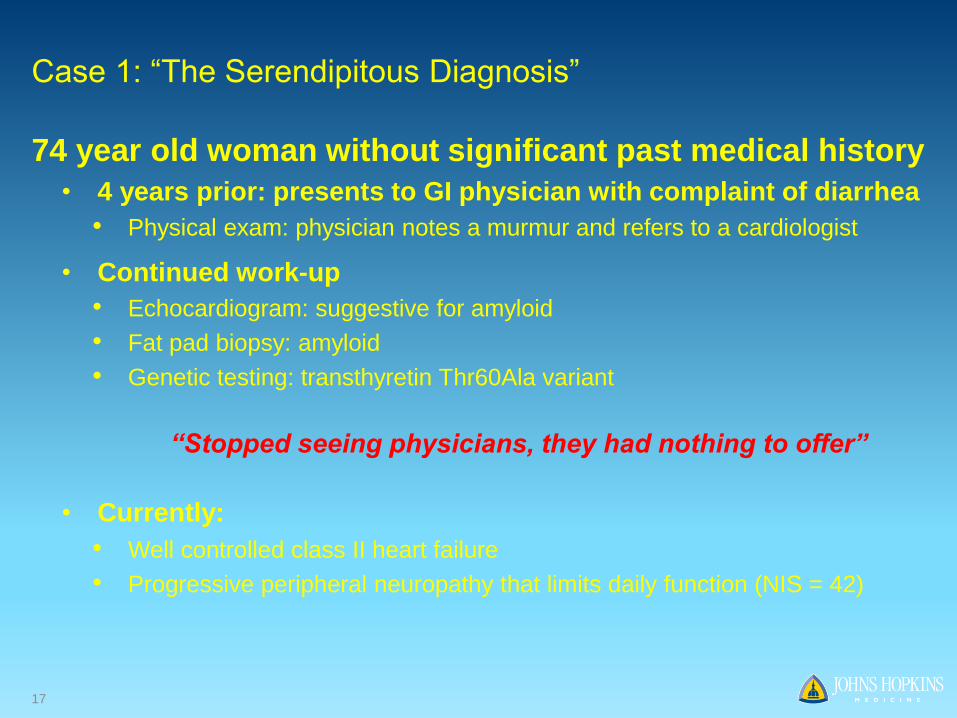
74 year old woman without significant past medical history
• 4 years prior: presents to GI physician with complaint of diarrhea
• Physical exam: physician notes a murmur and refers to a cardiologist
• Continued work-up
• Echocardiogram: suggestive for amyloid
• Fat pad biopsy: amyloid
• Genetic testing: transthyretin Thr60Ala variant
“Stopped seeing physicians, they had nothing to offer”
• Currently:
• Well controlled class II heart failure
• Progressive peripheral neuropathy that limits daily function (NIS = 42)
Case 1: “The Serendipitous Diagnosis”
18
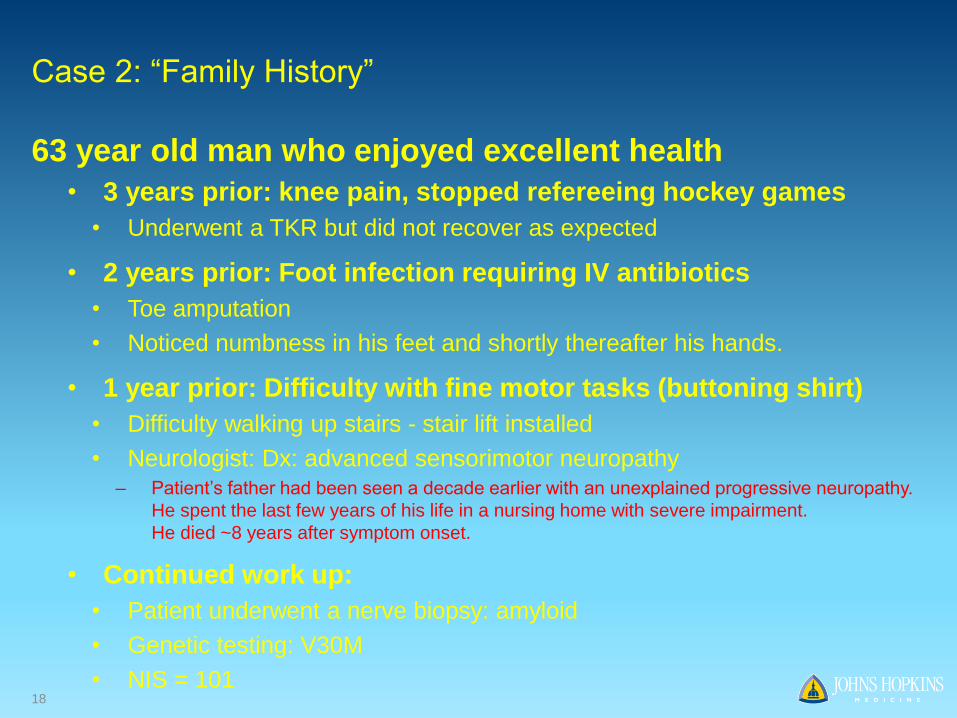
Case 2: “Family History”
63 year old man who enjoyed excellent health
• 3 years prior: knee pain, stopped refereeing hockey games
• Underwent a TKR but did not recover as expected
• 2 years prior: Foot infection requiring IV antibiotics
• Toe amputation
• Noticed numbness in his feet and shortly thereafter his hands.
• 1 year prior: Difficulty with fine motor tasks (buttoning shirt)
• Difficulty walking up stairs - stair lift installed
• Neurologist: Dx: advanced sensorimotor neuropathy– Patient’s father had been seen a decade earlier with an unexplained progressive neuropathy.
He spent the last few years of his life in a nursing home with severe impairment.
He died ~8 years after symptom onset.
• Continued work up:
• Patient underwent a nerve biopsy: amyloid
• Genetic testing: V30M
• NIS = 101
19
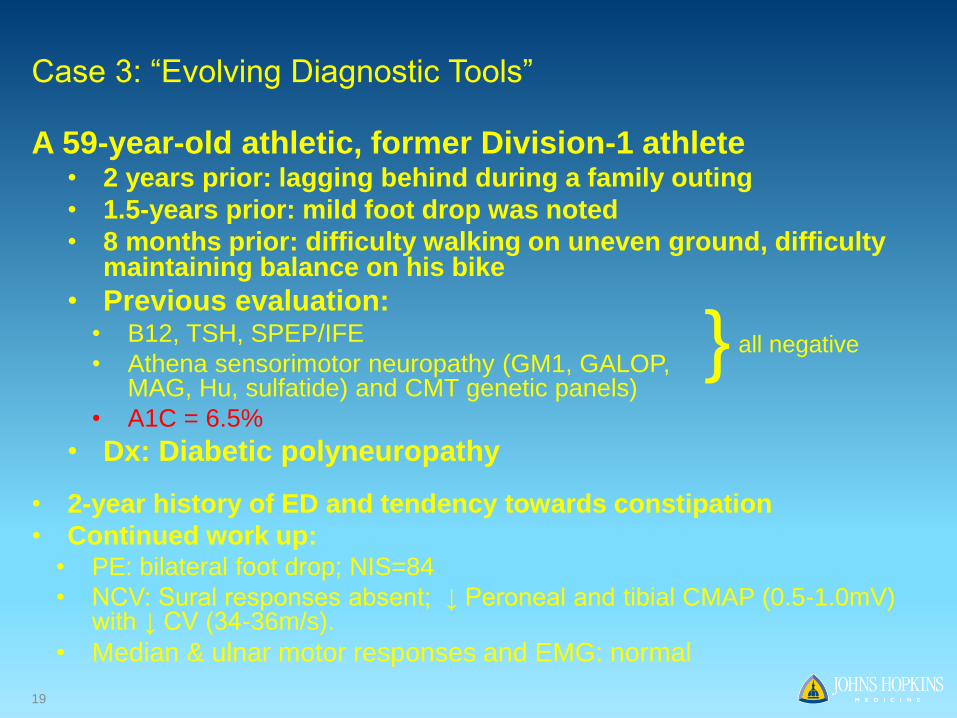
Case 3: “Evolving Diagnostic Tools”
A 59-year-old athletic, former Division-1 athlete • 2 years prior: lagging behind during a family outing
• 1.5-years prior: mild foot drop was noted
• 8 months prior: difficulty walking on uneven ground, difficulty maintaining balance on his bike
• Previous evaluation: • B12, TSH, SPEP/IFE
• Athena sensorimotor neuropathy (GM1, GALOP, MAG, Hu, sulfatide) and CMT genetic panels)
• A1C = 6.5%
• Dx: Diabetic polyneuropathy
• 2-year history of ED and tendency towards constipation
• Continued work up:• PE: bilateral foot drop; NIS=84
• NCV: Sural responses absent; ↓ Peroneal and tibial CMAP (0.5-1.0mV) with ↓ CV (34-36m/s).
• Median & ulnar motor responses and EMG: normal
} all negative

20
Biopsy Results
↓ IENFD, SGNFD
Case 3: “Evolving Diagnostic Tools,” continued
21
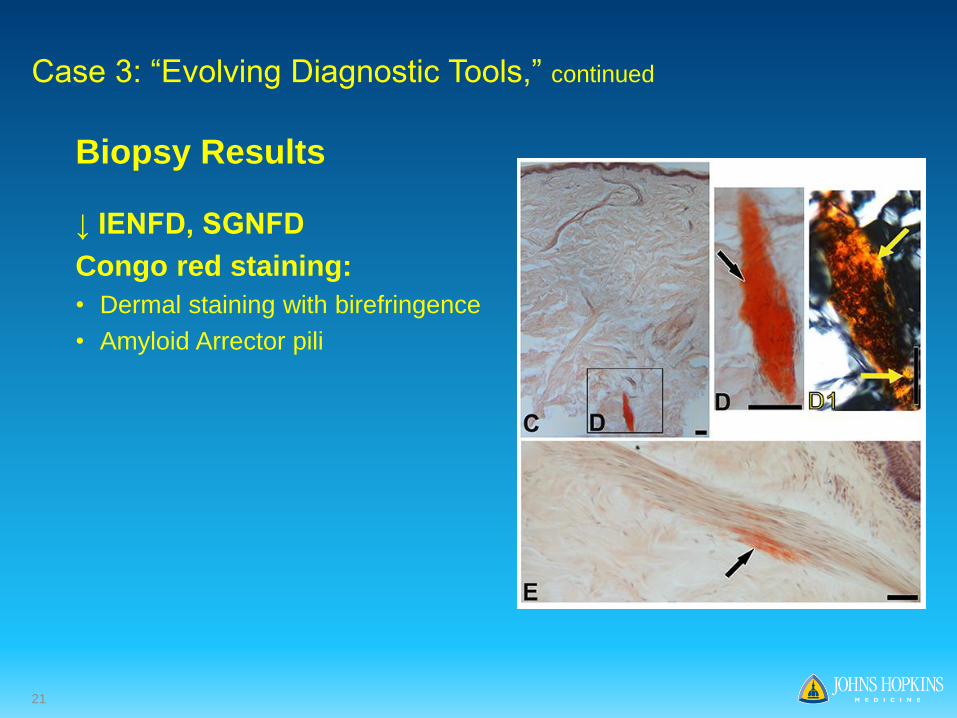
Biopsy Results
↓ IENFD, SGNFD
Congo red staining:
• Dermal staining with birefringence
• Amyloid Arrector pili
Case 3: “Evolving Diagnostic Tools,” continued
22
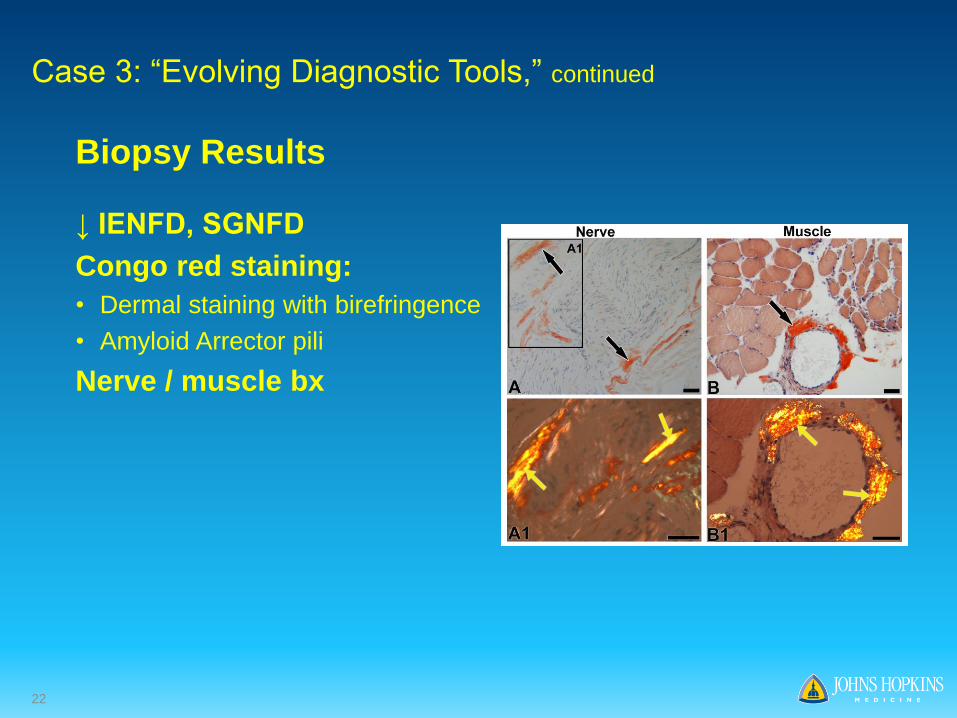
Biopsy Results
↓ IENFD, SGNFD
Congo red staining:
• Dermal staining with birefringence
• Amyloid Arrector pili
Nerve / muscle bx
Case 3: “Evolving Diagnostic Tools,” continued
23
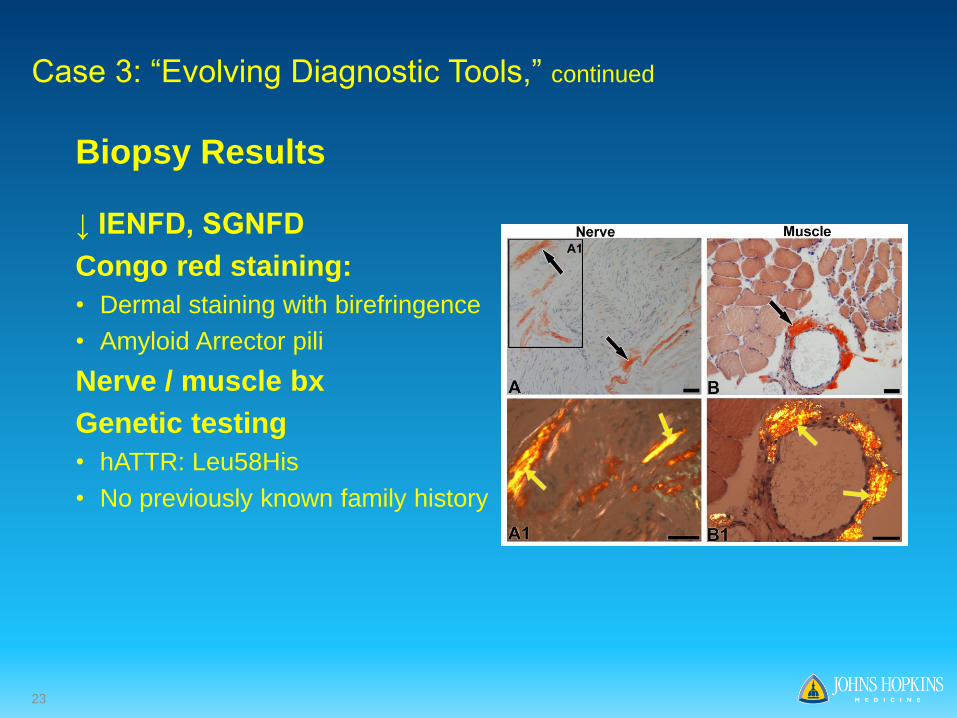
Biopsy Results
↓ IENFD, SGNFD
Congo red staining:
• Dermal staining with birefringence
• Amyloid Arrector pili
Nerve / muscle bx
Genetic testing
• hATTR: Leu58His
• No previously known family history
Case 3: “Evolving Diagnostic Tools,” continued
24
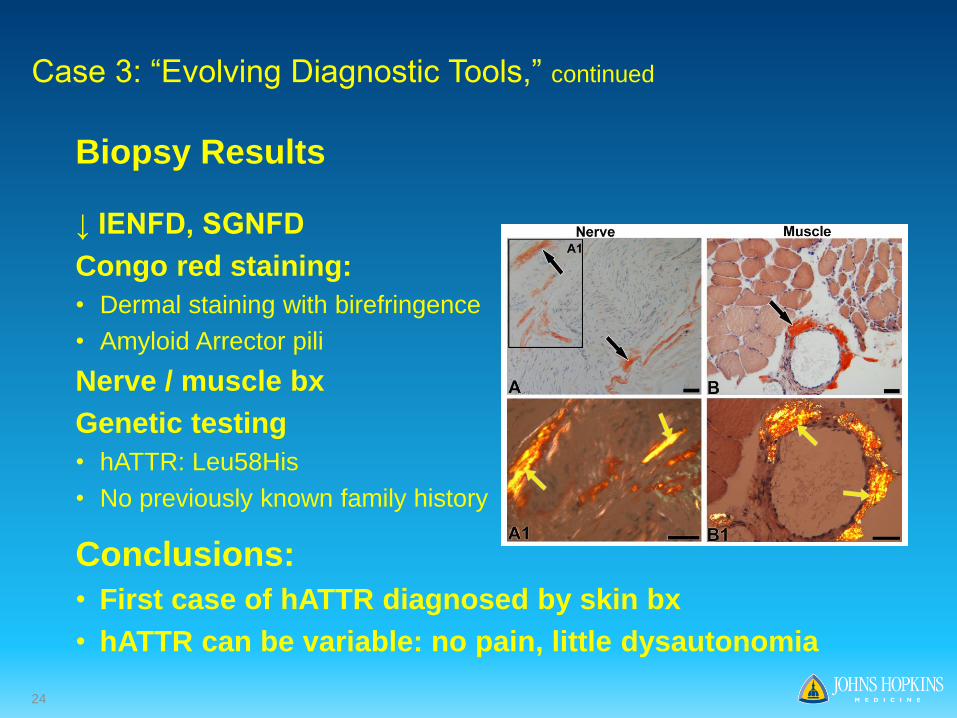
Biopsy Results
↓ IENFD, SGNFD
Congo red staining:
• Dermal staining with birefringence
• Amyloid Arrector pili
Nerve / muscle bx
Genetic testing
• hATTR: Leu58His
• No previously known family history
Conclusions:
• First case of hATTR diagnosed by skin bx
• hATTR can be variable: no pain, little dysautonomia
Case 3: “Evolving Diagnostic Tools,” continued
25
• hATTR has a heterogeneous presentation
◦ Diagnosed in their 50’s, 60’s and 70’s
◦ Presenting with GI, cardiac and peripheral nerve manifestations
◦ Tissue diagnosis by fat pad biopsy, nerve biopsy and skin biopsy.
• Amyloid deposition in the skin correlates with axon loss
• Amyloid burden in skin biopsy correlates with disability
Conclusions
26
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
27
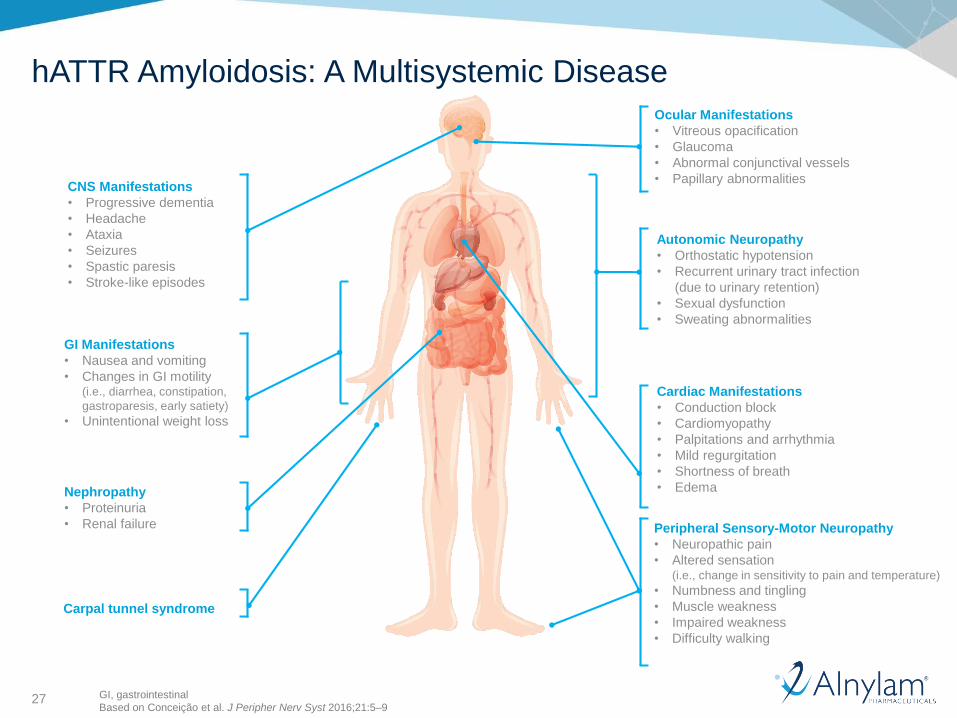
CNS Manifestations
• Progressive dementia
• Headache
• Ataxia
• Seizures
• Spastic paresis
• Stroke-like episodes
GI Manifestations
• Nausea and vomiting
• Changes in GI motility (i.e., diarrhea, constipation,
gastroparesis, early satiety)
• Unintentional weight loss
Autonomic Neuropathy
• Orthostatic hypotension
• Recurrent urinary tract infection
(due to urinary retention)
• Sexual dysfunction
• Sweating abnormalities
Peripheral Sensory-Motor Neuropathy
• Neuropathic pain
• Altered sensation (i.e., change in sensitivity to pain and temperature)
• Numbness and tingling
• Muscle weakness
• Impaired weakness
• Difficulty walking
Carpal tunnel syndrome
Ocular Manifestations
• Vitreous opacification
• Glaucoma
• Abnormal conjunctival vessels
• Papillary abnormalities
Nephropathy
• Proteinuria
• Renal failure
Cardiac Manifestations
• Conduction block
• Cardiomyopathy
• Palpitations and arrhythmia
• Mild regurgitation
• Shortness of breath
• Edema
GI, gastrointestinal
Based on Conceição et al. J Peripher Nerv Syst 2016;21:5–9
hATTR Amyloidosis: A Multisystemic Disease
28
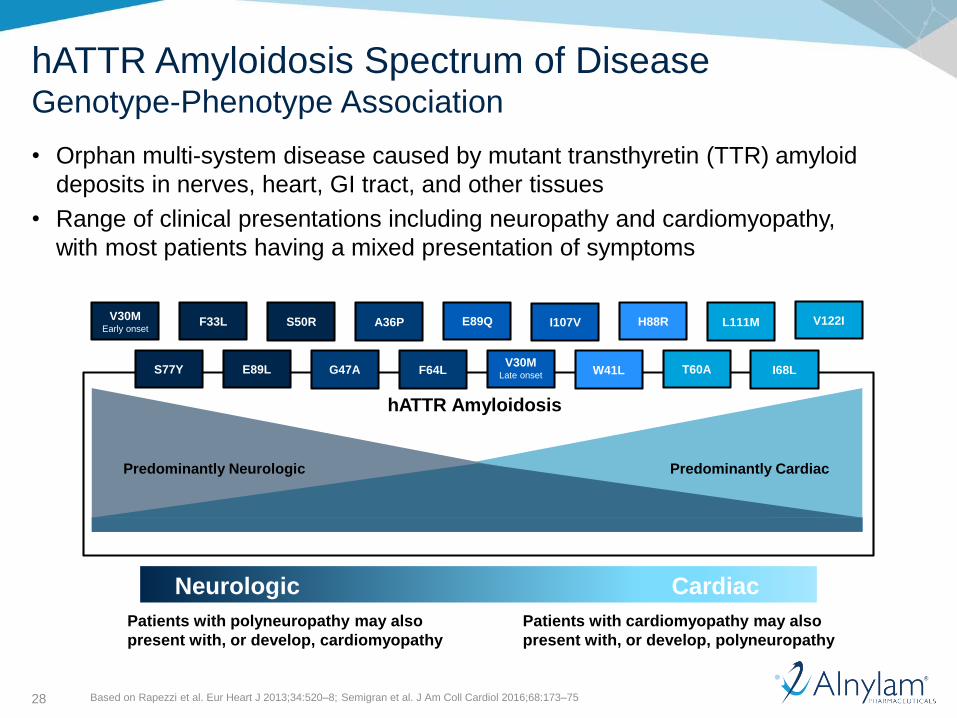
hATTR Amyloidosis Spectrum of DiseaseGenotype-Phenotype Association
Neurologic Cardiac
Patients with polyneuropathy may also
present with, or develop, cardiomyopathy
Patients with cardiomyopathy may also
present with, or develop, polyneuropathy
Based on Rapezzi et al. Eur Heart J 2013;34:520–8; Semigran et al. J Am Coll Cardiol 2016;68:173–75
hATTR Amyloidosis
Predominantly Neurologic Predominantly Cardiac
V30MEarly onset
F33L S50R A36P E89Q I107V H88R L111M V122I
S77Y E89L G47A F64LV30M
Late onset W41L T60A I68L
• Orphan multi-system disease caused by mutant transthyretin (TTR) amyloid
deposits in nerves, heart, GI tract, and other tissues
• Range of clinical presentations including neuropathy and cardiomyopathy,
with most patients having a mixed presentation of symptoms
29
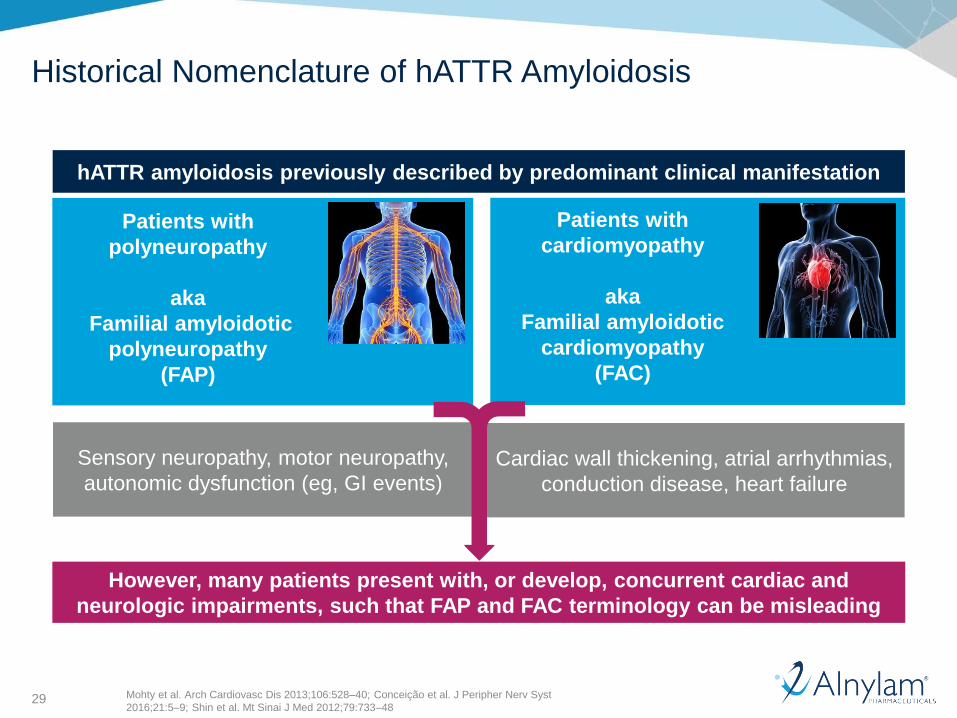
Patients with
polyneuropathy
aka
Familial amyloidotic
polyneuropathy
(FAP)
Historical Nomenclature of hATTR Amyloidosis
hATTR amyloidosis previously described by predominant clinical manifestation
However, many patients present with, or develop, concurrent cardiac and
neurologic impairments, such that FAP and FAC terminology can be misleading
Cardiac wall thickening, atrial arrhythmias,
conduction disease, heart failure
Sensory neuropathy, motor neuropathy,
autonomic dysfunction (eg, GI events)
Patients with
cardiomyopathy
aka
Familial amyloidotic
cardiomyopathy
(FAC)
Mohty et al. Arch Cardiovasc Dis 2013;106:528–40; Conceição et al. J Peripher Nerv Syst
2016;21:5–9; Shin et al. Mt Sinai J Med 2012;79:733–48
30
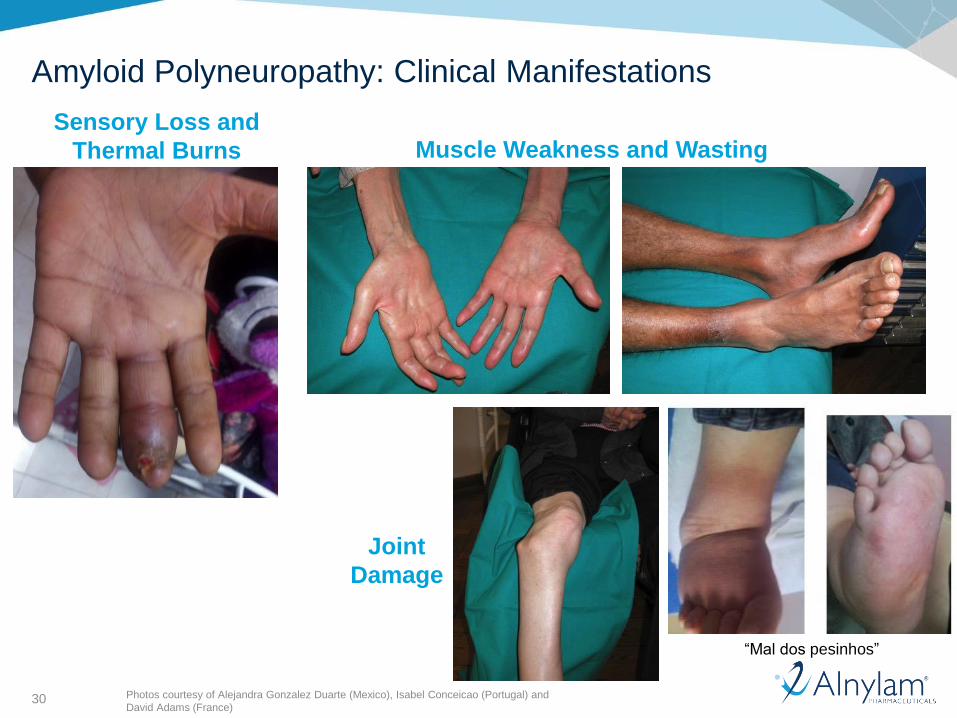
Amyloid Polyneuropathy: Clinical Manifestations
Photos courtesy of Alejandra Gonzalez Duarte (Mexico), Isabel Conceicao (Portugal) and
David Adams (France)
Sensory Loss and
Thermal Burns Muscle Weakness and Wasting
Joint
Damage
“Mal dos pesinhos”
31
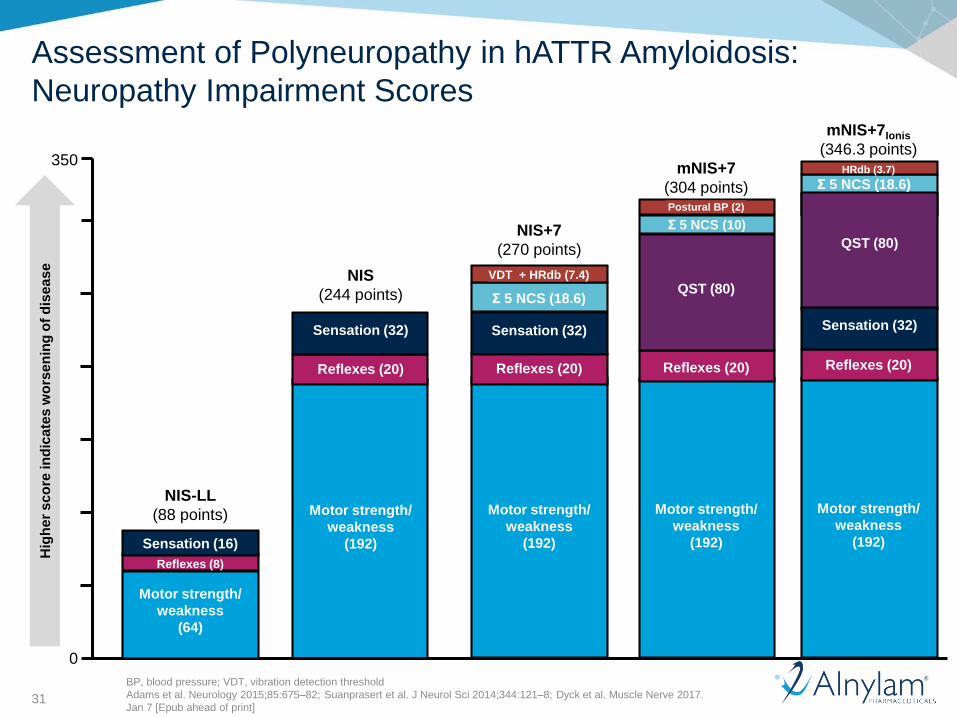
Assessment of Polyneuropathy in hATTR Amyloidosis:
Neuropathy Impairment Scores
mNIS+7
(304 points)
Motor strength/
weakness
(192)
Reflexes (20)
QST (80)
Σ 5 NCS (10)
Postural BP (2)
NIS
(244 points)
Motor strength/
weakness
(192)
Reflexes (20)
Sensation (32)
Hig
he
r s
co
re in
dic
ate
s w
ors
en
ing
of
dis
ea
se
NIS-LL
(88 points)
Motor strength/
weakness
(64)
Reflexes (8)
Sensation (16)
NIS+7
(270 points)
Motor strength/
weakness
(192)
Reflexes (20)
Sensation (32)
Σ 5 NCS (18.6)
VDT + HRdb (7.4)
Motor strength/
weakness
(192)
Reflexes (20)
Σ 5 NCS (18.6)HRdb (3.7)
mNIS+7Ionis
(346.3 points)
0
350
QST (80)
Sensation (32)
BP, blood pressure; VDT, vibration detection threshold
Adams et al. Neurology 2015;85:675–82; Suanprasert et al. J Neurol Sci 2014;344:121–8; Dyck et al. Muscle Nerve 2017.
Jan 7 [Epub ahead of print]
32
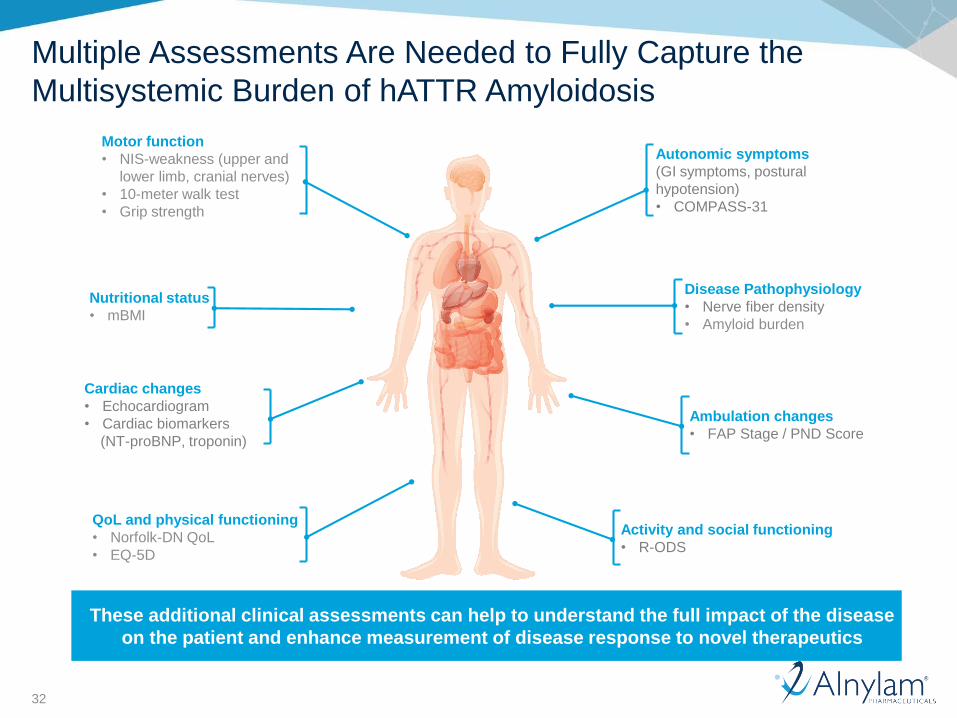
Multiple Assessments Are Needed to Fully Capture the
Multisystemic Burden of hATTR Amyloidosis
Motor function
• NIS-weakness (upper and
lower limb, cranial nerves)
• 10-meter walk test
• Grip strength
Nutritional status
• mBMI
Cardiac changes
• Echocardiogram
• Cardiac biomarkers
(NT-proBNP, troponin)
QoL and physical functioning
• Norfolk-DN QoL
• EQ-5D
Autonomic symptoms
(GI symptoms, postural
hypotension)
• COMPASS-31
Disease Pathophysiology
• Nerve fiber density
• Amyloid burden
Ambulation changes
• FAP Stage / PND Score
Activity and social functioning
• R-ODS
These additional clinical assessments can help to understand the full impact of the disease
on the patient and enhance measurement of disease response to novel therapeutics
33
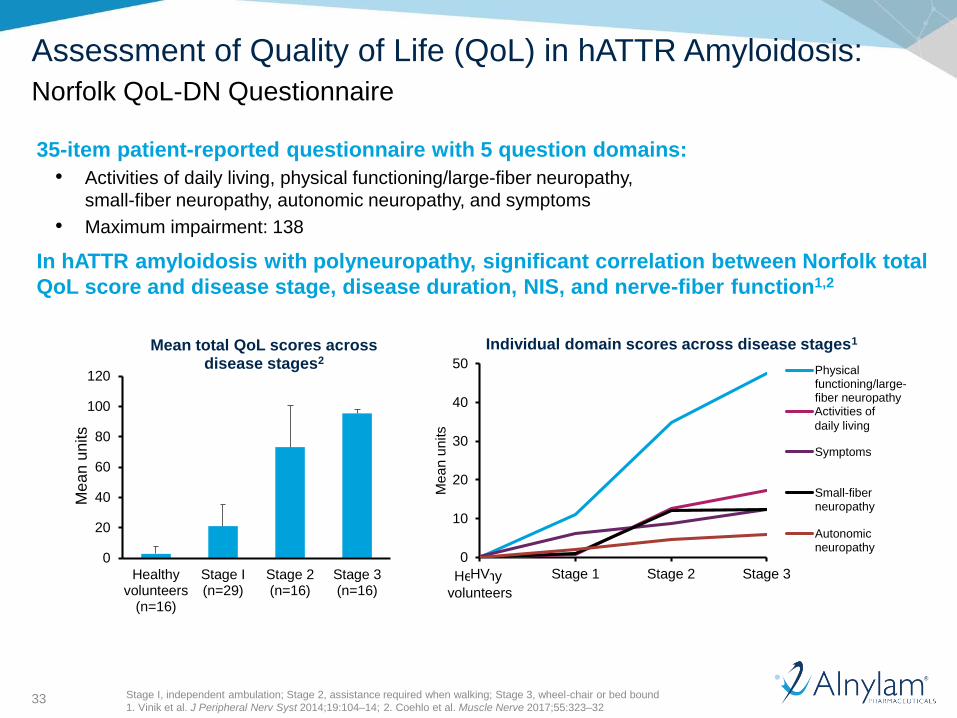
Assessment of Quality of Life (QoL) in hATTR Amyloidosis:
Norfolk QoL-DN Questionnaire
35-item patient-reported questionnaire with 5 question domains:
• Activities of daily living, physical functioning/large-fiber neuropathy,
small-fiber neuropathy, autonomic neuropathy, and symptoms
• Maximum impairment: 138
In hATTR amyloidosis with polyneuropathy, significant correlation between Norfolk total
QoL score and disease stage, disease duration, NIS, and nerve-fiber function1,2
Healthy
volunteers
Stage I, independent ambulation; Stage 2, assistance required when walking; Stage 3, wheel-chair or bed bound
1. Vinik et al. J Peripheral Nerv Syst 2014;19:104–14; 2. Coehlo et al. Muscle Nerve 2017;55:323–32
0
20
40
60
80
100
120
Healthyvolunteers
(n=16)
Stage I(n=29)
Stage 2(n=16)
Stage 3(n=16)
Me
an
un
its
Mean total QoL scores across disease stages2
0
10
20
30
40
50
HV Stage 1 Stage 2 Stage 3
Me
an
un
its
Individual domain scores across disease stages1
Physicalfunctioning/large-fiber neuropathyADL
Symptoms
Small-fiberneuropathy
Autonomicneuropathy
Activities of
daily living
34
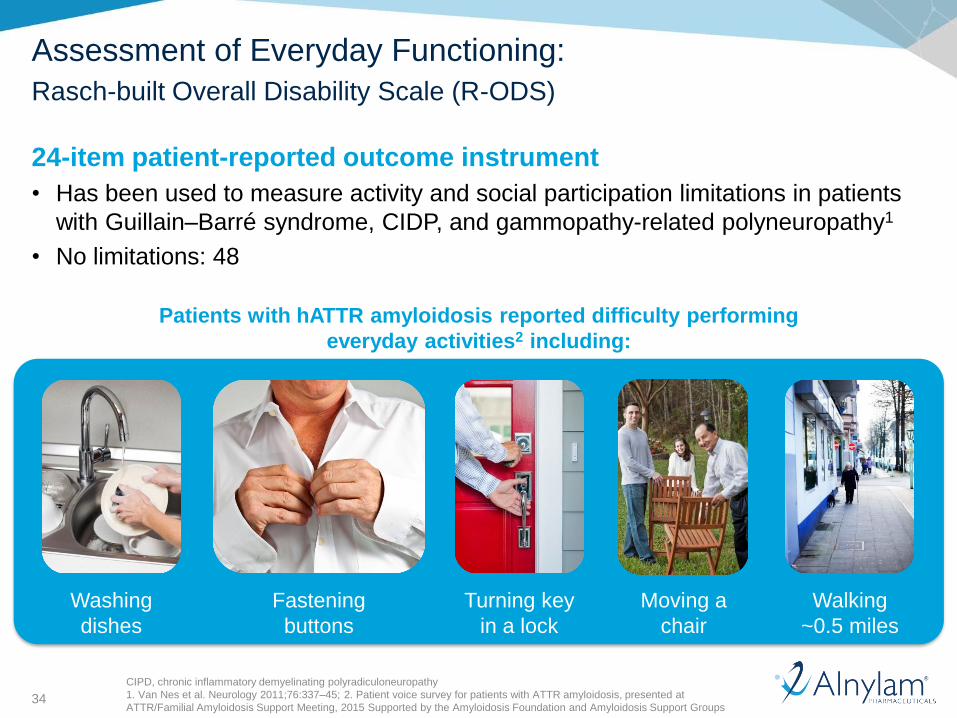
Assessment of Everyday Functioning:
Rasch-built Overall Disability Scale (R-ODS)
24-item patient-reported outcome instrument
• Has been used to measure activity and social participation limitations in patients
with Guillain–Barré syndrome, CIDP, and gammopathy-related polyneuropathy1
• No limitations: 48
Patients with hATTR amyloidosis reported difficulty performing
everyday activities2 including:
Washing
dishes
Fastening
buttons
Turning key
in a lock
Moving a
chair
Walking
~0.5 miles
CIPD, chronic inflammatory demyelinating polyradiculoneuropathy
1. Van Nes et al. Neurology 2011;76:337–45; 2. Patient voice survey for patients with ATTR amyloidosis, presented at
ATTR/Familial Amyloidosis Support Meeting, 2015 Supported by the Amyloidosis Foundation and Amyloidosis Support Groups
35
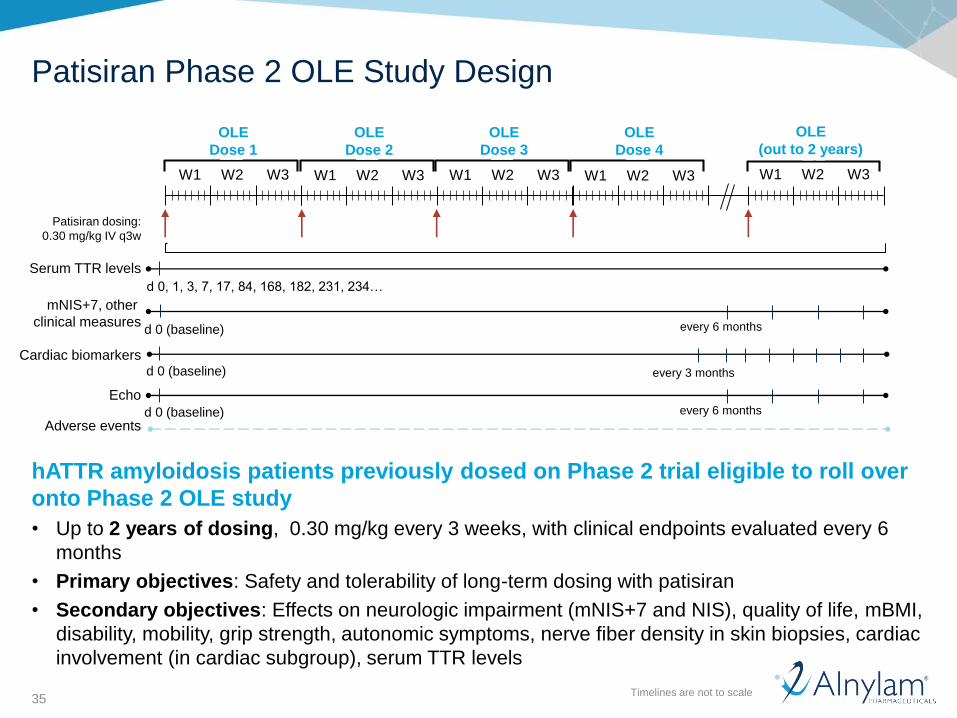
Patisiran Phase 2 OLE Study Design
Timelines are not to scale
hATTR amyloidosis patients previously dosed on Phase 2 trial eligible to roll over
onto Phase 2 OLE study
• Up to 2 years of dosing, 0.30 mg/kg every 3 weeks, with clinical endpoints evaluated every 6
months
• Primary objectives: Safety and tolerability of long-term dosing with patisiran
• Secondary objectives: Effects on neurologic impairment (mNIS+7 and NIS), quality of life, mBMI,
disability, mobility, grip strength, autonomic symptoms, nerve fiber density in skin biopsies, cardiac
involvement (in cardiac subgroup), serum TTR levels
W1 W2 W3
Adverse events
Serum TTR levels
mNIS+7, other
clinical measures
W1 W2 W3 W1 W2 W3
every 6 months
Cardiac biomarkers
d 0, 1, 3, 7, 17, 84, 168, 182, 231, 234…
0
0
0
0
W1 W2 W3 W1 W2 W3
Echo
d 0 (baseline)
d 0 (baseline)
d 0 (baseline)
every 3 months
every 6 months
OLE
Dose 1
OLE
Dose 2
OLE
Dose 3
OLE
Dose 4
OLE
(out to 2 years)
Patisiran dosing:
0.30 mg/kg IV q3w
36
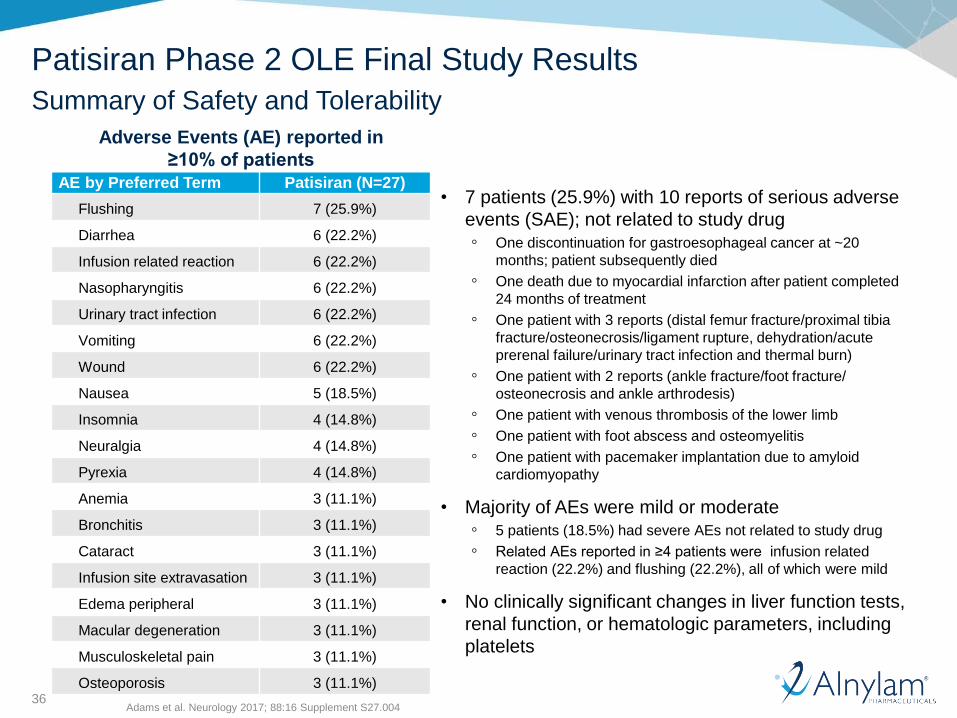
• 7 patients (25.9%) with 10 reports of serious adverse
events (SAE); not related to study drug
◦ One discontinuation for gastroesophageal cancer at ~20
months; patient subsequently died
◦ One death due to myocardial infarction after patient completed
24 months of treatment
◦ One patient with 3 reports (distal femur fracture/proximal tibia
fracture/osteonecrosis/ligament rupture, dehydration/acute
prerenal failure/urinary tract infection and thermal burn)
◦ One patient with 2 reports (ankle fracture/foot fracture/
osteonecrosis and ankle arthrodesis)
◦ One patient with venous thrombosis of the lower limb
◦ One patient with foot abscess and osteomyelitis
◦ One patient with pacemaker implantation due to amyloid
cardiomyopathy
• Majority of AEs were mild or moderate
◦ 5 patients (18.5%) had severe AEs not related to study drug
◦ Related AEs reported in ≥4 patients were infusion related
reaction (22.2%) and flushing (22.2%), all of which were mild
• No clinically significant changes in liver function tests,
renal function, or hematologic parameters, including
platelets
Adverse Events (AE) reported in
≥10% of patients
AE by Preferred Term Patisiran (N=27)
Flushing 7 (25.9%)
Diarrhea 6 (22.2%)
Infusion related reaction 6 (22.2%)
Nasopharyngitis 6 (22.2%)
Urinary tract infection 6 (22.2%)
Vomiting 6 (22.2%)
Wound 6 (22.2%)
Nausea 5 (18.5%)
Insomnia 4 (14.8%)
Neuralgia 4 (14.8%)
Pyrexia 4 (14.8%)
Anemia 3 (11.1%)
Bronchitis 3 (11.1%)
Cataract 3 (11.1%)
Infusion site extravasation 3 (11.1%)
Edema peripheral 3 (11.1%)
Macular degeneration 3 (11.1%)
Musculoskeletal pain 3 (11.1%)
Osteoporosis 3 (11.1%)
Patisiran Phase 2 OLE Final Study Results
Summary of Safety and Tolerability
Adams et al. Neurology 2017; 88:16 Supplement S27.004
37
Δm
NIS
+7
fro
m b
as
eli
ne
to
Mo
nth
24
-35
-30
-25
-20
-15
-10
-5
0
5
10
15
20
25
30
Me
an
(S
EM
) Δ
mN
IS+
7 f
rom
ba
se
lin
e a
t 2
4 m
os
~
-35
-30
-25
-20
-15
-10
-5
0
5
10
15
Natu
ral H
isto
ry
(no
nli
ne
ar;
N=
28
3)#
Diflunisal
Ph 3 Study+
//
Pla
ce
bo
(N=
66
)
Dif
lun
isa
l
(N=
64
)
//
Mean ΔmNIS+7 Across
hATTR Amyloidosis Studies
at 24 mos~
25.8
(9.4)
29.6
(3.1)
9.2
(2.7)
-7.0
(2.0)
20
25
30
Patisiran
Ph 2 OLE^
(N=26)
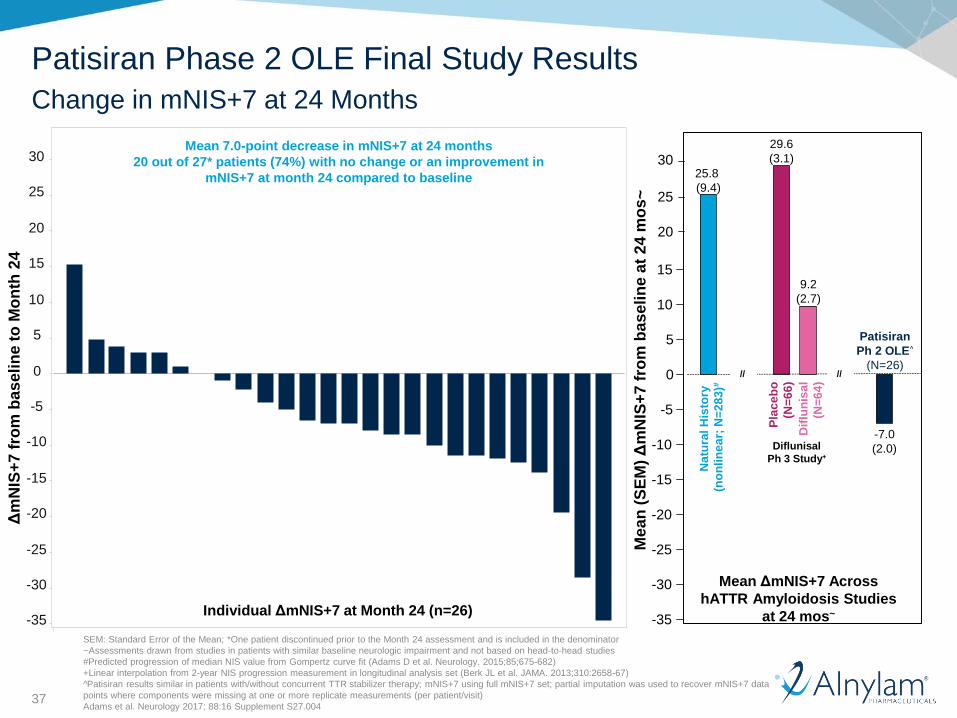
Mean 7.0-point decrease in mNIS+7 at 24 months
20 out of 27* patients (74%) with no change or an improvement in
mNIS+7 at month 24 compared to baseline
SEM: Standard Error of the Mean; *One patient discontinued prior to the Month 24 assessment and is included in the denominator
~Assessments drawn from studies in patients with similar baseline neurologic impairment and not based on head-to-head studies
#Predicted progression of median NIS value from Gompertz curve fit (Adams D et al. Neurology. 2015;85;675-682)
+Linear interpolation from 2-year NIS progression measurement in longitudinal analysis set (Berk JL et al. JAMA. 2013;310:2658-67)
^Patisiran results similar in patients with/without concurrent TTR stabilizer therapy; mNIS+7 using full mNIS+7 set; partial imputation was used to recover mNIS+7 data
points where components were missing at one or more replicate measurements (per patient/visit)
Adams et al. Neurology 2017; 88:16 Supplement S27.004
Individual ΔmNIS+7 at Month 24 (n=26)
Patisiran Phase 2 OLE Final Study Results
Change in mNIS+7 at 24 Months
38
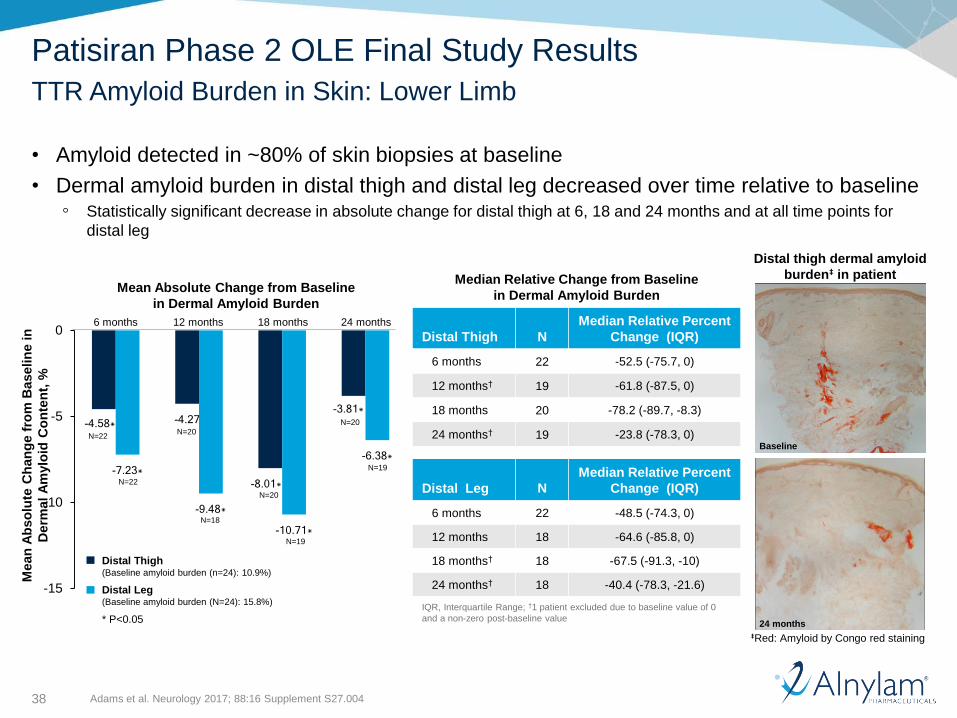
Median Relative Change from Baseline
in Dermal Amyloid Burden
Distal Thigh N
Median Relative Percent
Change (IQR)
6 months 22 -52.5 (-75.7, 0)
12 months† 19 -61.8 (-87.5, 0)
18 months 20 -78.2 (-89.7, -8.3)
24 months† 19 -23.8 (-78.3, 0)
Distal Leg N
Median Relative Percent
Change (IQR)
6 months 22 -48.5 (-74.3, 0)
12 months 18 -64.6 (-85.8, 0)
18 months† 18 -67.5 (-91.3, -10)
24 months† 18 -40.4 (-78.3, -21.6)
IQR, Interquartile Range; †1 patient excluded due to baseline value of 0
and a non-zero post-baseline value
Baseline
24 months
Distal thigh dermal amyloid
burden‡ in patient
‡Red: Amyloid by Congo red staining
-4.58* -4.27
-8.01*
-3.81*
-7.23*
-9.48*-10.71*
-6.38*
-15
-10
-5
0
Distal Thigh(Baseline amyloid burden (n=24): 10.9%)
Distal Leg(Baseline amyloid burden (N=24): 15.8%)
* P<0.05
Mean
Ab
so
lute
Ch
an
ge f
rom
Baselin
e in
Derm
al A
mylo
id C
on
ten
t, %
6 months 12 months 18 months 24 months
N=22
N=18
N=20
N=20
N=19
N=20
N=19
N=22
Mean Absolute Change from Baseline
in Dermal Amyloid Burden
Patisiran Phase 2 OLE Final Study Results
TTR Amyloid Burden in Skin: Lower Limb
• Amyloid detected in ~80% of skin biopsies at baseline
• Dermal amyloid burden in distal thigh and distal leg decreased over time relative to baseline◦ Statistically significant decrease in absolute change for distal thigh at 6, 18 and 24 months and at all time points for
distal leg
Adams et al. Neurology 2017; 88:16 Supplement S27.004
39
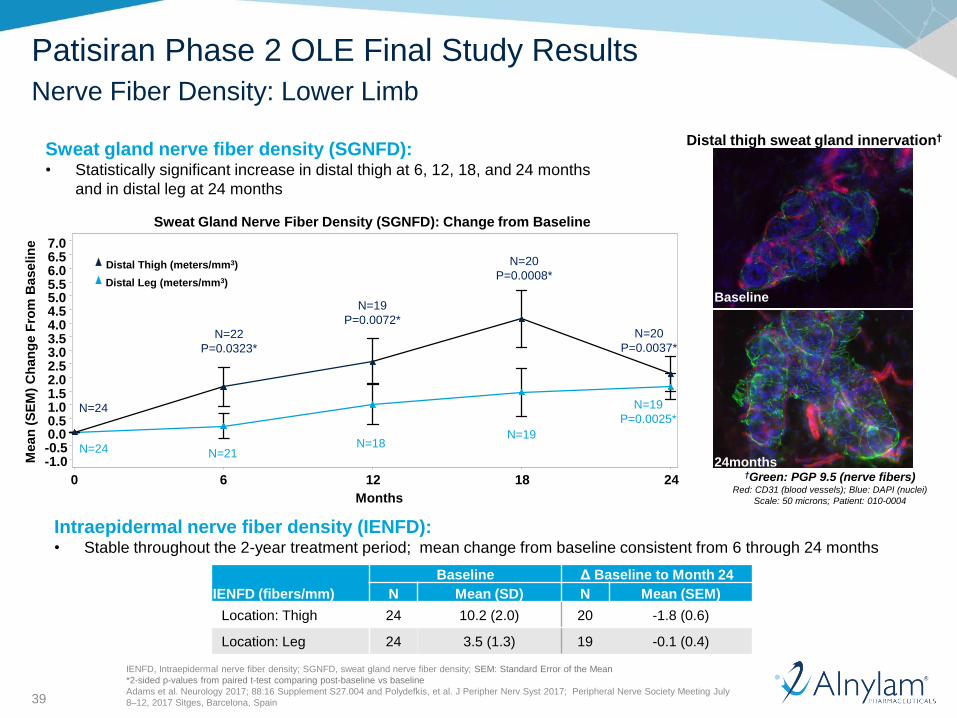
Sweat gland nerve fiber density (SGNFD): • Statistically significant increase in distal thigh at 6, 12, 18, and 24 months
and in distal leg at 24 months
Distal thigh sweat gland innervation†
†Green: PGP 9.5 (nerve fibers)Red: CD31 (blood vessels); Blue: DAPI (nuclei)
Scale: 50 microns; Patient: 010-0004
Baseline
24months
IENFD, Intraepidermal nerve fiber density; SGNFD, sweat gland nerve fiber density; SEM: Standard Error of the Mean
*2-sided p-values from paired t-test comparing post-baseline vs baseline
Adams et al. Neurology 2017; 88:16 Supplement S27.004 and Polydefkis, et al. J Peripher Nerv Syst 2017; Peripheral Nerve Society Meeting July
8–12, 2017 Sitges, Barcelona, Spain
Patisiran Phase 2 OLE Final Study Results
Nerve Fiber Density: Lower Limb
Mean
(S
EM
) C
han
ge F
rom
Baselin
e
-1.0-0.50.00.51.01.52.02.53.03.54.04.55.05.56.06.57.0
Months
0 6 12 18 24
N=19
P=0.0072*
N=20
P=0.0008*
N=21N=18
N=19
N=24
N=24
N=22
P=0.0323*
N=20
P=0.0037*
N=19
P=0.0025*
Distal Leg (meters/mm3)
Distal Thigh (meters/mm3)
Sweat Gland Nerve Fiber Density (SGNFD): Change from Baseline
Intraepidermal nerve fiber density (IENFD):• Stable throughout the 2-year treatment period; mean change from baseline consistent from 6 through 24 months
IENFD (fibers/mm)
Baseline Δ Baseline to Month 24
N Mean (SD) N Mean (SEM)
Location: Thigh 24 10.2 (2.0) 20 -1.8 (0.6)
Location: Leg 24 3.5 (1.3) 19 -0.1 (0.4)
40
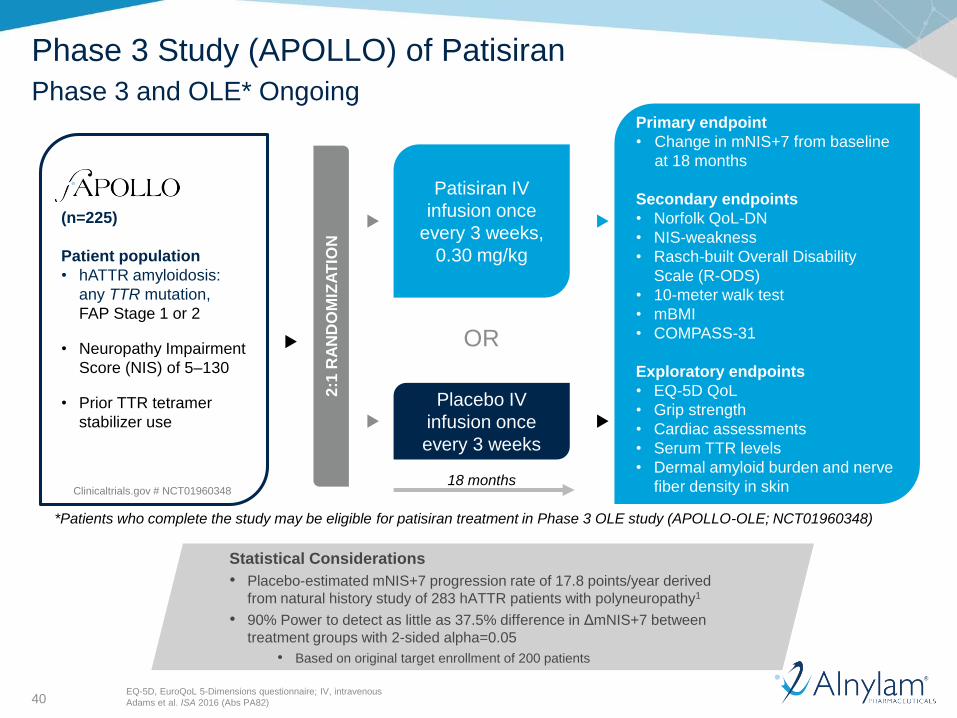
Phase 3 Study (APOLLO) of Patisiran
Phase 3 and OLE* Ongoing
(n=225)
Patient population
• hATTR amyloidosis:
any TTR mutation,
FAP Stage 1 or 2
• Neuropathy Impairment
Score (NIS) of 5–130
• Prior TTR tetramer
stabilizer use permitted
2:1
RA
ND
OM
IZA
TIO
N
Patisiran IV
infusion once
every 3 weeks,
0.30 mg/kg
Placebo IV
infusion once
every 3 weeks
Primary endpoint
• Change in mNIS+7 from baseline
at 18 months
Secondary endpoints
• Norfolk QoL-DN
• NIS-weakness
• Rasch-built Overall Disability
Scale (R-ODS)
• 10-meter walk test
• mBMI
• COMPASS-31
Exploratory endpoints
• EQ-5D QoL
• Grip strength
• Cardiac assessments
• Serum TTR levels
• Dermal amyloid burden and nerve
fiber density in skin
*Patients who complete the study may be eligible for patisiran treatment in Phase 3 OLE study (APOLLO-OLE; NCT01960348)
OR
18 monthsClinicaltrials.gov # NCT01960348
Statistical Considerations
• Placebo-estimated mNIS+7 progression rate of 17.8 points/year derived
from natural history study of 283 hATTR patients with polyneuropathy1
• 90% Power to detect as little as 37.5% difference in ΔmNIS+7 between
treatment groups with 2-sided alpha=0.05
• Based on original target enrollment of 200 patients
EQ-5D, EuroQoL 5-Dimensions questionnaire; IV, intravenous
Adams et al. ISA 2016 (Abs PA82)
41
Ionis Reported NEURO-TTR Phase 3 Topline Results
Statistically significant benefit observed for inotersen-treated patients as compared to placebo in both mNIS+7 and Norfolk QOL-DN endpoints at 15 months
• p<0.0001 and p=0.0006, respectively
• Statistically significant differences also observed for both endpoints at eight months
• Benefit in disease progression achieved regardless of TTR mutation and in both Stage 1 and Stage 2 patients
Key safety findings included thrombocytopenia and renal SAEs
• Three patients had SAEs of thrombocytopenia◦ Two patients recovered, and one patient died due to intracranial hemorrhage
◦ One additional patient discontinued inotersen treatment due to lower grade thrombocytopenia
• Four patients discontinued inotersen treatment due to renal observations◦ Two patients met a predefined renal stopping rule, and two experienced renal SAEs, one of whom
experienced chronic renal insufficiency
◦ One placebo-treated patient also met a predefined renal stopping rule
• Enhanced monitoring implemented during study to support management of these issues; Ionisanticipates that regulators will require safety monitoring in inotersen prescribing information if approved
• Treatment-emergent AEs considered related to treatment were seen more commonly with inotersen than placebo
• Detailed review of safety data ongoing
*Topline results from NEURO-TTR Phase 3 study of inotersen: http://ir.ionispharma.com/phoenix.zhtml?c=222170&p=irol-newsArticle&ID=2272828
42
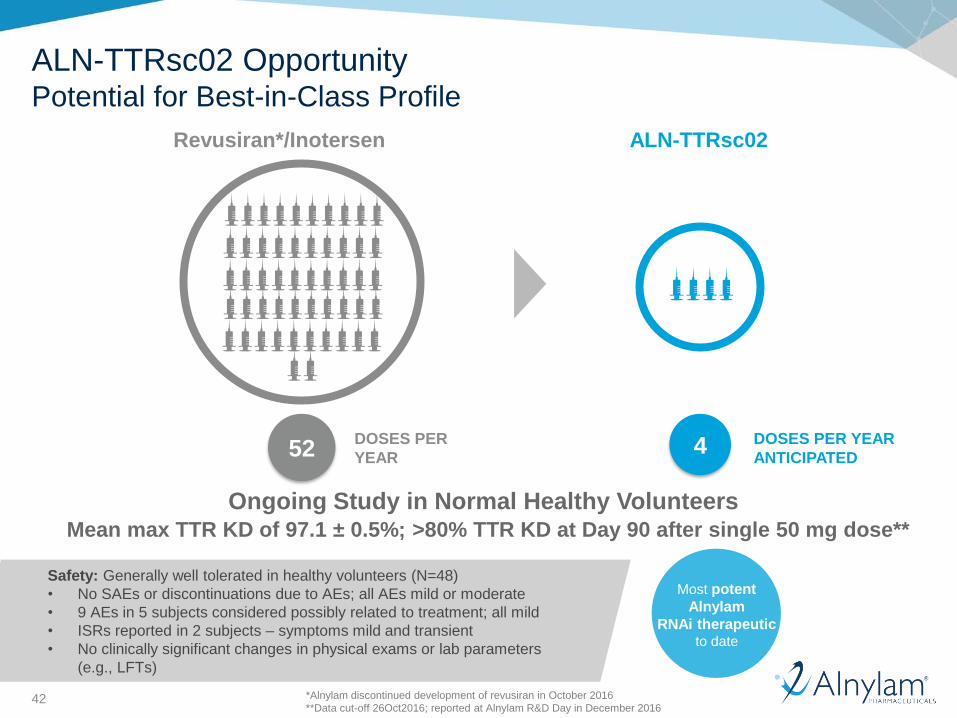
ALN-TTRsc02 OpportunityPotential for Best-in-Class Profile
Revusiran*/Inotersen ALN-TTRsc02
52DOSES PER
YEAR4 DOSES PER YEAR
ANTICIPATED
Ongoing Study in Normal Healthy VolunteersMean max TTR KD of 97.1 ± 0.5%; >80% TTR KD at Day 90 after single 50 mg dose**
Safety: Generally well tolerated in healthy volunteers (N=48)
• No SAEs or discontinuations due to AEs; all AEs mild or moderate
• 9 AEs in 5 subjects considered possibly related to treatment; all mild
• ISRs reported in 2 subjects – symptoms mild and transient
• No clinically significant changes in physical exams or lab parameters
(e.g., LFTs)
Most potent
Alnylam
RNAi therapeuticto date
*Alnylam discontinued development of revusiran in October 2016
**Data cut-off 26Oct2016; reported at Alnylam R&D Day in December 2016
43
Me
an
[+
/- S
EM
] T
TR
Re
lative
to
Ba
se
line
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Days since first dose
0 40 80 120 160 200 240 280 320
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Cohort Placebo (N=20) TTRSC02 (5mg) (N=6)TTRSC02 (25mg) (N=6) TTRSC02 (Optional; 25mg) (N=6)TTRSC02 (Subjects of Japanese descent; 25mg) (N=6) TTRSC02 (50mg) (N=6)TTRSC02 (Optional; 50mg) (N=6) TTRSC02 (Subjects of Japanese descent; 50mg) (N=6)TTRSC02 (100mg) (N=6) TTRSC02 (200mg) (N=6)TTRSC02 (300mg) (N=6)
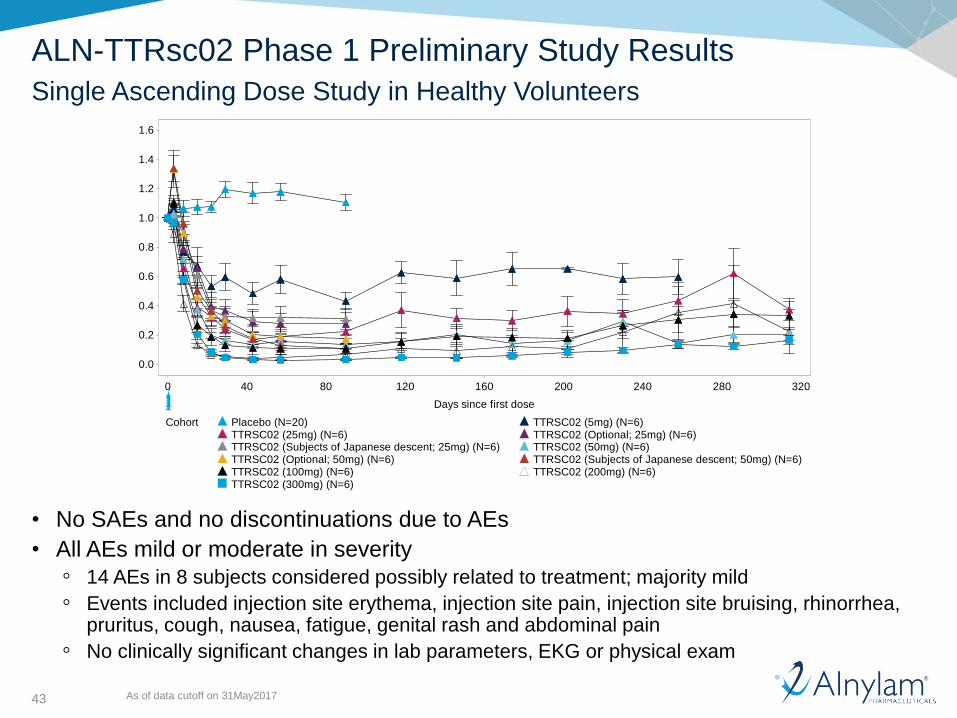
ALN-TTRsc02 Phase 1 Preliminary Study Results
Single Ascending Dose Study in Healthy Volunteers
• No SAEs and no discontinuations due to AEs
• All AEs mild or moderate in severity
◦ 14 AEs in 8 subjects considered possibly related to treatment; majority mild
◦ Events included injection site erythema, injection site pain, injection site bruising, rhinorrhea, pruritus, cough, nausea, fatigue, genital rash and abdominal pain
◦ No clinically significant changes in lab parameters, EKG or physical exam
As of data cutoff on 31May2017
44
Summary
• hATTR amyloidosis is a multisystemic disease with multiple different clinical manifestations of polyneuropathy, often accompanied by cardiac involvement, which could lead to progressive disability, diminished quality of life, and death
• Composite neuropathy impairment scores such as mNIS+7, along with additional clinical and biomarker endpoints, have the potential to demonstrate the clinical benefit of novel therapeutics in this disease
• The patisiran Phase 2 OLE study results suggest that TTR lowering has the potential to have a disease-modifying effect on the polyneuropathy in hATTR amyloidosis, as shown by the effects on mNIS+7, dermal amyloid burden, and sweat gland nerve fiber density
• The emerging results of randomized Phase 3 trials with patisiran and inotersen will further elucidate the utility of these and other endpoints in assessing the magnitude and clinical meaningfulness of the response to treatment
• ALN-TTRsc02 offers the potential of a best-in-class profile of quarterly, low-volume dosing with clamped knockdown of TTR
45
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
46
Key Targeted Milestones for Patisiran
APOLLO Data – Mid-’17
NDA / MAA Filed – Late’17
US / EU Launch – 2018
47
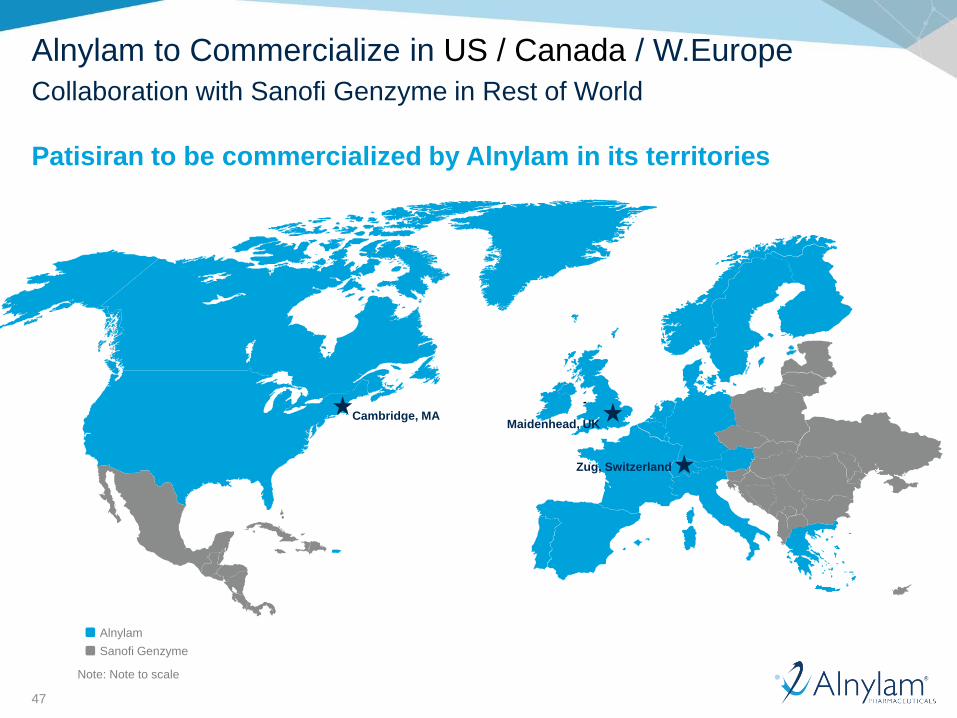
Alnylam to Commercialize in US / Canada / W.Europe
Collaboration with Sanofi Genzyme in Rest of World
Patisiran to be commercialized by Alnylam in its territories
Sanofi Genzyme
Alnylam
Note: Note to scale
Cambridge, MAMaidenhead, UK
Zug, Switzerland
48
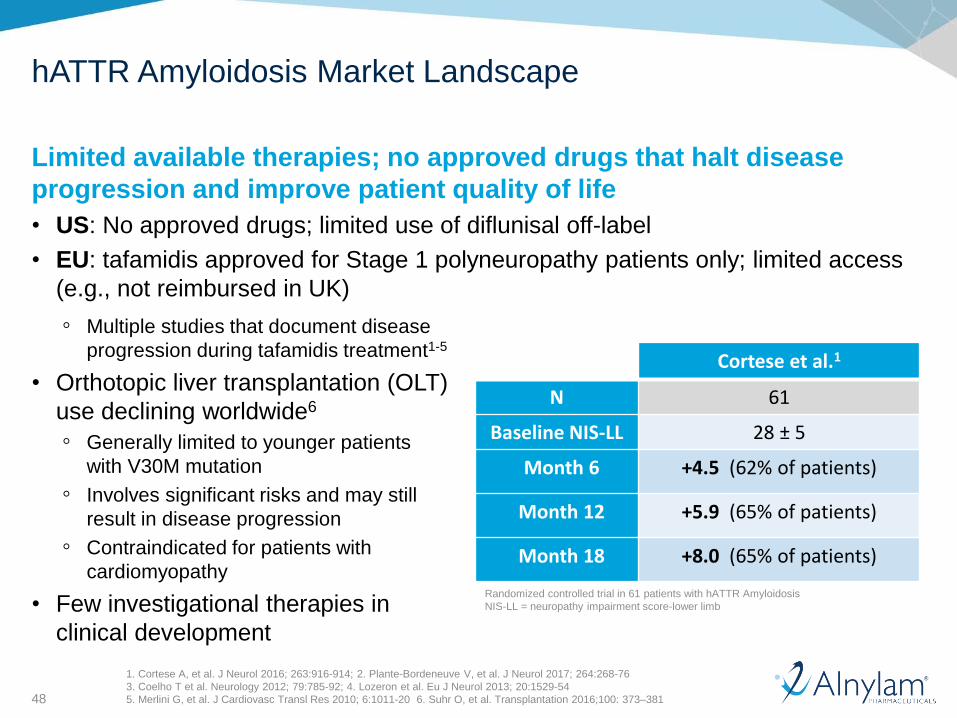
hATTR Amyloidosis Market Landscape
Limited available therapies; no approved drugs that halt disease
progression and improve patient quality of life
• US: No approved drugs; limited use of diflunisal off-label
• EU: tafamidis approved for Stage 1 polyneuropathy patients only; limited access
(e.g., not reimbursed in UK)
Cortese et al.1
N 61
Baseline NIS-LL 28 ± 5
Month 6 +4.5 (62% of patients)
Month 12 +5.9 (65% of patients)
Month 18 +8.0 (65% of patients)
Randomized controlled trial in 61 patients with hATTR Amyloidosis
NIS-LL = neuropathy impairment score-lower limb
◦ Multiple studies that document disease
progression during tafamidis treatment1-5
• Orthotopic liver transplantation (OLT)
use declining worldwide6
◦ Generally limited to younger patients
with V30M mutation
◦ Involves significant risks and may still
result in disease progression
◦ Contraindicated for patients with
cardiomyopathy
• Few investigational therapies in
clinical development
1. Cortese A, et al. J Neurol 2016; 263:916-914; 2. Plante-Bordeneuve V, et al. J Neurol 2017; 264:268-76
3. Coelho T et al. Neurology 2012; 79:785-92; 4. Lozeron et al. Eu J Neurol 2013; 20:1529-54
5. Merlini G, et al. J Cardiovasc Transl Res 2010; 6:1011-20 6. Suhr O, et al. Transplantation 2016;100: 373–381

49
hATTRAmyloidosis
Predominantly Neurologic Predominantly Cardiac
V30MEarly onset
F33L S50R A36P E89Q I107V H88R L111M V122I
S77Y E89L G47A F64LV30M
Late onset W41L T60A I68L
hATTR Amyloidosis Market Opportunity
Patisiran has potential to address unmet medical needs
• Evidence for potential halting or improvement of neuropathy in Phase 2 OLE study
• APOLLO Phase 3 study will evaluate mNIS+7 and multiple secondary endpoints
~50,000 patients WW
• ~10,000 with predominant
polyneuropathy plus
~20%-30% of remainder
with mixed phenotype
• Some mutations endemic
to certain regions
1. Hawkins PN, et al. Ann Med. 2015;47 (8 ):625 ‐ 638; 2. Ando Y, et al. Orphanet J Rare Dis. 2013;8:31;
3. Rapezzi C, et al. Eur Heart J. 2013;34 (7 ):520 ‐ 528; 4. Adams D, et al. The XVth International Symposium on
Amyloidosis. Uppsala, Sweden: ISA International Society of Amyloidosis; July 3 ‐ 7, 2016. PA 82; 5. Coelho T, et al.. Curr
Med Res Opin. 2013;29:63 ‐ 76
• Often misdiagnosed due to heterogeneity of disease
◦ Variable age of onset, disease penetrance, symptoms at presentation, and comorbidities
◦ Efforts underway to improve diagnosis rates and enable earlier intervention
Based on Rapezzi et al. Eur Heart J 2013;34:520–8; Semigran et al. J Am Coll Cardiol 2016;68:173–75
50
Succeeding in Rare Disease Requires a Specific Road Map
Engagement
and Advocacy
Educate
Access
Retain
Support and
Solutions
Best or First-in-Class
Product Profiles
RNAiTherapeutics
SuccessDiagnose

51
Digital Educational Initiatives
Recently launched two websites for disease education
https://hATTRamyloidosis.com/ https://hATTRbridge.com/
Health care professionals Patients and their families
52
Scientific Leadership and Education
• >20 primary abstracts and publications since 2013• Including manuscripts in New England Journal of Medicine, Neurology
and Orphanet Journal of Rare Diseases
• Attendance at >55 international, regional and
local congresses and ~4,000 peer
engagements
• Symposia and facilitation of dialogue among
specialists to increase awareness of disease
burden
53
Alnylam ActTM
No-charge third-party genetic testing and counseling program*
Individuals with a suspected diagnosis or a confirmed family history of
hATTR amyloidosis are eligible to take part in the
Genetic Screening performed by CLIA-certified
clinical diagnostic laboratory
• Three testing options now available via saliva or blood
◦ Neuropathy Panel
◦ Cardiomyopathy Panel
◦ Single TTR Gene Testing
Genetic counseling offered by a genetics services provider
• Counseling available before, during or after genetic testing
Exploring a supported diagnostic program in the EU
*Available in the United States Only
**Since program inception and as of July 22, 2017.
CLIA - Clinical Laboratory Improvement Amendments
At no time does Alnylam receive patient-identifiable information.
More information regarding
this program available at:
www.alnylamact.com
~2,000Tests
Submitted**
>300Accounts**
54
Patient Advocacy
Mutual goals of increasing awareness, enabling earlier diagnosis,
advancing the development of potential new therapies, and designing
initiatives that support the unique needs of patient communities
France Germany
Italy
United States
Spain
Sweden
Netherlands
Canada
2017 activities:
• Patient education: three educational webinars supported
• Initiatives that support the unique needs of patient communities: three Care Days hosted, in conjunction ThinkGenetic, across the US
• Advancing the development of potential new therapies:>25 Advocacy Support Meetings attended
• Collaboration with and support of a variety of patient support groups
55
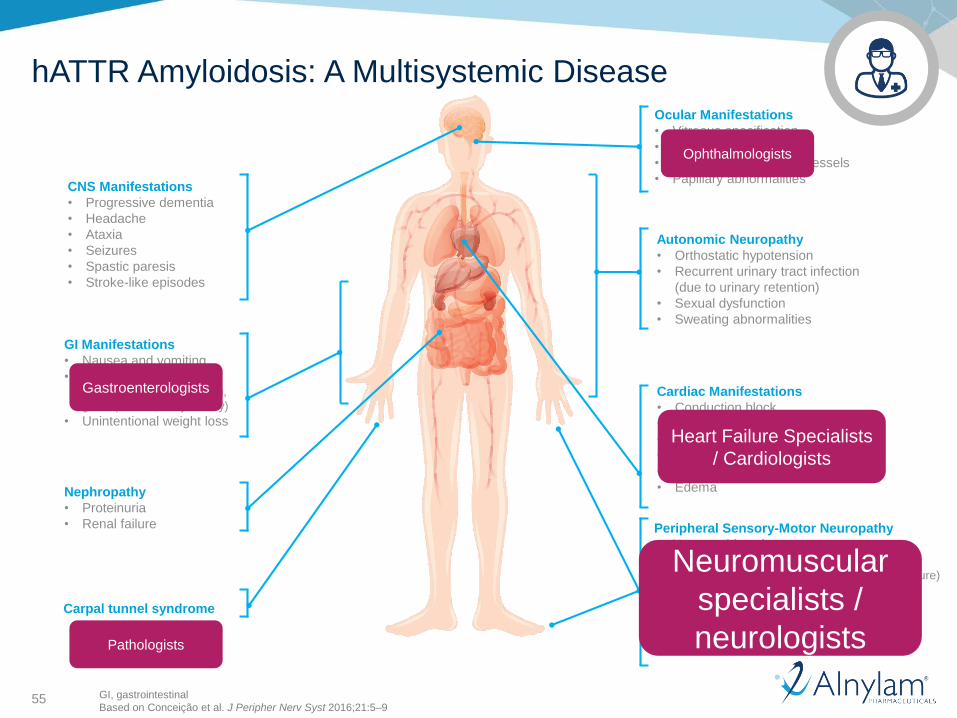
CNS Manifestations
• Progressive dementia
• Headache
• Ataxia
• Seizures
• Spastic paresis
• Stroke-like episodes
GI Manifestations
• Nausea and vomiting
• Changes in GI motility (i.e., diarrhea, constipation,
gastroparesis, early satiety)
• Unintentional weight loss
Autonomic Neuropathy
• Orthostatic hypotension
• Recurrent urinary tract infection
(due to urinary retention)
• Sexual dysfunction
• Sweating abnormalities
Peripheral Sensory-Motor Neuropathy
• Neuropathic pain
• Altered sensation (i.e., change in sensitivity to pain and temperature)
• Numbness and tingling
• Muscle weakness
• Impaired weakness
• Difficulty walking
Carpal tunnel syndrome
Ocular Manifestations
• Vitreous opacification
• Glaucoma
• Abnormal conjunctival vessels
• Papillary abnormalities
Nephropathy
• Proteinuria
• Renal failure
Cardiac Manifestations
• Conduction block
• Cardiomyopathy
• Palpitations and arrhythmia
• Mild regurgitation
• Shortness of breath
• Edema
GI, gastrointestinal
Based on Conceição et al. J Peripher Nerv Syst 2016;21:5–9
hATTR Amyloidosis: A Multisystemic Disease
Gastroenterologists
Pathologists
Neuromuscular
specialists /
neurologists
Heart Failure Specialists
/ Cardiologists
Ophthalmologists

56
US Go-to-Market Strategy
US Expected to be Alnylam’s First Launch
Patisiran expected to enter a competitive US market in a disease state
with significant unmet need and low physician and patient awareness
Our stakeholder-facing teams will interact with a wide variety of
external stakeholders:
• Health Care Professionals and Office Staff
• Patients and Caregivers
• Advocacy Organizations
• Payers
Patisiran will be supported by a number of stakeholder-facing roles
with an overall footprint similar to current orphan disease products
• High coordination across the field-based teams and HQ-based Patient Services
57
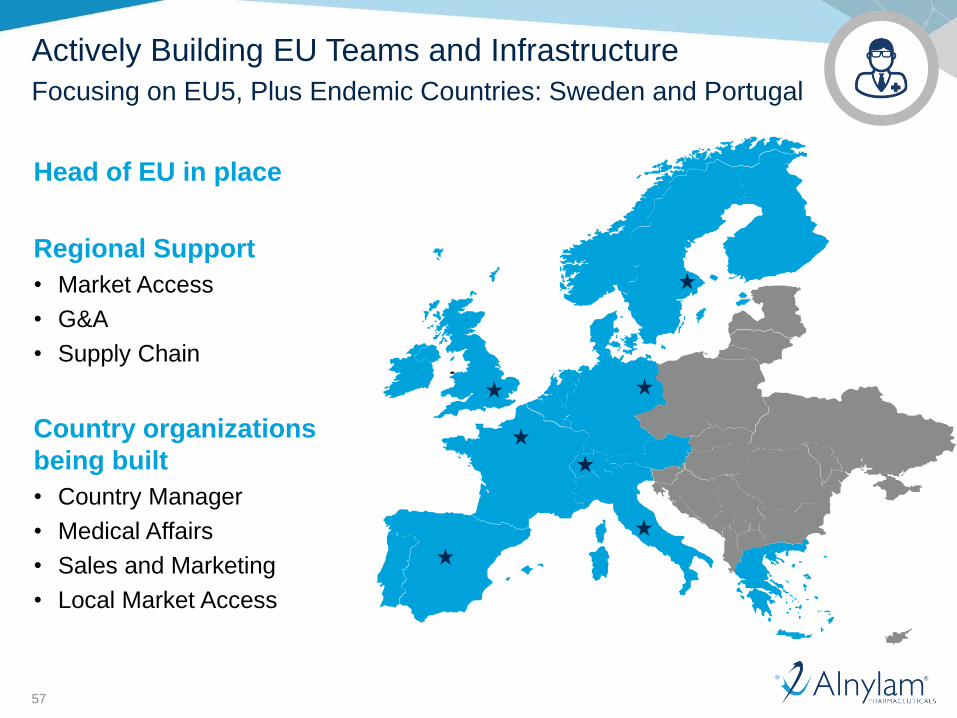
Actively Building EU Teams and Infrastructure
Focusing on EU5, Plus Endemic Countries: Sweden and Portugal
Head of EU in place
Regional Support
• Market Access
• G&A
• Supply Chain
Country organizations
being built
• Country Manager
• Medical Affairs
• Sales and Marketing
• Local Market Access
58
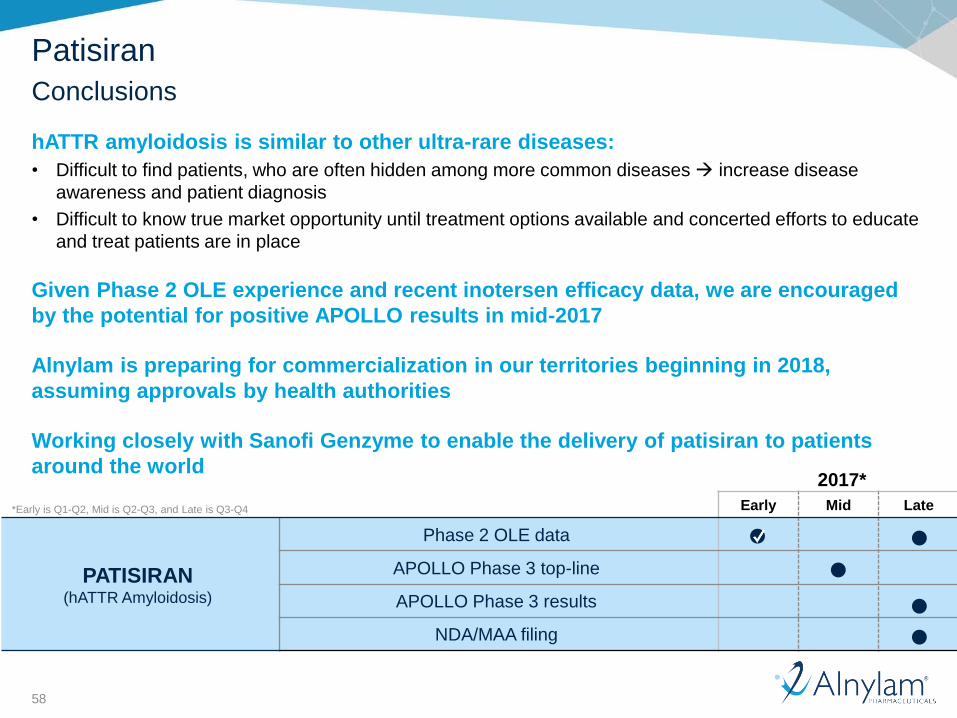
2017*
Early Mid Late
PATISIRAN (hATTR Amyloidosis)
Phase 2 OLE data
APOLLO Phase 3 top-line
APOLLO Phase 3 results
NDA/MAA filing
Patisiran
Conclusions
hATTR amyloidosis is similar to other ultra-rare diseases:
• Difficult to find patients, who are often hidden among more common diseases increase disease
awareness and patient diagnosis
• Difficult to know true market opportunity until treatment options available and concerted efforts to educate
and treat patients are in place
Given Phase 2 OLE experience and recent inotersen efficacy data, we are encouraged
by the potential for positive APOLLO results in mid-2017
Alnylam is preparing for commercialization in our territories beginning in 2018,
assuming approvals by health authorities
Working closely with Sanofi Genzyme to enable the delivery of patisiran to patients
around the world
*Early is Q1-Q2, Mid is Q2-Q3, and Late is Q3-Q4
59
Agenda
Welcome• Joshua Brodsky, Associate Director, Investor Relations and Corporate Communications
Introduction• Eric Green, Vice President, General Manager, TTR Program
Path to Diagnosis• Dr. Michael Polydefkis, M.D., Director, Cutaneous Nerve Lab, Professor of Neurology,
Johns Hopkins University School of Medicine
Overview of Disease and Patisiran Data• Jared Gollob, M.D., Vice President, Clinical Research
Commercial Opportunity and Preparation• Eric Green, Vice President, General Manager, TTR Program
Q&A Session
60
Upcoming RNAi Roundtables
Revusiran investigation results
• Wednesday, August 9, 12:30 pm ET
Platform advances in RNAi therapeutics
• Wednesday, August 23, 3:30 pm ET
Givosiran, in development for the treatment of acute hepatic porphyrias
• Thursday, September 7, 10:30 am ET
Fitusiran, in development for the treatment of hemophilia and rare
bleeding disorders
• Tuesday, September 12, 10:30 am ET
Additional details for upcoming RNAi Roundtables, including speakers, dates and times, will be
provided on the Capella section of the Company's website, www.alnylam.com/capella.

LeoLiving with hATTR Amyloidosis
Thank you